Embed Size (px)
Citation preview

The Impact of Education, Income, and Mortality on
Fertility in Jamaica
SUDHANSHU HANDA *
International Food Policy Research Institute, Washington, DC, USA
Summary. Ð The socioeconomic determinants of cumulative and recent fertility are investigatedwith micro data from Jamaica, a middle-income country with low rates of infant mortality andtotal fertility. Infant mortality has a signi®cant nonlinear in¯uence on fertility, peaking at amortality rate of 0.46. Both education and income have strong negative e�ects on births but theimpact of education is larger; for rural women the birth elasticities are ÿ0.15 and ÿ0.45 for incomeand education, respectively. Finally, the transmission of the education e�ect appears to be throughraising the value of time of the woman rather than changing preferences. Ó 2000 Elsevier ScienceLtd. All rights reserved.
Key words Ð fertility, infant mortality, education, Jamaica, Caribbean
1. INTRODUCTION
This paper investigates the socioeconomicdeterminants of fertility in Jamaica using one ofthe World Bank's Living Standard Measure-ment Surveys (LSMS)Ðthe Jamaica Survey ofLiving Conditions (SLC). Two speci®c ques-tions regarding the fertility decision are dealtwith. First, what is the impact of infantmortality on fertility in a low fertility society?Second, is the impact of female educationlarger than the impact of income in reducingfertility? Some initial explorations are alsoprovided on the way female education a�ectsfertility behavior: does education alter tastesfor children or does it increase the value of timeof the woman?
Unlike other developing countries whereLSMS data sets have allowed the opportunityto study fertility decisions, Jamaica is well onits way along the epidemiological transition, soits health problems resemble those of moredeveloped countries (Peters, 1994). Hence theoverall disease burden in Jamaica comes fromlife-style related noncommunicable chronicdiseases such as hypertension, heart disease,and nuero-psychiatric conditions includingsubstance dependency and schizophrenia.
Jamaica's impressive social developmentrecord in general, and success at combattinginfectious and childhood diseases in particular,are re¯ected in its gross indicators of health,
fertility and education. In 1970 the total fertilityrate (TFR) was 5.3, above the 4.6 average formiddle income countries (World Bank, 1994and various years). In 1993 the TFR was 2.5and below the 3.0 mean for middle-incomecountries. In this same time period infantmortality per 1,000 births dropped from 46 to15, well below the mean of 43 for middle-in-come countries (World Bank, 1994). Finally,primary school enrollment is universal, andfemale enrollment and grade attainment isactually higher than that of males.
Despite making the transition to a low-fer-tility society, Jamaica still su�ers from popu-lation pressure because of its small physicalsize. Population density is 218 per squarekilometer which is eight times the average formiddle-income countries and one of the highestin Latin America. This population pressure isputting enormous strain on Jamaica's envi-ronment. For example, during 1981±85 theaverage annual deforestation rate was 3.0%
World Development Vol. 28, No. 1, pp. 173±186, 2000Ó 2000 Elsevier Science Ltd. All rights reserved
Printed in Great Britain0305-750X/00/$ - see front matter
PII: S0305-750X(99)00114-Xwww.elsevier.com/locate/worlddev
* Thanks to the Planning Institute of Jamaica for kind
permission to use the data, Bill Milne for encouragement
and valuable discussion, and two anonymous referees
for useful comments. This research was conducted while
I was a Lecturer in the Department of Economics,
University of the West Indies-Mona, Jamaica. All errors
are my own. Final revision accepted: 25 May 1999.
173

compared to an average of 0.9% for all devel-oping countries (UNDP, 1994).
The next section of the paper describes thetheoretical framework guiding the analysis offertility behavior; section 3 presents the dataand variables used in the empirical estimationof the impact of infant mortality, income andeducation on fertility; results are presented anddiscussed in section 4 and section 5 concludesthe paper.
2. ANALYTICAL FRAMEWORK
The conceptual framework guiding theempirical implementation is a New HouseholdEconomics Model emphasizing the fact thathouseholds are both consumers and producersof goods and services (Becker, 1965). Thismodel is well known (Becker, 1981; Birdsall,1988; Rosenzweig & Schultz, 1983), and can beused to derive the demand for children as afunction of a set of exogenous variables whichcan be classi®ed into three broad groups, bio-logical, economic, and social or culturalÐhereI focus on the economic determinants of thefertility decision. Write the reduced formdemand for children as
F � F �M ;H ; P ; l�: �1�In this particular speci®cation, M representscharacteristics speci®c to the mother, H and Pare vectors of household characteristics andprices respectively, while l is a random errorwith the usual properties.
Variables speci®c to the mother include hereducation, age, previous fertility history, andher current union or marital status. Childservices are time intensive, hence the value of awoman's time (measured by the wage rate) is animportant cost in the household production ofchildrenÐin the absence of data on wages,education is often used as a proxy for the valueof time. In Jamaica a woman's education isstrongly associated with her earnings (Handa,1995) and is thus expected to have a negativeimpact on fertility. Education can also in¯u-ence the supply of children by changing tastes,through improvements in health and nutrition,and by increasing the e�ective use of birthcontrol as in ``synthesis'' models of fertility.While it is typically di�cult to disentangle thevarious e�ects of eduction on fertility, I explorethe extent to which education in¯uences ``tast-es'' for children by observing its impact on the
number of children a woman desiredÐthis isdiscussed further in section 4.
