Embed Size (px)
Citation preview
The History and Curmnt Use of Ankle Brace Technology
THOMAS Wm MMi%#SR4, PhD, ATG-L Director, Undergraduate Athletic Training Education University of Florida
Ankle injuries, especially lateral ligament sprains,
are common in sports
and restricting motion, especially subtalar joint motion, ankle stabil- ity will be increased (Miller & Hergenroeder, 1990). The goal is to prevent the talus from exceeding its physiologic range of motion within the ankle mortise. These ankle braces act as external ligaments helping to reduce the amount of anatomical motion in the subtalar joint, especially inversion.
A number of studies have reported on the effects of ankle bracing on range-of-motion and performance parameters, but few have examined their effectiveness in preventing ankle injury. Given the multitude of choices and styles available, it is important that the athletic therapist under- stand which features are most important.
s have s lges ovc
,-
lev- Ir tape
7 . ruing ease or appnca- and result in more time loss than any other single injury (Garrick, 1987). The high intensity nature of sports requires optimal neuromuscular development and control of the lower extremity. Basketball, volleyball, soccer, and football have the highest inci- dence of inversion sprains.
Prevention and treatment pro- grams for ankle injuries can be time consuming and costly. Ankle bracing has been part of the treat- ment and rehabilitation of ankle sprains for years. It is important that athletic therapists have a knowledge and understanding of the various types of ankle braces available today.
The majority of ankle sprains involve the lateral ligamentous structures, primarily the anterior talofibular and calcaneofibular ligaments. Most sprains occur with the foot inverted and the ankle plantar flexed. The dynamic stabilization offered by concentric contraction of the peroneals and eccentric action of the invertors is overcome, thus disrupting the
fort.
rthoses, s e m ~
Athl ~n 17 nderstandin~l o
etic the] CLLL U
varic bracc ~ 1 - - ..
>us type 2s so tht :-I.< -.-
V
!s of anl 2y can F
me r treat
ignr one Tor rnt ment 01
ligamentous constraints to this movement. As the physiologic range of motion is exceeded, in- jury occurs.
A common objective of many athletic therapists is to prevent this occurrence via external sup- port (taping or bracing). The ulti- mate goal is to prevent injury or
- reinjury. The rationale for ankle brac-
ing is based on the assumption that by reinforcing the ligamen- tous structures of the ankle joint
of Ankle Wcaces Ankle braces have several advan- tages over tape in that they can be self-applied without needing the expertise of qualified personnel; they are easy to apply and remove and are reusable, readjustable, and washable. Qualities to look for in the ideal ankle brace include
O 1998 Human Kinetics
32 b%ahleECe Thatmpy Today July 1998

the following (Miller & Hergen- roeder, 1990):
1. Ease of application;
2. Ability to retain a continuous degree of support through- out an exercise period;
3. Ability to provide an equiva- lent degree of support with each application;
4. Ability to limit the extremes of subtalar joint inversion and eversion while permit- ting talocrural joint dorsiflex- ion and plantar flexion;
5. Affordability.
A PHOTO 1 Typical lace-up ankle brace.
Other factors to consider in- clude comfort, personal prefer- ence, age, and type of sporting activity. Early ankle braces were made of heavy canvas materials that were cumbersome and unfor- giving. New braces utilize more lightweight and breathable syn- thetic materials that are just as durable and resilient.
Ankle braces may be classified into two primary categories: non- rigid stabilizers and semi-rigid orthoses (Photos 1 and 2). The non-rigid stabilizers, commonly re- ferred to as "lace-up" ankle braces, are made of lightweight canvas, vinyl laminate, or neoprene
materials that are comfortable and easy to slip on and off. Most have lacing features. The semi-rigid braces consist of two bimalleolar struts made of plastic materials connected via elasticized straps.
Although ready-made elastic pull-on and neoprene ankle sup- ports are part of this category, by far the majority of these types of stabilizers are the reusable lace-up ankle braces. These braces gener- ally can be made more rigid by in- serting plastic stays into the side pockets of the brace shell. These are designed to provide addi- tional stability to the ankle.
A number of off-the-shelf ankle braces are available today. Some of the more common brands include: McDavidm lightweight ankle support (McDavid Sports Medical Products, Chicago); Swede-O@ Ankle Lok ankle brace (Swede-0, Inc., North Branch, MN); Cramer@ ankle stabilizer (Cramer Products, Inc., Gardner, KS); and MuelleP Bi-Lateral ankle brace (Mueller Sports Medicine, Inc., Prairie Du Sac, WI).
