Embed Size (px)
Citation preview

The Hamburg, W. Germany, 1973 Report Questioning the Reliability o f Breath Alcohol Instruments for Medicolegal Use in Traffic CasesRolla N. Harger1
In the Hamburg area of W. Germany, and apparently in the entire nation, the only chemical test evidence accepted by the courts in traffic cases is that from the analysis of blood, which is drawn exclusively from the cubital (elbow) vein.
Around 1970, a Hamburg physician issued a statement proposing an extensive study using arrested drinking-drivers in which Breathalyzer readings would be compared with results of analysis of blood. This proposal was strongly criticized by v. Below, a Hamburg attorney (39), on the ground that breath alcohol analyses cannot be legally used in W. Germany. As a result of this argument, and further public interest in replacing blood alcohol analyses with breath analyses, and since the latter would save much time and avoid puncturing the body to draw blood samples, the Hamburg senate created a commission to investigate the reliability and legality of breath alcohol instruments.
Following what appears to have been a rather cursory investigation, this commission issued a report, dated April 26, 1973. It is a 15-page document, in German (25). Our rather free translation of the title of the report reads: “The Reliability of Methods of Breath Alcohol Analysis for Estimating the Blood Alcohol Concentration in Forensic Cases” .
Although the authors of the report, J. Lamprecht, a senate director, and K. Leuschner, a senate counsel, are not scientists, the text of the report indicates that the data presented in it were furnished by certain members of the staff of the Hamburg Institute of Forensic Medicine, who have conducted studies on the pharmacology of alcohol, and who are apparently the authors of the conclusions reached by the commission.
An English summary of this Hamburg report appeared in the International Comments section of the November 26,1973 issue of the Journal of the American Medical Association, and is headed, “Breath Alcohol Testing Cannot Replace Blood Alcohol Determination” (2). The anonymous author of this summary evidently did not consult the AM A Committee on Medicolegal Problems (1) regarding the numerous published blood-breath correlation studies with at least a dozen breath alcohol instruments which preceded this Hamburg report, and he is apparently convinced that the Hamburg pronouncements sound the death knell of breath alcohol analyses.
Professor Emeritus o f Biochemistry and Toxicology Indiana University School o f Medicine, Indianapolis, Indiana, U.S.A.
583

584 R. N. Harger
BREATH ALCOHOL INSTRUMENTS AND DEVICES CONSIDERED BY THE COMMISSIONThe scientific evidence on breath alcohol analytical procedures which was considered by the commission is presented in two sections. The first discusses the new Alcotest screening device, and the second deals briefly with three quantitative breath alcohol instruments.
N ew A lco tes t Screening D etecto r TubesThis section describes the results of a study of a new model of the Grosskopf Alcotest detector tube in which the yellow H2 S04-chromic acid section is divided into five subsections, separated by short sections of the white, supporting silica gel. Performance studies with the earlier Alcotest detector tubes have been reviewed by Harger and Forney (17, 18), and a 1968 paper by Day et al. (10) reported a further study with the earlier Alcotest detector tubes.
A supply of the new model Alcotest detector tubes and the suction pump which draws a fixed volume of the subject’s breath through the tube were furnished to the Hamburg police department by the manufacturer, Draeger Co. of nearby Lubeck, W. Germany. Under the supervision of the Hamburg Institute of Forensic Medicine, Hamburg police technicians tested the breath of arrested drinking-drivers with these new Draeger detector tubes, and blood samples from the subjects were analyzed for alcohol content. The correlation results were very disappointing, and the new model Alcotest tubes were rejected for use by the Hamburg police. The commission report makes no mention of the 1968 study by Day (10), or of any earlier studies.