Age is the primary biological factor in¯u-encing fertility, at ®rst positively, but thennegatively due to malnutrition, disease andmenopause. A woman's fertility history, inparticular the proportion of previous birthsthat have died, will be correlated with maternaldepletion and weaning and thus also in¯uencethe biological capacity for children. Infantmortality can also illicit two types of behavioralresponses from mothers. First, a replacementresponse will induce additional children toreplace the ones who die. Second, an anticipa-tory response will cause women to adapt theirfertility behavior to known existing levels ofchild mortality. The latter behavior will bemore common in high fertility societies; a mainfocus of this paper is to explore the relationshipbetween child mortality and the number ofbirths. The potential simultaneity betweenmortality and fertility is discussed in the nextsection.
Finally, a woman's demand for children willbe a�ected by her social and culturalsurroundings. These include the degree ofurbanization, the typical age of entry into long-term marital unions, and attitudes (religious orotherwise) toward sexual intercourse. Tomeasure the exposure to sexual intercourse adummy variable is used to indicate whether thewoman is currently in a stable marital union(either common-law or married) 1; religion isnot used since over 93% of Jamaicans practicesome form of Protestantism.
The primary household level variable ofinterest in this study is income, which will bepositively related to the demand for children ifchildren are normal goods. But if householdshave preferences over child quality and theincome elasticity for quality is greater than theincome elasticity for quantity, then income bemay have a depressing e�ect on the number ofchildren. Moreover, in some rural areas wherechild labor is an important source of familyoutput and thus wealth, income is found to bepositively related to the demand for children(Schultz, 1973), although this is unlikely to bethe case in the plantation-style agriculturetypical of Jamaica.
Finally, the availability and cost of contra-ception will in¯uence the demand for children,especially in low-fertility societies such asJamaica where families desire to control theircompleted family size. While the data set usedin this study does not contain information on
WORLD DEVELOPMENT174

the cost of family planning services, theseservices are primarily delivered through publichealth facilities so I include variables indicatingtravel time (in hours) to the nearest publichealth centre and public hospital (NationalFamily Planning Board, 1993). These traveltime variables are often used in reduced formdemand equations of human resource invest-ment in developing countries as a proxy forprices (Benefo & Schultz, 1994; Strauss, 1990).
3. DATA, EMPIRICAL SPECIFICATION,AND SUMMARY STATISTICS
The data used in the analysis come from thefertility module of the November 1989 round ofthe Jamaica SLC. 2 The fertility module of theSLC provides details on the number of births,deaths, and other fertility-related informationfor one woman age 15±45 in each household.This module is merged with various sections ofthe SLC to obtain information on age, educa-tion, region of residence and other relevantvariablesÐa total of 1,698 women are used inthe ®nal analysis of which 54% live in ruralareas.
A reduced form demand relationship is esti-mated using two common measures of fertilityas dependent variables: the total number ofsurviving births, and whether the woman waseither pregnant or had given birth in the last 12months, representing the ¯ow or addition to thestock of children. 3 I also present some reducedform regressions on the determinants of infantmortality, focusing on the economic factorsin¯uencing mortality and the interactionbetween education and community healthservices. Table 1 provides de®nitions andsummary statistics of the variables used in theanalysis.
Variables common to both fertility outcomesare total per capita household expenditure(proxy for income), age and age squared,highest grade completed and its square, adummy variable indicating if the woman ismarried or in a common-law union, travel timein hours to the nearest public health center andhospital, and the proportion of births that havedied and its square.
Per capita expenditure is used since the SLCdoes not contain income data; this is a commonprocedure in reduced-form household demandanalyses based on LSMS data sets because ofthe absence of reliable income data, andbecause expenditure tends to be more reliable
than income data in developing countries (e.g.,Thomas, Strauss & Henrique, 1990; Handa,1996). Household expenditure is treated asendogenous and predicted using durable goods,type of dwelling (detached house, apartment,etc), main material of outer walls (brick,concrete, adobe, etc.), and whether the house-hold received property income as identifyingvariables. The predicting regression had an R-square of 54% and is available from the authorsupon request.
The main empirical issue is the treatment ofthe mortality variable, which will be correlatedwith the error term of the fertility regressionsfor two reasons. First, there are likely to beunobserved factors (such as health-relatedknowledge) which a�ect both the propensity tohave children and their subsequent survivalprobability. Second, there is potential simulta-neity between the two variables since additionalbirths lead to maternal depletion (and lowerbirth weight babies) while infant mortalitycurtails breastfeeding which leads to earlyfecundity.
I follow the standard approach in the litera-ture by using the individual mortality rate ofeach woman instead of the number of deaths(Olsen, 1980; Hyatt & Milne 1993; Maglad1990; Chen, Bendarf & Hicks, 1987). In arecent paper, Benefo and Schultz (1994) treatthe mortality rate as endogenous as well, andinstrument it using health care access variables,but do not reject the null hypothesis of exoge-neity. 4 The mortality variable is included inquadratic form to allow for a ``discourage-ment'' e�ect whereby women curtail furtherattempts at childbirth after it becomes clearthat genetic or economic factors limit theirability to keep children alive.
