Embed Size (px)
Citation preview
Research in Developmental Disabilities 34 (2013) 730–738
Contents lists available at SciVerse ScienceDirect
Research in Developmental Disabilities
The impact of staff initiated referral and intervention protocols onsymptoms of depression in people with mild intellectual disability
Jane A. McGillivray *, Mavis M. Kershaw
School of Psychology, Deakin University, 221 Burwood Highway, Burwood, Victoria 3125, Australia
A R T I C L E I N F O
Article history:
Received 9 September 2012
Received in revised form 6 November 2012
Accepted 6 November 2012
Available online 5 December 2012
Keywords:
Intellectual disability (ID)
Depression
Primary health care
Staff-administered intervention pro-
gramme
A B S T R A C T
It has been estimated that people with ID experience the same and possibly higher levels of
depression than the general population. Referral to a General Medical Practitioner (GP) for
primary care is recommended practice for people with depression and cognitive
behavioural (CB) therapy is now an accepted evidence based intervention. A growing
body of literature indicates that people with ID and depression may benefit from CB
strategies. The aim of the current study was to compare (i) CB group intervention
strategies with referral to a GP; (ii) CB group intervention strategies only; and (iii) referral
to a GP only on symptoms of depression among people with mild ID. Staff from six
participating agencies received training in (a) how to identify and screen individuals with
mild ID for depressive symptoms and risk factors for depression, and (b) supportive
referral of identified individuals to GPs for mental health services. In addition, staff from
four of the agencies undertook (c) training on how to deliver group CB intervention
strategies. Eighty-two participants were allocated to one of the three intervention groups.
Depressive symptoms and negative automatic thoughts were assessed prior to the
intervention, at the conclusion of the intervention, and at eight months follow-up.
Compared to GP referral alone, those participants who received CB strategies both with
and without GP referral displayed significant reductions in depressive symptoms. The use
of CB strategies only also resulted in a significant reduction in frequency of negative
automatic thoughts. The findings of this study support routine screening of individuals
with mild ID for depression and the delivery of group CB intervention programmes by
trained staff within community-based disability agencies.
� 2012 Elsevier Ltd. All rights reserved.
It is generally recognised that people with intellectual disability (ID) are more likely to experience mental healthdisorders than the general population (Gibbs, Brown, & Muir, 2008; Lowry, 1998; Morin, Cobigo, Rivard, & Lepine, 2010;Moss, 2001). It has also been reported that people with ID have the same, if not higher, levels of depression than the generalpopulation (Smiley & Cooper, 2003). Prevalence estimates among adults with ID range from 2.2% to 8.9% (Cooper, Smiley,Morrison, Williamson, & Allan, 2007; Davis, Judd, & Herrman, 1997; Deb, Thomas, & Bright, 2001; White, Chant, Edwards,Townsend, & Waghorn, 2005) with reported rates likely to be an underestimate due to difficulties associated with detectionand diagnosis (Antonacci & Attiah, 2008; Kerker, Owens, Zigler, & Horwitz, 2004; McBrien, 2003; Perez-Achiaga, Nelson, &Hassiotis, 2009).
A number of life circumstances place people with ID at particular risk of developing mental health problems, includingdepression. Factors such as poverty, unemployment, impoverished social support and exclusion from social and community
* Corresponding author. Tel.: +61 3 9244 6426; fax: +61 3 9244 6858.
E-mail address: [email protected] (J.A. McGillivray).
0891-4222/$ – see front matter � 2012 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.ridd.2012.11.005

J.A. McGillivray, M.M. Kershaw / Research in Developmental Disabilities 34 (2013) 730–738 731
participation, family stress, and abuse are associated with poor mental health (Dagnan & Jahoda, 2006; Emerson, Hatton,Felce, & Murphy, 2001; Hastings, Hatton, Taylor, & Maddison, 2004; Lunsky & Benson, 2001; McGillivray & McCabe, 2007;Rose & Gerson, 2009). Furthermore, reduced psychological resources and cognitive abilities may render individuals with IDless able to adequately cope with adverse life events (van den Hout, Arntz, & Merckelbach, 2000). Individuals with mild IDmay be particularly vulnerable due to awareness of their plight. These vulnerabilities provide a strong rationale for the earlyidentification and treatment of those individuals at risk (McGillivray & McCabe, 2007).
There is some debate as to the treatment of choice for depression among people with ID. Treatment is commonlypharmacological, although there is relatively little research into the efficacy of antidepressant use in people with ID(Antonacci & Attiah, 2008; Sturmey, 2004) and findings remain equivocal. In a review of the treatment of mood disorders inadults with developmental disabilities, Antonacci and Attiah (2008) concluded that there is little evidence to support the useof antidepressants in the treatment of mood disorders among this population. However, a recent retrospective case-noteanalysis of 221 people with ID prescribed antidepressants for depression, generalised anxiety disorder, and obsessivecompulsive disorder found that approximately half of the sample demonstrated clinical improvement (Rai & Kerr, 2010).Given the ongoing debate around pharmacological efficacy in this population, it is prudent to consider other treatmentapproaches.
There is a growing body of literature indicating that people with ID and depression may benefit from cognitivebehavioural (CB) strategies (Dagnan & Chadwick, 1997; Ghafoori, Ratanasiripong, & Holladay, 2010; Lindsay, Howells, &Pitcaithly, 1993; Rose, West, & Clifford, 2000). While there is less research concerning the efficacy of CB strategies amongpeople with ID in comparison to the general population (Beail, 2003; Hatton, 2002; Willner, 2005), when appropriatelyadapted, CB interventions appear helpful for people with mild ID experiencing a range of mental health problems (Hatton,2002). In this population, we have demonstrated a reduction in depressive symptoms following participation in CB grouptreatment programmes and these positive effects were sustained over time (McCabe, McGillivray, & Newton, 2006;McGillivray & McCabe, 2007; McGillivray, McCabe, & Kershaw, 2008). The findings of a more recent study by Ghafoori et al.(2010) provide further support for a structured CB group treatment approach for individuals with mild-borderline ID whohave depression. In this study, levels of depression in participants significantly decreased post-treatment, althoughimprovements were not maintained at 4-month follow-up. There is also initial evidence that staff in disability agencies canbe trained to effectively deliver CB group programmes to individuals with symptoms of depression (McGillivray et al., 2008).Although these findings are promising, there remains a need for further examination of interventions and particularly howbest to facilitate access to depression treatment for this population.
