Embed Size (px)
Citation preview

The Health Franchise Initiative
May, 2004
Gijs Elzinga & Dominic Montagu
Gijs.elzinga@rivn [email protected]

2
Overview
• HFI introduction
• Selected Countries
• Operations of the Franchise
• Target Population
• Roll-out plans and cost
• Organization plan
• Timeline of activities

The Private Sector in HealthcarePrivate Expenditure on healthcare:
– Indonesia, 83% of all healthcare expenditure is private
– Kenya, 53%
– India, 70+%
Private Consultations:
– Vietnam, 60% of physician consultations in private sector
– Pakistan, 80%
Exclusively Private as % of all doctors:
– Nigeria, 78%– Malawi, 21%

# clinics in 5 years
National Population
Pop. Covered by Franchise
% of Pop HIV+
TB incidence
Kenya 525 31,293,000 10,500,000 8.0% 0.51%
Tanzania 600 35,965,000 12,000,000 4.2% 0.34%
Uganda 400 24,023,000 8,000,000 2.5% 0.32%
Nigeria 2000 116,929,000 40,000,000 3.0% 0.24%
Cameroon 250 15,203,000 5,000,000 6.1% 0.15%
Malawi 200 11,572,000 4,000,000 7.3% 0.43%
Zambia 200 10,649,000 4,000,000 11.3% 0.65%
Country Selection
4175 83,500,000

5
Operation 1: Overview
Franchisees:–Nurses and clinical officers–Urban slum, peri-urban, dense rural–Full time private practice
Services:–General practice–Essential drugs–TB diagnosis and treatment–HIV testing–HIV opportunistic infection treatment–ART

Operation 2:Drug Supply
• Quality generics for general meds• Global Drug Facility • ARV supplies uncertain
• Suppliers– MEDS– UNICEF – Crown Agents– International Dispensary Association (IDA)
Drug Supply Steps Product selection
Product registration
Forecasting
Funding
Acquisition
Shipment to country
Assembly in country
Storage
Security
In-country transportation
In-store managementFinal use by prescribers/patients
Key components Reliability
Flexibility
Scalability

Operation 3: Training
• Competency Based Training (CBT) • Certification • Collaboration
– DOTS
– ART management
– counseling
–Kenya and Tanzania:
Preparation• Needs Assessment
Training Modules1: Franchise management
2: Drug management
3: Financial management
4: Public Health
5: Clinical TB care
6: Clinical HIV/AIDS care
7 on ARV delivery
• NTLP• NAC• FHI Kenya• Moi University, Eldoret• Aga Khan Hospital
• Mildmay International• Kenya Assoc. of Professional Counselors• Network of Researchers in Eastern and Southern Africa

Operation 4: TBTable of Contents
of the technical policy document for TB:1. Introduction
1.1. Basic understanding of tuberculosis epidemiology
1.2. Tuberculosis and HIV
1.3. Basic understanding of pathology
1.4. The DOTS strategy for tuberculosis control
1.5. The National TB control program
2. Diagnosis of pulmonary tuberculosis in adults
2.1 Diagnostic approach
2.2. Clinical features
2.3. Sputum smear microscopy
2.4. Differential diagnosis of pulmonary TB
2.5. Chest X-rays in diagnosis
2.6. Culture and drug sensitivity testing
2.7. Biopsy
3. Diagnosis of pulmonary tuberculosis in children
4. Diagnosis of extra-pulmonary TB, adults & children
5. StandardizedTB case def. & treatment categories
5.1. Standardizedcase definitions
5.2. Category of patient for registration on diagnosis
5.3. Standardizedtreatment categories
6. Management of patients with tuberculosis
6.1. Anti-TB drugs
6.2. TB treatment regimens
6.2.1. New cases
6.2.2. Re-treatment cases
6.2.3. Children
6.2.4. Special situations: pregnancy, breast-feeding women, renal failure, liver disease
6.3. TB treatment for HIV infected persons
6.4. Monitoring of TB patients during treatment
6.5. Directly observed therapy (DOT)
6.6. Tracing of patients who interrupt treatment
7. Side effects of anti-TB drugs
7.1. Minor and major side-effects
7.2. Prevention of side effects
7.3. How to manage drug reactions and when to refer
8. TB/HIV co-infection and disease
8.1. HIV testing and counselling
8.2. Management of Opportunistic Infections
8.3. Cotrimoxazol preventive therapy (CPT)
8.4. Anti-retroviral therapy
8.5. Home based-care
9. Multi-Drug resistant tuberculosis
10. Communication & education of the patient & family
10.1. Confidentiality
11. When to refer a patient
12. Recording, reporting and notification
PTb testing $0.50
Active Tb treatment $4.00
Weekly drug re-supply free
Ancillary care/counseling free
Collection on-site by provider/ franchise staffTesting in DOTS-certified lab - 2 tests, then refer for x-ray
If positive: printed material and counseling about available government services (if any)
If non-compliance household follow-up by franchise-employed nurse
Successful treatment$15 bonus to provider
$4 bonus to client

