Embed Size (px)
Citation preview

PEDIATRIC ASTHMA, ALLERGY & IMMUNOLOGYVolume 8, Number 3, 1994Mary Ann Liebert, Inc., Publishers
The Impact of Poverty on Asthma
ROBIN ROSE, R.N., M.H.S.A. and KEVIN B. WEISS, M.D., M.P.H.
ABSTRACT
The epidemiologie and economic literature continues to illuminate important associations be¬tween socioeconomic status and asthma morbidity. While asthma prevalence and morbidityremains disproportionately high among minority populations, socioeconomic status appearsto explain much of the differences in rates. The economic costs of illness related to asthma andlow-income populations may be linked to direct medical expenditures in hospital-based versus
ambulatory-based asthma care. Problems in the financing and organization of health care forthe poor may also contribute to the burden of asthma. A better understanding of the interplaybetween people, risk factors, and health care environments is necessary if we are to designsuccessful health system improvements for the management of asthma in impoverishedpopulations.
INTRODUCTION
Recent studies have illuminated a disproportionate burden of asthma morbidity within impoverishedpopulations. Associated with the excess burden of illness for these populations are important social and
economic consequences that have been less clearly recognized. This paper explores some of the existingknowledge about the relationship between socioeconomic status (SES) burden and asthma. As part of thisoverview, the epidemiologie and economic literature that provides evidence for an association between asthmamorbidity and SES is presented. Following the discussion of the social and economic burden, we examinesome of the key issues that relate to asthma care—both organizational and financial—that make it difficult to
improve clinical outcomes for persons who live in poverty.
EXAMINING THE SOCIAL BURDEN OF ASTHMA INIMPOVERISHED POPULATIONS
The epidemiologie literature has illuminated several key relationships between asthma morbidity/mortalityand risk factors, such as race/ethnicity and poverty. In the United States, asthma is more prevalent in Blacksthan whites.'1' Blacks also have higher rates of hospitalization'2·3' and mortality'4·5' due to asthma. However,Blacks are not the only minority population disproportionately affected. Puerto Rican children living in theNew York City area are also reported to have some of the highest rates of asthma.'6' This suggests that race/eth¬nicity is one of several factors influencing asthma prevalence, morbidity, and mortality. Socioeconomic statusis another contributing factor.
Department of Health Care Sciences, George Washington University Medical Center, Washington, DC.
157

ROSE AND WEISS
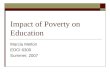
Studies have also demonstrated the extent to which SES contributes to asthma hospitalizations and mortal¬ity. Wissow, et al'7' examined asthma hospitalization data from the state of Maryland. They found that the largedifferences in hospitalization rates between Blacks and whites nearly disappeared when the data were adjustedby census tract income levels. A review of several public health reports indicates that an inverse relationshipbetween low SES and high asthma mortality rates emerged between the periods of 1969 and 1989.'8' In NewYork City, asthma morbidity and mortality have been reported to cluster in poor neighborhoods of predomi¬nately minority populations.'9' As seen in Figure 1, a similar relationship between poverty and high asthmamortality rates has been demonstrated in Chicago.'10'
Socioeconomic status appears to greatly influence asthma hospitalizations and mortality rates.Socioeconomic status also seems to affect the prevalence of asthma. Data from the 1981 National HealthInterview Survey Child Health Supplement noted that higher asthma prevalence among Black versus whitechildren was eliminated after controlling for SES.'n> A recent study of the Bronx area of New York emphasizesextremely high rates of asthma prevalence in the inner city and provides evidence that poverty is a significantrisk factor for asthma prevalence in poor urban populations.'12'
With the growing evidence of SES as a risk factor for asthma morbidity, it is no great surprise that asthmamorbidity appears to be increasing within our inner cities. During the 1980s, there was a trend toward childrenraised in single-parent families of limited financial resources."3' According to 1987 figures from the NationalCenter for Children in Poverty, the proportion of United States children under the age of six who were living inpoverty was nearly 50% of all Black children and 42% of Hispanic children, whereas only 10% of white chil¬dren were considered to be impoverished.'14' Forty-six percent of all poor children in the United States live inthe central cities and during the 12 year period from 1975 to 1987, the proportion ofchildren living in the poor¬est areas of the central cities rose from 54 to 61 percent.'15'
Also, an increasingly disproportionate number of families in the inner-city are headed by young, single,poorly educated women.'16' Single mothers on welfare often have inadequate social supports to help themthrough the stresses of caring for a chronically ill child.'17·18' Much of the disproportionate burden of asthmamorbidity is likely to remain until important social and environmental factors, such as these are addressed.
