Embed Size (px)
Citation preview
The successful completion of theHuman Genome Project onApril 14, 2003, marked the endof scientists’ monumental effortto sequence the three billion
DNA “letters” in the human geneticblueprint. However, for the millions ofpeople suffering from mental illness, April14, 2003, represents more of abeginning—the dawning of the genomeera in medicine.
Just as an architectural blueprint makesit easier for engineers to analyze problemsand make repairs to a building, the humangenetic blueprint will speed researchers’efforts to understand the biologicalpathways involved in mental illness and todevelop better methods of diagnosis andtreatment. Until recently, scientistsstudying mental illness have concentratedon a few hundred genes, mainly those thatencode neurotransmitters and theirreceptors. However, that focus is nowexpanding, due in part to a recent analysisof the mouse genome sequence that foundthat an amazing number of genes—nearly16,500—are active in the mammalianbrain.
Already, the genome era is generatingnew discoveries. Mapping and sequencingdata from the Human Genome Projecthave accelerated the identification ofgenes involved in relatively rare, single-gene disorders, some of which areproviding new insights into more commonconditions. The bad news, however, is thatthere are no single-gene models for themost common forms of mental illness.Instead, most mental illnesses fall into thecategory of complex genetic disorders,which includes many other commondiseases such as cancer, diabetes, andheart disease. The risk of developing theseconditions is thought to be influenced by amix of factors that may include one ormore genes, lifestyle factors, andenvironmental factors ranging from viralinfections to stress.
To identify the genetic roots of complex
disorders, the National Human GenomeResearch Institute recently tapped into thepower of genome data and technology tolaunch the International HapMap Project.During the next several years, aninternational consortium plans to build a
catalogue of human genetic variations anddetermine how these variations areorganized into neighborhoods, orhaplotypes, along the humanchromosomes. This map will serve as atool for researchers trying to discover thecommon genetic variations associatedwith complex diseases, as well asvariations responsible for differences indrug response.
Even with this map, piecing together thecomplicated genetic puzzle of all mentalillnesses will likely take many years.Scientists, however, have already begun touncover genetic clues to some of the morecommon conditions, including
schizophrenia, depression, bipolardisorder, and panic disorder. For example,in the past year alone, two teams studyinglarge populations in Iceland and Scotlandhave linked increased risk ofschizophrenia to a certain variant of agene that carries the instructions forneuregulin 1, a protein involved in braindevelopment.
Of course, it is not enough to discover
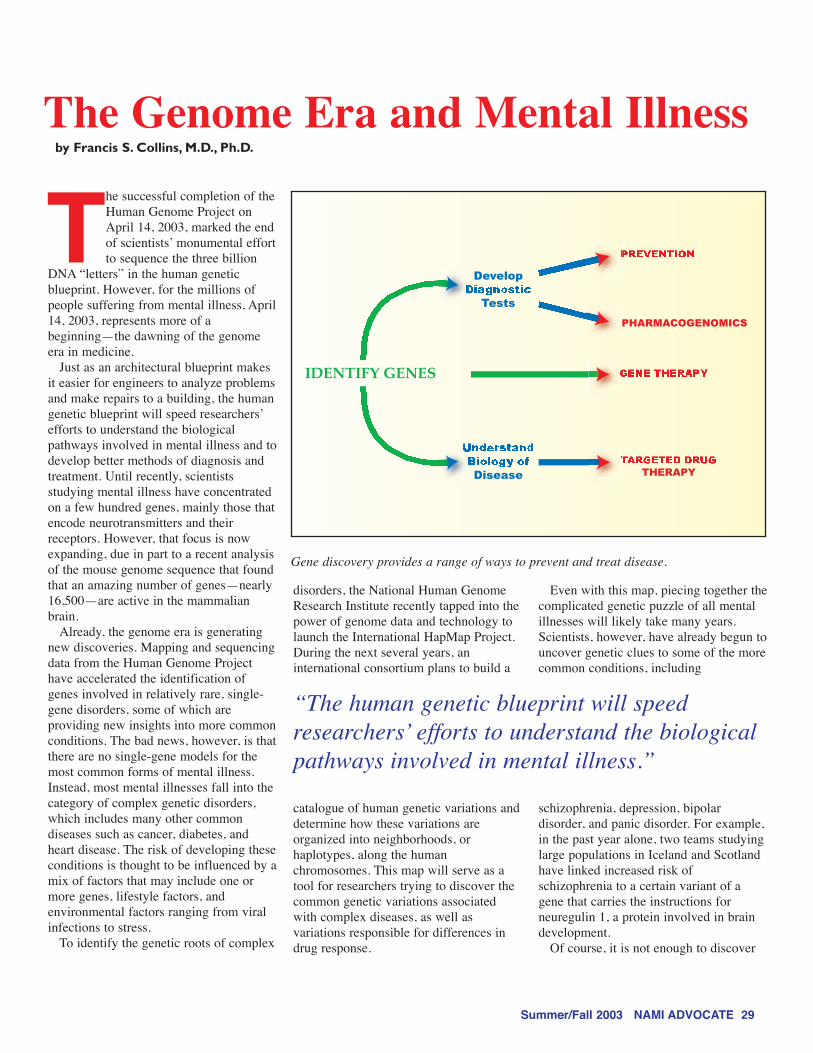
IDENTIFY GENES
Develop
Tests
Disease
PHARMACOGENOMICS
THERAPY
Gene discovery provides a range of ways to prevent and treat disease.
