Embed Size (px)
Citation preview

THE HEALTHCARE
NEIGHBORHOOD:
PHILANTHROPY'S ROLE
IN AGING WELL Grantmakers in Aging, October 2015

ROBYN GOLDEN, LCSW
DIRECTOR, HEALTH AND AGING
RUSH UNIVERSITY MEDICAL CENTER

Social Need
• Social factors influence health outcomes • Socioeconomic status
• Education
• Stress
• Early life
• Social exclusion
• Social support
• Addiction
• Food
• Transport
• Work/Unemployment

Health Care’s Blind Side
• 2011 Robert Wood Johnson Foundation survey of 1,000 primary care physicians
• 4 out of 5 not confident can meet social needs, hurting their ability to provide quality care
• Institute of Medicine recommendation: create “community links”
• Assessing psychosocial issues
• Delivering services in the community
• Communicating these issues with medical team

What’s Needed for Chronic Care
• Report from Georgetown Public Policy Institute
highlights opportunities for improving care for
people with chronic care needs:
• Comprehensive primary care
• Assessment of client and caregiver long-term services
and supports (LTSS) needs
• Coordination of LTSS and medical care
• Collaboration between care coordinators, PCPs,
patients, families
• Supportive care transitions
• Commitment to person- and family-centered care

Care Transitions
• Psychosocial issues are present all the time for
people
• needs during transition greater than simply medical
• Issues exacerbated post-hospitalization:
• Unanticipated needs emerge post-discharge
• Cognitive limitations after hospitalization
• Stress of hospitalization
• Differences in physical endurance and mobility
• Opportunity for intervention, community
engagement

But why are transitions so complicated?
• For these reasons, essential to involve medical care
as well as long-term services and supports (LTSS)
• Healthcare system to attend to medical needs
• LTSS system to provide continuous, coordinated services for
non-medical needs
• Psychosocial
• Environmental
• Emotional
• Financial
• Interpersonal
• Both systems sharing vital information
• Interprofessional collaboration key

Fundamental Change
• These efforts require interprofessional teams
• Physicians are critical - but others needed, too
• Nurse practitioners
• Physician’s assistants
• PT, OT
• Social workers
• Nutritionists
• Pharmacists
• Many more
• Also requires community
support systems, innovative
care models

Our History of Partnering Together
• Projects driven by Rush Health & Aging, Aging Care
Connections
• Care transitions: Bridge Model of transitional care
• Primary care: Ambulatory Integration of the Medical and the Social
(AIMS) Model
• Support of Community Memorial Foundation

A Health Neighborhood
• Flow of information between providers and patients
• Requires basic communication and coordination functions
• Each service provider needs… • to conceptualize itself as a team member
• a broad understanding of each patient’s medical and psychosocial needs
• Goals • Effectively coordinate all care
• Help the patient navigate the system
• Ensure that treatment plans from different providers work together as a whole

Older Adult Health Neighborhood Project
Designed to create a platform for a
comprehensive, well-integrated
“neighborhood” of health care resources
designed to foster preventative care,
further self management of chronic disease,
and create an intensive community
intervention for older adults who frequently
require healthcare

OAHN: Grant Agreement
Goal: To implement a network of for-profit and
non-profit organizations that will serve 1,000 older
adults in the Community Memorial Foundation
communities, across the continuum of aging –
from prevention to highly complex patients in
danger of unnecessary hospitalization and poor
health outcomes

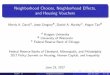
LTSS in a Neighborhood
Other LTSS
CDSMP
DSMP
Exercise Program
Mental Health and Substance Abuse
Falls Management and Prevention
Alzheimer's Programs Medication Management
Home Injury/ Risk Screenings
Other Health Prevention Programs
Home-delivered meals
Nutrition services or nutrition counseling
Caregiver Support
Personal care/ homemaker/ choremaker
services
Transportation
Source: Medical Expenditures Panel Survey, 2009

Optimize timely access to resources from multiple sites
Risk Stratified Care Management
Acute Health Care
Comprehensive Primary Care
for:
Patient Centered
Care
Better Health / Better Care
/ Lower Cost
Source: Medical Expenditures Panel Survey, 2009
Change Concept

Continuum
• Aging as a process
• Health occurs throughout the life span and health benefits
are cumulative
• Three work groups based on this concept:
Prevention, Chronic Illness, and “Hot spotters”

Prevention Group
• Action Plan
• Target local for- profit and nonprofit businesses to
increase community awareness
• Educate businesses on aging and health related issues
• Further cultural competence
• Ask consumers for feedback through focus groups

