Embed Size (px)
Citation preview

The impact of an informational website on behavioural
intentions and attitudes about patient engagement in
research: A mixed methods evaluation
by
Donna Plett
A thesis submitted in conformity with the requirements for the degree of Master of Science
Institute of Health Policy, Management and Evaluation University of Toronto
© Copyright by Donna Plett, 2020
ii
The impact of an informational website on behavioural intentions
and attitudes about patient engagement in research: A mixed
methods evaluation
Donna Plett
Master of Science
Institute of Health Policy, Management and Evaluation
University of Toronto
2020
Abstract
Patient engagement in research (PER) is a rapidly emerging practice and resources are needed to
prepare patients and researchers for collaboration. This study asked: What are the perceptions of
patients and researchers about an informational website about PER, and how did it impact
intentions and attitudes toward PER?
A mixed methods approach was used, entailing pre-post surveys, focus groups, and web
analytics. 49 patients and researchers participated. The findings revealed 1) intentions and
attitudes toward PER decreased after viewing the website, however participants reported that the
website did not impact, or positively impacted, their attitudes and intentions, and 2) overall
satisfaction with the website, with variation in preferences for design, and a desire for more PER
guidance, easily accessible information, and detail regarding diversity in engagement and
compensation for participants. These findings reveal considerations for the development of
online resources about PER and understanding divergent findings within mixed methods
research.
iii
Acknowledgments
First, I’d like to thank my thesis supervisor, Susan Law, and committee members Kerry Kuluski
and Judith Versloot for the many hours you’ve dedicated to helping me with this project. Your
feedback and advice have benefitted me in so many ways and will help to inform my decision-
making far beyond this thesis. Thank you also to Julia Ma, who offered fantastic tips and tricks
for analyzing and presenting the quantitative data.
Thank you to all my IHPME professors who not only taught me about research topics and
methods, but also took the time to help me clarify my research interests and aptitudes and
exemplified some of what I hope to accomplish in my career one day.
I’d also like to thank my friends and IHPME classmates who I had the pleasure of working
alongside while completing coursework and group assignments. Your humour and comradery
made the challenging times much more bearable, and your unique skills and interests inspired me
and opened my mind to new areas of inquiry.
Finally, I’d like to thank the two individuals who were nearest and dearest to me throughout this
process. To my cat, Tiki, thank you for curling up next to my keyboard as I write and cheering
me up with your eternal cuteness. And to my partner, Chirag, thank you for keeping me company
throughout COVID-19 social distancing, for listening to me ramble endlessly as I process my
ideas, for challenging and helping me to clarify those ideas, and of course for being a wizard in
all things tech.
iv
Table of Contents
Project Overview .....................................................................................................1
1.1 The Problem .........................................................................................................................1
1.2 Purpose of the Study ............................................................................................................2
1.3 Theoretical Framework ........................................................................................................3
1.4 Importance of the Study .......................................................................................................4
1.5 Scope & Limitations ............................................................................................................4
Literature Review.....................................................................................................6
2.1 What is Patient Engagement in Research?...........................................................................6
2.2 Why Patient Engagement in Research is Important ............................................................7
2.2.1 Defining ‘Patient’.....................................................................................................7
2.2.2 PER in Practice ........................................................................................................8
2.2.3 International Context ...............................................................................................9
2.3 Benefits & Challenges of PER ...........................................................................................10
2.3.1 Benefits for Research Projects ...............................................................................10
2.3.2 Personal Benefits to Research Partners ..................................................................11
2.3.3 Benefits for Communities ......................................................................................11
2.3.4 Logistical Constraints ............................................................................................12
2.3.5 Lack of Receptive Attitudes ...................................................................................13
2.3.6 Representativeness & Recruiting for Diversity .....................................................14
2.3.7 Building Relationships & Avoiding Tokenism......................................................15
2.3.8 Measuring Impact ..................................................................................................17
2.4 Building Capacity for PER: The Resource Landscape ......................................................18
v
2.4.1 The Need for Resources .........................................................................................18
2.4.2 Existing PER Learning Resources .........................................................................18
2.5 Evidence for the Benefits of Using Video Narratives .......................................................20
2.5.1 The Persuasive Power of Narratives ......................................................................20
2.5.2 The DIPEx Model ..................................................................................................21
2.6 Summary and Rationale for Further Evaluation ................................................................23
Methods..................................................................................................................24
3.1 Introduction to Methods .....................................................................................................24
3.1.1 Description of Website ..........................................................................................24
3.1.2 Institutional Context...............................................................................................25
3.1.3 Paradigmatic Perspective .......................................................................................25
3.1.4 Methodological Approach .....................................................................................26
3.2 Study Design ......................................................................................................................28
3.2.1 Overview of Methods ............................................................................................28
3.2.2 Survey Tool Development .....................................................................................31
3.2.3 Web Analytics Strategy .........................................................................................34
3.2.4 Ethical Considerations ...........................................................................................35
3.3 Sampling & Recruitment ...................................................................................................37
3.3.1 Recruitment Process...............................................................................................37
3.4 Data Collection ..................................................................................................................38
3.4.1 Consent Process .....................................................................................................38
3.4.2 Surveys ...................................................................................................................39
3.4.3 Focus Groups .........................................................................................................39
3.4.4 Web Analytics ........................................................................................................40
vi
3.5 Data Analysis .....................................................................................................................40
3.5.1 Survey Data ............................................................................................................40
3.5.2 Qualitative Data .....................................................................................................42
3.5.3 Web Analytics ........................................................................................................43
3.5.4 Integration & Interpretation ...................................................................................43
3.6 Dissemination Plan ............................................................................................................44
Results ....................................................................................................................45
4.1 Overview ............................................................................................................................45
4.2 Study Sample .....................................................................................................................45
4.3 Survey 1 Findings: Baseline Characteristics ......................................................................46
4.3.1 Participant Characteristics .....................................................................................46
4.3.2 Adapted eHIQ Part 1 ..............................................................................................46
4.3.3 Theory of Planned Behaviour at Baseline .............................................................48
4.4 Survey 2 Findings: Impact of Website...............................................................................51
4.4.1 Self-Reported Time on Website.............................................................................51
4.4.2 Adapted eHIQ Part 2 ..............................................................................................51
4.4.3 Theory of Planned Behaviour Post-Intervention ...................................................54
4.5 Website Utilization ............................................................................................................57
4.6 Focus Group Findings ........................................................................................................59
4.6.1 Theme 1: Desire for Practical, Action-Oriented Content ......................................59
4.6.2 Theme 2: Desire for Clarity of Purpose and Definitions .......................................61
4.6.3 Theme 3: Variance in Preferences for Design Aspects .........................................61
4.6.4 Theme 4: Importance Ascribed to Diversity and Compensation in PER ..............63
4.7 Integration of Findings .......................................................................................................64
vii
4.8 Summary of Findings .........................................................................................................68
Discussion ..............................................................................................................69
5.1 Overview ............................................................................................................................69
5.2 Comparison with Related Literature ..................................................................................70
5.3 Interpretation of Divergent and Unanticipated Findings ...................................................71
5.4 Contribution to Academic Knowledge ..............................................................................73
5.5 Implications for Policy & Practise .....................................................................................74
5.6 Opportunities for Future Research .....................................................................................75
5.7 Limitations .........................................................................................................................76
5.8 Conclusion .........................................................................................................................77
References ......................................................................................................................................78
Appendices .....................................................................................................................................86
viii
List of Tables
Table 1: Adapted eHIQ Part 1 results, by domain. ....................................................................... 47
Table 2: Baseline TPB findings by domain – between group comparisons. ................................ 49
Table 3: Barriers and facilitators to engaging in partnerships, selected quotes. ........................... 50
Table 4: Adapted eHIQ Part 2 results, by domain, patients and researchers. ............................... 52
Table 5: Feedback about website in open-ended survey responses, selected quotes by topic, and
number of patients (P) and researchers/research staff (R) who referred to topic in response.* ... 53
Table 6: Pre-post TPB findings by domain, patients and researchers. ......................................... 55
Table 7: Survey feedback about the impact of the website, selected quotes. ............................... 56
Table 8: Summary statistics for evaluation period. ...................................................................... 58
Table 9: Complementary findings. ............................................................................................... 66
Table 10: Divergent findings. ....................................................................................................... 67
Table 11: Original and adapted eHIQ. .......................................................................................... 87
Table 12: Adapted Theory of Planned Behaviour survey questions, by domain. ......................... 89
Table 13: Organizations contacted during recruitment process .................................................... 91
Table 14: Demographics. ............................................................................................................ 112
Table 15: Page views and unique pages views by person featured on website. ......................... 114
Table 16: Number of views by topic page and average length of time spent on page. .............. 115
Table 17: Average self-reported time on site, low and high estimates. ...................................... 116
ix
Table 18: Adapted eHIQ Part 1 data, aggregate, patients, and researchers, attitudes toward online
info about PRPs........................................................................................................................... 117
Table 19: Adapted eHIQ Part 1, aggregate, patients, and researchers, attitudes toward sharing
PRP experiences online............................................................................................................... 118
Table 20: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, confidence and
identification, part 1. ................................................................................................................... 119
Table 21: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, confidence and
identification, part 2. ................................................................................................................... 120
Table 22: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, information and
presentation, part 1. ..................................................................................................................... 121
Table 23: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, information and
presentation, part 2. ..................................................................................................................... 122
Table 24: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, understanding and
motivation, part 1. ....................................................................................................................... 123
Table 25: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, understanding and
motivation, part 2. ....................................................................................................................... 124
Table 26: Pre-post TPB data, patients and researchers, intentions. ............................................ 125
Table 27: Pre-post TPB data, patients and researchers, attitudes. .............................................. 126
Table 28: Pre-post TPB data, patients and researchers, subjective norms. ................................. 127
Table 29: Pre-post TPB data, patients and researchers, perceived behavioural control. ............ 128

x
List of Figures
Figure 1: Study design. ................................................................................................................. 28
Figure 2: Diagram of methods ...................................................................................................... 31
Figure 3: Theory of Planned Behaviour........................................................................................ 32
Figure 4: Recruitment flowchart. .................................................................................................. 45
Figure 5: Self-reported time on site. ............................................................................................. 51
Figure 6: Daily website page views. ............................................................................................. 57
Figure 7: Image of front page of website. ..................................................................................... 86
xi
List of Appendices
Appendix A Website Layout ........................................................................................86
Appendix B Survey Tool Development .......................................................................87
Appendix C Sample Recruitment Email ......................................................................90
Appendix D Organizations Contacted During Recruitment ........................................91
Appendix E Focus Group Consent Form .....................................................................92
Appendix F Interview Guide for Focus Groups ..........................................................95
Appendix G Pre and Post Surveys ...............................................................................97
Appendix H Demographic Data .................................................................................112
Appendix I Web Analytics Data ...............................................................................114
Appendix J Adapted eHealth Impact Questionnaire Data ........................................117
Appendix K Theory of Planned Behaviour Data .......................................................125
Abbreviations
PER patient engagement in research
PRP patient-researcher partnership
SLT Social Learning Theory
eHIQ eHealth Impact Questionnaire
TPB Theory of Planned Behaviour
PBC perceived behavioural control
Page 1 of 128
Project Overview
1.1 The Problem
The science on the benefits of patient engagement in research (PER) is still young, but there are
many compelling arguments for its widespread adoption: 1) engaging patients in research can
result in improved quality of care because research priorities are better aligned with patient
needs;1 2) PER creates an opportunity to engage marginalized populations, which could lead to
greater generalizability of research findings and more equitable healthcare delivery;1 3)
involving patients empowers them to take a more active role in their healthcare;2 4) research
findings reach a larger population when patients act as ambassadors in their communities;1 5)
PER improves accountability and responsiveness to citizens and contributes to democratic ideals
of transparency and accountability by providing assurance that resources are being used to
further public interests;1,3 and 6) some argue there is a moral imperative to include patients in
research because patients have a fundamental right to involvement in research that will have a
direct impact on them.1,4
It is now commonplace for funding agencies (e.g., Canadian Institutes of Health Research) to
require health researchers to include a plan to engage patients in their study protocol to be
eligible for funding.5,6 However, researchers often do not know how to meaningfully include
patients in their research7 and patients have reported feeling unclear about what their role is in a
partnership with researchers.8 Studies show that poor preparation and including patients just to
‘tick a box’ on a grant application has led to tokenistic patient involvement and ineffective
partnerships4 which are damaging to those involved and reinforces negative attitudes toward
patient engagement in research.9,10
In order to combat these challenges, well-designed resources are needed to demystify research
partnerships by providing information to patients and researchers about how to successfully work
together throughout every stage of the research lifecycle.7 While some educational resources are
already available to provide information about PER, there is ample opportunity for the
development of new resources that tackle the challenges of PER.
Page 2 of 128
1.2 Purpose of the Study
This study evaluates an innovative website, which is designed to build capacity for patient
engagement in research by providing experiential information about research partnerships. The
website features clips and transcripts from video-recorded interviews with patients, caregivers
and researchers describing their experiences of being involved in research partnerships.
To evaluate this website, we invited patients, caregivers and researchers to spend time on the
website and provide feedback in the form of surveys and focus groups. We utilized a convergent
mixed methods approach, in which quantitative data (from surveys and web utilization data) and
qualitative data (from focus groups) were collected and analyzed separately and then combined
during the interpretation of the results.11 A mixed methods approach was appropriate because
very little literature exists about the evaluation of resources for patient engagement in research,
and no literature exists to evaluate a resource that uses video narratives to provide information
about partnerships. Our mixed methods approach facilitated an analysis that was strong in both
breadth and depth – breadth through the inclusion of many survey participants and depth through
the discussions held in focus groups with a segment of the survey participants.
The research question that guided this study was: What are the perceptions of patients and
researchers about a website featuring experiential information about patient engagement in
research, and how did it impact behavioural intentions and attitudes toward PER? The primary
aims of the study were to:
1. Measure attitudes, subjective norms, perceived behavioural control, and intentions related
to PER before and after participants spent time on the website,
2. Analyze how participants navigated the website and which content they engaged with the
most,
3. Learn about the reactions of participants to the website’s design and content and their
perceptions about its usefulness as an informational resource about PER, and
4. Compare and contrast the results that emerged from the different methodologies.
Page 3 of 128
1.3 Theoretical Framework
This evaluation is underpinned by two theoretical frameworks: Social Learning Theory (SLT)
and the Theory of Planned Behaviour (TPB). These theories underlie the design of the website,
the approach to its evaluation and hypotheses about its effectiveness.
Social Learning Theory was developed to account for the role that observing the experiences of
others has in learning. Bandura, the theory’s first proponent, posited that most experiential
learning occurs vicariously through others’ experiences and that the ability to understand others’
experiences symbolically makes it possible to foresee probable consequences of actions without
having to first take the action.12 Other core tenets of SLT include that learning takes place in
social contexts and involves observing others’ behaviours and the consequences of those
behaviours.13
Based on SLT, some common methods of knowledge dissemination may not always be
maximally effective. For example, one common method of knowledge dissemination is to
present de-contextualized facts, statistics and recommendations (e.g., pamphlets, flyers, websites,
etc.). However, when information is presented this way, the learner does not have access to the
individual experiences that inform the aggregated information presented to them. According to
SLT, this could result in the information being less engaging and less likely to influence
behaviour. SLT underlies the design of the website, which includes excerpts from a maximum
variation sample14 of video-taped interviews of patients and researchers describing their
involvement in research partnerships, including lessons learned and recommendations for others.
This design allows website visitors to engage with multiple and varying individual experiences
in a way that is reflective of how people often gain knowledge in their day-to-day lives through
conversations and stories.
The Theory of Planned Behaviour pertains to the determinants of intention toward behavior.
According to the TPB the three determinants of behavioural intention are attitudes toward the
behavior, perceived social pressure to perform the behaviour and the degree of perceived
behavioral control (i.e., beliefs about factors that could facilitate or hinder the behaviour and
perceived ease or difficulty of the behavior).15 The website was developed to build capacity for
Page 4 of 128
patient engagement in research by providing a realistic account of the experiences of research
partners and by offering information and support for partnership. It was the believed that the
website would provide visitors with better insight and understanding of the benefits and
challenges of research partnerships and thereby better equipped to engage in them. It was also
believed that the website’s information would encourage increased participation in research
partnerships. By providing firsthand accounts of different experiences of research partnerships,
we hypothesized that the website would positively influence attitudes and behavioural intentions
toward patient engagement in research and that website visitors would find the experiential
content informative and relatable.
Both SLT and the TPB were built into the evaluation of this study, especially in the design of the
surveys administered to participants and the focus group discussion guide (see Methods).
1.4 Importance of the Study
The value of this study lies largely in its furtherance of knowledge about informational resources
about patient engagement in research, how people learn via online resources, and the usefulness
of using stories and narratives in teaching. It may prove valuable to others who may have found
that traditional models of knowledge dissemination have not been as effective as desired. It will
also add to rapidly emerging literature about the use of the internet for disseminating information
and its usefulness as a medium for influencing knowledge, attitudes and behaviour. This study
will also serve as an important resource for others who are developing tools for patient
engagement in research or other topics where an information resource that uses video narratives
may be useful. By utilizing a variety of methods, this study also offers important methodological
learnings related to mixed methods designs and the usefulness of the survey tools we employed.
1.5 Scope & Limitations
Our mixed methods design enabled an in-depth comparative analysis of the responses of patients
and researchers across Canada but leaves open many opportunities for future research in this
area. For instance, future research may benefit from the inclusion of a control group that was
exposed to a traditionally designed educational resource about PER, under traditional trial
conditions to focus on effectiveness. Also, a larger sample that is more representative of the

Page 5 of 128
Canadian population would aid the generalizability of results. A longer evaluation time period
would allow for more web analytics data collection. Future research may also address the
difficulty in recruiting researchers and patients/caregivers who do not already have a positive
attitude toward patient engagement in research, as those who are already interested in research
partnerships are more likely to be interested in participating in a study about research
partnerships. Unfortunately, those without reliable high-speed internet access (e.g., rural/remote
communities, homeless, and low-income individuals) could not participate in this study. Future
initiatives could encourage utilization of public internet access via libraries and community
centres to ensure these populations are not excluded. Limitations will be discussed further in the
discussion chapter.
Page 6 of 128
Literature Review
2.1 What is Patient Engagement in Research?
Patient engagement in research (PER) is one context for patient engagement, which includes a
very broad range of activities. Patient engagement has applications for every part of the
healthcare system, from direct care, to organizational design and governance to policy making.16
At a basic level, patient engagement takes the form of consultation, such as informing a patient
about their diagnosis, surveying patients about their care experience or conducting focus groups
to ask for opinions about a health care issue. A more involved form of patient engagement could
include asking patients about their preferences, including patients as advisers, or using patient
recommendations in funding decisions. At the highest level of involvement, patient engagement
takes the form of partnership and shared leadership. This includes making treatment decisions
based on patient preferences, patient co-lead committees, co-designing care services and policies,
and equal representation of patients on government agency committees.16
PER is a unique application of patient engagement in that it is not directly related to
policymaking, organizational decision-making, or clinical practice. PER is uniquely applicable to
the process of health research and can occur at specific points within the research process or
throughout the research life cycle. One way to understand PER is through the lens of knowledge
translation (KT). The role of KT is to address the ‘know-do’ gap in health research which occurs
when important findings are not disseminated effectively to the patients, practitioners, or others
who would benefit from the new knowledge.17 According to the Canadian Institutes of Health
Research (CIHR), KT is “a dynamic and iterative process that includes synthesis, dissemination,
exchange and ethically sound application of knowledge to improve the health of Canadians,
provide more effective health services and products and strengthen the health care system.”17
Most commonly KT takes place at the end of the research process, or ‘end-of-grant’ KT.18 In
end-of-grant KT, patients or other knowledge-users may be invited to participate in
dissemination planning but do not contribute to the research itself. A more expanded form of KT
is emerging, called integrated KT (iKT). Integrated KT is an approach that involves patients
contributing in various ways throughout the research process, such as to inform or create the
research question, select appropriate methodology, collect data, choose outcome measures,
Page 7 of 128
interpret findings and support dissemination.17 Depending on the duration and extent of patients’
involvement in research projects, PER can be end-of-grant KT or iKT.
2.2 Why Patient Engagement in Research is Important
The drive for patient engagement in research (PER) is part of a broader goal of patient
engagement in health and healthcare that has gained prominence throughout the world.16,19
Patient engagement at its core is a challenge to the paternalistic models of the past, in which
experts, academics, and healthcare professionals are the purveyors of knowledge and patients
and the lay public are recipients of that knowledge.20 In recent decades it has become clear that
failing to listen to and understand the experiences and perspectives of patients has contributed to
poor quality care, ineffective communication, inefficiencies, and a lack of trust in healthcare
professionals.20
Patients experience frustrations with the healthcare system when they are not adequately
informed about the realities of medical care and their own situation, including the extent of
medical uncertainty, the state of knowledge about effectiveness of their care, and the ways in
which medical practice can vary. Bringing patients into important healthcare conversations can
improve relationships between patients and the healthcare system. The role of patients and
families beyond recipients in healthcare is building momentum as they become more active,
informed and influential.16 PER has a role in improving patient-oriented care by producing
knowledge that is more relevant and focused on patient-centred priorities.
2.2.1 Defining ‘Patient’
The term ‘patient’ is used liberally in the context of patient engagement and clarification is
needed to understand which individuals are included under the label. This paper will use the
definition given by the Strategy for Patient-Oriented Research (SPOR) Patient Engagement
Framework which defines ‘patient’ as: “An overarching term inclusive of individuals with
personal experience of a health issue and informal caregivers, including family and friends.”21 In
PER, the role of the patient is to bring their experiential knowledge to the table, to communicate
their stories and interests and to assist the researchers in various aspects of the research project
Page 8 of 128
including priority setting, governance, KT and conducting research.21 Patients bring added value
to the project by offering a perspective based on their lived experience of the health condition or
service under study, and are not expected to act as a representative for any group.
2.2.2 PER in Practice
There are opportunities to engage with patients during all stages of the research lifecycle –
preparation, planning, study design, data collection, analysis and dissemination – although
engagement is often limited to preliminary activities.22 In early stages of the research lifecycle
(planning and preparation) advisory councils and focus groups can be used to gain an
understanding of the priorities of the patient population and to incorporate their feedback into the
research plan. There is opportunity also for patients to be involved in data collection in various
ways depending on the study design. This can include engagement in conducting interviews,
perhaps as co-researchers, particularly when the patient partner is a member of the community
being studied and can more easily communicate with community members than researchers. The
data analysis stage also creates opportunity, especially within qualitative research, since patient
partners may pick out themes and concepts that researchers would miss or not think were
relevant. During dissemination, consulting with patient partners can ensure that the resulting
product makes sense to lay readers and is sensitive to the concerns of the target population.
PER is not only applicable to formal academic research projects (e.g., clinical trials, health
services research, health policy research) but also to research priority setting and quality
improvement projects. The James Lind Alliance (JLA), initiated in the UK and now with global
spread, has a unique approach to involving patients in research through its Priority Setting
Partnerships (PSPs).23 The JLA believes that patients, caregivers and clinicians should work
together to agree about priorities and that it is important for clinicians to address uncertainties
about the effects of treatments. PSPs bring together patients, caregivers and clinicians that share
expertise about an illness or health experience (e.g., acne, kidney cancer, learning difficulties,
etc.). Through a series of workshops, the group develops a Top 10 list of priorities or research
questions. Following this, the identified priorities are promoted to key groups such as research
funders, researchers, patients, caregivers and the wider research community.23
Page 9 of 128
Experience-based co-design (EBCD) is an intra-organizational form of patient engagement used
in healthcare organizations to inform quality improvement projects.24 The co-design element of
EBCD draws upon participatory design principles and aims to open the boundaries of healthcare
service design to include new stakeholders and forms of expertise.24
2.2.3 International Context
PER has gained traction in many countries including Canada, the US, the UK, Australia, the
Netherlands, and Sweden.25 The UK is recognized as the forerunner in PER6,26 and engaging
patients became a part of its national research governance framework in 2005.6 The non-profit
INVOLVE was founded in 2003 with a mission to put people at the heart of decision-making.
Their projects include citizens’ assemblies on policy issues, priority setting and involving
members of the public in research.27 The JLA is also based in the UK and its research priority
setting techniques have inspired researchers all over the world.
The US is another PER leader. The Patient-Centered Outcomes Research Institute (PCORI) is a
non-profit organization that has funded hundreds of research studies since 2012.28 PCORI aims
to speed up the implementation and use of research evidence, influence other clinical and
healthcare research to be more patient-centered, and support clinical effectiveness research that
engages patients throughout the research process in order to increase the quantity, quality and
timeliness of useful, trustworthy information.28 The International Association for Public
Participation (IAP2) was founded in the US in 1990 with the goal of promoting public
involvement in government and industry decision-making.29 As of 2007 IAP2 had more than a
thousand members from 26 countries.29
Canada is emerging in the field of PER with the creation of CIHR’s SPOR initiative and the 11
provincial SUPPORT Units that act as conveners in their home province or territory.30 SPOR
acts as a catalyst for patient-oriented research by facilitating and directly funding research across
the country, and finding and supporting synergies between various stakeholders.31 Some of the
accomplishments of the Ontario SPOR Support Unit (OSSU) include a project that reduced
rehabilitation length of stay for people with stroke and work that resulted in patient-reported
experience measures being included in funding evaluations.32 Other Canadian organizations that
Page 10 of 128
conduct or support patient engagement in research include the Canadian Foundation for
Healthcare Improvement (CFHI) and the Canadian Common Drug Review Patient Advisors.
Established and emerging organizations have many roles to play, including creating a culture of
public participation, providing research funding for projects that engage patients throughout the
research process, and creating and developing guidelines and methods for engagement. These
organizations engage patients and other members of the public both in the research process and
in informing public and organizational policies. Their work need not all be related to patient
engagement in research, or even healthcare, to support the movement toward patient
engagement. Their broad efforts promote a culture of participation that spreads across sectors.
2.3 Benefits & Challenges of PER
2.3.1 Benefits for Research Projects
The contributions of patients have benefitted research projects in many tangible ways. Patients
help to clarify research questions, extend patient cohorts to include new members, suggest
reasons for low recruitment of study subjects and possible strategies to enhance recruitment,
review transcripts, suggest new outcome measures to include, assist with data analysis including
interpretation of results and identification of themes, and co-lead meetings.8
The most commonly cited quantitatively measurable benefits of PER is better recruitment and
retention of participants in clinical trials.4,33-35 A systematic review by Crocker et al found that
clinical trial studies that included patients in the research team significantly increased the odds of
a patient enrolling in the trial.34 This effect size was even larger when the patients involved in the
recruitment had lived experience of the condition under study, indicating that patients bring
significant added value to research studies as “experts in lived experience.”34 The researchers
noted that for many of the studies, patients were only involved in the recruitment process but if
they had been part of the research study from the beginning there was potential for the effect size
to be even larger.34
In a systematic review of the literature on involvement of patients in surgical studies, Jones et
al33 found two studies that included patients from the beginning and incorporated their
Page 11 of 128
suggestions into research topic identification and the design and conduct of the intervention. The
patients’ input had a direct and immediate effect on the study aim, protocol and outcome and
enhanced the face validity of the study. Some researchers believe that including patients in the
research process helps to ensure high participation rates because their contributions lead to more
salience of the research to the public.33
2.3.2 Personal Benefits to Research Partners
Researchers in the UK conducted a systematic review of the literature about the impact of patient
and public involvement on various stakeholders, including patients, researchers and the
community.25 Most benefits reported by patients are personal benefits, such as feeling listened to,
empowered and valued. Patients have also reported that their confidence increased because of
their research partnership experience and they felt a greater sense of self-worth.25 They also
reported feeling good about having an opportunity to give back to the research community.
Researchers who participated in research partnerships with patients reported that they benefitted
by an improved understanding of the health condition, greater respect for patients, having their
beliefs and attitudes challenged, new areas of research being opened, seeing their efforts
rewarded and gaining new friendships with community members.25
Patients have also reported that through their involvement in research they gained useful
professional skills, such as public speaking, interviewing and working in groups. They reported
that these new skills improved their chances of obtaining future employment.25
2.3.3 Benefits for Communities
The benefits of PER extend beyond the individuals directly involved in the partnership to the
communities that they are members of. These communities are sometimes geographically
defined but can also be broader communities defined by shared experiences of illness or shared
cultural/ethnic background. The benefits of PER to communities include mutual respect,
acceptability and trust of the research, a more research co-operative spirit, increased awareness
of disease, better distribution of information, increased membership for community groups, and a
sense of community ownership.25 Elliott et al summarized the benefits of engagement in research
prioritization among chronic kidney disease (CKD) patients as: increased integration of distinct
Page 12 of 128
stakeholder communities, an enhanced understanding of the CKD lived experience, and a refined
and refocused commitment to patient-centered CKD care. Patients in this study also reported that
their involvement in the research and the relationships with other CKD patients that it enabled
helped to address their perceived lack of community.36
PER has unique potential to benefit marginalized communities, such as Indigenous communities
that historically have had their perspectives and values excluded from decision-making and the
values of the Western medical establishment imposed on them. Research has been conducted to
review the effectiveness of community engagement in cancer control37 and arthritis38 studies
with Indigenous people in Australia, New Zealand, Canada and the US. The researchers found
communities were usually only engaged minimally, even though the most successful outcomes
resulted from engagement that included Indigenous community members throughout the research
process as true partners.37 Many opportunities still remain to build trust and genuine partnerships
with members of Indigenous and other marginalized communities that will facilitate health
research that results in better health outcomes in the community while respecting their unique
values, needs, and interests.
2.3.4 Logistical Constraints
The academic research process is laborious on its own and bringing patients into it introduces
additional logistical challenges for everyone involved. One of the most frequently cited
challenges of PER by both patients and researchers is the time commitment.25 For researchers
who don’t already have existing relationships with patients or patient groups, investing the time
and energy to establish these connections is time-consuming. While many funding agencies now
encourage or in some cases require PER, the amount of funding obtained may not include all that
is required to bring patients into the research process effectively.
Patients face many logistical challenges when joining research teams. In many cases they are not
compensated for their time,39 and they have to find a way to balance their responsibilities to the
research project with their other work or personal responsibilities. In some cases patients have
felt overburdened by the number of tasks required of them, such as reading unfamiliar
documents before meetings.25 Some patients have reported that they found the formal procedures
of research limiting and experienced emotional burdens related to sharing their personal
Page 13 of 128
experiences and feeling responsible for acting as a bridge between the researchers and the
community.25 These factors can limit which patients are able to participate.
There is currently a discussion within the field of engagement about compensating patient
participants, and many patients and researchers believe that engagement-related costs such as
parking, mileage and food should be covered by the research team.40 It is also believed by some
that a lack of compensation creates a power imbalance as it devalues the knowledge and
experiences that patients bring to the table.39 Despite this, the predominant culture in many
contexts resists the idea of compensating patient partners.39 However, some guidance is
emerging from various sources to ensure fairness and transparency in the process of considering
compensation.
2.3.5 Lack of Receptive Attitudes
Researchers are not always motivated to include patients in their research. This can be due to a
perception that patients lack the knowledge to contribute to research or a fear that allowing
people who are untrained in scientific methods to be part of a research team could have a
negative impact on the integrity of research.7 Researchers have reported feelings of skepticism
about the value of partnerships, concern about the value of the contributions that patients could
make, their competence to assist with research and the potential that they might have their own
lobbying agenda.25 In some cases researchers have found it difficult to accept the views of users,
to relinquish control, and to change working practices to accommodate partnerships.25
Researchers’ skeptical attitudes can create a vicious circle, where patients are only included to
fulfill a funder’s requirement, leading to patients feeling undervalued, unimportant and unable to
contribute, ultimately resulting in the partnership not producing results and reinforcing the
researchers’ skepticism.7
For PER to be successfully adopted, researchers need to believe that patients’ knowledge and
potential to be involved is of equal importance as their own and that PER has a meaningful
impact on research outcomes.7 For this to happen a cultural shift is required to lessen the
influence of traditionally positivist epistemology in order for qualitatively reported experiences
to be taken seriously and recognized as a legitimate form of knowledge.7 There are many

Page 14 of 128
variables from both researcher and patient perspectives to consider when engaging in
partnerships – including the capacity, skills, and attitudes that assure a good fit within the team
and enable collaborative working.
2.3.6 Representativeness & Recruiting for Diversity
The difficulty of recruiting a more diverse and representative group of patients is acknowledged
by many researchers40 and the strategy for recruiting vulnerable populations, such as those who
are socioeconomically disadvantaged, frail, or have chronic illness, remains unclear.36 Studies in
the UK emphasize that there is a need for more diverse research partners in terms of age, ability,
gender, class, ethnicity/race, geography, indigeneity, immigration status, religion and sexuality.40
The benefits of including these populations would be significant as their contributions could help
to address the lack of inclusiveness that currently exists in medical research samples, which
would ultimately lead to results that are more applicable to a wider range of patients.1
In a survey of Canadian cardiovascular researchers about PER one of the top concerns raised was
about how to identify and recruit patient partners that reflect the diversity within the patient
population under study.7 There was a sense that there is not an agreed upon criteria for what
constitutes a “good” patient to include as a research partner – should it be the smartest patient,
the sickest patient, the most articulate patient or the patient with the most time? If the patient is
chosen based on convenience or because of their existing knowledge of research or their
articulateness, certain socioeconomic groups and people with low health literacy may be
systematically excluded.7 In fact, there is a growing awareness of the fact that the majority of
those who are included in engagement activities are socioeconomically advantaged women from
ethnic majority groups.41 There is also the concern that if the same individuals are involved in
too many patient engagement activities they run the risk of becoming ‘super-patients.’40 This
occurs when a layperson becomes ‘socialized’ as a researcher and as a result of their formal
training and research experience they lose the ability to represent the voices of patients.40
It is not only logistical and socioeconomic factors that make recruiting for diversity difficult. A
scoping review of PER related to dementia found that there are unique barriers to including
people with dementia but also important reasons to make the effort to do so.42 The barriers that
people with dementia face are associated with cognitive and communication symptoms, but also

