Embed Size (px)
Citation preview
The importance of lipid
management in ACS patients
BACPR October 2016
Shahid JunejoConsultant Cardiologist & Lead for PCI
City Hospitals Sunderland NHS Foundation trust
Associate Lecturer
Newcastle University Medical School
Sessional Tutor
University of Sunderland
Founder Chairperson
Integrated Vascular Centre, IVasC South of Tyne
This session has been sponsored by MSD
Prescribing and Adverse Event Reporting information can be found on the final slide
The views of the speaker are their own and do not represent the opinions of MSD
CARD-1197520-0000 Date of Preparation October 2016,
Declarations
Sponsorship for Scientific meetings, Research and Data
registry work
Advisory board participation
Sponsorship for Speaker meetings
Aims
Review CHD prevalence & presentations
Review recurrence risk after index event
Review treatment strategies
Review Guidelines / recommendations
Background..
CVD causes 4 million deaths in Europe (almost 50% of all
cause mortality)
CHD contributes to 1.8 million deaths (almost 20% of all
cause mortality)
In UK CVD costs £14.7bn (1.4% of GDP) - expected to
rise to £17.9bn in 2020
1. Centre for Economics and business research: http://www.cebr.com/reports/the-rising-cost-of-cvd/assuming £:Euro = 1.29 Date accessed 05/09/2016,
Kotseva K. E-Journal of Cardiology Practice.
Vol.14N24-27 Sep 2016
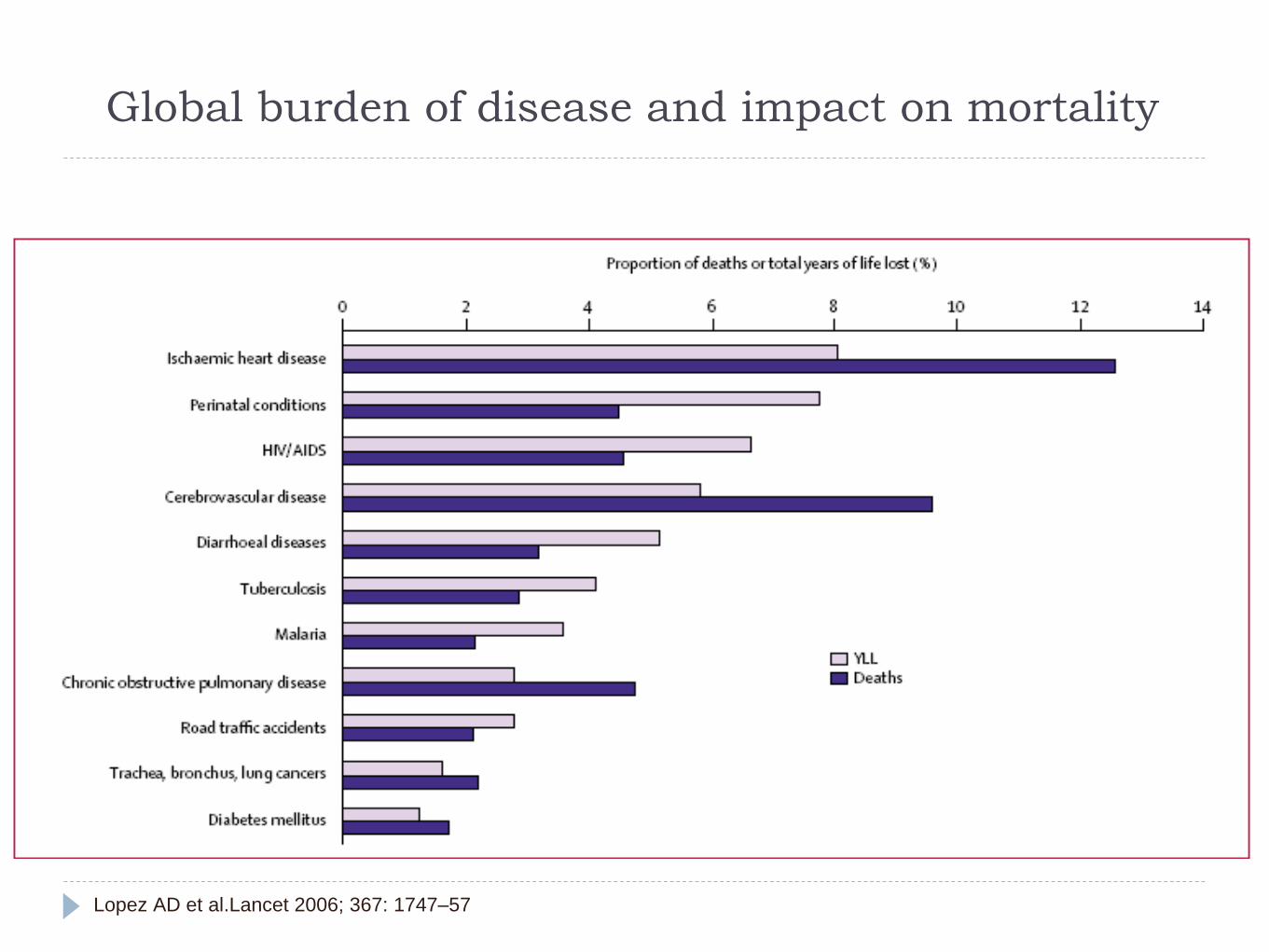
Global burden of disease and impact on mortality
Lopez AD et al.Lancet 2006; 367: 1747–57
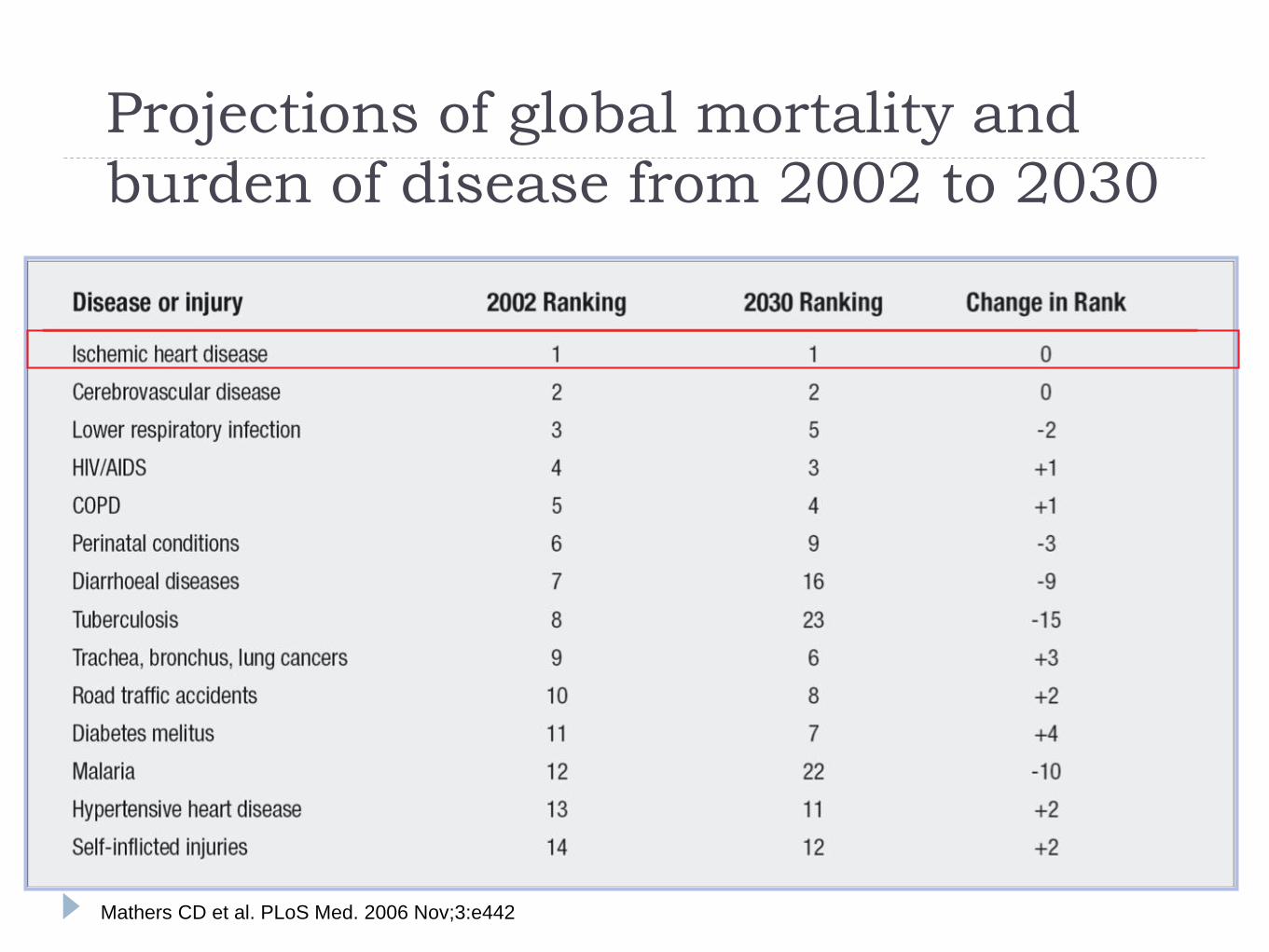
Projections of global mortality and
burden of disease from 2002 to 2030
Mathers CD et al. PLoS Med. 2006 Nov;3:e442
Disease presentation
New Angina - OP setting
UA / ACS (NSTeMI) or STeMI - de novo (Type 1)
UA / ACS (NSTeMI) or STeMI - secondary (Type 2)
CHD in the context of other cardiac presentation -Valve
disease, CCF, Arrhythmias etc
Other Vascular or Metabolic presentations - PVD, Stroke,
AAA, Diabetes, CKD
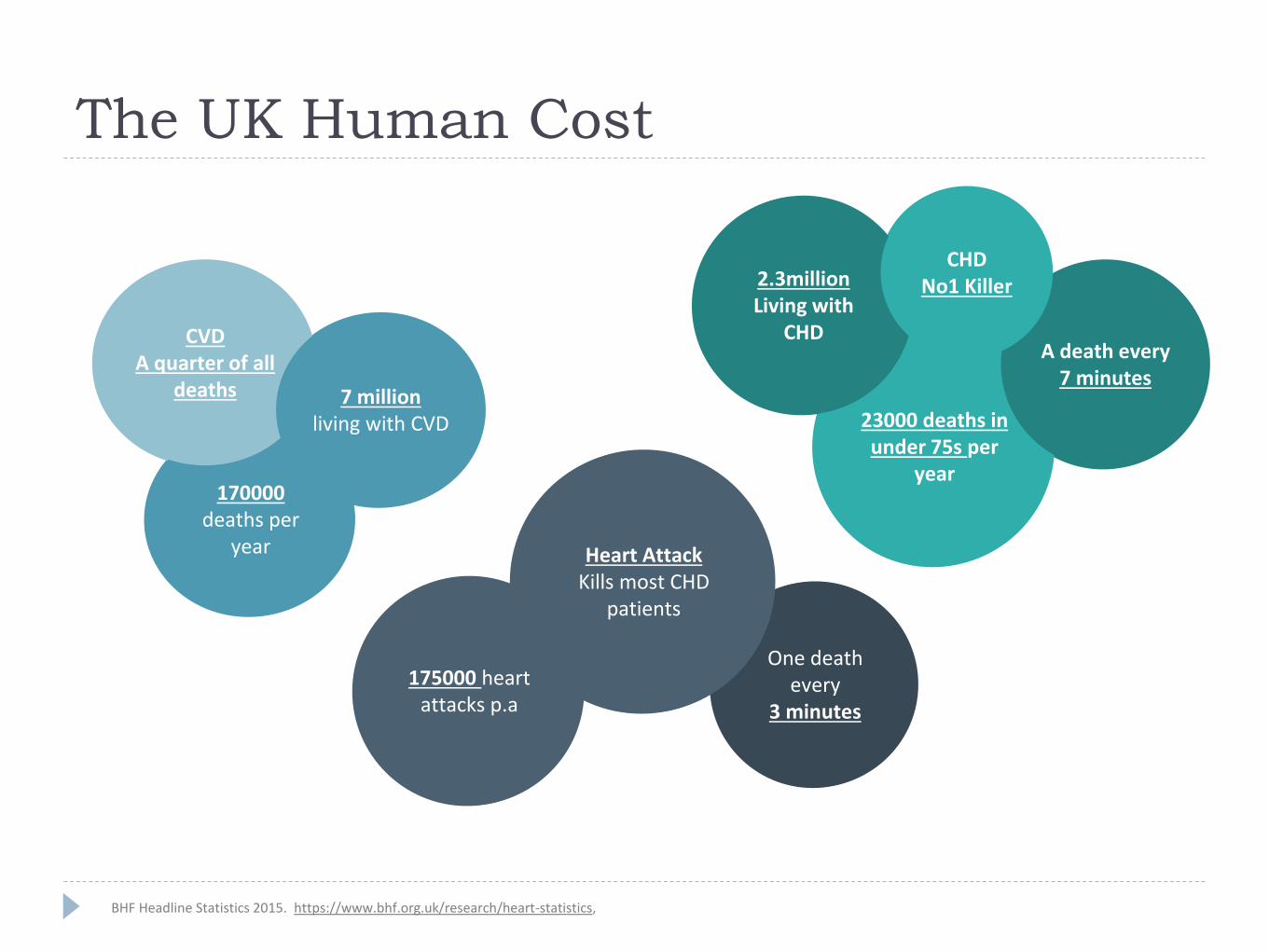
The UK Human Cost
170000deaths per
year
CVDA quarter of all
deaths 7 millionliving with CVD
175000 heart attacks p.a
One death every
3 minutes
Heart AttackKills most CHD
patients
23000 deaths in under 75s per
year
2.3millionLiving with
CHDA death every
7 minutes
CHDNo1 Killer
BHF Headline Statistics 2015. https://www.bhf.org.uk/research/heart-statistics,
170000deaths per
year
CVDA quarter of all
deaths 7 millionliving with CVD
175000 heart attacks p.a
One death every
3 minutes
Heart AttackKills most CHD
patients
23000 deaths in under 75s per
year
2.3millionLiving with
CHDA death every
7 minutes
CHDNo1 Killer
MINAP report 2013-14
80724 Heart attacks
31653 (39%) STeMI vs 49071 (61%) NSTeMI
PPCI & early PCI recommended respectively
MINAP report 2013-14
In STeMI presentation 27% (8010) did not get reperfusion
In NSTeMI presentation 34% (16802) did not get
diagnostic angiography (various reasons)
Risk profile at first presentation
33% patients on BP medications
30% on Lipid lowering treatments
20% women were Diabetic vs 18% of men
At discharge nearly 88% of eligible patients were on
secondary preventive medications [Antiplatelets, BB, Statins, ACE inhibitors]
against the NSF for CHD standard of 80% for 3
medications [Asp, BB, Statins])
MINAP 2013-14 Annual report
Residual risk …
Untreated disease (irrespective of reason not to treat)
Persistent or resistant risk factors (Smoking, BP, BMI, DM,
Lipids)
New or emergent risk (Stroke, CCF, Diabetes, CKD, age)
Novel risk factors - Heart Rate & cellular mechanism of
disease
EUROASPIRE IVCross-sectional survey 78 centres, 24 countries, patients 18-80 years
who have had CABG, PCI or ACS
16,426 medical records reviewed and 7998 patients interviewed
50% continue to smoke - younger patients more persistent smokers
60% do not perform moderate or vigorous activity
<33% reached 130/80 (only 40% met 140/90)
<66% had LDL-C <2.5 (20% had LDL-C <1.8)
33% had HbA1C 6.5%
BMI - unchanged or rising
EUROASPIRE IV : Kotseva K et al.
