Embed Size (px)
Citation preview

Pharmacoeconomics 2005; 23 (11): 1167-1181ORIGINAL RESEARCH ARTICLE 1170-7690/05/0011-1167/$34.95/0
© 2005 Adis Data Information BV. All rights reserved.
The Importance of Drug AdverseEffects Compared with SeizureControl for People with EpilepsyA Discrete Choice Experiment
Andrew Lloyd,1 Emma McIntosh2 and Martin Price3
1 The MEDTAP Institute at United BioSource Corporation, London, UK2 Health Economics Research Centre, University of Oxford, Oxford, UK3 Janssen-Cilag, Saunderton, Buckinghamshire, UK
Introduction: Antiepileptic drugs (AEDs) have been shown to reduce the severi-Abstractty and frequency of seizures for most patients. However, many patients experienceadverse effects in order to maintain seizure control.Study design: A stated preference discrete choice experiment (DCE) was used toexplore the preferences of people with epilepsy regarding the adverse effects andseizure control of AEDs.Methods: The main adverse effects of AEDs were identified through a literaturesearch and expert consultation. In addition, a national epilepsy patient advocacygroup helped to identify important attributes and commented on the attributes wehad already identified. The DCE included five attributes related to adverse effects(alopecia, nausea, skin rash, concentration effects and weight change) plus seizurecontrol and cost (to estimate willingness to pay [WTP]). A cost attribute wasincluded in the DCE in order to estimate people’s WTP for changes in attributelevels.
Five hundred members of a national patient advocacy group with a diagnosisof epilepsy were presented with pairs of hypothetical drug profiles with variedlevels of adverse effects, seizure control and cost; they were then asked to indicatewhich drug they preferred. Questions were also included to collect soci-odemographic data (including income) and information regarding experience ofadverse effects and medication. The survey was administered via the post and theInternet. Data were analysed using a random effects probit model.Results: A total of 148 surveys were returned. All attributes were significant andhad the expected polarity, i.e. participants showed a preference for less severeadverse effects, greater seizure control and less cost. To achieve 100% seizurecontrol and no adverse effects, participants were willing to pay £709 ($US1105)per month, 95% CI £451, £1278 (£1 = $US1.56, 2002 exchange rate). Partici-pants’ WTP was significantly influenced by different adverse effects; for exam-ple, people with epilepsy were willing to pay only £174 ($US271) per month for adrug that provided seizure freedom but also caused hair loss. Segmented modelsshowed that seizure frequency has a significant negative impact on respondents’

1168 Lloyd et al.
income levels. Also, women were willing to pay twice as much as men to avoidweight gain. Participants were also willing to trade changes in seizure control forimprovements in adverse effects.Conclusion: Participants placed a high value on gaining total seizure control withno adverse effects. This study underlines the importance that people with epilepsyplace on reducing adverse effects. The study also revealed how preferences forAEDs vary in different subgroups. Management of epilepsy is usually aimed atminimising seizures within a tolerable level of adverse effects. The present studysuggests that people with epilepsy have strong preferences for reducing adverseeffects as well as improving seizure control. These data may be considered usefulwhen making medical management decisions in epilepsy.
Antiepileptic drugs (AEDs) have been shown to It is unclear whether patients’ preferences regard-reduce the severity and frequency of seizures and, ing treatments and their potential adverse effects arefor most patients, are the cornerstone of their epilep- always considered in the clinical decision-makingsy management. It has been estimated that approxi- process, which is primarily concerned with balanc-mately 65% of patients can achieve full seizure ing seizure control and adverse effects. It has beencontrol with their first AED.[1] However, up to 35% advocated that the management of a disease likewill need to switch to other AEDs due to lack of epilepsy should incorporate a shared decision-mak-efficacy or tolerability problems. AEDs are success- ing process between doctor and patient.[9,10] Deci-ful in reducing or even eliminating seizures for sions regarding patients’ treatment generally followmany patients. While seizure freedom is the ultimate treatment guidelines based on evidence fromaim of treatment for all patients, it is also important clinical trials. Patient preferences may sometimes beto consider how adverse effects of AEDs will affect included in decision making, but this is probably intheir quality of life. the form of the physician’s perceptions of patient
preferences, which may be biased. To include pa-The range of AED adverse effects is very broadtients’ preferences in clinical decision making, thereand their pattern can be complex.[2] Relatively com-is a need for accurate information regarding themon non-life-threatening adverse effects include al-nature of their preferences.opecia, rash, disturbances in concentration, gastroin-
testinal irritation, weight gain or loss, dizziness, This study was designed to elicit patients’ prefer-tremor and lethargy.[3-7] AEDs are also occasionally ences regarding their epilepsy treatment using aassociated with very severe adverse effects that can stated preference discrete choice experiment (DCE).be life threatening. Skin rash can (rarely) be the sign DCEs are a useful method of eliciting preferencesof a severe hypersensitivity reaction called Stevens- because they are able to quantify the individualJohnson syndrome, which is fatal in about 10% of impact of each different attribute of the interventioncases.[8] Another rare but fatal toxic effect of AEDs on decision making. Hypothetical scenarios areis toxic epidermal necrolysis. Severe haematologi- presented and participants are asked to state whichcal reactions such as thrombocytopenia and aplastic option they prefer. Different attributes in the deci-anaemia have also been reported.[8] Hepatic and sion are considered simultaneously by the respon-cardiac life-threatening adverse events can also oc- dents, and analysis of the resulting choices allowscur. While these rare complications can have very the relative importance of each (main effect) to bedramatic effects on patients, it may well be that, for determined, as well as interaction effects if this isthe average patient, the more common non-life- accommodated in the design. The attributes in athreatening problems have a greater effect on health- healthcare DCE can represent the different elementsrelated quality of life. of the clinical decision and typically include attrib-
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