The ¯ow regression contains two additionalvariables not included in the stock regression.The ®rst is the total number of surviving births(and its square) at the start of the period. Thusthe decision to have another child is posited todepend on the current number of survivingchildren. Note that since fertility decisions aresequential the number of children at thebeginning of the period can be consideredexogenous to the current decision of whether toinvest in another child.
The second is a desire variable, which takesthe value 1 if the woman desired another childat the beginning of the period. The desirevariable is constructed by subtracting thenumber of surviving children at the beginningof the period from the total number of children
FERTILITY IN JAMAICA 175

desired by the woman. If this di�erence ispositive (so that the woman desired more chil-dren than she had at the beginning of theperiod) the desire variable is set to 1.
The desire variable may be a source ofmisspeci®cation because it is constructed froma potentially problematic question: the numberof children a woman desires in her life. Womenmay rationalize their present family size andthus overstate the number of desired children,while others may understate the number ofdesired children based on previous child bear-ing experience (Rosenzweig & Wolpin, 1993). Itry and minimize the misspeci®cation by notincluding desired children directly in theregression and constructing the dummy vari-able instead, but in general it is hard to predictthe direction of bias if any, 5 and equally di�-cult to think of an instrumental variable that
would a�ect the desired number of children butnot current pregnancy. 6
In the estimates below I report a model where``desire'' is instrumented using 14 religiousdummies, age of menstruation, and age ofcohabitation for identi®cation. These estimates,however, should be treated with caution. Onlyage of cohabitation was statistically signi®cant,and in the urban subsample the joint test forsigni®cance of the instrumental variables had ap-value of 0.17.
Formal statistical tests rejected the nullhypothesis of equality of coe�cients acrossregions in all regressions, hence separatemodels are estimated for rural and urbanwomen. 7 The means in Table 1 indicate thatrural women have more births (2.27 vs. 1.91)and are more likely to have had a recentfertility experience (17.2% vs. 12.2%) than
Table 1. Means (St. Dev.) of variables
Variable Rural Urban
Endogenous variablesNumber of live births 2.266 1.912
(2.45) (2.07)One if currently pregnant or had child in last year 0.172 0.122
(0.38) (0.33)Number of child deaths 0.139 0.128
(0.47) (0.53)Exogenous variablesPredicted household per capita expenditures 8.326 8.804
(0.59) (0.58)Age in years 27.254 27.316
(8.21) (7.89)Age squared 810.094 808.239
(476.30) (457.71)Highest grade completed 9.168 9.679
(2.31) (2.21)Highest grade squared 89.365 98.562
(37.36) (37.66)One if married or in common-law union 0.503 0.443
(0.50) (0.50)Surviving births in previous period 1.998 1.695
(2.24) (1.89)Previous period births squared 9.667 6.799
(18.62) (13.71)One if desired children greater than surviving birthsin previous period (desire)a
0.622 0.635
(0.49) (0.48)Mortality rate 0.037 0.035
(0.14) (0.13)Mortality rate squared 0.021 0.019
(0.12) (0.10)Hours to nearest public hospital 0.230 0.043
(0.57) (0.22)Hours to nearest public health center 0.818 0.148
(0.93) (0.40)Observations 912.00 786.00
a 904 observations for rural and 776 observations for urban due to missing values for desired number of children.
WORLD DEVELOPMENT176

urban women. The number of deaths is alsoslightly higher in rural areas (0.139 vs. 0.128)although the mortality rate is virtually the same(3.7% vs. 3.5%). Jamaica's excellent socialdevelopment record mentioned earlier isre¯ected in a mean grade attainment of womenof approximately nine. 8 Note also that ruralhouseholds are poorer and must travel longerto get to a public health facility.
4. RESULTS
(a) Mortality
The ®rst two columns of Table 2 present thecoe�cient estimates for the regressions deter-mining the number of child deaths, and theyindicate considerable di�erences by region. Forurban women none of the point estimates aresigni®cant although the regression as a wholeis. In contrast both income and education aresigni®cant determinants of child mortalityamong rural women. The e�ect of education issmallÐan additional year of schooling at themean reduces the number of deaths by 0.019,and the turning point is approximately seven
years of schooling. On the other hand aproportional increase in per capita expenditurereduces the number of deaths by 0.055. 9
The availability of public health services doesnot have a signi®cant direct in¯uence onmortality. But the bene®t of these services onchild health may depend on the level of edu-cation of the child's mother. For example,better educated mother's may be more e�cientusers of local health services in which case theseservices would be complements to education inthe production of child health. On the otherhand, health services may provide a greaterbene®t to less educated mothers and thus serveas substitute inputs to education in determiningchild health, and would also lessen the impactof educational di�erences (Rosenzweig &Schultz, 1982).
