Embed Size (px)
Citation preview
The Global Elimination of Lymphatic Filariasis
The Story of Zanzibar
WHO/CDS/CPE/SMT/2002.15
ACKNOWLEDGEMENTS
The lymphatic filariasis (LF) elimination programme in Zanzibar is the story of the hardwork and commitment, primarily of the people of Zanzibar. This document is an attemptto portray the dedication of the many people who were convinced of the importance ofthe LF programme and made the campaign a success. WHO is indebted to those who arementioned within the pages of this publication, and also those not mentioned whonevertheless saw a vital role for themselves in making a difference to the health of theircommunities.
This publication has been made possible by a contribution from the Bill and MelindaGates Foundation.
© World Health Organization 2002
This document is not a formal publication of the World Health Organization (WHO), and all rights are reserved by theOrganization. The document may, however, be freely reviewed, abstracted, reproduced or translated, in part or in whole, butnot for sale or for use in conjunction with commercial purposes. The views expressed in documents by named authors aresolely the responsibility of those authors.
WORLD HEALTH ORGANIZATION
The Global Elimination of Lymphatic Filariasis
The Story of Zanzibar

WHO Tanzania Country Office
WHO AFRO Regional Support
WHO HQ Social Mobilization Team (CPE/SMT)
WHO HQ Country Technical Support Team (CPE/CEE)
Contents
Letter from the WHO LF Support Team (HQ) 4
Lymphatic filariasis and the strategy for its elimination 6
Living with lymphatic filariasis 8
The partnership 9
Zanzibar profile 11
What is the value of eliminating LF? 12
The plan 14
The cost/value calculation 16
Personal sellers 18
Whose campaign is this? 20
Supporting the personal sellers 21
Radio script 23
The best laid plans... 24
Decision to postpone or continue 26
Politics 28
The vital link 30
F-Day 32
The Mop-Up Day 35
Keys to success 36
Partnerships: thinking global... and acting local 38
The future 40
Letter from the WHO LF Support Team (HQ)
4
Zanzibar was a challenge. Almost everyone inZanzibar, nearly a million people, needed to beconvinced that they had to swallow free butpotent drugs. And they all had to do it on thesame day, Saturday, 27 October 2001. It wouldbe one of the largest mass drug administrationsever attempted. And if it worked, then 27October would be the beginning of the end forthe stigmatizing and incurable parasitic diseaseknown as lymphatic filariasis (LF), the world’ssecond leading cause of disability. And with theelimination of LF, elephantiasis, the disfiguringdisease caused by the filariasis parasite, wouldvanish over time as well.
No longer would people be anchored in life bygiant legs or other horrors of the disease.
If the majority of the population did take thedrugs once a year for at least five years, then transmission would essentially be stopped.The risk was that if the target was not reached,the exercise would largely be a waste of time,effort and money.
The challenges in Zanzibar were enormous and,quite frankly, more than we expected. The
prevalence of LF parasite in the country is oneof the world’s highest. Around 15% of peoplecarry the parasite. In some villages, infectionrates were well over 30%. The social environ-ment also presented special challenges to adrug distribution programme. Prior to October,research revealed the presence of widespreadmisconceptions about LF — that the diseasewas caused by witchcraft or eating green coco-nuts. Once the campaign was launched,rumours began circulating that the free tabletswere a form of birth control or had unknown side-effects. If this wasn’t enough,logistical and financial problems arose thatthreatened to sink the entire effort. In fact, thedrugs themselves arrived in Zanzibar too closeto 27 October, "F-Day".
What follows is the story of the LF campaign inZanzibar. It is one of the most unusual healthcampaigns ever.
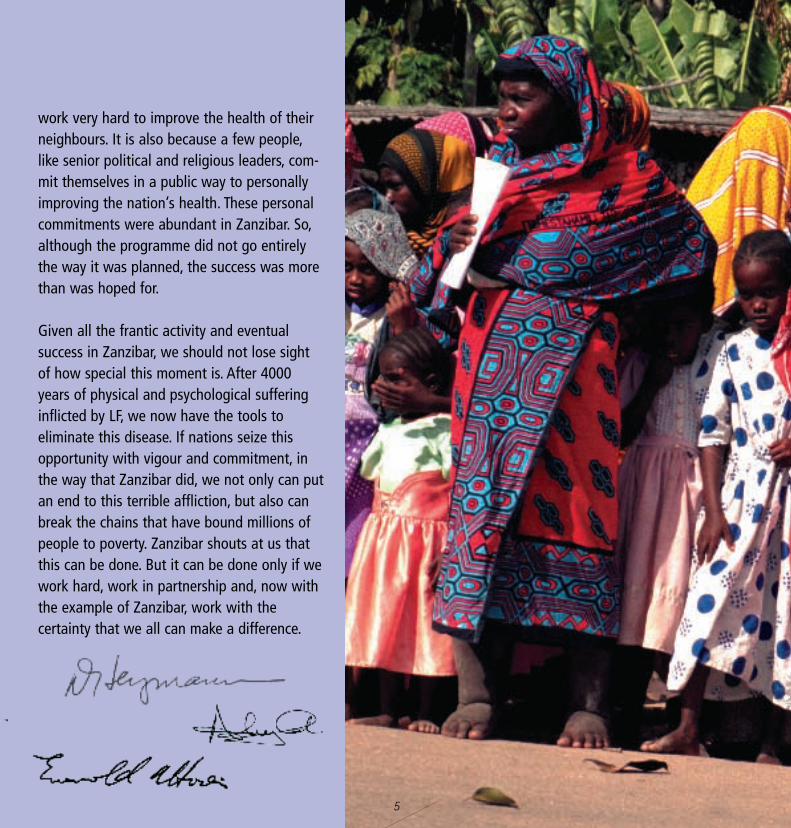
In Zanzibar, we were reminded again that WHO is a technical agency. We supply, primarily,expert advice. But no matter how good ouradvice is, if a health campaign is to be success-ful it is because thousands of ordinary people
5
work very hard to improve the health of theirneighbours. It is also because a few people,like senior political and religious leaders, com-mit themselves in a public way to personallyimproving the nation’s health. These personalcommitments were abundant in Zanzibar. So,although the programme did not go entirelythe way it was planned, the success was morethan was hoped for.
Given all the frantic activity and eventual success in Zanzibar, we should not lose sightof how special this moment is. After 4000years of physical and psychological sufferinginflicted by LF, we now have the tools to eliminate this disease. If nations seize thisopportunity with vigour and commitment, inthe way that Zanzibar did, we not only can putan end to this terrible affliction, but also canbreak the chains that have bound millions ofpeople to poverty. Zanzibar shouts at us thatthis can be done. But it can be done only if wework hard, work in partnership and, now withthe example of Zanzibar, work with the certainty that we all can make a difference.
Lymphatic filariasisand the strategy for its elimination
ore than 120 millionpeople are infected with the lymphaticfilariasis parasite. The lives of 40 mil-lion people are limited and disfiguredby the disease. For them, there is nocure. The remaining 80 million infectedpeople risk the same fate. Thesepeople have impaired immune systemsand are at risk of developing the grossdeformities.
Lymphatic filariasis does not kill, butin most countries of the world itinflicts an enormous physical and psychological destruction. LF hits hardest among the poorest peopleand, because its victims are renderedunable to work, they are shackled ineven more desperate poverty.
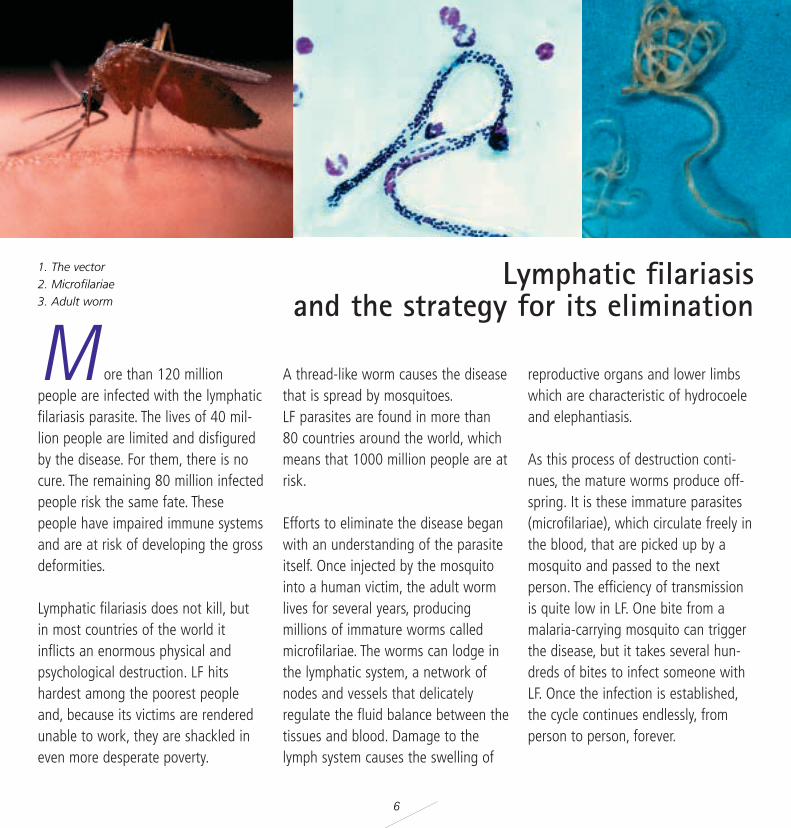
A thread-like worm causes the diseasethat is spread by mosquitoes.LF parasites are found in more than80 countries around the world, whichmeans that 1000 million people are atrisk.