Although these ankle braces are marketed with a variety of ad- vertising claims, they all have similar features: (a) bilateral sup- ports made of materials sewn to- gether allowing for an opening at the heel; (b) elasticized heel counter to prevent irritation of the Achilles tendon; (c) padded, elas- tic tongues beneath the laces; ard (d) built-in stays or side-pockets in which plastic stays can be in- serted freely.
The effectiveness of these ankle braces has often been com- pared to that of tape. Initially these braces provide less support than properly applied tape (Bunch et al., 1985). However, as
activity continues, tape tends to slacken whereas ankle braces can be retightened to provide continu- ous support and stability.
A retrospective study examin- ing ankle injuries in football play- ers concluded that ankle braces were more effective than tape in preventing ankle injuries (Rovere et al., 1988). Lace-up stabilizers tend to maintain range-of-motion re- strictions better than tape because of the retightening capabilities.
Semi-Rigid Stabilizers Another popular class of ankle braces include the semi-rigid orthoses. First mentioned in the medical literature in 1979 (Stover), these devices have been shown to be equally effective when com- pared with tape for restricting range of motion. They were originally designed for use in early immobilization of acute ankle sprains or stable lower leg and ankle fractures. As technology advanced, the changing design of these braces has enabled them to be used prophylactically.
A variety of semi-rigid ankle braces are available for the athletic therapist to choose from. They are designed to fit into the athlete's shoe and may be worn during activity. These braces contain a prefabricated, thermoplastic
PHOTO 2 Semi-rigid ankle orthosis.
July 1998 That Pr~IIessiolnal dsurwal Bov Athle%lc Tmlners and me?aaplsSs 33
.aoys e oquy JLJ 04 Bysea pue hpq ssal axe dnensn sascxq pods ayL sGnLugsod d~aqerpaurvuy dqy~~qeqs xaqeax2 mj sdnxqqs xa2uo1 pup
.-- 'hynyse 2upnp pasn aq ues qeyq sdqs xaqxoys yqy~ asexq pods e xajjo sxaxnqaejnuem ?son
.sxossasapaxd qayq my3 xaneurs Vnm axe sasoqlo awe p@p-was au .sasvap qayq jo uoyanysuos ayq q qeyaqeur alqeyqeaxq 'qy2ya~ -qy2yl jo asn ayq qnoq sxaxnqaq -nuem jo rijyxo~em ayL esxead ayq y2noxyq saxqeaj pue Bysap asexq alyue q~y~ pa2u~y3 spy a~q~y
'qsaaxyv) dnxxyqs-xyv @qsesxyv :apnpuy sasexq alyue py2yx -!mas aIqeIyE?AE d11~ysxammos ayq jo amos jo Buyldmes v
.&vqe-~eaysllyd 2qxnp as001 - aurosaq day4 p pauaqysy aq Leu day3 'spedxaqunoa p@p-uou qayq aTy .uoysxana pue uoysxanq 2ugy -q appi uoyxapsxop pup uoFaU xequeld ape xoj Moue oq pau%ys -ap axe sasexq asayL -%a1 xaMo1 ayq punoxe sdeqs arqsela xo oxaIaA 2uysn pamaas axe sasexq qsom
.sdwyqs ayq jo aprsuy ayq2uole xaqqru auaxdoau xo 2uypped meoj asn sasoyqxo p@p-yas apem-dpeax jo xaqmnu -v 'sitauTr 2eq x~e aIqeqewT xauq - -*