Page 15 of 128
stigma because of the societal view that they would not be capable of fully participating in
research. Putting in the work to bring people with dementia, or other conditions that are
stigmatized, into the research process could help to reduce stigma and negative stereotypes as
well as open the door to a much deeper understanding of the lived experiences of these
individuals.42
A systematic review by Bonevski et al found strategies for increasing the number of
socioeconomically disadvantaged populations in research.43 The authors suggest a multipronged
approach including: 1) taking a long-term view and investing the time to develop strong
relationships with communities and community groups, 2) including the additional costs in
funding applications for things like translations services, flexible data collection locations and
times, gifts or incentives, culturally tailored resources and materials, and additional staff training,
and 3) allowing time for authorship negotiations since data ownership may need to be negotiated
with non-academic collaborators.43
2.3.7 Building Relationships & Avoiding Tokenism
Effective, high quality relationships and communication are key components of successful
research partnerships.4 Unfortunately in some cases patients have reported feeling like they were
not being listened to or taken seriously and that health professionals and researchers were
insensitive, which lead to patients feeling low self-esteem and an unease about expressing their
opinions.25 They also reported a lack of feedback from the researchers about the value of their
impact which made them feel less motivated to be involved in future projects.25 This is a
significant problem because feeling part of the team is a strong predictor of whether patients feel
that their involvement made a difference.4,40 Additionally, patients are in a vulnerable position
when they are asked to share their painful, awkward, difficult or intimate experiences in order to
improve health care and contribute to the research. This can be traumatic for patients and
researchers’ insensitivity to it could cause rifts.39
There are a few factors that can contribute to good relationships in research partnerships. For
instance, early involvement of patient partners and including them in roles that are responsive
and managerial rather than oversight roles has been shown to contribute to higher perceived
Page 16 of 128
impact.4 Patients that are only brought into the research after important decisions have already
been made may feel that their role is not as important. Recognizing the circumstances of patient
partners and providing adequate compensation can also contribute to better relationships.
According to a group of patient partners, researchers should be mindful of the power imbalance
that exists if everyone on a research team is compensated except for patient partners.39
Tokenism is a predominant concern in engagement research.8-10 As patient engagement is
increasingly recognized as a priority by funding agencies, researchers are incentivized to include
a plan to engage patients in research protocols in order to be eligible for funding. However, not
all researchers who do this intend to genuinely involve patients in their research and have only
included a plan to engage patients in their protocol to increase their chances of obtaining
funding.6,9
Tokenism occurs within the patient engagement process when patients serve more of a window-
dressing role than as authentic research partners.9 This can be the result of uninformed or overly
simplistic assumptions about the knowledge and abilities that patients have and a belief that their
views don’t need to be taken seriously.8 Tokenism can also occur despite the best intentions of
researchers when the demands and challenges that are involved in building and maintaining
effective relationships with partners become too daunting.9
One of the ways researchers can build effective relationships with patient partners and avoid
tokenism is by ensuring that they have a detailed plan for patient engagement before starting.
The FIRST (facilitate, identify, respect, support, train) framework is a useful tool for creating a
non-tokenistic research partnership.8 To facilitate a partnership, researchers need to make a plan
to address potential barriers that patient partners may face. This could include creating a
reimbursement plan, choosing an accessible location for meetings and determining how patient
partners will be recognized for their contribution (e.g., coauthor on grant application and/or
publication). Researchers must also identify research projects that are conducive to partnerships,
patients who could add value to the project and the roles that those patients will have in the
project based on their skills and background. Any projects that stand to benefit from an
understanding of the lived experiences of patients have potential for patient partnership. Patients
who have in-depth experiential knowledge of the health condition under study (by having
Page 17 of 128
experienced it themselves or having cared for someone with the condition) have much to
contribute to the project. In addition to their lived experiences, patient partners often have other
skills and aptitudes that could make it possible for them to contribute in research activities such
as drafting protocols and questionnaires, analysis of data, and giving presentations. To respect a
patient means to acknowledge the value of their contribution and support means to ensure
ongoing working communication. Training is a key step that is needed to ensure that patient
partners have an adequate understanding of the research process to contribute meaningfully and
it is the responsibility of the researchers to ensure that patients have access to the training
resources that they need.8
Another way for researchers to avoid tokenism is to ensure that the entire research team is
engaged in the patient partnership, rather than having only one team member acting as a liaison
in a way that cordons off the patients from the rest of the team.6
2.3.8 Measuring Impact
PER is far from uniform in its application. It can range from full partnership to minor
consultation and can take place throughout the research lifecycle or only in one phase. These
factors make it difficult to establish a methodology for quantifying its impact. In fact, some
researchers argue that attempting to evaluate PER is fundamentally disingenuous because the
value gained from patient engagement is necessarily context-specific and the knowledge gained
by researchers in the process is experiential and therefore impossible to categorize or quantify.26
However, governments, funding organizations, researchers and patient organizations are
increasingly asking to see evidence for the benefits, value and return on investment of
engagement.44 Effective evaluation of PER could create evidence about the costs, benefits and
risks related to engagement for those who are critical of it and lead to more widespread use.
When the science around PER is strengthened, this knowledge can help to ensure that it becomes
an integral, robustly conducted and well-resourced component of research, and that the particular
gaps in our knowledge can be formally addressed in future research.44
A wide range of evaluation tools for PER have been developed, however most of them focus on
procedural aspects of research partnerships more than outcomes.44 Boivin et al conducted a
systematic review of evaluation tools for engagement in research and health system decision-
Page 18 of 128
making and assessed 27 tools using four criteria: scientific rigour, patient and public perspective,
comprehensiveness, and usability.44 Overall, the tools were lacking in scientific rigour, as
reliability testing was very rare and only a small number of them were informed by a literature
review – stakeholder experience was the most common source of knowledge. More than half of
the tools were developed with patients and members of the public, but their involvement was
usually limited to the pilot stage. Only five tools met all the criteria for comprehensiveness and
two for usability.44 Abelson and colleagues suggest that the fact that most evaluation tools are
questionnaires and surveys is a limitation because there are limits to the depth and breadth of
information gathered without personal interaction. They suggest a mixed methods approach is
best for evaluating PER.45 For example, researchers could administer surveys among research
partners and conduct one-on-one interviews.
2.4 Building Capacity for PER: The Resource Landscape
2.4.1 The Need for Resources
The set-up process for a successful research partnership requires detailed considerations so that
all parties involved are clear about expectations and have the necessary skills and resources to
fulfill those expectations.8,40 Research shows that whether or not researchers have clearly defined
goals and plans for a research partnership (other than to ‘tick a box’ on a grant application) is a
determinant of whether the partnership will have an impact.4 Failure to adequately prepare has
led to patients not feeling like they can participate and as a result, attending less meetings.25 Both
patients and researchers can benefit from resources that inform them about how research
partnerships work, what to expect and how to avoid or mitigate challenges.
2.4.2 Existing PER Learning Resources
A range of resources have been designed to increase knowledge about and build capacity for
PER for healthcare organizations, researchers, patients, families and caregivers. These resources
include webinars, online courses, one-day training courses, video resources, training modules,
and engagement evaluation tools. Many international organizations have developed tools,
particularly in the US and the UK. The Beryl Institute based in Texas provides on-demand
webinars which are led by patient experience leaders with the goal of sharing practises and
Page 19 of 128
strategies that can be implemented in healthcare organizations.46 Washington, DC-based PCORI
provides a series of webinars about patient-centered outcomes research that are designed to
present examples of engagement practises.47 The Warwick Medical School in the UK offers a
free one-day workshop to support patients or members of the public who are thinking about
getting involved in research or are already involved.48 INVOLVE is a national advisory group
established in 1996 by the UK’s National Institutes of Health Research (NIHR). INVOLVE
offers a one-day training course for researchers as well as patients and members of the public
who are already actively involved in research.49
Resource development for PER in Canada is on the rise as funding opportunities from CIHR’s
SPOR initiative increase and provincial SPOR support units provide grants for building capacity
in patient-oriented research. St. Michael’s Hospital in Toronto offers a free webinar course twice
a year called Partners in Research (PiR), designed for patients, caregivers and researchers. The
course consists of 4 live web-based sessions where participants receive personalized learning
through interactive activities and discussions with others who are interested in or already
involved in research.50 The Patient-Oriented Research Curriculum in Child Health (PORCCH)
was developed through the collaboration of various Canadian organizations. PORCCH is an
interactive online curriculum that is designed to build capacity in patient-oriented child health
research and enhance the skills of children, families, trainees, clinicians, scientists, educators and
administrators. It includes interactive tools, video vignettes and evaluation exercises.51 In 2018 a
training tool was developed at Western University in Ontario, called the Patient-Oriented
Research Training and Learning – Primary Health Care (PORTL-PHC) program. PORTL-PHC
is a free, online and self-directed program that focuses on skills development, context-specific
application, methods and examples of patient-oriented research in primary health care.52
The purpose of these supportive resources is to help people prepare for research partnerships and
the examples described show some of the range in format these resources can take. Although
some of these resources feature individual testimonials from people with partnership experience,
there are no resources to date that feature stories of researchers and patients with lived
experiences of partnerships, gathered in a rigorous way. This study evaluates such a resource.
Page 20 of 128
2.5 Evidence for the Benefits of Using Video Narratives
2.5.1 The Persuasive Power of Narratives
Communications literature provides ample evidence for the value of using narratives to influence
knowledge, attitudes and behavior in a wide range of areas. The use of narratives has been
evaluated for its impact on organ donor registration,53 cancer screening,54-56 medical cannabis
use,57 breastfeeding58 and communicating with people with intellectual/developmental
disabilities.59 A 2016 meta-analysis of studies that evaluated the persuasive influence of
narratives found that narratives positively influence message recipients’ beliefs, attitudes,
intentions and behaviors, moving them into closer alignment with the views presented in the
narrative: “Thus, we can categorically conclude that narrative does exert a causal influence on
four of the most common indices of persuasion” (pg. 461)60 (beliefs, attitudes, intentions and
behaviours).
The evidence for the persuasive power of narratives is strengthened further when narratives are
compared with non-narrative formats. In a study to measure the differential impact of messaging
format to promote organ donation compared the impact of video format on 781 study participants
(median age of 29 years, 41% female, 24% non-white). The study included six different videos:
four that included personal narratives, one purely informational and one unrelated to organ
donation (control). The video that had the highest impact on organ donation willingness was a
personal narrative video that featured a pediatric transplant recipient.53 A study that explored the
impact of messaging format for communicating breast cancer screening compared the impact of
video formats on 194 Italian-speaking women ages 18-30 years old. The study included a control
and four experimental formats: narrative video, didactic video, narrative infographic, and
didactic infographic. The results showed that the didactic video had the greatest impact on
awareness and knowledge about screening, while the narrative video had the most positive effect
on attitude and intention toward screening. In all cases the videos outperformed infographics.56
A study comparing narrative versus non-narrative video formats for presenting information about
medical cannabis use found that the narratives positively influenced attitudes, beliefs and
intentions toward medical cannabis use, and this in turn positively influenced attitudes, beliefs
Page 21 of 128
and intentions toward recreational cannabis use among 396 Israeli participants. Exposure to
narratives was particularly influential when the narrative presented the patient using medical
cannabis as not to blame for their illness.57 Authors investigating the differential impact of
informational versus narrative videos about breast cancer among African American women (n =
489; 67% with high school education or less; 77% with annual household income of $20,000 or
less; average age of 61 years) found a significant difference between groups in relation to
counterarguing (i.e., generating thoughts that counter, reject or discount a message), which is
associated with fatalistic beliefs about cancer and higher perceived barriers to mammography.
Those who watched the narrative video had lower counterarguing, higher engagement and talked
with family members more which increased message recall. The authors concluded that the
strength of cognitive and affective responses to narratives effects message processing and
behavioral correlates.61
2.5.2 The DIPEx Model
The internet is a major source of health information and support.62,63 Many online health
resources present “facts and figures” based on scientific evidence, however as social networking
sites continue to gain prominence in the online space, it has been found that many people are
using the internet not only to find technical information but also to find others with similar
experiences.62 A survey of 3,014 adults by the American thinktank Pew Research Center in 2012
found that 26% of adult internet users read or watched someone else’s health experience about
health or medical issues in the past 12 months, and 16% went online for the purpose of finding
others with similar health concerns.64 When people search for health information online they are
drawn to the parts of websites that show others’ experiences.63 Engaging with others’
experiences online can influence decision-making, decrease the sense of isolation and help a
person to adjust to their health condition.62
A unique way of presenting information was developed at the University of Oxford by the
Health Experiences Research Group (HERG) who initiated the Database of Individual Patient
Experiences (DIPEx). Both the HERG and DIPEx were founded by Dr. Ann McPherson, a
general practitioner who wanted to know more about the impact of health conditions on patients’
quality of life. The website that is now called healthtalk.org (formerly dipex.com and

Page 22 of 128
healthtalkonline.com) was created in 2001 to be a repository of evidence about personal
experiences of illness, gathered through rigorous qualitative research, accessible to the public.
Healthtalk.org is managed by the DIPEx charity in collaboration with the HERG, which is
responsible for the research that is displayed on the website.65 The HERG conducts in-depth
qualitative interviews with individuals living with various health conditions using diverse
sampling methods to produce a sample of 40-50 individuals per condition that includes a broad
range of experiences. The interview method combines an unstructured, open-ended narrative
approach with semi-structured prompts, so that the concerns, meanings and priorities of those
being interviewed can be emphasized66 The HERG researchers analyze the interviews to find key
themes and then write a lay summary of each theme which is displayed on healthtalk.org
alongside selected illustrative quotes and audio or video clips from the interviews. To date
healthtalk.org has more than 100 modules, each covering a different health condition.
This UK-based initiative is now a global movement. DIPEx International currently has members
from 14 countries: Australia, Canada, the Czech Republic, Brazil, Germany, Israel, Japan, Korea,
the Netherlands, Norway, Spain, the UK, Switzerland and the US. Each of these member groups
produces their own health experiences website using DIPEx research methodology to learn about
the health experiences of people living in their communities. The groups are all based within
accredited universities or university-affiliated research centers and led by senior scientists.65
With the websites from all of these countries combined there more than 140 health conditions
covered and interviews have been conducted in 11 different languages.65
The usefulness of this kind of internet resource has been subject to a few formal evaluations.
Researchers at Oxford evaluated the relevance of the DIPEx website for the information needs of
cancer patients.55 Before being shown the website, study participants were asked about what they
would like a health website to include and one of the things that they identified as important was
experiential information from other patients. After being shown the website, study participants
said that being able to hear the stories of patients like them would have made them feel less
isolated and afraid if they had access to it during their illness. Study participants also mentioned
that being able to access the emotional experiences of others without having to engage in return,
as would be expected in a support group, was perceived as valuable, especially for those who
experienced embarrassment about seeking help related to their condition. Participants also felt

Page 23 of 128
that the website would have assisted with decision-making and given them the confidence to be
more assertive when communicating their needs to health care professionals. Listening to others
describe experiences like their own created a sense of validation about their experiences and
perspectives.55 An evaluation of a DIPEx module on rheumatoid arthritis found that a majority of
the participants who completed the questionnaire found the website interesting and informative.
A majority also felt the website covered a wide range of information, covered experiences like
their own and would be useful to others.63 The need for further evaluation has been identified as
a priority amongst the DIPEx International members (Susan Law, personal communication).
2.6 Summary and Rationale for Further Evaluation
Patient engagement in research is emerging as an innovative way of involving patients in the
decision-making that impacts their care. It has gained prominence internationally and takes many
forms, some involving patients less and some more. The benefits of PER can include the
production of results that better align with patients’ needs, which can be applied in a way that
improves patient-centered care. Challenges include avoiding tokenism, achieving diverse
representation, and measuring the impact of PER. Several resources to support PER have been
developed in recent years but it is unclear how useful they are for patients and researchers. By
evaluating existing resources, we can gain valuable knowledge about what patients and
researchers need and want, and where the gaps are.

Page 24 of 128
Methods
3.1 Introduction to Methods
3.1.1 Description of Website
The website under evaluation in this study was designed using the Database of Individual Patient
Experiences (DIPEx) methodology.65 The first step in creating the website included recruiting 33
patients, caregivers, and researchers who had experience with patient-researcher partnerships,
using maximum variation sampling. Experienced qualitative researchers then conducted face-to-
face, semi-structured, audio and/or video-recorded, narrative interviews with the participants.65
These interviews took place at the participants’ home or another place that was convenient for
them (e.g., office). Next, the interviews were transcribed and thematically analyzed. Finally, the
website was constructed, with each theme represented as a topic page. Each topic page included
multiple short video/audio clips from the participant interviews and a short lay summary of the
theme. The website also included a page for each participant which included their first name (or
a pseudonym), their photo (if they’ve consented), and a short biography.
The patient-researcher partnership website (https://healthexperiences.ca/patient-researcher-
partnership/patient-researcher-partnerships) is housed within the Canadian DIPEx website
https://healthexperiences.ca/, which also contains other sections (e.g., breast cancer, family
caregiving). For the evaluation, links to the rest of the website were disabled, since the
evaluation was only meant to capture perceptions of the patient-researcher partnership website.
The patient-researcher partnership website contained 17 topic pages at the time of the evaluation,
and included clips from interviews with 33 different patients, caregivers, and researchers. Four of
the 17 topic pages had not yet been created at the time of the evaluation and ‘Coming Soon’ was
added to their title.
Topic pages were listed on the left side and other navigation along the top of the page. See
Appendix A for a screenshot of the website’s landing page.
Page 25 of 128
3.1.2 Institutional Context
This evaluation is part of a larger study that received funding from the Ontario Strategy for
Patient-Oriented Research (SPOR) Support Unit (OSSU). It was one of seven projects that
received funding from OSSU through an initiative that aimed to increase capacity for patient
engagement in research across Ontario. The research team for this study was based at the
Institute for Better Health (IBH) at Trillium Health Partners (THP), in collaboration with team
members from The Ottawa Hospital, University of Ottawa, and the University of Toronto. The
advisory team also included two patient/caregiver advisors in addition to other researchers and
educational as well as patient engagement leads. The overall study was led by Susan Law (PI)
and the evaluation component (the focus of this thesis) was led by student PI Donna Plett.
3.1.3 Paradigmatic Perspective
The design of this evaluation is rooted in pragmatism, identified by Peggy Shannon-Baker as one
of four paradigms used in mixed methods research (which also include transformative-
emancipation, dialectics, and critical realism).67 Though there is some disagreement among
researchers about its definition, paradigms in research can be understood as the beliefs a
researcher holds about how knowledge is created.68 These kinds of beliefs are at the root of the
“paradigm wars” which have been a source of antipathy between qualitative and quantitative
researchers for many decades. 67
Pragmatism is distinct from positivist (quantitative) and metaphysical (qualitative) approaches to
research in one key way: the use of abductive reasoning, which moves back and forth between
inductive (qualitative) and deductive (typically quantitative) reasoning.68 Pragmatism is
outcome-oriented, focuses on the product of research, and characterized by an emphasis on
creating practical solutions to social problems.67 By embracing the elements offered by
qualitative and quantitative methods, a pragmatic approach maintains a balance between
subjectivity and objectivity which lends itself to analysis that is both contextually-based and
transferable to other contexts.67
Page 26 of 128
Pragmatism informed the design of this study in a few ways: by the inclusion of qualitative and
quantitative data collection methods, the framing of the study design in multiple theories (i.e.,
Social Learning Theory and Theory of Planned Behaviour), and the blending of different forms
of data in the interpretation of the results. Abductive reasoning was applied throughout the
process, particularly in the interpretation phase, as learnings from qualitative methods were
combined with learnings from quantitative methods. The mixing of methods also served to
increase the practical value of the findings by giving a fuller picture of how the website was used
and how people responded to it in various contexts. In these ways the design of the evaluation
struck a balance between reflexivity and objectivity, with the ultimate goal of creating learnings
that are practically useful and academically sound.
3.1.4 Methodological Approach
Mixed methods research, generally defined as any research that combines qualitative (QL) and
quantitative (QN) methods, has gained prominence in recent decades.69 While some argue that
qualitative and quantitative methods are separate and opposing forces,70 the employment of
mixed methods rejects this dichotomy by using both methods with the belief that together, in
some circumstances, they can provide more robust answers to research questions than either
method alone.
Quantitative methods (e.g., clinical trials, surveys) often use large sample sizes and can be useful
for measuring previously defined entities, processes, and concepts. For example, a mental health
researcher who wishes to understand the impact of depression on a population could administer
surveys across the population to measure how many report pre-defined symptoms of depression.
Qualitative methods (e.g., interviews, field observation) tend to use smaller sample sizes and are
useful for gaining deep and nuanced understandings of new or existing entities, processes, and
concepts. An example of this would be if the mental health researcher chose to conduct
interviews with a selection of individuals to understand what depression means to them and how
it impacts their day-to-day life. The QN approach would provide information with a limited level
of detail about a large proportion of the population (i.e., whether they experience pre-defined
symptoms of depression), and the QL approach would give a more detailed and nuanced
understanding of the lived experience of depression for a smaller proportion of the population. A
Page 27 of 128
mixed methods approach would recognize the value both kinds of data could add to their
research and include both in the design of their study. By combining quantitative and qualitative
findings, the researcher may gain insight into how useful the quantitative measure was for the
target population using qualitative findings. For instance, the qualitative findings may indicate
that some members of the population don’t identify with the terms used in the survey but do
experience symptoms of depression. This could inform a redesign of the survey to match the
terminology used by the population.
This simple example represents one way in which mixed methods could add value to research,
however there are many reasons why researchers may choose to mix methods. According to a
typology developed by Greene et al. there are five rationales for combining methods:
triangulation (for comparison of findings), complementarity (to assess various dimensions of a
phenomenon), development (to design second method based on findings from first), expansion
(to measure different phenomenon), and initiation (to address the goal of divergence).71 Mixed
methods research also takes many forms. Ozawa & Pongpirul (2014) present six prototypes for
mixed methods research: convergent parallel (where QN and QL are collected simultaneously),
explanatory sequential (where QN preceded QL), exploratory sequential (where QL precedes
QN), embedded (where one is contained within the other), transformative (where QN precedes
QL within a framework), and multiphase (where there are at least three phases of data
collection).11,72 The appropriate design in any given circumstance will depend on the research
question, population under study, and available resources.
Mixed methods approaches are importantly different from multi-method approaches. A multi-
method approach employs more than one methodology but does not necessarily integrate
findings across methods. A multi-method study may present findings from different methods
next to each other, but not consider how each may complement or inform the other. Mixing
methods, in contrast, aims to combine the strengths, and compensate for the limitations, of
qualitative and quantitative methods.73
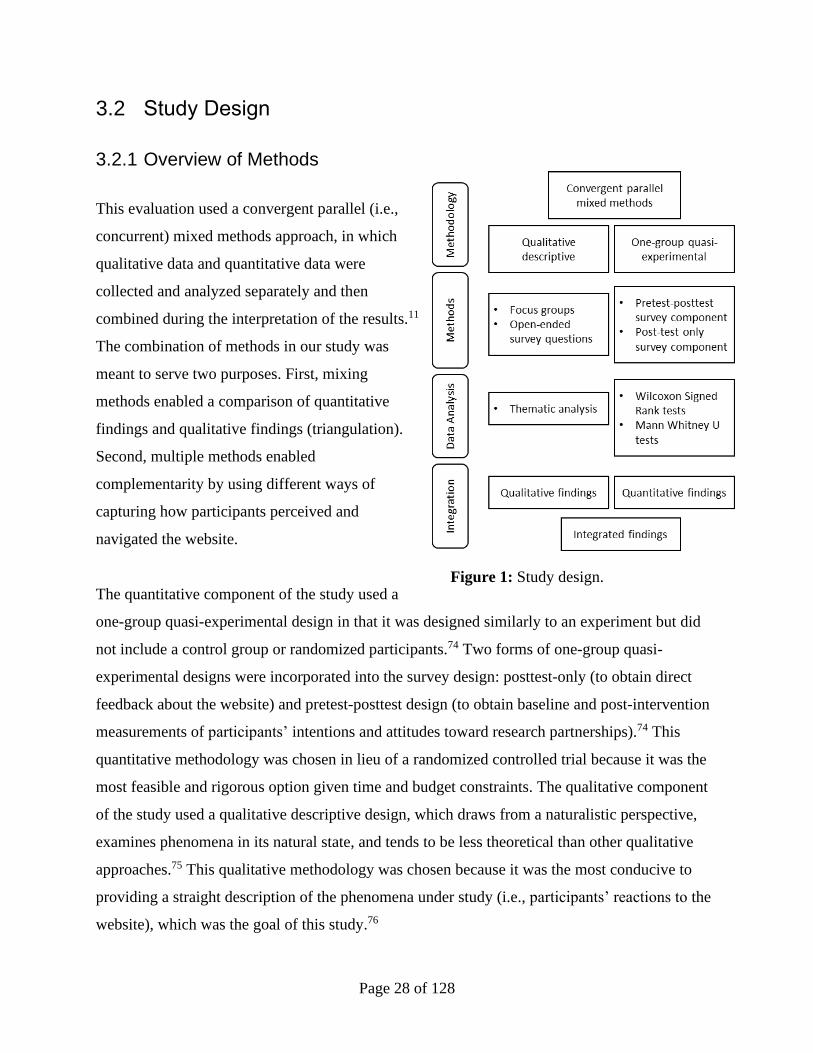
Page 28 of 128
3.2 Study Design
3.2.1 Overview of Methods
This evaluation used a convergent parallel (i.e.,
concurrent) mixed methods approach, in which
qualitative data and quantitative data were
collected and analyzed separately and then
combined during the interpretation of the results.11
The combination of methods in our study was
meant to serve two purposes. First, mixing
methods enabled a comparison of quantitative
findings and qualitative findings (triangulation).
Second, multiple methods enabled
complementarity by using different ways of
capturing how participants perceived and
navigated the website.
The quantitative component of the study used a
one-group quasi-experimental design in that it was designed similarly to an experiment but did
not include a control group or randomized participants.74 Two forms of one-group quasi-
experimental designs were incorporated into the survey design: posttest-only (to obtain direct
feedback about the website) and pretest-posttest design (to obtain baseline and post-intervention
measurements of participants’ intentions and attitudes toward research partnerships).74 This
quantitative methodology was chosen in lieu of a randomized controlled trial because it was the
most feasible and rigorous option given time and budget constraints. The qualitative component
of the study used a qualitative descriptive design, which draws from a naturalistic perspective,
examines phenomena in its natural state, and tends to be less theoretical than other qualitative
approaches.75 This qualitative methodology was chosen because it was the most conducive to
providing a straight description of the phenomena under study (i.e., participants’ reactions to the
website), which was the goal of this study.76
Figure 1: Study design.
Page 29 of 128
We utilized three data collection methods: surveys, focus groups, and website analytics. Surveys
are widely used by social researchers, as they offer a relatively quick way of obtaining
information from a large group of people. By using standardized questions, surveys make it
possible to quantify differences in responses between subgroups, which is useful for developing
an understanding of the needs of different groups.77 Despite the popularity and usefulness of
surveys, they are subject to some limitations. These include response and non-response biases
(e.g., when some groups are more likely to complete the survey than others) and measurement
error (e.g., when questions are poorly written and/or responses are open to misinterpretation).78
Focus groups are a qualitative method of data collection also commonly used by social
researchers. Focus groups typically include smaller groups of participants to enable open
discussion, guided by at least one skilled moderator. Focus groups leverage group interactions
and enable participants to exchange experiences and perspectives with each other.79 These group
dynamics are believed to help participants explore and clarify their views more easily than in a
one-on-one interview.79 Focus groups are also convenient, in that they enable simultaneous data
collection from multiple people. Some challenges or limitations of focus groups include the
possibility for some individuals to dominate the discussion, tendencies toward normative
discourse, and conflicts and arguments between group members.80
Web analytics is a relatively new method of data collection. It is commonly used for business
and market research in order to understand web traffic and to assess and improve a website’s
effectiveness or profitability. Web analytics services, such as Google Analytics, collect detailed
information about how websites are used, including (but not limited to) what visitors click on
within the website, how long visitors stay on the website, and how visitors got to the website.
Web analytics is limited as a research methodology in that it does not capture how visitors
perceive content or why some content is viewed more than other content.
Our study used two surveys, one administered before participants accessed the website and one
after they’d had access for approximately one week. The purpose of the first survey was to
collect demographic information, learn what participants felt about the internet as a resource to
Page 30 of 128
learn about PER, and what their intentions and attitudes toward PER were. The purpose of the
second survey was to learn about their perceptions of the website and whether their intentions
and attitudes toward PER had changed after spending time on the website. This quantitative
component added value by enabling measurement of variables (e.g., participants’ attitudes
toward patient engagement in research) and comparison of differences in responses between
groups (e.g., patients and researchers). It was also helped to give context to the qualitative
findings.
We invited some participants to partake in a focus group a few days after completing the
surveys. The purpose of the focus groups was to gain a richer understanding of participants’
response to the website by allowing them to share their thoughts and feelings in a semi-
structured discussion. This qualitative component added value because very little literature exists
about the evaluation of resources for patient engagement in research, and no literature exists to
evaluate a website that uses video narratives to provide information about partnerships. The
exploratory approach made it possible for study participants to bring new themes to light during
the focus groups.
Web analytics data were collected for the period that participants had access to the website. The
purpose of collecting this data was to gain insight into how participants navigated the website
and which content was the most engaging for participants. Web analytics measured a level of
detail about participants’ real-time utilization of the website in a way that could not be measured
by surveys or in focus groups. Web utilization data also added a unique and essential component
to the research because it is not self-reported, and in that way is not subject to some of the biases
associated with interview or survey data.
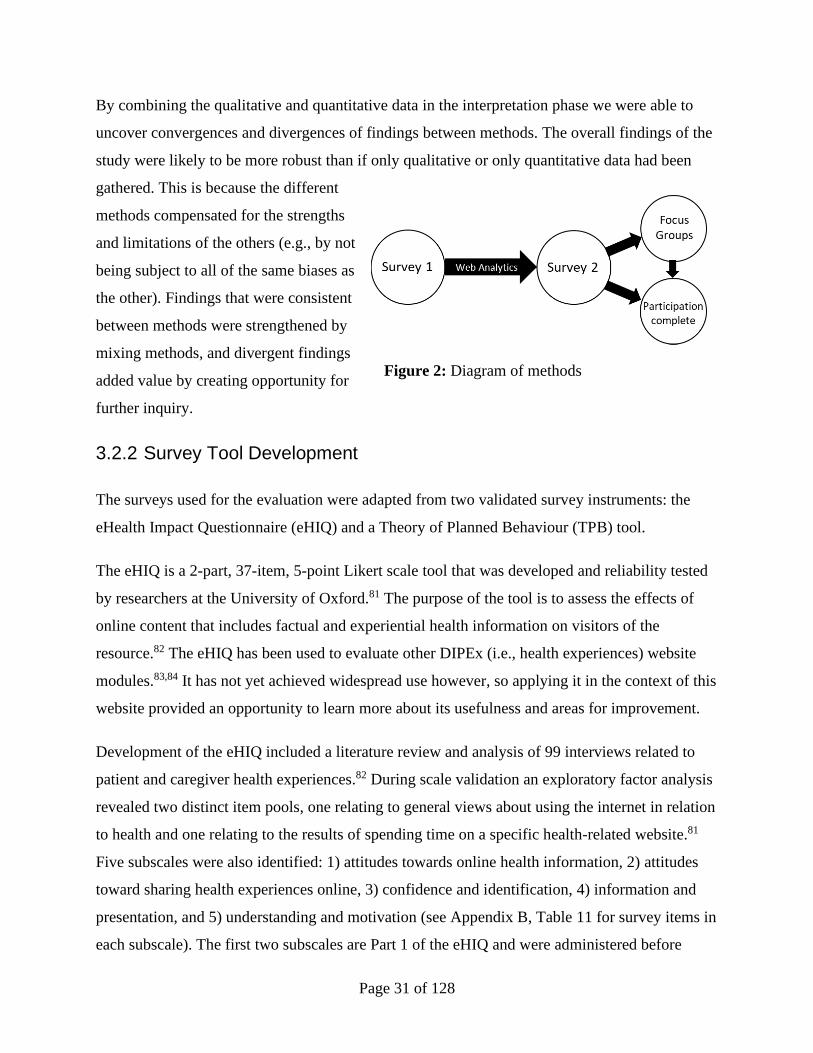
Page 31 of 128
By combining the qualitative and quantitative data in the interpretation phase we were able to
uncover convergences and divergences of findings between methods. The overall findings of the
study were likely to be more robust than if only qualitative or only quantitative data had been
gathered. This is because the different
methods compensated for the strengths
and limitations of the others (e.g., by not
being subject to all of the same biases as
the other). Findings that were consistent
between methods were strengthened by
mixing methods, and divergent findings
added value by creating opportunity for
further inquiry.
3.2.2 Survey Tool Development
The surveys used for the evaluation were adapted from two validated survey instruments: the
eHealth Impact Questionnaire (eHIQ) and a Theory of Planned Behaviour (TPB) tool.
The eHIQ is a 2-part, 37-item, 5-point Likert scale tool that was developed and reliability tested
by researchers at the University of Oxford.81 The purpose of the tool is to assess the effects of
online content that includes factual and experiential health information on visitors of the
resource.82 The eHIQ has been used to evaluate other DIPEx (i.e., health experiences) website
modules.83,84 It has not yet achieved widespread use however, so applying it in the context of this
website provided an opportunity to learn more about its usefulness and areas for improvement.
Development of the eHIQ included a literature review and analysis of 99 interviews related to
patient and caregiver health experiences.82 During scale validation an exploratory factor analysis
revealed two distinct item pools, one relating to general views about using the internet in relation
to health and one relating to the results of spending time on a specific health-related website.81
Five subscales were also identified: 1) attitudes towards online health information, 2) attitudes
toward sharing health experiences online, 3) confidence and identification, 4) information and
presentation, and 5) understanding and motivation (see Appendix B, Table 11 for survey items in
each subscale). The first two subscales are Part 1 of the eHIQ and were administered before
Figure 2: Diagram of methods
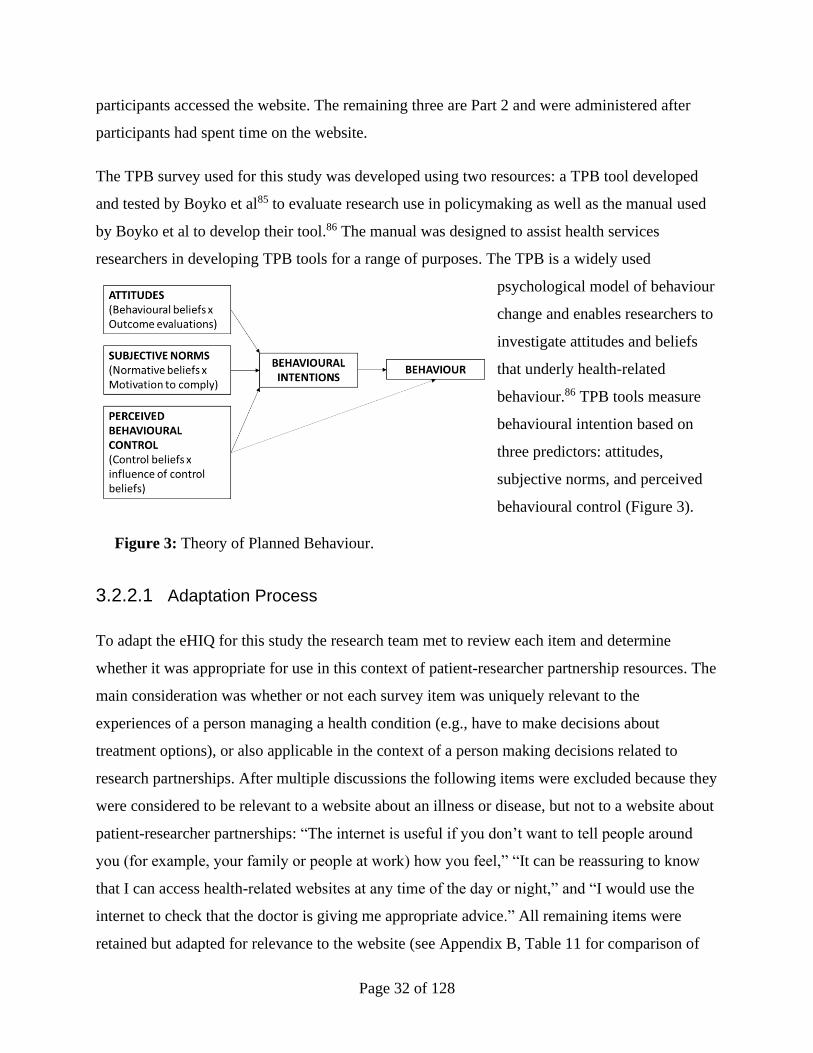
Page 32 of 128
participants accessed the website. The remaining three are Part 2 and were administered after
participants had spent time on the website.
The TPB survey used for this study was developed using two resources: a TPB tool developed
and tested by Boyko et al85 to evaluate research use in policymaking as well as the manual used
by Boyko et al to develop their tool.86 The manual was designed to assist health services
researchers in developing TPB tools for a range of purposes. The TPB is a widely used
psychological model of behaviour
change and enables researchers to
investigate attitudes and beliefs
that underly health-related
behaviour.86 TPB tools measure
behavioural intention based on
three predictors: attitudes,
subjective norms, and perceived
behavioural control (Figure 3).
3.2.2.1 Adaptation Process
To adapt the eHIQ for this study the research team met to review each item and determine
whether it was appropriate for use in this context of patient-researcher partnership resources. The
main consideration was whether or not each survey item was uniquely relevant to the
experiences of a person managing a health condition (e.g., have to make decisions about
treatment options), or also applicable in the context of a person making decisions related to
research partnerships. After multiple discussions the following items were excluded because they
were considered to be relevant to a website about an illness or disease, but not to a website about
patient-researcher partnerships: “The internet is useful if you don’t want to tell people around
you (for example, your family or people at work) how you feel,” “It can be reassuring to know
that I can access health-related websites at any time of the day or night,” and “I would use the
internet to check that the doctor is giving me appropriate advice.” All remaining items were
retained but adapted for relevance to the website (see Appendix B, Table 11 for comparison of
Figure 3: Theory of Planned Behaviour.

Page 33 of 128
original and adapted versions). As in the original version, all survey prompts were presented in a
5-point Likert agree/disagree format.
The TPB is a conceptual model that researchers adapt for their purposes, and there is not on
original survey tool. Instead, the TPB tool used for this study was developing using a guidebook
written for health researchers.86 The TPB tool was adapted to be relevant to the behaviour the
website was believed to inspire – participation in patient-researcher partnerships (see Appendix
B, Table 12 for survey items by domain). To determine the website’s influence, we used a pre
and post model for this tool. All survey participants responded to the TPB questions twice, once
before they were given access to the website, and once after they had had approximately one
week to review the website content. This measure was used to separate pre-existing attitudes and
intentions related to patient engagement in research from any changes resulting from their
experience engaging with the website content. As in the guidance materials used,85,86 all
questions were presented in a 7-point Likert format. Alternative formats are acceptable for some
constructs but for the sake of simplicity and consistency we chose to use the 7-point Likert
throughout.
Additional questions were added to the survey to capture participant details, including age,
gender, country of birth, self-described ethnic origin/cultural background, city and province of
residence, education, employment status, and occupation. Participants were also asked to identify
what their role in a patient-researcher partnership would be (researcher, patient/caregiver, either,
or other), their amount of prior experience as a research partner, and whether they had received
prior training in research partnerships. These questions were included to enable a descriptive
account of participants as well as options for stratification of responses to other survey questions
by participants partnership role (e.g., patient or researcher) (see Appendix G for full surveys).
The survey was reviewed by multiple members of the research team throughout the development
process. This was to ensure that questions were appropriate and worded clearly and in a way that
both patients and researchers would understand.
Page 34 of 128
3.2.2.2 Integration with Online Survey Software
We chose to administer the surveys online, rather than in person or by telephone, for a few
reasons: 1) it would be convenient for participants because they could complete the survey at
their location and time of choice, 2) it would enable us to broaden our recruitment strategy to
include participants across Canada, since involvement in the study could be completed entirely
online, and 3) since the subject of our evaluation was a website, we could only recruit
participants with internet access anyway (because non-internet users could not use the website),
so there was not a concern about excluding non-internet users from the evaluation.
We considered a variety of online survey platforms, including Google Forms, Qualtrics,
SurveyMonkey, and REDCap. Our main considerations were data privacy, user-friendliness,
cost, and the software’s ability to accommodate a pre and post survey design. Our first choice
was REDCap, as it offered the highest level of data privacy and functionality, was the most
likely to receive REB approval, and THP had an existing account that could be used for this
study at no additional cost. The surveys were imported into REDCap and tested by the research
team.
It was later learned that THP’s REDCap account only allowed for surveys to be completed by
those connected to THP’s intranet. This would have made it impossible for participants to
complete the surveys at home, so it was necessary to move the surveys to another platform and
submit a REB amendment before proceeding with data collection. We chose to move the surveys
to SurveyMonkey because of its user-friendly interface and because THP had an account that
could be used at no additional cost. This change caused a delay to data collection, but both REBs
(THP and University of Toronto) approved the change.
3.2.3 Web Analytics Strategy
In addition to obtaining direct feedback from participants through surveys and focus groups we
wanted to learn how website visitors navigated the website, which pages were clicked on the
most, how much time was spent on each page, and how much time was spent overall per session.
To capture this, and additional web utilization data we used Google Analytics. We created a
dashboard on Google Analytics to track visitor behaviour on the section of the website under
Page 35 of 128
evaluation (the patient-researcher partnership section), separating out traffic to other sections of
the website.
Since a large portion of the website content was video, we also accessed the YouTube account
where the videos embedded on the website were housed. YouTube provides highly detailed
information about video views, including frequency and timing of views, viewer location, and
referral source. This data would enable us to know which videos were most popular, whether
viewers watched videos in their entirety or only in part, and whether there was a difference in
views of audio-only and video clips. It was later learned that the way most videos were posted on
the website (with autoplay set to ‘on’) caused YouTube not to count their views or track any
statistics. As a result, we could not access reliable data about users’ interaction with video
content on the website.
The focus of our web analytics strategy was user behaviour (i.e., how users navigated the
website) rather than acquisition (i.e., how users got to the website) since at the time of the
evaluation the website was only accessible through a private link and there had been no formal
promotion through social media or otherwise. Therefore, we did not expect organic traffic (e.g.,
via web search) and knew that the only visitors to the website would be those we provided access
to (i.e., participants). We also did not use demographic data, such as age and gender, collected by
Google Analytics because 1) this data was only available for a small percentage of website
visitors, 2) it is unclear how reliable these data are, and 3) we collected demographic information
about participants in our surveys.
3.2.4 Ethical Considerations
Since the evaluation included human subjects, approval from the ethics boards of the institutions
where the research would be conducted was required. The ethical considerations we addressed
included potential conflicts of interest, recruitment methods, possible risks to participants, and
the protection of patients’ confidentiality and privacy.
Only one potential conflict of interest was identified, and that was prior relationships between
potential participants and the study PI (SL). This risk was minimized by clarifying that the
student PI (DP) would extend the invitations to participate.
Page 36 of 128
Ethical considerations related to recruitment were addressed by clarifying our target population
and our intention to include a diverse sample with respect to age, gender, ethnic background,
type of illness, and type/amount of previous engagement or health research experience.
The only potential risk to participants identified was the possibility the focus group participants
would disclose personal health information. This risk was mitigated by the inclusion of a highly
experienced facilitator (SL) who ensured that participants were comfortable and aware of their
rights as study participants, as well as the duty of all focus group participants to respect the
confidentiality of information shared during the session.
Confidentiality and privacy of participant information were protected in multiple ways. First, the
surveys did not request any identifying information (e.g., name, email address, birth date) so
survey responses could not be linked to any individual. A unique identifier was assigned to each
participant in SurveyMonkey (the online survey software used for this study) so that the research
team could link pre and post survey responses without recording identifying information.
Second, identifying participant information that was collected during recruitment (e.g., names,
email addresses) was stored securely on THP’s intranet, separate from survey responses and
other data. Third, after data collection was completed the files containing identifying participant
information linked to unique identifiers were permanently deleted and the email addresses used
to send survey invitations were removed from the SurveyMonkey account.
This evaluation received REB approval from the University of Toronto in September 2019. An
earlier version of the evaluation that only included focus groups had been approved by THP’s
REB as part of the larger research project, but an amendment was needed to approve the changes
made to the design of the evaluation. Approval for the amendment was received in October
2019. A further amendment was required from both REBs in April 2020 when it was learned that
the originally proposed survey software (REDCap) would not enable participants to complete the
surveys at home and we were required to switch to a different software (SurveyMonkey). Both
REBs approved this amendment in April 2020.

