Embed Size (px)
Citation preview

The Green LightMedicinal Cannabis in New York
Authored/Presented by Dave Porter, Pharm.D Candidate
via Albany College of Pharmacy and Health Sciences
Thursday, February 12th, 2015

Presentation Outline
• Background
• History
• A Case Study: Charlotte’s Web
• Science and Studies
• Proposed NYS Regulations
• Legal Challenges
• Conclusions
• Q&A Session
2

But First…
• Things I WILL NOT be doing in this presentation:
– Arguing for the legalization of recreational cannabis
– Supporting use of medicinal cannabis by non-patients
– Using street slang like pot, bud, kush, dope, chronic, etc.
• Things I WILL be doing in this presentation:
– Presenting a professional evidence-based viewpoint, supporting a reclassification of cannabis to Schedule II
– Reviewing published clinical studies
– Reviewing New York’s proposed regulations (2014)
– Withholding personal opinions, unless prompted3

General and Historical Background
• The cannabis plant (Cannabis sativa, C. indica and C. ruderalis) is an annual flowering herb
– It has more than 60 unique compounds (~480 total)
– Δ-9-tetrahydrocannabinol (THC) is psychoactive
– Cannabidiol (CBD) is not; may oppose some THC effects
• Earliest recorded use of medicinal cannabis (“ma”) dates back to 2900BC – Chinese Emperor Fu Hsi
– Emperor Shen Nung discovers healing property (2700BC)
• Used as sacramental, medicinal or recreational drug
– Arab physician Ibn Wahshiyah – potentially poisonous?4

5

History in the USA
• 1851 – United States Pharmacopoeia (USP) lists Cannabis sativa as a legitimate drug with many uses
• 1864 – USP described methods of extracting alkaloids
• 1911 – Massachusetts is first State to ban cannabis outright
• 1937 – Marijuana Tax Act placed a tax on cannabis products
• 1970 – Controlled Substances Act; Schedule I classification
• 1996 – California legalizes cannabis for medicinal purposes
• 1998 – 105th Congress upholds Schedule I classification
• 1999 – IOM’s Marijuana and Medicine report
• 2002-2005 – Gonsales vs. Raich trial
• 2012 – WA and CO legalize recreational cannabis
• 2014 – New York passes the Compassionate Care Act6
Case Study – Charlotte Figi
• Charlotte is a 5 year old female with Dravet Syndrome, a rare and severe form of profoundly treatment-resistant epilepsy. She suffers ~300 grand mal seizures per week. Unable to walk, talk and eat independently. Parents have tried all anti-seizure drugs indicated for Charlotte’s condition, as well as some experimental ones, to little or no effect. Brain damage and cognitive decline noted. Last-line brain surgery or induction of a medical coma?
• Parents found a video of a boy with severe epilepsy treated and controlled with an oil high in cannabidiol (CBD)
• Parents met with >100 doctors before they found two who would recommend medicinal cannabis to treat Charlotte
7

Case Study – Charlotte Figi

• Charlotte’s Parents obtained oil (“R4”) high in CBD
– Seizure rate decreased from 300/week to 1-2/week
• High CBD/Low THC cannabis was rare in Colorado
• Parents contacted the Stanley family, who own one of the largest cannabis dispensaries in Colorado
– They modified one of their existing strains of product to be even higher in CBD
Case Study – Charlotte Figi
– They called it “Charlotte’s Web”
– Extracted into oils called “Alepsia” and “Realm Oil” (~30:1 CBD:THC)
– Realm of Caring Foundation

Case Study – Charlotte Figi
• Charlotte today:
– Only has 2-3 seizures/month and regained the ability to walk, talk, eat, and lead a normal life
• “Charlotte’s Web” is now nationally known
– Featured by Dr. Sanjay Gupta (CNN’s Weed)
– 9,000 patients on the waiting list as of September 2014*

Prevalence of Use and Legal Status
• 23 States (plus the District of Columbia and Guam) have legislature in place for medicinal cannabis
– Some States have legalized it recently, but have no programs implemented yet (MD, MN, NH, NY)
• Estimates of over 2,000,000* medicinal cannabis patients in the USA in October 2014
– Some States have voluntary registration (CA, ME) or do not have any registration policies (WA)
• 11 States (AL, FL, IA, KY, MS, MO, NC, SC, TN, UT, WI) have passed laws legalizing some aspect*
11
The Institute of Medicine Report (1999)
• The Clinton Administration tasked the IOM with investigating alleged “gateway effects” of cannabis
– Published a 170 page report – Marijuana and Medicine
– “Gateway effect” greatly questioned (tobacco/alcohol)
– Cannabis treats chronic pain and physical symptoms with a different MOA in the brain than current drugs
– A lack of concrete recommendations and conclusions, but many statements calling for additional research*
• 15 out of 18 total recommendations!
– “The acute side effects of marijuana use are within the risks tolerated for many medications”
12

