Embed Size (px)
Citation preview

Health Policy and Education 1 (1980) 317-336 317 Elsevier Scientific Publishing Company, Amsterdam - Printed in The Netherlands
THE IMPACT OF NEW MEDICAL SCHOOLS AND THE ISSUES OF INCREASING ENROLLMENT
JOHN O. LOSTETTER and JOHN E. CHAPMAN
School of Medicme, l)-3300 Medzcal Center, Vanderbilt University, Nashville, Tennessee 37232, U.S.A
ABSTRACT
Is there an impending physician surplus? The authors' position is that there is an impending surplus. Health planners must be cognizant of this eventuality. The federal government as one of the major authors of health policy guidelines is currently reacting to the surplus question. But federal reaction can at times be too swift, too dramatic, and not in the best interests of those who must maintain previous investments. Therefore, both the supporters of health-related educational institu- tions and those who are responsible for program implementation must attempt to det'me and reach a common understanding of the situation. Policy development and planning aetivities must be collaborative efforts that emphasize involvement.
In this paper, the authors present a brief review of federal policies relative to the production of physicians and other health professionals. It is hoped that one can better understand the current situation and more effectively plan the future ff past developments are included. This should lead to a comprehensive analysis from a common perspective. The involvement of the Carnegie Com- mission (Carnegie Council) is also included for the same reasons.
All analyses lead to the current situation and the authors' positron that there is an impending physician surplus. The central problem has shifted from physician supply to the problem of physician maldistribution, both geographically and by specialty.
An examination of the history and development of the federal govern- ment's involvement in the process of medical education clearly shows that the initial emphasis of tying federal support to the concept of a substantial increase in the number of physicians as the necessary ingredient to improving health care in the U.S. has shifted. Now, the government's involvement does not emphasize sheer numbers of physicians but is tied to types of programs and the geographic distribution of physicians. These ideas are manifested in policy statements made by the Congress with the passage of the Health Professions Educational Assistance Act of 1976. In these statements Congress declares that " . . . there is no longer an insufficient number of physicians and surgeons in the U.S. such that there is no further need for affording preference to alien physicians and surgeons in admission to the United States under the Immigration and Nationality Act" (HPEA, 1976a). Federal support emphasis has shifted primarily from physicians to all of those health professionals involved in the health care system. Congress asserts that high quality health care is dependent on the avilability of qualified health professions personnel, an adequate number of physicians engaged in the delivery of primary care, and an adequate distribution of
0165-2281/80/0000-0000/$02.50 © 1980 Elsevier Scientific Publishing Company

318
health professions personnel throughout the U.S. (HPEA, 1976b). Considering that the federal government plays a major role in financing
medical education either directly or indirectly, one cannot ignore policy changes and subsequent changes in restricted support. If these changes are not in the best interests of particular groups or individuals, then involvement in the legislative process is necessary to make appropriate modifications. Basic to any method of modification would be an examination of past and current legislation for the purpose of analyzing trends and predicting future changes and directions. Certainly, such an examination would be appropriate for a study on the impact of new medical schools and the issues of increasing enrollment.
The decade of the 1960's began with the obvious realization of the absence of the federal government in the education of health professionals. The National Defense Education Act of 1958 increased the federal role in higher education. Also in the late 1950's, federal support of biomedical research increased greatly. The 1956 Health Amendments Act authorized advanced training for health professionals and was subsequently expanded; support was again increased.
The decade of the 1960's also began with the questioning of the quality of medical care in the U.S. Studies produced results that showed the U.S. to be well down on longevity and infant mortality lists as compared to other countries of the world. This was an embarrassing situation for the wealthiest and strongest country in the world to be in. The country with the highest standard of living did not necessarily have the highest standard of life. These and other pressures increased federal efforts into health related education. In 1961, the Kennedy Administrahon proposed a bill that included funds for the construction of new educational facilities for the training of physicians, dentists, and public health specialists. Funds were also to be included for scholarships to students. The bill was changed to include also schools of nursing, optometry, pharmacy, and podiatry. Scholarships were changed to loans. The basis for this program was that the quality of health care would be improved by increasing greatly the number of professionals involved in the delivery of health care. The Congress, after two years, finally passed a bill which became known as the 1963 Health Professions Education Assistance Act (P.L. 88-129). This act of Congress officially established the presence of the federal government in health related educational institutions. Other federal programs since 1963 are identified and highlighted in the outline as given in Appendix I.
An examination of Carnegie Commission reports on policy studies in higher education and special reports by this commission dealing with medical education and health care reveals trends similar to those found in the historical description of federal involvement in medical education presented above.