Page 37 of 128
3.3 Sampling & Recruitment
For the focus group and survey components of the study we aimed to recruit an equal number of
Canadian health researchers and patients/caregivers (individuals who have current or past lived
experience with, or caring for someone with, illness). We used a combination of convenience,
snowball and purposive maximum variation sampling in order to achieve a diverse sample with
respect to age, gender, ethnic background, type of illness and type/amount of previous
engagement or health research experience (no prior engagement experience was required).
Inclusion criteria for participants included: 1) minimum 18 years of age; 2) able to read and
express themselves in English; 3) able to participate independently in focus groups and/or filling
out surveys; 4) willing to be audio recorded (for focus group participants only) and, 5) have
access to the internet. Exclusion criteria included: 1) unable to communicate in English; and 2)
less than 18 years of age. We recruited health researchers and patients/caregivers to complete the
surveys and participate in focus groups.
With assistance from JV (thesis committee member) and JM, a THP biostatistician, a statistical
power analysis was conducted to estimate the sample size needed for statistical significance.
Assuming a moderate effect size, as recommended by the THP manual,86,87 a minimum of 34-44
participants was required. Our target sample size was 44, so that if some participants were lost to
follow-up our final number would still fall within the required range.
3.3.1 Recruitment Process
Our primary recruitment strategy was to reach out to organizations with existing databases of
patient advisors and/or health researchers and ask them to distribute an invitation to participate to
their membership via electronic mailing list and/or web posting (see Appendix D for list of
organizations we reached out to). We chose to target existing patient advisors in our recruitment
strategy for two reasons: 1) we believed that patients with prior experience with patient
engagement would be more likely to be familiar with patient engagement in research and be
interested in participating in our project, and 2) distributing our invitation through existing
networks enabled a broader reach than what would have been possible if we had built our own
Page 38 of 128
network for the purposes of this project. We included all forms of health researchers (e.g.,
clinical, biomedical, health services) in order to represent a range of researcher perspectives.
We provided organizations that expressed interest in sharing our invitation with details about the
study, including the project title, purpose, inclusion criteria, time commitment, and our contact
information (see Appendix C for sample recruitment email). Interested individuals who received
the invitation through their network were invited to contact us by email indicating their interest.
We informed interested individuals (i.e., those that contacted us by email) that a link to the
surveys and website under evaluation would be sent to them by email. In addition to the strategy
described above, we distributed the invitation among health researchers within the professional
networks of the research team.
Focus Group Recruitment. We contacted two patient and researcher groups to inquire about
group member’s interest in participating in the study by completing online surveys and
participating in a focus group. One group was a hospital-based research and innovation working
group located in Mississauga, whose membership included patient and caregiver advisors. The
other group was a university-based patient engagement working group located in Toronto, whose
membership included patient and caregiver advisors as well as health researchers.
3.4 Data Collection
3.4.1 Consent Process
A separate consent process was used for surveys and focus groups, as ethical considerations were
different for these methods. Participants indicated their consent to participate in each survey by
selecting ‘agree’ on the first page of the survey, which detailed the study, their involvement, and
any risks (see Appendix G for survey consent form). Consent for focus groups was obtained
through email. Participants were sent a copy of the focus group consent form (see Appendix E
for focus group consent form) and given time to read the forms and invited to ask any questions
they had. When they felt comfortable with the information, they could indicate their consent by
email, by signing the consent form and emailing it to us prior to the focus group, or verbally at
the beginning of the focus group after their questions had been answered. All participants were
Page 39 of 128
invited to share questions and concerns about consent at the start of the focus group. Permission
to audio record the session was requested both in the consent form and verbally at the start of the
focus group.
3.4.2 Surveys
Before being introduced to the website, participants were invited by email to complete the first of
two surveys, which included sociodemographic questions, Part 1 of the adapted eHIQ, the TPB
questions, as well as open-ended questions to enable participants to add additional comments and
clarification of their answers. Following the completion of this survey, participants were sent a
link to the website and invited to use the website at their convenience over a period of
approximately one week (participants could request an additional few days if required). A week
after completing the first survey, participants were sent a link to the final survey, which included
Part 2 of the adapted eHIQ, the TPB questions, and open-ended questions to enable participants
to add feedback about the website in their own words (see Appendix G for full surveys). All
surveys were administered online using SurveyMonkey online survey software.
3.4.3 Focus Groups
Focus groups were originally scheduled to take place at IBH and the University of Toronto but
were conducted online via Zoom because of COVID-19 social distancing guidelines. Participants
were contacted by email to ask if they could accommodate this change, and whether they
required any assistance with the videoconferencing technology.
The focus groups lasted one to two hours and took place after participants had completed both
pre and post surveys. This was to ensure that their experience during the focus group did not
influence their survey responses. Focus group discussions were led with the aid of an interview
guide designed according to similar themes as in the surveys. Questions were open-ended and
exploratory to allow for participants to direct the discussion toward what was most important to
them.14,88 The interview guide probed: (i) reactions to the website design and layout, (ii)
reactions to the website content and understanding of the information presented, (iii) perceptions
about the potential usefulness of the website, and (iv) the influence of the website on knowledge,
attitudes and intentions related to patient engagement in research (see Appendix F for interview

Page 40 of 128
guide). The discussion was co-led by an experienced moderator (SL, thesis supervisor) and the
student PI (DP). SL welcomed participants, introduced the discussions, fielded questions about
the consent form, and confirmed consent for audio-recording. DP provided details about the
study and led the discussion about the website, which included asking questions from the
interview guide and probing on topics brought up by participants during the discussions.14,88
At the end of the focus group participants were offered a small honorarium for their time. Since
the focus groups took place online and participants joined from home, no travel or parking costs
were incurred.
3.4.4 Web Analytics
No specific action was required to collect web utilization data since Google Analytics
automatically tracks user behaviour.
3.5 Data Analysis
3.5.1 Survey Data
Survey data was exported directly from SurveyMonkey into Microsoft Excel. All responses from
both surveys (which contained no identifying information) were compiled into a single
spreadsheet with a row for each respondent and a column for each survey item. Each participant
was assigned a unique identifier that included a number and ‘P’ for patients and caregivers, “R’
for researchers, ‘B’ for those who identified as both, and “O” for others (e.g., research staff).
Participants who identified as both were grouped into either ‘P’ or ‘R’ for the quantitative
analyses, based on which group they chose to identify as for the evaluation. Unique codes were
also created for each survey item. We linked each participants’ responses to Survey 1 and 2
using a unique identifier in SurveyMonkey. This made it possible to protect the privacy of
respondents by separating all identifiers (e.g., email addresses, IP addresses) from survey
responses while enabling us to link pre and post answers.
After importing into Excel, DP checked the data for missing, unusual, or inconsistent responses
(e.g., responses outside of the Likert response range or conflicting responses to similar questions
Page 41 of 128
by the same respondent). Open-ended responses were moved into a separate document, which
was sorted by survey question and each response was recorded verbatim alongside the
respondent’s unique identifier. To facilitate statistical analysis, all responses to Likert-type
questions and a selection of demographic information for stratification (i.e., role in partnership)
were copied from the spreadsheet containing all responses into a separate spreadsheet.
Statistical analysis was conducted in MS Excel and RStudio by DP, with guidance from JV and
JM, a Trillium Health Partner’s biostatistician. Individual survey responses from the adapted
eHIQ and TPB tool were grouped according to their source literature.81,86 The score for each
eHIQ subscale was calculated using the scoring algorithm used by the original authors, which
transforms the score to a 0-100 metric (where 0 indicates low perceived value and 100 indicated
high perceived value).81 Cronbach’s Alpha tests were run for all five sections of the adapted
eHIQ to find if adaptations to the survey tool reduced internal consistency of responses within
each grouping. A score of 0.70 or higher was considered acceptable (see Table 1 and Table 4 for
scores).
While the eHIQ has been formally validated81 conducting a test for internal consistency was
required to ensure that our revisions to the wording of questions and omissions of some
questions did not result in poor correlations. More robust forms of validation (e.g., factor
analysis) were determined not to be feasible for this study due to time constraints and our small
sample size. The four groupings of the TPB were organized according to the design manual86
with the score for each group defined as the average of per-item scores (see Appendix B, Table
12 for TPB items by domain).
Individual scores from the TPB survey tool were evaluated to determine changes before and after
interaction with the website using Wilcoxon Signed Rank tests. Mann-Whitney U tests were used
to compare differences in responses between groups (i.e., patients and researchers) for both eHIQ
and TPB data.89 These non-parametric tests were chosen because our sample size was small and
our data were not normally distributed, which made it unsuitable for parametric tests.
Demographic variables and responses to individual survey items were presented in counts and
percentages. Means and standard deviations were calculated for survey domains/subscales (e.g.,
Page 42 of 128
behavioural intention, attitudes). An alpha level of 0.05 was used to assess significance for the
pre-post analysis and between group comparisons.
3.5.2 Qualitative Data
Audio recordings from focus groups were transcribed verbatim (by DP) but excluded utterances
that did not contribute to the topic (e.g., ‘um,’ ‘uh’).90 Responses to open-ended survey questions
were compiled into a word document and sorted by question and type of participant (i.e.,
patient/caregiver, researcher, or other). To develop a detailed understanding of the information
provided by focus group participants we conducted a hybrid content analysis of the focus group
data,88 informed inductively and deductively by themes from the interview guides as well as
themes that emerged during the focus groups.
Analysis of data from the focus groups followed Braun and Clarke’s six step method.91 Before
coding began, DP checked the transcripts for accuracy and re-read to increase familiarity.91
Initial codes (i.e., recurrent topics or ideas) were created by DP to systematically categorize the
content.91 A separate document was created by DP with each code as a heading and data from
transcripts were copied into the document under the relevant code, alongside the participant’s
unique identifier. This was an iterative process that involved multiple readings of the transcripts.
After the initial codes were created, they were collated into categories (i.e., topics of discussion,
e.g., the website’s navigation) and a codebook was created. The codebook identified each
category and its codes and included a short definition of each code. Next, SL (who co-facilitated
the focus groups) and KK (thesis committee member) reviewed the codebook created by DP to
ensure accuracy and completeness. Using feedback from SL and KK, DP revised the coding
framework to include additional codes and created a concept map to explore relationships
between codes. The codes were then arranged into themes (i.e., meanings derived from the text),
which were reviewed again by KK and SL. Once agreement about the themes was reached, DP
wrote summaries of each theme, including selected quotes.
Responses to open-ended survey questions were analyzed separately and presented alongside the
quantitative survey findings to add context and explanation for the quantitative survey findings.
Page 43 of 128
3.5.3 Web Analytics
Website analytics data was exported from Google Analytics to MS Excel. We only analyzed data
collected within the evaluation period, defined as the period between the date the first participant
was given access to the website and the date when the final participant completed the final
survey. The exported data included the number and type (i.e., new or unique) of users, number
and average length of sessions, number and types of pages viewed, average length of time spent
on each page, number of pages viewed per day, and device types (desktop, mobile, or tablet).
Page view data was then organized by type of page (e.g., topic) and ordered by number of views
per page to show the most and least popular content within each category. A timeline was
created to illustrate daily page views over time (including the two weeks before and two weeks
after the evaluation period for context).
3.5.4 Integration & Interpretation
After analyzing the quantitative and qualitative data separately, the findings derived from each
analysis were compared to uncover divergence and convergence. This integrative technique is
one of four integrative processes identified by Creswell and Plano Clark (2011),11 in which only
findings are merged, not the data itself.92 The study was designed so that both components of the
research question (impact and overall impression of the website) were probed using both
quantitative and qualitative methods: impact was measured quantitatively through the pre-post
analysis of participants’ attitudes and intentions related to research partnerships, and qualitatively
through the inclusion of open-ended questions that asked directly about participants’ perceptions
of the website’s impact, and; overall impression was measured quantitatively through the eHIQ
survey questions, and qualitatively through open-ended survey questions and the focus groups.
By including this duplication, we aimed to gain a fuller and more accurate understanding of
participants’ overall perception of the website and its impact. Furthermore, duplication enabled
both qualitative and quantitative answers to the research question, which could then be compared
and contrasted to uncover complementarity and/or conflict among them.
Some integration also occurred during the writing phase, which involved transformation of
qualitative data from open-ended survey questions into quantitative data (“quantitizing”)93 to

Page 44 of 128
facilitate the creation of mixed data tables. The tables included direct quotes from participants
(qualitative data) as well as counts (quantitative data) that represented the proportion of
participants who gave a similar kind of response (e.g. agreed with a statement) or referred to a
similar topic in their answer.
3.6 Dissemination Plan
Upon completion of the research a mixed methods paper will be prepared for publication in an
academic journal (e.g., Patient Experience Journal), as well as a slide-deck and/or poster for
presentation at an academic conference (e.g., CAHSPR Academic Conference). These materials
will include a joint display of quantitative and qualitative findings to showcase convergent
and/or divergent results and illustrate the benefits of applying a mixed methods approach.
A plain language summary of the results will be created and disseminated to the advisory group
for the overarching study and the evaluation participants who indicated interest in seeing the
results. It will also be made available on the website (healthexperiences.ca). We will also reach
out to other teams that have developed or are developing resources for patient engagement in
research to inform them of our findings, refer them to the webpage where the evaluation findings
are summarized and extend an open invitation for further discussion or collaboration.
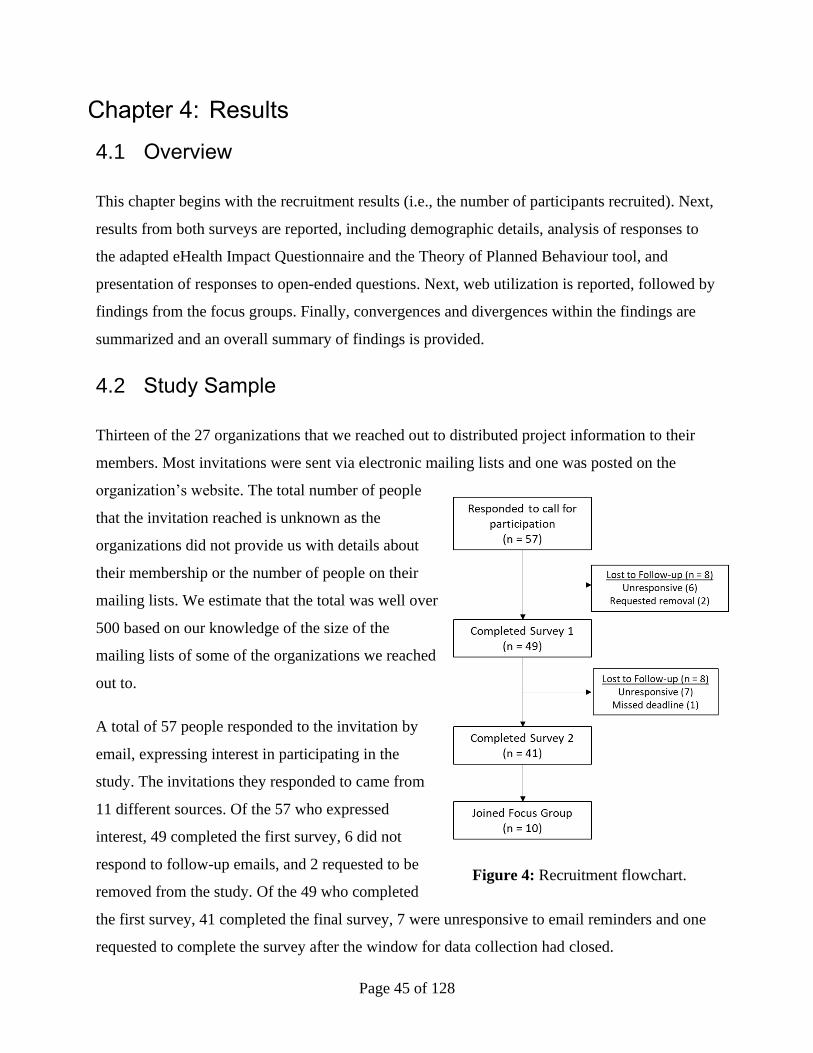
Page 45 of 128
Results
4.1 Overview
This chapter begins with the recruitment results (i.e., the number of participants recruited). Next,
results from both surveys are reported, including demographic details, analysis of responses to
the adapted eHealth Impact Questionnaire and the Theory of Planned Behaviour tool, and
presentation of responses to open-ended questions. Next, web utilization is reported, followed by
findings from the focus groups. Finally, convergences and divergences within the findings are
summarized and an overall summary of findings is provided.
4.2 Study Sample
Thirteen of the 27 organizations that we reached out to distributed project information to their
members. Most invitations were sent via electronic mailing lists and one was posted on the
organization’s website. The total number of people
that the invitation reached is unknown as the
organizations did not provide us with details about
their membership or the number of people on their
mailing lists. We estimate that the total was well over
500 based on our knowledge of the size of the
mailing lists of some of the organizations we reached
out to.
A total of 57 people responded to the invitation by
email, expressing interest in participating in the
study. The invitations they responded to came from
11 different sources. Of the 57 who expressed
interest, 49 completed the first survey, 6 did not
respond to follow-up emails, and 2 requested to be
removed from the study. Of the 49 who completed
the first survey, 41 completed the final survey, 7 were unresponsive to email reminders and one
requested to complete the survey after the window for data collection had closed.
Figure 4: Recruitment flowchart.
Page 46 of 128
Of the 41 who completed both surveys, 11 agreed to also participate in a focus group (one later
opted out). Two focus groups were held with five participants attending each.
4.3 Survey 1 Findings: Baseline Characteristics
4.3.1 Participant Characteristics
Demographic details were collected in the first survey, so we obtained participant characteristics
from all 49 participants who completed the first survey. The largest proportion of respondents
were patients or caregivers (51%), followed by researchers (39%), and research staff (e.g.,
patient engagement coordinator) (10%). Five participants indicated that they had experience both
as a researcher and as a patient or caregiver – three chose to take the perspective of a patient for
the purposes of this study and two chose a researcher perspective.
A large proportion of participants held postgraduate degrees (73%), were born in Canada (69%),
were female (67%), resided in Ontario (65%), were over the age of 54 (53%), and held full-time
employment (47%). Many had experience as a patient or researcher partner in three or more
projects (43%), while less than half had received formal training related to research partnerships
(37%). Of the 19 researchers, 11 identified as health services researchers.
Patient participants differed from researcher participants in age and employment status, as most
patients were 65+ (56%) and retired (52%), while almost no researchers identified as 65+ (5%)
or retired (5%). Patients and caregivers had experience with a wide range of health conditions
including cancer, diabetes, mental health conditions, dementia, allergies, osteoarthritis, chronic
pain, fibromyalgia, respiratory illness, kidney disease, and spina bifida. See Appendix H for full
demographic details.
4.3.2 Adapted eHIQ Part 1
Prior to being given access to the website, participants answered survey questions about their
attitudes toward online information about patient-researcher partnerships and the value of
experience-based information related to partnerships. Measuring these attitudes before
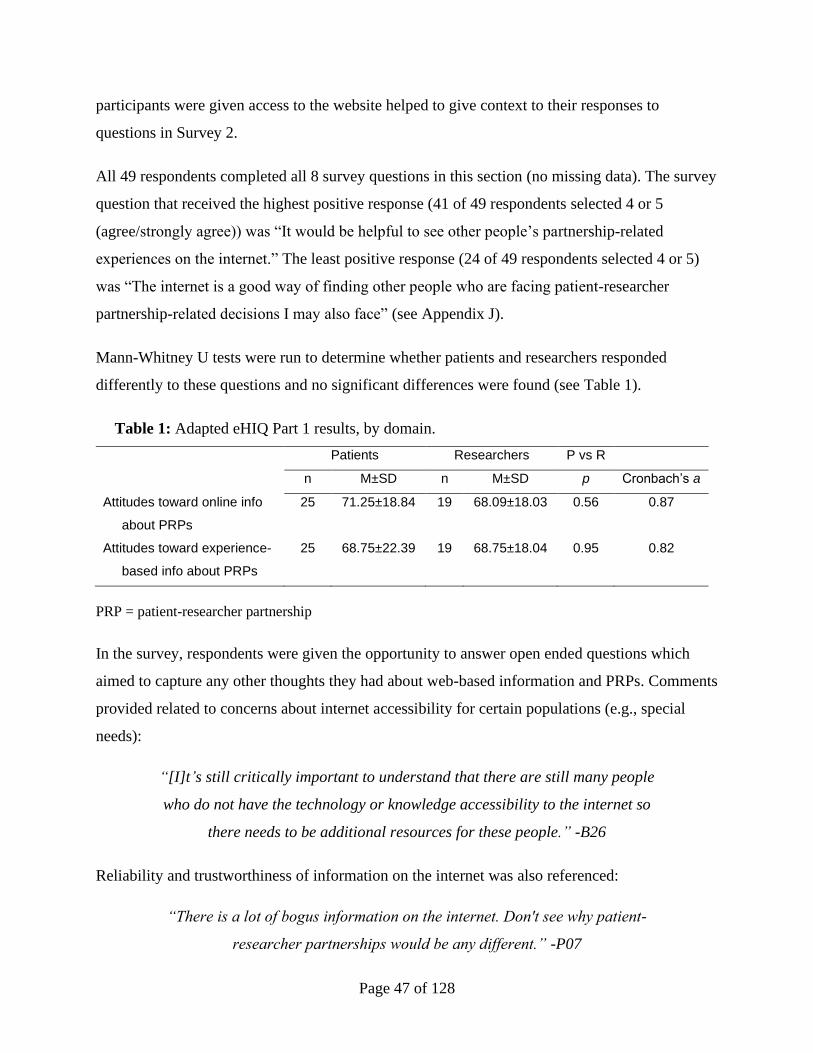
Page 47 of 128
participants were given access to the website helped to give context to their responses to
questions in Survey 2.
All 49 respondents completed all 8 survey questions in this section (no missing data). The survey
question that received the highest positive response (41 of 49 respondents selected 4 or 5
(agree/strongly agree)) was “It would be helpful to see other people’s partnership-related
experiences on the internet.” The least positive response (24 of 49 respondents selected 4 or 5)
was “The internet is a good way of finding other people who are facing patient-researcher
partnership-related decisions I may also face” (see Appendix J).
Mann-Whitney U tests were run to determine whether patients and researchers responded
differently to these questions and no significant differences were found (see Table 1).
Table 1: Adapted eHIQ Part 1 results, by domain.
Patients Researchers P vs R
n M±SD n M±SD p Cronbach’s a
Attitudes toward online info
about PRPs
25 71.25±18.84 19 68.09±18.03 0.56 0.87
Attitudes toward experience-
based info about PRPs
25 68.75±22.39 19 68.75±18.04 0.95 0.82
PRP = patient-researcher partnership
In the survey, respondents were given the opportunity to answer open ended questions which
aimed to capture any other thoughts they had about web-based information and PRPs. Comments
provided related to concerns about internet accessibility for certain populations (e.g., special
needs):
“[I]t’s still critically important to understand that there are still many people
who do not have the technology or knowledge accessibility to the internet so
there needs to be additional resources for these people.” -B26
Reliability and trustworthiness of information on the internet was also referenced:
“There is a lot of bogus information on the internet. Don't see why patient-
researcher partnerships would be any different.” -P07
Page 48 of 128
“The tool (internet) is great. The trustworthiness of its content is not.” -O31
Some expressed preference for in-person conversation as a source of information:
“The Internet is a good place to start but talking to people is much better for
the feeling of what researchers and patients can have in common.” -P32
Others noted the difficulty of portraying the complexity and context-dependant nature of
partnerships online:
“Its a great starting point, but not sure one can understand the complexities
involved without actually doing it!” -R35
“The internet can be helpful, but most patient-researcher partnerships are so
unique that it can be hard to draw on others experience.” -R03
4.3.3 Theory of Planned Behaviour at Baseline
The first survey also contained the TPB questions. Measuring participants’ attitudes, intentions,
subjective norms, and perceived behavioural control related to PRPs at baseline served two
purposes: 1) to enable a comparison between responses before and after visiting the website, and
2) to provide a deeper understanding of the participants recruited for this study, which informed
the interpretation of our findings.
All 49 participants responded to the TPB questions. Overall, only 2 of 588 possible responses
(49 participants x 12 survey items) were missing – a >99.9% response rate.
Results from the TPB tool measured at baseline showed high levels of intention to engage in
partnerships and positive attitudes about partnerships among both patients and researchers. The
median response to both intention questions (“I want to engage in PRPs” and “I intend to engage
in PRPs”) was 7, which is the highest level of agreement allowed on the 7-point scale.
Researchers reported feeling a higher degree of pressure from their peers (‘Subjective Norms’) to
engage in partnerships than patients (p = <0.01). Also, patients felt a moderately higher degree of
control over their decisions (‘Perceived Behavioural Control’) about whether to engage in
partnerships than researchers (p = 0.04) (see Table 2).
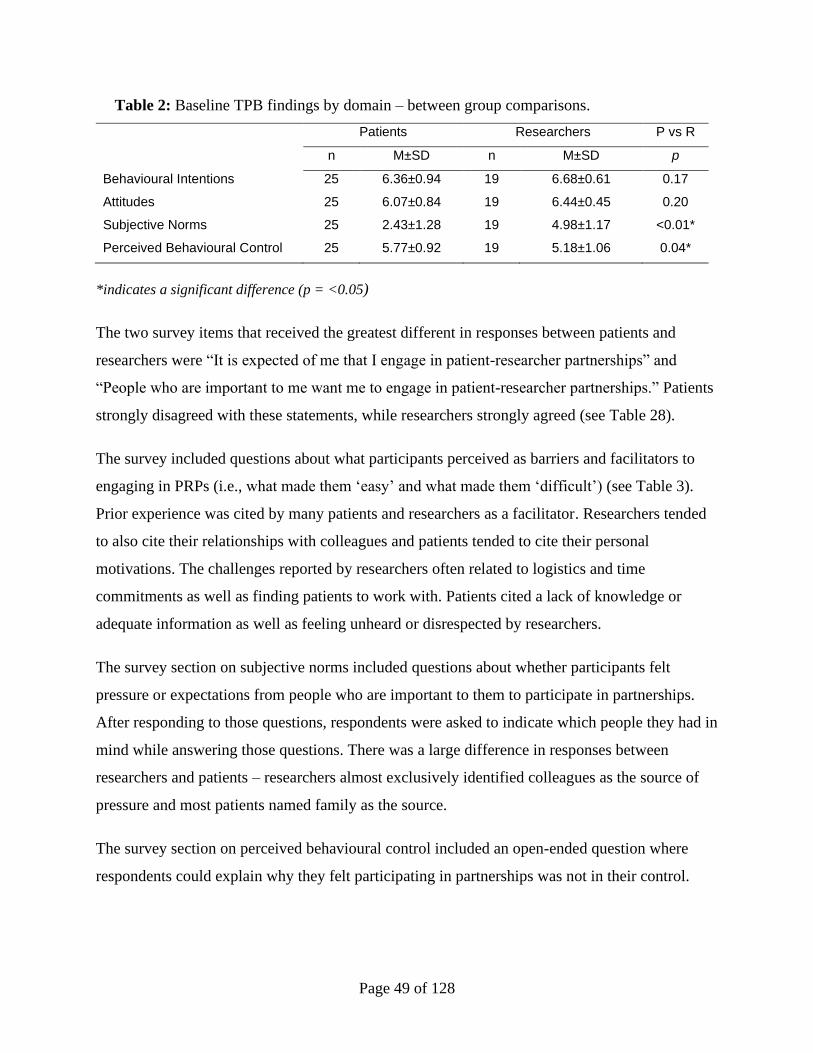
Page 49 of 128
Table 2: Baseline TPB findings by domain – between group comparisons.
Patients Researchers P vs R
n M±SD n M±SD p
Behavioural Intentions 25 6.36±0.94 19 6.68±0.61 0.17
Attitudes 25 6.07±0.84 19 6.44±0.45 0.20
Subjective Norms 25 2.43±1.28 19 4.98±1.17 <0.01*
Perceived Behavioural Control 25 5.77±0.92 19 5.18±1.06 0.04*
*indicates a significant difference (p = <0.05)
The two survey items that received the greatest different in responses between patients and
researchers were “It is expected of me that I engage in patient-researcher partnerships” and
“People who are important to me want me to engage in patient-researcher partnerships.” Patients
strongly disagreed with these statements, while researchers strongly agreed (see Table 28).
The survey included questions about what participants perceived as barriers and facilitators to
engaging in PRPs (i.e., what made them ‘easy’ and what made them ‘difficult’) (see Table 3).
Prior experience was cited by many patients and researchers as a facilitator. Researchers tended
to also cite their relationships with colleagues and patients tended to cite their personal
motivations. The challenges reported by researchers often related to logistics and time
commitments as well as finding patients to work with. Patients cited a lack of knowledge or
adequate information as well as feeling unheard or disrespected by researchers.
The survey section on subjective norms included questions about whether participants felt
pressure or expectations from people who are important to them to participate in partnerships.
After responding to those questions, respondents were asked to indicate which people they had in
mind while answering those questions. There was a large difference in responses between
researchers and patients – researchers almost exclusively identified colleagues as the source of
pressure and most patients named family as the source.
The survey section on perceived behavioural control included an open-ended question where
respondents could explain why they felt participating in partnerships was not in their control.
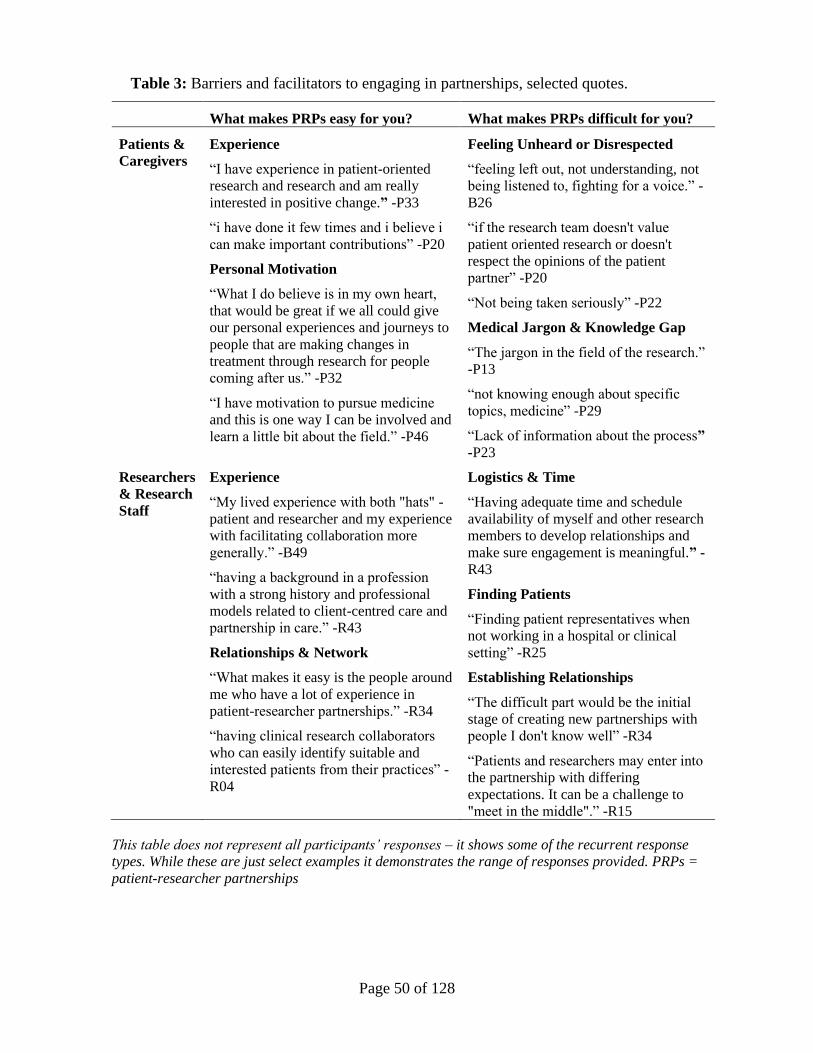
Page 50 of 128
Table 3: Barriers and facilitators to engaging in partnerships, selected quotes.
What makes PRPs easy for you? What makes PRPs difficult for you?
Patients &
Caregivers
Experience
“I have experience in patient-oriented
research and research and am really
interested in positive change.” -P33
“i have done it few times and i believe i
can make important contributions” -P20
Personal Motivation
“What I do believe is in my own heart,
that would be great if we all could give
our personal experiences and journeys to
people that are making changes in
treatment through research for people
coming after us.” -P32
“I have motivation to pursue medicine
and this is one way I can be involved and
learn a little bit about the field.” -P46
Feeling Unheard or Disrespected
“feeling left out, not understanding, not
being listened to, fighting for a voice.” -
B26
“if the research team doesn't value
patient oriented research or doesn't
respect the opinions of the patient
partner” -P20
“Not being taken seriously” -P22
Medical Jargon & Knowledge Gap
“The jargon in the field of the research.”
-P13
“not knowing enough about specific
topics, medicine” -P29
“Lack of information about the process”
-P23
Researchers
& Research
Staff
Experience
“My lived experience with both "hats" -
patient and researcher and my experience
with facilitating collaboration more
generally.” -B49
“having a background in a profession
with a strong history and professional
models related to client-centred care and
partnership in care.” -R43
Relationships & Network
“What makes it easy is the people around
me who have a lot of experience in
patient-researcher partnerships.” -R34
“having clinical research collaborators
who can easily identify suitable and
interested patients from their practices” -
R04
Logistics & Time
“Having adequate time and schedule
availability of myself and other research
members to develop relationships and
make sure engagement is meaningful.” -
R43
Finding Patients
“Finding patient representatives when
not working in a hospital or clinical
setting” -R25
Establishing Relationships
“The difficult part would be the initial
stage of creating new partnerships with
people I don't know well” -R34
“Patients and researchers may enter into
the partnership with differing
expectations. It can be a challenge to
"meet in the middle".” -R15
This table does not represent all participants’ responses – it shows some of the recurrent response
types. While these are just select examples it demonstrates the range of responses provided. PRPs =
patient-researcher partnerships
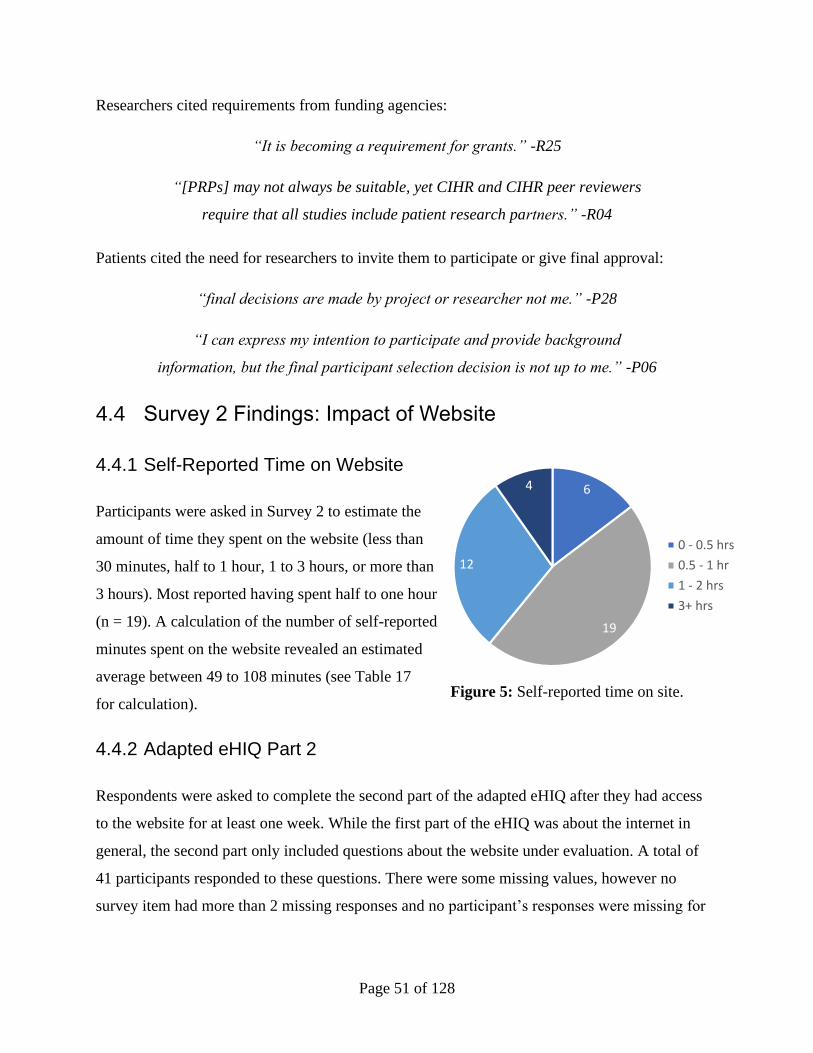
Page 51 of 128
Researchers cited requirements from funding agencies:
“It is becoming a requirement for grants.” -R25
“[PRPs] may not always be suitable, yet CIHR and CIHR peer reviewers
require that all studies include patient research partners.” -R04
Patients cited the need for researchers to invite them to participate or give final approval:
“final decisions are made by project or researcher not me.” -P28
“I can express my intention to participate and provide background
information, but the final participant selection decision is not up to me.” -P06
4.4 Survey 2 Findings: Impact of Website
4.4.1 Self-Reported Time on Website
Participants were asked in Survey 2 to estimate the
amount of time they spent on the website (less than
30 minutes, half to 1 hour, 1 to 3 hours, or more than
3 hours). Most reported having spent half to one hour
(n = 19). A calculation of the number of self-reported
minutes spent on the website revealed an estimated
average between 49 to 108 minutes (see Table 17
for calculation).
4.4.2 Adapted eHIQ Part 2
Respondents were asked to complete the second part of the adapted eHIQ after they had access
to the website for at least one week. While the first part of the eHIQ was about the internet in
general, the second part only included questions about the website under evaluation. A total of
41 participants responded to these questions. There were some missing values, however no
survey item had more than 2 missing responses and no participant’s responses were missing for
6
19
12
4
0 - 0.5 hrs
0.5 - 1 hr
1 - 2 hrs
3+ hrs
Figure 5: Self-reported time on site.
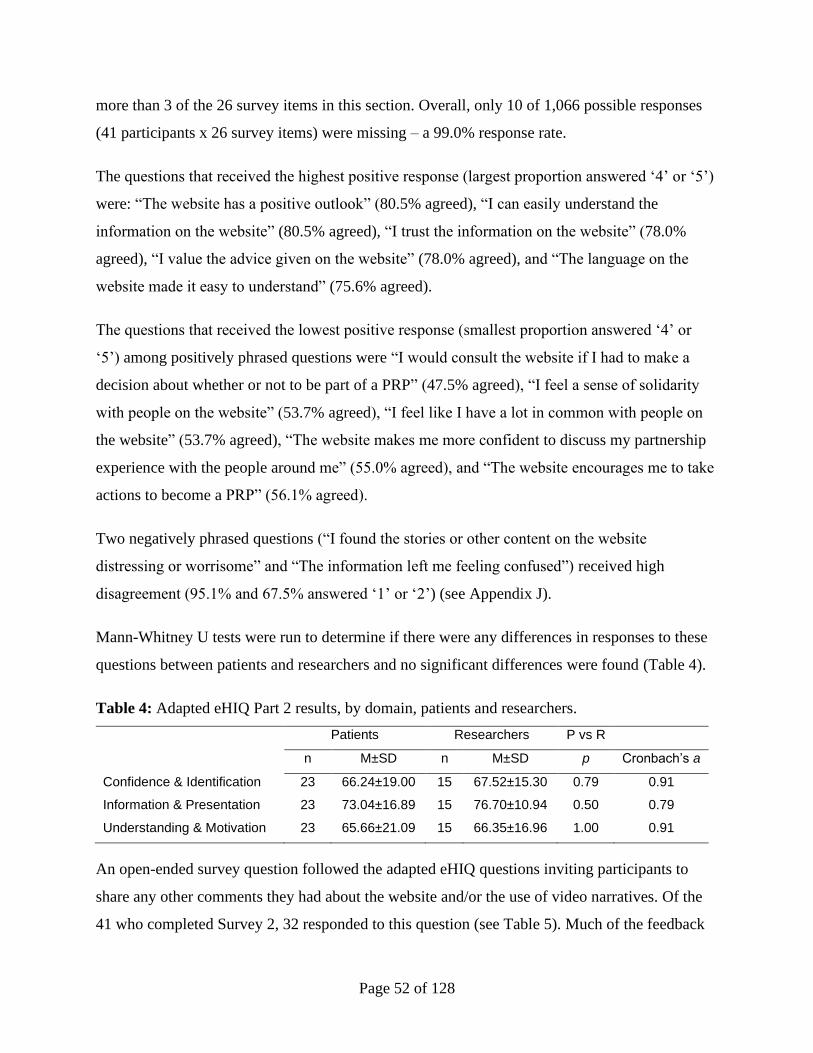
Page 52 of 128
more than 3 of the 26 survey items in this section. Overall, only 10 of 1,066 possible responses
(41 participants x 26 survey items) were missing – a 99.0% response rate.
The questions that received the highest positive response (largest proportion answered ‘4’ or ‘5’)
were: “The website has a positive outlook” (80.5% agreed), “I can easily understand the
information on the website” (80.5% agreed), “I trust the information on the website” (78.0%
agreed), “I value the advice given on the website” (78.0% agreed), and “The language on the
website made it easy to understand” (75.6% agreed).
The questions that received the lowest positive response (smallest proportion answered ‘4’ or
‘5’) among positively phrased questions were “I would consult the website if I had to make a
decision about whether or not to be part of a PRP” (47.5% agreed), “I feel a sense of solidarity
with people on the website” (53.7% agreed), “I feel like I have a lot in common with people on
the website” (53.7% agreed), “The website makes me more confident to discuss my partnership
experience with the people around me” (55.0% agreed), and “The website encourages me to take
actions to become a PRP” (56.1% agreed).
Two negatively phrased questions (“I found the stories or other content on the website
distressing or worrisome” and “The information left me feeling confused”) received high
disagreement (95.1% and 67.5% answered ‘1’ or ‘2’) (see Appendix J).
Mann-Whitney U tests were run to determine if there were any differences in responses to these
questions between patients and researchers and no significant differences were found (Table 4).
Table 4: Adapted eHIQ Part 2 results, by domain, patients and researchers.
Patients Researchers P vs R
n M±SD n M±SD p Cronbach’s a
Confidence & Identification 23 66.24±19.00 15 67.52±15.30 0.79 0.91
Information & Presentation 23 73.04±16.89 15 76.70±10.94 0.50 0.79
Understanding & Motivation 23 65.66±21.09 15 66.35±16.96 1.00 0.91
An open-ended survey question followed the adapted eHIQ questions inviting participants to
share any other comments they had about the website and/or the use of video narratives. Of the
41 who completed Survey 2, 32 responded to this question (see Table 5). Much of the feedback
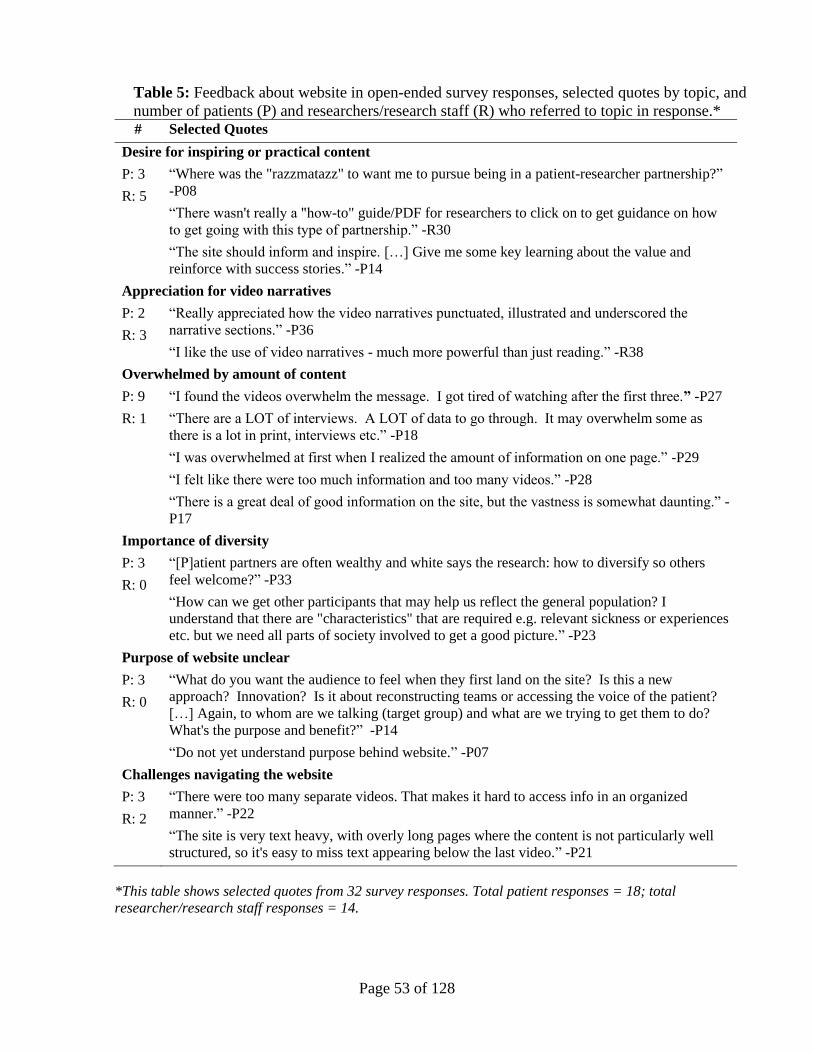
Page 53 of 128
Table 5: Feedback about website in open-ended survey responses, selected quotes by topic, and
number of patients (P) and researchers/research staff (R) who referred to topic in response.* # Selected Quotes
Desire for inspiring or practical content
P: 3
R: 5
“Where was the "razzmatazz" to want me to pursue being in a patient-researcher partnership?”
-P08
“There wasn't really a "how-to" guide/PDF for researchers to click on to get guidance on how
to get going with this type of partnership.” -R30
“The site should inform and inspire. […] Give me some key learning about the value and
reinforce with success stories.” -P14
Appreciation for video narratives
P: 2
R: 3
“Really appreciated how the video narratives punctuated, illustrated and underscored the
narrative sections.” -P36
“I like the use of video narratives - much more powerful than just reading.” -R38
Overwhelmed by amount of content
P: 9
R: 1
“I found the videos overwhelm the message. I got tired of watching after the first three.” -P27
“There are a LOT of interviews. A LOT of data to go through. It may overwhelm some as
there is a lot in print, interviews etc.” -P18
“I was overwhelmed at first when I realized the amount of information on one page.” -P29
“I felt like there were too much information and too many videos.” -P28
“There is a great deal of good information on the site, but the vastness is somewhat daunting.” -
P17
Importance of diversity
P: 3
R: 0
“[P]atient partners are often wealthy and white says the research: how to diversify so others
feel welcome?” -P33
“How can we get other participants that may help us reflect the general population? I
understand that there are "characteristics" that are required e.g. relevant sickness or experiences
etc. but we need all parts of society involved to get a good picture.” -P23
Purpose of website unclear
P: 3
R: 0
“What do you want the audience to feel when they first land on the site? Is this a new
approach? Innovation? Is it about reconstructing teams or accessing the voice of the patient?
[…] Again, to whom are we talking (target group) and what are we trying to get them to do?
What's the purpose and benefit?” -P14
“Do not yet understand purpose behind website.” -P07
Challenges navigating the website
P: 3
R: 2
“There were too many separate videos. That makes it hard to access info in an organized
manner.” -P22
“The site is very text heavy, with overly long pages where the content is not particularly well
structured, so it's easy to miss text appearing below the last video.” -P21
*This table shows selected quotes from 32 survey responses. Total patient responses = 18; total
researcher/research staff responses = 14.