Efforts to eliminate the disease beganwith an understanding of the parasiteitself. Once injected by the mosquitointo a human victim, the adult wormlives for several years, producing millions of immature worms calledmicrofilariae. The worms can lodge inthe lymphatic system, a network ofnodes and vessels that delicately regulate the fluid balance between thetissues and blood. Damage to thelymph system causes the swelling of
reproductive organs and lower limbswhich are characteristic of hydrocoeleand elephantiasis.
As this process of destruction conti-nues, the mature worms produce off-spring. It is these immature parasites(microfilariae), which circulate freely inthe blood, that are picked up by amosquito and passed to the next person. The efficiency of transmissionis quite low in LF. One bite from amalaria-carrying mosquito can triggerthe disease, but it takes several hun-dreds of bites to infect someone withLF. Once the infection is established,the cycle continues endlessly, fromperson to person, forever.
M
6
1. The vector2. Microfilariae 3. Adult worm
7
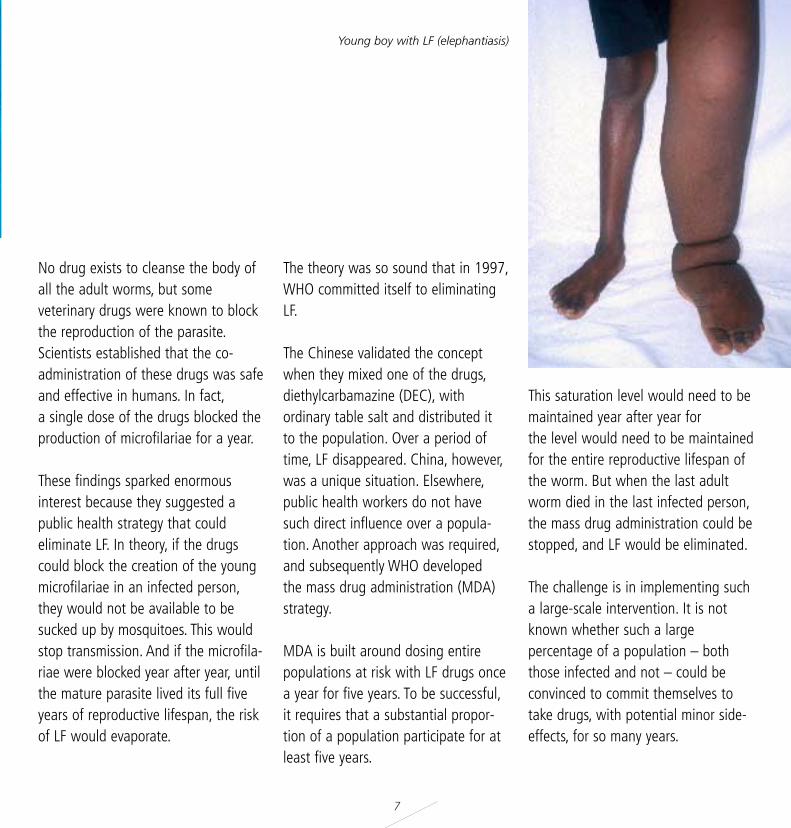
Young boy with LF (elephantiasis)
No drug exists to cleanse the body ofall the adult worms, but some veterinary drugs were known to blockthe reproduction of the parasite.Scientists established that the co-administration of these drugs was safeand effective in humans. In fact,a single dose of the drugs blocked theproduction of microfilariae for a year.
These findings sparked enormousinterest because they suggested apublic health strategy that could eliminate LF. In theory, if the drugscould block the creation of the youngmicrofilariae in an infected person,they would not be available to be sucked up by mosquitoes. This wouldstop transmission. And if the microfila-riae were blocked year after year, untilthe mature parasite lived its full fiveyears of reproductive lifespan, the riskof LF would evaporate.
The theory was so sound that in 1997,WHO committed itself to eliminatingLF.
The Chinese validated the conceptwhen they mixed one of the drugs,diethylcarbamazine (DEC), with ordinary table salt and distributed it to the population. Over a period oftime, LF disappeared. China, however,was a unique situation. Elsewhere,public health workers do not havesuch direct influence over a popula-tion. Another approach was required,and subsequently WHO developed the mass drug administration (MDA)strategy.
MDA is built around dosing entirepopulations at risk with LF drugs oncea year for five years. To be successful,it requires that a substantial propor-tion of a population participate for atleast five years.
This saturation level would need to bemaintained year after year for the level would need to be maintainedfor the entire reproductive lifespan ofthe worm. But when the last adultworm died in the last infected person,the mass drug administration could bestopped, and LF would be eliminated.
The challenge is in implementing sucha large-scale intervention. It is notknown whether such a large percentage of a population – boththose infected and not – could beconvinced to commit themselves totake drugs, with potential minor side-effects, for so many years.

8
Living with LFJaku Hassan Ali is a fishmonger and estimates he is about 65 years old although he is not certain. He has had elephantiasis since he was a child and believes heacquired the disease while playing in muddy water.
Today, his left leg is enormous. His toes, which stick out from the folds of his leg,are the only visible sign of feet. His pants are cut off above the knee and rippedthrough the crotch to accommodate the leg. A doctor recently advised him to havehis leg amputated, but he declined because he needs it to ride his bicycle.
Does he feel depressed?
- "No," he says. "This is God's plan. It is from God, so I will endure it."
Jaku is one of the lucky ones, he has managed to support a wife, raised a familyand now has grandchildren.
For many others, LF has a devastating psy-chological, economic and social impact.According to Kassim Ali, a community healthnurse: "They have shame to walk among thepeople. Working is reduced. Wounds makeoffensive smell. People tend to isolate themselves."
Jaku Hassan Ali

T
9
he theory of LF elimination wasgiven a chance to prove itself in 1998when the pharmaceutical firmGlaxoSmithKline (previously known asSmithKlineBeecham) offered to donateits product albendazole, which inassociation with DEC or ivermectinwill prevent the production of new,young worms. The pharmaceuticalcompany pledged, and reaffirmed itscommitment in a Memorandum ofUnderstanding with the World HealthOrganization, to provide albendazolefor as long as it was needed. And itwould be free. This would likely meandonating 4 to 6 billion tablets over 20years. The London Financial Times cal-led it "the biggest single act of corpo-rate philanthropy in any industry."
Another pharmaceutical firm, Merck &Co. Inc., which was providing its drugivermectin (Mectizan”) to help controlriver blindness, announced that it toowould provide its drug in Africancountries where the two diseases existside by side.
The agreement between WHO andGlaxoSmithKline attracted the supportof dozens of governments, universities,UN organizations, international deve-lopment agencies, NGOs and philan-thropists. They decided to join forcesto work towards eliminating LF. Thispublic–private partnership is known asthe Global Alliance to EliminateLymphatic Filariasis.
The Bill and Melinda GatesFoundation provided enough seedmoney to the Alliance to prove whe-ther or not mass drug administrationcould work.
When nations are committed to elimi-nating LF by working with the GlobalAlliance, they establish new synergies.This partnership generally includessome members of the Global Alliance,primarily WHO and the drug compa-nies, but it is always directed by thecountry concerned.
Zanzibar did this and WHO decided touse the Gates Foundation funds to runthe programme. Thus, Zanzibar beca-me a high-profile test of the strategyfor LF elimination.
The partnership
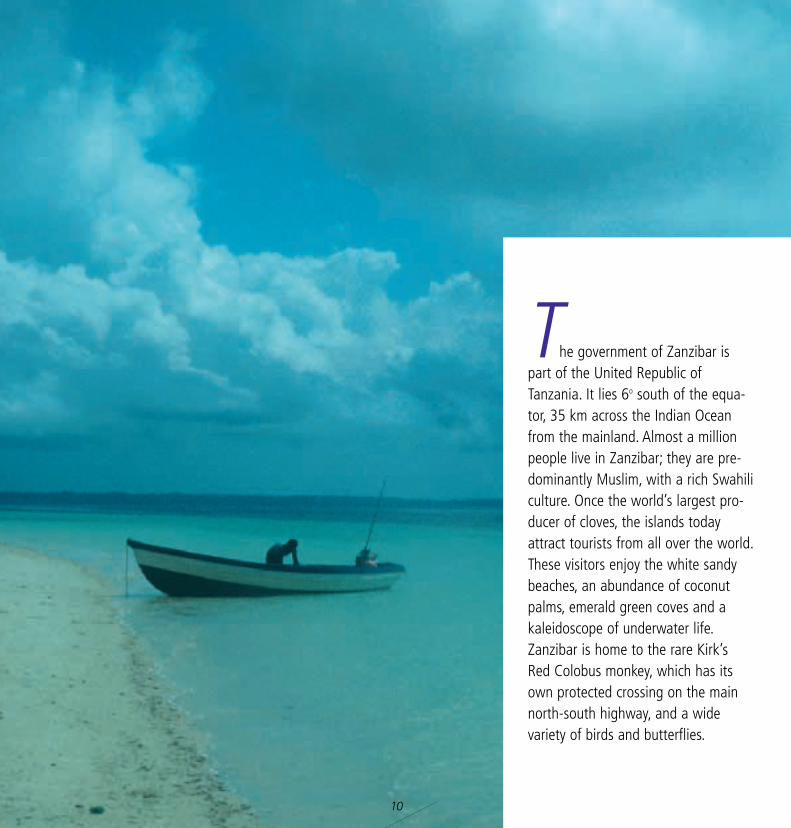
he government of Zanzibar ispart of the United Republic ofTanzania. It lies 6o south of the equa-tor, 35 km across the Indian Oceanfrom the mainland. Almost a millionpeople live in Zanzibar; they are pre-dominantly Muslim, with a rich Swahiliculture. Once the world’s largest pro-ducer of cloves, the islands todayattract tourists from all over the world.These visitors enjoy the white sandybeaches, an abundance of coconutpalms, emerald green coves and akaleidoscope of underwater life.Zanzibar is home to the rare Kirk’sRed Colobus monkey, which has itsown protected crossing on the mainnorth-south highway, and a widevariety of birds and butterflies.