319
In a 1968 report, the Carnegie Commission discussed medical and health services education as a particular concern for specific federal aid proposals (Carnegie Commission, 1968a). The major emphasis in this case was to greatly increase the facilities needed to increase the number of physicians. The commission estimated that new facilities would be needed to accom- modate an increase of 75% (as compared to the number of students in 1966) in the number of medical students by 1976-77. This was seen as the number necessary to meet the nation's needs for medical services. The recommenda- tions were also based on the fact that increases in enrollments for medical education were noticeably below the sharply increased rates for higher education in general. Since the 1920's to the time of this report (1966-67), the number of graduates had risen very slowly. It was also pointed out that in 1966-67, 20% of the new doctors practicing in the U.S. acquired their training in foreign medical schools with most receiving an education lower in quality than that offered by U.S. medical schools. An inadequate distribu- tion of physicians was also noted in this report. The commission's recommendations for federal aid were:
1. Stimulate expansion of capacity at existing medical schools. 2. Plan additional medical schools distributed on a geographical basis to provide needed service to areas not now served. 3. Expand educational facilities and develop new programs for the training of medical care support personnel. 4. Increase availability of health services in the community of the medical school and the quality of health care delivery (Carnegie Commission, 1968).
A special report of the Carnegie Commission issued in 1970 entitled Higher Education and the Nation's Health - Policies for Medical and Dental Education continued those recommendations of the 1968 report. The words more and better are characteristic of the 1970 report. Two of the four components for improving health care were:
1. More and better manpower. 2. More and better health care facilities (Carnegie Commission, 1970a).
The manpower shortage in health care was repeatedly emphasized with the specific suggestion that there would be a need for a 50% increase in the number of physicians during the decade of the 1970's. An adequate distribution of physicians was again recommended but was still tied to the theory that an increase in the number of physicians would help solve the distribution problem. To increase physician numbers at an accelerated rate, the Commission also suggested that the time needed to become a practicing

320
physician be reduced from eight years after the B.A. to six years. This would be accomplished by reducing from four to three the years it takes to get an M.D. with a similar reduction for residency training programs. It was projected that manpower shortages would continue through the 1970's and into the 1980's. Numbers projected by HEW were 50,000 more physicians, 200,000 more nurses, and 150,000 more technicians (Carnegie Commission, 1970b). Commission projections of the number of medical school entrants and the number of physicians per 100,000 population from 1967 to 2002 are included in Table I. Projection C is the recommended rate of increase and ratio.
The special report of 1970 also included joint statements made on March 5, 1968 and April 16, 1968 by representatives of the Board of Trustees of
TABLE I
Projections of Number of Physicians per 100,000 Population, Based on Three Alternative Projections of Number of Medical School Entrants, United States, 1967-2002
Year Medical school entrants j
A B C
Active physicians (M.D. and D.O.) per 100,000 population 2
A B C
1967 9,479 9,479 9,479 146.8 146.8 146.8 1968 9,863 9,683 9,863 1969 10,200 10,200 10,200 1970 10,800 10,800 10,800 1971 11,400 11,400 11,400 1972 12,000 12,000 12,000 153.9 153.9 153.9 1973 12,500 12,500 12,900 1974 13,000 13,000 13,800 1975 13,500 13,500 14,700 1976 14,000 14,000 15,300 1977 14,500 14,500 15,900 161.4 161.4 161.4 1978 15,000 15,000 16A00 1979 15,000 15,500 16,800 1980 15,000 16,000 17,100 1982 15,000 16,000 17,700 168.8 168.9 171.3 1987 15,000 16,000 19,200 175.3 177.0 182.1 1992 15,000 16,000 20,400 180.7 184.3 194.2 1997 15,000 16,000 21A00 183.4 188.5 205.0 2002 15,000 16,000 21,600 185.8 192.4 216.4
Excludes entrants to osteopathic medical schools. 2 Assumes 13,000 foreign medical school graduates will permanently enter the United States between 1968 and 1977, but none will enter permanently thereafter. Excluded from the data are 10,500 foreign medical graduates in the United States in 1967 who were judged to be here temporarily. However, some temporary foreign medical school graduates are assumed to be in the United States in all subsequent years, although they axe not included in the ratios above. Source: The Carnegie Commission on Higher Education (1970e). Htgher Education and the Nation's Health - Policies for Medical and Dental Education New York: McGraw-Hill, p. 42, Table 3. Reprinted with permission.

321
the AMA and the Executive Council of the AAMC at two joint meetings (Carnegie Commission, 1970c). These statements echoed comments presented above by the Carnegie Commission. The joint statements recom- mended substantial increases in the enrollment of medical schools, new medical schools, more efficient curriculums, and better health care delivery. The associations issued the joint statement that "at this time AMA and AAMC urge that increased emphasis be given to support of the educational component of academic medical center activities with the intent that the production of physicians and other health care personnel by such centers be assigned the highest possible priority" (Carnegie Commission, 1970d).
A general report entitled Financing Medical Education - An Analysis o f Alternative Policies and Mechanisms was prepared by Rashi Fein and Gerald I. Weber for the Carnegie Commission on Higher Education in 1971. The content of this report is based heavily on economic principles. Fein and Weber still tie better health care to an increase in the number of physicians and other health care personnel and re-emphasize the problems of physician distribution. The authors analyze these increases from an economic stand- point which stresses input (resources)-output (educated personnel) relation- ships. This seems to be the beginning of an analysis of health manpower which questions previous ideas promoting substantial increases in physicians and other health care personnel. Rather than basing better health care exclusively on increases in numbers, the authors examine other relationships dealing with the effectiveness and efficiency of the training process and health care delivery system. There are two. ways of analyzing this approach. One is, that if the training process and delivery system were more efficient then more personnel could be produced with the same resources. This is in response to those who claim that increases in the number of personnel can not be accomplished without parallel increases in financial support. On the other hand, if one examines the concept of improving the quality of health care in the U.S. from this standpoint, sheer increases in numbers may not be the only solution. A more efficient training program and delivery system may produce improvements in quality with only modest increases in personnel. In this context, Fein and Weber analyze training programs in relation to the needs for improvement in the quality of health care. The obvious question here is, are present training programs producing the personnel in line with identified needs? The answer to this question is in part related to the problems of distribution. But from an "economic" standpoint, one could argue that certain modifications in training programs could be made to meet needs without substantial increases in personnel. How effective are current training programs in meeting the needs of quality health care?
Fein and Weber also present an "economic" analysis of the relationship between the number of physicians and "other" health care professionals and