In the Australian context, primary mental health care is provided by General Practitioners (GPs) who may refer theirpatients to mental health specialists, such as psychologists or psychiatrists. There are indications, however, that manyindividuals with ID who exhibit symptoms of depression are not diagnosed by their GP and do not receive appropriatemental health services (McGillivray & McCabe, 2007). It appears that access to general health care by people with ID is poorerthan their non-disabled counterparts (Krahn, Hammond, & Turner, 2006; Ruddick, 2005; Webb & Rogers, 2002). A number ofbarriers have been identified, such as the absence of reliable and valid measures to explore health in people with ID, thepotential for communication difficulties between the GP and the patient (Ruddick, 2005), as well as their lack of knowledgeand experience with people with ID (Millar, Chorlton, & Lennox, 2004; Phillips, Morrison, & Davis, 2004). These barriers alsoapply to mental health care (Phillips et al., 2004), with the addition of barriers related to a lack of understanding of mentalhealth risks, presentations and treatment options for people with ID (Deb et al., 2001). As such, there is a strong need formore effective methods of detecting depression and more efficient pathways of care for this population.
Disability support staff are well-placed to identify and assist individuals with mild ID who are experiencing depressivesymptoms and may play a key role in either facilitating access to mental health care, or directly providing interventionstrategies. In previous research, we have investigated the views of key stakeholders (including support workers, caregivers,and health professionals) about the perceived risk factors and characteristics of depression among people with mild ID, aswell as the intervention needs of this population (McGillivray & McCabe, 2010). A key obstacle identified was the lack of stafftrained to undertake screening and assessment of depression and to provide support and basic prevention/interventionprogrammes to individuals with ID.
Screening of people with ID who may be at-risk of depression is essential in order to ascertain individuals in need ofreferral or intervention. Screening does not require specific expertise and can be undertaken by minimally trained supportstaff (Hermans & Evenhuis, 2010). The benefits of clinicians working collaboratively with support staff in order to gatheraccurate diagnostic information about individuals with ID has been emphasised (Hurley, 2008). However, barriers to thisprocess have also been identified. These include lack of knowledge about mental health concerns among caregivers(Borthwick-Duffy & Eyman, 1990), inadequate provision of mental health training for professional caregivers, and negativeattitudes held by caregivers towards mental health services for individuals with mental health concerns (Edelstein &Glenwick, 2001). However, knowledge and attitudes of support staff may be enhanced through training (Costello, Hardy,Tsakanikos, & McCarthy, 2010).
The primary aim of the current study was to compare the impact (immediate and follow-up) of three interventionoptions: (i) staff administered group CB intervention strategies with referral to a GP; (ii) staff administered CB groupintervention strategies only; and (iii) staff initiated referral to a GP only, on symptoms of depression among people with mildID. A secondary aim was to evaluate the extent to which staffs were able to identify and screen individuals at risk for, ordemonstrating symptoms of depression.
J.A. McGillivray, M.M. Kershaw / Research in Developmental Disabilities 34 (2013) 730–738732
1. Method
1.1. Participants
Participants were 82 adults (47 males, 35 females) aged 18–65 (M = 37) with mild intellectual disability (IQ: 50–55 toapproximately 70 as assessed with a standardised test of intelligence and with associated deficits in adaptive behaviour,evident during the developmental period) who lived in the community and attended one of six of the pre-vocational trainingand employment services for people with disabilities in Victoria, Australia. In order to access funded ID services, individualsneed to have been formally assessed as having an intellectual disability by a registered clinical psychologist. Agency staffprovided confirmation via client records of participants’ diagnoses of mild ID. Fourteen volunteer staff members who hadbeen trained in the detection of depression and associated risk factors in adults with mild ID identified prospectiveparticipants to be invited into the study. Staff confirmed that these individuals showed indications of risk for depression, andhad the necessary language and comprehension skills required for participation in the study. Eighty-four individualsconsented to be formally screened for symptoms of depression using a staff administered checklist as a prerequisite toinclusion in the study. Of the people screened, two people did not meet the inclusion criteria (i.e., >4 symptoms on thedepression screening checklist).
1.2. Materials
1.2.1. Assessment schedules
1.2.1.1. Demographic characteristics. Participants were asked to provide their gender, age, and their current and past state ofphysical health, medication use and specifically whether they were taking antidepressant medication. They were also askedabout their current living situation, the frequency of family and social contact, and the frequency with which they engaged inrecreational activities.
1.2.1.2. Beck depression inventory II (BDI-II) (Beck, Steer, & Brown, 1996). The BDI-II is a 21-item self-report scale designed toassess severity of depression symptoms corresponding to the American Psychiatric Association’s Diagnostic and Statistical
Manual of Mental Disorders – Fourth Edition (American Psychiatric Association, 1994). Each item consists of 4 statements fromwhich the respondent is asked to select the item that best represents his/her current mood over the last two weeks. It hasadequate sensitivity and specificity to be used as a screening tool to identify individuals with ID who required a referral fortreatment (Ailey, 2009). In the current study, Cronbach’s alpha for the 20 items BDI-II was 0.87.
1.2.1.3. Automatic thoughts questionnaire – revised (Kendall, Howard, & Hays, 1989). The ATQ-R consists of 40 itemsthat measure the frequency of automatic negative statements about the self. Fifteen of the most relevant items wereused in this study. For ease of responding, each item was reduced to a 3-point Likert scale where 1 = ‘not at all’,2 = ‘sometimes’, and 3 = ‘frequently’. Participants were asked to rate the 15 items for frequency of occurrence during theprevious week, with a greater score indicating more negative thinking. The ATQ has been effectively used as anassessment tool with ID populations in a number of studies (Esbensen & Benson, 2005; Glenn, Bihm, & Lammers, 2003;Nezu, Nezu, Rothenberg, DelliCarpini, & Groag, 1995). In the present study, the Cronbach’s alpha for the modified ATQ-Rwas 0.85.
1.2.1.4. Depression screening checklist. This informant checklist was developed for this study to assist staff members to detectdepressive symptoms/risk factors in people with mild ID. It comprises 22 items grouped into the following categories ofbehaviour: mood, activities, sleeping and eating, and physical signs/concentration/decision-making. Respondents areasked to indicate the presence of each item as observed in the person they are assessing. The checklist was trialled withsix staff members in two different agencies providing services to people with intellectual disability, prior tocommencing the study. In consultation with staff, and in order to promote early identification of individuals at risk, aminimum criteria of 4 checked items, including at least one mood item and/or one activities item, was set for inclusionin the study.
1.2.2. Referral protocol
A supportive referral protocol was developed for use by agency staff. The protocol recommended that staff membersrefer to a GP those clients who met four or more criteria on the depression screening checklist. To ensure that peoplewith ID did not feel pressured to accept the referral to see a GP staff were asked to use an informal suggestion, such as, ‘‘Inotice that you have been feeling rather down recently, and do not seem to have been enjoying your usual activities. . . itmight be a good idea to talk to your doctor about this. If you would like to do so I would be happy to help you organisethis.’’ It was made clear to staff that they were to provide a recommendation only and that it was the decision of theindividual as to whether they consulted their GP. Staff members were asked to follow-up with their client one weeklater and offer assistance in the form of use of telephone, making an appointment, and attending their appointment withtheir GP if they so wished.

