Embed Size (px)
Citation preview

This article was downloaded by: [Laurentian University]On: 03 November 2013, At: 23:14Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Health Communication:International PerspectivesPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/uhcm20
The Health Literacy Skills FrameworkLinda Squiers a , Susana Peinado a , Nancy Berkman a , VanessaBoudewyns a & Lauren McCormack aa RTI International , Research Triangle Park , North Carolina , USAPublished online: 03 Oct 2012.
To cite this article: Linda Squiers , Susana Peinado , Nancy Berkman , Vanessa Boudewyns &Lauren McCormack (2012) The Health Literacy Skills Framework, Journal of Health Communication:International Perspectives, 17:sup3, 30-54, DOI: 10.1080/10810730.2012.713442
To link to this article: http://dx.doi.org/10.1080/10810730.2012.713442
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. Taylor & Francis, our agents,and our licensors make no representations or warranties whatsoever as to the accuracy,completeness, or suitability for any purpose of the Content. Versions of published Taylor& Francis and Routledge Open articles and Taylor & Francis and Routledge Open Selectarticles posted to institutional or subject repositories or any other third-party website arewithout warranty from Taylor & Francis of any kind, either expressed or implied, including,but not limited to, warranties of merchantability, fitness for a particular purpose, or non-infringement. Any opinions and views expressed in this article are the opinions and viewsof the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy ofthe Content should not be relied upon and should be independently verified with primarysources of information. Taylor & Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Taylor & Francis and Routledge Open articles are normally published under a CreativeCommons Attribution License http://creativecommons.org/licenses/by/3.0/. However,authors may opt to publish under a Creative Commons Attribution-Non-Commercial
License http://creativecommons.org/licenses/by-nc/3.0/ Taylor & Francis and RoutledgeOpen Select articles are currently published under a license to publish, which is basedupon the Creative Commons Attribution-Non-Commercial No-Derivatives License, butallows for text and data mining of work. Authors also have the option of publishingan Open Select article under the Creative Commons Attribution License http://creativecommons.org/licenses/by/3.0/. It is essential that you check the license status of any given Open and OpenSelect article to confirm conditions of access and use.
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
Address correspondence to Linda Squiers, RTI International, 3040 Cornwallis Road, P.O. Box 12194, Research Triangle Park, NC 27709, USA. E-mail: [email protected]
30
Journal of Health Communication, 17:30–54, 2012Copyright © Taylor & Francis Group, LLCISSN: 1081-0730 print/1087-0415 onlineDOI: 10.1080/10810730.2012.713442
Articles
The Health Literacy Skills Framework
LINDA SQUIERS, SUSANA PEINADO, NANCY BERKMAN, VANESSA BOUDEWYNS, AND LAUREN McCORMACK
RTI International, Research Triangle Park, North Carolina, USA
Although there are a variety of models and frameworks that describe factors that are associated with health literacy skills, few illustrate the full pathway from development and moderators of health literacy skills, their application, and the outcomes that result all in one framework or model. This article introduces the Health Literacy Skills conceptual framework that does encompass this full continuum. To develop the framework, the authors reviewed and built upon existing health literacy frameworks. The Health Literacy Skills framework hypothesizes the relations between health literacy and health-related outcomes and depicts how health literacy functions at the level of the individual. The framework also reflects how factors external to the individual (e.g., family, setting, community, culture, and media) influence the constructs and relations represented in the framework. The framework is organized into 4 primary components: (a) factors that influence the development and use of health literacy skills; (b) health-related stimuli; (c) health literacy skills needed to comprehend the stimulus and perform the task; and (d) mediators between health literacy and health outcomes. Previous theoretical frameworks lend support to the proposed causal pathways it illustrates. The authors hope this conceptual framework can serve as a springboard for further discussion and advancement in operationalizing this complex construct. The Health Literacy Skills framework could also be used to guide the development of interventions to improve health literacy. Future research should be conducted to fully test the relations in the framework.
Health literacy is on the public health agenda. The goal to “improve the health literacy of the population” was included as an objective in Healthy People 2010 and 2020 Objectives. In 2004, the Institute of Medicine released Health Literacy: A Prescription to End Confusion, which recommended that “the Department of Health and Human Services and other government and private funders should support research leading to the development of causal models explaining the relationship among health literacy, the education system, the health system, and relevant social and cultural systems” (Nielsen-Bohlman, Panzer & Kindig, 2004, p. 55). The U.S. Department of Health and Human Services’ 2010 National Action Plan to Improve Health Literacy reinforces the need for conceptual advances in the field by calling for the development and implementation of health literacy
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

Health Literacy Skills Framework 31
interventions on the basis of theories and models, drawing from such related disciplines as communication, education, cognitive science, and medical sociology (p. 44).
Pleasant, McKinney, and Rickard (2011) indicated that there is a lack of true theoretical frameworks that explain health literacy. Theory should be the foundation for developing reliable and valid measures of health literacy, which will allow the field to better study and understand the role of health literacy in health behavior change. This lack of theory has caused researchers to define health literacy in many different ways (Peerson & Saunders, 2009) and, thus, studies vary significantly depending on the definition and measures used (DeWalt, Berkman, Sheridan, Lohr, & Pignone, 2004; Peerson & Saunders, 2009; Pignone, DeWalt, Sheridan, Berkman, & Lohr, 2005).
The absence of a common definition and understanding of health literacy may have slowed the field’s progress in developing measures and conducting solid methodological research. There are a variety of models and frameworks that describe factors associated with health literacy skills (Baker, 2006; Mancuso, 2008; Nutbeam, 2000; Paasche-Orlow & Wolf, 2007; von Wagner, Steptoe, Wolf & Wardle, 2009). A comprehensive health literacy theory or framework may spur more professional discussions to help lay the foundation for a new era of theory-driven research.
The majority of these frameworks illustrate the effects that health literacy has on health-related outcomes (Lee, Arozullah, & Cho, 2004; Manganello, 2008; Nutbeam, 2000; Paasche-Orlow & Wolf, 2007; Rootman et al., 2002; Schillenger, 2001; von Wagner et al., 2009). However, few illustrate the full continuum of relations among predictors, moderators, mediators, and outcomes of health literacy all in one theory or framework (Pleasant, 2011).
Purpose
The purpose of this article is to introduce a framework for conceptualizing health literacy that builds on existing theoretical frameworks. We undertake three activities in the article:
1. First, we review and synthesize the several existing theoretical frameworks for health literacy and describe their strengths and weaknesses.
2. Second, we describe how we have incorporated key concepts and constructs from existing frameworks to develop the Health Literacy Skills (HLS) conceptual framework.
3. Third, we suggest how the HLS conceptual framework could be further tested and used to guide future research, evaluation, and intervention development efforts.
Identifying Key Constructs: A Review of Theories on Health Literacy Skills
The Institute of Medicine (Nielsen-Bohlman et al., 2004) definition is pointed to most consistently and considers health literacy to represent a “constellation of skills” necessary to function effectively in the health care environment and act on health care information. These skills comprehensively include the ability to interpret documents and read and write prose (print literacy), use quantitative information (numeracy or quantitative literacy), and speak and listen effectively (oral literacy) (Berkman, Davis, & McCormack, 2010).
Not all theoretical frameworks of health literacy embrace the Institute of Medicine’s definition of health literacy as a skill or set of skills. For example, Sørensen and colleagues (2012) recently conducted a review of 17 definitions of health literacy
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
32 L. Squiers et al.
and developed a new definition that “captures the essence” of these definitions found in the literature. Sørensen and colleagues’ definition states the following:
Health literacy is linked to literacy and entails people’s knowledge, motivation, and competence to access, understand, appraise and apply health information in order to make judgments and take decisions in everyday life concerning healthcare, disease prevention, and health promotion to maintain or improve quality of life during the life course (Sørensen et al., 2012, p. 3).
Although their definition includes skills, it also includes concepts such as knowledge and motivation, which some researchers consider to be separate constructs from healthy literacy (Baker, 2006; Lee et al., 2004; Paasche-Orlow & Wolf, 2007; von Wagner et al., 2008). Because of this variation in conceptualizations and definitions of health literacy, we have limited our review of health literacy frameworks to those which focus on health literacy as a skill or set of skills.
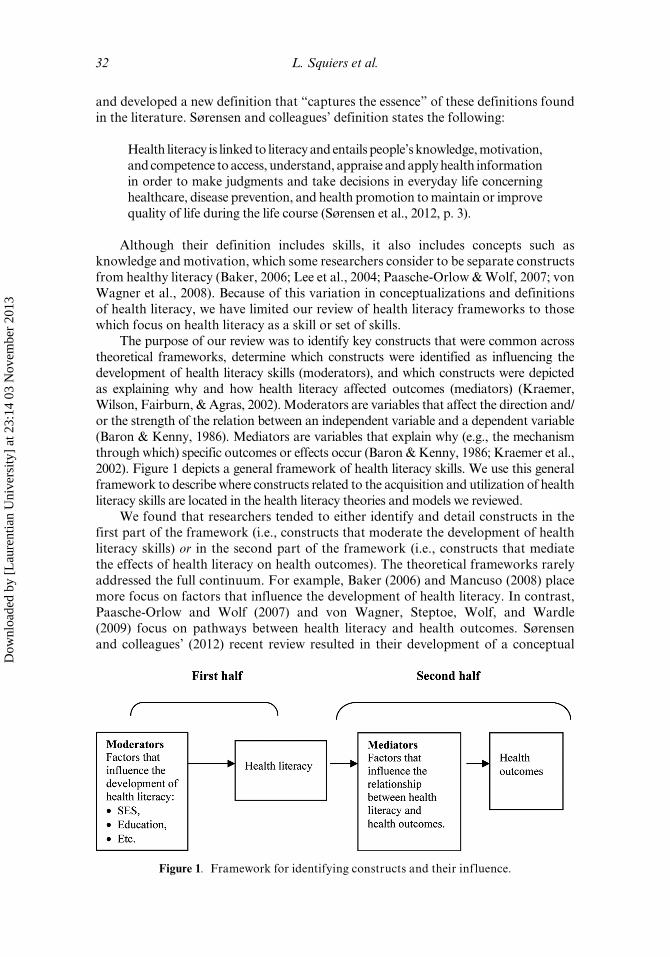
The purpose of our review was to identify key constructs that were common across theoretical frameworks, determine which constructs were identified as influencing the development of health literacy skills (moderators), and which constructs were depicted as explaining why and how health literacy affected outcomes (mediators) (Kraemer, Wilson, Fairburn, & Agras, 2002). Moderators are variables that affect the direction and/or the strength of the relation between an independent variable and a dependent variable (Baron & Kenny, 1986). Mediators are variables that explain why (e.g., the mechanism through which) specific outcomes or effects occur (Baron & Kenny, 1986; Kraemer et al., 2002). Figure 1 depicts a general framework of health literacy skills. We use this general framework to describe where constructs related to the acquisition and utilization of health literacy skills are located in the health literacy theories and models we reviewed.
We found that researchers tended to either identify and detail constructs in the first part of the framework (i.e., constructs that moderate the development of health literacy skills) or in the second part of the framework (i.e., constructs that mediate the effects of health literacy on health outcomes). The theoretical frameworks rarely addressed the full continuum. For example, Baker (2006) and Mancuso (2008) place more focus on factors that influence the development of health literacy. In contrast, Paasche-Orlow and Wolf (2007) and von Wagner, Steptoe, Wolf, and Wardle (2009) focus on pathways between health literacy and health outcomes. Sørensen and colleagues’ (2012) recent review resulted in their development of a conceptual
Figure 1. Framework for identifying constructs and their influence.
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

Health Literacy Skills Framework 33
framework that acknowledges some general categories of determinants of health literacy (e.g., society, environmental, personal, and situational) and general pathways between health literacy and population level outcomes; however, it does not specify concepts that mediate the relation between health literacy and outcomes.