322
the quality of health care in the U.S. The point here is that quality health care may not be entirely related to the number of physicians but includes the efforts of a number of different professionals functionhlg as a health care team. The suggestion then is that training programs are needed to produce more health professionals other than physicians.
Quality health care must be based on the sum total of its parts. Fein and Weber attempt to identify these parts and then apply economic principles to the best mix of these parts. The mix then should represent the most effective and efficient means of accomplishing the desired end - better health care.
In 1976, the Carnegie Council (previously called the Carnegie Commis- sion) issued the report Progress and Problems In Medical and Dental Educa- tion - Federal Support Versus Federal Control. Medical and dental education were again singled out because of "special controversies that have arisen over federal policies toward the training of physicians and dentists that are not present in the training of other health manpower" (Camegie Council, 1976a).
Again, the reason for presenting these reports is two-fold: one, to gain a historical perspective of the federal government's involvement in medical education (identify trends - predict future action); and two, to promote the participation of those outside governmental offices in the legislative process. These Carnegie reports are a form of participation and have shown to be influential. As an example, the Comprehensive Health Manpower Act of 1971 (see outline below), was strongly influenced by the 1970 Carnegie Commission report, Higher Education and the Nation's Health (described above). Other examples of results of this participation and influence are listed below:
1. The principle of providing a basic and continuing federal floor of sup- port for medical and dental schools in the form of capitation (per student) payments. 2. The provision of bonuses to the schools for expansion of places and acceleration of programs. 3. The provision of federal funds for curriculum reform and innovation. 4. Federal funds for an adequate program of student grants and loans. 5. Federal support for the training of physicians and dental assistants. 6. Creation of a national health service corps (actually created under separate legislation, adopted by Congress toward the end of 1970). 7. Federal funds for construction and start-up grants for new medical and dental schools. (The Commission warned, however, that too many com- munities were seeking to establish new medical schools and that only nine new schools were needed to achieve adequate geographic distribution.) 8. Federal funds to support the development of area health education centers, which would be affiliated with university health science centers

323
and would perform all the functions of those centers except for the basic education of M.D. and D.D.S. candidates. The area health education centers, for which the Commission suggested 126 geographically distributed locations, would improve the quality of health training and health care in the areas, help to overcome problems of geographic maldis- tribution of health manpower, and remove the pressure in many com- munities for the establishment of new medical schools (Carnegie Council, 1976b).
The 1976 report of the Carnegie Council represents a dramatic turnaround in recommendations related to increases in enrollments and the establish- ment of new medical schools. For the first time, the Council openly suggests that U.S. medical schools are currently producing an adequate supply of physicians, based on previous projections and, in fact, may be producing a surplus. This report also recognizes the problem of physician maldistribu- tion but ties this directly to incentives and training programs rather than increasing the number of physicians.
Reporting on findings in the spring of 1970 which estimated that there was a shortage of 50,000 physicians in the U.S., the Council found that between 1970 and the end of 1975 the number of physicians and osteopaths rose by about 55,000 (Carnegie Council, 1976c). This evidence seems to indicate that the shortage of physicians in absolute numbers is over and, in fact, at this production rate a surplus may be developing. The counter- arguments are obvious, however, and include the geographic maldistribution of physicians and the development of an "over-supply" of specialists'and an "under-supply" of primary care physicians. Under these conditions the Council Report includes several "warnings" and recommendations. These "wamings" and recommendations related to increases in the number of medical students and the impact of new medical schools are restated below.
At the time of this report (1976) there were 114 medical schools and 13 new medical schools at some stage of development with other additional schools also being proposed. To protect against an excessive increase in the number of physicians (at great costs) the Council believes that most of these developing and proposed schools are unnecessary and issues the following warning:
Warning: We are in serious danger of developing too many new medical schools, and decisive steps need to be taken by both federal and state governments to stop this trend (Carnegie Council, 1976d).
This Council report also examines the issues centered around foreign medical graduates as they relate to physician supply problems. The basis for the connection to the supply problem is that the U.S. in the past has been