10
T
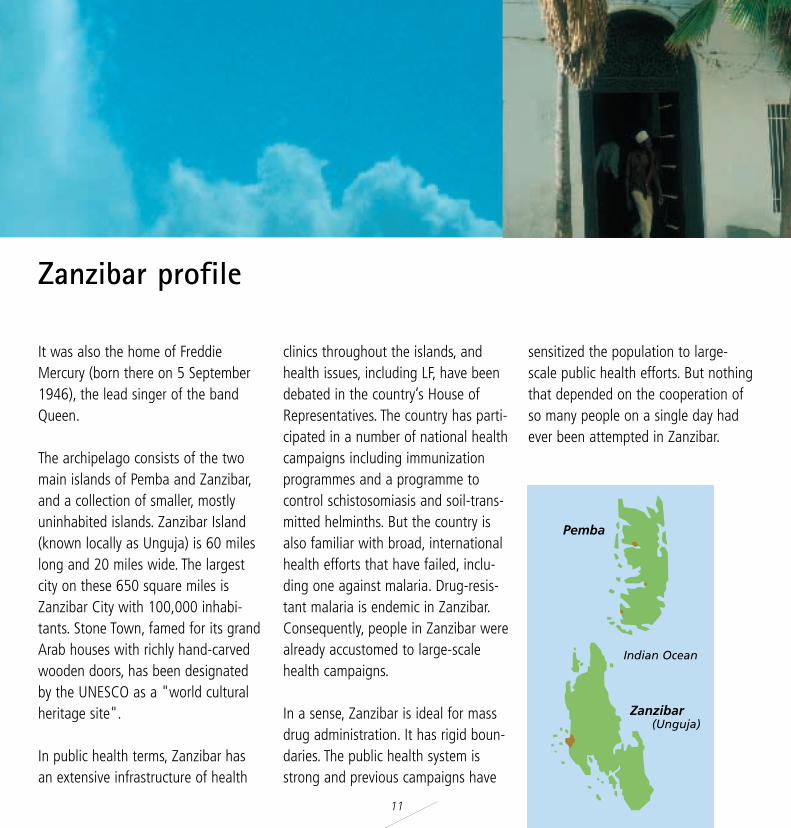
Pemba
Zanzibar (Unguja)
Indian Ocean
It was also the home of FreddieMercury (born there on 5 September1946), the lead singer of the bandQueen.
The archipelago consists of the twomain islands of Pemba and Zanzibar,and a collection of smaller, mostlyuninhabited islands. Zanzibar Island(known locally as Unguja) is 60 mileslong and 20 miles wide. The largestcity on these 650 square miles isZanzibar City with 100,000 inhabi-tants. Stone Town, famed for its grandArab houses with richly hand-carvedwooden doors, has been designatedby the UNESCO as a "world culturalheritage site".
In public health terms, Zanzibar has an extensive infrastructure of health
clinics throughout the islands, andhealth issues, including LF, have beendebated in the country’s House ofRepresentatives. The country has parti-cipated in a number of national healthcampaigns including immunizationprogrammes and a programme tocontrol schistosomiasis and soil-trans-mitted helminths. But the country isalso familiar with broad, internationalhealth efforts that have failed, inclu-ding one against malaria. Drug-resis-tant malaria is endemic in Zanzibar.Consequently, people in Zanzibar werealready accustomed to large-scalehealth campaigns.
In a sense, Zanzibar is ideal for massdrug administration. It has rigid boun-daries. The public health system isstrong and previous campaigns have
sensitized the population to large-scale public health efforts. But nothingthat depended on the cooperation ofso many people on a single day hadever been attempted in Zanzibar.
11
Zanzibar profile
12
When people were first told about the free drug programme for LF,they often asked: "Why are you givingus drugs for this when malaria is killing us?"
Indeed LF does not kill suddenly, but it kills slowly, gradually reducing life expectancy. And while it has been shown elsewhere to inflict a drain onthat nation’s economy amounting up to $1 billion annually, in Zanzibar onlyanecdotal reports link LF to erosion ofpersonal income.
Still, ending LF will have important benefits to the country’s health system.The most obvious is that children will be
saved from the disease. Also, funds nowused by the Ministry of Health for LF willbe freed for other pressing public healthneeds.
As the LF campaign in Zanzibar unfol-ded, it became clear that the implica-tions of ending LF extend far beyondpublic health.
Political leaders in Zanzibar acknowledgethat if LF is pushed out of the islands,faith will be revived in health initiativesbased on collaboration with internatio-nal agencies and commercial donors.Also, the LF campaign could help to instila medically-based sense of why diseasedevelops and how it can be cured.
What is the value of eliminating LF?
13
"It has a social value," says Dr H.Nyanga, the zonal medical officer for theIsland of Pemba. "We would like to getrid of the idea that filariasis is a result of witchcraft. We would like to eradicatethat idea. It is a belief that affects otherdiseases as well, such as cerebral mala-ria and strokes. If we eliminate this idea,we will have more hospital attendees.People will be coming to the hospitalinstead of going to witch doctors."
And if the Zanzibar government is ableto put an end to LF, it could also helprebuild the people's faith in their government."If it works, it will show thepeople that government takes care oftheir health," says Omar Mussa,
Principal Secretary of Zanzibar’s Ministryof Health and Social Welfare. "They willcome to conclude that government ismore caring of them."
Faith in government. Faith in internatio-nal health campaigns. Faith in medicine.More funds for other diseases. Healthierchildren. And a more robust economy.All this and more is riding on the LFcampaign in Zanzibar.
"If it works, it will show the people thatgovernment takes care of their health,"
Omar Mussa, Principal Secretary of Zanzibar’sMinistry of Health and Social Welfare.
14
ever before had a health campaign ever attempted to motivatenearly a million people to participate,by personally swallowing tablets for adisease they may or may not have.To do that, people would have to beconvinced that the disease was a riskfor them and their families. Theywould also have to believe that thedrugs, which have potential minorside-effects, would be effective and safe.
"This is more difficult than curativemedicine," said Dr. Hyanga Nyanga,the zonal medical officer for the islandof Pemba. "If somebody is not sickand then you tell them to swallowdrugs, they will not be willing."
To persuade people to take the medi-cine requires a well-informed public.But LF experts in Zanzibar warned thatthere were long-held and widely belie-ved misconceptions about the disease.For example, a substantial numberbelieved it resulted from witchcraft.And many people thought that elephantiasis of the legs and of thegenitals were two different diseases.
To help develop a social mobilizationplan, WHO sent two social mobiliza-tion experts to Zanzibar in late June2001 to work with the local authorities. One of the advisers hadoriginated a marketing strategy forpromoting health behaviours knownas COMBI (Communication-For-Behavioural-Impact).
The plan
NZanzibar Airport
15
The other adviser had experienceusing the COMBI approach for a poliocampaign in her homeland of“Somaliland”.
COMBI begins with an intimate appreciation of the "customer". At theheart of COMBI is an intimate unders-tanding and appreciation of the perspective of those who will benefitfrom the programme. That is what’sdifferent about this. COMBI also identifies the barriers and constraintsthat may prevent people from takingup the treatment.
Zanzibar’s health, media and govern-ment officials working with WHO staffand consultants, designed a broadsocial mobilization campaign.
The campaign consisted of manytasks, each of which needed to beperformed in the right sequence andat the right time. If it worked, it wouldbe a human symphony. A big failurecould capsize the project. If the cam-paign failed to get enough people toparticipate then the size of the remai-ning reservoir of infected peoplewould be too large to interrupt thecycle of transmission. The campaignwould fail.
One of the complications facing theplanners was that not everyone wouldbe eligible to take the drugs. About100,000 people would be unable toparticipate. They included the veryyoung and very sick, pregnant womenand women in the first week of lactation. So the target population in
Zanzibar was not 900,000 but800,000 persons. This meant that toprotect the entire population, LF drugshad to be taken by all of the eligiblepopulation. The LF campaign wouldhave little room for error.
A lot would be riding on the successof COMBI.
Zanzibar was split into 10 operationalunits. A team of four people headedby a District Supervisor were respon-sible for planning, implementation andco-ordination of the campaign fortheir districts.
The highly populated urban areas,including Stone Town, were furthersplit into three zones.
One of the markets in Zanzibar.
16
o better understand their custo-mers, the WHO social mobilizationadvisers began what they called "walking around research". They tra-velled to villages and talked with lea-ders, knocked on household doors andasked to chat. One of them metpeople while jogging, and they alsointerviewed taxi drivers and restaurant waiters. They studied theculture, politics and history of Zanzibarand what people knew about thedisease. While they found there was ageneral awareness about the disease,they also found something that wasdeeply troubling. "I didn’t get a sensethat people felt they were at risk ofthe disease," recalls one of WHO’sadvisers.
Unless people felt a personal risk, itwould be hard to motivate them totake the drugs. Many people did notknow that LF came from mosquitoes.With this understanding, the WHOteam met with members of the ministries of health and of education,and began to outline a potential campaign.
An initial proposal suggested establi-shing drug depots, like those that hadbeen used in the polio vaccinationprogramme, where people could go toget their LF drugs. WHO advised thatthis would not work. According to theCOMBI theory, individuals made deci-sions based on "cost versus benefit"calculations. Distribution centres hadbeen a success in the polio campaign,but with polio the risk was to one’s
child which has a greater urgencythan the risk to oneself. Moreover, incountries where the polio campaignswere operating, polio was a visiblerisk. Everyone was aware of it, andaware that his or her children were atrisk. Consequently, because the riskwas perceived as real and a risk totheir children, the "cost" (time, effort,money) of going to a health centrewas low.