J.A. McGillivray, M.M. Kershaw / Research in Developmental Disabilities 34 (2013) 730–738 733
1.2.3. Cognitive behavioural intervention programme
The ‘Think happy, Feel happy, Be happy’ group programme comprises CB strategies and is designed to be conducted over a12-week period, in 1.5 h weekly sessions. Materials used in the creation of the programme were adapted from varioussources (Infrapsych CBT program for depression; Lindsay et al., 1993; Moodgym Training Program; Stenfert Kroese, Dagnan,& Konstantinos, 1997). These materials were adapted for use with adults with mild ID with exercises and handoutsconceptually simplified and presented in plain English. The programme comprises three modules. The first module focuseson feelings. The general aim of this module is to provide group members with a comfortable environment in which they feelsafe enough to discuss personal issues, and to derive an understanding of what depressive symptoms are and why they havebeen selected to participate in the group. Other aims include enabling group members to understand how behaviour impactson feelings, and how to improve ability to cope with stress. Module two focuses on thoughts. The aim of this module is tointroduce the CB concept, to provide group members with the opportunity to practice identifying thoughts, and to teachmembers to reduce negative thoughts. Module three focuses on social interactions, improving social skills (e.g., making andmaintaining friends) and communication skills (e.g., recognising different styles of communication, appropriate use of bodylanguage) as well as communicating assertively.
1.3. Procedure
The first phase of this project involved the development and trial of a checklist for use by staff in detecting depressivesymptoms and risk factors for depression in people with mild ID and the development of a supportive referral protocol toenable staff to refer the individuals they identified as having depressive symptoms/risk factors for depression to GPs formental health services. Volunteer staff from participating vocational and community based agencies providing services toadults with mild ID then received training in (a) how to screen individuals with mild ID for depressive symptoms, and (b)supportive referral of individuals with symptoms of depression to GPs for mental health services. In addition, staff membersfrom four of the agencies were provided with (c) training on how to deliver the CB intervention strategies.
Through an informed consent process, staff members from six participating agencies recruited and screened people withmild ID for symptoms of depression using the depression screening checklist. Those individuals identified by staff as havingdepressive symptoms or risk factors for depression were then assigned to one of three groups: (1) staff-administered groupCB intervention together with a staff-initiated referral to a GP (n = 32); (2) staff-administered group CB strategies only(n = 24); and (3) referral to a GP only (n = 26). Participants comprising the three groups were comparable on key variables butwere recruited from different agencies to minimise confounding of intervention protocols. Participants were allocated to theintervention type based on the basis of the agency they attended. Participants were allocated to particular groups withintheir agency on the basis of the advice from staff about people who worked well together and in the interests of intra-groupdynamics. Each of the CB groups was comprised of 6 or 7 individuals.
To examine the efficacy of the three intervention options, participants were independently assessed on measures ofdepressive symptoms and automatic negative thoughts by a fully registered psychologist with clinical training andlongstanding experience in assessing individuals with intellectual and developmental disabilities. These assessments wereundertaken prior to the intervention (pre-test), at the conclusion of the intervention (post-test) and eight months later(follow-up test). Participants who were referred to GPs for mental health care were monitored over time to determinereferral pathways and outcomes.
2. Results
2.1. Demographic characteristics
The majority of participants (n = 32) lived with their parents or family (39%). Twenty-eight (34%) lived in supportedaccommodation, and 19 (23%) lived independently. Forty-six participants (56%) said they had regular contact with familymembers, 26 (32%) had some contact with family members, and 10 people (12%) said they had no family contact. Mostparticipants (n = 46) reported that they engaged in one to two activities per week (56%), fourteen (17%) reported taking partin three or more recreational activities per week, and 22 participants (27%) reported that they did not take part in anyrecreational activities. At pre-test, 18 participants (22%) reported taking antidepressant medication and 25 participants(31%) reported taking at least one prescribed medication other than antidepressants. Thirty-nine participants (46%) were nottaking any prescribed medication prior to the commencement of the study.
2.2. Range of depressive symptoms at pre-test
Based on the recommended cut-off scores on the BDI-II for depressive symptoms in the normal population (Beck et al.,1996), 34 of the total sample of participants (41%) were in the minimally depressed range; 15 participants (19%) were in themildly depressed range; 15 participants (19%) were in the moderately depressed range; and 18 participants (21%) were in theseverely depressed range. Ten people in the ‘CB group intervention with referral to a GP’ group, three people in the ‘CB groupintervention only’ group, and seven people in the ‘referral to a GP only’ group, reported taking antidepressant medication atpre-test.
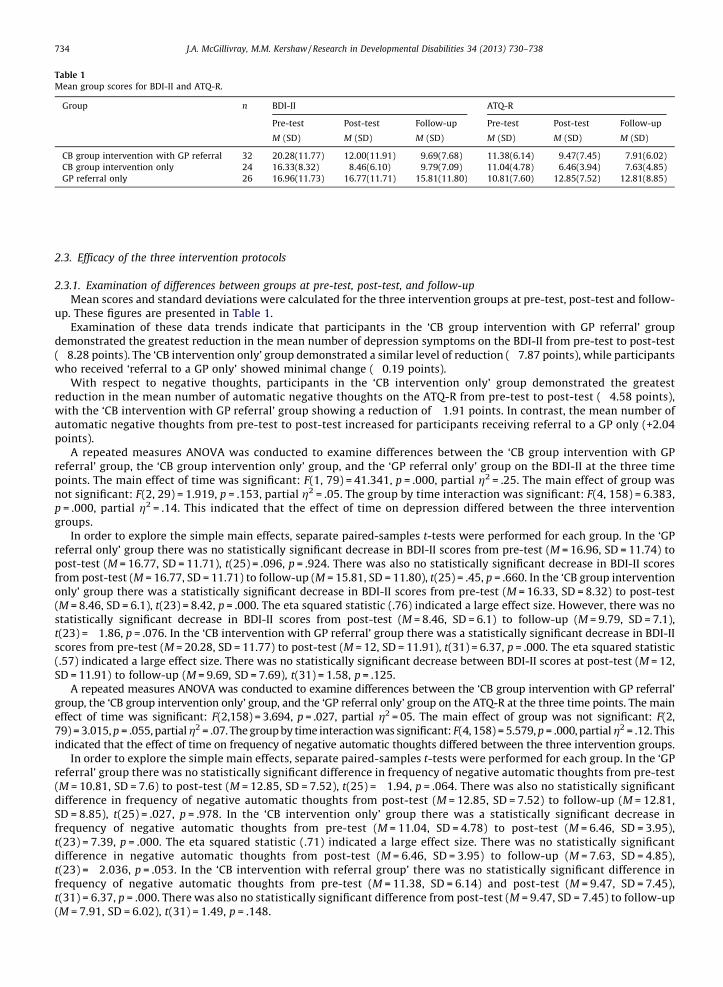
Table 1
Mean group scores for BDI-II and ATQ-R.
