Embed Size (px)
Citation preview
The health risks of low-dose ionizing radiation
Abel Russ
Community-Based Hazard Management ProgramGeorge Perkins Marsh Institute
Clark University
Radiation BasicsRadiation Basics
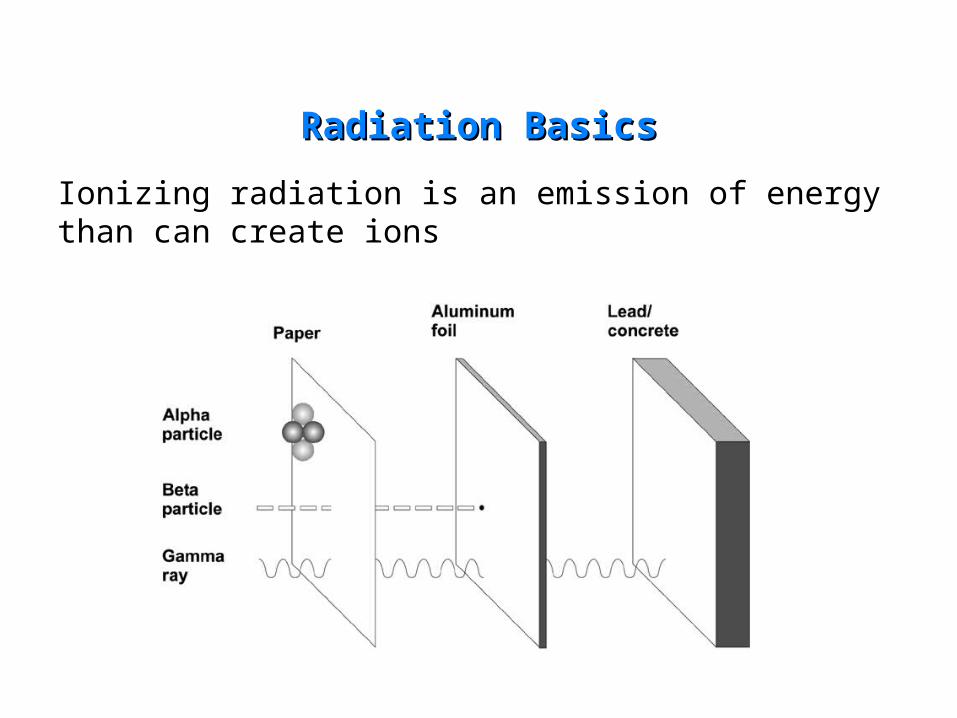
Ionizing radiation is an emission of energy than can create ions
Radiation BasicsRadiation Basics

Radiation BasicsRadiation Basics
A cell that is “hit” by radiation reacts to the event in several ways:
The cell has defense mechanisms that are triggered-Cell-cycle checkpoints
Cell death
Repair machinery
The hit cell interacts with nearby cells (bystander effect),
The hit cell may also produce unstable daughter cells as it divides (genomic instability)
Ultimately, affected cells may be altered and may begin to behave differently.
Radiation BasicsRadiation Basics
• Cells that grow out of control become cancers
• leukemia/lymphoma and “solid cancer”
• Noncancer effects of radiation include blood disorders, circulatory problems, thyroid problems, liver disease, others
• The magnitude of these effects depends on the radiation dose and other variables

Radiation BasicsRadiation Basics
Dose units are confusing!
• The mean dose received by the atomic bomb survivors was 0.2 Sv
• A “low dose” of radiation is generally thought of as less than 0.1 Sv
• The average nuclear worker is exposed to 0.02 Sv
• Average background exposure to radiation is ~ 0.003 Sv per year
Atomic bomb survivorsAtomic bomb survivors
• The main source of data used to estimate radiation risk
• ~100,000 people in Hiroshima and Nagasaki
• 440 solid cancer deaths 1950-1997
• 87 leukemia deaths 1950-1990
• 472 noncancer deaths 1950-1997