To see if the bene®t of local health services isdi�erent for women with di�erent levels ofeducation, the travel time variables are inter-acted with education and included in thereduced form regression for mortality in thelast two columns of Table 2. The results indi-cate no signi®cant interaction among ruralwomen, but a signi®cant interaction betweeneducation and public hospitals for urban
Table 2. OLS estimates for number of child deathsa
Variable (1) (2) (3) (4)Rural Urban Rural Urban
Log PC expenditure ÿ0.055� ÿ0.026 ÿ0.055� ÿ0.026(1.89) (0.73) (1.87) (0.73)
Age 0.009 0.016 0.009 0.011(0.60) (0.85) (0.60) (0.61)
Age squared 0.000 0.000 0.00 0.00(0.18) (0.19) (0.18) (0.05)
Highest grade 0.071�� 0.075 0.070�� ÿ0.025(2.33) (1.56) (2.10) (0.49)
Grade squared ÿ0.005�� 0.002 ÿ0.005�� 0.000(2.55) (0.89) (2.47) (0.13)
Married 0.028 ÿ0.005 0.028 ÿ0.004(0.75) (0.11) (0.75) (0.10)
Hours to hospital 0.010 0.014 ÿ0.009 0.517��
(0.49) (0.28) (0.10) (2.06)Hours to health centre ÿ0.032 0.121 ÿ0.005 0.527�
(0.97) (1.30) (0.27) (1.72)Hospital� grade 0.002 ÿ0.050��
(0.21) (2.04)Health center� grade ÿ0.005 ÿ0.045
(0.27) (1.45)Adjusted R-squared 5.91 5.14 4.80 7.45F-Test 6.60�� 6.03�� 5.28�� 5.90��
Mean of Dep. variable 0.14 0.13 0.14 0.13
a Constant term not reported. Absolute t-statistics in parenthesis below coe�cient estimates.* Signi®cant at the 10% level.** Signi®cant at the 5% level.
FERTILITY IN JAMAICA 177

women. The negative in¯uence of education oninfant mortality is enhanced the farther awoman lives to an urban public hospital. Hencein urban Jamaica, public hospitals andwomen's education are substitutes.
The SLC questionnaire does not explicitlyspecify an age limit for child deaths, hence thereis the possibility that the death of older childrenmay be included in the mortality data. Tocontrol for the possible exposure time to deathimplied by this problem, I also estimated themodels in Table 2 using the mortality rate (orpropensity to child death) as the dependentvariable. These models were poorly de®ned,however, with no statistically signi®cant coef-®cient estimates, and in the rural sample themodel as a whole was also insigni®cant.
(b) Number of births
Table 3 presents the estimation results for thestock of children by region. The regressionsexplain approximately 50% of the variation in
births, and almost all the coe�cients arestatistically signi®cant.
The individual infant mortality rate has astrong statistical and nonlinear impact on thetotal number of births in the hypothesizedmanner. The mortality rate coe�cients, whenevaluated at the mean, imply that a doubling ofthe individual mortality rate will increase thenumber of births by 0.45 for rural women and0.28 for urban women. 10 The mortality ratehas a depressing e�ect on births after approxi-mately 0.46 for both subsamples 11 and theimplied replacement response is very high.
Table 4 summarizes the replacement responseestimated using the various techniques found inthe literature. In the ®rst row, the ordinary leastsquares (OLS) coe�cient of deaths on births iscorrected using recommendation (D) fromTrussell and Olsen (1983, p. 38). 12 In thesecond row the number of deaths is instru-mented with the mortality rate as discussed inOlsen (1980), and in row 3 the mortality rate isentered linearly and the replacement response
Table 3. Estimates for total births and recent fertilitya
Variable Number of births (OLS) Recent fertility (Probit)
Rural Urban Rural Urban
Log PC expenditure ÿ1.270�� ÿ0.884�� ÿ0.559�� ÿ0.434��
(12.43) (8.86) (5.14) (3.57)Age 0.201�� 0.392�� 0.217�� 0.209��
(3.94) (7.71) (3.26) (2.86)Age squared ÿ0.001 ÿ0.005�� ÿ0.005�� ÿ0.004��
(1.01) (5.24) (4.00) (3.00)Highest grade 0.257�� 0.335�� 0.031 0.027
(2.41) (2.49) (0.27) (0.16)Grade squared ÿ0.020�� ÿ0.026�� ÿ0.002 ÿ0.002
(2.98) (3.40) (0.32) (0.10)Married 0.818�� 0.415�� 0.771�� 0.656��
(6.32) (3.50) (5.63) (4.68)Mortality rate 13.171�� 8.560�� 4.921�� 1.360
(11.95) (7.99) (2.52) (0.82)Mortality rate squared ÿ14.078�� ÿ9.437�� ÿ10.238�� ÿ2.847
(10.68) (6.53) (2.06) (0.95)Hours to hospital ÿ0.054 ÿ0.019 ÿ0.035 ÿ0.191
(0.75) (0.13) (0.53) (0.99)Hours to health centre 0.018 ÿ0.093 0.112 ÿ0.218
(0.16) (0.36) (1.05) (0.05)Previous period births ÿ0.254 ÿ0.417��
(3.68) (4.87)Previous period births squared 0.029 0.044��
(4.65) (5.20)Adjusted R-squared 57.37 48.91F-Test 115.11�� 72.13��
Log likelihood 332.65 249.15Chi-squared 136.78�� 68.37��
a Constant term not reported. Absolute t-statistics in parenthesis below coe�cient estimates.** Signi®cant at the 5% level.