“The human genetic blueprint will speedresearchers’ efforts to understand the biologicalpathways involved in mental illness.”
The Genome Era and Mental Illnessby Francis S. Collins, M.D., Ph.D.
Summer/Fall 2003 NAMI ADVOCATE 29

the genes involved in mental illness—ournewfound understanding must be movedinto the clinic, where it can benefit peoplestruggling with these conditions. Theidentification of a gene or set of genesinvolved in disease represents just the firststep in what may be a long road towardbetter diagnostic tests, drug therapies, andprevention strategies (see Figure 1).
For people affected by mental illness,some of the first benefits of the genomeera are likely to be in the way drugs areprescribed. Rather than the current trial-and-error method of figuring out whichmedications work best for a patient,doctors will be able to examine eachperson’s genomic information to predictwhich drug will be most effective andproduce the fewest side effects for thatindividual. Research in this rapidlyemerging field, called pharmacogenomics,has already identified genetic variationsthat influence responses to antipsychoticsand antidepressants. In the long run,genome-based research will play adominant role in the development of newdrugs for mental illnesses, enablingresearchers to design more powerful, yetless toxic, compounds targeted at specificbiological pathways.
Clearly, the genome era holdstremendous promise for improving theoutlook for all those whose lives havebeen shaken by mental illness. At thesame time, our society must take steps toensure that people are not discriminatedagainst based on their geneticpredisposition to mental illness or anyother medical condition. Congress is now
considering legislation that will outlawsuch discrimination in health insuranceand the workplace. With such protectionsfirmly in place, genomic research willhelp to ease the societal stigma manypeople still face by providing moreprecise methods of diagnosing mentalillness and by furnishing conclusiveevidence of the biological roots of suchconditions.
In the same way that antibioticsrevolutionized the treatment of infectiousdiseases in the 20th century, genomeresearch stands ready to revolutionize thetreatment of mental illness in the 21stcentury. But we in the biomedical researchcommunity cannot do this alone. We needthe support of all those who have foughtso hard over the years to raise awarenessof mental illness and help the millionsstruggling with these conditions. Workingtogether, we can build the bridge betweentoday’s dreams and tomorrow’s reality.
Additional ReadingW. M. Cowan, K.L. Kopkinsky, and S.E.Hyman, “The Human Genome Project andIts Impact on Psychiatry,” Annual Reviewof Neuroscience 2002, 25: 1–50.
T.R. Insel and F.S. Collins, “Psychiatry inthe Genomics Era,” The American Journalof Psychiatry, 160: 616–620, 2003.
Francis S. Collins, M.D., Ph.D., isDirector of the National Human GenomeResearch Institute (NHGRI) at theNational Institutes of Health. He overseesthe Human Genome Project, aninternational, multidisciplinary enterprisethat completed mapping of the humangenome sequence in April 2003. Buildingupon that success, Dr. Collins is leadingNHGRI’s effort to use genomic knowledgeto improve human health. His lab iscurrently searching for genes thatcontribute to type II diabetes. Dr. Collins’previous research led to the identificationof genes responsible for progeria, cysticfibrosis, neurofibromatosis, andHuntington’s disease.
Francis S. Collins, M.D., Ph.D.
30 NAMI ADVOCATE Summer/Fall 2003