Operation 5: HIV OIs
• Continuing Education– Initiation
– 4 times / year
• HIV testing
• Prophylaxis– CPT
– IPT for established patients
• Referral to cooperating hospital and/or consulting physician
Table of Contents
of the technical policy document for HIV/AIDS:1. Background information
1.1. HIV and AIDS
1.2. HIV/AIDS epidemiology
1.3. HIV Transmission
1.4. Prevention of HIV transmission in health units
1.5. Immuno-pathogenesis of HIV infection
1.6. Natural history of HIV infection
1.7. AIDS
1.8. WHO case definitions for AIDS where HIV testing is not available
1.9. WHO staging system for persons who are HIV-seropositive
2. Diagnosis and management of Opportunistic Infections
3. Tuberculosis infection & disease in HIV+ individuals
3.1. Intensified case finding of tuberculosis disease
3.2. Isoniazid preventive therapy (IPT)
4. Antiretroviral therapy for treatment of HIV infection
4.1. Antiretroviral drugs
4.2. Principles of antiretroviral therapy
4.3. Initiation of antiretroviral therapy
4.4. Adults and adolescents with documented HIV infection
4.5. Infants and children
4.6. Doses of ARVs in adults and adolescents
4.7. Doses of ARVs in children
4.8. Choice of ARV treatment regimen
4.9. Adults
4.10. Children
4.11. Monitoring antiretroviral therapy
4.12. Side-effects
4.13. Interactions between ARV drugs and other drugs
4.14. Antiretroviral drugs and TB treatment
4.15. Drug interactions
4.16. Treating TB and HIV together
4.17. Immune reconstitution syndrome
4.18. Options for ARV treatment in TB patients
5. Prevention of Mother To Child transmission
6. HIV/AIDS care services
6.1. Home and community care
6.2. Primary care
6.3. Secondary care
6.4. Tertiary care
7. Communication and patient education
7.1. HIV testing and counselling
7.2. Confidentiality
7.3. Supporting the patient and his family
8. Recording, reporting, notification

Operation 6: ART
• Phase 1: Govt & Mission Hospital– HIV testing, CD4 tracking, initiation of ART
– Franchisees: ARV supply and treatment support
• Phase 2: NFO Consulting Physicians– CD4 tracking, initiation of ART
– Franchisees: HIV testing, ARV supply & treatment support
• Phase 3: CO & Nurse delivery of ART– Franchisees: HIV testing, initiation of ART, ARV supply & treatment support, patient ed. & adherence support
– consulting physician supervision
Consulting Physicians• Initiation of ART• patient record tracking• referrals
Collaboration with
local community-based
NGOs for:1: VCT
2: Patient education
3: Patient identification
4: Pre-ARV counseling
5: Adherence support

11
Operation 7: quality
• Inputs– Medicine, stockage, timing– Equipement– Facility
• Providers– Selection– Training at start-up– Continuing ed
• Processes– External testing– Multi-system monitoring (MIS, random checks, mystery
clients)– Patient follow-up– Regular support
• Control of assets

12
Clients
• Demographics– 3rd and 4th SES quintiles– Slums & dense rural areas (eg. Kibera or Nyanza)
• Price of services– General consultation $0.20-$0.50– TB testing $0.50– TB drugs free– TB consultation and care $4.00– Opportunistic Infections according to disease– HIV testing $0.50– AIDS-related tests free– ARV free– ART $0.40/ weekly visit ~ $20/yr
Special support -TB5% of all TB and clients can be treated free of care, with the franchise reimbursing the provider for fees equivalent to what would have been paid
Special support -ARTVouchers for free care will be available for up to 10% of ART clients. Vouchers given by initiating physician, and collected as payment by franchisees

13
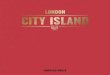
Number of clinics
-
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7
MalawiZambiaNigeriaCameroonUgandaTanzaniaKenya
PHASE 1 PHASE 2 Continuation

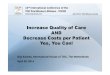
14$0
$2,000,000
$4,000,000
$6,000,000
$8,000,000
$10,000,000
$12,000,000
$14,000,000
$16,000,000
Year 1 Year 2 Year 3 Year 4 Year 5 year 6 year 7
Malawi
Zambia
Nigeria
Cameroon
Uganda
Tanzania
Kenya
HFI expense
SubsidyPHASE 1 PHASE 2 Continuation