Specific Concepts Presented in Theories on Health Literacy Skills
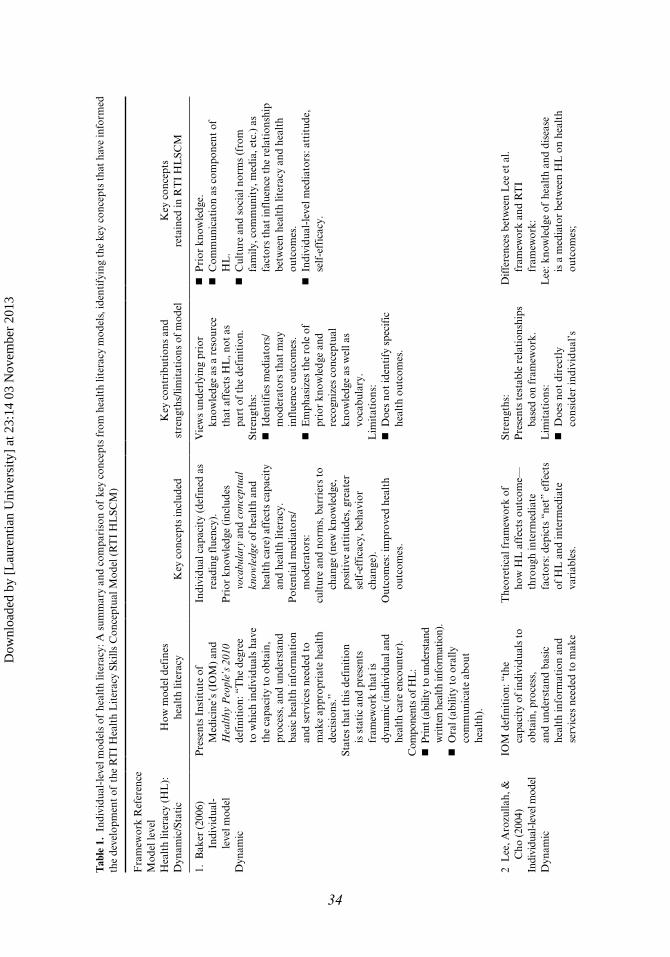
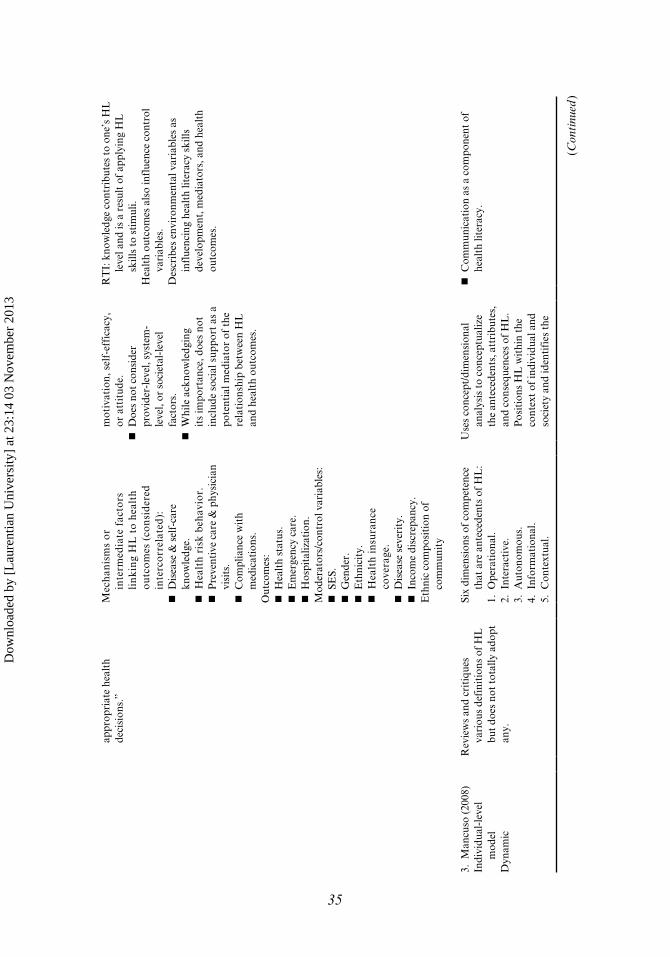
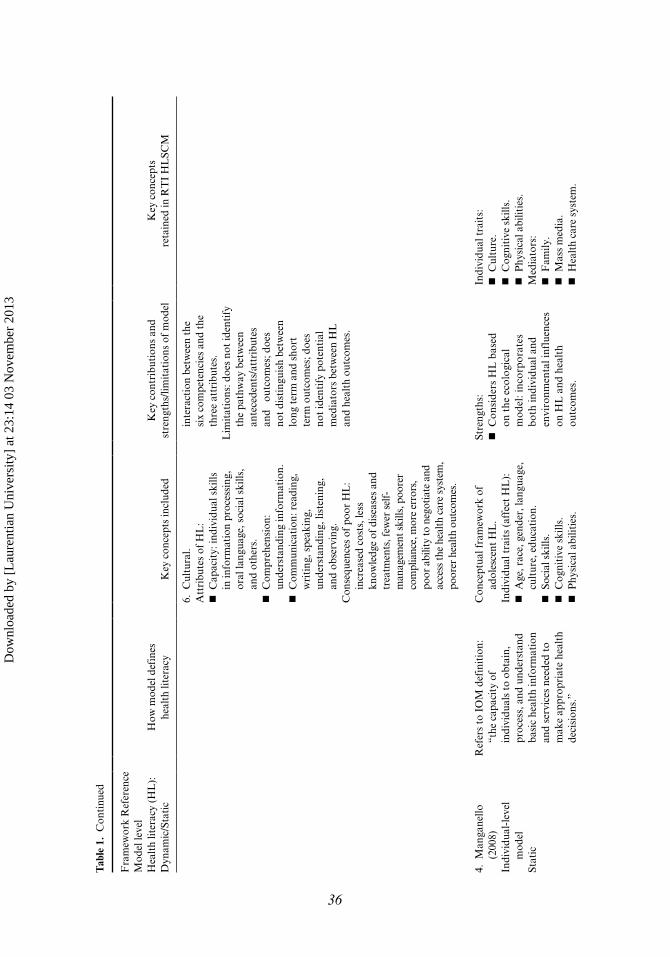
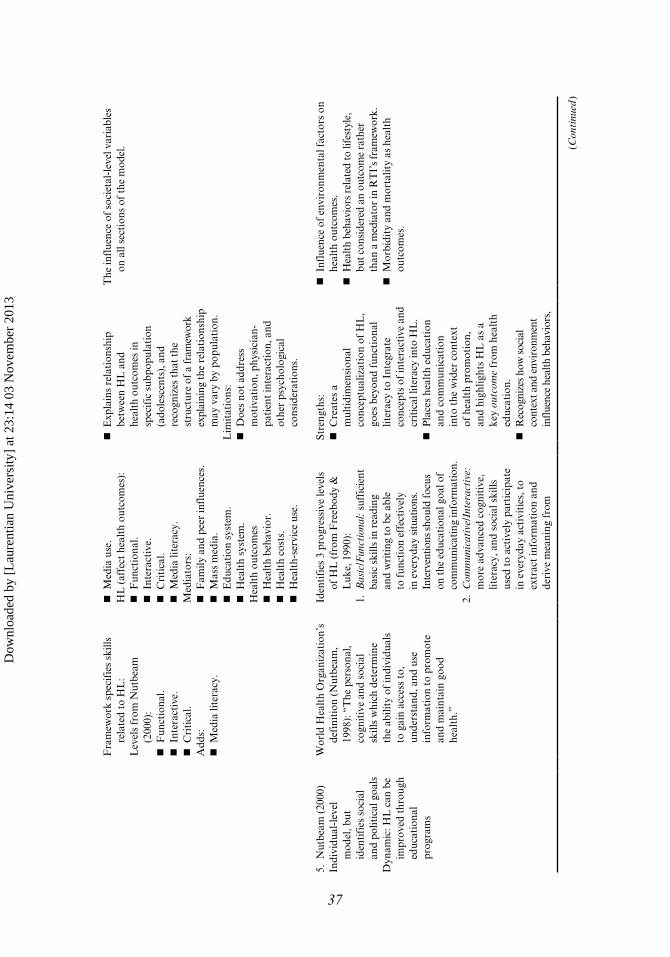
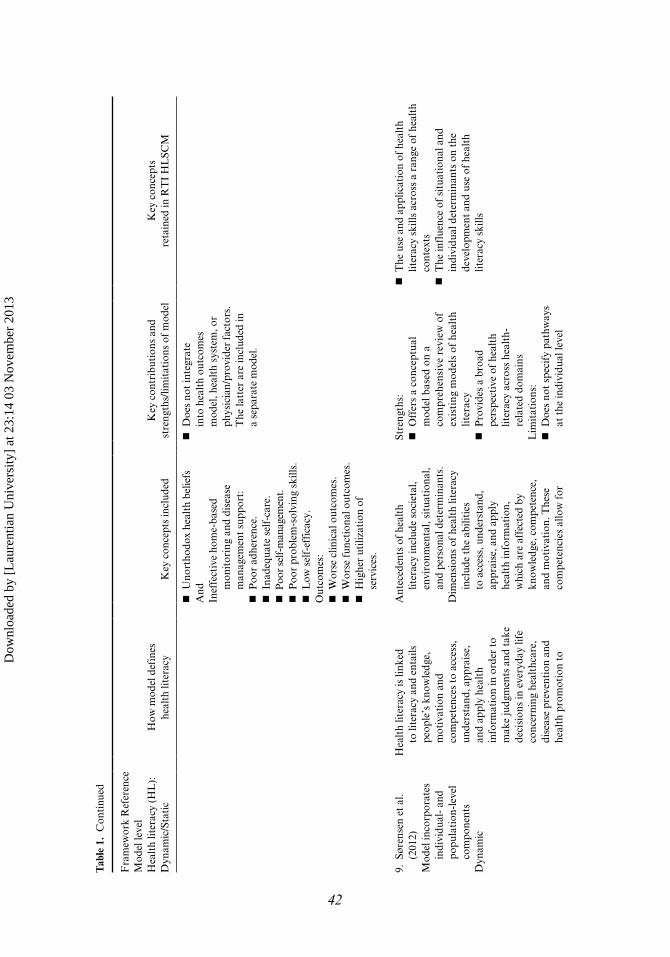
In Table 1, we summarize and compare key characteristics and constructs from 10 different theories about health literacy skills and identify concepts from each that have informed the development of the HLS. Table 1 also indicates if the framework treats health literacy skills as dynamic or static, the definition of health literacy used by the authors and key contributions, strengths, and limitations of the framework. Next, we describe the key concepts found in our review of the different theoretical frameworks. Several concepts can be found in multiple theoretical frameworks and are subsequently described.
Communication
Communication is included within different parts of health literacy frameworks. Some include communication as a component of health literacy (Baker, 2006; Mancuso, 2008; Manganello, 2008; Nutbeam, 2000). The Institute of Medicine includes oral literacy—listening and speaking skills—as a component of the general literacy skills that are necessary for health literacy and is essentially the same as communication skills. Rootman and colleagues (2002) include communication as a factor that influences the development of health literacy, and as a component of general literacy. Paasche-Orlow and Wolf (2007) include communication within the patient-provider interaction as a mediator of the relation between health literacy and health outcomes. The quality and effectiveness of patient-clinician communication is also an important mediator of the relation between health literacy and health outcomes in Schillinger’s (2001) framework.
Knowledge
Health-related knowledge is another concept that appears in various locations within health literacy frameworks. The Institute of Medicine includes cultural and conceptual knowledge (e.g., “an understanding of health and illness and a conceptualization of risks and benefits”) as components of literacy and health literacy (Nielsen-Bohlman et al., 2004, p. 37). Nutbeam (2000), Rootman and colleagues (2002), and Sørensen and colleagues (2012) also include knowledge as a component of health literacy, yet still consider health literacy to be a set of skills. However, other frameworks consider knowledge as a factor that influences the development of health literacy skills. Baker (2006) uses the term “prior knowledge” to indicate that it is a factor that contributes to the development of health literacy and suggests that prior knowledge consists of vocabulary and conceptual knowledge of health and health care. In their framework, von Wagner and colleagues (2009) include knowledge in two places: as a factor that influences health literacy and as a mediator of the relation between health literacy and health actions (which affect outcomes). Paasche-Orlow and Wolf (2007) include a patient’s knowledge as a factor that affects the patient-provider interaction, which in turn influences health outcomes. Lee and colleagues (2004) include knowledge of disease and self-care as a mediator of the relation between health literacy and health outcomes.
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
Tab
le 1
. In
divi
dual
-lev
el m
odel
s of
hea
lth
liter
acy:
A s
umm
ary
and
com
pari
son
of k
ey c
once
pts
from
hea
lth
liter
acy
mod
els,
iden
tify
ing
the
key
conc
epts
tha
t ha
ve in
form
ed
the
deve
lopm
ent
of t
he R
TI
Hea
lth
Lit
erac
y Sk
ills
Con
cept
ual M
odel
(R
TI
HL
SCM
)
Fra
mew
ork
Ref
eren
ceM
odel
leve
lH
ealt
h lit
erac
y (H
L):
D
ynam
ic/S
tati
cH
ow m
odel
def
ines
heal
th li
tera
cyK
ey c
once
pts
incl
uded
Key
con
trib
utio
ns a
nd
stre
ngth
s/lim
itat
ions
of
mod
elK
ey c
once
pts
reta
ined
in R
TI
HL
SCM
1. B
aker
(20
06)
In
divi
dual
-
leve
l mod
elD
ynam
ic
Pre
sent
s In
stit
ute
of
Med
icin
e’s
(IO
M)
and
Hea
lthy
Peo
ple’
s 20
10
defi
niti
on: “
The
deg
ree
to w
hich
indi
vidu
als
have
th
e ca
paci
ty t
o ob
tain
, pr
oces
s, a
nd u
nder
stan
d ba
sic
heal
th in
form
atio
n an
d se
rvic
es n
eede
d to
m
ake
appr
opri
ate
heal
th
deci
sion
s.”
