Embed Size (px)
Citation preview

SPECIAL FEATURE—
IHS Annual Reportto Members
PROFESSIONALPROFESSIONALHEARINGHEARING
Official Journal of the International Hearing Society
THETHE
MARCH–APRIL 2007

Finally the hearing impaired will become the hearing empoweredThe enabling power of connectivity will provide the most improved communication experience available.
The RISE wireless microchip platform is the fi rst
hearing instrument architecture built from the
ground up with connectivity as a key capability.
Bluetooth connectivityWith embedded Bluetooth connectivity, the RISE
wireless micro chip platform will transform hearing
instruments into personal communication systems –
one might even say the world’s smallest binaural
headsets – opening the world of effortless mobile
phone communication with clean and clear sound
in both ears.
Binaural broadband processingGone are the days when hearing instruments “only”
corrected for a hearing loss. New hearing instruments
containing RISE will act as the interface between the
user’s auditory system and the world of sound through
binaural broadband processing. Users will obtain a more
accurate understanding of the sound environment and
the ability to identify where sounds are coming from.
For more information please call 1-800-526-3921
or visit www.oticonusa.com

THE HEARING PROFESSIONAL 1
VOLUME 56, No. 2 • MARCH–APRIL 2007(USPS 036-940)
16880 Middlebelt Rd., Ste. 4, Livonia, Michigan 48154Telephone: 734.522.7200 • FAX: 734.522.0200 • Website: ihsinfo.org
THE HEARING PROFESSIONAL (ISSN 0004-7473) is published bimonthly for members of theInternational Hearing Society (IHS), 16880 Middlebelt Road, Ste. 4, Livonia, Michigan 48154. Peri-odicals postage paid at Livonia, Michigan and additional mailing offices. POSTMASTER: Send ad-dress changes to The Hearing Professional, 16880 Middlebelt Road, Ste. 4, Livonia, Michigan 48154.
THE HEARING PROFESSIONAL is the official journal of IHS, a nonprofit association of profes-sional Hearing Instrument Specialists.® Its purpose is to present authoritative technical and businessinformation that will help hearing aid specialists serve hearing impaired people.
Copyright © 2007 International Hearing Society
IHS members, Hearing Instrument Specialists,® are engaged in the practice of testing human hearingand selecting, fitting and dispensing hearing instruments. Special membership categories of the Societyoffer membership to those who are involved in or have an interest in the hearing instrument profes-sion, but are not actively fitting and dispensing hearing aids. Call 734.522.7200 for informationabout IHS membership.
OFFICERS AND GOVERNORS
EDITORIAL COMMITTEE EDITORIAL STAFFPatricia Connelly, PhD, CCCA, ABA (Chair) Cindy Helms, PublisherGranville Brady, AuD Autumn Kovach, Managing EditorKathy-Jo Facteau, BC-HISKenneth Laferle, BC-HISRaymond Loercher, BC-HIS, ACA
THE HEARING PROFESSIONAL is circulated to all Hearing Instrument Specialists,® other membersof IHS and to selected hearing aid manufacturers and suppliers. Advertising rate cards available on re-quest. Subscription is free to all members of the Society. Paid subscriptions are available for $35 inthe United States and Canada and $45 in all other countries. Contact IHS for additional details.
INFORMATION contained in articles, editorials or paid advertising does not represent the endorsementof any specific product nor is IHS responsible for opinions or interpretations expressed by contributors.
MICROFILM BACKFILES available from University Microfilms, Inc., Serials Acquisitions, 300 N.Zeeb Road, Ann Arbor, Michigan 48106.
Manuscripts: Researchers, practitioners, and others are invited to submit articles and papers for publica-tion. THE HEARING PROFESSIONAL assumes no responsibility for return of unsolicited materials.
MARCH–APRIL 2007
ContentsTHE HEARING PROFESSIONAL
James Ogurek, BC-HIS 715.842.9882PresidentChris Gustafson, BC-HIS, ACA 503.472.8850President-ElectLarry Farris, BC-HIS, ACA 210.342.2299SecretaryBruce Sharp, BC-HIS, ACA 801.484.3277TreasurerHarlan Cato, BC-HIS 704.333.9055Immediate Past President
J. Scott George, BC-HIS 417.466.7184John Letts, BC-HIS 306.343.9516Alan Lowell, BC-HIS, ACA 407.905.2950Marsha Mattingly, BC-HIS 304.525.7221Jay McSpaden, PhD,
BC-HIS, CCCA 541.979.3422Therese Wolf, BC-HIS, ACA 616.988.2158
2 President’s MessageBy James Ogurek, BC-HIS
3 IHS Annual Report 2006
11 Continuing Education:Counseling Theories Applied to Fitting Hearing LossesBy Granville Y. Brady, Jr., AuD
14 Global Spotlight:A Report from the Canadian Hearing InstrumentPractitioners Society (CHIPS)
16 Research ReviewBy Patricia E. Connelly, PhD, CCCA, ABA
18 Membership Matters:One Professional’s JourneyBy Sandra Hubbard, BC-HIS, ACA
20 ChapterTrack
23 IHS Membership Application
25 Soundbytes
26 IIHIS Approved Courses
27 IIHIS Continuing Education Test
28 Classifieds
28 Ad Index
THE HEARING PROFESSIONAL 1
Power Shopping Without Dropping!We’ve all enjoyed the ease and convenience of online shopping. From thecomfort of our homes or offices, we can evaluate products, compare pricesand make our selections without the time-consuming hassles of a trip tothe mall.
And now there’s an even better reason to reach for your keyboardinstead of your car keys.
IHS has a new and exciting fundraising opportunity called MyFundrazor, an online shoppingcommunity with hundreds of major retailers. Each time you shop through IHS.myfundrazor.org,we receive a percentage of the purchase. It’s simple, secure and requires no registration fee orpersonal information—a fun and easy way to support your professional association.
Think IHS first whenever it’s time to shop for gifts, office supplies, household goods,and more. Just go to the IHS website and hit the MyFundrazor access button.Your favorite stores are just a click away, and the onlinedeals are often better than store prices. Everyone wins!

PRESIDENT’S MESSAGE
MARCH • APRIL 20072
Greetings from all of us at IHS.
One of the important roles IHS fills is to monitor and affect the regulatory and legislative
environment in which we all work. The only way we can effectively serve the hearing impaired is to
create and maintain a regulatory environment that allows the public to choose their provider.
There has been a surge in legislative efforts in the last six months that could affect open access
or create advantages to one profession over another. IHS employs a legislative reporting service that
monitors legislative proposals nationwide. Occasionally, however, members and chapters become
aware of proposals in advance of IHS or the reporting service. It is imperative that members and
chapters contact IHS immediately if their states or provinces are advancing proposals. IHS has
tremendous experience and resources that can assure that these legislative initiatives result in open
access for all qualified providers. It is equally important that no provider group gain a competitive
advantage because of legislation. A level playing field for all providers is in the best interest of the
consumers we serve.
As legislative challenges arise, we must use a team approach to assure a positive result. IHS
leadership, staff, membership, and chapters must pool their resources, knowledge, and talent.
If chapters or members attempt to address these issues alone the results may have serious
consequences to our future success. It is important to remember that what happens in other states
and provinces can and will affect other markets. We must take this leadership role to create and
maintain a legislative environment that serves all qualified members of the hearing healthcare team.
The hearing impaired public deserves this kind of delivery system.
IHS can and will continue its appropriate role as the international organization committed to
assuring quality hearing healthcare by all qualified provider groups. With your support and effort,
IHS will continue to build on a 55-year history of leadership.
Thank you for your membership and your dedication to the care of the hearing impaired.
Best wishes for a successful 2007.
James Ogurek
President
P.S. Register now for the IHS Convention and Expo in Reno, Nevada, September 26–30, 2007.
By James Ogurek, BC-HISIHS President

THE HEARING PROFESSIONAL 3
Mission StatementThe Society advocates and supports
the highest standards of professional
competency, business integrity, and excellence
in serving the hearing impaired.
2006

MARCH • APRIL 20074
As we proudly present the 2006 annual report, I wish to thank the members of the International Hearing Society
for their loyalty and trust. The Society’s 55th year was immensely successful and you all played a part in helping
us soar to even higher levels of excellence, stature, and growth.
This stellar year of achievement ended with a resounding note of triumph. We are pleased to announce that 2006
finished with revenue well over expenses—to the tune of $100,000 plus. The bulk of this net gain is due to membership
development and retention, reinvigorated sources of non-dues revenue, administrative and program improvements,
and a commitment to top-quality service by the Board of Governors and staff.
This report highlights some of the more noteworthy accomplishments for 2006. You will see that our advocacy
efforts are still front and center and we broadened our legislative reach in safeguarding your right to practice.
In addition, we strengthened chapter relations and found new ways in which to share resources, consolidate our efforts,
and energize our partnerships. We restructured the convention to maximize its value. We demonstrated that our
educational programs continue to be the best in the business. We fortified our collaboration with AAO-HNS and other
hearing health organizations. We expanded our global presence and welcomed new members from around the world.
And it’s on behalf of our members—both new and old—that we’ve worked so hard to provide the best possible
value for your dues contribution. We’ve shone a brighter spotlight on our members by seeking your thoughts, opinions,
and ideas in order to better represent your wants and needs. We’ve become more interactive with the members by
increasing the volume of communications to you and encouraging your direct contact with leadership and staff.
2006 was indeed a banner year and we can all take pride in its extraordinary success. Together, we will build
on these victories as we capitalize on the exciting opportunities the future holds for the Society and the profession
at large.2006
An
nu
al R
epo
rtF R O M T H E E X E C U T I V E D I R E C T O R
A Victorious Year:Introduction to the
2006 IHS Annual Report
By Cindy J. Helms