WORLD DEVELOPMENT178

derived according to the formula in Olsen(1980, p. 433). Both rural and urban replace-ment is very high, with the estimates reaching 1for the model where the mortality rate isentered linearly. These replacement rates aremuch higher than the 0.20 range reported byBenefo and Schultz (1994) for Ghana and Coted'Ivoire LSMS data sets, and are among thehighest reported for developing countries.
The other results are plausible and intuitive.The number of births decreases with householdincome (quadratics in income are not signi®-cant), and increases linearly with age for ruralwomen but decreases after age 39 for urbanwomen. The e�ect of education is highlysigni®cant and nonlinear: at low levels of edu-cation there is a positive relationship between
schooling and births, which peaks at grade 6(end of primary school in Jamaica), the mini-mum level of education required to achieve andmaintain functional literacy. Education has alarger impact in reducing fertility than income.Evaluated at the means, the elasticity of birthswith respect to income is ÿ0.15 for ruralwomen (ÿ0.10 for urban) compared to anelasticity with respect to education of ÿ0.45(ÿ0.86 for urban). 13
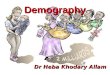
The interaction between mortality, educationand total fertility can be seen clearly in Figures1 and 2 which traces the relationship betweennumber of deaths and births for a marriedwoman of age 27 with various levels ofschooling, based on the coe�cient estimates inthe ®rst two columns of Table 3. 14 The ®gure
Figure 1. Estimated relationship between births and mortality rate by education (rural) (OLS).
Table 4. Estimates of replacement response
Estimation method Coe�cient estimate Implied replacement
Rural Urban Rural Urban
OLSa 1.708 1.189 0.70 0.66(14.57) (12.12)
IVb 0.943 0.691 0.94 0.69(5.52) (5.20)
Linear mortality ratec 2.245 2.124 0.99 1.10(5.14) (4.91)
a Births regressed on number of deaths via OLS, and coe�cient corrected using method described in text.b Number of deaths instrumented using the mortality rate as instrument.c Births regressed on the mortality rate in linear form using OLS and the replacement response recovered usingmethod described in text.
FERTILITY IN JAMAICA 179

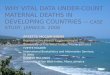
shows the nonlinear relationship between birthsand the individual mortality rate which peaksat approximately 0.46 in both regions. Thereare three salient features about the graphs.First, the urban graph is lower and ¯atter thanthe rural one indicating that urban women havefewer children, and the impact of mortality onbirths is larger among rural women. Second,the relationship between the mortality rate andbirths is virtually the same among women withprimary education (grade 6) and the mean levelof education (grade 9); the e�ect of educationon the mortality±births relationship is not feltuntil grade 12 education is attained. Third, theimpact of grade 12 versus grade 9 education isgreater in urban areas. The latter is consistentwith both a ``value of time'' hypothesis and a``tastes and preferences'' hypothesis of the roleof education in determining fertility behavior.Secondary school graduates have more income-earning opportunities in urban areas ofJamaica, and are also more likely to be exposedto alternative life-styles and social groupswhich would a�ect preferences. In either casethe results indicate that the expansion ofsecondary schooling beyond grade 9 for womencan have an important impact on fertility.
The OLS estimates presented in Table 3include a quadratic in age but this may not fullycontrol for the fact that the number of births isa truncated variable since younger women willhave had less time to have children. To assessthe robustness of the results in Table 3, I esti-
mated the model specifying the number ofbirths as a Poisson variable and using thewoman's age to explicitly measure exposuretime. Full results of this procedure are availablefrom the author, but simulations based on thesePoisson estimates using the same assumptionsas before are presented in Figures 3 and 4. Theresults are virtually identical to those of Figures3 and 4 based on the OLS speci®cation: therelationship between births and the mortalityrate is stronger in rural areas, and the biggestdi�erence in fertility is between 9th and 12thgrade.
(c) Recent or current fertility
Columns 3 and 4 in Table 3 present theprobit results for probability of a recent preg-nancy by region, and there are some interestingdi�erences between these estimates and thosefor the stock of children. The most importantdi�erence is the lack of signi®cance of theeducation variables in determining currentfertility behavior. It could be that the e�ect ofeducation is primarily transmitted through thestock variable, but when these variables aredropped the education terms are still notsigni®cant, nor are they signi®cant when themortality variables are excluded. 15
The stock variable itself is somewhat anom-alous, indicating the probability of a recentpregnancy ®rst declines with the number ofsurviving children until 4.6 for rural women
Figure 2. Estimated relationship between births and mortality rate by education (urban) (OLS).
WORLD DEVELOPMENT180

(4.4 for urban) and then increases. Hence in thissample the women most likely to have just hada child are those with either very small or largefamilies. The impact of age in the probitequations is also signi®cantly nonlinear, butpeaks at a much earlier age (21 for rural and 27for urban women) than in the stock regressions.
