Embed Size (px)
Citation preview

ARTICLE IN PRESS
0277-9536/$ - se
doi:10.1016/j.so
�CorrespondE-mail addr
teixeira@email.
(A. Shiell).
Social Science & Medicine 63 (2006) 165–178
www.elsevier.com/locate/socscimed
The health of nations in a global context: Trade, globalstratification, and infant mortality rates
Spencer Moorea,�, Ana C. Teixeirab, Alan Shiellc
aUniversite de Montreal Montreal, Que., CanadabUniversity of North Carolina, NC, USA
cUniversity of Calgary, Canada
Available online 2 February 2006
Abstract
Despite the call for a better understanding of macro-level factors that affect population health, social epidemiological
research has tended to focus almost exclusively on national-level factors, such as Gross Domestic Product per capita
(GDP/c) or levels of social cohesion. Using a world-systems framework to examine cross-national variations in infant
mortality, this paper seeks to emphasize the effects of global trade on national-level population health. Rather than
viewing national-level health indicators as autonomous from broader global contexts, the study uses network analysis
methods to examine the effects of international trade on infant mortality rates. Network data for countries were derived
from international data on the trade of capital-intensive commodities in 2000. Using automorphic equivalence to measure
the degree to which actors in a network perform similar roles, countries were assigned into one of six world-system blocks,
each with its own pattern of trade. These blocks were dummy-coded and tested using ordinary least squares (OLS)
regression. A key finding from this analysis is that after controlling for national-level factors, the two blocks with the
lowest density in capital-intensive exchange, i.e., the periphery, are significantly and positively associated with national-
level infant mortality rates. Results show the effects of peripherality and stratification on population health, and highlight
the influence of broader macro-level factors such as trade and globalization on national health.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Global health; Health inequalities; Trade; World-systems theory; Infant mortality; Automorphic equivalence
Introduction
Despite the relative proliferation of studiesexamining cross-national variations in populationhealth, recently greater attention has been given tothe development of contextual understandings ofglobal health inequalities (Coburn, 2004, 2000;
e front matter r 2006 Elsevier Ltd. All rights reserved
cscimed.2005.12.009
ing author. Tel.: +514 890 8000.
esses: [email protected] (S. Moore),
unc.edu (A.C. Teixeira), [email protected]
Labonte & Torgerson, 2002; Shandra, Nobles,London, & Williamson, 2004). The developmentof such understandings has led scholars to examineinter- rather than intra-national factors that influ-ence population health. While more recent studieshave led us to think critically about the effects ofinternational factors and pro-market ideologiessuch as ‘‘neo-liberalism’’ on population health, theyhave yet to provide a framework that we might useto measure how countries are differentially posi-tioned within the global system and examine howthis global stratification among countries influences
.

ARTICLE IN PRESSS. Moore et al. / Social Science & Medicine 63 (2006) 165–178166
population health. There has thus been a tendencywithin the literature on cross-national variations inpopulation health to neglect the importance ofsystemic-level factors on national-level health,thereby treating nations as individual actors auton-omous from broader global contexts.
Contradicting this model and the assumption thatnations are independent and relatively equal actorsin the global system, this study demonstrates theeffects of world-system role and global stratificationon infant mortality rates. We argue that populationhealth is not simply a reflection of national-levelfactors but must be understood contextually as aproduct of the differential positions that countrieshave in the global system. Our approach builds on aworld-systems framework to understand, measure,and assess the effects of global stratification andhierarchical trading structures on population health.This conception of global contexts is based on astructural instead of a geographical understandingof contexts. In this case, world-system role refers tothe structural position that nations have within aglobal pattern of trade relations; the concept ofglobal stratification refers to the inequalities anddependencies that ensue from countries beingdifferentially located within this global pattern. Byassessing cross-national variations in infant mortal-ity through such a lens, we demonstrate the utility inthinking about systemic influences on populationhealth and studying how global trade affectspopulation health.
Despite the potential strength of political econo-my approaches for studying global stratification andhealth, such approaches have yet to be fullyappreciated within the health sciences literature.When such approaches have been applied, they haveraised critical attention to the effects of macro-levelsocial factors on national-, community-, and in-dividual-level health (Baer, Singer, & Susser, 2003).We see the application of a political economyapproach as providing a conceptual framework inwhich the linkages between global-level factors andpopulation health can be identified and measured.While national-level economic, social, and politicalfactors have significant effects on population health,our analysis focuses primarily on the global leveland the effects of trade on health.
Background
At the expense of macro-level factors, currentcross-national research on population health has
tended to focus on the effects of national-levelfactors such as income distribution, strength oflabor, or social capital on population health (cf.Kawachi & Kennedy, 2002; Kennelly, O’Shea, &Garvey, 2003; Macinko, Shi, & Starfield, 2004;Wilkinson, 2002, 1996). Such analyses commonlytreat nation-states as if they are equal with regard topower and influence in the global system. If adistinction is made among countries, it is frequentlyexpressed in terms of a ‘‘high/low income’’ divisionbased on national Gross Domestic Product percapita (GDP/c). For example, Wilkinson divideshigh- and low-income countries at $5000 annualGDP/c (Wilkinson, 1996).
For present purposes, we identify two limitationsin current cross-national studies on populationhealth. First, based as they are on a single attributeof a country, GDP/c, the ‘‘high/low income’’typology does not capture the overall structure ofinternational relationships through which globalinequalities emerge. We argue that an income-basedtypology is unidimensional and limited in itscapacity to measure power and global stratification.Second, cross-national studies tend to focus oneither high- or low-income countries, therebyremoving from analysis the broader global contextin which high- and low-income status develops.Instead, we suggest that a critical conceptualizationof the global system rooted in the study ofinternational trade and global stratification leadsto a fuller understanding of cross-national varia-tions in population health and the potential inter-action between global contexts and nationalinstitutions and policies.