Preferences for Epilepsy Treatments 1169
utes such as treatment efficacy, adverse effects, 3. Decide the appropriate participation model (e.g.standards of care and waiting time. DCEs have been binary, multinomial or nested).used in other areas of health to elicit patients’ prefer- 4. Pair the scenarios such that the properties ofences.[11-15] orthogonality are retained, ensuring minimal over-
By including the sacrifice-based attribute ‘cost’, lap on the attribute levels.[16]
it is also possible to estimate the amount that partici- 5. Produce a survey instrument containing relevantpants would be willing to pay for improvements in explanation of the choice exercise as well as theattributes such as different adverse effects or treat- pairwise choices.ment effectiveness. This places the DCE within the 6. Elicit preferences (postal survey or interviews).realms of economic theory and allows the estimation 7. Analyse the preference data.of welfare values for use within economic evalua-tion, namely cost-benefit analysis. In the present Identify Attributes and Rangesstudy, a DCE was designed to elicit the preferences
The attributes to be included in the DCE shouldof people with epilepsy for changes in adverse ef-represent the cogent elements of the clinical scena-fects and the level of seizure control. The studyrio and therefore must have face validity. In order toincluded cost as an attribute in order to determineidentify the relevant attributes for inclusion in thewillingness to pay (WTP) for improvements in ad-present study, we undertook a detailed literatureverse effects and seizure frequency.search. This was designed to identify studies thatdescribed the adverse effects of different AEDs.Methods
Two recent review articles were identified fromthe literature search.[6,8] These articles were re-
Rationale for Using Discrete viewed in order to determine the different adverseChoice Experiments effects that are associated with AEDs and also to
document the ranges of probabilities associated withIn the absence of any available data on how these adverse effects. One of these articles related to
patients feel about experiencing different potential the use of AEDs in the treatment of bipolar disorder.adverse effects of AEDs, it was decided to use the Many AEDs also have an indication for bipolarstated preference DCE approach to elicit prefer- disorder and so information regarding adverse ef-ences for the adverse effect profiles of various ‘hy- fects would be relevant. Supplemental informationpothetical’ AEDs. The aim was to identify the rela- on commonly prescribed AEDs was also derivedtive importance of the individual adverse effects of from the product monographs, which included de-such drugs in order to inform policy makers and tailed information on the frequencies of adverseclinicians of the importance of various adverse ef- events associated with the product.[17-21] A large listfect drug profiles to epilepsy patients. One of the of different adverse effects was identified throughkey features of a DCE is its ability to identify this process.marginal values for individual attributes of a drug or More than 20 relatively common, non-life-threat-intervention. This information can then be used to ening adverse effects were identified together with adetermine participants’ WTP for any combination of substantial number of rare but potentially life-threat-adverse effects and seizure control. There are a ening adverse events that have been linked withnumber of stages in a DCE, as follows. AEDs. Using a DCE methodology, it is not possible1. Identify the relevant attributes and the appropriate to include an unlimited number of different attrib-levels. utes and so it was necessary to identify a limited set2. Use statistical design theory to produce an orthog- of the most important adverse effects from amongonal matrix of scenarios combining the attributes the total list. The number of attributes was limited toand levels (ensuring level balance). seven so that the decision making was not unrealisti-
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

1170 Lloyd et al.
cally complicated and the number of choices was in widely reported with commonly used AEDs. Hairthe range recommended in questionnaire design loss was included because, while it is essentially juststudies.[22] Other studies have been reported that a cosmetic adverse effect, it can have a detrimentalhave included a similar number of attributes.[13,23] effect on quality of life. An attribute describing
concentration deficits was included. Problems withA concerted attempt was made to ensure that theconcentration could affect a person’s ability to workattributes included were meaningful and importantand undertake many leisure activities. Nausea orto participants. The attributes and levels are shownsickness1 was included because nausea could have ain table I. The list of attributes chosen had to includeserious impact on quality of life but may not be aseizure control, as this is clearly an important con-threat to health. Finally, weight change was alsosideration in treatment choice. Skin rash was includ-included because most of the AEDs can affected because it, in itself, causes concern for partici-weight (both weight gain and weight loss). Weightpants, but it is also associated with the small risk ofchange can also affect a participant’s health andStevens-Johnson syndrome, a potentially life-threat-their quality of life.ening complication. It was felt necessary to include
The relative strength of preference placed on theone of the rare but potentially fatal adverse effects ofavoidance of these adverse effects (attributes) willAEDs, and Stevens-Johnson syndrome is the mosthelp to indicate whether risks to health or quality oflife are most important to people. The rationale forthe selection of different adverse effects included inthe DCE was discussed with a national epilepsypatient advocacy group (Epilepsy Action™) in theUK, as well as a physician involved in epilepsyresearch. Once the attributes had been identified andagreed, it was necessary to specify the attributelevels, such as the risk of rash, level of weight gainand the degree of seizure control. The level rangesused in the DCE were guided by our review of theliterature as described above.
In order to compare how much people valuechanges in adverse effect profiles and seizure con-trol within an economic evaluation framework,transformation of attribute values into a commonnumeraire is required. A commonly used approachis to include ‘cost’ as an attribute. The present studyincluded cost in monetary terms (£ per month) andcan be used to estimate people’s WTP for differentdrug profiles. The levels of the cost attribute wereselected to broadly capture the range of list pricesfor the main AEDs on the UK market.
Participants were asked to imagine that their cur-rent epilepsy therapy was no longer working andthey now required an additional drug. Participantswere all informed that this was a purely hypothetical
Table I. Attributes and levels selected for the discrete choice exper-iment
Attribute Level
Seizure control You become free of seizuresYour seizures are reduced by more than half(75%)Your seizures are reduced by half (50%)
Weight change You gain 26lbsYou gain 13lbsYou lose 13lbs
Skin rash You have no skin rashYou have a 1 in 10 chance (10%) of developingskin rashYou have a 1 in 5 chance (20%) of developingskin rash
Concentration Your concentration is unaffectedYou have a 1 in 10 chance (10%) of the drugaffecting your concentrationYou have a 1 in 5 chance (20%) of the drugaffecting your concentration
Alopecia You have no hair lossYou have a 1 in 10 chance (10%) of hair lossYou have a 1 in 5 chance (20%) of hair loss
Feeling sick You do not feel sickYou have a 1 in 10 (10%) chance of feeling sickor being sickYou have a 1 in 3 (33%) chance of feeling sickor being sick
Payment vehicles
cost The drug will cost you an extra £25 per monthThe drug will cost you an extra £50 per monthThe drug will cost you an extra £75 per month
1 In the current context, the word ‘sick’ is used to refer to nausea and vomiting and not just general illness as in the USsense of the word.
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