324
too dependent on the inflow of foreign medical graduates and by the "early 1970's about one-fifth of all practicing physicians and nearly one-third of those in internships and residencies were foreign medical graduates (FMGs)" (Carnegie Council, 1976e). This situation coupled with the position that the physician shortage no longer exists would only lead to larger potential surpluses. With this in mind the Council issued the following warning.
Warning: The time has come to cease relying on foreign medical graduates to meet the need for physicians in the United States. The number of U.S. medical graduates is now increasing so rapidly that we can expect ample future increases in supply from existing medical schools (Carnegie Council, 19760.
The Carnegie Council considers the problems of physician maldistribution and the disproportion of primary care physicians to be serious and of high priority. Again, these problems have been detached from the absolute number of physicians. In solving these problems, however, the Council emphasizes that federal initiatives should be in the form of incentives, not rigid controls. These incentives should be offered to physicians to practice in underserved areas and to educational institutions for developing appropriate training programs. The Council's warning and recommendations are given below.
Warning: There is a critical danger that concern over geographic maldistri- bution of health manpower and overspecialization in medicine will lead to excessive and unwieldy federal controls rather than to policies emphasiz- ing incentives to effect the required changes (Carnegie Council, 1976g).
Urgent recommendation: The geographic disparities in the supply of health manpower will be overcome only with great difficulty and through a combination of policies that provide positive incentives for physicians, dentists, and other health professionals to practice in underserved areas. There should be more effective coordination among existing federal programs and greater emphasis on federal-state cooperation in over- coming geographic maldistribution (Carnegie Council, 1976h).
Urgent recommendation: The federal government should continue to provide incentives for both students and schools to emphasize primary- care training, rather than establish complex federal controls (Carnegie Council, 1976i).

325
Before entering into a discussion of the current statistics, the stage can best be set by continuing in a more detailed context those statistics and circumstances presented in the above-mentioned 1976 Carnegie Council Report. Previous projections and actual statistics are used as a basis for both presenting the current scene and to make recommendations on the findings (facts).
As stated above, a major question presented in this report regards whether or not there is a physician shortage or in fact a production rate that will eventually (in the near future) produce an oversupply (surplus) of physicians. The analysis at this point deals with absolute numbers and subsequent ratios per segments of a population and not with problems of distribution (see above). "The increase in the size of medical school entering classes has been more rapid than expected (see 1970 Carnegie Commission projections) - from 11,300 in 1970 to 15,300 in 1975, or 35 percent" (Carnegie Council, 1976j). The Commission's 1970 projection for 1975 was 14,700 with a projection for 1978 of 16,400. It was suggested that when the 1978 projections were attained, demand and supply relationships should be re-examined. These increases have been accomplished in two w a y s - established schools increasing their enrollments and the establishment of new schools. The force behind the increases has been demand-supply relationships with the main initiator (and controller) being the federal government. Pressures to increase minority segments have also, at least in an indirect way, contributed to the increase of graduates.
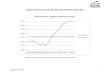
By examining ratios of physicians to population segments (100,000), the increase in physician supply is clearly evident. Estimates prepared by ~lum- berg in 1971 revealed ratios of 147 in 1967, 154 in 1972, and 182 by 1987 with the actual ratio in 1972 being 167 (Carnegie Council, 1976k). It should be noted here that these ratios were based on the highest projections of medical school entrants. In another projection, former HEW secretary, Casper W. Weinberger, estimated that ratios would rise to between 207 and 217 by 1985 which would put the U.S. near the top of all industrialized nations (Carnegie Council, 19761). Weinberger's estimates included a 40 percent reduction in the inflow of FMGs on the basis that as the domestic supply of physicians (who are better trained) increases, the demand for foreign trained physicians will decrease. As mentioned above, if this decrease does not occur naturally (supply-demand for quality) or by external controls (government policies) then a physican surplus could indeed be a reality and a costly one at that.
One argument supporting the influx of FMGs is to help overcome the problem of physician maldistribution. While the inclusion of FMGs increases the physician/population ratio, their inclusion in the U.S. health care system does not necessarily solve the distribution problem. It was found that in 1970, FMGs "represented the highest percentages of physicians in New York

326
(35 percent), Rhode Island (30 percent), and Illinois (28 percent), which have tended to be states with comparatively high physician/population ratios, whereas FMGs tended to account for small proportions of physicians in most of the southern states, which have had the lowest physician/popula- tion ratios" (Carnegie Council, 1976m). Some other interesting facts reveal that only about one-third of the FMGs were in an office-based practice com- pared to two-thirds for U.S. and Canadian graduates. Also, most FMGs were practicing in institutions not affiliated with a medical school.
The point to be made here is that the line between the number of physicians, as an indication of access to medical care, and high quality medical care is becoming more distinct since higher quality domestic training institutions are able to produce a sufficient physician supply to meet the access demands. With sufficient numbers established, the emphasis has shifted to quality. Other socio-economic factors began to receive more attention - especially those related to physician maldistribution.
The impact of new medical schools is obvious. The emphasis of the past has been to increase the enrollments of established schools. This has been accomplished to such a degree that all projections have been exceeded and the possibility of a surplus exists. Therefore, the establishment of new medical schools is questionable in the least. However, the Carnegie Council Report of 1976 suggests that there is some basis for new medical schools if they tend to ameliorate the problems associated with the geographic distribution of health manpower (not physicians only). The basis for this support lies in the fact that medical schools do attract health personnel. The evolution of such subsequent growth can be termed an area (regional) health education-service center. Certainly, medical schools (centers) do attract health manpower. However, other studies have shown that physicians tend to practice in the city, county, state, or region of their post-graduate experience. In any event, the Carnegie Commission would encourage the establishment of new medical schools if their impact was positive in distributing health manpower and services.
As a bench mark in 1970, the Carnegie Commission suggested that every metropolitan area with a population of 350,000 or more should have a university health science center (Carnegie Council, 1976n). Several centers were identified as needing medical schools. In most of these areas (7 of 9), new schools or branches of existing schools were built. The issue brought up by the Commission was that 13 new medical schools were being planned and developed in areas not recommended by the Commission. The Commission's view of course is that some of these new schools are not needed to increase the number of graduates and most are not in the best interests of overcoming the problems of physician distribution. A summary of the bases for the warning (stated above) that we are developing too many medical schools is given below.