THE HEARING PROFESSIONAL 5
2006
An
nu
al R
epo
rt
We are very pleased to announce a robust bottom line for2006, with year-end revenue over expenses in the amountof $106,537. This dramatic comeback from the financialchallenges of recent years underscores the diligence ofmanagement and the Board of Governors in their effortsto ensure the utmost regard for fiscal responsibility.
The Society’s remarkable financial success in 2006 isalso largely attributable to the continued support of our
membership. Your Board of Governors and staff havehonored your commitment to the Society by putting yourmembership dollars to work in ways that provide themaximum return on your investment. On your behalf wewill continue to be guided by our mission to protect andpromote the hearing instrument specialist profession,provide the highest level of member advocacy and sup-port, and grow the Society for a prosperous future.
2006 STATEMENT OF OPERATIONS
REVENUEMembership $ 573,012
Advocacy $ 79,028
Education $ 454,140
Convention $ 266,130
Administration $ 24,941
Advertising (incl. misc. sales) $ 60,281
Total $1,457,532
EXPENSESMembership $ 8,831
Advocacy (incl. legal services) $ 87,976
Education $ 131,522
Meetings (incl. convention, governors,and committees) $ 331,644
Administration $ 706,734
Communications $ 84,288
Total $ 1,350,995
Revenue over expenses — $106, 537
Federal Government RelationsOne of the most important member services provided bythe Society is federal advocacy and outreach. This workto affect legislation and regulations and to develop rela-tionships and coalitions with others in the hearing healthsector is designed to expand the benefits of amplificationto an increasing number of the hearing impaired andtheir families, and to safeguard your ability to servethem. For more than thirty years, the Society has main-tained the same Washington Counsel, Tim Waters ofMcDermott Will & Emery LLP. For more than a decade,Karen Sealander, also of McDermott Will & Emery LLP,has advocated with Waters on the Society’s behalf.
TAX CREDIT LEGISLATIONIHS and others in the hearing health community haverallied in support of a proposal designed to expand thebenefits of amplification to an increasing number ofAmericans. Significant progress was made in 2006 toadvance legislation that would provide a tax credit forthe purchase of hearing aids.
The Hearing Aid Assistance Tax Credit Act wouldallow a non-refundable income tax credit, availableevery five years, of up to $500 per hearing aid for thepurchase of a hearing aid for those age 55 or older andthose claimed as a taxpayer’s dependent. Importantly,the legislation has no restrictions on who may dispense
the device and no restrictions on the technology avail-able to the patient.
Because the legislation was not enacted prior to the ad-journment of the 109th Congress in 2006, it must be rein-troduced in the 110th Congress. IHS and others will workvigorously toward its passage. IHS members are encour-aged to thank their manufacturers for their leadership onthe hearing aid tax credit legislation and also to contacttheir U.S. Senators and Representatives regarding cospon-sorship when it is reintroduced later this year. IHS head-quarters can provide talking points on the proposal, sam-ple letters to legislators, and other related materials.
BETTER HEARING AND SPEECH MONTHIn May 2006, in appreciation of National Better Hear-ing and Speech Month, IHS, along with the AmericanAcademy of Audiology (AAA), the American Academyof Otolaryngology—Head and Neck Surgery (AAO-HNS), the American Speech-Language-Hearing Associa-tion (ASHA), the American Tinnitus Association (ATA),the Hearing Industries Association (HIA), and the Hear-ing Loss Association of America (HLAA), hosted ahearing screening and issues forum in the U.S. Capitol.
This event was convened by the Congressional Hear-ing Health Caucus. The Society is pleased to serve onthe Friends of Hearing Health Care, the advisory groupknown formerly as the Congressional Hearing HealthCaucus Advisory Committee.
ADVOCACY AND OUTREACH

IHS MEETS WITH WHITE HOUSE LEADERSIn November 2006, IHS and representatives of other or-ganizations in the hearing health sector met with theAssociate Director of President Bush’s Domestic PolicyCouncil Olegario Cantos.
The meeting discussed the importance of hearing healthto overall health and general well-being, efforts to makehearing instruments more accessible, and the proposedhearing aid tax credit.
IHS AND AAO-HNS PARTNERSHIPIHS collaborates very effectively with AAO-HNS on fed-eral legislative, regulatory, and public affairs matters. We
MARCH • APRIL 20076
2006
An
nu
al R
epo
rthave, for example, written numerous joint letters to theFDA and conducted numerous joint meetings with FDAofficials, Members of Congress, and congressional staffto advance our shared view that entry into the hearinghealthcare delivery system through all three providers(physicians, hearing instrument specialists, and audiolo-gists) must be preserved. We also joined together to formAmerica’s Hearing Healthcare Team (AHHT), which ad-vocates a multidisciplinary team approach with access toall qualified providers.
The leadership of both organizations meets annually todiscuss issues of critical importance and explore new waysin which their partnership can be mutually supportive.
Snapshot of Recent Successes• Withdrawal of the FDA rulemaking from the U.S. Department of Health and Human Services’ (HHS) Unified Agenda.
The FDA repeated rejection of Citizen Petitions seeking a new over-the-counter classification for “one size fits most”hearing aids.
• HHS Secretary Tommy Thompson applauded IHS for its work in expanding the benefits of amplification to an increasingnumber of Americans and expressed the secretary’s intent to raise the visibility of the importance of hearing health andto urge Americans to have their hearing loss treated.
• The U.S. Senate passed a Congressional Resolution urging Americans to get their hearing checked regularly.
• IHS and AAO-HNS launched a state liaison effort affording state chapters the opportunity to work together on statelegislative and regulatory issues.
• HIA united the hearing health community in support of legislation calling for a tax credit for the purchase of hearing aids.IHS, along with AAA, ASHA, HLAA, and HIA, conducted joint congressional visits on Capitol Hill.
• Members of Congress formed the Congressional Hearing Health Caucus and IHS was invited to serve on the CaucusAdvisory Board. A meeting was held and referral cards with links to provider directories on the IHS, AAA, ASHA, andAAO-HNS websites were provided to congressional staff and legislators.
• An article in the Journal of the American Medical Association (JAMA) stated that hearing loss is the third most commonchronic condition in older Americans and that, despite the availability of effective treatment, hearing loss is substantiallyunderdetected and undertreated in primary care settings.
• The National Institute of Deafness and Communication Disorders and the Veterans Administration published a jointstudy in JAMA which states that hearing aids work.
• A hearing guide published by AARP heralded the praises of amplification and cautioned potential hearing aid users againstunrealistic expectations.
• A study by the National Council on the Aging found that the use of hearing aids improves quality of life and health.
• The federal government recognized hearing aid specialists as healthcare practitioners in the Standard OccupationalClassification Manual.
• BHI released a documentary for public television stations entitled “Spotlight on Hearing Loss,” which is designedto help overcome the widespread resistance to dealing with hearing loss. The program, which has a guaranteedminimum viewing by 3 million viewers, recognized audiologists, hearing instrument specialists, and physicians as hearinghealthcare providers.

COOPERATIVE ADVOCACYIHS recognizes the value and importance of coalitionsand seeks to work cooperatively with other organiza-tions in hearing health advocacy efforts whenever possi-ble. In June 2006, IHS joined with more than twentyother organizations including the Academy of Dispens-ing Audiologists, AAA, AAO-HNS, the American Med-ical Association, and ASHA to sign a joint letter sent toall Members of Congress urging support for and fund-ing of early hearing detection and intervention pro-grams at the Health Resources and Services Administra-tion and the National Center on Birth Defects andDevelopmental Disabilities.
EYE ON THE FDAEven though in 2001 we were successful in halting theFood and Drug Administration’s efforts to rewrite thehearing aid rule, the Society’s vigilance in Washington isabsolutely imperative. Though the monumental battle iswon, renewed efforts to revamp the nation’s federal dis-pensing rules could occur and we need to be on thealert. The federal government has the power to shapeboth the public’s perception of hearing instruments andhearing instrument providers as well as the authority torewrite the rules governing the labeling and conditionsfor sale of hearing aids.
State and ProvincialGovernment RelationsAnother important aspect of our advocacy efforts is atthe local level, primarily in providing assistance to affili-ate chapters to supplement their respective efforts.
MODEL LEGISLATION FORHEARING AID SPECIALISTS
One important project undertaken in 2006 was the de-velopment of model legislation for the dispensing ofhearing instruments. This new model legislation moreaccurately reflects current dispensing practice standardsand is designed to be the benchmark in defining theprofession. The draft model legislation is available forchapter leaders to use as a template for the IHS vision ofcomprehensive licensure standards.
PROTECTING CONSUMERSFROM GATEKEEPERS
Select audiology organizations endorsed their ownmodel legislation for the regulation of audiology whichprovides a blueprint for positioning audiologists as thegatekeepers to hearing healthcare. IHS performed an in-depth analysis of the provisions contained in the modellegislation, and distributed this evaluation to affiliatechapter leaders. While IHS does not oppose recognizingaudiologists who attain a doctoral degree and incorpo-rating such into existing state statutes, this model legis-lation contains provisions that are not in the consumer’sbest interest and hinders open access to other hearinghealthcare professionals.
IHS AND AAO-HNS STATE LIAISONEFFORT YIELDS RESULTS
IHS and AAO-HNS maintain a state liaison effort whichaffords the Society’s chapters the opportunity to estab-lish an official liaison relationship with otolaryngologistsin their state. Activities that have resulted from this pro-gram include sharing of information with respect to statelegislative developments, increasing coordination ofgrassroots efforts to promote the importance of hearinghealth, and working to ensure that state legislators un-derstand the hearing healthcare delivery system.
IHS BOARD OF GOVERNORSOUTREACH PROGRAM
The IHS Board of Governors is actively engaged in out-reach efforts to state and provincial chapters. One keyelement of this effort is the Governors Outreach Pro-gram, which is now in its eighth successful year. TheOutreach program represents the Society’s coordinatedeffort to share detailed information about governmentrelations, education, and other activities undertaken bythe Society to protect and advance your profession.
IHS MEMBERS SERVE IN STATE LEGISLATURESThe Society is proud that two of its members serve instate legislatures. Clark Barnes, BC-HIS, serves in theWest Virginia State Senate. He is also the president ofthe West Virginia Hearing Aid Society. Senator Barneshas been an IHS member since 1989.
Tracy King, BC-HIS, ACA, a former president of theTexas Hearing Aid Association, serves in the TexasHouse of Representatives. He was first elected in 1994and is currently serving his sixth term. RepresentativeKing delivered the keynote address at the 2006 IHS con-vention and has been a member since 2004.
LEGISLATIVE MONITORINGAn electronic reporting service allows IHS to daily mon-itor legislative activity throughout the U.S. that couldimpact the hearing healthcare profession and the hear-ing impaired. IHS notifies the appropriate chapter andworks with their leadership to provide strategic develop-ment and implementation, documentation, bill analysis,and coordinate strategic contacts.
IHS Must Maintain Its VigorousGovernment Relations EffortsIHS will continue its vigorous membership advocacy andliaison efforts on behalf of the hearing impaired weserve. The Society urges its members to participate ac-tively in the political process, and develop and sustain re-lationships with their elected representatives at the state,provincial, and federal level. IHS members must also beinvolved in state and provincial licensure boards and reg-ulatory bodies with authority over hearing healthcare.Chapters must work to ensure that scope of practicestatutes encompass the full range of services provided byhearing aid specialists, including hearing assessments.
THE HEARING PROFESSIONAL 7
2006
An
nu
al R
epo
rt

