Embed Size (px)
Citation preview

Vision Research 50 (2010) 1612–1617
Contents lists available at ScienceDirect
Vision Research
journal homepage: www.elsevier .com/locate /v isres
The global shape detection deficit in strabismic amblyopia: Contributionof local orientation and position
Richard Dallala, Yi-Zhong Wang, Robert F. Hess *
McGill Vision Research, Dept. of Ophthalmology, McGill University, Montreal, Quebec, CanadaThe Retina Foundation of the SouthWest, Dallas, TX, USA
a r t i c l e i n f o
Article history:Received 15 June 2009Received in revised form 30 April 2010
Keywords:Radial frequencyCircular contour frequencyAmblyopiaStrabismusOrientationPosition
0042-6989/$ - see front matter � 2010 Elsevier Ltd. Adoi:10.1016/j.visres.2010.05.023
* Corresponding author at: McGill Vision Research,University, Montreal, Quebec, Canada.
E-mail address: [email protected] (R.F. Hess).
a b s t r a c t
We extended a previous study (Hess et al. (1999). A deficit in strabismic amblyopia for global shape detec-tion. Vision Research, 39, 901–914) where it was claimed that strabismic amblyopes exhibit a deficit for thedetection of continuous radial frequency patterns, a task that is thought to involve global processing and inparticular, a contribution of extra-striate area V4. We confirm this previous report using a novel Gabor-sampled stimulus and show that the deficit for the amblyopic eye occurs across a range of circular contourfrequencies, that is the number of radial cycles per circular contour length in degrees. By arranging theGabor-samples to coincide with either the peaks/troughs or zero-crossings of the radial modulation, wewere able to tease apart the relative contributions of local position and local orientation respectively tothe shape processing deficit. The deficit for the amblyopic eye involves both anomalous position and ori-entation coding with the latter being more affected than the former. While this suggests that ventral extra-striate processing is anomalous, it leaves open the possibility that the striate input may be responsible.
� 2010 Elsevier Ltd. All rights reserved.
1. Introduction
Previous studies have characterized specific deficits in vision foramblyopic patients, such as contrast sensitivity (Hess, 1976; Levi &Harwerth, 1977), positional uncertainty (Hess & Holliday, 1992;Levi & Klein, 1983; Sireteanu, Lagreze, & Constantinescu, 1993)and global processing of motion (Simmers, Ledgeway, Hess, &McGraw, 2003) and form (Simmers, Ledgeway, & Hess, 2005).Although more attention has been paid to the global deficits affect-ing the dorsal processing of visual motion (Aaen-Stockdale & Hess,2008; Simmers, Ledgeway, Mansouri, Hutchinson, & Hess, 2006;Simmers et al., 2005), two studies have highlighted a global pro-cessing deficit involving the ventral processing of form (Hess,Wang, Demanins, Wilkinson, & Wilson, 1999b, Simmers et al.,2005). One of these (Hess, Wang, Demanins et al., 1999b) involvesglobal shape detection for which there is fMRI evidence (Wilkinsonet al., 2000) implicating area V4 in normals. In this study we set outto better understand this deficit by establishing its dependence onstimulus circular contour frequency (Jeffrey, Wang, & Birch, 2002)and by assessing whether it is the result of deficient orientation ordeficient position processing.
Jeffrey et al. (2002) have argued that a critical parameter in nor-mal shape detection of radial frequencies patterns is the circularcontour frequency of the stimulus. This is defined as the number
ll rights reserved.