Clinical Trial Evidence
• “Cannabis in painful HIV-associated sensory neuropathy” – Abrams et al. (2007)
• Prospective, randomized placebo-controlled trial
– Adults with HIV and an average baseline daily pain score of 50mm on the 100mm visual analog scale (VAS)
• 223 screened, 55 randomized, 50 completed (25/25)
– Primary outcome: ≥30% reduction in VAS pain intensity
– Patients were randomly assigned to smoke 3.56% THC cannabis cigarettes or placebo cigarettes lacking alkaloids TID x 5 days
13

Clinical Trial Evidence
• Results:
– 50 patients completed the trial
– ≥30% reduction in pain variables reported by 53% in the cannabis group vs. 24% in the placebo group (p=0.04)
– Median reduction of pain on the VAS was 34%, compared to 17% in placebo group (p=0.03)
– Median 72% pain reduction with the first cannabis cigarette vs. 15% with placebo (p<0.001)
– No serious adverse events were reported
• Mild: Anxiety, sedation, disorientation, confusion, dizziness
• No patients left the study due to adverse effects14
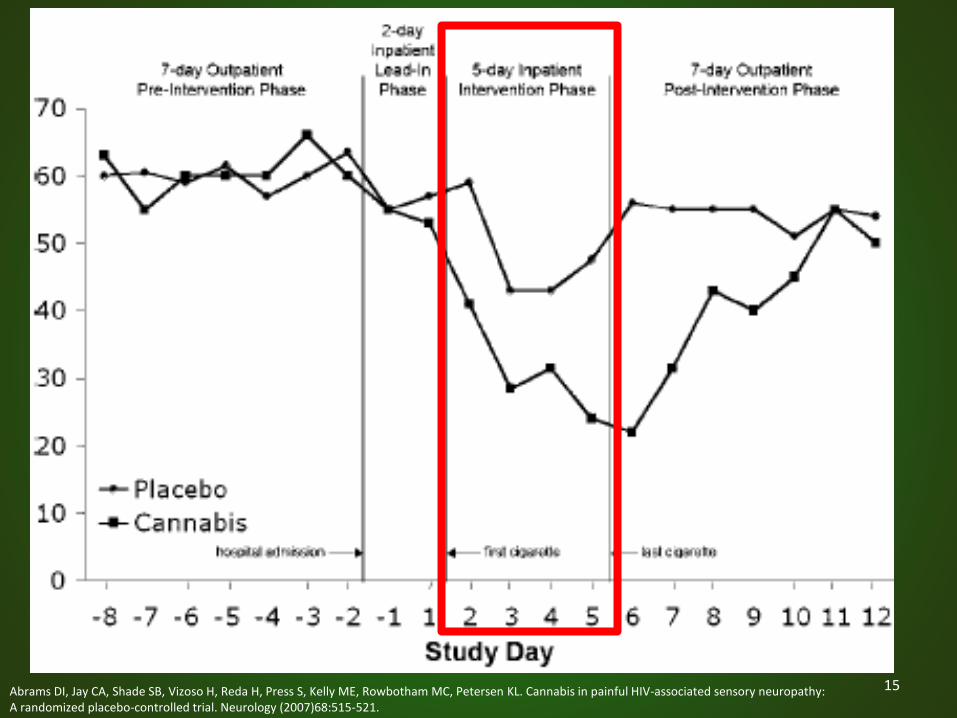
15Abrams DI, Jay CA, Shade SB, Vizoso H, Reda H, Press S, Kelly ME, Rowbotham MC, Petersen KL. Cannabis in painful HIV-associated sensory neuropathy: A randomized placebo-controlled trial. Neurology (2007)68:515-521.
Clinical Trial Evidence
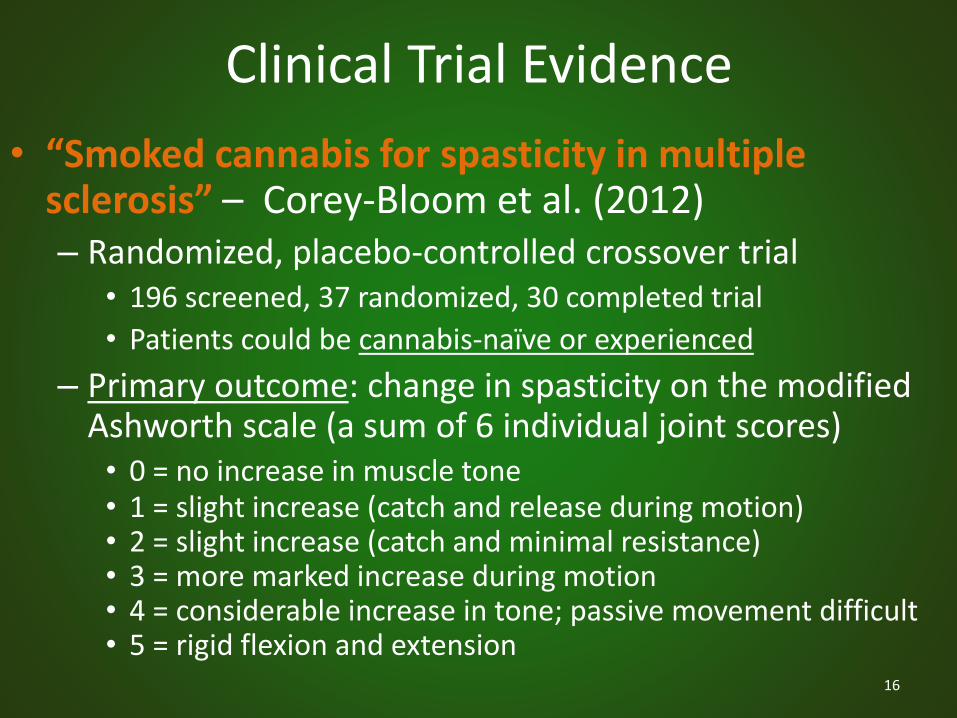
• “Smoked cannabis for spasticity in multiple sclerosis” – Corey-Bloom et al. (2012)– Randomized, placebo-controlled crossover trial
• 196 screened, 37 randomized, 30 completed trial
• Patients could be cannabis-naïve or experienced
– Primary outcome: change in spasticity on the modified Ashworth scale (a sum of 6 individual joint scores)• 0 = no increase in muscle tone• 1 = slight increase (catch and release during motion)• 2 = slight increase (catch and minimal resistance)• 3 = more marked increase during motion• 4 = considerable increase in tone; passive movement difficult• 5 = rigid flexion and extension
16

