Embed Size (px)
Citation preview

The Future of IV Preparation:
Why technology matters
Jerry Fahrni, Pharm.D.

Disclaimer
I am a consultant, and have provided services to companies in the pharmacy automation and technology space. I am speaking today in my individual capacity. The views and opinions presented here are entirely my own.


PHARMACY IS SIMPLE!

The 5 Rights of Medication Administration:
1. Patient 2. Drug 3. Dose 4. Route 5. Time
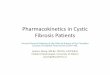
Medication Use Process Where Adverse Drug Events (ADEs) and Error Occur
Adopted from: Claussen. (2013) HIT and CPOE Simulator Update. Bates et al., JAMA 1995; Leape et al., JAMA 1995; Classen et al., JAMA 1997
Diagnostic/Therapeutic Decisions
Made
Medication Ordered
Order verified and submitted
Formulary, purchasing decisions
Inventory management
Evaluate order
Select medication
Prepare medication
Dispense/ distribute
medication
Intervene as indicated for
adverse reaction/
error
Assess and document
patient response to
med according to parameters
Document admin and associated
information
Administer according to
order and standards for
drug
Select the correct drug for correct
patient
Educate patient
regarding medication
Educate staff regarding
medications
Ordering
Medication Inventory Management
Pharmacy Management
Administration Management
Monitor/Evaluate Response Document Administer Medication Education
ADEs = 49% Prescribing Errors = 39%
ADEs = 11% Transcription Errors = 12%
ADEs = 14% Dispensing Errors = 11%
ADEs = 26% Admin Errors = 38%

Traditional Storage IV Room
Refrigerated Storage Controlled Storage

0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
The scope of this problem is daunting since an estimated 90% of hospitalized patients receive medication via the IV route
“
Husch, M, et al., Quality & Safety in Health Care. 2005; 14:80-86.
”

Risk associated with Injectable Medications
1. Barker KN, et al. Arch Intern Med. 2002;162:1897-1903.
Highest risk for error and most severe harm1
High degree of complexity
High-risk / high-alert
High-risk routes of administration
High-risk populations
1
2
3
4
5

Errors Associated with CSPs
Flynn EA et al. American Journal of Health-System Pharmacy. 1997; 54 (8):904-912 Bateman R et al. Qual Saf Health Care. 2010; 19:1-6
Wrong dose most common error found
9% mean compounding error rate
2% were clinically relevant
25% may have mild to catastrophic impact on patients
CSPs = compounded sterile products

Bateman R et al. Quality and Safety in Health Care. 2010; 19:e29

Image Source: Jerry Fahrni 2017©

Bateman R et al. Quality and Safety in Health Care. 2010; 19:e29

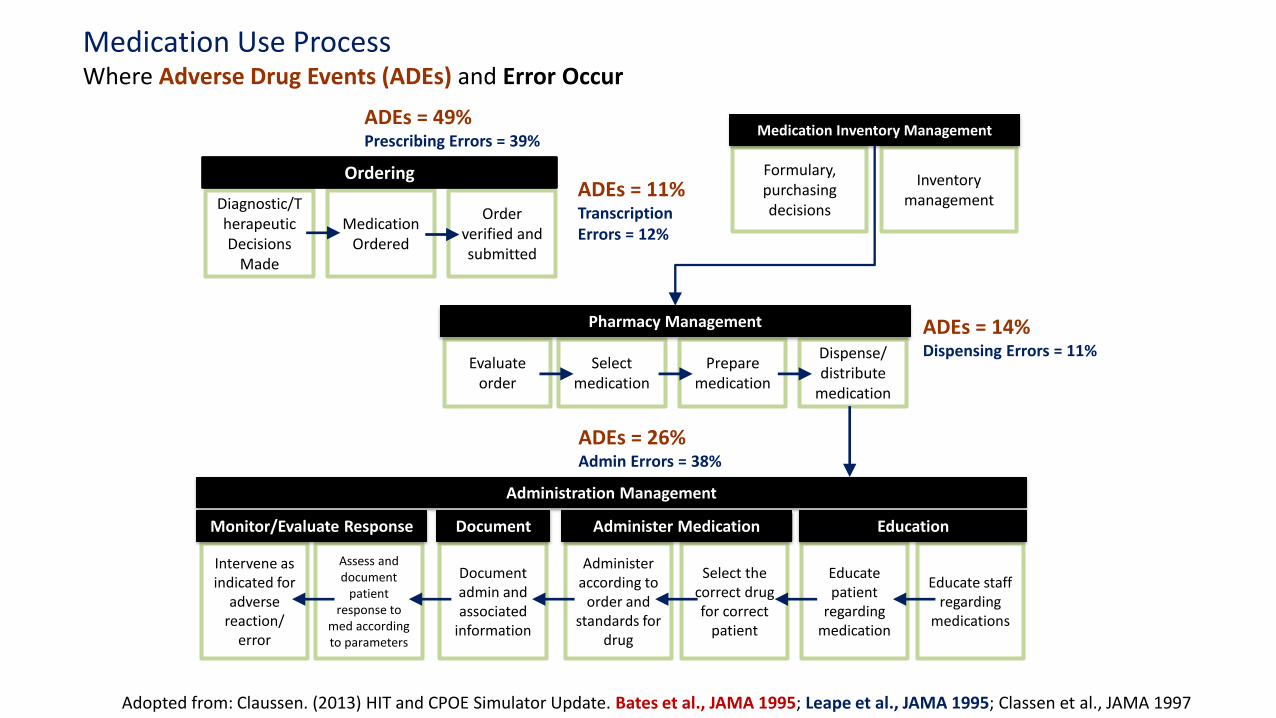
Deng, Y. et al. Am J Health-Syst Pharm. 2016; 73:887-93.
Deng Y et al. Am J Health-Syst Pharm. 2016; 73:887-93.