World-systems perspectives
Central to world-systems perspectives is a con-ception of the global system as consisting of‘‘intersocietal networks in which the interactions(e.g., trade, warfare) are important for the repro-duction of the internal structures of the compositeunits (e.g., nation-states)’’ (Chase-Dunn & Hall,1993, p. 855). Within these inter-societal networks,three structural positions can be identified: core,periphery, and semi-periphery (Wallerstein, 1974).The core is seen as being rich and economicallydiversified, having powerful and strong state in-stitutions, and independent of external controls; theperiphery is economically overspecialized, moredependent on foreign capital, and subject toexploitation and control by core states (Hall, 1996;

ARTICLE IN PRESSS. Moore et al. / Social Science & Medicine 63 (2006) 165–178 167
Wallerstein, 1974); the semi-periphery rests midwaybetween the core and periphery on a series ofdimensions including the complexity and diversityof economic activities and strength of state institu-tions (Hall, 1996; Van Rossem, 1996; Wallerstein,1974). These zones are linked to one another invarious asymmetric exchange relationships throughwhich a global division of labor and a hierarchicalsystem of political, economic, and cultural relationsemerge.
While nation-states may within certain limitschange zones within the system, the hierarchicalcore/periphery structure of the system remains.Peripheral states remain in a structurally dependentrelationship that perpetuates their subordinateposition to the core (Hall, 1996). The world-systemroles, or strata, thus reflect underlying global powerrelations that structure the opportunities for thosestrata. A country’s role is more than a product of itsGDP, it is a measure of its interaction within anoverall hierarchy of relationships. The particularcharacteristics of nation-states are seen as influ-enced by the role that those states play in thishierarchical structure (Smith & White, 1992; Snyder& Kick, 1979). For example, changes in nationallevels of economic development and the degree ofinequality within countries have been suggested tobe a product of a state’s position in the worldsystem (London & Smith, 1988; Snyder & Kick,1979). In other words, cross-national variations areto be understood contextually, as the historicalproduct of the complex interaction of local societieswith an expanding world system (Chase-Dunn &Grimes, 1995). The focus is thus on the interactionsamong the different zones of the system, rather thanthe nation-state itself. These interactions affect theinternal dynamics and social structures of nation-states (Hall, 1996).
Political economy and world-systems perspec-tives, although underrepresented in cross-nationalstudies of population health, have found limitedempirical application in the health sciences litera-ture (Dyches & Rushing, 1996, 1993; Elling, 1994;Lena & London, 1993). For example, Dyches andRushing (1996) argue that the status of women’shealth must be understood within the context ofinternational stratification and the global division oflabor; Elling (1994) argues that the cross-nationalstudy of health systems requires those nationalhealth systems to be understood in relation to theirposition in the ‘‘capitalist political economic worldsystem.’’ World-system perspectives have also been
applied to the study of infant mortality (cf., Lena &London, 1993; Shandra et al., 2004).
In terms of our current analysis, however, earlierapplications have been incomplete in several ways.First, those studies have yet to examine the directeffects of world-system role on infant mortalityrates. For example, Shandra et al. (2004) use a non-core/peripheral country typology based on the workof Snyder and Kick (1979) to examine if economicand sociopolitical factors have unique effects innon-core as compared to core countries. While thisis a useful method to examine if different dynamicsexist in the two groups, it does not specificallyaddress the question of the overall effects of world-system role on infant mortality. Second, previousstudies have relied on world-system position mea-sures that originate from 1960s international tradedata (Bollen, 1983; Snyder & Kick, 1979). Whilesuch measures are well-established, they do notreflect the geopolitical changes that have occurredsince the 1960s. Finally, previous world-systemposition measures in the health literature have beenbased on a structural rather than an automorphicmeasure of equivalence. Structural equivalencemeasures have been shown to conflate geographicalproximity with a country’s role in the system(Borgatti & Everett, 1992; Smith & White, 1992;Van Rossem, 1996). The world-system positionmeasures that we develop are based on recent2000 international trade data and an automorphicequivalence measure, and thus provide a more up-to-date and accurate picture of global stratification.
Methods
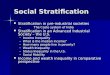
Fig. 1 illustrates the conceptual model underlyingour analysis. To examine if world-system perspec-tives contribute to our understanding of the effectsof the global system on population health, wecombine network and ordinary least squares (OLS)regression methods. First, our study employsestablished network analysis procedures to assigncountries to specific roles in the world system. Theseassignments derive from blockmodeling techniquesusing circa 2000 international trade data. Afterassigning countries to these roles, we use OLSregression to test the effects of world-system role oninfant mortality rates while controlling for national-level socioeconomic and geographical factors.Although we recognize possible reciprocal effectsoccurring between global- and national-level fac-tors, our analysis and discussion focuses primarily

ARTICLE IN PRESS
Global-Level Context National-Level Variables Population Health
World-System Role
Core 2Semi-Periphery 1Semi-Periphery 2Periphery 1Periphery 2
Economic, Social, Political Factors
GDP per capitaAid per capitaTrade as percentage of GDPFemale Literacy RatesVoice and AccountabilityPolitical Stability
Population Health Outcome
Infant Mortality Rates
Geographical Control Variables
Tropical CountryLandlocked Country
Fig. 1. Conceptual model of world-system effects on IMR.
S. Moore et al. / Social Science & Medicine 63 (2006) 165–178168
on the effects of world-system role on populationhealth.
Network analysis
Network data
International trade data were collected from theUnited Nations Commodity Exchange Database(United Nations Statistics Division, 2004), whichcontains over 40 years of trade data on over 1000commodities. These data follow the StandardInternational Trade Classification (SITC), whichorganizes commodity items into diverse commoditygroupings. Such data are frequently used to measureworld-system position (Breiger, 1982; Nemeth &Smith, 1985). Although some studies supplementtrade data with political or cultural ties amongcountries (Snyder & Kick, 1979; Van Rossem,1996), we collected international trade data exclu-sively on four capital-intensive, production-basedcommodities. Our choice of commodities is basedon a factor analysis of international commoditytrading from 1965–1980 (Smith & Nemeth, 1988).1
1Smith and Nemeth (1988) identify five factors—(1) hi-tech/
heavy manufacture, (2) low-wage/light manufacture, (3) sophis-
ticated extracted, (4) simple extractive, and (5) food products—
We collected national trade data on the fourcommodities having the highest loadings on thehi-tech and heavy-manufacturing factor. Thosecommodities were (1) non-electrical machinery(SITC ]71), (2) plastics and synthetics (SITC ]58),(3) transportation equipment (SITC ]71), and (4)metal manufactures (SITC ]69). Compared to thefour other factors in the Smith & Nemeth analysis,the hi-tech/heavy-manufacturing factor representscapital-intensive, production-based commodities(Smith & Nemeth, 1988). Since commodities fallinginto this factor are capital-intensive, the use of theseparticular commodities to measure global tradestructures incorporates certain dimensions of na-tional economic development beyond GDP/c andprovides arguably a better measure of globalstratification than the other factors.