Page 54 of 128
related to the design and layout of the website as well as the amount of content. Feedback about
the video content was mixed, with some stating that it was engaging and helpful, and others
expressing dissatisfaction with the way the videos were presented. Of the 18 patients who
responded to the survey prompt, 9 characterized the amount of content (e.g., number of videos,
length of pages, amount of text) as excessive or overwhelming. Of the 12 researchers who
responded to the survey prompt, five expressed desire for a form of summarized content (e.g.,
checklists, how-to guide, highlighted main points of videos). A few patients (n=3) referenced
diversity among patient partners in research as a point of concern and something they wished to
see represented more on the website and in practise. Other topics that were brought up by
participants include appreciation for video narratives, lack of clarity about the website’s purpose,
and challenges navigating the website.
4.4.3 Theory of Planned Behaviour Post-Intervention
The same TPB questions that were asked in the first survey were asked again in the second
survey. This was to detect if spending time on the website changed how participants responded
to these questions. Forty-one participants responded to these questions. There were some missing
values, but no survey item had more than 2 missing responses and no participant’s responses
were missing for more than one of the 12 survey items in this section. Overall, only 2 of 492
possible responses (41 participants x 12 survey items) were missing – a >99.9% response rate.
Wilcoxon signed rank tests were conducted to measure differences in pre and post responses to
TPB questions among patients and researchers. No significant differences were found between
pre and post responses for subjective norms or perceived behavioural control. Some significant
differences were found for intentions to participate in research partnerships and attitudes toward
them. A slight decrease in intention was observed among patients (p=0.01). A slight decrease in
attitudes was observed among researchers (p=0.02), but not among patients (see Table 6).
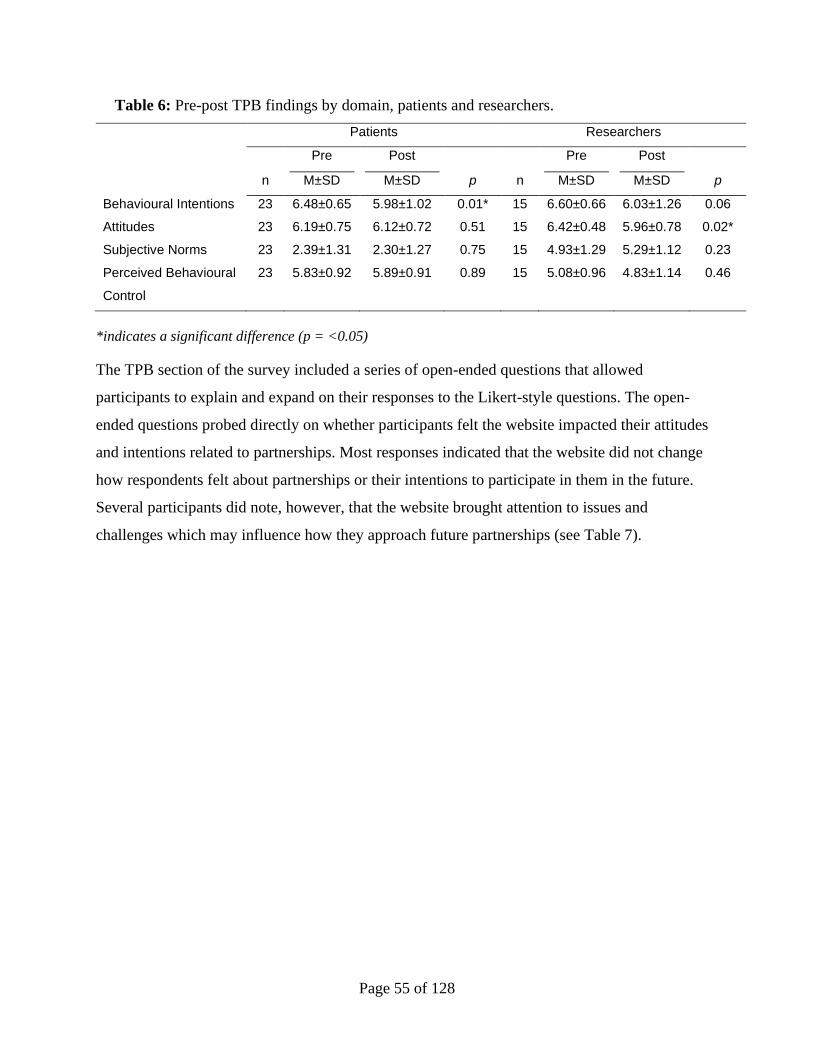
Page 55 of 128
Table 6: Pre-post TPB findings by domain, patients and researchers.
Patients Researchers
n
Pre
M±SD
Post
M±SD p n
Pre
M±SD
Post
M±SD p
Behavioural Intentions 23 6.48±0.65 5.98±1.02 0.01* 15 6.60±0.66 6.03±1.26 0.06
Attitudes 23 6.19±0.75 6.12±0.72 0.51 15 6.42±0.48 5.96±0.78 0.02*
Subjective Norms 23 2.39±1.31 2.30±1.27 0.75 15 4.93±1.29 5.29±1.12 0.23
Perceived Behavioural
Control
23 5.83±0.92 5.89±0.91 0.89 15 5.08±0.96 4.83±1.14 0.46
*indicates a significant difference (p = <0.05)
The TPB section of the survey included a series of open-ended questions that allowed
participants to explain and expand on their responses to the Likert-style questions. The open-
ended questions probed directly on whether participants felt the website impacted their attitudes
and intentions related to partnerships. Most responses indicated that the website did not change
how respondents felt about partnerships or their intentions to participate in them in the future.
Several participants did note, however, that the website brought attention to issues and
challenges which may influence how they approach future partnerships (see Table 7).
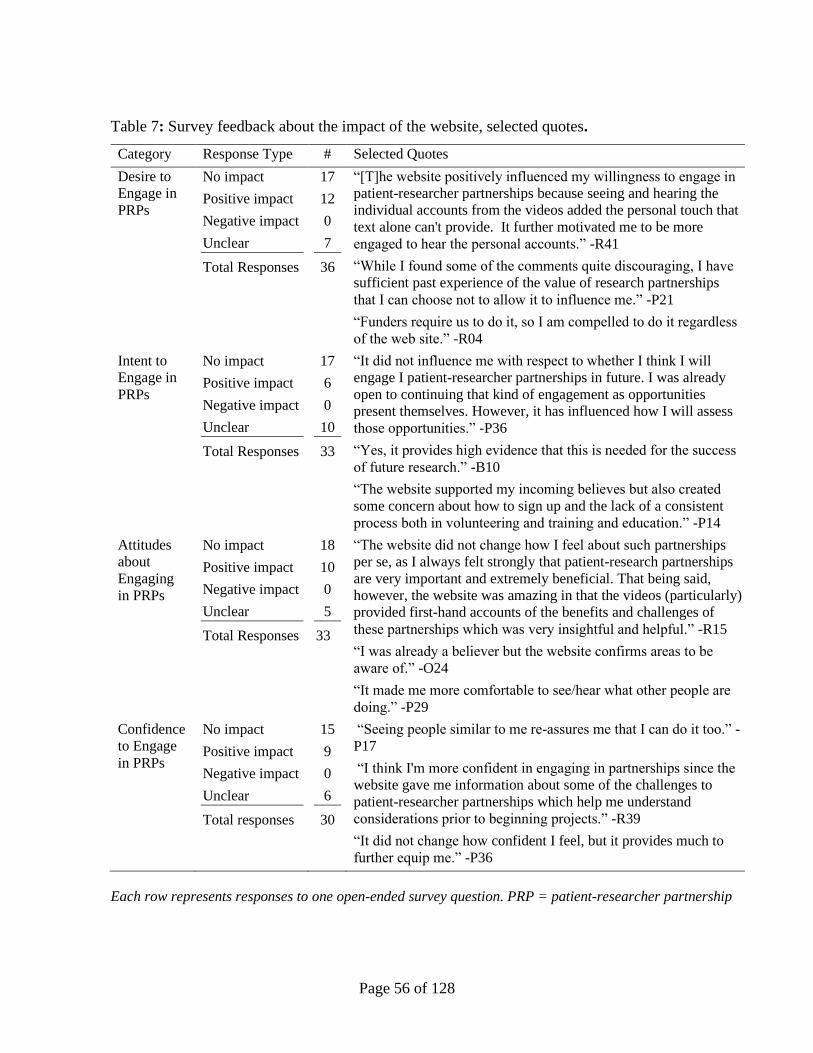
Page 56 of 128
Table 7: Survey feedback about the impact of the website, selected quotes.
Category Response Type # Selected Quotes
Desire to
Engage in
PRPs
No impact
Positive impact
Negative impact
Unclear
Total Responses
17
12
0
7
36
“[T]he website positively influenced my willingness to engage in
patient-researcher partnerships because seeing and hearing the
individual accounts from the videos added the personal touch that
text alone can't provide. It further motivated me to be more
engaged to hear the personal accounts.” -R41
“While I found some of the comments quite discouraging, I have
sufficient past experience of the value of research partnerships
that I can choose not to allow it to influence me.” -P21
“Funders require us to do it, so I am compelled to do it regardless
of the web site.” -R04
Intent to
Engage in
PRPs
No impact
Positive impact
Negative impact
Unclear
Total Responses
17
6
0
10
33
“It did not influence me with respect to whether I think I will
engage I patient-researcher partnerships in future. I was already
open to continuing that kind of engagement as opportunities
present themselves. However, it has influenced how I will assess
those opportunities.” -P36
“Yes, it provides high evidence that this is needed for the success
of future research.” -B10
“The website supported my incoming believes but also created
some concern about how to sign up and the lack of a consistent
process both in volunteering and training and education.” -P14
Attitudes
about
Engaging
in PRPs
No impact
Positive impact
Negative impact
Unclear
Total Responses
18
10
0
5
33
“The website did not change how I feel about such partnerships
per se, as I always felt strongly that patient-research partnerships
are very important and extremely beneficial. That being said,
however, the website was amazing in that the videos (particularly)
provided first-hand accounts of the benefits and challenges of
these partnerships which was very insightful and helpful.” -R15
“I was already a believer but the website confirms areas to be
aware of.” -O24
“It made me more comfortable to see/hear what other people are
doing.” -P29
Confidence
to Engage
in PRPs
No impact
Positive impact
Negative impact
Unclear
Total responses
15
9
0
6
30
“Seeing people similar to me re-assures me that I can do it too.” -
P17
“I think I'm more confident in engaging in partnerships since the
website gave me information about some of the challenges to
patient-researcher partnerships which help me understand
considerations prior to beginning projects.” -R39
“It did not change how confident I feel, but it provides much to
further equip me.” -P36
Each row represents responses to one open-ended survey question. PRP = patient-researcher partnership
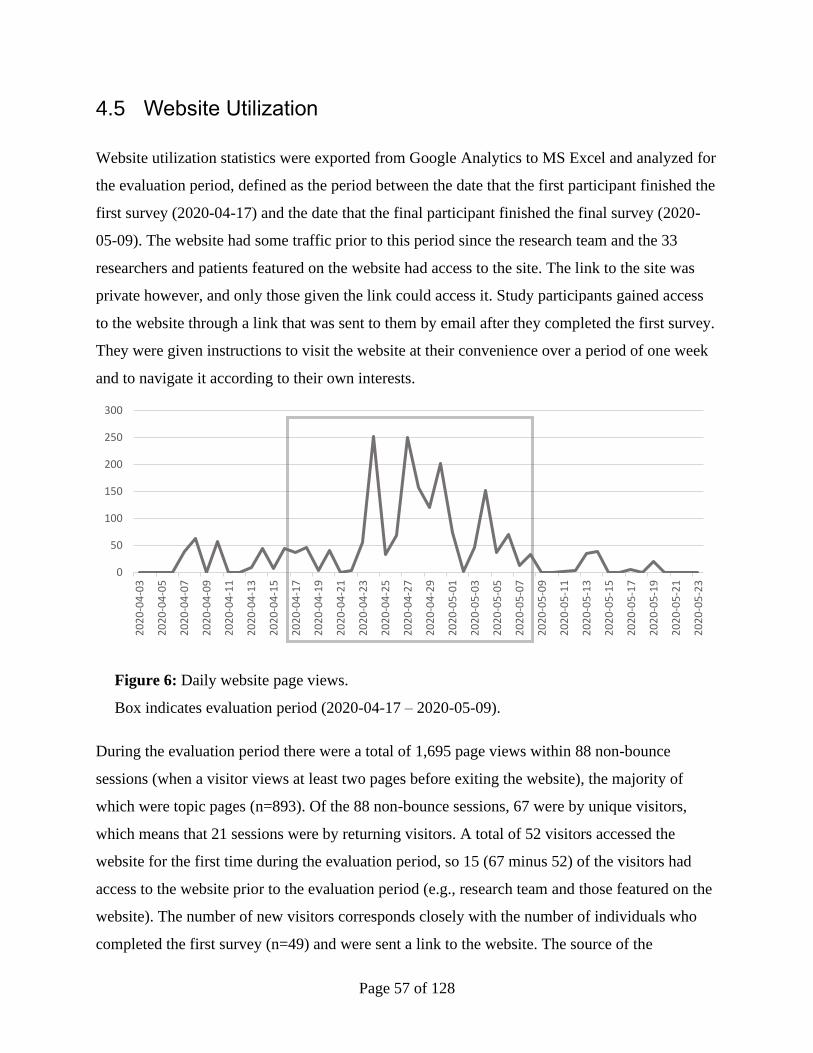
Page 57 of 128
4.5 Website Utilization
Website utilization statistics were exported from Google Analytics to MS Excel and analyzed for
the evaluation period, defined as the period between the date that the first participant finished the
first survey (2020-04-17) and the date that the final participant finished the final survey (2020-
05-09). The website had some traffic prior to this period since the research team and the 33
researchers and patients featured on the website had access to the site. The link to the site was
private however, and only those given the link could access it. Study participants gained access
to the website through a link that was sent to them by email after they completed the first survey.
They were given instructions to visit the website at their convenience over a period of one week
and to navigate it according to their own interests.
Figure 6: Daily website page views.
Box indicates evaluation period (2020-04-17 – 2020-05-09).
During the evaluation period there were a total of 1,695 page views within 88 non-bounce
sessions (when a visitor views at least two pages before exiting the website), the majority of
which were topic pages (n=893). Of the 88 non-bounce sessions, 67 were by unique visitors,
which means that 21 sessions were by returning visitors. A total of 52 visitors accessed the
website for the first time during the evaluation period, so 15 (67 minus 52) of the visitors had
access to the website prior to the evaluation period (e.g., research team and those featured on the
website). The number of new visitors corresponds closely with the number of individuals who
completed the first survey (n=49) and were sent a link to the website. The source of the
0
50
100
150
200
250
300
20
20
-04
-03
20
20
-04
-05
20
20
-04
-07
20
20
-04
-09
20
20
-04
-11
20
20
-04
-13
20
20
-04
-15
20
20
-04
-17
20
20
-04
-19
20
20
-04
-21
20
20
-04
-23
20
20
-04
-25
20
20
-04
-27
20
20
-04
-29
20
20
-05
-01
20
20
-05
-03
20
20
-05
-05
20
20
-05
-07
20
20
-05
-09
20
20
-05
-11
20
20
-05
-13
20
20
-05
-15
20
20
-05
-17
20
20
-05
-19
20
20
-05
-21
20
20
-05
-23
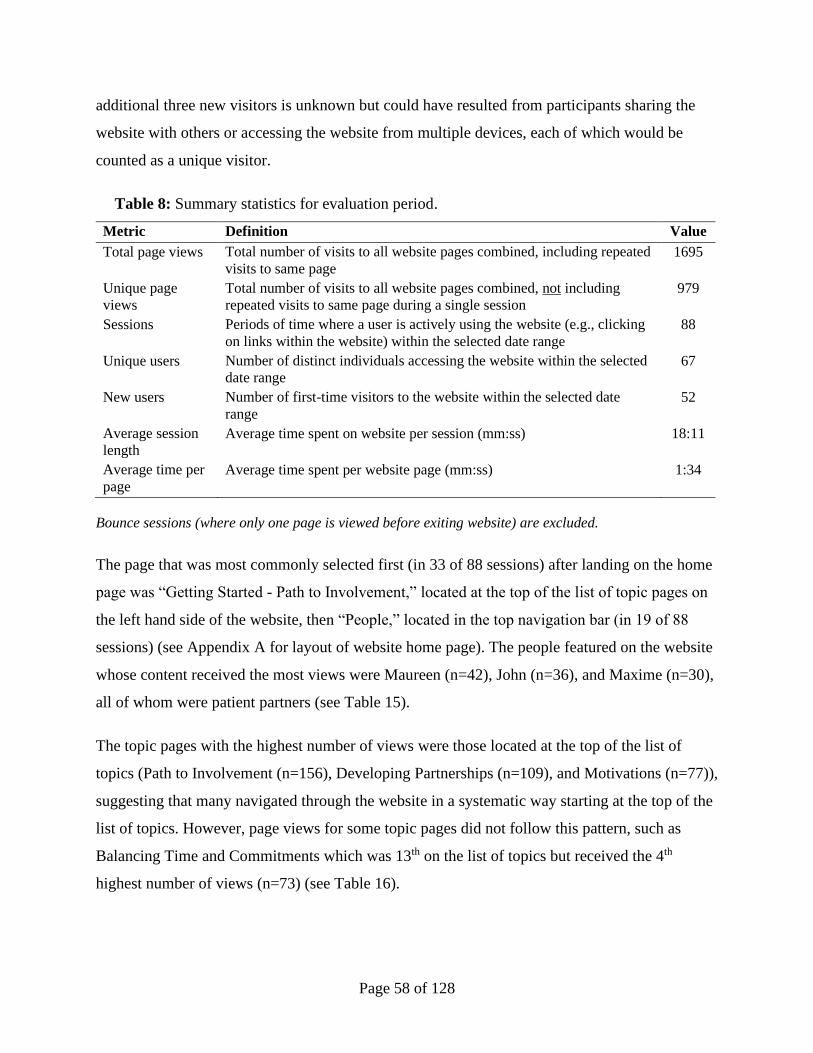
Page 58 of 128
additional three new visitors is unknown but could have resulted from participants sharing the
website with others or accessing the website from multiple devices, each of which would be
counted as a unique visitor.
Table 8: Summary statistics for evaluation period.
Metric Definition Value
Total page views Total number of visits to all website pages combined, including repeated
visits to same page
1695
Unique page
views
Total number of visits to all website pages combined, not including
repeated visits to same page during a single session
979
Sessions Periods of time where a user is actively using the website (e.g., clicking
on links within the website) within the selected date range
88
Unique users Number of distinct individuals accessing the website within the selected
date range
67
New users Number of first-time visitors to the website within the selected date
range
52
Average session
length
Average time spent on website per session (mm:ss) 18:11
Average time per
page
Average time spent per website page (mm:ss) 1:34
Bounce sessions (where only one page is viewed before exiting website) are excluded.
The page that was most commonly selected first (in 33 of 88 sessions) after landing on the home
page was “Getting Started - Path to Involvement,” located at the top of the list of topic pages on
the left hand side of the website, then “People,” located in the top navigation bar (in 19 of 88
sessions) (see Appendix A for layout of website home page). The people featured on the website
whose content received the most views were Maureen (n=42), John (n=36), and Maxime (n=30),
all of whom were patient partners (see Table 15).
The topic pages with the highest number of views were those located at the top of the list of
topics (Path to Involvement (n=156), Developing Partnerships (n=109), and Motivations (n=77)),
suggesting that many navigated through the website in a systematic way starting at the top of the
list of topics. However, page views for some topic pages did not follow this pattern, such as
Balancing Time and Commitments which was 13th on the list of topics but received the 4th
highest number of views (n=73) (see Table 16).
Page 59 of 128
A large majority of page views were via desktop (91.7%). A very small amount of page views
were via tablet (5.4%) and mobile (2.9%).
See Appendix I for more details about website utilization.
4.6 Focus Group Findings
A total of two focus groups took place, and five participants took part in each. The majority of
the 10 participants were patients or caregivers (n=7), two were researchers, and one identified as
both a patient and researcher. All had prior experience with patient-researcher partnerships. One
group was composed of only patients and caregivers and the other was composed of two
researchers, two patients/caregivers and one who identified as both.
A thematic analysis of the focus group data uncovered four overarching themes: 1) a desire for
the website to include more practical, action-oriented content, 2) desire for clarity of purpose and
definitions, 3) variance in preferences for design aspects, and 4) importance ascribed to diversity
and compensation in PER.
4.6.1 Theme 1: Desire for Practical, Action-Oriented Content
Participants offered perspectives about what purposes they felt a website about PER should
serve. For instance, many patients felt that its purpose should be to draw potential patient
partners in and inspire interest and enthusiasm about participating in partnerships:
“I think that there’s got to be a little bit of pizzazz on how helping people to
get motivated, what are the benefits, how am I going to be a help in this
situation?” -P08
Patients also expressed disappointment in some of the aspects of the website that they felt didn’t
inspire interest in partnerships, such as negative phrasing and the inclusion of negative
engagement experiences:
“They all have their own take on positive, negative and neutral, but it’s the
way the headings are set up. It puts me off from even wanting to participate if I
Page 60 of 128
didn’t know anything about it. Because all I see is it’s a lot of work, I’ve got to
juggle my personal life with this, why am I doing this?” -P06
In addition to a desire for the website to inspire interest in partnerships, patients wished that the
website would provide direct or indirect links to patient engagement opportunities, so that if
someone visiting was inspired to participate in a research partnership they could be linked to an
opportunity to do so:
“That is one of the problems I had, if you had a frequently asked questions,
like how do I get involved? Or who do I contact if I want more information?” -
P13
“Ok, here’s something. I go through, I’m interested, I’ve gone in through
enough. What’s the next step then? I apply? Or, am I redirected somewhere?
But what is the next step after I’ve gone through. I’ve listened, whatever, what
happens next?” -P06
Researchers also expressed a desire for the website to include action-oriented content, however
what they felt was lacking related to guidance for decision-making and summarized messages
and tip sheets:
“For me too I think just being able to find information faster so say I’m a
researcher I want to be involved in patient engagement, but how do I do that?
How do you send me to a tip sheet? Something to summarize the information in
a more quick digestible way.” -R25
“Today, just so you know, I’ve been struggling between a research team that
has no money and a patient partner who wants to be compensated and I’ve
been the go-between back and forth between them, right. And as I looked
through the content on the site I want to know like, where’s the right answer?”
-B26
Page 61 of 128
4.6.2 Theme 2: Desire for Clarity of Purpose and Definitions
The website was designed to be an informational resource about patient-researcher partnerships
that displayed the experiences and perspectives of a broad range of patients and researchers with
PER. However, this purpose was met with confusion by many focus group participants:
“I guess one question is, and maybe I’ve just clued out, what is the objective of
the site? And, who are you hoping to get to the site and what their takeaway is
from the site?” -P17
“I don’t know if what your goal is to have that too much information and give
perspective. But then if it is, is it guidance on how to do patient partnerships?”
-B26
The variety of perspectives represented on the website were not perceived as valuable for other
participants who wished to see more concrete definitions on the website:
“If you’re looking to draw people in, they’re giving their own personal
experience and that’s great except if I just want to know in general what a
patient partner relationship is I’m looking more for an overall definition and
these videos could show a more personal take on it.” -P06
“I think we could also sort of describe in more detail what the partnership
really did and how it benefits the research, because I think even that gets lost
in the information that we have already.” -P13
4.6.3 Theme 3: Variance in Preferences for Design Aspects
Content on the website was organized by topics, with multiple, short video clips on each topic
page, along with accompanying transcripts and short descriptive text. Participants could also
navigate the website by viewing the profiles of patients and researchers featured on the site. This
formatting was met with an assortment of sometimes conflicting critiques and criticisms. Some
patients reacted strongly to the amount of content that the website contained, expressing that it
was overwhelming:
Page 62 of 128
“I found the number of videos to be excessive and also as [name] pointed out,
the script that was presented in the videos it was an awful lot to go through.” -
P08
In contrast, some patients and researchers felt that the depth of information as well as the
representation of multiple views and perspectives was valuable:
“I was quite impressed by it. I thought that there was quite a depth of
information provided.” -P02
Many participants offered suggestions for how the website could maintain its richness and depth
of information and representation of various perspectives, while also being attractive and easy to
navigate for some of the specific groups that might visit the website:
“Maybe there’s a box that says “new patient interested in partnerships” or
“new researcher” or maybe it just says “patient” and “researcher”, even if
behind those click boxes the information is identical, I would immediately think
that it’s tailored to me. You can kind of play with my mind a little bit, right.” -
R03
Participants expressed appreciation for some of the website’s design elements, such as the use of
videos and the inclusion of accompanying transcripts:
“Sometimes I have time to sit and like to review and certainly they’re so
different, the videos just brings it to life, but sometimes I’ve just got to skim a
transcript, I only have time to skim the transcript.” -B26
“I like both. Often what I would do is I would watch the video but if it’s too
long I wouldn’t watch at all but it gave me the sense of the voice that I was
then going to read in the transcript.” -P02
Page 63 of 128
4.6.4 Theme 4: Importance Ascribed to Diversity and Compensation in
PER
Participants initiated conversations about the page titled ‘Valuing Contributions’ in both focus
groups, without prompting from the facilitators. Some of the conversation centered around the
perceived focus of the page on compensation instead of the value of patients’ contributions to
research projects or non-monetary ways to value their contributions:
“Even the lead paragraph is all about how can we value it and then it’s
guidelines on compensation, honorarias, the whole thing speaks to
compensation rather than the value of the contribution the right person can
make.” -P06
“As soon as I started reading I thought, oh my god, this section is about money
when I thought it was going to be about so many other – how to really value
contributions.” -O12
Even though this page generated some negative reaction, it was also appreciated for its
publicizing of an important and challenging topic:
“The fact that you have done, the information about the whole payment, not
just payment, but compensation, I think is really good. You know, that’s a topic
that does not ever get attacked in any other website that I’ve seen. It’s really
important, so I think that was good to put that out there at the forefront.” -R03
The topic of diversity was also highlighted by participants, who recognized it as an ongoing
challenge in PER, and wished it was addressed in a better way on the website:
“I really felt that the diversity issue was not as visible as I might have thought
it needed to be. One of the observations I have around patient engagement and
it is changing rapidly which is a great thing, but I’m finding the diversity isn’t
perhaps as well as represented as it needs to be given who the users of the
systems are.” -P02
Page 64 of 128
“How do you go about trying to ensure you do have diverse representation?
It’s something that I’m always aware of [in the work] I do in spinal cord
injury. It’s just trying to ensure that you have diversity in the voices and
making sure you’re not getting the same type of individual that’s involved in
the partnerships.” -R25
4.7 Integration of Findings
Findings from different methods were compared to examine convergences and divergences.
While each method captured some unique, non-overlapping elements of participants’ use of and
perceptions about the website, some findings overlapped in complementary and conflicting
ways.
Three findings were consistent between quantitative and qualitative data collection methods.
Two related to how participants navigated the website and the pages that received relatively high
views. It was not anticipated that the four topics pages that included ‘Coming Soon’ in their title
and contained no content would receive much, if any, traffic. Three of these four pages received
the lowest number of views of all topic pages, as expected. ‘Impact on Research,’ however,
received higher traffic than the other three empty pages. It also received more views than two
completed topic pages (‘Diversity’ and ‘Looking Forward’). The unexpected traffic to this
section matched with qualitative findings in which participants referred to impact on research as
something of interest:
“And of course Impact o[n] Research is something everyone wants to see so
that will be an interesting section once it's written and produced.” -P33
“I think when the "Impact/Making a Difference" section is complete, it will
impact views about the value/helpfulness of patient-researcher partnerships.”
-P17
“the website probably would have had even greater influence if the
Impact/Making a difference content was available.” -R41
Page 65 of 128
Another topic page that received relatively high views (higher than expected based on its order in
the list of topic pages) was ‘Advice to Others,’ which was 15th on the list of topic pages, but
received the 9th highest number of views (n=47). This corresponds with focus group findings in
which participants expressed desire for guidance:
“There’s not a lot of guidance for researchers in this topic [of compensation]
and whenever you have the conversation it always makes people feel
uncomfortable so I think having it out there and having more guidance I do
think it’s helpful to provide guidance for having that discourse and not feeling
uncomfortable with bringing it up and talking about it.” -R25
“Can you do both? Can you provide a wealth of information that shows the
different perspectives and provide a path forward that guides people in their
practical, day-to-day research life?” -B26
Responses to the TPB tool showed a significant difference in responses between patients and
researchers to questions related to perceived behavioural control (‘PBC’) and influence of
pressure from others (‘Subjective Norms’) related to engaging in partnerships. Patients reported
feeling a higher level of PBC than researchers and lower level of pressure from others than
researchers when deciding whether to be part of a partnerships. The differences in responses
corresponds with the differences in factors patient and researcher participants described as
challenges, barriers, and facilitators to engagement in partnerships in responses to open-ended
survey questions. For instance, many patients referenced their personal or internal motivation as
a facilitator for their participation in partnerships (see Table 3), which corresponds with the
finding that patients feel little pressure from others to engage in partnerships as well as the
finding that patients feel the decision to engage is mostly up to them. Patients largely identified
their family as the source of pressure to engage in partnerships, but that this pressure was not
strong. Researchers, who reported a much higher sense of pressure from others, identified their
colleagues and funders as the source of that pressure.
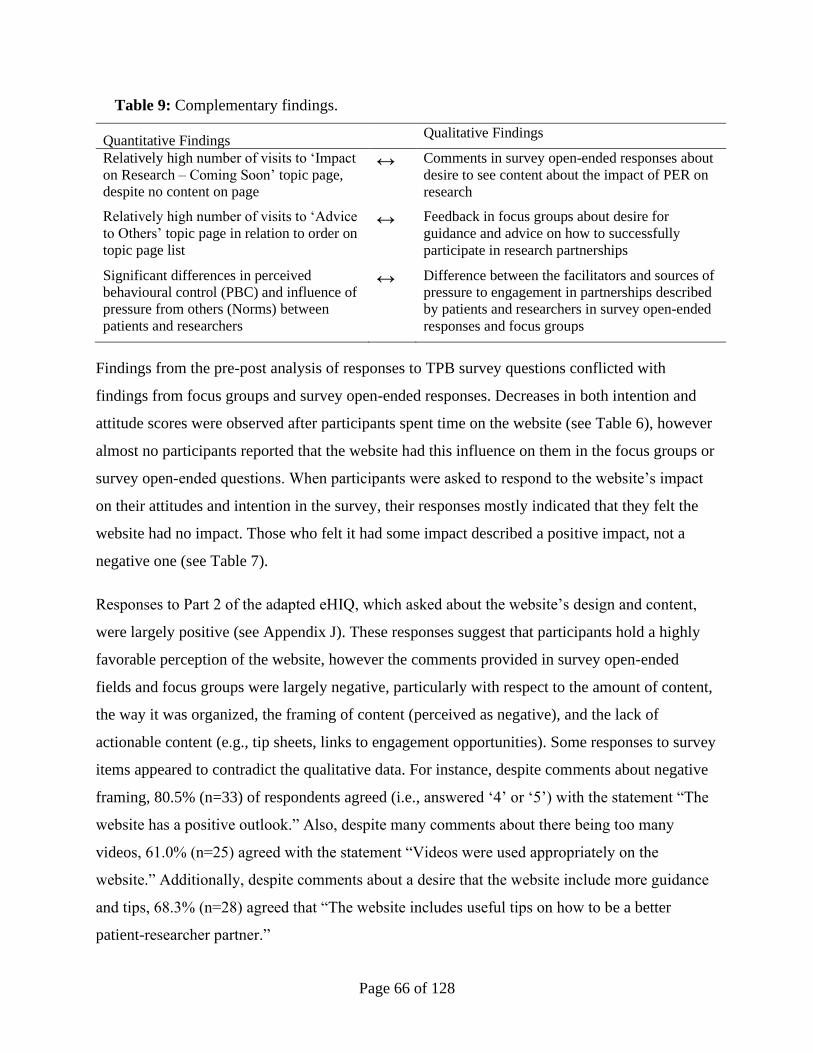
Page 66 of 128
Table 9: Complementary findings.
Quantitative Findings Qualitative Findings
Relatively high number of visits to ‘Impact
on Research – Coming Soon’ topic page,
despite no content on page
↔ Comments in survey open-ended responses about
desire to see content about the impact of PER on
research
Relatively high number of visits to ‘Advice
to Others’ topic page in relation to order on
topic page list
↔ Feedback in focus groups about desire for
guidance and advice on how to successfully
participate in research partnerships
Significant differences in perceived
behavioural control (PBC) and influence of
pressure from others (Norms) between
patients and researchers
↔ Difference between the facilitators and sources of
pressure to engagement in partnerships described
by patients and researchers in survey open-ended
responses and focus groups
Findings from the pre-post analysis of responses to TPB survey questions conflicted with
findings from focus groups and survey open-ended responses. Decreases in both intention and
attitude scores were observed after participants spent time on the website (see Table 6), however
almost no participants reported that the website had this influence on them in the focus groups or
survey open-ended questions. When participants were asked to respond to the website’s impact
on their attitudes and intention in the survey, their responses mostly indicated that they felt the
website had no impact. Those who felt it had some impact described a positive impact, not a
negative one (see Table 7).
Responses to Part 2 of the adapted eHIQ, which asked about the website’s design and content,
were largely positive (see Appendix J). These responses suggest that participants hold a highly
favorable perception of the website, however the comments provided in survey open-ended
fields and focus groups were largely negative, particularly with respect to the amount of content,
the way it was organized, the framing of content (perceived as negative), and the lack of
actionable content (e.g., tip sheets, links to engagement opportunities). Some responses to survey
items appeared to contradict the qualitative data. For instance, despite comments about negative
framing, 80.5% (n=33) of respondents agreed (i.e., answered ‘4’ or ‘5’) with the statement “The
website has a positive outlook.” Also, despite many comments about there being too many
videos, 61.0% (n=25) agreed with the statement “Videos were used appropriately on the
website.” Additionally, despite comments about a desire that the website include more guidance
and tips, 68.3% (n=28) agreed that “The website includes useful tips on how to be a better
patient-researcher partner.”
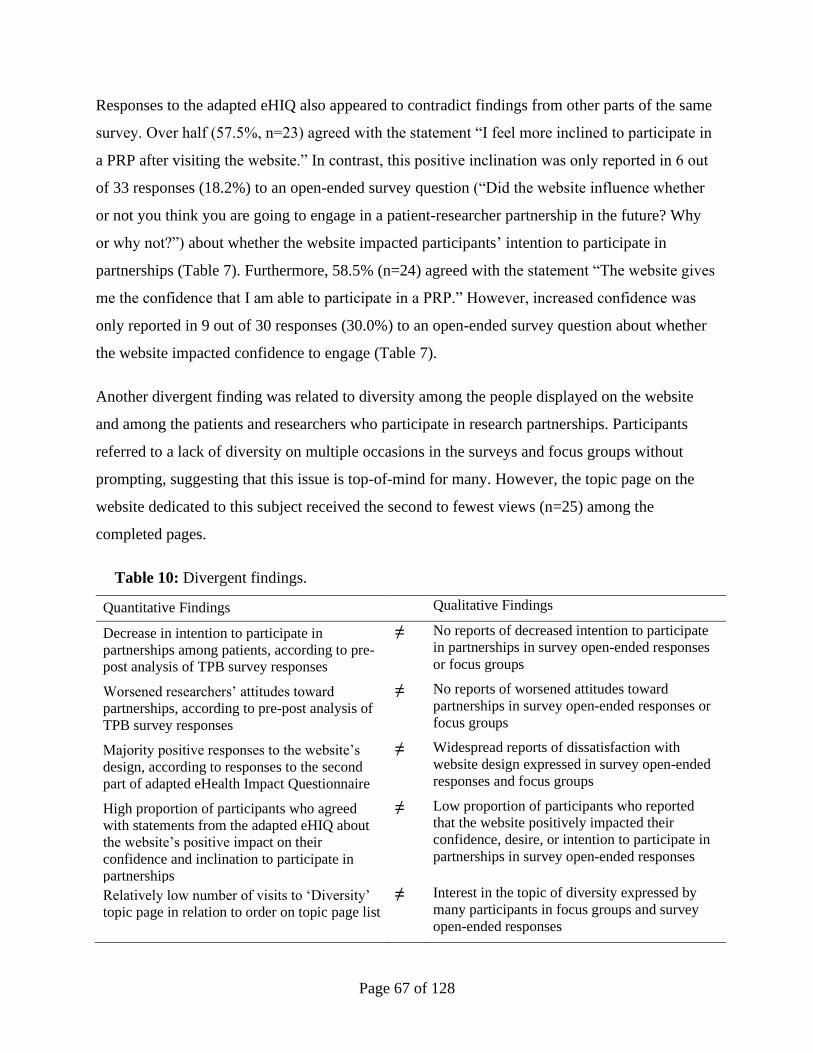
Page 67 of 128
Responses to the adapted eHIQ also appeared to contradict findings from other parts of the same
survey. Over half (57.5%, n=23) agreed with the statement “I feel more inclined to participate in
a PRP after visiting the website.” In contrast, this positive inclination was only reported in 6 out
of 33 responses (18.2%) to an open-ended survey question (“Did the website influence whether
or not you think you are going to engage in a patient-researcher partnership in the future? Why
or why not?”) about whether the website impacted participants’ intention to participate in
partnerships (Table 7). Furthermore, 58.5% (n=24) agreed with the statement “The website gives
me the confidence that I am able to participate in a PRP.” However, increased confidence was
only reported in 9 out of 30 responses (30.0%) to an open-ended survey question about whether
the website impacted confidence to engage (Table 7).
Another divergent finding was related to diversity among the people displayed on the website
and among the patients and researchers who participate in research partnerships. Participants
referred to a lack of diversity on multiple occasions in the surveys and focus groups without
prompting, suggesting that this issue is top-of-mind for many. However, the topic page on the
website dedicated to this subject received the second to fewest views (n=25) among the
completed pages.
Table 10: Divergent findings.
Quantitative Findings Qualitative Findings
Decrease in intention to participate in
partnerships among patients, according to pre-
post analysis of TPB survey responses
≠ No reports of decreased intention to participate
in partnerships in survey open-ended responses
or focus groups
Worsened researchers’ attitudes toward
partnerships, according to pre-post analysis of
TPB survey responses
≠ No reports of worsened attitudes toward
partnerships in survey open-ended responses or
focus groups
Majority positive responses to the website’s
design, according to responses to the second
part of adapted eHealth Impact Questionnaire
≠ Widespread reports of dissatisfaction with
website design expressed in survey open-ended
responses and focus groups
High proportion of participants who agreed
with statements from the adapted eHIQ about
the website’s positive impact on their
confidence and inclination to participate in
partnerships
≠ Low proportion of participants who reported
that the website positively impacted their
confidence, desire, or intention to participate in
partnerships in survey open-ended responses
Relatively low number of visits to ‘Diversity’
topic page in relation to order on topic page list
≠ Interest in the topic of diversity expressed by
many participants in focus groups and survey
open-ended responses

