Embed Size (px)
Citation preview
www.england.nhs.uk @robertvarnam
The future of general practice: what have we learned?
Dr Robert VarnamHead of general practice development
@robertvarnam
bit.ly/151010fdaFamily Doctor Association10 Oct 15
www.england.nhs.uk @robertvarnam
Is general practice finished?
What size should we be?
What form should we adopt?
We’re a federation. What now?
Top questions
www.england.nhs.uk @robertvarnam
The founding principles of UK primary care are admired the world over, and rightly so. General practice is a jewel in the crown of this country. Right now, general practice feels in a bad place. Constrained, hemmed-in and, to some, marginalised. Whatever the state of things in your part of the country, in general, I think it’s fair to say that, at the very least, general practice is currently constrained from delivering its full potential. We need to see increases in funding, a growth in the workforce, and improvements to premises. Without those, existing services may not be sustainable.
Is general practice finished?
www.england.nhs.uk @robertvarnam
At the heart of the case for change is not the workload of practices – important though that is – it is the needs of patients, and they way they are changing. When the NHS was founded, its purpose was fairly simple. Every now and then, people got ill. When they did, they consulted their doctor. If it was a straightforward problem, they would give a prescription, the person would get better, return to work and, in a year or two, they might need the doctor again. If it was less straightforward, they would be referred to a clever doctor – who would give a prescription or cut out the offending part. The patient would then get better, return to work, and, in a year or two, they might become ill again.
That accounted for the majority of the anticipated work of the NHS. And, for some patients, that’s still the kind of care that’sneeded.
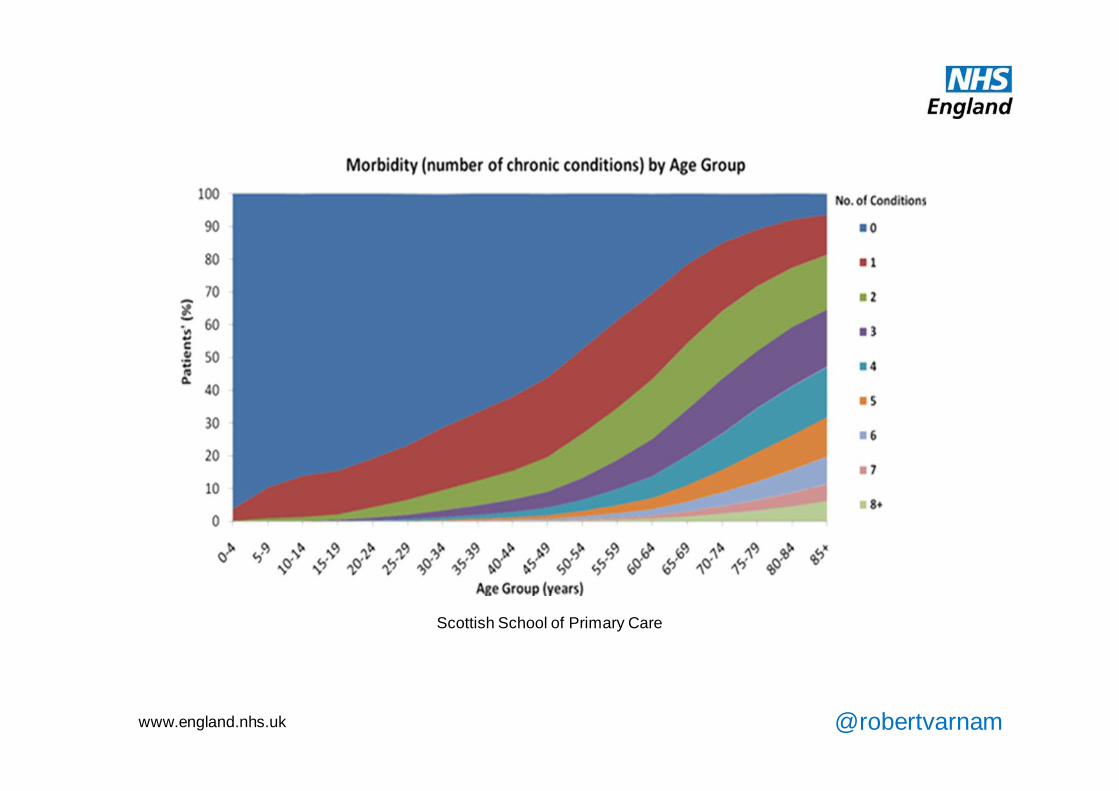
However, a growing proportion of our work is fundamentally different. This now seminal chart illustrates the central fact underlying the quantitative and qualitative change in the work of primary care. It illustrates the rise in multimorbidity with age. As people get older, they have more simultaneous longterm conditions. So that, by the age of 75, for example, at least a third of people are living with four or more LTCs. And, as our demography changes, the proportion of older people increases. Dealing with longterm conditions already accounts for over half of work in primary care. It is set to increase.