asn may4 jo Ile qou 'sdnxx~qs-xye se 03 paxxajax uaqjo axe sasexq jo saddq asayq y2noyqlv
-goallem ayq anoqe sayauy Iexanas puaqxa uayq sdnx -xgs ayL yoa1lem yqoq pue qooj ay? $0 y3" aayq punoxv $?j 2eyq sapys syqse~d paplow xo dnxxrqs
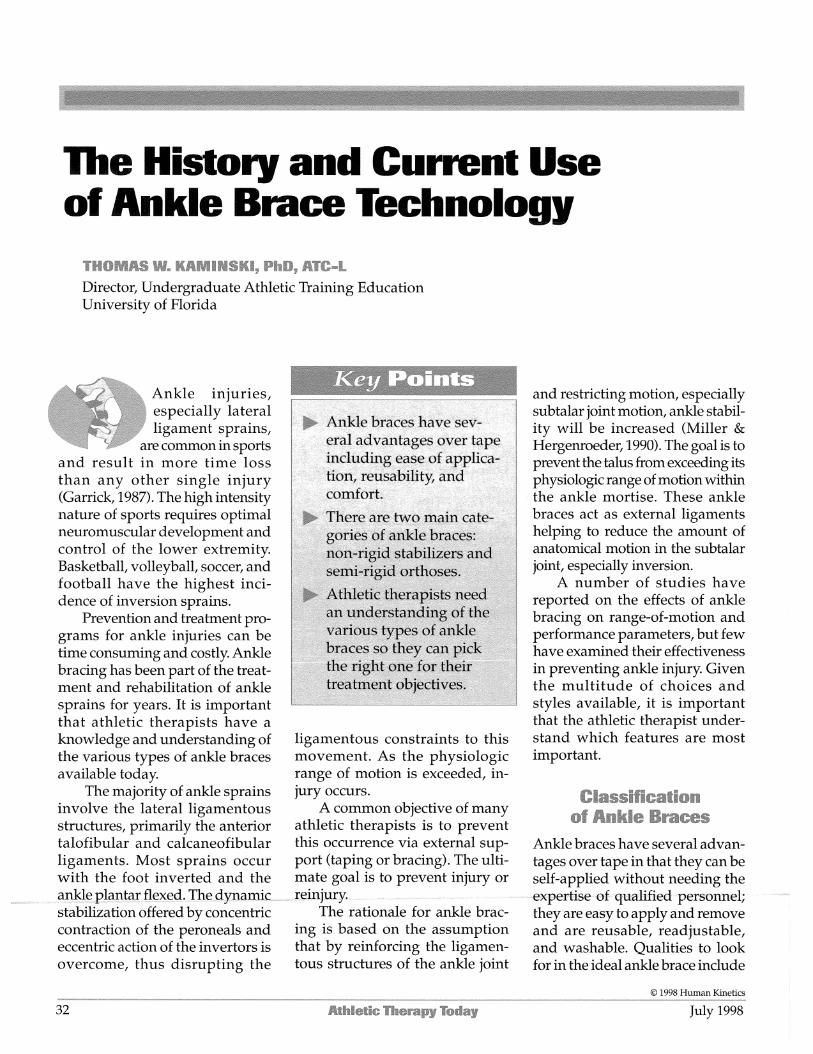
-asueunojxad xoqour llemaao uo qsajja Iequamyxqap alqqy aney sasoyqxo asayq qeyq sy snsuasuos ayq 'pauymexa sy asueuuojxad uo sasexq anue py2p -:mas asayq jo qsajja ayq uayM .saaexq alyue py2p-!mas 2upea~ saqalyqe Suome sayxnLuy alyue jo ales ayq 2uyqenlena ysxeas -ax aIUy1 uaaq sey axayL 'Suldeq xano 2uysexq alyue 2ulsooya uayM uoyqesyldde jo asea pue qxoj -mos all3 uaqjo sxaxealzl asexg
'(P66T "1" 4a UOSUYO~
asysxaxa jo sassaxqs ayq xapun sayqy~rqedes any~syxqsax-a2uex xyayq uyeqax oq dqylyqe quaxayuy ue aney sasoyqxo py2yx-ymas asayL -aspxaxa xaqje pue axoj -aq yqoq uorsxana pue uoysxanuy qsyxqsax 03 punoj uaaq aney sasexq py2yx-!mas $son '(1 alqq aas) 2uydeq alyue oq suospedmos panlonuy sey sasexq alyue py2~ -!mas asayq jo daesyjja ayq uo ysxeasax jo dqyxo[sw ayL
'(-st11 '0-apa~s) aaexg ,,moqv pue i(v3 'peqs~.1~3 '-~UI /rioluoa) xopaTox6 quame2y~ anuv doluoa !(AX 'allynslnoy "3u1 'smaqsds alyuv anyqsv) aaexg 2uyuyex~ alyuv an:q3v !(IN 'qlmmns '-2111
a2 rrr 33v.1
2L?$J"P 01
Both the non-rigid and semi- son of support provided by a semirigid Paris, D.L., Vardaxis, V., & Kokkaliaris, J. (1995). orthosis and adhesive ankle taping before, Ankle ranges of motion during extended
rigid ankle braces offer a cost- during, and after exercise. American Jour- activity periods while taped and braced. effective way to restrict ankle nal of Sports Medicine, 18,498-506. Journal of Athletic Training, 30,223-228.
range of motion. Athletic thera- pists should base their decisions to use ankle bracing on a careful cost-benefit analysis as compared to ankle taping. Ankle bracing offers a nice alternative to taping and has become a popular form of ankle injury prophylaxis. Fur- ther study is needed to determine the extent to which braces are used and their efficacy in prevent- ing ankle sprains.
As the cost of ankle taping has risen through the years, ankle bracing has offered a viable and cost-effec- tive alternative. Athletic therapists need an understanding of the vari- ous types of ankle braces available so they can match their injury prevention/ treatment objectives with a particular kind of brace.
It is generally agreed that both the non-rigid and semi-rigid forms of ankle bracing are equilly if not more effective than tape in helping to restrict ankle range of motion. Furthermore, braces tend to retain these restrictive qualities longer than tape. Since there is not much literature examining the ex- tent to which braces can prevent ankle injury or reinjury, however, one must give careful consideration before deciding to use a brace.