Preferences for Epilepsy Treatments 1171
exercise and that it was designed to find out how binary choice ‘forcing’ responses to unrealisticimportant the different aspects of antiepilepsy ther- choices.apy are for each individual.
Pair the Scenarios so that the Properties ofOrthogonality are RetainedUse Design Theory to Produce an
Orthogonal Matrix of Scenarios Combining The scenarios from the orthogonal design werethe Attributes and Levels randomly paired up into choice sets, ready for elicit-
ing preferences. The differences between the choiceA number of design criteria are recommended
sets were then tested to ensure that orthogonality inwhen devising DCEs; three key features are
differences was maintained, and appropriate correla-orthogonality, level balance and minimal overlap.[16]
tion tests for discrete and continuous data wereOrthogonality is the requirement that the attribute
employed to test this. The choice sets were thenlevels are uncorrelated, and level balance requires
replicated and a model simulated using LIMDEPthat the attribute levels appear an equal number of
software to ensure absence of significant correla-times. Level balance was achieved by giving all
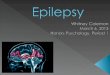
tion. An example of a choice set from the survey isattributes the same number of levels (three), and the
shown in figure 1.software package SPEED[24] (Hague ConsultingLtd, 1997) was used to combine the attributes and Development of Survey Instrumentlevels from table I into an orthogonal matrix. When
The questionnaire included an introduction re-pairing up choice sets, care was taken to ensuregarding the purpose of the DCE and instructions onminimal overlap. Too much overlap reduces thehow to complete the exercise. The questionnaireinformation obtained on trade-offs between attributeincluded a description of each attribute and itslevels.levels. There was also a discussion of the cost attri-bute and why it had been included. The reasoningDecide the Appropriate Participation Modelfor the inclusion of cost was included in a sectionentitled ‘Making Difficult Choices’. The phrasingIt is necessary to decide on the nature of thewas as follows:response that participants are asked to make and
“We are going to ask you to make a series ofwhether, for example, they can choose not to acceptdifficult choices regarding your treatment. For ex-the hypothetical therapy offered in the DCE. Duringample we are going to ask to you to think aboutthis stage, the most ‘realistic’ decision format withinwhether you would be willing to accept a drug thatwhich to present the choices must be decided. Ayou would have to pay for. These choices are allbinary choice (a forced choice between drug A orhypothetical, but they will help us understand howdrug B) represents an unconditional demand modelstrongly you feel about side-effects and seizure re-and generally does not incorporate an ‘opt-out’ op-duction; your answers here will in no way affect thetion (neither drug A nor drug B) or a status quotreatment you receive.”option. It was decided that, with this group of par-
ticipants, because they were already identified as The second section of the questionnaire con-‘demanders’, i.e. they currently used drugs to con- tained the ten DCE choice sets. In this study, antrol their epilepsy, opting out of their drug therapy extra choice set was added to the questionnairewas not a realistic option for them. Essentially, the (choice 6) to explore consistency of preferences.aim of the study was to explore preferences for This option was clearly superior to other scenarioscurrent attributes and not to predict demand. There- in the questionnaire. Participants who failed to pickfore, a binary model was employed and efforts were this option were considered to have not understoodmade to identify realistic levels to produce meaning- the task adequately and their data were excludedful choice sets so as to minimise the chances of the from the final analysis. In the final section, there was
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

1172 Lloyd et al.
Weight change?
Choice 1
Which drug wouldyou prefer?
Chance of skin rash?
Concentration affected?
Hair loss?
Reduction in seizures?
Gain 12kg (26lbs)
Add-on Drug A
1 in 5 chance (20%)
1 in 10 chance (10%)
You have no hair loss
Your seizures are reduced by half (50%)
Monthly cost to you? £50
Feeling sick? 1 in 3 chance (33%)
Gain 6kg (13lbs)
Add-on Drug B
1 in 10 chance (10%)
Your concentration isunaffected
You have no hair loss
Your seizures are reduced by more than half (75%)
£25
You do not feel sick
Prefer Drug A Prefer Drug B
Fig. 1. Example of a choice set.
a series of questions regarding demographics, the of decision making on simple qualitative representa-tions that represent the gist of the differentnature of participants’ epilepsy and their medica-probabilities. We have attempted to provide a sim-tion. Participants were also asked to indicate wheth-plified description of the uncertainty around seizureer they had previously experienced any of the ad-control in order to reduce the chance of misinterpre-verse effects listed in the questionnaire and howtation.important the adverse effect was to them.
As shown in table I, several of the attributes inEliciting Preferencesthe DCE contained uncertainty or risk. Individuals
may find it difficult to understand uncertainties and Data collection took place in two stages. Thethen incorporate them into a decision.[25,26] In order questionnaire was piloted with 30 participants into help people understand the uncertainties, the in- order to check for any problems in interpretation andformation was always presented in more than one face validity. Participants were recruited for theformat, as recommended by Entwistle et al.,[27] and pilot phase by contacting all members of an onlineBennett and Calman.[28] Evidence indicates that peo- epilepsy community supported by Epilepsy Ac-ple find it much easier to understand absolute fre- tion™. The pilot study demonstrated that partici-quencies rather than percentages.[25,29] The risks pants were easily able to complete the questionnairewere always presented in the questionnaire as ‘1 in and that all the attributes chosen for inclusion in theX’ followed by the probability re-expressed as a questionnaire were significant predictors of choice,percentage in brackets. One exception to this was and were in the expected direction. The pilot alsothe description of the improvement in seizure con- confirmed that the levels of the cost attribute weretrol, which was described as reducing seizures by a appropriate. Following the pilot phase, 500 WTPhalf, by more than a half, or as being free from questionnaires were posted out to a random selec-seizures. The levels were further qualified as a re- tion of members of Epilepsy Action™ who hadduction of 50%, 75% or 100%, respectively. Work previously expressed an interest in taking part inby Reyna et al.[30-32] suggests that people base a lot surveys. This postal questionnaire was identical in
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