The cost/value calculation for LF wasjust the opposite. The value of thedrugs was already perceived to be lowsince most people felt they were notat risk or they could avoid the riskaltogether by not eating green coco-nuts or taking other preventativesteps. The "cost" of acquiring thesedrugs would be high if people were
The cost/value calculation
T
17
required to leave home. The highcoverage threshold would not be reached, the WHO social mobilizationexperts said, if it relied on drugdepots.
For the LF campaign to succeed, theperceived cost had to be lowered.WHO advised and the Zanzibariauthorities agreed that delivering thefree drugs directly to the home wouldentail the lowest possible cost. Withhome delivery, the only need was toswallow the tablets.
In addition to lowering the cost, thecampaign needed to increase the perceived value of the drugs. Thegovernment/WHO team decided thatLF information had to reach into thehome. People had to know that the
disease was caused by parasites delivered in the bite of a mosquito,that it could lie dormant for years,that the disease was incurable when it appeared, and most importantly that everyone was at considerable personal risk.
The people of Zanzibar had to understand that the drugs could killthe parasites but in order to protectthe entire community, everyone had to take the drugs.
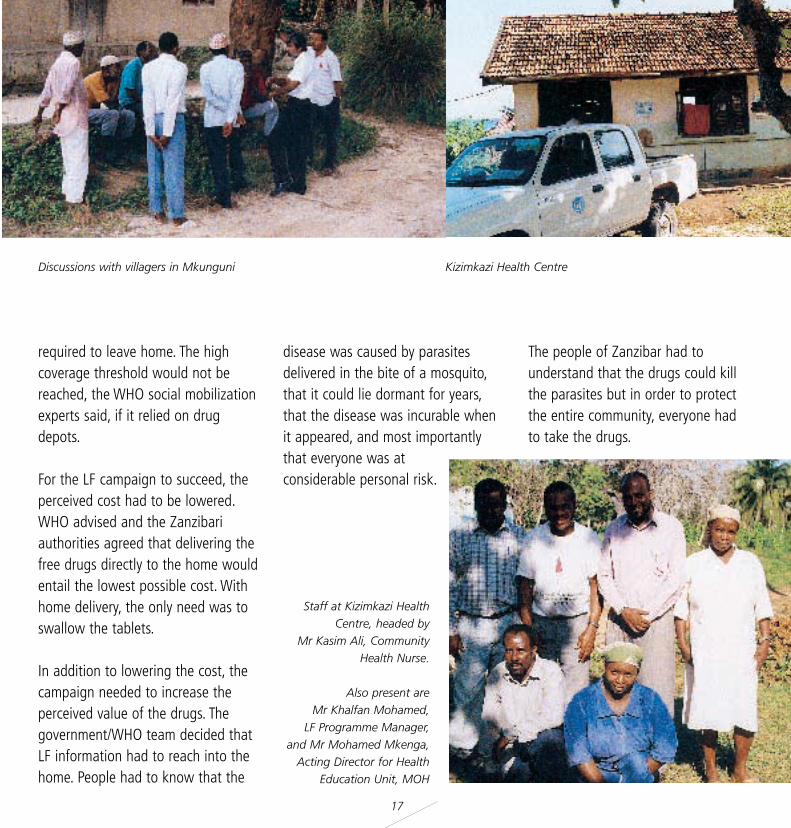
Staff at Kizimkazi HealthCentre, headed by
Mr Kasim Ali, CommunityHealth Nurse.
Also present are Mr Khalfan Mohamed,
LF Programme Manager,and Mr Mohamed Mkenga,
Acting Director for HealthEducation Unit, MOH
Discussions with villagers in Mkunguni Kizimkazi Health Centre
18
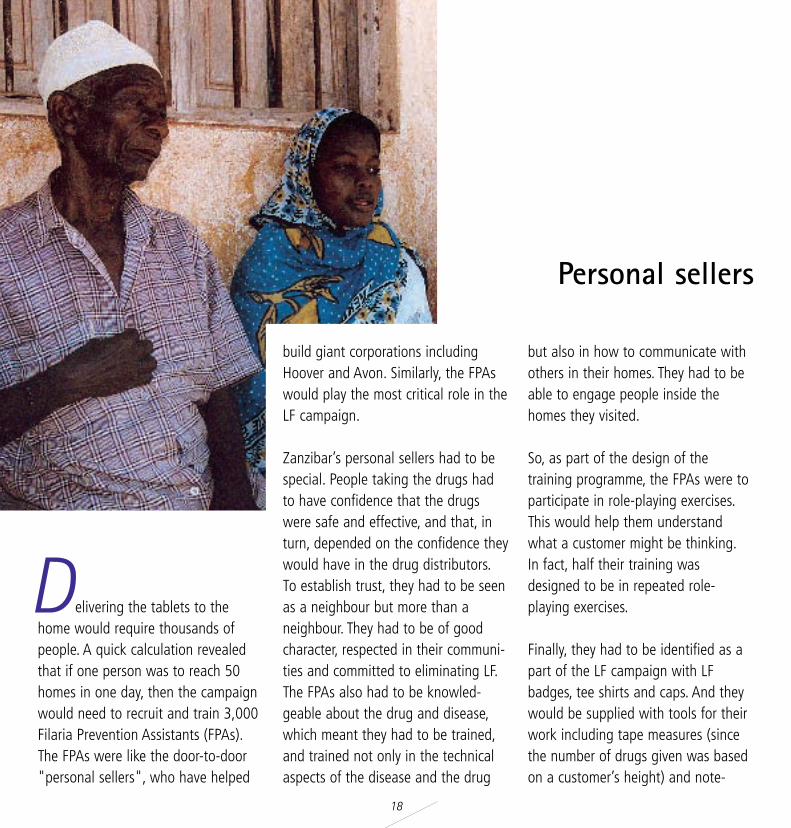
elivering the tablets to thehome would require thousands ofpeople. A quick calculation revealedthat if one person was to reach 50homes in one day, then the campaignwould need to recruit and train 3,000Filaria Prevention Assistants (FPAs).The FPAs were like the door-to-door"personal sellers", who have helped
build giant corporations includingHoover and Avon. Similarly, the FPAswould play the most critical role in theLF campaign.
Zanzibar’s personal sellers had to bespecial. People taking the drugs hadto have confidence that the drugswere safe and effective, and that, inturn, depended on the confidence theywould have in the drug distributors.To establish trust, they had to be seenas a neighbour but more than aneighbour. They had to be of goodcharacter, respected in their communi-ties and committed to eliminating LF.The FPAs also had to be knowled-geable about the drug and disease,which meant they had to be trained,and trained not only in the technicalaspects of the disease and the drug
but also in how to communicate withothers in their homes. They had to beable to engage people inside thehomes they visited.
So, as part of the design of the training programme, the FPAs were toparticipate in role-playing exercises.This would help them understandwhat a customer might be thinking.In fact, half their training was designed to be in repeated role-playing exercises.
Finally, they had to be identified as apart of the LF campaign with LFbadges, tee shirts and caps. And theywould be supplied with tools for theirwork including tape measures (sincethe number of drugs given was basedon a customer’s height) and note-
Personal sellers
D
19
books to record who participated(vital for validating the total numberof participants). For nearly a week’sworth of work, the Ministry of Healthdecided the central players in this programme would be given the equivalent of US$16 for food andtransportation. This would consumenearly half of the campaign budget.
The FPAs would make three visits toeach home. The first visit, three weeksbefore Filaria Day or "F-Day", was toestablish a bond, to register eligiblefamily members and explain the purpose of F-Day. They would informpeople that everyone would need totake the tablets every year for the nextfive years. They would also talk about possible side-effects like headache orpain in the stomach or genitals. If this
happened, they said, it would meanthe drugs were working to clear theparasites. Mostly importantly, the FPAswould listen and respond to theconcerns of their "customers".
On the second visit, two weeks beforeF-day, the FPA would go over thesame messages, give each familymember a pencil with the F-Day logoand date as a reminder, and show thetablets. Showing the tablets wasimportant so that people could seeand hold the tablets they would betaking on Filaria Day. On this secondvisit too, the FPAs would inform thosein the home that each FPA would berequired to watch each person swallow their tablets, as well as answering any questions or concerns.
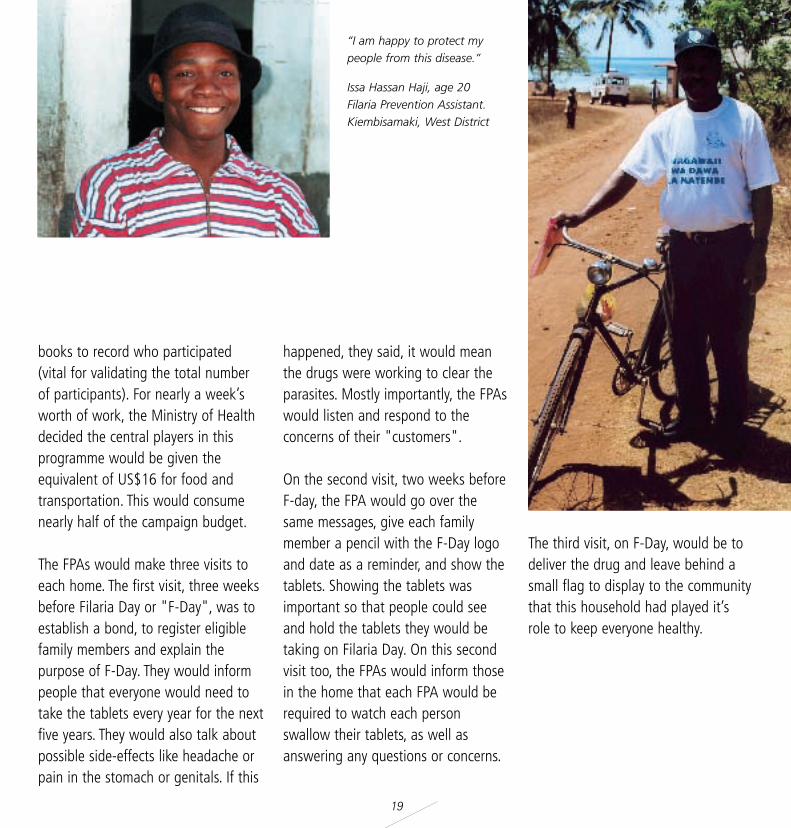
The third visit, on F-Day, would be todeliver the drug and leave behind asmall flag to display to the communitythat this household had played it’srole to keep everyone healthy.