Dept. Ophthalmology, McGill
of radial cycles per contour length in degrees. Circular contour fre-quency depends not only the influence of the radial frequency,about which we know a lot (Wilkinson, Wilson, & Habak, 1998)but also on the influence of the radius, about which we know less.More recently, Jeffrey, Wang, and Birch (2004) showed that thisparameter, critical contour frequency, is also a key for understand-ing the shape detection deficit in humans with deprivation ambly-opia. In deprivation amblyopia, the global shape deficit depends onthe circular contour frequency of the stimulus; the higher the cir-cular contour frequency, the greater the shape processing deficit.There is reason to believe that the neural deficit is different in stra-bismic as opposed to deprivation amblyopia and that this differ-ence may be relevant to shape processing. Only strabismicamblyopes exhibit spatial accuracy deficits (Hess & Holliday,1992; Levi & Klein, 1983; Sireteanu et al., 1993) and report percep-tual spatial distortions. This raises the first of two questions thatwe address here concerning the global shape deficit in strabismicamblyopia, namely, does the deficit in strabismic amblyopes for thedetection of radial frequency patterns depend on the circular contourfrequency, as it does for deprivation amblyopes? Deprivation amblyo-pes (Constantinescu, Schmidt, Watson, & Hess, 2005; Ellemberg,Lewis, Maurer, Brar, & Brent, 2002), like strabismic amblyopes(Aaen-Stockdale & Hess, 2008; Simmers et al., 2003, 2006) exhibitdeficits for global motion detection, implicating deficient dorsalextra-striate function. We wanted to know if similar deficits occurin these two forms of amblyopia for the ventral extra-striate anal-ysis of global shape.

R. Dallala et al. / Vision Research 50 (2010) 1612–1617 1613
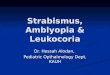
A second issue involves the nature of any deficit underlyingdeficient global shape processing. In a study of normal vision,Wang and Hess (2005) showed that the detection of radial fre-quency stimuli is supported by two different sources of informa-tion, one involving the global integration of local positionestimates and the other, local orientation estimates. They used Ga-bor-sampled, radially-modulated stimuli in order to assess the rel-ative contribution of each of these factors by manipulating thephase of the Gabor-samples relative to the radial modulation(see Fig. 1c–f). When the samples were positioned at the zero-crossing of the radial frequency modulation (see Fig. 1d), they car-ried the relevant orientation information with no positional com-ponent. When the samples were positioned at the peaks/troughsof the radial frequency modulation (Fig. 1e), they carried the rele-vant position information with no orientation component. Theyfound that in normal vision both sources of information are used,although orientation information is more heavily relied upon. Thisprompted the question, is the deficit for the detection of radial fre-quency patterns in adults with strabismic amblyopia the result of defi-cient processing of orientation or position or both?
To answer the first question, we used stimuli that were Gabor-sampled radial frequency patterns sampled at both peaks andzero-crossings of the radial modulation (Fig. 1c) to compare perfor-mance in normals and strabismic amblyopes for the detection ofradial contour patterns of different circular contour frequency. Toanswer the second question, we compared performance for
Table 1Clinical details of strabismic amblyopes.
Obs Age Type Refraction VA
KS 40 RE strab +5.00–1.00 � 180� 20/100LE + 0.50DS 20/20
GH 45 RE �1.75 + 0.5 � 90� 20/20LE strab + 1.25DS 20/63
AM 30 RE strab +0.50DS 20/32LE plano 20/20
MS 35 RE plano 20/20LE strab plano 20/125
KG 33 RE strab �1.00DS 20/80LE �0.50DS 20/15
JG 31 RE �2.00–0.50 � 150 20/20LE strab –1.50DS 20/100
ADS 21 RE Plano 20/120LE strab �0.50DS 20/20
S 25 RE strab +3.00DS 20/50LE + 3.00DS 20/25
AR 40 RE Plano 20/20LE strab Plano 20/50
Abbreviations: strab = strabismus; RE = right eye; LE = left eye; ET = esotropia; XT = exot
Fig. 1. The top row shows an unmodulated circular stimulus and the bottom row a radfrequency (RF) of 4 c/360�; (b) continuous RF patterns; (c–f) micropatch-sampled RF (Mchanges (combined MSRF patterns); (d) orientation-defined deformation (orientation pattusing Gaussian blobs instead of Gabor patches to sample RF patterns.
Gabor-sampled radial frequency patterns where the radial modula-tion was sampled at either the zero-crossings (to assess orientationprocessing) or the peaks/troughs (to assess position processing).
2. Methods
2.1. Subjects
The details of the strabismic amblyopes are shown in Table 1.Nine strabismic amblyopes and five normal controls participatedin this study (including one of the authors). All normal observershad a visual acuity of 20/20 or greater (with correction if neces-sary). All subjects consented after the purpose of the study andthe procedures were explained to them. The research projectmethods were in accordance with the standards of the local ethicscommittee as well as the Declaration of Helsinki.