And, crucially, this represents a qualitative change in the nature of work. These are not people who visit the GP every year or two to get cured of their problem. These are people with problems that we cannot cure – they are living with multiple issues which will not go away, and they visit the GP six, seven, eight or more times a year. At least. Furthermore, the more simultaneous problems someone has, or the greater their frailty, the less helpful it is to pass their care to a doctor specialising in one part of the body. These people need treating as people, not diseases.
So the population of people who need what only primary care can offer has grown, the amount of time they need has grown –and both are set to continue growing. This is the chief case for change in primary care, the pressure of patients’ needs.
This is not a blip requiring a short-term correction to the priorities of the NHS. It is a fundamental shift which requires every developed nation on earth to turn away from what Muir Gray has termed the ‘century of the hospital’, and place the emphasis where the population’s need is. Scottish School of Primary Care

www.england.nhs.uk @robertvarnam
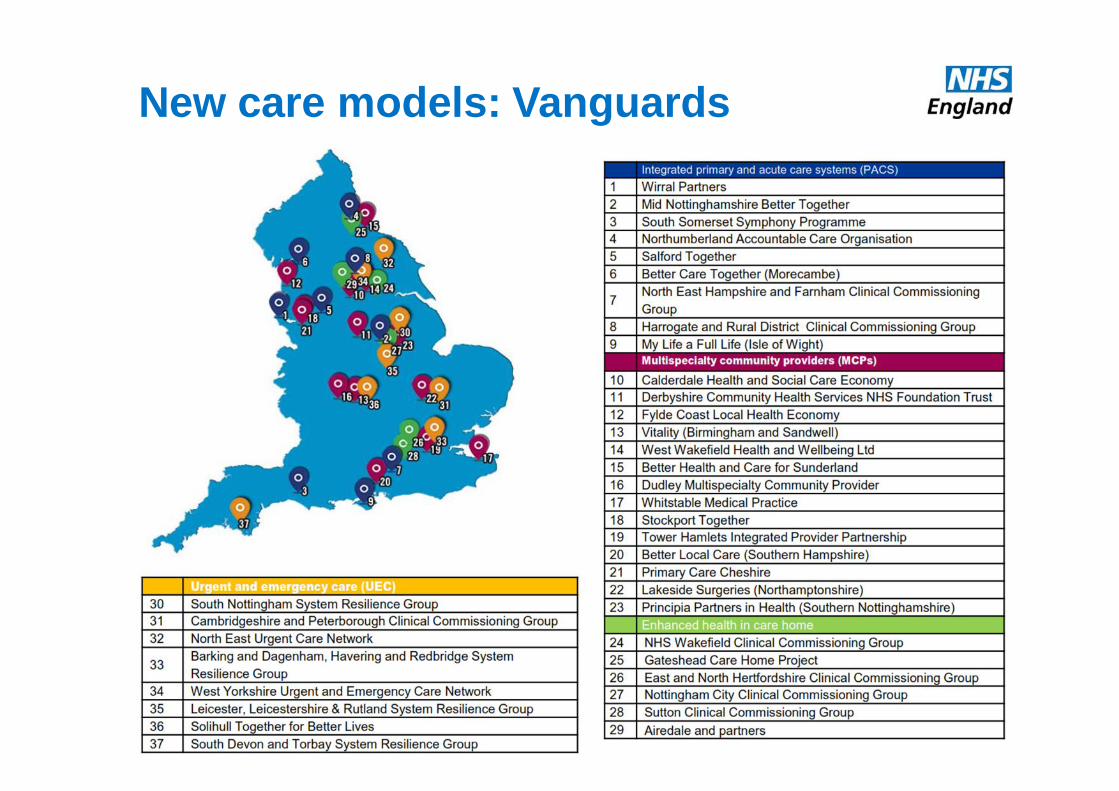
New care models: Vanguards
www.england.nhs.uk @robertvarnam
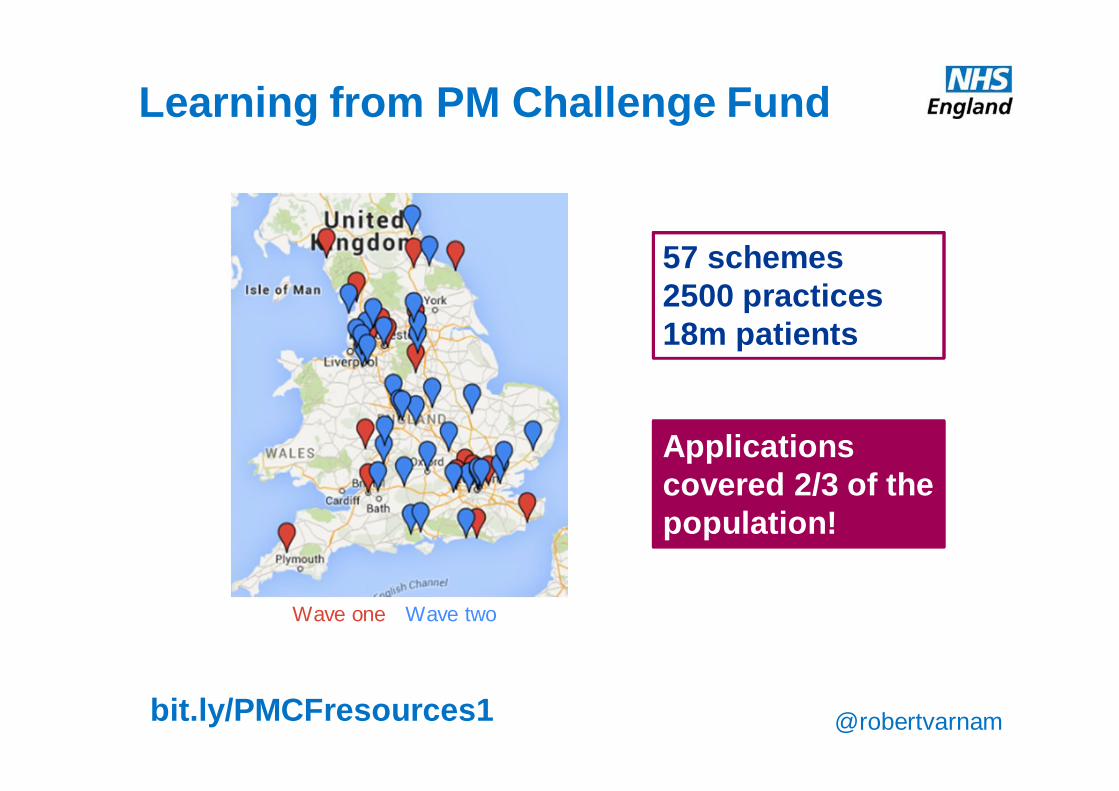
An example of this in practice at the moment is the Prime Minister’s GP Access Fund. Now covering a significant proportion of the country, practices in this are implementing quite wide-ranging redesign of their services, acknowledging that extended hours are only one part of good access. The practices participating in this programme are already beginning to implement many of the transformational changes envisaged by the Five Year Forward View. This is generating valuable learning about the specific changes required, including the ways in which the system can make progress easier and more sustainable.
Wave one Wave two
57 schemes2500 practices18m patients
Learning from PM Challenge Fund
bit.ly/PMCFresources1
Applications covered 2/3 of the population!
www.england.nhs.uk @robertvarnam
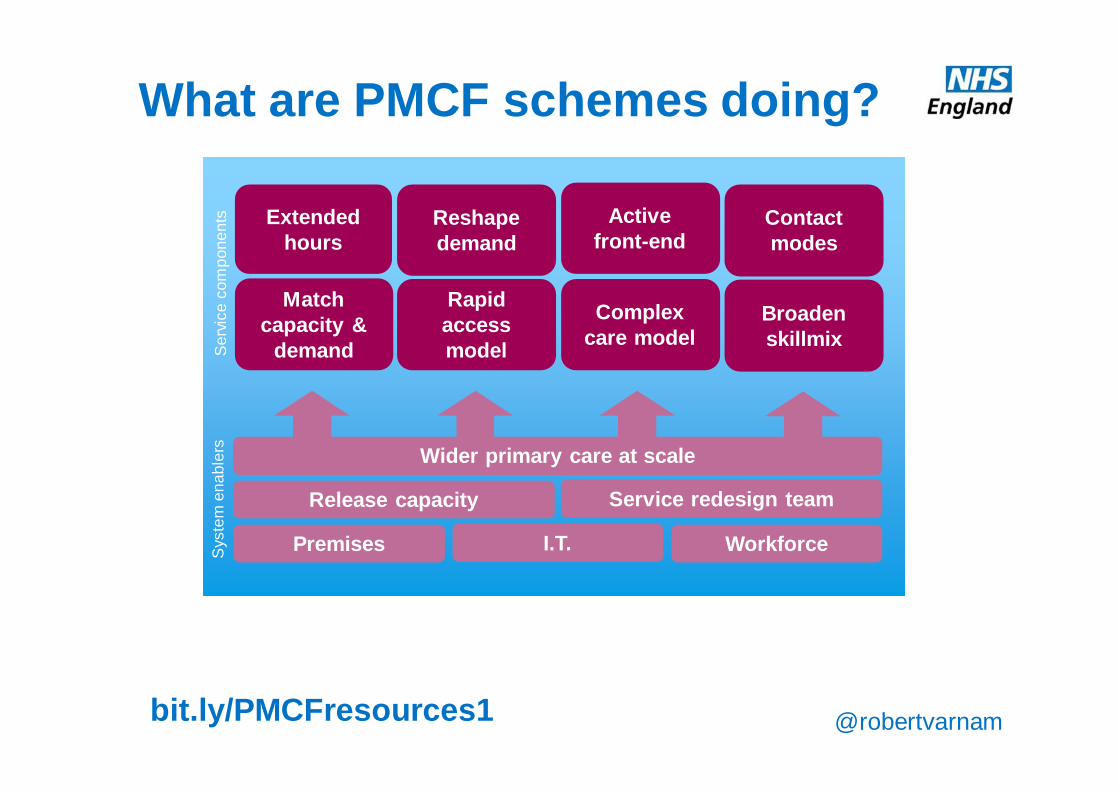
What are PMCF schemes doing?