Group n BDI-II ATQ-R
Pre-test Post-test Follow-up Pre-test Post-test Follow-up
M (SD) M (SD) M (SD) M (SD) M (SD) M (SD)
CB group intervention with GP referral 32 20.28(11.77) 12.00(11.91) 9.69(7.68) 11.38(6.14) 9.47(7.45) 7.91(6.02)
CB group intervention only 24 16.33(8.32) 8.46(6.10) 9.79(7.09) 11.04(4.78) 6.46(3.94) 7.63(4.85)
GP referral only 26 16.96(11.73) 16.77(11.71) 15.81(11.80) 10.81(7.60) 12.85(7.52) 12.81(8.85)
J.A. McGillivray, M.M. Kershaw / Research in Developmental Disabilities 34 (2013) 730–738734
2.3. Efficacy of the three intervention protocols
2.3.1. Examination of differences between groups at pre-test, post-test, and follow-up
Mean scores and standard deviations were calculated for the three intervention groups at pre-test, post-test and follow-up. These figures are presented in Table 1.
Examination of these data trends indicate that participants in the ‘CB group intervention with GP referral’ groupdemonstrated the greatest reduction in the mean number of depression symptoms on the BDI-II from pre-test to post-test(�8.28 points). The ‘CB intervention only’ group demonstrated a similar level of reduction (�7.87 points), while participantswho received ‘referral to a GP only’ showed minimal change (�0.19 points).
With respect to negative thoughts, participants in the ‘CB intervention only’ group demonstrated the greatestreduction in the mean number of automatic negative thoughts on the ATQ-R from pre-test to post-test (�4.58 points),with the ‘CB intervention with GP referral’ group showing a reduction of �1.91 points. In contrast, the mean number ofautomatic negative thoughts from pre-test to post-test increased for participants receiving referral to a GP only (+2.04points).
A repeated measures ANOVA was conducted to examine differences between the ‘CB group intervention with GPreferral’ group, the ‘CB group intervention only’ group, and the ‘GP referral only’ group on the BDI-II at the three timepoints. The main effect of time was significant: F(1, 79) = 41.341, p = .000, partial h2 = .25. The main effect of group wasnot significant: F(2, 29) = 1.919, p = .153, partial h2 = .05. The group by time interaction was significant: F(4, 158) = 6.383,p = .000, partial h2 = .14. This indicated that the effect of time on depression differed between the three interventiongroups.
In order to explore the simple main effects, separate paired-samples t-tests were performed for each group. In the ‘GPreferral only’ group there was no statistically significant decrease in BDI-II scores from pre-test (M = 16.96, SD = 11.74) topost-test (M = 16.77, SD = 11.71), t(25) = .096, p = .924. There was also no statistically significant decrease in BDI-II scoresfrom post-test (M = 16.77, SD = 11.71) to follow-up (M = 15.81, SD = 11.80), t(25) = .45, p = .660. In the ‘CB group interventiononly’ group there was a statistically significant decrease in BDI-II scores from pre-test (M = 16.33, SD = 8.32) to post-test(M = 8.46, SD = 6.1), t(23) = 8.42, p = .000. The eta squared statistic (.76) indicated a large effect size. However, there was nostatistically significant decrease in BDI-II scores from post-test (M = 8.46, SD = 6.1) to follow-up (M = 9.79, SD = 7.1),t(23) = �1.86, p = .076. In the ‘CB intervention with GP referral’ group there was a statistically significant decrease in BDI-IIscores from pre-test (M = 20.28, SD = 11.77) to post-test (M = 12, SD = 11.91), t(31) = 6.37, p = .000. The eta squared statistic(.57) indicated a large effect size. There was no statistically significant decrease between BDI-II scores at post-test (M = 12,SD = 11.91) to follow-up (M = 9.69, SD = 7.69), t(31) = 1.58, p = .125.
A repeated measures ANOVA was conducted to examine differences between the ‘CB group intervention with GP referral’group, the ‘CB group intervention only’ group, and the ‘GP referral only’ group on the ATQ-R at the three time points. The maineffect of time was significant: F(2,158) = 3.694, p = .027, partial h2 = 05. The main effect of group was not significant: F(2,79) = 3.015, p = .055, partial h2 = .07. The group by time interaction was significant: F(4, 158) = 5.579, p = .000, partial h2 = .12. Thisindicated that the effect of time on frequency of negative automatic thoughts differed between the three intervention groups.
In order to explore the simple main effects, separate paired-samples t-tests were performed for each group. In the ‘GPreferral’ group there was no statistically significant difference in frequency of negative automatic thoughts from pre-test(M = 10.81, SD = 7.6) to post-test (M = 12.85, SD = 7.52), t(25) = �1.94, p = .064. There was also no statistically significantdifference in frequency of negative automatic thoughts from post-test (M = 12.85, SD = 7.52) to follow-up (M = 12.81,SD = 8.85), t(25) = .027, p = .978. In the ‘CB intervention only’ group there was a statistically significant decrease infrequency of negative automatic thoughts from pre-test (M = 11.04, SD = 4.78) to post-test (M = 6.46, SD = 3.95),t(23) = 7.39, p = .000. The eta squared statistic (.71) indicated a large effect size. There was no statistically significantdifference in negative automatic thoughts from post-test (M = 6.46, SD = 3.95) to follow-up (M = 7.63, SD = 4.85),t(23) = �2.036, p = .053. In the ‘CB intervention with referral group’ there was no statistically significant difference infrequency of negative automatic thoughts from pre-test (M = 11.38, SD = 6.14) and post-test (M = 9.47, SD = 7.45),t(31) = 6.37, p = .000. There was also no statistically significant difference from post-test (M = 9.47, SD = 7.45) to follow-up(M = 7.91, SD = 6.02), t(31) = 1.49, p = .148.
J.A. McGillivray, M.M. Kershaw / Research in Developmental Disabilities 34 (2013) 730–738 735
2.4. Clinical significance of change in individual scores on the BDI-II at pre-test, post-test and follow-up
To determine clinically meaningful change in scores on the BDI-II, individual scores for symptoms of depression wereexamined at pre-test, post-test and follow-up using the cut off score (0–13 = minimal depression) recommended by Becket al. (1996). The results for each intervention group are presented below.
‘CB group intervention with GP referral’ group: at pre-test, 63% (n = 20) of the 32 participants in this group scored >13 onthe BDI-II. At post-test, 40% (n = 8) of these participants had improved (scored <13 on the BDI-II) with 88% (n = 7) of theseparticipants continuing to score <13 at follow-up.
‘CB group intervention only’ group: at pre-test, 67% (n = 16) of the 24 participants in this group scored >13 on the BDI-II.At post-test, 75% (n = 12) of these participants had improved (<13 on BDI-II) with 83% (n = 10) continuing to score <13 atfollow-up.
