Embed Size (px)
Citation preview

The Health Commons Project
OHA Transformation CenterComplex Care Collaborative
November 5, 2013Eugene, Oregon

The Health Commons Grant, an award of $17.3 million over three years from the CMS Innovation Center, is a springboard for Health Share of Oregon to create a regional system to better serve the Medicaid population in the Portland metro area.
3-Year Funding Amount $17,337,093 Estimated 3-Year Savings: $32,542,9133-Year Population Impact: 19,000 patients
At the end of the Grant, all initiatives should be financially sustainable
The project is one of 107 nationally in the first round of funding, one of the largest single-state projects
Overview
“We can do this!”
• RFP occurs during early formation of Tri County CCO
• Multi system collaborative application for CMS “Innovations Challenge Grant” (Nov-Dec 2011)
• Alignment with Tri County Assets and Challenge– History of multi party collaboration– Projects must take cost out of system rapidly– Existing projects that can be taken to scale– Focus on “high utilizer” / complex patients as first step in
building CCO system of care?
November 2011…

Defining The “High Utilizer” Target Population
9248 high cost members/12 mos

Clinic View of Target PopulationMultiple High Volume Complex Patient Clinics
10% mbrs = 51% Total Paid Cost/12 mos
Population Segment # Members
% Members
Avg Total Paid Cost per Member/ 12 mos
% Paid Cost/12 mos of Segment
# ED visits
# IP Admits
No inpatient/6+ ED visits
81 3% $8743 5% 786 0
1 Non-OB inpatient and 0-5 ED visits
97 4% $18,767 14% 147 97
2+ Non-OB inpatient OR 1 Non-OB inpatient AND 6+ ED visits
71 3% $59,440 32% 383 189
Multnomah County Health Department-NE Clinic Population


Health Commons Grant Interventions
ED GUIDES: Non-clinical staff assist patients to a primary care home and make referrals to other programs.
STANDARD HOSPITAL TRANSITIONS TO PRIMARY CARE: All metro-area hospitals will use the same discharge summary template; primary care home will develop standard processes for receiving and responding to discharged patients
LEVEL ONE STRATEGIES produce small per patient per month savings across a large number of patients.

Health Commons Grant InterventionsLEVEL TWO STRATEGIES produce large per patient per month savings across a smaller number of patients.
COMMUNITY OUTREACH WORKERS provide high-touch support to high acuity patients within the community, addressing their social determinants of health and encouraging wellness.
TRANSITIONAL CARE NURSES AND PHARMACISTS provide intensive discharge planning and home visiting support post-discharge; facilitate effective connection to primary care home.
LICENSED BEHAVIORAL HEALTH SPECIALISTS provide intensive transitional support to patients admitted to the hospital psychiatrically; facilitate effective connection to behavioral health home.

Partner organizations for interventions
Intervention Team Year OneOutreach (CareOregon)
Interdisciplinary Community Care Teams (ICCT)
CareOregon, MCHD, CCHD, Virginia Garcia, Central City Concern, Providence, Legacy IM clinics, OHSU Richmond, OHSU ED, EMS, Cascadia, Neighborhood Health Clinics, The Oregon Clinic
Hospital-to-home(OHSU)
Care Transition Innovation (C-Train)
OHSU, Legacy (Good Sam, Emanuel and Mt. Hood)
Mental Health(Wash Co MH)
Intensive Transition Team Multnomah, Clackamas and Washington Counties
ED Guide(Prov)
ED Guide Leadership Team Providence Milwaukie, Providence Portland, Providence St. Vincent
Discharge(Legacy)
Standardized Hospital Discharge and Transition
Legacy Emanuel Hospital with Legacy and MCHD clinics(Years 2 & 3: Providence and OHSU)
Interventions were based on existing work by Health Share providers, ready for scale up, with the opportunity for spread across all partner organizations.