MARCH • APRIL 20078
2006
An
nu
al R
epo
rtPROFESSIONAL EDUCATION AND TRAINING
IHS continues to be a leader in hearing healthcare educa-tion. Managed by IHS’s educational division, the Inter-national Institute for Hearing Instrument Studies (IIHIS),our programs are widely acclaimed for their standardsof excellence.
Sales and distribution of the Society’s distance learningprogram for entry-level training, Distance Learning forProfessionals in Hearing Health Sciences, continues toflourish at an all-time high. Over 700 programs were soldin 2006 and nearly 500 students completed the program.
IIHIS published a supplement to the distance learningprogram entitled Digital Signal Processing for HearingAids, written by Dr. David Preves. Dr. Preves was at the2006 IHS convention to autograph copies of his newbook and was a featured seminar instructor.
IIHIS is the largest provider of accreditation for con-tinuing education programs in hearing instrument sci-ences. With nearly 300 course approvals, 2006 was anexceptional year for provider-sponsored programs. Ap-proximately 15,000 certificates of completion were is-sued to course attendees. IHS developed and adminis-tered 14 seminars at the 2006 IHS convention.
The American Conference of Audioprosthology (ACA)continues to thrive. This advanced educational programis a 13-month course available to interested hearing healthprofessionals in the U.S. Classes started in 2006 were inFlorida, Arizona, and Michigan.
IHS has created a position statement on the Audio-prosthology title.
MEMBERSHIPThe Society is only as strong as its membership and
we are pleased to announce the addition of 430 newmembers in 2006. Further good news is that membersare recognizing the value of their allegiance to the Soci-ety more than ever before, with our retention rate at22% higher than the previous year. In 2006 we createda new staff position to manage our membership recruit-ment, communications, and marketing to ensure that we
provide the best possible service to our members. Oneof the responsibilities of that position is to expand ourrange of member benefits to provide even more valuefor your membership dollar.
We wish to congratulate the following individualswho stepped forward in 2006 to become members ofIHS. We salute your dedication to the profession andthe hearing impaired you serve.
Clarence I. AllenDana D. Alvarez
Richard C. Amon, BC-HISArt A. Anderson, BC-HIS
Charles L. Anderson, BC-HISJanice O. Anderson, BC-HIS
John Charles AndersonJeannette Y. Andrew
Christina ArcidiaconoHelene L. Arrow
James F. Atkins, IIIJ. Kiely Ball, BC-HIS
Kyle E. Bamberg, BC-HISDan J. Barchie
Kevin Wayne BarnesMarjorie Kay Barton, BC-HIS
Bruce A. BelcherRichard M. Bertacini, BC-HIS
Nina Jo Best, BC-HISMartin C. BeylerRodney E. Bill
Charles M. BinnsSteven Biondi, BC-HIS
Janelle BlairDeborah Lynn Bleich, BC-HIS
Brenda Ann Bone, BC-HISJoann A. BorlandSean J. Borland
Richard E. BotelhoVictoria Bottoms, BC-HIS, ACA
Brian R. BoucherJeanine M. Breakstone
Richard T. Brooke, BC-HISRobert D. Brooke, BC-HIS
Jaclyn Elizabeth Brosius, BC-HIS
Mark BrownWalter W. Browning, Jr.
Paul BryantCarmen Buechel-Brown
Lori Kay Bunkholt, BC-HISWalter Swift Burbank
Charles H. BurnsLarry E. Burt
Stephen W. Bush, BC-HISBong-Su Byun
Ralph Rene Canales, Jr., ACALianne R. CarboneSteve J. Carbone
G. Richmond CargillJames R. Carlson, ACA
Teressa Lynn Carpenter, BC-HISSamantha J. Carruth
Neil L. Cassanelli, BC-HISCamille C. Catalano
Lee R. Champ, BC-HISScott C. Chase
Karen E. ChisholmHey-Kyoung ChoiRichard A. Cipolla
Christi ClarkDick A. Clay, BC-HIS
Robin Ann ClayEan E. Clough
Marie Noelle CotePaul Cote
Maxwell T. Cotter, MDThomas Benton CoughlinKimberly A. Coy, BC-HIS
James A. CraigDennis A. Craycraft, BC-HIS
Melinda CrittendenScott Andrew Crohn
Peter Noel CullenAllison Cummins-Caruso
Hyam Peter CurlenderSiobhan Dalton
Fred W. Dando, BC-HISLinda Jimerson Daniel, BC-HIS
Robert D. DavisRuth Ann Davis, BC-HIS
Joy DayDonald R. Deardorff
Boyd Demchyna, BC-HIS, ACALarry Troy DeMorrow
Linda E. DempsterJesus M. Diaz, BC-HIS
M. Sherwood Dixon, BC-HISJacqueline C. Dolan
Shelley L. DorrEsther E. Dow, BC-HIS
Karl DrouinGerald J. DuBrino, BC-HIS
Virginia G. DuclosStephanie J. DunnTimothy A. DunnIrene A. DunneRichard Dunne
Pieter Jeroen DunningRichard Earnest
Perry EbelRonald Arthur Eberhardt
Larry EganPeter Eklof
David M. ElderAnita Brown Elks, BC-HIS
Terri Marie EllertBeth Ergas
Scott E. Erickson, BC-HISJerome C. Eslinger, BC-HIS
Linda FallGerard Feeney
Rafael F. Fernandez, BC-HISJames B. FerrenIlynca FiedlerVicki L. Fisher
Garrett David FlemingJohn Joe Fleming
Jerome L. FlotkoetterPaul Fontaine
Curtis H. FooteJames S. Formoso
Russell M. Foss, BC-HISMichelle Fournier
Nancy C. FoxCindy FrankCarol Fraser
Becky FredetteKenneth A. Freia, BC-HISMarianne Fritz, BC-HIS
Dorothy J. Fry, BC-HIS, ACAJames Fulham
James P. Gagnon, BC-HISJean M. Gallagher, BC-HIS
Lisa Galliher, BC-HISTerrence P. Galvin, BC-HIS
Alan Lee GambillTraci M. Gamble, BC-HIS
Nathan Robert Gammon, BC-HISJoel V. Gann, BC-HIS
Gilbert M. Garcia

Susan E. Garnic-NewhallMichael S. Gatto, BC-HIS, ACA
Patricia J. GeretyScott Jeffrey Giard
Jason W. Gillard, BC-HISMichael A. Glassman, BC-HIS
Todd GodfreyJay W. Goldman, BC-HIS
Sharon D. GoodaleDavid D. Goodyear, BC-HIS
James M. GottJohn T. Gray, BC-HIS, ACA
Bryan L. GreenDouglas Barton Green, BC-HIS
Ray W. GuillotGordon Guinette, BC-HIS
Vladimir A. GutierrezRodney J. Guza, BC-HIS
Deanna M. Hallahan, BC-HISCarol G. Hamilton
Todd J. HandyJames A. Hanerhoff, ACA
Jeffrey D. HanleyWilliam J. Harrington, BC-HIS
Jeffrey A. Hartney, BC-HISMatthew J. Havens
Tamara Rose HaydonRichard G. Hayhurst
Tracey L. HaysElizabeth Heitman
Rachel E. HendricksGladys A. Henning, BC-HIS
Brian J. HerbRobert H. Heygster, BC-HIS
Jesse Hidalgo, Jr.Brian Lee Hillesland, BC-HIS
Bradd E. HilstonCarolyn A. Hocking
Carla Hoffman, BC-HISApril Dawn Hogeland
Gary K. Hollensteiner, BC-HISRobyn S. HopperCraig A. Horgan
Lorance Reed HudsonSandy Hughes
Jonna Hull, ACAArlene L. HulwiHeather L. IrvingJoseph C. JacksonYoung-Sun Jang
Candi JarvisClifford W. Johnson, Jr., BC-HIS
Angela M. JonesRichard C. Jones, BC-HIS
Victor JovanWendy R. Juarez, BC-HIS
Ga-Lam JungDouglas W. KaySandra L. KellyLarry G. Kenny
Robert J. Kille, BC-HISByeoung-Woo Kim
Hyang-Suk KimYong-Kyun KimYoung-In Kim
Mark W. Kind, BC-HISHolly Elizabeth King
Heath KirkpatrickRonald N. Kittner
Debrah A. Klapperich, BC-HISCorey W. Kline, PhD
Clint E. KnoellMarla J. Knutson
Brenda L. KokerSteven J. Kolodin
Rebecca Jane KruerHo-Lim Ku
Tony La FondGreg L. Lamb
Robert James LandryBeth E. Larson
Scott A. Larson, BC-HISPaul Christian Lawrence, BC-HISDeborah J. Leasure, BC-HIS, ACA
Trudy A. LeclercWilliam H. Lenz
Uk-Bin LimErik A. Lindberg
Kim Rice LineweaverScott E. LineweaverJoan Logan, BC-HIS
James David Lucas, BC-HISWilliam J. Lucas
Misti Lutt-Chmiel, BC-HISDolores Madden
Daniel MakkJames P. MalleKaren E. MalleTim L. Martens
Patricia J. MartinJonathan Bryan Matchell, BC-HIS
Marie MathotEdward Anton Maznio
Paula J. McDonaldSamuel P. McFaul, BC-HISBonnie Derringer McGrath
Randy Glyn McKeyReginald McRae
Tammy Lynn MeffordBrad B. Melancon
Maria MeyerRobert M. Michalsen, PhD
David L. MidgleyMichael A. Miller, BC-HIS
Roland Miller, BC-HIS,ACADavid D. Mittag, BC-HIS
Glen A. MohlerMaria Monaghan
Richard Fay MooreRodger Allen MooreFrancine MorrissetteFrancis J. Napoletano
Melody E. NashRick A. NelsonEugene H. New
H. William Noel, III, BC-HISRobert D. Nugen
Larry C. Oberg, BC-HISPaul B. O’Connor
Ronald L. Odum, BC-HISSi-On Oh
Young-Hwan OhGeorgett S. Olbrysh, BC-HIS
Jason OrsikDavid R. Oswalt, BC-HIS
David J. Ott, BC-HISNicole OttPaul Owen
Rocky W. OwenCurtis J. PargeonByung-Ki Park
Richard J. PatushAndrew J. Pavlucik
Daniel Barham PearceRichard Matthew PersianiMerlyn J.W. Peterson, Jr.
Rayana V. PiescoStephanie PinterGeorge Pitalo, Jr.Jonathan Plechaty
William H. Plum, BC-HISBlair Post, BC-HIS
Ronda C. PottsSusan Prather
Lorraine M. ProvostJulie A. Pruitt, BC-HISSteven Michael Purnell
Daryn D. QuickDavid W. RaderJanet K. Raiwet
Mary Anne Rankin, BC-HISMark A. Rau
Laurence G. RedmondJudith A. Remaly, BC-HISDouglas L. Ressler, BC-HIS
William J. RevilleFred R. Reyes
David T. Richard, BC-HISLaura Jayne Richardson
Geraldine RiethmeierRichard L. Rogers, BC-HISCarla Jane Rogstad, BC-HIS
Farrah L. Rose, BC-HISKeith Ross
Alyre Joseph Roy, Jr., BC-HISWilliam M. Ryan, BC-HIS
Joel SableTalley April Saekan, BC-HIS
Darlene Ada Saiz, BC-HIS, ACAIrma Cecilia Salcido
Katherine M. Sample, BC-HISJeanne Marie Sanders, BC-HIS
Bertha L. SaundersScott J. Sayer
Renee SchafferRonald D. Schick, BC-HIS
Anne C. SchnappDiane Ely Schneider
Shaine Schnurman, BC-HISRoslyn R. Seibold, BC-HISMichael A. Sexton, CCCA
Jenelle J. SharpSang-Don Shim
Jay Shin, BC-HISNancy Ann SideriCynthia L. Sims
Hazel Virginia SingletaryCatherine A. Skelly, BC-HIS
James SkogstadBlaine H. Smith, BC-HIS, ACA
Daniel M. Smith, BC-HISSteve D. Smith
Victoria L. Smith, BC-HISGloria L. Snell, ACAThomas G. Snoozy
Brian SnowdenCarly Marie Snyder
Un-Ki SoBill Somers
Carolyn L. SpinaKenneth L. Startz
Mark W. States, BC-HIS, ACAJames D. Steele
Debra Lynn StefaSteven R. Stein
Thomas R. StephensJoseph Yarnell Stock, BC-HIS
Sharon Ann Stoor, BC-HISJulie Lynn Storie
Steven Daniel StoutJulie Anna Stuart
Stephanie Feldman Suissa,BC-HIS
Donald SuttonSunan R. Sutton
James William SwigerOhumaya Takaoki
Thomas J. TamblingKeith D. Taylor
Sheri L. Taylor, BC-HISVoncile Taylor, BC-HIS
Robert B. TerbanAlea Anne Thomas
Margaret G. ThomasAlan R. Thompson
Jenny L.V. ThompsonBetty Lou Tighe
Dennis M. Tobin, BC-HISRobert Thomas Torrie, BC-HIS
Ronald K. TroastMichael A. Trujillo, BC-HIS
Benjamin M. TurpinEleonora S. TysiacCarole Van Straten
Derry Albert VanSicklenDarleen E. Vieira
Rachel VinsonRita M. ViolaTim V. Votava
Joseph Leo Wadden, BC-HISKerri A. Walchli
Darryl W. WalkerGregory S. Waller
Mary E. WaltzPatricia A. Wasson
Gary K. WeaverBlake James Webb, BC-HIS
Kamalini Chandrika WeeratnaCarol Ann Weidman, BC-HIS
Laurie WeissStephen P. Welch
Raymond F. Wenck, BC-HISSharon J. Wendling
Sandra K. WestmorelandOtis A. Whitcomb
Janice S. WhiteKeith Weldon Wiggins
Katharine O. Wiley, BC-HISPaul C. Wilke, ACA, BC-HIS
David WillhiteJeffrey Burt Williams, BC-HISKatherine Williams, BC-HIS
Mary Beth WilliamsJohn K. Winkler, Jr.
Theda M. Witt, BC-HISRobert C. WittkoBernard Witunski
Amanda B. Woika-LillbackJacquelyn H. Wolf, BC-HIS
Jon S. WoodPaul R. Yaun, BC-HISJeanette Ann Young
Maxine L. Young, CCCAHyung-Min YuAlan Zamansky
John L. Zara, BC-HISJohn Zchau
James T. Zemba, BC-HISJun Zhao
Thomas D. Ziliak, BC-HIS
THE HEARING PROFESSIONAL 9
2006
An
nu
al R
epo
rt