Stat
es th
at th
is d
efin
itio
n is
sta
tic
and
pres
ents
fr
amew
ork
that
is
dyna
mic
(ind
ivid
ual a
nd
heal
th c
are
enco
unte
r).
Com
pone
nts
of H
L:
P
rint
(abi
lity
to u
nder
stan
d w
ritt
en h
ealth
info
rmat
ion)
. O
ral (
abili
ty t
o or
ally
co
mm
unic
ate
abou
t he
alth
).
Indi
vidu
al c
apac
ity
(def
ined
as
read
ing
flue
ncy)
.P
rior
kno
wle
dge
(inc
lude
s vo
cabu
lary
and
con
cept
ual
know
ledg
e of
hea
lth
and
heal
th c
are)
aff
ects
cap
acit
y an
d he
alth
lite
racy
.P
oten
tial
med
iato
rs/
mod
erat
ors:
cu
ltur
e an
d no
rms,
bar
rier
s to
ch
ange
(ne
w k
now
ledg
e,
posi
tive
att
itud
es, g
reat
er
self
-eff
icac
y, b
ehav
ior
chan
ge).
Out
com
es: i
mpr
oved
hea
lth
outc
omes
.
Vie
ws
unde
rlyi
ng p
rior
kn
owle
dge
as a
res
ourc
e th
at a
ffec
ts H
L, n
ot a
s pa
rt o
f th
e de
fini
tion
. St
reng
ths:
I
dent
ifie
s m
edia
tors
/ m
oder
ator
s th
at m
ay
infl
uenc
e ou
tcom
es.
E
mph
asiz
es t
he r
ole
of
prio
r kn
owle
dge
and
reco
gniz
es c
once
ptua
l kn
owle
dge
as w
ell a
s vo
cabu
lary
.L
imit
atio
ns:
D
oes
not
iden
tify
spe
cifi
c he
alth
out
com
es.
P
rior
kno
wle
dge.
C
omm
unic
atio
n as
com
pone
nt o
f H
L.
C
ultu
re a
nd s
ocia
l nor
ms
(fro
m
fam
ily, c
omm
unit
y, m
edia
, etc
.) a
s fa
ctor
s th
at in
flue
nce
the
rela
tion
ship
be
twee
n he
alth
lite
racy
and
hea
lth
outc
omes
. I
ndiv
idua
l-le
vel m
edia
tors
: att
itud
e,
self
-eff
icac
y.
2 L
ee, A
rozu
llah,
&
Cho
(20
04)
Indi
vidu
al-le
vel m
odel
Dyn
amic
IOM
def
init
ion:
“th
e ca
paci
ty o
f in
divi
dual
s to
ob
tain
, pro
cess
, an
d un
ders
tand
bas
ic
heal
th in
form
atio
n an
d se
rvic
es n
eede
d to
mak
e
The
oret
ical
fra
mew
ork
of
how
HL
aff
ects
out
com
e—th
roug
h in
term
edia
te
fact
ors:
dep
icts
“ne
t” e
ffec
ts
of H
L a
nd in
term
edia
te
vari
able
s.
Stre
ngth
s:
Pre
sent
s te
stab
le r
elat
ions
hips
ba
sed
on fr
amew
ork.
Lim
itat
ions
: D
oes
not
dire
ctly
co
nsid
er in
divi
dual
’s
Diff
eren
ces
betw
een
Lee
et
al.
fram
ewor
k an
d R
TI
fr
amew
ork:
Lee
: kno
wle
dge
of h
ealt
h an
d di
seas
e is
a m
edia
tor
betw
een
HL
on
heal
th
outc
omes
;
34
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
35
appr
opri
ate
heal
th
deci
sion
s.”
Mec
han
ism
s o
r in
term
edia
te f
acto
rs
lin
kin
g H
L t
o h
ealt
h o
utc
om
es (
con
sid
ered
in
terc
orr
elat
ed):
D
isea
se &
sel
f-ca
re
know
ledg
e. H
ealt
h ri
sk b
ehav
ior.
P
reve
ntiv
e ca
re &
phy
sici
an
visi
ts.
C
ompl
ianc
e w
ith
med
icat
ions
.O
utco
mes
: H
ealt
h st
atus
. E
mer
genc
y ca
re.
H
ospi
taliz
atio
n.M
oder
ator
s/co
ntro
l var
iabl
es:
S
ES.
G
ende
r. E
thni
city
. H
ealt
h in
sura
nce
cove
rage
. D
isea
se s
ever
ity.
I
ncom
e di
scre
panc
y.E
thni
c co
mpo
siti
on o
f co
mm
unit
y
mot
ivat
ion,
sel
f-ef
fica
cy,
or a
ttit
ude.
D
oes
not c
onsi
der
prov
ider
-lev
el, s
yste
m-
leve
l, or
soc
ieta
l-le
vel
fact
ors.
W
hile
ack
now
ledg
ing
its
impo
rtan
ce, d
oes
not
incl
ude
soci
al s
uppo
rt a
s a
pote
ntia
l med
iato
r of
the
re
lati
onsh
ip b
etw
een
HL
an
d he
alth
out
com
es.
RT
I: k
now
ledg
e co
ntri
bute
s to
one
’s H
L
leve
l and
is a
res
ult
of a
pply
ing
HL
sk
ills
to s
tim
uli.
Hea
lth
outc
omes
als
o in
flue
nce
cont
rol
vari
able
s.D
escr
ibes
env
iron
men
tal v
aria
bles
as
infl
uenc
ing
heal
th li
tera
cy s
kills
de
velo
pmen
t, m
edia
tors
, and
hea
lth
outc
omes
.
3. M
ancu
so (
2008
)In
divi
dual
-lev
el
mod
elD
ynam
ic
Rev
iew
s an
d cr
itiq
ues
vari
ous
defi
niti
ons
of H
L
but
does
not
tot
ally
ado
pt
any.
Six
dim
ensi
ons
of c
ompe
tenc
e th
at a
re a
ntec
eden
ts o
f H
L:
1. O
pera
tion
al.
2. I
nter
acti
ve.
3. A
uton
omou
s.4.
Inf
orm
atio
nal.
5. C
onte
xtua
l.
Use
s co
ncep
t/di
men
sion
al
anal
ysis
to
conc
eptu
aliz
e th
e an
tece
dent
s, a
ttri
bute
s,
and
cons
eque
nces
of
HL
. P
osit
ions
HL
wit
hin
the
cont
ext
of in
divi
dual
and
so
ciet
y an
d id
enti
fies
the
C
omm
unic
atio
n as
a c
ompo
nent
of
heal
th li
tera
cy.
(Con
tinu
ed)
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
Fra
mew
ork
Ref
eren
ceM
odel
leve
lH
ealt
h lit
erac
y (H
L):
D
ynam
ic/S
tati
cH
ow m
odel
def
ines
heal
th li
tera
cyK
ey c
once
pts
incl
uded
Key
con
trib
utio
ns a
nd
stre
ngth
s/lim
itat
ions
of
mod
elK
ey c
once
pts
reta
ined
in R
TI
HL
SCM
6. C
ultu
ral.
Att
ribu
tes
of H
L:
C
apac
ity:
indi
vidu
al s
kills
in
info
rmat
ion
proc
essi
ng,
oral
lang
uage
, soc
ial s
kills
, an
d ot
hers
. C
ompr
ehen
sion
: un
ders
tand
ing
info
rmat
ion.
C
omm
unic
atio
n: r
eadi
ng,
wri
ting
, spe
akin
g,
unde
rsta
ndin
g, li
sten
ing,
an
d ob
serv
ing.
Con
sequ
ence
s of
poo
r H
L:
incr
ease
d co
sts,
less
kn
owle
dge
of d
isea
ses
and
trea
tmen
ts, f
ewer
sel
f-m
anag
emen
t ski
lls, p
oore
r co
mpl
ianc
e, m
ore
erro
rs,
poor
abi
lity
to n
egot
iate
and
ac
cess
the
heal
th c
are
syst
em,
poor
er h
ealth
out
com
es.
inte
ract
ion
betw
een
the
six
com
pete
ncie
s an
d th
e th
ree
attr
ibut
es.
Lim
itat
ions
: doe
s no
t id
enti
fy
the
path
way
bet
wee
n an
tece
dent
s/at
trib
utes
an
d o
utco
mes
; doe
s no
t di
stin
guis
h be
twee
n lo
ng t
erm
and
sho
rt
term
out
com
es; d
oes
not
iden
tify
pot
enti
al
med
iato
rs b
etw
een
HL
an
d he
alth
out
com
es.
4. M
anga
nello
(2
008)
Indi
vidu
al-l
evel
m
odel
Stat
ic
Ref
ers
to I
OM
def
init
ion:
“t
he c
apac
ity
of
indi
vidu
als
to o
btai
n,
proc
ess,
and
und
erst
and
basi
c he
alth
info
rmat
ion
and
serv
ices
nee
ded
to
mak
e ap
prop
riat
e he
alth
de
cisi
ons.
”
Con
cept
ual f
ram
ewor
k of
ad
oles
cent
HL
.In
divi
dual
tra
its
(aff
ect
HL
): A
ge, r
ace,
gen
der,
lang
uage
, cu
ltur
e, e
duca
tion
. S
ocia
l ski
lls.
C
ogni
tive
ski
lls.
P
hysi
cal a
bilit
ies.
Stre
ngth
s:
C
onsi
ders
HL
bas
ed
on t
he e
colo
gica
l m
odel
: inc
orpo
rate
s bo
th in
divi
dual
and
en
viro
nmen
tal i
nflu
ence
s on
HL
and
hea
lth
outc
omes
.
Indi
vidu
al t
rait
s: C
ultu
re.
C
ogni
tive
ski
lls.
P
hysi
cal a
bilit
ies.
Med
iato
rs:
F
amily
. M
ass
med
ia.
H
ealt
h ca
re s
yste
m.
36
Tab
le 1
. C
onti
nued
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
37
Fra
mew
ork
spec
ifie
s sk
ills
rela
ted
to H
L:
Lev
els
from
Nut
beam
(2
000)
: F
unct
iona
l. I
nter
acti
ve.
C
riti
cal.
Add
s: M
edia
lite
racy
.
M
edia
use
.H
L (
affe
ct h
ealt
h ou
tcom
es):
F
unct
iona
l. I
nter
acti
ve.
C
riti
cal.
M
edia
lite
racy
.M
edia
tors
: F
amily
and
pee
r in
flue
nces
. M
ass
med
ia.
E
duca
tion
sys
tem
. H
ealt
h sy
stem
.H
ealt
h ou
tcom
es H
ealt
h be
havi
or.
H
ealt
h co
sts.
H
ealt
h-se
rvic
e us
e.
E
xpla
ins
rela
tion
ship
be
twee
n H
L a
nd
heal
th o
utco
mes
in
spec
ific
sub
popu
lati
on
(ado
lesc
ents
), a
nd
reco
gniz
es t
hat
the
stru
ctur
e of
a fr
amew
ork
expl
aini
ng th
e re
lati
onsh
ip
may
var
y by
pop
ulat
ion.
Lim
itat
ions
: D
oes
not
addr
ess
mot
ivat
ion,
phy
sici
an-
pati
ent
inte
ract
ion,
and
ot
her
psyc
holo
gica
l co
nsid
erat
ions
.
The
infl
uenc
e of
soc
ieta
l-le
vel v
aria
bles
on
all
sect
ions
of
the
mod
el.
5. N
utbe
am (
2000
)In
divi
dual
-lev
el
mod
el, b
ut
iden
tifi
es s
ocia
l an
d po
litic
al g
oals
Dyn
amic
: HL
can
be
impr
oved
thr
ough
ed
ucat
iona
l pr
ogra
ms
Wor
ld H
ealt
h O
rgan
izat
ion’
s de
fini
tion
(N
utbe
am,
1998
): “
The
per
sona
l, co
gnit
ive
and
soci
al
skill
s w
hich
det
erm
ine
the
abili
ty o
f in
divi
dual
s to
gai
n ac
cess
to,
un
ders
tand
, and
use
in
form
atio
n to
pro
mot
e an
d m
aint
ain
good
he
alth
.”
Iden
tifi
es 3
pro
gres
sive
leve
ls
of H
L (
from
Fre
ebod
y &
L
uke,
199
0):
1. B
asic
/Fun
ctio
nal:
suf
fici
ent
basi
c sk
ills
in r
eadi
ng
and
wri
ting
to b
e ab
le
to fu
ncti
on e
ffec
tive
ly
in e
very
day
situ
atio
ns.
