Embed Size (px)
Citation preview

THE HEALTH COST OF URBAN AIR POLLUTION IN COSTA RICA
1. Summary
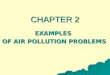
The health cost of urban air pollution in Costa Rica amounts to about 210 Bl. Colones, or around
1.1% of the national GDP in 2010. Mortality represents roughly 0.8% of the GDP and 69% of the
total social cost of this environmental risk (see Figure 1.1 below). Around 655 premature deaths
and close to 9,000 lost DALYs were attributable to urban air pollution (PM exposure).The health
damage of urban air pollution in the country is largely concentrated in the core of the Greater
Metropolitan Area (GMA) around San Jose, the capital.
Figure 1.1. Health cost of urban air pollution in Costa Rica as a percentage of GDP in 2010
Source: estimates by the authors
The GMA presents a high concentration of economic and commercial activity in a small area. Such
concentration, along with a fast rate of motorization, ageing vehicle fleet and abundant point
sources, entails difficult challenges for an effective air quality management of the area. However,
authorities have scaled up efforts towards an effective reduction of air pollutants, in particular
those related to mobile sources. In this regard, the “Program to improve air quality in the greater
metropolitan area of Costa Rica” (2008-2013) notes the efforts of the Costa Rican government in
the reduction of congestion and improvement of mass transit systems, along with other
governmental initiatives. The guiding principles of these initiatives have been mainly the
generation of reliable information on air pollution and the gradual reduction of pollutants to levels
compliant with national standards. As for the current lines of governmental action, these
encompass six main areas of work: 1) Emissions reductions from point sources 2) Public
participation 3) Clean transportation 4) Energy efficiency 5) Renewable energies and 6) Decision
support systems. Consistently, strong efforts are being made regarding monitoring and research.
The number or monitoring stations measuring PM10 in the GAM has increased from 2 in 2005 to 5

in 2008 and up to 14 in 2010. Authorities recognize, however, that much remains to be done, in
particular regarding the monitoring of mobile sources on the road.
These and previous efforts are paying off; from a reported annual average of 62 µg/m3 in 1997
(Alfaro 1998) concentrations of PM10 have gone down to values generally below the national
standards (50 µg/m3) in the last five years. The National University (UNA) is currently conducting a
comprehensive study on the environmental, social and economic effects of air pollution involving
data including comprehensive emission sources inventories, dispersion modeling, epidemiologic
surveillance, and complete economic valuations. This evidence base will likely prove highly
valuable as a baseline reference for expected gains of an effective air quality management in the
urban areas of Costa Rica.
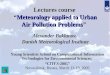
Similar analyses were conducted in several countries of Latin America and the Caribbean starting
in 2006 up until today, which could give some context for comparison of the findings of this report
(Figure 1.2).
Figure 1.2 Annual cost of urban air pollution as a proportion of GDP in selected LAC countries
Source: World Bank Environmental Assessment Studies, this report for Costa Rica.
The methodology in this report was shifted towards application of value of statistical life (VSL) only
for outdoor air pollution mortality valuation (as opposed to the average between human capital
approach and VSL in other studies). In the practice that means a higher value compared to the
combined HCA-VSL approach. On the other hand, no willingness-to-pay proxy was applied to the
calculation of the cost of illness of some health outcomes, which contributes to a comparatively
lower cost estimate for morbidity. A relatively high cost of hospitalization and of the value of time
lost may also contribute to explain the comparatively high health cost of urban air pollution.

2. The health impact of urban air pollution
Outdoor air pollution is a major environmental risk to public health, particularly in urban settings.
The evidence on the health effects of poor urban air quality worldwide has been substantial for
decades now, with extensive studies showing associations between certain pollutants and
respiratory and cardiovascular mortality, chronic bronchitis, respiratory infections and several
other related disorders. Of all common urban air pollutants, most studies show the strongest
association for inhalable particulate matter, specifically PM10 and PM2.5 (smaller than 10 and 2.5
microns in diameter, respectively). To the reviews by Ostro (1994) and Pope (2002, 2007) have
followed several comprehensive analyses (including cohort, case-crossover and meta-analysis
studies) involving multiple locations, mostly in Europe and North America (Samet et al. 2000).
Several large cohort studies have confirmed significant effects of inhalable particles on public
health, in different age groups (Eftim et al. 2008, Samet et al. 2007a, 2007b). A recent
comprehensive review (Brook et al. 2010) that pooled together many large scale studies on the
association between cardiovascular disease and PM confirmed that short-term exposure to PM2.5
can trigger health effects from mild to increased risk of cardiovascular disease-related premature
death, and that long term exposure increases the risk of cardiovascular mortality and reduces life
expectancy. Though not the only outcomes related to air pollution, cardiovascular and respiratory
health effects are the most important in magnitude and strength of the association. Besides the
well-established evidence in Europe and North America, a substantial body of evidence is now
available from cities in developing countries of Asia (E.g. HEI 2008) and, most importantly for this
update, from cities in Latin American countries (Gouveia et al. 2004, Martins et al. 2004, Bell et al.
2006, O´Neill et al. 2008, Bell et al. 2011, among others).
Inhalable particulate matter has the strongest effect of all common urban air pollutants and it is
used in this report as the environmental exposure representing urban air pollution in Costa Rica.
However, many other anthropogenic pollutants have proven to be associated with adverse health
outcomes, including (but not limited to) Sulphur oxides, Nitrogen oxides, Volatile organic
compounds, Lead, Carbon monoxide, and –notably- Ozone (USEPA 2011a). Tropospheric (I.e.
ground level) Ozone can trigger a large number of respiratory effects and aggravate certain
chronic diseases, thus increasing societally costly outcomes like increased healthcare usage or
absenteeism from work and school (USEPA 2011b). Moreover, an association between Ozone
concentrations and long term mortality has been found, albeit it was statistically significant only
when PM2.5 concentrations were taken into account (Jerrett et al. 2009). A detailed discussion on
the epidemiology of air pollution is beyond the scope of this report, and a large body of evidence
is widely available both in academic journals and in governmental sources worldwide. In general,
evidence shows that the strongest association and magnitude of effect in the interaction between
air pollutants and premature mortality/health is related to fine particulate matter, and in
particular the smallest diameter fraction. The analytical approach to the estimation of the damage
value of air pollution follows the same main steps used in most World Bank Country
Environmental Analyses including air pollution: 1) Identification of air pollutants and
determination of concentrations 2) Population exposed and their baseline vulnerability 3)