First Class Accommodations
You’ll experience the best atthis year’s host conventionhotel.
John Ascuaga’s Nugget is oneof the world’s greatest resortcasinos. It features a luxuri-ous indoor/outdoor pool area,eight award-winning restau-rants, top-name entertain-ment and a breathtaking viewof the beautiful Sierra NevadaMountains.
Seeing is believing!
EVERYONE’SA WINNER AT THEIHS CONVENTION
AND EXPO!
Register online at www.ihsinfo.org or call IHS at 734.522.7200.
See you in Reno!
For a one-of-a-kind
convention jam-packed with
rich education experiences
and professional networking the
International Hearing Society’s
56th Annual Convention and
Exposition HAS IT ALL!
Unite with colleagues
from around the world,
September 26-30, 2007
in Reno, Nevada for this
premier event which celebrates
individual success and
industry-wide achievement.
Never before has there
been such an explosion of
opportunites awaiting you!
For more information call IHS at 734.522.7200 or visit our website at www.ihsinfo.org.
September 26-30, 2007

CONTINUING EDUCATION
It is estimated that there are 28 million Americans with ahearing loss. More than 22 million have never triedhearing aids as a solution to their hearing loss.1 Issues
such as cost, fear that hearing aids will make the user feelold, and the perception that they don’t work effectivelyhave been cited as reasons why people do not get them.However, there is an emotional component about the deci-sion to accept amplification that may not apply to othertypes of disabilities. Psychologist Michael Harvey’s column,“What’s on Your Mind?” (Hearing Loss, January–February2004) discusses the stages a person may go though beforemaking the decision to get help. Precontemplation, a lack ofawareness of the problem, and contemplation, the ambiva-lence experienced when one weighs the pros and cons ofgetting hearing aids, are the first cognitive steps many peo-ple take. This is followed by the determination to accept achange and get hearing help.
The emotional components of the process leading up tohearing aid selection may take years to resolve before aperson with a hearing loss seeks amplification. The finalstage, determination to seek help, may never occur asmany people with a treatable hearing loss go to their gravewithout getting help. How many times has a survivingspouse lamented, “I kept after Bob to get hearing aids buthe was too vain to accept help?” This is a shame because itis avoidable. To believe that this behavior is tolerable is likeaccepting that a treatable disability should be ignored sim-ply because the person with the disability is not aware thatit exists. While the concept of denial may be one explana-tion for not seeking help, the reason for a lack of aware-ness of a hearing loss might have more to do with the per-ception of normal than anything else.
Humans are generally not aware of subtle changes inbody function. For example, a sudden hearing loss is usu-ally detected and acted upon immediately, whereas a grad-ual sensorineural hearing loss is insidious. Humans cannotobjectively measure their level of hearing. The slow natureof hearing deterioration gives the person little feedbackthat the loss is getting worse. Because we are social crea-tures, we depend upon others to tell us when our hearingstarts to fail. The problem is what our brain tells us oftenconflicts with reality. “If the rest of the world would justspeak up” is a phrase often heard by hearing specialists. Ifour brain tells us we are normal, it is very difficult for anoutsider to overcome this perception.
The result is that most people with significant hearingloss wait until the problem becomes so noticeable that theirbrain can no longer be fooled into believing everything isstill normal. Family and friends who attempt to compen-sate for a hearing loss by repeating questions, increasingthe volume of the voice, or tolerating a very loud televisionreinforce the sense of normalcy. As the problem gets worsethe person is nagged, coerced, and badgered into “gettinga hearing aid.” It is understandable why the messenger, thehearing healthcare provider, is blamed for pushing a per-son into getting hearing aids. In fact, the person has likelybeen pushed for years and still may believe he or she hasnormal hearing because the brain has relatively little per-ception that the distortion of auditory stimuli is internalrather than external.
THE HEARING PROFESSIONAL 11
Mr. Brady owns a private audiology–hearing aid dispensing prac-tice in New Jersey. Correspondence: [email protected]
IHS offers a diversity of options for obtaining continuing education credit: seminars and classroom training,institutional courses, online studies and distance learning programs. This article represents yet another opportunity.
Upon successful completion of the accompanying test on page 27, you will earn one CEU.(Please check with your licensing board to verify acceptance of continuing education credit for this activity.)
This article and test are also available on the IHS website at www. ihsinfo.org.
Counseling Theories Appliedto Fitting Hearing Losses
By Granville Y. Brady, Jr., AuD

CONTINUING EDUCATION
What, if anything, can be done to inform and motivate aperson with a loss to accept help? The first consideration isthe level of loss, both for intensity and for word recogni-tion. As the overall pure tone thresholds approach 50–60dB, the point at which conversational speech is presented,the more likely the person with a loss will become aware ofit. It is not uncommon to hear a patient complain that theirhearing was not too bad until recently when it becamemuch more difficult to hear conversation. The other issueis how good word recognition is, not only in noise, butalso for quiet speech. As speech becomes more difficult todiscriminate a person may be more likely to seek help. Ofcourse, the person’s age, level of socialization, and physicalcondition are important variables.
Once a patient seeks help the need for a counseling proc-ess to take them from disability to ability is imperative.Counseling may take one or more of the following ap-proaches: changing behavior, dealing with the emotional as-pects of hearing loss, and coping with the changes in cogni-tion that occur when hearing is deprived. Two counselingtechniques used are behaviorism2 and phenomenology.3 Athird approach, developed by Albert Ellis, seeks to combinebehaviorism and phenomenology with known physiologicalprinciples.4 This is often referred to as cognitive counseling.Although it is beyond the scope of this article to analyzeeach counseling theory as a psychotherapeutic tool, theseapproaches have a practical application for evaluating andfitting patients with amplification.
One widely accepted learning technique has been operantconditioning. Good behavior is reinforced and the morepositive the behavior the more reinforcement is used untilthe behavior becomes habituated.5 An example of operantconditioning applied to fitting a hearing aid occurs when anolder patient can be motivated to use hearing aids if she re-ceives a phone call each day from her daughter. The rein-forcement is the positive attention from the daughter. Thehearing aid, with an automatic telephone coil, enables theperson to hear her daughter. Since the daughter does not al-ways call at the same time the patient must use the hearingaids all day. After a few weeks, hearing aid use becomes ha-bituated and the daughter may not need to call every day. Insituations where the relatives live with the hearing aid user,positive reinforcement from being included in family activi-ties is a strong motivator to use the instruments regularly.
Counseling based upon a theory developed by psycholo-gist Carl Rogers (phenomenology) takes into account theemotional nature of language. A patient with a hearingloss becomes socially isolated. Use of amplification willallow for better social interaction. The patient is encour-aged to use hearing aids because he or she feels more ac-cepted by family and friends. Awareness of the hearing lossin this case is not a focus of counseling. The goal is to re-duce the feelings of isolation and detachment from familyand friends. The objective is to improve communicationand encourage the patient to develop positive feelings. Am-plification is simply a means to a positive end. The hearingprofessional counsels the patient to increase his or her in-volvement socially and emotionally and to keep a diary ofexperiences in various listening situations. The emphasis is
on developing improved self-worth and feelings of accep-tance. Levine and others describe poor self-image and feel-ings of isolation characteristic of patients with hearingloss.6 By improving self-image, the patient learns to dependupon hearing aids as a means to fulfill life’s expectations.The goal is to counsel the person—not the disability.
Cognitive counseling attempts to modify the person’svalue systems, in this case related to hearing loss. By en-hancing what could be achieved with better hearing as op-posed to the negative thoughts about how the hearing lossimpairs the ability to communicate, the patient is able to re-focus his thinking to accept amplification. In essence thecognitive processes of the hearing impaired person are mod-ified from a negative-disability model to a positive-normalmodel. Once the hearing aid wearer begins to modify hisoutlook on life, the social structures (family and friends) ofsociety reinforce the person’s cognition that he has im-proved. This might be the reason why many patients whouse hearing aids become so happily dependent on them.
Combining emotional and cognitive approaches is an-other method to counsel patients. Hearing loss leads to dis-tortion of the signal, which impairs cognitive function.Neural plasticity of the auditory nervous system is facili-tated when the patient is introduced to amplification. Byincreasing the stimulus in several steps, often referred to asacclimatization, the patient is able to adapt to hearing aids.Cognitive improvement, coupled with a better self-imageand more confidence in a listening situation, allows the pa-tient to habituate hearing aid use with a minimum of diffi-culty. In this case, the hearing healthcare professional sup-plements counseling with a shaping strategy. The hearinginstruments are programmed in such a way as to give mini-mal change initially. The patient can detect the changes inhearing but is not overloaded to the point where thechange is uncomfortable. This is not to be confused withuncomfortable loudness levels, which are unacceptable.The changes that occur when the hearing aids are activatedallow the patient to hear better without violating thebrain’s perception that the sounds are unacceptably differ-ent. Programming hearing aids to approximate the pa-tient’s just noticeable difference (JND) takes into accountthe human’s ability to detect the smallest changes in fre-quency or intensity that can be recognized. This is not tobe confused with recruitment, which sometimes is found insensorineural hearing loss and results in a disproportionateincrease in the sensation of loudness.7 Most high-end digi-tal hearing aid programs have the capability to makeminute changes that assist in the patient’s ability to im-prove hearing without causing any discomfort.
By working with and not against the JND, the patient’sperceptions of improvement are shaped slowly enough forthe auditory nervous system to change without becomingconsciously annoying to the hearing aid user. Since theplasticity of the auditory nervous system is variable andnot static, changes in amplitude and signal frequency fromone time to the other are barely noticed by the patient.
Evidence of the human’s poor visual and auditory mem-ory is evident when witnesses to a crime or accident are
MARCH • APRIL 200712
continued on page 17


