Embed Size (px)
Citation preview

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 1 -
PATRON: Steve McNaughton, BE (NSW)
Volume 17 Number 2
The Hypoglycemic Health Association
Phone: (02) 9553-0084, Fax: (02) 9588-5290
PRESIDENT: Dr George SamraSecretary: Nicole SamraTreasurer: Sue LitchfieldEditor: Jurriaan Plesman, B.A. (Psych), Post. Grad. Dip. Clin. Nutr.
Steering CommitteeMembers:
Auditor: Hugh D Macfarlane, Chartered Accountant
The NEWSLETTER of the Hypoglycemic Health Association is distributed to members of the Associationand to Health Professionals with an interest in nutritional medicine and clinical ecology.
Catering Committee: Reg & Lynnette Grady
Dr Katrina WatsonJoy SharpTed Grant
Our Next Public Meeting will be at 2.00 PM
on Saturday, the 2 June, 2001
at YWCA
5-11Wentworth Ave, SYDNEY
and our guest speaker is
Dr Ramesh Manocha
who will be speaking
on the subject of
“Why Meditation?”
Correspondence: THE HYPOGLYCEMIC HEALTH ASSOCIATION, P.O. BOX 830, KOGARAH, N.S.W. 1485
NEWSLETTERJune 2001
ABN: 65-846-851-613Registered Charity CFN 16689
Dr Ramesh Manocha, from the naturaltherapy Unit of the Royal Hospital for Womenat Randwick, obtained his medical degree in1994. He has worked in several Sydney hospi-tals in various capacities. Following receipt ofseveral grants he is conducting research intoStress Management for Asthma, Daily Migraineand relaxation, Meditation for Menopausal HotFlushes, Brain imaging elite meditators, Emo-tional Intelligence, Meditation for OccupationalStress and the effects of Brahmi on Brain Func-tion.
Dr Manocha is a well-known speaker onnatural health covering areas of Stress Manage-ment for GPs and nurses, midwives and present-ing a holistic approach for many degenerativedisease, such osteoarthritis and cancer.
His main interest is the influence of medita-tion on health and we are pleased to have DrRamesh Manocha give a talk on this fascinatingtopic.
This year we are very lucky that the Association have been blessed with donations from enthusiastic supporters. This has made our accountslook pretty good. However, it would be a great mistake to rest on our laurels. In fact, membership has declined to a point that without the generousdonors we would be strapped for cash. We can not rely on donations alone and we need the support of paying members to pursue our aimsto educate the public and professionals of hypoglycemia and related disorders. Presently, we are sending out Newsletters to a large numberof unfinancial members who may have overlooked to forward their membership fees to the Association. Please note the Expiry date on the right-hand top corner of your address label. At this time of the year it should show 31 December 2001. If you have forgotten to send in your fees,please fill in the Application Form on the last page of this Newsletter and forward it to the Association. Fees have been kept low despite risingcosts and they are: $20 p.a. and $15 for pensioners and students. Members are invited to encourage their friends to become memebrs of theAssociation.
Since the founding of this Association in 1985, we have made considerable progress in making the community aware of hypoglycemia andits allied disorders. In spite of accelerating social expenditure on medicine degenerative disease are on the rise; diabetes which is the follow-up disease of hypoglycemia has now been described in terms of an epidemic. There are approximately half a million Australians walking aboutwithout knowing that they are diabetic. This Association, dealing with the forerunner of diabetes, is in a unique position to turn this around. Thetelltales of this disease are in fact the hypoglycemic symptoms, and by treating these conditions we are as a matter of fact preventing the furtherdevelopment of not only diabetes, but other degenerative diseases. Therefore, your support will contribute to this turnaround.

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 2 -
Any opinion expressedin this Newsletter does notnecessarily reflect theviews of the Association.
Books for sale at the meetingSue Litchfield: SUE’S COOKBOOKDr George Samra's bookThe Hypoglycemic Connection(now out of print) is only available in
public libraries).Jurriaan Plesman: GETTING OFF THE
HOOKThis book is also available in most public
libraries (state and university). By buyingthis book at the meetings you are supporting
the Hypoglycemic Health Association.
The Newcastle branch of the Associationare still meeting with the assistance of BevCook. They now meet at ALL PURPOSECENTRE, Thorn Street, TORONTO. Turnright before lights at Police Station, the Centreis on the right next to Ambulance Station. Formeeting dates and information ring Mrs. BevCook at 02-4950-5876.
Entrance donations at meetings Entry donation is tax deductible and for
non-members will be $5, for members $3 andfamily $5. People requiring a receipt for taxa-tion purposes will be issued when asked for it.
Donations for raffleOne way of increasing our income is by
way of raffles. If any member has anything todonate towards the raffle, please contact DrGeorge Samra’s surgery at 19 Princes High-way, Kogarah, Phone 9553-0084 or Sue Litchfieldat 9971-5657 or ([email protected]).
At the last meeting on the 3 March 2001,Jadzig Bzowska won the lucky door prize.This consisted of a frame with an beautifullyembroidered picture made and donated byMarie Grady of Canberra. The Association
thanks her very much for her lovely donation.Marie Grady is the mother of Reg Grady.
Ms Joy Sharp won the raffle, consisting ofa fan.
Fund raising activitiesWe need money, ideas, donations, bequests
(remember us in your will), donations over $2are tax deductible.
The Association wishes to thank ElaineCampbell of Gymea for her patch work cush-ion she has donated to the Association for araffle.
RafflesRaffle tickets are available for towels at $1
each or 3 tickets for $2, which will be drawnat the next meeting of 3 March 2001. After thatdate an Alarm Radio Clock will be raffled.Tickets will be $2.00 each or $3 for fivetickets.
All tickets can be bought at Dr GeorgeSamra's surgery, 19 Princes Highway Kogarahor at the next meeting.
The Hypoglycemia support group meetsevery 3 months and the next meeting will beheld on 12th August 2001 at 19 Princes High-way Kogarah (1st floor Dr. Samra's surgery)at 1.45 p.m. The cost is $l. This is a mutualsupport and discussion group with guest speak-ers whenever possible. Afternoon tea pro-vided - family and friends welcome. Forfurther information please telephone - Lor-raine on - 95209887 or Jeanette on -95259178
Previous Copies of theHypoglycemic Newsletter
Back issues of the HypoglycemicNewsletters are available at the NSWState Library, Macquarie Street, Syd-ney. They are filed underNQ616.466006/1 in the General Ref-erence Library.
Other libraries holding copies are:Stanton Library, North Sydney;Leichhardt Municipal Library; TheTasmanian State Library; The Syd-ney University; The University of NSWand Newcastle University. The Asso-ciation will provide free copies in PDFformat to any library upon request [email protected]
The Association also has a web siteat: <www.companyontheweb.com/hypoglycemia_australia> where thereare some Newsletters in PDF format,as well as articles on clinical nutritionand self-help psychotherapy.
MY JOURNEY ALONGTHE HYPOGLYCEMIC
TRAIL by Mrs Pamela Dean
Here is my story:During the last six to eight months I was
undergoing what I thought was an extremecase of stress at my workplace – normallybeing a fairly organized person I found my-self not being able to discipline myself towork through a project to completion and feltlike I was jumping from pillar to post eachtime I began a new task. Combined withsymptoms of not relaxing when eating ameal, becoming quite teary on frequent occa-
Report from
Sue LitchfieldMany thanks to all those members for the
great support of the hypoglycemic associa-tion it is because of the support of you all andthe hard work my fellow committee membersin particular Jur Plesman and Dr. Samra thatwe are in the position that we are in.
You all may have noticed that our balancesheet for the year is looking very good at thispoint of time how ever we still have not paidone account but we are hoping to rectify thatin the near future.
It is very satisfying to note that during theyear we received $1771.00 in the form ofdonations. Because of those very generousdonations we were able to keep are subscrip-tions at the previous years amount of $15.00for pensioners and $20.00 for full member-ship. So in order to maintain those pricesplease keep those donations rolling in.
I would also like to thank all those whohave supported our Raffles during the year.Again I am always open to any ideas or evenbetter still the donation of an item that wouldbe of interest to the average member E.G agift voucher for a particular store any electri-cal appliance etc.
Another matter I would like to mention isthat some of our regular meetings have beendone in numbers in order to maintain the high
standard of our meetings. Please everyone puton those thinking caps to come up with somegreat ways of enticing more to come and joinin, meet fellow members and also to enjoy thegreat afternoon tea we provide for all thosethat attend.
I am still up at the Gold Coast and will bereturning home hopefully at the end of Junethat is providing the film hat my husband isworking on does not go over time with thefilming. So will catch up with everyone at theSeptember meeting .
Good luckSue Litchfield
sions (thank goodness for a wonderful sup-portive husband), the feelings of my body/heart racing, not sleeping well, poor memoryretention and lack of concentration, I had noidea at all of what was actually happening tome both physically and mentally. Quite scaryI can tell you! My husband was not having thesame symptoms but he was quite tired most ofthe time as well.
Through a contact at my husband’s work,it was suggested that we seek the advice of anutritionist and we were highly recommendedDr George Samra, who is an expert in the fieldof hypoglycemia. After our initial visit inearly April, Dr Samra got us to have blood andallergy tests which resulted in my husbandbeing diagnosed a “borderline hypoglycemic”and myself being diagnosed as a type 2 abso-lute hypoglycemia and the possibility of type3 combined relative and absolute hypoglyce-mia. Just my luck to be the worst case sce-nario!! I cannot put a time frame on when Istarted with hypoglycemia but I feel that it hasprobably been around for many years and nowat 44 years of age, feel very fortunate to havestumbled onto the fact that I now have a“label” and know the reasons for the manysymptoms I have been encountering. If I hadnot done anything about the symptoms at thispoint in time, I would probably have “rolled
Continued page 12

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 3 -
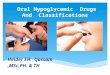
From: Fox, S.I.(1993), HUMAN PHYSIOLOGY, Wm.C.Brown, Dubuque IA Page 357
Diagram of the sructure of an atheroma
It will be seen from the diagrams how inatherosclerosis the plaque is buildingup, blocking the artery and with time it
can completely obstruct the artery.
