Embed Size (px)
Citation preview

The Future of Hypertension and the Optometrist
Kuniyoshi Kanai, OD
________________________________________________________________________________________________
Hypertensive Crisis in the Optometry Office
A 59 year-old patient presented to your clinic for an eye examination. During pretesting, your office staff measured the
patient’s blood pressure. The automated blood pressure device produced these numbers:
Systolic blood pressure of 202mmHg
Diastolic blood pressure of 125mmHg
Is this a scene familiar to you? How would you manage a case like this?
The Centers for Medicare & Medicaid Services (CMS) incentivized routine measurement of blood pressure through the
Meaningful Use program. Over the last decade, blood pressure and the understanding of its role in pathogenesis of
ocular diseases have evolved, such as the role of ocular perfusion pressure in glaucoma. As blood pressure measurement
has become a routine part of the optometrists’ examination, a scenario like this has become a more common clinical
encounter in the office.
Hypertensive crises
It is estimated that 32.5% of the adult population in the US is diagnosed with hypertension1. Of those, approximately 1%
experience severely elevated blood pressure in one’s lifetime2. “Severely elevated blood pressure” is generally defined
as systolic blood pressure (SBP) higher than 180mmHg or diastolic blood pressure (DBP) higher than 1103 or 120mmHg4.
Severely elevated blood pressure is associated with two crises: emergency and urgency. In the 7th report of the Joint
National Committee, hypertensive emergency is defined as a “severe elevation in BP complicated by evidence of
impending or progressive target organ dysfunction”4. Target-organ-dysfunctions or target-organ-damages (TODs) involve
the brain, heart, kidney, and large vessels: stroke, encephalopathy, acute heart failure with pulmonary edema, acute
renal failure, and aortic dissection. Patients with hypertensive emergency need to be admitted immediately for
antihypertensive treatment.
In contrast to the consensus over a hypersensitive emergency, “hypertensive urgency” is less defined. Patients with
hypertensive urgency have severely elevated blood pressure; however, they do not have the signs and symptoms of
pending TODs. Clinical dilemma often exists in the management of these individuals because a certain degree of this
Author’s Bio
Dr. Kuniyoshi Kanai is an assistant clinical professor at
University of California, Berkeley School of Optometry. He
completed his degree of Doctor of Optometry and a residency in
primary care at UC Berkeley. His current clinical duty involves
community service at the clinic in the Alameda Health System
where many patients present with cardiovascular diseases.

condition can pose an immediate threat while the other spectrum of patients is not at immediate risk for morbidities
and mortality.
In order to ensure proper management of hypertensive crises in the optometry office, the following 5 key steps will be
discussed:
1. Accuracy check 2. Symptomatology 3. Fundus examination 4. Review of history 5. Timing of referral
#1: Accuracy of blood pressure value
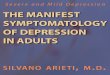
Blood pressure values can vary depending on the choice of the device and technique. Optometry offices are usually
equipped with a manual aneroid sphygmomanometer, automated arm device, and/or automated wrist device (Figure 1).
Blood pressure measurement is hydrostatic, and its outcome is highly dependent on the cuff location in respect to the
right atrium of the heart. While using wrist devices, patients tend to drop the wrist down from the heart level. This
would result in a higher blood pressure value than what would be found with proper technique. In order to reduce this
tendency, manufacturers have applied position sensors to alert clinicians when the device is mal -positioned. Despite this
improvement, automated wrist devices have been considered lacking accuracy and are not endorsed by the American
Heart Association for diagnosis and management of hypertension. For this reason, optometrists should not make a
critical management decisions based on the values measured with wrist devices.
Figure 1: Blood pressure measurement devices
Proper measurement technique is also essential to ensure accuracy. The following list shows important techniques
recommended by the American College of Cardiology Foundation and the American Heart Association5, 6.