GLOBAL SPOTLIGHT
MARCH • APRIL 200714
Global Spotlight is a special feature of The Hearing Professional that shines a greater focuson hearing healthcare throughout the world.
For more information please contact CHIPS, 185-9040 BlundellRd., Ste. 259, Richmond, BC, Canada V6Y 1K3.
A Report from theCanadian Hearing InstrumentPractitioners Society (CHIPS)
It’s the time of year when we all tend to reflect on the pastand look toward a brighter tomorrow. The hearing health-care profession should be thankful because the exposure onthe national and provincial levels is at an all-time high! Icontinue to be thoroughly impressed with the accomplish-ments from our provincial representatives. It takes a spe-cial group of people to dedicate time away from their busi-nesses and families to volunteer their expertise and committo moving our profession forward. I am thankful that themanufacturers continue to support our association in allour endeavors, but mostly I am thankful for having theopportunity to serve you, the hearing instrument practi-tioner, for I believe as I know you all do that we are an in-tricate part of the hearing healthcare chain. I am thankfulfor the friendships and look forward to even more.
I’d like to take this opportunity to welcome Susan Arnoldas the new administrative assistant for CHIPS. For over 20years, Susan has been part owner, office manager, andbookkeeper for Arnold Hearing Centres. Over the last 34years, she and her husband have attended most of the On-tario symposiums and numerous IHS conventions. As a re-sult, she’s met many hearing instrument specialists, audiol-ogists, and manufacturers’ representatives and has come tovalue their friendship. As administrative assistant Susan islooking forward to seeing more friendships evolve and de-velop. No doubt having an administrative assistant with somuch industry experience will dramatically assist CHIPSin progressing with its initiatives.
I would also like to mention that CHIPS is indebted toStarkey Canada for their generous donation of our brandnew booth. Annette Cross, BC-HIS, from Nova Scotia haskindly offered to give the CHIPS booth a long overduemakeover—be sure to check it out at upcoming meetings.
CHIPS wishes to congratulate John Roberts, who re-cently was awarded with the honor of having a local hear-ing business named after him. John has been instrumentalin the advancement of the hearing healthcare professionand is a true inspiration.
Please take a few minutes to read through the provincialhighlights and check out our website at www.hearcanada.com for upcoming events and the most current up-to-dateinformation.
John Letts, BC-HISPast CHIPS ChairIHS Governor—Canada
P R OV I N C I A L H I G H L I G H T S
College of Hearing AidPractitioners of AlbertaThe continuing competency program is complete. The pro-gram was designed to help hearing aid practitioners testtheir knowledge in seven different areas with subsectionsin each area. The program will be available on the Internetas well as hard copy.
The government of Alberta and British Columbia signed theTrade, Investment, and Labor Mobility Agreement (TIMLA)to coincide with the Labor Mobility Agreement signed byall the provinces last August. The mandate of TIMLA is tostandardize the requirements to practice between Albertaand British Columbia for hearing aid practitioners.
Hearing Instrument SpecialistsSociety of British Columbia(HISS-BC)Participation on the provincial licensing board continues tobe active. In 2006 there were approximately 30 new licensesissued to hearing instrument practitioners and audiologists.

GLOBAL SPOTLIGHT
The Mutual Recognition Agreement was signed by repre-sentatives from each provincial regulatory authority, andprovincially (labor mobility agreements between BritishColumbia and Alberta government). HISS-BC is workingwith the speech language pathology and audiology com-munity by making the transition from regulation under alicensing board to self-regulation under a joint College.
New Brunswick Hearing Aid SocietyNew Brunswick is in the process of changing its continuingeducation requirements. All members will be required tobe certified by the National Board for Certification inHearing Instrument Sciences (NBC-HIS) within one year ofbeing a member. All existing members must provide cur-rent certification through NBC-HIS or must provide eighthours of continuing education.
Newfoundland Associationof Hearing Instrument SpecialistsThere is still not a signed contract with the Workplace Health,Safety, and Compensation Commission (WHSCC).
The reasons for this include:• one dispensing audiologist refused to be a provider for
WHSCC;• one clinic initially refused to be a part of the program
but has since changed its position.
Hearing Aid Societyof Nova ScotiaThere is a review over the present potentially biased protocolfor licensing. In order to be licensed an individual needs towork six months and then take a written and practical exam.
Association of Hearing InstrumentPractitioners of Ontario (AHIP)Despite having the largest number of hearing instrumentpractitioners in Canada (over 400), Ontario still struggles inobtaining formal regulation through the Ministry of Health.
Shelley Randall has proved her dedication to the hearinghealthcare profession and was appointed by the Board ofDirectors to serve as the AHIP president until the next an-nual meeting.
Saskatchewan Hearing InstrumentPractitioners SocietyA policy manual is in place; however, it does not appear tohave complete compliance. There are problems with com-plaints (they must come directly from the consumer). Prac-tices have been inspected to meet government standards.Audiologists and practitioners must take the NBC-HISexam for government certification.
THE HEARING PROFESSIONAL 15
We’d like to know. Wewelcome your submissionof articles for publication inThe Hearing Professional.If you have something to say,this is the place to say it—your opportunity toshare with practitionersthroughout the hearinghealthcare field.
As long as the topic isrelevant to the hearing health industryor general business management, the specific natureof the subject matter is entirely up to you.Feel free to write from a very personal perspectiveor from a broad industry overview.
So get creative. And don’t worry about yourwriting skills or the “roughness” of the draft.The job of our editors is to make you and yourarticle look good.
Email a Word document to Autumn Kovachat [email protected]. Length should beapproximately 500–1,000 words. Graphics, includingphotos, charts, diagrams, etc. that are notincorporated into the Word document should alsobe sent electronically, if possible.
All submissions will be considered for publication,but not all are guaranteed for acceptance. All copy issubject to editing at our discretion. We will make everyeffort to allow your review of edited copy prior topublication, but cannot guarantee it. Photos arewelcome and will be returned. Hard copy documentsand CDs will not be returned.
SPECIAL FEATURE—IHS Annual Reportto Members
PROFESSIONALPROFESSIONAL
HEARINGHEARING
Official Journal of the International Hearing SocietyTHETHE
MARCH–APRIL 2007
What’s OnYour Mind?What’s OnYour Mind?
Order of Hearing Aid Acousticiansof QuébecThe Ministry of Health and Social Security adopted thenew regulation agreement for the hearing aid program.The program has been adopted exactly as published in itsfirst version despite the Association’s effort to evoke changes.A press conference was held, together with the ENTs andassociations representing seniors, in order to expose somepoints of this regulation (specifics can be accessed byCHIPS members on the CHIPS website).
The Association signed a historic agreement with theWorkers’ Compensation Board. The negotiations have lastedfor more than seven years. This agreement is much better,for the workers and for the hearing aid practitioners. THP

RESEARCH REVIEW
MARCH • APRIL 200716
The QuestionPatients with Ménière’s disease (MD) can present at youroffice with reports of hearing loss, tinnitus, aural fullness,and/or dizziness. They report that their symptoms can fluc-tuate over time and vary widely in intensity and duration.As if all that weren’t bad enough, they often have emo-tional issues related to feeling terrible from the vertigo andmay be constantly concerned about having a sudden, un-predicted attack. Given these challenges, what is the hear-ing instrument professional’s best practice model for ampli-fication management of patients with MD?
The StudyThis paper by Valente, et al. is not a report of a researchstudy. Rather, it is a compilation of both anecdotal evidenceand evidence-based practice that recommends technologiesand approaches for handling the challenges encounteredwhen addressing the unique hearing needs of patients withMD. It is a well organized paper and very readable. Thesuggestions provided can be applied immediately, not onlyto patients with MD, but also to those not suffering fromMénière’s who have similar complaints or hearing issues.
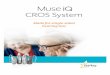
RecommendationsThe best practice recommendations made by Valente, et al.can be categorized as those that are technology based andthose that address the MD patients’ audiometric or symp-tomatic presentations. They applied the various features af-
forded by DSP and wireless technology to address specifichearing and listening issues as indicated in Table 1.
Dr. Connelly is an assistant professor of surgery at the New Jer-sey Medical School and director of audiology service at theUMDNJ–University Hospital in Newark, New Jersey.
Research ReviewBy Patricia E. Connelly, PhD, CCCA, ABA
Unilateral/Asymmetric CROS or BiCROS (wirelessHearing Loss available); BAHA
Fluctuating Hearing Loss Hearing Aid with > 1User Program
Poor Word Recognition Scores Directional Microphones;Counseling for RealisticExpectations, ALDs
Rising Audiometric Frequency Shaping toConfiguration Audiogram Not Best Method
Reduced Dynamic Range/ Measure Individual LoudnessRecruitment Discomfort Levels
Table 2: Fitting Approaches to Various Audiometric/Listening Issues
Audiometric/Listening Issue Fitting Approach
Flexible Frequency Shaping 2 to 20 Bands/Channels of and Reduced Dynamic Range Signal Processing and Low
Compression Kneepoints
Feedback Control Most Effective with GreaterNumber of Bands/Channels
Occlusion Use of More Open Fittingsas a Result of FeedbackManagement Algorithms
Listening Comfort in Noise Noise Reduction Algorithms
Speech Recognition in Noise Directional Microphones
CROS/BiCROS Fittings Wireless Technology
Better Listening with ALDs DSP and Wireless Combination
Table 1: DSP Solutions to Fitting Issues
Fitting Issue DSP Solution
Valente M, Mispagel K, Valente LM, Hullar T. Problemsand solutions for fitting amplification to patients withMénière’s disease. Journal of the American Academy ofAudiology 2006;17:6–15.
LEARNING OUTCOMESAs a result of reading this article you are expected to:1. discuss the unique issues related to amplification man-
agement for patients with Ménière’s disease;2. apply the various features of digital signal processing
(DSP) for improved listening outcomes.
Valente, et al. then went on to incorporate the abovetechnologies into suggestions for managing hearing and lis-tening problems, as outlined in Table 2.
In this section of the paper, the authors used more evi-dence-based recommendations than anecdotal suggestionsthat were seen in the technology-based approaches to am-plification management. The authors mentioned that therewas “limited evidence published” (page 7) on which tobase their recommendations. However regrettable this may