@ ESC 2015
European Journal of Preventive Cardiology
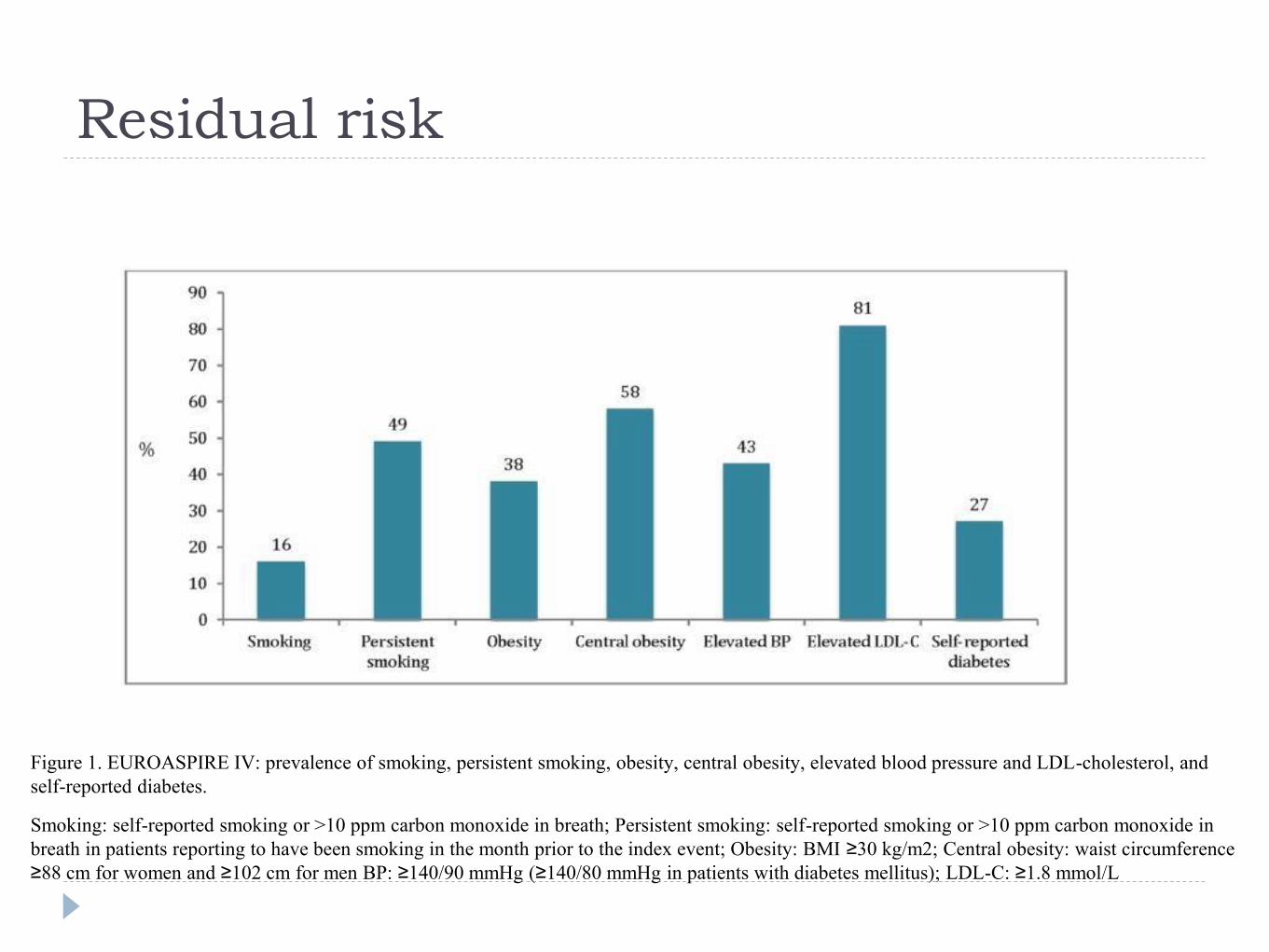
Residual risk
Figure 1. EUROASPIRE IV: prevalence of smoking, persistent smoking, obesity, central obesity, elevated blood pressure and LDL-cholesterol, and
self-reported diabetes.
Smoking: self-reported smoking or >10 ppm carbon monoxide in breath; Persistent smoking: self-reported smoking or >10 ppm carbon monoxide in
breath in patients reporting to have been smoking in the month prior to the index event; Obesity: BMI ≥30 kg/m2; Central obesity: waist circumference
≥88 cm for women and ≥102 cm for men BP: ≥140/90 mmHg (≥140/80 mmHg in patients with diabetes mellitus); LDL-C: ≥1.8 mmol/L
Impact of residual risk
High disease and symptom burden
High resource utilisation and costs
Poor quality of life

Patients most at risk..
ACS patients :13% readmission within 1 month after
initial presentation (*1) A UK audit of 158 UA/NSTeMI patients from an Acute Cardiac Unit.
After MI : 18% probability of nonfatal MI, nonfatal CVA,
or CV death in first 12 months after MI (2)
1. Alfakih et al. British J Cardiology 2009;16:132-134 2. Jernberg et al. Eur Heart J 2015;36(19):1163-1170
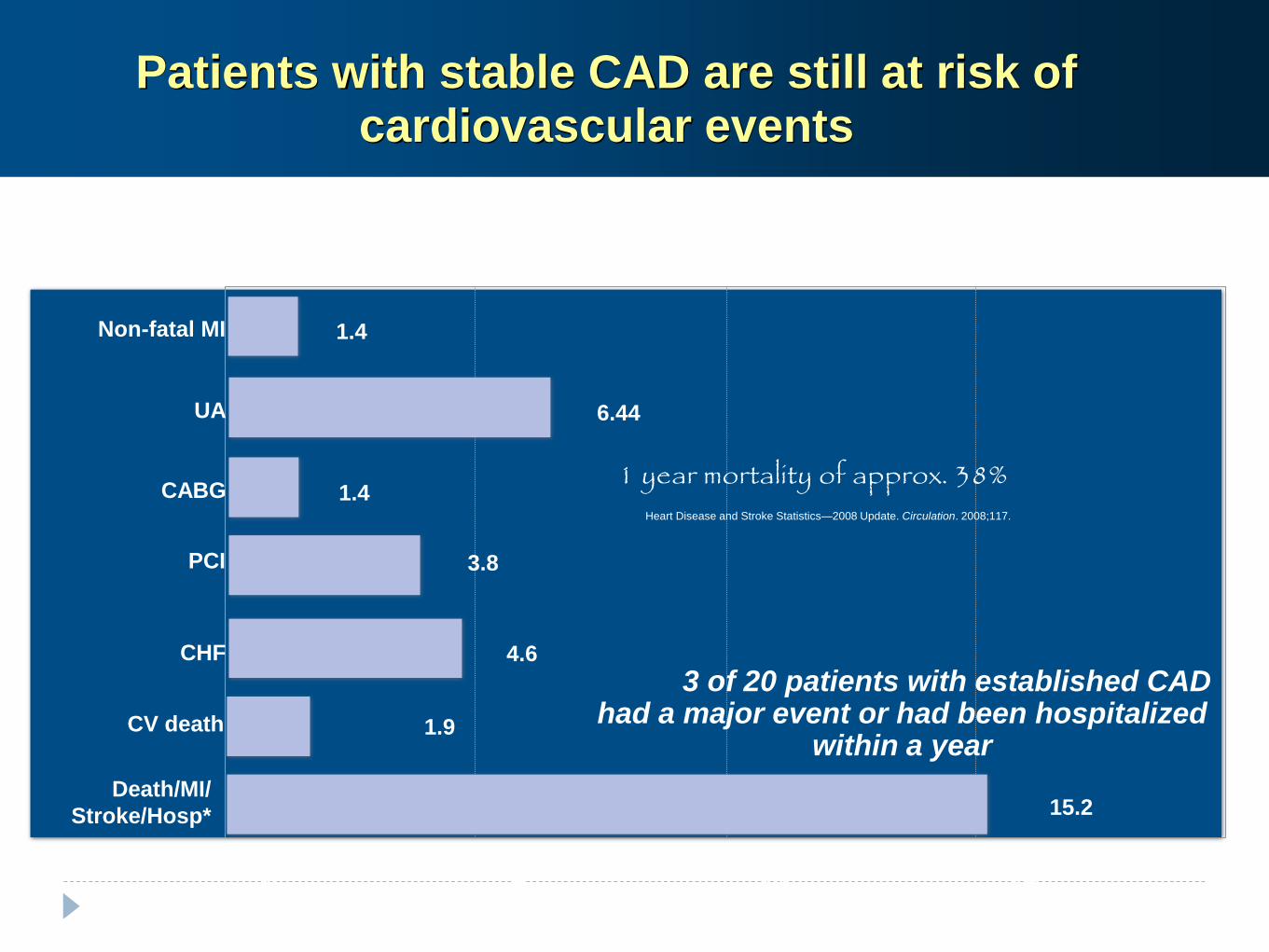
Patients with stable CAD are still at risk of cardiovascular events
Adapted from Steg PG et al. JAMA. 2007;297: 1197-1206.
1.9
3.8
4.6
0 5 10 15 20
CV death
PCI
6.44UA
1.4
1.4
Non-fatal MI
CABG
CHF
15.2Death/MI/
Stroke/Hosp*
Annual event rates adjusted for sex and age in stable CAD outpatients, REACH registry: CAD outpatients (n=38602), 1-year follow-up
3 of 20 patients with established CAD had a major event or had been hospitalized
within a year
1 year mortality of approx. 38%Heart Disease and Stroke Statistics—2008 Update. Circulation. 2008;117.