Three Quantitative Breath A lcoh ol Instrum entsBreathalyzer and Ethanographe. The Ethanographe is manufactured by
Etzlinger of Switzerland, and is also called the Alcolinger Automatic. The Hamburg report states, “The Ethanographe is a simplified and technically much improved modification of the Breathalyzer” . However, the report adds that both instruments have the same defect as the Widmark blood alcohol method, namely, the determination of ethanol by the well-known dichromate-H2 S 04 reagent. Since this reagent is not absolutely specific for ethanol, the commission arbitrarily rejected both instruments for use in W. Germany, where the traffic authorities had earlier banned the Widmark blood alcohol method for this reason.
Reliability o f the G-C Intoximeter. The remainder of this 7-page section is devoted to the G-C Intoximeter, including a description of the instrument and a summary of the results of two performance studies of it made by certain staff members of the Hamburg Institute of Forensic Medicine. The report devotes only a few sentences to the procedures and results of these two studies, so I will summarize them more fully.
(a) The 1972 Report of Schmutte, Naeve, Wilhelmi and Brinkmann (34): A 1971 model of the G-C Intoximeter was presented by the manufacturer to the Hamburg Institute of Forensic Medicine for this study. During a period of one hour, 18 subjects ingested alcohol beverages to give blood alcohol concentration (BAC) peak levels of 70 mg/100 ml to 200 mg/100 ml. At ten intervals during 130 minutes after the end of drinking, the subject’s breath was tested with the G-C Intoximeter and blood was simultaneously drawn from the cubital vein for analysis by the Machata

Reliability o f Breath Alcohol Instruments 585
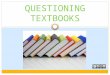
G-C, headspace procedure (26). The paper does not give the raw data for all of these analyses, but does give a peculiar scatter diagram showing the percent deviation between breath and blood values for the 18 blood-breath pairs taken at each of the ten time intervals following the end of drinking (Figure 1).
Figure 1 A type of scatter diagram showing the per cent deviation of G-C Intoximeter readings from cubital vein BAC of 18 drinking subjects at 10 intervals after a 1-hour drinking period. The BAC peaks ranged from 70 to 200 mg/l00 ml. The ordinate scale is in % deviation, with breath > blood above the zero line and the reverse below. Each double triangle encloses all data for that time interval. Abscissa scale, minutes after end of drinking. The ordinate scale magnifies the degree of deviation. Eight horizontal lines have been drawn parallel to the zero line to facilitate estimating the data which are presented as study 24 in Table I. From Schmutte et al. (34).
While the ordinate scale in this graph magnifies the per cent deviations of G-C Intoximeter readings from the corresponding BAC values, it will be seen that at 10 minutes after the end of drinking, the deviations with 14 of the 18 blood-breath pairs were within ±5%, with an average of about +2%, which average decreased to about -8% during the last four test periods. The greatest per cent deviation of breath from blood occurred at 130 minutes after the end of drinking and was about -30% . For four of the subjects, the authors gave the complete blood-breath data as curves, which they call “characteristic” (Figure 2).

586 R. N. Harger
■P
Minuten nach TrinkendeFigure 2 Curves showing G-C Intoximeter readings and cubital vein BAC for 4 of the 18 subjects tested by Schmutte et al. (34). These have been assembled in one figure for comparison. Ordinate scale, °/oo (mg/ml) BAC; to translate to mg/100 ml, multiply by 100. Abscissa scale, minute after end o f drinking. Note that the X axis, if given, would be much below the horizontal lines in the graphs. Heavy lines, cubital vein BAC; dotted lines, G-C Intoximeter readings. The authors term these curves “characteristic”. These data, translated to percentage deviations between breath and blood, are included in Figure 1. From Schmutte et al. (34).
If these four pairs of curves are compared with the X axis, which is not shown, it will be seen that, for three of the subjects, the blood-breath correlation is really quite satisfactory. With three of the subjects, there was a tendency for the breath values to exceed the BAC for 20 to 40 minutes after the end of drinking. This phenomenon is discussed below. Even with the pair of curves in the lower right graph, the breath- blood deviation is fairly uniform, averaging about —16% during the period of 40 to 130 minutes after the end of drinking.