327
1. The increase in medical school entrants and graduates was even more pronounced in the first half of the 1970's than had been predicted and will continue to be substantial for a number of years without the con- tributions of schools that have not yet enrolled any students. 2. It is a virtual certainty that the physician/population ratio will reach unprecedented levels by 1985, even if the net inflow of FMGs is drastical- ly curtailed. 3. The cost of establishing a new medical school is exceedingly high. 4. Communities that lack a medical school can, in most cases, be served more effectively and at much more modest cost by an area health educa- tion center than by a full-fledged medical school (Carnegie Council, 19760).
Congress has reflected this lack of need by drastically reducing authorization levels for construction grants, particularly for medical schools.
Statistics of the current situation tend to manifest earlier warnings and re- emphasize past recommendations. Current statistics used in this report were taken from the 78th annual report on medical education as published in the Journal o f the American Medical Association.
Current statistics, as of October 1978, include 112 U.S. medical schools and 16 Canadian schools fully accredited to award the M.D. degree. One school is fully accredited to offer the first two years of medical school while eleven others have provisonal accreditation. As of the fall of 1978, 122 schools existed in the United States with either full or provisional accreditation to offer the M.D. degree (AMA, 1978a). Several bther additional medical schools are in the planning and developing stages and will be seeking some type of accreditation in the near future. Compounding the situation is the development of a host of foreign medical schools, most of which are not accredited. Subsequently, the potential total of medical schools exceeds previous projections and recommendations and personifies the earlier warnings that we are developing too many new medical schools.
Logically, the next step is to examine the current supply of graduates produced by increasing enrollments and additional new schools. In the 1 9 7 7 - 7 8 academic year there were 60,456 students enrolled in 122 accredited or provisionally accredited medical and basic science schools. This number is an increase of over 2,000 students as compared to the previous year. The first-year class of 1 9 7 7 - 7 8 included 16,134 students. Table II lists the numbers of schools, graduates, and students from 1940-1978 . Table III projects the number of new first-year students and subsequent graduates of 122 medical schools for the next five academic years.
Because the demand (number of applicants) far exceeds the number of positions available in U.S. medical schools, several "medical schools" have

328
TABLE II
Students and Graduates in Medical and Basic Science Schools
Year No. Total First- Intermediate Graduates Schools 1 Enrollment Year Years
1940-1941 77 21,379 5,837 10~67 5,275 1945-1946 77 23,216 6,060 11,330 5,826 1950-1951 79 26,186 7,177 12,874 6,135 1955-1956 82 28,639 7,686 14,108 6,845 1956-1957 85 29,130 8,014 14,320 6,796
1957-1958 85 29,473 8,030 14,582 6,861 1958-1959 85 29,614 8,128 14,626 6,860 1959-1960 85 30,084 8,173 14,830 7,081 1960-1961 86 30,288 8,298 14,996 6,994 1961-1962 87 31,078 8,483 15,427 7,168
1962-1963 87 31,491 8,642 15,585 7,264 1963-1964 87 32,001 8,772 15,893 7,336 1964-1965 88 32,428 8,856 16,163 7,409 1965-1966 88 32,835 8,759 16,502 7,574 1966-1967 89 33,423 8,964 16,716 7,743
1967-1968 94 34,538 9,479 17,086 7,973 1968-1969 99 35,833 9,863 17,911 8,059 1969-1970 101 37,699 10,401 18,901 8,367 1970-1971 103 40,487 11,348 20,165 8,974 1971-1972 108 43,650 12,361 21,738 9,551
1972-1973 112 47,546 13,726 23:29 10,391 1973-1974 114 50,886 14,185 25,088 11,613 1974-1975 114 54,074 14,963 26,397 12,714 1975-1976 114 56,244 15,351 27,332 13,561 1976-1977 116 58,266 15,667 28,992 13,607 1977-1978 122 60,456 16,134 29,929 14,393
1 Prior to 1956-1957, schools in development were not included. Source: AMA (1978b). "78th Annual Report on Medical EducaUon in the United States (1977-78)," Journal o f the American Medlcal Association 240 (26): 2822, Table 6. Reprinted with permission.
emerged on foreign soil. Previously, this "demand" was one of the bases for increasing enrollments. But as enrollments increased and warnings of surpluses arose, this demand has taken a new meaning. The result is that large numbers of U.S. citizens are enrolling in foreign medical schools as a way of obtaining an M.D. degree with the anticipation of returning to the U.S. to practice medicine or gaining admission at some stage to the educational-training process. These schools are typically lower in quality than U.S. schools and most are not accredited by the LCME. A combination of things such as increased domestic enrollments, the demand for the highest quality of medical care available and more restrictive policies by both federal