Preferences for Epilepsy Treatments 1173
appearance to the online version. A donation of £10 sponse model is to be interpreted as the outcome of awas made to the charity for every questionnaire that utility maximising choice, the argument of the stan-was returned, and participants were informed of this. dard normal cumulative density function in theParticipants themselves received no payment for probit model must take the form of a utility differ-participating. The questionnaire data were entered ence. Hanemann notes that this condition provides aonto an Excel spreadsheet. The same questionnaires criterion for determining whether a given statisticalwere then re-entered by another person onto a sepa- model is compatible with the economic hypothesisrate spreadsheet. The two spreadsheets were com- of utility maximisation. Apart from this theoreticalpared and any discrepancies were corrected. advantage, such a difference model offers a practical
procedure for specifying the functional form of theAnalysis of Preference Data statistical model.
This study estimated WTP for all attributes byThe random effects probit model, readily availa-taking the marginal rates of substitution between theble on LIMDEP, was used to analyse the data.[33]
attribute ‘monthly cost of the drug’ and the remain-The indirect utility function is the maximum attaina-ing attributes. ‘Marginal rates of substitution’ de-ble utility given prices (p) and outlay (x). The inclu-scribes the rate at which people are willing to givesion of cost as an attribute in the utility function ψup units of one good in exchange for more units of(x,p) allows for the derivation of marginal WTP foranother good. Font[37] shows that for random utilityeach of the other attributes in line with economicmodels, such as those in DCEs, the compensatingtheory.[34]
variation (CV) [or difference in cost that compen-Assuming a linear additive function, the follow-
sates for the difference in the good] for a givening unconditional indirect utility function was esti-
change is the amount of CVti needed to leave themated for the WTP survey (equation 1):
individual indifferent between the original attributesstructure, vti (say option A) and the new structure v‘ti(say option B) [equation 3]:
v‘ti + CVti = vti
Δψ = �1(weightB − weightA) + �2(rashB − rashA) +
�3(concentrationB − concentrationA) + �4(hairlossB −hairlossA) + �5(seizureB − seizureA) + �6(costB − costA)
+ �7(sicknessB − sicknessA) + e + u(Eq. 3)
(Eq. 1)Because of the role the cost parameter plays in
which is equal to (equation 2): estimating CV, the coefficient on cost would beexpected to have a statistically significant (and neg-ative) impact on utility. Confidence intervals (CIs)for the welfare estimates were obtained by boot-
Δψ = �1Difweight + �2Difrash + �3Difconc +
�4Difhair + �5Difseiz + �6Difcost + �7Difsick + e + u
strapping from the multivariate normal distribution(Eq. 2)of coefficients and their variance-covariance ma-where Δψ is the change in utility in moving fromtrix.[33] The 95% CIs are the 2.5 and 97.5 percentileoption A to option B, where e is the unobservablevalues from the bootstrapped distribution.error term due to differences among observations,
and u is the unobservable error term due to differ- In addition to the standard aggregate model out-ence among respondents.[35] The units of the vari- lined in equation 1 and equation 2, segmented (sub-ables are as expressed in the questionnaire, so the group) analyses were performed to explore howunits of weight are pounds; units of cost are £, etc. preferences vary depending on socioeconomic fac-α1–6 represent the weights, or specifically prefer- tors. WTP values were explored for variations de-ence weights, that we are trying to estimate. In this pending on individuals’ income levels to test thesurvey, a difference model was estimated. theoretical validity of the model. Participants wereHanemann[36] notes that if a statistical binary re- asked to indicate their household income on a ten-
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

1174 Lloyd et al.
of sex. This analysis was exploratory and so nospecific hypotheses were tested. All segmentedanalyses were undertaken through the use of dummyvariables (for income level, seizure frequency,seizure type and sex). Wald tests of linear restric-tions were used to test whether differences betweenthe subgroups were statistically significant.
Results
In total, 148 usable questionnaires were returned,a response rate of 28%. The demographic and dis-ease-related characteristics of the sample arepresented in table II.
The median salary was approximately equivalentto that of the UK general population. However, thisis likely to represent an above-average earninggroup of people with epilepsy because of the knownsocioeconomic effects of epilepsy on people’s in-come. There was evidence of bimodal salary distri-bution showing that people were most likely to earn<£15 000 or >£50 000 per year.
Generally, participants in this survey had exper-ienced epilepsy for many years and had a broadexperience of different AEDs. The mean number ofdrugs reported in table II represents participants’
Table II. Demographic and disease-related information related tothe participants in the survey
Parameter Value
Number of participants 148
Female (%) 58
Mean age (years) 41.2
Proportion with children (%) 43
Mean number of children 1.56
Education (%)
no qualifications 7
school only (≤18 years) 44
vocational diploma 17
university degree or higher 32
Median salary range £20 000–25 000
Years since diagnosis 17.6
Type of epilepsy (%)
partial 21
partial with secondary generalisation 14
general tonic-clonic 52
other 13
Seizure frequency (%)
>1 per week 21
2–3 per month 12
1 per month 13
1 every 3–4 months 13
1–2 per year or less 41
Current medication to control seizures (%)
monotherapy 55
polytherapy (two drugs) 25
polytherapy (more than two drugs) 20current medication. Participants also reported howthey were familiar with different adverse effects.
point scale that varied from <£10 000 to >£50 000. Participants reported a high level of familiarity withIt was hypothesised that participants with a higher the adverse effects of AEDs, which suggests thatincome would be willing to pay more for unit im- people had well formed preferences regarding theprovements in attributes. The theoretical validity of adverse effects included in the DCE.the DCE model was tested by creating dummy vari- There were ten discrete choices per respondent,ables for three income groups: low, medium and which gave rise to 1480 observations in total. Ofhigh. these, however, there were 29 missing responses. In
Preferences for the attribute ‘seizure frequency’ addition to this, choice 6 was removed for all re-were explored according to participants’ actual spondents because this was a non-design consisten-seizure frequency and type of seizures experienced. cy check. Hence, the final analyses of the DCE dataData regarding actual seizure frequency (from >1 included 1303 observations. Of the 148 respondents,per week to ≤1–2 per year) and type of seizures were the consistency rate was 98% (145 of 148), i.e. 145recorded in the questionnaire. It was hypothesised out of 148 respondents answered the consistencythat participants who experienced more frequent check (choice set 6) correctly. This result demon-seizures would be willing to pay more for seizure strates a high level of understanding among studycontrol. Finally, preferences for adverse effects such respondents regarding the nature of the DCE exer-as weight gain and hair loss were explored in terms cise.
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