2.2. Stimuli
Micropatch-sampled radial frequency patterns (Fig. 1) wereused as visual stimuli to study the contribution of local orientationand position features to shape integration. A continuous radial fre-quency (RF) pattern (Fig. 1b) was generated by modulating the ra-dius of a circle sinusoidally according to the following formula
R ¼ R0½1þ A sinðfaþ hÞ� ð1Þ
Squint History, stereo
XT 4� Detected age 10 yr, patching for 1 m, glassesfor 1 yr, no stereopsis
ET 6� Detected at 11 yr, no surgery & patching, eyeexercise 1–2 yr, glasses since 12 yr, no stereopsis
XT 1� Detected age 8 yr, no patching or surgery, stereopsis 70 s
ET 1� Detected age 8 yr, Rx at 9 yrs. No patching, nosurgery, no local stereopsis
ET 4� Detected age 5 yr, patching for 2 yr, No surgery,no stereopsis
ET 3� Detected at age 6 m, surgery at 6 m and 2 yr,patching for 1 yr no stereopsis
ET 15� Detected age 4 yr, patching for 4 m, surgery age 7 yr
XT 10� Detected age 12 yr, no treatment,no stereopsis
XT 1� Detected at 6 yrs, no patching therapy,no surgery no stereopsis
ropia; DS = dioptre sphere.
ially-modulated circular stimulus; (a) sinusoidal modulation of a circle with radialSRF) patterns; (c) shape deformation defined by both local orientation and positionerns); (e) position-defined deformation (position MSRF patterns); (f) same as (e) but

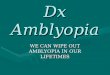
Fig. 2. Radial deformation thresholds in either seconds of arc (A) or percentage ofthe radius (B) are plotted against the circular contour frequency of the Gabor-sampled radial frequency pattern. Results are compared for the dominant eye ofnormal observers (unfilled circles and dashed line) and the fixing (filled circles andgrey lines) and fellow amblyopic (filled circles and black lines) eyes of strabismicamblyopes. The stimulus was Gabor-sampled at both peaks/troughs and zero-crossings of the radial modulation (Combined stimulus). The error bars represent±SE.
1614 R. Dallala et al. / Vision Research 50 (2010) 1612–1617
where R0 is the mean radius; A is the percent modulation ampli-tude; f is the radial modulation frequency; h is the phase of modu-lation; a is the polar coordinate angle (�p to p); and R is themodulated radius. The cross-section luminance profile of the con-tinuous circular contour is the fourth derivative of a Gaussian(Swanson, Wilson, & Giese, 1984; Wilkinson et al., 1998). Continu-ous RF patterns have the dual advantage of being spatial frequencynarrowband (fourth derivative of a Gaussian) and having well con-trolled shape perturbations of different magnitudes or scale.
Micropatch-sampled radial frequency (MSRF) patterns weregenerated according to the methods of Wang and Hess (Wang &Hess, 2005) by placing Gabor patches or Gaussian blobs alongthe trace of sinusoidal modulation of a circle (Fig. 1a), as definedby Eq. (1). The size of Gabor (or Gaussian blob) was defined bythe standard deviation of Gaussian envelope, and the actual patchsize was four times of the standard deviation. When Gabor patcheswere used as sampling elements, the carrier orientation was de-fined as tangential to the deformed circle at the placement posi-tion, and was the same as the local contour orientation of thecorresponding continuous RF pattern at the same location. Whenthe sampling elements in an MSRF pattern are integrated by the vi-sual system, the radially-modulated stimulus will be detectable(Fig. 1c–f), and the global shape perception of these sampled pat-terns is comparable to that of continuous RF patterns (Fig. 1b).
2.2.1. Separating local orientation changes from local positionalperturbations
Sinusoidal modulation of the radius introduces both local orien-tation changes and local positional perturbation from circularity(Fig. 1a). For a given modulation amplitude, zero-crossings of mod-ulation correspond to maximum local orientation changes fromcircularity but no positional perturbation, while peaks and troughsof modulation correspond to maximum positional perturbationsfrom circularity but no orientation change. If micropatches areplaced at zero-crossings, an orientation MSRF pattern (or orienta-tion pattern) with no positional change is obtained (Fig. 1d). Incontrast, if micropatches are placed at peaks and troughs, a posi-tion MSRF pattern (or position pattern) with no orientation changeis obtained (Fig. 1e). The local orientation information can be elim-inated from a position pattern when using circular Gaussian blobsas sampling elements (Fig. 1f). A combined pattern is obtainedwhen micropatches are placed at peaks and troughs, as well as atzero-crossings (Fig. 1c). In this way, one can create shape deforma-tion defined only by local orientation changes (orientation pattern)and that defined only by local position changes (position pattern).Furthermore, these two types of shape deformation can be gaugedby the same physical measurement, i.e. the amount of radial mod-ulation. With this arrangement of micropatches, there are twosampling elements per modulation cycle in either an orientationor a position pattern, which is the Nyquist sampling rate accordingto the sampling theorem (Shannon, 1949).