Chronic Disease Group
• Statistically important group
• Traditional interventions focus on deficits
• Health system focused on acute episodes and
disease process
• Intervention needed at multiple sites; mental
health clinics, primary care offices, home of the
patient and throughout the community
• Access to tools for health behavioral change

Hot spotters – Who are They?
• Top 1% of high cost patients who consume 28%
of all health care costs
• Approximately 75% adults, 25% pediatrics
• Despite the high cost care they receive Hot
spotters are not getting well
• 5 year mortality rate = 26%
• Hot spotters say they need more help in
understanding complex follow up care

Hot spotters – Who are they?
• They describe their quality of life as fair to poor
• By a 2-1 margin they attributed their health problems to themselves
• 63% suffer from depression
• 77% have chronic conditions (cardiovascular, renal disease, cancer, stroke, arthritis, etc.)
Scott B Pingree, Harvard Business Review

Challenges and Opportunities
• Time limitations for neighborhood partners
• Careful selection of partners based on their assets and
role in the community
• Establishing a leadership format that reflects the
collaboration while providing a sense of direction
The Opportunities in the health care are now
Changes in the payments system, transformation from an
acute care model to a continuity of care model of care
OPPORTUNITIES FOR SOME, LOSS FOR OTHERS

GREG DIDOMENICO
PRESIDENT/CEO
COMMUNITY MEMORIAL FOUNDATION

Vision Statement for the Neighborhood
“To collaboratively transform the healthcare
of aging adults through the creation of a
health neighborhood that assists the whole
person, affirms the benefits of a life long
process of wellness and prevention.”

Community Memorial Foundation’s Vision
The Foundation,
together with the community,
will transform the western suburbs of Chicago
into the healthiest region in the country

Shared Vision
Vision Statement for the
Neighborhood
To collaboratively transform
the healthcare of aging
adults through the creation
of a health neighborhood
that assists the whole
person, affirms the benefits
of a life long process of
wellness and prevention
Community Memorial
Foundation’s Vision
The Foundation,
together with the
community,
will transform the western
suburbs of Chicago
into the healthiest region in
the country

Shared Vision

Healthy Cities
Healthy Regions
Healthy Neighborhoods

Achieving Our Vision for a Healthy Region
Three Strategic Priorities:
1. Develop coordinated, efficient and
effective health and human service
systems
2. Collaboratively establish a regional health
and human services agenda
3. Build healthy organizations

Foundation’s Role:
grantmaker
changemaker

catalyst
educator
convener
advocate
changemaker
grantmaker

Board’s
Role

Foundation’s Commitment


The Trifecta
Hospital Grantee Foundation

Health Neighborhood Outcomes Current readmission data provided by our partner hospital
shows a reduction in 30 day readmissions from 22% to 9%
for patients who receive the Bridge Intervention.
Successfully intervened with 287 older adults and/or their
caregivers onsite at Primary Care Physician’s sites in the
last year reports show high levels of physician satisfaction
and improved health literacy.
Developed a network of 15 separate community entities
committed to moving toward the goal of integrated
healthcare for all older adults residing in the Community
Memorial Foundation’s footprint called the Aging Well
Health Neighborhood

With Thanks to Our Partners

LOUISE STARMANN, LCSW
AGING CARE CONNECTIONS

Achievements by the Older Adult Health
Neighborhood • Prevention Group
• Conducted community focus (N=34)
• Piloted and created a business training integrating nursing, social
work, and public health expertise
• Reached out to 30 local businesses and slated to train 13 businesses
• Chronic Disease Group
• Coordinated 4 medication reviews and blood pressure screenings
• Coordinating and building capacity Chronic Disease Self-Management
Program (Lorig) and other evidence-based health promotion
• High Utilizers
• Partnerships secured with two PCP practices
• 10 referrals received
• Anticipating data coordination with health system

Next Steps • Submission for year 2 funding for the Older Adult Health
Neighborhood Project submitted by Aging Care Connections
• Establishment of outcomes that can be measured across
community partner sites
• Work towards sustainability from multiple sources by demonstrating
quality and cost savings to health care providers
• Streamlined communication
• Acquiring data on health outcomes from several sources within
HIPPA guidelines
Continued development of the collaboration between Community
Memorial Foundation, Rush Health and Aging, and Aging Care
Connection holds great promise for the future of aging in our
community

Thank you
• Our thanks to the Community Memorial Foundation for
their vision and belief in the collective impact that can be
achieved when communities work together.
• Thanks for your role as conveners of discussion and
action to bring about change
• Thanks to Rush Health and Aging; they bring such
knowledge and expertise to our community so that we can
continue to learn and grow.

Small Group Brainstorming
If you were developing a model
to engage neighborhood assets
to help keep seniors safe and
well in the community, what are
three elements or resources or
strategies that MUST be
included?