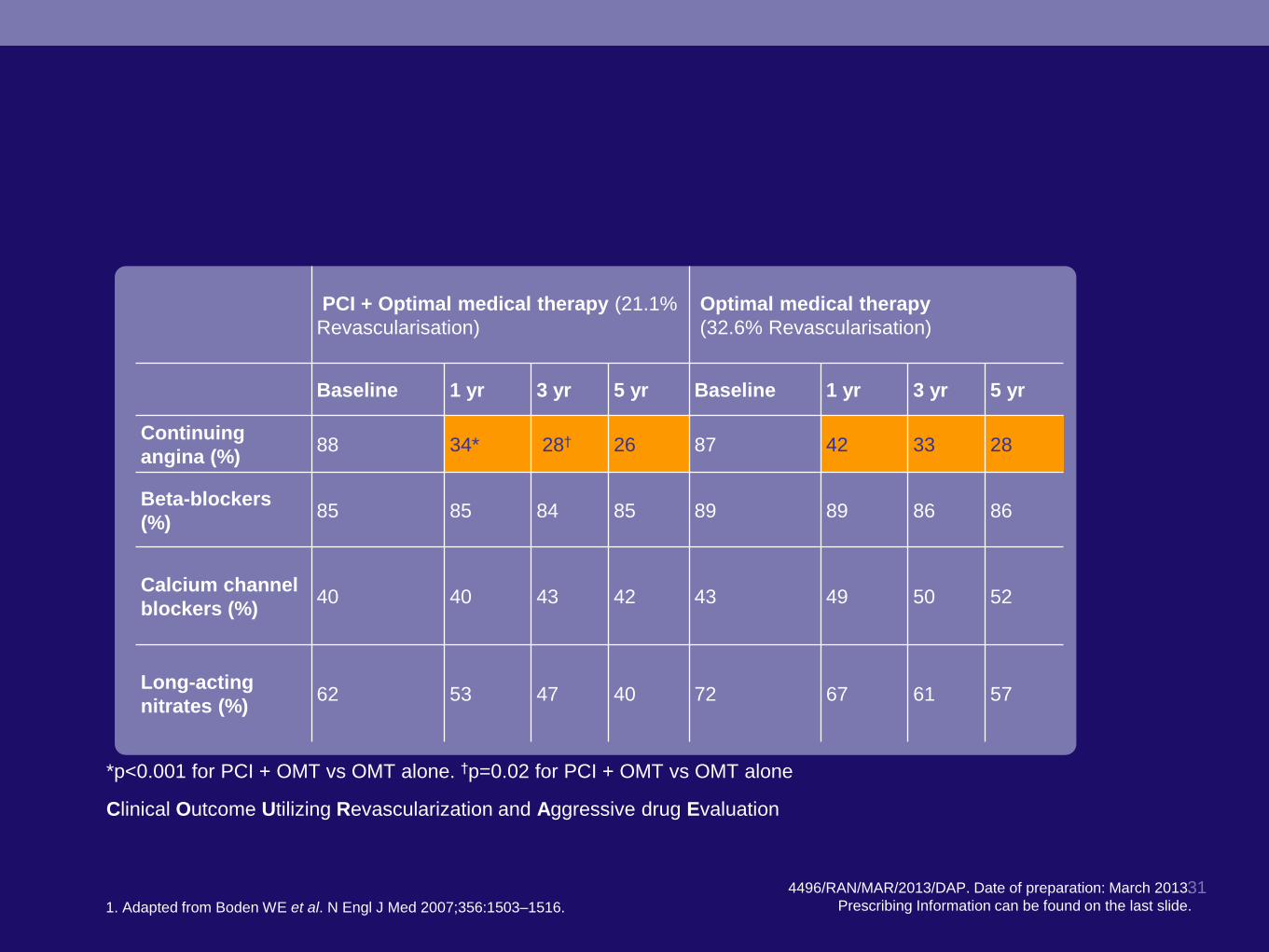
COURAGE1
Angina symptoms persist in many patients despite
receiving PCI and/or optimal medical therapy
194496/RAN/MAR/2013/DAP. Date of preparation: March 2013.
Prescribing Information can be found on the last slide.31
PCI + Optimal medical therapy (21.1%
Revascularisation)
Optimal medical therapy
(32.6% Revascularisation)
Baseline 1 yr 3 yr 5 yr Baseline 1 yr 3 yr 5 yr
Continuing
angina (%)88 34* 28† 26 87 42 33 28
Beta-blockers
(%)85 85 84 85 89 89 86 86
Calcium channel
blockers (%)40 40 43 42 43 49 50 52
Long-acting
nitrates (%)62 53 47 40 72 67 61 57
*p<0.001 for PCI + OMT vs OMT alone. †p=0.02 for PCI + OMT vs OMT alone
Clinical Outcome Utilizing Revascularization and Aggressive drug Evaluation
1. Adapted from Boden WE et al. N Engl J Med 2007;356:1503–1516.
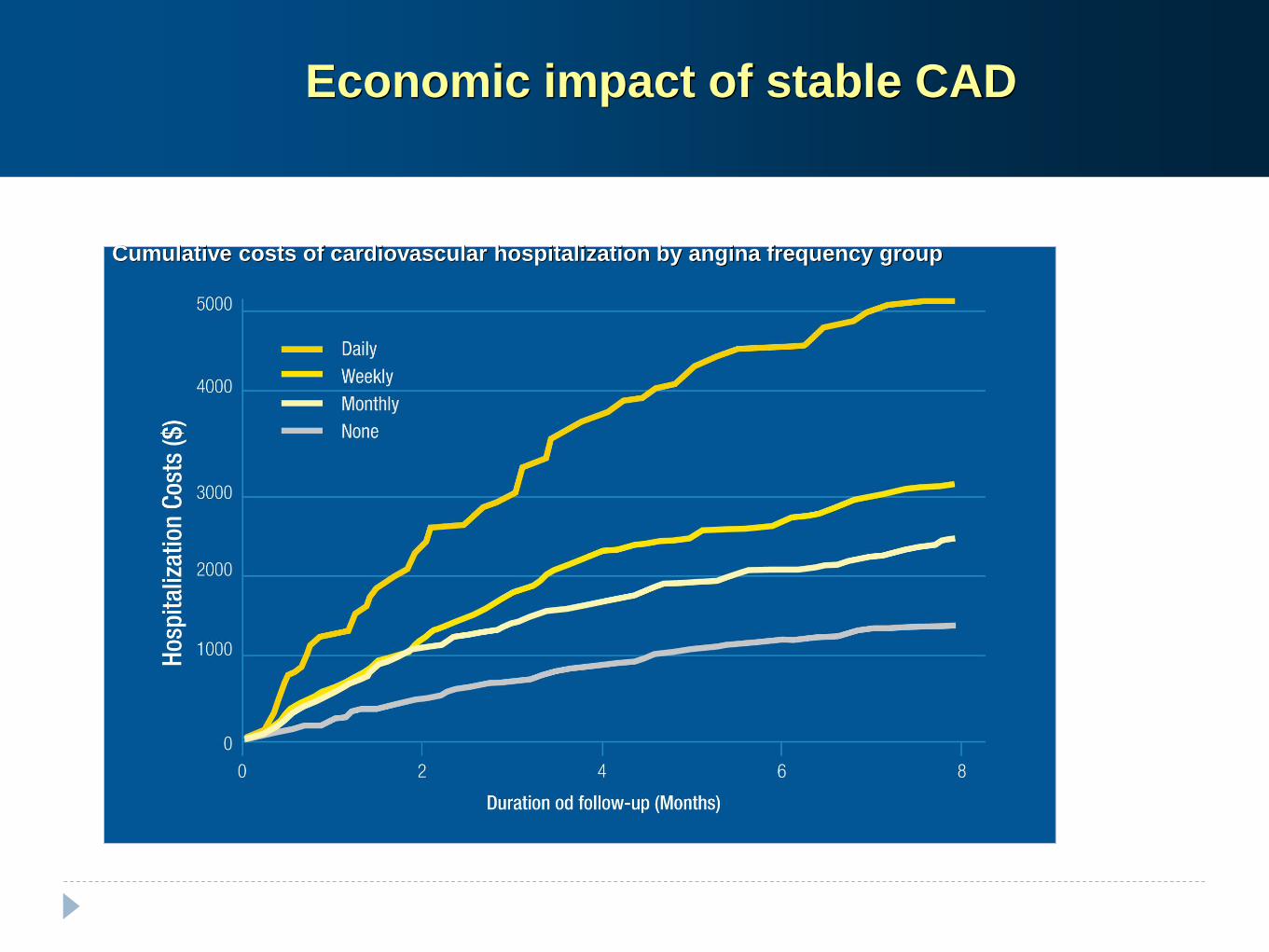
Analysis from MERLIN-TIMI 36 trial; 5460 stable outpatients after ACS; meadian follow up of 12 months
Cumulative costs of cardiovascular hospitalization by angina frequency group
Arnold SV et al. Circ Cardiovasc Qual outcomes. 2009;2:344-353
Economic impact of stable CAD
Reducing risk..
Assess residual risk and treat with evidence based
interventions - established as well as new
Educate Health professionals, Patients and carers about
the threat from untreated or under-treated risk factors
New evidence……
Heart rate reduction
PCSK9 Inhibitors
Ezetimibe - Improve-IT
New evidence……
Heart rate reduction
PCSK9 Inhibitors
Ezetimibe - Improve-IT
Heart Rate
Well recognised as a risk marker
Good evidence for Risk ‘factor’ status from observational
data as well as secondary prevention studies (Beautiful,
Shift & others)
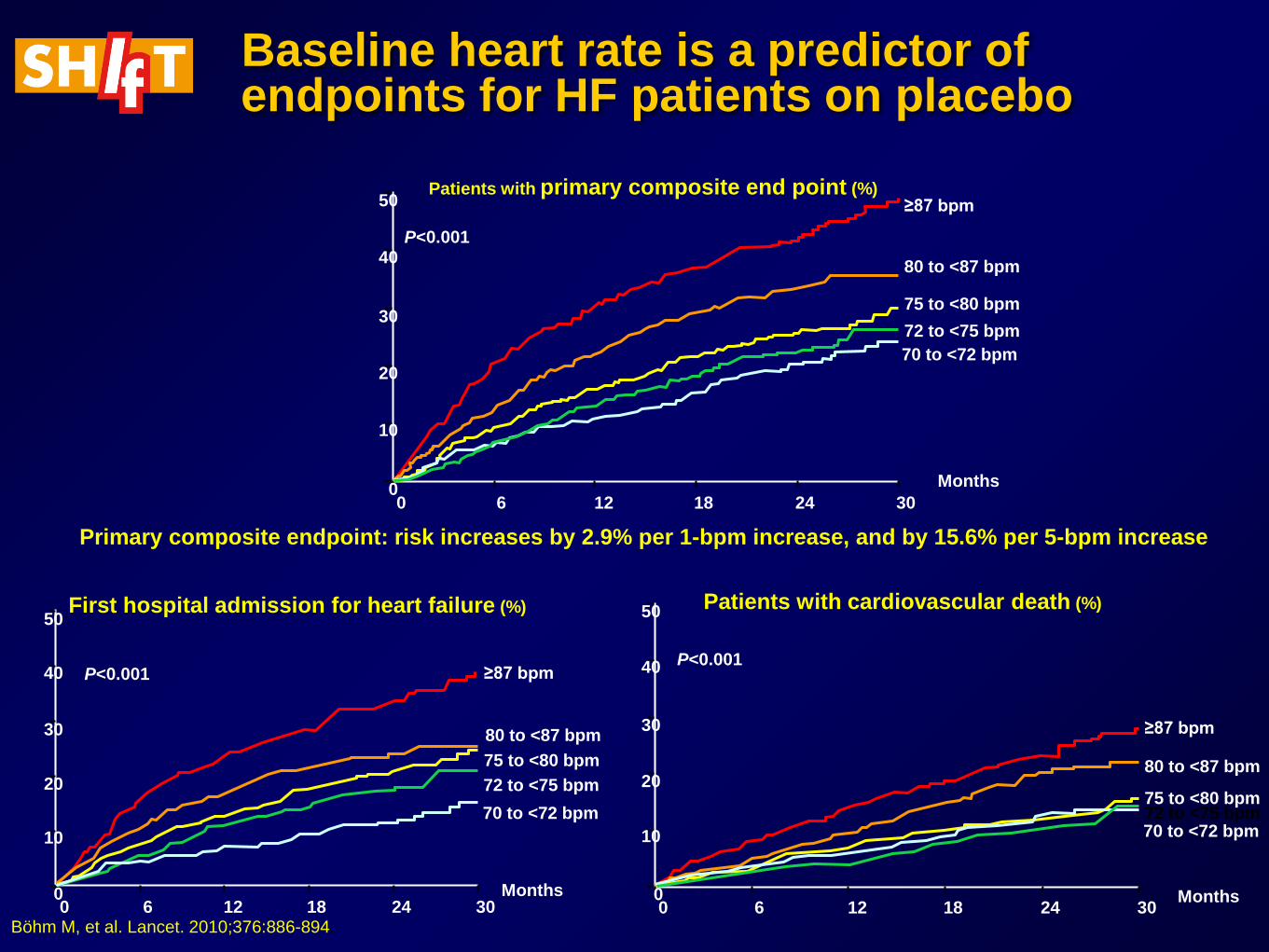
Baseline heart rate is a predictor of endpoints for HF patients on placebo
Primary composite endpoint: risk increases by 2.9% per 1-bpm increase, and by 15.6% per 5-bpm increase
50
40
30
20
10
00 6 12 18 24 30
Months
≥87 bpm
80 to <87 bpm
75 to <80 bpm
72 to <75 bpm
70 to <72 bpm
P<0.001
Patients with primary composite end point (%)
50
40
30
20
10
00 6 12 18 24 30
Months
≥87 bpm
80 to <87 bpm
75 to <80 bpm
72 to <75 bpm
70 to <72 bpm
P<0.001
First hospital admission for heart failure (%)
≥87 bpm
80 to <87 bpm
75 to <80 bpm72 to <75 bpm70 to <72 bpm
50
40
30
20
10
00 6 12 18 24 30
Months
Patients with cardiovascular death (%)
P<0.001
Böhm M, et al. Lancet. 2010;376:886-894.