Clinical Trial Evidence
• Participants smoked either a placebo or a cannabis cigarette (4% THC), using the Foltin Puff Procedure
– 3 visits per treatment phase
• Phase 1 was followed by 11-day washout, then patients crossed over to opposite group for phase 2
• Results:
– Cannabis use decreased spasticity an additional 2.74 points vs. placebo on the modified Ashworth scale
– Cannabis reduced VAS scores by 5.28 points
– 7 dropouts did not affect results in sensitivity analysis*17

Clinical Trial Evidence
18Adapted from Corey-Bloom J, Wolfson T, Gamst A, Jin S, Marcotte T, Bentley H, Gouaux B. Smoked cannabis for spasticity in multiple sclerosis: a randomized, placebo-controlled trial. CMAJ (2012);184(10):1143-50.

19Corey-Bloom J, Wolfson T, Gamst A, Jin S, Marcotte T, Bentley H, Gouaux B. Smoked cannabis for spasticity in multiple sclerosis: a randomized, placebo-controlled trial. CMAJ (2012);184(10):1143-50.

Study Limitations
• Small sample sizes in all studies
– Restrictive nature of Schedule I research
• Difficult to blind the subjects
– Not difficult for patients to realize they ingested THC…
• Most studies haven’t included patients who were cannabis-naïve at onset of trial
– Abrams et al. (2007) didn’t have authorization from NIH to expose naïve patients to cannabis
• Difficult to standardize the cannabinoid doses
– Foltin Puff Procedure used in most clinical trials20

New York State Bills and Regulations
• New York Assembly Bill A06357
– Introduced 3/26/2013, passed 6/19/2014
– Introduced by Assembly member Richard Gottfried (D)
– Passed Senate on 6/20/2014
– Signed into law by Gov. Andrew Cuomo on 7/5/2014
– Regulations drafted 12/18/2014
• Title 10 of Official Compilation of Codes, Rules and Regulations of the State of New York was amended to include §80-1: Medical Use of Marihuana
21

Requirements for Prescribers
• Must have a medical license in good standing in NYS
• Must complete a NYSDOH-approved 4 hour course– This course WILL NOT count for CE credit
– Course must include pharmacology, CI’s, W/P’s, ADR’s, OD/abuse prevention, DDI’s, dosing, and the approved products and their routes of administration
– Course would be somewhat similar to a buprenorphine prescribing course to treat opioid dependence
• Eligible Prescribers may issue Certifications to eligible Patients and/or Caregivers– Must include a statement saying other treatment
options have not provided adequate relief to the Patient

Requirements for Prescribers
• Prescribers must be qualified to treat ≥1 of the following chronic health conditions:1. Cancer2. HIV/AIDS3. Epilepsy4. Neuropathies5. Amyotrophic lateral sclerosis (ALS)6. Huntington’s disease7. Parkinson’s disease8. Multiple sclerosis (MS)9. Inflammatory bowel disease (IBD)10. Damage to spinal cord nervous tissue with intractable spasticity
• The Commissioner may add or remove approved conditions and must decide by January 2016 to add PTSD, muscular dystrophy, Alzheimer’s, dystonia, and rheumatoid arthritis