(b) The 1973 Report of Schmutte, Stromeyer and Naeve (35): This is a continuation of the above-mentioned study reported by Schmutte et al. in 1972. The chief purpose of the 1973 investigation was to test the effect of a minute or two of vigorous exercise and, or, hyperventilation, on the G-C Intoximeter reading and the BAC of drinking subjects. The study employed 27 subjects, the drinking time was 1 ,2 or 4 hours, and the maximum BAC did not exceed 190 mg/100 ml. At 12 time intervals, beginning 10 minutes and ending about 200 minutes after the end of drinking, the subject, while resting, was given a G-C Intoximeter test and a sample of cubital vein blood was taken. Shortly afterwards he underwent a brief period of physical exercise and, or, hyperventilation, and breath and blood samples were immediately taken for analysis.

Reliability o f Breath Alcohol Instruments 587
Physical exercise + hyperventilation caused a drop of up to 20 m g/100 ml in the G-C Intoximeter readings, and hyperventilation alone caused an average decrease of about 6 mg/100 ml in the breath readings. In 1965, Monnier reported a similar fall in breath alcohol after vigorous exercise (27). These results are obviously of little importance in practical breath testing of arrested drivers.
The data for the resting phase show a fair correlation between the breath and blood values, with the average G-C Intoximeter reading about 16 mg/100 ml below the BAC. The authors felt that the breath-blood deviations observed were not due to instrumental deficiency of the G-C Intoximeter, but to inherent variations in the blood-breath ratio.CONCLUSIONS OF THE COMMISSION REGARDING QUANTITATIVE BREATH ALCOHOL INSTRUMENTSThese pronouncements of the commission are evidently the conclusions of the staff members of the Hamburg Institute of Forensic Medicine who made the two studies with the G-C Intoximeter.
1. The chief objection of the commission to the use of breath analyses in W. German traffic cases is that, during the period of rising BAC, the breath instrument reading is frequently much above the BAC in the cubital vein. The reason for this discrepancy was apparently known to the Forensic Institute scientists, because the reports states (our translation):
The chief physiological cause for the lack o f agreement between the breath alcohol and blood alcohol readings during the absorption phase is that the alcohol concentration in the blood o f the lungs, which controls the concentration o f alcohol in the alveolar air, is higher than the alcohol concentration o f venous blood in the extremities, which are the officially prescribed sources for blood sampling (by the police physician).
Therefore, under existing W. German regulations, the commission held that the accused driver should have the benefit of the lower BAC of cubital vein blood.
2. While the commission would apparently accept a maximum divergence of ± 10% between the breath instrument reading and the result of direct blood analysis, in the 1972 study of the G-C Intoximeter by Schmutte et al. (34) this requirement was met by only about two-thirds of the blood-breath pairs. However, an examination of Figure 1 will show that, of the 180 blood-breath pairs analyzed by Schmutte et al., there were only 10 pairs wherythe G-C Intoximeter reading exceeded the BAC by more than 10%. About one-fourth of the pairs did have negative deviations exceeding —10%, but according to the reasoning in objection No. 1, such negative deviations should be accepted.
3. While blood samples may be stored for months without alteration of alcohol content, this cannot be done with breath.
4. Under W. German law, blood samples may be taken from the accused driver without his consent, but there is no provision for compulsory breath sampling.
5. Proper analysis of breath requires active cooperation of the subject, and with comatose subjects breath analysis is impossible.
6. Conventional, quantitative breath alcohol instruments are too expensive, cumbersome and fragile to be routinely carried in a police car.
7. There appear to be no scientific grounds for recommending that breath alcohol procedures should replace the official blood alcohol testing program, or even be used for screening purposes.