Calculation of the health impact of the exposure to air pollution based on epidemiologic
techniques and 4) Estimation of the value of that health impact.
3. Baseline population and dose-response coefficients
In Costa Rica, most of the population exposed to significant levels of urban air pollution lives in the
Greater Metropolitan Area (GMA), which represents only 4% of the national territory, but
concentrates more than 60% of the population along with roughly 75% of the vehicle fleet and a
large proportion of the industry (INEC 2011). As per consultations with the Costa Rican Ministry of
the Environment, the network of air pollution monitoring stations covers the majority of districts
within the GMA where air pollution is of significant concern, comprising 31 municipalities (see
Map 3.1.). The total population within this area amounts to roughly 2.3 Million people, a sizeable
proportion of the total national population of 4.3 Million. Some of these municipalities (notably
Heredia, Alajuela and Cartago) are on a net population growth path, largely based on internal
migration (INEC 2011). Overall, more than 65% of Costa Rica’s population lives in urban areas.
Map 3.1. Municipalities within the GMA covered in the analysis
Source: adapted from INEC data with ArcGIS™ 10.1

The inhalable particles exposure assessment is based on annual average data from fourteen
monitoring stations placed in nine municipalities within the GMA (4 in San Jose, 2 in Belen and 1
each in Heredia, Moravia, Santa Ana, Escazu, Heredia, Santo Domingo, Alajuela and Cartago). We
pondered measurements by exposure category based on simple interpolation (Kriging and Inverse
Distance Weighting). Results are summarized in Table 3.1. A complete dispersion modeling would
be appropriate in this case, but time and data availability constraints determined our analytical
choice. The ratio PM2.5/PM10 of 0.67 is based on the average measurements in the monitoring
stations that measure PM2.5.
Table 3.1. Population and weighted average concentration of PM10 and PM2.5 in 2010 in the
Greater Metropolitan Area of Costa Rica
PM2.5 Annual Avg. Concentration intervals, µg/m3
Population exposeda
Annual Avg. PM2.5 concentration, µg/m3
Population exposedc
Up to 15 664,878 21 2,329,410
16 - 20 927,824
21 - 25 296,573
26 - 30 378,695
30 - 35 61,440
Total 2,329,410
PM10 Annual Avg. Concentration intervals, µg/m3
Population exposedb
Annual Avg. PM10 concentration, µg/m3
Population exposedc
Up to 20 135,574 31 2,329,410
21 - 25 904,301
26 - 30 495,479
30 - 35 218,724
36 - 40 273,675
41 - 45 225,883
46 - 50 56,834
51 - 55 18,940
Total 2,329,410 aKriging interpolation using ArcGIS™ bIDW interpolation using ArcGIS™ cTotal population of GMA
There has been a substantial increase in available evidence on the links between air pollution and
mortality in Latin America in the last decade, although most studies have dealt with short term
effects. A recent study (O´Neill et al. 2009) analyzed the effect of education in the association
between PM10 concentrations and short term mortality in Mexico city, Sao Paulo and Santiago de
Chile, and found 1-day lagged increases of 0.39%, 1.04% and 0.61% respectively of total non-
accidental adult mortality for an increase of 10- µg/m3 in concentration. In Brazil, studies have
found associations between exposure to PM10 and low birth weight (Gouveia et al. 2004) and also
with elderly respiratory mortality (Martins et al. 2004)

