Embed Size (px)
Citation preview

1
The Hall Technique: Food for Thought
A novel technique using preformed metal crowns for managing
carious primary molars in general practice – A retrospective
analysis. Innes et al. BDJ (2006) 200: 451-454.− No local analgesia or tooth preparation− Ultraconservative (no) caries removal; sealed under SSC

2
Hall’s Clinical Trial Design
Patient
1 toothTreated with crown
Contralateral toothtreated with filling
Age 4-9; good quality radiographsMatched decay in similar teeth
procedure detailsrecorded
procedure detailsrecorded

3
Hall’s Clinical Trial Algorithm
treatment appointment
1 year recall
2 year recall
emergency appointments
recorded
emergency appointments
recorded

4
Hall Technique Procedure
● Child upright● Smallest size of
crown which would seat was chosen
● Should cover all cusps with feeling of “spring back”
● No attempt to seat crown at try in

5
Hall Technique Procedure, cont● Crown placed over tooth
and partially seated until crown engaged with the contact points
● Finger removed and child encouraged to bite into place
• Or crown fully seated with firm finger pressure alone
● Extruded cement removed from margins
● Child asked to bite firmly on the crown for 2 – 3 minutes or crown held with firm finger pressure

6
Results from DDS View
Dentists’ estimation of
discomfort experienced by child
Hall Technique
Conventional Technique
1 - no apparent discomfort 61 33
2 - very mild, almost trivial 32 36
3 - mild, not significant 25 34
4 - moderate, but child coped 12 23
5 - significant and unacceptable 2 6
Total number of patients 132 132

7
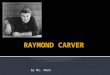
Preferred Technique by DDS, Child and Parent
Patient/ carer/ dentist preference (n= 132)
83
97
28
17
23
9
32
12
95
0
20
40
60
80
100
120
child parent dentist
Hall technique
Conventional technique
No preference expressed
Child Parent Dentist

8
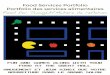
The PedoNatural Crown
The Future?Esthetic full coverage restorationsUsed with a GIC and acrylic systemCrown form concept has adaptable margins and reported good seal and strength
Pre-op Post-op Crown Forms
TM
www.PedoNaturalCrown.com

9
Summary of Evidence
● SSCs outlast other restorations● Manipulation of the tooth and the crown can
be minimalized with no apparent effect on quality
● No posterior non-metal crown has been shown to perform as well as the stainless steel crown

10
Shadow of a Doubt: A New Clinical Dilemma in Composite
DentistryComposite dentistry has created a new set of clinical dilemmas for the pediatric dentist. Caries sealed into teeth is advised to be arrested. Shadows under sealants may be stain or caries. Radiolucencies under various composite formulations may be bases, caries or voids.

11
Shadow of a Doubt: Evidence?
● Reseal all broken sealants● Caries is arrested under
sealants● Visual caries diagnosis is as
good as explorer or digital● Composite longevity
<amalgam< stainless steel crown

12
Today’s Teen Dilemma: Treating Incipiencies in Permanent Teeth
The advent of “Dew Mouth” and similar carbonated beverage related caries patterns challenges the pediatric dentist’s traditional skills to manage these with least invasive techniques

13
Beyond Prevention But Before Restoration – Resin Infiltration
● When bitewings show incipient lesions beyond remineralization
● Hydrochloric acid (15%) for 90-120 seconds
● Infiltrate with fluid resin, floss excess away and light cure
● Preliminary evidence suggests that enamel is resistant to decalcification

14
Does It Work: Early Results
Paris S, Meyer-Lueckel H. Radiographic comparison of lesion progression after infiltration and standard therapy – in vivo-18 months follow-up.
● Split mouth design● One tooth received infiltration● All patients were instructed on
F toothpaste use and flossing

15
Management of Occlusal Surfaces
● No compelling evidence for how best to manage these surfaces on young permanent teeth
● Risk assessment has marginal sensitivity and specificity• We really don’t know which teeth should be sealed,
receive enameloplasty, or have composites placed● The type of composite (filler content) is also a clinician’s
choice● The use of bases also has little evidentiary support



More Fluoride Myths ?
Fluoride use in infants and pre-school aged children is controversial. Mechanisms of action and dosages continue to be debated. Initial fluoride supplement dosages were empirical. Fluoride is ubiquitous in a child’s diet. Fluorosis reports are increasing. Should caries risk of children be performed before fluoride prescribing? The ‘shotgun’ approach is no longer acceptable. Is fluorosis preferable to caries? Should non-dentists apply fluoride varnish? We are ‘floundering in a fluoride fog’! Will EBD lead us out of the fog?
MYTHBUSTERSMYTHBUSTERS
Trooth-Trooth-bustersbusters

Recent fluoride factoids
● Bottled water and caries increase.● Formula, breast milk and fluoride.● Risk periods for dental fluorosis● Fluoride toothpaste- a pea, a smear or none?