• Utilization & Cost trends• Quality of CareClaims Analysis
• Provider & Patient perspectives• Program Improvement feedback
Qualitative Interviews
• Workforce /Caseloads/Effort• Type & Frequency of Services / ROI
Program Process Data
• Patient Experience / Satisfaction• Quality of CarePatient Surveys
Evaluation StrategiesCenter for Outcomes Research and Education (CORE)
• Community-wide Care Coordination Registry
• Managing & Tracking Intervention Cohorts
• Event Notifications to relevant care teams
• One ‘stop’ source for key evaluation data
Information Systems are Critical!
+Standardized Hospital Discharge Summary – Hospital EHRs
What can users do? • Create lists of individuals (registry cohorts) engaged in a SPECIFIC
intervention• Track individuals through steps/phases of a SPECIFIC intervention
• Collect data on encounters, assessments, checklists and other intervention-specific activities or ‘touches’
• Receive daily notifications of ED and Inpt events for clients
• View member-level health services profile, past 12 mos
• Track mileage and/or patient support funds disbursement
• View dashboards displaying progress on key processes/outcomes
• See what other intervention teams are or have worked w/ patient

Year 1 Roll Out• Grant Oversight (GO) Team formed to monitor and guide work
– Grant Metrics Dashboard, Evaluation Plan, Operational Plans for each initiative
• Intervention Clinical Leads, Steering Cttes, Project Managers in place
• Staff for all 5 interventions hired, trained and fully functional in roles
• “Intersections” Group formed to coordinate and synchronize efforts
• Project Management Office (PMO) established – Lean Training to support increased efficiency, effectiveness
• Learning Collaborative meetings held: All Staff Kickoff; Leadership Outcomes Improvement Collaborative
• Communications Strategy with monthly updates, website, Board and stakeholder communications

Year 1: Individuals Served To Date
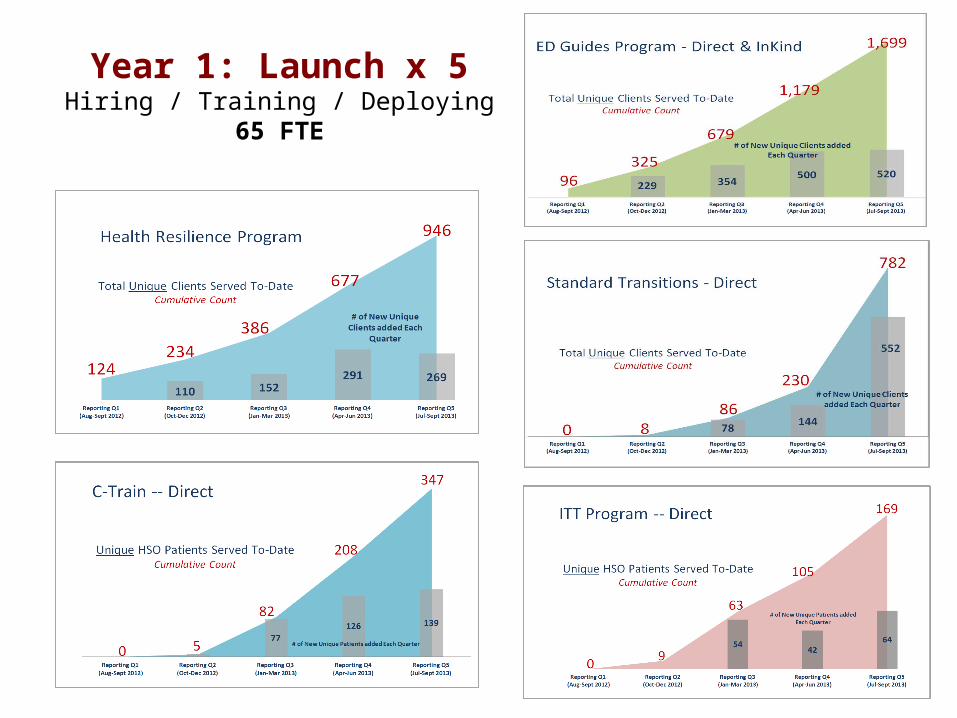
Year 1: Launch x 5 Hiring / Training / Deploying
65 FTE

Year 1 Challenges • How do you engage providers / leaders: in clinics, in hospitals, in EDs,
etc?– Intensive work with hospital and clinic leaders
• What is the right workforce to address patient/ client needs?– Rn vs Social Worker vs “outreach worker”
• Who are the patients / clients? What do they really, really need?– And which are the ones we can really, really help? Archetypes?
• What is a reasonable case load for each type of intervention?– What kind of supervision is needed?– What case load is needed for financial sustainability?
• How do we coordinate with and learn from each other?– Who needs to meet with whom about what?– How does this fit into other organizational care management work?– How do we create a rapid learning system?