Disease-Accompanying Symptoms
• One or more of the conditions must include:
1. Severe or chronic pain causing a substantial limitation of function
24
2. Severe nausea
3. Seizures
4. Cachexia or wasting syndrome
5. Severe or persistent muscle spasms
• The Commissioner may add or remove disease-accompanying symptoms

Prescribing or Recommending?
• Prescribers can’t prescribe medicinal cannabis on an Official New York State Prescription Blank, but they can “recommend” it on separate forms
• On the recommendation form must be written:– Patient-specific information (like a regular prescription)
– Authorized cannabis brand and formulation
– Dosing information for patient’ proper use
– Any limitations to the use of the approved product
– The total amount of product that can be dispensed
• Quantity can NEVER exceed a 30 day supply!
• Prescriber must retain records for 5 years25

26Grant I, Atkinson JH, Gouaux B, Wilsey B. Medical Marijuana: Clearing Away the Smoke. The Open Neurology Journal (2012);6:18-25.

Requirements for Patients or Caregivers
• Prescriber-issued Certifications expire in ONE year
– Terminally ill certifications last until death or revocation
• Patients or Caregivers must register with NYSDOH to be added in registry and pay annual fee of $50*
• Dependent Patients may appoint TWO Caregivers
– Each approved Caregiver can have FIVE Patients
– Persons under 18 require approved Caregivers ≥21
• Patient may not vaporize Products in public places or any place that has banned smoking cigarettes
• Purchasing party must pay cash to buy products27

Example Registration Cards (New Jersey)
28

Requirements for Manufacturer Applications
• Each Applicant must pay fees to submit Application
– Application fee is a nonrefundable $10,000
– Registration fee is a refundable $200,000, if approved
• Each Manufacturer must submit:
– Standard operating procedures (SOPs)
– Disposal, security and control procedures
– Product details
– Architecture plans
– Quality assurance plans
– Lab test protocols29

Requirements for Manufacturer Applications
• Must renew Certification every 2 years (same fees)
– Renewal must be received no less than FOUR months before Manufacturer Certification expiration
– Applicant must include all complaints received, SOPs changes, lab test reports and theft/loss reports
– Applicant must include quality assurance summary for all Products tested in prior year, and any shortage dates
• The Commissioner can reject or void Certifications, Applications (including renewals) at any time and without advance notice if NYSDOH believes that medicinal cannabis endangers public health!
30

Requirements for Manufacturers
• FIVE Manufacturers will be established in New York
– NYSDOH expects over 100 Applications
• Each Manufacturer can produce up to FIVE Products
– Samples of which must be retained for future testing
– Must have at least one cannabis Product that is high in CBD and low in THC (think “Charlotte’s Web”)
– Must have at least one cannabis Product that has an approximately 1:1 ratio of THC and CBD.
• A Manufacturer may have up to FOUR contracted Dispensaries, setting a maximum of 20 in the State
31

Requirements for Manufacturers
• Manufacturer must be able to ensure the availability of a ONE YEAR supply of all Products
• All records must be readily available for inspection
• Manufacturers can ONLY hire union workers ≥21!
• Manufacturer may work with banks to manage taxes and money accounts*– In Colorado, suitcases or strong-
box safes stuffed with cash are delivered to government offices

Some Difficulties With Banking
• Financial institutions disallow payment for illegal drugs
– Federal Law states the businesses cannot deposit their cannabis revenues at their banks (money laundering?)
• 2009 – Deputy AG David Ogden stated companies in states with legal cannabis won’t be prosecuted
– 2011 – Deputy AG James M. Cole stated this memo wasn’t intended to shield cannabis companies from the Feds
• 2014 – AG Eric Holder stated banks could work with cannabis industries and won’t be prosecuted
– Financial Crimes Enforcement Network: banks may choose
– Must still file Federal “suspicious activity reports”33

Approved Medicinal Cannabis Products
• Each brand must have a total THC and CBD concentration within 5% of labeled value (mg/dose)
• Brand names must be alphanumeric combinations!
• Maximum of 10mg THC per dose!
• Approved dosage forms:
– Extract in oil for SL administration
– Extract for vaporization (metered and uniform doses)
– Extract in a capsule for ingestion
– Edible food product only by Commissioner approval
34

Approved Products*

Approved Medicinal Cannabis Products
• Product label must include ALL these alkaloids:– Tetrahydrocannabinol (THC)
– Tetrahydrocannabinol acid (THCA)
– Tetrahydrocannabivarin (THCV)
– Cannabidiol (CBD)
– Cannabinadiolic acid (CBDA)
– Cannabidivarine (CBDV)
– Cannabinol (CBN)
– Cannabigerol (CBG)
– Cannabichromene (CBC)
– Any other cannabinoid component at >0.1% 36