Stimuli were generated digitally in MATLAB (The MathWorks,Inc.) and displayed on a gamma-corrected, 8-bit grey-scale moni-tor that was controlled by a PowerMac computer using the Psycho-physics Toolbox (Brainard, 1997), which provides high-level accessto the C-language VideoToolbox (Pelli, 1997). The mean luminanceof the monitor was 55 cd/m2 and the stimulus contrast was 100%.The stimulus screen subtended 6.4-by-4.8� at the viewing distanceof 3.2 m. The radius was varied from 1� to 0.375�. The radial fre-quency was fixed at 4 c/360� and the luminance spatial frequencyvaried between 3 and 6 c/d. The Gabor patch size was 0.07� SD.
2.3. Psychophysical procedures
A temporal 2AFC paradigm was employed. Subjects were askedto look at a fixation target positioned at the center of the screen
where the stimulus patterns were presented during the experi-ment. In each trial, one interval contained a deformed MSRF pat-tern and the other interval contained an undeformed MSRFpattern. Subjects were asked to indicate which interval containedthe deformed one. The duration of each stimulus interval was0.5 s. Audio signals were used to prompt the subject before eachinterval and at the end of each trial, but no feedback about the cor-rectness of responses was provided.
The experiments were controlled by 2-down, 1-up staircaseprocedures (Swanson & Birch, 1992), and ended after eight rever-sals. A maximum likelihood fitting procedure was used to fit a Wei-bull function (Nachmias, 1981; Weibull, 1951) to the data obtainedfrom each experimental run. The estimated modulation thresholdcorresponded to 75% correct responses. The dominant eye of nor-mal observers was determined using a sighting test.
3. Results
Fig. 2 shows a comparison of sensitivity for detecting radial fre-quency patterns (radial frequency = 4) for the fixing and amblyopiceye of strabismic amblyopes and the dominant eye of normals. Thestimulus is the combined Gabor-sampled radial frequency pattern(Fig. 1C). In Fig. 2A, the threshold modulation of the fixing (grey sym-bols and line) and amblyopic eye (black symbols and line) of amblyo-pes and the dominant eye (white symbols and dashed line) ofnormals is plotted in terms of absolute threshold in arc secondsagainst the circular contour frequency of the stimulus in cycles/con-tour length in degrees. In Fig. 2B, threshold is expressed as a percent-age of the radius. The results in A, show that amblyopic eyes haveelevated thresholds in absolute terms compared with either the fel-low fixing eyes or dominant eyes of normal observers. We subjectedthe data to a 3 � 4 ANOVA with repeated measurements for circularcontour frequency and non-repeated measurements for eyes. The

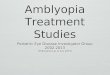
Fig. 4. Average detection thresholds for a group of normal and amblyopic observersplotted as a percentage of the radius for three conditions; the combined stimuluswhere the Gabor-samples are at both peaks/troughs and zero-crossings, theorientation stimulus where the Gabor-samples are confined to the zero-crossingsand the position stimulus where the Gabor-samples are confined to the peaks/troughs of the radial modulation. The stimulus has a radial frequency of 4 c/360�and a circular contour frequency of 1.2 c/cl in degrees. The error bars represent ±SE.