EXAMINING THE ECONOMIC BURDEN OF ASTHMA
Further exploration of the economic burden of asthma morbidity and impoverished populations requires areview of the fundamental aspects of health economics, specifically the costs of illness.
Mortality rate per million population
<14 5 14.5-20.1 20.2-23.9 >24.0Income (in thousands)
-DSS*FIG. 1. Annual asthma mortality rates by race and median community income. Chicago, 1980-1988 (5-34 y.o.). Source:Marder DM, Chest 1992;101:428S.
158

POVERTY AND ASTHMA
Costs of illness
There are substantial costs associated with asthma. Traditionally, the burden of illness is divided into threecategories: direct medical expenditures, indirect costs, and intangible costs.'19' The direct medical expendi¬tures are those costs associated with use of health care services, such as physician visits, laboratory tests, andmedications. Indirect costs are associated with the value of time lost from school and work. Intangible costs re¬
flect the value of the psychosocial impact of the disease. There are conventional methods for assigning valuesto the direct and indirect costs, however, there are currently no standard mechanisms for assessing the value ofthe psychosocial impact of an illness.'20' Therefore, most of the economic studies of asthma to date are an un¬
derestimate of the total social costs of this illness.Also, the economic costs of illness can be viewed from at least three different perspectives: society, the
health care organization, and the individual with asthma. From the societal perspective, the 1990 cost of illnessfor asthma in the United States has been estimated at 6.2 billion dollars.'21' Direct medical care costs accountedfor approximately 59% (3.6 billion dollars) of the total cost. The remaining 41 % was attributed to the value ofindirect productivity loss per year.
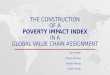
The provider perspective, viewed by the health care organization, is most apparent in terms of direct utiliza¬tion ofthe health care system. Cost of illness studies in the United States indicate that asthma accounts for sub¬stantial health care utilization, including more than 460,000 hospitalizations, 1.8 million emergency room vis¬its, and eight million doctor visits annually.'21' As seen in Table 1, a recent study of preventable hospitalizationstays in Massachusetts identified asthma as the most common diagnosis for preventable hospitalizations in thatstate during 1989.'22'
For the individual or family, the costs of asthma mount quickly. Studies suggest that a large proportion of a
family's income may be spent on the direct costs of asthma care.'23·24' In addition, the indirect costs associatedwith transportation, child care, and time lost from work are also likely to substantially add to the economicburden.
While the overall costs of illness related to asthma have been characterized, there have been no specific stud¬ies of the costs of illness for impoverished populations, such as those persons living within our inner cities.Nevertheless, those aspects unique to the costs of asthma for impoverished populations can be easily envi¬sioned. For example, the heavy use ofemergency rooms as a source ofprimary care will likely increase the pro¬portion of direct medical expenditures. Discontinuity in asthma management will likely lead to loss of follow-up care and increased costs. The lack of follow-up care, in turn, may contribute to subsequent morbidity and anincrease in the proportion of total direct expenditures for hospitalizations at the expense of primary care
services.
ASTHMA, SOCIOECONOMIC STATUS, AND HEALTH CARE WITHINTHE INNER CITY
While the preceding sections have examined the socioeconomic impact of asthma on impoverished popula¬tions, there are many factors related to health care organization and finance that also appear to contribute to theburden of asthma within our inner cities.
Organization of care
For the majority of persons with mild to moderate asthma, the primary care physician oversees the manage¬ment of care.'25' However, in the inner city, routine primary care is not easily accessible. There are many orga¬nizational problems that confront the inner-city person with asthma. For example, people living in poverty are
much more likely than wealthier people to report no regular source of health care.'26' Similarly, poorer popula¬tions are far more likely to receive their care from overburdened hospital outpatient and emergency depart¬ments rather than individual physicians.'27' Fragmented, episodic care does not promote the provider-patientrelationships necessary to foster adequate asthma co-management skills. The overcrowded clinics and emer¬
gency rooms have little opportunity to provide patients with the education and reinforcement necessary for op¬timal asthma management.
159

ROSE AND WEISS
Table 1. Preventable Hospitalization in Massachusetts: 10 MostFrequent Diagnoses, All Short Stay Hospitals, 1989-90 Data
NumberCondition of cases ChargesAsthma 20,118 $62mBacterial pneumonia 15,790 $88mAngina 12,590 $39mKidney/urinary infection 7,432 $33mCongestive heart failure 7,091 $51mDehydration 7,055 $24mGastroenteritis 6,811 $16mDiabetic complications 5,466 $26mGrand Mai epilepsy 4,613 $28mChronic lung disease 4,321 $28m
Source: Massachusetts Rate Setting Commission, 1994.