Ref ere wces Bunch, R.P., Bednarski, K., Holland D., &
Macinanti, R. (1985). Ankle joint support: A comparison of the reusable lace-on braces kith taping and wrapping. Physi- cian and Sportsmedicine, 13,59-62.
Frankey, J.R., Jewett, D.L., Hanks, G.A., & Sebastianelli, W.J. (1993). A comparison of ankle tape methods. Clinical Journal of Sports Medicine, 3,20-25.
Garrick, J.G. (1987). Epidemiology of foot and ankle in'ies. Medicine 8 S& Science, 23.1-7.
Greene, T.A., &Wight, C.R. (1990). Acompara- tive support evaluation of three ankle orthoses before, during, and after exercise. Journal of Orthopedic and Sports Physical Therapy, 11,453-466.
Gross, M.T., Bradshaw, M.K., Ventry, L.C., & Weller, K.H. (1987). Comparison of sup- port provided by ankle taping and semi- rigid orthosis. Journal of Orthopedic and Sports Physical Thempy, 9,190-193.
Gross, M.T., Batten,A.M., Lamm,A.L., Lorren, J.L., Stevens, J.J., Davis, J.M., et al. (1994). Comparison of DonJoy ankle ligament protector and subtalar sling taping in re- stricting foot and ankle motion before and after exercise. Journal of Orthopedic and Sports Physical Therapy, 19,33-41.
Johnson, R.E., Veale, J.R., & McCarthy, G.J. (1994). Comparative study of ankle sup- port devices. Journal of the American Podi- atric Medical Association, 84,107-114.
Lindley, T.R., & Kernozek, T.W. (1995). Taping and semirigid bracing may not affect func- tional range of motion. Journal of Athletic Training, 30,109-122.
MacKean, L.C., Bell, G., & Burnham, R.S. (1995). Prophylactic ankle bracing vs. tap- ing: Effects of functional performance in female basketball players. Journal of Ortho- pedic and Sports Physical Therapy, 22,77-81.
Miller, E.A., & Hergenroeder, A.C. (1990). Pro- phylactic ankle bracing. Pediatric Clinics of North America, 37,1175-1185.
Rovere, G.D., Clarke, T.J., Yates, C.S., & Burley, K. (1988). Retrospective comparison of taping and ankle stabilizers in preventing ankle injuries. American Journal of Sports Medicine, 16,228-233.
Sitler, M., Ryan, J., Wheeler, B., McBride, J., Arciero, R., Anderson, J., & Horodyski, M. (1994). The efficacy of a semirigid ankle stabilizer to reduce acute ankle injuries in basketball. Arandomized clinical study at West Point. Amerimn Journal of Sports Medi- cine, 22,454-461.
Stover, C.N. (1979). A functional semirigid sup- port system for ankle injuries. Physician and Sportsmedicine, 7,71-78.
Surve, I., Schwellnus, M.P., Noakes, T., & Lom- bard, C. (1994). Afivefold reduction in the incidence of recurrent ankle sprains in soccer players using the sport-stirrup orthosis. American ~ournal of Sports Medi- cine, 22,601-606.
Verbugge, J.D. (1996). The effects of semirigid Aircast a i rs t i rp bracing vs. adhesive ankle taping on motor performance. Journal of Or- t w i c a n d Sports Physical Thevapy, 23,320-325.
9"" ' "m
Thomas W. Kaminski is an assistant professor and director of the undergraduate athletic training education program at the University of Florida. He also serves as an athletic training consultant to the women's soccer team there.
The Pro1 econon
educatic
Thi
'essional Ac . -0nvenient and L I ~ L ~ J W ~ V LU CIUI~IJCC VUUJ ~ l ~ l ~ 3 3 1 ~ l l d l CAUCJL~SC UI C A ~ continuing )n credits. '
s new COUI
-
se teaches apply to f
. .
V
Self-study .-
Program (I .-:,.-..I
PASS) is a ( -A:-- --
i,gy ~ ] ~ ~ o r
athletes ba acilitate tht
t I n j u ~ is c
sic psycho1 :ir rehabilit . . , .
ogical skill atlon.
2 new cour
s they can
lete details about this tlmely new course, Human Kinetics at or visit the Human Kinetics
://www.humankinetics.com/
Human Kinetics and the NATA
nun KINE'
Green, T.A:, & Hillman, S.K. (1990). Compari-
- -,...-..----- - -- - -- - --- - -A- ----- -- -- - - July 1998 The b k s s l o n a l Jourmabi far A%hhie%ic Tml~ew and Thempists 35