Trade data for the year 2000 were sought for allnations with a population over one million. Tomaximize available trade data, we used a two-yearreporting window around 2000. If there were nodata available for a nation in 2000, we sought datafor that country in 1999. If no data were reported
(footnote continued)
located along a capital—labor-intensive and production—extrac-
tion-based scale.

ARTICLE IN PRESSS. Moore et al. / Social Science & Medicine 63 (2006) 165–178 169
for a country in 2000 or 1999, we sought exchangedata for 1998, followed by 2001. In total, weobtained data on the trade of hi-tech and heavymanufacture commodities for 128 countries: 117 for2000, six for 1999, four for 2000, and one for 1998.We used these data to construct a network data set,which consists of an n� n matrix X, where n equalsthe number of countries in the analysis (128� 128).Each cell in the non-valued data matrix, Xij, recordssimply the occurrence or non-occurrence of tradebetween countries i and j, and not the specific valueof the trade. Since the data revealed differencesamong countries between import and export ties,the X matrix was asymmetrical, meaning that somecountries might import but not export (or viceversa) to another country.
Blockmodeling techniques
Blockmodeling can be seen as both an approachto the analysis of network data in which theore-tical importance is given to the concept of socialroles and positions and a set of analytic proce-dures to delineate those roles within a socialnetwork (Doreian, Batagelj, & Ferligoj, 2005). Ablockmodel consists of a matrix that describesthe ties among the different roles and a descrip-tion of which actors, e.g., countries, are assigned towhich roles (White, Boorman, & Brieger, 1976;Wasserman & Faust, 1994). To identify specificnational roles within the global system, we applyblockmodeling techniques to the network tradedata. Those techniques involve: (1) the derivationof automorphic equivalence measures for eachcountry–country relationship, (2) the use of corre-spondence analysis to represent graphically thedegree of automorphic equivalence among coun-tries and begin assignment of national roles, (3) theapplication of a hierarchical clustering procedureto refine assigned country roles, and (4) testingthe reliability of the blockmodel against core–periphery blockmodel structures. Although weemploy certain methodological variations, ourgeneral approach replicates established proceduresfor conducting positional network analyses anddelineating world-system roles (Smith & Nemeth,1988; Smith & White, 1992; Van Rossem, 1996;Wasserman & Faust, 1994). In contrast to earlierwork, however, we (1) update national role assign-ments using international trade data circa 2000,(2) apply an automorphic equivalence measurethat reduces the conflation of geographical proxi-mity with role structures, and (3) assign world-
system role according to the internationaltrade in capital-intensive, production-based com-modities.
In contrast to structural equivalence, whichmeasures role similarity based on actors’ ties tothe same specific actors, automorphic equivalencemeasures role according to how comparable actors’ties are in a network (Borgatti & Everett, 1992; VanRossem, 1996). For example, to be consideredequivalent, Honduras and Moldova do not bothneed to trade with the United States (although theymight), they both only need to trade with countriesthat themselves have similar roles in the network,i.e., Honduras may trade with the US and Moldovawith Germany. We used the MAXSIM algorithm inthe network analysis software package UCINET(Borgatti, Everett, & Freeman, 2002) to measure themaximal (dis)similarity of the 128 countries. Theresult was a symmetrical matrix Z in which thevalue in each cell, Zij, equals the degree ofautomorphic equivalence between countries i and j
(Zij ¼ Zji).A correspondence analysis was then conducted
on the resulting automorphic equivalence matrix.The analysis converts a matrix of data into agraphical representation such that its rows andcolumns are depicted as points in a space (Gatrell,Popay, & Thomas, 2004; Salisbury & Barnett, 1999;van der Heijden & de Leeuw, 1989). Points that liecloser together in space have a higher degree ofautomorphic equivalence. Since the equivalencematrix was symmetrical, the analysis results in anidentical set of coordinates for the rows andcolumns (Salisbury & Barnett, 1999). The graphicaldisplay was visually examined for distinct clusters ofpoints, i.e., countries. Based on the visual inspec-tion, we classified countries into different rolesaccording to the world-system division of core,semi-peripheral, and peripheral zones.
To refine the groupings derived from visualinspection, we complemented the correspondenceanalysis with a hierarchical clustering procedure.We used the Johnson complete-link algorithm onthe automorphic equivalence matrix to clustercountries with similar patterns of trade. Thealgorithm begins with each country as its owncluster (identity partition) and then joins pairs ofcountries together that are considered most similar.It continues to join together pairs until all countriesare a single cluster (the complete partition). Theclustering procedure indicates the degree of similar-ity among countries at different levels of association

ARTICLE IN PRESSS. Moore et al. / Social Science & Medicine 63 (2006) 165–178170
(Borgatti et al., 2002). We used the number ofgroupings found in the correspondence analysis toestablish the significant level of association in thepartition. For example, if visual inspection of thecorrespondence analysis revealed six groupings, weset the level of association at six partitions higherthan the identity partition. This level was used asthe ‘‘cutoff point.’’ If a country was found clusteredbelow that level with a different block of countriesthan suggested by the correspondence analysis, wereassigned that country into the role indicated bythe hierarchical clustering procedure.
The final step in our blockmodeling procedureswas to test our blockmodel against previousspecifications of core–periphery blockmodel struc-tures (Breiger, 1982; Snyder & Kick, 1979; Wasser-man & Faust, 1994). A central concept inblockmodel analyses is density, which refers to thedegree of interconnectivity among actors in anetwork. Density is a proportional measure of thenumber of ties present in a network over the numberof all possible ties in the network. A networkcharacterized by perfect density means that eachactor is connected to all other actors in the network.In terms of core–periphery specifications, core areasare characterized by high internal density whereasperipheral areas tend to maintain lower internaldensities (Wasserman & Faust, 1994). In world-system terms, core areas have a high level ofhorizontal and vertical exchange ties, i.e., they tendto be well-connected to core and non-core countries.Peripheral areas are better characterized by verticalexchange. In other words, peripheral nations tend toexchange with core countries rather than maintain-ing a high density of exchange with other peripheralcountries (Chase-Dunn & Hall, 1993).