Sacks, GS. et al. Pharmacotherapy. 2009;29(8): 966–74.

Parshuram CS, et al. CMAJ. 2008; 178:42-48

Profession Total 118 participants
Anesthesia 20
Pharmacy 17
Nursing 81
Years of professional experience
< 5 39
6-10 41
> 10 38
Infusion prepared in previous week
0 27
1-5 50
6-10 23
> 10 18
Adopted from Table 2 in Parshuram CS, Y. et al. CMAJ. 2008; 178:42-48

Overall, 34.7% of the morphine infusions had errors

Parshuram CS, Y. et al. CMAJ. 2008; 178:42-48

3 factors
associated with error of
> 10%
Fewer infusions prepared in the previous week
Increased number of years professional experience
Profession
Parshuram CS, Y. et al. CMAJ. 2008; 178:42-48

Parshuram CS, Y. et al. CMAJ. 2008; 178:42-48
Our findings challenge the dogma that expertise is synonymous with seniority, and they highlight the distinction between recent practice and cumulative experience.
“
”

4 deaths after exposure to
cardioplegia soln from compounding
pharmacy
2 patients blinded by contaminated
injection from compounding
pharmacy
Death from decimal error in
compounding in a hospital pharmacy
3 deaths from injection made by
compounding pharmacy
9 deaths resulted from contaminated parenteral nutrition
NECC produced and distributed 3 lots of PF
methylprednisolone acetate injection
Death from overly concentrated
injection used in hospital pharmacy
33 fungal eye infections – some with loss of vision –
resulting from contaminated preparations
made by compounding pharmacy
2005 2006 2007 2011 2012
Myers CE. AJHP. 2013;70(16): 1414-1427
2014
St. Charles Hospital in Bend, OR dispenses
rocuronium instead of fosphenytoin. Patient
receives dose and dies.

medication errors have a tremendous impact on
the entire healthcare system
PATIENT CAREGIVER FINANCIAL

PATIENT CAREGIVER FINANCIAL
Preventable ADEs from injectable medications were estimated to occur in 1.2 million inpatient hospitalizations annually in the United States
Example: Eric Cropp. Involved in a compounding error that took the life of 2 year old Emily Jerry 2006. Lost job, lost license, received a fine, and was ultimately sentenced to prison.
According to data from Bates 1997 study, cost can add more than $5000 to the cost of a hospital stay Estimated inpatient preventable ADEs associated with injectable medications increase the annual US payer costs by $2.7 - $5.1 billion

Why?
Image credit: Heather Katsoulis [CC BY-SA 2.0 (http://creativecommons.org/licenses/by-sa/2.0)], via Wikimedia Commons

Image Source: Jerry Fahrni 2014©
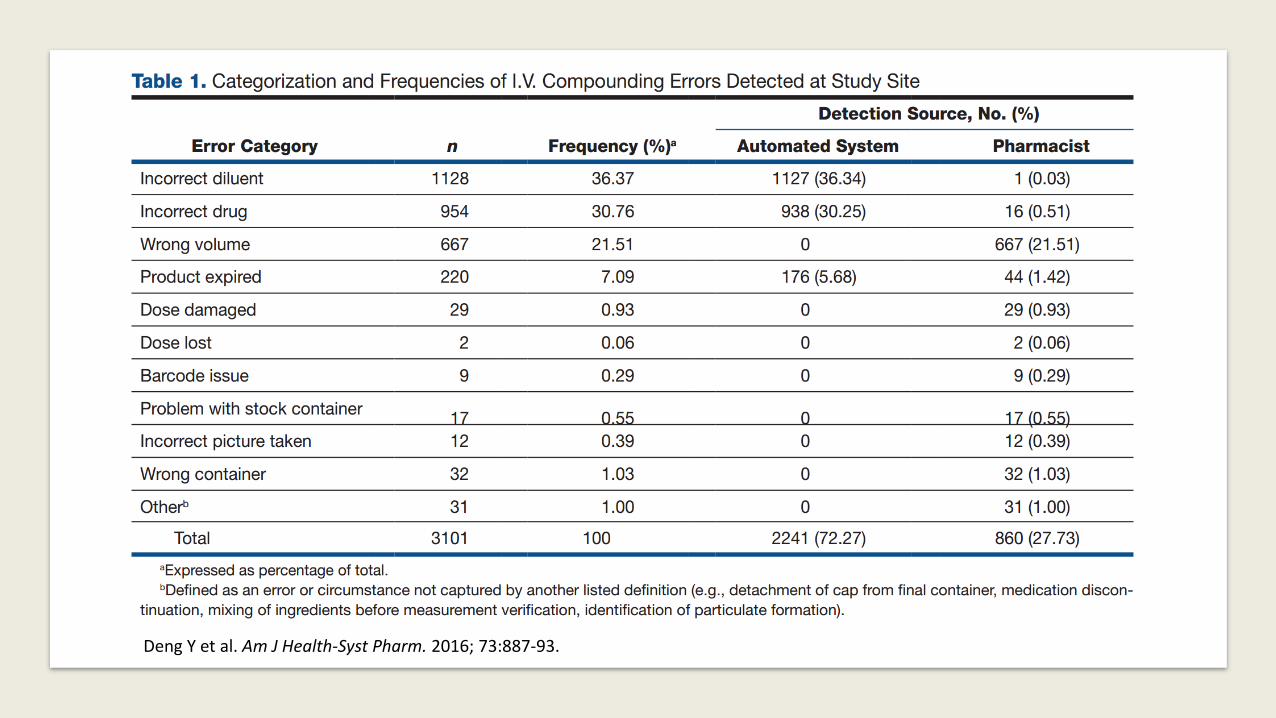
Basic Tenets of Human Error …......................................................................................................................
Anatomy of an Error. Patient Safety – Quality Improvement. Available at: http://patientsafetyed.duhs.duke.edu/module_e/basic_tenets.html. Accessed March 11, 2017.
Everyone commits errors
Human error is generally the result of circumstances beyond the control of those committing the errors
Systems or processes that depend on perfect human performance are inherently flawed
Classification of Errors
Skill-based errors – slips and lapses
Knowledge-based mistakes
Rule-based mistakes
“strong but wrong”
Reason James (1990). Human error. Cambridge University Press (New York, USA), 1990. ISBN: 9780521314190.