‘GP referral only’ group: at pre-test, 50% (n = 12) of the 24 participants in this group scored >13 on the BDI-II. However, atpost-test only 25% (n = 3) of these participants had improved (<13 on BDI-II). At follow-up all three participants had revertedto scoring >13 on the BDI-II.
With respect to overall improvement (i.e., any reduction in BDI-II score from pre-test to post-test), the results alsoindicated that 100% (n = 24) in the ‘CB group intervention only’ group, 91% (n = 29) in the ‘CB group intervention with GPreferral’ group and 54% (n = 14) in the ‘GP referral only’ group, improved on BDI-II scores at post-test. From post-test tofollow-up, 21% (n = 5) in the ‘CB group intervention only’ group, 44% (n = 14) in the ‘CB group intervention with GP referral’group and 46% (n = 12) in the ‘GP referral only’ group improved on BDI-II scores from post-test to follow-up.
2.5. Effectiveness of referral pathways and intervention outcomes
Participants were tracked over time to ascertain referral pathways and evaluate the effectiveness of the referral process.
2.5.1. Referral to GP
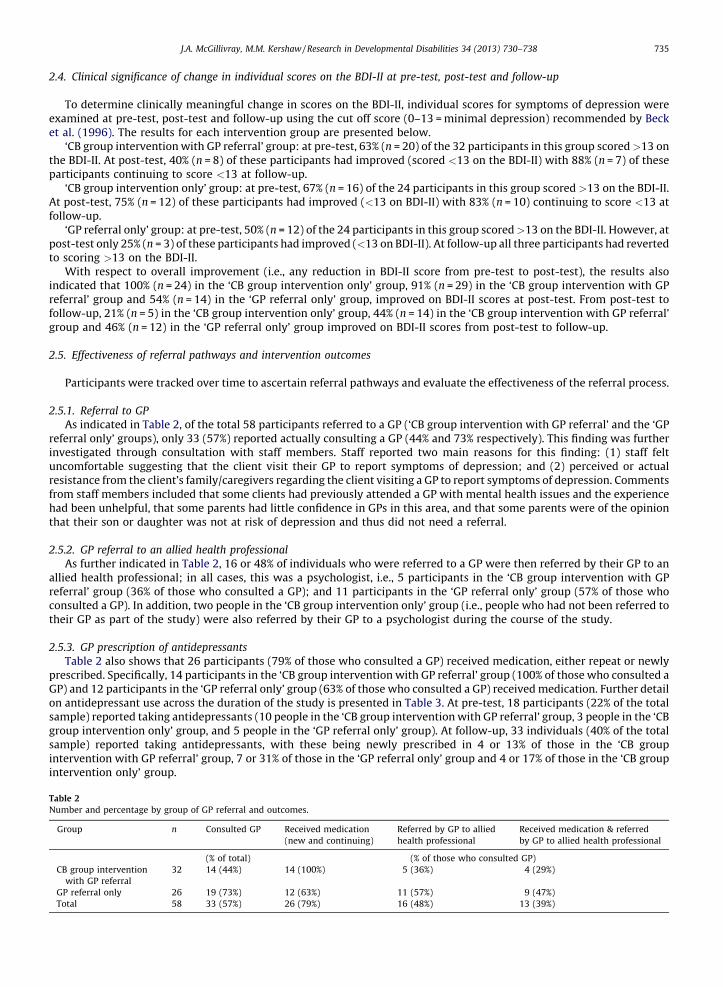
As indicated in Table 2, of the total 58 participants referred to a GP (‘CB group intervention with GP referral’ and the ‘GPreferral only’ groups), only 33 (57%) reported actually consulting a GP (44% and 73% respectively). This finding was furtherinvestigated through consultation with staff members. Staff reported two main reasons for this finding: (1) staff feltuncomfortable suggesting that the client visit their GP to report symptoms of depression; and (2) perceived or actualresistance from the client’s family/caregivers regarding the client visiting a GP to report symptoms of depression. Commentsfrom staff members included that some clients had previously attended a GP with mental health issues and the experiencehad been unhelpful, that some parents had little confidence in GPs in this area, and that some parents were of the opinionthat their son or daughter was not at risk of depression and thus did not need a referral.
2.5.2. GP referral to an allied health professional
As further indicated in Table 2, 16 or 48% of individuals who were referred to a GP were then referred by their GP to anallied health professional; in all cases, this was a psychologist, i.e., 5 participants in the ‘CB group intervention with GPreferral’ group (36% of those who consulted a GP); and 11 participants in the ‘GP referral only’ group (57% of those whoconsulted a GP). In addition, two people in the ‘CB group intervention only’ group (i.e., people who had not been referred totheir GP as part of the study) were also referred by their GP to a psychologist during the course of the study.
2.5.3. GP prescription of antidepressants
Table 2 also shows that 26 participants (79% of those who consulted a GP) received medication, either repeat or newlyprescribed. Specifically, 14 participants in the ‘CB group intervention with GP referral’ group (100% of those who consulted aGP) and 12 participants in the ‘GP referral only’ group (63% of those who consulted a GP) received medication. Further detailon antidepressant use across the duration of the study is presented in Table 3. At pre-test, 18 participants (22% of the totalsample) reported taking antidepressants (10 people in the ‘CB group intervention with GP referral’ group, 3 people in the ‘CBgroup intervention only’ group, and 5 people in the ‘GP referral only’ group). At follow-up, 33 individuals (40% of the totalsample) reported taking antidepressants, with these being newly prescribed in 4 or 13% of those in the ‘CB groupintervention with GP referral’ group, 7 or 31% of those in the ‘GP referral only’ group and 4 or 17% of those in the ‘CB groupintervention only’ group.
Table 2
Number and percentage by group of GP referral and outcomes.