RESEARCH REVIEW
be, it’s nonetheless the state of affairs in trying to developbest practice guidelines for hearing aid fittings—there’s justnot a lot of evidence out there.
Who May be Affectedby These Findings?Clearly, this paper focuses on MD. However, the audiomet-ric and listening issues presented are typical of many pa-tients that come to us for hearing help. The symptomsmight not be as variable as they are with MD, but we needto develop management plans that address the complaintswhether they appear in isolation or in combination, as inpatients with MD. The recommendations proposed in theValente, et al. article certainly apply.
Learn more about facing the challenges of managing theamplification and listening needs of patients with Ménière’sdisease by reading the entire article. For a pdf copy of theValente, et al. article, contact Pat Connelly, PhD, CCCA,ABA, at [email protected]. THP
THE HEARING PROFESSIONAL 17
800.525.7936www.discovear.com
4318 Downtowner Loop N.Suite K • Mobile, AL 36609
from Loss,
Damageor
Failure
Protectyourclients’
HearingAids
Best CoverageBest ServiceBest Price
CONTINUING EDUCATION
questioned. Police will confirm that the accuracy of the wit-ness’s description of what was seen or heard deteriorates sig-nificantly when the amount of time from the event to the in-terrogation is longer than a few minutes. Humans have a wayof selectively remembering what they see and hear. Therefore,a patient who has worn a hearing aid for a few weeks soonforgets how difficult it was to adjust initially to amplification.If the patient can just get through the first few days or weeks,hearing aid use will become much more successful.
Hearing instrument specialists who use these psychologi-cal and physiological principles in their practice will findthat patients are more responsive to amplification. They willenhance the objective tools such as real-ear measurementsthat have been developed to improve fitting strategies. THP
References1. Kochkin, Sergei. “Hearing Solutions—Why People Delay a Solution,”
Better Hearing Institute website www.betterhearing.org.
2. Bandura, A. Principles of Behavior Modification, New York, Holt,Rinehart & Winston, 1969.
3. Rogers, Carl. Client-Centered Therapy: Its Current Practice, Implica-tions and Theory, Boston: Houghton Mifflin, 1951.
4. Ellis, A. and Greiger, R. Handbook of Rational Emotive Therapy,New York: Springer-Verlag, 1977.
5. Brady, Granville. Speech Sound Acquisition and Resultant carryoverto Conversation Using Behavior Analysis Techniques, Seattle: WesternPsychological Association conference, 1969.
6. Levine, Edna Simon. The Psychology of Deafness, New York: Colum-bia University Press, 1960. P. 273–277.
7. Delk, James. Comprehensive Dictionary of Audiology, Sioux City: TheHearing Aid Journal, 1973.
Counseling Theories Appliedto Fitting Hearing Lossescontinued from page 12

MEMBERSHIP MATTERS
Many of you may be familiar with George Harri-son’s saying, “If you don’t know where you’regoing, any road will take you there.” In looking
back over the last 15 years of my career, I realize that whileI didn’t know exactly where I was going I did know Iwanted to experience as many different facets of our indus-try as I could. I believed that in doing so I would find myright place within it.
When I look ahead, I believe there has never been a bet-ter time to be a hearing healthcare professional. More im-portantly, the future belongs, as it always has, to thosewho see learning as a lifelong opportunity; a journey thatoccurs both inside and outside the classroom.
I’ve been asked to share my story with you as an exam-ple of how a little education and a lot of hard work and ex-perience gained over time have resulted in the realization ofa dream.
My journey began shortly after I received my bachelor ofscience in communication disorders from the University ofWashington in 1992. I was struggling with the idea ofgoing to graduate school so I began exploring other op-tions. Little did I know that my first inquiry for employ-ment would be my last; and every future opportunity wouldbe presented to me through my ever-growing network ofcontacts within the industry.
On a cold, rainy day in January 1993, I made whatproved to be a great decision when I walked into the localBeltone Hearing Aid Center in Renton, Washington. Mygoal was to obtain a volunteer position in order to see whatthe business was all about and if it might be the right thingfor me. An hour later, I left with a full-time job and an op-portunity to train as a hearing instrument specialist, andlearn the business from the ground up. More importantly,what I found at that first visit were two mentors and lifelongfriends, Tom and Shari Utigard, owners of the business.
Despite having a college degree, I was told that my train-ing would begin as an office assistant so I would learn thetrue value of the front office position. Over the next ninemonths I learned how to convert phone calls to appoint-ments, how to schedule appointments, the importance ofroutine check-up programs, how to ask for referrals, and
most importantly, that I was an integral part of the successof the company. My position was a sales position and Iwas responsible, along with the dispenser, for growing thebusiness! We were a team and we would be held account-able for achieving sales goals.
In the fall of 1993, I passed the Washington State Licens-ing Exam and began learning the art of dispensing hearingaids. Tom and Shari made a commitment to regular, hands-on training of the entire sale, delivery, service and follow-up process. Tom and I had regular meetings to discussmonthly sales, expenses, marketing plans, profitability, andgrowth opportunities for the business. I was taught the valueof outside service centers and community networking. I at-tended every Tri-State Hearing convention, completed oneof the first American Conference of Audioprosthologycourses offered in the country, joined the InternationalHearing Society and my state chapter, and met with everyindustry representative that called on me. I joined the Ki-wanis Club in my local area and made weekly visits to thephysicians in my community.
After eight years with Beltone, and over the naturalcourse of time, I got an “itch” to see what else the industrycould offer. I had an interest in owning my own business,but also felt I had more to learn before making such an im-portant decision.
Out of the blue, I received a call from Miracle-Ear andaccepted a position managing eight corporate retail hear-ing centers. I immediately found another mentor by thename of Rick Frasier. At Miracle-Ear I was introduced tothe industry’s most comprehensive programs for customercare and service delivery. Over the next three years, withRick’s coaching and guidance, I was asked to manage over40 locations throughout the western United States. Thisposition afforded me the opportunity to see the corporateside of the industry. I learned that in order to properlymanage a business you must be present with your staff ona regular basis. Managing from cell phones, computers,and airport terminals from eight different states proved anineffective business formula both for the company and forme personally. In a larger corporate realignment, Miracle-Ear began franchising their corporate-owned locations.
MARCH • APRIL 200718
Membership Matters is an open forum for IHS members to shareindustry-related news and experiences. IHS does not necessarily endorse,approve, concur with or otherwise advocate material that appears here.
The opinions expressed are solely those of the author.
One Professional’s JourneyBy Sandra Hubbard, BC-HIS, ACA

MEMBERSHIP MATTERS
This decision gave many existing dispensers the opportu-nity to become business owners and has resulted in im-proved service delivery to the hearing impaired and in-creased sales and profitability for the company.
During this transition from corporate to franchise loca-tions, I received a call from the American Hearing Aid As-sociates (AHAA) and was offered a position as western di-visional manager. For the first time, I had the opportunityto interact with over 30 different manufacturers and sev-eral hundred independent providers in my territory. I sawhow services were delivered in a wide variety of settings;from hospitals and university clinics, to nonprofit organi-zations, and private practice dispensing clinics. I met thevery best of our industry. I must admit, there were thosewho balked at the idea of having a hearing instrument spe-cialist from Miracle-Ear advise them on ways to improvetheir practices. I’ve always had the belief that when all issaid and done, whether hearing instrument specialist or au-diologist, we are more alike than we are different so I ap-proached every phone call and office visit as an opportu-nity to offer AHAA’s proven programs for running aprofitable retail dispensing practice. In return I learnedmore about diagnostics, research, nonprofit organizations,and pediatrics. I met dedicated providers of all educationand experience levels, manufacturer representatives, andindustry leaders and found we all have something to learnfrom each other.
Shortly over a year ago, while on my way to another air-port, I received a phone call with yet another opportunity.The call was from my “old” friend and mentor, RickFrasier. Yes, the same mentor who originally hired me atMiracle-Ear. After 15 years in the industry, Rick offeredme an opportunity to become a partner with him in 18
Miracle-Ear hearing centers in Washington and California.Once again, the timing was perfect. This time I was readyto accept the challenge of ownership! Having seen much ofwhat the industry has to offer, I know my “right” place isin the dispensing of hearing instruments. In many ways,my journey has come full circle. My daily routine oftentakes me back to the place I started. Tomorrow I willspend my day training a new member of our team—an of-fice assistant. Who knows, maybe one day she will want toown her own business!
So, as we go forward together, my recommendation tothose of all experience levels is to find a mentor, or two, orthree; they are all around you. Develop a plan for your fu-ture and begin implementing your plan. Make adjustmentsas you go and be willing to take a risk. Keep your eyesopen to the opportunities available to you. And, in the end,you will also find your right place.
Remember, while our credentials signify a level of aca-demic achievement, they do not define who we are. To ourpatients, it’s not about our titles or the letters we placeafter our names. It’s about what’s in our hearts. I learnedthis from a patient who told me that I should not identifymyself as BC-HIS but rather as GFS. When I asked himwhat he meant by GFS he looked me right in the eyes andsaid, “Good and Faithful Servant—those are the only cre-dentials you’ll ever need!”
So, here’s to all the “Good and Faithful Servants” I’vemet over the years who have given of their time and theirtalents to help me grow in this wonderful industry. Thebest way I know to thank you for all you’ve added to myjourney is to embrace the opportunity I now have to men-tor the next generation of hearing healthcare providers.Heck, what more could I ask for? THP
THE HEARING PROFESSIONAL 19
IHS wishes to recognize Beltone and Miracle-Ear for being the firstto answer our kick-off call to manufacturers for corporate support of
important new initiatives for the hearing healthcare industry!
We extend a special thanks for their generous contribution to theIHS Advocacy Alliance and truly appreciate their commitment to achieving ever higher levels of success for the benefit of all.
For more information about this program please contact IHS headquarters at 734.522.7200.