TABLE III
New First-Year Students and MD Graduates Projected by 122 Medical Sehools (Spring 1978)
329
Year First-Year MD Graduates Class
1978-1979 15,977 15,123 1979-1980 16,290 15,539 1980-1981 16,462 16,102 1981-1982 16,604 16,319 1982-1983 16,636 16,582
Source: AMA (1978). "78th Annual Report on Medical Education in the United States (1977-78)," Journal o f the American Medical Association 240: 2822, Table 7. Reprinted with permission.
and state governments concerning FMGs have all diminished the demand and opportunities for health manpower trained in this way. James R. Schofield, M.D., head of the AAMC's accreditation department has strongly criticized some of these new foreign schools and has stated very bluntly that "the students who go there will never have a chance to practice medicine in this country" (Caribbean Schools, 1977). John A.D. Cooper, president of the AAMC, stated that "these schools do not have the resources to provide an adequate education. Tuitions are high, application procedures are expensive and the students will have difficulty obtaining a license to practice in the United States" (Maeroff, 1977).
In making concluding remarks, the structure of this paper has been to develop a position, based on a historical context, that further increazes in medical school enrollments and additional new medical schools are no longer needed. The only cases in which new medical schools (within area health centers) would be recommended is for the purposes of overcoming geographic maldistribution of health manpower and for the purposes of improving health care, and educational and training opportunities, in areas with high concentrations or populations of minorities. The number of first-year entrants, the number of graduates, and physician ratios have all met or in some cases exceeded projected needs for high quality health care. These needs have been established through a number of studies, mainly by private organizations but carry governmental approval as noted above in various policy changes and conditional "incentives". To reiterate and emphasize this point Congress included in a policy statement for the Health Professions Educational Assistance Act of 1976 that the "Congress further finds and declares that there is no longer an insufficient number of physicians and surgeons in the United States such that there is no further need for affording preference to alien physicians and surgeons in admission to the United States under the Immigration and Nationality Act."
The position of this paper obviously echoes those warnings and supports

330
those recommendations issued by the Carnegie Council in its 1976 report. What is the evidence that supports warnings of potential surpluses? Robert M. Hendrickson, in an article entitled "Shortage to Surplus?", summarizes some data that dramatizes past increases to the point that potential surpluses can be anticipated. Some of this data over the past 25 years include:
1. A 28% increase in the ratio of physicians to population. In 1950, there were 141 doctors for every 100,000 persons. By 1975, the number had grown to 181 per 100,000 population. 2. A 44% increase in medical schools. In 1950 we had 79 medical schools, in 1975, 114. 3. A 121% increase in medical school graduates. In 1950-51 U.S. medical schools produced 6,135 physicians. By 1975-76 the total number of graduates reached 13,561. 4. A 180% increase in newly licensed physicians (including foreign medical graduates). In 1950 6,002 new licentiates; by 1975; 16,859. (Hendrick- son, 1977).
This data, accompanied by the current statistics listed above and projected figures, clearly indicate an impending over-supply or at the very least an adequate supply if current levels are maintained.
Producing physicians and other health care professionals is certainly an expensive endeavor. Those who maintain that increasing the supply of health professionals, even to the point of an over-supply, would result in lower costs for health care, may not find this to be the result. Reinhardt suggests that an over-supply would actually increase costs and expenditures since economic demand-supply relationships do not exist in the medical profession (Reinhardt, 1977). An increase in supply would simply increase the demand for services with consumers willing to pay the going rates which would not necessarily be lowered. Reinhardt also emphasizes the high costs passed on to society that are needed to produce each additional physician.
The impact of new medical schools would add a new dimension to an impending surplus. "Unplanned" new medical schools also are contributing to the distribution problem in the name of physician supply to satisfy "needs". The geographic distribution of health manpower is a real problem that must be considered. Increasing the number of physicians and adding new medical schools will not solve the problem. A great variety of factors beyond sheer numbers of personnel must be analyzed and included in the context of the distribution problem. Incentives at both the educational training program level and at the point of practical application are suggested as being positive alternatives to increasing the number of physicians. The caution emphasized here is that there be a difference between incentives being supportive and not controlling.

331
The positions taken in this paper were emphasized in an address of DHEW Secretary Joseph A. Califano, Jr., to a plenary session of the annual meeting of the Association of American Medical Colleges on October 24, 1978. A fitting conclusion is a summarized selection of the points made by Califano:
1. Medical schools are producing too many doctors. An over-supply of doctors is predicted within the next decade. 2. The number of medical graduates has virtually doubled since 1963. The physician]population ratio has increased from 143 per 100,000 in 1960 to 177 per 100,000 today. By 1990 he estimates the supply of physicians to increase another 57 percent to 594,000 active physicians or a ratio of 242 physicians per 100,000 people. 3. An excess or over-supply of phsicians will increase health caxe costs. The supply of physicians and total health care costs do not necessarily follow basic economic price-supply-demand relationships. 4. The general rule will be to discourage enrollment increases and the estabfishment of new medical schools except under unusual and compelling circumstances. 5. The central problem is physician maldistnq~ution both geographically and in specialty applica- tion.
Appendix I
Only those sections of federal programs related to numbers of health personnel and educational programs are included. The outline up to the 1971 Act represents a selection from the efforts of Grupenhoff and Strickland (1972).
1. 1964 Amendment (P.L. 88-654) of HPEA of 1963: a. included students of optometry in the loan program to increase the
number of optometrists.
2. Nurse Training Act (Amendments to the Public Health Service Act) of 1964 (P.L. 88-581): a. matching grants for the construction and rehabilitation of teaching
facilities; b. curriculum improvement grants; c. 1966 (P.L. 89-751) - additional authority for grants and support of
loan funds.
3. HPEA Amendments of 1965 (P.L. 89-290) a. extended construction and student loan programs for three years; b. increased construction authorization; c. expanded loan program to students of pharmacy and podiatric
medicine; d. increased loan amount to $ 2500 and helped support schools share of
loan fund;