Inte
rven
tions
sho
uld
focu
s on
the
educ
atio
nal g
oal o
f co
mm
unic
atin
g in
form
atio
n.2.
Com
mun
icat
ive/
Inte
ract
ive:
m
ore
adva
nced
cog
niti
ve,
liter
acy,
and
soc
ial s
kills
us
ed t
o ac
tive
ly p
arti
cipa
te
in e
very
day
acti
viti
es, t
o ex
trac
t in
form
atio
n an
d de
rive
mea
ning
fro
m
Stre
ngth
s: C
reat
es a
m
ulti
dim
ensi
onal
co
ncep
tual
izat
ion
of H
L,
goes
bey
ond
func
tion
al
liter
acy
to I
nteg
rate
co
ncep
ts o
f int
erac
tive
and
cr
itic
al li
tera
cy in
to H
L.
P
lace
s he
alth
edu
cati
on
and
com
mun
icat
ion
into
the
wid
er c
onte
xt
of h
ealt
h pr
omot
ion,
an
d hi
ghlig
hts
HL
as
a ke
y ou
tcom
e fr
om h
ealt
h ed
ucat
ion.
R
ecog
nize
s ho
w s
ocia
l co
ntex
t and
env
iron
men
t in
fluen
ce h
ealth
beh
avio
rs,
I
nflu
ence
of
envi
ronm
enta
l fac
tors
on
heal
th o
utco
mes
. H
ealt
h be
havi
ors
rela
ted
to li
fest
yle,
bu
t con
side
red
an o
utco
me
rath
er
than
a m
edia
tor
in R
TI’
s fr
amew
ork.
M
orbi
dity
and
mor
talit
y as
hea
lth
outc
omes
.
(Con
tinu
ed)
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
Fra
mew
ork
Ref
eren
ceM
odel
leve
lH
ealt
h lit
erac
y (H
L):
D
ynam
ic/S
tati
cH
ow m
odel
def
ines
heal
th li
tera
cyK
ey c
once
pts
incl
uded
Key
con
trib
utio
ns a
nd
stre
ngth
s/lim
itat
ions
of
mod
elK
ey c
once
pts
reta
ined
in R
TI
HL
SCM
diff
eren
t fo
rms
of
com
mun
icat
ion,
and
to
appl
y ne
w in
form
atio
n to
ch
angi
ng c
ircu
mst
ance
s.
Inte
rven
tion
s sh
ould
foc
us
on t
he e
duca
tion
al g
oal o
f de
velo
ping
per
sona
l ski
lls.
3. C
riti
cal l
iter
acy:
mor
e ad
vanc
ed c
ogni
tive
ski
lls
whi
ch, t
oget
her
wit
h so
cial
sk
ills,
can
be
appl
ied
to c
riti
cally
ana
lyze
in
form
atio
n, a
nd t
o us
e th
is in
form
atio
n to
exe
rt
grea
ter
cont
rol o
ver
life
even
ts a
nd s
itua
tion
s.
Inte
rven
tion
s sh
ould
foc
us
on t
he e
duca
tion
al g
oal o
f pe
rson
al a
nd c
omm
unit
y em
pow
erm
ent.
Out
com
e m
odel
cat
egor
izat
ion
( m
odel
incl
udes
mea
sure
s fo
r ea
ch c
ateg
ory)
:H
ealt
h pr
omot
ion
acti
ons:
ed
ucat
ion,
soc
ial
mob
iliza
tion
, adv
ocac
yH
ealt
h pr
omot
ion
outc
omes
(i
nter
vent
ion
impa
ct
mea
sure
s): h
ealt
h lit
erac
y,
soci
al a
ctio
n an
d in
flue
nce,
whi
ch in
turn
, aff
ect h
ealth
ou
tcom
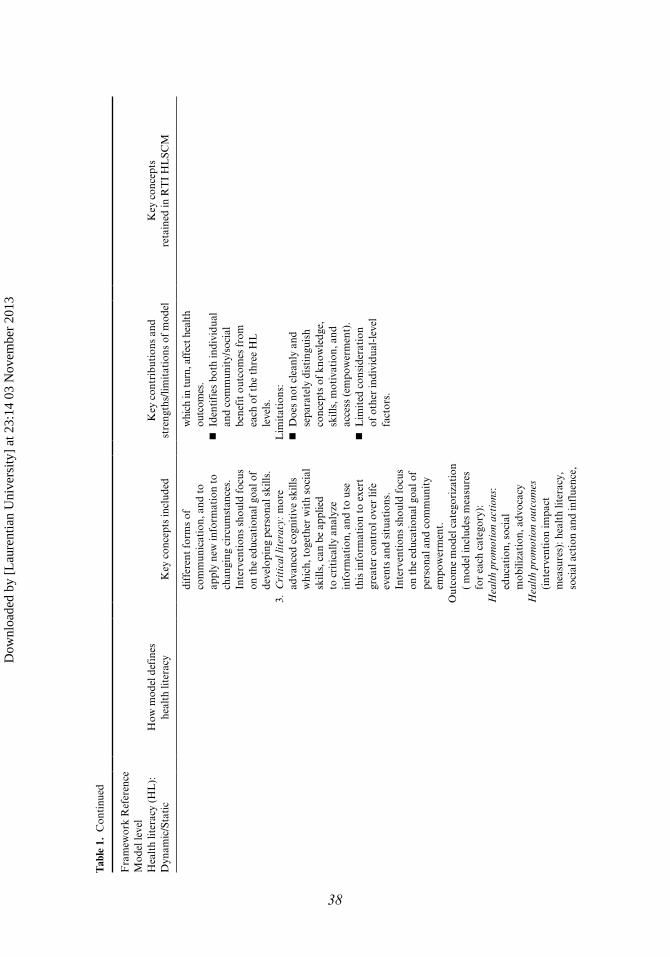
es.
I
dent
ifie
s bo
th in
divi
dual
an
d co
mm
unit
y/so
cial
be
nefi
t ou
tcom
es f
rom
ea
ch o
f th
e th
ree
HL
le
vels
.L
imit
atio
ns:
D
oes
not
clea
nly
and
sepa
rate
ly d
isti
ngui
sh
conc
epts
of
know
ledg
e,
skill
s, m
otiv
atio
n, a
nd
acce
ss (
empo
wer
men
t).
L
imit
ed c
onsi
dera
tion
of
oth
er in
divi
dual
-lev
el
fact
ors.
38
Tab
le 1
. C
onti
nued
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
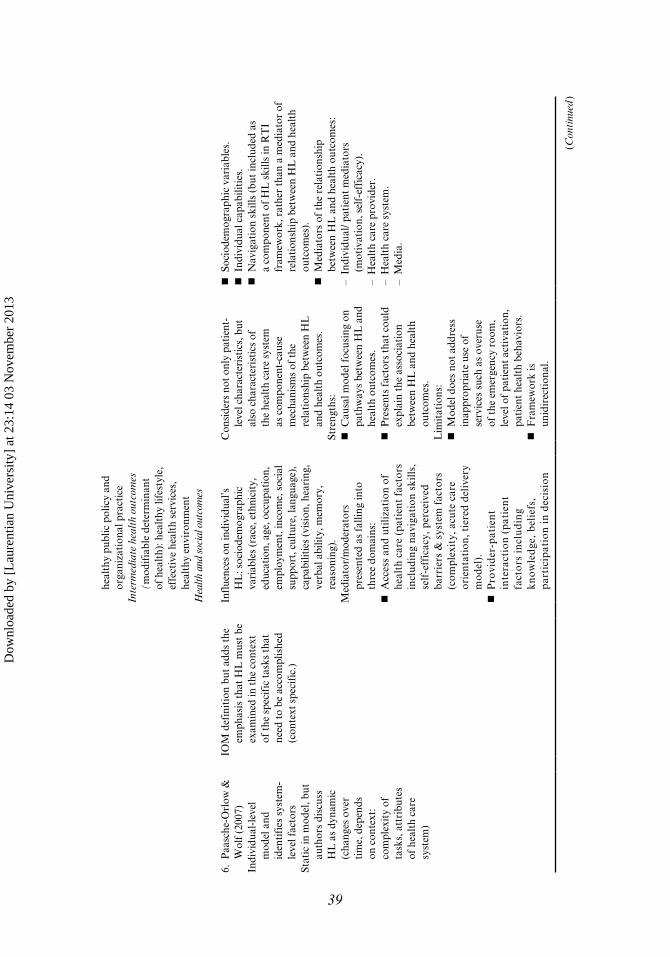
he
alth
y pu
blic
pol
icy
and
orga
niza
tion
al p
ract
ice
Inte
rmed
iate
hea
lth
outc
omes
(m
odif
iabl
e de
term
inan
t of
hea
lth)
: hea
lthy
life
styl
e,
effe
ctiv
e he
alth
ser
vice
s,
heal
thy
envi
ronm
ent
Hea
lth a
nd s
ocia
l out
com
es
6. P
aasc
he-O
rlow
&
Wol
f (2
007)
Indi
vidu
al-l
evel
m
odel
and
id
enti
fies
sys
tem
-le
vel f
acto
rsSt
atic
in m
odel
, but
au
thor
s di
scus
s H
L a
s dy
nam
ic
(cha
nges
ove
r ti
me,
dep
ends
on
con
text
: co
mpl
exit
y of
ta
sks,
att
ribu
tes
of h
ealt
h ca
re
syst
em)
IOM
def
init
ion
but
adds
the
em
phas
is t
hat
HL
mus
t be
ex
amin
ed in
the
con
text
of
the
spe
cifi
c ta
sks
that
ne
ed t
o be
acc
ompl
ishe
d (c
onte
xt s
peci
fic.
)
Infl
uenc
es o
n in
divi
dual
’s
HL
: soc
iode
mog
raph
ic
vari
able
s (r
ace,
eth
nici
ty,
educ
atio
n, a
ge, o
ccup
atio
n,
empl
oym
ent,
inco
me,
soc
ial
supp
ort,
cul
ture
, lan
guag
e),
capa
bilit
ies
(vis
ion,
hea
ring
, ve
rbal
abi
lity,
mem
ory,
re
ason
ing)
.M
edia
tor/
mod
erat
ors
pres
ente
d as
fal
ling
into
th
ree
dom
ains
: A
cces
s an
d ut
iliza
tion
of
heal
th c
are
(pat
ient
fac
tors
in
clud
ing
navi
gati
on s
kills
, se
lf-e
ffic
acy,
per
ceiv
ed
barr
iers
& s
yste
m f
acto
rs(c
ompl
exit
y, a
cute
car
e or
ient
atio
n, t
iere
d de
liver
y m
odel
). P
rovi
der
-pat
ien
t in
tera
ctio
n (
pat
ien
t fa
cto
rs i
ncl
ud
ing
kn
ow
led
ge,
bel
iefs
, p
arti
cip
atio
n i
n d
ecis
ion
Con
side
rs n
ot o
nly
pati
ent-
leve
l cha
ract
eris
tics
, but
al
so c
hara
cter
isti
cs o
f th
e he
alth
car
e sy
stem
as
com
pone
nt-c
ause
m
echa
nism
s of
the
rela
tion
ship
bet
wee
n H
L
and
heal
th o
utco
mes
.St
reng
ths:
C
ausa
l mod
el f
ocus
ing
on
path
way
s be
twee
n H
L a
nd
heal
th o
utco
mes
. P
rese
nts
fact
ors
that
cou
ld
expl
ain
the
asso
ciat
ion
betw
een
HL
and
hea
lth
outc
omes
.L
imit
atio
ns:
M
odel
doe
s no
t ad
dres
s in
appr
opri
ate
use
of
serv
ices
suc
h as
ove
ruse
of
the
em
erge
ncy
room
, le
vel o
f pa
tien
t ac
tiva
tion
, pa
tien
t he
alth
beh
avio
rs.
F
ram
ewor
k is
un
idir
ecti
onal
.
S
ocio
dem
ogra
phic
var
iabl
es.
I
ndiv
idua
l cap
abili
ties
. N
avig
atio
n sk
ills
(but
incl
uded
as
a co
mpo
nent
of
HL
ski
lls in
RT
I fr
amew
ork,
rat
her
than
a m
edia
tor
of
rela
tion
ship
bet
wee
n H
L a
nd h
ealt
h ou
tcom
es).
M
edia
tors
of
the
rela
tion
ship
be
twee
n H
L a
nd h
ealt
h ou
tcom
es:
– In
divi
dual
/ pat
ient
med
iato
rs
(mot
ivat
ion,
sel
f-ef
fica
cy).
– H
ealt
h ca
re p
rovi
der.
– H
ealt
h ca
re s
yste
m.
– M
edia
.