Financing of asthmaIt is well known that health care in the United States is financed by a complex collection of private and pub¬
lic insurance mechanisms. Inner-city populations living in poverty are at high risk for inadequate insurancecoverage. Health care coverage is typically provided via one of three financing options: limited private healthinsurance, public health insurance (such as Medicaid), or no insurance coverage at all. Private insurance plansfor unemployed or low wage earning populations are likely to have high déductibles and co-payments.'28·29'Some private plans—even for middle-income wage earners—do not provide adequate coverage for the outpa¬tient services, medications, and devices that comprise the majority of asthma care management.'30' In addition,individuals with chronic conditions, such as asthma, may experience difficulties in obtaining private health in¬surance because they have pre-existing conditions.'31'
Public health programs, such as Medicaid, provide coverage for certain eligible segments of inner-city pop¬ulations. These programs—which are especially targeted to low income women and children—appear to offera fairly wide scope ofbenefits, including outpatient care. A majority of states also cover pharmacy services andmedical equipment.'32' Unfortunately, there are many access problems associated with the public medical as¬
sistance programs.'33' Low reimbursement rates have contributed to a scarcity of providers willing to care forMedicaid patients.'34·35' This often results in long waits and increased use of emergency room facilities. Thepublic system is also administratively complex, requiring the recipient to navigate a maze of confusingprocesses. For many single-parent families, transportation and child care pose enormous difficulties.'36'
Individuals and families ofchildren with asthma may face one or more subtle barriers in addition to the usualaccess problems associated with public assistance programs. Medicaid pharmacy policies often place dispens¬ing limits on medications.'37' This practice requires the recipient to return to the pharmacy for a refill once amonth. Some pharmacies in the inner city may not even accept Medicaid reimbursement. Also, not all stateMedicaid programs opt to cover the durable medical equipment (DME), such as spacer devices, peak flow me¬
ters, and home nebulizers commonly used in asthma management.'30' Of the programs that cover DME, some
require prior authorization. The extra steps created by these program policies may appear small from the orga¬nizational perspective, yet they may effectively deter many low income individuals, who quickly redirect theirefforts to overcoming one or more other daily problems that accompany a life of poverty, such as obtainingfood and housing or dealing with violence.
Individuals who do not qualify for public assistance and who are unable to afford private coverage fall intothe category of the uninsured. More accurately, these individuals are "self-insured" to the limits of their abilityto pay. The uninsured encompass those who are self-employed, employed part-time, and or work full-time foremployers who do not provide health insurance, as well as low-income adult males who are, by category, noteligible for Medicaid.
In 1985, among children under the age of six, 30% of the poor and 32% of the near poor were without health
160

POVERTY AND ASTHMA
insurance."5' An additional 13% of families who were more than 150% above the poverty line were uninsured.The financial burdens facing asthmatics in this segment of the population are tremendous. Monthly out-of-pocket expenditures range from hundreds to thousands of dollars per month.'36' For persons with asthma, thisoften results in decreased utilization of routine and preventative health care services, sporadic use of medica¬tion, and inadequate follow-up of asthma exacerbations. One study found that poor, uninsured children made38% fewer visits to a physician than those with insurance.'38'
Individuals living in poverty often transition in and out of funding sources. The "medically needy" are at
particular risk of receiving inadequate management of chronic conditions, such as asthma, because they do notqualify for assistance until their medical expenses place them within the required range of the poverty level.Families of children with mild to moderate disease may not incur enough expenses to access the system untilthe children become sick enough to require hospitalization.
INTEGRATING OUR KNOWLEDGE OF THE SOCIAL AND ECONOMICBURDENS OF ASTHMA TO PROMOTE IMPROVEMENTS IN
IMPOVERISHED POPULATIONS
Recognizing the possible relationships between the social and economic impact of asthma on impoverishedpopulations illustrates the need for a better understanding of how the complex interactions between person,risk factor, and health care environment may lead to excess morbidity in populations at risk. These complex in¬teractions present a challenge to the epidemiologists, health service researchers, physicians, and health care
administrators who struggle to reduce the social and economic morbidity associated with this disease.Carefully designed intervention strategies that appear to work in non-inner-city environments may indeed beineffective when attempted in the inner city.