Wider primary care at scale
Reshapedemand
Activefront-end
Contact modes
Match capacity &
demand
Rapid access model
Extended hours
Release capacity Service redesign team
Broaden skillmix
Complex care model
Premises I.T. Workforce
Ser
vice
com
pone
nts
Sys
tem
ena
bler
s
bit.ly/PMCFresources1
www.england.nhs.uk @robertvarnam
Observations aboutat-scale primary care
www.england.nhs.uk @robertvarnam
Association
Network
Federation
Partnership
Superpractice
A federation by any other name…
5 yearsContemplation
www.england.nhs.uk @robertvarnam
Clarity Buy-in Agility
Size
Alignment Priorities Partnerships
2 300+
www.england.nhs.uk @robertvarnam
• Ad hoc• Relational network• CCG locality• Collaboration agreement• Seed funded company• Jointly owned company• Single company
Form
www.england.nhs.uk @robertvarnam
• Monthly colloquium
• Quarterly colloquium
• Committee
• Executive team
• The Boss
Decision making
Bulletin
Visits
Online forum
www.england.nhs.uk @robertvarnam
• Outsourced management• Spare time• New managers• Distributed leadership
Leadership & infrastructure
Vision-casting
Data gathering
Programme management I.T.
Procurement
Workforce
Mobilisation
Governance
Practice engagement Patient engagement Stakeholder partnerships
Analysis

www.england.nhs.uk @robertvarnam
1. Stop obsessing about form2. Create shared purpose3. Invest in development4. Design the form deliberately
Top tips
www.england.nhs.uk @robertvarnam