Atomic bomb survivors/ Epidemiology basicsAtomic bomb survivors/ Epidemiology basics
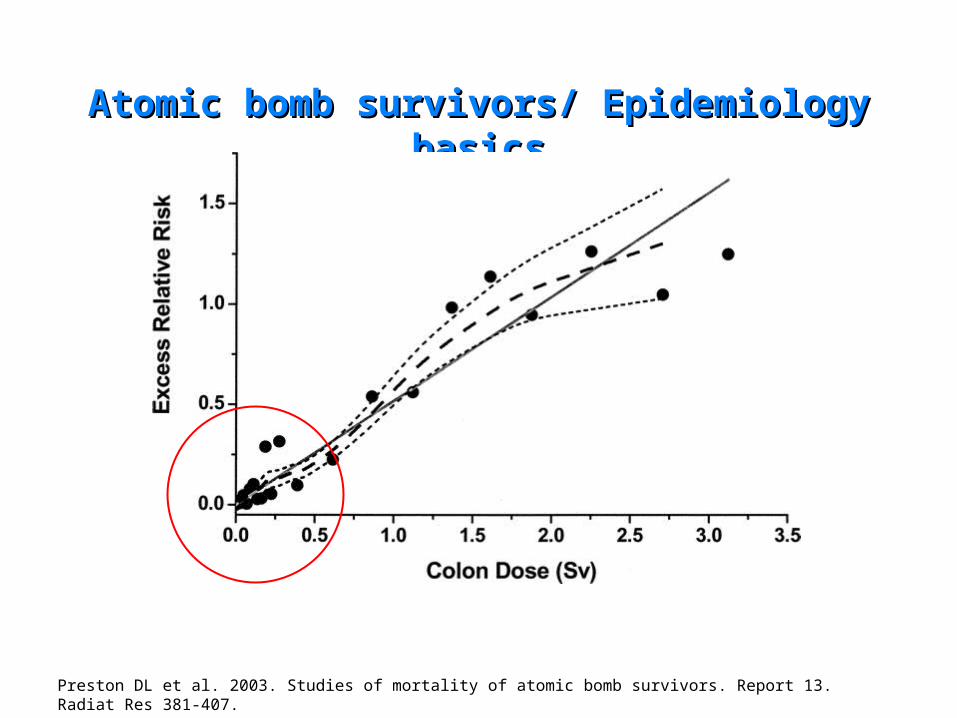
Between 1950 and 1997 there were 9,335 deaths from solid cancer.
Based on background rates only 8,895 were expected.
Relative Risk = 9,335/8,895 = 1.05
Excess Relative Risk = 0.05
Atomic bomb survivors/ Epidemiology basicsAtomic bomb survivors/ Epidemiology basics
Preston DL et al. 2003. Studies of mortality of atomic bomb survivors. Report 13. Radiat Res 381-407.
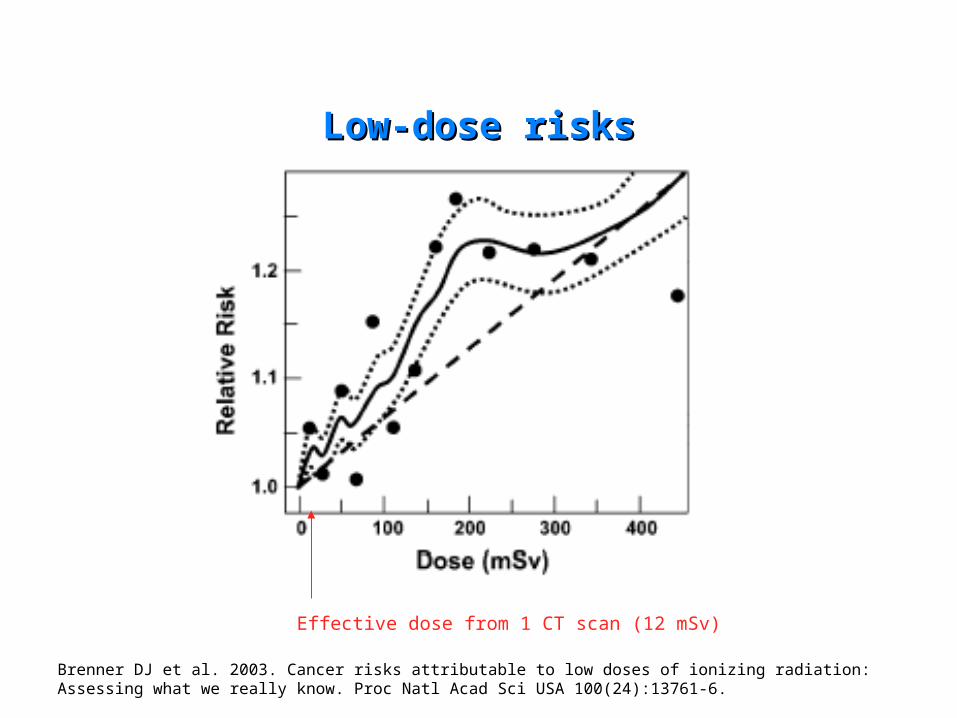