● Wait 5 minutes at rest ● Brachial measurement ● Proper patient positioning and back support ● Placement of the proper size cuff at the heart level ● Proper deflation rate of 2mmHg per second ● Multiple measurements for confirmation
One of the common sources for error is an inappropriate-sized cuff. The diaphragm of the cuff should encircle 80% of
the arm circumference6.
Despite careful measurement technique, the measured blood pressure could still be inaccurate compared to its true
value. A number of physiological factors may influence in-office values: such as the white coat effect, diurnal fluctuation,
bladder distension, caffeine intake, emotion, and noise exposure. True BP value can be investigated by using certain
techniques, such as 24-hour ambulatory blood pressure monitoring and invasive intra-arterial measurement. However,
those methods are unrealistic in the optometry office.
With an effort to increase the accuracy of in-office measurement, one can utilize the “time” patients spend in the office.
It has been identified that blood pressure may significantly drop while the patients sit quietly in the office7, and the
value may mimic that of ambulatory blood pressure measurement8. Grass, et al. applied this concept to 549 patients in
the Emergency Department (ED) who presented with severely elevated blood pressure9. Patients in this study were all
asymptomatic for acute organ damage, and they were instructed to rest and wait in the exam room for 30 minutes. 32%
of them showed a spontaneous drop in blood pressure well below SBP of 180mmHg and DBP of 110mHg. Those
patients with reduced BP were sent home without antihypertensive treatment. No adverse events occurred.
Key:
● Proper selection of BP device ● Proper technique ● Confirm BP value over 30 minutes
#2: Symptomatology
Symptomatology often dictates the urgency of management. Zampaglione and his colleagues 2 tabulated the signs and
symptoms of patients with hypertensive emergency and urgency (Table 1). The listed signs and symptoms are consistent
with involved end organs. For example, a patient with pulmonary edema from acute heart failure may experience chest
pain and difficulty in breathing.
If a patient has any of the signs and symptoms below, optometrists should consider that individual as having a possib le
hypertensive emergency. The patient should be transported to ED immediately for investigation of target organ
damage.
Signs and Symptoms Emergencies (%) Urgencies (%)
Headache 3.0 22.0%
Epistaxis 0.0 17.0%

Chest pain 27.0 9.0
Dyspnea 22.0 9.0
Faintness 10.0 10.0
Psychomotor agitation 0.0 10.0
Neurological deficit 21.0 3.0
Vertigo 3.0 7.0
Paresthesia 8.0 6.0
Vomitus 3.0 2.0
Arrhythmia 0.0 6.0
Other 3.0 2.0
Table 1: Signs and symptoms of hypertensive crises*
*Adapted from Zampaglione B, Pascale C, Marchisio M, Cavallo-Perin P. “Hypertensive Urgencies and Emergencies Prevalence and
Clinical Presentation” Hypertension. 1996; 27: 144-147
One exception can be made for a non-specific mild headache. Mild headache in severely elevated blood pressure is
relatively common. In the absence of other signs and symptoms of central nervous system involvement, routine
neuroimaging is unlikely to reveal CNS involvement10.
Key:
● Symptomatic patients should be considered hypertensive emergency until proven otherwise
#3: Fundus examination
The fundus provides a tremendous amount of information about the integrity of the microvasculature. Different stages
of hypertensive retinopathy represent different pathological processes.
The Keith-Wagener-Barker 4-stage classification has historically been applied to clinical practice. More recently, Wong
and Mitchell simplified this classification to 3 stages11.
The advantage of this simplified scheme is a linear correlation of retinopathy to target-organ-damages (TODs) that were
identified from community studies.
Keith-Wagener-
Barker
Wong-Mitchell
Classification
Clinical findings Pathogenesis Target-Organ-Damages
Risks

Classification
1 Mild ▪ Focal or general
arteriolar narrowing
▪ Copper/silver wiring
▪ AV nicking
▪ Normal autoregulation
response ▪ Hyalinization ▪ Sclerosis
▪ Concurrent ventricular
hypertrophy14
▪ Future coronary heart
diseases16, 17
▪ Future stroke
15
2
3 Moderate ▪ Retinal hemorrhage
▪ Soft exudate ▪ Hard exudate
▪ Loss of BRB integrity Concurrent damages in
● Glomerular fi ltration barrier
● Blood brain barrier
4 Severe ▪ Optic disc edema ▪ Loss of BRB integrity ▪ Autoregulation
breakthrough
▪ Death
Table 2: Clinical picture of hypertensive retinopathy
Two pathological changes progress as hypertensive retinopathy worsens: a loss of autoregulation ability and a
breakdown of Blood-Retinal-Barrier (BRB) integrity.
In early stages of hypertensive retinopathy, arteriolar attenuation first becomes apparent. This is a normal
autoregulation response to elevated blood pressure. The innate autoregulation ability of blood vessels allows for
changes in its lumen size in an effort to maintain a steady perfusion pressure (Figure 4). When blood pressure rises,
vessels become attenuated. If hypertension is controlled at this point, reversal of attenuation will occur. Chronic
elevation in blood pressure eventually damages the inner lining of the vessel and causes a pathological process, called
hyalinization, and eventually leads to sclerotic change. This morphological change can be clinically seen as copper and
more advanced silver wiring (Figure 2). Findings from the Blue Mountain Eye Study 12 and the Beaver Dam Eye Study13
suggest that reversal of attenuation is unlikely to occur once vessels undergo sclerosis even if blo od pressure is
controlled afterwards.