Page 68 of 128
4.8 Summary of Findings
This study found that 1) attitudes toward research partnerships and intentions to participate in
them were very high among those who participated in the study, 2) patients report significantly
lower pressure from others to participate in research partnerships and higher perceived
behavioural control than researchers, 3) perceptions about the website’s design and content were
conflicting, with highly positive perceptions reported in the quantitative survey questions and
low perceptions reported in focus groups and open-ended survey questions, 4) participants
reported lower (but still high) intentions to participate in research partnerships after spending
time on the website, according to the pre-post analysis of survey responses, but reported no
impact or a positive impact on intentions in responses to open-ended questions about the impact
of the website on intentions, 5) researchers reported lower (but still high) attitudes toward
research partnerships after spending time on the website, according to the pre-post analysis of
survey responses, but reported no impact or a positive impact on attitudes in responses to an
open-ended survey question, 6) participants expressed a desire for action-oriented content about
research partnerships, including guidance for researchers seeking decision-making support and
links to engagement opportunities for patients seeking to be part of a research partnership, 7)
participants had mixed feelings about how information was presented on the website – some
(mostly researchers) appreciated the rich content and presentation of varied perspectives, and
others (mostly patients) were overwhelmed by the amount of content and wished there were
more clear definitions, and 8) according to website analytics, participants tended to navigate the
website by starting at the top of the list of topic pages and moving down.
Page 69 of 128
Discussion
5.1 Overview
The research question that guided this study asked: What are the perceptions of patients and
researchers about a website featuring experiential information about patient engagement in
research, and how did it impact behavioural intentions and attitudes toward PER? We employed
a mixed methods approach that utilized surveys, focus groups, and web analytics. Our findings
indicated that participants had highly positive attitudes toward research partnerships and high
intentions to participate in them both before and after using the website. Our findings also
revealed a significant different between patients and researchers in the amounts and types of
pressures to be part of research partnerships. Integration of the findings between methods
revealed some divergence. In responses to open-ended Survey 2 questions participants reported
that the website had no impact or a positive impact on their attitudes and intentions. However, in
the same survey participants recorded lower agreement with the statements “I want to engage in
PER” and “I intend to engage in PER” than they did in Survey 1 (before visiting the website).
Furthermore, in Survey 2 most participants agreed with almost all positively phrased questions
about the website. However, in the same survey, when asked if they have “Any other comments
you would like to add about the website and/or the use of video narratives?” their responses
largely contained criticisms and negative critiques of the website.
Unfortunately, divergence between findings from different methods make it difficult to make
conclusive statements about either of these factors (i.e., overall perception of the website and its
impact on intentions and attitudes). Despite this, our findings contribute to dialogues on several
related topics. For instance, the discovery that patients and researchers report significantly
different amounts and sources of pressure to engage in research partnerships contributes to an
understanding of the factors that lead to the decision to engage in partnerships. Also, the
discovery that participants are interested in action-oriented information about research
partnerships, including guidance and links to opportunities, adds to an understanding of the kind
of content that future developers of online content about research partnerships may want to
include. Our findings also contribute to discussions about evaluation methods, including the use

Page 70 of 128
of mixed methods and the usefulness of the eHealth Impact Questionnaire and Theory of Planned
Behaviour tools as evaluative tools.
5.2 Comparison with Related Literature
Our findings can be compared with literature in a few fields, including research about the
usefulness of video narratives. The meta-analysis by Braddock & Dillard60 on the persuasive
effect of narratives found that exposure to narratives can result in movement of the audience’s
perceptions to closer alignment with those portrayed in the narratives. Since the website included
the narratives of 33 different people expressing a variety of perspectives and experiences it’s
difficult to determine the overall impact of the narratives. However, it’s possible that hearing
stories from others that included their challenging experiences shifted the perspective of website
visitors from a more optimistic and idealistic point of view to a view that included some less
pleasant and challenging aspects of research partnerships. This would support our finding that
participants felt they had been made aware of key issues in research partnerships.
While few published studies used the eHIQ, it is worth considering how our findings compare
with the findings of others who also used it. A 2019 study by Heath and colleagues83 used the
eHIQ to evaluate a similarly designed website (includes patient narratives) about burn-injury in
children. Parents of burn-injured children (n=9) and health care providers (n=22) participated in
the evaluation. Their findings for the five eHIQ subscales were slightly higher than what we
found, as nearly all were above 70 (out of 100, using the eHIQ subscale formula81) and most of
ours were slightly below 70. Their qualitative findings had some similarities to ours in that
participants commented about the amount of content, the need for diverse representation on the
website, and the use of technical terminology. A 2020 study by Talboom-Kamp and colleagues84
used the eHIQ to evaluate an online resource for communicating laboratory results. Findings
from the two eHIQ subscales they employed (Information and Presentation, and Motivation and
Confidence to Act) were slightly lower than what we found. However, given the different
purpose their website aimed to serve it is difficult to draw a comparison with our results.
Our findings can also be compared with other studies that evaluation websites designed using the
DIPEx methodology. Newman and colleagues (2009)63 evaluated a website about rheumatoid
Page 71 of 128
arthritis. One theme that came out in their evaluation was that some (22%) participants felt the
content was too negative and may be depressing for people newly diagnosed with RA. This
matches with our finding that some participants felt the content didn’t represent research
partnerships in a good light and may discourage some from wanting to participate. An evaluation
of a DIPEx website in 2004 about prostrate and breast cancer found that participants found it
highly valuable.55 There were few correlation between their findings and ours, but both studies
suggest there is an interest in websites that includes both experiential and reliable health
information (in our case, information about research partnerships).
Our findings align with PER literature about diversity and compensation. Diversity has been
cited by many as an area in need of improvement,40 and our findings confirm that this is an area
of concern as it was brought up by multiple participants without prompting. The issue of
compensation is an ongoing debate within PER,39 and our study hosted a microcosm of this
debate. Participants expressed a range of passionate, and often conflicting, opinions about this
subject, which reflects the lack of consensus about compensation that still exists and is a source
of confusion and stress for researchers and patient partners.
5.3 Interpretation of Divergent and Unanticipated Findings
The divergent finding that intention scores were lower after spending time on the website and
that no participants indicated decreased intention when asked in the survey open-ended questions
invites a discussion about factors that could have contributed to this. One factor to consider is in
the details respondents provided in their responses to open-ended survey questions, where
multiple participants indicated that the website increased their awareness of challenges and
issues to consider when engaging in partnerships or choosing which opportunities to pursue
(Table 7). It is possible that the website’s presentation of challenging aspects of research
partnerships dampened the enthusiasm that participants held before engaging with the website
content. According to Fading Affect Bias (FAB), which is the tendency of positive memories to
fade more slowly than negative memories,94 participants’ memories of past negative experiences
with research partnerships may have been weak or faded when filling out the first survey. Then,
the website’s portrayal of challenging aspects of research partnerships refreshed their memory,
which impacted the way in which they responded to the TPB prompts in the second survey.

Page 72 of 128
According to this interpretation, the website may cause participants to think more critically about
partnerships and consider factors that can make them successful or unsuccessful, thereby slightly
dampening their desire and intention to engage.
Another bias may explain the divergence between the pre-post analysis of intention scores and
participants reporting of the website’s impact in open-ended survey questions. Response Shift
Bias (RSB) occurs when a person’s frame of reference toward the construct being measured
changes as the result of an intervention. Some researchers argue that the influence of changed
frames of reference can compromise evaluations of educational interventions that use pre and
post measurements.95 This is because what was measured in the first test is fundamentally
different from what is being measured in the second test, and therefore not comparable. The
constructs we aimed to measure in this case was participants’ attitudes and intention to engage in
research partnerships and the intervention was spending time on the website. The website may
have changed participants’ frame of reference by changing their mental image/memory of
research partnerships. The initial frame of reference may have been an idealized memory or
understanding of research partnerships, and the frame of reference at the second measurement
was a more grounded and realistic understanding of partnerships, resulting from spending time
on the website.
To account for the confounding influence of RSB, some researchers have employed a
retrospective pre-test method design, in which both pre and post perceptions are collected at the
same time, after the intervention.95 In this design participants are asked to recall their prior
perceptions to compare with their post-intervention perceptions.95 In this way the participant uses
the same frame of reference for their assessment of their current and past perceptions. Our study
approximated this model with the inclusion of open-ended questions in the second survey that
directly asked respondents if they believed that the website impacted their desires, intentions,
feelings, and confidence related to research partnerships (Table 7). By asking about impact, the
questions required participants to reflect on their prior perceptions and contrast them with their
current perceptions, like what would occur in a retrospective pre-test method design. Responses
to these questions contradicted the findings from the pre-post analysis, by not including any
reports of decreased intention and by including some reports of positive impact. This
contradiction in findings may be explained by RSB. According to this interpretation, the pre-post
Page 73 of 128
analysis is less reliable than self-reported perceptions of impact in the open-ended survey
questions, where most reported that the website had no impact. Following from this, the website
did not change participants’ intentions to engage in research partnerships, but rather influenced
their frame of reference for considering research partnerships.
Another discrepancy that deserves further discussion is the majority positive responses to nearly
all Likert-scale survey questions about the website in contrast to the largely negative statements
about the website made by participants in open-ended survey questions and focus groups. There
are a few response biases known to impact responses to questions using Likert scales (e.g., social
desirability, acquiescence).96 Confirmation bias, which is the tendency for respondents to
activate beliefs that are consistent with the way an item is stated,97 holds promise as an
interpretation of our divergent findings. Since the website contained a broad range of content, it
would be possible for participants to recall how an aspect of the website aligned, even if only in
a small way, with each positively phrased survey items. For example, the highly positive
response to the survey item “Videos were used appropriately on the site” conflicts with the
feedback from many participants that the number of videos was excessive and overwhelming.
Participants may have read the prompt and thought of some ways in which the videos were
appropriate and selected ‘agree,’ even though they felt there were too many of them.
An alternative interpretation of this divergent finding is that participants did hold an overall
positive perception of the website, as indicated in responses to Likert-style survey questions, and
the critical feedback found in the qualitative data skewed negative because participants chose to
highlight potential areas for improvement instead of discussing their overall impression.
These interpretations do not provide a conclusive answer to the divergence within our data, but
they do introduce interesting lines of inquiry to be taken up in future research.
5.4 Contribution to Academic Knowledge
This study contributes to knowledge about the use of mixed methods, specifically how it can
uncover conflicts within the data which may necessitate further consideration of the influence of
biases. If this study had only utilized one method, the findings may have been more conclusive,
however those results may have been less robust due to uninterrogated biases. The study also

Page 74 of 128
contributes to knowledge about the kinds of online resources that patients and researchers desire.
Our findings suggest that there is a strong desire for practical guidance and links to engagement
opportunities. Our findings also uncovered differences in the levels and amounts of pressure to
engage in partnerships experienced by patients and researchers. This is an area that has not yet
been explored in the context of research partnerships and may be interesting for other researchers
to investigate further.
The study also adds to literature about informational or educational interventions, and cases
where there may not be clarity in the intervention’s objectives with respect to ‘informing,’
‘inspiring,’ and ‘advising.’ Our findings revealed conflicts about the purpose of the website in
these three domains. It was designed to be informative, yet patients expressed a desire for it to
also be inspiring and researchers that it also provide guidance. This adds an interesting nuance to
discussions about the purpose of educational interventions, and the need to consider potential
unintended consequences when developing these interventions (e.g., if providing more
information about challenges associated with an activity may result in reduced enthusiasm to
participate in that activity).
5.5 Implications for Policy & Practise
Our findings are particularly useful for the website development team, providing feedback to
enables revisions that better match the preferences and needs of patients and researchers as
potential users. The findings could also prove useful to other teams who are considering creating
online resources about research partnerships.
The topic of diversity and achieving representation in patient engagement in research was raised
by multiple participants and deserves further attention. PER laudably aims to move healthcare
toward a post-paternalistic future by giving voice to the lived experiences of patients. However,
if the patients whose voices are heard are not representative, PER risks inadvertently stalling
healthcare’s progress by perpetuating the tired tradition of over-representing the voices of
wealthy, white, urban-dwelling, highly educated individuals. If achieving diverse representation
in PER is currently a nice-to-have, decision-makers may wish to consider taking steps to make it
a requirement. For instance, research ethics boards could require researchers who propose to

Page 75 of 128
include patient partners in their study to ensure that they include more traditionally underserved
populations (e.g., ethnic minorities, low income populations) than traditionally overserved
populations.
This study may also prove useful for the Database of Individual Patient Experiences (DIPEx)
community and those who maintain each member countries’ websites. Our findings reveal that
participants struggled to navigate the website content, and many felt overwhelmed by the volume
of material. Since all DIPEx websites use a similar format it may be worthwhile to investigate
whether other websites are also perceived this way and whether guidelines for formatting of
content should be revisited. It may also invite a conversation about the usefulness of applying the
DIPEx model outside of the direct context of patient experiences, which is what it is designed
for. Research partnerships are not a health experience so much as they are an experience of a
relationship or collaboration, and they may be better represented using a different method.
5.6 Opportunities for Future Research
Our finding that patients report very low pressure from others (subjective norms) to participate in
research partnerships, but at the same time report extremely high intention to engage in research
partnerships, suggests there may be limitations to the Theory of Planned Behavior. Our findings
suggest that many patients’ motivations are internal and personal. However, the TPB describes
subjective norms and a sense of pressure from others as a key predictor of behavioural intention.
This invites further research into the role of internal motivations as a factor in behavioural
intention in the context of research partnerships and otherwise.
Another aspect of the Theory of Planned Behaviour that deserves further inquiry relates to
perceived behavioural control. When participants were asked about factors that make them feel
engaging in partnerships is outside of their control, researchers mostly identified factors that
would require them to participate in partnerships (e.g., funding agencies) and patients identified
factors that could exclude them from participating (e.g., the need for the research team to
approve their involvement). Both kinds of factors contribute to decreased perceived control, but
one could increase intention to participate (requirements from funders) and the other could
decrease it (feeling that researchers make the final decision). According to the Theory of
Page 76 of 128
Planned Behaviour, high perceptions of control should correlate with high behavioural intention.
However, in the case of researchers, low perceptions of control resulting from funder
expectations may correlate with high behavioural intention (which is what PER advocates may
wish for). This invites further research into cases where decreases in perceived behavioural
control can result in higher behavioural intention. It also invites a discussion about whether
pressure from funders may contribute to insincere or tokenistic PER, and whether there are better
ways to incentivise researchers to participate in PER.
5.7 Limitations
One of the limitations to this study is the small sample size, which limits the generalizability of
our results. Another is that, despite our goal to recruit a diverse sample, our sample over-
represented white, Canadian-born, Ontario-dwelling, highly educated women over the age of 55
who had prior experience with PER. This limits the generalizability of our findings to large
segments of the Canadian population, including ethnic minorities, young people, people without
university degrees, non-Ontarian Canadians, and those not familiar with PER. This lack of
diversity in our sample is reflective of the lack of diversity in PER, and likely results from many
of the same factors (e.g., challenges researchers face in establishing relationships with some
population groups).
Additional limitations include the fact that the website was incomplete, which may have
influenced participants’ perceptions of the website, as may have the short period of time
participants were given access to the website. Also, the inability to separate the research team’s
web traffic from the participants’ web traffic may have skewed the web analytics data, which
limits the reliability of this data. Furthermore, the fact that we could not access analytics data
about participants’ engagement with video content caused us to rely on self-reported
information, which is subject to memory and other biases. These limitations were recognized in
the interpretation of our findings, as we chose not to overemphasize the findings from less
reliable data.
Some other limitations arose due to COVID-19 restrictions. Some technical issues arose during
the focus groups, including audio and video connectivity problems. This resulted in some