Brenner DJ et al. 2003. Cancer risks attributable to low doses of ionizing radiation: Assessing what we really know. Proc Natl Acad Sci USA 100(24):13761-6.
Low-dose risksLow-dose risks
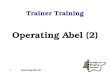
Effective dose from 1 CT scan (12 mSv)
Low-dose risksLow-dose risks
0
0.4
0.8
1.2
1.6
2
0 20 40 60 80 100
mean dose (mSv)
ER
R/S
v (S
E)
0-50 mSv
0-100 mSv0-125 mSv
0-150 mSv 0-200 mSv
0-500 mSv
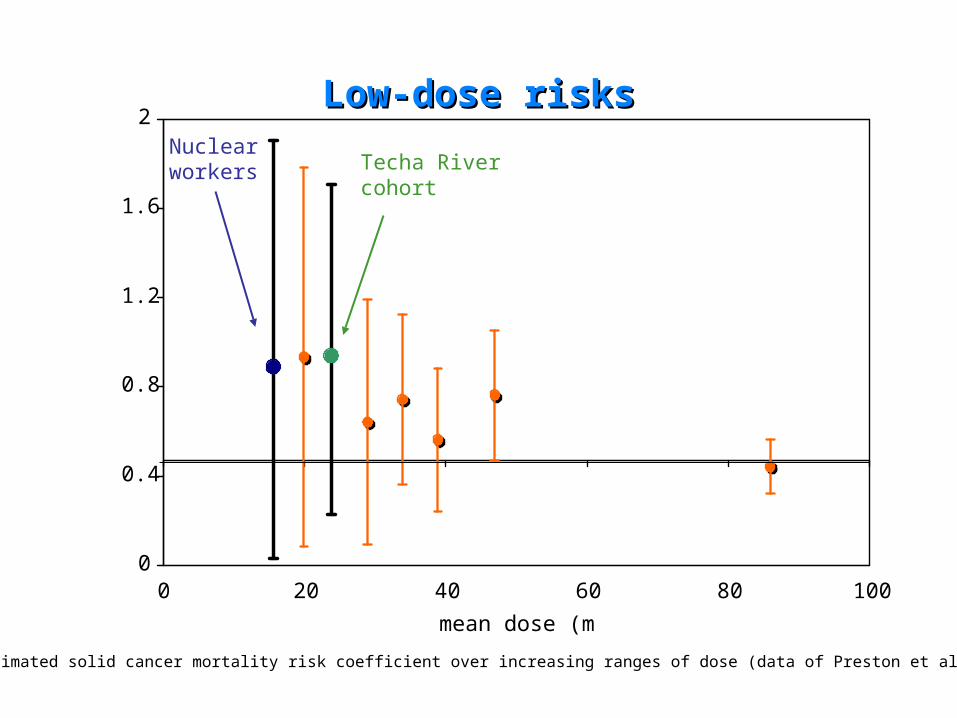
Estimated solid cancer mortality risk coefficient over increasing ranges of dose (data of Preston et al. 2003).
Nuclear workers Techa River
cohort