Key Year 1 Learning: Understanding the people we trying to help…
“62 year old with multiple hospital admissions”
Moving from: “What is wrong with him…”
To: “What has happened to him…”
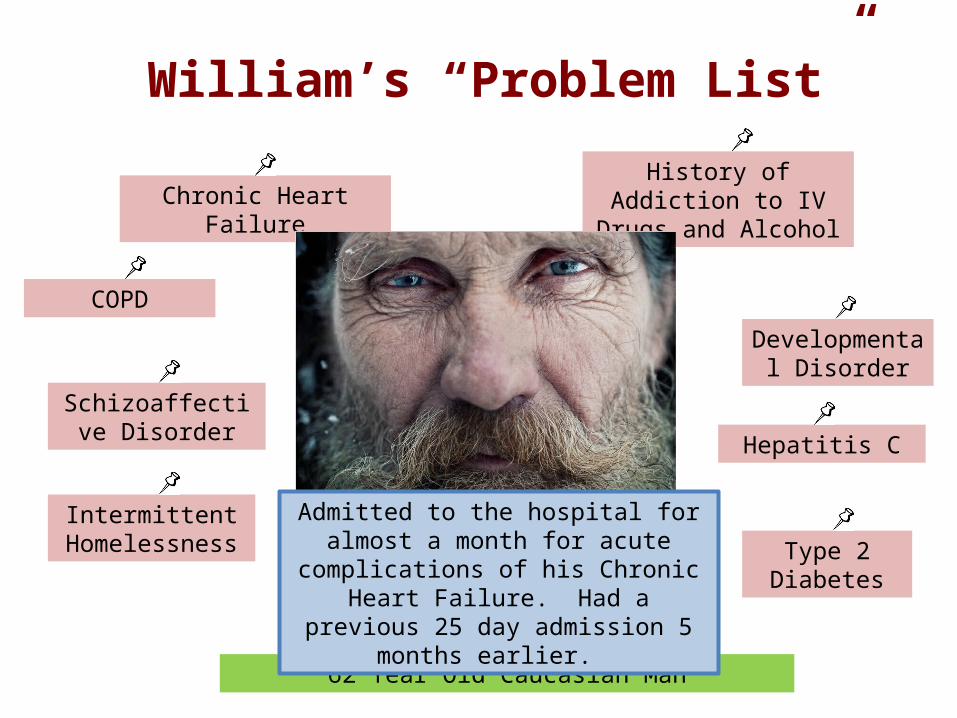
William’s “Problem List”
Chronic Heart Failure
Schizoaffective Disorder
History of Addiction to IV Drugs and Alcohol
COPD
Hepatitis C
Type 2 Diabetes
Intermittent Homelessness
Developmental Disorder
62 Year Old Caucasian Man
Admitted to the hospital for almost a month for acute complications of his
Chronic Heart Failure. Had a previous 25 day admission 5 months earlier.