332
e. introduced provision of 50% forgiveness of loans for serving in a man- power shortage area;
f. formula grants for scholarships; g. basic and special improvement grants.
4. Veterinary Medical Education Act of 1966 (P.L. 89-709): a. amended HPEA Act to extend construction grants and studentqoan
programs to schools of veterinary medicine.
5. Allied Health Professions Personnel Training Act of 1966 (P.L. 89-751): a. new-aid programs for training in allied health professions; b. increased loan forgiveness amounts; c. established student loan revolving fund;
6. Health Manpower Act of 1968 (P.L. 90-490): a. extended HPEA for two years; b. expanded construction grants to include teaching space in multi-
purpose facilities; c. increased construction grant matching from 50% to 66.66% in some
cases; d. provided for construction of teaching space in hospitals; e. included construction of space for graduate, continuing and advanced
training; f. extended and expanded support of nursing schools; g. extended student loan program with minor changes.
7. The comprehensive Health Manpower Training Act of 1971 (P.L. 92-157) (and companion Nurse Training Act) - to amend Title VII of the Public Health Service Act:
Note This act became the most comprehensive piece of health manpower legislation to date. The 1971 Act extended and expanded the 1963 Act. It also added several new programs with the general
purpose of increasing the number of physicians and other health care professionals ("national goal"). A shift from support to control was evident in this bill. The federal government was becoming more concerned with products than process and physical facilities. Capitation grants based on the number (especially increases in numbers) of students began to erode construction grant funds - a previous top priority.
a. construction support: 1. extended construction grants to health education facilities; 2. start-up grants; 3. loan guarantees and interest subsidies;
b. formula (capitation) grants to Health Professions Schools: 1. replaced previous institutional grants;

333
2. specified amounts per student which were designed to increase enrollments and shorten curriculums;
3. conditioned these grants on specified enrollment increases and participation in a number of special projects;
c. payments to two-year schools of medicine converting to M.D. degree schools;
d. start-up assistance grants: 1. for schools of medicine, osteopathy, and dentistry;
e. health manpower education initiative awards: 1. encourage new programs designed to alleviate health manpower
shortages and improve the delivery of health care; f. student aid (loans):
1. extends HPEA loan program; 2. provides loans to U.S. students in foreign medical schools; 3. forgiveness allowances on loans for practicing in a shortage area; 4. increased loan maximum;
g. scholarships: 1. based on a formula and student financial need; 2. special allocations to students who agree to practice in a shortage
area; 3. available to U.S. students in foreign medical schools;
h. physician shortage area scholarship program: 1. awards scholarships to students who agree to practice primary care
in a shortage area - service payback requirement; i. training in family medicine:
1. grants to hospitals for training, traineeships, and fellowships in family medicine;
j. graduate training for physicians and dentists: 1. capitation grants for hospitals and schools providing graduate
training in primary care or other shortage area; k. training for health professions teaching personnel:
1. authorizes project grants.
8. Continued resolutions of the 1971 Act for fiscal years 1975 and 1976.
9. The Health Professions Educational Assistance Act of 1976 (P.L. 94-484) - amend Public Health Service Act (Title VIII), and revise the National Health Service Corps program and scholarship training program
and
The Amendment: Health Services Extension Act of 1977 (P.L. 95-83, Title III)