Preferences for Epilepsy Treatments 1175
Table III. Random effects probit model (148 individuals providing 1303 observations)a showing the influence of attributes on choice oftreatment: willingness to pay (WTP) data
Variable Coefficients (95% CI) SE p-Value WTP (£) per month perunit (95% CI)
Weight (lb) –0.0143134 (–0.0089, –0.0248) 0.002534 0.000 0.76 (0.47, 1.31)
Chance of skin rash (%) –0.04628796 (–0.0346, –0.0760) 0.007169 0.000 2.45 (1.83, 4.02)
Chance of concentration being –0.01070777 (–0.0034, –0.03185) 0.004491 0.006 0.57 (0.18, 1.68)affected (%)
Chance of hair loss (%) –0.050474203 (–0.0373, –0.0847) 0.006272 0.000 2.67 (1.97, 4.48)
Chance of reduction in seizure –0.010406686 (–0.00543, 0.002306 0.000 0.55 (0.29, 1.27)control (%) –0.02395)
Monthly cost to you (£) –0.0189126927 (–0.0109, –0.0487) 0.002978 0.000 NA
Chance of feeling sick (%) –0.012429432 (–0.00204, 0.003106 0.000 0.66 (0.11, 0.99)–0.01868)
a Log likelihood function –605.89, restricted log likelihood –605.97, chi squared 524.22, McFadden’s R2 0.3%, correct predictions76%.
NA = not applicable; SE = standard error.
Table III provides the results of the random ef- pay £0.76 per month for a treatment that caused 1lbfects probit model and the WTP results with 95% less weight gain and £2.45 per month for a 1%CIs. All the attribute coefficients have the expected reduction in the chance of developing a skin rash.sign (negative) and are all significant predictors of Based on the unit WTP values provided in tablechoice (as shown by the p-values). This indicates III, in table IV these values have been extrapolatedthat respondents were less likely to choose a scena- to a number of identifiable epileptic health states torio with higher weight gain, higher chance of rash, obtain absolute WTP values. Health state 1 ‘seizurehigher chance of concentration problems, higher freedom with no adverse effects’ is valued atchance of hair loss, poorer level of seizure control, £708.66 per month. These figures have been ob-higher chance of nausea or higher monthly cost. The tained by multiplying the unit WTP value from tablerandom effects model correctly predicted 76% of III and inflating it to the relevant value. For instance,participants’ choices. health state 1 reflects 100% seizure control and 0%
The unit WTP estimates provided in table III of all other adverse effects. The figure of £708.66 isreflect the mean value of a unit improvement in each obtained by summing the individual identified WTPattribute level. For example, people are willing to values for avoiding each of the adverse effects:
Table IV. Absolute willingness to pay (WTP) values for identified epileptic health states
No. Health state Absolute WTP value 95% CI (£)
(£ per month) lower upper
1 Seizure free with no adverse effects 709 451 1278
2 Seizure free with 13lb weight gain 679 433 1227
3 Seizure free with no weight gain 669 427 1210
4 Seizure free with hair loss 175 56 382
5 Seizure free with rash 219 84 474
6 Seizure free with sickness 577 429 1081
7 Seizure free with concentration reduced by 50% 680 442 1194
8 50% reduction in seizures with no adverse effects 681 437 1215
9 50% reduction in seizures with 13lb weight gain 671 431 1198
10 50% reduction in seizures with hair loss 147 42 319
11 50% reduction in seizures with rash 192 70 411
12 50% reduction in seizures with sickness 550 415 1017
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

1176 Lloyd et al.
higher income were willing to pay more for theirepilepsy treatments.
By comparing the mean WTP estimates with themean income levels, it is possible to estimate theproportion of their income that individuals would bewilling to part with each month in order to gainseizure freedom with no adverse effects. While theestimates are rather crude, this analysis suggests that
Table V. Extent of additional seizure control that participants arewilling to give up to improve units of adverse effects
Amount seizure control For unit improvement inwilling to give up adverse effects
1.37% seizure control 1lb reduction in weight gain
4.45% seizure control 1% reduction in risk of rash
1.03% seizure control 1% reduction in risk ofconcentration loss
4.85% seizure control 1% reduction in risk of hair loss
1.19% seizure control 1% reduction in risk of sicknesspeople would be willing to pay somewhere between34% to 42% of their household income for seizure
100% seizure freedom (100 × £0.55), no weight gain freedom with no adverse effects (i.e. full health).(26 × £0.76), 0% chance of rash (100 × £2.45), 0% This illustrates the value that people with epilepsychance of concentration loss (100 × £0.57), 0% place on gaining control over their illness.chance of hair loss (100 × £2.67) and 0% chance ofsickness (100 × £0.66). Similarly, the health state Segmented Model 2: Actual Seizure Frequency of‘seizure freedom with hair loss’ is estimated by Individuals/Reduction in Frequency of Seizuredetermining WTP for 100% seizure control and 0% Model 2 was segmented according to the actualon all other attributes apart from hair loss. This seizure frequency of individuals answering thehealth state was valued at £174.90 per month. questionnaire. The aim here was to explore whether
individuals’ preferences for the attribute ‘seizureImportance of Seizure Control and reduction’ were influenced by individuals’ actualAdverse Effects seizure frequency. A question in the survey asked
participants to estimate their actual seizure frequen-The DCE also allows us to explore whether par-cy and, for the segmented analysis, this was coded asticipants are willing to trade seizure control againstweekly, monthly or yearly. Participants experienc-improvements in adverse effects. In the DCE, par-ing seizures weekly had a WTP of £27 per month toticipants were presented with hypothetical drugavoid seizures, for those with monthly seizures thisprofiles that were all associated with 50%, 75% orfigure was £38, and for yearly seizures the WTP100% reduction in seizure frequency. This analysisamount was £89. The marginal effects for each ofindicated that, on average, participants were willingthe subgroups were compared using Wald tests ofto forego some improvements in seizure control inlinear restrictions. These tests revealed that thereorder to avoid adverse effects. Table V shows thewere significant differences between ‘seizure week-extent to which people were willing to trade im-ly’ to ‘seizure yearly’ and between ‘seizure month-provements in seizure control for unit changes inly’ and ‘seizure yearly’.adverse effects.
Examining the Influence of Other Variableson Preferences
Segmented Model 1: Testing the TheoreticalValidity of the Willingness-to-Pay EstimatesTable VI shows that WTP for improvements in
attribute levels increases as income levels increase.While these differences are not significant, the trendis in the a priori expected direction and providesevidence for the theoretical validity of the model.This analysis indicates that people who have a
Table VI. Segmented income model showing willingness to pay(WTP) for improvements in attribute levels, according to incomelevel
Attribute Segmented WTP values (£)
low medium highincome income income
Weight change 0.66 0.72 0.90
Skin rash 2.16 2.38 2.96
Concentration 0.61 0.67 0.83
Hair loss 2.39 2.64 3.28
Seizure frequency 0.56 0.61 0.76
Nausea/sickness 0.61 0.67 0.84
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