While the accurate determination of air pollutants’ concentrations and distribution has improved
greatly in Costa Rica in the last years (Herrera and Rodriguez 2009, 2010), the evidence base for
health risks of air pollution is still under development. While ongoing local studies are needed to
obtain a greater understanding of the health effects of urban air pollution in Costa Rica, a large
body of evidence is required to provide reliable estimates of health effects applicable at the
national level. In the absence of local data, for the association between exposure to inhalable
particulate matter and mortality, the coefficients of Pope et al. (2002) continue to be among the
most solid results for long term effects. Pope et al (2002) utilized ambient air quality data from
metropolitan areas across the United States for the two periods 1979-83 and 1999-2000, and
information on certified causes of mortality of adults in the American Cancer Society (ACS)
database over a period of 16 years. The details of the study (which confirms previous
observations, E.g. Dockery et al. 1993, Pope et al. 1995) have been discussed extensively
elsewhere, and the results still stand as the best available evidence for the association between
exposure to inhalable particulate matter and mortality. Although the locally relevant evidence of
health effects from air pollution has increased greatly in the last decade, new results are not
significantly changing the estimates of relative risk associated to PM exposure. In the context of
Latin America and the Caribbean there are not enough local studies to constitute a body of
evidence solid enough to displace (at least for long-term risk) the risk ratios and dose response
coefficients from Pope et al. (2002, 2007) (mortality effects of PM2.5) and from Ostro (1994, 2004)
and Abbey et al. (1995) (morbidity effects of PM10 and Chronic Bronchitis attributable to PM10,
respectively). These are summarized in table 3.2.
Table 3.2. Urban Air Pollution Dose-response coefficients
Annual Health Effect Dose-response
coefficient
Per 1 µg/m3 annual average
ambient concentration of:
Mortality (% change in cardiopulmonary
and lung cancer mortality)
0.8% PM 2.5
Chronic bronchitis (% change in annual
incidence)
0.9% PM 10
Respiratory hospital admissions (per
100,000 population)
1.2 PM 10
Emergency room visits (per 100,000
population)
24 PM 10
Restricted activity days (per 100,000
adults)
5,750 PM 10
Lower respiratory illness in children (per
100,000 children)
169 PM 10
Respiratory symptoms (per 100,000
adults)
18,300 PM 10
Source: Pope et al (2002) for the mortality coefficient. Ostro (1994, 2004) and Abbey et al (1995)
for the morbidity coefficients.

4. The health impact of inhalable particles in Costa Rica
In order to ascertain the share of mortality that is attributable to air pollution, baseline data on
certain causes of mortality are required. These are routinely collected and reported by Costa Rica’s
National Institute of Statistics on a yearly basis. The baseline mortality considered is the total non-
accidental and the types for determination of attributable mortality are cardiopulmonary causes
and lung cancer. It is also necessary to establish a lower threshold level for PM 2.5, below which it
is assumed there are no mortality effects. WHO (2002) recommended this threshold to be 7.5
µg/m3 in the World Health Report for mortality. However, a recent review by Krewski et al. (2009)
lowers the threshold to 5 µg/m3. Although there is much debate about the usefulness of these
lower limits (WHO recognizes there is no safe threshold for inhalable particles), they are widely
regarded as necessary for practical matters regarding air quality management. We applied the 5
µg/m3 threshold, more consistent with epidemiologic evidence.
Regarding nonfatal outcomes with known associations to air pollution, perhaps the most
burdensome for patients and health systems is Chronic Bronchitis (CB).Largely (but not
completely) attributable to tobacco use, not only does this disease entail intense suffering for the
patient (Nicolson & Anderson 2000), but it also constitutes a large-bill item for healthcare systems
(Blanchette et al. 2011). However, estimates of incidence are as yet not widespread, and are
exceedingly rare in non-OECD countries. There are no general estimates on either prevalence or
incidence of the disease in Costa Rica. The country´s efficient health information systems capture
all hospital discharges from the disease; however, estimating incidence from those would be
inaccurate on two accounts: firstly, not all (or even the majority) of CB patients would necessarily
require or seek hospitalization; and secondly, the discharge records did not reflect whether the
patient was firstly diagnosed or it was a recurrent event. Therefore, the rates applied are those
from WHO (2001) and Shibuya (2001) for the AMRO-B sub-region within the WHO region of the
Americas. A PM10 concentration threshold of 10 µg/m3 is used for the determination of
attributable CB (Abbey et al. 1995).
Aside from Chronic Bronchitis, the other health endpoints considered in this update are listed in
Table 4.1. below. These specific health effects have become standard health endpoints considered
in several worldwide studies on air pollution. In order to facilitate magnitude comparisons with
other risk factors, health effects can be converted to disability adjusted life years (DALYs)1. To do
so, disability weights and average duration of each outcome are assigned to each health effect.
Larsen (2004) used weights from the USNIH for lower respiratory illness (LRI) and chronic
bronchitis (CB) in the LAC region, and came up with his own estimates for other weights and
duration of illnesses. Years lost to premature mortality from air pollution were estimated from
age-specific mortality data for cardiopulmonary and lung cancer deaths, discounted at 3 percent
1 DALYs are the sum of the present value of future years of lifetime lost to premature mortality (referred to
life expectancy) and the present value of future years of lifetime adjusted by the severity of a disability caused
by disease or injury. For further details on DALY calculation, details can be found at (Fox-Rushby & Hanson
2001) and at the WHO website on the matter
http://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/