TWO STEPS TO TAKE RIGHT NOW TO MINIMIZE RISK IN THE IV ROOM

Step 1
FOLLOW ESTABLISHED GUIDELINES AND REGULATIONS

1975 NCCLVP published
last recommendations
1998
FDAMA signed into law
1992
ASHP Technical
Assistance Bulletin
“Quality Assurance for
Pharmacy-Prepared
Products”
1997
FDA Modernization Act
1995
USP <1206> “Sterile
Drug Products for Home
Use”
2000
ASHP Guidelines on
Quality Assurance for
Pharmacy-Prepared
Sterile Products
2008
USP <797> revision
official June 1, 2008
2004
USP <797> becomes
official January 1
2001
Section 503A of FDAMA
declared unconstitutional
2006
Proposed Revisions to
USP <797> published
2010
ASHP Guidelines on
Outsourcing Sterile
Compounding Services
2013
Drug Quality and Security
Act (DQSA) becomes law
2014
FDA publishes 503A and
503B guidance
2016
USP publishes chapter
<800>
1970’s 1990’s 2000’s 2010’s


“Compounding personnel are responsible for ensuring that CSPs are accurately identified, measured, diluted, and mixed; and are correctly purified, sterilized, packaged, sealed, labeled, stored, dispensed, and distributed.”
United States Pharmacopeial Convention (USP). General chapter <797>: Pharmaceutical Compounding Sterile Preparations – Responsibility of Compounding Personnel

“The use of technologies, techniques, materials, and procedures other than those described in this chapter is not prohibited so long as they have been proven to be equivalent or superior with statistical significance to those described herein.”
United States Pharmacopeial Convention (USP). General chapter <797>: Pharmaceutical Compounding Sterile Preparations

“All compounding personnel…are
responsible for compounding and dispensing sterile products of correct ingredient identity, purity, strength, and sterility and for dispensing them in appropriate containers, labeled accurately and appropriately for the end user.”
ASHP guidelines on quality assurance for pharmacy-prepared sterile products. Am J Health Syst Pharm. 2000 Jun 15;57(12):1150-69.
“Use technology to assist in
the verification process (e.g., barcode scanning verification of ingredients, gravimetric verification, robotics, IV workflow software) to augment the manual processes.”
ISMP 2016-2017 Targeted Medication Safety Best Practices for Hospitals

“Data submitted to the ISMP MERP has repeatedly shown that the manual inspection of IV admixture ingredients by pharmacy technicians and pharmacists is not a totally effective deterrent in preventing preparation and dispensing errors..”
ISMP 2016-2017 Targeted Medication Safety Best Practices for Hospitals

ISMP 2016-2017 Targeted Medication Safety Best Practices for Hospitals

Bottom line
There is nothing in the current USP General Chapters or other U.S. regulatory documentation that directly addresses the use of automation and
technology during the sterile compounding process or their use inside the hood.