As Often Viewed By Others / Providers…
IrritableHostile
Cannot give clear health
history
Chronic poor self
care
Extremely needy / demanding
Stoic, reluctant to admit health problems
Problems with pain / pan tolerance
Intermittent job history
Chronic relationship problems

What really drives health decline and high-cost utilization in our population?
We got to know William, and others like him, we have found: • Poor health literacy• Prevalence of SA and mental health conditions but lack of access to services• Mild to moderate cognitive deficits• Homelessness and food insecurity; chaotic lives burdened with cumbersome
eligibility requirements for social programs• Inability to access basic resources such transportation, healthy food,
medications, place to exercise, etc• Extensive care coordination needs, particularly between sites of care
• Very high prevalence of adverse life events, trauma, and toxic stress: childhood trauma, school failure, job instability, relationship failure, self medication with substance use, high risk behaviors, poor decision making skills…

Impact of Trauma on World View: Chronically Scared Individuals
• “Emotional brain” on alert, hyper vigilant– Focus: short-term survival, not long-term strategy– “The world is an unsafe place to live in”
• “Thinking brain” less available, poor concentration– Learning difficult; complexity gives way to simplicity– “My own thoughts and feelings are unsafe”
• Chronic stress result: “Threat” oriented world view– See threats where none exist– Feel slights where none were intended– React passively or aggressively in order to assess the “threat”– “Other people are unsafe and cannot be trusted”
• Do not work as efficiently or effectively – Too busy “staying alive”– Circle the wagons and shoot inward– “I expect crisis, danger and loss”

Obvious conclusion• “Usual medical care” – even really really good usual
medical care – will not be enough for the high acuity population.– New forms of “Trauma Informed” care management /
case management are needed– Access to mental health and addictions resources is
critical– Socially determined risks cannot be ignored or assumed
outside of “health care”– New (and less costly) approaches will be required for
success
“Health Resilience Program”• Building a Trauma Informed Care System for
high needs Medicaid members
• Key elements: Safety, Empowerment, Trust, Collaboration, Choice– Comprehends the impact of violence – Provides service in ways that do not re traumatize
• Will launch 50 new direct service FTE over 3 years in all high acuity touch points
24
Health Resilience Specialists are paired with primary health homes and specialty practices to enhance the practices’ ability to provide individualized ‘high touch’ support to patients with exceptional utilization
* Staff with engagement skills, compassion, non-judgmental attitude, outreach experience
* “Trauma Informed Care” approach * Outreach worker incorporated into the practice team * Clinical Supervision by mental health trained managers; regular huddles; rounds
* Transparency: ask permission * Trust :be non judgmental, create safety
* Time: slow things down, help process * Tailoring to client: be open, listen
Outreach Worker Interventions• Motivational Interviewing to resolve ambivalence about health-related
behavior change• Client advocacy within and among multiple systems • Role modeling advocacy and relational skills• Assistance in navigating health care system • Care coordination• Health literacy education• Self management skill development• Assistance with complex problem solving related to living in poverty with
multiple health issues• Providing opportunities to identify as something other than a “patient”• Providing opportunities to experience success and feel confident• Deep listening, acknowledgment and respect for each individual