39
(Con
tinu
ed)
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
Fra
mew
ork
Ref
eren
ceM
odel
leve
lH
ealt
h lit
erac
y (H
L):
D
ynam
ic/S
tati
cH
ow m
odel
def
ines
heal
th li
tera
cyK
ey c
once
pts
incl
uded
Key
con
trib
utio
ns a
nd
stre
ngth
s/lim
itat
ions
of
mod
elK
ey c
once
pts
reta
ined
in R
TI
HL
SCM
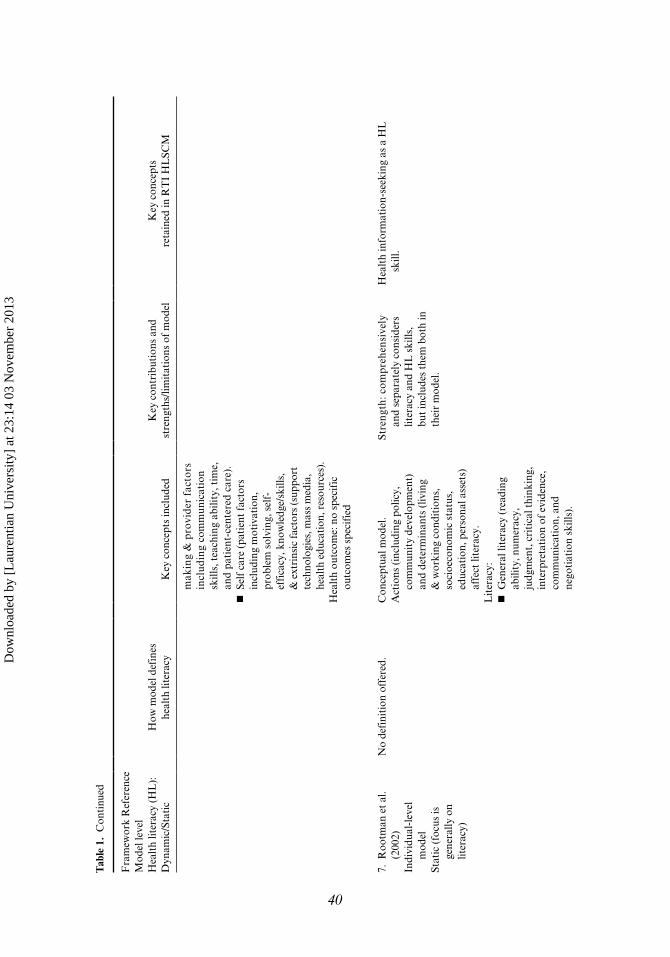
mak
ing
& p
rovi
der
fact
ors
incl
udin
g co
mm
unic
atio
n sk
ills,
tea
chin
g ab
ility
, tim
e,
and
pati
ent-
cent
ered
car
e).
S
elf
care
(pa
tien
t fa
ctor
s in
clud
ing
mot
ivat
ion,
pr
oble
m s
olvi
ng, s
elf-
effi
cacy
, kno
wle
dge/
skill
s,
& e
xtri
nsic
fact
ors
(sup
port
te
chno
logi
es, m
ass
med
ia,
heal
th e
duca
tion
, res
ourc
es).
Hea
lth
outc
ome:
no
spec
ific
ou
tcom
es s
peci
fied
7. R
ootm
an e
t al
. (2
002)
Indi
vidu
al-l
evel
m
odel
Stat
ic (
focu
s is
ge
nera
lly o
n lit
erac
y)
No
defi
niti
on o
ffer
ed.
Con
cept
ual m
odel
. A
ctio
ns (
incl
udin
g po
licy,
co
mm
unit
y de
velo
pmen
t)
and
dete
rmin
ants
(liv
ing
& w
orki
ng c
ondi
tion
s,
soci
oeco
nom
ic s
tatu
s,
educ
atio
n, p
erso
nal a
sset
s)
affe
ct li
tera
cy.
Lit
erac
y: G
ener
al li
tera
cy (
read
ing
abili
ty, n
umer
acy,
ju
dgm
ent,
cri
tica
l thi
nkin
g,
inte
rpre
tati
on o
f ev
iden
ce,
com
mun
icat
ion,
and
ne
goti
atio
n sk
ills)
.
Stre
ngth
: com
preh
ensi
vely
an
d se
para
tely
con
side
rs
liter
acy
and
HL
ski
lls,
but
incl
udes
the
m b
oth
in
thei
r m
odel
.
Hea
lth
info
rmat
ion-
seek
ing
as a
HL
sk
ill.
40
Tab
le 1
. C
onti
nued
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
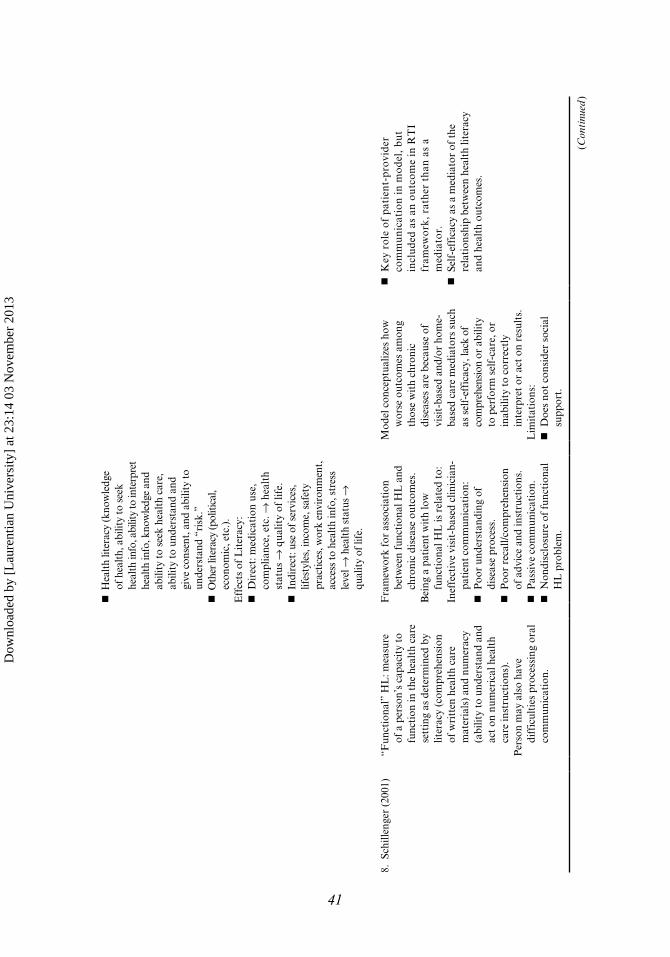
H
ealt
h lit
erac
y (k
now
ledg
e of
hea
lth,
abi
lity
to s
eek
heal
th in
fo, a
bilit
y to
inte
rpre
t he
alth
info
, kno
wle
dge
and
abili
ty to
see
k he
alth
car
e,
abili
ty to
und
erst
and
and
give
con
sent
, and
abi
lity
to
unde
rsta
nd “
risk
.” O
ther
lite
racy
(pol
itica
l, ec
onom
ic, e
tc.)
.E
ffec
ts o
f L
iter
acy:
D
irec
t: m
edic
atio
n us
e,
com
plia
nce,
etc
. → h
ealt
h st
atus
→ q
ualit
y of
life
. I
ndir
ect:
use
of s
ervi
ces,
lif
esty
les,
inco
me,
saf
ety
prac
tice
s, w
ork
envi
ronm
ent,
ac
cess
to h
ealt
h in
fo, s
tres
s le
vel →
hea
lth
stat
us →
qu
alit
y of
life
.
8. S
chill
enge
r (2
001)
“Fun
ctio
nal”
HL
: mea
sure
of
a p
erso
n’s
capa
city
to
func
tion
in t
he h
ealt
h ca
re
sett
ing
as d
eter
min
ed b
y lit
erac
y (c
ompr
ehen
sion
of
wri
tten
hea
lth
care
m
ater
ials
) an
d nu
mer
acy
(abi
lity
to u
nder
stan
d an
d ac
t on
num
eric
al h
ealt
h ca
re in
stru
ctio
ns).
P
erso
n m
ay a
lso
have
di
ffic
ulti
es p
roce
ssin
g or
al
com
mun
icat
ion.
Fra
mew
ork
for
asso
ciat
ion
betw
een
func
tion
al H
L a
nd
chro
nic
dise
ase
outc
omes
.B
eing
a p
atie
nt w
ith
low
fu
ncti
onal
HL
is r
elat
ed t
o:In
effe
ctiv
e vi
sit-
base
d cl
inic
ian-
pati
ent
com
mun
icat
ion:
P
oor
unde
rsta
ndin
g of
di
seas
e pr
oces
s. P
oor
reca
ll/co
mpr
ehen
sion
of
adv
ice
and
inst
ruct
ions
. P
assi
ve c
omm
unic
atio
n. N
ondi
sclo
sure
of
func
tion
al
HL
pro
blem
.
Mod
el c
once
ptua
lizes
how
w
orse
out
com
es a
mon
g th
ose
wit
h ch
roni
c di
seas
es a
re b
ecau
se o
f vi
sit-
base
d an
d/or
hom
e-ba
sed
care
med
iato
rs s
uch
as s
elf-
effi
cacy
, lac
k of
co
mpr
ehen
sion
or
abili
ty
to p
erfo
rm s
elf-
care
, or
inab
ility
to
corr
ectl
y in
terp
ret
or a
ct o
n re
sult
s.
Lim
itat
ions
: D
oes
not
cons
ider
soc
ial
supp
ort.
K
ey r
ole
of p
atie
nt-p
rovi
der
com
mun
icat
ion
in m
odel
, but
in
clud
ed a
s an
out
com
e in
RT
I fr
amew
ork,
rat
her
than
as
a m
edia
tor.
S
elf-
effi
cacy
as
a m
edia
tor
of t
he
rela
tion
ship
bet
wee
n he
alth
lite
racy
an
d he
alth
out
com
es.
41
(Con
tinu
ed)
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
Fra
mew
ork
Ref
eren
ceM
odel
leve
lH
ealt
h lit
erac
y (H
L):
D
ynam
ic/S
tati
cH
ow m
odel
def
ines
heal
th li
tera
cyK
ey c
once
pts
incl
uded
Key
con
trib
utio
ns a
nd
stre
ngth
s/lim
itat
ions
of
mod
elK
ey c
once
pts
reta
ined
in R
TI
HL
SCM
U
nort
hodo
x he
alth
bel
iefs
And
Inef
fect
ive
hom
e-ba
sed
mon
itor
ing
and
dise
ase
man
agem
ent
supp
ort:
P
oor
adhe
renc
e. I
nade
quat
e se
lf-c
are.
P
oor
self-
man
agem
ent.
P
oor
prob
lem
-sol
ving
ski
lls.
L
ow s
elf-
effi
cacy
.O
utco
mes
: W
orse
clin
ical
out
com
es.
W
orse
fun
ctio
nal o
utco
mes
. H
ighe
r ut
iliza
tion
of
serv
ices
.
D
oes
not
inte
grat
e in
to h
ealt
h ou
tcom
es
mod
el, h
ealt
h sy
stem
, or
phys
icia
n/pr
ovid
er fa
ctor
s.
The
latt
er a
re in
clud
ed in
a
sepa
rate
mod
el.
9. S
øren
sen
et a
l. (2
012)
Mod
el in
corp
orat
es
indi
vidu
al-
and
popu
lati
on-l
evel
co
mpo
nent
sD
ynam
ic
Hea
lth
liter
acy
is li
nked
to
lite
racy
and
ent
ails
pe
ople
’s k
now
ledg
e,
mot
ivat
ion
and
com
pete
nces
to
acce
ss,
unde
rsta
nd, a
ppra
ise,
an
d ap
ply
heal
th
info
rmat
ion
in o
rder
to
mak
e ju
dgm
ents
and
tak
e de
cisi
ons
in e
very
day
life
conc
erni
ng h
ealt
hcar
e,
dise
ase
prev
enti
on a
nd
heal
th p
rom
otio
n to
Ant
eced
ents
of
heal
th
liter
acy
incl
ude
soci
etal
, en
viro
nmen
tal,
situ
atio
nal,
and
pers
onal
det
erm
inan
ts.
Dim
ensi
ons
of h
ealt
h lit
erac
y in
clud
e th
e ab
iliti
es
to a
cces
s, u
nder
stan
d,
appr
aise
, and
app
ly
heal
th in
form
atio
n,
whi
ch a
re a
ffec
ted
by
know
ledg
e, c
ompe
tenc
e,
and
mot
ivat
ion.