Bottled water and caries
● Bottle water sales leveled off in 2008.
● Most bottled water has little fluoride.
● FDA ‘health claim’ for bottled water?
● Evidence?● No conclusive evidence of
an association between increased caries and bottle use.
1. Cochrane- nothing
2. ADA EBD- nothing
3. PubMed-• An investigation of bottled water use and caries in the mixed dentition.
• Broffitt B, Levy SM, Warren JJ, Cavanaugh JE.
• J Public Health Dent. 2007 Summer;67(3):151-8.
• For the dental patient. The facts about bottled water.• J Am Dent Assoc. 2003
Sep;134(9):1287.

Formula, breast milk and fluoride
Myths or facts?● Breast milk has little fluoride.● Infant formula should be mixed
with fluoride free water.● Soy based formula has little
fluoride.● All infants should receive a
fluoride supplement beginning shortly after birth.
● Pregnant mothers should receive a fluoride supplement.
Evidence● Breast milk- 0.02 ppm. Koparal et al 2000
● Fluoride in infant formula causing fluorosis- weak evidence.
Hujoel et al 2009
● Soy based formula-up to 0.70ppm. Pagliari et al 2006
Prenatal fluoride supplements have no benefits Leverett et al 1997
● Reexamine the use of fluoride supplements during the first 6 years.
Ismail and Hasson 2008

Risk period for dental fluorosis
● Cochrane Collaboration: 1. Topical fluoride as a cause of dental fluorosis in children
(In preparation)May CM Wong1, Anne-Marie Glenny2, Boyd WK Tsang1, Edward CM Lo1, Helen V Worthington2, Valeria CC Marinho3
ADA EBD: 1. Fluoride supplements, dental caries and fluorosis
: a systematic review Ismail AI, Hasson H. Journal of the American Dental Association. 2008; 139(11):1457-68
2. Risk periods" associated with the development of dental fluorosis in maxillary permanent central incisors: a meta-analysis Bardsen A. Acta Odontol Scand. 1999; 57(5):247-56
PubMed: 1. Fluoride supplements, dental caries and fluorosis
: a systematic review. Ismail AI, Hasson H. J Am Dent Assoc. 2008 Nov;139(11):1457-68.
2.Considerations on optimal fluoride intake using dental fluorosis and dental caries outcomes--a longitudinal study.
Warren JJ, Levy SM, Broffitt B, Cavanaugh JE, Kanellis MJ, Weber-Gasparoni K.
J Public Health Dent. 2009 Spring;69(2):111-5. 3. Timing of fluoride intake in relation to development of
fluorosis on maxillary central incisors. Hong L, Levy SM, Broffitt B, Warren JJ, Kanellis MJ, Wefel JS, Dawson
DV. Community Dent Oral Epidemiol. 2006 Aug;34(4):299-309
EB response:
Maxillary permanent central incisors appear most at risk from fluoride during the first 24 months of life, especially between 6 and 24 months.
Timing is important but the cumulative duration of a fluoride level must also be noted.
Duration of fluoride exposure rather than the specific period better explains the development of fluorosis.
22

Ribbon, Pea or smear- how much toothpaste on the
brush?
● Ribbon of 1000ppm F toothpaste=1g=1mg of fluoride
● Children under 6 years swallow 24-60% toothpaste from their brush
● Pea size amount= ¼ g● Unregulated amounts of fluoride
toothpaste can contribute to fluorosis 1. Prevention and management of
dental decay in the preschool child. SIGN 2005
2. Fluoride recommendations for high-risk children MCHB- DHHS 2007
3. Guideline on Fluoride therapy. AAPD 2008.
1. Brushing twice a day- one just before bed and supervised
2. Smear for high risk children under 2 years
3. Pea sized amount for children 2-5 years.
4. Rinsing after brushing should be kept to a minimum
5. Tooth brushing should began as soon as the primary teeth erupt
6. No evidence to support the ‘wiping’ of the infants predent alveolar ridges
23


25
Medical Advances in Pediatric Health
MYTHBUSTERS
Trooth-Busters

26
Myths About Devices
“If it’s embedded, it’s premedded”
is a common misconception in
dentistry. With more foreign
objects being used in pediatric
health care, what is the evidence
for using antibiotics?