Page 77 of 128
members being asked to repeat statements because their audio cut out and some members were
unable to join by video at all, and instead called in to the meeting. Videoconferencing does not
facilitate some of the norms of in-person meetings, such as eye contact with the speaker and the
informal interactions that occur before and after meetings begin. The full extent to which this
impacted the focus groups is unknown, but participants expressed some frustration about the
videoconferencing format during the groups. Another limitation related to COVID-19 was its
impact on the recruitment process. We had not yet reached out to all the organizations we had
planned to when travel restrictions and work-from-home orders came into place in March 2020.
With consideration for the need for organizations to commit extra time and resources to adapting
to this change, we chose to stop reaching out to organizations to distribute our invitation to
participate during this time. This limited both the number of participants we recruited as well as
their representativeness, as we had not yet reached out to organizations in provinces east of
Ontario.
5.8 Conclusion
While this study did not provide a definitive or succinct answer to the question of whether the
website was perceived as useful or whether it had a positive impact on attitudes or intentions
related to research partnerships, it opened many interesting dialogues. It demonstrated the value
of mixed methods in uncovering the role of biases and potential weaknesses in some methods
and survey tools, as well as challenges in interpreting and integrating the results. It elucidated
some of the desires patients and researchers have for online content about research partnerships.
It uncovered some of the differences between patients and researchers in their motivations to
engage in research partnerships. It introduced avenues of inquiry related to the Theory of
Planned Behaviour and its relevance for behaviours that are internally motivated and cases where
higher perceived behavioural control may result in lower behavioural intention. It added to
knowledge about the desire to learn from research partnerships that feature diversity amongst
patient partners, as well as for decisive guidelines and supports for compensating patient partners
in a way that demonstrates respect for their contributions and consideration of their economic
circumstances.
Page 78 of 128
References
1. Esmail L, Moore E, Rein A. Evaluating patient and stakeholder engagement in research:
moving from theory to practice. J. 2015;4:133-45.
2. Mullins CD. Integrating Patients' Voices in Study Design Elements with a Focus on
Hard-to-reach Populations. Washington, DC, USA: Patient-Centered Outcomes
Research Institute (PCORI),;2012.
3. Abelson J, Forest PG, Eyles J, Smith P, Martin E, Gauvin FP. Deliberations about
deliberative methods: issues in the design and evaluation of public participation
processes. Social Science & Medicine. 2003;57:239-51.
4. Dudley L, Gamble C, Preston J, et al. What difference does patient and public
involvement make and what are its pathways to impact? Qualitative study of patients and
researchers from a cohort of randomised clinical trials. PLoS ONE. 2015;10:e0128817.
5. Crocker JC, Boylan AM, Bostock J, Locock L. Is it worth it? Patient and public views on
the impact of their involvement in health research and its assessment: a UK-based
qualitative interview study. Health Expect. 2017;20:519-28.
6. Wilson P, Mathie E, Poland F, et al. How embedded is public involvement in mainstream
health research in England a decade after policy implementation? A realist evaluation.
Journal of Health Services Research & Policy. 2018;23:98-106.
7. Carroll SL, Embuldeniya G, Abelson J, McGillion M, Berkesse A, Healey JS.
Questioning patient engagement: research scientists' perceptions of the challenges of
patient engagement in a cardiovascular research network. PATIENT PREFERENCE AND
ADHERENCE. 2017;11:1573-83.
8. Hewlett S, De Wit M, Richards P, et al. Patients and professionals as research partners:
Challenges, practicalities, and benefits. Arthritis Care and Research. 2006;55:676-80.
9. Belisle-Pipon JC, Rouleau G, Birko S. Early-career researchers' views on ethical
dimensions of patient engagement in research. BMC MEDICAL ETHICS. 2018;19:21-10.
10. Price A, Albarqouni L, Kirkpatrick J, et al. Patient and public involvement in the design
of clinical trials: An overview of systematic reviews. Journal of Evaluation in Clinical
Practice. 2018;24:240-53.
11. Creswell JW, Plano CVL. Designing and conducting mixed methods research. Third ed:
SAGE Publications, Inc.; 2018.
12. Bandura A. Social Learning Theory: General Learning Corporation; 1971.
13. Grusec J. Social Learning Theory and developmental psychology: The legacies of Robert
Sears and Albert Bandura. Developmental Psychology. 1992;28:776-86.
Page 79 of 128
14. Patton MQ. Qualitative research and evaluation methods. Thousand Oaks, Calif: Sage
Publications; 2002.
15. Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision
Processes. 1991;50:179-211.
16. Carman KL, Dardess P, Maurer M, et al. Patient and family engagement: a framework for
understanding the elements and developing interventions and policies. Health Aff
(Millwood). 2013;32:223-31.
17. Canadian Institutes of Health Research (CIHR). Guide to Knowledge Translation
Planning at CIHR: Integrated and End-of-Grant Approaches. Ottawa, CA 2012.
18. Parry D, Salsberg J, Macaulay AC, Participatory Research at McGill (PRAM). A Guide
to Researcher and Knowledge-User Collaboration in Health Research. 2015.
19. Domecq JP, Prutsky G, Elraiyah T, et al. Patient engagement in research: a systematic
review. BMC Health Serv Res. 2014;14:89.
20. Richards T, Montori VM, Godlee F, Lapsley P, Paul D. Let the patient revolution begin:
Patients can improve healthcare: it's time to take partnership seriously. BMJ: British
Medical Journal. 2013;346:7-.
21. Canadian Institutes of Health Research (CIHR). Strategy for Patient-Oriented Research -
Patient Engagement Framework 2014; http://www.cihr-irsc.gc.ca/e/48413.html. Accessed
April 13, 2019.
22. Kirwan JR, de Wit M, Frank L, et al. Emerging Guidelines for Patient Engagement in
Research. Value Health. 2017;20:481-6.
23. James Lind Alliance (JLA). The James Lind Alliance. 2019; http://www.jla.nihr.ac.uk/.
Accessed April 13, 2019.
24. Donetto S, Pierri P, Tsianakas V, Robert G. Experience-based Co-design and Healthcare
Improvement: Realizing Participatory Design in the Public Sector. The Design Journal.
2015;18:227-48.
25. Brett J, Staniszewska S, Mockford C, et al. A Systematic Review of the Impact of Patient
and Public Involvement on Service Users, Researchers and Communities. The Patient -
Patient-Centered Outcomes Research. 2014;7:387-95.
26. Staley K. 'Is it worth doing?' Measuring the impact of patient and public involvement in
research. Research involvement and engagement. 2015;1:6.
27. INVOLVE. Our Projects. 2019; https://www.involve.org.uk/our-work/our-projects.
Accessed April 15, 2019.
Page 80 of 128
28. Patient-Centered Outcomes Research Institute (PCORI). Our Story. 2017;
https://www.pcori.org/about-us/our-story. Accessed April 15, 2019.
29. International Association for Public Participation (IAP2). About IAP2. 2019;
https://www.iap2.org/page/A3. Accessed April 15, 2019.
30. Canadian Institutes of Health Research (CIHR). Strategy for Patient-Oriented Research:
Patient Engagement Framework. 2014; http://www.cihr-irsc.gc.ca/e/48413.html.
Accessed April 15, 2019.
31. Canadian Institutes of Health Research. About SPOR. 2018; http://www.cihr-
irsc.gc.ca/e/51036.html. Accessed April 28, 2019.
32. Ontario SPOR Support Unit (OSSU). Our Impact. 2019; https://ossu.ca/our-impact/.
Accessed April 28, 2019.
33. Jones EL, Williams-Yesson BA, Hackett RC, Staniszewska SH, Evans D, Francis NK.
Quality of Reporting on Patient and Public Involvement Within Surgical Research: A
Systematic Review. Annals of Surgery. 2015;261:243-50.
34. Crocker JC, Ricci-Cabello I, Parker A, et al. Impact of patient and public involvement on
enrolment and retention in clinical trials: systematic review and meta-analysis. BMJ-
BRITISH MEDICAL JOURNAL. 2018;363:k4738.
35. Evans D, Bird E, Gibson A, et al. Extent, quality and impact of patient and public
involvement in antimicrobial drug development research: A systematic review. Health
Expect. 2018;21:75-81.
36. Elliott MJ, Goodarzi Z, Sale JEM, et al. Perceived Significance of Engagement in
Research Prioritization Among Chronic Kidney Disease Patients, Caregivers, and Health
Care Professionals: A Qualitative Study. Canadian Journal of Kidney Health and
Disease. 2018;5:205435811880748.
37. Miller J, Knott VE, Wilson C, Roder D. A review of community engagement in cancer
control studies among Indigenous people of Australia, New Zealand, Canada and the
USA. European Journal of Cancer Care. 2012;21:283-95.
38. Chu Yang L, Loyola-Sanchez A, Hurd K, et al. Characterization of indigenous
community engagement in arthritis studies conducted in Canada, United States of
America, Australia and New Zealand. Seminars in Arthritis and Rheumatism. 2018.
39. Richards DP, Jordan I, Strain K, Press Z. Patient partner compensation in research and
health care: the patient perspective on why and how. Patient Experience Journal. 2018;5.
40. Black A, Strain K, Wallsworth C, et al. What constitutes meaningful engagement for
patients and families as partners on research teams? Journal of Health Services Research
& Policy. 2018;23:158-67.
Page 81 of 128
41. Pii KH, Schou LH, Piil K, Jarden M. Current trends in patient and public involvement in
cancer research: A systematic review. Health Expect. 2019;22:3-20.
42. Bethell J, Commisso E, Rostad HM, et al. Patient engagement in research related to
dementia: A scoping review. Dementia. 2018;17:944-75.
43. Bonevski B, Randell M, Paul C, et al. Reaching the hard-to-reach: A systematic review of
strategies for improving health and medical research with socially disadvantaged groups.
BMC Medical Research Methodology. 2014;14:42-.
44. Boivin A, L'Esperance A, Gauvin FP, et al. Patient and public engagement in research
and health system decision making: A systematic review of evaluation tools. Health
Expect. 2018;21:1075-84.
45. Abelson J, Humphrey A, Syrowatka A, Bidonde J, Judd M. Evaluating Patient, Family
and Public Engagement in Health Services Improvement and System Redesign.
Healthcare Quarterly. 2018;21:31.
46. The Beryl Institute. Improving the Patient Experience. http://www.theberylinstitute.org/.
Accessed Feb 23, 2019.
47. Patient-Centered Outcomes Research Institute (PCORI). Engagement.
https://www.pcori.org/engagement. Accessed Feb 23, 2019.
48. Warwick Medical School. Patient Public Involvement – Training. 2018;
https://warwick.ac.uk/fac/sci/med/research/ctu/ppitraining/. Accessed April 27, 2019.
49. INVOLVE. Training case study four: Introduction to patient and public involvement in
research. 2012; https://www.invo.org.uk/posttyperesource/planning-training-general-
overview/training-case-study-four/. Accessed April 27, 2019.
50. St. Michael's Hospital. Patient Engagement: Tools & Resources.
http://stmichaelshospitalresearch.ca/patient-engagement-resource/. Accessed Feb 23,
2019.
51. Canadian Child Health Clinician Scientist Program (CCHCSP). New Partnership to
Advance Building Capacity in Patient-Oriented Research. https://www.child-
bright.ca/new-blog/2017/10/11/training-partnership. Accessed Feb 23, 2019.
52. Terry M. New Patient Engagement in Primary Health Care Research online training
program launched. [Monthly eNewsletter]. 2018;
https://www.schulich.uwo.ca/familymedicine/about_us/newsletter/2018/december/new_p
atient_engagement_in_primary_health_care_research_online_training_program_launche
d.html. Accessed April 27, 2019.
53. Rodrigue JR, Fleishman A, Vishnevsky T, Fitzpatrick S, Boger M. Organ donation video
messaging: differential appeal, emotional valence, and behavioral intention. Clinical
transplantation. 2014;28:1184-92.
Page 82 of 128
54. Occa A, Suggs LS. Communicating Breast Cancer Screening With Young Women: An
Experimental Test of Didactic and Narrative Messages Using Video and Infographics.
Journal of Health Communication. 2016;21:1-11.
55. Rozmovits L, Ziebland S. What do patients with prostate or breast cancer want from an
Internet site? A qualitative study of information needs. Patient Educ Couns. 2004;53:57-
64.
56. Shaw BR, Han JY, Baker T, et al. How women with breast cancer learn using interactive
cancer communication systems. Health Education Research. 2007;22:108-19.
57. Sznitman SR, Lewis N. Examining effects of medical cannabis narratives on beliefs,
attitudes, and intentions related to recreational cannabis: A web-based randomized
experiment. Drug and Alcohol Dependence. 2018;185:219-25.
58. Taylor AM, Hutchings M. Using video narratives of women's lived experience of
breastfeeding in midwifery education: Exploring its impact on midwives' attitudes to
breastfeeding. Maternal and Child Nutrition. 2012;8:88-102.
59. Coret A, Boyd K, Hobbs K, Zazulak J, McConnell M. Patient Narratives as a Teaching
Tool: A Pilot Study of First-Year Medical Students and Patient Educators Affected by
Intellectual/Developmental Disabilities. Teaching and Learning in Medicine.
2018;30:317-27.
60. Braddock K, Dillard JP. Meta-analytic evidence for the persuasive effect of narratives on
beliefs, attitudes, intentions, and behaviors. Communication Monographs. 2016;83:446-
67.
61. McQueen A, Kreuter MW, Kalesan B, Alcaraz KI. Understanding Narrative Effects: The
Impact of Breast Cancer Survivor Stories on Message Processing, Attitudes, and Beliefs
Among African American Women. Health Psychology. 2011;30:674-82.
62. Ziebland S, Wyke S. Health and Illness in a Connected World: How Might Sharing
Experiences on the Internet Affect People's Health? Milbank Quarterly. 2012;90:219-49.
63. Newman MA, Ziebland S, Barker KL. Patients' views of a multimedia resource featuring
experiences of rheumatoid arthritis: pilot evaluation of www.healthtalkonline.org. Health
Inform J. 2009;15:147-59.
64. Fox S. The social life of health information. FactTank: New in the Numbers 2014;
https://www.pewresearch.org/fact-tank/2014/01/15/the-social-life-of-health-information/.
65. DIPEx International. Research. 2019; http://www.dipexinternational.org/research.
Accessed April 11, 2019.
66. University of Oxford. Health Experiences Research Group. 2019;
https://www.phc.ox.ac.uk/research/health-experiences. Accessed April 11, 2019.
Page 83 of 128
67. Shannon-Baker P. Making Paradigms Meaningful in Mixed Methods Research. Journal
of Mixed Methods Research. 2016;10:319-34.
68. Morgan DL. Paradigms Lost and Pragmatism Regained: Methodological Implications of
Combining Qualitative and Quantitative Methods. Journal of Mixed Methods Research.
2007;1:48-76.
69. Sandelowski M. Unmixing Mixed‐Methods Research. Research in Nursing & Health.
2014;37:3-8.
70. Pope C, Mays N. Reaching The Parts Other Methods Cannot Reach: An Introduction To
Qualitative Methods In Health And Health Services Research. BMJ: British Medical
Journal. 1995;311:42-5.
71. Greene J, C. , Caracelli V, J. , Graham W, F. . Toward a Conceptual Framework for
Mixed-Method Evaluation Designs. Educational Evaluation and Policy Analysis.
1989;11:255-74.
72. Ozawa S, Pongpirul K. 10 best resources on … mixed methods research in health
systems. Health Policy and Planning. 2014;29:323-7.
73. Pluye P, Hong QN. Combining the power of stories and the power of numbers: Mixed
methods research and mixed studies reviews. Annual Review of Public Health.
2014;35:29-45.
74. Privitera GJ, Ahlgrim-Delzell L. Research Methods for Education: SAGE Publications;
2018.
75. Kim H, Sefcik JS, Bradway C. Characteristics of Qualitative Descriptive Studies: A
Systematic Review. Research in nursing & health. 2017;40:23-42.
76. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health.
2000;23:334-40.
77. Groves RM, Fowler Jr FJ, Couper MP, Lepkowski JM, Singer E, Tourangeau R. Survey
methodology. Vol 561: John Wiley & Sons; 2011.
78. Coughlan M, Cronin P, Ryan F. Survey research: Process and limitations. International
Journal of Therapy and Rehabilitation. 2009;16:9-15.
79. Kitzinger J. Introducing Focus Groups. BMJ: British Medical Journal. 1995;311:299-
302.
80. Smithson J. Using and analysing focus groups: Limitations and possibilities.
International Journal of Social Research Methodology. 2000;3:103-19.
Page 84 of 128
81. Kelly L, Ziebland S, Jenkinson C. Measuring the effects of online health information:
Scale validation for the e-Health Impact Questionnaire. Patient Education and
Counselling. 2015;98:1418-24.
82. Kelly L, Jenkinson C, Ziebland S. Measuring the effects of online health information for
patients: Item generation for an e-health impact questionnaire. Patient Education and
Counseling. 2013;93:433-8.
83. Heath J, Williamson H, Williams L, Harcourt D. Supporting children with burns:
Developing a UK parent-focused peer-informed website to support families of burn-
injured children. Patient Educ Couns. 2019;102:1730-5.
84. Talboom-Kamp E, Tossaint-Schoenmakers R, Goedhart A, Versluis A, Kasteleyn M.
Evaluating an online patient portal for communicating laboratory test results: A real-
world study into patients' attitude using the eHealth Impact Questionnaire (eHIQ). JMIR
Form Res. 2020;04:04.
85. Boyko JA, Lavis JN, Dobbins M, Souza NM. Reliability of a tool for measuring theory of
planned behaviour constructs for use in evaluating research use in policymaking. Health
Research Policy and Systems. 2011;9:29-.
86. Francis J, Eccles MP, Johnston M, et al. Constructing questionnaires based on the theory
of planned behaviour: A manual for health services researchers. Newcastle upon Tyne,
UK: Centre for Health Services Research, University of Newcastle upon Tyne; 2004.
87. Cohen DJ. Statistical power analysis (2nd ed.). Hillsdale, NJ.: Erlbaum.; 1988.
88. Morgan DL, Hoffman K. "Focus Groups". In: Flick U, ed. The SAGE Handbook of
Qualitative Data Collection. 55 City Road: SAGE Publications Ltd; 2018:250-63.
89. Field A. Discovering Statistics Using SPSS. Third ed: SAGE Publications Ltd; 2009.
90. Roulston K. "Analysing Interviews". In: Flick U, ed. The SAGE Handbook of Qualitative
Data Analysis. 55 City Road: SAGE Publications, Inc.; 2014:297-312.
91. Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in
Psychology. 2006;3:77-101.
92. Vogl S. Integrating and Consolidating Data in Mixed Methods Data Analysis: Examples
From Focus Group Data With Children. Journal of mixed methods research.
2018;13:536-54.
93. Sandelowski M, Voils CI, Knafl G. On Quantitizing. Journal of mixed methods research.
2009;3:208-22.
94. Skowronski JJ, Walker WR, Henderson DX, Bond GD. Chapter Three - The Fading
Affect Bias: Its History, Its Implications, and Its Future. In: Olson JM, Zanna MP, eds.
Advances in Experimental Social Psychology. Vol 49: Academic Press; 2014:163-218.
Page 85 of 128
95. Drennan J, Hyde A. Controlling response shift bias: the use of the retrospective pre-test
design in the evaluation of a master's programme. Assessment & Evaluation in Higher
Education. 2008;33:699-709.
96. Kreitchmann RS, Abad FJ, Ponsoda V, Nieto MD, Morillo D. Controlling for Response
Biases in Self-Report Scales: Forced-Choice vs. Psychometric Modeling of Likert Items.
Frontiers in Psychology. 2019;10.
97. Davies MF. Confirmatory Bias in the Evaluation of Personality Descriptions: Positive
Test Strategies and Output Interference. Journal of Personality and Social Psychology.
2003;85:736-44.
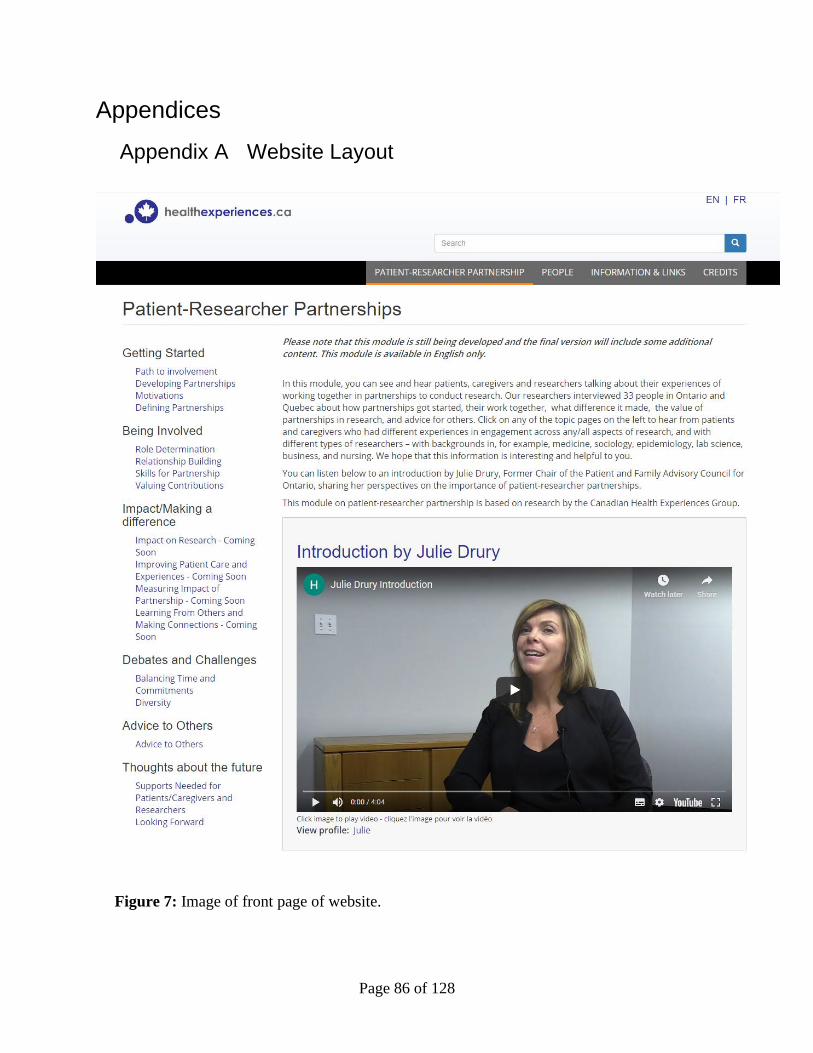
Page 86 of 128
Appendices
Appendix A Website Layout
Figure 7: Image of front page of website.
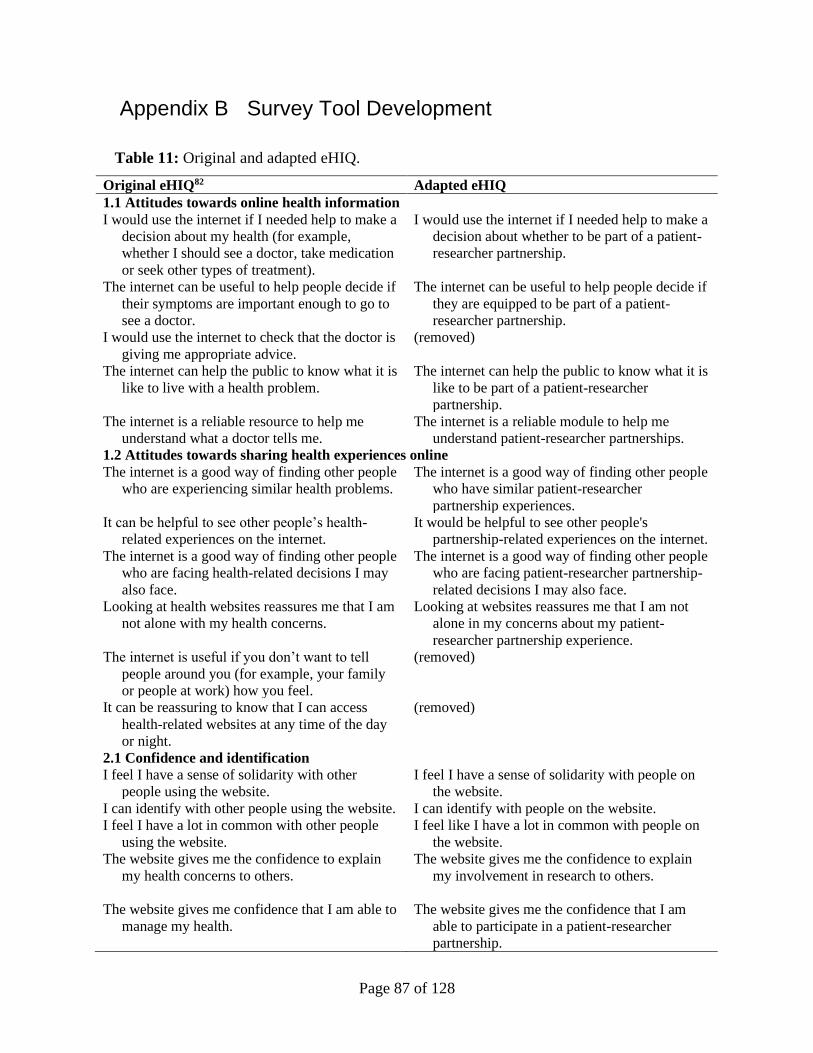
Page 87 of 128
Appendix B Survey Tool Development
Table 11: Original and adapted eHIQ.
Original eHIQ82 Adapted eHIQ
1.1 Attitudes towards online health information
I would use the internet if I needed help to make a
decision about my health (for example,
whether I should see a doctor, take medication
or seek other types of treatment).
I would use the internet if I needed help to make a
decision about whether to be part of a patient-
researcher partnership.
The internet can be useful to help people decide if
their symptoms are important enough to go to
see a doctor.
The internet can be useful to help people decide if
they are equipped to be part of a patient-
researcher partnership.
I would use the internet to check that the doctor is
giving me appropriate advice.
(removed)
The internet can help the public to know what it is
like to live with a health problem.
The internet can help the public to know what it is
like to be part of a patient-researcher
partnership.
The internet is a reliable resource to help me
understand what a doctor tells me.
The internet is a reliable module to help me
understand patient-researcher partnerships.
1.2 Attitudes towards sharing health experiences online
The internet is a good way of finding other people
who are experiencing similar health problems.
The internet is a good way of finding other people
who have similar patient-researcher
partnership experiences.
It can be helpful to see other people’s health-
related experiences on the internet.
It would be helpful to see other people's
partnership-related experiences on the internet.
The internet is a good way of finding other people
who are facing health-related decisions I may
also face.
The internet is a good way of finding other people
who are facing patient-researcher partnership-
related decisions I may also face.
Looking at health websites reassures me that I am
not alone with my health concerns.
Looking at websites reassures me that I am not
alone in my concerns about my patient-
researcher partnership experience.
The internet is useful if you don’t want to tell
people around you (for example, your family
or people at work) how you feel.
(removed)
It can be reassuring to know that I can access
health-related websites at any time of the day
or night.
(removed)
2.1 Confidence and identification
I feel I have a sense of solidarity with other
people using the website.
I feel I have a sense of solidarity with people on
the website.
I can identify with other people using the website. I can identify with people on the website.
I feel I have a lot in common with other people
using the website.
I feel like I have a lot in common with people on
the website.
The website gives me the confidence to explain
my health concerns to others.
The website gives me the confidence to explain
my involvement in research to others.
The website gives me confidence that I am able to
manage my health.
The website gives me the confidence that I am
able to participate in a patient-researcher
partnership.
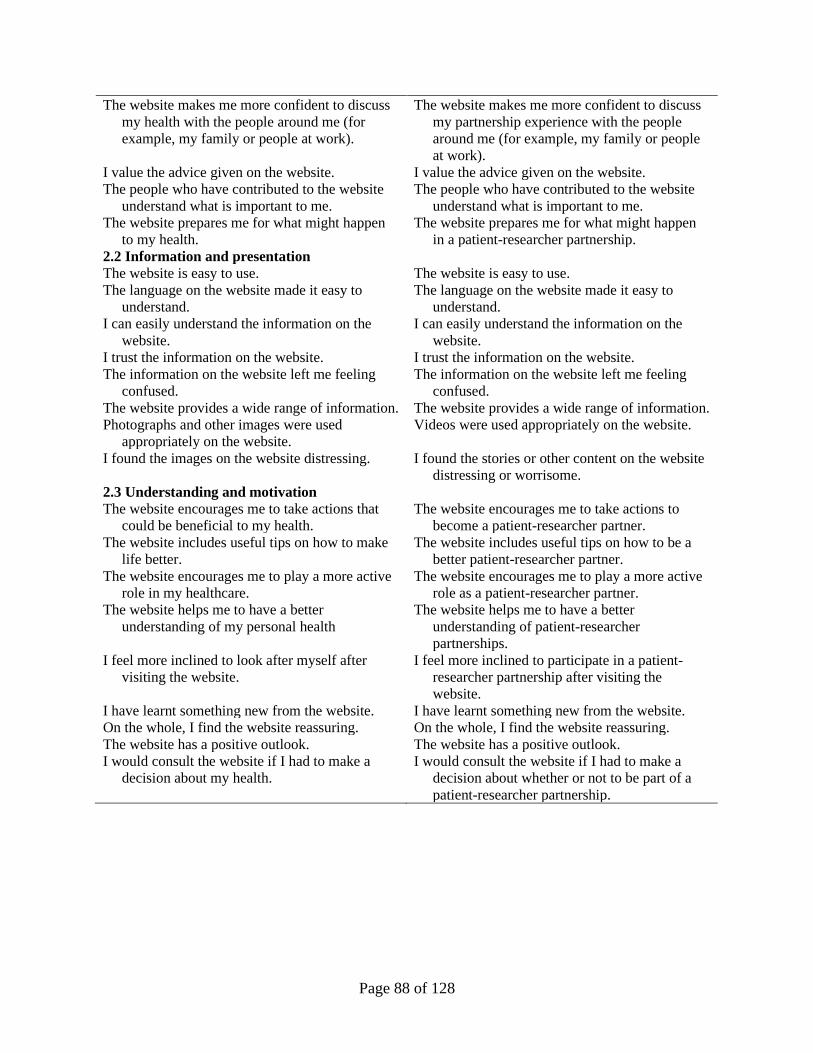
Page 88 of 128
The website makes me more confident to discuss
my health with the people around me (for
example, my family or people at work).
The website makes me more confident to discuss
my partnership experience with the people
around me (for example, my family or people
at work).
I value the advice given on the website. I value the advice given on the website.
The people who have contributed to the website
understand what is important to me.
The people who have contributed to the website
understand what is important to me.
The website prepares me for what might happen
to my health.
The website prepares me for what might happen
in a patient-researcher partnership.
2.2 Information and presentation
The website is easy to use. The website is easy to use.
The language on the website made it easy to
understand.
The language on the website made it easy to
understand.
I can easily understand the information on the
website.
I can easily understand the information on the
website.
I trust the information on the website. I trust the information on the website.
The information on the website left me feeling
confused.
The information on the website left me feeling
confused.
The website provides a wide range of information. The website provides a wide range of information.
Photographs and other images were used
appropriately on the website.
Videos were used appropriately on the website.
I found the images on the website distressing. I found the stories or other content on the website
distressing or worrisome.
2.3 Understanding and motivation
The website encourages me to take actions that
could be beneficial to my health.
The website encourages me to take actions to
become a patient-researcher partner.
The website includes useful tips on how to make
life better.
The website includes useful tips on how to be a
better patient-researcher partner.
The website encourages me to play a more active
role in my healthcare.
The website encourages me to play a more active
role as a patient-researcher partner.
The website helps me to have a better
understanding of my personal health
The website helps me to have a better
understanding of patient-researcher
partnerships.
I feel more inclined to look after myself after
visiting the website.
I feel more inclined to participate in a patient-
researcher partnership after visiting the
website.
I have learnt something new from the website. I have learnt something new from the website.
On the whole, I find the website reassuring. On the whole, I find the website reassuring.
The website has a positive outlook. The website has a positive outlook.
I would consult the website if I had to make a
decision about my health.
I would consult the website if I had to make a
decision about whether or not to be part of a
patient-researcher partnership.
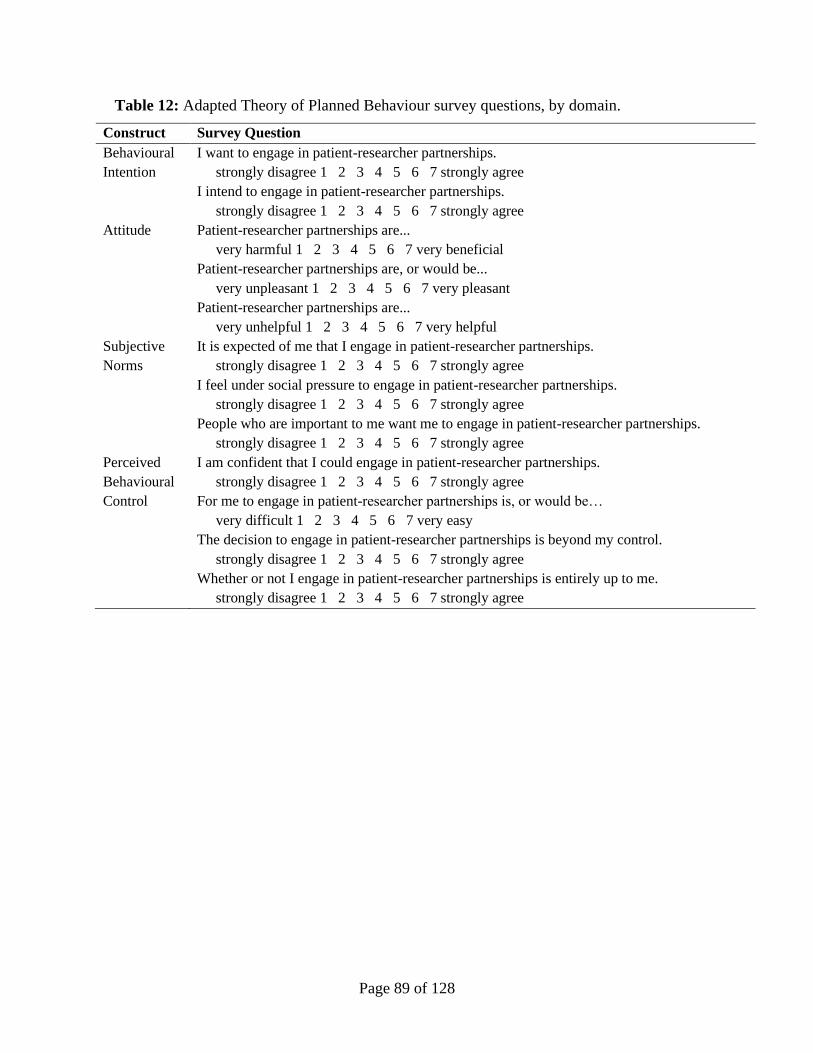
Page 89 of 128
Table 12: Adapted Theory of Planned Behaviour survey questions, by domain.
Construct Survey Question
Behavioural
Intention
I want to engage in patient-researcher partnerships.
strongly disagree 1 2 3 4 5 6 7 strongly agree
I intend to engage in patient-researcher partnerships.
strongly disagree 1 2 3 4 5 6 7 strongly agree
Attitude Patient-researcher partnerships are...
very harmful 1 2 3 4 5 6 7 very beneficial
Patient-researcher partnerships are, or would be...
very unpleasant 1 2 3 4 5 6 7 very pleasant
Patient-researcher partnerships are...
very unhelpful 1 2 3 4 5 6 7 very helpful
Subjective
Norms
It is expected of me that I engage in patient-researcher partnerships.
strongly disagree 1 2 3 4 5 6 7 strongly agree
I feel under social pressure to engage in patient-researcher partnerships.