The heart is a pump. In one person’s life-time, say eighty years it will be:
80 years x 365 (days in the years)x 24 (hours in the day)x 60 (minutes in the hourx 72 beats (per minute)
And that will be approximately 3.0725Billion Beats in your lifetime!
The exercise is trying to get that extrabillion. The Queen Mother is almost there,but a billion beats takes about twenty sevenyears roughly so she really has to live to 107to have the extra billion. Some people missout they die at 50 but they’ve almost had twobillion beats.
Several things can go wrong with thepump.
1. The blood supply to the pump. Thecoronary arteries atherosclerosis.
We have all seen pumps like pressurepumps and swimming pool pumps around.The blood supply to the pump is through thecoronary artery, so even though its pumpinglots of blood through your whole body largevolumes every minute, theheart itself doesn’t get the ac-tual blood that is within thechambers. It has a coronaryartery system on its surfaceand they alone are what is go-ing to feed the heart. This is abit unfortunate, because if onecould utilize the blood that ison the inside one wouldn’t getheart attacks.
2. Electrical pathwayswithin the pump. CardiacArrhythmias (that is irregularheart beats).
3. Muscle strength and in-tegrity of the pump. The topicof Cardiomyopathy. Smallheart size is better for musclestrength. Viruses are the mostcommon cause for Cardiomy-opathy, but its not always thecase. In fact cardiomyopathyis the most common conditionthat brings people to needingheart transplants. The viraldamage has weakened theheart.
4. Valve integrity of thepump - subjects like Rheu-matic Fever, Endocarditis,Sclerosis (which is hardeningand particularly hardening ofthe valves), and Regurgitation(or leakage of the valves).
Healthy Hearts and Hypoglycemicsby
Dr George Samra, MB, BS (Sydney), FACNEM
5. Damage to the pipes CVA, claudica-tion, Vascular insufficiency also atheroscle-rosis.
The arteries and the veins are the pipes.Damage to the arteries occurs with strokesand claudication which is muscle pain usu-ally in the back of the calf muscle.
Atherosclerosis is a disease of the arterialwall. The diagram shows thickening of thewall. (FIGURE 1) The representation offatty matter follows the insidious accumula-tion of cholesterol complex to proteins withinthe inner lining or the endothelial lining ofthe artery. (FIGURE 2)
Coronary heart disease together with othercardiovascular diseases such as strokes ac-count for about 45% of all deaths in Aus-tralia. There are a lot of routine investiga-tions done for heart problems. The mostbasic is an ECG where one has electricalwires on their chest. This produces someindirect information about the electricity onthe surface of the skin and the chest wall, butmost of the electricity in that area is reallycoming from the heart. There are twelveleads and twelve print outs and we get an ideaof what is going on. If there are irregularitiesof the heart like rapid rates or slow rates orirregular beats (atrial fibrillation) or fast beatswe can find these using ECGs.
We can get clues about whether a personis having a heart attack at the time if they’vegot heart pain. The ECG is limiting, often a
person with a bad heart can have a normalresting ECG because they are resting, sincethe pump isn’t being challenged with work orexercise.
An exercise ECG is more interesting. It’sperformed with electrical leads on you whilston an exercise bike or a treadmill and yourheart is pumping away. This test is morelikely to show if the heart is under strainunder a workload.
The doctor can tell the location of a heartattack, whether its in the front or the back ofthe heart or the side, and they can recognisethe patterns.
The Holtor ambulatory monitor is atwenty-four hour monitor. For somebody whosays to you “I get this chest pain or racy heartor my heart stops for five seconds at a time,but it happens twice a day”, using a twentyfour hour monitor we might pick it up and beable to explain just exactly what is going onin your body.
The echo cardiogram, is a wonderful noninvasive test and you can see the heart cham-bers pumping away. There are other noninvasive tests like arterial ultrasounds look-ing for flow in different arteries particularlygoing to the brain or other major organs.
The most useful invasive test is the angi-ogram, but we won’t discuss this right now.Hopefully you can avoid an angiogram withnon invasive tests because there is a morbid-ity and a slight mortality associated with evenjust doing an angiogram.

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 4 -
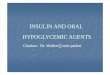
Progression of Atherosclerosis
From: Murray M & Pizzorno J(1990), Encyclopedia of Natural Medicine, P159
RISK FACTORSRisk factors in the development of athero-
sclerosis include heredity, smoking, obesity,Diabetes, Reactive Hypoglycemia, advancedage and high blood cholesterol concentra-tions. This is a degenerative process and withnutritional medicine there is now an argu-ment that it need not occur if one takes theright supplements, but since it is a degenera-tive process, the older you are the moreblocking to arteries you’re likely to have.The more cholesterol you have in your arter-ies the more chance you’re going to have ofblockages.
Other risk factors associated with Athero-sclerosis include deficiency in Vitamin C,magnesium, selenium, a high sugar intakeand high iron levels.
THE ROLE OF CHOLESTEROL INATHEROMA FORMATION
Studies have shown that high blood cho-lesterol levels are not necessarily associatedwith the development of atherosclerosis. Al-though the avoidance of saturated fats in thediet prevalent in foods of animal origin andtropical oils such as coconut and palm oil isuniversally recommended, 80% of plasmacholesterol comes from synthesis of the liverand only 20% comes from the diet. Thatwould be true of modern people but certainlyin the olden days high cholesterol levelswere common to people who were eatingbacon and eggs for breakfast everyday andfrying their food in lard. Changing the dietsof these people resulted in massive reduc-tions in their cholesterol levels.
It seems like we’re not as good at reduc-ing cholesterol anymore because modernpeople, especially as they get older are al-ready choosing their food fairly intelligently.I notice that when the patients I see have achoice between a low fat product and aproduct with a higher fat content they willinstinctively choose the product that con-tains less fat. This sort of rationale makes itmuch harder, a change of diet can makeminor changes to a persons cholesterol read-ing, and we don’t really get the sort ofdramatic results like we used to.
Most people with very high cholesterollevels possess a liver which is usually theculprit because it is capable of manufactur-ing excessive cholesterol. If we were able tomeasure the cholesterol levels of peoplewho died young historically, we would prob-ably find that their liver was manufacturingtoo much cholesterol and it actually blockedtheir coronary artery prematurely. In thepast we didn’t know about cholesterol sothere was nobody who could warn them.
High blood cholesterol can also occur asa result of the inherited condition known asfamilial hypercholesterolaemia. This con-dition is inherited as a single dominant gene;individuals who inherit both of these geneshave a lot more trouble with high choles-terol concentrations regardless of diet. Thisgroup would certainly be vulnerable toatherosclerotic heart disease.
CHOLESTEROL TYPES AND NOR-MAL VALUES
On the handout we have given you, youcan see the normal ranges for cholesterol.
Serum cholesterol < 5.4 mm/L but the
lower the better.LDL < 4 mm/LHDL > 1.2 mm/L
So there is a type of cholesterol that isprotective. The HDL we’re actually measur-ing in terms of the more the better but I don’tthink I like it to be much above 2 mm/L butcertainly it should be above 1.2 mm/L togive you some protection.
The LDL is the heavy or sticky type ofcholesterol and it is responsible for thisatherosclerotic in the illustrations. Just togive you a bit of history on cholesterol lev-els, 9.3 was once the cut off for high choles-terol, now it is 5.4. What has happened havepeople changed?
(Audience member volunteers) Knowl-edge has changed.
Yes, knowledge has changed. Previouslyit was based on the bell curve (a populationdistribution curve based on height or weight).So with height, everybody above 7 foot istoo tall and everybody below 5 foot is tooshort. On the bell curve 9.2 was a reasonablecut off, but everybody who had a bloodcholesterol of 8.5 was dropping dead withheart attacks, so doctors now base the cut offlevels on heart risk , which is quite intelli-gent when you think about it. Now 5.4 is anupper limit. Interestingly we haven’t alteredthe lower limit, but I would generally say thelower the better. A wonderful cholesterollevel is probably 2, but below that you mighthave trouble making your sex hormonesbecause they have the cholesterol moleculeas a base.
HEART PAIN OR ANGINA PECTORISThe atheroma we’re looking at (Figure 1),
looks to me like 70% of the artery is blocked,but normal flow is still going through it.Angina is another word for heart pain. If thearteries are blocked to such a degree that partsof the heart are not getting enough oxygen,then angina or heart pain occurs. With physi-cal work or exercise the work load and oxygenrequirement of the heart increases and anginais more likely to occur.
Angina is described as excruciating painthat is crushing, constricting, strangulating,suffocating, burning felt in the chest. When Iwas working in casualty, the most commondescription patients with angina gave was likean elephant sitting on my chest. There may beweakness, sweating, anxiety, palpitations, nau-sea.
There are two types of angina - stable andunstable anginas. If you have stable anginayou should be able to predict what brings onthe angina such as walking up two flights ofsteps, emotional stress can be a trigger or evencold weather. But unstable angina, certainlyfrom a medical point of view, is a more diffi-cult and more serious type of angina to dealwith. Unstable angina could result in a heartattack much more easily. In a practical physi-cal sense, stable angina has a plaque in it, butit’s not doing anything, a bit like an old scar.However, when you want more blood to gothrough the artery, such as climbing up thesteps, the blocked artery doesn’t have thecapacity to allow more blood through thereand angina occurs.
The mechanism for a heart attack is a crack

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 5 -
in the plaque, then a leakage of plaque mate-rial which blocks the artery completely fur-ther on. That is why we try to dissolve it.
In order to prevent Atherosclerosis pro-gression it is reasonable to take measures tolower serum lipids and also measures to re-duce platelet adhesiveness and or aggrega-tion, as well as lowering blood pressure ifelevated.
To lower serum lipid levels:-• A low fat, low cholesterol, high fiber
diet, with a high ratio of polyunsaturates tosaturated fat has been well validated. It maywell be of value to avoid sugar and there aresome studies that show that sugar is impli-cated in atherosclerosis production and thereare statistical correlations now you can feedeverything into computers that suggest cof-fee consumption is associated with highercholesterol levels and hypercholesterolae-mia. But that is not necessarily the cause andeffect.