In a time of potential major health care reform, it is prudent to seek changes in the organizational and finan¬cial structures of health care delivery for inner-city populations that will specifically lead to improvements inthe care and clinical outcomes for persons with chronic illnesses, such as asthma. However, while waiting forhealth care reform, it is important to recognize that there are a number ofcurrent projects related to low-incomepopulations that have the potential to effect improved clinical outcomes for persons with asthma. For example,several Medicaid programs are adopting strategies for primary care case management. This "gatekeeper" typeof arrangement is designed to link each enrollee with a single primary care provider who is, in turn, responsi¬ble for coordinating all of the patient's medical care. There are also some Medicaid waiver programs for tar¬
geted case management of other chronic conditions that could easily be used as a model for improving asthmacare.'39' In addition, these waiver programs have the potential to facilitate improvements in continuity and co¬
ordination of services. Although Medicaid projects specific to asthma are scarce, there is at least one Medicaidprogram that has begun to examine the usefulness of asthma education services.'36'
Other projects emphasizing asthma education have also demonstrated an ability to effectively reduceasthma hospitalizations.'40' In addition, the National Institute of Allergy and Infectious Diseases has taken a
special interest in the inner-city populations. The agency is currently sponsoring a multi-city study to examinerisk factors and possible interventions associated with inner-city pediatrie asthma morbidity.'41'
CONCLUSION
In summary, research over the past few years has focused our attention on a disproportionately high rate ofasthma morbidity for populations living in poverty. This morbidity should be viewed not only in terms of so¬cial impact bui also in terms of economic burden to individuals, health systems, and society. There are manyreasons to suspect that much of the socioeconomic burden of asthma is related to dysfunctional health care de¬livery systems and financing mechanisms. On the other hand, there are also efforts underway to further under¬stand the problems of asthma unique to populations living in poverty, such as those in our inner cities. We hopethat these efforts will lead to a better understanding of primary prevention of asthma as well as improvementsin medical management of this chronic condition.
161

ROSE AND WEISS
REFERENCES
1. Gergen PJ, Mullally DI, Evans RIH. National Survey of Prevalence of asthma among children in the United States,1976to 1980. Pediatrics 1988;81:1-7.
2. Evans RIII, Mullally DI, Wilson RW, et al. National trends in the morbidity and mortality of asthma in the US:Prevalence, hospitalization and death from asthma over two decades: 1965-1984. Chest 1987;91:65S-74S.
3. Gergen PJ, Weiss KB. Changing patterns of asthma hospitalization among children: 1979 to 1987. JAMA1990;264:1688-1692.
4. Sly RM. Mortality from asthma in children 1979-1984. Ann Allergy 1988;60:433^H2.5. Weiss KB, Wagener DK. Changing patterns of asthma mortality: Identifying target populations at high risk. JAMA
1990;264:1683-1687.6. Carter-Pokras OD, Gergen PJ. Reported asthma among Puerto Rican, Mexican-American, and Cuban-American chil¬
dren, 1982-1984. Am J Public Health 1993;83:580-582.7. Wissow LS, Gittelsohn AM, Szklo M, Starfield B, Mussman M. Poverty, race, and hospitalization for childhood
asthma. Am J Public Health 1988;78:777-782.8. Weiss KB, Gergen PJ, Wagener DK. Breathing better or wheezing worse? The changing epidemiology of asthma mor¬
bidity and mortality. Ann Rev Pubi Health 1993;14:491-513.9. Carr W, Zeitel L, Weiss K. Variations in asthma hospitalizations and deaths in New York City. Am J Public Health
1992;82:59-65.10. Marder D, Targonski P, Orris P, Persky V, Addington W. Effect of racial and socioeconomic factors on asthma mor¬
tality in Chicago. Chest 1992;101:426S^t29S.11. Weitzman M, Gortmaker S, Sobol A. Racial, social, and environmental risk factors for childhood asthma. Am J Dis
Child 1990;144:1189-1194.12. Hersh MS, Crain EF, Weiss KB, Westbrook LE, Stein RE. An estimate of asthma prevalence among inner-city chil¬
dren. (Abstr) First National Conference on Asthma Management, Washington DC, October 1992.13. Helmick SA, Zimmerman JD. Trends in the distribution of children among households and families. Child Welfare
1984:LXffl;401^M)9.14. Data sourcebook: Five million children. New York: Columbia University National Center for Children in Poverty,
1990, 9.
15. Five million children: A statistical profile of our poorest young citizens. New York: Columbia University NationalCenter for Children in Poverty, 1990, 22.
16. Wood DL, Valdez RB, Hayashi T, Shen A. Health of homeless children and housed, poor children. Pediatrics1990;86:858-866.