27
VP Shunts: Anything New?
● Used for CSF drainage● Classically have been
premedicated with ABs● Now may have electronic
controls so sensitive to some office devices
• No need for ABs except maybe in first six months while epithelialization is taking place

28
Baclofen PumpContinuous Medication for CP
● Baclofen is a muscle relaxant to address spasticity in CP
● The baclofen pump system is intrathecal delivery of GABA
● The system is a catheter and pump - a round metal disc, about 1 inch thick and 3 inches in diameter surgically placed under the skin at the abdomen
• No IE coverage needed
29
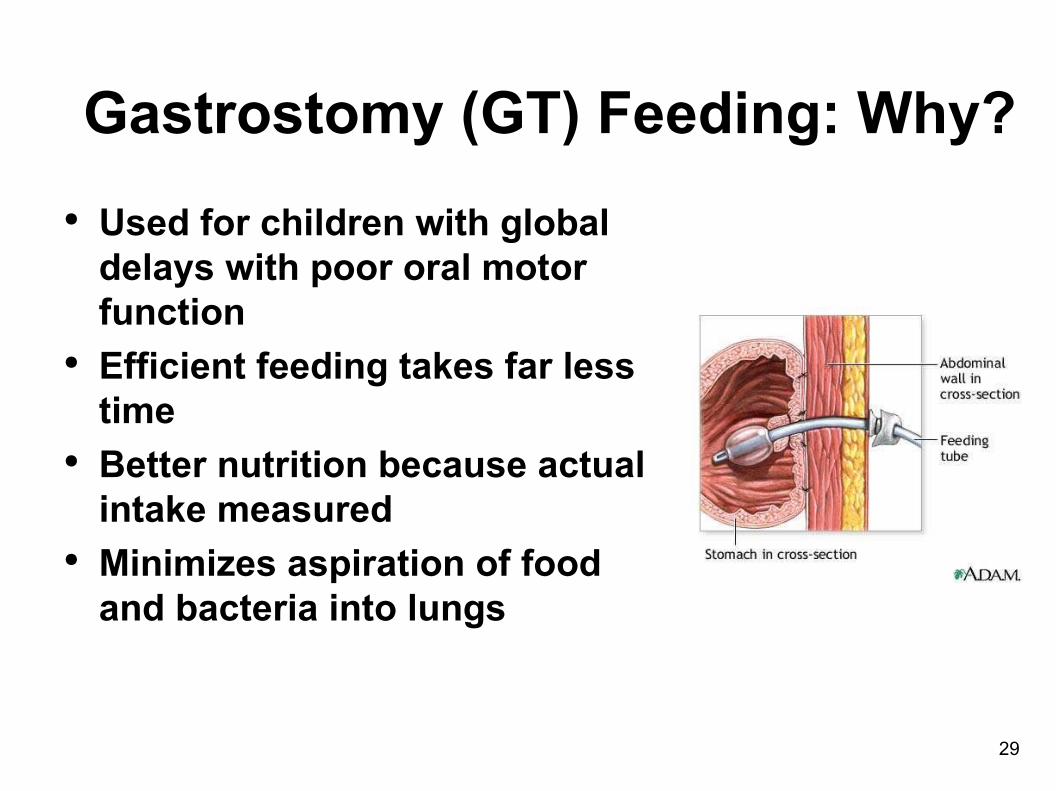
Gastrostomy (GT) Feeding: Why?
● Used for children with global delays with poor oral motor function
● Efficient feeding takes far less time
● Better nutrition because actual intake measured
● Minimizes aspiration of food and bacteria into lungs

30
Why So Much Calculus?● Salivary gland changes?● Decreased saliva flow due
to medications?● Chronic state of
dehydration?● Lack of hygiene?● Lack of chewing and food
abrasion?● Increased serum calcium?