HFI
Organizational and operational development

16
Four Steps
1. Secure funding start-upsNairobi meeting June/July
2. Temporary housingFollowing June/July meeting
3. Growing independentAfter implementation start-ups
4. Scale upBased on evaluation start-ups
PHASE 2
PHASE 1

17
Board of key stakeholders
Internationalfranchiser
MAC FAC
Nationalfranchiser
FFF FF
FF
FF
FF
Nationalfranchiser
Nationalfranchiser
Nationalfranchiser
NTPNAC
Nationalfranchiser
Oversight, quality, and reporting
Structure

18
Before 30-06-04
a. Organizational clarity: roles, rules and responsibilities.
b. Financial transparency: structure & legal and fiscal implications.
c. M&E: content and finances & timing with go/no-go’s.
Selection of
these elements
is following the
advice of the
Price Waterhouse
Coopers Global
Risk Management
Group in The Netherlands.

19
Organizational clarity
done/in process• overall structure• overall functions• brand development• selection of host• full support Kenya &
Tanzania• high potentials interest
to do• tasks & responsibilities• national franchiser
capabilities• code of conduct• host arrangement
(MoU)• dispute & termination
clauses
For the execution of phase I and 2, that is the period before the real franchise is established, the development of a temporary Dutch foundation is recommended.

20
done/in process• financial incentive
structure of service provision
• cost estimates, cost-efficiencies
• funding required
to do• overall financial
structure and flows• fiscal/legal challenges
and solutions• responsibilities and
liabilities
Financial transparency
The final home country of the international component of the franchise depends on a number of considerations. One thereof are the legal and financial consequences of the preferred country.

21
M&E
For a well focused and close to real time M&E process, a tailor made management and information system (MIS) is essential.
done/in process• Identification and
specification of M&E components
• Go/no-go decision points and the timing thereof
to do• Organizational and
operational M&E components
• Reporting scheme of financial & operational variables for funding agencies

• MIS prior to operation (phase 2), • Qualitative evaluation at 12 months• Impact Evaluation - clients• Operations evaluation - organization• Impact evaluation - population
preparation 0 12 24 36 48 60
MIS
Process Evaluation
Qualitative evaluation
ImpactEvaluation: clients
Impact Evaluation on client health outcomes
Impact Evaluation: population
Impact Evaluation on community health outcomes
MIS data on providers and clients begins to be collected, ongoing, monthly
Community-level survey on access to
healthcare using DHS
instruments
Timeline: months
OperationsEvaluation onorganization
M&E
OperationsEvaluation

23
Timeline & go/no-go’s
• $8 M funding secured• formal countrysupport
• Start Start-ups• Activate MoUwith host
Go/no go conditions
Activities
• qualitative evaluation positive
• $ 100 M funding secured• impact & operational evaluation positive
• Establish independent organization
• Scale up to 7 countries
12 months 24 months
PHASE 1 PHASE 2

24
Before 30-06-04
• “done/in process” items completed by HFI team, GAG , and MAG
• “to do list” items executed by consultancy firm
- - -
• Price Waterhouse Coopers proposal:116 k euro (ex VAT)
• funding of this essential to avoid “Catch 22”

end
Additions to the ‘to do before 30-04’ list welcome !!

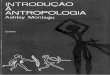
Acute respiratory infection and
treatment <5, 10 countries
0%
10%
20%
30%
40%
50%
60%
70%
poorest 2nd Q mid 4th Q richest0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Treated in the Private Sector
Treated in the Public Sector
Illness during previous 2 weeks (right hand axis)

Cameroon
Ethiopia
Malawi
Mozambique
Nigeria
Rwanda
Tanzania
Uganda
Burkina Faso NA
NA
NA
Country Existence of private
providers1
Geographic Dispersion
Legal status of private providers
Private providers legally prescribe
Government attitude on TB & ART franchising
SUMMARY OF IHSD COUNTRY REPORT
Country Selection
Kenya
Zambia
Footnote: 1. Private providers includes private sector doctors, nurses, clinical officers, lab technicians and pharmacists

Country Selection
Scale Existence of private providers
Geographic Dispersion
Legal status of private providers
Private providers legally prescribe
Government attitude on TB & ART franchising
KEY TO IHSD COUNTRY RANKINGS
0-10 providers per million
10-30 providers per million
30-60 providers per million
100-250 providers per million
60-100 providers per million
95% - 100% Urban
90% - 94% Urban
81% - 89% Urban
69% - 74% Urban
75% - 80% Urban
Franchise could function only with doctor oversight
Some restrictions on nurses but could operate franchise
No restrictions on nurses
NA
NA
Doctors, but not nurses, can prescribe
Nurses ability to prescribe limited
No restriction on nurses
NA
NANot interested in
franchising TB or ART
NA
Interested in franchising ART
but not TB
Interested in franchising ART and possibly TB
Interested in franchising ART
and TB