588 R. N. Harger
COMMENTS ON THE CONCLUSIONS AND PRONOUNCEMENTS OF THE HAMBURG COMMISSIONThe scientific evidence presented to the Hamburg commission involves just one breath alcohol instrument, namely the 1971 model of the G-C Intoximeter. At least six other quantitative breath alcohol instruments were available in 1972, most of which had been used for evidential purposes for years. A search of the literature would have revealed a large number of blood-breath correlation studies with several of these instruments. On this matter, see reviews by Harger and Forney (17, 18). In Table I, the results of 27 such blood-breath correlations, which have been published during the past 20 years, and which involve nine quantitative breath alcohol instruments, are summarized. We will discuss some of these studies in the following paragraphs where some of the conclusions and pronouncements of the Hamburg commission are considered in more detail.
TABLE I Blood/Breath Alcohol Correlations Conducted by Various Investigators with Nine Quantitative Breath Alcohol Instrumentsa
ACCURACY OF BLOOD-BREATH CORRELATIONStudyNumber Date
Percentage o f cases Instrument within and Investigator(s) ±5% ±10% ±15%Fractionbeyond±15%
Arith. mean of Br/Bl. deviation
1 1956 Drunkometer; Reb. Air Harger et al (20) 54 87 98 2 1.3%2 1957 Breathalyzer Chastain et al. (8) 38 62 91 9 -6.7%3 1957 Alcometer Chastain et al (8) 53 78 95 5 -1.3%4 1959 Breathalyzer Coldwell & Smith (9) 30 51 68 32 -10%5 1959 Breathalyzer Fennell (11) 40 68 84 16 -6.1%6 1960 Breathalyzer
Bayley et al. (3) 26 52 72 28 -8.5%7 1963 Breathalyzer
Scroggie (36)Results given in m g/100 ml only:
8 1964 Breathalyzer Begg et al. (4) 5 17 38 62 -17.5% b9 1964 Kitagawa-Wright, Hermes
Begg et al. (4) 31 49 68 32 —1.9%b10 1964 Drunkometer; Reb. Airc Forney et al. (12) 64 86 93 7 -4.0%11 1969 Breathalyzer; w. blood
Franklin (14) 33 59 87 13 -9.7%12 1969 Breathalyzer; Plasma
Franklin (14) 28 59 76 24 -9.9%13 1969 Breathalyzer
Shupe & Pfau (37) 42 61 84 16 -0.3%14 1969 G.C. Alco Analyzer Shupe & Pfau (37) 60 70 75 25 -4.9%15 1969 Alco TectorShupe & Pfau (37) 51 78 88 12 1.7%

Reliability o f Breath Alcohol Instruments 589TABLE I continued
16 1969 G.C. Intoximeter Penton & Forrester(32) 58 61 73 27 -4.3%
17 1969 Breathalyzer Harger & Forney (19) 25 61 80 20 -7.1%
18 1969 Breathalyzer; Reb. Air*1 Harger & Forney (19) 57 74 92 8 -2.2%19 1970 Alcolinger Automatic Bonte et al. (5) 45 66 85 15 +3.6%20 1971 Intoxilyzer; 12 tests only; +2% to -11% Harte (22) -3.2%21 1971 Breathalyzer Prouty & O’Neill (33) 25 57 74 26 -5.2%22 1972 Breathalyzer Morales (28) 31 58 82 18 -0.7%23 1972 G-C Alco Analyzer Morales (28) 15 31 66 34 —13.7%e24 1972 G-C Intoximeter Schmutte et al. (34) 45 65 82 23 —4.4%e25 1973 G-C Intoximetera. Direct analysisb. Indium capsules Hoday (23)
1561
6379 7797 233 —10.2% + 1.8%
26 1974 G-C Intoximeter Morales (28) 34 82 90 9 -6.6% e27 1974 Intoxilyzer Morales (28) 28 65 86 14 -10% e
aAdjusted to employ the 2100/1 ratio for blood/alveolar air, or blood/rebreathed air.^In studies 8 and 9, BAC values below 50 mg % are omitted. cArterial blood.dThese tests followed the preceding tests almost immediately, using the same Breathalyzer and
subjects.Correlation values in the five columns were estimated from a scatter diagram in the authors’ paper,
or report.
