Embed Size (px)
Citation preview

CHAPTER 6
The Foramen Magnum
Albert L. Rhoton, Jr., M.D.Department of Neurological Surgery, University of Florida, Gainesville, Florida
Key words: Cranial nerves, Craniovertebral junction, Foramen magnum, Microsurgery, Vertebral artery
The foramen magnum is located in the occipital bone,which has three parts: a squamosal part located behindthe foramen magnum; a basal (clival) portion located
anterior to the foramen magnum; and a condylar part thatconnects the squamosal and clival parts (Fig. 6.1). The suboc-cipital approaches are directed through the squamosal partand the anterior approaches through the clival part. The con-dylar part, which includes the occipital condyle, posteriormargin of the jugular foramen, and hypoglossal canal, isexposed in the far-lateral approach and its transcondylar,retrocondylar, and supracondylar modifications described inthe chapter on the far lateral approach. Structures involved inforamen magnum lesions include the lower cranial and upperspinal nerves, the caudal brainstem and rostral spinal cord,the vertebral artery and its branches, the veins and duralsinuses at the craniovertebral junction, and the ligaments andmuscles uniting the atlas, axis, and occipital bone (5, 26). Theforamen magnum is most commonly approached from pos-teriorly through the suboccipital and upper cervical region orfrom anteriorly through the nasal and oral cavities, the phar-ynx, or maxilla.
THE FORAMEN MAGNUM
Osseous relationships
The osseous structures that must be considered in planningan approach to the region of the foramen magnum are theoccipital bone, the atlas, and the axis.
Occipital boneThe occipital bone surrounds the foramen magnum (Fig.
6.1). The foraminal opening is oval shaped and is widerposteriorly than anteriorly. The wider posterior part transmitsthe medulla, and the narrower anterior part sits above theodontoid process. The occipital bone is divided into a squa-mosal part located above and behind the foramen magnum, abasal part situated in front of the foramen magnum, andpaired condylar parts located lateral to the foramen magnum.
The squamous part is an internally concave plate locatedabove and behind the foramen magnum. Its upper marginsarticulate with the parietal bones at the lambdoid sutures andits lower margins articulate with the mastoid portion of the
temporal bones at the occipitomastoid sutures. The convexexternal surface has several prominences on which the mus-cles of the neck attach. The largest prominence, the externaloccipital protuberance or inion, is situated at the central partof the external surface. The inion is located an average of 1 cmbelow the apex of the internal occipital protuberance and theinferior margin of the confluence of the sagittal and transversesinuses. Two parallel ridges radiate laterally from the protu-berance: the highest nuchal line is the upper and thinnerridge, and the superior nuchal line is the lower and moreprominent one. The area below the nuchal lines is rough andirregular and serves as the site of attachment of numerousmuscles. A vertical ridge, the external occipital crest, descendsfrom the external occipital protuberance to the midpoint ofthe posterior margin of the foramen magnum. The inferiornuchal lines run laterally from the midpoint of the crest.
The internal surface of the squamous part is concave andhas a prominence, the internal occipital protuberance, near itscenter. The internal surface is divided into four unequal fos-sae by the sulcus of the superior sagittal sinus that extendsupward from the protuberance, the internal occipital crest, aprominent ridge that descends from the protuberance, and thepaired sulci for the transverse sinuses that extend laterallyfrom the protuberance. The sulcus for the right transversesinus is usually larger than the one on the left. The upper twofossae are adapted to the poles of the occipital lobes. Theinferior two fossae conform to the contours of the cerebellarhemispheres. The internal occipital crest bifurcates above theforamen magnum to form paired lower limbs, which extendalong each side of the posterior margin of the foramen. Adepression between the lower limbs, the vermian fossa, isoccupied by the inferior part of the vermis. The falx cerebelliis attached along the internal occipital crest.