Figure 2: Sclerosis and copper/silver wiring (blue arrows)
Another clinical implication of mild hypertensive retinopathy is risks of TODs. The risks are generally linked with
longitudinal data rather than cross sectional analysis. For example, the Atherosclerosis Risk in Community (ARIC) Study
found a positive correlation between arteriolar attenuation and concurrent left ventricular hypertrophy in the African
American population14. Left ventricular hypertrophy is an enlargement of the left ventricle muscle in order to
counteract vascular resistance. This condition itself is not considered a disease, but it is a manifestation of chronic stres s
to the heart. Patients with left ventricular hypertrophy are at a greater risk of eventual heart diseases. Thus, the
presence of mild hypertensive retinopathy in patients with severely elevated blood pressure is unlikely to imply an
immediate risk of acute organ damages.
The other characteristic pathological change is seen in moderate hypertensive retinopathy patients, the presence of
hemorrhages and exudates. This presence of hemorrhages and exudates is a manifestation of a compromised blood-
retinal-barrier (BRB). Capillary endothelial cells and tight junctions create a tight seal around the blood vessels forming
the BRB. A compromise in the BRB results in the leakage of blood constituents that is clinically evident as hemorrhages
and edema. Retinal capillaries share embryological and morphological similarities with those in the brain and kidney. It is
no surprise that a compromise in the BRB is suggestive of the same pathological change in the brain as well as the
glomeruli of kidney. In the aforementioned ARIC Study, patients with moderate retinopathy had more than 2 fold -
increased risks of glomerular filtration dysfunction18 and cognitive impairment19. Both conditions are linked with
abnormal leakage of protein that should be concealed by the organs’ barrier function. Thus, the presence of moderate
retinopathy implies concurrent damage in other organ capillary systems.

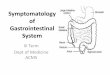
Figure 3: Severe hypertensive retinopathy with disc edema, hemorrhage and exudates
Severe hypertensive retinopathy represents a breakdown in both BRB and autoregulation. This stage of retinopathy is
characterized by the presence of choroidopathy, macular star, optic disc edema, and focal intraretinal peri-arteriolar
transudates (FIPTs). FIPTs are leakage from dilated pre-capillary arterioles20. If the retinal vasculature retains
autoregulation ability, vessels will maintain a small caliber to cope with high blood pressure. However, their
autoregulation ability eventually comes to an end, and vessels cannot remain attenuated and will start dilating. This end
process is called “autoregulation breakthrough”, and organ tissues suffer from hyper-perfusion under this condition.
Optic disc edema suggests an even more alarming issue. There are conflicting opinions in its underlying mechanism:
encephalopathy23, intracranial hypertension23, and ischemia in short posterior ciliary arteries20. A study showed that
patients with severe hypertension suffer from impaired autoregulation in the brain 21 and thus, this stage of retinopathy
likely represents an impaired autoregulation in both the retina and the brain. Considering the high mortality rate 22,
patients with severe retinopathy should be considered as a hypertensive emergency and admitted to the ED
immediately.
Key:
● Progressively increased risk of TODs with worsening hypertensive retinopathy.
#4: Review of history

If the patient is asymptomatic and the fundus shows no retinopathy or only mild retinopathy, is he/she a non -urgent
patient? To address this question, a careful review of their history is critical.
Experts suggest that true hypertensive urgency should be distinguished from “severe uncontrolled hypertension” among
asymptomatic patients based on the presence of risk factors for progressive organ damages 3, 10. These risk factors
include, but are not limited to, the established history of cardiovascular, cerebral and renal diseases such as congestive
heart failure, unstable angina, coronary artery disease, renal insufficiency, transient ischemic attack, or stroke 10. Patients
with such histories should be given greater attention and should be considered “hypertensive urgency” even if they are
asymptomatic and have no clear signs of damages in the BRB or autoregulation.
Attention should also be paid to how rapidly the blood pressure rose to this severe level. Autoregulation has an amazing
adaptability of adjusting itself to chronically elevated blood pressure to provide a steady perfusion pressure to protect
organs (Figure 4). Its effect is prominent in certain organs and vessels, such as the brain, coronary artery, kidney, aorta,
and retina. However, this shift takes months and years to occur. Therefore, patients who experience sudden pressure
rise are more likely to fall outside the protective range of autoregulation. High-risk profiles include younger individuals,
pregnancy, use of recreational drugs, and no prior diagnosis of hypertension.
Figure 4: Autoregulation
Overall, the risk assessment should be made based on a global analysis of age, chronicity of hypertension, rapidity of
blood pressure increase, and preexisting TODs rather than the actual severity of hypertension10.
#5: Timing of referral
How urgently should patients with severely elevated pressure be managed?