The
se
com
pete
ncie
s al
low
for
Stre
ngth
s: O
ffer
s a
conc
eptu
al
mod
el b
ased
on
a co
mpr
ehen
sive
rev
iew
of
exis
ting
mod
els
of h
ealt
h lit
erac
y P
rovi
des
a br
oad
pers
pect
ive
of h
ealt
h lit
erac
y ac
ross
hea
lth-
rela
ted
dom
ains
Lim
itat
ions
: D
oes
not
spec
ify
path
way
s at
the
indi
vidu
al le
vel
T
he u
se a
nd a
pplic
atio
n of
hea
lth
liter
acy
skill
s ac
ross
a r
ange
of
heal
th
cont
exts
T
he in
flue
nce
of s
itua
tion
al a
nd
indi
vidu
al d
eter
min
ants
on
the
deve
lopm
ent
and
use
of h
ealt
h lit
erac
y sk
ills
42
Tab
le 1
. C
onti
nued
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
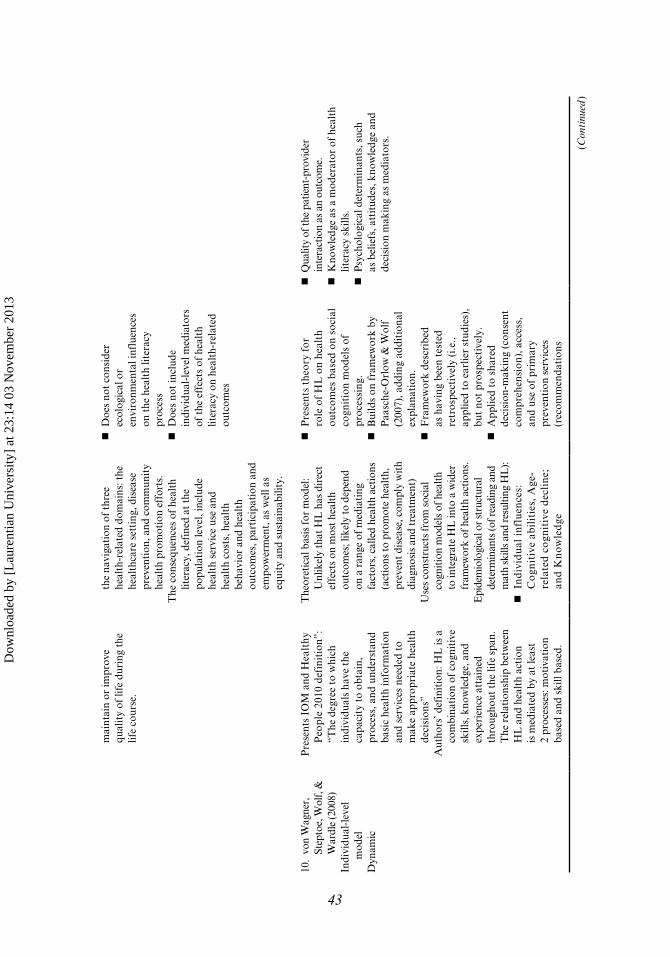
mai
ntai
n or
impr
ove
qual
ity
of li
fe d
urin
g th
e lif
e co
urse
.
the
navi
gati
on o
f th
ree
heal
th-r
elat
ed d
omai
ns: t
he
heal
thca
re s
etti
ng, d
isea
se
prev
enti
on, a
nd c
omm
unit
y he
alth
pro
mot
ion
effo
rts.
The
con
sequ
ence
s of
hea
lth
liter
acy,
def
ined
at
the
popu
lati
on le
vel,
incl
ude
heal
th s
ervi
ce u
se a
nd
heal
th c
osts
, hea
lth
beha
vior
and
hea
lth
outc
omes
, par
tici
pati
on a
nd
empo
wer
men
t, a
s w
ell a
s eq
uity
and
sus
tain
abili
ty.
D
oes
not
cons
ider
ec
olog
ical
or
envi
ronm
enta
l inf
luen
ces
on t
he h
ealt
h lit
erac
y pr
oces
s D
oes
not
incl
ude
indi
vidu
al-l
evel
med
iato
rs
of t
he e
ffec
ts o
f he
alth
lit
erac
y on
hea
lth-
rela
ted
outc
omes
10.
von
Wag
ner,
St
epto
e, W
olf,
&
War
dle
(200
8)In
divi
dual
-lev
el
mod
elD
ynam
ic
Pre
sent
s IO
M a
nd H
ealt
hy
Peo
ple
2010
def
init
ion”
: “T
he d
egre
e to
whi
ch
indi
vidu
als
have
the
ca
paci
ty t
o ob
tain
, pr
oces
s, a
nd u
nder
stan
d ba
sic
heal
th in
form
atio
n an
d se
rvic
es n
eede
d to
m
ake
appr
opri
ate
heal
th
deci
sion
s”A
utho
rs’ d
efin
itio
n: H
L is
a
com
bina
tion
of
cogn
itiv
e sk
ills,
kno
wle
dge,
and
ex
peri
ence
att
aine
d th
roug
hout
the
life
spa
n.
The
rel
atio
nshi
p be
twee
n H
L a
nd h
ealt
h ac
tion
is
med
iate
d by
at
leas
t 2
proc
esse
s: m
otiv
atio
n ba
sed
and
skill
bas
ed.
The
oret
ical
bas
is fo
r m
odel
: U
nlik
ely
that
HL
has
dir
ect
effe
cts
on m
ost h
ealt
h ou
tcom
es; l
ikel
y to
dep
end
on a
ran
ge o
f med
iati
ng
fact
ors,
cal
led
heal
th a
ctio
ns
(act
ions
to p
rom
ote
heal
th,
prev
ent d
isea
se, c
ompl
y w
ith
diag
nosi
s an
d tr
eatm
ent)
Use
s co
nstr
ucts
from
soc
ial
cogn
itio
n m
odel
s of
hea
lth
to in
tegr
ate
HL
into
a w
ider
fr
amew
ork
of h
ealt
h ac
tion
s.E
pide
mio
logi
cal o
r st
ruct
ural
de
term
inan
ts (o
f rea
ding
and
m
ath
skill
s an
d re
sulti
ng H
L):
I
nd
ivid
ual
in
flu
ence
s:
Co
gnit
ive
abil
itie
s, A
ge-
rela
ted
co
gnit
ive
dec
lin
e;
and
Kn
ow
led
ge
P
rese
nts
theo
ry f
or
role
of
HL
on
heal
th
outc
omes
bas
ed o
n so
cial
co
gnit
ion
mod
els
of
proc
essi
ng.
B
uild
s on
fra
mew
ork
by
Paa
sche
-Orl
ow &
Wol
f (2
007)
, add
ing
addi
tion
al
expl
anat
ion.
F
ram
ewor
k de
scri
bed
as h
avin
g be
en t
este
d re
tros
pect
ivel
y (i
.e.,
appl
ied
to e
arlie
r st
udie
s),
but
not
pros
pect
ivel
y. A
pplie
d to
sha
red
deci
sion
-mak
ing
(con
sent
co
mpr
ehen
sion
), a
cces
s,
and
use
of p
rim
ary
prev
enti
on s
ervi
ces
(rec
omm
enda
tion
s
Q
ualit
y of
the
patie
nt-p
rovi
der
inte
ract
ion
as a
n ou
tcom
e. K
now
ledg
e as
a m
oder
ator
of
heal
th
liter
acy
skill
s. P
sych
olog
ical
det
erm
inan
ts, s
uch
as b
elie
fs, a
ttit
udes
, kno
wle
dge
and
deci
sion
mak
ing
as m
edia
tors
.
43
(Con
tinu
ed)
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
Fra
mew
ork
Ref
eren
ceM
odel
leve
lH
ealt
h lit
erac
y (H
L):
D
ynam
ic/S
tati
cH
ow m
odel
def
ines
heal
th li
tera
cyK
ey c
once
pts
incl
uded
Key
con
trib
utio
ns a
nd
stre
ngth
s/lim
itat
ions
of
mod
elK
ey c
once
pts
reta
ined
in R
TI
HL
SCM
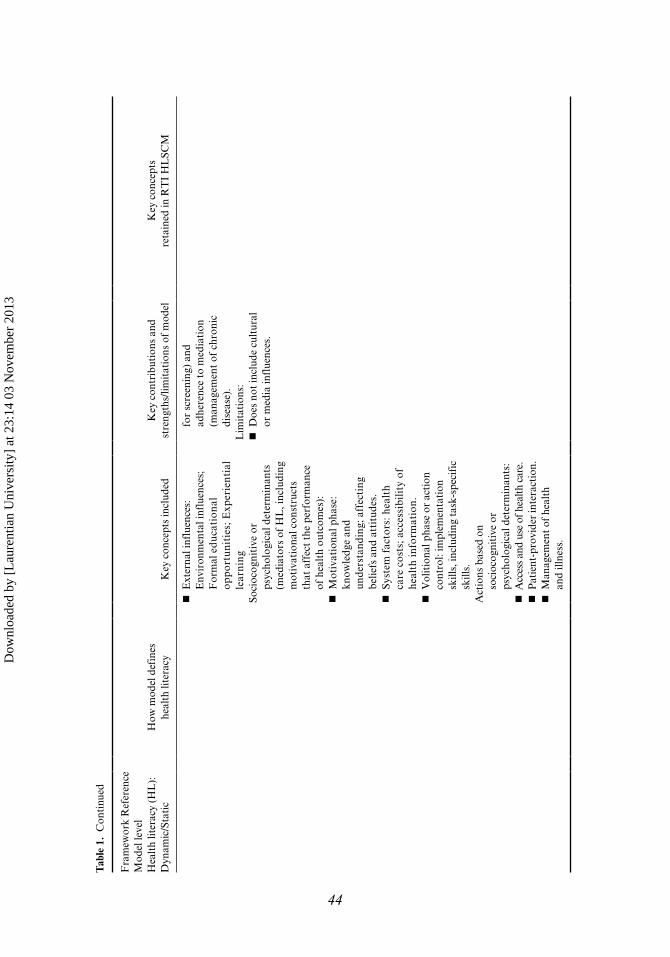
E
xter
nal i
nflu
ence
s:
Env
iron
men
tal i
nflu
ence
s;
For
mal
edu
cati
onal
op
port
unit
ies;
Exp
erie
ntia
l le
arni
ngSo
cioc
ogni
tive
or
psyc
holo
gica
l det
erm
inan
ts
(med
iato
rs o
f H
L, i
nclu
ding
m
otiv
atio
nal c
onst
ruct
s th
at a
ffec
t th
e pe
rfor
man
ce
of h
ealt
h ou
tcom
es):
M
otiv
atio
nal p
hase
: kn
owle
dge
and
unde
rsta
ndin
g; a
ffec
ting
be
liefs
and
att
itud
es.
S
yste
m f
acto
rs: h
ealt
h ca
re c
osts
; acc
essi
bili
ty o
f he
alth
info
rmat
ion.
V
olit
iona
l pha
se o
r ac
tion
co
ntro
l: im
plem
enta
tion
sk
ills,
incl
udin
g ta
sk-s
peci
fic
skill
s.A
ctio
ns b
ased
on
soci
ocog
niti
ve o
r ps
ycho
logi
cal d
eter
min
ants
: A
cces
s an
d us
e of
hea
lth c
are.
P
atie
nt-p
rovi
der
inte
ract
ion.
M
anag
emen
t of
hea
lth
and
illne
ss.
for
scre
enin
g) a
nd
adhe
renc
e to
med
iati
on
(man
agem
ent
of c
hron
ic
dise
ase)
.L
imit
atio
ns:
D
oes
not
incl
ude
cult
ural
or
med
ia in
flue
nces
.
44
Tab
le 1
. C
onti
nued
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

Health Literacy Skills Framework 45
Health Outcomes
How the frameworks specify health outcomes is another key difference among them. Some frameworks identify no specific health outcomes (Baker, 2006; Paasche-Orlow & Wolf, 2007), while others include multiple levels of health outcomes. Whereas some frameworks include morbidity and mortality as outcomes (Nutbeam, 2000), others only consider mediators such as health behaviors and use of health services as outcomes (Sørensen et al., 2012; von Wagner et al., 2009). However, some frameworks include both types of outcomes (Lee et al., 2004; Manganello, 2008; Rootman et al., 2002; Schillinger, 2001; Sørensen et al., 2012).
Societal Influences
In addition to individual-level factors, societal influences (e.g., culture, community, and media) are also included in different places in the frameworks. Sometimes they are included as moderators (e.g., Sørensen et al., 2012; von Wagner et al., 2009) and other times they are presented as mediators (e.g., Baker, 2006). Most frameworks demonstrate the effect of societal influences in both parts of the model (Lee et al., 2004; Paasche-Orlow & Wolf, 2007; Mancuso, 2008; Manganello, 2008; Nutbeam, 2000; Rootman et al., 2002; Sørensen et al., 2012). Societal factors likely exert an influence in both areas as they not only affect the extent and development of health literacy skills, but they also influence how they are applied in health care systems and interactions with health care providers. This presents a challenge to disentangling effects and confirming direct causal pathways.