Lag in B A C o f Cubital Vein B lood During Rising BACWhile the commission report acknowledges this phenomenon and admits that the readings of a breath alcohol instrument will usually exceed the venous BAC during active absorption, the authors should have added that the arterial BAC controls the alcohol concentration of the brain and, therefore, the degree of intoxication. From this, it follows that, during rising BAC, alveolar or rebreathed air, is far more reliable than cubital vein blood for diagnosing intoxication. In the 1972 paper by Schmutte et al (34), quoted by the commission, the bibliography contains a reference to a 1963 paper by Harger (16) with the title, “Blood Source and Alcohol Level; Errors From Using Venous Blood During Active Absorption” , but the commission report does not acknowledge such errors in W. Germany.
That erroneously low cubital vein BAC values during rising BAC almost certainly occur in traffic cases in W. Germany, is amply confirmed by the results of four studies (6, 7, 29, 31) published by investigators of the group which conducted the performance tests with the G-C Intoximeter described above.
The following is an example of one of these studies (7): Eighteen subjects were used who ingested about 1.15 gm of alcohol per kg of body weight during a period of

590 R. N. Harger
20 minutes. Cubital vein blood samples were taken just prior to, and just after, the drinking period, and at 10-minute intervals ending at 100 minutes after the end of drinking. At each test period, the subject was examined for symptoms of intoxication by two experienced police physicians. The venous BAC values and the clinical diagnosis for each of the 18 subjects obtained immediately after the end of the drinking period, and at the BAC peak, are given in Table II.TABLE II Cubital Vein BAC and Degree o f Intoxication, Following Rather
Rapid Drinking bSubjectNumber
Ten minutes after end of drinking
At time of blood alcohol peak
BAC in m g/100 ml
Degree of intoxication
BAC in m g/100 ml
Degree of intoxication
1 15 Mild intox. 170 Mild intox.2 30 Frank intox. 130 Frank intox.3 30 Frank intox. 135 Frank intox.4 40 Mild intox. 130 Frank intox.5 50 Frank intox. 140 Frank intox.6 50 Mild intox. 153 Frank intox.7 55 Mild intox. 130 Frank intox.8 65 Frank intox. 130 Frank intox.9 65 Mild intox. 155 Frank intox.
10 70 Mild intox. 155 Frank intox.11 75 Frank intox. 130 Frank intox.12 75 Frank intox. 160 Frank intox.13 80 Frank intox. 165 Frank intox.14 85 Mild intox. 130 Mild intox.15 85 Mild intox. 130 Frank intox.16 90 Mild intox. 175 Frank intox.17 100 Frank intox. 140 Frank intox.18 120 Frank intox. 180 Frank intox.
aAlcohol dosage, 1.1 to 1.2 gm/kg ingested in 20 minutes. ^Condensed from two tables in paper by Brinkmann et al. (7)
Immediately after the end of drinking, the cubital vein BAC values ranged from only 15 mg/100 ml to 120 mg/100 ml, but all 18 subjects were diagnosed as intoxicated, half of the subjects showing mild intoxication and half frank intoxication. The BAC peaks were reached in 10 to 90 minutes after the end of drinking and these peak values ranged from 130 to 180 mg/100 ml. At the peak time, two subjects had mild intoxication and the other 16 exhibited frank intoxication. All during the rising BAC phase, most subjects with cubital vein BAC values below 80 mg/100 ml exhibited frank intoxication. In most jurisdictions, the cubital vein BAC findings immediately after the end of the drinking period would have freed all but two of the 18 subjects from a charge of driving under the influence, but a quantitative breath analysis would probably have resulted in a charge of intoxication for all of the subjects. In this study, and in the other three mentioned in the preceding paragraph, no breath alcohol analyses were performed, which is a most unfortunate omission.