New evidence……
Heart rate reduction
PCSK9 Inhibitors
Ezetimibe - Improve-IT
PCSK9 Inhibitors
PCSK9 is a protein which binds to LDL Receptor and
helps to degrade it
LDL Receptor degradation allows higher levels of LDL in
circulation
Monoclonal antibodies blocking PCSK9 help preserve
LDL Receptors thus increasing removal of LDL from
circulation
PCSK9 Inhibitors
Evidence from RCTs
Recommended by NICE - The National Institute for Health and
Care Excellence (NICE) has recommended the PCSK9 inhibitors alirocumab
and evolocumab for patients with primary hypercholesterolaemia, or mixed
dyslipidaemia that is not controlled with statins, or who cannot tolerate
statins because of their side effects or have another condition which means
they cannot take them
in final draft guidance based on manufacturers providing the drugs at
discounted prices.
BMJ 2016; 353 doi: http://dx.doi.org/10.1136/bmj.i2609 (Published 09 May 2016)
Cite this as: BMJ 2016;353:i2609
https://www.nice.org.uk/news/press-and-media/nice-draft-guidance-recommends-new-drugs-for-cholesterol-disorder. date accessed 03.10.16
New evidence……
Heart rate reduction
PCSK9 Inhibitors
Ezetimibe - Improve-IT
please refer to relevant SPC for full prescribing information
rs2228671
rs646776
rs4420638
rs4299376
rs11206510rs12916
rs6511720
0%
30%
10%
20%
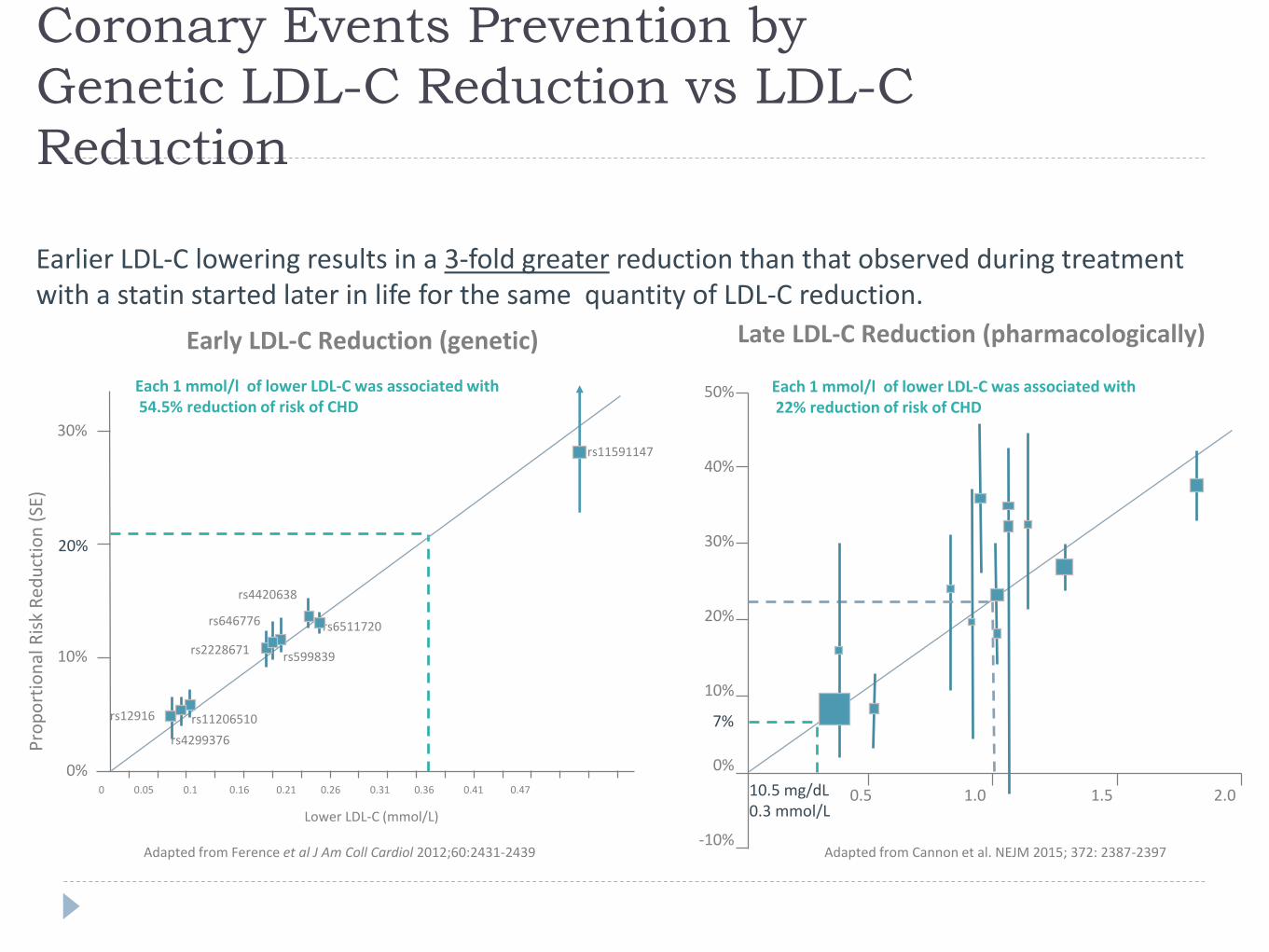
Coronary Events Prevention by
Genetic LDL-C Reduction vs LDL-C
Reduction
Earlier LDL-C lowering results in a 3-fold greater reduction than that observed during treatment with a statin started later in life for the same quantity of LDL-C reduction.
Adapted from Ference et al J Am Coll Cardiol 2012;60:2431-2439 Adapted from Cannon et al. NEJM 2015; 372: 2387-2397
Early LDL-C Reduction (genetic) Late LDL-C Reduction (pharmacologically)
50%
40%
30%
20%
10%
0%
-10%
0.5 1.0 1.5 2.0
Pro
po
rtio
nal
Ris
k R
edu
ctio
n (
SE)
7%
10.5 mg/dL0.3 mmol/L
0 0.05 0.1 0.16 0.21 0.26 0.31 0.36 0.41 0.47
rs599839
rs11591147
Lower LDL-C (mmol/L)
Each 1 mmol/l of lower LDL-C was associated with54.5% reduction of risk of CHD
Each 1 mmol/l of lower LDL-C was associated with22% reduction of risk of CHD
Ezetimibe
Interacts with NPC1L1 receptor in the gut
Reduces Cholesterol absorption
Complements the action of Statins in the Liver
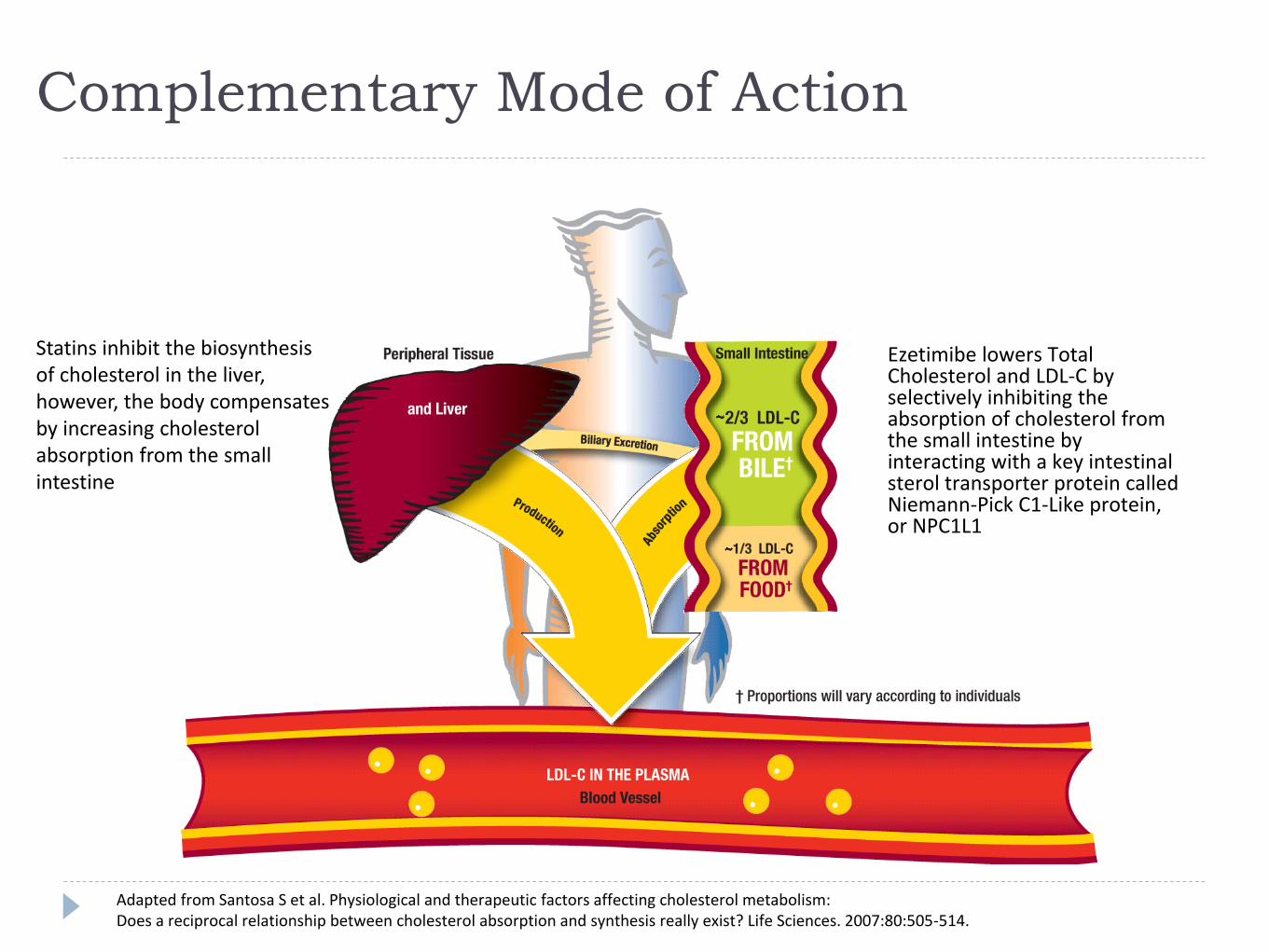
Complementary Mode of Action
Statins inhibit the biosynthesis of cholesterol in the liver, however, the body compensates by increasing cholesterol absorption from the small intestine
Peripheral tissue
Ezetimibe lowers Total Cholesterol and LDL-C by selectively inhibiting the absorption of cholesterol from the small intestine by interacting with a key intestinal sterol transporter protein called Niemann-Pick C1-Like protein, or NPC1L1
Adapted from Santosa S et al. Physiological and therapeutic factors affecting cholesterol metabolism:Does a reciprocal relationship between cholesterol absorption and synthesis really exist? Life Sciences. 2007:80:505-514.