Strengths and Limitations of Existing Frameworks
Each framework provides a unique contribution to developing a theoretical base for the development and influence of health literacy skills on health-related outcomes. While there are constructs that are consistently included in the frameworks we reviewed, how each relates to health literacy and health outcomes varies. The frameworks also vary in terms of what they are trying to explain (e.g., how skills are acquired versus how the application of skills affects health behaviors and other outcomes) and in terms of context as some are void of context and present health literacy skills and health outcomes very generally (Baker, 2006; Lee et al., 2004; Nutbeam, 2000; Rootman et al., 2002; Sørensen et al., 2012), while others present the application of health literacy skills specific to interactions within health care settings (e.g., Paasche-Orlow & Wolf, 2007). To date, most of the health literacy frameworks discussed do not appear to have been tested empirically to determine if the proposed relations, moderators, and mediators are accurate (Sørensen et al., 2012). As some frameworks do not define outcomes, testing these frameworks is difficult. In addition, many frameworks do not clarify how included constructs, such as mass media or patient-centered care, would be operationalized to test the framework.
Development of the HLS Conceptual Framework
Even though a number of frameworks for health literacy exist, there is no widely agreed upon framework for health literacy (Nielsen-Bohlman et al., 2004).
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

46 L. Squiers et al.
We used findings from our review of existing frameworks (Baker, 2006; Mancuso, 2008; Nutbeam, 2000; Paasche-Orlow & Wolf, 2007; Schillinger, 2001; Zarcodoolas et al., 2005) to inform the development of a conceptual framework explaining how individuals acquire and apply health literacy skills and how health behaviors and outcomes are affected by health literacy skills. To create our conceptual framework, we took Paasche-Orlow and Wolf ’s (2007) invitation to build on their framework and on other earlier frameworks, and we also employed a socioecological perspective (Stokoles, 1992) under the assumption that health literacy is a social and dynamic construction (Pleasant et al., 2009). This perspective recognizes external factors that influence an individual’s exposure to and cognitive processing and understanding of health-related information. In addition, this framework describes the relation between health literacy, comprehension of health information, health behaviors, and outcomes and incorporates concepts from health behavior theories by explicitly positioning a set of mediators between comprehension and health behavior.
Sørensen and colleagues (2012) recently reviewed health literacy definitions and models and developed an integrated conceptual model of health literacy that strives to bridge the gap between “medical” and “public health” literacy models. Their model is useful in providing a macro-level view of the domains and contexts in which health literacy operates and both supports and complements the HLS conceptual framework. The HLS framework depicts in more detail how an individual may respond to health-related stimuli by identifying clear pathways that can be empirically tested.
Three frameworks had the greatest influence on the development of the HLS conceptual framework presented in this article. Namely, Paasche-Orlow and Wolf (2007), Manganello (2008), and Baker (2006) each presented frameworks of health literacy that served as a basis for the development of a more comprehensive representation of the constructs that are related to the acquisition and utilization of health literacy skills. Our framework sought to simplify a multitude of complex relations, while also elucidating the nature of causation, with some variables operating as mediators and others as moderators. We hope this framework can serve as a springboard for further discussion and advancement in operationalizing this complex construct.
We developed the HLS conceptual framework to describe factors that influence an individual’s development of health literacy skills, how health literacy skills influence comprehension, and how comprehension and a variety of other influencing agents (e.g., community, health care system, media, and family) affect variables that are associated with health-related outcomes. In addition, the framework presents a variety of different types of variables that have been shown to affect health-related outcomes as mediators to health literacy. To establish theoretical linkages between these constructs, we drew from extant literature that lends support to the proposed causal pathways.
The HLS conceptual framework (see Figure 1) hypothesizes the relations between health literacy and health-related outcomes and illustrates how health literacy functions at the level of the individual, while acknowledging that factors external to the individual (e.g., family, setting, community, culture, and media) influence all relations represented in the framework. It is organized into four primary components: (a) factors that influence the development and use of health literacy skills, (b) health-related stimulus, (c) health literacy skills needed to comprehend the stimulus and
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13
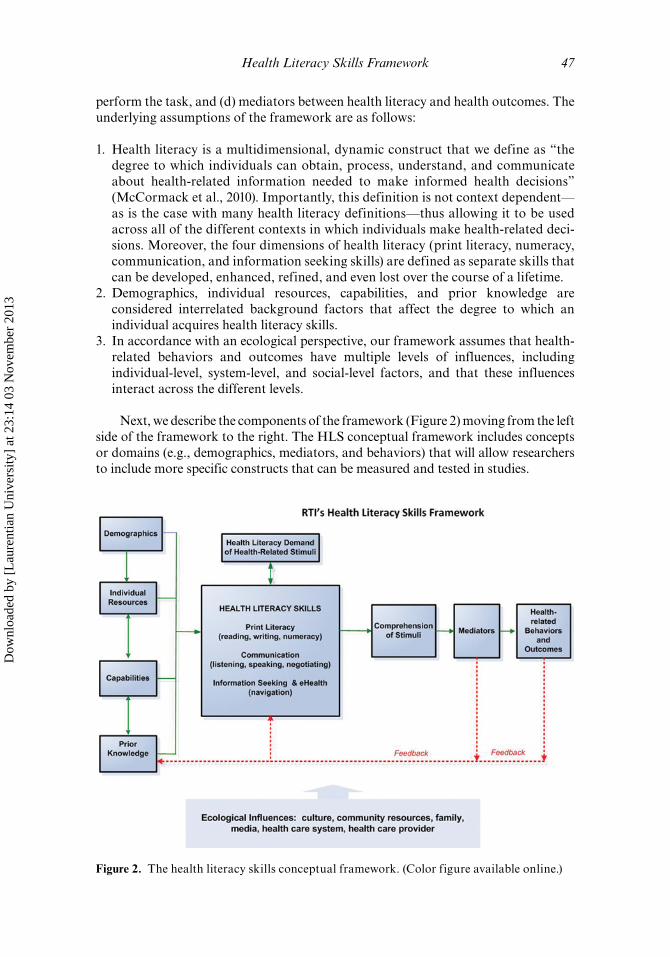
Health Literacy Skills Framework 47
perform the task, and (d) mediators between health literacy and health outcomes. The underlying assumptions of the framework are as follows:
1. Health literacy is a multidimensional, dynamic construct that we define as “the degree to which individuals can obtain, process, understand, and communicate about health-related information needed to make informed health decisions” (McCormack et al., 2010). Importantly, this definition is not context dependent—as is the case with many health literacy definitions—thus allowing it to be used across all of the different contexts in which individuals make health-related deci-sions. Moreover, the four dimensions of health literacy (print literacy, numeracy, communication, and information seeking skills) are defined as separate skills that can be developed, enhanced, refined, and even lost over the course of a lifetime.
2. Demographics, individual resources, capabilities, and prior knowledge are considered interrelated background factors that affect the degree to which an individual acquires health literacy skills.
3. In accordance with an ecological perspective, our framework assumes that health-related behaviors and outcomes have multiple levels of influences, including individual-level, system-level, and social-level factors, and that these influences interact across the different levels.
Next, we describe the components of the framework (Figure 2) moving from the left side of the framework to the right. The HLS conceptual framework includes concepts or domains (e.g., demographics, mediators, and behaviors) that will allow researchers to include more specific constructs that can be measured and tested in studies.
Figure 2. The health literacy skills conceptual framework. (Color figure available online.)
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

48 L. Squiers et al.
Factors That Influence the Development and Use of Health Literacy Skills
Our framework acknowledges the interdependence of various background factors and posits that these factors influence health-related behaviors and outcomes directly and indirectly. We hypothesize that demographic characteristics (e.g., age, race and ethnicity, income, and gender), prior knowledge (e.g., disease and illness experiences, conceptual knowledge of health and health care, and familiarity with health care vocabulary), resources (e.g., employment/occupation, social support, culture, language, literacy, and education), and capabilities (e.g., vision, hearing, verbal ability, memory, and cognitive functioning) influence the degree to which an individual develops, refines, and uses health literacy skills.
As described by Baker (2006), we believe that prior knowledge of the health topic influences the degree to which health literacy skills need to be used to understand a stimulus. For example, someone with more conceptual knowledge of health (e.g., how the body works, how bacteria can cause infection) will find it easier to understand a stimulus that references their current knowledge base. Consequently, prior knowledge influences an individual’s ability to develop and utilize their health literacy skills to encode, store, and retrieve information (Lang, 2006).
Health Literacy Skills Needed to Comprehend the Stimuli and Perform the Task
To be able to obtain, process, understand, and communicate about health information, individuals must use a variety of skills. We specify print literacy, numeracy, communication, and information-seeking skills in the framework. Being able to navigate search engines and websites has become increasingly important as 74% of Americans use the Internet and, in 2008, 61% of these Internet users looked for health or medical information online (Fox & Jones, 2009). However, individuals not only need to be able to navigate websites, but to navigate through other stimuli such as print materials (e.g., brochures, fact sheets, and booklets). Sometimes referred to as reading fluency, print literacy is the ability to process written materials and includes the ability to read and understand text (prose literacy) and the ability to locate and use information in documents (document literacy; Baker, 2006). Numeracy skills are defined as the ability to apply arithmetic operations and the use of numerical information in printed materials; it is sometimes referred to as quantitative literacy (Baker, 2006; Rothman, Montori, Cherrington, & Pignone, 2008). As health information is often conveyed orally, especially during medical visits, communication skills are important in obtaining and sharing health information and include the ability to listen, speak, and negotiate. These dimensions of health literacy contribute independently to the overarching construct of health literacy skills.
Demand of Health-Related Stimulus
The HLS conceptual framework incorporates health-related stimuli that people receive in their daily life (e.g., a brochure, a prescription label, and a conversation with a doctor). When individuals encounter stimuli, they select the important parts of the messages to encode. Health literacy skills interact with characteristics of stimuli to influence how well they are encoded, stored, and retrieved, which affects
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

Health Literacy Skills Framework 49
comprehension of the messages, their assimilation into an individual’s current knowledge base use, and their use in decision making (Lang, 2006).
Health literacy demand is defined as the complexity and difficulty of a stimulus. According to our framework, after exposure to a stimulus, the health literacy demand of the stimulus interacts with a person’s health literacy skills to influence comprehension of the message.
In addition to the sheer number and frequency of stimuli exposure, there are three important message characteristics that need to be considered when determining the health literacy demand of a message: communication channel, message content, and message source (Zarcadoolas, 2010). In terms of the communication channel, health-related stimuli can be transmitted through interpersonal or mediated channels. Within mediated channels, there are also a number of formats to convey health information, such as print materials, audio recordings, video presentations, radio announcements, and so forth.
The content of the message can also vary in terms of language (e.g., plain language versus jargon and complex versus simple messages) and orientation (e.g., health promoting versus disease prevention, costs versus benefits, use of fear appeals, and narrative versus non-narrative). Decisions regarding the orientation of the message and the language used have important implications for comprehension (Rothman, Mano, Bedell, Detweiler, & Salovey, 1999).
Last, the source of the message, or the messenger, also plays a major role in influencing an individual’s ability to process health information. In terms of interpersonal communication (e.g., between a doctor and patient) the communication skills of the messenger are critical to an individual’s skill in interpreting the message being delivered. In addition, the relation of messenger to recipient can also influence comprehension of the stimuli (e.g., family member, friend, or doctor). Credibility of the messenger has been cited as being crucial in the public’s trust of health information and messages (Hesse et al., 2005; Nelson, Hesse & Croyle, 2009).
Comprehension of the Stimuli
Comprehension involves learning what to do as well as how to do it (i.e., skill acquisition (McGuire, 2001)). We conceptualize comprehension of the stimuli or health information as a primary indicator of health literacy that is moderated by the health literacy demand of the stimulus. This framework supports the tenet that although comprehension is essential, it is often not sufficient to affect health outcomes (e.g., behaviors such as exercise, healthy eating, and drug use) and health status (e.g., morbidity, mortality, and health, or well-being) directly. While health literacy skills and message characteristics determine what someone will learn from a stimulus, mediating factors affect whether they will accept or adopt what they learn. Here, the basic assumption is that the effects of a stimulus depend on two factors: comprehension of the message and acceptance of what is learned (McGuire, 1968).
Other Mediating Factors Between Health Literacy and Health Outcomes
Mediating factors affect whether people retain, retrieve, and decide to use the information in the stimulus when making health-related decisions. While research has found that there is a direct relation between an individual’s health literacy skills and
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

50 L. Squiers et al.
his or her health outcomes (Berkman et al., 2010), many factors may also mediate this relation including health status, attitudes, emotions, motivation, and self-efficacy, which are further affected by ecological influences (e.g., culture, social support, community health care resources, the media, and access to health care resources including health insurance). Depending on the specific health behavior and outcome of interest, numerous mediators could potentially influence the relation between comprehension of a stimuli and health behaviors (e.g., motivation, attitude toward/perceived effectiveness of the behavior, fatalism, and decision-making skills).