Auxiliary Labels
• “Medical marihuana products must be kept in the original container in which they were dispensed and removed from the original container only when ready for use by the certified patient”;
• “Keep secured at all times”;
• “May not be resold or transferred to another person”;
• “This product might impair the ability to drive”;
• “KEEP THIS PRODUCT AWAY FROM CHILDREN (unless medical marihuana product is being given to the child under a practitioner’s care”); and
• “This product is for medicinal use only. Women should not consume during pregnancy or while breastfeeding except on the advice of the certifying practitioner, and in the case of breastfeeding mothers, including the infant’s pediatrician.”
37

Unapproved Medicinal Cannabis Products
• NO RAW PLANT MATERIAL FOR SMOKING!
– NYS is trying to cut down on statewide smoking rates!
• NO RAW PLANT MATERIAL FOR INGESTION!
– Edibles must be premade and prepackaged
• NO FLASHY BRAND NAMES OR ADVERTISEMENTS!
• NO REFERENCES TO 420 CULTURE!
• NO MOLD OR CONTAMINANTS!
• NO ADDITIVES UNLESS PHARMACEUTICAL GRADE!
• NO STATING YOUR PRODUCT IS MOST EFFECTIVE!38

Unapproved Cannabis Products
39
Dispensing Facilities (Dispensaries)
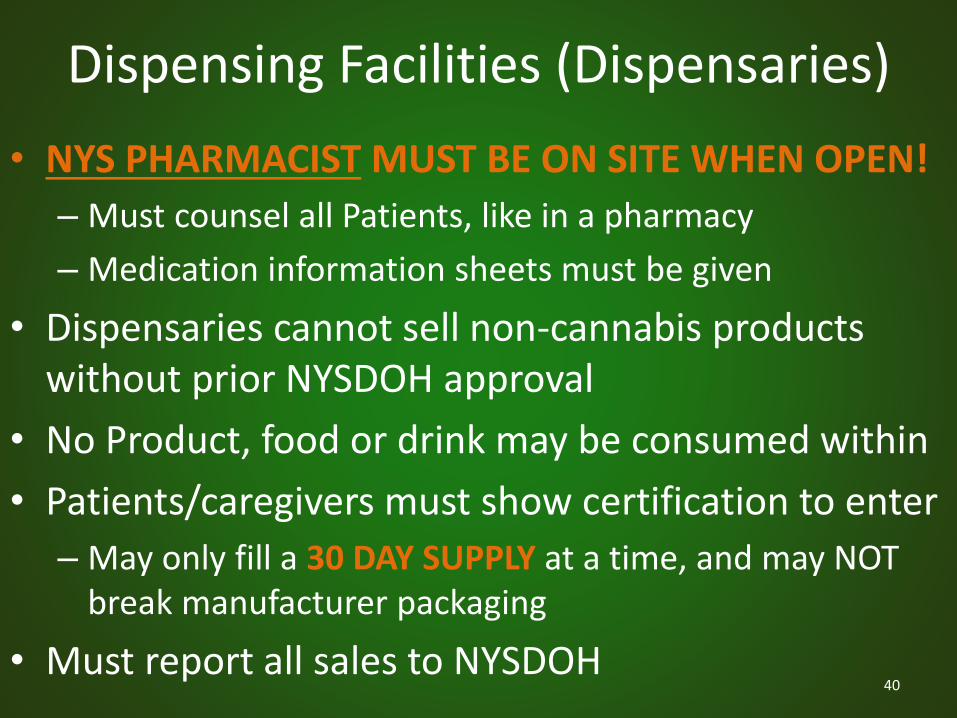
• NYS PHARMACIST MUST BE ON SITE WHEN OPEN!
– Must counsel all Patients, like in a pharmacy
– Medication information sheets must be given
• Dispensaries cannot sell non-cannabis products without prior NYSDOH approval
• No Product, food or drink may be consumed within
• Patients/caregivers must show certification to enter
– May only fill a 30 DAY SUPPLY at a time, and may NOT break manufacturer packaging
• Must report all sales to NYSDOH40

Dispensary Exterior (New Jersey)

Dispensary Interior (California)

Dispensing Facilities (Dispensaries)
• Sufficient security measures must safeguard Facilities and Products and must include the following items:– Perimeter alarm– Motion detectors– Lighting around the perimeter of the facility– Video cameras at all entries/exits and at product storage– 24 hour recording capability (≥90 days of storage space)– A duress alarm (for forced shut down of security)– A panic alarm (to alert police of emergency situation)– A hold-up alarm (to signal police to the robbery)– Automatic voice dialer, that will send prerecorded message– Failure notification for security (notification within 5 minutes)– Backup generator for power outages– Capability to take clear, color photos with 9600dpi resolution– Back-up alarm system for non-operational hours
43