Preferences for Epilepsy Treatments 1177
Segmented Model 3: Type of Seizure/Reduction in month. For a 50% reduction in seizures accompa-Frequency of Seizure nied by nausea, people were still willing to paySegmented model 3 explored the impact on pref- £549. The values describe the relative importance of
erences for improvements in seizure frequency as a marginal changes in the unit of one attribute com-function of the type of seizures people currently pared with another, and the WTP values represent aexperience. Participants were broadly classified as useful metric for making such comparisons.follows: partial; partial with secondary generalisa-
The relatively high absolute WTP values ob-tion; and generalised tonic-clonic (grand mal)served in this study may be related to a number ofseizures. For the purposes of subgroup analyses,factors. A significant subgroup of our sample (15%)these seizures were re-categorised into partial andrecorded an annual income of over £50 000. Ourtonic-clonic. The results show that those with tonic-analyses also indicated that the richer participantsclonic seizures are willing to pay slightly more (£60were willing to pay more. However, there may beper month) to avoid seizures compared with thosesome other explanations for why the WTP valueswho predominantly experience partial seizures (£54were high. The survey was conducted with membersper month). While this result is what would beof the British general public (who also have a diag-expected a priori, the difference is not significant.nosis of epilepsy) and, as such, most participants
Segmented Model 4: Sex/Attributes will not have had direct experience of paying forModel 4 explored the impact of values for im- their medication. Most people with epilepsy in the
provements in ‘cosmetic’ attributes as a function of UK receive their medical care through the UK NHS,sex. These analyses show that preferences for im- which remains free at the point of contact. There-provements in hair loss and rash do not differ be- fore, people may not have fully comprehended thetween males and females; however, women have a consequences of having to pay for their medicationsignificantly higher WTP to avoid weight gain. (they may not comprehend the opportunity cost) andWomen’s valuations for avoiding weight gain the associated impact on their household expendi-(£0.99 per month to avoid a 1lb gain in weight) are ture. Instead, participants may have considered whatmore than double those of males (£0.45 per month). the change in drug profiles was worth, or what theThis result implies that weight gain is an important hypothetical value of it was, rather than what theyadverse effect of AEDs for women. would actually be willing to pay.
The WTP values expressed in this study wereDiscussion compared with values derived from studies in other
clinical areas. Unutzer et al.[38] reported that, forThe current study was designed to determine thedepression treatment, participants were willing toimportance of different attributes of AEDs to peoplepay $US270 ± 187 per month (year of value 2001)with epilepsy. The results of the study suggest thatfor a treatment that would eliminate their symptomspeople with epilepsy attach considerable importanceof depression. This was reported to be approximate-to the level and type of adverse effects they experi-ly 9% of the participants’ household income.ence. While participants valued changes in seizureLenert[39] reported that the mean WTP for an idealfrequency, they also attached significant value tomigraine remedy (i.e. one that was 100% effective,improvements in the adverse effect burden of AEDs.worked quickly and had no adverse effects) wasThe DCE indicated that participants were willing to$US130 per month (1999 values). Jacobs et al.[40]
pay substantial amounts per month in order toreported that Americans were willing to payachieve better control of their seizures and adverse$US2000 (2001 values) for the risk-free preventioneffects, indicating the value of reducing symptomsof hepatitis A.and adverse effects to epilepsy patients. For a treat-
A study from Norway also indicated the highment with 100% seizure control and avoidance of allvalue that patients with epilepsy place on a cure.[41]adverse effects, people were willing to pay £709 per
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

1178 Lloyd et al.
Stavem[41] reported a study of 57 people with epilep- seizure control may be lower than the importancesy who were asked to complete a contingent valua- they place on reducing weight gain or avoidingtion (WTP) survey, as well as interviews. The medi- nausea. This is an important finding because it sug-an WTP for a one-off payment for a total cure of gests that the preferences of people who rarely expe-their epilepsy was 150 000 Norwegian kroner rience seizures are probably quite different to those($US20 000 or £11 800 – year not stated but study of people who experience them commonly. For peo-published in 1999). This figure was equivalent to ple who experience infrequent seizures, it is likely47% of the annual household income. The only that they will place a greater emphasis on minimis-variable that predicted WTP was household income. ing adverse effects than patients who experienceWTP was not associated with participants’ values more frequent seizures. Given that up to 70% offor their current health state utility – as assessed patients become seizure free on monotherapy,using time trade-off, standard gamble and EQ-5D or choosing a treatment to match the patient’s prefer-15D. Stavem’s results are very similar to the find- ences is very important. Our survey showed thatings from the current study and reinforce the conclu- adverse effects such as hair loss and rash (with thesion that people with epilepsy place considerable potential serious consequences of Stevens-Johnsonvalue on the avoidance of the burden of epilepsy. syndrome) were of particular concern. It also
demonstrated that treatments with the potential forThe WTP figures in the current study thereforeweight gain were of much more concern to womenfall within the range of WTP values reported in thethan they were to men.literature and seem to highlight the importance of
the condition in the patient’s everyday life and the The finding that cosmetic adverse effects are ofdesire to avoid adverse effects associated with po- such importance to this group may be related totential treatment options. In our study, people with stigma. Stigma associated with epilepsy has beenepilepsy were willing to pay somewhere between well documented in the literature[42] and it is possi-34% and 42% of their household income to have the ble that treatments causing visible changes in a‘perfect’ AED and achieve seizure freedom without patient’s appearance may only increase this prob-adverse effects. lem. This survey demonstrated that a dialogue be-
tween patient and physician on the relative adverseThe study also demonstrated that people wereeffect profiles of different treatments is an importantwilling to trade seizure control against a better ad-aspect of prescribing decisions. A more satisfied andverse effect profile. Participants did not alwaysmotivated patient is likely to be more compliantchoose the option with the best level of seizurewith their prescribed treatment.control – a so-called dominant preference. The data
reported in table V indicate that people traded im- In our study, we expected that people with moreprovements in adverse effects against further gains frequent seizures would be willing to pay a higherin seizure control. This is an illustration of just how amount to achieve better seizure control than thoseimportant consideration of adverse effects is for with less frequent seizures, but this hypothesis wasparticipants. However, the finding should be consid- not substantiated by our analysis. The WTP resultsered within the context of the group of participants show that as seizures become less frequent, peoplerecruited into the study. are willing to pay more for unit improvements in
Table II indicates that the median seizure fre- seizure control. However, further analysis revealedquency for participants was one seizure every 3–4 a strong, significant correlation with reportedmonths. In the questionnaire, participants are asked seizure frequency and income levels. This correla-to imagine that the hypothetical add-on drugs would tion result is an important finding because it revealsreduce their seizures by 50%, 75% or 100%. There- that people with frequent seizures (weekly andfore, if people were experiencing relatively few monthly) have lower income levels than those withseizures, the importance of gaining additional infrequent seizures (yearly). This result implies that
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