Although it is tempting to want to identify someone as being “health literate” if they demonstrate a desired behavior (e.g., quitting smoking), there are far too many mediating factors that influence whether or not an individual engages in a behavior or has a positive health outcome to be able make this direct association. For example, an individual may understand that smoking can cause lung cancer, but may not have the motivation, health care, or social support to quit. Thus, a smoker may very well comprehend the health message but is not be able to act on it for other reasons. Other types of mediators include social support, decision-making skills, access to health care, trust in information/source/stimulus, fatalism, and perceived relevance of the message.
Health-Related Behaviors and Outcomes
The HLS conceptual framework includes two large categories that represent the application of health literacy skills: health-related behaviors (e.g., smoking, exercise, or medication adherence) and health status or outcomes (e.g., morbidity/mortality, disease state, health care service utilization, quality of life, or health/well-being).
Ecological Moderators
Our framework posits there are a variety of ecological influences (e.g., culture, community resources, family, media, health care system, and health care providers) that can moderate components of the conceptual framework in various ways. Health system-level moderators are generally believed to influence the relation between health literacy and health outcomes, but can also affect health literacy development (e.g., see Manganello, 2008; Paasche-Orlow & Wolf, 2007). Last, societal-level moderators include the environment, cultural differences, and access to different types of media, and can influence health literacy and health outcomes (e.g., see Mancuso, 2008; Manganello, 2008; Nutbeam, 2000).The dotted arrow in Figure 1 represents a feedback loop and shows that health behaviors and health status influence mediators, health literacy skills, and knowledge. This feedback supports the idea that health literacy skills are dynamic, and that as individuals interact with health-related stimuli, skills are learned or unlearned, reinforced, or degraded. In addition, the framework represents how health literacy skills can both develop and deteriorate as individuals’ capabilities such as vision, hearing, and cognitive capacity change over time.
Discussion
Theoretical frameworks that advance our understanding of health literacy and how it relates to health-service use and health outcomes are clearly needed (Pleasant et al., 2011). Theoretical frameworks provide the necessary basis for reliable measurement
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

Health Literacy Skills Framework 51
and the development of interventions to improve health literacy. Yet, current frameworks are limited because they often present only part of the causal pathway (moderators to health literacy skills, or health literacy skills to outcomes) rather than reflect the full continuum that includes both the acquisition and application of health literacy skills. The HLS conceptual framework offers another perspective about conceptualizing the complex interrelations between the myriad of factors that influence and are influenced by health literacy. It is distinct from other models because it illustrates how health literacy skills influence comprehension of a health-related stimuli and that health literacy’s effect on health-related behaviors and outcomes is mediated by a variety of constructs (e.g., emotions, perceived norms, motivation, self-efficacy, access to health care, and perceived relevance of the message).
We propose the HLS conceptual framework as a springboard for further exploration of the relations between the various elements of health literacy and to encourage additional research such as
• empirically testing the framework; • identifying the degree to which demographic variables, resources, capabilities,
and prior knowledge affect individuals’ health literacy skills;• investigating the degree to which health literacy skills influence different media-
tors and outcomes; and• determining the pathway(s) through which health literacy skills affect different
health-related behaviors directly or indirectly (through certain mediators).
Future studies could apply the conceptual framework to a single health behavior (e.g., diabetes management) or more globally (e.g., health-lifestyle behaviors) to help assess its utility in different contexts. In addition, investigating how experiences with health and health care can influence development, enhancement, and application of health literacy skills is needed.
The conceptual framework can be used to guide the development of interventions to improve the health literacy of individuals. The framework identifies barriers to acquiring health literacy skills (e.g., individual resources such as social support, language, and general literacy; capabilities such as memory, cognitive functioning, vision, and hearing), which can provide insight for health care systems interested in self-assessment. The HLS framework can inform the development of strategies to improve access to health information and navigation of the health care system. For example, if a health care system designed strategies for overcoming certain barriers, the effect of these strategies could be assessed by measuring health literacy skills, mediators, and relevant outcomes before and after the strategies have been implemented.
While the HLS conceptual framework advances current theoretical frameworks of health literacy by including both the determinants and outcomes of health literacy, it is not without limitations. To make the HLS conceptual framework applicable across health topics and behaviors, we did not include the universe of the potential mediators and moderators to health literacy and outcomes. Rather, we included these as conceptual categories that will allow researchers to include the specific mediators, moderators, and outcomes that are relevant to their particular research question. However, this lack of specificity may in fact limit the utility of the framework for some researchers.
In addition, the framework does not address key measurement issues that could affect the assessment of the underlying dimensions of health literacy skills (see
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

52 L. Squiers et al.
McCormack et al., 2010). Using valid and reliable measures of health literacy skills will be vital to testing the conceptual framework. McCormack and colleagues (2010) developed the Health Literacy Skills Instrument, which assesses three domains of health literacy: print literacy, oral health literacy (listening skills only), and Internet information-seeking skills. In terms of content domains, it reflects health-related issues across the life course for health promotion and disease prevention, health care maintenance and treatment, and health system navigation. The Health Literacy Skills Instrument can be self-administered via a computer, which can reduce data collection costs and minimize potential discomfort or embarrassment among participants. The instrument can be accessed at http://www.rti.org/page.cfm?objectid=66F893E4-5056-B100-OC834F234F368198. Measuring prior knowledge will also be important in testing the HLS conceptual framework. For example, if a study or intervention focuses on cardiovascular disease, specific knowledge of this health issue should be assessed. To fully test the HLS conceptual framework in the general population, individuals’ broader conceptual knowledge of health and science should be assessed.
Research to more thoroughly investigate how age and culture influence the acquisition and application of health literacy skills will also advance the field by helping to identify where interventions can be most effective. For example, studies can be designed to determine whether community-based or system-based interventions that address issues related to the acquisition of health literacy skills are more effective than interventions that focus on enhancing individuals’ use of health literacy skills (e.g., interventions that focus on enhancing self-efficacy). Last, learning how to develop and/or adapt educational materials and messages so that those with different levels of health literacy skills can use the health information to make informed health decisions is paramount to addressing health disparities in our nation. The HLS conceptual framework is a first step toward developing a framework that can guide these efforts.
References
Baker, D. W. (2006). The meaning and measure of health literacy. Journal of General Internal Medicine, 21, 878–883.
Baron, R., & Kenny, D. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182.
Berkman, N., Davis, T., & McCormack, L. (2010). Health literacy: What is it? Journal of Health Communication, 15 (Suppl. 2.), 9–19.
Campbell, F. A., Goldman, B. D., Boccia, M. L., & Skinner, M. (2004). The effect of format modifications and reading comprehension on recall of informed consent information by low-income parents: A comparison of print, video, and computer-based presentations. Patient Education and Counseling, 53, 205–216.
DeWalt, D., Berkman, N., Sheridan, S., Lohr, K., & Pignone, M. (2004) Literacy and health outcomes: A systematic review of the literature. Journal of General Internal Medicine, 19, 1228–1239.
Fox, S., & Jones, S. (2009). The social life of health information. Washington, DC: Pew Internet & American Life Project. Retrieved from http://www.pewinternet.org/~/media//Files/Reports/2009/PIP_Health_2009.pdf
Hesse, B., Nelson, D., Kreps, G., Croyle, R., Arora, N., Rimer, B., & Viswanath, K. (2005). Trust and sources of health information: The impact of the Internet and its implications for health care providers: Findings from the first Health Information National Trends Study. Arhives of Internal Medicine, 165, 2618–2624.
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

Health Literacy Skills Framework 53
Kraemer, H., Wilson, T., Fairburn, C., & Agras, W. (2002). Mediators and moderators of treatment effects in randomized clinical trials. Archives of General Psychiatry, 59, 877–883.
Lang, A. (2006). Using the limited capacity model of motivated mediated message processing to design effective cancer communication messages. Journal of Communication, 56(Suppl. 1.), S57–S80.
Lee, S., Arozullah, A., & Cho, Y. (2004). Health literacy, social support, and health: A research agenda. Social Science and Medicine, 58, 1309–1321.
Mancuso, J. M. (2008). Health literacy: A concept/dimensional analysis. Nursing and Health Sciences, 10, 248–255.
Manganello, J. A. (2008). Health literacy and adolescents: A framework and agenda for future research. Health Education Research, 23, 840–847.
McCormack, L., Bann, C., Squiers, L., Berkman, N., Squire, C., Schillinger, D., Hibbard, J., … (2010). Measuring health literacy: A pilot study of a new skills-based instrument. Journal of Health Communication, 15(Suppl 2), 51–71.
McGuire, W. J. (2001). Input and output variables currently promising for constructing persuasive communications. In R. E. Rice & C. K. Atkin (Eds.), Public communication campaigns (3rd ed., pp. 22–48). Thousand Oaks, CA: Sage.
McGuire, W. J. (1968). Theory of the structure of human thought. In R.P. Abelson, E. Aronson, W. J. McGuire, T. M. Newcomb, M. J. Rosenberg, & P. H. Tannenbaum (Eds.), Theories of Cognitive Consistency: A Sourcebook (pp. 140–162), Chicago, IL: Rand McNally.
Nelson, D. E., Hesse, B. W., & Croyle, R. T. (2009). Making Data Talk: Communicating Public Health Data to the Public, Policy Makers, and the Press. New York, NY: Oxford University Press.
Nielsen-Bohlman, L., Panzer, A., & Kindig, D. (2004). Health Literacy: A Prescription to End Confusion. Washington, DC: The National Academies Press.
Nutbeam, D. (2000). Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International, 15, 259–267.
Paasche-Orlow, M. K., & Wolf, M. S. (2007). The causal pathways linking health literacy to health outcomes. American Journal of Health Behavior, 31(Suppl. 1.), S19–S26.
Peerson, A., & Saunders, M. (2009). Health literacy revisited: What do we mean and why does it matter? Health Promotion International, 24, 285–296.
Pignone, M., DeWalt, D., Sheridan, S., Berkman, N., & Lohr, K. (2005). Interventions to improve health outcomes for patients with low literacy: A systematic review. Journal of General Internal Medicine, 20, 185–192.
Pleasant, A., McKinney, J., & Rickard, R. (2011). Health literacy measurement: A proposed research agenda. Journal of Health Communication, 16(Suppl. 3), 11–21.
Rootman, I., Gordon-El-Bihbety, D., Frankish, J., Hemming, H., Kaszap, M., Langille, L., Quantz, D., & Ronson, B. (2002). National literacy and health research program needs assessment and environmental scan. Ottawa, ON: Canadian Public Health Association. Retrieved from http://www.cpha.ca/uploads/portals/h-l/needs_e.pdf
Rothman, A. J., Mano, S. C., Bedell, B. T., Detweiler, J. B., & Salovey, P. (1999). The systematic influence of gain and loss-framed messages on interest in and use of different types of health behavior. Personality and Social Psychology Bulletin, 25, 1355–1369.
Rothman, R. L., Montori, V. M., Cherrington, A., & Pignone, M. P. (2008). Perspective: The role of numeracy in health care. Journal of Health Communication, 13, 583–595.
Schillinger, D. (2001). Improving the quality of chronic disease management for populations with low functional health literacy: A call to action. Disease Management, 4, 103–109.
Sørensen, K., Van den Broucke, S., Fullam, J., Doyle, G., Pelikan, J., Slonska, Z., & Brand, H. (2012). Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health, 12: 80. Retrieved from http://www.biomedcentral.com/1471-2458/12/80
Stokoles, D. (1992). Establishing and maintaining healthy environments: Toward a social ecology of health promotion. American Psychologist, 47, 6–22.
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13

54 L. Squiers et al.
U.S. Department of Health and Human Services. (2010). National action plan to improve health literacy. Washington, DC: Author. Retrieved from http://health.gov/communication/HLActionPlan/
Vahabi, M. (2007). The impact of health communication on health-related decision making: A review of evidence. Health Education, 107, 27–41.
von Wagner, C., Steptoe, A., Wolf, M. S., & Wardle, J. (2009). Health literacy and health actions: A review and a framework from health psychology. Health Education & Behavior, 36, 860–877.
Zarcadoolas, C. (2010). The simplicity complex: Exploring simplified messages in a complex world. Health Promotional International, 26, 338–350.
Zarcadoolas, C., Pleasant, A., & Greer, D. (2005). Understanding health literacy: An expanded model. Health Promotion International, 20, 195–203.
Dow
nloa
ded
by [
Lau
rent
ian
Uni
vers
ity]
at 2
3:14
03
Nov
embe
r 20
13