strongly disagree 1 2 3 4 5 6 7 strongly agree
People who are important to me want me to engage in patient-researcher partnerships.
strongly disagree 1 2 3 4 5 6 7 strongly agree
Perceived
Behavioural
Control
I am confident that I could engage in patient-researcher partnerships.
strongly disagree 1 2 3 4 5 6 7 strongly agree
For me to engage in patient-researcher partnerships is, or would be…
very difficult 1 2 3 4 5 6 7 very easy
The decision to engage in patient-researcher partnerships is beyond my control.
strongly disagree 1 2 3 4 5 6 7 strongly agree
Whether or not I engage in patient-researcher partnerships is entirely up to me.
strongly disagree 1 2 3 4 5 6 7 strongly agree
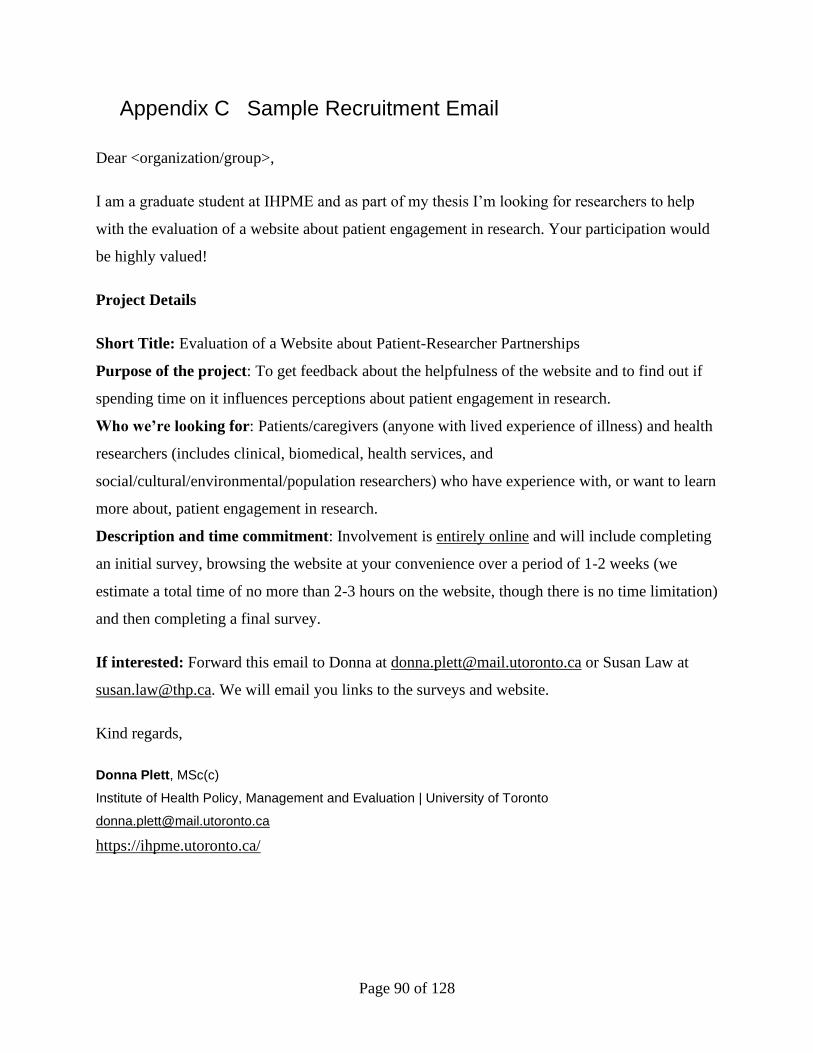
Page 90 of 128
Appendix C Sample Recruitment Email
Dear <organization/group>,
I am a graduate student at IHPME and as part of my thesis I’m looking for researchers to help
with the evaluation of a website about patient engagement in research. Your participation would
be highly valued!
Project Details
Short Title: Evaluation of a Website about Patient-Researcher Partnerships
Purpose of the project: To get feedback about the helpfulness of the website and to find out if
spending time on it influences perceptions about patient engagement in research.
Who we’re looking for: Patients/caregivers (anyone with lived experience of illness) and health
researchers (includes clinical, biomedical, health services, and
social/cultural/environmental/population researchers) who have experience with, or want to learn
more about, patient engagement in research.
Description and time commitment: Involvement is entirely online and will include completing
an initial survey, browsing the website at your convenience over a period of 1-2 weeks (we
estimate a total time of no more than 2-3 hours on the website, though there is no time limitation)
and then completing a final survey.
If interested: Forward this email to Donna at [email protected] or Susan Law at
[email protected]. We will email you links to the surveys and website.
Kind regards,
Donna Plett, MSc(c)
Institute of Health Policy, Management and Evaluation | University of Toronto
https://ihpme.utoronto.ca/
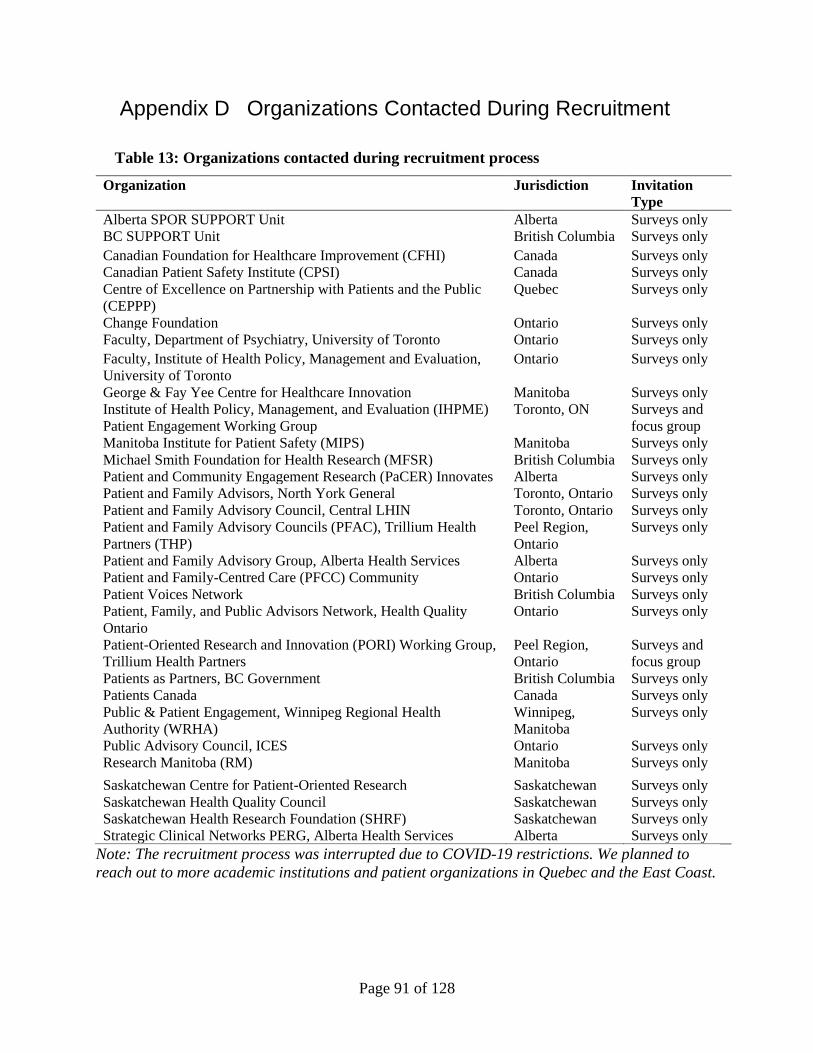
Page 91 of 128
Appendix D Organizations Contacted During Recruitment
Table 13: Organizations contacted during recruitment process
Organization Jurisdiction Invitation
Type
Alberta SPOR SUPPORT Unit Alberta Surveys only
BC SUPPORT Unit British Columbia Surveys only
Canadian Foundation for Healthcare Improvement (CFHI) Canada Surveys only
Canadian Patient Safety Institute (CPSI) Canada Surveys only
Centre of Excellence on Partnership with Patients and the Public
(CEPPP)
Quebec Surveys only
Change Foundation Ontario Surveys only
Faculty, Department of Psychiatry, University of Toronto Ontario Surveys only
Faculty, Institute of Health Policy, Management and Evaluation,
University of Toronto
Ontario Surveys only
George & Fay Yee Centre for Healthcare Innovation Manitoba Surveys only
Institute of Health Policy, Management, and Evaluation (IHPME)
Patient Engagement Working Group
Toronto, ON Surveys and
focus group
Manitoba Institute for Patient Safety (MIPS) Manitoba Surveys only
Michael Smith Foundation for Health Research (MFSR) British Columbia Surveys only
Patient and Community Engagement Research (PaCER) Innovates Alberta Surveys only
Patient and Family Advisors, North York General Toronto, Ontario Surveys only
Patient and Family Advisory Council, Central LHIN Toronto, Ontario Surveys only
Patient and Family Advisory Councils (PFAC), Trillium Health
Partners (THP)
Peel Region,
Ontario
Surveys only
Patient and Family Advisory Group, Alberta Health Services Alberta Surveys only
Patient and Family-Centred Care (PFCC) Community Ontario Surveys only
Patient Voices Network British Columbia Surveys only
Patient, Family, and Public Advisors Network, Health Quality
Ontario
Ontario Surveys only
Patient-Oriented Research and Innovation (PORI) Working Group,
Trillium Health Partners
Peel Region,
Ontario
Surveys and
focus group
Patients as Partners, BC Government British Columbia Surveys only
Patients Canada Canada Surveys only
Public & Patient Engagement, Winnipeg Regional Health
Authority (WRHA)
Winnipeg,
Manitoba
Surveys only
Public Advisory Council, ICES Ontario Surveys only
Research Manitoba (RM) Manitoba Surveys only
Saskatchewan Centre for Patient-Oriented Research Saskatchewan Surveys only
Saskatchewan Health Quality Council Saskatchewan Surveys only
Saskatchewan Health Research Foundation (SHRF) Saskatchewan Surveys only
Strategic Clinical Networks PERG, Alberta Health Services Alberta Surveys only
Note: The recruitment process was interrupted due to COVID-19 restrictions. We planned to
reach out to more academic institutions and patient organizations in Quebec and the East Coast.
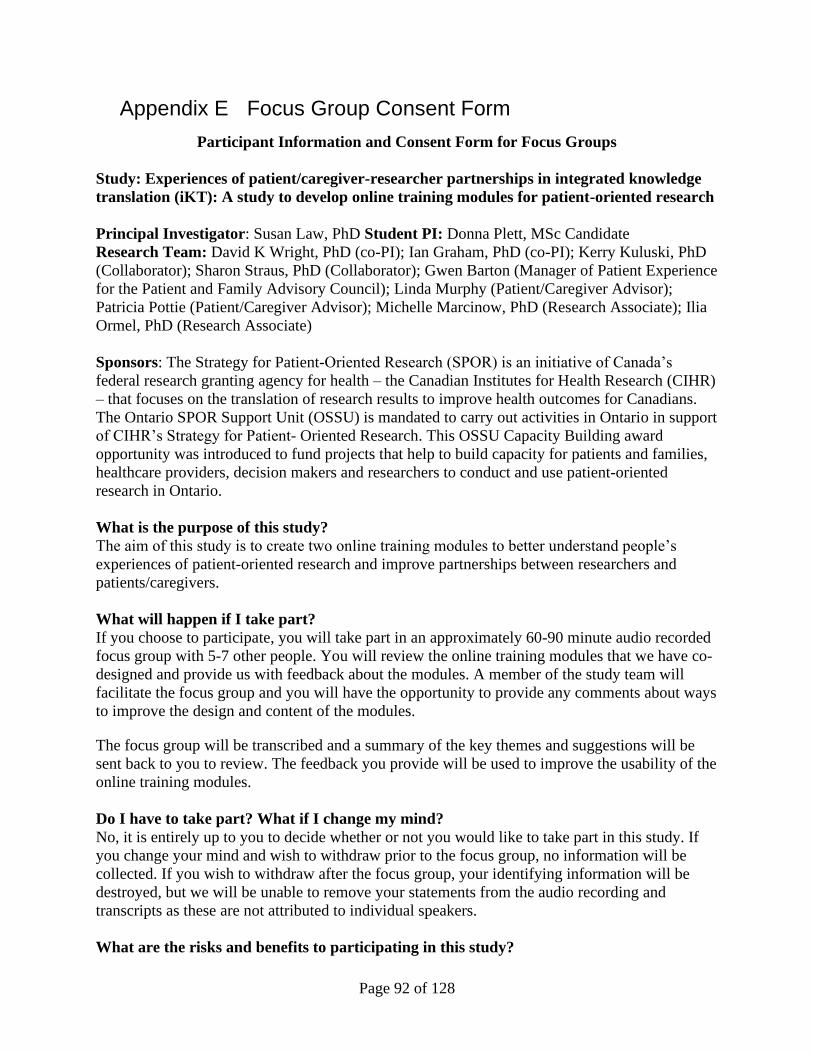
Page 92 of 128
Appendix E Focus Group Consent Form
Participant Information and Consent Form for Focus Groups
Study: Experiences of patient/caregiver-researcher partnerships in integrated knowledge
translation (iKT): A study to develop online training modules for patient-oriented research
Principal Investigator: Susan Law, PhD Student PI: Donna Plett, MSc Candidate
Research Team: David K Wright, PhD (co-PI); Ian Graham, PhD (co-PI); Kerry Kuluski, PhD
(Collaborator); Sharon Straus, PhD (Collaborator); Gwen Barton (Manager of Patient Experience
for the Patient and Family Advisory Council); Linda Murphy (Patient/Caregiver Advisor);
Patricia Pottie (Patient/Caregiver Advisor); Michelle Marcinow, PhD (Research Associate); Ilia
Ormel, PhD (Research Associate)
Sponsors: The Strategy for Patient-Oriented Research (SPOR) is an initiative of Canada’s
federal research granting agency for health – the Canadian Institutes for Health Research (CIHR)
– that focuses on the translation of research results to improve health outcomes for Canadians.
The Ontario SPOR Support Unit (OSSU) is mandated to carry out activities in Ontario in support
of CIHR’s Strategy for Patient- Oriented Research. This OSSU Capacity Building award
opportunity was introduced to fund projects that help to build capacity for patients and families,
healthcare providers, decision makers and researchers to conduct and use patient-oriented
research in Ontario.
What is the purpose of this study?
The aim of this study is to create two online training modules to better understand people’s
experiences of patient-oriented research and improve partnerships between researchers and
patients/caregivers.
What will happen if I take part?
If you choose to participate, you will take part in an approximately 60-90 minute audio recorded
focus group with 5-7 other people. You will review the online training modules that we have co-
designed and provide us with feedback about the modules. A member of the study team will
facilitate the focus group and you will have the opportunity to provide any comments about ways
to improve the design and content of the modules.
The focus group will be transcribed and a summary of the key themes and suggestions will be
sent back to you to review. The feedback you provide will be used to improve the usability of the
online training modules.
Do I have to take part? What if I change my mind?
No, it is entirely up to you to decide whether or not you would like to take part in this study. If
you change your mind and wish to withdraw prior to the focus group, no information will be
collected. If you wish to withdraw after the focus group, your identifying information will be
destroyed, but we will be unable to remove your statements from the audio recording and
transcripts as these are not attributed to individual speakers.
What are the risks and benefits to participating in this study?
Page 93 of 128
Taking part in the focus groups will take 60-90 minutes. This may cause you to be tired.
However, your contributions to this study will benefit those who view the online training
modules in the future.
Who has reviewed the study?
This study has been reviewed and approved by the Research Ethics Board at Trillium Health
Partners (Study #880).
Who is organising and funding the research?
The Institute for Better Health, based at Trillium Health Partners, is collaborating with the
University of Ottawa and St. Mary’s Research Centre to complete this research. The project
“Experiences of patient/caregiver-researcher partnerships in integrated knowledge translation: a
study to develop online training modules for patient-oriented research” is financially supported
by the Ontario SPOR Support Unit’s Patient-Oriented Research Capacity Building Initiatives
Awards.
Contact for further information
If you have any questions at all about the project or wish to discuss anything, please contact Dr.
Susan Law by telephoning (416) 270-6643, or emailing at [email protected].
If you want to talk to someone not connected with the study about your rights as a study
participant, or if you have any complaints about the research, you can call Trillium Health
Partners’ Research Ethics Board at (905) 848 7580 x1682 or the University of Toronto Review
Ethics Board at (416) 946-3273 or [email protected].
Page 94 of 128
DOCUMENTATION OF INFORMED CONSENT
Study Title: Experiences of patient/caregiver-researcher partnerships in integrated knowledge
translation: A study to develop online training modules for patient-oriented research
Participant:
By signing this form, I confirm that:
• I have read each page of this form and this study has been fully explained to me.
• I understand the research being done, what is required to participate in this study, and what is
expected of me.
• I have had a chance to have all of my questions answered to my satisfaction.
• If I choose not to participate, I can hand back an unsigned copy of the consent form to the
research team member.
• I understand that your consent does not waive any of your legal rights, nor relieve the research
team from any legal responsibility.
• I agree to participate in this study.
I wish to receive general information in the future about the health experiences research (e.g.,
newsletter, announcements regarding new modules, etc.) YES/NO
I can be contacted about future research on health experiences. YES/NO
Preferred phone number: __________________________
Preferred email: ________________________________
_______________________________ ________________________ _______________
Name of Participant (print) Signature Date
Statement of Research Team Member:
I will respect the rights and wishes of the participant as described in this informed consent
document, and conduct this study according to all applicable laws, regulations, and guidelines
relating to the ethical and legal conduct of research. I have explained the purpose of the study to
the participant and have answered all of his or her questions.
_______________________________ ________________________ _______________
Name of Person Obtaining Consent Signature Date
Page 95 of 128
Appendix F Interview Guide for Focus Groups
Introduction, Purpose and Consent (20 minutes)
Thank everyone for attending.
Hello, my name is Susan Law and I am working with a research team investigating patient-
researcher partnerships and the potential value of an online learning module that features the
experiences of patients/caregivers and researchers as partners in research, using video/audio
excerpts from individual interviews. The purpose of this group session is to discuss your
perceptions of patient-researcher partnerships and the online resource that you have had access to
over the last few weeks. We will aim to be finished in no more than 2 hours today.
Roundtable introductions – name, role, experience of research and partnerships
Consent form
• Review consent form
• Request permission to record the session for purposes of analysis
• Participants will be requested not to disclose statements made by other participants
during the session
Brief Overview of the Project and Results to Date (20 minutes)
Susan, Donna – present overview of purpose, methods, results to date.
Focus group questions – for discussion (60 minutes):
A. Initial Reflections about the Online Resource and Survey Results to Date
1. Tell me about your overall impression of the use and value of the website?
2. Would you use the website? How/why? Examples? Who else might find it useful?
3. Any suggestions for improving the design or layout of the website?
4. Any content that might be missing or removed?
5. Any concerns/risks regarding the information presented?
B. KNOWLEDGE: Existing understanding about partnerships
1. In what sorts of ways was the website helpful in your understanding of partnerships –
what it is and how it works? Examples of what you learned, what was new, what was
surprising?
Page 96 of 128
2. Do you think this information might change people’s attitudes towards partnerships?
Why? What about yours – change or no change?
3. To what extent do you feel that (patients, caregivers, researchers) receive adequate
information about patient-researcher partnerships?
a. positive and negative examples?
b. examples of how
4. Tell me about particular information gaps that should be addressed? Examples?
a. Does the website address any of these gaps?
C. ATTITUDES: Perceptions about value of partnerships
1. What do you believe are the advantages of patient-researcher partnerships?
a. For yourself and in general
2. What do you believe are the disadvantages of patient-researcher partnerships?
a. For yourself and in general
3. How, if at all, did the website influence your attitude toward patient-researcher
partnerships?
D. BARRIERS & FACILITATORS: Motivations to participate in partnerships
1. What factors or circumstances would enable you to participate in patient-researcher
partnerships?
2. What factors or circumstances might make it difficult or impossible for you to participate
in patient-researcher partnerships?
3. Are there any other issues that come to mind when you think about participating in
patient-researcher partnerships?
4. In what ways did the website influence how prepared you would feel to participate in a
research partnership? More or less motivated to participate in partnership?
Wrap-up and Next Steps (20 minutes)
Susan to sum up key messages
Participants to comment – final comments or additional ideas
Explain what we will do with the results – inform any changes to online module, contribution to
evaluation results.
Thank you for participating in the focus group and sharing your feedback!
Page 97 of 128
Appendix G Pre and Post Surveys
PRE SURVEY
Title: Evaluation of a Website about Patient-Researcher Partnerships: Survey 1
Consent Form
Principal Investigator: Susan Law, PhD, Director - Research, Institute for Better Health -
Trillium Health Partners
Student Investigator: Donna Plett, MSc Student - Health Services Research, IHPME, University
of Toronto
Hello! You are invited to participate in this web-based survey to help evaluate a website about
engagement between patients and researchers as partners in research, featuring video/audio
excerpts from interviews about their experiences.
This evaluation is in two parts:
1) Before reviewing the website, we will ask about you and your interests in patient-researcher
partnerships;
2) Then, after providing some time (approximately 1 week) to review the website and explore the
various themes and topics featured there, we will ask you to complete a follow-up survey to
obtain your views about the value and potential usefulness of this website and thoughts about
patient-researcher partnerships.
It should take a maximum of 10-15 minutes to complete each survey (pre and post).
PARTICIPATION: Your participation in this survey is voluntary. You may refuse to take part in
the research or exit the survey at any time without penalty. You are free to decline to answer any
particular question you do not wish to answer for any reason. If you would like to exclude your
responses from the study please contact us within 2 weeks and we will delete them.
BENEFITS: You will receive no direct benefits from participating in this research study.
However, your responses may help us learn more about a website about patient-researcher
partnerships.
RISKS: There are no foreseeable risks involved in participating in this study.
CONFIDENTIALITY: The email address that you have already provided to the research team
will only be accessed by the principal investigator (PI) and student PI. It will only be used for the
purposes of follow-up communication, after which your e-mail will be deleted. No names or
identifying information will be included in any publications or presentations based on these data,
and your responses to this survey will remain confidential. Our records of participants' email
addresses will be stored securely on Trillium Health Partners servers (accessible only to the
research team) and will remain separate from your survey responses.
Page 98 of 128
IP address tracking will be turned off on the survey tool. Survey responses from SurveyMonkey
are sent over a secure, SSL encrypted connection. Since SurveyMonkey is a company located in
the United States, USA authorities under the provisions of the Patriot Act may access the survey
data in rare instances.
CONTACT: If you have questions at any time about the study or the procedures, you may
contact the PI, Susan Law, via phone at (905) 848-7580 x1659 or email at [email protected].
If you feel you have not been treated according to the descriptions in this form, or that your
rights as a participant in research have not been honored during the course of this project, or you
have any questions, concerns, or complaints that you wish to address to someone other than the
investigator, you may contact either the Research Ethics Board at Trillium Health Partners at
(905) 848-7580 ext.1682 or [email protected], OR the University of Toronto Review Ethics Board
at (416) 946-3273 or [email protected].
ELECTRONIC CONSENT: Please select your choice below. You may print a copy of this
consent form for your records.
Clicking on the "Agree" button indicates that:
• You have read the above information and fully understand the research that is being done and
what is being asked of you
• You voluntarily agree to participate in this study
• You understand that you may withdraw from the study at any time and your withdrawal does
not waive any of your legal rights, nor relieve the research team from any legal responsibility
• You are 18 years of age or older
Agree
Disagree
Part 1
Please provide the following details about yourself.
Note: For the purposes of this study, we are defining patient-researcher partnerships as
activities where patients and/or caregivers and researchers are working together in any or all
aspects of planning studies, reviewing literature, collecting and analyzing data/information
and/or disseminating the results of research.
Page 99 of 128
1.1 Age (circle):
18-24 25-34 35-44 45-54 55-64 65+
1.2 Gender (circle)
Female Male Other: ____________________
1.3 Country of Birth: __________________________________
1.4 Self-Identified Ethnic Origin and/or Cultural Background:
_____________________________________________
1.5 Town/City of Residence: _____________________
1.6 Province of Residence: ______________________
1.7 Highest Level of Education Attained (circle one):
Less than high school High school College Undergraduate Postgraduate
1.8 Employment Status (circle all that apply):
Full-time Part-time Retired Student Unemployed
Other:_______________________
1.9 Occupation: _______________________________
1.10 My primary role in patient-researcher partnerships is or would be as a… (circle one)
Patient or Caregiver (includes anyone with lived experience of illness)
Researcher (with formal training and/or academic appointment)
Could be either (role varies depending on the project)
Other: ____________________________
1.11 FOR ‘COULD BE EITHER’: Which perspective would you like to use for this study?
Patient/Caregiver
Researcher
Page 100 of 128
1.12 FOR PATIENTS/CAREGIVERS: What illness or problem(s) did you or a loved one
experience?
__________________________________________________________________________
1.13 FOR RESEARCHERS: What is your primary field of research?
Health Services & Policy Population & Public Health Basic Biomedical Clinical Other:
_______________
1.14 I have been part of (circle)… 0 1 2 3+ …research projects that included patient-
researcher partnerships.
1.15 Have you received formal training in research partnerships? (circle) Yes No
Part 2
This section is about the internet as a place to learn about patient-researcher partnerships. Please
answer as best you can even if you have no prior experience with patient-researcher partnerships.
2.1 The internet is a reliable module to help me understand patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.2 The internet can help the public to know what it is like to be part of a patient-researcher
partnership.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.3 The internet can be useful to help people decide if they are equipped to be part of a patient-
researcher partnership.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.4 I would use the internet if I needed help to make a decision about whether to be part of a
patient-researcher partnership.
Strongly Disagree 1 2 3 4 5 Strongly Agree
Page 101 of 128
2.5 The internet is a good way of finding other people who have similar patient-researcher
partnership experiences.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.6 It would be helpful to see other people’s partnership-related experiences on the internet.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.7 The internet is a good way of finding other people who are facing patient-researcher
partnership-related decision I may also face.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.8 Looking at websites reassures me that I am not alone in my concerns about my patient-
researcher partnership experience.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.9 Do you have any other comments about patient-researcher partnerships and web-based
information?
___________________________________________________________________________
___________________________________________________________________________
Part 3
This section is about how you think and feel about patient-researcher partnerships. Please give
your best answer, even if you have no prior experience with patient-researcher partnerships.
Note: For the purposes of this study, we are defining patient-researcher partnerships as activities
where patients and/or caregivers and researchers are working together in any or all aspects of
planning studies, reviewing literature, collecting and analyzing data/information and/or
disseminating the results of research.
3.1 I want to engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
Page 102 of 128
3.2 I intend to engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.3 Patient-researcher partnerships are, or would be…
Very Harmful 1 2 3 4 5 6 7 Very Beneficial
Very Unpleasant 1 2 3 4 5 6 7 Very Pleasant
(for me) (for me)
Very Unhelpful 1 2 3 4 5 6 7 Very Helpful
3.4 Do you have any comments to add regarding your expectations, intentions or thoughts about
engaging in patient-researcher partnerships?
___________________________________________________________________________
___________________________________________________________________________
3.5 It is expected of me that I engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.6 I feel under social pressure to engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.7 People who are important to me want me to engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.8 Which types of people did you have in mind while answering the last three questions (e.g.,
family, friends, colleagues, work-related superiors, etc.)?
___________________________________________________________________________
___________________________________________________________________________
3.9 I am confident that I could engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
Page 103 of 128
3.10 For me to engage in patient-researcher partnerships is, or would be…
Very Difficult 1 2 3 4 5 6 7 Very Easy
3.11 What makes engaging in patient-researcher partnerships easy for you?
___________________________________________________________________________
___________________________________________________________________________
3.12 What makes engaging in patient-researcher partnerships difficult for you?
___________________________________________________________________________
___________________________________________________________________________
3.13 The decision to engage in patient-researcher partnerships is beyond my control.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.14 Whether or not I engage in patient-researcher partnerships is entirely up to me.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.15 If you feel it is not in your control, why not?
___________________________________________________________________________
___________________________________________________________________________
3.16 Do you have any further comments about patient-researcher partnerships and your
involvement?
___________________________________________________________________________
___________________________________________________________________________
Part 4
Next Steps:
1. Go to the website (the link will be emailed to you when you press 'submit'). Please note that
this website is still being developed and the final version will include some additional content.
Page 104 of 128
2. Spend time on the website at your convenience over the next week. The website consists of
many different themes, topics and pages related to patient-researcher partnerships. We ask that
you navigate through the website and engage with whichever content is interesting or relevant to
you.
3. Complete final survey in approximately one week (you will receive a link by email)
If you have any questions please don't hesitate to contact Donna at [email protected]
or Susan at [email protected].
This information will be sent to your email address when you press 'submit.'
Thank you for filling out this survey!
Page 105 of 128
POST SURVEY
Title: Evaluation of a Website about Patient-Researcher Partnerships: Survey 2
Consent Form