• Nutritional supplementation with Ni-acin e.g. Vitamin B3, and Omega 3 fattyacids may be useful to promote increases inthe protective cholesterol, the HDL.
To reduce platelet adhesiveness and/oraggregation:-
Sugar has been shown to increase bothadhesiveness and aggregation (clumping ofplatelets) and should be restricted. A numberof nutrients have been shown to be of benefit,including pyridoxine (50 -150 mg), vitaminC (1-3 gm), vitamin E (400 - 1200 IU),magnesium, selenium, as well as bromelain,omega-3 and omega-6 fatty acids, pantethine,garlic, ginger and onions.
I’d like to refer to a few interesting ab-stracts relevant to this topic.
FIRSTLY, IS MARGARINE GOODFOR YOU AS OPPOSED TO BUTTER?
I think there is a bit of luck with somemargarines, some of them have a high con-
tent of trans fatty acids which elevate choles-terol. Hydrogenated vegetable oils have ahigh content of trans fatty acids (these are thebad types that don’t usually occur in nature)which elevate cholesterol perhaps because oftheir anti essential fatty acid action (Extractfrom the Journal of Nutritional Medicine,1979), while the natural cis isomer lowers it.
An animal study showed pigs fed a hydro-genated fat which contained 50% trans fattyacids, the serum cholesterol levels were 14mg/100 mL higher than those fed animal fateven though the animal fat contained 25%more saturated fatty acids. In addition, theserum lipoproteins isolated from pigs fed abasal diet that had been supplemented withanimal or hydrogenated vegetable fat from 6months old did not differ significantly incomposition (J. Lipid Res., 1977).
The new type of margarines are based onthe phytosterols, Logicol and Proactive arethe brand names. These types of margarinesare actually useful. 300 mg daily based onbeta-sibesterol content suggests that choles-terol analogues found in vegetables may lowerserum cholesterol by decreasing cholesterolabsorption.
In an experimental study, ingestion ofphytosterols like Proactive with a meal de-creased cholesterol absorption by as much as64% (American Journal of Nutrition, 1982).
There are studies that show that there areclever fats based on plant sterols that canactually lower cholesterol. Some of the stud-ies are dated in the early 1980s but the mar-garines with phytosterols have only beenaround for just a few years, which is a sadindictment on where we are up to.
WHAT ABOUT COFFEE?An observation study (from the British
Medical Journal in 1985) of 1007 men and589 women, demonstrated that there was asignificant linear association between coffeeconsumption in men and plasma cholesteroland LDL cholesterol. So the more coffee youdrink the higher your cholesterol level andthe higher the concentration of the bad type
of cholesterol (LDL). Men who drank 5 ormore cups of coffee had plasma cholesterolconcentrations about 0.5 micro moles perLitre higher than non drinkers after matchingthis up with people of similar age, ethnicity,body mass, and so on. In women, adjustedmean cholesterol levels were 0.34 mmol/Lhigher in coffee drinkers. The incidence ofheart attacks was also shown to correlate withcoffee consumption but not with tea con-sumption.
The epidemiological link between coffeeconsumption, hyperlipidaemia and athero-sclerosis may be at least partly due to anassociation between coffee consumption andsaturated fats, rather than to the effects ofcoffee. So what they’ve actually done in thisobservational study (American Journal ofEpidemiology, 1985) is asking people howmuch coffee they drink and measured theircholesterol levels, but also asked about howmuch red meat they consumed. It was foundthat heavy coffee drinkers ate approximately24% more saturated fats than non coffeedrinkers, so it might not be due to the fact thatpeople are drinking more coffee. Instead thisstudy might actually demonstrate that peoplewho drink lots of coffee don’t look after theirdiet and are more likely to eat a greasy meatpies and a lot of red meat.
Strangely enough, when thirty three peo-ple with high cholesterol were asked to ab-stain from coffee for 5 weeks, the total serumcholesterol levels fell 10% after ten weeks,and this is from a study published in BritishMedical Journal, 1985. So there must besome association with drinking coffee andhigh cholesterol levels.
SO WHERE DOES SUGAR FIT IN?Reactive hypoglycemia is a major cause
of atherosclerosis. It is clear that people witha glucose intolerance, that is reactive hypo-glycemics and diabetics or those with hyper-insulinism, are especially at risk of develop-ing atherosclerosis. The idea that fats andcholesterol in the diet may not be the mainvillains but rather excess sugar, is not new.Ross Hall, quoting many epidemiologicalstudies and flawed evidence in contemporaryresearch said categorically: The villain issugar. And Yudkin agrees following a studyof a group of people who were fed sucrose(cane sugar) and who then showed an in-crease of all the factors necessary in thedevelopment of atherosclerosis.
People with type 2 diabetes, Hypoglycae-mia and Syndrome X all have Hyperinsulin-ism (too much insulin in their systems). Hypo-glycemics who eat sugar have a delayed andexcessive secretion of insulin. Those Hypo-glycemics that continue eating sugar are themost likely to become the Syndrome X andthen the Maturity Onset Diabetics. Their highinsulin levels remain high practically all thetime. This excess insulin causes resistance atthe actual Receptor Site. The role of insulin istoo push sugar out of the blood supply intothe body cells so it can be used to make fuel.Insulin is a powerful anabolic hormone thatpushes sugar out of the blood supply into thebody cells to produce glycogen for storagelater or can be utilized for energy. The insulinalso pushes small fatty acids from the bloodstream into the body cells (particularly the fatcells) to make triglycerides (more complexfats) and also pushes amino acids (basic pro-

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 6 -
tein units) across the membrane to form pro-teins. So insulin is a building block (ana-bolic) hormone.
Doctors generally think of insulin on aglucose level only, that your blood sugar andinsulin are all tied up, and they are. But if onehas Insulin Resistance, one has very highinsulin levels and its moving sugar out of theblood stream into the body cells, but is alsomoving the fats from the bloodstream into theendothelial lining of the blood vessels. Oncethings go wrong and hyperinsulinism is es-tablished, there is a predisposition to causingatherosclerosis. Sugar doesn’t actually pushcholesterol into your arteries, but on the axisof free fatty acids and triglycerides this ac-tion of insulin is ultimately blocking arterieswith cholesterol. (FIGURE 3)
The first recommendation would be toadopt the hypoglycemic diet, this helps thepancreas stop pumping out excessive insulin.The most important mineral supplements arechromium and zinc, because they are activeat the insulin receptor site. Healing thereceptor site by eating a hypoglycemic diethelps to switch off the mechanism ofhyperinsulinaemia and therefore stop insulinultimately pushing cholesterol into arterywalls.
IS THERE ANY VALUE TO ANOATBRAN DIET?
In a study, control and oat bran diets weregiven in alternating sequence to eight hyper-cholesterolaemic men receiving standardiseddiets. On the experimental diet, the LDLcholesterol was reduced by 14%, and HDLcholesterol was unchanged (Am. J. Clin. Nutr.,1981).
A study published in the American Jour-nal of Clinical Nutrition in 1983 examinedthe blood pressure of twenty healthy normo-tensive men after they had ingested varioussugar solutions following an overnight fast,similar to our modern day GTT (GlucoseTolerance Test). Different solutions weregiven to the men to see if their blood pressurewould change, but it was not altered by inges-tion of water, lactose or galactose. With glu-cose, the systolic blood pressure after onehour rose significantly (10 mg of Mercury)and it stayed high for two hours. After inges-tion of sucrose blood pressure levels rosesignificantly (9 mm Mercury) and that lastedfor one hour. So sugar actually pushed up theblood pressure. Obviously we see high bloodpressure in heart attacks and heart disease, sosugar is tied up with these as well.
WHAT ABOUT BLOOD PRESSURECONTROL?
A study on increased consumption of rawfoods from Southern Medical Journal, 1985.For a mean duration of 6.7 months, thirty twopeople volunteered to eat an average of 62%of their calories in the form of uncookedfood. The average blood pressure droppedsignificantly by 17.8 mm Hg. In additionthere was significant weight loss of 3.8kg and80% of those who smoked or drank alcoholspontaneously ceased.
An article by Linus Pauling talks aboutatherosclerosis in a totally different light. It’sto do with evolution that human species arecomplicated, we are different to other crea-tures except the higher primates like chim-panzees and gorillas who also have lost their
ability to make vitamin C in the adrenalglands of their bodies. We are unique inanimal kingdom in that we cant make vita-min C, and Linus Pauling has written thisthesis called “A Unified Theory of HumanCardiovascular Disease Leading the Wayto the Abolition of This Disease as a Causefor Human Mortality”. He is suggestingthat a higher dose of vitamin C (say 8000 mgdaily) would stop humans developing athero-sclerosis.
There are studies that show a 70kg bull-dog makes about 10,000 mg of vitamin Cevery day, so the vitamin C we are getting isnowhere near as much as a bulldog. To pre-vent scurvy you need 25 mg per day, so weare preventing scurvy if we have an apple ororange every day, but were not getting the10,000 mg that the bulldog is.
OTHER HEART CONSIDERATIONSProblems with electrical pathways of the
heart pump Arrhythmias.Drugs used include Digoxin from the Fox-
glove Herb (Digitalis), Quinine,Ameodorone, and Beta Blockers.
To reduce cardiac arrhythmias, severalstudies have suggested magnesium supple-mentation may be beneficial, perhaps be-cause it corrects a magnesium deficiency inthe myocardium. Potassium supplementa-tion may also be beneficial, and there ispreliminary evidence that taurine might be ofvalue.
20% of forty five consecutive patientswith symptomatic atrial fibrillation had defi-cient serum magnesium levels (AmericanJournal of Cardiology, 1986).
Two elderly patients with ventriculartachycardia received magnesium infusionswhich resulted in magnesium retention andcessation of the attacks (Acta Medica Scan-dinavia, 1982).
Problems with muscle strength and integ-rity of the pump - Cardiomyopathy.