per year with full age weighting. This approach is not free from controversy, since there is
considerable uncertainty to duration estimates and weights include a substantial subjective
component. However, it is widely used for convenience in this type of calculations. No threshold is
applied for morbidity effects other than CB.
Table 4.1. Calculation of DALYs per case of health Effect
Disability weight Average duration of illness
Mortality 1.0 (7.5 years lost)
Lower respiratory illness - children 0.28 10 days
Respiratory iymptoms – adults 0.05 0.5 days
Restricted activity aays – adults 0.1 1 day
Emergency room visits 0.30 5 days
Hospital admissions 0.40 14 days*
Chronic Bronchitis 0.2 20 years
Source: Larsen (2004) * Includes days of hospitalization and recovery period after hospitalization.
Once health effects of air pollution are converted to disability adjusted life years (DALYs), we can
make quick comparisons with regard to health effects from other environmental risk factors. A
calculation of DALYs lost per 10 thousand cases of the considered health end-points is presented
in Table 4.2.
Table 4.2. DALYs lost per selected health effect attributable to air pollution
Health effect DALYs lost per 10,000 cases
Mortality 75,000
Chronic Bronchitis (adults) 22,000
Respiratory hospital admissions 160
Emergency Room visits 45
Restricted activity days (adults) 3
Lower respiratory illness in children 65
Respiratory symptoms (adults) 0.75
Source: Larsen 2004
The estimated health impact of urban air pollution in Costa Rican cities is in table 4.3. The values
are calculated by applying relative risks and particle concentrations (minus thresholds, where

applicable) to population exposed, adjusting for age groups when necessary and extracting the
fraction of these health outcomes that is attributable to this specific exposure. DALYs are
calculated simply by multiplying the number of cases by the factors in table 4.2.
Table 4.3. Estimated Health Impact of Urban Air Pollution in cities with PM monitoring data
Health categories Total cases Total DALYs
Premature mortality 655 4,909
Chronic bronchitis 353 776
Hospital admissions 881 14
Emergency room /Outpatient hospital visits 17,275 78
Restricted activity days 4,219,757 1,266
Lower respiratory illness in children 124,024 806
Respiratory symptoms 13,429,835 1,007
TOTAL N/A 8,857
Source: estimates by the authors
Around 655 premature deaths and close to 9,000 lost DALYs were attributable to urban air
pollution (PM exposure) in the Greater Metropolitan Area of Costa Rica in 2010. The only available
previous results for comparison come from a similar study conducted in the mid 2000s by the
Ministry of Health (Allen et al. 2005). Reported premature mortality related to PM was of over
3,400 attributable deaths annually. However, some factors preclude a direct comparison. Firstly,
the calculation was made in relation with PM10, not PM2.5 (for which there was no measurement
at the time). Secondly, the considered exposure was far greater; with their data, over 68% of the
population in the GMA was exposed to PM10 concentrations of over 60 µg/m3. At the time, only
two monitoring stations measured PM10. In our dataset, the maximum exposure category is over
55 µg/m3, and less than 1% of the population in the GMA is in that category. Exposure was
possibly overestimated in the mentioned study, probably in relation with scarce data availability.

5. Estimated Cost of Health Impacts
The estimated annual cost of health impacts from urban air pollution is presented in Table 5.1. The
cost of mortality is based on the Value of a Statistical Life (VSL). We are not reporting a cost based
on the Human Capital Approach, since we feel that an indicator based on foregone income due to
premature mortality severely underestimates the true cost to society of that excess mortality
represents in a setting like Costa Rica. There are no primary studies on the Willingness To Pay
(WTP) to avoid mortality or morbidity risks related to air pollution in Costa Rica. A VSL was recently
obtained through a primary survey (Schram 2009) but the risks of focus in the study were of
difficult application for the case of air pollution. Instead, we extrapolated an estimate from a
recent study (Ortiz et al. 2009) that estimated the population’s WTP to reduce risks of death
associated with “typical” air pollution policies and, consequently, the value of a statistical life in
São Paulo, Brazil. Details on the extrapolation are available in Annex 1.
Table 5.1. Estimated Annual Cost of Health Impacts (Billion LCU)
Health categories Total annual cost
(Billion Colon)
Percent of total cost*
(Mean)
Mortality 130 - 162 69
Morbidity:
Chronic bronchitis 3 1
Hospital admissions 7 3
ER visits/Outpatient hospital visits 9 4
Restricted activity days (adults) 21 10
Lower respiratory illness in children 20 10
Respiratory symptoms (adults) 4 2
Total cost of Morbidity 64 31
TOTAL COST (Mortality and Morbidity) 194 - 226 100
* Annual cost is rounded to nearest billion, and percentages are rounded to nearest percent.
The total cost of air pollution in Costa Rica in 2010 was around 210 Billion Colones on average,
which represented roughly 1.1% of the GDP. Almost 70% of the cost was related to premature