For the blockmodels to compare reliably withworld-systems theory, intra-block trading, i.e.,the horizontal ties among members of specificblocks, should be the most dense in core 1 anddecrease steadily toward the periphery (Wasserman& Faust, 1994). The block with the least intra-blockdensity should be the periphery, which wouldrepresent the relative lack of exchange of hi-techand heavy manufactures among peripheral na-tions. In addition, the core should have the highestinter-block density of trade with the other blocks,thereby showing the strength of its vertical tieswith other world-system areas. The peripheryshould have the lowest overall inter-block densityof trade, but its inter-block ties should be thehighest with the core.
OLS regression analysis
Using the roles assigned, the OLS regressionanalysis tests the direct effects of world-systems roleon infant mortality rates. We build two models: (1)the control model in which we regress infantmortality rates on six national-level socioeconomicand two geographical variables, and (2) the testmodel in which we add world-system role alongwith any significant interaction variables to model 1.In addition to examining the significance of specificworld-system roles, we use an incremental F-test todetermine if the overall R2 change between models 1and 2 is significant, thereby indicating the signifi-cance of world-system role itself as a predictor ofinfant mortality rates. Several regression diagnosticprocedures were used to test for the presence ofoutliers and influential cases, multicollinearity, andheteroscedasticity (Fox, 1991).
Data and measurement
Dependent variable. Infant mortality rates: Infantmortality is seen as a sensitive mortality indicatorthat is in general highly correlated with overallmortality rate (Wahdan, 1996) and one of the bestindicators of a nation’s overall health status (Shen &Williamson, 2001). While other indicators of na-tional health status may reflect a latency periodbetween the indicator and earlier social conditions,infant mortality rates are commonly assumed toreflect present conditions (Coburn, 2004).Infant mortality rates were obtained from the United
Nations Development Programme and are from 2001(UNDP, 2004). Infant mortality rates represent theprobability of dying between birth and one year ofage, expressed per 1000 live births. Following previousapplications of infant mortality rates as a dependentvariable, we logged the national infant mortality ratesto reduce the potential problem of heteroscedasticity(Shandra et al., 2004).
Independent variables. World-system role: To testthe effects of world-system role on infant mortalityrates, we dummy-code countries into the previouslyassigned roles. We exclude the core 1 role from theregression as reference.
National-level economic variables
Economic development
Using World Bank data (2004), we measureeconomic development based on a country’s GDP/c

ARTICLE IN PRESS
2There are countries with a percentage greater than 100 in all
six blocks. For example, the Netherlands found in core 1 has a
value of 111, while Moldova, a periphery 2 country, has a value
of 122.
S. Moore et al. / Social Science & Medicine 63 (2006) 165–178 171
adjusted for Purchasing Power Parity (PPP) values.GDP/c has been shown to be a significant predictorof infant mortality rates (Bradshaw & Tshandu,1990; Frey & Field, 2000; Lena & London, 1993;Shandra et al., 2004; Shen & Williamson, 2001).To reduce the effect of incidental transactions ofunusual size (cf. Kim & Shin, 2002), we averaged acountry’s reported GDP/c figures from 1991–2000.As is standard in such analyses, the GDP/cvariable was logged to correct for its highly skeweddistribution (Frey & Field, 2000; Lena & London,1993; Shandra et al., 2004; Shen & Williamson,2001).
Economic dependency
In contrast to relational data, dependency per-spectives tend to use national attribute data tomeasure specific two-way relationships betweencountries, countries and a corporation, or countriesand international lending agencies (van Rossem,1996). Economic dependency measures have beenshown to have indirect effects on infant mortalityand act as potentially significant intervening vari-ables affecting child mortality (Bradshaw, Noonan,Gash, & Sershen, 1993), infant mortality (Wimber-ley, 1990), infant survival (Shen & Williamson,2001), and life expectancy (Wimberley, 1990). Weuse two measures of economic dependency: (i) aiddependency and (ii) trade market dependency. Datafor both come from the World Bank, and representan average value for each country from 1991–2001.Aid dependency was measured using national levelsof aid per capita. Aid per capita is seen to capturethe degree to which countries are dependent onextra-territorial capital and financing to ensure aminimal functioning of the national system. Theadverse effects of aid dependency on national healthoutcomes have been linked to such factors as (1)reduced governmental financial capacities to spendin the social, educational, and health fields and (2)reduced flexibility in responding to economic orsocial crises (Shen & Williamson, 1997).
Trade market dependency was operationalized asthe ratio of gross trade flows (merchandise importsand exports) to national GDP. The variablerepresents the importance of trade to the nationaleconomy and a country’s level of exposure to theinternational economy (Frey & Field, 2000; Shen &Williamson, 1997; Van Rossem, 1996; World Bank,2005). Since the measure is based on gross flows(value of exports plus imports) rather than net flows(value of exports minus imports), countries may
have a gross-trade flows to GDP ratio greater than100.2 Trade market dependency has been linked tospecific national health outcomes through thereduced capacity of governments to raise revenuesand to spend in the social, educational, and healthfields (Shen & Williamson, 1997).
National-level sociopolitical variables
Female educational status
Gender stratification theory argues that genderequality and female education reduces infantmortality (Frey & Field, 2000). To operationalizethe effects of female education, we use femaleliteracy rates. Female literacy is based on thereported literacy of women over the age of 15during the 1990s. Female literacy rates werecollected from the World Bank and supplementedwith data from UNDP and the United NationsEducational, Scientific, and Cultural Organization(UNESCO, 2004).
Political democracy
Political democracy has been associated withhigher population health status (Lena & London,1993). Previous studies have relied on Bollen’s(1983) index of political democracy to measurenational levels of political democracy. As analternative indicator of political democracy, we useWorld Bank Governance indicators of ‘‘Voice andAccountability.’’ The measure reflects the processesby which national authorities are selected andreplaced, and thus the extent to which a country’scitizens are able to participate in selecting theirpolitical representatives (Kaufmann, Kray, & Mas-truzzi, 2003). These measures are based on theperceptions of over 18 different organizations andderived from a country’s relative score compared toother nations in the sample (Kaufmann et al., 2003).World Bank governance indicators are relativelyrecent and, as a result, we average estimates onlyfrom 1996 to 2000.
Political stability
Political stability has been used in previousstudies to examine its role in the deterrence orfacilitation of foreign direct investment in countries

ARTICLE IN PRESS
3Follow-up tests revealed that the reassignment of country
roles had no significant effect on final regression results. Variables
that were significant remained so after testing for changes due to
hierarchical clustering reassignment.