Thirty four patients with severe conges-tive cardiomyopathy received 100 mg CoQ10daily. 82% improved as shown by increasedstroke volume and cardiac index. Mean ejec-tion fraction increased from about 25% toabout 40%. Two year survival rate was 62%,compared to 25% for a similar series ofpatients treated by conventional methodsalone (Amsterdam, Elsevier/North HollandBiomedical Press, 1984).
In an experimental double blind study,daily administration of CoQ10 for twelveweeks increased cardiac ejection fraction sig-nificantly, reduced shortness of breath andincreased muscle strength. These improve-ments lasted as long as 3 years in patientstreated continuously, but cardiac functiondeteriorated when CoQ10 was discontinued.Of the eighty patients treated, 89% improvedwith supplementation (Proc. Natl. Acad. Sci.,1985).
Selenium supplementation may help.
Damage to the Pipes. (Claudication,CVA, Vascular Insufficiency and Athero-sclerosis).
Vitamin C, E and Selenium help keep thepipes clean.
Intermittent claudication is merely an-other sign associated with general athero-sclerosis or the degenerative disease of bloodvessels feeding the calf muscles. It typically
presents with cramps of the calf after walkingfor a certain distance. The reason for the painis that as with angina pectoris, muscles arestarved of oxygen by a poor blood supply andalso the muscle is unable to get rid of thewaste products during exercise.
In a controlled experimental study, thirtytwo out of forty seven men with severe symp-toms received 100 IU Vitamin E three timesdaily while the control group received drugs.After about three months, 54% of the men onvitamin E vs. 23% of the controls could walka kilometer. After about eighteen months,twenty nine of the thirty two men on vitaminE demonstrated increased calf blood flowwhile ten out of fourteen men in the controlgroup demonstrated a decrease (AmericanJournal Clinical Nutrition, 1974).
Blood pressure and alcohol consump-tion
In an observational study alcohol con-sumption was studied in relation to bloodpressure for 883 men and 959 women agedbetween twenty and seventy four who werenot on anti-hypertensive drugs. After the datawas controlled for smoking, exercise andmedication, the amount of alcohol consump-tion was directly correlated with increases inboth systolic and diastolic blood pressure(American Journal of Epidemiology, 1983).
Blood pressure and a vegetarian dietIn another observational study, ninety eight
vegetarians were compared to a matchedgroup of non vegetarians. The average bloodpressure was 126/77 for vegetarians and 147/88 for the control group, a significant de-crease. Only 2% of the vegetarians had hy-pertension (BP above 160/95) compared to26% of the non vegetarians. Both groups hada similar sodium intake and excreted thesame amounts of sodium. (American Journalof Clinical Nutrition, 1983).
Dos and don’ts.FOODVegetarian diet fish is goodAvoid allergy foodsLower your cholesterol.Avoid excessive amounts of red meatAvoid high cholesterol foods.Reduce coffee intake.ALCOHOL: 2 drink limit Avoid excess
alcohol.TOBACCO: Avoid passive smoking.
don’t smoke.BLOOD PRESSURE:Keep blood pres-
sure under control.EXERCISE: 45 minutes x 3 times per
week walking will do. Don’t vegetate, beactive!
WEIGHT: Maintain healthy body weight,lose weight if overweight don’t over-eat. VITAMINS: Supplement diet with Vita-min C, E, and CoQ10.
MINERALS: Supplement diet with Chro-mium, Magnesium, Selenium and Zinc.
HERBS: Supplement diet with garlic,Hawthorne berry, Fenugreek, Bromelain(from pineapple).
OTHER: Supplement diet with essentialfatty acids, EPO.
MEDICATIONS: Aspirin and conven-tional blood pressure and heart drugs may benecessary

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 7 -
S chizophrenia is probably the mostserious of all the psychotic disorders that can afflict not only the
person, but the whole of his family and hisimmediate social environment.
Treatment of schizophrenia should alwaysbe under the supervision of a medical practi-tioner, despite the fact that patients and mem-bers of the family may experience frustrationwith the palliative nature of drug-orientedpsychiatry as it exists today. It is stronglysuggested here, that treatment be sought fromcomplementary doctors - meaning specialistswho have combined their traditional medicalknowledge with alternative approaches, inparticular nutritional medicine.
Unfortunately, psychiatrists with postgraduate diplomas in clinical nutrition are fewand far between in Australia as perhaps else-where.
Post graduate diplomas can be obtainedfrom
The Australia College of Nutritional andEnvironmental Medicine, 13 Hilton Street,Beaumaris, Vic, 03-9589-6088 (see: http://www.acnem.org) or
The International Academy of ClinicalNutrition, PO Box 370, Manly NSW, 2095(See: http://www.intacad.com.au)
I also recommend that patients and theirfamily members join mutual support groupsfor orthomolecular psychiatry, who may of-ten be able to put you in contact with nutrition-ally oriented psychiatrists. (Also ACNEM hasa referral service). It is only through pressurefrom patients and their family that will forcepsychiatric practitioners to respond to “mar-ket forces” and loosen the ties to the pharma-ceutical companies that dominate the treat-ment modality of mental illness.
There is a web site, The Australian Inte-grative Medicine Association, (AIMA) pro-viding names and addresses of complemen-tary doctors in Australia at:
<http://www.vanzyl.com.au/aima/>
It is imperative that the complementarymedical fraternity make their presence feltand publish access to their services more openlyin our community.
A good mutual support organisation is:
SOMA, which aims to see medical hori-zons expanded to include complementarymethods in psychiatric practice, has monthlymeetings, every third Monday, 10 am at StFrancis Xavier Church Hall, 19 Mackenzie St
The Nutritional Aspects ofSchizophrenia
Jurriaan Plesman, BA (Psych),Post Grad Dip Clin Nutr
Lavender Bay (behind North Sydney Station),Postal Address; PO Box 7180 Bondi Beach,2026, Phone: 02-9789-4805, Fax: 02-9922-5747
Its patron is Dr Chris Reading, well-knownorthomolecular psychiatrist in Australia andpioneer in clinical nutrition.
Symptoms of schizophreniaIt is a disease that affects the patients
ability to recognize reality, characterized byhallucinations, which does not result fromexternal stimuli but from distortions in any ofthe senses. Accordingly, they can be classifiedas auditory (affecting hearing), gustatory (af-fecting taste buds), olfactory (affecting senseof smell), tactile (affecting touch) and visual(affecting vision). Victims of the disease mayshow disorganized speech and behaviour.There usually is a lack of insight, especiallyduring the initial stages of the disease, butpatients who gain some insight into their ill-ness, stand a better chance of prognosis.
In delusions the person tends to misinter-pret incoming stimuli.
Symptoms in schizophrenia may also bedefined as ‘positive’ or ‘negative’. Positivesymptoms refer to the hallucinations, delu-sions and disorganized behaviour, whereasnegative symptoms reflects a tendency to-wards a restricted emotional range, inexpres-sive speech and inability to initiate productiveactivity or pursue goal directed behaviour.
There appears to be a gradual deteriorationin logical thinking, social skills and erraticbehaviour. It usually is a life-long illness,although if treated early in its development itcould remain in remission for long periods oftime. Orthomolecular psychiatrists and doc-tors are somewhat more optimistic in believ-ing that psychotic disorders are treatable bynot only pharmaceutical as well as nutritionalor other means in the not too distant future.
Schizophrenia has been subdivided intofive subtypes:
Paranoid schizophrenia is often associ-ated with schizophrenia in popular thinking,although in reality they account for a minorityin the disease. They display the ‘positive’symptoms of hallucinations and delusions.These delusions are not always paranoid -marked by suspicions - but may concern reli-gion or ideas of grandeur. Only a small per-centage of this category may pose a danger tothemselves or others.
Disorganized schizophrenia refers to dis-organized behaviour or emotional responsesthat are either blunted, “flat affect” or unusual.
Catatonic schizophrenia characterized bysevere psychomotor disturbances, resulting inimmobility or increased physical activity, be-coming mute and displaying unusual or inap-propriate behaviour.
Undifferentiated schizophrenia although‘positive’ symptoms are present, they fail tofit in with any category.
Residual schizophrenia when negativesymptoms predominate, but without majorpsychotic symptoms.
CausesUnderlying causes of schizophrenia are
unknown. Some researchers believe schizo-phrenia is hereditary, and there is some evi-dence that some cases of the disorder are theresult of an inherited defect in body chemistryin which brain chemicals called neurotrans-mitters function abnormally. Others theorizethat it results from external factors, such ascomplications during birth, head injury, reac-tion to a virus, or environmental poisons thatdamage the brain. Horrobin speculates thatduring the evolution of the human speciesbrain connectivity may have been improvedthrough abnormalities in phospholipid me-tabolism. Thus schizophrenia may be seen asa intermediate step in the development of thehuman brain. He proposed that the changeswhich resulted in the schizophrenic genome“caused the emergence of humanity, and that,especially in their milder forms, they arestrongly positively associated with humanachievement”. (Horrobin)
DiagnosisJust as fever is a sign of various underlying
illnesses, so in schizophrenia, the clinicianneeds to consider a variety of other possibili-ties, such as mood disorders, and any funda-mental medical condition that could accountfor the symptoms. Foremost among these arehypoglycemia, allergies and/or food sensi-tivities to which we will return later.
Conventional treatment of schizophreniais by means of various antipsychotic drugs,psychotherapy and social support.
Some well-known pharmacological agentsare: chlorpromazine, clozapine, fluphenazine,haloperidol, paroxetine, phenothiazines,thioridazine, trifluoprazine, and many others.Most of these are effective for positive symp-toms, with the exception of clozapine, whichalso acts in the case of schizophrenia withnegative symptoms. However, clozapine issaid to have very serious side effects in one percent of cases: it seems to destroy white blood

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 8 -
cells needed to fight infection. It also mayalter the heart rate, increase blood pressure,cause excessive salivation and constipation.But on the plus side it does not cause tardivedyskinesia (muscle rigidity), as with most ofthe other drugs. Lithium is sometimes pre-scribed in schizophrenia to stabilize moods.The kidney handles lithium and sodium thesame way and when there is too much sodiumin the body, lithium levels drop. If the body isdepleted of sodium, lithium can build up andtoxic reactions are possible. (Graedon, 291)Thus avoid low salt diets. Supplementationwith low-dose natural lithium from vegetableconcentrates may sometimes be preferable(Lithomin, Nutridyn 50 µg with meals) andshould be tried. (Fierro AA 1988)
Many if not most major tranquilizersdeplete riboflavin, vitamin B12, folic acid andvitamin C. The latter may reduce the effec-tiveness of the drugs (Graedeon 291). Sideeffects of psychotropic drugs seem to be causedby interference with nutrients. Knowledge ofthe drug/nutrient interactions may providesteps to reduce adverse reactions. Neverthe-less, by any objective standards, chemotherapyalone for psychotic disorders has remaineddisappointing.