Reliability o f Breath Alcohol Instruments 591
Discrepancies Between the G-C In toxim eter Readings and the Cubital Vein BAC
In Table I, included as study 24, are the results of the first investigation of the G-C Intoximeter by Schmutte et al. (34), in which the data from the scatter diagram in Figure 1 are estimated. Three other blood-breath correlations with this instrument are listed in Table I as studies 16, 25 and 26. The distribution of deviations is about the same in study 24 by Schmutte et al., study 25-a by Hoday, and study 16 by Penton and Forrester. However, in study 25-b, and in study 26 by Morales, the G-C Intoximeter results are much better than those reported by Schmutte et al.
An inspection of Table I will show that, in eight of the correlation studies, 1 ,3 , 10, 14, 15, 18, 25-b, and 27, the breath instrument reading and the direct analysis of the subjects’ blood agreed within ±10% for 70 out of 100 to 87 out of 100 of the blood-breath pairs, the average fraction being 79 out of 100. In six of these eight studies, the fraction of the total blood-breath pairs in which the deviation was beyond ±15% was only 2 out of 100 to 9 out of 100. Thus, the performance of some of these breath alcohol instruments does approach the ±10% limits of accuracy which the Hamburg commission would apparently accept.
In the U.S.A., several of the breath alcohol instruments listed in Table I have met the standards of accuracy adopted by the chemical test control agencies of some of the states, and the use of certain ones have been endorsed by the American Medical Association Committee on Medicolegal Problems (1).
Storage o f Breath SamplesContrary to the pronouncement of the Hamburg commission, reliable methods for storing the alcohol from a given volume of alveolar air have been published by Forrester (13), Jones (24), and Harger et al. (20). Also, Penton and Forrester (32) have developed a sterilized indium tube capsule in which alcoholic breath may be stored for months.
The Question o f Com pulsory Breath AnalysisThe members of the Hamburg commission and their scientific advisors were apparently not familiar with the implied consent laws of the U.S.A. and several other countries. With this law, the subject is not forced to give a sample of his breath, but if he refuses his driver’s license is suspended for several months. Fear of this penalty has resulted in very few refusals to furnish a breath sample.
Breath Analyses w ith Unwilling or Comatose SubjectsHarger et al. (21) have reported that, with the Drunkometer procedure employing the alcohol-C02 ratio, it is possible to make reasonably accurate breath alcohol analyses by using a rubber bulb pump to suck the expired air through the instrument after it has left the body and becomes common property.

592 R. N. Harger
ARTERIO VENOUS AND VENO-VENOUS BAC DISCREPANCIES DURING RISING BAC
Arterio-Venous Discrepancies in B A CAs mentioned above, the Hamburg commission did recognize that there may be gross arterio-venous BAC discrepancies during rising BAC, and they point to such discrepancies in the BAC levels of cubital vein and pulmonary vessels, with the latter BAC controlling the alcohol concentration of alveolar air. However, they failed to give the primary physiological reason for the arterio-venous BAC difference. The reason is that the voluntary muscles, which comprise about 40% of the body weight, have relatively poor rate of flow of blood per kg of tissue, as compared with brain, liver and kidney, which reach alcohol storage equilibrium with the arterial blood within a few seconds. With the voluntary muscles, V2 to PA. hours are required to reach alcohol storage equilibrium, and during this time the BAC of the venous return from these muscles lags far behind the corresponding arterial BAC, which, at all times, is practically identical throughout the circulatory system. During this period, there is usually an ‘overshooting’ of the alcohol concentrations in the arterial blood and in the tissues of the brain, liver, kidney, etc. having a very rich blood flow/min/kg. This abnormally high brain alcohol concentration may cause marked intoxication with very low cubital vein BAC. Here, a serious discrepancy between cubital vein BAC and alveolar breath alcohol concentration does not indicate an error in the breath analysis, but an error in using cubital vein blood to estimate the degree o f alcoholic impairment at this time. A review of experimental evidence supporting the above statements appears in the 1 9 6 3 paper of Harger (16), which was mentioned earlier. Later studies with humans by Forney et al. (12), and with rabbits by Gostomyzk et al. (15), give further confirmation of our explanation of the arterio-venous BAC differences and the resulting effects on the degree and course of the alcoholic impairment.