31
Managing Calculus Build UpEvidence on more frequent cleaning:● Jawadi A et al. found that there was an
association between calculus and aspiration pneumonia (AP)
● Brown L et al. found that use of an OTC tartar reduction dentifrice was more effective than regular fluoride-containing child toothpaste in preventing calculus accumulation in tube fed children
● Calculus reduced > 50% with TCTP

32
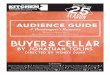
Imaging: What You Need to Know● MRIs are distorted because of
metallic dental restorations, but do not compromise treatment
● Increased use of interventional radiology and 3D imaging make this an issue
• Is CT or MRI needed for improved outcomes?
• Cone beam CT and risk of future cancers and evidence of any benefit – medicine is seeing a rash of new unexpected cancers now being attributed to CAT scans
Vitamin capsule
ssc
Titanium implant

33
Non-Invasive Heart Procedures
● Pacemakers● Stints and other
devices● Ask the MD
• The underlying heart disease is usually the determinant of need for IE

34
Other Concerns
● Pacemakers and other programmable devices are susceptible to electromagnetic radiation
● Shielding and refinements in cellphones and devices reducing risk
• No IE coverage needed

35
What About Solid Tumors?
● Limb sparing rather than amputation is becoming more common in bone tumors
● Consult with heme/onc MD about antibiotic coverage

36
MD/DDS Joint-Joint Statement• American Dental Association/American Academy of
Orthopaedic Surgeons. Antibiotic prophylaxis for dental patients with total joint replacements. JADA 2003;134:895-9.
● This was update of 1997 policy● No antibiotics for pins, plates, and screws and none for most● The risk-benefit ratio for use of antibiotics does not support
use in joint replacement patients● Might consider use of antibiotics if patient is
immunocompromised , in first 6 months post-operatively or has a history of previous replacement gone bad due to infection
● Consult with orthopedic surgeon when in doubt

37
What is a Vagal Nerve Stimulator ?
● Alters blood flow in thalamus● Thalamic blood correlated
with seizure thresholds● Exact mechanism of action is
unknown…● Intractable epilepsy● Treatment-resistant clinical
depression
• No IE coverage needed

38
Central Venous Access Devices● CVADs may be used in
cancer, cystic fibrosis, IDDM, bleeding disorders for TPN, blood products and sampling
● AKA: in-dwelling cath, Hickman, Broviac, Medi-port
● Prone to infection but almost always due to skin organisms
• Antibiotics are not necessary and in fact discouraged
39
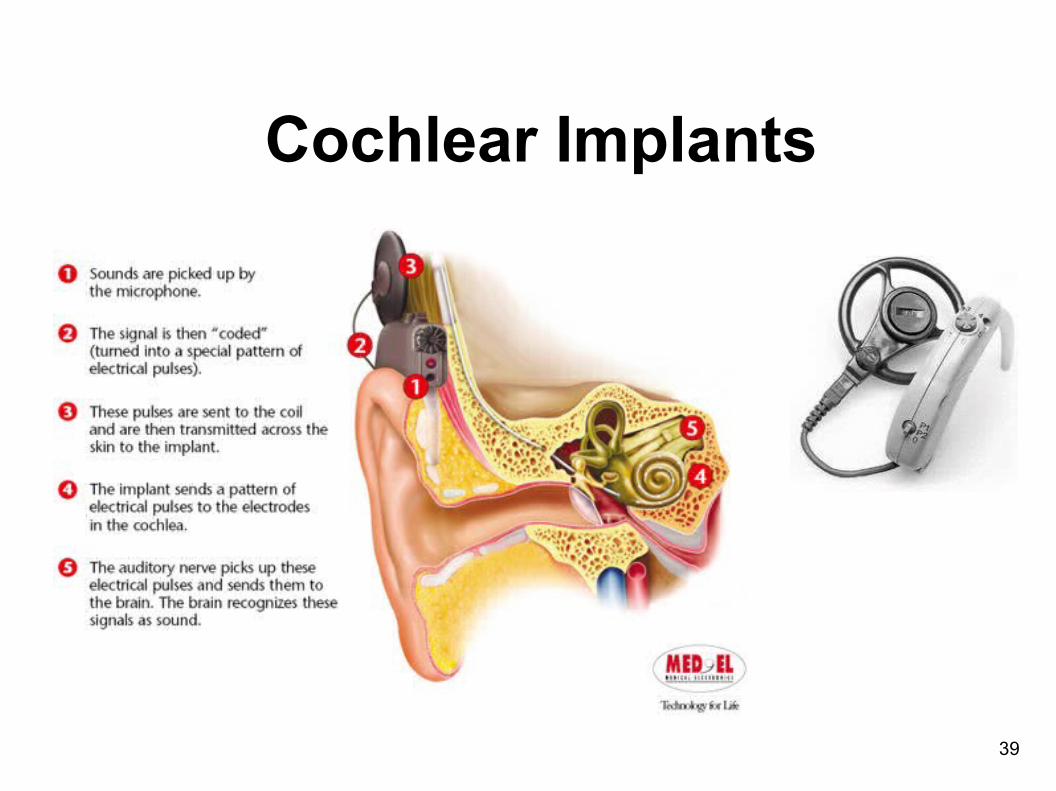
Cochlear Implants