Since other mental disorders may mimicschizophrenia, other medications are tried,such as anti-anxiety drugs, or those treatingagitation.
Term schizophrenia under attackIt should be noted that there are a number
psychiatrists who have serious doubts aboutthe stigmatization of patients with the label“schizophrenia”: and even doubts the useful-ness of diagnosis. They argue that there islittle scientific evidence in support of theexistence of the schizophrenia, and that itwould be more beneficial to treat the distress-ing symptoms of patients directly. (Boyle)
Tardive dyskinesia (TK)Long term use of antipsychotic drugs, such
as chlorpromazine, thioridazine, trifluopera-zine or phenothiazine and many others maycause tardive dyskinesia. “Tardive” meanslate (later on in treatment) and “dyskinesia”means impairment of voluntary movement.Patients may display repetitive movements,lip smacking, swinging of legs to and fro.These side effects appear to be irreversible,and may cause patients to abandon treatment.It is therefore essential to prevent the disease.It appears that the dyskinesia is associatedwith a errors in dopamine metabolism.(Pearson et al. 134)
Studies with a large numbers of patientshave shown that megavitamin supplementa-tion can prevent the development of these sideeffects.(Tkacz, Toll))
Administration of these supplementsshould be under strict supervision by a medi-cal practitioner, because they ought to beconsidered part in the overall treatment pro-gram, and some may interact with drug treat-ment.
Vitamins administered were:Vitamin C up to 4 grams a dayVitamin B3 (Niacin or nicotinamide) up to
4 grams a day. Nowadays inositolhexaniacinate may be the preferred form, be-cause of unpleasant but harmless side effectsof niacin (Head KA)
Vitamin B6 up to 800 mg per day, thesehigh doses may have side effects and needmonitoring by a doctor. Some scientists do notrecommend such high doses.
Vitamin E 1,200 IU per day (Dabiri,Lohr). Vitamin E is thought to play a role inthe antioxidation of neuroleptic drugs in cer-tain parts of the brain.
Vitamin B-complexManganese 15mg per day, (Vayda, 158,
Kunin RA, Norris)Lecithin providing choline has been suc-
cessfully used. (Pearson, 134)
Only few studies have reported benefitswith evening primrose oil in the treatment ofTK.
Some researchers believed that tardivedyskinesia was associated with the body’sinability to synthesize certain amino acidsinvolving phenylalanine and branched chainamino acids (BCAA), such as valine, isoleu-cine, and leucine. The latter was believed tocompete with excesses of phenylalanine lev-els. Some improvement was noted among afew patients with supplementation BCAAs.(Richardson et als.)
Non-pharmacological TreatmentStudies have shown that exercising can
reduce the symptoms of both depression andanxiety. (Taylor et als., Adams). It has evenbeen demonstrated to reduce aggressive hal-lucinatory behaviour. (Belcher, Conroy et als.).
It is well known that schizophrenic pa-tients generally have a poor diet. They tend tobe overweight, but this may well be due totheir medication. In addition, they seem to beheavy smokers. This could be explained bythe fact that nicotine binds to nicotinicreceptors in the brain, augmenting the releaseof numerous neurotransmitters, includingdopamine, serotonin, norepinephrine, acetyl-choline, gamma-aminobutyric acid, and gluta-mate. This provides them with psychologicalreward and cause addiction (Quattrocki etals.).
There are reports of psychotic episodesbeing precipitated by excessive caffeine use.Caffeine is a methylxanthine that has an be-havioural effects one hour after consumption.It increases norepinephrine and serotonin andhas a biphasic effect on dopamine in the CNS.(Mikkelsen). Caffeine increases the anxiogeniceffects among many patients.(Bruce M)
Cognitive therapyAny method that aims at reducing psycho-
logical anxiety and stress, which could triggera major depression in sensitive people, shouldhelp the patient cope with frustration. Somewill therefore benefit from psychotherapy.
A study compared the results of patients ingroups with different treatments, 1) receivingchemotherapy alone, 2) patients receivingchemotherapy and supportive counselling and3) chemotherapy plus intensive cognitivetherapy (psychotherapy).
It was found that patients receiving cogni-tive behaviour therapy showed the greatestimprovement in positive symptoms. Patientsreceiving routine care alone showed minimalchange, and those who received supportivecounselling showed some improvement butless so than those receiving cognitive behav-iour therapy. This difference was significantfor cognitive behaviour therapy compared withroutine care alone. (Tarrier 1998)
Nutritional factors affecting the course ofschizophrenia
For many years it has been speculated thatdietary factors contribute to the symptoms ofschizophrenia. Apart from poor diets, someindividuals may require more than the RDAsof vitamins and minerals even if diets are‘adequate’.
In fact, schizophrenia or any other psy-chotic disorders could be affected by a numberof dysfunctions along the route of nutritionaldigestion. There are about 22 digestive en-zymes capable of digesting carbohydrates,proteins, sugars and fats. Magnesium is in-volved in about 400 enzymatic reactions, 1 percent of which is in the extracellular fluid, thusnormal magnesium levels can exist in situa-tions of intracellular depletion.(LopezMJ,1997) Zinc is a constituent of about 200enzymes (Florence et al. 58).
Patients should ensure that they have ad-equate intake of vitamins by taking a B-com-plex vitamin supplements as a starting point.But let us be aware that normal dosages maybe ineffective in some individuals. For exam-ple a deficiency of vitamin B1 (Thiamine)alone may present symptoms of chronic fa-tigue, irritability, memory loss, personalitychanges (such as aggression), insomnia, anxi-ety, restlessness, night terrors, appetite loss,sensitivity to noise, numbness and tingling inhands and feet, and circulation problems forthose requiring higher doses.
Another example is, the finding that manyschizophrenic patients lack hydrochloric acidin the stomach, which is a protective barrieragainst diseases further down the digestivetract. Consequently, proteins are partially bro-ken down into polypeptides setting up auto-immune reactions which result in ‘schizo-phrenic’ symptoms. Thus it may pay for pa-tients to take digestive enzymes; such as betainehydrochloride, Papain, probiotics (acido-philus), dandelion root, gentian, Goldenseal,Milk thistle, Yarrow, chamomile. AHeidelberg analysis can tell if the stomachacid level is within normal range.
In my experience with people sufferingfrom a mental and/or psychotic disorders theadoption of the hypoglycemic diet markedlyimproved symptoms, but no claims can bemade that this diet alone would remedy thecondition. Common sense would tell us thatfluctuating blood glucose levels supplyingenergy to brain cells would contribute to andaggravate psychotic symptoms. However, thehypoglycemic diet, just as the diabetic diet -though close to a natural diet - would neces-sarily include some foods to which the schizo-phrenic patient may well be allergic.
A high intake of total fat predominantly of

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 9 -
saturated fat derived from land animals wassignificantly associated with unfavourableratings in the outcome of schizophrenia fromsurvey in 8 national centers. (Christensen etal, McCready R et al).
Hydrolysis of gliadin fraction of glutenproteins from wheat in the presence of pepsinare known to produce schizophrenic symp-toms in gluten/gliadin sensitive patients.(Washburn CF et al, Ross-Smith P et al.). Butnot all schizophrenics demonstrated evidenceof inflammatory response to gluten. (StormsLH et al., Potkin et al).
The same applies to sensitivity to casein,the major protein found in cow’s milk (DohanFC et al).
Results suggest that some, but not all,people with schizophrenia may benefit from agluten-free/dairy-free diet and the best way isto have this tested by your doctor or by trialand error. (See “Finding your Allergies” at theHypoglycemic Health Association of Aus-tralia” web site).
There has been several studies showingthat schizophrenics have elevated copper lev-els, although this has been disputed by others.When copper levels are high, the levels ofvitamin C and zinc drop. Some researchershave theorized that prenatal zinc deficiencymay be the root cause of schizophrenia. Zincdeficiency may have resulted in the damage ofthe pineal area of the brain. The incidence ofschizophrenic episodes, they argue, tends topeak in cold weather months, when zinc in-take is lower. Thus there may also be a mela-tonin connection.
Pfeiffer found that nearly half of thosesuffering from schizophrenia had low levelsof histamine, so called histapenics. They werefound among those classified paranoid schizo-phrenics, severely depressive and suicidal,and having hallucinations. Apart from thehigh levels of copper, they were deficient inzinc and folic acid. On the other hand, thehistadelics, consisting of about one third ofpatients, had too much histamine levels (bloodbasophils - white blood cells that store hista-mine) and were associated with those classi-fied as obsessive-compulsive and delusionalwith severe impairment of thinking. Theycould be suicidal or catatonic. (Pfeiffer 1978.73)
He suggested that supplementation withmanganese could increase urinary copper ex-cretion (Pfeiffer 1978, 66). He claims thatexcess copper causes a nutrient imbalancecreating deficiencies in folic acid, vitaminB12, niacin, zinc and manganese. Supple-menting zinc (50mg), manganese (3mg) andpyridoxine (50mg) would increase copperexcretion in patients. (Pfeiffer et als.1983).But the elevated copper factor in schizophre-nia has not been universally accepted.(Werbach, 232)
IV supplementation with manganese mayimprove the clinical condition, as shown in 58per cent of cases (22/38pts) in one experimen-tal study. (English WM). Nevertheless, whenhair manganese levels are either elevated ordepressed it could result in aberrant behaviouras shown among a group of violent maleprisoners. (Gottschalk LA ). Furthermore,abnormal environmental manganese levels
have lately also been associated with the oc-currence of the prion diseases, thought tocause a group of human and animal diseasesaffecting the brain (Creutzfeldt-Jacob disease,kuru, scrapie, bovine spongiform encephali-tis) or ‘mad cow disease’.