Automated compounding device and balance
The automated compounding device (ACD) must be positioned in the C-PEC such that compounding occurs while critical sites are exposed to first air.
The ACD must be calibrated at least once a day, then as needed…
The balance must be calibrated before each use, after it is moved, after disinfecting and as needed…
The results of calibration must be documented
Model Standards for Pharmacy Compounding Sterile Preparations Approved by the NAPRA Board of Directors April 2015, published September 2016

Image Source: Jerry Fahrni 2016©

Camera and computer equipment
Audio-visual and computer equipment* used for verification during compounding is allowed in the clean room under certain conditions. Preference must be given to audiovisual and computer equipment that features “hands-free” operation and that is made of smooth, nonporous, cleanable materials with low particulate emission and resistance to damage from cleaning and disinfecting products.
Model Standards for Pharmacy Compounding Sterile Preparations Approved by the NAPRA Board of Directors April 2015, published September 2016 *camera, monitor, pedal system

Image Source: Jerry Fahrni 2017©
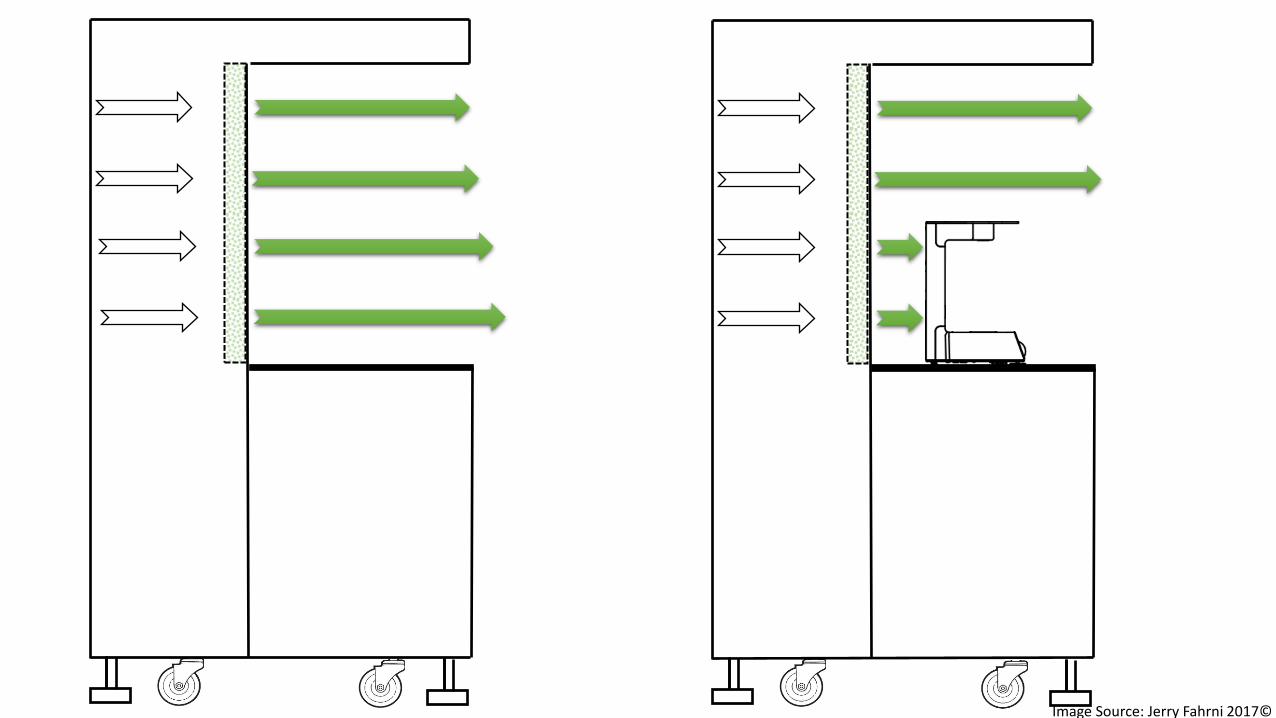
Image Source: Jerry Fahrni 2017©

Image Source: Jerry Fahrni 2014©

Step 2
IMPLEMENTATION OF AUTOMATION AND TECHNOLOGY IN THE IV ROOM

One of the advantages of technology is that it can enhance human performance to the extent that the human plus technology is more powerful than either is alone.
Institute of Medicine. (1999). To Err is Human: Building a Safer Health System.
“
”