R. Dallala et al. / Vision Research 50 (2010) 1612–1617 1615
main effect of eye was significant (F(2, 70) = 10.0, MSe = 13,031,P < .001). The Tukey’s post hoc test showed that the difference wassignificant between amblyopic eye and normal eye (p = .021), butnot between amblyopic eye and fellow fixing eye (p > .05). Thisthreshold elevation is similar for the different circular contour fre-quencies investigated (no significant interaction, p > .05). Therewas a significant main effect of circular contour frequency(F(3, 36) = 12.5, MSe = 10,567, P < .001), suggesting that radial defor-mation threshold depends on this variable. The results in B providefurther insight. For normal vision, thresholds are constant when ex-pressed in terms of a percentage of the radius. In amblyopes, this isalso true for the fellow fixing eye, albeit at a slightly larger percent-age. However, the amblyopic eyes exhibit thresholds that representsan increasing fraction of the radius as the circular contour frequencydecreases below about 1.2 c/cl-deg.
Fig. 3 shows results for the positional (Fig. 1E) and orientational(Fig. 1D) sampled radial frequency patterns (radial frequency = 4,circular contour frequency = 1.27 c/cl-degs, contrast = 80%, lumi-nance spatial frequency = 6 c/deg) compared with that of the com-bined stimulus (Fig. 1C). To obtain a more meaningful comparisonof the threshold differences for normal, fixing and amblyopic eyes,we compare thresholds separately for stimuli containing orienta-tion and position cues. Results are shown for five normal observersin Fig. 3. The threshold for the two subsampled patterns is greaterthan that of the combined stimulus, suggesting that both orienta-tion and position information are playing roles in performance forthe combined stimulus. An earlier report by Wang and Hess (2005)showed that there was a greater reliance on the orientation infor-mation contained in the stimulus than for the positional informa-tion (i.e. lower orientation thresholds). The pattern of results forour normal observers is very similar from subject to subject andsupportive of this previous claim (Wang & Hess, 2005) in that ori-entation information dominates (i.e. lower thresholds) over that ofposition information. The individual results for all subjects exceptNC show a significantly lower threshold for the orientation stimu-lus (t-test, one tailed; p < 0.05). For one subject (Fig. 3E) we com-pare results for right and left eye stimulation and find nosignificant difference (t-test, one tailed; NS).
Fig. 3. Detection thresholds for individual normal observers (A–D) plotted as a percensamples are at both peaks/troughs and zero-crossings, the orientation stimulus where ththe Gabor-samples are confined to the peaks/troughs of the radial modulation. The stfrequency of 1.27 c/cl in degrees. Normal observers are more sensitive to the orientationsensitivity of each eye for one subject. The error bars represent ±SE.
In Fig. 4 we show the group averages for normals and amblyo-pes derived from the individual results. We subjected the data to a3 � 3 ANOVA with mixed design of repeated and non-repeatedmeasurements. Thresholds were higher for amblyopic eye thanfor fellow fixing and normal eyes (F(2, 20) = 19.3, MSe = 0.857,p < .001). The combined stimulus produced better performancethan either of the component stimuli (F(2, 40) = 39.3, MSe = .542,p < .001). This is consistent with previous findings (Wang & Hess,2005) on normals, showing that that both orientation and positionare utilized. The Tukey’s post hoc test showed no significant differ-ence between the fellow fixing and the normal eyes across condi-tions (p > .05). The interaction between eyes and stimulusconditions was significant (F(4, 40) = 4.18, MSe = .542, p < .001),suggesting that threshold elevation for the amblyopic eye was lar-ger for the orientation condition than the position condition. This
tage of the radius for three conditions; the combined stimulus where the Gabor-e Gabor-samples are confined to the zero-crossings and the position stimulus whereimulus has a radial frequency of 4 c/360�, a radius of 0.5� and a circular contour
information in the stimulus. The results in E show a comparison of the threshold

1616 R. Dallala et al. / Vision Research 50 (2010) 1612–1617
trend was verified by an additional one-way ANOVA between ori-entation and position conditions for the amblyopic eye(F(1, 16) = 14.3, MSe = 1.401, p = .002).