Low-dose risksLow-dose risks
Low-dose atomic bombsurvivors (Preston et al. 2003)
Nuclear workers(Cardis et al. 2005)
Techa River(Krestinina et al. 2005)
Mean dose 0.02 Sv1 (colon) 0.02 Sv (colon) 0.03 Gy (stomach)
ERR forsolid cancer
0.93/Sv(SE 0.85)
0.87/Sv(0.0-1.9)
0.92/Gy(0.2-1.7)
1 This group received colon doses of 0-0.05 Sv.
1This group received colon doses of 0-0.05 Sv.
Recent data from nuclear workers and Techa River cohort
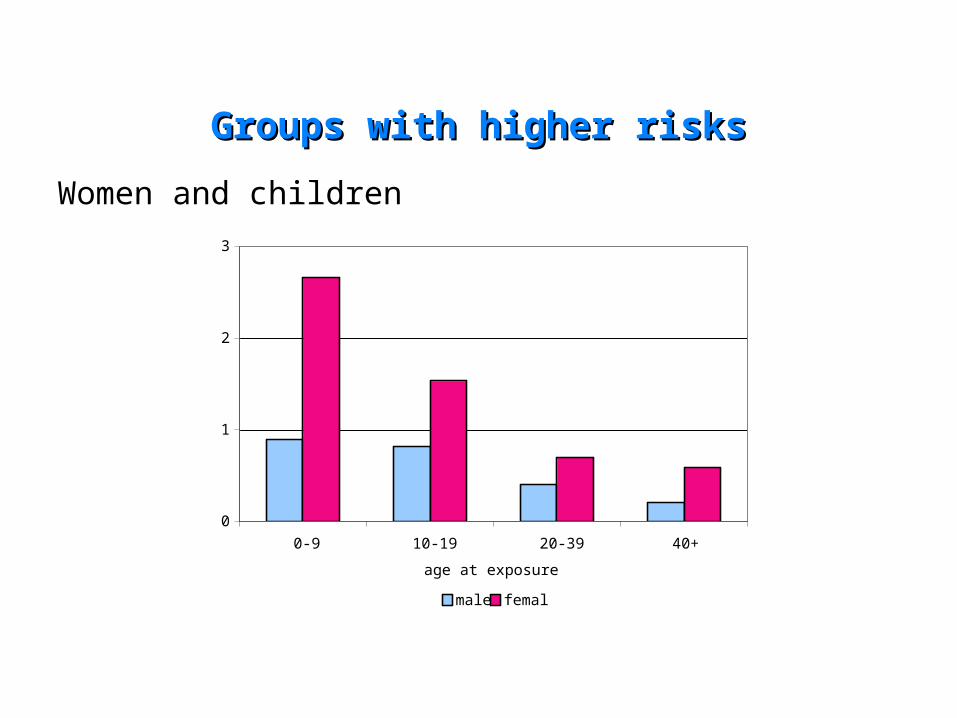
Groups with higher risksGroups with higher risks
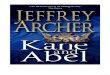
Women and children
0
1
2
3
0-9 10-19 20-39 40+
age at exposure (years)
ER
R p
er S
v
male female
Other sources of epidemiological informationOther sources of epidemiological information
•Nuclear workers
•Techa River residents
•People exposed to medical radiation
•Nuclear test site downwinders