mortality, and the rest distributed among several health outcomes. Such high mortality-related
proportion of costs is consistent with most international studies (Hunt 2011).
The cost of morbidity was estimated through the cost of illness (comprising the cost of treatment
and the opportunity cost of time lost to illness). The calculated cost of treatment was based on
consultations with health authorities and the upper bound of the publicly listed prices that the
public healthcare financing authority pays to healthcare providers, which in turn are deemed the
most adequate reflection of the true cost of treatment in Costa Rica. Some explanation on
healthcare financing and provision in Costa Rica is useful to understand the cost of treatment
values for health effects attributable to air pollution used in this report. Such costs are based on
public prices for medical and hospital services as reported by the Costa Rican Social Security
Administration (Caja Costarricense del Seguro Social - CCSS). More so than in other Latin American
countries, public prices for medical and healthcare services are in Costa Rica an accurate reflection
of the cost of treatment for the society. The CCSS pays for and administers a large proportion of
healthcare services provided in the country (Giedion et al. 2010). The small and decreasing
percentage of uninsured population usually has publicly paid healthcare alternatives. Moreover,
evidence suggests that the widespread usage of public healthcare services in Costa Rica is not
affected by income, so high income groups are not necessarily more likely to use private
healthcare (ECLAC 2001). Whereas public healthcare services prices may represent a distorted
indicator for the valuation of the true health cost of environmental risks in certain markets, they
are an accurate and readily available indicator in several Latin American countries, and specifically
in Costa Rica.
Beyond the actual cost of treating illness, there is sound evidence that individuals place a much
higher value on avoiding pain and discomfort associated to illness than that reflected solely in
medical costs; this has been observed also specifically in connection with air pollution risks
(Cropper and Oates 1992, Alberini and Krupnick 2000, Arigoni et al. 2009). Therefore, we apply a
WTP proxy based on various estimates (PDDB 2009, Cifuentes et al. 2005, Lozano 2004, Alberini
and Krupnick 2000) which used Benefit transfer to calculate the WTP value. Alberini and Krupnick
also note that such ratios are similar to those for the United States, despite the differences
between countries, which further reinforces the solidity of such a proxy for WTP value. For
morbidity outcomes involving the provision of medical services we used a WTP/COI ratio 2,26.
Chronic Bronchitis (CB) is an example of severe decrease of welfare beyond medical costs, which
could justify an even larger WTP proxy. While we agree on placing a comparatively large cost in a
burdensome illness like CB, we would rather apply consistent WTP values for air pollution-related
outcomes in the absence of specific information for CB. The estimated cost per case of premature
mortality or specific health endpoint is presented in table 5.2. The cost per case (comprising Cost
of illness plus the proxy for WTP) is the basis for the estimation of the annual costs in table 5.1. by
multiplying each unit case cost by the cases in table 4.3.

Table 5.2. Estimated Unit Cost by Health End-Point
Health categories Total cost Per case
(000 Colon)
Cost-of-illness
Per case (000
Colon)
WTP proxy
(000 Colon)
Mortality 199,000 – 248,000 N/A N/A
Chronic bronchitis 8,888 2,718 6,170
Hospital admissions 7,917 2,421 5,496
Emergency room /Outpatient hospital visits 523 160 363
Restricted activity days (adults) 5 5 N/A
Lower respiratory illness in children 164 50 114
Respiratory symptoms (adults) 0.3 0.3 N/A
Source: estimates by authors
Table 5.3. details the baseline data that were used for the estimation of the cost of illness and the
costs of time lost to illness. For consistency with other World Bank evaluations in the context of
Latin America, we kept the same assumptions regarding duration of illness, rate and length of
hospitalization, average time lost per health endpoint, frequency of doctor visits and discount rate
used by Larsen (2004). We valued time lost to illness at 75% of average urban wage, and applied
such cost both to working and non-working individuals, based on the assumption of an equivalent
opportunity cost for both categories.
There is still little evidence of healthcare usage and costs of patients regarding the cost of a new
case of Chronic Bronchitis. In the case of Costa Rica, we could not find local data either on
incidence or on the usage and cost of healthcare by patients. Therefore, we relied on the
information used by Schulman et al (2001) and Niederman et al (1999) from the United States and
Europe and applied them to Costa Rica. The estimate of lost work days per year is based on
frequency of estimated medical treatment plus 7 additional days for each hospitalization and one
extra day for each doctor and emergency visit. These days are added to reflect time needed for
recovery from illness. The estimated cost of a new case of CB assumes a 20-years duration of
illness over which medical costs and value of time experience an annual real increase of 2 percent,
and costs are discounted at a 3% rate per year, a value commonly applied by WHO for health
effects.