As long as the Hamburg authorities persist in confining their chemical tests for intoxication to cubital vein blood, they surely cannot expect a satisfactory agreement of their blood alcohol values with results from breath analysis, particularly during the rising BAC phase.
Veno-Venous Discrepancies in B A C o f Bilateral VeinsA 1971 paper by Naeve et al. (30) describes a study in which 10 subjects ingested alcohol slowly during 1 Vi hours to give BAC values of 26 to 142 m g/100 ml within the following hour. They then ingested alcohol, 1 gm/kg in 10 minutes. Following this “sturztrunk” , blood samples were taken simultaneously from the right and left cubital veins at 11 intervals during the next 2lA hours, and were analyzed by a modified Widmark method.
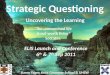
Of the 107 pairs of blood, the BAC of 76 agreed within ±7 mg/100 ml, while with the remaining 31 pairs, the right and left BAC values differed by 10 to 36 m g/100 ml, with an average discrepancy of 20 m g/100 ml. Figure 3 presents the results of this study.
We have translated these absolute deviations into per cent deviations and find that they range from 7% to 21%, with an average of 12.5%. When the per cent deviations for the 107 blood pairs are classified in the manner used in Table I, the deviation distribution becomes: within ±7%, 71 out of 100; within ± 10%, 84 out of 100; within ±15%, 93 out o f 100; and beyond ±15%, 7 out of 100. A survey of the

Reliability o f Breath Alcohol Instruments 593
discrepancies between the BAC levels of right and left cubital veins, makes it evident that, in the simple matter of estimating the BAC of the right cubital vein from that of the corresponding left vein, or vice versa, the degree of inaccuracy is even greater than that of some of the breath alcohol procedures for estimating BAC. It is true that the rate of alcohol intake in the “sturztrunk” is abnormal, but it should be noted that the veno-venous discrepancies continued, unabated, for 2% hours after the “sturztrunk” . From these results, one wonders if some of the blood-breath correlations using cubital vein blood, which have been reported in the literature, might have been different if the opposite cubital vein had been the blood source.
% • BAK
Figure 3 Significant deviations between BAC of right, and of left, cubital veins o f 10 subjects at 11 time intervals during 2‘A hours after ingestion of alcohol, 1 gm/kg, in 10 minutes (“Sturztrunk” = drinking spurt). Ordinate scale, °/oo (mg/ml); to translate to mg/100 ml, multiply by 100. Each black column is the BAC difference for a single veno-venous pair. These comprise 31 of the 107 veno-venous pairs. Only differences above 0.1 °/oo (10 mg/100 ml) are given. Shaded area, average analytical error. Curve, average BAC for the 10 subjects, with standard deviations. We have addedthree parallel lines to facilitate calculation o f the approximate per cent deviation.From Naeve et al. (30).
A 1974 paper by Teige et al. (38) reports an extensive follow-up study of this matter, and states that they could not confirm the findings of Naeve et al. However their experimental procedures differed significantly. In the experiment of Teige et al. each subject’s forearms were immobilized by being held to the arms of his chair, and indwelling catheters remained in the cubital veins during the blood sampling period of two to four hours, with blood samples drawn at one minute or two minute intervals. With the subjects used by Naeve et al., if one forearm was inadvertently exercised more than the other during the experimental period, the difference in rate of bloodflow to the tissues of the two forearms might have caused one to reach storageequilibrium much sooner than the other, altering the BAC of the venous return. Also, the indwelling catheters may have somewhat impeded the venous return from both arms.