Other States Involve Pharmacists
• Connecticut (2012)– Only pharmacists can have dispensary licenses
– Pharmacists must check and send records to the PMP
– Dispensary workers must be registered pharmacy techs
• Minnesota (2014)– Only pharmacists can dispense cannabis to Patients or
Caregivers and counsel on its proper use
• Rhode Island (2006)– Legal literature safeguarding RPh licensure (counseling)
• Illinois, Maryland, Minnesota, New Hampshire– Must have a pharmacist sitting on advisory boards
44

Miscellaneous Points
• Under NO circumstances can cannabis products manufactured in New York be taken out of NYS!
• These proposed regulations would sunset SEVENyears after the approval date if not reapproved
• Cannabis tax of 7% (paid by Facilities)
• Manufacturers can NOT give free samples
• NY Manufacturers can’t dispense from same facility
• No Product may be delivered without DOH approval
• Only female plants can be used for extraction45

Some Dollars and Cents
• Medicinal cannabis programs have mixed success
• Successes:– Arizona received $7.9 million in taxes and fees from April
2011 – June 2012 (cost the state just $2.4M to run)
– Michigan took in $9.9M in 2012, spending just $3.6M
– Oregon siphoned $900K in 2005, Nevada proposed siphoning $700,000/year for substance abuse education
• Disappointments and failures-to-launch:– Rhode Island took in $566,655 in fees but spent
$589,086 in the 2011-2012 fiscal year
– New Jersey approved laws in 2010; in 2013, Greenleaf Compassion Center was the only operating dispensary

Summary of Legal Challenges
• Information vs. misinformation
– Fear-mongering (“gateway drug”)
– Supporters sensationalizing benefits
– Internet shock sites and blogs
– Inherent and persistent biases
– YouTube® and Reddit® “activists”
• Topic is very politically charged
– Federal vs. State
– Democrats vs. Republicans
– Boomers vs. Gen X/Millennials47

Summary of Legal Challenges
• Large-scale trials require approval from the FDA
– Cannabis catch-22: restricted in large part because there isn’t enough research to support medical uses, but research is difficult to conduct due to tight restrictions!
• Obtaining product for studies is very prohibitive
– National Institute on Drug Abuse (NIDA) is the ONLY legal body authorized to cultivate large amounts
– Extension site located at the University of Mississippi
– This single site cannot supply enough product for a large-scale clinical trial (ex. Phase III)
48

Summary of Legal Challenges
• California
– Gonsales vs. Raich landmark trial
– SCOTUS ruled that even with favorable State law, the Federal Government can criminalize medicinal cannabisproduction under the Federal Commerce Clause
• Massachusetts
– As recently as 9/2014, DEA agents have visited MDs to give an ultimatum: sever ties with medicinal cannabis or have their DEA licenses permanently revoked
• US Attorney General Eric Holder said the Feds will be laissez-faire (he’s announced his resignation)
49

Conclusions
• There is a universally acknowledged lack of large scale, long term medicinal cannabis clinical trials!
• Politics continue to prevent cannabis research
– Reclassification to Schedule II is paramount for more research to be approved and completed
• New York’s medicinal cannabis regulations, when approved, will be the strictest in the nation
• Medicinal cannabis paves the way for a renewed investigation into the medical accuracy and current application of the Controlled Substances Act (1970)
50