S. Moore et al. / Social Science & Medicine 63 (2006) 165–178172
(Bandelj, 2002; London & Ross, 1995). We used themeasure of political stability found in the WorldBank governance indicators to capture the per-ceived likelihood that the government in power willbe destabilized or overthrown in the near future(Kaufmann et al., 2003).
Control variables
Geographical context
Recent macro-economic studies of global povertyand national development have highlighted theimportance of geographical and ecological factorsinfluencing economic growth and disease prevalence(Gallup & Sachs, 1999; Sachs, 2005). Such analyseshave stressed the disadvantages in economic devel-opment that (1) tropical countries experiencerelative to temperate countries due potentially tohigher disease burdens and limitations on agricul-tural productivity, and (2) landlocked countrieshave compared to coastal regions because of hightransport costs associated with trade (Gallup &Sachs, 1999; Sachs, 2005). To control for thepossible effects of geographical context in ourmodels, we included two variables: (1) a dummyvariable representing whether a country was land-locked, and (2) a dummy variable representing if acountry was located in the tropics. A tropicalcountry is defined as being located between theTropics of Cancer and Capricorn. Data for both aredrawn from the Center for International Develop-ment, Harvard University (Gallup & Sachs, 1999).
Results
Network analysis
Blockmodeling
The correspondence analysis has a flat U-shape(Fig. 2). Moving right to left along the curve, onemoves along a continuum from core to periphery.Visual inspection reveals six distinct groupings,which are labeled core 1, core 2, semi-periphery 1,semi-periphery 2, periphery 1, and periphery 2. Thisfinding conforms with other analyses that havefound subgroups among the three world-systemzones (c.f. Smith & White, 1992).
Based on the hierarchical clustering procedure,the significant level of association in the partitionwas set at 141.99. Using this partition level as the‘‘cut-off,’’ we changed the role of countries thatwere found associated below this level with a
different block of countries than suggested by thecorrespondence analysis. To refine the assignedcountry roles, we thus changed the position ofseven countries: Norway and South Korea wererepositioned from core 2 to core 1; Croatia wasrepositioned from semi-periphery 2 to semi-periph-ery 1; Egypt was repositioned from semi-periphery 1to semi-periphery 2; and, Cuba, Ecuador, andHonduras were repositioned from periphery 1 toperiphery 2.3
In total, 128 countries were classified into one ofsix mutually exclusive blocks. Table 1 lists countriesby world-system role assignment. There were 21nations placed in core one; 11 in core 2; 17 in semi-periphery 1; 17 in semi-periphery 2; 10 in periphery1; and 52 in periphery 2.
Blockmodel reliability testing
Table 2 shows the intra- and inter-block densityof ties within and among the six blocks. The intra-block density is shown on the diagonal of thematrix. For example, the intra-block density forcore 1 is 1.0, thereby representing a completelydense network. In other words, each nation in core 1exchanges hi-tech and heavy manufacture commod-ities with each of the other nations in core 1.Moving from the core to the periphery, we observe adecrease in intra-block density values. There is anoticeable decrease in the move from semi-periph-ery 1 to semi-periphery 2, from .938 to .460. Whilesemi-periphery 1 countries are relatively well-con-nected to one another in terms of the trade ofcapital-intensive commodities, trade-tie densityamong semi-periphery 2 countries is slightly underone half of that among semi-periphery 1 countries.The intra-block density among periphery 2 coun-tries is the lowest among all blocks at 10%,demonstrating that periphery 2 countries do notmaintain dense trade ties in such commodities withother periphery 2 countries.
Results show that the core has the highest densityof export (rows) and import (columns) trade withother blocks in the system. The inter-block densityvalues show that the periphery trades primarily withthe core. Results also demonstrate that the periph-ery has a higher density of import than export tieswith the core. Intra- and inter-block density values

ARTICLE IN PRESS
Fig. 2. Correspondence analysis with assigned world-system roles.
S. Moore et al. / Social Science & Medicine 63 (2006) 165–178 173
thus conform to previous specifications of core–per-iphery blockmodel structures (Breiger, 1982; Snyder& Kick, 1979; Wasserman & Faust, 1994).
Regression analysis
For the purpose of the regression analysis,countries with missing cases for any of the variableswere dropped from the sample.4 The final numberof countries in the sample was 116. The countrieswere dummy-coded into six roles: core 1 (reference),core 2, semi-periphery 1, semi-periphery 2, periph-ery 1, and periphery 2.
Regression diagnostics
Outlier analysis using studentized residuals andhat values (Freund & Littell, 2000; Neter, Kutner,Nachtsheim, & Wasserman, 1996) detected thepresence of six outliers. To identify any influentialcases in our sample, we used Cook’s D, Dffits, andDfbetas (Neter et al., 1996). Ten cases were signaledby the diagnostics. As a result, outlying andinfluential cases were analyzed and then checkedfor any possible data inaccuracies. Secondly, wefollowed conventional procedures to rerun theregression models omitting different combinationsof outlying and influential cases while checking for
4Countries dropped were Azerbaijan, Bhutan, Cuba, Czech
Republic, Gabon, Georgia, Guinea, Kyrgyz Republic, Libya,
Macedonia, Serbia and Montenegro, and Singapore.
changes in the parameter estimates and significancelevels (Bollen & Appold, 1993; Freund & Littell,2000; Neter et al., 1996). One country (SouthAfrica) influenced the significance level of the core2, i.e., when model 2 is run without this case, core 2is no longer significant. The observation scoredamong the highest in Dffits and Cook’s D statistics.South Africa is considered a core 2 country, but ithas an infant mortality rate that is markedly higherthan the remaining core 2 countries, i.e., SouthAfrica has an IMR of 56 although the averageinfant mortality rate for other core 2 countries is15.22. Given these findings, the decision was madeto suppress this case, leaving the final sample size at115 (Table 3).
To detect potential problems of multicollinearity,we used Variance Inflation Factors (VIF) andanalyzed the structure of the X0X matrix, neitherof which revealed evidence of multicollinearity(Freund & Littell, 2000; Neter et al., 1996). Theplot of residuals against estimates did not show thepresence of heteroscedasticity in the data.