ICCT Programs
• Health Resilience Program: 14 Health Resilience Specialists (HRS) in primary care clinics; 1 in Pulmonary Clinic; 1 in Liver Clinic
• Central City Concern Health Improvement Project (CHIP): 5 staff including a Recovery Specialist, RN, Mental Health Specialist
• New Directions: 3 social workers in OHSU ED for frequent ED users with Mental Health dx
• Tri County 911 Program: 4 social workers for frequent 911 callers, ambulance users.
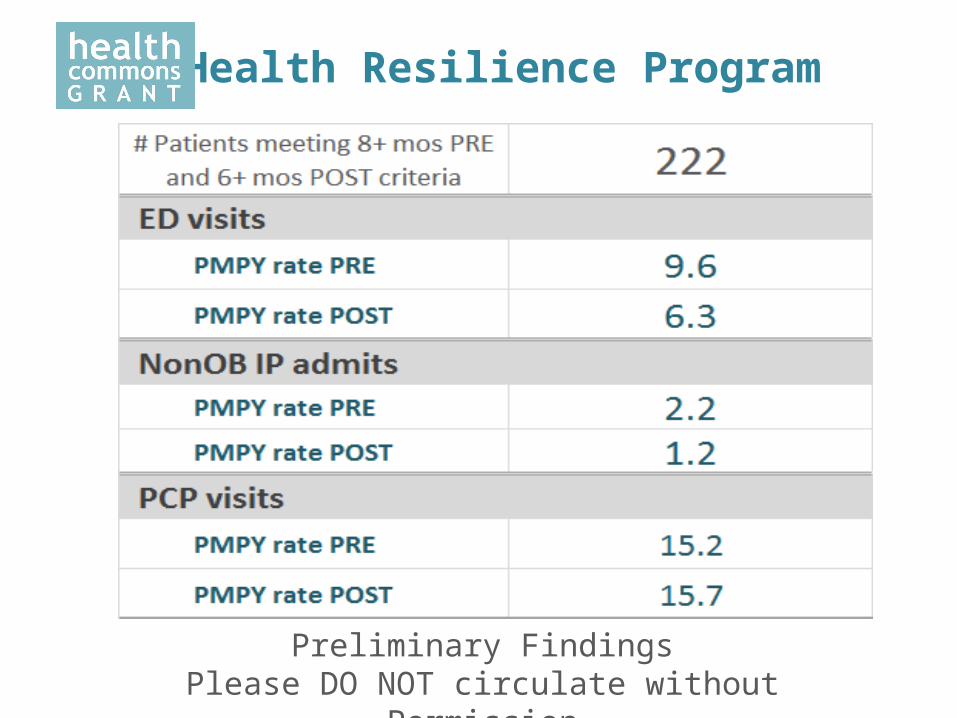
Preliminary FindingsPlease DO NOT circulate without Permission
Health Resilience Program
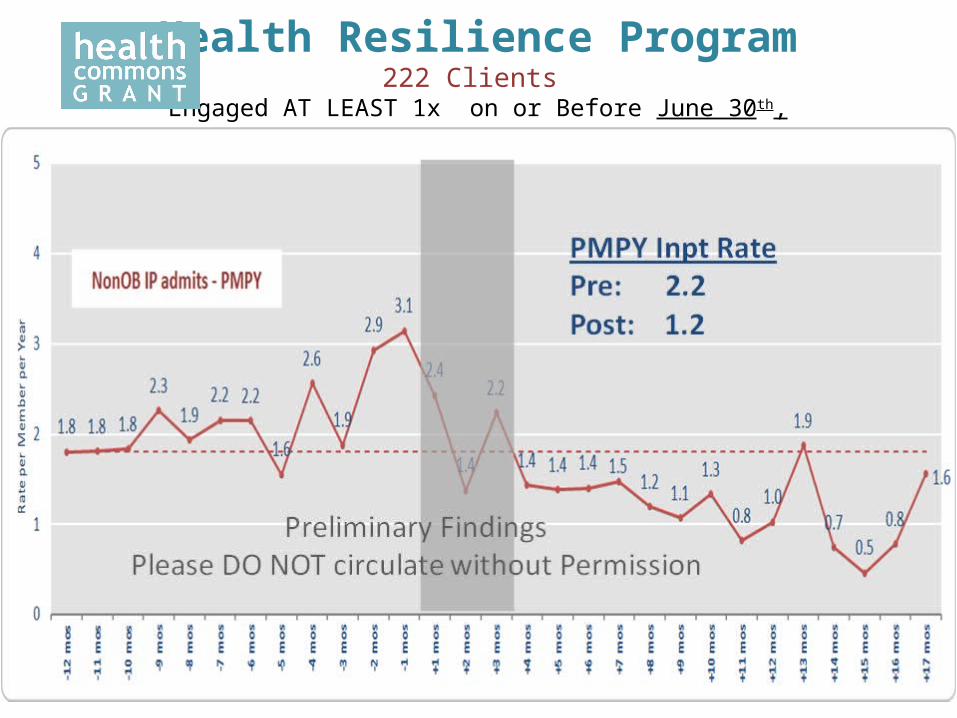
Health Resilience Program222 Clients
Engaged AT LEAST 1x on or Before June 30th, 2013

Health Resilience Program222 Clients
Engaged AT LEAST 1x on or Before June 30th, 2013