4. Discussion
Radial frequency patterns of the type used here are thought toprobe global spatial mechanisms that combine orientation andpositional information across space (Hess, Wang, & Dakin, 1999a,Wilkinson et al., 1998). Such mechanisms are thought to be locatedin the ventral extra-striate stream, possibly involving area V4 (Wil-kinson et al., 2000). The initial report (Hess, Wang, Demanins et al.,1999b) of a deficit in detecting radial frequency patterns by theamblyopic eye is suggestive of a deficit to this processing streamin extra-striate cortex for which there is other independent evi-dence (Simmers, Ledgeway, & Hess, 2004). The results of the pres-ent study support and extend this earlier observation by showingthat the deficit (ratio of amblyopic to normal eye thresholds) isnot only invariant with radial frequency (Hess, Wang, Demaninset al., 1999b) but also it is invariant with circular contour fre-quency (Jeffrey et al., 2002), over the range we investigated. Thisdeficit cannot be ascribed to the contrast sensitivity deficit becausethe luminance spatial frequency of these stimuli were well withinthe restricted passband of the amblyopic eyes. For example, thegrating acuity of our subject with the deepest amblyopia (MS)was 24 c/deg which is a factor of four higher than the highest lumi-nance spatial frequency used in the radial frequency patterns.Although a deficit for the fellow fixing eye appears to be a featureof global tasks in general (i.e. motion coherence, and motion-de-fined form) relevant to dorsal pathway function (Aaen-Stockdale& Hess, 2008; Giaschi, Regan, Kraft, & Hong, 1992; Ho & Giaschi,2006; Ho et al., 2005), we did not find significant fixing eye deficitsfor this global ventral task. The deficit in strabismic amblyopiadoes not appear to be that different from that already reportedfor deprivation amblyopia (Jeffrey et al., 2004): the magnitude ofthe deficit in strabismic amblyopia is smaller and it appears tobe less dependent on circular contour frequency, however therange of circular contour frequencies investigated here was notas extensive as that investigated by Jeffrey et al. (2004).
By designing stimuli that allowed assessment of the two poten-tial sources of information contained in a radial frequency pattern(Wang & Hess, 2005), we were able to answer the question, ‘‘is anyglobal deficit in adults with strabismic amblyopia involving the detec-tion of radial frequency patterns, the result of deficient processing oforientation, position or both?” The amblyopic deficit for detectingradial frequency patterns is due to anomalous processing of bothposition and orientation, with a significantly greater deficit occur-ring for orientation processing. This contrasts with a recent report(Wang, Wilson, Felius, & Birch, 2006) in which a similar investiga-tion was undertaken in children with strabismic amblyopia and itwas shown that the deficit for stimuli of large radii (i.e. 1.6�) is lim-ited to position coding. The present results in adults suggests thatstimuli of small radii (i.e. 0.5�) may be necessary to reveal a greaterdeficit for orientation coding.
4.1. Possible role of curvature detectors
While there is no direct evidence that curvature detectors areinvolved in the detection of radial frequency patterns, it has beenargued that ventral processing of shape is best thought of withina curvature space (Pasupathy & Connor, 1999, 2002) and thereare models of radial frequency detection that explicitly use curva-ture detectors (Cadieu et al., 2007; Poirier & Wilson, 2006). Thuswhen we talk of orientation and position information underlyingthe detection of radial frequency patterns, it may be that this infor-
mation is used separately or, by way of curvature detectors, com-bined. Since the present results suggest that the relationshipbetween orientation and positional information found in normalsis upset in amblyopia (i.e. orientational processing is more defi-cient than positional processing) then it follows that the site ofthe deficit is unlikely to be beyond a putative curvature detectorstage. It leaves open the possibility that either these two types ofinformation are processed separately, albeit globally, within theextra-striate cortex or that the site of the deficit is at or beforethe point where these two sources of information are combined(e.g. the striate source of this information could be deficient).
4.2. Relation to previous studies
It is generally accepted that extra-striate cortical areas are in-volved in more global processing. In strabismic amblyopia, it hasbeen shown that global tasks involving motion (Aaen-Stockdale& Hess, 2008; Mansouri & Hess, 2006; Simmers et al., 2003,2006) and orientation (Mansouri & Hess, 2006; Simmers et al.,2004) reflect anomalies in dorsal and ventral extra-striate regionsrespectively. Here we have shown that performance on anothertask that is thought to require global processing (Hess, Wang & Da-kin, 1999a, Wilkinson et al., 1998) and to be associated with extra-striate area V4 (Wilkinson et al., 2000) is also defective in strabis-mic amblyopia. We have also shown that while both position andorientation information that underlie this task are anomalouslyprocessed by the amblyopic visual system, there is a greater deficitfor orientation coding. What is not clear is whether this loss ofpositional and orientational processing occurs in the striate cortexor in the extra-striate cortex. It is possible that although this task isaccomplished in area V4, the information received from V1 interms of local orientation and position is sufficiently disrupted toexplain the global processing deficit. There is ample evidence fordeficits to the coding of position (Bedell & Flom, 1981; Hess & Hol-liday, 1992; Levi & Klein, 1983; Sireteanu et al., 1993) that arethought to be a consequence of a disrupted retinotopy in V1 (Li,Dumoulin, Mansouri, & Hess, 2007). There is also evidence for adeficit to the discrimination of orientation (Barrett, Pacey, Bradley,Thibos, & Morrill, 2003; Demanins, Hess, Williams, & Keeble, 1999;Skottun, Bradley, & Freeman, 1986; Vandenbussche, Vogels, & Or-ban, 1986) that is thought to be low-level in nature. However,the low-level orientation deficit is restricted to high spatial fre-quencies and as such may not provide a complete explanationfor the present results since the radial frequency stimuli used herewere of relatively low spatial frequencies (3 or 6 c/deg).