Children’s riskChildren’s risk
• Many examples of childhood sensitivity to radiation
•Exposures to x-rays in the womb:
• Significant childhood cancer risks at doses as low as 0.006 Sv
• ERR 30 to 50/Sv
• Childhood leukemia near the Nevada Test Site and Chernobyl

Solid cancer mortality in Techa River residents (Krestinina 2005): • ERR 0.6/Gy (men), 1.2/Gy (women)
Solid cancer mortality among nuclear workers from three countries (Cardis et al. 1995):• ERR for men- -0.07/Sv (90%CI -0.4-0.3)• ERR for women- 0.97/Sv (90%CI <0.9-8.2)
Women’s riskWomen’s risk
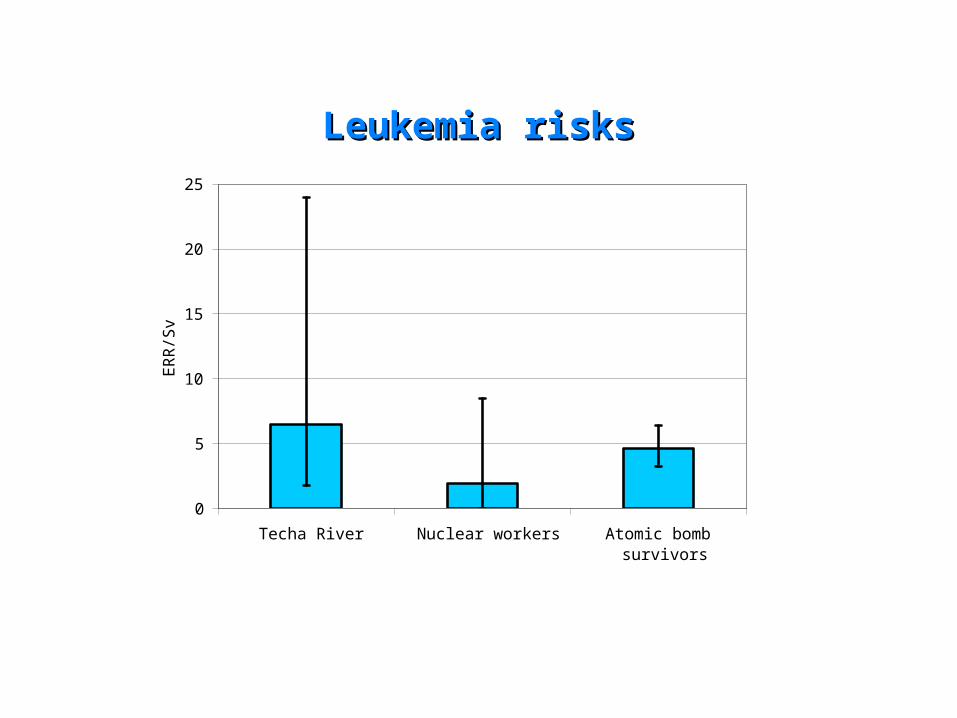
Leukemia risksLeukemia risks
0
5
10
15
20
25
Techa River Nuclear workers Atomic bombsurvivors
ER
R/S
v

Noncancer risksNoncancer risksCirculatory disease mortality:
Atomic bomb survivors: ~165 deaths associated with exposure
1.00
1.01
1.02
1.03
1.04
atomic bombsurvivors (heart
disease)
atomic bombsurvivors (stroke)
3-country workers Chernobyl workers
Rela
tive
Ris
k at
20 m
Sv

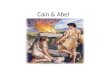
Noncancer risks: Noncancer risks: exposure age and disease incidenceexposure age and disease incidence
1
1.5
2
10 25 40
age at exposure
RR
at
1 S
V thyroid disease
liver disease
uterine myoma
cataract
hypertension
myocardial infarction

National Academy of Sciences: BEIR VIINational Academy of Sciences: BEIR VII
Reaffirms that the linear, no threshold model for radiation and cancer is the most appropriate available model. ATSDR Public Health Assessments are inconsistent with this idea by supporting the use of a threshold.
Rejects the idea of hormesis for purposes of assessing radiation risks
Uses a DDREF (dose- and dose-rate effectiveness factor) to reduce risk estimates below the linear model predictions for low levels of exposure; risk estimates are lower than those produced by the UN Scientific Committee on the Effects of Atomic Radiation (UNSCEAR), which does not use this factor.

Health Effects of Ionizing Radiation: Health Effects of Ionizing Radiation: Half-time reviewHalf-time review
• Radiation increases the risk of cancer and other disease
• There is no “safe” dose of radiation
• Risk is related to dose, although simple extrapolations from high doses may underestimate risk
• Women and children are relatively sensitive to radiation

Communities near nuclear facilitiesCommunities near nuclear facilities
Maximum allowable doses are less than average background radiation exposures
Community members are routinely exposed to many carcinogens
Individual exposure information is not available
If exposures are kept within allowable limits, we should not expect to see clear evidence of a health impact