3 3 4
a n d
T h e A m e n d m e n t : P .L . 9 5 - 2 1 5 , D e c e m b e r , 1977
Note: Generally, the HPEA Act of 1976 extended most of the provisions of the Health Manpower Act of 1971. Differences are in degree of both federal support and control. Conditions for funds have been both redefined and have become morn stringent. The emphasis of producing greater numbers of health professionals has changed to specific programs (primary care, ambulatory services, etc.) and the problem of geographic distribution of health professionals. Congress proclaims in this Act that " . . . there is no longer an insufficient number of physicians and surgeons in the United S ta tes . . . " Congress re-states that high quality health care is a national goal and that health professionals are a national health resource Therefore, the federal government establishes in thts Act the responsibihty to assure that the American people have qualified personnel available to meet their needs. Subsequent- ly, "appropriate" federal support should be directed and focused on specific programs to meet this national goal.
Most exasting authorities are extended without change through FY 1977 Most of the new authorities go into effect in FY 1978 and extend for a period of three years. National Health Service Corps Scholarships authorizations have been greatly increased. Capitation funds are continued with additional conditions and restrictions attached to their receipt (specified percentage of residents in primary care and the requirement of admitting a specified number of U.S. students studying at foreign medical schools). It should be noted here that the U.S.F.M S. issue has been heatedly contested and as of December 1977, after Senate rejection, conference committee compromise, and compromise approval and acceptance by both houses, the provisions of this condition have been greatly modified but the residuals are slall attached to capitation funds. A few of the major provisions of this Act as presented in the Fact Sheet are included in the following outline(DHEW 1977)
a. c a p i t a t i o n g r a n t s :
1. e x p a n d s t o i n c l u d e p u b l i c h e a l t h s c h o o l s ;
2. d e c r e a s e s in a u t h o r i z a t i o n a m o u n t s f r o m p r e v i o u s A c t s ;
3. m e d i c a l s c h o o l s m u s t have a s p e c i f i e d p e r c e n t a g e o f p r i m a r y ca re
r e s i d e n t s in a f f i l i a t e d p r o g r a m s ;
4 . U . S . F . M . S . c o n d i t i o n s ;
5. s p e c i f i c c o n d i t i o n s o n s c h o o l s o f p u b l i c h e a l t h , d e n t i s t r y , o s t e o -
p a t h y , v e t e r i n a r y m e d i c i n e , o p t o m e t r y , p o d i a t r y , a n d p h a r m a c y
( e n r o l l m e n t i n c r e a s e s a n d t y p e o f p r o g r a m s ) ;
b . h e a l t h p r o f e s s i o n s s p e c i a l p r o j e c t s / g r a n t s c a t e g o r i e s ;
1. d e p a r t m e n t s o f f a m i l y m e d i c i n e ;
2. f a m i l y m e d i c i n e , g e n e r a l d e n t i s t r y t r a i n i n g ;
3. g e n e r a l i n t e r n a l m e d i c i n e , g e n e r a l p e d i a t r i c s ;
4. p h y s i c i a n a s s i s t an t s , e x p a n d e d f u n c t i o n d e n t a l a ux i l i a r i e s , d e n t a l
t e a m s ;
5. a s s i s t ance t o d i s a d v a n t a g e d s t u d e n t s ;
6. o c c u p a t i o n a l h e a l t h t r a i n i n g c e n t e r s ;
7. e m e r g e n c y m e d i c a l s e rv i ces t r a i n i n g ;
c. c o n s t r u c t i o n a s s i s t a n c e :
1. o f t h e t o t a l a p p r o p r i a t i o n 50% is o b l i g a t e d fo r t h e c o n s t r u c t i o n o f
a m b u l a t o r y f ac i l i t i e s ;

335
2. the other 50% is for health professions and public health schools; 3. maximum federal share is 80%; 4. FY 1977 only - authority for VOPP schools to expand or establish
regional health professions programs; d. student assistance:
1. NHSC scholarships have been revised, expanded, and authorizations have increased g r e a t l y - service obligation pay-backs are estab- lished;
2. Lister Hill scholarships - limited to students who agree to enter family practice in a manpower shortage area;
3. health professions loan repayment program - applies mainly to HPSL ' s - establishes forgiveness percentages for service in pre- scribed areas;
4. Indian health scholarships - established as a separate authority by the Indian Health Care Improvement Act (P.L. 94-437);
e. foreign medical graduates: 1. because of the declaration by Congress that there is no longer an
insufficient number of physicians, special regulations have been provided to restrict the entry of alien physicians;
f. allied health programs: 1. special projects for the development of allied health personnel and
programs; g. public health and health administration programs;
1. special projects; 2. public health traineeships; 3. health administration grants; 4. health administration traineeships;
h. other provisions: 1. definition and designation of shortage areas; 2. health manpower data collection by HEW; 3. shared residency positions in family practice and primary care
programs.
References
American Medical Association (1978). "78th Annual Report on Medical Education in the United States (1977-78)" , Journal o f the American Medical Association 240 (26), Dec. 22•29, a = pp. 2819-20 , b = p. 2822, Tables 6, 7.
"Caribbean Schools Criticized by AAMC Official" (1977), American Medwal News, Nov. 28: 3. The Carnegie Commission on Higher Education (1968). Quality and Equality. New Levels o f Federal
Responsibility for Higher Education New York: McGraw-Hill, a = pp. 32 - 36 , b = p. 34. The Carnegie Commission on Higher Education (1970). Higher Education and the Nation's Health -
Policies for Medtcal and Dental Education. New York' McGraw-Hill, a = p. 1, b = p. 18, c = pp. 101-106, d = pp. 103-104, e = p. 42,

336
The Carnegie Council on Policy Studies in Higher Education (1976). Progress and Problems in Medical and Dental Education - Federal Support Versus Federal Control. San Francisco: Jossey-Bass, a = p. xi, b = pp. ix -x , c = p. 1, d = p. 3, e= p. 6, f= p. 8, g = p. 6, h= p. 11, i= p. 12,j =p. 23, k = p. 24, 1 = p. 24, m = p. 27, n = p. 86, o = pp. 90-92.
Grupenhoff, John T. and Strictland, Stephen P. (1972). Federal Laws: Health/Environment Man- power. Washington, DC: The Science and Health Communication Group, pp. 1-41.
Health Professions Educational Assistance Act of 1976, Public Law 94-484, Washington, DC, October 12, 1976, a = See. 2. (c), b = Sec. 2. (a).
Hendrickson, Robert M. (1977). "Shortage to surplus?", American Medical News Nov. 28: Impact Section, p. 1.
Maeroff, Gene I. (1977), "New schools in Carribean worry medical educators," New York T~mes June 15.
Reinhardt, Uwe (1977), "Health cost culprit may be manpower policy, argues economist," Health Manpower Report July 20: pp. 4 - 5 .
U.S. Department of Health, Education, and Welfare (1977). "HPEA Act of 1976 (P.L. 94-484), Amended by Health Services Extension Act of 1977 (P.L. 95-83, Title III);'Fact Sheet, Revised Sept. 1, 1977, pp. 1-26.