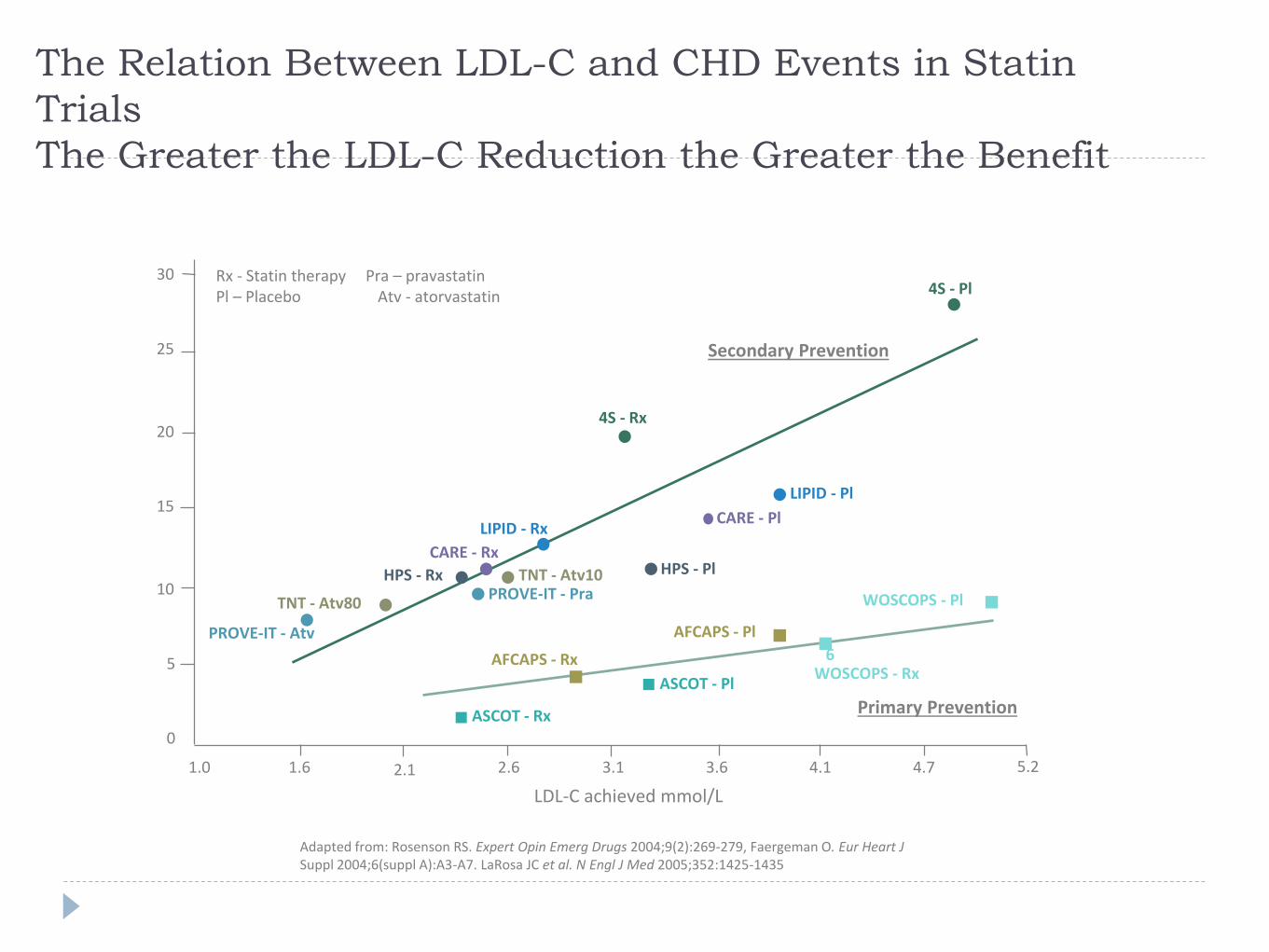
The Relation Between LDL-C and CHD Events in Statin
Trials
The Greater the LDL-C Reduction the Greater the Benefit
LDL-C achieved mmol/L
WOSCOPS - Pl
AFCAPS - Pl
ASCOT - Pl
AFCAPS - RxWOSCOPS - Rx
ASCOT - Rx
4S - Rx
HPS - Pl
LIPID - Rx
4S - Pl
CARE - Rx
LIPID - Pl
CARE - Pl
HPS - Rx
0
5
10
15
20
25
30
1.0 1.6 2.1 2.6 3.1 3.6 4.1 4.7
6
Secondary Prevention
Primary Prevention
Rx - Statin therapy Pra – pravastatinPl – Placebo Atv - atorvastatin
5.2
PROVE-IT - Pra
PROVE-IT - Atv
TNT - Atv10
TNT - Atv80
Adapted from: Rosenson RS. Expert Opin Emerg Drugs 2004;9(2):269-279, Faergeman O. Eur Heart J Suppl 2004;6(suppl A):A3-A7. LaRosa JC et al. N Engl J Med 2005;352:1425-1435
5.2
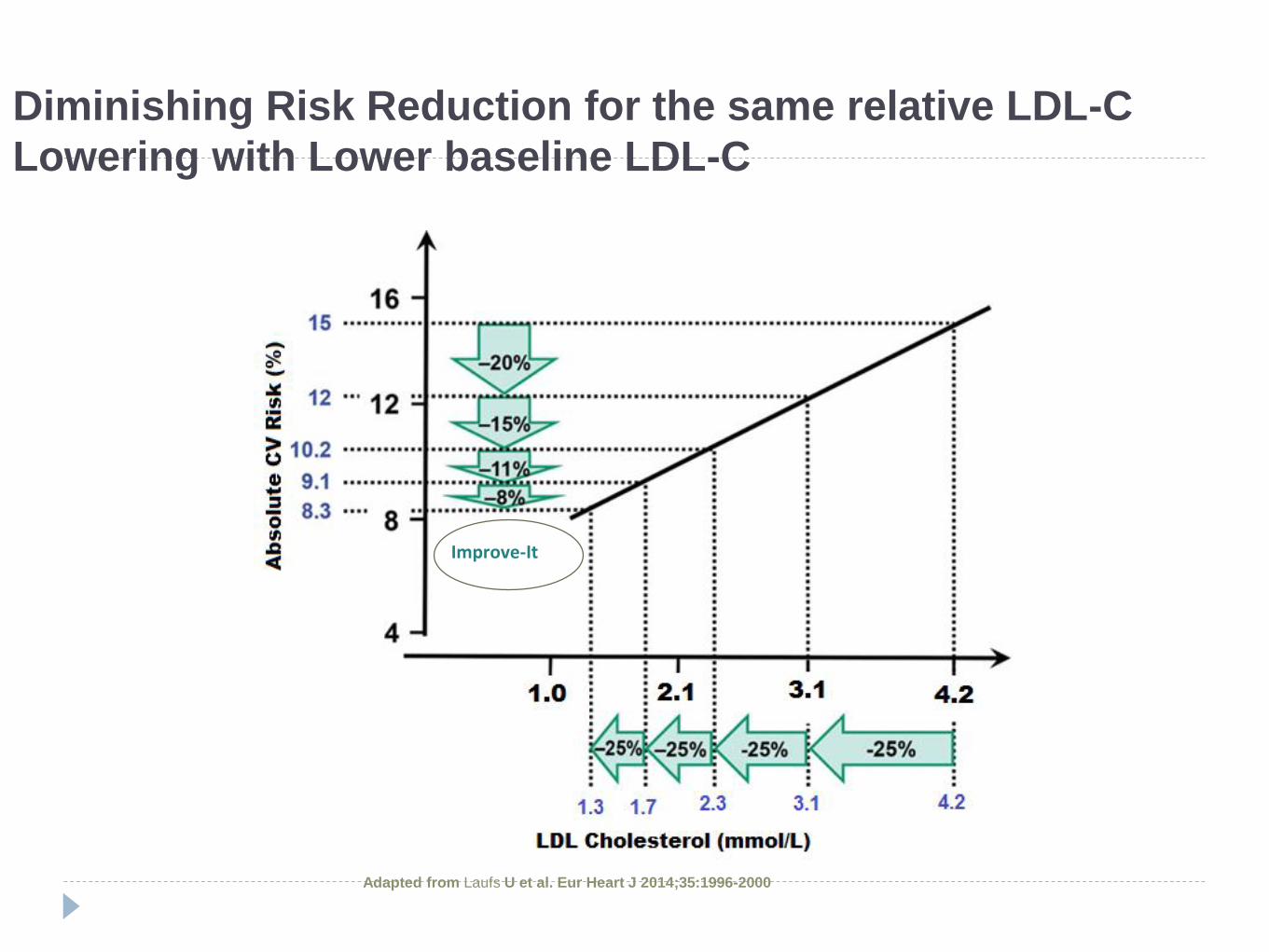
Diminishing Risk Reduction for the same relative LDL-C
Lowering with Lower baseline LDL-C
Adapted from Laufs U et al. Eur Heart J 2014;35:1996-2000
Improve-It
IMProved Reduction of Outcomes: Vytorin
Efficacy International Trial
A multicenter, double-blind, randomized study to establish the clinical benefit and safety of Vytorin (ezetimibe/simvastatin tablet) vs simvastatin monotherapy in high-risk subjects presenting with acute coronary syndrome
Aim: This study was designed to evaluate whether addition of ezetimibe to statin therapy translates into increased clinical benefit on CV outcomes relative to simvastatin alone in patients with ACS Does lowering LDL-C with the non-statin agent ezetimibe reduce cardiac events?