Purpose > function > form Purpose > function > form Purpose > function > form
1. Stop obsessing about form
Purpose > function > form Purpose > function > form
a) Pick something to improve for patients
b) Improve it together
c) Build infrastructure to enable, accelerate & sustain

www.england.nhs.uk @robertvarnam
2. Create shared purpose
• A sense of shared identity sufficiently strong to allow collaboration that crosses boundaries of organisational sovereignty. • We share ideas, data, resources• We will adopt a standard approach• We can call on each other
• A purpose beyond ourselves, orienting us around the needs of our patients.
• Commitment to us and our purpose sufficiently strong to make compliance unnecessary
www.england.nhs.uk @robertvarnam
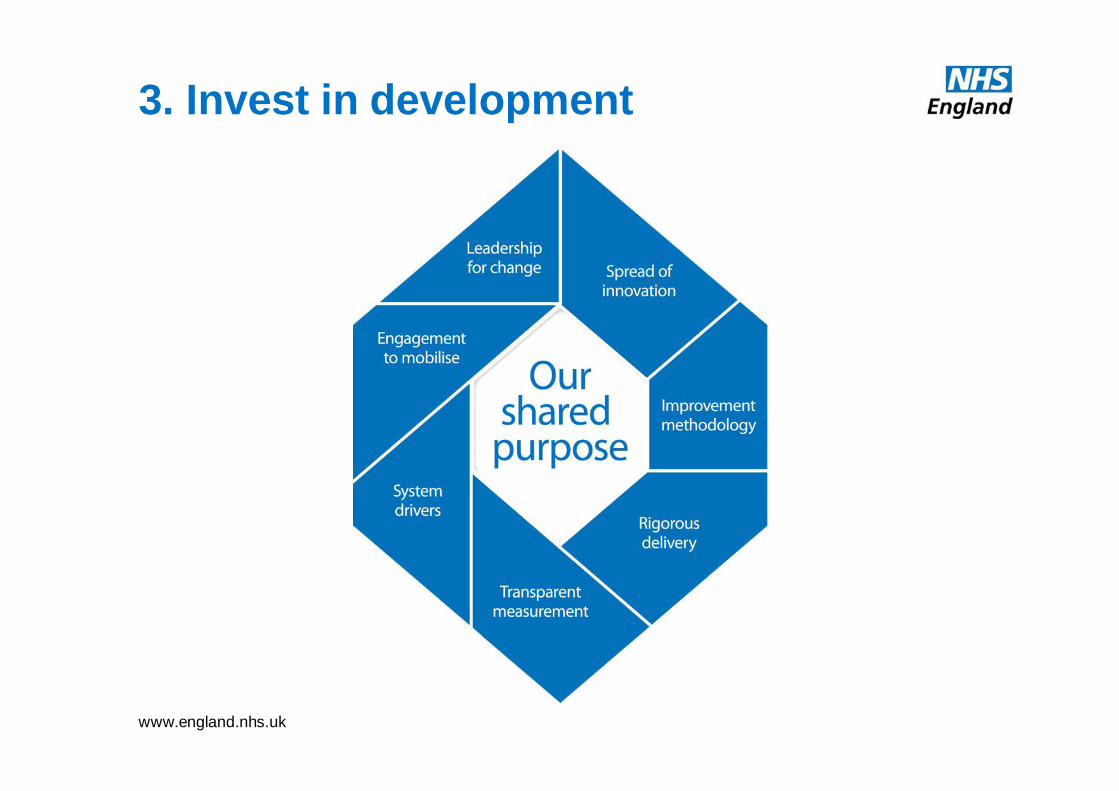
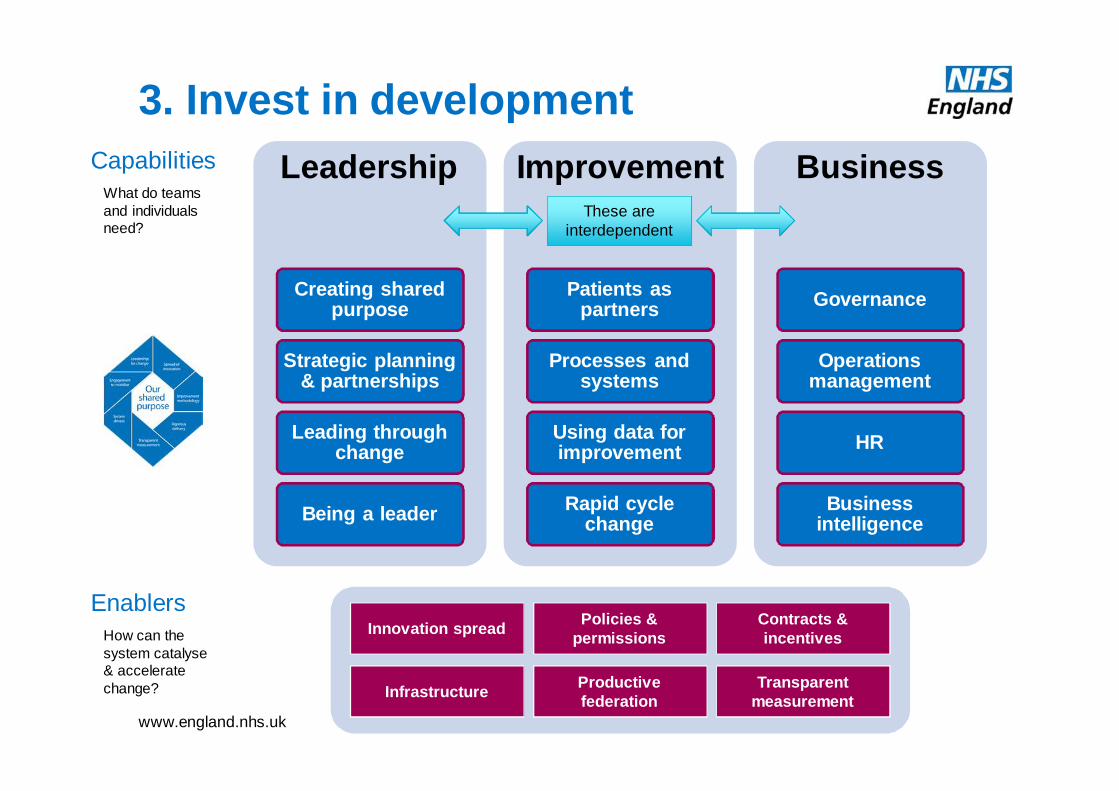
3. Invest in development
www.england.nhs.uk @robertvarnam
Leadership
Creating shared purpose
Strategic planning & partnerships
Leading through change
Being a leader
Improvement
Patients as partners
Processes and systems
Using data for improvement
Rapid cycle change
Business
Governance
Operations management
HR
Business intelligence
Capabilities
EnablersInnovation spread Policies &
permissionsContracts & incentives
Infrastructure Productive federation
Transparent measurement
3. Invest in development
What do teams and individuals need?
These are interdependent
How can the system catalyse & accelerate change?