Dose and volume verification Syringe pull-back method Human visual inspection
CSP ingredients and components Human visual inspection
Final CSP verification Calculation review
Reconciliation
Highly manual process
Dose and volume verification Gravimetrics
Computer vision
CSP ingredients and components Bar-code scanning Computer vision
Final CSP verification Computer vision
Gravimetrics Real-time concentration validation
Highly automated process (Robotics)
http://www.cgpgrey.com [CC BY 2.0 (http://creativecommons.org/licenses/by/2.0)], via Wikimedia Commons
http://www.cgpgrey.com [CC BY 2.0 (http://creativecommons.org/licenses/by/2.0)], via Wikimedia Commons
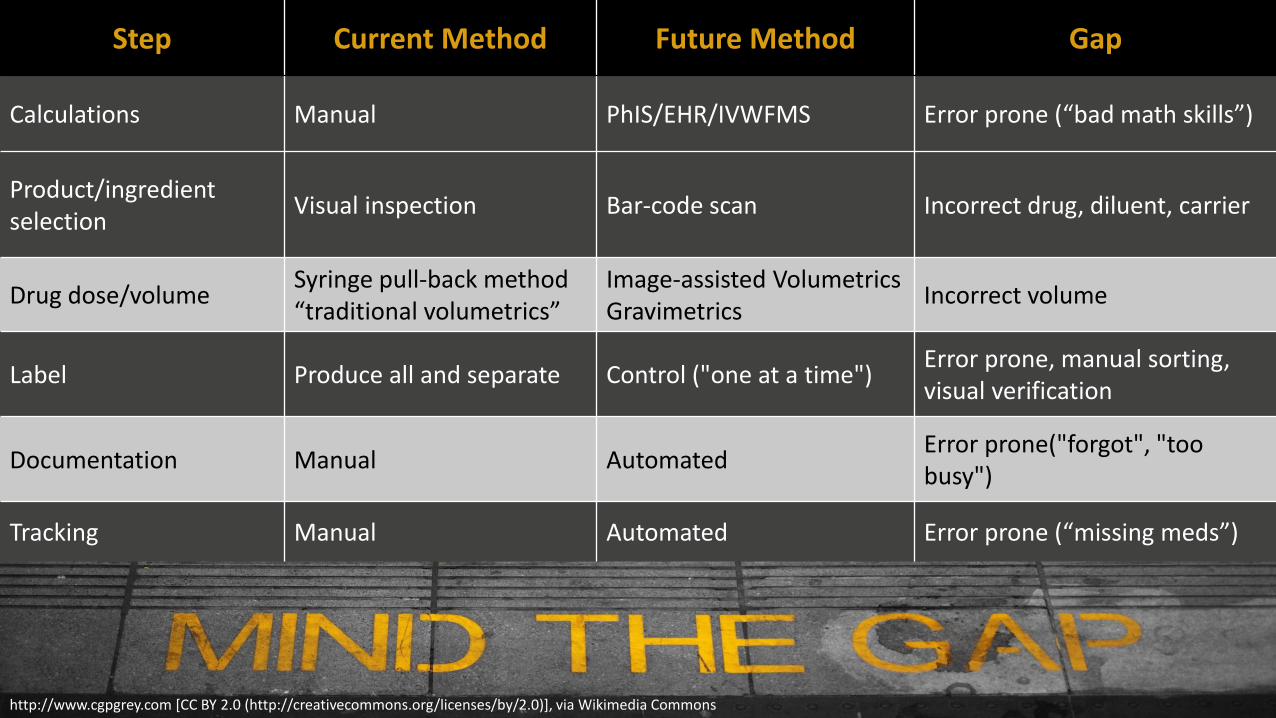
Step Current Method Future Method Gap
Calculations Manual PhIS/EHR/IVWFMS Error prone (“bad math skills”)
Product/ingredient selection
Visual inspection Bar-code scan Incorrect drug, diluent, carrier
Drug dose/volume Syringe pull-back method “traditional volumetrics”
Image-assisted Volumetrics Gravimetrics
Incorrect volume
Label Produce all and separate Control ("one at a time") Error prone, manual sorting, visual verification
Documentation Manual Automated Error prone("forgot", "too busy")
Tracking Manual Automated Error prone (“missing meds”)

Image source: Jerry Fahrni, Pharm.D. 2014 Image Source: Jerry Fahrni 2014©

Image Source: Jerry Fahrni 2016©

IVWFMS
9 Robotic
6 EHR
3

CSP-ASSITANCE TECHNOLOGY FEATURES
Interfaced to PhIS
Web-based UX/UI Remote Access /
Telepharmacy Workflow / Queue
Management
Assistive technologies (Bar-code scanning)
Gravimetrics
Reference and Compounding Aids
Recipe Catalogues ("Master Formulas")
Image Capture/Archive (Documentation)

forcing function
mechanisms built into the
workflow to prevent
specific errors or reduce
their impact
enforcing function
mechanisms built into the
workflow to warn users
when something is outside
safety parameters

Currently only bar-code scanning technology can positively identify an ingredient during the
compounding process.

ASHP Statement on Bar Code Technology
ASHP statement on bar code verification during inventory, preparation, and dispensing of medications. Am J Health‐Syst Pharm. 2011; 68:442‐5.
“The American Society of Health‐System Pharmacists encourages hospital and health‐system pharmacies to incorporate bar‐code scanning into inventory management, dose preparation and packaging, and dispensing of medications.”

ISMP Medication Safety Alert!
“Now is the time for hospital leadership to support the acquisition of IV workflow technologies that utilize barcode scanning of products during pharmacy IV admixture preparation. Systems … that utilize barcode scanning support can assure proper drug selection….”
ISMP. Tragic Error With Neuromuscular Blocker Should Prompt Risk Assessment By All Hospitals. ISMP Medication Safety Alert! 2014.

BAR CODE SCANNING
Galbraith W, et al. Int J Pharm Compd 2012;16 (3)

Targeted Dispensing Errors Pre- and Post-implementation of Preparation Barcode Scanning
PRE-BCAS POST-BCAS
Total Dosages Dispensed 413,085 558,229
Wrong Dosage 29 0
Wrong Drug 14 1
Wrong Volume 3 0
Wrong Procedure 3 0
Wrong Patient 2 0
Total Targeted Dispensing Errors 0.012% 0.002%
BCAS: barcode assistance system Table adopted from Galbraith W, et al. Int J Pharm Compd 16 (3): 253–256 (2012)