“Is (Even) Lower (Even) Better?” (estimated mean LDL-C ~1.4 vs. ~ 1.8 (mmol/L)
Safety of ezetimibe
Canon CP et al. NEJM (2015); 372: 2387-2397
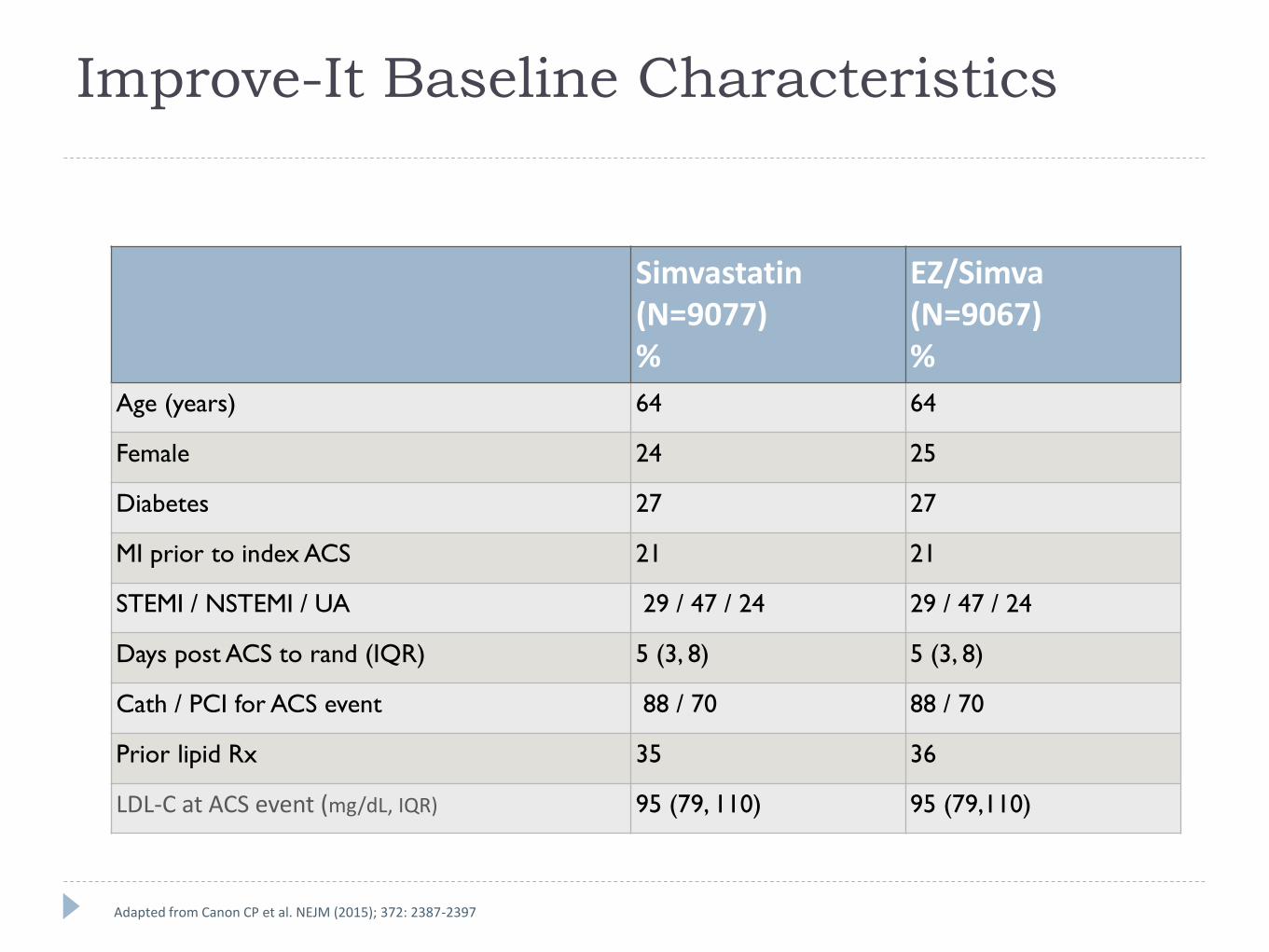
Improve-It Baseline Characteristics
Simvastatin(N=9077)%
EZ/Simva(N=9067)%
Age (years) 64 64
Female 24 25
Diabetes 27 27
MI prior to index ACS 21 21
STEMI / NSTEMI / UA 29 / 47 / 24 29 / 47 / 24
Days post ACS to rand (IQR) 5 (3, 8) 5 (3, 8)
Cath / PCI for ACS event 88 / 70 88 / 70
Prior lipid Rx 35 36
LDL-C at ACS event (mg/dL, IQR) 95 (79, 110) 95 (79,110)
Adapted from Canon CP et al. NEJM (2015); 372: 2387-2397
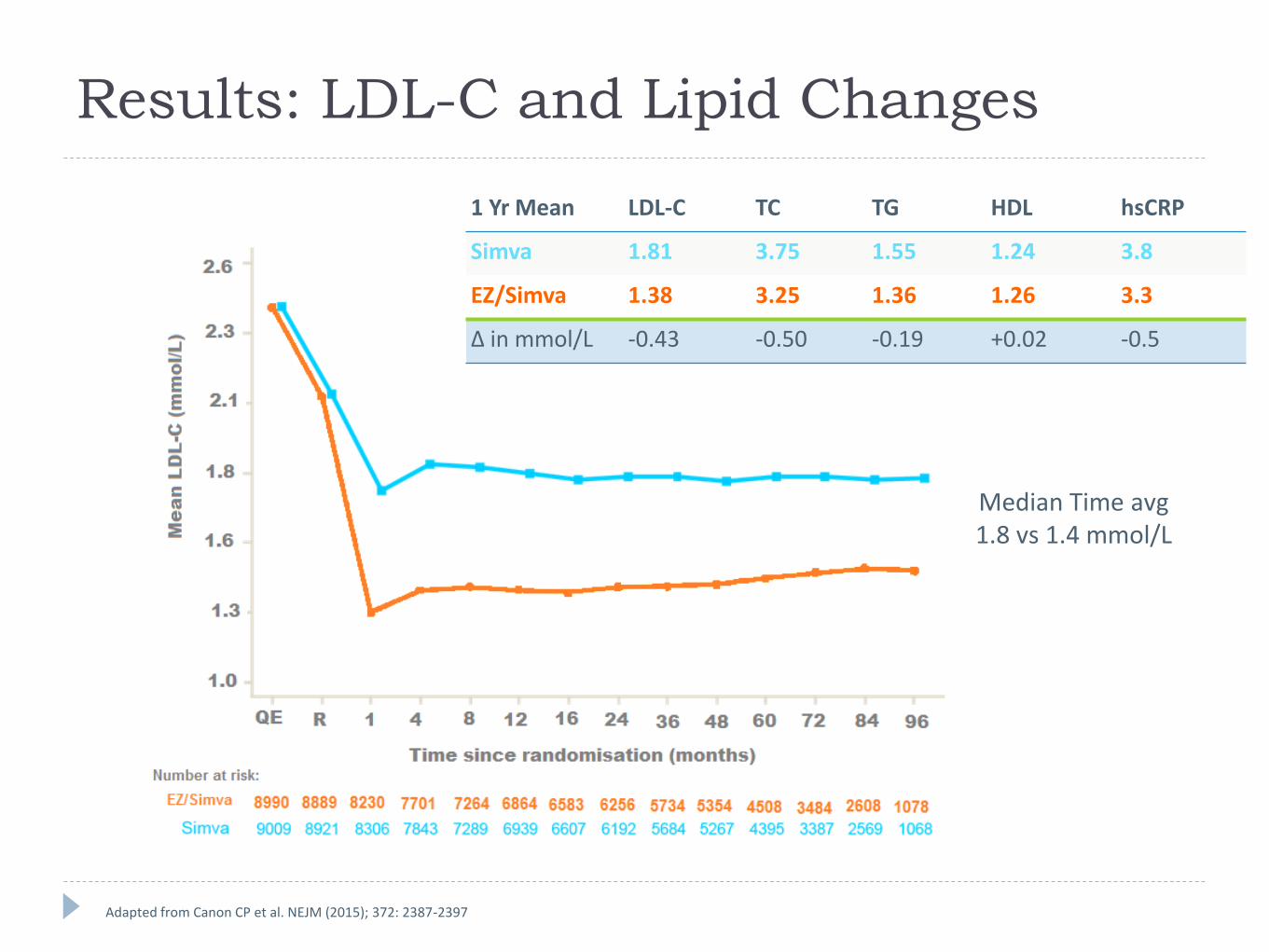
Results: LDL-C and Lipid Changes
1 Yr Mean LDL-C TC TG HDL hsCRP
Simva 1.81 3.75 1.55 1.24 3.8
EZ/Simva 1.38 3.25 1.36 1.26 3.3
Δ in mmol/L -0.43 -0.50 -0.19 +0.02 -0.5
Median Time avg1.8 vs 1.4 mmol/L
Adapted from Canon CP et al. NEJM (2015); 372: 2387-2397
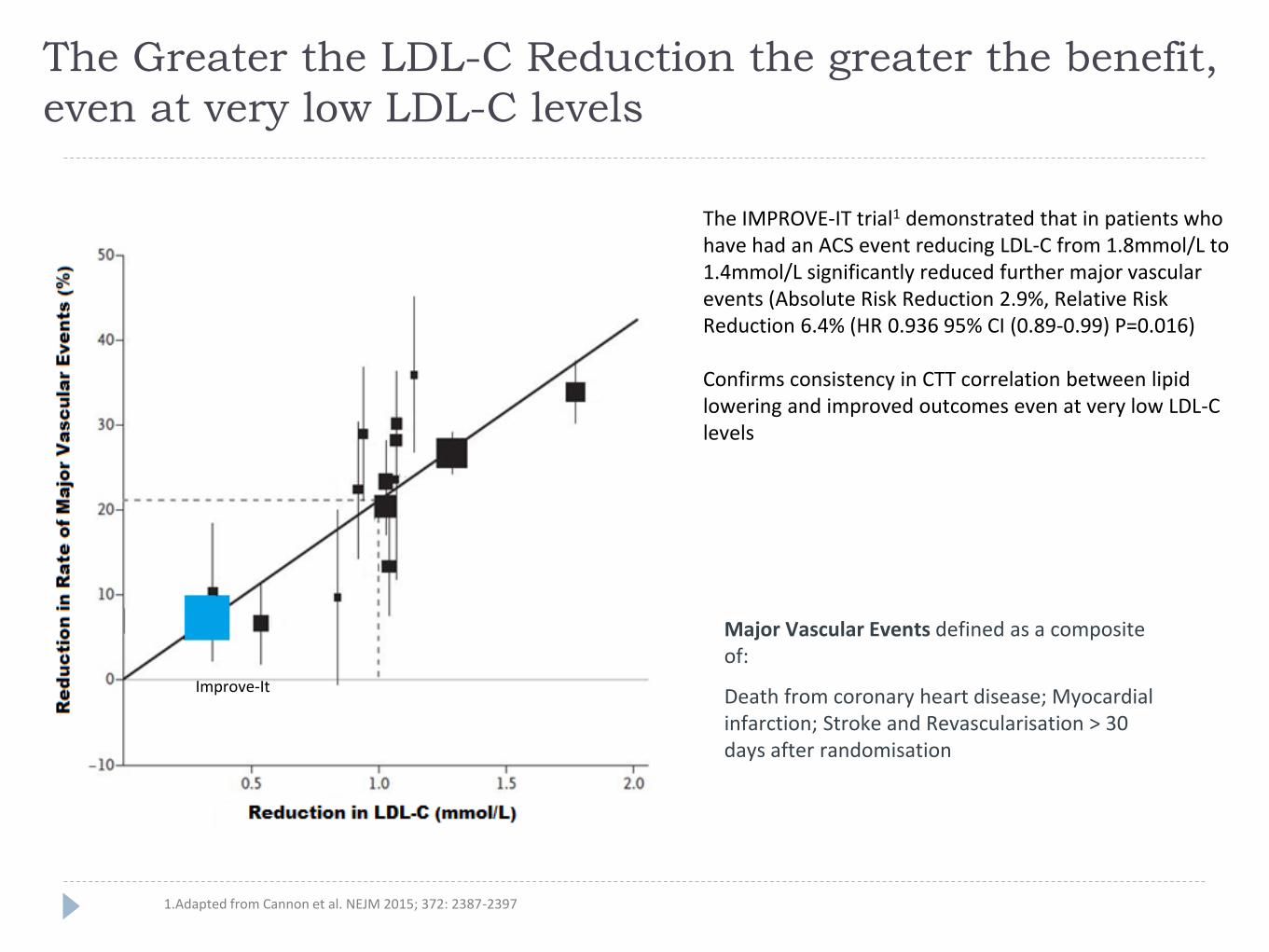
The Greater the LDL-C Reduction the greater the benefit,
even at very low LDL-C levels
Major Vascular Events defined as a composite of:
Death from coronary heart disease; Myocardial infarction; Stroke and Revascularisation > 30 days after randomisation
The IMPROVE-IT trial1 demonstrated that in patients who have had an ACS event reducing LDL-C from 1.8mmol/L to 1.4mmol/L significantly reduced further major vascular events (Absolute Risk Reduction 2.9%, Relative Risk Reduction 6.4% (HR 0.936 95% CI (0.89-0.99) P=0.016)
Confirms consistency in CTT correlation between lipid lowering and improved outcomes even at very low LDL-C levels
1.Adapted from Cannon et al. NEJM 2015; 372: 2387-2397
Improve-It
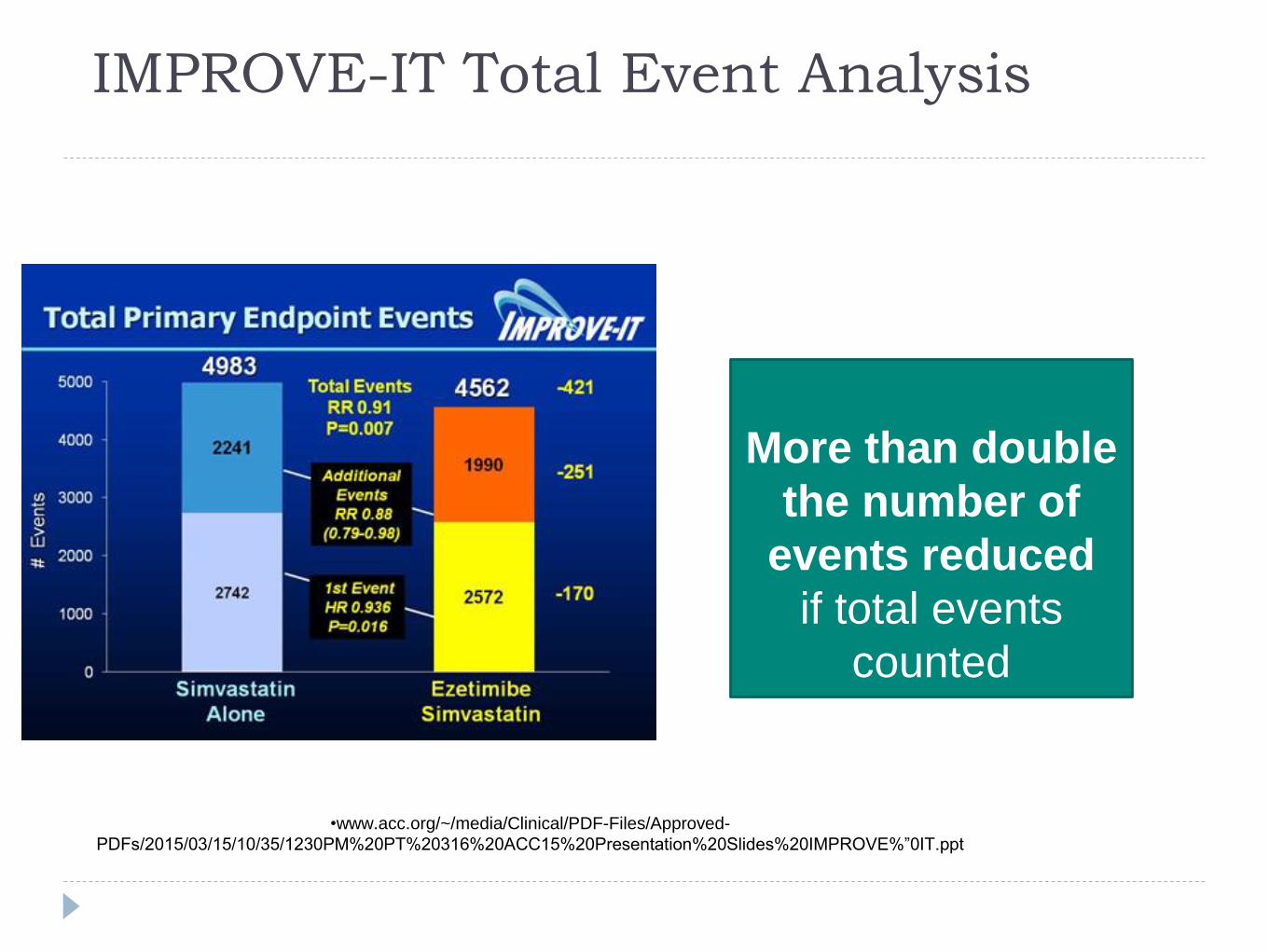
IMPROVE-IT Total Event Analysis
39
More than double
the number of
events reduced
if total events
counted
•www.acc.org/~/media/Clinical/PDF-Files/Approved-
PDFs/2015/03/15/10/35/1230PM%20PT%20316%20ACC15%20Presentation%20Slides%20IMPROVE%”0IT.ppt
What do guidelines say? NICE CG181
ESC Hyperlipidemia, August 2016
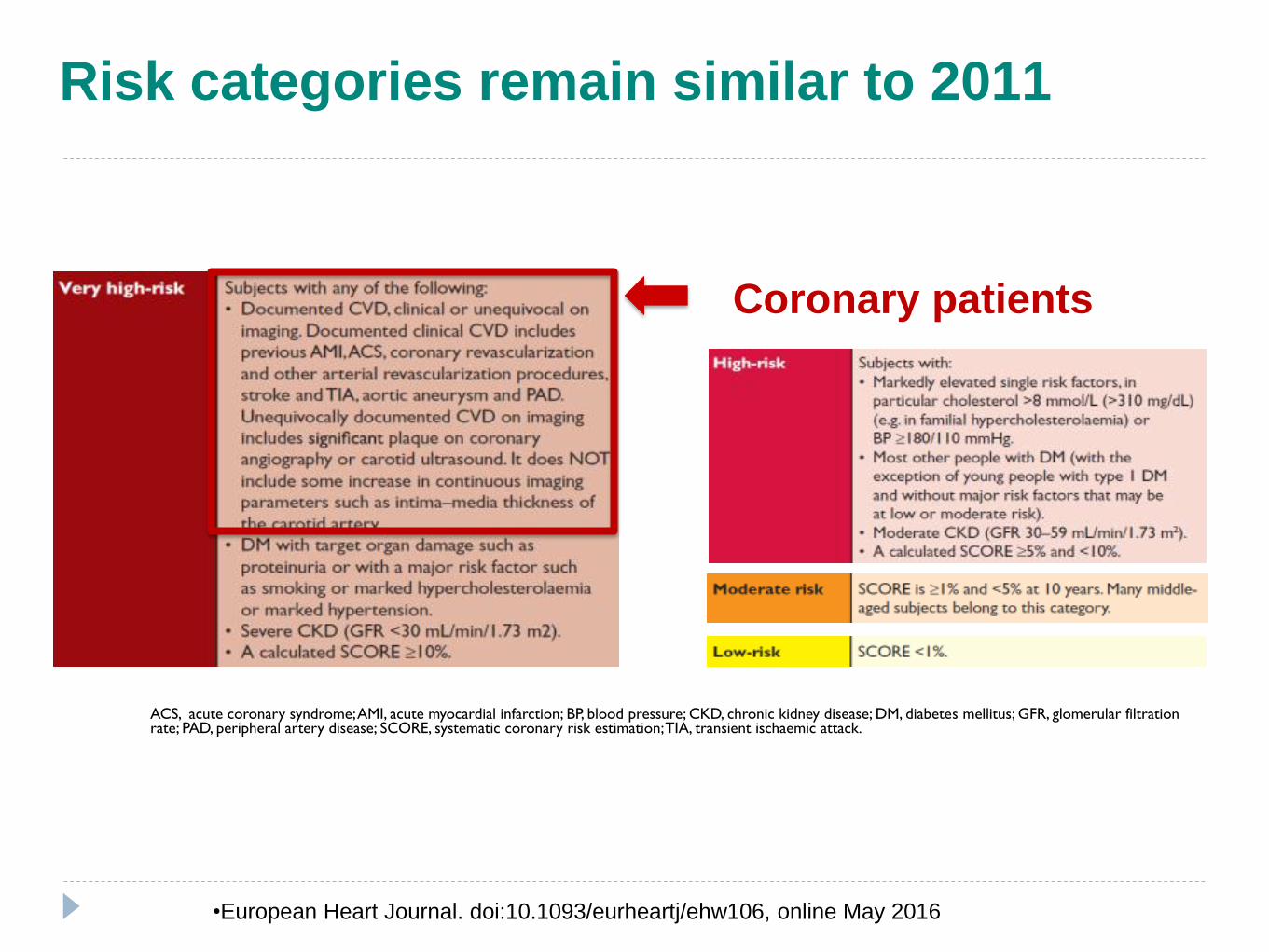
ACS, acute coronary syndrome; AMI, acute myocardial infarction; BP, blood pressure; CKD, chronic kidney disease; DM, diabetes mellitus; GFR, glomerular filtration rate; PAD, peripheral artery disease; SCORE, systematic coronary risk estimation; TIA, transient ischaemic attack.