CHAPTER TRACK
MARCH • APRIL 200720
2007 Chapter Meetings
MEETING DATE LOCATION CONTACT
Hearing Healthcare Providers July 13–14 Glendale, AZ Robert Baber, BC-HISof Arizona 623.582.6699
Arkansas Hearing Society August 2–4 Little Rock, AR LeAnn Jackson, [email protected]
Hearing Healthcare Providers May 17–19 Monterey, CA Tricia Rae Hunterof California 916.447.1975
Colorado Hearing Society June 21–23 Winter Park, CO Nonean Price, [email protected]
Florida Society of Hearing July 13–15 Clearwater Beach, FL Neil Waingrow, BC-HISHealthcare Professionals 954.553.4045
Georgia/Alabama Society August 2–5 Lake Lanier, GA Ralph Jackson, Jr.of Hearing Professionals 229.432.0053
Illinois Hearing Society May 11–12 Springfield, IL Michael [email protected]
Massachusetts Hearing Aid Society May 4–5 Foxwoods, CT Gary Rachins, [email protected]
Mid-America Conference June 7–9 Lexington, KY Debra Drewryon Hearing 859.283.5404
midamericaconferenceonhearing.com
Minnesota Hearing Healthcare September 14–15 Bloomington, MN Gregory Wales, BC-HISProviders 320.266.2379
Montana Hearing Society May 26–27 Helena, MT Bill Harrington, BC-HIS406.628.4498
New Jersey Association May 4–6 Mt. Laurel, NJ David Weesner, AuDof Hearing Health Professionals 609.926.0700
Hearing Healthcare Alliance June 7–10 Saratoga Springs, NY Fred Goossen, BC-HISof New York 585.419.9702
North Dakota Hearing Aid April 13–14 Grand Forks, ND Brenda Haugen, BC-HISSociety 701.746.8421

2007 Chapter Meetings (continued)
CHAPTER TRACK
THE HEARING PROFESSIONAL 21
MEETING DATE LOCATION CONTACT
Association of Hearing Instrument April 25–28 Richmond Hill, ON Joanne SproulePractitioners of Ontario 705.328.0907
Oregon Hearing Society June 8–10 Lincoln City, OR Rosalind Sinclair-Sjue, [email protected]
South Dakota Hearing Aid April 13–14 Sioux Falls, SD Vicki CarlsonDispensers Association 605.229.3688
Texas Hearing Aid Association May 31–June 2 Dallas, TX Scott [email protected]
Hearing Health Providers of Utah September 14–15 Salt Lake City, UT Darlene Saiz, BC-HIS, [email protected]
PLEASE PHOTOCOPY THIS FORM ANDRETURN WITH YOUR CONTRIBUTION TO:
International Hearing Society Advocacy Alliance16880 Middlebelt Rd., Ste. 4 • Livonia, MI 48154
Name
� My check for $ is enclosed(make payable to IHS Advocacy Alliance)
� Charge my credit card in the amount of $
� VISA � MasterCard
Name on Card
Signature
Account #
Expiration Date
Help fund the ongoing fight for your rightsbefore governmental bodies.
Contribute to the IHS Advocacy Allianceand do your part to protect
the profession and the hearing impairedyou serve.
It’s your future and theirs…
THANK YOUFOR YOUR SUPPORT!
Make Your Voice Heard!


THE HEARING PROFESSIONAL 23
NAME: Last, First, Middle: SS/SI Number:
Company Name: Date of Birth:
Street Address: Business Phone:
Business Fax:
City: State/Province: Country: Zip/Postal Code:
Home Address: Home Phone:
City: State/Province: Country: Zip/Postal Code:
Email: � Male � Female
Spread the Word About IHS MembershipHelp strengthen the Society by encouraging membership growth.
This application form can be submitted to IHS headquarters or individuals can join onlineat the IHS website where they’ll find detailed information on the benefits of membership.
� $275—Board Certified in Hearing Instrument Sciences � $125—International� $275—Audiologist � $50—Associate� $275—Audioprosthologist � $50—Affiliate� $275—Physician � $35—Student� $275—Provisional
GENERAL INFORMATION
PROFESSIONAL/EDUCATION INFORMATION
PAYMENT METHOD
What year did you begin dispensing hearing instruments?
Credentials: � BC-HIS (Certificate No.) � ACA (Date) � CCCA (Certificate No.)
Completed IIHIS Training Manual for Professionals in the Field of Hearing Instrument Sciences
Course #: Date Completed:
Education Level: � High School � College/Trade (Degree) � Post-Graduate (Degree)
Visa or MasterCard #: Exp. Date:
Check #: Amount: Signature:
I agree to abide by the bylaws and code of ethical practices as established by the International Hearing Society.
Signature/Title: Date:
International Hearing Society16880 Middlebelt Rd., Ste. 4 • Livonia, MI 48154 • phone 734.522.7200 • fax 734.522.0200
www.ihsinfo.org
/ /

The National Board for Certification in Hearing Instrument Sciences has implemented a computer-based National Competency examination (CBT). The advantages of the CBT are tremendous. Exam sites are available throughout the US and Canada. The initial or BETA exam is only available in the US and Canada. International sites will be available soon.
The logistics required to set up an exam are less complicated and scheduling is more flexible. NBC-HIS is currently accepting applications for the BETA exam scheduled from April 16, 2007 through May 18, 2007. Get your applications in now to register.
The initial exam is offered at a substantially reduced cost to encourage a large number of applicants. Fees will increase after the initial exam period. After the BETA exam is completed it will be about six weeks before the online exam will be available on a permanent basis. Contact the NBC-HIS office for information about exam dates and locations.
BETA EXAM FEES
Non-IHS Member IHS Member
Application Fee: $60.00 Application Fee: $30.00 Exam Fee: $65.00 Exam Fee: $40.00
Retakes
IHS Member: $40.00
Non- IHS Member: $65.00
National Board for Certification in Hearing Instrument Sciences, 16880 Middlebelt Road, Ste. 3, Livonia, MI 48154
Phone: 734.522.2900, Fax: 734.522.0900 Visit our NEW website: www.nbc-his.com

SOUNDBYTES
Hearing Health Legend RememberedIHS Life Member Ernest Zelnick recently passed away atthe age of 85. He joined IHS in 1962 and last October wasawarded with the IHS Empowerment Award, which recog-nizes extraordinary achievement in advancing the hearinghealthcare profession.
Zelnick was very active on the local level and in the pastserved as president of the New York Hearing Aid Society.
Zelnick received his bachelor’s degree from BrooklynCollege. After military service, he received a law degree atSt. John University, Jamaica, New York, and practiced lawfor some time, but then took over a surgical supply com-pany, which he converted into a hearing aid sales and serv-ice business.
With limited knowledge in the field of hearing, he de-cided to take courses in hearing disorders and rehabilita-tion at Brooklyn College. Before the term was over, hisplan to attend classes for only one semester had changed;he stayed on to receive a master’s degree in speech andhearing, and later received his doctorate degree in audiol-ogy from The Graduate Center of The City University ofNew York.
Zelnick taught courses in hearing aid selection and eval-uation at the Technical College of The City University ofNew York. He conducted these courses for 16 years.
He also edited an IHS textbook entitled Hearing Instru-ment Selection and Evaluation, which was published in 1987.
IHS Leadership Works toStrengthen Coalition-BuildingIHS President James Ogurek, BC-HIS, and Executive Di-rector Cindy Helms attended the annual meeting of theHearing Industries Association (HIA) on February 15–17,2007. It was an excellent venue for networking with HIAand Better Hearing Institute staff, manufacturers, and al-lied associations. We thank HIA for the invitation to par-ticipate in this important event.
President-Elect Chris Gustafson, BC-HIS, ACA; Past Pres-ident Kathy Harvey-Jones, BC-HIS, CCCA; Executive Di-rector Helms; and Washington Counsel Karen Sealanderrepresented IHS on March 3, 2007 at the joint leadershipmeeting between IHS and the American Academy of Oto-laryngology–Head and Neck Surgery. This is an annualevent that reconfirms the commitment of both organizationsto continuing to grow their successful, ongoing partnership.Gustafson and Sealander spent March 2 on Capitol Hill vis-
iting with legislators and staff to advocate for issues of criti-cal importance to the hearing healthcare profession.
Celebrities Present Children withHearing Aids and Music DevicesSamsung Electronics America and the Starkey HearingFoundation teamed up to give the gift of hearing and musicto 200 children in the greater South Florida area. TheStarkey Hearing Foundation and Samsung Electronics pre-sented children with personally fitted hearing aids alongwith Samsung K5 digital audio players collectively valuedat over $1,000,000. At the Seminole Hard Rock Hotel, thechildren received gifts from stars such as Leslie Nielsen,Marion Ross, Paul Williams, Extreme Makeover HomeEdition’s Eduardo Xol, former Miss America HeatherWhitestone McCallum, and NFL stars Shaun Gayle andEmery Moorhead.
“Samsung is continually looking for opportunities towork with charitable organizations that help children andtheir families, and we are honored to be part of such awonderful cause,” said DJ Oh, president and CEO of Sam-sung Electronics.
The Starkey Hearing Foundation has helped bring thegift of hearing to children around the world through theirgenerous donations to those in need. Every year, the StarkeyHearing Foundation conducts more than 100 hearing mis-sion trips worldwide and provides more than 20,000 hear-ing aids to the hearing impaired.
“It is important for us to help children because they arethe future of the world—and if we neglect our children, wecan’t have a good future,” said William Austin, founder ofthe Starkey Hearing Foundation.
IHS Member Wins Dream HomeAn IHS member since 1998, Christine Feige, BC-HIS, fromOntario, Canada had the winning lottery ticket in a recentcharity event fundraiser. After purchasing seven tickets,Feige is now the lucky recipient of a 3,000-square-footbungalow home valued between $375,000–400,000.
“I just wish everyone could experience something likethis in their lifetime,” said Feige.
The Bluewater Health Foundation raised approximately$250,000 from the lottery, which will go toward newequipment for the hospital emergency department. Feige,who has been buying tickets since the lottery began 12years ago, said her dream finally came true. THP
THE HEARING PROFESSIONAL 25
Soundbytes