ENSURING THE RIGHT DOSE

VOLUMETRIC METHOD
DETERMINING DOSE BY VOLUME

ISO 7886-1 SYRINGE ACCURACY

1156 doses included in study
0.53% mean deviation
64.9% - 94.2% range
Poppe L et al. Journal of Oncology Pharmacy Practice. 2016
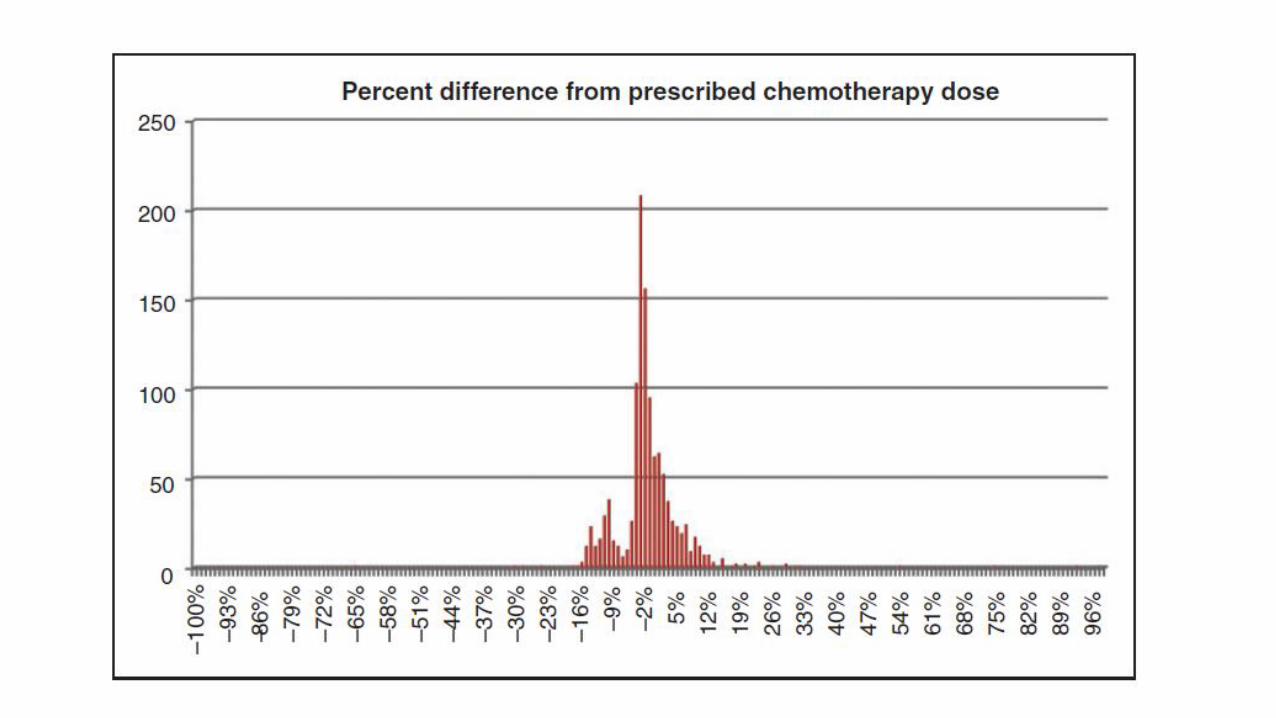

Table 3 – Poppe L, et al. Journal of Oncology Pharmacy Practice. 2016;22(1)
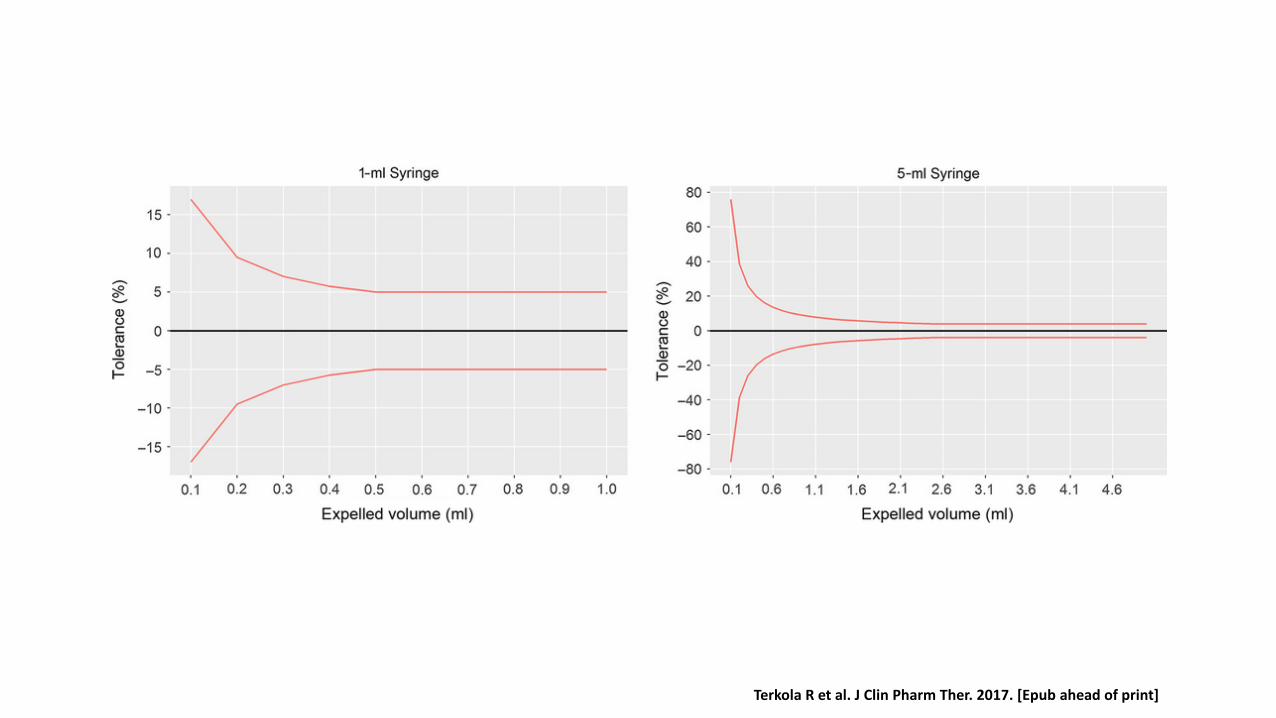
Terkola R et al. J Clin Pharm Ther. 2017. [Epub ahead of print]