Reports have shown that chronic manga-nese intoxication may cause potentially irre-versible movement and other neurologicaldisorders. (Donaldson J)
Manganese deficiency is marked by fa-tigue, irritability, memory losses, and ear noisessuch as ringing. Tests for manganese levelsshould be conducted.
Deficiency of vitamin B12 alone can mimicsymptoms of schizophrenia and patients areadvised to have periodic injections of vitaminB12 and folic acid by their doctor. Absorptionof B12 from food depends on the presence ofthe intrinsic factor, a glycoprotein synthe-sized in the stomach wall which binds withB12. It is subsequently bound by a specialreceptor in the ileum, where it is released by areleasing factor into the blood system. Anabnormality along this pathway can causesevere B12 deficiency, with physical andemotional consequences. Sublingual vitaminB12 are also available and may be preferablein some circumstances.
Zinc and copper are in balance, meaningthat high levels of one causes lower levels ofthe other and vice versa. There are severalstudies that patients with low zinc levels - maybe due to high copper levels - respondedpositively with zinc sulphate and pyridoxine.(for studies see Werbach 236). Zinc defi-ciency is associated with apathy, lethargy,amnesia and mental retardation often withconsiderable irritability, depression and para-noia. On the other hand high zinc levels maylower manganese levels. (Pfeiffer CC, LaMolaS, 1983). Zinc deficiency can also blockomega-6 essential fatty acid metabolism intogamma-linolenic acid (GLA) anddihomogamma-linolenic acid (DGLA).(Cunnane SC et al.) As in diabetes, patientsmay have dysfunctional desaturases (enzymes)causing a blockage in the conversion of essen-tial fatty acids into GLA or EPA. A naturalforerunner of essential fatty acids, both omega-6 and omega-3 is flaxseed oil or walnut oil. Inany case, supplementation with essential fattyacids in the form of GLA (found in EveningPrimrose Oil) and fishoil (Max EPA) havebeen shown to improve symptoms, includingside effects of anti-psychotic medication.(Laugharne JD)
Some believe that schizophrenics have ahigher need for niacin. Thus some schizo-phrenics may be vulnerable to pellagra. Thisis a disease resulting from a deficiency ofniacin or tryptophan, or a metabolic defectthat interferes with the conversion of the pre-cursor tryptophan to niacin. Symptoms arelikely to be drying dermatoses, autonomicneuropathies, tinnitus and fatigue. (Rudin).
Several studies have shown that manyschizophrenics (about 36% in one study) havelow red-cell folate levels and that histapenicsin particular were deficient. It was suggestedthat folic acid therapy along with vitamin B12,niacin, vitamin C and zinc was effective in the
treatment of “histapenic” schizophrenics af-ter 5-6 months with a rise in blood histamineand reduction in copper levels. (Pfeiffer CC etal.1979). However there is a warning thatsupplementation with folic acid can also causean exacerbation of psychotic behaviour if bloodlevels become elevated.(Werbach 221). Thusfolic acid should only be used in proven defi-ciency.
Early reports claimed that treatmentwith high doses of niacin (vitamin B3)would improve psychotic symptoms inschizophrenia.(Hawkins) But treatment withNiacin appears to be beneficial only in casesof deficiency. Niacin treatment of schizophre-nia has remained controversial following anextensive review of a series of clinical trials,which were generally negative. (Ban TA)Adverse side effects of niacin therapy werereported, including nausea, GI irritation, in-creased blood sugar and uric acid. The alterna-tive in the form of niacinamide may howeverproduce depression and could cause hepatictoxicity. (Werbach 224). It is not clear whetherthe alternative form of inositol hexaniacinatewould overcome these problems.
Studies conducted with vitamin B6 (pyri-doxine) are equally contradictory. There isone case report of 2 catatonic schizophrenics,unable to tolerate neuroleptics, who respondedpositively to the administration of 500 mgdaily of vitamin B6. (Brooks SC). But Werbachwarns that doses more than 50 mg daily maycause neuropathy (Werbach 227). Excess B6can affect the binding properties of serotoninreceptors in the brain according to one study(Schaeffer et als. 1998). Excess B6 can causea deficiency of other B vitamins or othersubstances that are in balance with B6.
A group of female patients on oral contra-ceptives (which may cause a vitamin B6 defi-ciency) and showing psychiatric symptomsresponded to pyridoxine 50 mg daily.(Baumblett et al.). The results of pyridoxinesupplementation at 100 mg daily in one schizo-phrenic patient included dramatic reduction inside effects from medication, as well as reduc-tion in schizophrenic symptoms (Sandyk R,1990). In another study only one out twentypatients benefited from B6.
Nevertheless, the role of vitamin B6 inpsychotic disorder can not be underestimated.It is required for the conversion of glutamineto GABA. Pfeiffer claims that when the bloodcirculation shows elevated amounts of“kryptopyroles”, it binds with both B6 (pyri-doxine) and zinc, which are then excreted inthe urine thereby causing theirdeficiencies.(Pfeiffer CC et al.1988). Otherstudies suggested that Pfeiffer’s observationsmay have been on patients whose schizo-phrenic symptoms were secondary to a meta-bolic disease similar to porphyria, also associ-ated with B6 deficiency. (Cruz WT al 1978)
The administration of an amino acid, Gly-cine, not only plays a role in maintaining thehealth of the prostate gland, but also appears toinfluence the function of neurotransmitter inthe brain, involved in memory and cognition.(File SC et al.) Glycine is used in liver detoxi-fication as part of glutathione (as well ascysteine and glutamic acid) and perhaps de-toxification may be responsible for the reduc-

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 10 -
tion of negative symptoms, depression andmental symptoms of schizophrenia. Severalstudies have shown improvements in schizo-phrenic behaviour with glycine therapy.(Heresco-Levy U 1996 & 1999, Waziri R1996)
Vitamin C is also involved with detoxifi-cation and its supplementation has been re-ported to benefit patients. (Sandyk R 1993,Kanofsky 1992) In an uncontrolled trial,some schizophrenic patients continued a courseof vitamins (4 to 10 grams of niacin or niaci-namide, 4 grams of vitamin C, and 50 mg ormore of vitamin B6) after being dischargedfrom the hospital, while a control group ofpatients discontinued the vitamins upon dis-charge. Both groups continued to take theirpsychiatric medications. Those who contin-ued to take the vitamins had a 50% lowerreadmission rate compared with those whodid not. (Hawkins et al 1970) Yet some subse-quent studies have not been able to confirmthese results.
Tryptophan is an essential amino acid andthe precursor of the important neurotransmit-ter Serotonin in the presence of vitamin B6.Tryptophan levels appear to be lower amongschizophrenic patients compared to non-schizophrenics. Tryptophan is also needed tosynthesize niacin. Sixty milligrams of tryp-tophan yields 1 mg of niacin (Kirshmann, 36),which could explain a abnormality in serot-onin metabolism among schizophrenics.
In an uncontrolled trial, patients withschizophrenia were given 2–8 grams of L-tryptophan and 100 mg of vitamin B6 daily.This resulted in decreased agitation and lessfear and anxiety, but these improvements werenot as great as those achieved with psychiatricmedications. (Bowers 1970) It appears thatschizophrenics use L-tryptophan in a differentway. In a survey in populations from severalEnglish-speaking countries it was found thatwhen tryptophan intake was low, suicide rateswere high. (Kitahara). Thus tryptophan sup-plementation should be considered as a possi-bility in the treatment of schizophrenia.
Werbach reports that studies of serum lev-els of magnesium in schizophrenics is contra-dictory. It appears that with patients onneuroleptics magnesium levels may be low-ered, compared to drug-free schizophrenicswho have normal levels. (Werbach 234) Cal-cium and magnesium levels are in a ratio of2:1. Biochemical tests should indicate whetherthere are any abnormalities, as these mineralsare associated with many symptoms, such asanxiety, insomnia, fatigue and high bloodpressure.
Some nutritional sources of brainchemistry
It is essential that any experimentationwith nutrients to treat schizophrenia or anyother psychotic disorder should be under thesupervision of a medical practitioner.
Some scientists theorize that manic-de-pressive illness results from a derangement ofa balance between two important nerve sig-nals transmitters: norepinephrine and acetyl-choline (ACh). Choline levels are too high indepression and norepinephrine are too high inmania.
Acetylcholine is a neurotransmitter whichis important in the parts of the brain affecting
primitive emotions like sex and a degree ofresponsiveness to outside stimuli, as in alert-ness versus sleep. It plays a role in memory,learning and long-term planning. When AChlevels are low, the person is easily distractedby irrelevant stimuli in the environment. Ace-tylcholine is used in the brain and nerve cells,and required for memory, appetite, and sexualbehaviour. Many hyperactive children respondpositively to choline in lecithin, and this mayalso be useful in withdrawal from alcoholduring treatment of alcoholism. (Pearson 274)
The body manufactures acetylcholine fromphosphatidyl choline which is found in leci-thin. Other sources are: soy, egg, brewer’syeast, grains, legumes, fish, wheat germ. Egglecithin may be more effective for those suf-fering AIDS, herpes, chronic fatigue, immunedisorders. For our purpose soy lecithin gran-ules or capsules would be the more conven-ient.
Vitamin B5 (pantothenic acid or Pantoth-enate) is required for the conversion ofphosphatidyl choline in lecithin to acetylcho-line. (Pearson 274). Pure lecithin contains 15-20 per cent of phosphatidyl choline and thissource of choline is more effective than fromcholine alone according to Wade. (Wade, C1980).
Thus in the depressive phase of manic-depression (when acetylcholine levels arehigh) lecithin should be avoided, but in themanic phase it should counterbalance the highnorepinephrine levels, which is thought to beresponsible for the mania.