Another interesting di�erence between thestock and ¯ow results is the estimated impact ofthe mortality rate. For urban women mortality
is insigni®cant, but for rural women it continuesto be signi®cant and nonlinear, peaking at 0.24.The impact of the death rate on the probabilityof a recent pregnancy is shown in Fig. 5 for amarried woman, 27 years of age and grade 9education (other variables evaluated at theirmeans) using the probit coe�cients in Table 3.The graph indicates that for rural women, theprobability of a recent or current pregnancydrops to zero at very high rates of mortality.
Figure 3. Estimated relationship between births and mortality rate by education (rural) (POISSON).
Figure 4. Estimated relationship between births and mortality rate by education (urban) (POISSON).
FERTILITY IN JAMAICA 181

The relationship for urban women is also plottedbut the coe�cient estimates in this subsampleare not signi®cantly di�erent from zero.
(d) Desired fertility
Columns 1 and 2 in Table 5 include the desiredummy variable in the recent fertility probitmodel and it is positive and highly signi®cantfor both urban and rural women. Inclusion ofthis variable reduces the estimated impact ofprevious births and mortality (and theirsquares) on the probability of a recent preg-nancy, and the linear births term becomesinsigni®cant for rural women.
The quantitative impact of desiring anotherchild on the probability of becoming pregnantis shown in Figures 6 and 7 for a marriedwoman, aged 27 with grade 9 education (othervariables evaluated at their means). 16 Theimpact is much greater for rural women,peaking at around age 23 when the estimatedincrease in the probability of becoming preg-nant is 30%, and remaining positive until age44. For urban women the probability of arecent pregnancy is generally lower than forrural women, and so is the estimated impact ofdesiring another child, although this (smaller)impact persists for a longer period. The e�ect ofdesiring a child is low at young ages, peaks atage 27 when the increase in the probability ofbecoming pregnant is 10%, and ®nally dimin-ishes at age 46.
The urban±rural di�erence in the estimatedimpact of desiring another child shown in Figs.6 and 7 suggest that urban women tend to delaychild bearing to later in the life-cycle, and thosewho desire a child are less likely to immediatelyhave one than rural women, possibly becauseof the higher cost of raising a child in urbanareas. 17 It is interesting to note that in thisdata set the mean of the ``desire'' variable isactually slightly higher for urban women. Thisis because the mean desired number of children(not shown) is higher among urban than ruralwomen (2.8 vs. 2.76) even though urban womenhave lower fertility. This suggests that urbanwomen continue to have a preference for chil-dren but must modify their fertility behaviordue to economic or other constraints. Hencethe negative impact of education observed inthe births regressions must primarily representa ``value-of-time'' e�ect for urban women.When desired number of children is regressedon income and schooling, each are negative butonly marginally signi®cant for urban women (pvalues of approximately 0.12). But income ishighly signi®cant and negative for rural women(with a coe�cient 33% higher than the coe�-cient for urban women) but education is insig-ni®cant. These results also imply that educationdoes not a�ect fertility through changing tastesfor children.
The last two columns of Table 5 present theresults when desire is predicted using a probitregression with religion (14 dummies), age of
Figure 5. Estimated relationship between recent pregnancy and mortality rate by region.
WORLD DEVELOPMENT182

Table 5. Probit estimates of the impact of desiring a child on recent fertilitya
Variable Rural Urban Instrumental Variableb
Rural Urban
Log PC expenditure ÿ0.557 ÿ0.443 ÿ0.401 ÿ0.306(5.02) (3.55) (2.73) (1.69)
Age 0.214 0.214 0.089 ÿ0.017(3.15) (2.84) (1.06) (0.14)
Age squared ÿ0.005 ÿ0.004 ÿ0.003 ÿ0.001(3.87) (2.99) (2.30) (0.30)
Highest grade 0.008 ÿ0.003 ÿ0.101 ÿ0.105(0.06) (0.02) (0.77) (0.57)
Grade squared ÿ0.001 0.001 0.005 0.008(0.13) (0.08) (0.63) (0.75)
Married 0.781 0.676 0.681 0.621(5.57) (4.57) (4.57) (3.86)
Mortality rate 3.736 1.074 3.793 0.611(1.92) (0.66) (1.92) (0.24)
Mortality rate squared ÿ8.165 ÿ2.394 ÿ8.485 ÿ3.166(1.69) (0.84) (1.74) (0.55)
Hours to hospital ÿ0.034 ÿ0.195 ÿ0.034 ÿ0.331(0.49) (0.99) (0.46) (1.50)
Hours to health centre 0.097 ÿ0.228 0.121 ÿ0.099(0.89) (0.69) (1.05) (0.27)
Previous period births ÿ0.064 ÿ0.288 ÿ0.118 ÿ0.326(0.81) (2.97) (1.41) (3.22)
Previous period births squared 0.019 0.037 0.021 0.040(2.93) (4.16) (3.20) (4.36)
Desire 0.788 0.560 ÿ0.153 ÿ0.554(4.59) (2.85) (0.19) (0.56)
Desire (residual)c 0.863 1.130(1.11) (1.14)
Log likelihood ÿ319.67 ÿ242.31 ÿ294.12 ÿ215.35Chi-squared 155.81�� 77.16�� 140.11�� 75.18��
a Constant term not reported. Absolute t-statistics in parenthesis.b Desire treated as endogenous and instrumented with religion, age of menstruation, and age of ®rst cohabitation.c Residual from stage one regression predicting desire.** Signi®cant at the 5% level.