Preferences for Epilepsy Treatments 1179
people’s productive lives, i.e. capacity to work and pages) and there was no direct incentive for theparticipant other than a £10 donation to Epilepsyearn income, are adversely affected by their epilep-Action™. Alternatively, people may have objectedsy. It is also possible that people with very infre-to answering questions regarding their health, in-quent seizures may place a high premium on mainte-come and medical care.nance of seizure control because of the potential loss
of a driving licence, which could impact on their Another potential limitation of this study is theindependence and employment status. Given the manner in which the DCE attributes were selected. Itcurrent sample size, it was not possible to further was not possible to select all or even most of theexplore the relationship between WTP for seizure different adverse effects that are associated withcontrol, actual seizure frequency and income. This AEDs. Therefore, we attempted to choose a repre-finding suggests that epilepsy patients with more sentative selection of attributes that included com-severe epilepsy suffer from inequity in terms of their mon non-health-threatening effects such as alopecia,income. When one considers that such patients also and potentially health-threatening effects such ashave lower quality of life,[17] higher healthcare weight gain and skin rash. The attribute skin rashcosts[43] and a greater chance of premature mortali- also made reference to the rare but life-threateningty,[44] it re-emphasises the devastating impact that condition Stevens-Johnson syndrome.this condition has on people. The choice sets were combined in the survey by
pairing them randomly and testing for any residualThere are limitations to this study that should becorrelation. A more efficient experimental designhighlighted. A convenience sample of participantscould be produced by pairing choice sets systemati-was recruited from among the membership of Epi-cally so as to maximise D-efficiency – which is alepsy Action™. The extent to which the participantsmeasure of statistical efficiency. It should also beare representative of epilepsy patients generally isnoted that the addition of a further consistencyunclear. Slightly more than half (58%) of the re-check may have been able to distinguish whether thespondents were women and most of the sample were2% inconsistency detected by the consistency testbetween the ages of 30 and 50 years. The age andwas due to random error or true inconsistency.sex of our sample was similar to a much larger
survey conducted with the same group.[45] The re- Finally, the risk attributes presented in the modelported breakdown of cases by type of seizure (e.g. were designed specifically to aid in respondents’partial seizure, generalised tonic-clonic) was very understanding of risk percentages and probabilities.similar to that reported previously in a similar sur- These risk data were then analysed on a continuumvey,[45] although compared with the general popula- assuming the respondents interpreted the levels astion our sample had a higher proportion of partici- such. However, further ongoing analysis aims topants with generalised tonic-clonic seizures.[20] The explore the sensitivity of the results when makingsample was derived from all areas of the UK and so the assumption that respondents interpreted the riskmay be more representative than a sample from, for levels in a more qualitative fashion.example, a specific neurology clinic. It would actu- Medical decisions regarding patient care shouldally be difficult to recruit a national sample of epi- incorporate the views or preferences of those pa-lepsy patients without going through a patient tients, and a DCE is one approach that has been usedgroup. Therefore, this approach represents an appro- as an accurate method of eliciting preferences. Anal-priate means of collecting national survey data from ysis of DCE data can also identify how preferencespatients. vary between important subgroups, which provides
It should also be mentioned that the response rate useful information in helping understand the impor-in this survey was quite low at 28%. This represents tance of various attributes of treatments. The prefer-only a modest response rate, but is not untypical of ence data emerging from this study indicate thatpostal surveys. The questionnaire was quite long (18 people with epilepsy are entirely able to make deci-
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