•European Heart Journal. doi:10.1093/eurheartj/ehw106, online May 2016
Coronary patients
Risk categories remain similar to 2011
NICE CG 181
Lipid Modification : Secondary prevention
Initiate atorvastatin 80 mg* for patients with established CVD unless:
Potential drug interactions exist
There is a high risk of adverse events
Patient preference
Aim for a greater than 40% reduction in non-HDL cholesterol after 3 months of treatment with high intensity statin
Consider ezetimibe if cholesterol is not appropriately controlled on initial statin or as monotherapy in statin intolerant patients
Acute coronary syndrome – do not delay treatmentTake a lipid sample on admission and 3months after treatment
*At the time of publication (July 2014), atorvastatin did not have UK marketing authorisation for CVD
NICE Clinical Guideline 181. July 2014. Reproduced with permission. NICE Technology Appraisal Guidance 132. November 2007. Reproduced with permission
please refer to atorvastatin SPC for full prescribing information
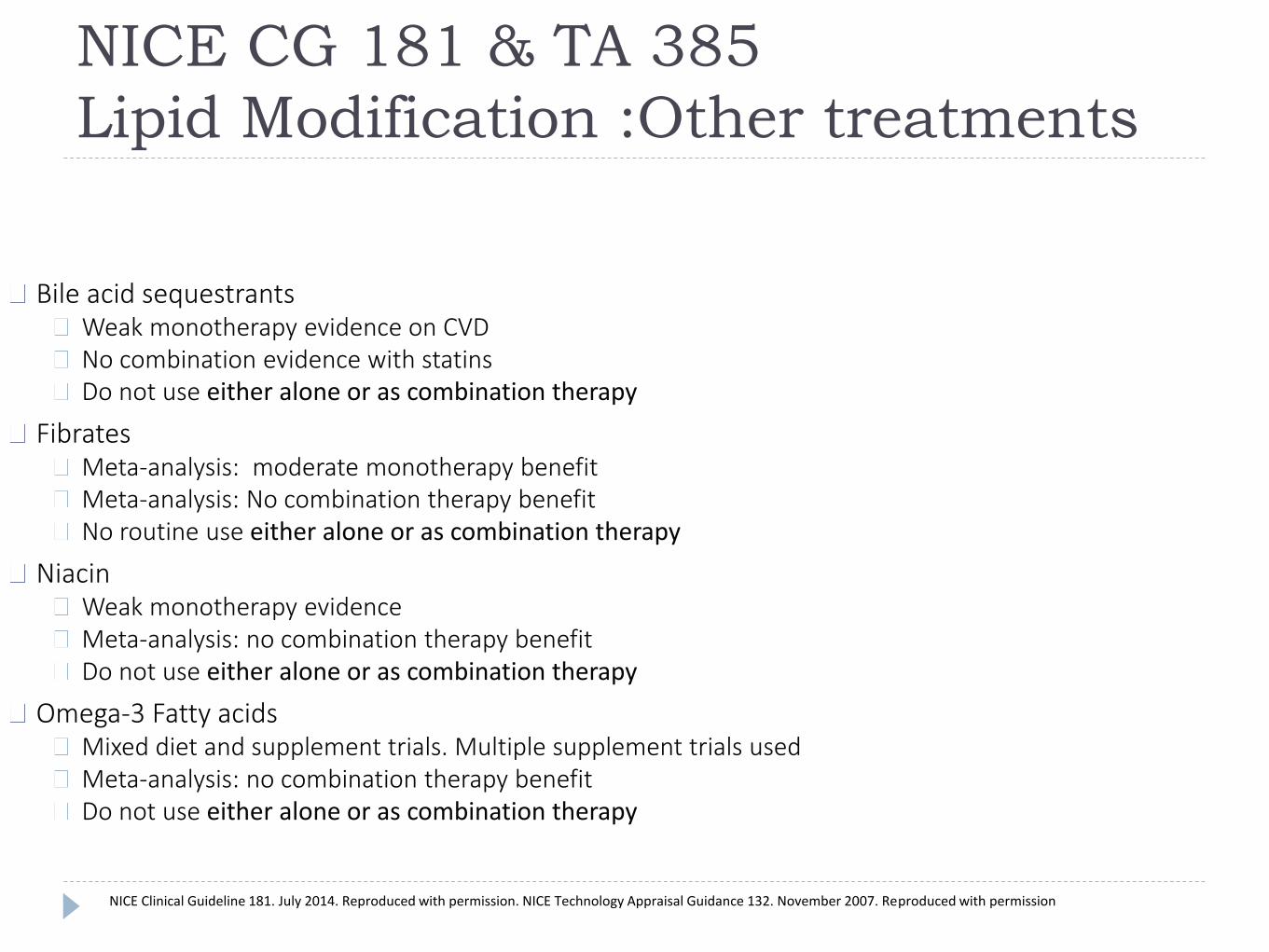
NICE CG 181 & TA 385
Lipid Modification :Other treatments
Bile acid sequestrantsWeak monotherapy evidence on CVDNo combination evidence with statinsDo not use either alone or as combination therapy
FibratesMeta-analysis: moderate monotherapy benefitMeta-analysis: No combination therapy benefitNo routine use either alone or as combination therapy
NiacinWeak monotherapy evidenceMeta-analysis: no combination therapy benefitDo not use either alone or as combination therapy
Omega-3 Fatty acidsMixed diet and supplement trials. Multiple supplement trials usedMeta-analysis: no combination therapy benefitDo not use either alone or as combination therapy
NICE Clinical Guideline 181. July 2014. Reproduced with permission. NICE Technology Appraisal Guidance 132. November 2007. Reproduced with permission
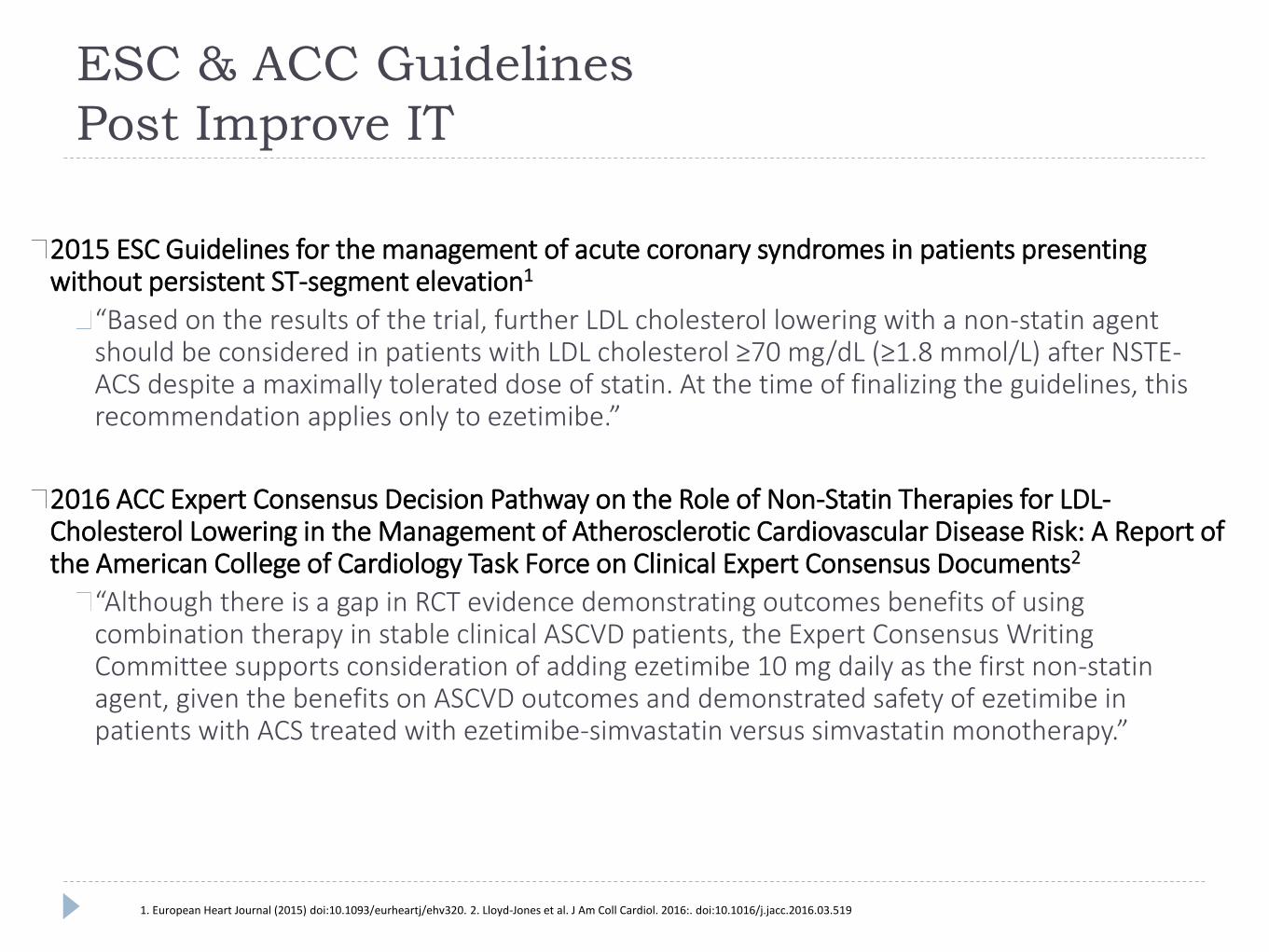
ESC & ACC Guidelines
Post Improve IT
2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation1
“Based on the results of the trial, further LDL cholesterol lowering with a non-statin agent should be considered in patients with LDL cholesterol ≥70 mg/dL (≥1.8 mmol/L) after NSTE-ACS despite a maximally tolerated dose of statin. At the time of finalizing the guidelines, this recommendation applies only to ezetimibe.”