Figure 6. One-year probability of child birth for women who desire and do not desire a childÐrural region.
FERTILITY IN JAMAICA 183

menstruation, and age of ®rst cohabitation asidentifying instruments. Following the recom-mendation of Rivers and Vuong (1988) for thetreatment of an endogenous variable in a probitmodel, the residual from the stage one regres-sion predicting desire, as well as the originaldesire variable, are both included in the probitregression. The t-test on the coe�cient of theresidual term is actually a test for endogeneityof the desire variable (the null hypothesis isexogeneity).
In both rural and urban areas the coe�cientof desire is reduced and no longer signi®cant,while the t-tests for the coe�cient of theresidual terms, though greater than 1, are alsoinsigni®cant. As mentioned earlier there areseveral potential sources of contaminationassociated with desire: the results here indicatethat endogeneity is the dominant source ofmisspeci®cation since the estimated coe�cientsbecome smaller, but this should not beemphasized because of the poor performance ofthe identifying instruments in the stage oneregression.
5. CONCLUSIONS
The e�ect of mortality on fertility in Jamaicais highly signi®cant and nonlinear, peaking at amortality rate of 0.46 with a replacementresponse close to 1. This high replacement
response exists, however, in a low-fertilityenvironment where the mean number of deathsis only 0.13, and is thus unlikely to have asigni®cant e�ect on the size of the population.Indeed the World Bank (1994) has predictedthat Jamaica will reach replacement levels offertility by the year 2000.
Both income and education have signi®cantnegative e�ects on the number of births, withthe impact of education being larger than thatof income: the point elasticities in rural areasare ÿ0.45 and ÿ0.15 for education andincome, respectively. The in¯uence of educa-tion becomes negative only after grade 6, andthe simulations show that expanding educa-tion beyond grade 9 can have a particularlylarge e�ect on fertility, especially for urbanwomen. In addition, the transmission of theeducation e�ect appears to occur throughraising the value of time for the womanrather than changing tastes or desire forchildren.
There are substantial di�erences in the esti-mated impact of education and infant mortalitywhen recent fertility is used as the outcomemeasure. Education is no longer signi®cant andmortality becomes insigni®cant among urbanwomen. One possible explanation for this isthat the impact of education is long term innature and thus more likely to in¯uence lifetime fertility rather than fertility in any givenyear.
Figure 7. One-year probability of child birth for women who desire and do not desire a childÐurban region.
WORLD DEVELOPMENT184

NOTES
1. Montgomery, Kouame and Oliver (1995) and others
have argued that marital status is endogenous to fertility
decisions and should not be included in the reduced
form. In Jamaica, however, most ®rst pregnancies occur
outside of stable unions, and in fact, the country has
one of the highest rates of teenage pregnancies in the
world. In the present context therefore, the potential
simultaneity bias associated with this variable seems
minimal.
2. Technical details of the sample design and survey
method can be found in Grosh (1991).
3. Only current pregnancy is reported in the fertility
module. Recent fertility (last 12 months) was
constructed by matching women with the age of their
children from the household roster.
4. Their estimates are based on the assumption that
health care access a�ects infant mortality but not
fertility. In the present data, however, access to health
facilities will in¯uence the cost of acquiring contracep-
tives and birth control informationÐthis information
therefore also belongs in the fertility regressions.
5. It is possible the two sources of reporting error
cancel each other. On the other hand, there is another
source of measurement error due to the fact that women
may interpret the question in di�erent ways (e.g., how
many more children do you desire?).
6. Family background variables such as parental
education or number of siblings might arguably be used
as identifying instruments but these are not available in
the SLC except for women under 18 years of age.
7. For the OLS speci®cations this is an F-Test; for the
probits it is a likelihood ratio test. Results are available
from the author upon request.
8. Jamaica is one of the few developing countries
where women outperform men in virtually all aspects of
education including primary school achievement
(measured by Common Entrance Examination scores),
secondary and tertiary enrolment, and grade attainment
(Handa, 1995).
9. When an independent variable is measured in logs,
its coe�cient represents the change in the dependent
variable given a proportional change in the independent
variable.
The SLC questionnaire does not explicitly specify an
age limit for child deaths, hence there is the possibility
that the death of older children may be included in the
mortality data. To control for the possible exposure time
to death implied by this problem, I also estimated the
models in Table 2 using the mortality rate (or propensity
to child death) as the dependent variable. These models
were poorly de®ned, with no statistically signi®cant
coe�cient estimates, and in the rural sample the model
as a whole was also insigni®cant.
10. This is calculated by evaluating the derivative of
births with respect to the mortality rate at the mean
mortality rate for each region, and then multiplying by
the respective mean for each region.