www.england.nhs.uk @robertvarnam
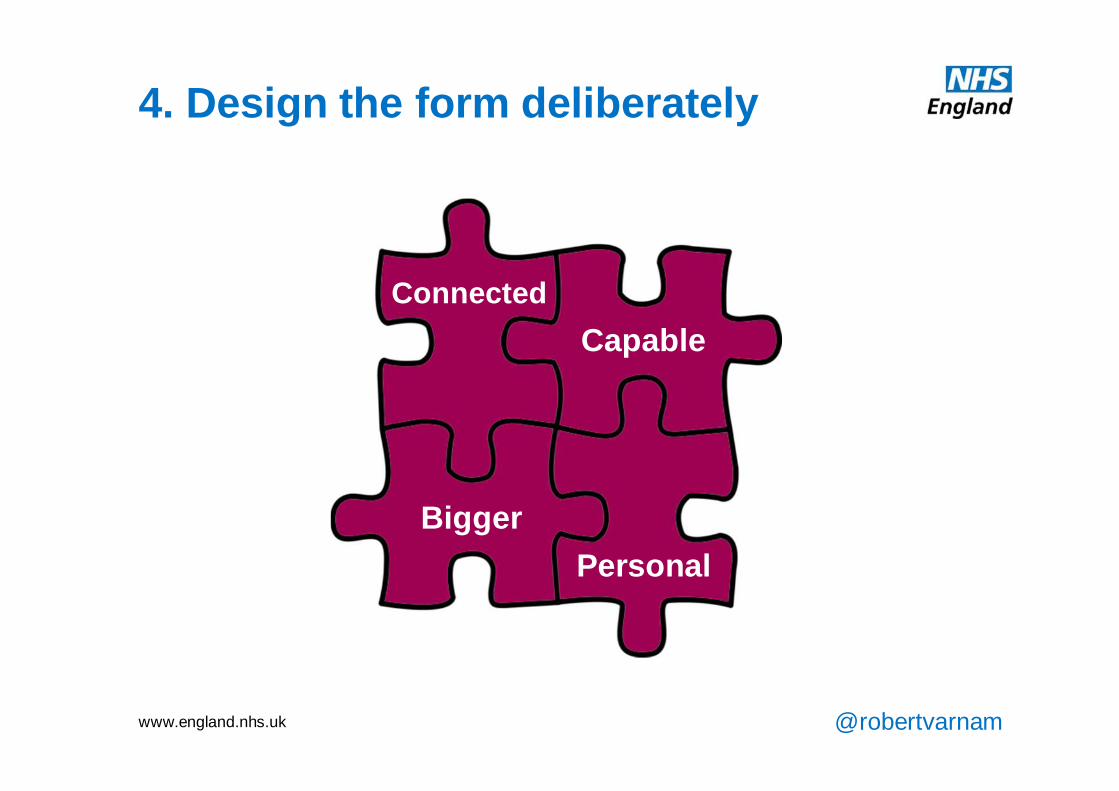
At an organisational level, what will wider primary care at scale look like? Again, the precise details should be locally determined. But we should aim for it to be bigger, in a way that brings real patient to patients and staff, not just creating a new organisation because it makes us feel safer. Our new networks, federations or mergers should have enhanced capabilities, for leadership, management, services and improvement. We also need to ensure that, as we operate at large scale, we maintain the personal care which is so hugely important for many patients (and staff). That will take deliberate design: it won’t just happen. Finally, it should like it’s ‘yours’ – by which I mean that staff will need to have the same sense of belonging, ownership and commitment as in the best practices now. Regardless of the actual business model. That, too, will take planning and skill.
At an organisational level, what will wider primary care at scale look like? Again, the precise details should be locally determined. But we should aim for it to be bigger, in a way that brings real patient to patients and staff, not just creating a new organisation because it makes us feel safer. Our new networks, federations or mergers should have enhanced capabilities, for leadership, management, services and improvement. We also need to ensure that, as we operate at large scale, we maintain the personal care which is so hugely important for many patients (and staff). That will take deliberate design: it won’t just happen. Finally, it should like it’s ‘yours’ – by which I mean that staff will need to have the same sense of belonging, ownership and commitment as in the best practices now. Regardless of the actual business model. That, too, will take planning and skill.
4. Design the form deliberately
BiggerPersonal
CapableConnected
www.england.nhs.uk @robertvarnam
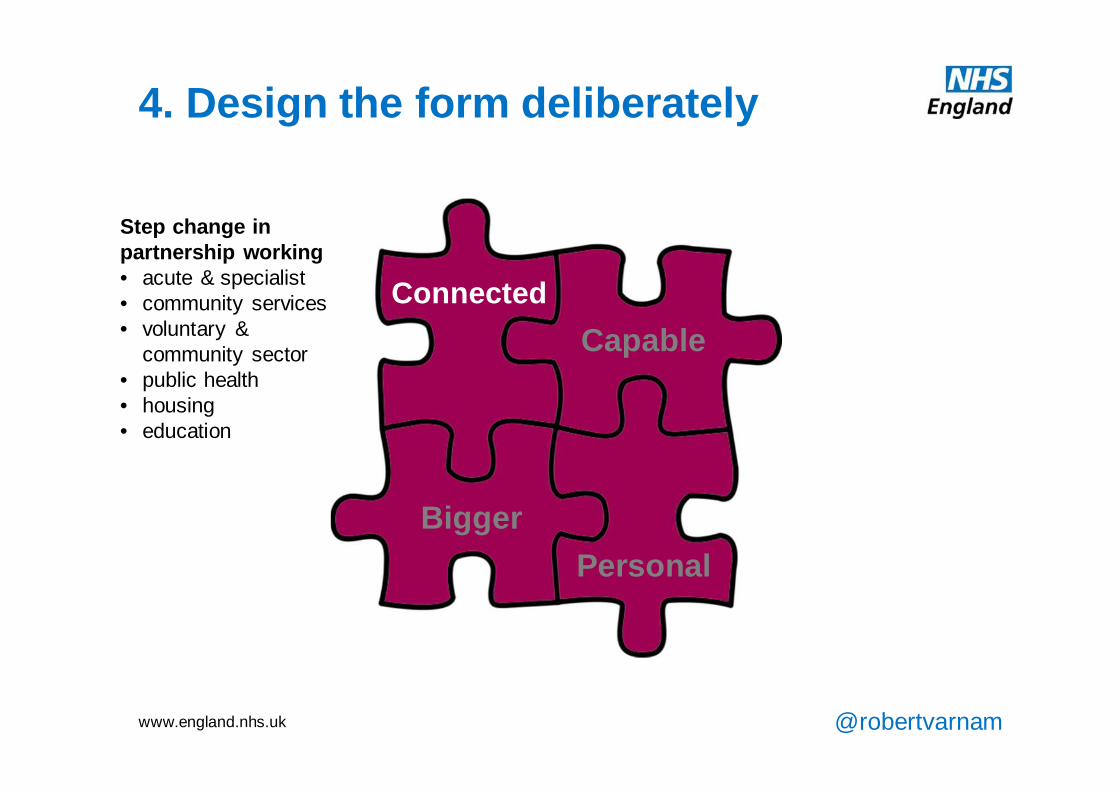
Delivering improved access and expanded care in the community require primary care providers to be working in significantly enhanced partnership with other bodies across the health and care system. In many respects, this will feel like a return to the roots of general practice, acting as an integral part of the local community. However, realising this promise in the present day will involve a great deal of work to establish strategic relationships and formal partnerships.