“I am happy to protect mypeople from this disease.”
Issa Hassan Haji, age 20Filaria Prevention Assistant.Kiembisamaki, West District

20
Whose campaign is this?
The World Health Organization supplied technical assistance,negotiated with pharmaceutical companies to have the drugs provided
without cost, and channelled the Gates Foundation’s donation to finance the project.
Beyond that, this programme belonged to Zanzibar.
This is an important key to success. It helps explain why the LF programme team worked far into the night to overcome the obstacles that arose. And it explains why thousands
of drug distributors visited 50 to 90 homes time and again, even when the receptionwas sometimes hostile.
"They were motivated," says Zanzibar’s Principal Secretary of Health,Omar Mussa. "They felt this project was their own. It was not
owned by WHO. This was our project."
And the benefits, including building astronger relationship between the
government and the governed, areZanzibar’s as
well.
21
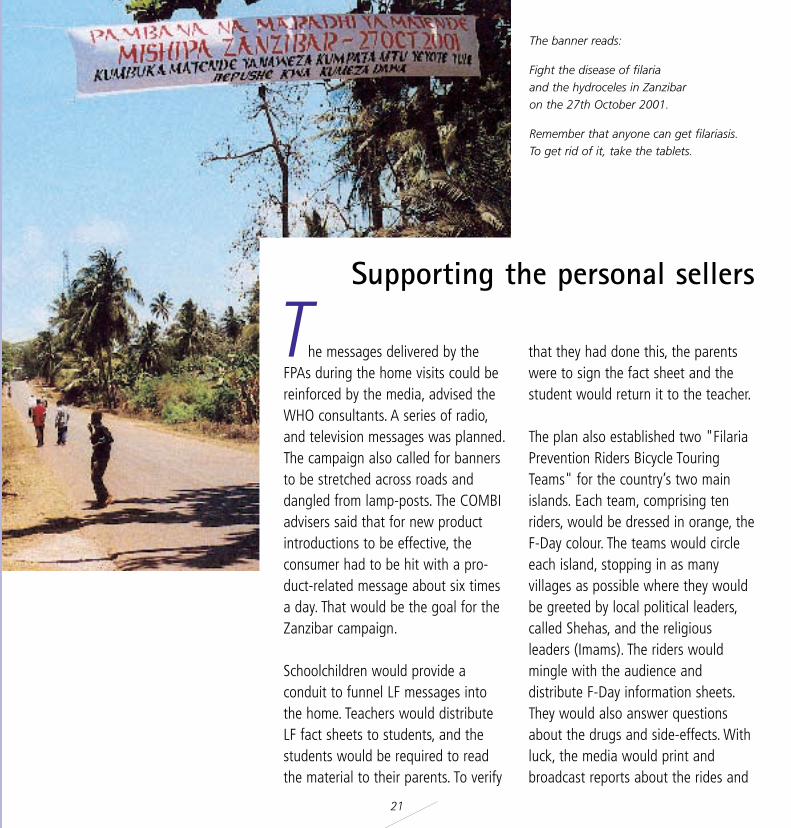
he messages delivered by theFPAs during the home visits could bereinforced by the media, advised theWHO consultants. A series of radio,and television messages was planned.The campaign also called for bannersto be stretched across roads and dangled from lamp-posts. The COMBIadvisers said that for new productintroductions to be effective, theconsumer had to be hit with a pro-duct-related message about six timesa day. That would be the goal for theZanzibar campaign.
Schoolchildren would provide aconduit to funnel LF messages intothe home. Teachers would distributeLF fact sheets to students, and the students would be required to readthe material to their parents. To verify
that they had done this, the parentswere to sign the fact sheet and thestudent would return it to the teacher.
The plan also established two "FilariaPrevention Riders Bicycle TouringTeams" for the country’s two mainislands. Each team, comprising tenriders, would be dressed in orange, theF-Day colour. The teams would circleeach island, stopping in as many villages as possible where they wouldbe greeted by local political leaders,called Shehas, and the religious leaders (Imams). The riders wouldmingle with the audience and distribute F-Day information sheets.They would also answer questionsabout the drugs and side-effects. Withluck, the media would print andbroadcast reports about the rides and
Supporting the personal sellers
T
The banner reads:
Fight the disease of filaria and the hydroceles in Zanzibar on the 27th October 2001.
Remember that anyone can get filariasis.To get rid of it, take the tablets.

22
thus deliver another LF message intothe home.
A lottery was also included in theplan. During the second home visit ofthe FPAs, residents would be allowedto enter their names in a lottery. Thoseselected and their FPAs would receiveprizes of donated colour televisionsets, bicycles and mopeds.
Closer to F-Day, a new series of eventswould be launched. The village political leaders would be asked tospread the LF messages at communitymeetings. Imams would be asked toinclude a mention of the programmeas part of their sermons in themosques on Friday, the day before F-Day. Sound trucks would announcethat F-Day had arrived. And on F-Dayitself, radio and television would
broadcast the news of Zanzibar’sPresident swallowing the tablets himself.
Not to be announced, but still part ofthe strategy, was a "mopping up"day, on the day following F-Day, to getat those people who had somehowbeen missed.
That was the plan. It was built aroundpersonal sellers who were backed by abroad advertising campaign, commu-nity leader involvement, promotionalincentives and intense media coverage.
Mrs Riziki Selele District Supervisor, Urban West District
Community Meeting: Mchangani shehia
23
Radio script "LF is endemic in our country. Everyone is at risk.About 15% have the parasites, worms, which aretransmitted from one infected person to another bymosquitoes. You know the problems of the disease.Once you have the disease there is no cure. Theseworms in the body cause the disease, and the wormscan exist in your body without any effect on you foryears. You will be as normal as everyone else, evenwith the worms in you. But a person infected with theworms will most likely get the first signs of filaria inabout five years or longer. If we kill these worms, thenwe don’t get the disease...We should assume that weall have the worms in us. If we can eliminate all theworms in everyone in our community, then we canget rid of the disease. We have the drugs to do justthis. For adults, just four tablets taken once a year forfive years will destroy the worms, which cause Filaria."The Ministry of Health will begin a campaign to eliminate Filaria on 27 October.
Our health workers will come to your home with thepills, which will destroy the worms that cause Filaria.These pills are free. They are usually very expensive,but the World Health Organization is making themavailable to us free. They are small tablets, easy toswallow. Yes, like every drug you take, some peoplemay have some side-effects such as headache andnausea. These are all temporary and will go away.People who are infected with the worms will proba-bly experience more of the side-effects as the drugsbegin their effect of killing the worms. Everyone mustjoin in taking the pills. If only some do, the mosqui-toes can still transmit the worms from the infectedwho did not take the pills to those who did take thepills.On Filaria Day, welcome our health workers, take thepills and swallow them. Protect yourself and yourfamily and your neighbours from the disease of Filariaand destroy the Filaria worms."

24
he WHO advisers had finished themost difficult part of their work andleft the island. Now it would be up tothe people and government ofZanzibar to discuss, adapt and executethe plan, with continued support andadvice from the WHO team.
The COMBI plan had been developedby members of the Zanzibar communi-ty, staff members of the Ministry ofHealth, and the technical advisersfrom WHO. Senior government officialsendorsed the plan, but dropped someof the proposed activities.
The areas dropped were thought of asthe "glitter" components of the plan.They included the cycling tour, theflags to be hung from houses of
participants, the dangle banners and,most importantly, the lottery.
Government officials would laterexplain that the nation had just finished an intense political campaignthat did not use any of these promo-tional activities. What, they askedthemselves, would people think ofsuch an extravagant effort to providetablets to them? The officials worriedthat such an intense effort might itselfcreate suspicion. ("If the programmewas so good, why spend so mucheffort?") And they didn’t want toconfuse a health campaign with political trappings.
The best laid plans...
T

25
Finally, they thought that severalaspects of the plan would produce afestive atmosphere rather than sensitize people to fight an unpleasanthealth situation.
More threatening was bureaucracy.Typically, requests for funds are pas-sed through a series of intermediariesfrom the country to WHO headquar-ters in Geneva; the money itself flowsthrough these same intermediariesfrom Geneva back to the country. Thesystem of accounting procedures isdesigned to prevent abuse and waste,and those involved in financial matters(WHO and counterparts) need to havean understanding and comply withthese procedures. In this case, the flow
of the funds lagged behind the needto fund activities as F-Day rapidlyapproached and the budget break-downs submitted were not detailedenough. The system was also jammedwhen estimates for printing postersseemed to be extraordinarily high.Dialogue, cooperation and transparency between WHO and theMinistry of Health has since ensuredthat a new system is in place whichpromises clarity and speed in financialaccountability.
For a time, the LF campaign wasunable to purchase anything. Justthree weeks before F-Day, there wereno posters, banners, tee shirts, badges,or balloons. And the FPAs were alsoleft without the tools they had expected.