Year 2: Going to Scale
• How do we move from a “portfolio of projects” to a new regional system for high needs members?– How do “Standard Transitions” and “Transitional Care
Teams” become a system of seamless transitions between acute and outpatient care?
• Spreading to more hospitals, engaging more PCP clinics, then specialty, SNFs; care plans that follow patients from outpatient to ED, to hospital … and back
• How do we coordinate all of these efforts at the center of care: PCPH?
Year 2: “Advanced Primary Care”
• 2014: APC Collaborative for PCPCH clinics managing large numbers of high needs patients:– Clinic multi professional teams accountable for the overseeing
management of defined “high needs” panel segment• Dedicated time and resources• Team formed to meeting needs of patients• Defined outcomes and goals for program and enrollees• Structured relationships with mental health, addictions, key specialty• Development of new payment models
– Development of clinic specific models based on resources and needs; collaborative learning
– Supported by Transformation Fund, Health Commons Grant, Health Plans

Year 2: Course Corrections Toward Sustainability
• Who benefits financially from each intervention and would be a potential funder?– Standard Transitions, C Train, ITT: hospitals and health plans wanting to
decrease readmissions– ICCT / HRS: Those at full risk (Health Plans, CCOs, Full risk provider groups)
• “Course correction” mini summits for each intervention with potential “funders:” – What would you do if this were “your” program– What results do you need to see to continue this program for our
members in your organization?
• If a project is not going to be sustainable, shouldn’t we redeploy the resources to meet CCO and CMMI goals?
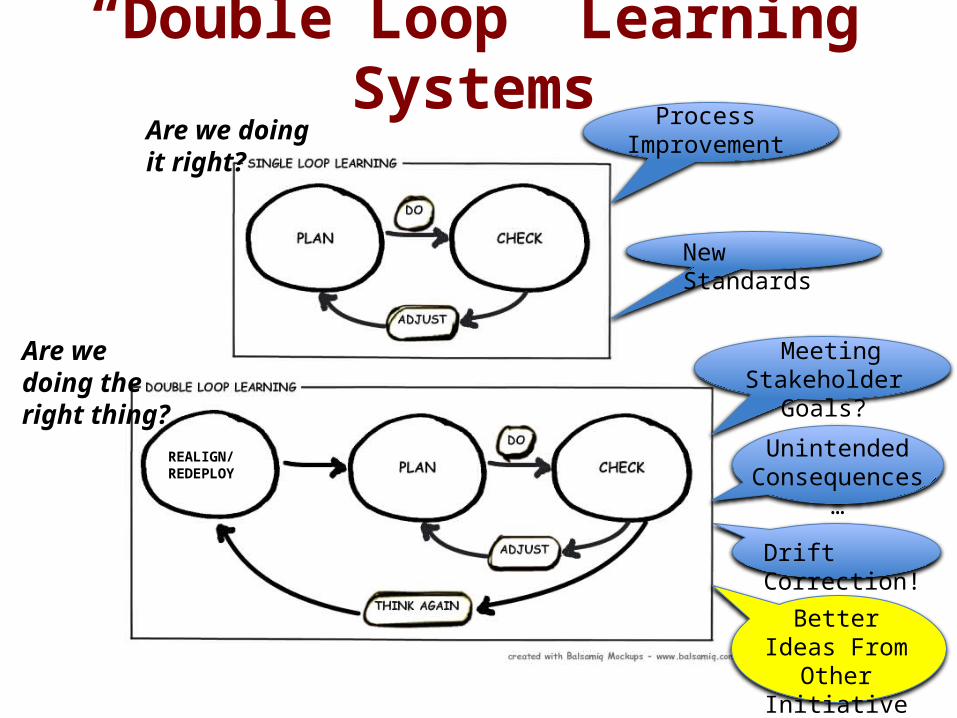
“Double Loop” Learning Systems
REALIGN/ REDEPLOY
Are we doing it right?
Are we doing the right thing?
Process Improvement
New Standards
Meeting Stakeholder Goals?
Unintended Consequences…
Drift Correction!
Better Ideas From Other Initiatives!!!

Year 2: State Complex Care Collaborative
There are mountains beyond mountains...What can we share along
the way?