INTERNATIONAL INSTITUTE FOR HEARING INSTRUMENTS STUDIES
MARCH • APRIL 200726
IIHIS Approved Courses
Contact individual sponsors for locations and for program dateswhere not specified.
Accreditation of educational courses for continuing
education credit by the International Institute
for Hearing Instruments Studies does not imply
endorsement of a specific product or procedure.
Sponsor: Advanced BionicsDescription: Basic Hearing Instrument Technology;
Cochlear Implants; High-Resolution BionicEar System (3 hours)
Contact: Carissa Moeggenberg, 517.783.5383
Sponsor: Amplifon USADescription: Define Signal-to-Noise Ratio; The Quick
SIN Test; Directional Microphone Benefits(3 hours)
Contact: Jennifer Kolde, 763.268.4074
Sponsor: Audina Hearing InstrumentsDescription: Repair and Service; Final Wiring; Hands-On
Shell Lab; Shell Assembly (40 hours)Contact: Jennifer Brown, 800.223.7700, ext. 229
Sponsor: BeltoneDescription: Introduction to New Software; Beltone
Access; The Edge Collection; The OpenEvolution (8 hours)
Contact: Carrie Manning, 847.832.3751
Sponsor: GN ReSoundDescription: Fitting Sound Quality Hearing Instruments;
Occlusion; Case Studies (4 hours)Contact: April Bennett, 952.769.8481
Sponsor: Micro-TechDescription: Intro to New Technology; Feedback
Intercept; Directional Speech Detector(6 hours)
Contact: Lindsay Olson, 800.328.8602
Sponsor: OticonDescription: Patient Counseling; Advanced Signal
Processing; Amplification Strategies;Pediatric Hearing Aid Fittings (16 hours)
Contact: Dena Abood, 800.526.3921
Sponsor: Phonak Hearing SystemsDescription: Three New Product Features; Sound Relax;
User Preference (4 hours)Contact: Suzanne Smoak, 630.821.5114
Sponsor: Saskatchewan Hearing InstrumentPractitioners Society
Description: Signal-to-Noise; Present Hearing InstrumentTechnology; Effective Customer Interaction;When Hearing Aids Are Not Enough(11 hours)
Contact: Robin Dunlop, 306.771.4944
Date: May 10–11, 2007
Sponsor: Siemens Hearing Instruments
Description: Instruction on Industry Trends; Latest SignalProcessing Algorithms; Hands-On Training(10 hours)
Contact: Tom Powers, 732.562.6637
Sponsor: Sonic Innovations
Description: New Product Features; Noise Reduction;Directionality; Software Upgrades(2 hours)
Contact: Leah Drullinger, 503.819.9206
Sponsor: Starkey Laboratories
Description: New Hearing Aid Technology;Rehabilitative Techniques; Enhancingthe Hearing Aid Fitting Process(12 hours)
Contact: Lindsay Olson, 800.328.8602
Sponsor: Widex
Description: Rationale and Features of Different ProductFamilies; Fitting and Programming ofDifferent Products (2 hours)
Contact: Francis Kuk, 630.245.0025
This is a partial list of approved courses. For a complete roster, contact IIHIS at 734.522.7200.

THE HEARING PROFESSIONAL 27
Name
Address
City State/Province Zip/Postal Code
Office Telephone
SS/SI#
Professional and/or Academic Credentials:
(PHOTOCOPY THIS FORM AS NEEDED)Please check one: □ $20.00 (member) □ $40.00 (non-member)
COUNSELING THEORIES—MARCH/APRIL 2007—DEADLINE: APRIL 2008
1. a b c d
2. a b c d
3. a b c d
4. a b c d
5. a b c d
6. a b c d
7. a b c d
8. a b c d
9. a b c d
10. a b c d
ANSWER SECTION(Circle the correct response from the test questions above.)
IIHIS ContinuingEducation Test:Counseling TheoriesApplied to FittingHearing Losses
1. According to psychologist Michael Harvey, a person whodecides to get hearing aids is often at which stage in thedecision-making process?a. lack of awareness of the hearing lossb. ambivalencec. rejection of the thought of hearing aidsd. determination to accept a change and get hearing help
2. Which condition is most likely to trigger immediateaction?a. mild ear infection with aural fullness and no painb. sudden idiopathic unilateral hearing lossc. gradual bilateral sensorineural hearing lossd. mixed hearing loss resulting from otosclerosis
3. At what level in decibels is normal conversational speechusually presented?a. 50–60 dB HLb. 15–25 dB HLc. above 80 dB HLd. at the SRT level
4. Psychologist B. F. Skinner is remembered for:a. teaching dogs to salivate when a stimulus is presentedb. using positive reinforcement as a way to change behaviorc. discovering the concept of the egod. teaching the interpretation of dreams
5. Reducing the feelings of isolation caused by a hearing lossis associated with the work of:a. Sigmund Freudb. Dr. Joyce Brothersc. Carl Rogersd. Dr. Phil
6. What is the term for the subtle physiological changesmade by the auditory nervous system in acceptingamplification?a. neural plasticityb. habituationc. JNDd. none of the above
7. Cognitive counseling seeks to:a. allow the hearing aid wearer to determine the type of
instruments best suited for the lossb. give visual input through real-ear measures to set the hearing
aids to the best levelc. combine behaviorism and phenomenology with known
physiological principlesd. utilize a multisensory approach in fitting hearing aids
8. A method which allows a person to adjust to amplificationis to:a. utilize the concept of JNDb. gradually increase the gain/output to allow for the patients to
acclimate to amplificationc. set the instruments at the highest output and reduce the gain/
output after the instruments have been worn for several weeksd. a and b
9. One technique for encouraging hearing aid use might be tohave a relative call the hearing aid user at different timesof the day. This is an example of:a. positive reinforcementb. monitoring the hearing aid wearer to be sure the aids are
being usedc. operant conditioningd. a, b, and c
10. By enhancing the benefits of amplification as opposed tothe negatives, the patient is:a. refocusing his thinking to accept amplificationb. overcoming the masking effects of ambient noisec. being influenced by advertising meant to be deceptived. trying to put on the best show for the family who insists on the
use of amplification
For continuing education credit, complete this test and send the answer section at the bottomof the page to: International Institute for Hearing Instruments Studies
16880 Middlebelt Rd., Ste. 4, Livonia, MI 48154• After your test has been graded, you will receive a copy of the correct answers and a
certificate of completion from the International Institute for Hearing InstrumentsStudies (IIHIS).
• All questions regarding the examination must be in writing and directed to IIHIS.• Credit: IIHIS designates this professional development activity for one (1) continuing
education unit (CEU).• Fees: $29.00 IHS members $59.00 non-members (Payment in U.S. funds only.)
✁

CLASSIFIEDS
28 MARCH • APRIL 2007
AD INDEX
Avada. . . . . . . . . . . . . . . . . . . . . . . . . . . . . IBC
Discovery Hearing AidRepair . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Discovery Hearing AidWarranties . . . . . . . . . . . . . . . . . . . . . 17
NBC-HIS . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Oticon . . . . . . . . . . . . . . . . . . . . . . . . . . . . IFC
Siemens . . . . . . . . . . . . . . . . . . . . . . . . OBC
Email classified ad copy to [email protected] or fax to 734.522.0200. The ad rate is $.99 per regularword and $1.15 per boldface or all-capped word, with a minimum rate of $50.00. There is an additionalcharge of $20 for boxed ads. For additional information call 734.522.7200.
EDUCATION
PREPARE FOR YOUR NBC-HIS ORSTATE LICENSING EXAM—Revisedand recorded on-site in 2004, our Profes-sional Seminars provide the latest up-dated information. Power point slides, studymaterials and sample exams included. Since1977, we have helped over 3,500 hearinghealthcare professionals earn their credentialsand are recognized as the industry’s leading re-source in preparation for competency exams.State Licensing (DVD $395 or CD $265),NBC-HIS (DVD $295 or CD $245). 10% dis-count with purchase of any two programs.Also, brand new for beginners with no ex-perience, The Hearing Aid Evaluation forNew Dispensers (2-DVD set) $195. Toorder, please call Alan Lowell Seminars800.749.4644. Visa/MC/AMEX/Check ($10S&H per program/two day delivery). Visit:www.alanlowellseminars.com.
If you or your staff need training to pass theState License or the NBC-HIS Exam,then look no further, you have found theright place.Total Hearing MarketingConcepts is currently helping the hearinghealth care field and has for the past 18years with a 90% passing rate for all statesand NBC-HIS exams. We are the only onethat teaches from experience in that wehave been licensed in 16 states and havetaken the exams ourselves; also we havebeen a proctor and administrator for theNBC-HIS exam over 40 times, with over30 years dispensing experience. The courseis continually being updated so that youhave the most current information. You willreceive not only the training manual, but acopy of every slide that is shown with aplace to make notes along with a practiceexam of 500 questions. So give Dave Os-walt a call at 651.455.7500 to set up aclass and get ready to shine at your exam.
HAVE YOUR CAKE AND EAT IT TOO!Looking for hearing specialists/audiologists inCA, NV, and HI. We will build your office in thestyle and location of your preference at no costto you. 80K+, Benefits. Send Résumé: Fax:805.449.1164, [email protected]. Calltoday for your dream job! 801.205.2581.
FABULOUS MENTORING OPPORTUNITY
Looking for experienced Board CertifiedHearing Instrument Specialists and/or Audiol-ogists willing to mentor a trainee for one totwo weeks in your office. Our company, Ac-tivEars Hearing Centres, is growing in South-Western Ontario and we want our intelligent,motivated and trustworthy employees to bethe best! But we can only do this with yourhelp. This is a unique opportunity for you tohelp future hearing specialists and teach themwhat you know. Please contact Christine FeigeBC-HIS at [email protected] for more de-tails if this sounds interesting for you. Our em-ployees can only be the best if they learn fromthe best! Email today!
FOR SALE
BUSINESS FOR SALEVery busy hearing aid practice for sale in Mis-souri, approximately 50 miles north and west ofSt. Louis. Two offices in rapidly growing com-munities. The practice could accommodate twodispensers or could keep one dispenser verybusy. Last year the practice grossed $330K.Please mail inquiries to Cleo Norman, P.O. Box254, O’Fallon, Missouri 63366.
LOCATION FOR SALEUnusual opportunity. 28 years continual use ashearing aid dispensing office on busy Highway17-92 in Casselberry, FL. Site has excellentlighted sign. Building has built-in sound room,3 small consultation rooms and waiting roomoffice. Property for sale. 407.805.0246 or407.620.9682.
POSITIONSAVAILABLE
FLORIDA EMPLOYMENTOPPORTUNITYHearing aid capital of the world.Seeking determined, ethical, Nationally BoardCertified Specialists or Audiologists for loca-tions in several Florida retirement communi-ties. Join our team of motivated, successful,Hearing Care Providers with proven practicedevelopment support! Fax résumé to H&MHearing Associates to 772.219.9703, Email:[email protected] or call John Hoglund at941.704.5753.
Hearing Instrument Specialist/Audiologist
Outstanding career opportunity in beautifulMontana available in several locations offeredby a well-established firm. $100,000 + po-tential, benefits package. 406.755.5077 [email protected], fax 406.755.5995.
Our Website provides a host ofexciting opportunities for improved
communications betweenmembers, staff, and leadership.Send an email to Tami Bethune
at [email protected]—we’ll do the rest!
Got Email?