The basilar part of the occipital bone, which is also referredto as the clivus, is a thick quadrangular plate of bone thatextends forward and upward, at an angle of about 45° fromthe foramen magnum. It joins the sphenoid bone at the sphe-noccipital synchondrosis just below the dorsum sellae (7). Thesuperior surface of the clivus is concave from side to side andis separated on each side from the petrous part of the tempo-ral bone by the petroclival fissure. This fissure has the inferiorpetrosal sinus on its upper surface and ends posteriorly at thejugular foramen. On the inferior surface of the basilar part, in
S155Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

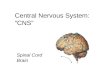
FIGURE 6.1. Occipital bone and foramen magnum. A, inferior view. B, posteroinferior view. C, anterior-inferior view. D,superior view. E, posterosuperior view. F, oblique posterosuperior view. The occipital bone surrounds the oval-shaped fora-men magnum, which is wider posteriorly than anteriorly. The narrower anterior part sits above the odontoid process and itencroached on from laterally by the occipital condyles. The wider posterior part transmits the medulla. The occipital bone isdivided into a squamosal part located above and behind the foramen magnum; a basal (clival) part situated in front of theforamen magnum; and paired condylar parts located lateral to the foramen magnum. The squamous part is internally con-cave. Its upper margin articulates with the parietal bone at the lambdoid suture, and its lower margin articulates with themastoid portion of the temporal bone at the occipitomastoid suture. The convex external surface of the squamosal part hasseveral prominences. The largest prominence, the external occipital protuberance (inion), is situated at the central part of the
S156 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

front of the foramen magnum, a small elevation, the pharyn-geal tubercle, gives attachment to the fibrous raphe of thepharynx.
The paired lateral or condylar parts are situated at the sidesof the foramen magnum. The occipital condyles, which artic-ulate with the atlas, protrude from the external surface of thispart. These condyles are located lateral to the anterior half ofthe foramen magnum. They are oval in shape, convex down-ward, face downward and laterally, and have their long axesdirected forward and medially. A tubercle that gives attach-ment to the alar ligament of the odontoid process is situatedon the medial side of each condyle. The hypoglossal canal,which transmits the hypoglossal nerve, is situated above thecondyle, and is directed forward and laterally from the pos-terior cranial fossa. The canal may be partially or completelydivided by a bony septum. Septated hypoglossal canals werefound on one or both sides in 6% of the dry skulls (15).
The condylar fossa, a depression located on the externalsurface behind the condyle, is often perforated to form theposterior condylar canal through which an emissary veinconnects the vertebral venous plexus with the sigmoid sinus.One or both condylar foramina may be absent or incompletelyperforated (9). The jugular process, a quadrilateral plate ofbone, extends laterally from the posterior half of the condyleto form the posterior border of the jugular foramen. It servesas a bridge between the condylar and squamosal portions ofthe occipital bone. The jugular process articulates laterallywith the jugular surface of the temporal bone. On the intra-cranial surface of the condylar part an oval prominence, thejugular tubercle, sits just superior to the hypoglossal canaland just medial to the lower extent of the petroclival fissure.The caudal part of the tubercle often presents a shallow fur-row above which the glossopharyngeal, vagus, and accessorynerves course. The groove of the sigmoid sinus curves medi-
ally and forward around an upwardly directed, hook-shapedprocess, on the superior surface of the jugular process, andends at the jugular foramen. The posterior condylar canalopens into the posterior cranial fossa close to the medial endof the groove for the sigmoid sinus.
The jugular foramen is situated lateral and slightly superiorto the anterior half of the condyles. It is bordered posteriorlyby the jugular process of the occipital bone, and anteriorly andsuperiorly by the jugular fossa of the petrous portion of thetemporal bone (14). The foramen sits at the posterior end ofthe petroclival suture. The jugular foramen is divided intotwo parts by the intrajugular processes on the opposing edgesof the petrous and occipital bones, which either join directlyor are connected by a fibrous band. The smaller anteromedialpart, the petrous part, transmits the inferior petrosal sinus,and the larger posterolateral part, the sigmoid part, transmitsthe sigmoid sinus. The intrajugular part, situated along theintrajugular processes, transmits the glossopharyngeal, vagus,and accessory nerves. The enlarged part of the internal jugularvein located within the foramen is referred to as the jugular bulb.The jugular process also serves as the site of attachment of therectus capitis lateralis muscle behind the jugular foramen.