Table 5.3. Baseline Data for Cost Estimation
Baseline Source:
Cost Data for All Health End-Points:
Cost of hospitalization (Colones per day) 370,000 Per consultations with medical
service providers and health
authorities Cost of emergency visit (Colones) – urban 120,000
Cost of doctor visit (Colones) – urban 30,000
Value of time lost to illness (Colones per day) 20,000 Based on urban wages in
Costa Rica
Chronic Bronchitis (CB):
Average duration of Illness (years) 20 Based on Shibuya et al (2001)
Percent of CB patients being hospitalized per year 1.5 % From Schulman et al (2001)
and Niederman et al (1999) Average length of hospitalization (days) 10
Average number of doctor visits per CB patient per
year
1
Percent of CB patients with an emergency
doctor/hospital outpatient visit per year
15 %
Estimated lost work days (including household work
days) per year per CB patient
2.6 Estimated based on frequency
of doctor visits, emergency
visits, and hospitalization
Annual real increases in economic cost of health
services and value of time (real wages)
2 % Estimate
Annual discount rate 3 % Applied by WHO for health
effects
Hospital Admissions:
Average length of hospitalization (days) 6 Estimates
Average number of days lost to illness (after
hospitalization)
4
Emergency Room Visits:
Average number of days lost to illness 2
Restricted Activity Days:
Average number of days of illness (per 10 cases) 2.5
Lower Respiratory Illness in Children:
Number of doctor visits 1
Total time of care giving by adult (days) 1 Estimated at 1-2 hours per day

6. Reference
Abbey, D. et al (1995). Long-Term Ambient Concentrations of Particulates and Oxidants and
Development of Chronic Disease in a Cohort of Nonsmoking California Residents. Inhalation
Toxicology, Vol 7: 19-34.
Albert Schram (2009) Análisis de costo-efectividad y costo-beneficio Programa de Detección
Temprana de Cáncer Gástrico en Costa Rica. Población y Salud en Mesoamérica Volumen 6,
número 2, artículo 3 Enero - junio, 2009.
Alfaro, R. Informe de Calidad del Aire de las Capitales Centroamericanas, 1998. Escuela de Ciencias
Ambientales, Universidad Nacional, Costa Rica.
Allen, P., Vargas, C., Araya, M., Navarro, L., Salas, R. L. (2005). Costos en salud por la
contaminación del aire debida al transporte automotor. Un proyecto de evaluación del impacto de
Costa Rica. Preparado por el Ministerio de Salud. Unidad de Gasto y Financiamiento. Dirección de
Desarrollo de la Salud. Ministerio de Salud. Costa Rica. 2005.
Anna Alberini and Alan Krupnick (2000) Cost-of-Illness and Willingness-to-Pay Estimates of the
Benefits of Improved Air Quality: Evidence from Taiwan Land Economics Vol. 76, No. 1 (Feb.,
2000), pp. 37-53
Bell et al. (2006). The avoidable health effects of air pollution in three Latin American cities:
Santiago, Sao Paulo, and Mexico City. Environmental Research 100 (2006) 431–440
Bell ML, Cifuentes LA, Davis DL, Cushing E, Telles AG, Gouveia N.(2011) Environmental health
indicators and a case study of air pollution in Latin American cities. Environ Res. 2011
Jan;111(1):57-66. Epub 2010 Nov 13.
Blanchette CM, Roberts MH, Petersen H, Dalal AA, Mapel DW.(2011) Economic burden of chronic
bronchitis in the United States: a retrospective case-control study.Int J Chron Obstruct Pulmon Dis.
2011 Jan 13;6:73-81.
Bowland B, Beghin J (2001) Robust estimates of value of a statistical life for developing economies.
Journal of policy modeling: 385-389
Brook RD. et al. (2010) Particulate Matter Air Pollution and Cardiovascular Disease : An Update to
the Scientific Statement From the American Heart Association. Circulation. 2010;121:2331-2378
Cifuentes A. et al. (2005) Urban air quality and human health in Latin America and the Caribbean.
IADB, Washington DC, USA.
Dockery D.W., Pope C.A. III, Xu X, et al (1993). An association between air pollution and mortality
in six US cities. New England Journal of Medicine, 329: 1753-1759.