The appropriate timeframe for a suspected case of hypertensive emergency is clear and simple: immediate referral to
the ED. The case warrants immediate workup for acute TODs. Upon confirmation, the patient will be admitted to the
intensive care unit and receive intravenous antihypertensive treatment to lower BP by 20~25% depending on the
underlying condition.
Patients with hypertensive urgency are not manifesting signs and symptoms of acute organ damages. However, these
patients possess certain risks for progressive organ damage. The risks may be apparent in their fundus or in thei r
medical histories. At this time, it is still unclear when these patients will convert to hypertensive emergency. Therefore,
a timely referral should be made without delay within 24~48 hours3, 10. Depending on the circumstance, referral to the
ED may be appropriate in these cases.
What about asymptomatic patients with zero to minimal risks? Should they still be sent to the ED?
In their recent clinical policy, the American College of Emergency Physicians reviewed the evidence and expert opinions
on how to manage asymptomatic patients with markedly elevated blood pressure in the emergency department 24. This
review did not find sufficient evidence to support routine work-ups (ex: serum creatinine, urinalysis, ECG) and the
practice of lowering blood pressure at the ED. It is noteworthy that experts did recommend that care should be given to
patients with poor follow-up, limited health care access, older age, or an African American racial background. This
recommendation is not based on a patient’s blood pressure value, rather on a patient’s profile.
You may wonder why a more aggressive treatment approach was not recommended in this review. The key is in
autoregulation. When the patient has no overt signs, including in the fundus, and symptoms of organ damage from
severe hypertension, it is very likely that the patient’s autoregulation has shifted to a rightward direction maintaining a
steady perfusion pressure to vital organs even at a higher mean arterial pressure (Figure 4). This “right” shift ironically
makes patients more vulnerable for a risk of hypo-perfusion by an abrupt drop in blood pressure in an attempt to
normalize it. These patients may suffer ischemia in vital organs, such as myocardial ischemia and infarction, stroke, and
death from treatment itself25. To minimize this risk while achieving a substantial anti-hypertensive effect, long-acting
medications should be administered by a provider who can monitor their progress regularly. This allows a gradual shift
in autoregulation to a leftward direction. Thus, patients with low risks are more likely to achieve long-term success in
the hands of their own primary care physicians.
Summary
Management of patients with severely elevated blood pressure brings a number of dilemmas to optometrists.
Inappropriate management of this condition could result in significant disability and mortality. While some patients
need immediate care at the ED, others do not necessarily benefit from ED referral. Studies have noted a disappointing
follow-up rate at the primary care physician’s office after an ED visit26, 27. Meanwhile, budgetary constraints have
recently made the CMS focus on reducing the cost for non-emergent ED visits. Optometrists need a strategy.
Optometrists are unique health care providers who are capable of making accurate assessments on the integrity of the
microvasculature. By carefully examining a patient’s symptoms, fundus, and medical histories (Table 3), optometrists
can triage this challenging condition and guide the patients to long-term success in their lives.
Severe uncontrolled HTN Hypertensive urgency Hypertensive emergency