Group n Consulted GP Received medication
(new and continuing)
Referred by GP to allied
health professional
Received medication & referred
by GP to allied health professional
(% of total) (% of those who consulted GP)
CB group intervention
with GP referral
32 14 (44%) 14 (100%) 5 (36%) 4 (29%)
GP referral only 26 19 (73%) 12 (63%) 11 (57%) 9 (47%)
Total 58 33 (57%) 26 (79%) 16 (48%) 13 (39%)
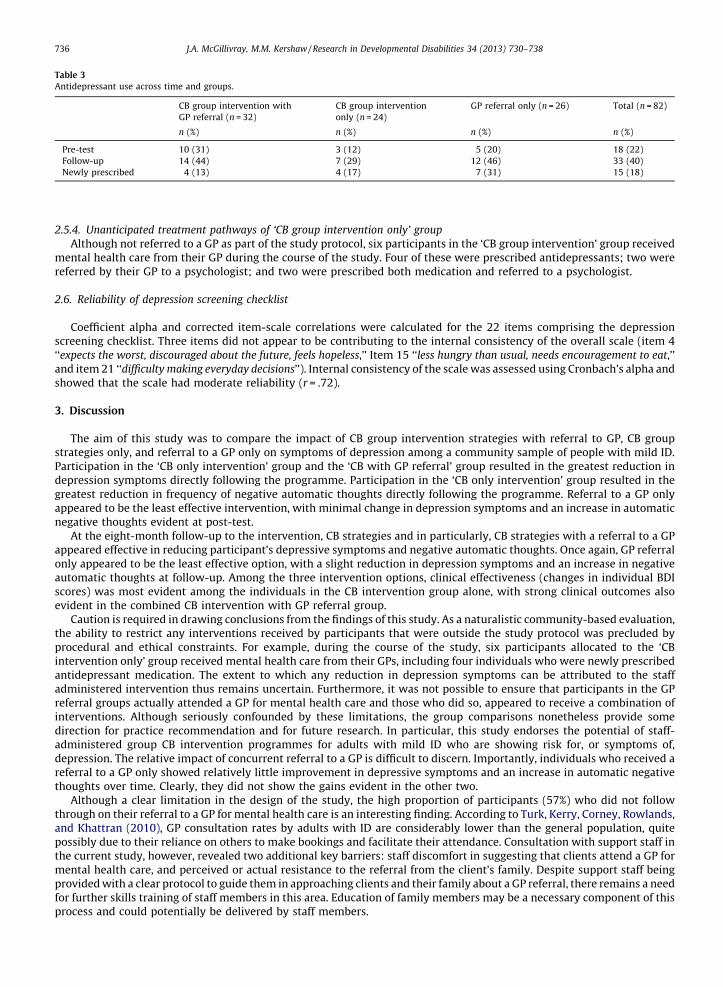
Table 3
Antidepressant use across time and groups.
CB group intervention with
GP referral (n = 32)
CB group intervention
only (n = 24)
GP referral only (n = 26) Total (n = 82)
n (%) n (%) n (%) n (%)
Pre-test 10 (31) 3 (12) 5 (20) 18 (22)
Follow-up 14 (44) 7 (29) 12 (46) 33 (40)
Newly prescribed 4 (13) 4 (17) 7 (31) 15 (18)
J.A. McGillivray, M.M. Kershaw / Research in Developmental Disabilities 34 (2013) 730–738736
2.5.4. Unanticipated treatment pathways of ‘CB group intervention only’ group
Although not referred to a GP as part of the study protocol, six participants in the ‘CB group intervention’ group receivedmental health care from their GP during the course of the study. Four of these were prescribed antidepressants; two werereferred by their GP to a psychologist; and two were prescribed both medication and referred to a psychologist.
2.6. Reliability of depression screening checklist
Coefficient alpha and corrected item-scale correlations were calculated for the 22 items comprising the depressionscreening checklist. Three items did not appear to be contributing to the internal consistency of the overall scale (item 4‘‘expects the worst, discouraged about the future, feels hopeless,’’ Item 15 ‘‘less hungry than usual, needs encouragement to eat,’’and item 21 ‘‘difficulty making everyday decisions’’). Internal consistency of the scale was assessed using Cronbach’s alpha andshowed that the scale had moderate reliability (r = .72).
3. Discussion
The aim of this study was to compare the impact of CB group intervention strategies with referral to GP, CB groupstrategies only, and referral to a GP only on symptoms of depression among a community sample of people with mild ID.Participation in the ‘CB only intervention’ group and the ‘CB with GP referral’ group resulted in the greatest reduction indepression symptoms directly following the programme. Participation in the ‘CB only intervention’ group resulted in thegreatest reduction in frequency of negative automatic thoughts directly following the programme. Referral to a GP onlyappeared to be the least effective intervention, with minimal change in depression symptoms and an increase in automaticnegative thoughts evident at post-test.
At the eight-month follow-up to the intervention, CB strategies and in particularly, CB strategies with a referral to a GPappeared effective in reducing participant’s depressive symptoms and negative automatic thoughts. Once again, GP referralonly appeared to be the least effective option, with a slight reduction in depression symptoms and an increase in negativeautomatic thoughts at follow-up. Among the three intervention options, clinical effectiveness (changes in individual BDIscores) was most evident among the individuals in the CB intervention group alone, with strong clinical outcomes alsoevident in the combined CB intervention with GP referral group.
Caution is required in drawing conclusions from the findings of this study. As a naturalistic community-based evaluation,the ability to restrict any interventions received by participants that were outside the study protocol was precluded byprocedural and ethical constraints. For example, during the course of the study, six participants allocated to the ‘CBintervention only’ group received mental health care from their GPs, including four individuals who were newly prescribedantidepressant medication. The extent to which any reduction in depression symptoms can be attributed to the staffadministered intervention thus remains uncertain. Furthermore, it was not possible to ensure that participants in the GPreferral groups actually attended a GP for mental health care and those who did so, appeared to receive a combination ofinterventions. Although seriously confounded by these limitations, the group comparisons nonetheless provide somedirection for practice recommendation and for future research. In particular, this study endorses the potential of staff-administered group CB intervention programmes for adults with mild ID who are showing risk for, or symptoms of,depression. The relative impact of concurrent referral to a GP is difficult to discern. Importantly, individuals who received areferral to a GP only showed relatively little improvement in depressive symptoms and an increase in automatic negativethoughts over time. Clearly, they did not show the gains evident in the other two.
Although a clear limitation in the design of the study, the high proportion of participants (57%) who did not followthrough on their referral to a GP for mental health care is an interesting finding. According to Turk, Kerry, Corney, Rowlands,and Khattran (2010), GP consultation rates by adults with ID are considerably lower than the general population, quitepossibly due to their reliance on others to make bookings and facilitate their attendance. Consultation with support staff inthe current study, however, revealed two additional key barriers: staff discomfort in suggesting that clients attend a GP formental health care, and perceived or actual resistance to the referral from the client’s family. Despite support staff beingprovided with a clear protocol to guide them in approaching clients and their family about a GP referral, there remains a needfor further skills training of staff members in this area. Education of family members may be a necessary component of thisprocess and could potentially be delivered by staff members.

J.A. McGillivray, M.M. Kershaw / Research in Developmental Disabilities 34 (2013) 730–738 737
Of course, access is only part of the story. It is imperative that the experience of people with ID and their carers when theyattend a GP for mental health care is one that is supportive, collaborative and helpful, thus instilling confidence andencouraging an ongoing professional relationship. The widespread reluctance to take up the referral to a GP in this study,together with the comments from staff regarding negative previous experience, suggests that many GPs may not be wellequipped to assist individuals with mild ID who have depressed mood or who are at risk for depression. These findingsendorse the claims of others that Australian GPs frequently lack training in the assessment and management of psychiatricdisorders among people with ID (Lennox, Diggens, & Ugoni, 2000; Phillips et al., 2004). In addition to the 57% of participantswho did not respond to the GP referral, only 48% of those who did attend were referred by the GP to allied health careprofessionals. Furthermore, there was a high level of antidepressant medication prescribed to participants who attended aGP. There appears to be a priority need to educate GPs about the potential benefits of CB interventions for individuals withmild ID.