GRAVIMETRIC METHOD
QUANTITATIVE ANALYSIS BY WEIGHT
Image Source: Jerry Fahrni 2014©

Reece K et al. AJHP. 2016;73(3)

Reece K et al. AJHP. 2016;73(3) Figure 2

Study period: Nov 2012 to Nov 2013
15,843 doses prepared
1,126 (7.1%) errors detected
292 (26%) detected by barcode scan
797 (71%) deviation and 37 (3%) vial reconstitution errors by gravimetric weighing
Technician production time ↓ by 34%
Pharmacist checking time ↓ by 37%
Labor savings estimated at $158,000 annually
Decreased waste

Pros Utilized in analytical chemistry because it is extremely accurate.
Serves as a forcing function, in that preparers cannot proceed to next steps without scales having confirmed volumes in previous steps
Prevents upstream errors in the preparation process
Cons Volumetrics generally considered as accurate as gravimetrics
Additional time-consuming steps of weighing each item before and after drawing and injecting liquids.
Sensitive to air movement in PECs, requiring time to settle and register weights of products placed on them.

© 2014 Jerry Fahrni, Pharm.D./Mark Neuenschwander
Highly Automated Robotics

Pros and Cons
Image Source: Jerry Fahrni 2014©

Image Source: Jerry Fahrni 2014©

EHR Integrated BCMP Systems
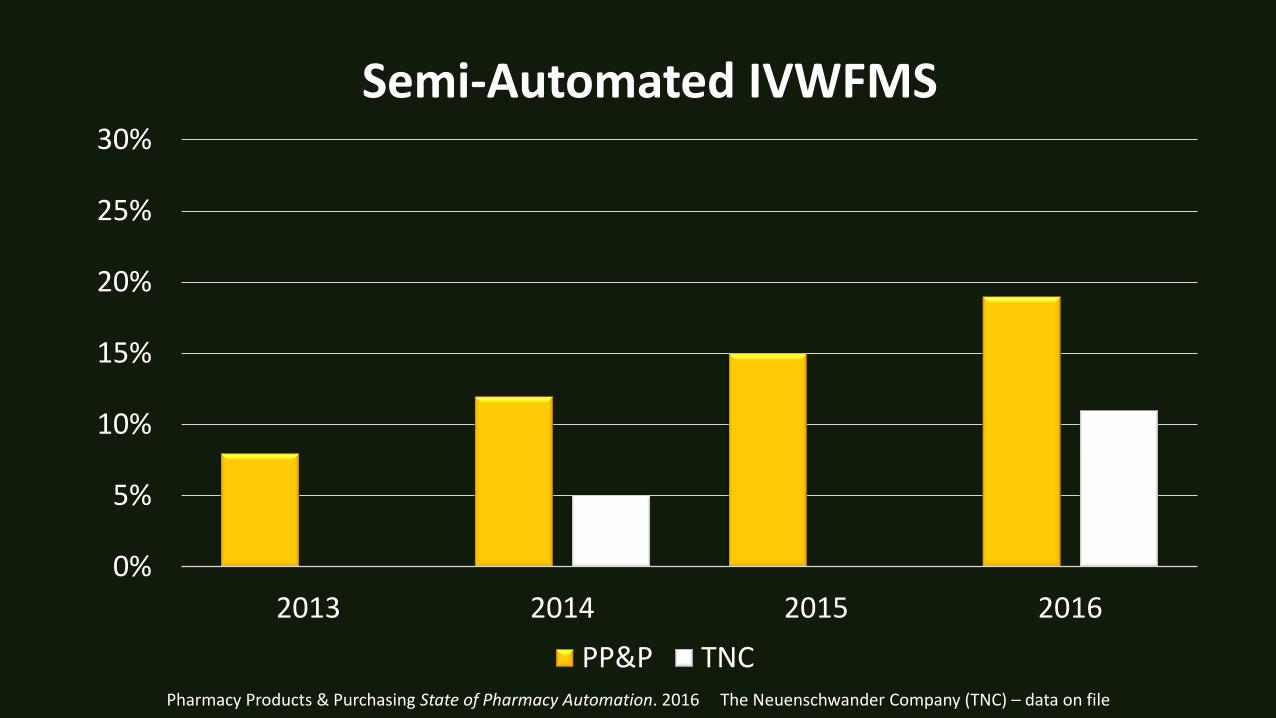
Pharmacy Products & Purchasing State of Pharmacy Automation. 2016 The Neuenschwander Company (TNC) – data on file
0%
5%
10%
15%
20%
25%
30%
2013 2014 2015 2016
Semi-Automated IVWFMS
PP&P TNC