Symptomatology Asymptomatic or non-
specific mild headache
Asymptomatic or non-
specific mild headache
Symptomatic of acute TODs
Fundus No or mild retinopathy Moderate retinopathy Severe retinopathy
Medical History No pertinent history History of preexisting organ
injury
May or may not have
pertinent history
Timing of referral Within 1 week to PCP Within 24~48 hours to PCP
or ED
Immediate referral to ED
Table 3: Management strategy for patients with severely elevated blood pressure
Acknowledgment: I would like to thank Sean Umamoto, Ph.D. for his insightful comments on this manuscript.
For comments and questions, please contact Dr. Kanai at [email protected]
Reference
1. The Centers for Disease Control and Prevention. “Health, United States, 2014”
http://www.cdc.gov/nchs/data/hus/hus14.pdf#059 retrieved at 10:36 2/2/2016. 2. Zampaglione B, Pascale C, Marchisio M, Cavallo-Perin P. “Hypertensive Urgencies and Emergencies Prevalence and Clinical
Presentation” Hypertension. 1996; 27:144-147. 3. Kessler CS, and Jourdeh Y. “Evaluation and Treatment of Severe Asymptomatic Hypertension.” Am Fam
Physician. 2010 Feb 15;81(4):470-476. 4. National Heart, Lung, and Blood Institute. “The Seventh Report of the Joint National Committee on Prevention, Detection,
Evaluation, and Treatment of High Blood Pressure”. August 2004.; NIH Publication No. 04 -5230.
5. Aronow WS, et al. “A Report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents Developed in Collaboration With the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of Hypertension”. J Am Coll Cardiol. 2011;57(20):2037-2114.
6. Pickering TG, Hall JE, and et al. “Recommendations for Blood Pressure Measurement in Humans and Experimental Animals.” Circulation 2005; 111:697-716.
7. Scherpbier-de Haan N, van der Wel M, Schoenmakers G, and et al. “Thirty-minute compared to standardised office blood pressure measurement in general practice.” Br J Gen Pract. 2011 Sep;61(590):e590-7.
8. van der Wel MC, Buunk IE, van Weel C, et al. “A novel approach to office blood pressure measurement: 30-minute office blood pressure vs daytime ambulatory blood pressure.” Ann Fam Med. 2011 Mar-Apr;9(2):128-35.
9. Grassi D, O’Flaherty M, Pellizzari M, et al. “Hypertensive urgencies in the emergency department: evaluating blood pressure
response to rest and to antihypertensive drugs with different profiles.” J Clin Hypertens. 2008;10:662-667. 10. Shayne PH, Pitts SR. Severely increased blood pressure in the emergency department. Ann Emerg Med. 2003;41(4):513–
529. 11. Wong TY, Mitchell P. “The eye in hypertension.” Lancet, 2007 Feb 3;369(9559):425-35.
12. Leung H, Wang JJ, Rochtchina E, Wong TY, Klein R, Mitchell P. “Impact of current and past blood pressure on retinal arteriolar diameter in an older population.“ J Hypertens 2004; 22: 1543–49.
13. Klein R, Myers CE, Knudtson MD, et al. “Relationship of blood pressure and other factors to serial retinal arteriolar diameter
measurements over time: the Beaver Dam Eye Study. “ Arch Ophthalmol. 2012;130:1019-1027. 14. Tikellis G, Arnett DK, Skelton TN, Taylor HW, Klein R, Couper DJ, Richey SA, Yin WT. Retinal arteriolar narrowing and left
ventricular hypertrophy in African Americans. the Atherosclerosis Risk in Communities (ARIC) study. Am J Hypertens. 2008;21:352-359.
15. Wong TY, Klein R, Couper DJ, Cooper LS, Shahar E, Hubbard LD, Wofford MR, Sharrett AR. Retinal microvascular abnormalities and incident stroke: the Atherosclerosis Risk in Communities Study. Lancet. 2001;358:1134 -1140.
16. Wong TY, Klein R, Sharrett AR, Duncan BB, Couper DJ, Tielsch JM, Klein BE, Hubbard LD. Retina l arteriolar narrowing and risk of coronary heart disease in men and women. The Atherosclerosis Risk in Communities Study. JAMA. 2002;287:1153 -1159.