OLS regression analysis
Table 4 provides the regression results. Model 1shows the significance of our control variables. Bothgeographical variables appear to be significantlyand positively associated with infant mortality,meaning tropical and landlocked countries tend tohave higher levels of infant mortality. As expected,GDP/c (�.542, po:001) and female literacy (�.002,

ARTICLE IN PRESS
Table 1
Nation-state roles based on exchange of capital-intensive, production-based commodities (n ¼ 116)
Core 1 (20) Semi-periphery 1 (17) Periphery 1 (8) Periphery 2 (cont’d)
Australia Argentina Kazakhstan Gambia
Austria Bulgaria Kenya Guatemala
Belgium Croatia Mauritius Honduras
Canada Hungary Namibia Jamaica
China Indonesia Senegal Lesotho
Denmark Iran Sri Lanka Madagascar
France Lebanon Trinidad and Tobago Malawi
Germany Luxembourg Zimbabwe Mali
India Mexico Moldova
Ireland New Zealand Mongolia
Italy Pakistan Nepal
Japan Philippines Nicaragua
Netherlands Poland Niger
Norway Romania Nigeria
Spain Slovakia Panama
South Korea Slovenia Papua New Guinea
Sweden Ukraine Paraguay
Switzerland Rwanda
United Kingdom Saudi Arabia
USA Sudan
Core 2 (10) Semi-Periphery 2 (16) Periphery 2 (45) Swaziland
Brazil Belarus Albania Syria
Finland Chile Algeria Tanzania
Greece Colombia Armenia Togo
Israel Costa Rica Bangladesh Turkmenistan
Malaysia Cote d’Ivoire Benin Uganda
Portugal Egypt Bolivia Uruguay
Russian Federation Estonia Botswana Viet Nam
South Africaa Jordan Burkina Faso Yemen
Thailand Kuwait Burundi Zambia
Turkey Latvia Cameroon
Lithuania Central African Rep.
Morocco Dominican Rep.
Oman Ecuador
Peru El Salvador
Tunisia Ethiopia
Venezuela
aSouth Africa was excluded from regression analyses based on regression diagnostic results.
Table 2
Average intra- and inter-block density of ties
Core 1
(n ¼ 20)
Core 2
(n ¼ 12)
Semi-peri 1
(n ¼ 17)
Semi-peri 2
(n ¼ 17)
Periphery 1
(n ¼ 10)
Periphery 2
(n ¼ 52)
Core 1 1.000 1.000 .994 1.000 1.000 .982
Core 2 1.000 .991 .968 .936 .936 .846
Semi-peri 1 .997 .963 .930 .886 .706 .555
Semi-peri 2 .961 .829 .592 .460 .353 .346
Periphery 1 .883 .464 .312 .300 .244 .219
Periphery 2 .469 .206 .107 .126 .102 .101
S. Moore et al. / Social Science & Medicine 63 (2006) 165–178174

ARTICLE IN PRESS
Table 3
World-system role descriptive statisticsa
W-S
role
Infant
mortality
rates
GDP/c
(PPP) $
Aid/c $ Trade/
%GDP
Female
literacy
rates
Voice and
accountability
estimates
Political
stability
estimates
Core 1 9.15 20,046 .13 65.36 95.16 1.14 1.03
Core 2 15.22 10,585 27.27 73.83 88.92 .47 .25
Semi 1 20.29 8928 15.66 82.38 88.59 .24 .25
Semi 2 24.06 6136 27.92 82.79 76.02 �.09 .19
Peri 1 50.0 3902 36.81 86.38 76.75 �.07 �.21
Peri 2 68.73 2398 38.69 69.02 58.70 �.40 �.29
aDescriptive statistics based on final sample size of 115.
Table 4
Unstandardized regression coefficients of infant mortality rates (log) on world-systems role and selected control variables for 116 countries
Model 1: control variables Model 2: world-system role
Constant 3.524��� (12.60) 3.393��� (11.61)Tropical climate .117�� (2.91) .096� (2.33)Landlocked country .136��� (3.35) .117�� (2.89)
GDP per capita (log) �.542��� (�7.81) �.494��� (�6.75)Aid per capita .001 (1.84) .000 (.98)
Trade % GDP (log) �.058 (�.67) �.113 (�1.29)
Female literacy �.002� (�2.55) �.002�� (�3.07)Voice and accountability �.120��� (�3.80) �.112��� (�3.54)Political stability .008 (.25) .041 (1.20)
Core 2 (n ¼ 9) .101 (1.33)
Semi-periphery 1 (n ¼ 17) .097 (1.56)
Semi-periphery 2 (n ¼ 16) .068 (1.00)
Periphery 1 (n ¼ 8) .257�� (2.89)Periphery 2 (n ¼ 45) .159� (2.11)Core 2 political stability� �.169� (�2.32)
R-Square .889 .902
Adjusted R-square .881 .889
F-change 2.211�
N 115 115
Note: The numbers in parenthesis are the t-values.�po:05.��po:01.���po:001.
S. Moore et al. / Social Science & Medicine 63 (2006) 165–178 175
po:05) act as significant variables influencing infantmortality. While the economic dependency variablesare not significant, the political democracy variableis (�.120, po:001). In other words, higher levels ofeconomic development, female literacy, and politi-cal democracy predict lower levels of infantmortality.
Model 2 tests the effects of world-system role oninfant mortality controlling for geographical andnational-level variables. Results indicate that per-ipheral roles within the world system are signifi-
cantly and positively associated with infantmortality (p1: .257, po:01; p2: .159, po:05). Thestronger effect found among periphery 1 comparedto periphery 2 countries may be due to the greaterimportance that trade has for periphery 1 econo-mies. In testing for interaction effects amongvariables, we found that the interaction bet-ween core 2 and political stability had a signifi-cant and negative effect on infant mortality rates.As political stability increases in core 2 countries,infant mortality rates decrease and vice versa. An

ARTICLE IN PRESSS. Moore et al. / Social Science & Medicine 63 (2006) 165–178176
incremental F test revealed that the R2 changebetween model 1 and 2 was significant (F(6,100) 2.21,po:05).