The atlasThe atlas, the first cervical vertebra, differs from the other
cervical vertebrae by being ring shaped and by lacking avertebral body and a spinous process (Fig. 6.2). It consists oftwo thick lateral masses situated at the anterolateral parts ofthe ring. The lateral masses are connected in front by a shortanterior arch and behind by a longer curved posterior arch.The position of the usual vertebral body is occupied by theodontoid process of the axis. The anterior arch is convexedforward and has a median anterior tubercle. The posterior
Š
external surface. The superior nuchal line radiates laterally from the protuberance. A vertical ridge, the external occipitalcrest, descends from the external occipital protuberance to the midpoint of the posterior margin of the foramen magnum.The inferior nuchal lines run laterally on both sides from the midpoint of the crest. The internal surface of the squamous partis concave and has a prominence, the internal occipital protuberance, near its center. The internal surface is divided into fourunequal fossae by the sulcus of the superior sagittal sinus, the internal occipital crest, and the sulci for the transverse sinuses.The internal occipital crest bifurcates above the foramen magnum to form a V-shaped ridge between the limbs of which isthe vermian fossa. The basilar part of the occipital bone, which is also referred to as the clivus, is a thick quadrangular plateof bone that extends forward and upward to join the sphenoid bone just below the dorsum sellae. The superior surface of theclivus slopes upward from the foramen magnum and is concave from side to side. The clivus is separated on each side fromthe petrous part of the temporal bone by the petroclival fissure that ends posteriorly at the jugular foramen. The occipitomas-toid suture extends posterolateral from the jugular foramen. On the inferior surface of the basilar part, a small elevation, thepharyngeal tubercle, gives attachment to the fibrous raphe of the pharynx. The condylar parts of the occipital bone, on whichthe occipital condyles an located, are situated lateral to the foramen magnum on the external surface. The alar tubercle,which gives attachment to the alar ligament, is situated on the medial side of each condyle. The hypoglossal canal is situatedabove the condyle. The condylar fossa, which may be converted into a foramen for the passage of an emissary vein, islocated behind the condyle. The jugular process of the occipital bone extends laterally from the posterior half of the condyleand articulates with the jugular surface of the temporal bone. The sulcus of the sigmoid sinus crosses the superior surface ofthe jugular process. The jugular foramen is bordered posteriorly by the jugular process of the occipital bone and anteriorlyby the jugular fossa of the petrous temporal bone. The jugular tubercle lies on the internal surface above the hypoglossalcanal. A., artery; Ac., acoustic; Car., carotid; Cond., condyle; Digast., digastric; Ext., external; Fiss., fissure; For., foramen;Hypogl., hypoglossal; Inf., inferior; Jug., jugular; Occipitomast., occipitomastoid; Occip., occipital; Petrocliv., petroclival;Pharyng., pharyngeal; Proc., process; Protrub., protuberance; Sag., sagittal; Sig., sigmoid; Sup., superior; Trans., transverse.
Foramen Magnum S157
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

arch is convex backward and has a median posterior tubercleand a groove on the lateral part of its upper-outer surface inwhich the vertebral artery courses. The groove may be partlyor fully converted into a foramen by a bridge of bone thatarches backward from the posterior edge of the superiorarticular facet of the atlas to its posterior arch. The first cer-vical spinal nerve also lies in the groove, which is locatedbetween the artery and the bone. The upper surface of eachlateral mass has an oval concave facet that faces upward andmedially and articulates with the occipital condyle that facesdownward and laterally. The inferior surface of each lateralmass has a circular, flat, or slightly concave facet that facesdownward, medially, and slightly backward, and it articu-lates with the superior articular facet of the axis. The medialaspect of each lateral mass has a small tubercle for the attach-ment of the transverse ligament of the atlas, which passesbehind the dens. Each transverse foramen, which transmits avertebral artery, and upon which the nerve root sits, is situ-ated between the lateral mass and the transverse process.