594 R. N. Harger
At any rate, the study by Teige et al. covered 667 veno-venous pairs and the deviations for 94% of the pairs were within ±8 mg/100 ml. With the remaining pairs, the deviations ranged from ±9 mg/100 ml to ±16 mg/100 ml. With one subject, the paired samples read 112 and 110 mg/100 ml at 30 minutes, fell to 92 and 96 mg/100 ml at 33 minutes, and then rose to 110 and 108 mg/100 ml at 44 minutes. The maximum change was 20 mg/100 ml in three minutes, indicating at least some inconstancy in cubital vein BAC.
CONCLUDING REMARKSWe trust that our Hamburg co-workers will continue their investigations of quantitative breath alcohol instruments, testing not only the improved G-C Intoximeter, but also several other instruments that show reasonable accuracy (Table I). In these further studies, we hope they will employ arterial blood, or at least fingertip blood, but not cubital vein blood during rising BAC. They might also try rebreathed air, which yielded about the best blood-breath correlations listed in Table I.
REFERENCES1. Anon., Tests for the Determination of Ethyl Alcohol, in Manual on the Medicolegal Aspects of Chemical Tests for Intoxication, C. H. Hine (Ed), American Medical Association, Chicago, 1970. Chapter VI.2. Anon., Breath Alcohol Testing Cannot Replace Blood Alcohol Determinations, International Comments, Journal o f the American Medical Association, 226, 1129 (1973).3. Bayly, R. C., McCallum, N.E.W. and Preston, W.E.L., The Determination o f Blood Alcohol Concentration by Breath Analysis, Proceedings o f the Royal Australian Chemical Institute 27, 157 (1960).4. Begg, T. B., Hill, I. D. and Nickolls, L. C., Breathalyzer and Kitagawa-Wright Methods of Measuring Breath Alcohol British Medical Journal I, 9-15 (1964).5. Bonte, W., Philipp, J-H. and Berg, S., Results o f Breath Alcohol Analyses with the “Alcolinger-Automatic” in the Absorption Phase, Blutalkohol 7 ,454-462 (1970).6. Brinkmann, B., Koops, E. and Naeve, W., The Course o f the Blood Alcohol Curve in the Early Phase After the End o f Drinking, Blutalkohol 9, 94-98 (1972).7. Brinkmann, V. B., Wilhelmi, F., Naeve, W. and Janssen, W., Rapid Drinking (Sturztrunk) and Degree o f Intoxication at Low Blood Alcohol Concentrations, Beitrage zur Gerichtlichen Medizin 30, 65-71 (1973).8. Chastain, J. D., Strauss, H. J. and Maupin, C. W., A Correlation Study o f Blood Alcohol Levels as Determined by Alcometer, Breathalyzer and Direct Blood Analyses Including Blood-Urine Ratio. Texas Department o f Public Safety, Austin, Texas, 1957.9. Coldwell, B. B., and Smith, H. W., Alcohol Levels in Body Fluids After Ingestion o f Distilled
Spirits, Canadian Journal o f Biochemistry and Physiology 37, 43-52 (1959).10. Day, M., Muir, G. G. and Watkins, J., Evaluation o f ‘Alcotest R 80’ Reagent Tubes, Nature
219, 1051-1052(1968).11. Fennell, E. J., Address in Panel on Chemical Tests, Proceedings of the Symposium on Alcohol and Road Traffic, Indiana Univ., 1958, Department o f Police Administration,
Indiana University, Bloomington, Indiana (1969). Pp 88-109.12. Forney, R. B., Hughes, F. W., Harger, R. N. and Richards, A. B., Alcohol Distribution in the Vascular System; Concentration o f Orally Administered Alcohol in Blood from Various
Points in the Vascular System, and in Rebreathed Air, During Absorption, Quarterly Journal of Studies on Alcohol 25, 205-217 (1964).13. Forrester, G. C., Photoelectric Intoximeter Manual. Intoximeter Association, Niagara Falls, N.Y., 1958.