-
QueenslandCentre for MentalHealthResearch
The global burden of ADHD &
a meta-analysis of long-term outcomes
Dr Holly ErskineThe University of Queensland Centre for Clinical
Research;School of Public Health, The University of
Queensland;Queensland Centre for Mental Health Research;Institute
for Health Metrics and Evaluation, University of Washington
-
Introduction
Disclosures: Dr Erskine has previously received an honorarium
from Shire
-
The Global Burden of Disease Study (GBD)
The Global Burden of Disease Study (GBD) quantifies health loss
from hundreds of diseases, injuries, and risk factors, so that
health systems
can be improved and disparities can be eliminated.
-
History of measuring burden of disease
• A common unit of measurement is required
for comparison of disease burden between
diseases, countries, age groups, sex, years, etc.
• Historically, the most common unit of
measurement for burden was mortality.
• However, it is important to consider both
mortality and morbidity when measuring
burden.
-
Measuring burden of disease
Years of life lost due to premature mortality (YLLs)YLLs =
number of deaths x life expectancy at age of death
Years lived with disability (YLDs)YLDs = prevalent cases x
disability weight
YLLs + YLDs =Disability-adjusted life years (DALYs)
-
History of GBD• GBD 1990 (Murray & Lopez, 1996)
– 107 diseases and injuries, 8 regions, 5 age groups, 1 time
point
• GBD 2000-2004 (WHO collaboration)– 136 diseases and injuries,
14 regions, 4 time points
• GBD 2010 (led by IHME)– 296 diseases and injuries, 187
countries, (21 regions and 7 super-regions), 20
age groups, 5 time points
• GBD 2013 (led by IHME)– 306 diseases and injuries, 188
countries + subnational estimates for 3 countries
(21 regions and 7 super-regions), 20 age groups, 6 time
points
• GBD 2015 (led by IHME)– 315 diseases and injuries, 195
countries + subnational estimates for 11 countries
(21 regions and 7 super-regions), 20 age groups, 6 time
points
• GBD 2016 (led by IHME)– 333 diseases and injuries, 195
countries + subnational estimates for 12 countries
(21 regions and 7 super-regions), 20 age groups, every year from
1990 onwards
-
ADHD in GBD
• Not included until GBD 2010
• Estimate burden across the lifespan
• Only non-clinical epidemiological data
is accepted
• Data scarcity in older ages, for LMICs,
and for non-prevalence parameters
• No YLLs, only YLDs
-
Prevalence of ADHD in ages 5-14 years, 2016
-
Prevalence of ADHD in Australia by age, 2016
-
Prevalence in Australia, 5-14 years, 1990-2016
-
DALYs in Australia, ages 5-14 years, 2016
-
Rate of DALYs over time, 5-14 years
-
DALY rankings, 5-14 years, 2016
-
Implications of GBD
• Recognition of ADHD in the
global health/mental health fields
• Vital information for countries
with young populations
• Potential support ratio –
importance of healthy young
people
-
Limitations of GBD
• Data scarcity
• Low disability weight for ADHD
• No YLLs – does not mean no increased
risk of mortality
• Disability only considered in terms of
‘current within-the-skin health loss’
– No future burden
– No impact on other areas e.g.