The axisThe axis, the second cervical vertebra, more closely resem-
bles the typical vertebrae than the atlas, but is distinguishedby the odontoid process (dens), which projects upward fromthe body (Fig. 6.2). The dens is 1.0- to 1.5-cm long, and
approximately 1-cm wide. On the front of the dens is anarticular facet that forms a joint with the facet on the back ofthe anterior arch of the atlas. The dens has a pointed apex thatis joined by the apical ligament, has a flattened side where thealar ligaments are attached, and is grooved at the base of itsposterior surface where the transverse ligament of the atlaspasses. The dens and body are flanked by a pair of large ovalfacets that extend laterally from the body onto the adjoiningparts of the pedicles and articulate with the inferior facets ofthe atlas. The superior facets do not form an articular pillarwith the inferior facets, but are anterior to the latter. Theanterior aspect of the body is hollowed out on each side ofthe midline in the area where the longus colli muscles at-tach. The lamina are thicker than on any other cervical verte-brae, the pedicles are stout, and the spinous process is large.
The transverse processes of the axis are small. Their blunttips present a single tubercle, the anterior tubercle, situated ator near the junction of the anterior root of the transverseprocess and the body. Each transverse foramen faces supero-laterally, thus permitting the lateral deviation of the vertebralartery as it passes up to the more widely separated transverseforamina in the atlas. The inferior articular facets are situatedat the junction of the pedicles and laminae, and face down-ward and forward. The spade-shaped vertebral foramen isrelatively large.
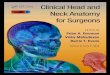
FIGURE 6.2. A–D. The atlas. A, superior view; B, inferior view; C, anterior view; D, posterior view. The atlas consists of twothick lateral masses situated at the anteromedial part of the ring, which are connected in front by a short anterior arch andposteriorly by a longer curved posterior arch. The anterior and posterior tubercles are at the anterior and posterior mid-line. The superior articular facet is an oval, concave facet that faces upward and medially to articulate with the occipital con-dyle. The inferior articular facet is a circular, flat, or slightly concave facet that faces downward, medially, and slightly back-ward and articulates with the superior articular facet of the axis. The medial aspect of each lateral mass has a small tuberclefor the attachment of the transverse ligament of the atlas. The transverse process projects from the lateral masses. The trans-verse foramina transmit the vertebral arteries. The upper surface of the posterior arch adjacent to the lateral masses haspaired grooves in which the vertebral arteries course. A., artery; Ant., anterior; Art., articular; For., foramen; Lat., lateral;Mass., masses; Post., posterior; Proc., process; Trans., transverse; Vert., vertebral.
S158 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

The atlantoaxial jointsThe articulation of the atlas and axis comprises four syno-
vial joints: two median ones on the front and back of the dens,and paired lateral ones between the opposing articular facetson the lateral masses of the atlas and axis (Figs. 6.2-6.4). Eachof the median joints, situated on the front and back of the dens,has its own fibrous capsule and synovial cavity. The anterior oneis situated between the anterior surface of the dens and theposterior aspect of the anterior arch of the atlas. The posteriorone has an even larger synovial cavity and lies between thecartilage-covered anterior surface of the transverse ligament ofthe atlas and the posterior surface of the dens.