Resources
• New York State Department of Health– www.health.ny.gov/regulations/medical_marijuana/
• The Marijuana Policy Project– www.mpp.org
• The Multidisciplinary Association for Psychedelic Studies– www.maps.org
• ProCon– www.medicalmarijuana.procon.org
• Dave Porter, Pharm.D candidate– [email protected]
51
1. Abrams DI, Jay CA, Shade SB, Vizoso H, Reda H, Press S, Kelly ME, Rowbotham MC, Petersen KL. Cannabis in painful HIV-associated sensory neuropathy: A randomized placebo-controlled trial. Neurology (2007)68:515-521.
2. Ahmet Ulugöl. The Endocannabinoid System as a Potential Therapeutic Target for Pain Modulation. Balkan Med J (2014);31:115-20.
3. Alan Zarembo. Exploring therapeutic effects of MDMA on post-traumatic stress. LA Times: Mar 15, 2014. Available from: < http://articles.latimes.com/2014/mar/15/local/la-me-mdma-20140316>.
4. Basch E, Prestrud AA, Hesketh PJ, et al. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol2011;29(31):4189-98.
5. Baumeister D, Barnes G, Giaroli G, Tracy D. Classical hallucinogens as antidepressants? A review of pharmacodynamics and putative clinical roles. Ther Adv Psychopharmacol (2014);4(4):156-69.
6. Carhart-Harris RL, Leech R, Williams TM, Erritzoe D, Abbasi N, Bargiotas T, et al. Implications for psychedelic-assisted psychotherapy: functional magnetic resoinance imaging study with psilocybin. British Journal of Psychiatry (2012);200:238-44.
7. Clark PA, Capuzzi K, Fick C. Medical marijuana: Medical necessity versus political agenda. Med Sci Monit (2011);17(12):249-261.
8. Compassionate Care New York. Frequently Asked Questions about New York’s Medical Marijuana Bill. (2014). Compassionate Care New York. Available from <www.compassionatecareny.org>.
9. Corey-Bloom J, Wolfson T, Gamst A, Jin S, Marcotte T, Bentley H, Gouaux B. Smoked cannabis for spasticity in multiple sclerosis: a randomized, placebo-controlled trial. CMAJ (2012);184(10):1143-50.
10. Dronabinol, THC. In: Clinical Pharmacology [database on the Internet]. Tampa (FL): Gold Standard; 2008 [updated 6Jan 2014; cited 26 Jan 2015]. Available from: www.clinicalpharmacology.com. Subscription required to view.
11. Dronabinol. In: Lexi-drugs online [database on the Internet]. Hudson (OH): Lexicomp, Inc.; 2013 [updated 15 Jan 2015; cited 27 Jan 2015]. Available from: http://online.lexi.com. Subscription required to view.
12. Ellis RJ, Toperoff W, Vaida F, van den Brande G, Gonzales J, Gouaux B, Bentley H, Atkinson JH. Smoked Medicinal Cannabis for Neuropathic Pain in HIV: A Randomized, Crossover Clinical Trial. Neuropsychopharmacology (2009);34(3):672-80.
13. Ethan B Russo. Cannabinoids in the management of difficult to treat pain. Ther Clin Risk Manag (2008);4(1):245–59.
14. Food and Drug Administration. Controlled Substances Act. Updated Jun 2009. Available from: <http://www.fda.gov/regulatoryinformation/legislation/ucm148726.htm#cntlsbb>.
15. Garcia-Romeu A, Griffiths RR, Johnson MW. Psilocybin-Occasioned Mystical Experiences in the Treatment of Tobacco Addiction. Current Drug Abuse Reviews (2014);7(2):e-pub ahead of print.
16. Gasser P, Holstein D, Michel Y, Roblin R, Yazar-Klosinski B, Passie T, et al. Safety and Efficacy of Lysergic Acid Diethylamide-Assisted Psychotherapy for Anxiety Associated with Life-threatening Diseases. J Nerv Ment Dis (2014):4(202):513-20. 52
References

17. Gasser P, Holstein D, Michel Y, Roblin R, Yazar-Klosinski B, Passie T, et al. Safety and Efficacy of Lysergic Acid Diethylamide-Assisted Psychotherapy for Anxiety Associated with Life-threatening Diseases. J Nerv Ment Dis (2014):4(202):513-20.
18. Gerald J McKenna. The Current Status of Medical Marijuana in the United States. Hawai’I J of Med & Pub Health (2014);73(4):105-8.
19. Grob CS, Danforth AL, Chopra GS, Hagerty M, McKay CR, Halberstadt et al. Pilot Study of Psilocybin Treatment for Anxiety in Patients With Advanced-Stage Cancer. Arch Gen Psychiatry (2011);68(1):71-78.
20. Grotenhermen F, Müller-Vahl K. The Therapeutic Potential of Cannabis and Cannabinoids. Deutsches Ärzteblatt International (2012);109(29–30):495–501.
21. Gonzalez R, Martin EM, Grant I, Neuropsychology and Substance Use, Taylor & Francis Group. (2007) Marijuana (Chapter 5, 139-170).
22. Grant I, Atkinson JH, Gouaux B, Wilsey B. Medical Marijuana: Clearing Away the Smoke. The Open Neurology Journal (2012);6:18-25.
23. Grant I, Atkinson JH, Mattison A, Coates TJ. Report to the Legislature and Governor of the State of California presenting findings pursuant to SB847 which created the CMCR and provided state funding. Center for Medicinal Cannabis Research. 2010 Feb 11. Available from:<www.cmcr.ucsd.edu>.
24. Griffiths RR, Johnson MW, Richards WA, Richards BD, McCann U, Jesse R. Psilocybin occasioned mystical-type experiences: Immediate and persisting dose-related effects. Psychopharmacology (Berl) (2011);218(4):649-65.
25. Jennifer Donnelly. The Need for Ibogaine in Drug and Alcohol Addiction Treatment. Journal of Legal Medicine (2011);32:93-114.
26. Johnson MW, Garcia-Romeu A, Cosimano MP, Griffiths RR. Pilot study of the 5-HT2aR agonist psilocybin in the treatment of tobacco addiction. Journal of Psychopharmacology (2014);28(11):983-92.
27. Johnson MW, Richards WA, Griffiths RR. Human hallucinogen research: guidelines for safety. Journal of Psychopharmacology (2008);22(6):608-20.
28. Joseph Gregorio. Physicians, Medical Marijuana, and the Law. AMA J of Ethics (2014):16(9):732-738.
29. Kahan M, Srivastava A, Spithoff S, Bromley L. Prescribing smoked cannabis for chronic noncancer pain: Preliminary recommendations. Canadian Family Physician (2014);60:1083-90.
30. Kraehenmann R, Preller KH, Scheidegger M, Pokorny T, Bosch OG, Seifritz E, et al. Psilocybin-induced Decrease in Amygdala Reactivity Correlates with Enhanced Positive Mood in Healthy Volunteers. Biol Psychiatry (2014);e-pub.
31. Krebs TS and Johansen PO. Lysergic acid diethylamide (LSD) for alcoholism: meta-analysis of randomized controlled trials. Journal of Psychopharmacology (2012):26(3):996-1002.
32. Krebs TS and Johansen PO. Psychedelics and Mental Health: a Population Study. PLoS ONE (2013);8(8):e63972.
33. Lynch ME, Campbell F. Cannabinoids for treatment of chronic non-cancer pain; a systematic review of randomized trials. Br J Clin Pharmacol(2011);72(5):735-44. 53
References