Areas at riskAreas at risk
Studies often count cancer cases within a certain distance from a facility or in a convenient administrative unit (county)
Black RJ et al. 1994. Leukemia and non-Hodgkin’s lymphoma: incidence in children and young adults resident in the Dounreay area of Caithness, Scotland in 1968-91. J Epidemiol Community Health 48:232-6.
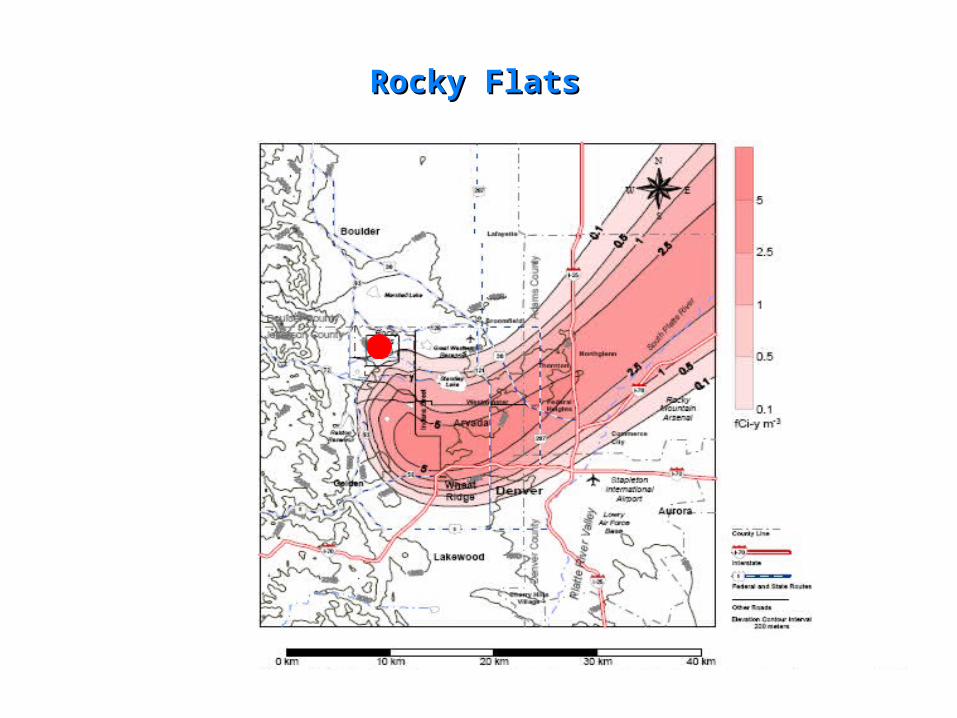
Rocky FlatsRocky Flats

Rocky FlatsRocky Flats
Significant correlations between soil plutonium and total cancer and radiosensitive cancer in males for both periods
Significant correlations between soil plutonium and total cancer and radiosensitive cancer in females for the 1979-1981 period
Cancer incidence significantly elevated closer to Denver; the association between soil plutonium and cancer incidence diminishes when controlling for this effect
Crump et al. 1987.
Childhood leukemia: USChildhood leukemia: US
The National Cancer Institute conducted a nationwide survey of cancer data at the county level near nuclear facilities.
• 52 nuclear power plants
• 10 DOE sites
Incidence data were only available for counties in Connecticut and Iowa. In the four eligible counties there were 81 cases of leukemia under age 10 diagnosed between the date of plant start-up and 1984. The incidence ratio, 1.36, was significantly elevated (p<0.01).
There were 2,572 deaths from leukemia under age 10 in counties with a nuclear facility. This represents a relative risk of 1.03 compared to control counties (confidence information not provided).
Jablon et al. 1991.

LLNL workers and melanomaLLNL workers and melanoma
Excess melanoma between 1969-1980 related to:•Occupational exposures (chemicals and ionizing radiation)•Other factors (sun exposure, skin tone, etc.)
Odds Ratio 2.3 (95%CI 1.0-7.6)
Atomic bomb survivors Relative Risk 3.1 (95%CI 0.7-13.5)
Melanoma excess declining over time
Data from Los Alamos National Lab are not consistent with such a large excess (SIR 105, 95%CI 51-198)

Precautionary principlePrecautionary principle
The burden of proof should fall on the proponent of an activity and not the public
“Proof” vs. “reasonable cause of concern”
The decision-making process should be open and democratic and should involve affected parties
The full range of alternatives should be considered, including no action

Transgenerational effects of radiationTransgenerational effects of radiation
• A 1984 government survey found 6 childhood leukemia deaths in Seascale between 1968 and 1978 (1.4 expected). A formal case-control study was published in 1990.
• LNHL before age 25, 1950-1985
• 52 cases of leukemia, 22 cases of non-Hodgkin’s lymphoma, 1001 controls
• Children of radiation workers employed at conception showed a RR of 1.48 (0.59-3.75) for LNHL
MJ Gardner et al. 1990. Results of case-control study of leukaemia and lymphoma among young people near Sellafield nuclear plant in West Cumbria. BMJ 300:423-9.