References
Aaen-Stockdale, C., & Hess, R. F. (2008). The amblyopic deficit for global motion isspatial scale invariant. Vision Research, 48(19), 1965–1971.
Barrett, B. T., Pacey, I. E., Bradley, A., Thibos, L. N., & Morrill, P. (2003). Nonveridicalvisual perception in human amblyopia. Investigative Ophthalmology & VisualScience, 44(4), 1555–1567.
Bedell, H. D., & Flom, M. C. (1981). Monocular spatial distortion in strabismicamblyopia. Investigative Ophthalmology & Visual Science, 20(2), 263–268.
Brainard, D. H. (1997). The psychophysics toolbox. Spatial Vision, 10, 433–446.Cadieu, C., Kouh, M., Pasupathy, A., Connor, C. E., Riesenhuber, M., & Poggio, T.
(2007). A model of V4 shape selectivity and invariance. Journal ofNeurophysiology, 98(3), 1733–1750.
Constantinescu, T., Schmidt, L., Watson, R., & Hess, R. F. (2005). A residual deficit forglobal motion processing after acuity recovery in deprivation amblyopia.Investigative Ophthalmology & Visual Science, 46, 3008–3012.
Demanins, R., Hess, R. F., Williams, C. B., & Keeble, D. R. (1999). The orientationdiscrimination deficit in strabismic amblyopia depends upon stimulusbandwidth. Vision Research, 39(24), 4018–4031.
Ellemberg, D., Lewis, T. L., Maurer, D., Brar, S., & Brent, H. P. (2002). Betterperception of global motion after monocular than after binocular deprivation.Vision Research, 42(2), 169–179.
Giaschi, D. E., Regan, D., Kraft, S. P., & Hong, X. H. (1992). Defective processing ofmotion-defined form in the fellow eye of patients with unilateral amblyopia.Investigative Ophthalmology & Visual Science, 33, 2483–2489.

R. Dallala et al. / Vision Research 50 (2010) 1612–1617 1617
Hess, R. F. (1976). Threshold contrast sensitivity in amblyopia. (University ofMelbourne).
Hess, R. F., & Holliday, I. E. (1992). The spatial localization deficit in amblyopia.Vision Research, 32(7), 1319–1339.
Hess, R. F., Wang, Y.-Z., & Dakin, S. C. (1999). Are judgements of circularity local orglobal? Vision Research.
Hess, R. F., Wang, Y.-Z., Demanins, R., Wilkinson, F., & Wilson, H. R. (1999). A deficitin strabismic amblyopia for global shape detection. Vision Research, 39,901–914.
Ho, C. S., & Giaschi, D. E. (2006). Deficient maximum motion displacement inamblyopia. Vision Research, 46, 4595–4603.
Ho, C. S., Giaschi, D. E., Boden, C., Dougherty, R., Cline, R., & Lyons, C. (2005).Deficient motion perception in the fellow eyes of amblyopic children. VisionResearch, 45, 1615–1627.
Jeffrey, B. G., Wang, Y. Z., & Birch, E. E. (2002). Circular contour frequency in shapediscrimination. Vision Research, 42(25), 2773–2779.
Jeffrey, B. G., Wang, Y. Z., & Birch, E. E. (2004). Altered global shape discrimination indeprivation amblyopia. Vision Research, 44(2), 167–177.