References34. Mačiulaitis R, Kontrimavičiūtė V, Bressolle FMM, Briedis V. Ibogaine, an anti-addictive drug: pharmacology and time to go further in
development. A narrative review. Human and Experimental Toxicology (2008);27:181-194.
35. Michael Winkelman. Psychedelics as Medicines for Substance Abuse Rehabilitation: Evaluating Treatments with LSD, Peyote, Ibogaine and Ayahuasca. Current Drug Abuse Reviews (2014);7:101-16.
36. Mithoefer MC, Wagner MT, Mithoefer AT, Jerome L, Doblin R. The safety and efficacy of 3,4-methylenedioxymethamphetamine-assisted psychotherapy in subjects with chronic, treatment-resistant posttraumatic stress disorder: the first randomized controlled pilot study. Journal of Psychopharmacology (2011);25(4):439-452.
37. Mithoefer MC, Wagner MT, Mithoefer AT, Jerome L, Martin SF, Yazar-Klosinski, et al. Durability of improvement in post-traumatic stress disorder symptoms and absence of harmful effects or drug dependency after 3,4-methylenedioxy-methamphetamine-assisted psychotherapy:a prospective long-term follow-up study. Journal of Psychopharmacology (2013);27(1):28-39.
38. Muni Rubens. Political and Medical Views of Medical Marijuana and its Future. Social Work in Public Health (2014);29:121-31.
39. Nabilone. In: Clinical Pharmacology [database on the Internet]. Tampa (FL): Gold Standard; 2008 [updated 21 Jul 2014; cited 26 Jan 2015]. Available from: www.clinicalpharmacology.com. Subscription required to view.
40. Nabilone. In: Lexi-drugs online [database on the Internet]. Hudson (OH): Lexicomp, Inc.; 2013 [updated 20 Nov 2014; cited 27 Jan 2015]. Available from: http://online.lexi.com. Subscription required to view.
41. New York State Assembly Bill 6357. 2013 Mar 26. Available from <http://assembly.state.ny.us/leg/?sh=printbill&bn=A06357&term=2013>.
42. New York State Department of Health. New York State Medical Marijuana Program. Dec 2014. Available from: <http://www.health.ny.gov/regulations/medical_marijuana/>.
43. ProCon. Medical Marijuana Pros and Cons. Last updated 11/13/2014. Available from: <http://medicalmarijuana.procon.org/>.
44. Schenberg EE,de Castro Comis MA, Rassmussen Chaves B, da Silveira DX. Treating drug dependence with the aid of ibogaine: A retrospective study. Journal of Psychopharmacology (2014);28(11):993-1000.
45. Tylš F, Páleníček T, Horáčeka J. Psilocybin – Summary of knowledge and new perspectives. European Neuropsychopharmacology (2014);24:342-56.
46. Wallace M, Schulteis G, Atkinson JH, Wolfson T, Lazzaretto D, Bentley H, et al. Dose-dependent Effects of Smoked Cannabis on Capsaicin-induced Pain and Hyperalgesia in Healthy Volunteers. Anesthesiology (2007);107(5):785-96.
47. Wilsey B, Marcotte T, Deutsch R, Gouaux B, Sakai S, Donaghe H. (2013). Low-Dose Vaporized Cannabis Significantly Improves Neuropathic Pain. J Pain, 14(2):136-48.
48. Wilsey B, Marcotte T, Tsodikov A, Millman J, Bentley H, Gouaux B, Fishman S. (2008) A Randomized, Placebo-Controlled, Crossover Trial of Cannabis Cigarettes in Neuropathic Pain. J Pain, 9(6):506-21.
54
55
Any Questions?
Thanks for Listening!