1180 Lloyd et al.
11. van der Pol M, Cairns JA. Estimating time preferences forsions regarding their own treatment. It also supportshealth using discrete choice experiments. Soc Sci Med 2001;
the case for entering into a shared decision-making 52: 1459-7012. van der Pol M, Cairns J. Establishing patient preferences forprocess between the doctor and patient. For some
blood transfusion support: an application of conjoint analysis.patients, their decision may be to relinquish treat- J Health Serv Res Policy 1998; 3 (2): 70-6ment decisions to their physician. However, for 13. Ratcliffe J, Buxton M. Patients’ preferences regarding the pro-
cess and outcomes of life saving technology: an application ofothers, shared decision making may enable them toconjoint analysis to liver transplantation. Int J Technol Assess
take greater control over their epilepsy and so lead to Health Care 1999; 15: 340-5114. Bryan S, Buxton M, Sheldon R, et al. Magnetic resonanceimprovements in their quality of life.
imaging for the investigation of knee injuries: an investigationof preferences. Health Econ 1998; 7 (7): 595-603
Conclusion 15. Ryan M, Scott DA, Reeves C. Eliciting public preferences forhealthcare: a systematic review of techniques. Health TechnolAssess 2001; 5 (5): 1-186This study indicates that people with epilepsy
16. Huber J, Zwerina K. The importance of utility balance inhave strong preferences for reducing adverse effects efficient choice designs. J Mark Res 1996; 33: 307-17as well as improving seizure control. These data 17. Baker GA, Jacoby A, Buck D, et al. Quality of life of people
with epilepsy: a European study. Epilepsia 1997; 38: 353-62may be considered usefully when making medical18. Berto P. Quality of life in patients with epilepsy and impact of
management decisions in epilepsy. treatments. Pharmacoeconomics 2002; 20 (15): 1039-5919. GlaxoSmithKline. Lamictal monograph, GlaxoSmithKline,
2001 [online]. Available from URL: http://us.gsk.com/prod-Acknowledgementsucts/assets/us_lamictal.pdf [Accessed 2005 Sep 15]
20. Hart YM, Shorvon SD. The nature of epilepsy in the generalThis work was supported by Janssen-Cilag UK Ltd. There population II: medical care. Epilepsy Res 1995; 21: 51-8
are no other conflicts of interest. Andrew Lloyd was the 21. Novartis Pharmaceuticals. Tegretol® (carbamazepine) prescrib-principal investigator on this study and was the primary ing information, Novartis Pharmaceuticals, 1999 [online].
Available from URL: http://www.pharma.us.novartis.com/author of the manuscript. Emma McIntosh advised on theproduct/pi/pdf/tegretol.pdf [Accessed 2005 Sep 15]correct approach to the methodology, produced the orthogo-
22. Froberg DG, Kane RL. Methodology for measuring health-statenal design, completed all of the statistical analyses and au-preferences: I. measurement strategies. J Clin Epidemiol 1989;thored much of the paper. Martin Price had the original idea 42: 345-54
for the study, fed into the design of the study including 23. Ryan M. Using conjoint analysis to take account of patientselection of attributes and interpretation of results and wrote preferences and go beyond health outcomes: an application toparts of the manuscript. in vitro fertilisation. Soc Sci Med 1999 Feb; 48 (4): 535-46
24. Bradley M. User’s manual for SPEED v 2.1 The Hague: HagueConsulting Group, 1991
25. Gigerenzer G. Reckoning with risk: learning to live with uncer-Referencestainty. London: Penguin Books, 20021. Feely M. Drug treatment of epilepsy. BMJ 1999; 318: 106-9
26. Slovic P, editor. The perception of risk. London: Earthscan2. Mattson RH. Efficacy and adverse effects of established andPublications Ltd, 2000new antiepileptic drugs. Epilepsia 1995; 36 Suppl. 2: S13-26
27. Entwistle V, Watt I, Davis H, et al. Developing information3. Swann AC. Major system toxicities and side effects of anticon-materials to present the findings of technology assessments tovulsants. J Clin Psychiatry 2001; 62 Suppl. 14: 16-21consumers. Int J Technol Assess Health Care 1998; 14 (1):4. Matsuo F, Bergen D, Faught E, et al. Placebo-controlled study47-70of the efficacy and safety of lamotrigine in patients with partial
seizures. Neurology 1993; 43: 2284-91 28. Bennet P, Calman K. Risk communication and public health.Oxford, UK: Oxford University Press, 19995. Mercke Y, Sheng H, Khan T, et al. Hair loss in
psychopharmacology. Ann Clin Psychiatry 2000; 12 (1): 35-42 29. Gigerenzer G, Hoffrage U. How to improve Bayesian reasoningwithout instructions: frequency formats. Psychol Rev 1995;6. Strakowski SM, DelBello MP, Adler CM. Comparative efficacy98: 506-28and tolerability of drug treatments for bipolar disorder. CNS
Drugs 2001; 15 (9): 701-18 30. Reyna V, Brainerd C. Fuzzy-trace theory and framing effects in7. Greenwood RS. Adverse effects of antiepileptic drugs. Epilep- choice: gist extraction, truncation and conversion. J Behav
sia 2000; 41 Suppl. 2: S42-52 Decis Making 1991; 4: 249-628. Arroyo S, de la Morena A. Life-threatening adverse events of 31. Reyna V, Brainerd C. Fuzzy-trace theory: an interim synthesis:
antiepileptic drugs. Epilepsy Res 2001; 47: 155-74 learning and individual differences. Learn Individ Differ 1995;7: 1-759. Coulter A, Entwistle V, Gilbert D. Sharing decisions with
patients: is the information good enough? BMJ 1999; 318: 32. Reyna V, Lloyd F, Brainerd C. Memory, development and318-22 rationality: an integrative theory of judgment and decision-
10. Holmes-Rovner M, Llewellyn-Thomas H, Entwistle V, et al. making. In: Schneider S, Shanteau J, editors. Emerging per-Patient choice modules for summaries of clinical effective- spectives in judgment and decision making. Mahwah (NJ):ness: a proposal. BMJ 2001; 322: 664-7 Erlbaum, 2001
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)

Preferences for Epilepsy Treatments 1181
33. Green W. LIMDEP Version 8, Users Manual. Econometric 41. Stavem K. Willingness to pay: a feasible method for assessingSoftware Inc, 1998 treatment benefits in epilepsy? Seizure 1999; 8: 14-9
34. Roe B, Boyle KJ, Teisl MF. Using conjoint analysis to derive 42. Jacoby A, Snape D, Baker GA. Epilepsy and social identity: theestimates of compensating variation. J Environ Econ Manage
stigma of a chronic neurological disorder. Lancet Neurol 2005;1996; 31: 145-94: 171-835. Manski CF. The structure of random utility models. Theory
43. Jacoby A, Buck D, Baker G, et al. Uptake and costs of care forDecis 1977; 8: 229-54epilepsy: findings from a UK regional study. Epilepsia 1998;36. Hanemann WM. Welfare evaluations in contingent valuation
experiments with discrete responses. Am J Agric Econ 1984; 39: 776-8666: 332-41 44. Remak E, Hutton J, Peeters K, et al. Estimated impact of seizure
37. Font AR. Mass tourism and the demand for protected naturalfrequency on survival in epilepsy. Association of British Neu-
areas: a travel cost approach. J Environ Econ Manage 2000;rologists Spring Scientific Meeting April 2-4, 2003; Cardiff,39: 97-116Wales, UK38. Unutzer J, Katon WJ, Russo J, et al. Willingness to pay for
depression treatment in primary care. Psychiatr Serv 2003 45. British Epilepsy Association. The treatment of epilepsy: a pa-Mar; 54 (3): 340-5 tient’s viewpoint. Leeds: British Epilepsy Association, 1996.
39. Lenert LA. Use of willingness to pay to study values forpharmacotherapies for migraine headache. Pharmacoeco-nomics 2002; 20 (11): 739-47 Correspondence and offprints: Dr Andrew Lloyd, The
40. Jacobs RJ, Moleski RJ, Meyerhoff AS. Valuation of sympto- MEDTAP Institute at UBC, 20 Bloomsbury Square,matic hepatitis A in adults: estimates based on time trade-off
London, WC1A 2NS, UK.and willingness-to-pay measurement. Med Care 2003 Feb; 41E-mail: [email protected](2): 299-308
© 2005 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2005; 23 (11)