11. 2.3% of rural women and 3.1% of urban women
had mortality rates greater than 0.46.
12. In the Jamaican case, the within parity variance
in mortality is small, but the variance of deaths is
much smaller than predicted by equation (3) in Trussell
and Olsen (1983). This implies that the mortality rate is
not random, and the OLS correction shown in Table 4
is likely to underestimate the true replacement
response.
13. In the current sample 10% of women are still
studying. Since these tend to be younger women who
would have had less time to have children, the impact of
education reported here is probably slightly underesti-
mated.
14. The regression is estimated at the means of the
other variables (income and travel time to health
facilities).
15. Models were also estimated for older and younger
age groups to see if the education variables were
important for younger cohorts of women but they were
not.
16. Note that the variable ``age squared'' will also vary
according to the value of age. This is what generates the
particular nonlinear pattern in these graphs, since in
principle probit predictions must always generate
nonlinear e�ects given that the functional form itself is
nonlinear.
17. Urban jobs are often more in¯exible and thus less
compatible with child care.
FERTILITY IN JAMAICA 185

REFERENCES
Becker, G. (1965). A theory of the allocation of time.Economic Journal, 75, 493±517.
Becker, G. (1981). A treatise on the family. Cambridge,MA: Harvard University Press.
Benefo, K. B., & Schultz, T. P. (1994). Determinants offertility and child mortality in Cote d'Ivoire andGhana. Living Standards Measurement Study No.103, The World Bank, Washington, DC.
Birdsall, N. (1988). Economic approaches to populationpolicy. In H. Chenery, & T. N. Srinivasan (Eds.),Handbook of development economics, vol 1. Amster-dam: North-Holland.
Chen, J., Bendarf, I., & Hicks, W. (1987). The ``synthesisframework'' and determinants of fertility in Syria.Economic Development & Cultural Change, 36, 145±159.
Grosh, M. (1991). The household survey as a tool forpolicy change: Lessons from the Jamaica Survey ofLiving Conditions. Living Standards MeasurementStudy No. 80, The World Bank, Washington, DC.
Handa, S. (1995). Employment, income and laboursupply: An analysis using the 1993 SLC time-usemodule. The Planning Institute of Jamaica, Kings-ton, Jamaica.
Handa, S. (1996). Expenditure behavior and children'swelfare: An analysis of female headed households inJamaica. Journal of Development Economics, 50 (1),165±187.
Hyatt, D., & Milne, W. J. (1993). Determinants offertility in urban and rural Kenya: Estimates and asimulation of the impact of education policy. Envi-ronment and Planning A, 25, 371±382.
Maglad, N. E. (1990). Fertility in rural Sudan: The e�ectof landholding and child mortality. Economic Devel-opment & Cultural Change, 42 (4), 761±772.
Montgomery, M., Kouame, A., & Oliver, R. (1995). Thetrade-o� between the number of children and theirschooling: Evidence from Cote d'Ivoire and Ghana.Working Paper No. 82, Research Division, ThePopulation Council, New York.
National Family Planning Board. (1993). ContraceptivePrevalence Survey, Kingston, Jamaica.
Olsen, R. J. (1980). Estimating the e�ect of childmortality on the number of births. Demography, 17(4), 429±443.
Peters, T. J. (1994). Paediatric and perinatal epidemiol-ogy (special issue). Perinatal Morbidity in Jamaica, 8(1).
Rivers, D., & Vuong, Q. (1988). Limited informationestimators and exogeneity tests for simultaneousprobit models. Journal of Econometrics, 39, 347±366.
Rosenzweig, M., & Schultz, T. P. (1982). Child mortalityand fertility in Colombia: Individual and communitye�ects. Health Policy and Education, 2, 305±348.
Rosenzweig, M., & Schultz, T. P. (1983). Consumerdemand and household production: The relationshipbetween fertility and child mortality. AmericanEconomic Review, 13 (2), 38±42.
Rosenzweig, M., & Wolpin, K. (1993). Maternal expec-tations and ex post rationalizations: The usefulnessof survey information on the wantedness of children.Journal of Human Resources, 28 (2), 205±229.
Schultz, T. P. (1973). A preliminary survey of economicanalyses of fertility. American Economic Review, 63(2), 71±78.
Strauss, J. (1990). Households, communities, and pre-school children's nutrition outcomes: Evidence fromrural Cote d'Ivoire. Economic Development & Cul-tural Change, 38, 231±261.
Thomas, D., Strauss, J., & Henrique, M.-H. (1990).Child survival, height for age, and household char-acteristics in Brazil. Journal of Development Econom-ics, 33, 197±234.
Trussell, A., & Olsen, R. J. (1983). Evaluation of theOlsen technique for estimating the fertility responseto child mortality. Demography, 20 (3), 391±405.
World Bank. (1994). Jamaica: A strategy for growth andpoverty reduction. Country Economic Memoran-dum, The World Bank, Washington DC.
World Bank. (various years) World DevelopmentReport. New York: Oxford University Press.
UNDP. (1994). Human Development Report 1994. NewYork: the United Nation.
WORLD DEVELOPMENT186