Eftim SE, Samet JM, Janes H, McDermott A, Dominici F. (2008) Fine particulate matter and
mortality: a comparison of the six cities and American Cancer Society cohorts with a medicare
cohort. Epidemiology. 2008 Mar;19(2):209-16.
Giedion U. et al (2010). Los sistemas de salud en Latinoamérica y el papel del seguro privado.
Fundación MAPFRE, Madrid, España.
Gouveia, N., Bremner, S. and Novaes, H. (2004) Association between ambient air pollution and
birth weight in São Paulo, Brazil. J Epidemiol Community Health 2004;58:11-17
HEI (2008) Public Health and Air Pollution in Asia (PAPA): Key Results from Bangkok, Hong Kong,
Shanghai, and Wuhan. Health Effects Institute, Boston, Massachusetts, USA.
Herrera Murillo, Jorge y Rodríguez Román, Susana. Validación de un método de análisis para la
determinación de metales pesados en partículas pm10 colectadas en aire ambiente. Tecnología en
Marcha, Vol. 23, N.° 3, Julio-Setiembre 2010, pp. 33-46.
Herrera-Murillo, Jorge; Rodríguez Román, Susana. Evaluación de los niveles de partículas PM10 y
dioxido de nitrógeno en la Ciudad de San José, Costa Rica: 2005-2006 Tecnología en Marcha, Vol.
22, N.° 3, Julio-Setiembre 2009, pp.42-55.
Hunt, A. (2011), “Policy Interventions to Address Health Impacts Associated with Air Pollution,
Unsafe Water Supply and Sanitation, and Hazardous Chemicals”, OECD Environment Working
Papers, No. 35, OECD Publishing.
INEC, Censo de Población de la República de Costa Rica, 2011.
Jerrett M. et al. (2009) Long-Term Ozone Exposure and Mortality N Engl J Med 360;11, 1085-1095.
Krewski D, Jerrett M, Burnett RT, Ma R, Hughes E, Shi Y, Turner C, Pope CA, Thurston G, Calle EE,
Thunt MJ (2009). Extended follow-up and spatial analysis of the American Cancer Society study
linking particulate air pollution and mortality. HEI Research Report, 140. Boston, MA: Health
Effects Institute, 2009.
Larsen B. (2004). Cost of environmental damage in Colombia: A Socio-Economic and
Environmental Health Risk Assessment. World Bank, Washington DC, USA.
Martins, M.C.H., Fatigati, F.L., Ve´ spoli, T.C., Martins, L.C., Pereira, L.A.A., Martins, M.A., Saldiva,
P.H.N., Braga, A.L.F. (2004). Influence of socioeconomic conditions on air pollution adverse health
effects in elderly people: an analysis of six regions in Sao Paulo, Brazil. J. Epidemiol. Community
Health 58, 41–46.
Niederman, M. et al. (1999). Treatment Cost of Acute Exacerbations of Chronic Bronchitis. Clinical
Therapy, 21(3): 576-91.

O'Neill MS, Bell ML, Ranjit N, Cifuentes LA, Loomis D, Gouveia N, Borja-Aburto VH.(2008) Air
pollution and mortality in Latin America: the role of education. Epidemiology. 2008 Nov;19(6):810-
9.
Ortiz, R.A., Markandya, A., and Hunt, A. (2009). Willingness to Pay for Mortality Risk Reduction
Associated with Air Pollution in São Paulo. RBE, Rio de Janeiro, V. 63 n. 1, p. 3–22, Jan-Mar 2009.
Ostro, B. (1994). Estimating the Health Effects of Air Pollution: A Method with an Application to
Jakarta. Policy Research Working Paper, World Bank.
Ostro, B. (2004). Outdoor Air Pollution - Assessing the environmental burden of disease at national
and local levels. Environmental Burden of Disease, Series, No. 5. Geneva: WHO.
Pope CA III, Burnett RT, Thun MJ, et al (2002). Lung cancer, Cardiopulmonary mortality, and Long-
term exposure to Fine particulate air pollution. Journal of the American Medical Association, 287:
1132-1141.
Pope CA III, Thun MJ, Nambudiri MM, et al (1995). Particulate air pollution as a predictor of
mortality in a prospective study of US adults. American Journal of Respiratory and Critical Care
Medicine, 151: 669-674.
Pope CA III (2007) Mortality effects of longer term exposures to fine particulate air pollution:
review of recent epidemiological evidence. Inhalant Toxicol. 19(suppl I):S33–S38.
Samet JM, Dominici F, Curriero FC, Coursac I, Zeger SL. (2000) Fine particulate air pollution and
mortality in 20 U.S. cities, 1987-1994.N Engl J Med. 2000 Dec 14;343(24):1742-9.
Samet J, Krewski D. (2007a) Health effects associated with exposure to ambient air pollution. J
Toxicol Environ Health A. 2007 Feb 1;70(3-4):227-42.
Samet JM. (2007b) Traffic, air pollution, and health. Inhal Toxicol. 2007 Sep;19(12):1
Schulman, Ronca and Bucuvalas, Inc. (2001). Confronting COPD in North America and Europe: A
Survey of Patients and Doctors in Eight Countries.
Shibuya, K., Mathers, C., and Lopez, A. (2001). Chronic Obstructive Pulmonary Disease (COPD):
Consistent Estimates of Incidence, Prevalence, and Mortality by WHO Region. Global Programme
on Evidence for Health Policy. World Health Organization. November 2001.
USEPA (2011a). United States Environmental Protection Agency website on air pollution trends.
Available online at http://www.epa.gov/airtrends/
USEPA (2011b). United States Environmental Protection Agency website on ground level ozone.
Available online at http://www.epa.gov/groundlevelozone/health.html
WHO (2001). Global Burden of Disease 2001. The World Health Organization, Geneva,
Switzerland.