17. Duncan BB, Wong TY, Tyroler HA, Davis CE, Fuchs FD. Hypertensive retinopathy and incident coronary heart di sease in high risk men. Br J Ophthalmol. 2002;86:1002-1006.
18. Wong TY, Coresh J, Klein R, et al. “Retinal Microvascular Abnormalities and Renal Dysfunction: The Atherosclerosis Risk in Communities Study”. J Am Soc Nephrol 15: 2469–2476, 2004.
19. Wong TY, Hubbard LD, Klein R, et al. “Retinal microvascular abnormalities and blood pressure in older people: the Cardiovascular Health Study. “Br J Ophthalmol 2002; 86: 1007–13.
20. Hayreh SS, Servais GE, Virdi PS. “Fundus lesions in malignant hypertension. IV. Focal intra retinal periarteriolar transudates.” Ophthalmology 1986. Jan; 93(1): 60-73.
21. Immink RV, van den Born VH, and et al. “Impaired cerebral autoregulation in patients with malignant hypertension”. Circulation 2004; 110: 2241-45.
22. Lane DA. “Improving Survival of Malignant Hypertension Patients Over 40 Years.“ Am J Hypertens 2009; 22: 1199~1204. 23. Dinsdale H. “Hypertensive encephalopathy” in Bernett H, Stein B, Morh J, Yatsu F, (eds): Stroke. New York, Churchill
Livingstone, 1986, vol 2, 869-74.
24. The American College of Emergency Physicians Clinical Policies Subcommittee. “Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients in the Emergency Department With Asymptomatic Elevated Blood Pressure.” Ann Emerg Med. 2013;62:59-68.
25. Decker WW, Godwin SA, Hess EP, and et al. “Clinical policy: critical issues in the evaluation and management of adult
patients with asymptomatic hypertension in the emergency department” Ann Emerg Med. 2006;47:237-249. 26. Baumann BM, Cienki JJ, Cline DM, et al. Evaluation, management, and referral of elderly emergency department patients
with elevated blood pressure. Blood Press Monit. 2009; 14:251-256.
27. Collins K, Gough S, Clancy M. Screening for hypertension in the emergency department. Emerg Med J. 2008;25:196-199.

CE@Home Online March April
Name__________________ Lisence_____________________
1. Which of the following devices is the least ideal to determine blood pressure in patients with suspected hypertensive crises?
a. Manual aneroid sphygmomanometer
b. Automated arm device c. Automated wrist device d. All above is equally ideal
2. Which of the following techniques likely results in a faulty blood pressure value?
a. Placement of a cuff at the heart level
b. Deflation of a cuff at the rate of 2mmHg per second
c. Having a patient seated in a chair with no back support
d. The diaphragm of a cuff encircles 80% of the arm circumference
3. Which of the organs/vessels can hypertensive emergency involve?
a. Brain b. Kidney c. Heart d. Aorta e. All above
4. True or False: a patient with systolic blood pressure of 200mmHg and diastolic blood pressure of 120mmHg is at the immediate risk of acute organ failure regardless of their symptoms, fundus appearance, and medical history.
5. Which of the following symptoms is suggestive of progressive target-organ-damages?
a. Shortness of breath b. Severe headache c. Chest pain d. Speech slur e. All above
6. True or False: the retinal vasculature exhibits autoregulation response to a variety of blood pressure.
7. True or False: mild hypertensive retinopathy exemplifies “autoregulation breakthrough”.
8. True or False: moderate hypertensive retinopathy is suggestive of a compromise in the glomerular filtration barrier of the kidney.
9. True or False: when blood pressure is severely elevated, a patient with known history of unstable angina should be given an extra caution in management.
10. Which of the following statement is true in regards to autoregulation?
a. In chronic hypertension, autoregulation gradually shifts to a rightward direction.
b. If blood pressure rises acutely, the organ may undergo hyper-perfusion.
c. If blood pressure is abruptly reduced, the organ may undergo hypo-perfusion.
d. Slow anti-hypertensive treatment allows autoregulation to shift gradually to a leftward direction.
e. All above

Please fill out this form completely. Mail or fax (along with payment) to:
Mail:
COA – Education Coordinator
2415 K Street
Sacramento, CA 95816
Fax: 916-448-1423
RECEIVING YOUR TRANSCRIPT
Name: ___________________________________
License Number: ___________________________
Phone Number: ____________________________
□ Please check here if you would like to receive your transcript via MAIL.
Mailing Address:
_________________________________________
_________________________________________
_________________________________________
□ Please check here if you would like to receive your transcript via E-MAIL.
E-mail Address
_________________________________________
PAYMENT INFORMATION
□ COA Member - $15
□ Non-Member - $35
□ Check or Money Order enclosed (payable to the California Optometric Association)
□ Credit Card: □ VISA □ MC □ AMEX
Card Number: _____________________________________ Expiration Date: ______________

CCV#: ___________ (VISA & MC – 3 digit # on back; AMEX – 4 digit # on front)
Name on Card: ____________________________________
Authorized Signature: ______________________________ _
FOR OFFICE USE ONLY
Date Received Invoice Batch ID Number