Levi, M., & Harwerth, R. S. (1977). Spatio–temporal interactions in anisometropicand strabismic amblyopia. Investigative Ophthalmology & Visual Science, 16(1),90–95.
Levi, D. M., & Klein, S. A. (1983). Spatial localization in normal and amblyopic vision.Vision Research, 23(10), 1005–1017.
Li, X., Dumoulin, S. O., Mansouri, B., & Hess, R. F. (2007). The fidelity of the corticalretinotopic map in human amblyopia. European Journal of Neuroscience, 25,1265–1277.
Mansouri, B., & Hess, R. F. (2006). The global processing deficit in amblyopiainvolves noise segregation. Vision Research, 46(24), 4104–4117.
Nachmias, J. (1981). On the psychometric function for contrast detection. VisionResearch, 21, 215–223.
Pasupathy, A., & Connor, C. E. (1999). Responses to contour features in macaquearea V4. Journal of Neurophysiology, 82(5), 2490–2502.
Pasupathy, A., & Connor, C. E. (2002). Population coding of shape in area V4. NatureNeuroscience, 5(12), 1332–1338.
Pelli, D. G. (1997). The VideoToolbox software for visual psychophysics:Transforming numbers into movies. Spatial Vision, 10(4), 437–442.
Poirier, F. J., & Wilson, H. R. (2006). A biologically plausible model of human radialfrequency perception. Vision Research, 46(15), 2443–2455.
Shannon, C. E. (1949). Communication in the presence of noise. Proceedings of theIRE, 37, 10–21.
Simmers, A. J., Ledgeway, T., & Hess, R. F. (2004). The influences of visibility andanomalous integration processes on the perception of global spatial form versusmotion in human amblyopia. Vision Research, 45(4), 449–460.
Simmers, A. J., Ledgeway, T., & Hess, R. F. (2005). The influences of visibility andanomalous integration processes onb the perception of global spatial formversus motion in human amblyopia. Vision Research, 45(4), 449–460.
Simmers, A. J., Ledgeway, T., Hess, R. F., & McGraw, P. V. (2003). Deficits to globalmotion processing in human amblyopia. Vision Research, 43, 729–738.
Simmers, A. J., Ledgeway, T., Mansouri, B., Hutchinson, C. V., & Hess, R. F. (2006). Theextent of the dorsal extra-striate deficit in amblyopia. Vision Research, 46,2571–2580.
Sireteanu, R., Lagreze, W. D., & Constantinescu, D. H. (1993). Distortions in two-dimensional visual space perception in strabismic observers. Vision Research, 33,677–690.
Skottun, B. C., Bradley, A., & Freeman, R. D. (1986). Orientation discrimination inamblyopia. Investigative Ophthalmology & Visual Science, 27(4), 532–537.
Swanson, W. H., & Birch, E. E. (1992). Extracting thresholds from noisypsychophysical data. Perception & Psychophysics, 51(5), 409–422.
Swanson, W. H., Wilson, H. R., & Giese, S. C. (1984). Contrast matching datapredicted from contrast increment thresholds. Vision Research, 24(1), 63–75.
Vandenbussche, E., Vogels, R., & Orban, G. A. (1986). Human orientationdiscrimination: Changes with eccentricity in normal and amblyopic vision.Investigative Ophthalmology & Visual Science, 27(2), 237–245.
Wang, Y.-Z., & Hess, R. F. (2005). Contributions of local orientation and positionfeatures to shape integration. Vision Research, 45, 1375–1383.
Wang, Y.-Z., Wilson, C. E., Felius, J., & Birch, E. E. (2006). The roles of position andorientation features in shape discrimination deficits of amblyopia. InvestigativeOphthalmology & Visual Science, 47 (E-Abstract 5407).
Weibull, W. (1951). A statistical distribution function of wide applicability. Journalof Applied Mechanics, 18, 293–297.
Wilkinson, F., James, T. W., Wilson, H. R., Gati, J. S., Menon, R. S., & Goodale, M. A.(2000). An fMRI study of the selective activation of human extrastriate formvision areas by radial and concentric gratings. Current Biology, 10(22),1455–1458.
Wilkinson, F., Wilson, H. R., & Habak, C. (1998). Detection and recognition of radialfrequency patterns. Vision Research, 38(22), 3555–3568.