Glutamine is another important nutrienthaving effects on neurotransmitters in thebrain. In the breakdown of amino acids nitro-gen is produced, which can form free ammo-nia that is especially toxic to the brain. Theliver can convert nitrogen to urea, which isthen excreted as urine. Nitrogen can also com-bine with glutamic acid to form glutamine.(Chaitow, 79) Glutamine is stored in muscletissues and needed for synthesis of skeletalmuscle protein.
More importantly, glutamine is the precur-sor of GABA (or Gamma-aminobutericAcid) which is inhibitory transmitter control-ling the synthesis of dopamine. GABA keepsthe brain and body from going into “over-drive”. GABA seems to be quite effective foranxiety disorders as well as insomnia (espe-cially the type of insomnia where racingthoughts keep the individual from fallingasleep). At dosages above the 250 mg it maysometimes cause slight side effects marked bytingling. It is also a precursor of glutathioneamong others. Vitamin B6 is required toconvert glutamine to GABA, which then playsan important role in regulating the synthesis ofdopamine from dopamine cells. The impor-tance of this is that schizophrenia is thought bedue to a disordered dopamine metabolism.GABA is available in supplemental form andshould be taken with water (do not take milk),together with vitamin B6 and vitamin C.
Valium & Librium are tranquilizers themolecules of which are believed to fit into thebenzodiazepine receptors in the brain. Scien-tists claim that niacinamide, inositol, gammaaminobutyric acid (GABA) occupy the samebenzodiazepine receptors. (Use B3, 1g; inosi-tol 3g; 500mg GABA sublingually), and hencethese may form an alternative to chemical
tranquilizers. (Pearson 282).Taurine, GABA and zinc are known to be a
calming agent in the brain. [Pfeiffer,C.C.(1978),77], Taurine has been shown in human trials tohave an anticonvulsive effect. Its apparent role is tonormalize the balance of other amino acids, whichin epilepsy are disordered. Serum zinc has alsobeen found to be low in epileptics. Full spec-trum light exposure results in increased lev-els of taurine being concentrated in the pitui-tary and pineal glands. Continued exposure toartificial light might cause the concentrationto be reversed.
Phenylalanine is an essential amino acidand is a forerunner of a group of substancesknown as catecholamines, which play impor-tant roles in brain chemistry. The metabolicpathway can be represented as; Phenylalanine> tyrosine > dopa > dopamine > norepine-phrine (noradrenaline) > adrenaline(epinephrine). (Lehninger, 728)
D-Phenylalanine can be decarboxylatedto phenylethylamine (PEA) which has am-phetamine-like stimulatory properties (foundin high quantities in chocolate) and requiresvitamin B6 for its conversion (Werbach, 142).
Methionine an other essential amino acidcan be converted through the action of me-thionine-adeosyl-transferase (MAT) to S-Adenosyl-L-Methionine or SAM. Both SAMand folic acid affect the turnover ofmonoamines, including serotonin anddopamine. In a study of 90 psychiatric in-patients normalization of enzyme activity wasassociated with clinical improvement. Therewas however a warning that SAM could in-duce mania in patients with bipolar illness.(For studies see Werbach, 143)
Ginkgo biloba has a vasodilatory effectand supplementation after 3-6 months hasbeen shown to have positive outcomes incognition among people suffering from Alzhe-imer’s Disease without hardly any adverseeffects. (Pken BS). It could therefore play arole in schizophrenia.
St John’s Wort (Hypericum) seems to beworking in the same way as SSRIs (SpecificSerotonin Reuptake inhibitors) and may be analternative antidepressant medication in mod-erate depression.
Pycnogenol or grape seeds extracts is apotent antioxidant and said to benefit patientswith dementia and brain syndrome. (Balch etal 1997, 466)
Coenzyme Q10 improves cerebral circu-lation.
ConclusionOn reason why many psychiatrists are re-
luctant to embrace nutritional therapy may bedue to the contradictory results of clinicalstudies in nutrition of groups of schizophren-ics. This assumes that there is such a categoryas ‘schizophrenia’.
These studies completely overlook RogerWilliams concept of Biochemical Individu-ality (Williams, Roger 1971) which empha-sizes the uniqueness of patients from a bio-chemical point of view. If the quantity of allthe natural chemical substances in our bodycould be represented as spokes emanatingfrom a central point, then individuals wouldpresent three dimensional constellationsuniquely different from one another. It can

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 11 -
also be assumed that the deviation from thenorm may be greater among schizophrenics.If this is the case, then the statistical compari-sons of subgroups of ‘schizophrenics’ intocontrol and experimental groups is inappro-priate as a scientific tool. There is no controlgroups, because all are different.
The popularity of the present scientificmethodology stems from studies concerningthe effects of xenobiotic chemicals on thehuman body, where other confounding bio-logical factors (such as age, gender, height,economic income etc) are controlled. Psy-chiatrists, using pharmaceuticals as their maintool, would be well versed in this methodol-ogy. This scientific model does fit the ‘onefactor’ experimental design. But if we look athumans through the eyes of Roger Williamsthen it is obvious that studies investigating theinfluence of nutrients on mental health cannotdescribe people assigned into groups and sub-groups (experimental and control) for statisti-cal purposes.
It is apparent that psychiatry will have togo into a different direction if they are really totreat psychotic disorders. Future psychiatristswill have to be thoroughly trained in clinicalnutrition (even herbalism), patients need to beintensively analyzed. They need to be testedfor biochemical abnormalities, for vitaminsand mineral deficiencies or excesses (for in-stance by means of hair analyses, blood andbiochemical assays, allergies and food sensi-tivities and so on). Psychiatrists may evenhave to reassess their scientific methodology.Thus in the future, the curriculum for studiesin psychiatry would have to place greateremphasis on extensive biochemical diagno-sis, followed by remedies other than pharma-ceuticals - away from xenobiotic to naturalsymbiotic remedies - which are patient-friendly.
The patient needs to be understood in termsof his biochemical individuality. There ap-pears to be no treatment for schizophrenia assuch, but there is for an individual sufferingfrom ‘schizophrenic’ symptoms. We maycome to understand his unique biochemicalmake-up and treat him accordingly.
In the meantime, it is up to the patients andtheir families to seek out ‘psychiatrists’ whoare familiar with not only pharmaceutical in-terventions - if these remain viable in thefuture - but more importantly with the princi-ples of clinical nutrition and other possiblemodalities that can alleviate the suffering ofmental disorders.
FootnotesAdams L. How exercise can help people with
mental health problems. Nurs Times1995;91: 37–9.
Balch JF & Balch PA (1997), PRESCRIPTIONFOR NUTRITIONAL HEALING: A practicalA to Z reference to drug-free remediesusing vitamins, minerals, herbs & foodsupplements, Avery Publishing Group, NY
Ban TA (1975), Nicotinic acid in the treatment ofschizophrenias: Practical and theoreticalconsiderations, Neuropsychobiol 1: 133-145
Baumblett MJ, Winston F (1970), Pyridoxine andthe pill. Letter, Lancet 1: 832-33
Belcher TL. Behavioral reduction of overthallucinatory behavior in a chronicschizophrenic. J Behav Ther ExpPsychiatry 1988;19: 69–71.
Bowers MB Jr.(1970) Cerebrospinal fluid 5-hydroxyindoles and behavior after L-tryptophan and pyridoxine administration
to psychiatric patients.Neuropharmacology 1970;9: 599–604.
Boyle M. Schizophrenia: a scientific delusion?New York: Routledge, 1990
Brooks SC el al.(1983) An unusual schizophrenicillness responsive to pyridoxine HCl (B6)subsequent to phenothiazine andbutyrophenone toxicities, Biol Psychiatry18(110: 1321-28
Bruce M, Lader M (1989), Caffeine abstention inthe management of anxiety disorders,Psychol Med 19: 211-14
Chaitow,L(1985), AMINO ACIDS IN THERAPY,Thorsons Pub. Inc N.Y.
Christensen O, Christensen E (1988), Fatconsumption and schizophrenia, ActaPsychiatr Scand 78: 587-591
Conroy RW, Smith K, Felthous AR. The value ofexercise on a psychiatric hospital unit. HospCommunity Psychiatry 1982;33: 641–5.
Cunnane SC, Horrobin DF (1980), Parentallinolenic and gamma-linolennic acidsameliorate the gross effects of zincdeficiency, Proc Soc Exp Biol Med 164:583
Cruz R, Vogel WH (1978), Pyroluria: A poormarker in chronic schizophrenia, Am JPsychiatry 135(10): 1239-1240
Dabiri LM, PastaD, Darby JK, Mosbacher D(1994), Effectiveness of vitamin E fortreatment of long-term tardive dyskinesia,Am J Psychiattry 151: 925-926
Dohan FC, Grasberger JC. Relapsedschizophrenics: earlier discharge from thehospital after cereal-free, milk-free diet. AmJ Psychiatry 1973;130: 685–8
DonaldsonJ, Barbeau A Managanese toxicity:Possible clues to the etiology of humanbrain disorders, in S Gabay et al Eds. MetalIons in Neurology and Psychiatry NYAlan R Liss 1985, pp259-85
Fierro AA (1988), Natural low dose lithiumsupplementation in manic-deprtessivedisease, Nutr Perspectives January 1988:10-11, as reported Werbach 86
File SE, Fluck E, Fernandes C. Beneficial effectsof glycine (Bioglycin) on memory andattention in young and middle-aged adults.J Clin Psychopharmacol 1999; 19:506–12.
Florence TM & Setright RT (1994), THEHANDBOOK OF PREVENTIVEMEDICINE, Kingsclear Books
Gottschalk La et al (1991), Abnormalities in hairtrace-elements as indicators of aberrantbehavior, Compr Psychiatry, 1991 quotedin Werbach, 10
Hawkins DR, Bortin AW, Runyon RP (1970).Orthomolecular psychiatry: niacin andmegavitamin therapy. Psychosomatics1970;11: 517–21 [review].
Head KA (2000), Inositol Hexanicotinate: a saferalsternative to niacin, Townsend Letter201: 88-92
Heresco-Levy U, Javitt DC, Ermilov M, et al(1996). Double-blind, placebo-controlled,crossover trial of glycine adjuvant therapyfor treatment-resistant schizophrenia. Br JPsychiatry 1996;169: 610–7.