Principal Investigator: Susan Law, PhD, Director - Research, Institute for Better Health -
Trillium Health Partners
Student Investigator: Donna Plett, MSc Student - Health Services Research, IHPME, University
of Toronto
Hello! You have reached the second and final stage of this study. Please complete this follow-up
survey so we can obtain your views about the value and potential usefulness of the website and
your thoughts about patient-researcher partnerships.
It should take a maximum of 10-15 minutes to complete this survey.
PARTICIPATION: Your participation in this survey is voluntary. You may refuse to take part in
the research or exit the survey at any time without penalty. You are free to decline to answer any
particular question you do not wish to answer for any reason. If you would like to exclude your
responses from the study please contact us within 2 weeks and we will delete them.
BENEFITS: You will receive no direct benefits from participating in this research study.
However, your responses may help us learn more about a website about patient-researcher
partnerships.
RISKS: There are no foreseeable risks involved in participating in this study.
CONFIDENTIALITY: The email address that you have already provided to the research team
will only be accessed by the principal investigator (PI) and student PI. It will only be used for the
purposes of follow-up communication, after which your e-mail will be deleted. No names or
identifying information will be included in any publications or presentations based on these data,
and your responses to this survey will remain confidential. Our records of participants' email
addresses will be stored securely on Trillium Health Partners servers (accessible only to the
research team) and will remain separate from your survey responses.
IP address tracking will be turned off on the survey tool. Survey responses from SurveyMonkey
are sent over a secure, SSL encrypted connection. Since SurveyMonkey is a company located in
the United States, USA authorities under the provisions of the Patriot Act may access the survey
data in rare instances.
CONTACT: If you have questions at any time about the study or the procedures, you may
contact the PI, Susan Law, via phone at (905) 848-7580 x1659 or email at [email protected].
If you feel you have not been treated according to the descriptions in this form, or that your
rights as a participant in research have not been honored during the course of this project, or you
have any questions, concerns, or complaints that you wish to address to someone other than the
investigator, you may contact either the Research Ethics Board at Trillium Health Partners at
Page 106 of 128
(905) 848-7580 ext.1682 or [email protected], OR the University of Toronto Review Ethics Board
at (416) 946-3273 or [email protected].
ELECTRONIC CONSENT: Please select your choice below. You may print a copy of this
consent form for your records.
Clicking on the "Agree" button indicates that:
• You have read the above information and fully understand the research that is being done and
what is being asked of you
• You voluntarily agree to participate in this study
• You understand that you may withdraw from the study at any time and your withdrawal does
not waive any of your legal rights, nor relieve the research team from any legal responsibility
• You are 18 years of age or older
Please indicate if you agree or disagree.
Agree
Disagree
Part 1
Approximately how much time did you spend on the website in total?
Less than 30 minutes
30 minutes to 1 hour
1 to 3 hours
3+ hours
Part 2
This section is about your thoughts about the website. Please answer as best you can even if you
have no prior experience with patient-researcher partnerships.
Note: For the purposes of this study, we are defining patient-researcher partnerships as activities
where patients and/or caregivers and researchers are working together in any or all aspects of
planning studies, reviewing literature, collecting and analyzing data/information and/or
disseminating the results of research.
Page 107 of 128
2.10 The website encourages me to take actions to become a patient-researcher partner.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.11 The website has a positive outlook.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.12 The information on the website left me feeling confused.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.13 The website includes useful tips on how to be a better patient-researcher partner.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.14 The website provides a wide range of information.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.15 The language on the website made it easy to understand.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.16 I feel more inclined to participate in a patient-researcher partnership after visiting the
website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.17 I have learnt something new from the website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.18 I can easily understand the information on the website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.19 The website prepares me for what might happen in a patient-researcher partnership.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.20 The people who have contributed to the website understand what is important to me.
Strongly Disagree 1 2 3 4 5 Strongly Agree
Page 108 of 128
2.21 I trust the information on the website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.22 I would consult the website if I had to make a decision about whether or not to be part of a
patient-researcher partnership.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.23 I feel I have a sense of solidarity with people on the website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.24 I can identify with people on the website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.25 On the whole, I find the website reassuring.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.26 I value the advice given on the website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.27 The website gives me the confidence that I am able to participate in a patient-researcher
partnership.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.28 I feel like I have a lot in common with people on the website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.29 The website gives me the confidence to explain my involvement in research to others.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.30 The website helps me to have a better understanding of patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 Strongly Agree
Page 109 of 128
2.31 The website encourages me to play a more active role as a patient-researcher partner.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.32 The website makes me more confident to discuss my partnership experience with the
people around me (for example, my family or people at work).
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.33 Videos were used appropriately on the website.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.34 I found the stories or other content on the website distressing or worrisome.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.35 The website is easy to use.
Strongly Disagree 1 2 3 4 5 Strongly Agree
2.36 Any other comments you would like to add about the website and/or the use of video
narratives?
___________________________________________________________________________
___________________________________________________________________________
Part 3
This section asks about your thoughts and attitudes toward patient-researcher partnerships after
spending time on the website (note: many questions are the same as in the last survey). Please
answer as best you can even if you have no prior experience with patient-researcher partnerships.
Note: For the purposes of this study, we are defining patient-researcher partnerships as activities
where patients and/or caregivers and researchers are working together in any or all aspects of
planning studies, reviewing literature, collecting and analyzing data/information and/or
disseminating the results of research.
3.17 I want to engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
Page 110 of 128
3.18 I intend to engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.19 Did the website influence whether or not you want to engage in a patient-researcher
partnership in the future? Why or why not?
___________________________________________________________________________
___________________________________________________________________________
3.20 Did the website influence whether or not you think you are going to engage in a patient-
researcher partnership in the future? Why or why not?
___________________________________________________________________________
___________________________________________________________________________
3.21 Patient-researcher partnerships are, or would be…
Very Harmful 1 2 3 4 5 6 7 Very Beneficial
Very Unpleasant 1 2 3 4 5 6 7 Very Pleasant
(for me) (for me)
Very Unhelpful 1 2 3 4 5 6 7 Very Helpful
3.22 Did the website change how you feel about patient-researcher partnerships? Why or why
not? If so, how?
___________________________________________________________________________
___________________________________________________________________________
3.23 It is expected of me that I engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.24 I feel under social pressure to engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
Page 111 of 128
3.25 People who are important to me want me to engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.26 I am confident that I could engage in patient-researcher partnerships.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.27 For me to engage in patient-researcher partnerships is, or would be…
Very Difficult 1 2 3 4 5 6 7 Very Easy
3.28 Did the website change how confident you feel about engaging in partnerships? If so, how?
___________________________________________________________________________
___________________________________________________________________________
3.29 The decision to engage in patient-researcher partnerships is beyond my control.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.30 Whether or not I engage in patient-researcher partnerships is entirely up to me.
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
3.31 Any other comments you would like to add?
___________________________________________________________________________
___________________________________________________________________________
Thank you for participating in this research!
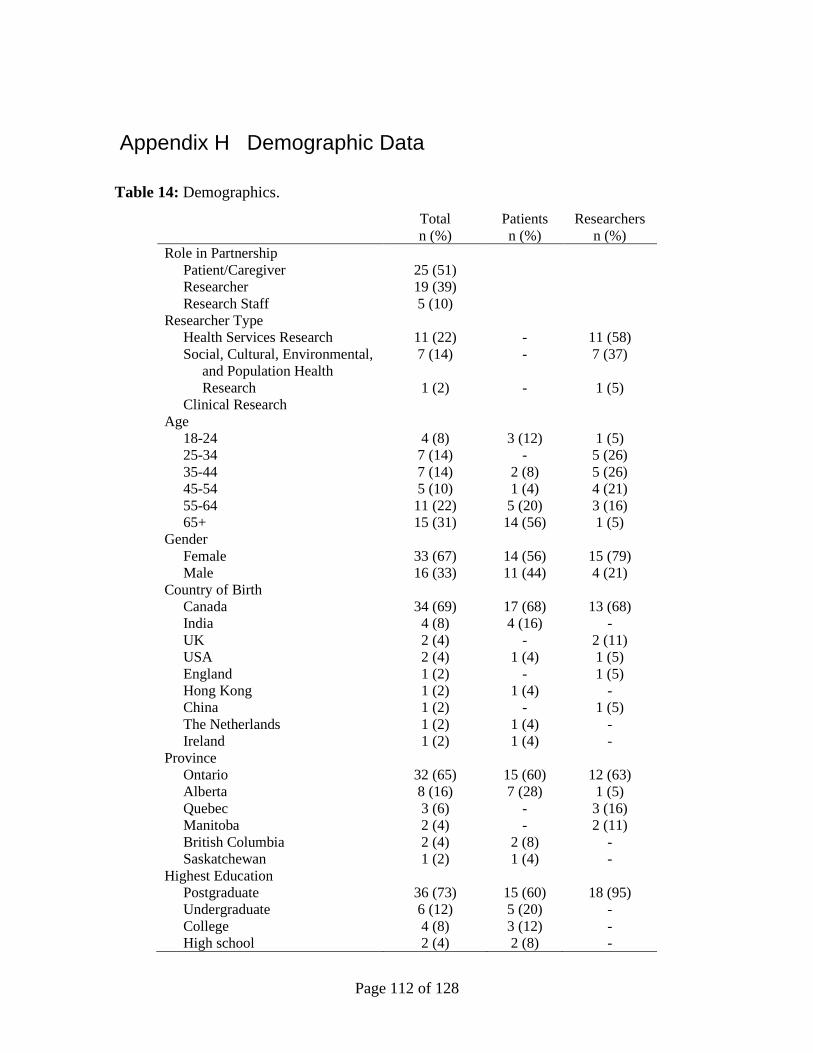
Page 112 of 128
Appendix H Demographic Data
Table 14: Demographics.
Total
n (%)
Patients
n (%)
Researchers
n (%)
Role in Partnership
Patient/Caregiver
Researcher
Research Staff
25 (51)
19 (39)
5 (10)
Researcher Type
Health Services Research
Social, Cultural, Environmental,
and Population Health
Research
Clinical Research
11 (22)
7 (14)
1 (2)
-
-
-
11 (58)
7 (37)
1 (5)
Age
18-24
25-34
35-44
45-54
55-64
65+
4 (8)
7 (14)
7 (14)
5 (10)
11 (22)
15 (31)
3 (12)
-
2 (8)
1 (4)
5 (20)
14 (56)
1 (5)
5 (26)
5 (26)
4 (21)
3 (16)
1 (5)
Gender
Female
Male
33 (67)
16 (33)
14 (56)
11 (44)
15 (79)
4 (21)
Country of Birth
Canada
India
UK
USA
England
Hong Kong
China
The Netherlands
Ireland
34 (69)
4 (8)
2 (4)
2 (4)
1 (2)
1 (2)
1 (2)
1 (2)
1 (2)
17 (68)
4 (16)
-
1 (4)
-
1 (4)
-
1 (4)
1 (4)
13 (68)
-
2 (11)
1 (5)
1 (5)
-
1 (5)
-
-
Province
Ontario
Alberta
Quebec
Manitoba
British Columbia
Saskatchewan
32 (65)
8 (16)
3 (6)
2 (4)
2 (4)
1 (2)
15 (60)
7 (28)
-
-
2 (8)
1 (4)
12 (63)
1 (5)
3 (16)
2 (11)
-
-
Highest Education
Postgraduate
Undergraduate
College
High school
36 (73)
6 (12)
4 (8)
2 (4)
15 (60)
5 (20)
3 (12)
2 (8)
18 (95)
-
-
-
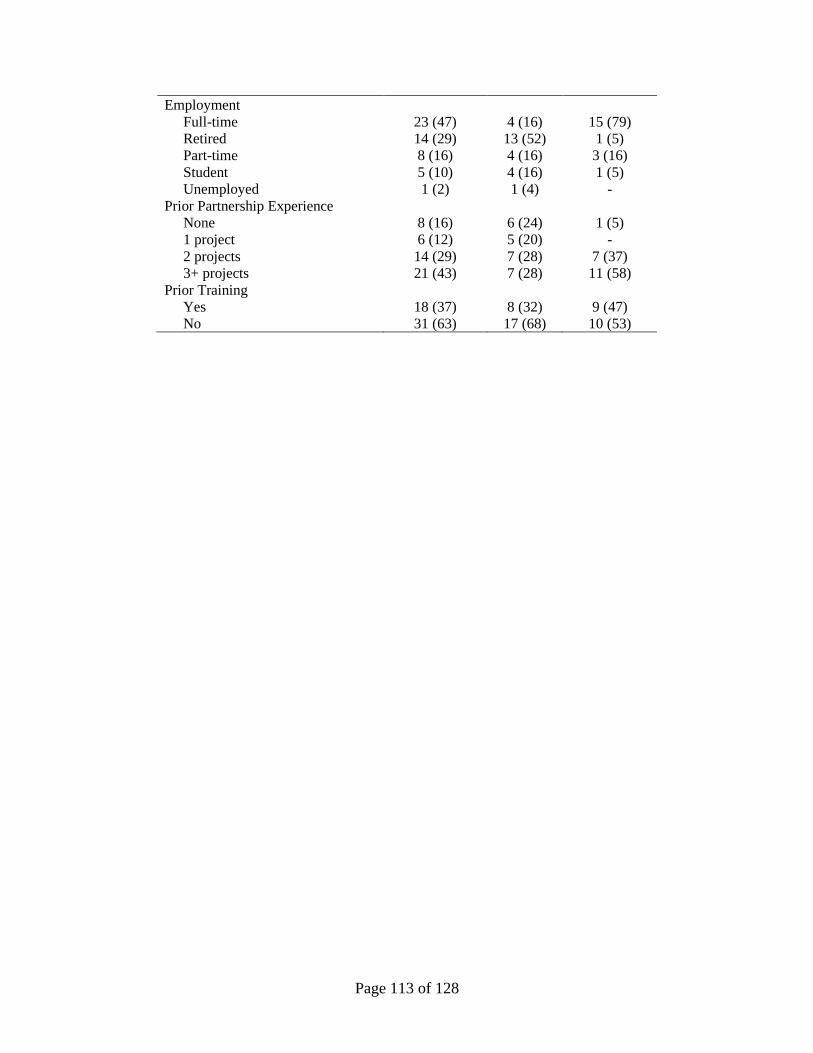
Page 113 of 128
Employment
Full-time
Retired
Part-time
Student
Unemployed
23 (47)
14 (29)
8 (16)
5 (10)
1 (2)
4 (16)
13 (52)
4 (16)
4 (16)
1 (4)
15 (79)
1 (5)
3 (16)
1 (5)
-
Prior Partnership Experience
None
1 project
2 projects
3+ projects
8 (16)
6 (12)
14 (29)
21 (43)
6 (24)
5 (20)
7 (28)
7 (28)
1 (5)
-
7 (37)
11 (58)
Prior Training
Yes
No
18 (37)
31 (63)
8 (32)
17 (68)
9 (47)
10 (53)
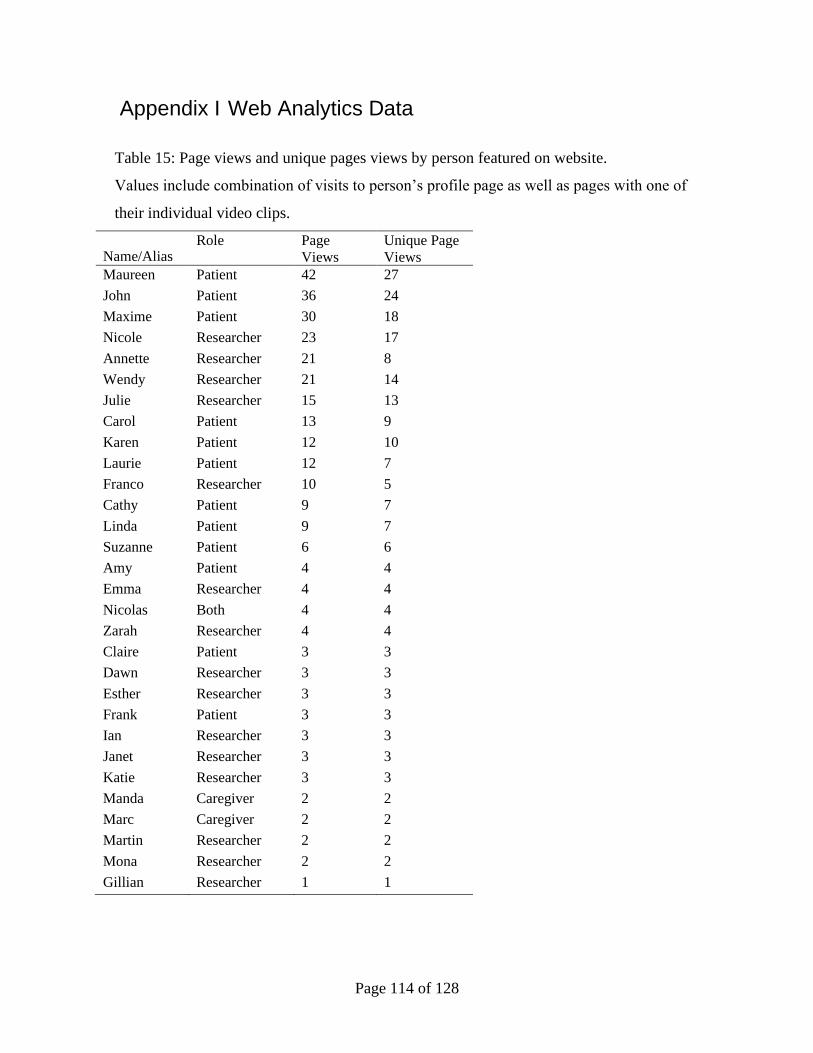
Page 114 of 128
Appendix I Web Analytics Data
Table 15: Page views and unique pages views by person featured on website.
Values include combination of visits to person’s profile page as well as pages with one of
their individual video clips.
Name/Alias Role Page
Views
Unique Page
Views
Maureen Patient 42 27
John Patient 36 24
Maxime Patient 30 18
Nicole Researcher 23 17
Annette Researcher 21 8
Wendy Researcher 21 14
Julie Researcher 15 13
Carol Patient 13 9
Karen Patient 12 10
Laurie Patient 12 7
Franco Researcher 10 5
Cathy Patient 9 7
Linda Patient 9 7
Suzanne Patient 6 6
Amy Patient 4 4
Emma Researcher 4 4
Nicolas Both 4 4
Zarah Researcher 4 4
Claire Patient 3 3
Dawn Researcher 3 3
Esther Researcher 3 3
Frank Patient 3 3
Ian Researcher 3 3
Janet Researcher 3 3
Katie Researcher 3 3
Manda Caregiver 2 2
Marc Caregiver 2 2
Martin Researcher 2 2
Mona Researcher 2 2
Gillian Researcher 1 1
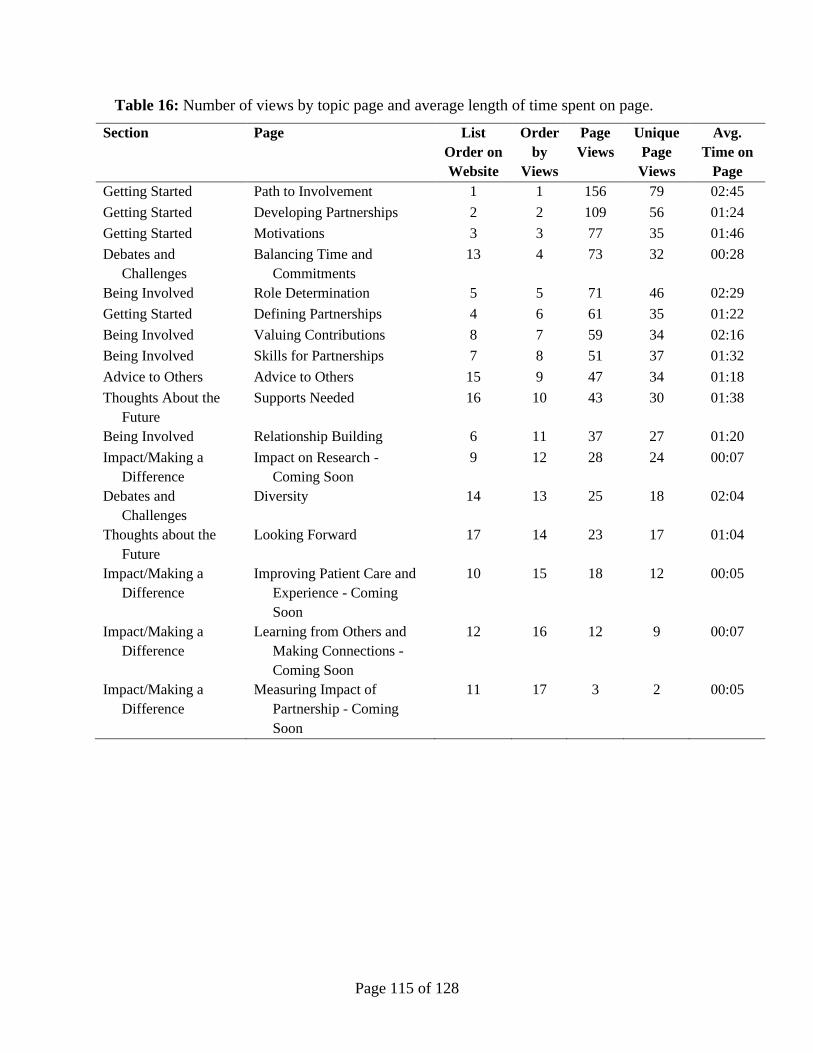
Page 115 of 128
Table 16: Number of views by topic page and average length of time spent on page.
Section Page List
Order on
Website
Order
by
Views
Page
Views
Unique
Page
Views
Avg.
Time on
Page
Getting Started Path to Involvement 1 1 156 79 02:45
Getting Started Developing Partnerships 2 2 109 56 01:24
Getting Started Motivations 3 3 77 35 01:46
Debates and
Challenges
Balancing Time and
Commitments
13 4 73 32 00:28
Being Involved Role Determination 5 5 71 46 02:29
Getting Started Defining Partnerships 4 6 61 35 01:22
Being Involved Valuing Contributions 8 7 59 34 02:16
Being Involved Skills for Partnerships 7 8 51 37 01:32
Advice to Others Advice to Others 15 9 47 34 01:18
Thoughts About the
Future
Supports Needed 16 10 43 30 01:38
Being Involved Relationship Building 6 11 37 27 01:20
Impact/Making a
Difference
Impact on Research -
Coming Soon
9 12 28 24 00:07
Debates and
Challenges
Diversity 14 13 25 18 02:04
Thoughts about the
Future
Looking Forward 17 14 23 17 01:04
Impact/Making a
Difference
Improving Patient Care and
Experience - Coming
Soon
10 15 18 12 00:05
Impact/Making a
Difference
Learning from Others and
Making Connections -
Coming Soon
12 16 12 9 00:07
Impact/Making a
Difference
Measuring Impact of
Partnership - Coming
Soon
11 17 3 2 00:05
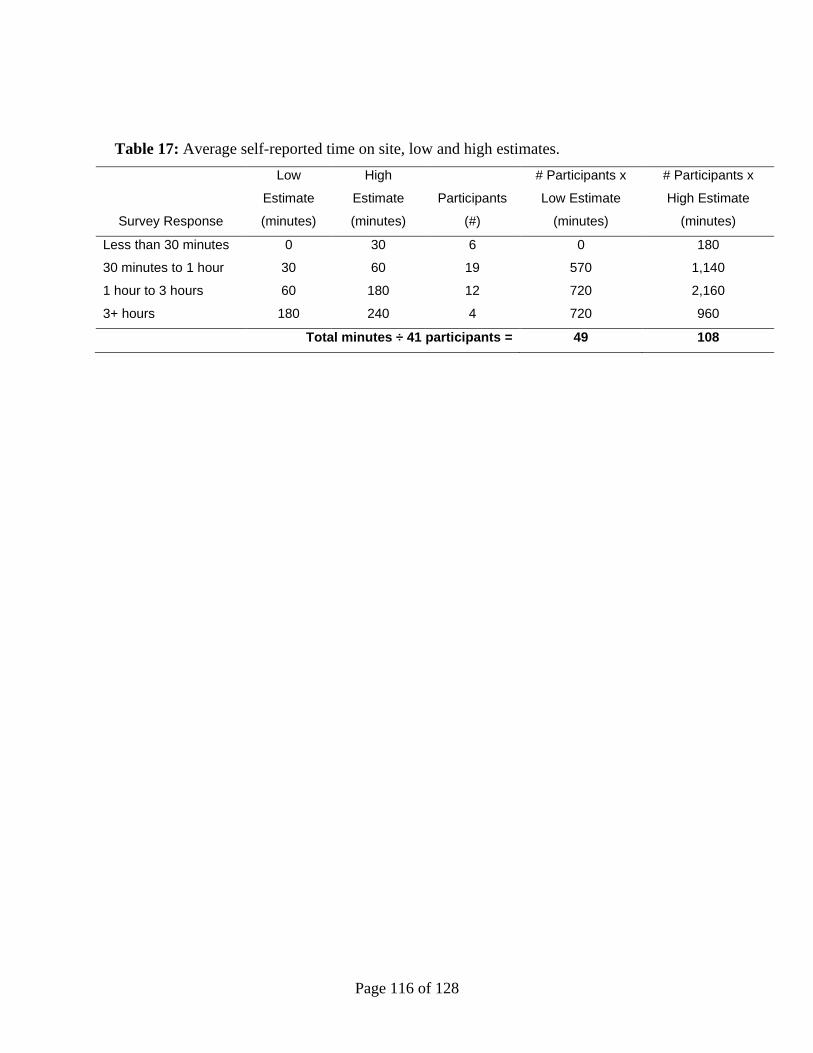
Page 116 of 128
Table 17: Average self-reported time on site, low and high estimates.
Survey Response
Low
Estimate
(minutes)
High
Estimate
(minutes)
Participants
(#)
# Participants x
Low Estimate
(minutes)
# Participants x
High Estimate
(minutes)
Less than 30 minutes 0 30 6 0 180
30 minutes to 1 hour 30 60 19 570 1,140
1 hour to 3 hours 60 180 12 720 2,160
3+ hours 180 240 4 720 960
Total minutes ÷ 41 participants = 49 108
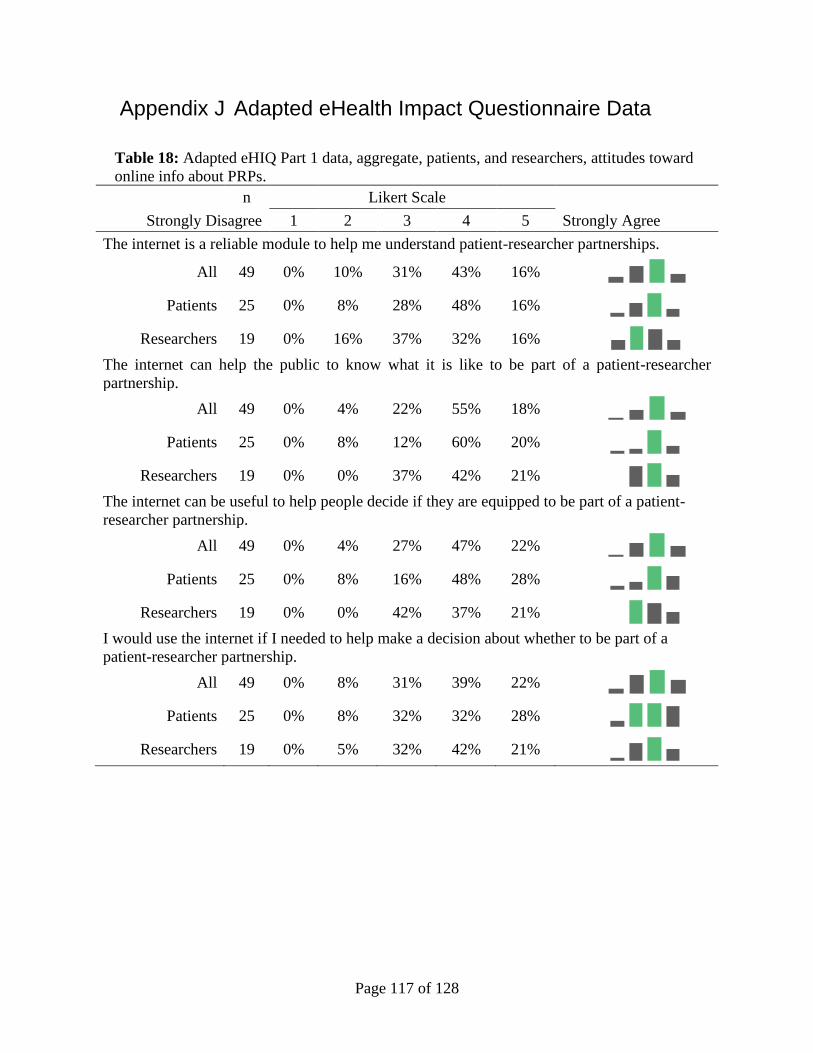
Page 117 of 128
Appendix J Adapted eHealth Impact Questionnaire Data
Table 18: Adapted eHIQ Part 1 data, aggregate, patients, and researchers, attitudes toward
online info about PRPs.
n Likert Scale
Strongly Disagree 1 2 3 4 5 Strongly Agree
The internet is a reliable module to help me understand patient-researcher partnerships.
All 49 0% 10% 31% 43% 16%
Patients 25 0% 8% 28% 48% 16%
Researchers 19 0% 16% 37% 32% 16%
The internet can help the public to know what it is like to be part of a patient-researcher
partnership.
All 49 0% 4% 22% 55% 18%
Patients 25 0% 8% 12% 60% 20%
Researchers 19 0% 0% 37% 42% 21%
The internet can be useful to help people decide if they are equipped to be part of a patient-
researcher partnership.
All 49 0% 4% 27% 47% 22%
Patients 25 0% 8% 16% 48% 28%
Researchers 19 0% 0% 42% 37% 21%
I would use the internet if I needed to help make a decision about whether to be part of a
patient-researcher partnership.
All 49 0% 8% 31% 39% 22%
Patients 25 0% 8% 32% 32% 28%
Researchers 19 0% 5% 32% 42% 21%
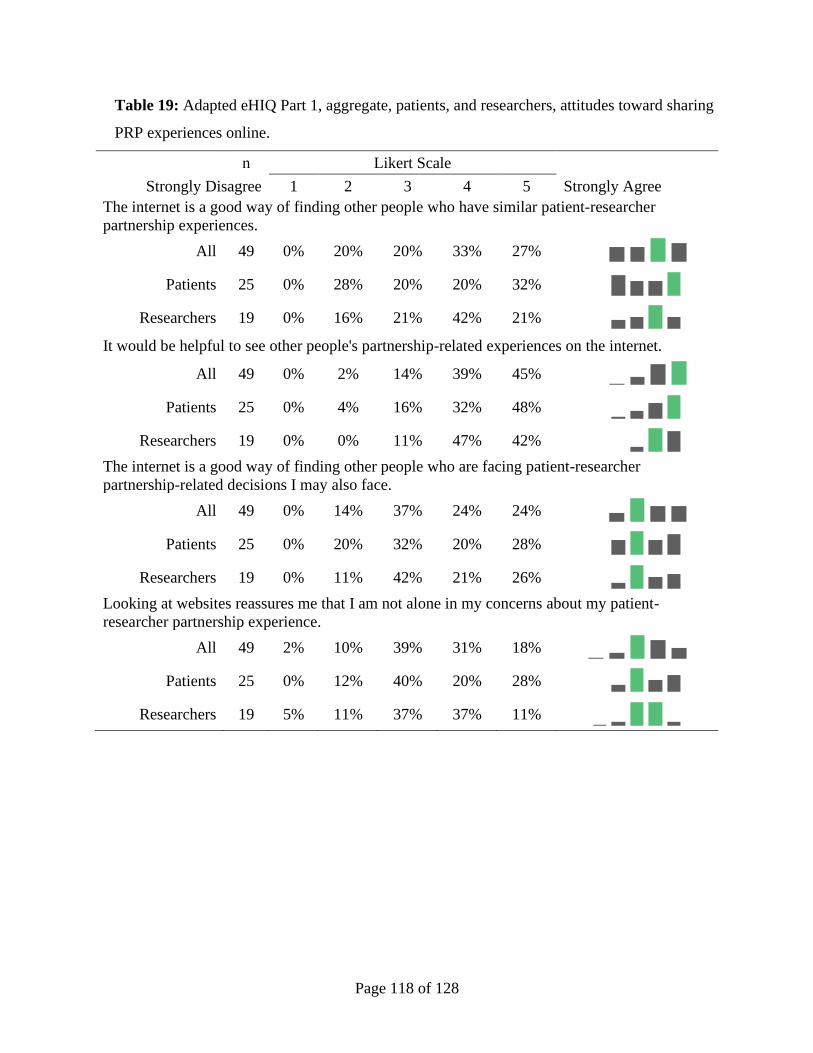
Page 118 of 128
Table 19: Adapted eHIQ Part 1, aggregate, patients, and researchers, attitudes toward sharing
PRP experiences online.
n Likert Scale
Strongly Disagree 1 2 3 4 5 Strongly Agree
The internet is a good way of finding other people who have similar patient-researcher
partnership experiences.
All 49 0% 20% 20% 33% 27%
Patients 25 0% 28% 20% 20% 32%
Researchers 19 0% 16% 21% 42% 21%
It would be helpful to see other people's partnership-related experiences on the internet.
All 49 0% 2% 14% 39% 45%
Patients 25 0% 4% 16% 32% 48%
Researchers 19 0% 0% 11% 47% 42%
The internet is a good way of finding other people who are facing patient-researcher
partnership-related decisions I may also face.
All 49 0% 14% 37% 24% 24%
Patients 25 0% 20% 32% 20% 28%
Researchers 19 0% 11% 42% 21% 26%
Looking at websites reassures me that I am not alone in my concerns about my patient-
researcher partnership experience.
All 49 2% 10% 39% 31% 18%
Patients 25 0% 12% 40% 20% 28%
Researchers 19 5% 11% 37% 37% 11%
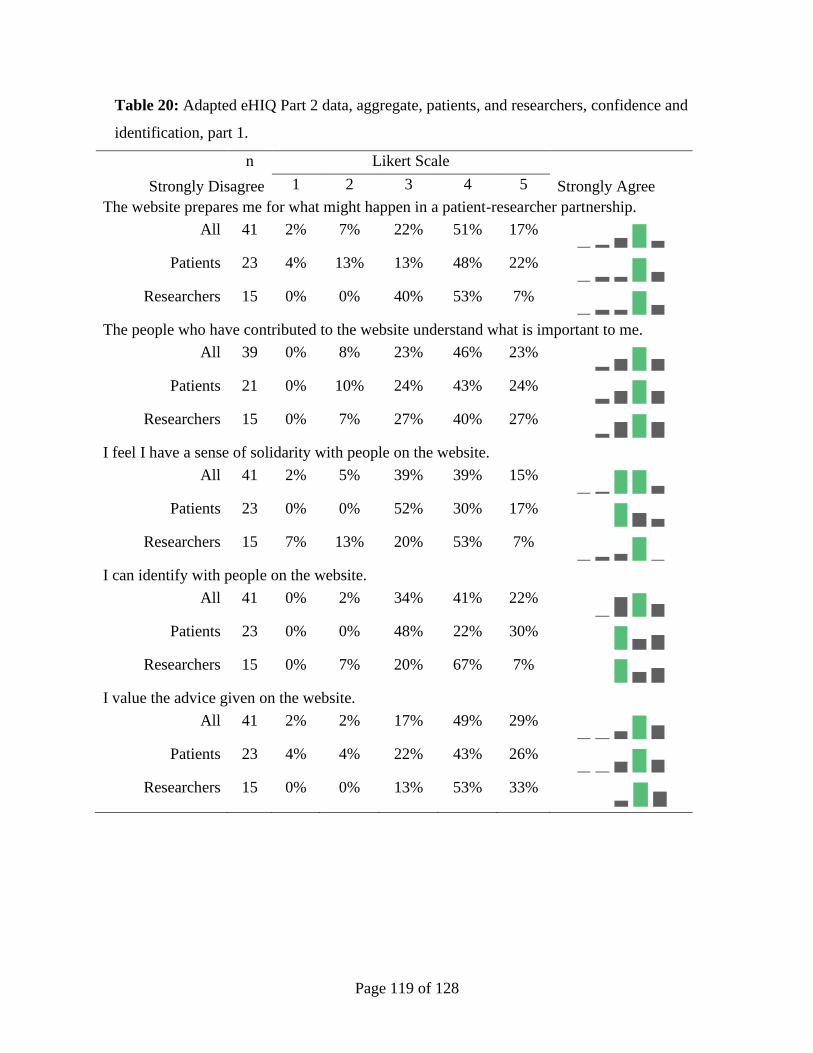
Page 119 of 128
Table 20: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, confidence and
identification, part 1.
n Likert Scale
Strongly Disagree 1 2 3 4 5 Strongly Agree
The website prepares me for what might happen in a patient-researcher partnership.
All 41 2% 7% 22% 51% 17%
Patients 23 4% 13% 13% 48% 22%
Researchers 15 0% 0% 40% 53% 7%
The people who have contributed to the website understand what is important to me.
All 39 0% 8% 23% 46% 23%
Patients 21 0% 10% 24% 43% 24%
Researchers 15 0% 7% 27% 40% 27%
I feel I have a sense of solidarity with people on the website.
All 41 2% 5% 39% 39% 15%
Patients 23 0% 0% 52% 30% 17%
Researchers 15 7% 13% 20% 53% 7%
I can identify with people on the website.
All 41 0% 2% 34% 41% 22%
Patients 23 0% 0% 48% 22% 30%
Researchers 15 0% 7% 20% 67% 7%
I value the advice given on the website.
All 41 2% 2% 17% 49% 29%
Patients 23 4% 4% 22% 43% 26%
Researchers 15 0% 0% 13% 53% 33%
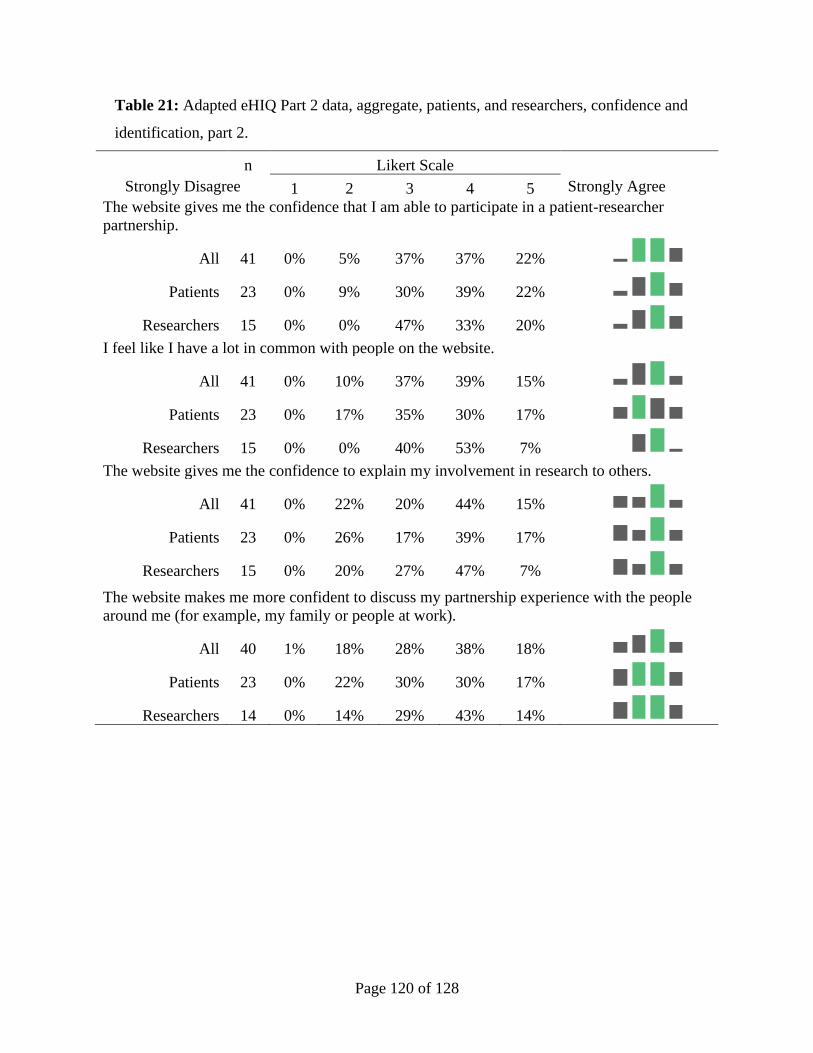
Page 120 of 128
Table 21: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, confidence and
identification, part 2.
n Likert Scale
Strongly Disagree 1 2 3 4 5 Strongly Agree
The website gives me the confidence that I am able to participate in a patient-researcher
partnership.
All 41 0% 5% 37% 37% 22%
Patients 23 0% 9% 30% 39% 22%
Researchers 15 0% 0% 47% 33% 20%
I feel like I have a lot in common with people on the website.
All 41 0% 10% 37% 39% 15%
Patients 23 0% 17% 35% 30% 17%
Researchers 15 0% 0% 40% 53% 7%
The website gives me the confidence to explain my involvement in research to others.
All 41 0% 22% 20% 44% 15%
Patients 23 0% 26% 17% 39% 17%
Researchers 15 0% 20% 27% 47% 7%
The website makes me more confident to discuss my partnership experience with the people
around me (for example, my family or people at work).
All 40 1% 18% 28% 38% 18%
Patients 23 0% 22% 30% 30% 17%
Researchers 14 0% 14% 29% 43% 14%
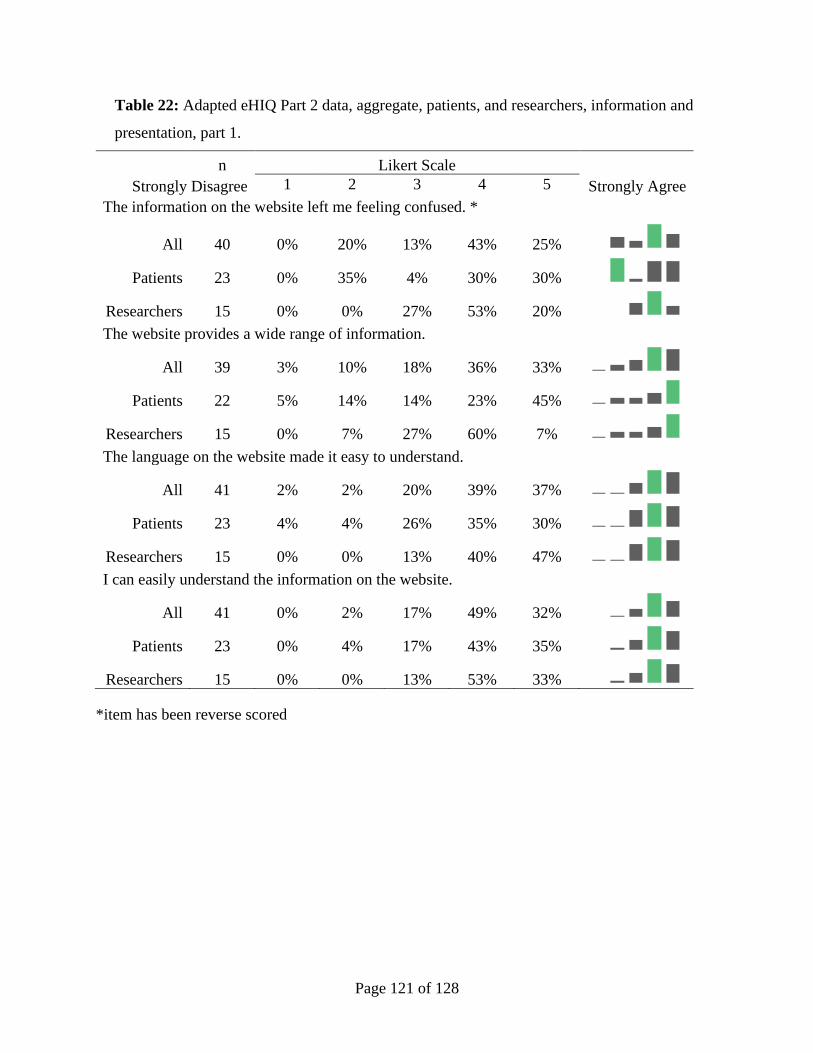
Page 121 of 128
Table 22: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, information and
presentation, part 1.
n Likert Scale
Strongly Disagree 1 2 3 4 5 Strongly Agree
The information on the website left me feeling confused. *
All 40 0% 20% 13% 43% 25%
Patients 23 0% 35% 4% 30% 30%
Researchers 15 0% 0% 27% 53% 20%
The website provides a wide range of information.
All 39 3% 10% 18% 36% 33%
Patients 22 5% 14% 14% 23% 45%
Researchers 15 0% 7% 27% 60% 7%
The language on the website made it easy to understand.
All 41 2% 2% 20% 39% 37%
Patients 23 4% 4% 26% 35% 30%
Researchers 15 0% 0% 13% 40% 47%
I can easily understand the information on the website.
All 41 0% 2% 17% 49% 32%
Patients 23 0% 4% 17% 43% 35%
Researchers 15 0% 0% 13% 53% 33%
*item has been reverse scored
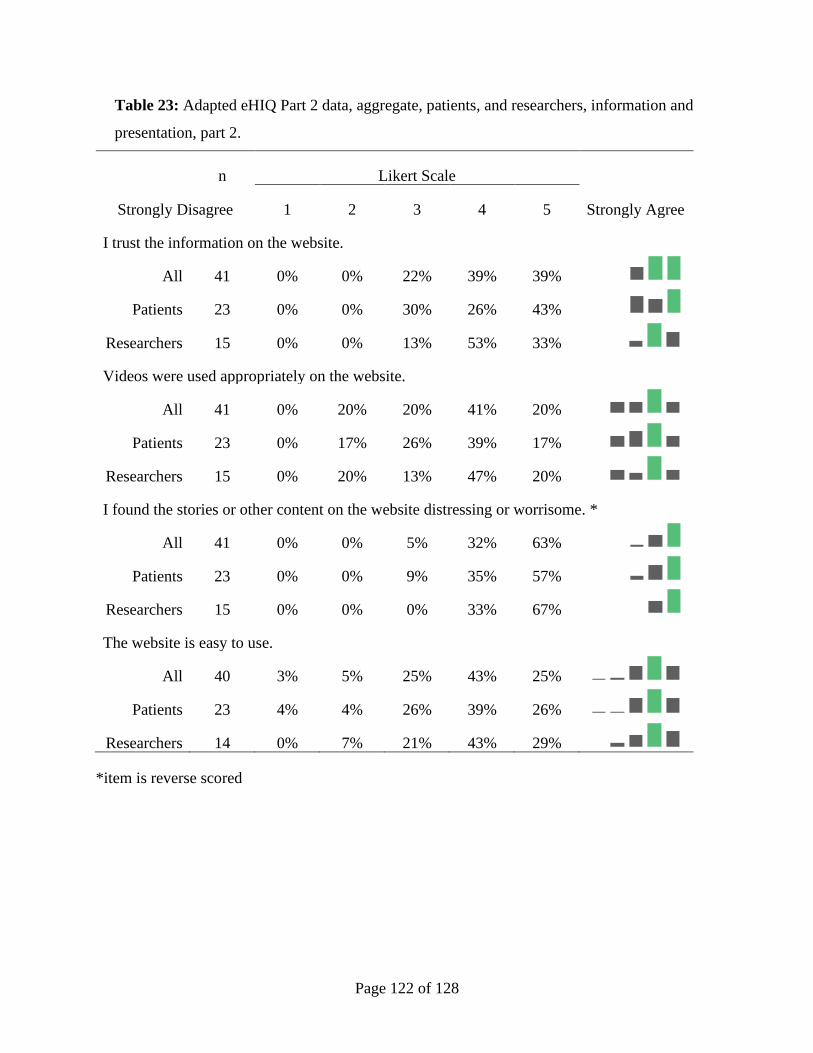
Page 122 of 128
Table 23: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, information and
presentation, part 2.
n Likert Scale
Strongly Disagree 1 2 3 4 5 Strongly Agree
I trust the information on the website.
All 41 0% 0% 22% 39% 39%
Patients 23 0% 0% 30% 26% 43%
Researchers 15 0% 0% 13% 53% 33%
Videos were used appropriately on the website.
All 41 0% 20% 20% 41% 20%
Patients 23 0% 17% 26% 39% 17%
Researchers 15 0% 20% 13% 47% 20%
I found the stories or other content on the website distressing or worrisome. *
All 41 0% 0% 5% 32% 63%
Patients 23 0% 0% 9% 35% 57%
Researchers 15 0% 0% 0% 33% 67%
The website is easy to use.
All 40 3% 5% 25% 43% 25%
Patients 23 4% 4% 26% 39% 26%
Researchers 14 0% 7% 21% 43% 29%
*item is reverse scored
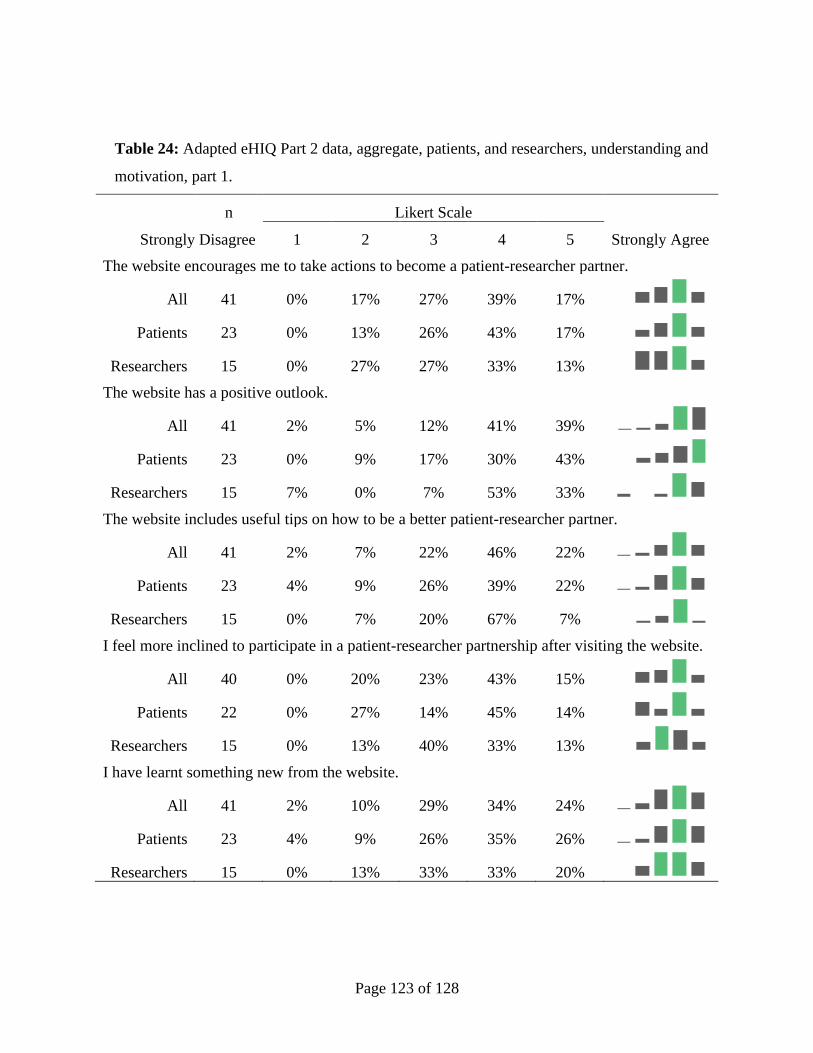
Page 123 of 128
Table 24: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, understanding and
motivation, part 1.
n Likert Scale
Strongly Disagree 1 2 3 4 5 Strongly Agree
The website encourages me to take actions to become a patient-researcher partner.
All 41 0% 17% 27% 39% 17%
Patients 23 0% 13% 26% 43% 17%
Researchers 15 0% 27% 27% 33% 13%
The website has a positive outlook.
All 41 2% 5% 12% 41% 39%
Patients 23 0% 9% 17% 30% 43%
Researchers 15 7% 0% 7% 53% 33%
The website includes useful tips on how to be a better patient-researcher partner.
All 41 2% 7% 22% 46% 22%
Patients 23 4% 9% 26% 39% 22%
Researchers 15 0% 7% 20% 67% 7%
I feel more inclined to participate in a patient-researcher partnership after visiting the website.
All 40 0% 20% 23% 43% 15%
Patients 22 0% 27% 14% 45% 14%
Researchers 15 0% 13% 40% 33% 13%
I have learnt something new from the website.
All 41 2% 10% 29% 34% 24%
Patients 23 4% 9% 26% 35% 26%
Researchers 15 0% 13% 33% 33% 20%
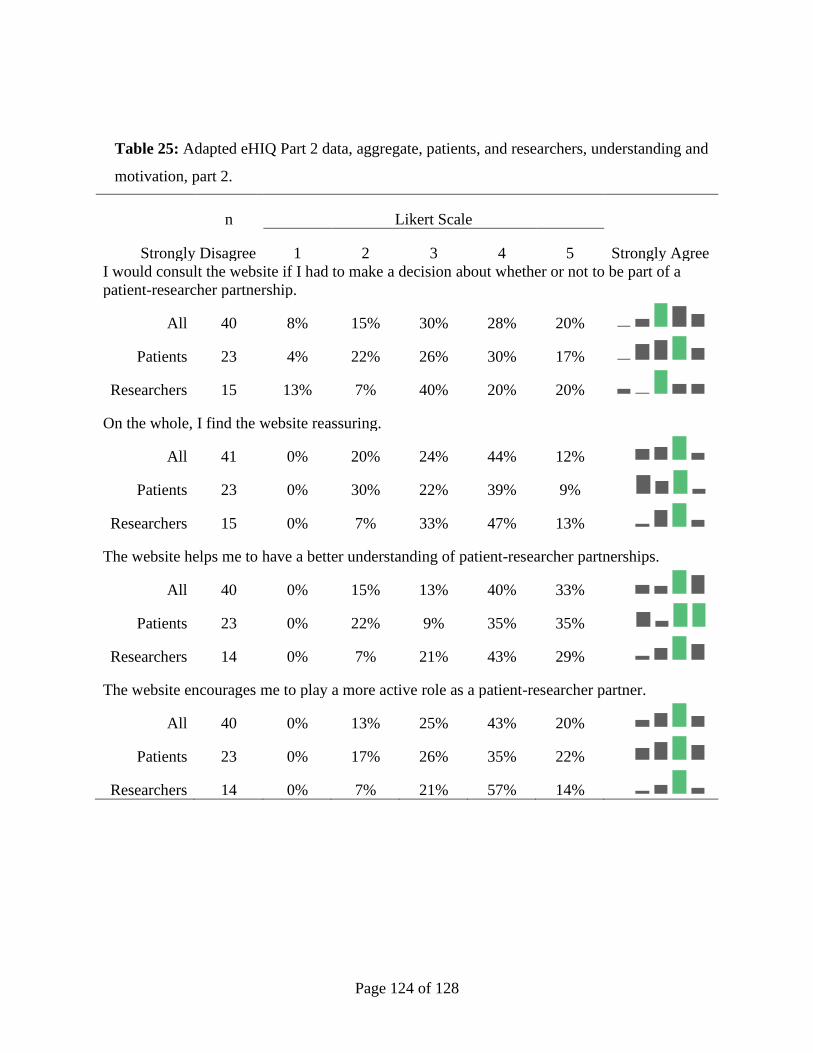
Page 124 of 128
Table 25: Adapted eHIQ Part 2 data, aggregate, patients, and researchers, understanding and
motivation, part 2.
n Likert Scale
Strongly Disagree 1 2 3 4 5 Strongly Agree
I would consult the website if I had to make a decision about whether or not to be part of a
patient-researcher partnership.
All 40 8% 15% 30% 28% 20%
Patients 23 4% 22% 26% 30% 17%
Researchers 15 13% 7% 40% 20% 20%
On the whole, I find the website reassuring.
All 41 0% 20% 24% 44% 12%
Patients 23 0% 30% 22% 39% 9%
Researchers 15 0% 7% 33% 47% 13%
The website helps me to have a better understanding of patient-researcher partnerships.
All 40 0% 15% 13% 40% 33%
Patients 23 0% 22% 9% 35% 35%
Researchers 14 0% 7% 21% 43% 29%
The website encourages me to play a more active role as a patient-researcher partner.
All 40 0% 13% 25% 43% 20%
Patients 23 0% 17% 26% 35% 22%
Researchers 14 0% 7% 21% 57% 14%
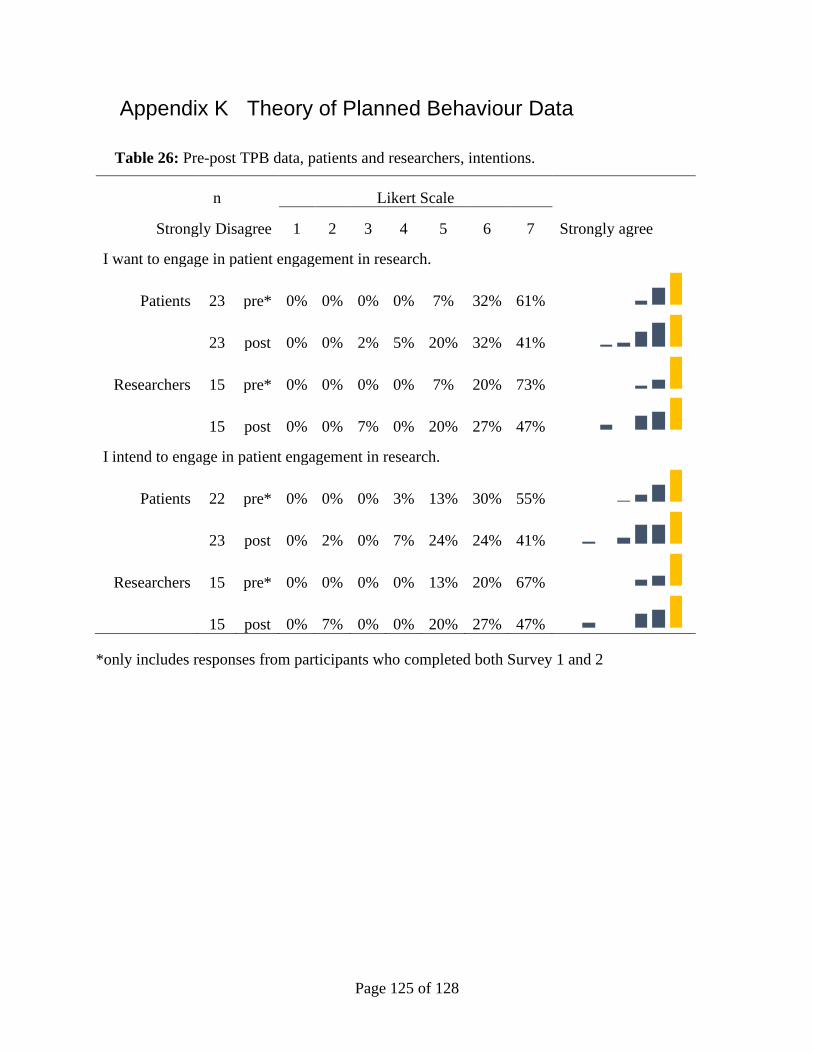
Page 125 of 128
Appendix K Theory of Planned Behaviour Data
Table 26: Pre-post TPB data, patients and researchers, intentions.
n Likert Scale
Strongly Disagree 1 2 3 4 5 6 7 Strongly agree
I want to engage in patient engagement in research.
Patients 23 pre* 0% 0% 0% 0% 7% 32% 61%
23 post 0% 0% 2% 5% 20% 32% 41%
Researchers 15 pre* 0% 0% 0% 0% 7% 20% 73%
15 post 0% 0% 7% 0% 20% 27% 47%
I intend to engage in patient engagement in research.
Patients 22 pre* 0% 0% 0% 3% 13% 30% 55%
23 post 0% 2% 0% 7% 24% 24% 41%
Researchers 15 pre* 0% 0% 0% 0% 13% 20% 67%
15 post 0% 7% 0% 0% 20% 27% 47%
*only includes responses from participants who completed both Survey 1 and 2
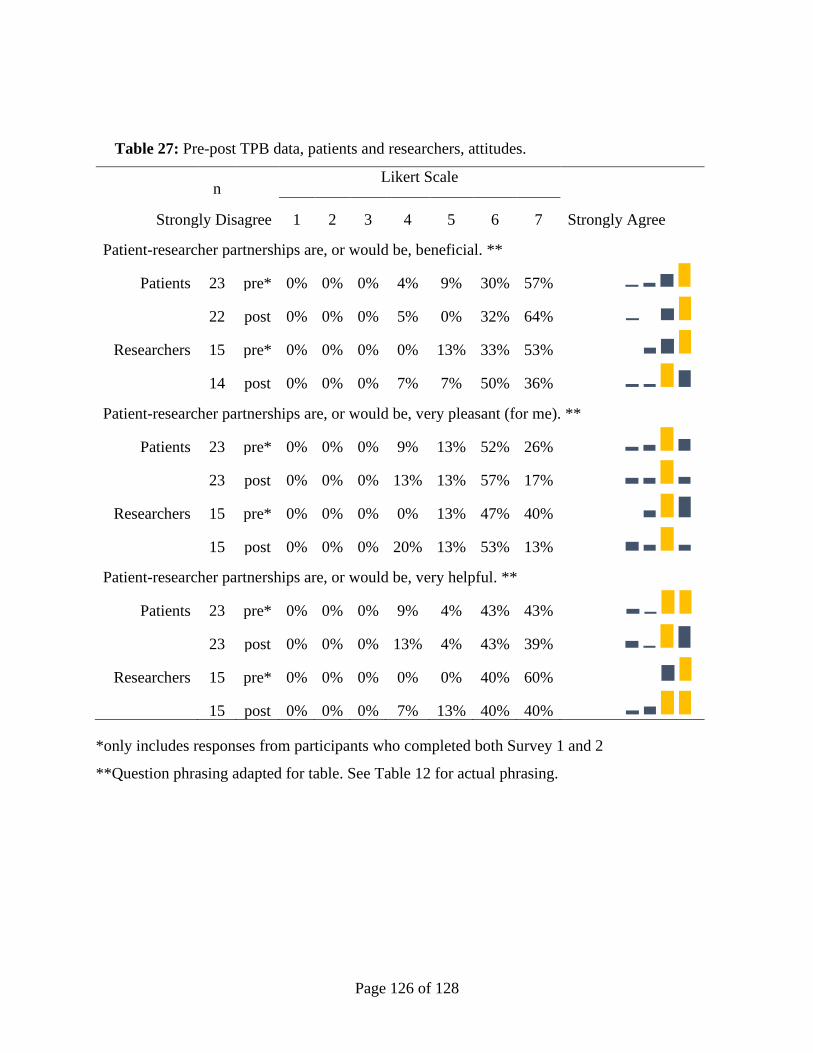
Page 126 of 128
Table 27: Pre-post TPB data, patients and researchers, attitudes.
n
Likert Scale
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
Patient-researcher partnerships are, or would be, beneficial. **
Patients 23 pre* 0% 0% 0% 4% 9% 30% 57%
22 post 0% 0% 0% 5% 0% 32% 64%
Researchers 15 pre* 0% 0% 0% 0% 13% 33% 53%
14 post 0% 0% 0% 7% 7% 50% 36%
Patient-researcher partnerships are, or would be, very pleasant (for me). **
Patients 23 pre* 0% 0% 0% 9% 13% 52% 26%
23 post 0% 0% 0% 13% 13% 57% 17%
Researchers 15 pre* 0% 0% 0% 0% 13% 47% 40%
15 post 0% 0% 0% 20% 13% 53% 13%
Patient-researcher partnerships are, or would be, very helpful. **
Patients 23 pre* 0% 0% 0% 9% 4% 43% 43%
23 post 0% 0% 0% 13% 4% 43% 39%
Researchers 15 pre* 0% 0% 0% 0% 0% 40% 60%
15 post 0% 0% 0% 7% 13% 40% 40%
*only includes responses from participants who completed both Survey 1 and 2
**Question phrasing adapted for table. See Table 12 for actual phrasing.
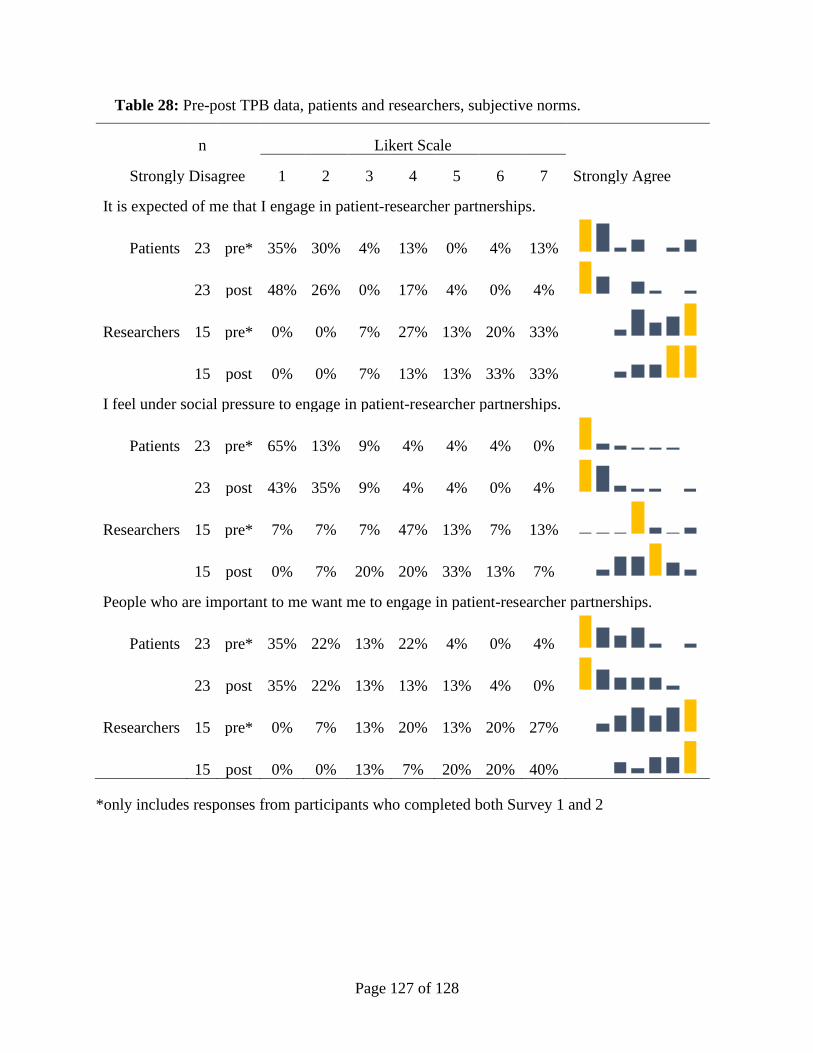
Page 127 of 128
Table 28: Pre-post TPB data, patients and researchers, subjective norms.
n Likert Scale
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
It is expected of me that I engage in patient-researcher partnerships.
Patients 23 pre* 35% 30% 4% 13% 0% 4% 13%
23 post 48% 26% 0% 17% 4% 0% 4%
Researchers 15 pre* 0% 0% 7% 27% 13% 20% 33%
15 post 0% 0% 7% 13% 13% 33% 33%
I feel under social pressure to engage in patient-researcher partnerships.
Patients 23 pre* 65% 13% 9% 4% 4% 4% 0%
23 post 43% 35% 9% 4% 4% 0% 4%
Researchers 15 pre* 7% 7% 7% 47% 13% 7% 13%
15 post 0% 7% 20% 20% 33% 13% 7%
People who are important to me want me to engage in patient-researcher partnerships.
Patients 23 pre* 35% 22% 13% 22% 4% 0% 4%
23 post 35% 22% 13% 13% 13% 4% 0%
Researchers 15 pre* 0% 7% 13% 20% 13% 20% 27%
15 post 0% 0% 13% 7% 20% 20% 40%
*only includes responses from participants who completed both Survey 1 and 2
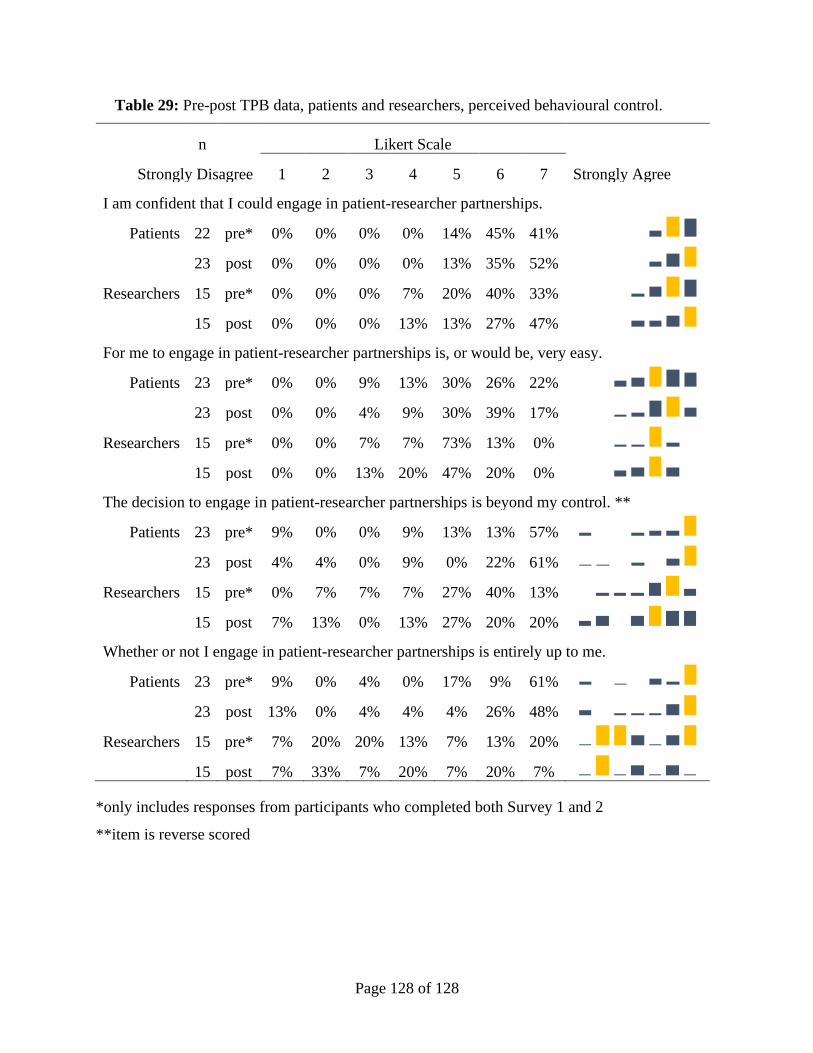
Page 128 of 128
Table 29: Pre-post TPB data, patients and researchers, perceived behavioural control.
n Likert Scale
Strongly Disagree 1 2 3 4 5 6 7 Strongly Agree
I am confident that I could engage in patient-researcher partnerships.
Patients 22 pre* 0% 0% 0% 0% 14% 45% 41%
23 post 0% 0% 0% 0% 13% 35% 52%
Researchers 15 pre* 0% 0% 0% 7% 20% 40% 33%
15 post 0% 0% 0% 13% 13% 27% 47%
For me to engage in patient-researcher partnerships is, or would be, very easy.
Patients 23 pre* 0% 0% 9% 13% 30% 26% 22%
23 post 0% 0% 4% 9% 30% 39% 17%
Researchers 15 pre* 0% 0% 7% 7% 73% 13% 0%
15 post 0% 0% 13% 20% 47% 20% 0%
The decision to engage in patient-researcher partnerships is beyond my control. **
Patients 23 pre* 9% 0% 0% 9% 13% 13% 57%
23 post 4% 4% 0% 9% 0% 22% 61%
Researchers 15 pre* 0% 7% 7% 7% 27% 40% 13%
15 post 7% 13% 0% 13% 27% 20% 20%
Whether or not I engage in patient-researcher partnerships is entirely up to me.
Patients 23 pre* 9% 0% 4% 0% 17% 9% 61%
23 post 13% 0% 4% 4% 4% 26% 48%
Researchers 15 pre* 7% 20% 20% 13% 7% 13% 20%
15 post 7% 33% 7% 20% 7% 20% 7%
*only includes responses from participants who completed both Survey 1 and 2
**item is reverse scored





