Discussion
At a time in which attention is turning to theeffects of geography and climate on health, ouranalysis highlights the sociopolitical and historicaldimensions of global disparities in health. Beingperipheral, unlike being tropical, reflects a histo-rical and social process of marginalization in whichcountries have been excluded and disempo-wered from more symmetrical trading relationships.Moreover, peripherality implies an ongoing socio-political process that weakens the capacity ofcountries to maintain sovereignty over their ownborders and the health of their populations. If, asour findings suggest, being peripheral affects popu-lation health in a way that being in the semi-periphery or core does not, trade and stratificationhave disproportionate effects on population healthdepending on the role countries play in the globalsystem. Rather than assuming then that economicglobalization or neoliberalist policies affect allcountries evenly, we suggest that economic globa-lization has different implications for peripheralthan it does for core or semi-peripheral countries.This is not only due to national-level variations inclass structure or the welfare state (Coburn, 2004)but to global-level variations in power and influ-ence. In this regard, we argue for a macro-levelunderstanding of economic globalization that viewsthe uneven effects of neo-liberalism at the nationallevel as influenced by asymmetric trading relation-ships at a global level.
Although we emphasize macro-level influenceson health, we recognize that global processes cannot account fully for intra-national socioecono-mic processes (Knoke, 1990). The effects ofnational-level factors on population health and thereciprocal effects occurring between global- andnational-level factors remain important areas ofresearch. Yet, global structures and processesshould be seen as setting the parameters fornational-level influences on health (Woodward,Drager, Beaglehole, & Lipson, 2001). Globalstructures and processes, such as internationaltrade, generate systems of stratification in whichcountries are differentially positioned. The multi-dimensional character of such strata may not besufficiently captured with a ‘‘high/low income’’
typology based on national GDP/c. Instead ofusing national attribute data to classify coun-tries, the use of relational trade data along withblockmodeling techniques allows us to generatealternative typologies and approaches to thestudy of global inequalities in health. In so doing,we draw attention to the effects of trade, power,and peripherality on global health. While a six-tiercore–periphery classification may only be aninitial step in that direction, it is one that helpsidentify the effects of peripherality on populationhealth.
Conclusion
While national-level factors play an importantrole in population health outcomes, such factorsoccur within particular global contexts. Thesecontexts are not the same for all countries.Depending on a country’s position in the system,globalization and trade may have disproportionateeffects on national institutions, policies, and health.As recent commentaries on trade and public healthhave argued, international trade agreements posechallenges to the sovereignty that national govern-ments have over public health policy (Shaffer,Waitzkin, Brenner, & Jasso-Aguilar, 2005). Forexample, World Trade Organization (WTO) agree-ments can supersede the internal laws and regula-tions of any WTO member country. In the event ofa trade dispute between member countries, thosecountries must comply with the decision of a WTOtribunal with regard to that dispute, or face either afinancial penalty or an authorized trade sanction bythe ‘‘winning’’ country (Shaffer et al., 2005).Powerful countries remain however at a consider-able advantage over less powerful ones in thedispute settlement process (Howse, 2004). Yet,power is not restricted to formal bilateral andmultilateral negotiation processes, it is an inte-gral feature of the global system. Peripheralcountries are structurally disempowered and maybe viewed as being at a higher level of vulnera-bility to the negative effects of globalization andtrade. As a result, there may be the need for greaterattention to the disproportionate effects of interna-tional trade on vulnerable countries and the furtherdevelopment of international agreements and reg-ulations that grant peripheral countries specialrights in developing and protecting their publichealth systems from the negative effects of globa-lization.

ARTICLE IN PRESSS. Moore et al. / Social Science & Medicine 63 (2006) 165–178 177
Acknowledgements
This work was supported through funding by theAlberta Heritage Foundation for Medical Research(AHFMR).
References
Baer, H., Singer, M., & Susser, I. (2003). Medical anthropology
and the world system (2nd ed.). Westport, Conn: Praeger
Paperback.
Bandelj, N. (2002). Embedded economies: Social relations as
determinants of foreign direct investment in Central and
Eastern Europe. Social Forces, 81(2), 411–444.
Bollen, K. (1983). World system position, dependency, and
democracy: The cross-national evidence. American Socio-
logical Review, 48(4), 468–479.
Bollen, K., & Appold, S. (1993). National industrial structure and
the global system. American Sociological Review, 58(2),
283–301.
Borgatti, S. P., & Everett, M. G. (1992). Notions of position in
social network analysis. Sociological Methodology, 22, 1–35.
Borgatti, S. P., Everett, M. G., & Freeman, L. (2002). UCINET 6
for Windows: Software for social network analysis. Harvard:
Analytic Technologies.
Bradshaw, Y. W., Noonan, R., Gash, L., & Sershen, C. B. (1993).
Borrowing against the future: Children and third world
indebtedness. Social Forces, 71(3), 629–656.
Bradshaw, Y. W., & Tshandu, Z. (1990). Foreign capital
penetration, state intervention, and development in Sub-
Saharan Africa. International Studies Quarterly, 34(2),
229–251.
Breiger, R. (1982). Structures of economic interdependence
among nations. In P. Blau, & R. Merton (Eds.), Continuities
in Structural Inquiry (pp. 353–380). Beverly Hills, CA: Sage.
Chase-Dunn, C., & Grimes, P. (1995). World-systems analysis.
Annual Review of Sociology, 21, 387–417.
Chase-Dunn, C., & Hall, T. D. (1993). Comparing world-
systems: Concepts and working hypotheses. Social Forces,
71(4), 851–886.
Coburn, D. (2000). Income inequality, social cohesion and the
health status of populations: The role of neo-liberalism. Social
Science & Medicine, 51, 135–146.
Coburn, D. (2004). Beyond the income inequality hypothesis:
Class, neo-liberalism, and health inequalities. Social Science
&Medicine, 58, 41–56.
Doreian, P., Batagelj, V., & Ferligoj, A. (2005). Generalized
blockmodeling. Cambridge: Cambridge University Press.
Dyches, H., & Rushing, B. (1993). The health status of women in
the world-system. International Journal of Health Services,
23(2), 359–371.
Dyches, H., & Rushing, B. (1996). International stratification and
the health of women: An empirical comparison of alternative
models of world-system position. Social Science & Medicine,
43(7), 1063–1072.
Elling, R. H. (1994). Theory and method for the cross-national
study of health systems. International Journal of Health
Services, 24(2), 285–309.
Fox, J. (1991). Regression diagnostics. Newbury Park, CA: Sage.
Freund, R. J., & Littell, R. C. (2000). SAS system for regression.