At an organisational level, what will wider primary care at scale look like? Again, the precise details should be locally determined. But we should aim for it to be bigger, in a way that brings real patient to patients and staff, not just creating a new organisation because it makes us feel safer. Our new networks, federations or mergers should have enhanced capabilities, for leadership, management, services and improvement. We also need to ensure that, as we operate at large scale, we maintain the personal care which is so hugely important for many patients (and staff). That will take deliberate design: it won’t just happen. Finally, it should like it’s ‘yours’ – by which I mean that staff will need to have the same sense of belonging, ownership and commitment as in the best practices now. Regardless of the actual business model. That, too, will take planning and skill.
4. Design the form deliberately
BiggerPersonal
CapableConnected
Step change in partnership working• acute & specialist• community services• voluntary &
community sector• public health• housing• education
www.england.nhs.uk @robertvarnam
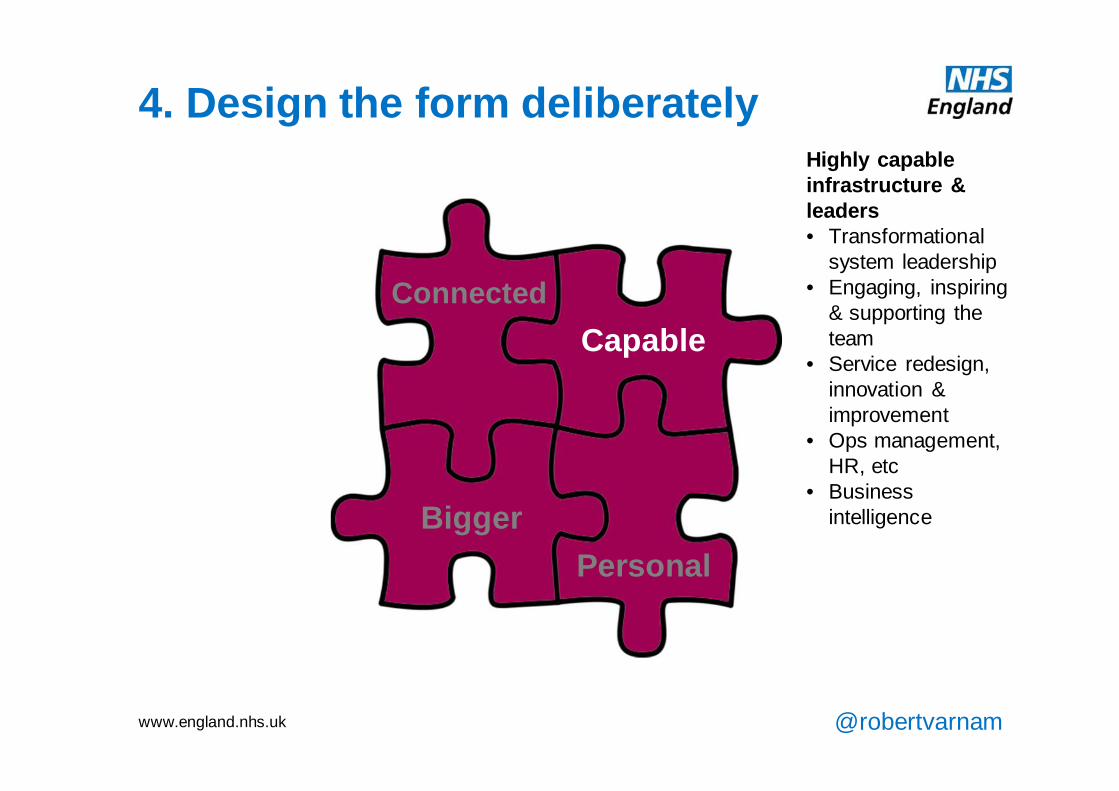
The creation and ongoing delivery of enhanced 7 day services in the community will require a range of capabilities in providers. Leading service transformation and working at greater scale will involve a new corporate infrastructure, with specialised professional management and exceptional clinical leadership. Traditionally general practice has operated much more on the basis of goodwill and hard work than is appropriate for at-scale operations. The NHS has not invested in developing leadership, management and business capabilities in primary care, but this is now a significant and pressing requirement before enhanced services or improved access can be delivered.