Perhaps most threatening of all, withless than two weeks to go before F-Day, the drugs had not arrived.Actually, they had been transported toDar Es Salaam, but they were heldthere for a month. When the shipmentwas finally cleared, the drugs were puton a boat for Zanzibar. But when theregular ferry arrived, no drugs were onboard. In fact, the drugs had beensent on another boat and when noone claimed them at the dockside,they were returned to the mainland.More telephone calls followed, andthe shipment finally arrived inZanzibar to be claimed the followingday, just 11 days before F-Day.

26
hen one of the WHO advisersreturned to Zanzibar in early October,two-thirds of the COMBI plan had notbeen completed. Immediately, she wasasked if F-Day should be postponed.But first she conducted an assessmentof her own, by meeting with FPAsfrom rural and urban areas and fin-ding out what people knew of theprogramme.
The Zanzibar media campaign wasgoing well. The radio station, forexample, had done several talk-showsabout the campaign and regularlymentioned the campaign just beforeand just after the regular, widelybroadcast news programmes as wellas incorporating it into the mostpopular programmes.
A bigger problem was the impact onthe FPAs. They did not have their teeshirts and caps to identify them aspart of the LF campaign in their com-munities. They also were not providedwith the registration books to recordthe names of individuals eligible forthe treatment.
However, items in the campaign thatdidn’t require a cash payout had beenaccomplished. A National Task Forcewas formed along with a NationalTechnical Committee. The Task Forceset 27 October as F-Day. It was aSaturday, so most people would be athome. The Zanzibar LF team met withevery community leader, known asshehas, on both islands. Meetings withteachers were held and the teachersagreed to participate in the campaign
by distributing the information sheetsand balloons to pupils under 10. Noballoons or information had beenprinted, however, because of the disbursement snag. Members of theTask Force and Technical Committeevisited the main Islamic institutions in the country and won their supportas well.
The work of selecting and trainingdrug distributors had been completed.Many were teachers, which led tosome professional jealousy with regular health staff. Because initialestimates of households were basedon unreliable census data, it soonbecame apparent that more FPAswere needed. The corps of FPAs, whichwas initially set at 3,000 persons, roseto 4,077 in October. The training
Decision to postpone or continue
W

27
programme was robust enough toabsorb over 1,000 unplanned FPAs,but the budget remained fixed. Thesededicated people then decided amongthemselves to keep within the budgetby reducing their own reimbursementfor expenses from an equivalent ofUS$16 a person to just under $12.In this way, everyone could be paidand the programme would not be jeopardized.
Essentially, the WHO adviser foundthat there was a high awareness ofthe programme in the country and theFPAs had carried out the first visit.So, the decision of those involved inthe programme was not to postponebut to rapidly unfreeze the funds, dowhat could get done, and continuewith F-Day as planned.
The plan was triaged. The most important items were re-ordered intoa list of those items that could beaccomplished in the three weeksremaining. Quickly 7,000 posters wereprinted and distributed to the urbanareas only. The posters announced theprogramme and showed a mosquitobiting a human and a man swallowingwhite tablets. The 150 banners, askingpeople to participate and support the
programme, had already been printedand were waiting to be hung acrossroads and junctions throughout theIslands. Two hundred thousand information sheets were produced anddistributed to schoolchildren (someparents refused to sign them, fearingthat the tablets were dangerous andsigning relieved the provider from liability). FPAs were given the answersto the questions that had stumpedthem on their home visits.
Everything was now rushed: printingof extra posters, tee shirts, registrationbooks, badges and distributing materials, as well as the drugs.
With the critical support and facilitation of the WHO office and theMOH, time lost would be gained.
Essential tools for the FPAs being packed at the MOH warehouse before being collected and distributed by the District SupervisorsLeft page: Mr Ali Rashid, Co-ordinator for Pemba Island and Mr Said Uthman, Social Mobilization Consultant
28
PoliticsThe LF campaign unfolded during a politically sensitive year in Zanzibar. There wereminor misunderstandings between the ruling (CCM) and opposition party, and allegiance to one’s party is high. Hence the government could count on getting lessthan the majority of the population required to support the programme. However,reconciliation was high on the agendas of both parties.
"We don’t have such bad politics to go so far as to hurt the health of the people,"said Ismail Jussa Ladhu, an official with the opposition Civic United Front (CUF)."We want our people to be healthy to take part in the political developments of thecountry."
The success of the programme rested on the cooperation of both parties and the reconciliation conference that took place during October was the ideal opportunityfor a public display of unity. A chance for both parties to show that they had resolvedtheir differences and were working together for the future of their people.

29
"This disease doesn’t know the difference between the opposition and the government," says Uledi Mwita Kisumku, the Ministry of Health’s Deputy PrincipalSecretary. "It affects everybody. In the war against any disease, we have to collect allour forces. This is not really a political issue. It is a common problem for the wholecountry."
It is becoming apparent in Zanzibar that public health is an issue outside the boundaries of politics. After working together last year, the Principal Secretary ofHealth has pledged to give a more prominent role to the opposition in this year’smass drug administration campaign. In fact, senior members of the ruling party havesuggested that both the Chief Minister and the leader of the CUF be televised takingthe pills together on the next F-Day.
In its own way, the LF campaign is helping to repair tension in the country’s politicalsystem.
30
he FPAs, originally envisioned asthe heart of the project, had indeedturned out to be the dedicated peoplethe LF campaign needed. The localofficials had chosen people who weregenerally highly regarded in their com-munities, often teachers or healthworkers. Yet the job they faced was
tougher than anyone envisioned.Some FPAs had to cover not 50 homesas planned, but 60 or 70. (On F-Day,some would be asked to reach asmany as 90 homes.) The FPAs sometimes ran into hostile sentimentsin the homes they entered. And theyworked long hours; sometimes walking through rural areas at 11 p.m., to reach all the homes theywere responsible for.
"This is the first programme in whichwe worked so hard and received solittle," said one FPA, Mzee SalehAbdalla, a physical therapist fromPemba. "But this is our place. This isfor the benefit of our people."
The vital link
TUrban District Supervisors
31
The FPAs had attended a six-hour training programme and they hadconducted their initial visits. Withoutfunds to pay for the registrationbooks, the personal sellers had to usetheir own funds to buy school exercisebooks for the record-keeping.
After the first home visits, the FPAsfound that they needed further trai-ning. They were asked questions theycould not answer. Why are the drugsfree? Why not test our blood first?Why you, and not a medical doctor?Why LF, and not malaria? Why do Ihave to take the drug in front of thedistributor? What effect would thedrug have on people with diabetes,high blood pressure, heart problems,and ulcers?
A number of activities were undertaken to support the FPAs.
The WHO team asked the media toincrease their coverage and boost thenumber of LF ads running everyday.The BBC Swahili World Service prepared a report on 22 October forbroadcast before F-Day. Press releasesproduced news stories about the LFprogramme and interviews with officials in the Ministry of Health. Eventhe President of Zanzibar followed theLF programme through the media.
The FPAs conducted their secondhome visits, still without their tools.During the final week, the shehas heldextra community meetings about LF.On Thursday, 25 October, all school-children were asked to carry the
message home that the Saturdaywould be F-Day. During Friday sermons (khutbah) in the mosques,the Imams encouraged people to participate in the mass drug distribution.
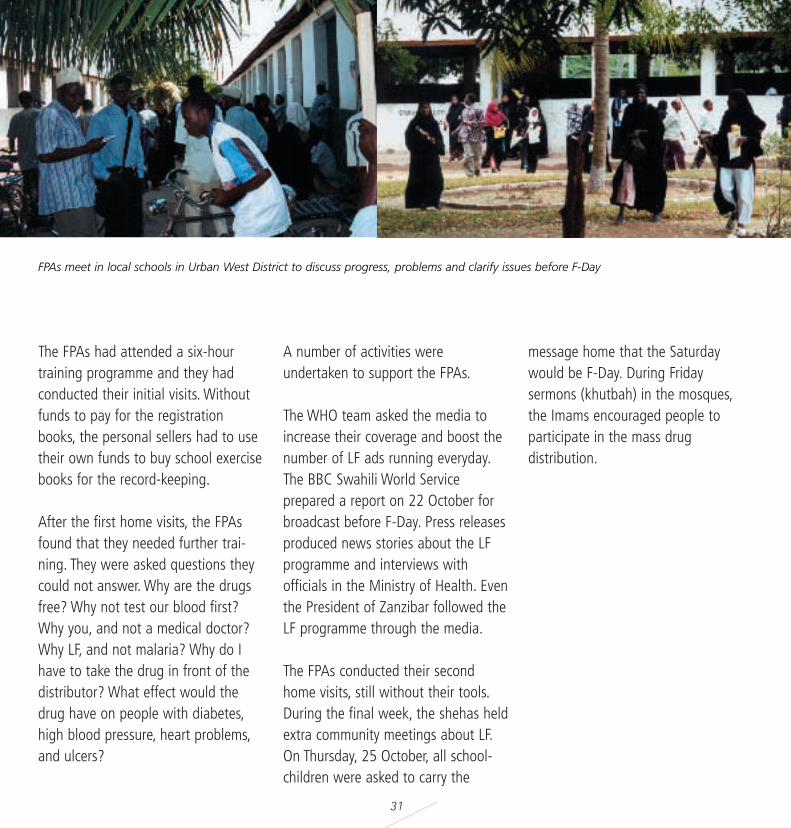
FPAs meet in local schools in Urban West District to discuss progress, problems and clarify issues before F-Day
32
verything was focused on 27October. This was the day the pro-gramme had to get the majority of thepopulation to participate and take thetablets.
The social mobilization campaign didits job of mobilizing the entire popula-tion. A substantial percentage ofZanzibaris had heard the LF messagesthrough radio and television, at community meetings, or from theirchildren, and seen the posters andbanners. The people were informedand motivated.