17. Haggerty RJ. Life stress, illness and social supports. Develop Med Child Neurol 1980;22:391^t00.18. McLanahan S, Garfinkel I. Single mothers, the underclass, and social policy. Annals Amer Academy Pol Soc Sci
1989;501:92-104.19. Rice DP. Estimating the cost of illness. Health Economics Series No. 6, Publication No. 947-6. US Government
Printing Office, Washington, DC, 1966.20. Drummond MF. Cost-of-illness studies: A major headache? PharmacoEconomics 1994;2:1-4.21. Weiss KB, Gergen PJ, Hodgson TA. An economic evaluation of asthma in the United States. Engl J Med
1992;326:862-866.22. Preventable hospitalization in Massachusetts. Massachusetts Rate Setting Commission, Boston, MA: Pub. No. 17497-
81-2000-2-94 C.R. January 1994.23. Marion RJ, Creer TL, Reynolds RVC. Direct and indirect costs associated with the management of childhood asthma.
Ann Allergy 1985;54:31-34.24. Vance VJ, Taylor WF. The financial cost of chronic childhood asthma. Ann Allergy 1971 ;29:455^160.25. National Heart, Lung and Blood Institute. Guidelines for the diagnosis and management of asthma, report of the expert
162

POVERTY AND ASTHMA
panel. National Asthma Education Program, National Institutes of Health, US Department of Health and HumanServices, Public Health Service, Bethesda, MD: Publication No. 91-3042. January 1991.
26. Freeman HE, Blendon RJ, Aiken LH, Sudman S, Mullinix CF, Corey CR. Americans report on their access to healthcare. Health Aff 1987;6:6-18.
27. Access to health care in the United States. Special Report No. 2. Princeton, NJ: Robert Wood Johnson Foundation,1987, pp 4-10.
28. Higgins AF. Health care benefits survey 1987. Princeton, NJ: A. Foster Higgins & Company Inc., 1988.29. Bureau of Labor Statistics. Employee benefits in medium and large firms, 1988. Washington, DC: US Department of
Labor, June 1989.30. Henderson R, Buist A, Weiss KB, Rose R. Asthma care financing in the US: A pilot study to examine the variations in
public and private benefit coverage [internal interim report]. American Lung Association Office of GovernmentalAffairs, Washington, DC: January 1994.
31. Sheils JF, Wolfe PR. The role of private health insurance in-children's health care: The future of children: US HealthCare for Children 1992;2:115-133.
32. US Department of Health and Human Services. Medicaid: State profile data system, characteristics of Medicaid stateprograms, Vol. 1, Baltimore, MD: Health Care Financing Administration, HCFA Pub. No. 02178, 1992.
33. St. Peter RF, Newacheck PW, Halfon N. Access to care for poor children. JAMA 1992;267:2760-2764.34. McManus M, Hint S, Kelly R. The adequacy ofphysician reimbursement for pediatrie care under Medicaid. Pediatrics
1991;87:909-920.35. Yudkowsky BK, Cartland JDC, Flint SS. Pediatrician participation in Medicaid. Pediatrics 1990;85:567-577.36. Task Force on Cost-Effectiveness, Quality of Care, and Financing of Asthma Care. Public hearings on financing of
asthma care: summary report [internal interim report]. National Asthma Education Program, National Heart, Lung andBlood Institute, National Institutes of Health, Bethesda, MD: January 1994.
37. National Pharmaceutical Council. Pharmaceutical benefits under state medical assistance programs. NationalPharmaceutical Council, Inc., Washington, DC: September 1992.
38. Parker S, Greer S, Zuckerman B. Double jeopardy: The impact of poverty on early childhood development. PediatrClinNAm. 1988;35:1227-1240.
39. Health Systems Analysis, Policy and Health Statistics Administration. Maryland medical assistance program: Theyear in review (fiscal year 1992). Baltimore MD: Department of Health and Mental Hygiene, January 1993, 20-21.
40. Mayo PH, Richman J, Harris HW. Results of a program to reduce admission for adult asthma. Ann Intern Med1990;112:864-871.
4L Prograis LJ, Plaut M, Weiss KB, Gergen PJ. The National Institute of Allergy and Infectious Diseases' NationalCooperative Inner City Asthma Study. Amer J Asthma and Allergy Ped 1993;6:61-66.
Address reprint requests to:Kevin B. Weiss, M.D., M.P.H.
DHCS/GWUMCRoom 2B-401
2150 Pennsylvania Avenue, N. W.Washington, DC 20037
163