40
Cochlear Implants: What Do I Need to Know?
● If infected, probably due to OM or skin organisms
● Chorda tympani injured in about 40% of surgeries so taste may be altered temporarily
• No antibiotic premed is needed

41
Juvenile Diabetes: The Pump
● Insulin pumps are becoming more common
● Patients with pumps went from 6600 to 195,00 from 1990-2002
● Clinically shown to reduce hypoglycemia and glycosuria
● Provide insulin small doses into abdominal subcutaneous fat
• No antibiotic coverage needed

42
I’m No Slug – I Know My Drugs!
But Do You?
Pediatric care has advanced rapidly and many medications are being re-examined for use in conditions previously treated with other medications – some may surprise challenge your understanding of disease pathophysiology

43
Botox: Hope for Sialorrhea?
Jongerius et al: Effect of botulinum toxin in the treatment of drooling: a controlled study. Pediatrics 2004;114(3):620-27.
● Both transdermal scopolamine and injected Botox reduced drooling but Botox had fewer and less significant side effects
● Maximum effect was at 2-8 weeks post-injection

44
Botox: Replacing Surgery for Limb Contractures in Cerebral Palsy
● Abnormal muscle balance in CP leads to contractures
● Selective dorsal rhizotomy and tendon release surgery may be replaced by Botox

45
Botox: Self-Mutilation Management
● Botox is being tested to reduce neuropathologic chewing in cases of closed head injury, toxic coma, and other neurologic conditions
● Botox offers the advantage of localized rather than systemic effects

46
Methotrexate: Low Dose Use
● Traditional anticancer drug used in many pediatric cancers
● Now used for rheumatoid arthritis, psoriasis, cancers, lupus and other immune-based disorders
• Always check blood counts

47
Thalidomide: For Immune Disorders
● Thalidomide caused an epidemic of phocomelia in Great Britain in the second half of the 20th century when used by pregnant women for nausea
● Children, adolescents and young adults with refractory JRA, psoriasis, severe ulcerative conditions, sickle cell and lupus may take thalidomide
• Sarmadi M, Ship JA. Refractory major apthous stomatitis with systemic immunosuppressants: a case report. Quintessence Int 2004;35:39-48

48
What About Induced (Intended or Not) Hypocoagulation
● Aspirin and Coumadin for heart disease
● Aspirin or similar compounds for joint pain in JRA
● Heparin for dialysis at any age (can be reversed)
● Discontinuation for dental surgery not always necessary
● When taking low dose for reduction of platelet aggregation, may not be necessary
• Blood tests such as bleeding time and platelet function tests unreliable

49
Aspirin: Keep Taking It!Douketis JD, Berger PB, Dunn AS et al. The perioperative management of antithrombotic therapy. American College of Chest Physicians’ evidenced-based clinical practice guidelines (8th edition). Chest 2008;133:299S-339S.
● No need to discontinue aspirin for dental procedures● No need to do platelet function assays which may be
equivocal● Be sure to advise the MD because it may be assumed ASA
will be stopped● Nasal intubation is not contraindicated in patients taking
low dose ASA
50
Flip-Flop for 1st Line Asthma Drugs
• Redding GJ et al. Changes in recommended treatment for mild and moderate asthma. J Family Pract 2004;53:692-700.
● Children with exacerbations < 6 weeks apart, > 4 episodes of wheezing per year and have risk factors of atopy, allergic rhinitis and wheezing qualify for controller therapy and are considered to have persistent asthma
• Inhaled corticosteroids now the first line of defense● ICs improve lung function● Cromolyn not considered front line● Long-acting beta-2 adrenergic agonists no longer used as monotherapy
because of lung deterioration