Heresco-Levy U, Javitt DC, Ermilov M, et al.(1999)Efficacy of high-dose glycine in the treatmentof enduring negative symptoms ofschizophrenia. Arch Gen Psychiatry1999;56: 29–36.
Horrobin DF (1999), Lipid metabolism, humanevolution and schizophrenia, Prost LeukEssent Fatty Acids 60(5&6): 431-437
Kanofsky JD, Sandyk R (1992). Antioxidants inthe treatment of schizophrenia. Int JNeurosci 1992;62:97–100 [letter].
Kirschmann, JD(1979), NUTRITION ALMANAC ,McGraw-Hill Book Co. N.Y.
Kitahara M (1987), Dietary tryptophan ratio andsuicide in the United Kingdom, Ireland, TheUnited States, Canada, Australia and NewZealand, Omega J Death Dying 18: 71-76,from Werbach 145.
Kunin RA.(1976) Manganese in dyskinesias. AmJ Psychiatry 1976;133:105
Laugharne JD, Mellor JE, Peet M (1996), Fattyacids and schizophrenia. Lipids 1996;31Suppl: S163–5.
Lehninger AL(1982), PRINCIPLES OFBIOCHEMISTRY, Worth PublishersInc.N.Y.
Lohr JB, Caliguiri MP (1996), A double-blindplacebo-controlled study of vitamin E
treatment of tardive dyskinesia, J ClinPsychiatry 57, 167-173
López MJ, Sánchez CM, García de Lorenzo MA,Culebras F (1997), Magnesium: metabolismand requirements, Nutr Hosp 12(1): 4-14
McCreadie R, Macdonald E, Blacklock C et al(1998), Dietary intake of schizophrenicpatients in Nithsdale, Scotland: case-controlstudy, Br Med J 317: 784-785
Mikkelsen EJ (1980), Caffeine and schizophrenia,Behavioral Med Dec.
Norris JP, Sams RE. (1997) More on the use ofmanganese in dyskinesia. Am J Psychiatry1997;134:1448.
Pearson,D. & Shaw,S.(1982), LIFE EXTENSION;A Practical Approach, Warner Books,NY
Pfeiffer CC, Bravermann ER (1979), “Folic acidand vitamin B12 therapy for the low-histamine, high copper biotype ofschizophrenia, in MI Botez, EN ReynoldsEds Folic Acid in Neurology, Psychiatryand Internal Medicine, NY, Ravens Press1979: 483-487
Pfeiffer CC, Lamola S (1983), Zinc andmanganese in schizophrenia, J OrthomolPsychiatry 12: 215-234
Pfeiffer,CC.(1978), ZINC AND OTHER MICRO-NUTRIENTS, Keats Publishing Inc. NewCanaan,Connecticut
Pfeiffer CC, Audette L (1988), Pyroluria - Zincand B6 deficiencies, Int Clin Nutr Rev8(3): 107-110
Pken BS, Storzbach DM, Kaye JA (1998), Theefficacy of Ginkgo Biloba on cognitivefunction in Alzheimer’s disease, ArchNeurol 55(1): 1409-15
Potkin SG et al (1981), Wheat gluten challenge inschizophrenic patients, Am J Psychiatry138(9): 1208-11
Quattrocki E, Baird A, Yurgelun-Todd D (2000),Biological aspects of the link betweensmoking and depression. Harv RevPsychiatry 2000 Sep;8(3): 99-110
Ross-Smith P, Jenner FA (1980). Diet (gluten)and schizophrenia. J Hum Nutr1980;34: 107–12 [review].
Rudin DO (1981), The major psychoses andneuroses as omega-3 essential fatty aciddeficiency syndrome: Substrate pellagra,Biol Psychiatry 16(9): 837-50
Sandyk R, Kanofsky JD (1993). Vitamin C in thetreatment of schizophrenia. Int J Neurosci1993;68: 67–71.
Sandyk R, Pardeshi R.(1990) Pyridoxineimproves drug-induced parkinsonism andpsychosis in a schizophrenic patient. Int JNeurosci 1990;52: 225–32.
Schaeffer MC, Gretz D, Gietzen DW, Rogers QR(1998), Dietary excess of vitamin B-6 affectsthe concentrations of amino acids in thatcaudate nucleus and serum and the bindingproperties of serotonin receptors in the braincortex of rats, J Nutr 128: 1829-1835
Storms LH et al (1982), Effetcs of gluten onscizophrenics, Arch Gen Psychiatry 39:323-27
Tarrier, N (1998), Randomised controlled trial ofintensive cognitive behaviour therapy forpatients with chronic schizophrenia. BritishMedical Journal, 1998)
Taylor CB, Sallis JF, Needle R. The relation ofphysical activity and exercise to mentalhealth. Public Health Rep 1985; 100:195–202 [review].
Tkacz C. (1984) A preventive measure for tardivedyskinesia. J Int Acad Prev Med1984;8: (5)5–8.
Toll N,(1982) To the editor. J OrthomolecPsychiatry;11:42.
Vayda,William(1992), PSYCHONUTRITION:How to control your moods with foods,Lothian Publishing Co P/L, Melbourne
Wade, C (1980), LECITHIN BOOK, KeatsPub.Inc.,New Canaan,Conn.
Washburn CF, Reichert RG (1990), An hypothesisfor a mechanism for the pathogenesis ofpsychomimetic symptoms in gluten/gliadinsensditive individuals, J Orthom Med 5(3):175-78
Waziri R (1996). Glycine therapy of schizophrenia:Some caveats. Biol Psychiatry 1996;39:155–6.
Werbach,M.R.(1991), NUTRITIONALINFLUENCES ON MENTAL ILLNESS,Third Line Pres,Inc.,Tarzana,Cal.
Williams,R.J.(1971), NUTRITION AGAINSTDISEASE , A Bantam Book

The Hypoglycemic Health Newsletter June, 2001, Vol 17 No 2- 12 -
THE HYPOGLYCEMIC HEALTH ASSOCIATIONP.O.Box 830, KOGARAH NSW 1485
MEMBERSHIP APPLICATIONPLEASE PRINT
Surname:
First Name:
Address:
Town/City: Postcode:
Phone: Age:Membership $ 2 0 . 0 0 p aPens ioners $15 paLife Membership $ 2 0 0
RENEWAL
NEW MEMBER
Please t ick
Occupation
Do you have hypoglycemia? YES/NO Does a family member have hypoglycemia? YES/NO
2001 MEETING DATES ON FIRST SATURDAYSOF MARCH - JUNE - SEPTEMBER - DECEMBER
INTERNATIONALCLINICAL NUTRITION
REVIEW
By Editor
Dr Robert Buist, Editor in Chief ofthe ICNR, has indexed the InternationalClinical Nutrition Review which willbe updated in the last issue of each year.
This makes the series of InternationalClinical Nutrition Review a valuablecommodity in one’s private library foranyone who is interested in the scientificbasis of clinical nutrition.
Researchers from all corners of theworld review medical and other scien-tific literature and cull out the latest newson the clinical application of nutrients inthe treatment of disease. The serial alsopublishes in-depth-editorials written byexperts on various topics of concern toclinical nutritionists.
No longer can it be argued that thisnew branch of medicine is without sci-entific foundation.
A “must” for naturopaths and doctorswith an interest in nutrition, practition-ers and interested members of the publiccan subscribe to this quarterly publica-tion by sending $54.00 (New ZealandSubscribers $64) to:
Integrated TherapiesPO Box 370MANLY NSW 2095Australiahttp://www.intacad.com.au
Serious students might also considerthe one year correspondence course inNutritional Medicine. The course is reg-istered with ATMS and the $850 feeincludes all texts, tapes and study guidesas well as subscription to ICNR.
Please write to the above address forbrochure.
Doctor wanted to share apractice with Dr GeorgeSamra in Kogarah. Must
have an interest innutritional medicine or keento learn. Excellent terms and
conditions. Please ring9553-0084 for further
enquiries.
WANTED:The Editor is looking for amember who is willing to helpout in transcribing lecturesfrom tape a recording. Thevolunteer should have accessto a computer and should havefacilities to email reports to theEditor. We would appreciate itvery much if you could help usout.
over” into a diabetic, sooner than later.
We have both been put on new nutritionaldiets – sugar free and yeast free – and for mealso soybean free – for me personally, both asa cook and consumer, this has been extremelyfrustrating. Sometimes its very hard to change,even though you know its for the better in thelong term, and you certainly miss the “sweet”taste of foods. When shopping you quicklydiscover that well over 90% of our foods havesome content of sugar, yeast and preserva-tives contained in them. It has been ex-tremely frustrating for me to find recipes toprepare which fit the diet schedule, as I havebeen so used to preparing meals with saucesand ingredients which have been sugar/yeastbased, but am continually trying new ideas.Our new diet consists of chicken, fish, lamb,fresh fruit (for me only to be eaten with ameal) and vegetables, and lots of home cook-ing which is sugar/yeast free! Out go all mycookery books!! Both my husband and I havenoticed the changes in ourselves – he has lost4-5lbs – I don’t wish to as I only weigh 8stone! We both eat six small meals a day andI myself need to eat every two and a half-hours! I know that if I miss this time framethen I become extremely hungry and light-headed, start to feel anxious and even feel“weepy”. At time I find this very hard to cometo terms with as I have never undergone thisgreat a change in my body before.
But thanks to the wonderful support of myhusband, and my doctor who has put us both
on the right track back to good health, I feelnow that there is a light at the end of the tunneland life is not as gloomy nor stressful as it wasonce before.
From Page 2
Attention is drawn to our new Web Site at:w w w . c o m p a n y o n t h e w e b . c o m /
hypoglycemia_australiawhere you'll find articles on clinical nutrition and
self-help psychotherapy. We also have an article dealingwith the treatment of drug addiction. Copies of Newslet-ters are also available.
The following Committee Members can be con-tacted by email at:
Sue Litchfield, [email protected] Plesman, [email protected] & Reg Grady,[email protected]