2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: A Report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents2
“Although there is a gap in RCT evidence demonstrating outcomes benefits of using combination therapy in stable clinical ASCVD patients, the Expert Consensus Writing Committee supports consideration of adding ezetimibe 10 mg daily as the first non-statin agent, given the benefits on ASCVD outcomes and demonstrated safety of ezetimibe in patients with ACS treated with ezetimibe-simvastatin versus simvastatin monotherapy.”
1. European Heart Journal (2015) doi:10.1093/eurheartj/ehv320. 2. Lloyd-Jones et al. J Am Coll Cardiol. 2016:. doi:10.1016/j.jacc.2016.03.519
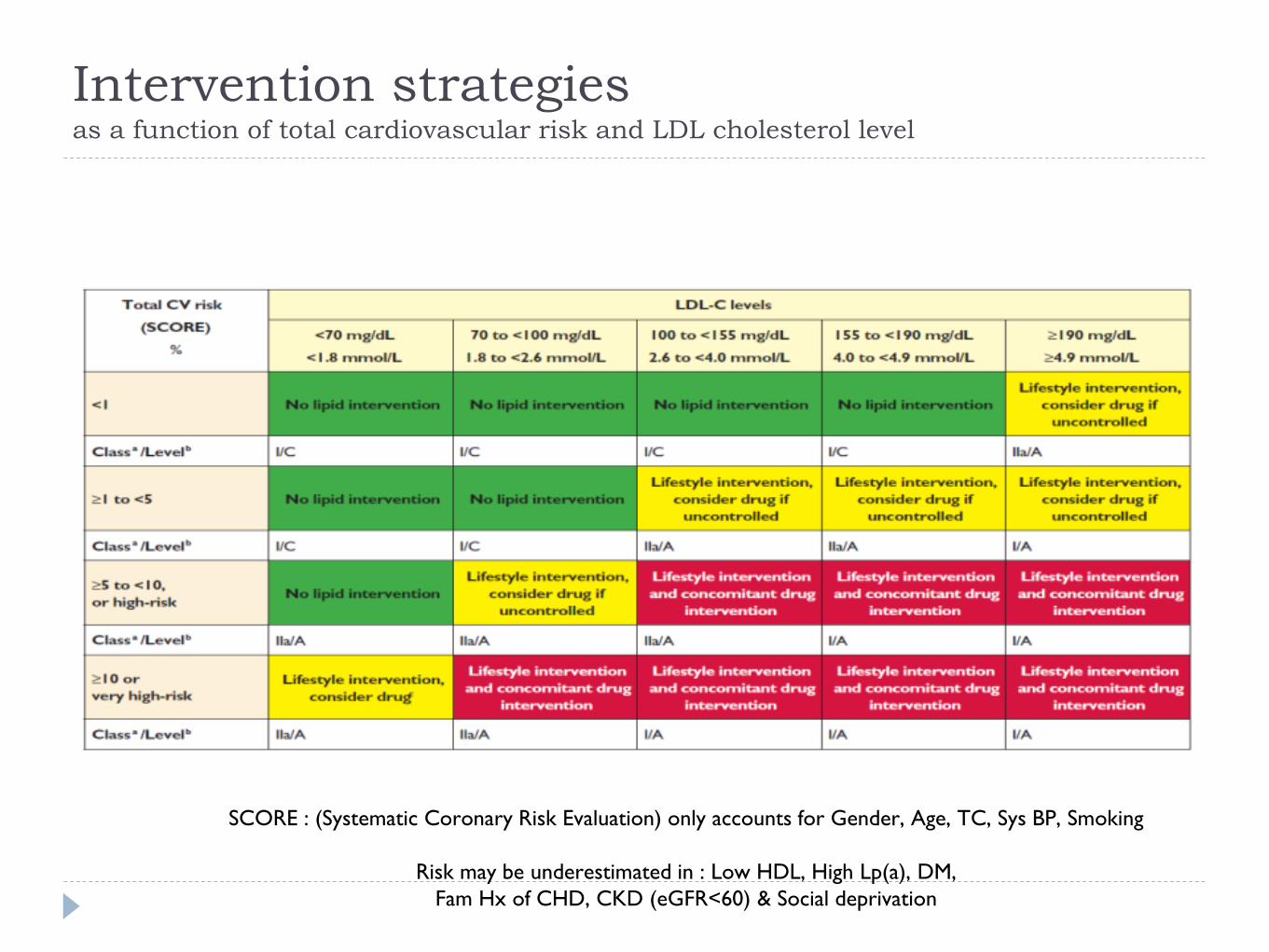
Intervention strategies as a function of total cardiovascular risk and LDL cholesterol level
SCORE : (Systematic Coronary Risk Evaluation) only accounts for Gender, Age, TC, Sys BP, Smoking
Risk may be underestimated in : Low HDL, High Lp(a), DM,
Fam Hx of CHD, CKD (eGFR<60) & Social deprivation
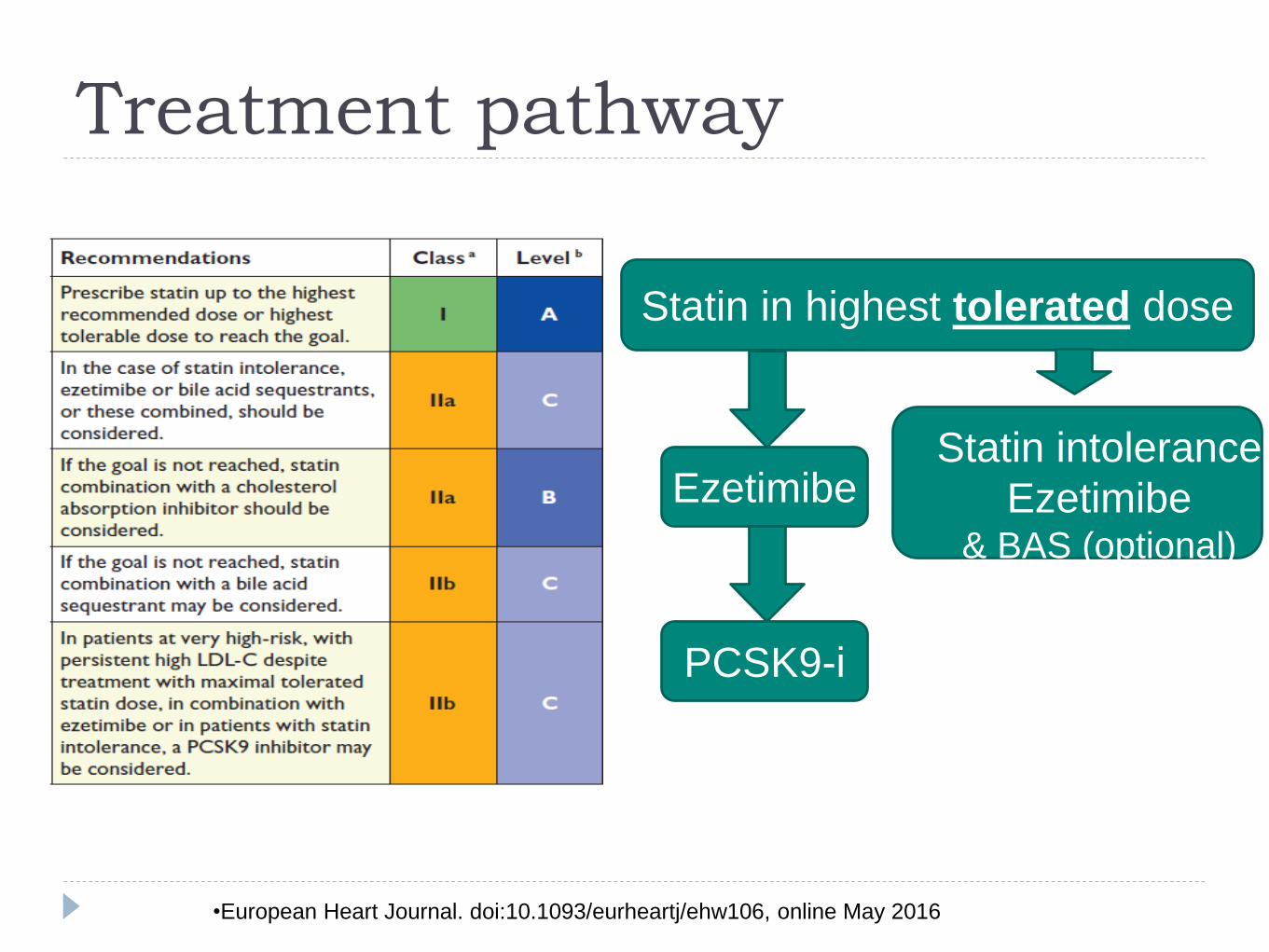
Treatment pathway
Statin in highest tolerated dose
Ezetimibe
PCSK9-i
Statin intolerance
Ezetimibe& BAS (optional)
•European Heart Journal. doi:10.1093/eurheartj/ehw106, online May 2016
Conclusions….1
Identify “all” risk factors : modifiable and non modifiable
Address and direct management of each to target level
Crucial to recognise residual risk despite excellent first
line management
Poor risk control is common and increases with time but
can be multifactorial
Conclusions….2
Prevention & Rehabilitation is “everyone’s” business and
starts from first contact with patient
Encourage and educate patient and carers to continue
“prevention & rehabilitation”
The Human Cost: Coronary Heart Disease
(CHD)3
CHD is the UK's single biggest killer
Nearly one in six men and one in ten women die from coronary heart disease
CHD is responsible for around 73,000 deaths in the UK each year, an average of 200 people each day, or one every seven minutes
Around 23,000 people under the age of 75 in the UK die from CHD each year
2.3 million people are living with CHD in the UK
Most deaths from coronary heart disease are caused by a heart attack
There are up to 175,000 heart attacks in the UK each year; that’s one every three minutes
3. BHF Cardiovascular Disease Statistics 2014 p.54