academics, employment
– No burden on families, carers, schools,
etc
5.5%
-
Potential adverse outcomes of ADHD
-
Findings
• 101 studies across North America,
Western Europe, and the Asia Pacific
• Sample sizes ranged from 71 to almost
2 million participants
• Years of follow up ranged from 2-40 yrs
• Attrition ranged from 60% to 0%
• Number of outcomes able to be meta-
analysed = 52
• Number of significant odds ratios (ORs)
= 37
-
Substance use disorders
Long-term outcome Odds ratio 95% CIs No. of data points
Substance use disorder 1.73 1.24-2.41 13
Illicit drug use 2.24 1.43-3.52 8
Illicit drug use disorder 2.57 2.06-3.20 6
Cannabis use 1.67 1.23-2.26 14
Cannabis use disorder 2.51 0.67-9.30 5
Alcohol use 1.00 0.70-1.44 7
Alcohol dependence 1.39 1.06-1.83 8
Regular smoking 2.16 1.77-2.63 13
Tobacco dependence 2.41 1.67-3.48 8
-
Mental disorders and suicide
Long-term outcome Odds ratio 95% CIs No. of data points
ODD 7.05 2.63-18.85 6
CD 5.40 2.53-11.55 8
ASPD 3.17 1.98-5.08 8
Bipolar disorder 7.09 2.03-24.75 4
Depression 2.31 1.45-3.70 13
Anxiety disorders 1.48 0.89-2.46 9
Panic disorder 2.47 1.10-5.53 4
Suicide attempts 2.48 1.63-3.77 7
-
Academics and employment
Long-term outcome Odds ratio 95% CIs No. of data points
Failure to complete high school
3.70 1.96-6.99 11
Grade retention 3.64 2.39-5.56 9
Suspension 6.31 2.53-15.73 5
Expulsion 3.19 2.15-4.74 4
No tertiary education 6.47 4.58-9.14 9
Fired 3.92 2.68-5.74 4
Unemployment 1.97 1.01-3.85 4
-
Criminality
Long-term outcome Odds ratio 95% CIs No. of data points
Criminal acts 1.81 0.94-3.50 7
Arrest 2.43 1.62-3.65 10
Drug-related arrest 1.69 0.75-3.77 4
Violence-related arrest 3.63 2.31-5.70 5
Convictions 2.01 1.25-3.24 6
Incarceration 2.53 1.38-4.63 4
-
Other outcomes
Long-term outcome Odds ratio 95% CIs No. of data points
Early pregnancy (< 23 years) 2.77 0.67-11.37 5
Vehicular accidents 1.15 0.67-1.99 6
At-fault vehicular accidents 1.98 1.03-3.81 4
Vehicular accidents with injury 2.75 1.47-5.15 4
Driving citations 2.13 1.09-4.19 5
DUI driving citations 1.60 1.00-2.57 5
License revoked/suspended 1.95 1.30-2.92 5
Service use – education 6.37 2.58-15.73 8
Service use – mental health 2.35 1.42-3.89 9
-
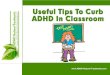
Impact of diagnosis vs symptoms: SUDs
OR1086420
Study
Reef, 2010
Fischer, 2002
Overall
Q=5.13, p=0.16, I2=42%
Fergusson, 2007
Sourander, 2007
OR (95% CI) % Weight
0.70 ( 0.30, 1.30) 25.6
1.04 ( 0.59, 1.84) 33.4
1.23 ( 0.76, 2.00) 100.0
1.84 ( 0.95, 3.55) 28.8
2.40 ( 0.70, 8.30) 12.3
OR1086420
Study
Monuteaux, 2007 Copeland, 2009
Biederman, 2008
Mannuzza, 1993
Overall Q=18.15, p=0.02, I2=56%
DeSanctis, 2014
Mannuzza, 1998
Biederman, 1999
Milberger, 1997b
Gau, 2007
OR (95% CI) % Weight
0.70 ( 0.25, 1.99) 8.4 1.00 ( 0.20, 4.50) 4.8
1.20 ( 0.70, 2.07) 15.0
1.48 ( 0.66, 3.32) 11.0
2.02 ( 1.37, 2.98) 100.0
2.12 ( 1.15, 3.92) 13.8
2.19 ( 0.85, 5.65) 9.3
2.67 ( 1.41, 5.05) 13.4
3.75 ( 1.74, 8.07) 11.6
4.79 ( 2.41, 9.51) 12.7
Symptom scales Diagnostic instruments
1.23 (0.76-2.00) 2.02 (1.37-2.96)
-
Limitations & Implications
Limitations
• Insufficient data for some outcomes
• Varying quality of the studies
• Control for confounding factors
Implications
• Many health outcomes are serious and persistent
• Not a ‘self-fulfilling prophecy’
• Importance of appropriate treatment at the appropriate
time
• Significant potential benefits of prevention
The global burden of ADHD &�a meta-analysis of long-term
outcomes�IntroductionThe Global Burden of Disease Study
(GBD)History of measuring burden of diseaseMeasuring burden of
diseaseHistory of GBDADHD in GBDPrevalence of ADHD in ages 5-14
years, 2016Prevalence of ADHD in Australia by age, 2016Prevalence
in Australia, 5-14 years, 1990-2016DALYs in Australia, ages 5-14
years, 2016Rate of DALYs over time, 5-14 yearsDALY rankings, 5-14
years, 2016Implications of GBDLimitations of GBDPotential adverse
outcomes of ADHDFindingsSubstance use disordersMental disorders and
suicideAcademics and employmentCriminalityOther outcomesImpact of
diagnosis vs symptoms: SUDsLimitations & Implications