WHO (2002). The World Health Report 2002. The World Health Organization, Geneva,
Switzerland.
Annex 1. Economic basis for choice of VSL (Source: text and calculations adapted from an
original contribution by Elena Golub)
Our choice of a Value of a Statistical Life (VSL) for Costa Rica is based on a recent study by Ortiz et
al. (2009). This study aims to estimate the population’s willingness to pay (WTP) to reduce risks of
death associated with “typical” air pollution policies and, consequently, the value of a statistical
life (VSL) in São Paulo, Brazil. Uniquely for that country, the study uses a methodology that has
previously been tested in several industrialized countries (USA, Japan, Canada, South Korea,
England, France and Italy) and involves a computer-based contingent valuation survey. This survey
instrument was adapted to the Brazilian context and used to elicit willingness-to-pay measures of
reductions in risk of death in Brazil.
Key features of the survey instrument involve eliciting the health status of the respondents and
their family; explaining basic concepts of probability, and proposing simple practice questions to
familiarize the respondents with the probabilities concepts introduced; presenting the leading
causes of death for a Brazilian individual of the respondent’s age and gender, and setting these in
the context of common risk-mitigating behaviors; and finally, asking individual’s willingness to pay
for risk reductions of a given magnitude that occur at a specified time.
The mean and median willingness-to pay values were estimated using the interval data model that
can be generated from the dichotomous choice with follow-up question format. The responses to
willingness-to-pay and follow-up questions were combined to generate intervals in which the
unobservable respondents’ willingness to pay are to be found. Weibull probability distribution was
selected for the random variable willingness to pay. The statistical willingness-to-pay model using
the Weibull distribution is estimated using the maximum likelihood method.
The corresponding values of a statistical life were estimated using both median willingness-to-pay
estimates (conservative estimates) and mean willingness-to-pay values. They were obtained by
dividing the willingness-to-pay figures by the corresponding annual risk reduction being valued. It

was assumed that respondents implicitly considered the risk reduction evenly over the ten-year
period, which makes it possible to avoid discounting the respondents’ annual payments.
The values of a statistical life estimated from 1-in-1000 risk reductions are much higher than those
estimated using the 5-in-1000 risk reduction. This is purely due to the lack of proportionality
between the willingness-to-pay estimates regarding the differences in the size of risk reductions. It
is suggested that the VSL estimates derived from mean and median willingness-to-pay estimates
for a 5-in-1000-risk reduction are of greater policy relevance since they represent more
conservative estimates than those estimated using willingness-to-pay estimates for 1-in-1000-risk
reduction. Thus, for policy assessments in São Paulo it is suggested conservative values of a
statistical life ranging between US$ 0.77 – 1.31 million.
When compared with European and North American estimates these values seem to be higher
than expected. Given the close link between willingness-to-pay estimates and the population
income, lower willingness-to-pay values for developing countries might be expected. A possible
reason for the high WTP and VSL estimates found in the current study might have been the
’cooperative’ behavior observed in many of the respondents. It is possible that, those respondents
tried to be “cooperative” or helpful by saying “yes” to every question. We believe that the
relatively high figures in this valuation exercise may be partly due to this bias. Value of a statistical
life excluding possible ‘yeah-say’ responses using parametric estimation of mean and median
annual willingness to pay in US$ 2003 (Weibull distribution, 95% CI ) is US$ 0.4-0.5 million and in
US$2009 0.45-0.56 million2.
WDI (2009) Countries Brazil Costa Rica GDP per capita (current US$) 8,251 6,373 GDP (current US$) 1,594,489,675,024 29,255,751,296 Population, total 193,246,610 4,590,790 GDP (current LCU) 3.19E+12 16.76E+12 Exchange rate 2 573 Value of Statistical Life (VSL): VSL estimates from Brazil (Ortiz et al, 2009) 0.45 0.56 Costa Rica GDP (US$ billion) in 2009 29 29 Costa Rica Population (million) in 2009 4.59 4.59 Costa Rica GDP per capita (US $) in 2009 6,373 6,373 Average GDP/capita differential to Costa Rica in 2009 77.24% 77.24% Exchange rate (year average 2003) 573 573 Income elasticity of VSL 1 1 VSL in Costa Rica for adult individuals dying from pollution, mln US$. 0.35 0.43 VSL in Costa Rica for adult individuals dying from pollution, mln LCU. 199 248
2 Adjusted using CPI presented by U.S. Department Of Labor, Bureau of Labor Statistics (2012)
ftp://ftp.bls.gov/pub/special.requests/cpi/cpiai.txt.

Annex 2. List of Acronyms
Acronym Meaning
CB Chronic bronchitis
CCSS Caja costarricense del seguro social (Costa Rican Social Security Administration)
COI Cost of illness
DALY Disability-adjusted life year
GDP Gross domestic product
GMA Greater metropolitan area
HCA Human capital approach
IDW Inverse distance weighting
LAC Latin America and the Caribbean
LCU Local currency unit
LRI Lower respiratory illness
OECD Organization for the economic cooperation and development
PM2.5 Particulate matter with a diameter smaller than 2.5 microns
PM10 Particulate matter with a diameter smaller than 10 microns
UNA Universidad Nacional de Costa Rica (Costa Rican National University)
USNIH United States National Institutes of Health
VSL Value of a statistical life
WHO World Health Organization
WTP Willingness to pay