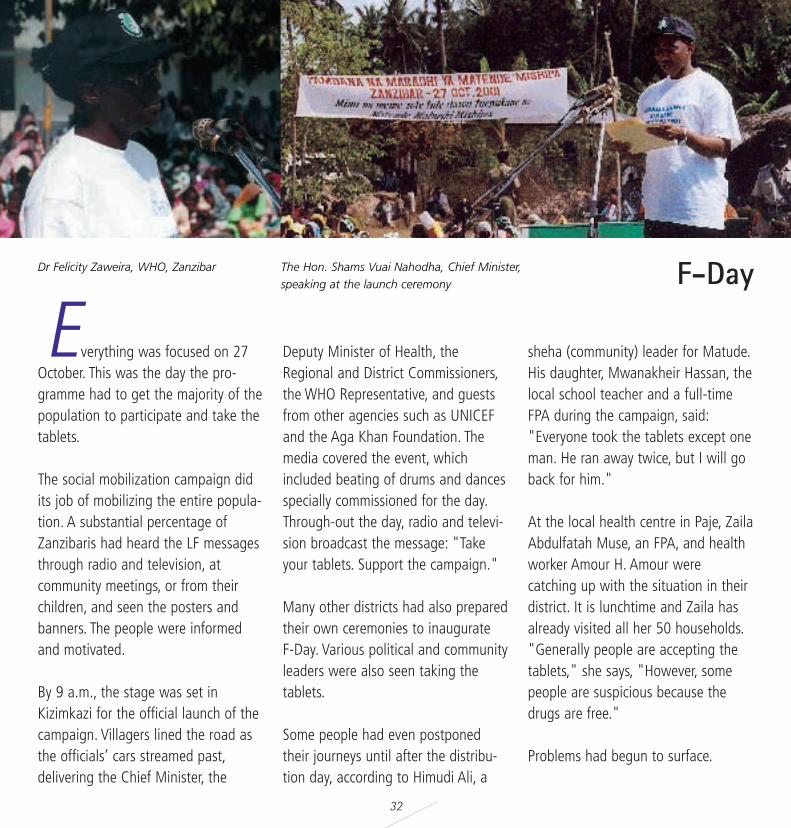
By 9 a.m., the stage was set inKizimkazi for the official launch of thecampaign. Villagers lined the road asthe officials’ cars streamed past,delivering the Chief Minister, the
Deputy Minister of Health, theRegional and District Commissioners,the WHO Representative, and guestsfrom other agencies such as UNICEFand the Aga Khan Foundation. Themedia covered the event, which included beating of drums and dancesspecially commissioned for the day.Through-out the day, radio and televi-sion broadcast the message: "Takeyour tablets. Support the campaign."
Many other districts had also preparedtheir own ceremonies to inaugurate F-Day. Various political and communityleaders were also seen taking thetablets.
Some people had even postponedtheir journeys until after the distribu-tion day, according to Himudi Ali, a
sheha (community) leader for Matude.His daughter, Mwanakheir Hassan, thelocal school teacher and a full-timeFPA during the campaign, said:"Everyone took the tablets except oneman. He ran away twice, but I will goback for him."
At the local health centre in Paje, ZailaAbdulfatah Muse, an FPA, and healthworker Amour H. Amour were catching up with the situation in theirdistrict. It is lunchtime and Zaila hasalready visited all her 50 households."Generally people are accepting thetablets," she says, "However, somepeople are suspicious because thedrugs are free."
Problems had begun to surface.
F-Day
EThe Hon. Shams Vuai Nahodha, Chief Minister, speaking at the launch ceremony
Dr Felicity Zaweira, WHO, Zanzibar

33
"The main difficulties are that peopleare scattered," according to Amour,"There are people working in hotelsthat have not been registered at all."His solution was to quickly dispatchan FPA to register and distribute thedrugs to all workers in the hotels andrestaurants in the area. Also, seasonalfishermen who were registered in theirhome villages with their families, butwere working on the East coast andstaying in temporary accommodationalso had to be registered and giventheir tablets.
One woman had walked to her localhealth centre for the drugs becauseshe had been away from home in themorning. She had been visited twiceby her FPA and had also heard aboutthe programme through the radio and
television. Some of her family andfriends had accepted the programme,but others were reluctant.
By late afternoon, one sheha afteranother, in urban and peri-urban dis-tricts, were reporting that they hadrun out of drugs. The FPAs were sittingunder trees with no drugs to deliver.People were flocking to the healthcentres and sheha headquarters andleaving empty-handed. This was thesituation in the urban and peri-urbanareas of Unguja.
"The registration did not tally with therequired amount of drugs," saidShambani Mwiny Mzee, the leader ofSheha Fuani. "There are still 2–3000people without tablets. We have alrea-dy run out of tablets to cover the
population." By early evening, theradio and television station beganbroadcasting news from the campaignofficials that F-Day was formally beingextended to the next day. Everyonewould get their tablets.
Later that evening, district supervisorsmet to figure out where there was anoversupply of drugs and how to getthose tablets to districts that hadexhausted their supply. Cars were dispatched to shehas and healthcentres to try and estimate the shortages. Khalfan Mohamed, theMOH Programme Manager, visited thechief pharmacist, who was at homehaving dinner with his family, to provide access to the medical storesthe next day.
The Deputy Minister of Health, Hon. Zainab Shamari
The Chief Minister The Regional Commissioner

34
Throughout the day, constant phonecalls were made between Khalfan andAli Rashid, the Coordinator in Pemba.There had been problems related tothe selection of FPAs. A substantialnumber were chosen from the rulingparty. However, these difficulties wereresolved by the public support fromthe opposition party.
The experience of Mzee Saleh Abdalla,an FPA from the island of Pemba,illustrates the concern. "People werenot ready," he told a WHO staff member months after the campaign."They were opposed to it. Because itwas free, they asked a lot of ques-tions. They thought that maybe therewas something behind it. They said,"We don’t need these drugs. Pleasedon’t come here. If it is somethingbeneficial to us, you would never bringit to us."
However, phone calls confirmed thatthe people of Pemba were participa-ting in the programme.
FPA in Bwaje on F-Day
35
arly on Sunday morning, a motorbike was buzzing through Zanzibar’sbiggest city, Stone Town, deliveringdrugs. The programme managers hadspent the night locating unusedtablets and planning ways to distribu-te them, including by motor bike inareas where the streets and alleyswere too narrow for cars.
Some people had refused to take thetablets the previous day. Their suspi-cions were aroused by two compo-nents of the programme: The drugswere free and they were delivered tothe home. On F-Day those suspicionshad kept this group of people whohad been offered the drugs fromactually taking them.
On Day Two, however, media reportsand personal accounts began reachingthe reluctant population with word that national and village leaders hadtaken the drugs. This was a practical
endorsement of the drug’s safety and value.
And something else started to hap-pen. Those who had been keeping thedrugs now swallowed them. Andthose who had rejected the drugswent searching for them. It was amass movement. Crowds surroundedthe homes of many FPAs and localcommunity leaders. They all wantedthe drugs.
As hoped, the people of Zanzibar hadmade a rational cost/value decision atsome point between day 1 and day 2.Zanzibar needed high coverage. Initialreports, based on the drug distribu-tors’ own registration, indicated thatthe majority of the eligible populationhad taken the drugs. An independent survey confirmed this number to havereached 76% of the total population.Zanzibar was on its way to elimina-ting LF.
One of the benefits of the treatment isthat it also destroys intestinal worms.In Pemba, some schoolchildrendischarged intestinal worms throughstools and vomiting. This validated thepotency of the drugs. Most important-ly, there were no severe adverse reac-tions that endangered anyone’s life.
The number of people with side-effects in some villages was quitehigh. In Kizimkazi Dimbani (Unguja), aplace highly endemic with the disease,136 people in a population of 248reported to the health clinic with side-effects. However, they had been pre-pared by the FPAs and the mild effectswere treated with paracetamol.
"Even now people are asking for thetablets," says Saada Ali, the nurse incharge of Kizimkazi Dimbani’s healthclinic. "This programme should conti-nue."
The Mop-Up Day
E
“Some people only registered themselves duringthe campaign. This has caused a problem
because the numbers of tablets given to us wasbased on the initial registers.”
Vuai Ali HajiSheha Leader
Keys to success
The nation’s sense of ownership motivated thousands of people. They were
making life better for themselves and their neighbours.
A massive health campaign, based on the COMBI principles and modified to meet cultural conditions, engaged with individuals,
families and communities.
Dedicated personal sellers, who visited every home to promote the programme, brought theCOMBI lessons into the home.
Involvement of every sector of influence, including district commissioners, religious leaders, widely respected teachers, and the entire public health staff, eventually generated confidence
in the campaign.
Political commitment and personal involvement of senior officials in the rulingand opposition parties also built confidence in the safety of
the drugs.
And most of all, dedication to making this campaigna success - no matter what the challenges
were - compelled people to work long,hard hours to improve the
health of everyone in Zanzibar.
36
37

38
ublic-private partnerships at glo-bal level have been promoted by WHO’sDirector- General, Dr Gro HarlemBrundtland, since the beginning of hermandate. Dr Brundtland is convincedthat a strong, broad-based partnershipbetween the private and public sector isone of the most efficient ways to increa-se and diversify additional investment inpublic health leading to sustainablehealth interventions. Influential donorshave come to adopt this view as well,and the number of partnerships keepsmultiplying.
In the context of communicablediseases, a number of global partner-ships are advocating political and publiccommitment to eliminate or eradicatetargeted infectious diseases, by givingto the poorest in the world greateraccess to affordable and effective treat-ments. They also pool research experti-se, raise financial resources, and supportgovernments to acquire new tools andstrategies against communicablediseases.
Today, partnerships that include civilsociety, NGOs, academic and researchinstitutions, governments, UN agencies,private businesses and philanthropistsare among the most widely used meansto achieve sustainable health outcomes.