Cary, NC: SAS Institute Inc.
Frey, R. S., & Field, C. (2000). The determinants of infant
mortality in the less developed countries: A cross-national test
of five theories. Social Indicators Research, 52, 215–234.
Gallup, J., & Sachs, J. (1999). Geography and economic
development. Center for International Development, Harvard
University, Working Paper 1, http://www.cid.harvard.edu/
Gatrell, A., Popay, J., & Thomas, C. (2004). Mapping the
determinants of health inequalities in social space: Can
Bourdieu help us? Health & Place, 10, 245–257.
Hall, T. D. (1996). The world-system perspective. Sociological
Inquiry, 66(4), 440–454.
Howse, R. (2004). The WHO/WTO study on trade and public
health: A critical assessment. Risk Analysis, 24(2), 501–507.
Kaufmann, D., Kray, A., & Mastruzzi, M. (2003). Governance
matters III: Governance indicators for 1996– 2002. Washing-
ton, DC: The World Bank.
Kawachi, I., & Kennedy, B. (2002). The health of nations. New
York: New Press.
Kennelly, B., O’Shea, E., & Garvey, E. (2003). Social capital. life
expectancy and mortality: A cross-national examination.
Social Science & Medicine, 56, 2367–2377.
Kim, S., & Shin, E.-H. (2002). A longitudinal analysis of
globalization and regionalization in international trade: A
social network approach. Social Forces, 81(2), 445–468.
Knoke, D. (1990). Political networks. Cambridge: Cambridge
University Press.
Labonte, R., & Torgerson, R. (2002). Frameworks for analyzing
the links between globalization and health. Geneva: World
Health Organization (WHO) (p. 71).
Lena, H. F., & London, B. (1993). The Political economic
determinants of health outcomes: A cross-national analysis.
International Journal of Health Services, 23(3), 585–602.
London, B., & Ross, R. J. (1995). The political sociology of
foreign direct investment: Global capitalism and capital
mobility, 1965–1980. International Journal of Comparative
Sociology, 36(3–4), 198–218.
London, B., & Smith, D. A. (1988). Urban bias, dependence, and
economic stagnation in non-core nations. American Socio-
logical Review, 53, 454–463.
Macinko, J. A., Shi, L., & Starfield, B. (2004). Wage inequality,
the health system, and infant mortality in wealthy industria-
lized countries, 1970–1996. Social Science & Medicine, 58,
279–292.
Nemeth, R., & Smith, D. (1985). International trade and world-
system structure: a multiple network analysis. Review, 8,
517–560.
Neter, J., Kutner, M., Nachtsheim, C., & Wasserman, W. (1996).
Applied linear statistical models. Boston, MA: McGraw-Hill.
Sachs, J. (2005). The end of poverty. New York: The Penguin
Press.
Salisbury, J., & Barnett, G. (1999). The world system of
international monetary flows: A network analysis. The
Information Society, 15, 31–49.
Shaffer, E., Waitzkin, H., Brenner, J., & Jasso-Aguilar, R. (2005).
Global trade and health. American Journal of Public Health,
95, 23–34.
Shandra, J. M., Nobles, J., London, B., & Williamson, J. B.
(2004). Dependency, democracy, and infant mortality: A
quantitative, cross-national analysis of less developed coun-
tries. Social Science & Medicine, 59, 321–333.

ARTICLE IN PRESSS. Moore et al. / Social Science & Medicine 63 (2006) 165–178178
Shen, C., & Williamson, J. B. (1997). Child mortality, women’s
status, economic dependency, and state strength: A cross-
national study of less developed countries. Social Forces,
76(2), 667–694.
Shen, C., & Williamson, J. B. (2001). Accounting for cross-
national differences in infant mortality decline (1965–1991)
among less developed countries: Effects of women’s status,
economic dependency, and state strength. Social Indicators
Research, 53, 257–288.
Smith, D. A., & Nemeth, R. J. (1988). An empirical analysis of
commodity exchange in the international economy: 1965–80.
International Studies Quarterly, 32(2), 227–240.
Smith, D. A., & White, D. R. (1992). Structure and dynamics of
the global economy: Network analysis of international trade
1965–1980. Social Forces, 70(4), 857–893.
Snyder, D., & Kick, E. L. (1979). Structural position in the world
system and economic growth, 1955–1970: A multiple-network
analysis of transnational interactions. American Journal of
Sociology, 84(5), 1096–1126.
UNDP. (2004). United Nations Development Programme. http://
www.undp.org, Accessed March 2004.
UNESCO. (2004). United Nations Educational, Scientific, and
Cultural Organization. http://www.unesco.org, Accessed
March 2004.
United Nations Statistics Division. Commodity Trade Statistics
Database (COMTRADE). (2004). http://unstats.un.org/unsd/
comtrade, Accessed January 2004.
van der Heijden, P., & de Leeuw, J. (1989). Correspon-
dence analysis, with special attention to the analysis of panel
data and event history data. Sociological Methodology, 19,
43–87.
van Rossem, R. (1996). The world system paradigm as general
theory of development: A cross-national test. American
Sociological Review, 61(3), 508–527.
Wahdan, M. H. (1996). The epidemiological transition, World
Health Bulletin. Geneva: World Health Organization (WHO)
(pp. 8–20).
Wallerstein, I. (1974). The modern world system I. New York:
Academic Press, Inc.
Wasserman, S., & Faust, K. (1994). Social network analysis:
Methods and applications. Cambridge: Cambridge University
Press.
White, D. R., Boorman, S. A., & Breiger, R. (1976). Social
structure from multiple networks I: Blockmodels of roles and
positions. American Journal of Sociology, 81, 730–780.
Wilkinson, R. (1996). Unhealthy societies. New York: Routledge.
Wilkinson, R. (2002). Income inequality and population health.
British Medical Journal, 324(7343), 978.
Wimberley, D. W. (1990). Investment dependence and alternative
explanations of third world mortality: A cross-national study.
American Sociological Review, 55(1), 75–91.
Woodward, D., Drager, N., Beaglehole, R., & Lipson, D. (2001).
Globalization and health: a framework for analysis and action.
Bulletin of the World Health Organization, 79(9), 875–881.
World Bank. (2004). World Bank Development Indicators. http://
www.worldbank.org, Accessed March 2004.
World Bank. (2005). Integration with the global economy: World
Development Indicators, http://www.worldbank.org.