The depression screening checklist used in this study was found to have moderate reliability and shows promise as a briefscreening tool for use by staff in identifying individuals with mild ID at-risk of depression. Psychometric investigation intothe validity and reliability of this instrument for use with people with mild ID is recommended. The provision of staff trainingabout depression in people with mild IDs and how to undertake screening appears to be an effective strategy for the earlyidentification of individuals at risk. The importance of screening for depression in adults with ID is clear given theirvulnerability as well as the value of early intervention (Dagnan & Jahoda, 2006; Hastings et al., 2004; McGillivray & McCabe,2007; Rose & Gerson, 2009). Given that individuals with ID do not frequently attend generic mental health services, there is astrong rational for the introduction of screening within the community-based facilities that they do readily attend(McGillivray & McCabe, 2010).
While this research provides useful data on the effectiveness of staff-administered group CB intervention programmeseither on their own, or in combination with GP referral, further research is clearly necessary before firm recommendationscan be made. While evidence for the effectiveness of CB strategies for individuals with ID and depression is building(Ghafoori et al., 2010; Lindsay et al., 1993; McCabe et al., 2006; McGillivray & McCabe, 2007; McGillivray et al., 2008), there isa need for larger controlled trials to confirm these apparent positive effects and to determine the extent to which they can bemaintained over time. A number of factors may impact on how effectively people with ID engage with CB strategies and theseinclude the participant’s level of motivation, confidence, self-efficacy and self-determination in undertaking psychologicalwork (Willner & Hatton, 2006). Such factors determine an individual’s ‘readiness’ for treatment and may be important to thesuccess or otherwise of CB approaches with this population (Howells & Day, 2003). There remains a need for more researchinto ‘readiness’ for group CB-based depression treatment programmes in order to ascertain the characteristics of individualsmost likely to benefit from this form of intervention.
Notwithstanding the methodological limitations of this study, the findings provide support for the routine screening fordepression of individuals with mild IDs by staff members at community-based agencies. Screening for depression in thesesettings increases the likelihood that people with ID experiencing symptoms of depression or risk will be identified and willreceive appropriate treatment. This study has also indicated the potential of group CB intervention programmes delivered bytrained staff within community-based settings that are familiar to, and easily accessed by, people with mild ID. At the sametime, it appears that there may be a need for greater GP education around non-pharmacological options for the managementof depression among people with mild ID. Together, these findings will hopefully facilitate intervention options that aretailored to meet the needs of the individual.
Acknowledgements
We acknowledge beyondblue Victorian Centre of Excellence for funding this research. We also wish to recognise theagencies, staff and individuals with intellectual disability who participated.
References
Ailey, S. H. (2009). The sensitivity and specificity of depression screening tools among adults with intellectual disabilities. Journal of Mental Health Research inIntellectual Disabilities, 2(1), 45–64.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders, fourth edition (DSM-IV). Washington DC: American PsychiatricAssociation.
Antonacci, D. J., & Attiah, N. (2008). Diagnosis and treatment of mood disorders in adults with developmental disabilities. Psychiatric Quarterly, 79, 171–192.Beail, N. (2003). What works for people with mental retardation? Critical commentary on cognitive-behavioural and psychodynamic psychotherapy research.
Mental Retardation41.Beck, A. T., Steer, R. A., & Brown, M. J. (1996). Manual for the beck depression inventory-II (BDI-II). San Antonio: The Psychological Corporation Harcourt Brace and
Company.Borthwick-Duffy, S. A., & Eyman, R. K. (1990). Who are the dually diagnosed? American Journal of Mental Retardation, 94, 586–595.Cooper, S. A., Smiley, E., Morrison, J., Williamson, A., & Allan, L. (2007). Mental ill-health in adults with intellectual disabilities: Prevalence and associated factor.
British Journal of Psychiatry, 190, 27–35.Costello, H., Hardy, S., Tsakanikos, E., & McCarthy, J. (2010). Training professionals, family carers and support staff to work effectively with people with intellectual
disability and mental health problems. In N. Bouras & G. Holt (Eds.), Mental health services for adults with intellectual disability: strategies and solutions (pp. 117–136). New York, NY, US: Psychology Press.
Dagnan, D., & Chadwick, P. (1997). Cognitive therapy with people with learning disabilities: Toward a new synthesis. British Journal of Clinical Psychology, 34: 485–503.

J.A. McGillivray, M.M. Kershaw / Research in Developmental Disabilities 34 (2013) 730–738738
Dagnan, D., & Jahoda, A. (2006). Cognitive-behavioural intervention for people with intellectual disability and anxiety disorders. Journal of Applied Research inIntellectual Disabilities, 19, 91–97.
Davis, J. P., Judd, F. K., & Herrman, H. (1997). Depression in adults with intellectual disability. Part 1. A review. Australian and New Zealand Journal of Psychiatry, 31,232–242.
Deb, S., Thomas, M., & Bright, C. (2001). Mental disorder in adults with intellectual disability. 1. Prevalence of functional psychiatric illness among a community-based population aged between 16 and 64 years. Journal of Intellectual Disability Research, 45, 495–505.
Edelstein, T. M., & Glenwick, S. (2001). Direct-care workers’ attributions of psychopathology in adults with mental retardation. Mental Retardation, 39, 368–378.Emerson, E., Hatton, C., Felce, D., & Murphy, G. (2001). Learning disabilties: the fundamental facts. London: Foundation for People with Learning Disabilities.Esbensen, A. J., & Benson, B. A. (2005). Cognitive variables and depressed mood in adults with intellectual disability. Journal of Intellectual Disability Research, 49(7),
481–489.Ghafoori, B., Ratanasiripong, P., & Holladay, C. (2010). Cognitive behavioral group therapy for mood management in individuals with intellectual disabilities: A
pilot study. Journal of Mental Health Research in Intellectual Disabilities, 3(1), 1–15.Gibbs, S. M., Brown, M. J., & Muir, W. J. (2008). The experience of adults with intellectual disabilities and their carers in general hospitals: A focus group study.