Diffusion of Innovation

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pe
rce
nt
Pe
net
rati
on
Year/Years Required for Penetration
Penetration Rates of Consumer Technologies (1876 - Present)
Telephone
Electricity
Radio Sets B&W TV
Color TV Cable
CD Player
VCR
Cellular
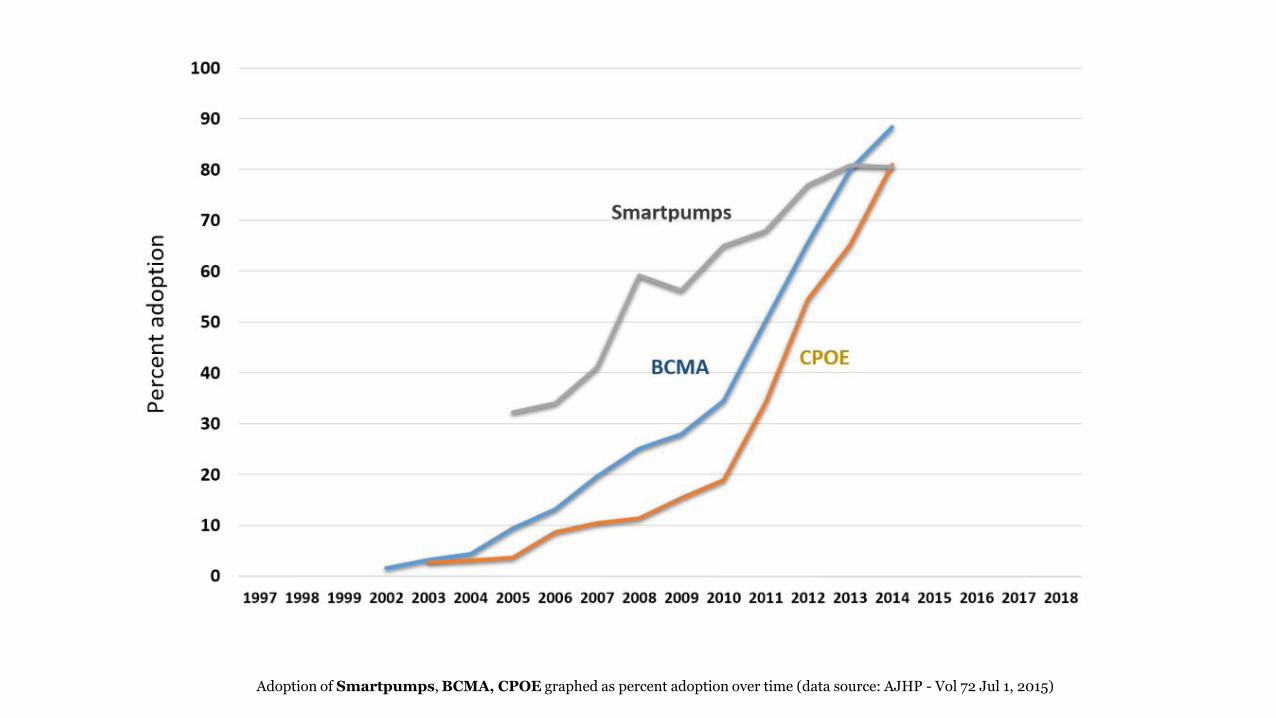
Adoption of Smartpumps, BCMA, CPOE graphed as percent adoption over time (data source: AJHP - Vol 72 Jul 1, 2015)

"Ninety-nine percent of the failures come from people who have the habit of making excuses." ~ George Washington Carver
Fear of….
Not enough
….
Too slow
Too hard
Too much $$$
RATIONALE FOR NOT ADOPTING
SAFETY
BIAS MULTI-TASKING
DATA
TRANSFORM THE ROLE OF THE TECHNICIAN STANDARDIZE IV ROOM WORKFLOW
COST
EFFICIENCY
REASONS TO ADOPT

Professionals entrusted with the delivery and administrations of pharmaceuticals have a
fundamental responsibility to identify and implement interventions that will improve patient quality outcome measures and also reduce overall health-care costs. These interventions
include timely and judicious use of therapeutic and technological advances.
“
Meyer GE, et al. AJHP. 1991 May 1;48:953-966 Image Source: Jerry Fahrni 2015©
”




















![Community Acquired Pneumonia[1] - Canadian Society of …cshpontario.ca/_CMS/files/Community Acquired Pneu… · · 2014-11-25Objectives To give a brief description of the pathophysiology](https://img.pdfslide.us/doc/110x75/5ab545f17f8b9a2f438c5924/community-acquired-pneumonia1-canadian-society-of-acquired-pneu2014-11-25objectives.jpg)