At an organisational level, what will wider primary care at scale look like? Again, the precise details should be locally determined. But we should aim for it to be bigger, in a way that brings real patient to patients and staff, not just creating a new organisation because it makes us feel safer. Our new networks, federations or mergers should have enhanced capabilities, for leadership, management, services and improvement. We also need to ensure that, as we operate at large scale, we maintain the personal care which is so hugely important for many patients (and staff). That will take deliberate design: it won’t just happen. Finally, it should like it’s ‘yours’ – by which I mean that staff will need to have the same sense of belonging, ownership and commitment as in the best practices now. Regardless of the actual business model. That, too, will take planning and skill.
4. Design the form deliberately
BiggerPersonal
CapableConnected
Highly capable infrastructure & leaders• Transformational
system leadership• Engaging, inspiring
& supporting the team
• Service redesign, innovation & improvement
• Ops management, HR, etc
• Business intelligence
www.england.nhs.uk @robertvarnam
All of the above requires primary care to operate at larger scale. This may provide economies of scale which will sustain providers through the current workload challenges. More fundamentally, working at-scale is necessary to generate the kind of critical mass required for working in greater partnership as a credible system partner in the local health and care system. In operational terms, it allows financial and staff headroom to be created, making service improvement easier, and it increases the attractiveness of primary care as an employer for staff from other parts of the health and care system.
At an organisational level, what will wider primary care at scale look like? Again, the precise details should be locally determined. But we should aim for it to be bigger, in a way that brings real patient to patients and staff, not just creating a new organisation because it makes us feel safer. Our new networks, federations or mergers should have enhanced capabilities, for leadership, management, services and improvement. We also need to ensure that, as we operate at large scale, we maintain the personal care which is so hugely important for many patients (and staff). That will take deliberate design: it won’t just happen. Finally, it should like it’s ‘yours’ – by which I mean that staff will need to have the same sense of belonging, ownership and commitment as in the best practices now. Regardless of the actual business model. That, too, will take planning and skill.
4. Design the form deliberately
BiggerPersonal
CapableConnected
At-scale organisational form• Attractive system
partner• Sustainable platform
for expanded services
• Intrinsic headroom• Credible NHS
employer
www.england.nhs.uk @robertvarnam
In the course of the transition to being more corporate entities, it will be important for primary care providers to include measures to preserve and even enhance aspects of the status quo which are essential to the value of primary care. The role of primary care at the heart of the local community, and connected with people and their families throughout their life, is a valuable aspect of its ability to contribute to wellbeing and population health. Similarly, the personal continuity of care provided in general practice adds considerable value to patients with complex needs as well as to taxpayers. Finally, the small scale nature of traditional practices creates a level of personal commitment and discretionary effort which the NHS can ill afford to lose.
It should be noted that all three of these potential benefits of the traditional ‘cottage industry’ model of primary care organisations are already waning in England. Patients at larger GP practices already report lower satisfaction with continuity of care, and there are growing concerns about the disenfranchisement of many salaried GPs.
Providers will need to ensure there are specific measures in place to ensure that the personal touch is not only preserved but enhanced. This is likely to have implications for ownership models, organisational culture, structures and processes, as well as the design of teams and clinical care models.
At an organisational level, what will wider primary care at scale look like? Again, the precise details should be locally determined. But we should aim for it to be bigger, in a way that brings real patient to patients and staff, not just creating a new organisation because it makes us feel safer. Our new networks, federations or mergers should have enhanced capabilities, for leadership, management, services and improvement. We also need to ensure that, as we operate at large scale, we maintain the personal care which is so hugely important for many patients (and staff). That will take deliberate design: it won’t just happen. Finally, it should like it’s ‘yours’ – by which I mean that staff will need to have the same sense of belonging, ownership and commitment as in the best practices now. Regardless of the actual business model. That, too, will take planning and skill.
4. Design the form deliberately
BiggerPersonal
CapableConnected
Deliberate design to stay personal• Lifelong family care• Integral part of the
community• Personal LTC & EOL
care• Sense of commitment
& ownership for all staff

















![Selenide Alternative in Practice - Implementation & Lessons learned [SeleniumCamp 2016]](https://img.pdfslide.us/doc/110x75/586fd51a1a28ab18428b4a75/selenide-alternative-in-practice-implementation-lessons-learned-seleniumcamp.jpg)