Journal of Intellectual Disability Research, 52, 1061–1077.Glenn, E., Bihm, E. M., & Lammers, W. J. (2003). Depression, anxiety and relevant cognitions in persons with mental retardation. Journal of Autism and
Developmental Disorders, 33, 69–76.Hastings, R. P., Hatton, C., Taylor, J. L., & Maddison, C. (2004). Life events and psychiatric symptoms in adults with intellectual disabilities. Journal of Intellectual
Disability Research, 48, 42–46.Hatton, C. (2002). Psychosocial interventions for adults with intellectual disabilities and mental health problems. Journal of Mental Health11.Hermans, H., & Evenhuis, H. M. (2010). Characteristics of instruments screening for depression in adults with intellectual disabilities: Systematic review. Research
in Developmental Disabilities, 31(6), 1109–1120.Howells, K., & Day, A. (2003). Readiness for anger management: Clinical and theoretical issues. Clinical Psychology Review, 23, 319–337.Hurley, A. D. (2008). Depression in adults with intellectual disability: Symptoms and challenging behaviour. Journal of Intellectual Disability Research, 52(11), 905–
916.Infrapsych CBT program for depression. (2003). Retrieved from http://www.infrapsych.com/root/1033/Depression/Depression_CBTMain.htm.Kendall, P. C., Howard, B. L., & Hays, R. C. (1989). Self-referent speech and psychopathology: The balance of positive and negative thinking. Cognitive Therapy and
Research, 13, 583–598.Kerker, B. D., Owens, P. L., Zigler, E., & Horwitz, S. M. (2004). Mental health disorders among individuals with mental retardation: Challenges to accurate
prevalence estimates. Public Health Reports, 119, 409–417.Krahn, G. L., Hammond, L., & Turner, A. (2006). A cascade of disparities: Health and health care access for people with intellectual disabilities. Mental Retardation
and Developmental Disabilities Research Reviews, 12, 70–82.Lennox, N. G., Diggens, J., & Ugoni, A. (2000). Health care for people with an intellectual disability: General practitioners’ attitudes, and provision of care. Journal of
Intellectual and Developmental Disability, 25(2), 127–133.Lindsay, W. R., Howells, L., & Pitcaithly, D. (1993). Cognitive therapy for depression with individuals with intellectual disabilities. British Journal of Medical
Psychology, 66(2), 135–141.Lowry, M. A. (1998). Assessment and treatment of mood disorders in persons with developmental disabilities. Journal of Developmental and Physical Disabilities, 10,
387–406.Lunsky, Y., & Benson, B. A. (2001). Association between perceived social support and strain, and positive and negative outcome for adults with mild intellectual
disability. Journal of Intellectual Disability Research, 45, 106–114.McBrien, J. A. (2003). Assessment and diagnosis of depression in people with intellectual disability. Journal of Intellectual Disability Research, 47, 1–13.McCabe, M. P., McGillivray, J. A., & Newton, D. C. (2006). Effectiveness of treatment programmes for depression among adults with mild/moderate intellectual
disability. Journal of Intellectual Disability Research, 50(4), 239–247.McGillivray, J. A., & McCabe, M. P. (2007). Early detection of depression and associated risk factors in adults with mild/moderate intellectual disability. Research in
Developmental Disabilities, 28(1), 59–70.McGillivray, J. A., & McCabe, M. P. (2010). Detecting and treating depression in people with mild intellectual disability: The views of key stakeholders. British
Journal of Learning Disabilities, 38(1), 68–76.McGillivray, J. A., McCabe, M. P., & Kershaw, M. M. (2008). Depression in people with intellectual disability: An evaluation of a staff-administered treatment
program. Research in Developmental Disabilities, 29(6), 524–536.Millar, L., Chorlton, M. C., & Lennox, N. (2004). People with intellectual disability: Barriers to the provision of good primary care. Australian Family Physician, 33,
657–658.Moodgym Training Program. (2003). Retrieved from http://moodgym.au.edu.au/.Morin, D., Cobigo, V., Rivard, M., & Lepine, M. (2010). Intellectual disabilities and depression: How to adapt psychological assessment and intervention. Canadian
Psychology, 51, 185–193.Moss, S. (2001). Assessment: conceptual issues. In N. Bouras (Ed.), Psychiatric and behavioural disorders in developmental disabilities and mental retardation. London:
Cambridge Press.Nezu, C. M., Nezu, A. M., Rothenberg, J. L., DelliCarpini, L., & Groag, I. (1995). Depression in adults with mild mental retardation: Are cognitive variables involved?
Cognitive Therapy and Research, 19, 227–239.Perez-Achiaga, N., Nelson, S., & Hassiotis, A. (2009). Detecting depression: Instruments for the detection of depressive symptoms in people with intellectual
disabilities: A systematic review. Journal of Intellectual Disabilities, 13, 55–76.Phillips, A., Morrison, J., & Davis, R. W. (2004). General practitioners’ educational needs in intellectual disability health. Journal of Intellectual Disability Research,
48(2), 142–149.Rai, P. R., & Kerr, M. (2010). Antidepressant use in adults with intellectual disability. The Psychiatrist, 34(4), 123–126.Rose, J., & Gerson, D. F. (2009). Assessing anger in people with intellectual disability. Journal of Intellectual and Developmental Disability, 34, 116–122.Rose, J., West, C., & Clifford, D. (2000). Group interventions for anger in people with intellectual disabilities. Research in Developmental Disabilities, 21, 171–181.Ruddick, L. (2005). Health of people with intellectual disabilities: A review of factors influencing access to health care. British Journal of Health Psychology, 10, 559–
570.Smiley, E., & Cooper, S. (2003). Intellectual disabilities, depressive episode, diagnostic criteria and diagnostic criteria for psychiatric disorders for use with adults
with learning disabilities/mental retardation (DC-LD). Journal of Intellectual Disability Research, 47, 62–71.Stenfert Kroese, B., Dagnan, D., & Konstantinos, L. (Eds.). (1997). Cognitive-behaviour therapy for people with learning disabilities. London: Routledge.Sturmey, P. (2004). Cognitive therapy with people with intellectual disabilities: A selective review and critique. Clinical Psychology & Psychotherapy, 11(4), 222–
232.Turk, V., Kerry, S., Corney, R., Rowlands, G., & Khattran, S. (2010). Why some adults with intellectual disability consult their general practitioner more than others.
Journal of Intellectual Disability Research, 54(9), 833–842.van den Hout, M., Arntz, A., & Merckelbach, H. (2000). Contributions of psychology to the understanding of psychiatric disorders. In M. G. Gelder, J. L., Lopez-Ibor,
Jr., & N. C. Andreasen (Eds.), New oxford textbook of psychiatry (pp. 277–292). Oxford: Oxford University Press.Webb, O. J., & Rogers, L. (2002). The health care of people with intellectual disabilities. Continuing Medical Education, 29, 188–194.White, P., Chant, D., Edwards, N., Townsend, C., & Waghorn, G. (2005). Prevalence of intellectual disability and comorbid mental illness in an Australian
community sample. Australian and New Zealand Journal of Psychiatry, 39, 395–400.Willner, P. (2005). Readiness for cognitive therapy in people with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 19, 5–16.Willner, P., & Hatton, C. (2006). CBT for people with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 19(1), 1–3.





