Challenges to the Gardner hypothesisChallenges to the Gardner hypothesis
• Unlikely biological mechanism; childhood cancer is not known to have a strong heritable component
• No leukemia in the children of atomic bomb survivors
• Other explanations for the West Cumbria cluster including a virus spread during population mixing
• No evidence of similar leukemia clusters in other communities
R Doll et al. 1994. Paternal exposure not to blame. Nature 367:678-80.
MP Little et al. 1995. A review of the risks of leukemia in relation to parental pre-conception exposure to radiation. Health Phys 68(3):299-310.
JD Boice Jr. et al. 2003. Genetic effects of radiotherapy for childhood cancer. Health Phys 85(1):65-80.

SpermatogenesisSpermatogenesis
Spermatocyte stage is proficient in the repair of DNA damage; spermatozoa stage is deficient
K Shiraishi et al. 2002. Persistent induction of somatic reversions of the pink-eyed unstable mutation in F1 mice born to fathers irradiated at the spermatozoa stage. Radiat Res 157:661-7.

Pink-eyed Jackson micePink-eyed Jackson mice
• Induced reversion of unstable allele is visible as black coat spots or retinal spots
• Male mice were exposed to x-rays and mated immediately or 15 weeks later
• After irradiation of spermatozoa (1-6 Gy):
• 1.8-fold increase in mutations at paternal allele
• 1.5-fold increase in mutations at maternal allele
• Eye spots of all sizes were found; irradiation did not determine timing of mutation
K Shiraishi et al. 2002. Persistent induction of somatic reversions of the pink-eyed unstable mutation in F1 mice born to fathers irradiated at the spermatozoa stage. Radiat Res 157:661-7.

Atomic bomb survivorsAtomic bomb survivors
• 31,150 children of exposed parents (16 cases)
• 41,066 controls (17 cases)
• Rate Ratio for childhood leukemia 1.2 (0.6-2.5)
• Fewer than 2% of the F1 cohort were conceived within 6 months of the bombings and roughly half of these parents were men
Y Yoshimoto et al. 1990. Malignant tumors during the first 2 decades of life in the offspring of the atomic bomb survivors. American Journal of Human Genetics 46:1041-52.

Childhood leukemia in Northeastern US 1959-62; any x-rays before conception
Childhood leukemia in urban Shanghai 1974-86; any x-rays before conception
Infant leukemia in Children’s Cancer Group (US and Canada) 1983-88; any x-rays within 1 year of conception
Childhood LNHL in German Childhood Cancer Registry 1992-94; any x-rays within 2 years of conception
Combined estimateCombined estimate
OR 1.3 (0.9-1.9)
OR 2.2 (1.5-3.3)
OR 1.3 (0.5-3.5)
OR 1.3 (1.1-1.6)
OR 1.4 (1.2-1.7)OR 1.4 (1.2-1.7)
Paternal preconceptional x-ray examsPaternal preconceptional x-ray exams
S Graham et al. 1966. Preconception, intrauterine, and postnatal irradiation as related to leukemia. National Cancer Institute Monographs 19:347-71.
XO Shu et al. 1988. A population-based case-control study of childhood leukemia in Shanghai. Cancer 62:635-44.
XO Shu et al. 1994. Association of paternal diagnostic x-ray exposure with risk of infant leukemia. Cancer Epidemiology, Biomarkers and Prevention 3:645-53.
R Meinert et al. 1999. Associations between childhood cancer and ionizing radiation: results of a population-based case-control study in Germany. Cancer Epidemiology, Biomarkers and Prevention 8:793-9.

ConclusionsConclusions
Epidemiologic studies of preconceptional exposure tend to support the association with childhood leukemia risk
Animal studies suggest new mechanisms that might explain this association:
• Genomic instability originating in late-stage spermatids or spermatozoa
• Radiation-induced sensitivity to second mutagenic exposure
Preconceptional radiation exposure and other etiologies are not mutually exclusive