The Global Alliance to EliminateLymphatic Filariasis has a strong globalcommitment, a major component beinga private–public partnership where twopharmaceutical companies have committed themselves to providing substantial drug donations to LF endemic countries. The goal is to elimi-nate the disease within a specific andlimited timeframe.
owever, the resources and expertise of global partnerships must betranslated into local benefits andactions to have any impact, and thechallenge is how to translate globalpromises into local realities.
Criticisms of partnerships have beenthat, in most developing countries,
public health systems are poorly equip-ped to provide even the most basichealth services to meet the main healthneeds of the population. Global partner-ships are therefore entering an arena ofunder-financed health services, withpoor surveillance and reporting systems.Furthermore, economic factors such asdebt burdens, and adjustment policiesalso contribute to a fragile health infra-structure. The result is a failure of sus-tainability. Why? Because, critics argue,programmes are dependent upon exter-nal drug donations, and scarce nationalhealth resources could be diverted fromestablished priorities and lead to thecreation of phantom health agendas.The critics also say that partnershipsoften generate vertical programmes,which do nothing to enhance a nation’sexisting public health infrastructure.
These are legitimate concerns as thebiggest challenge facing many govern-ments in developing countries is to findnew solutions and strategies to improvethe nation’s health, against the ons-laught of infectious diseases and abackground of dwindling resources.More effective use of nationalresources, the creation of local partner-ships based on sharing of resources andexpertise between private and public
Partnerships: Thinking global…
P
...and acting local
H
39
sectors, and the widespread inclusion ofcivil society are becoming increasinglyvital to address the needs for improvedand expanded health care. And thismeans introducing changes and diversi-fying at a pace appropriate to eachcountry's capacity, while planning longer-term improvements.
The challenge of the Global Alliance isnot only to provide resources, butequally to work alongside governmentsto facilitate and support the formationof self-supporting new partnerships andsynergies within countries. Based on theexperiences of the first year, the LF elimination programme in Zanzibar ispoised to make such progress based ona number of features, such as:
• LF was accepted as a national healthpriority when the Zanzibar governmentcreated a special unit to deal with thedisease in 1995. Since then, the govern-ment has undertaken several activitiesto control the disease. The LF elimina-tion programme is being deliveredthrough the existing health structure,and an important part of the strategywill be the inclusion of activities addres-sing the prevention and alleviation ofmorbidity related to LF infection, as wellas the rehabilitation of those who alrea-
dy have the disease. Morbidity preven-tion, control and rehabilitation will bedeveloped with communities and delive-red through active participation of thepatients, households, and the existinglocal health systems.
• LF has long been high on Zanzibar'spublic health agenda and been debatedmany times in its House ofRepresentatives. When the opportunityarose to eliminate LF, a calculated deci-sion was made by Zanzibar's publichealth officials. Moreover, the majorityof the programme was paid for bydonor grants, and WHO provided itstechnical experts without cost so thatnational health resources were notdiverted. The LF programme is alsostrengthening integration with otherservices, for example, the intestinalparasite control programme and themalaria control programme.
• While the claim on Zanzibar’sresources was comparatively small, itwas still a significant contribution forZanzibar. Through the FPAs more LF suf-ferers have been identified and thesepeople can now be helped. The elimina-tion of LF from Zanzibar could have far-reaching economic implications, giventhe perceived link between the disease
and poverty. Although no research existson the economic benefits of the LF programme in Zanzibar, India claimsthat LF costs the economy $1 billion ayear.
Vital to the success of the programmewas the strong and committed leader-ship of the government and civil service,the dedication of health workers, tea-chers, and young people, as well as theownership of the programme by localcommunities. A strong foundation hasbeen laid in Zanzibar which can be fur-ther enhanced by attracting and tappinginto local resources, talent and experti-se, and through creating meaningfulpartnerships with other stakeholders,private businesses, individuals andsocial groups.
The personal and collective responsibili-ty and ownership shown by the peopleof Zanzibar in the first year of the programme has to be maintained andextended for the next four years. If thishappens, and there is no reason why itshould not, LF should be eliminatedfrom Zanzibar in five years, leavingbehind a legacy of an enhanced healthsystem capable of delivering other health interventions through mass campaigns.
The future
Everyone is excited about the results of the 2001 campaign, and modifications arebeing made to make the 2002 campaign even better. A total observed coverage rate of76% of the entire population is an excellent achievement and there are also partner-ships being forged with other programmes.
Much of the success of the 2001 LF campaign in Zanzibar was due to personal commitment. But health workers in Zanzibar have experienced two very different broadpublic health initiatives and they know that commitments can change.
In the first, an international campaign supported by WHO and UNICEF began focusingprimarily on reducing the mosquito population. The programme had spectacular results.Within ten years, malaria rates had plummeted to 7.6% and 1.7% in the two majorislands. However, in 1968, the malaria programme stopped most of its activities andthe disease quickly rebounded. Today, the rates are high, making malaria one of themajor public health problems in Zanzibar.
Secondly, government commitment to the schistosomiasis and soil-transmitted helminth control programme has yielded benefits for a generation of children who arenow adults leading active and productive lives. The programme, which began in 1986,with strong collaboration between the Ministry of Health and Ministry of Education,regularly carries out deworming of schoolchildren. The effect has been a reduction inthe intensity of infection, improvement in nutritional uptake, and a positive impact.Children are learning better and growing better. As a result, this programme has laid a solid foundation for sustaining health interventions and has changed people’s perceptions namely, a disease without outward signs of illness can be treated.
40
However, people in Zanzibar who have worked in these and other large public health campaigns in the past know that one outstandingyear does not ensure continuing success.
Success will only be achieved if commitment is maintained at thepolitical and community level and through the continuedsupport of the Global Alliance Partnership.
"We don’t want the malaria experience to comeback," says one experienced health worker."We are afraid of that. If we stop theprogramme, the vectors are there (tocontinue spreading the disease).People fear that this (commitment)will not be sustained."
Zanzibar has completed one year of the campaign and faces four moreyears. The present high coverage rate has to be maintained. To achieve that, an all-out effort will berequired by all the players year after year.
Then and only then can the LF campaign in Zanzibarbe declared a success.
United Republic of Tanzania
42
43
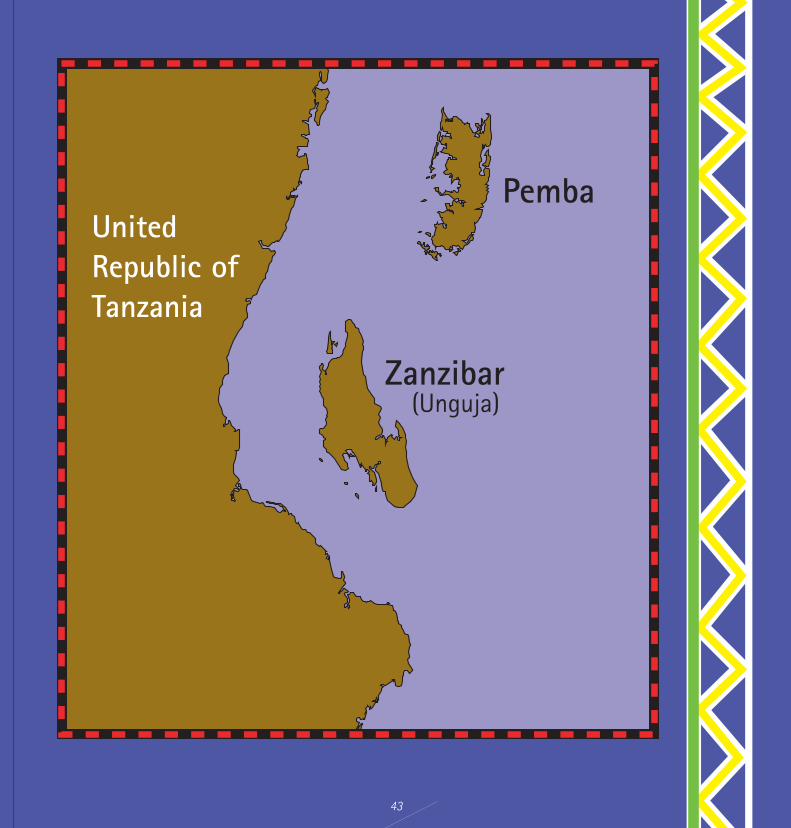
Zanzibar
Pemba
(Unguja)
UnitedRepublic ofTanzania
44
CCM Chama Chama Mapinduzi (The Revolutionary Party)
CUF Civic United Front
COMBI Communication for Behavioural Impact
FPA(s) Filaria Prevention Assistant(s)
LF Lymphatic filariasis
MDA Mass Drug Administration
MOH Ministry of Health
WHO World Health Organization
ABBREVIATIONS

Project Manager: Ms Asiya Odugleh
Writer: Mr Dick Thompson
Additional Writing Contribution: Ms Asiya Odugleh
Editorial contributions: Dr Claudio Beltramello, Dr Everold Hosein, Dr Elil Renganathan, Dr Francesco Rio, Dr Nevio Zagaria
Technical input: Dr Claudio Beltramello, Dr Gautam Biswas, Dr Francesco Rio, Dr Nevio Zagaria
Designer: Ms Isabelle Goudal
Photographs: Dr Marco Albonico, Dr Claudio Beltramello, C. Dieutete, Liverpool School of Tropical Medicine, Ms Asiya Odugleh, Dr Eric Ottesen, Mr Dick Thompson
Printed in France
WORLD HEALTH ORGANISATION
20, AVENUE APPIA, CH - 1211 GENEVA, SWITZERLAND
Tel.: +41 22.791.21.11WEBSITE: http://www.who.int
THE GLOBAL ALLIANCE TO ELIMINATE LYMPHATIC FILARIASISWEBSITE: http://www.filariasis.org