The atlas and axis are united by the cruciform ligament, theanterior and posterior longitudinal ligaments, and the articu-lar capsules surrounding the joints between the opposingarticular facets on the lateral masses. The cruciform ligament has
transverse and vertical parts that form a cross behind the dens.The transverse part, called the transverse ligament, is a thickstrong band that arches across the ring of the atlas behind thedens and divides the vertebral canal into a larger posteriorcompartment containing the dura and the spinal cord and asmaller anterior compartment containing the odontoid process.The transverse ligament is broader in the middle behind thedens than at the ends where it is attached to a tubercle on themedial side of the lateral masses of the atlas. As it crossesthe dens, small longitudinal bands are directed upward anddownward from its posterior surface. The cranial extension isattached to the upper surface of the clivus between the apicalligament of the dens and the tectorial membrane. The lowerband is attached to the posterior surface of the body of the axis.The neck of the dens is constricted where it is embraced poste-riorly by the transverse ligament.
FIGURE 6.2. E–H. The axis. E, anterior view; F, lateral view; G, superior view; H, inferior view. The axis is distinguished by theodontoid process (dens). On the front of the dens is an articular facet that forms a joint with the facet on the back of the anteriorarch of the atlas. The dens is grooved at the base of its posterior surface where the transverse ligament of the atlas passes. The ovalsuperior articular facets articulate with the inferior facets of the atlas. The superior facets are anterior to the inferior facets. Thepedicles and laminae are thicker than on the other cervical vertebra and the lamina fuse behind to form a large spinous process.The transverse foramina are directed superolaterally, thus permitting the lateral deviation of the vertebral arteries as they pass upto the more widely separated transverse foramina in the atlas. The inferior articular facets face downward and forward.
Foramen Magnum S159
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

In front, the atlas and axis are connected by the anteriorlongitudinal ligament, which is a wide band fixed above tothe lower border of the anterior arch of the atlas and belowto the front of the body of the axis. The posterior longitudinalligament is attached below to the posterior surface of the body
of the axis, and above to the transverse part of the cruciformligament and the clivus. Posterior to the spinal canal, the atlasand axis are joined by a broad, thin membrane in series withthe ligamentum flavum that is attached above to the lowerborder of the posterior arch of the atlas, and below to the
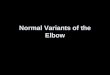
FIGURE 6.3. A–D. Foramenmagnum. Posterior view. Stepwisedissection. A, the cerebellar tonsils,the foramen of Magendie, and lowerpart of the fourth ventricle aresituated above the foramen magnum.The vertebral artery penetrates thedura below the foramen magnum andascends through the foramen in frontof the dentate ligament and accessorynerves. The glossopharyngeal, vagus,and accessory nerves pass throughthe jugular foramen, which is locatedlateral to the anterior half of theforamen magnum. B, the cerebellumhas been removed. The vertebralarteries pass through the foramenmagnum to reach the front of themedulla. C, enlarged view of the lefthalf of the foramen magnum. Thevertebral artery passes behind andbelow the atlanto-occipital joint,penetrates the dura, and passes infront of the dentate ligament andaccessory nerve. The rostral end ofthe dentate ligament attaches tothe dura at the level of the foramenmagnum. The C1 nerve penetratesthe dura with the vertebral artery.The hypoglossal nerve passes behindthe vertebral artery and enters thehypoglossal canal. The hypoglossalnerve is separated into severalbundles as it penetrates the dura. Theposterior spinal artery arises as thevertebral artery enters the dura andgives rise to ascending anddescending branches. D, alongitudinal strip of the medulla andfloor of the fourth ventricle has beenremoved to expose thevertebrobasilar junction, the origin ofthe anterior spinal artery, andthe median anterior medullary andmedian anterior spinal veins. A.,artery; A.I.C.A., anteroinferiorcerebellar artery; Ant., anterior; Asc.,ascending; Atl., atlanto-; Bas., basilar;Br., branch; Bridg., bridging; CN,
cranial nerve; Cruc., cruciform; Dent., dentate; Desc., descending; Flocc., flocculus; For., foramen; Horiz., horizontal; Lig.,ligament; Med., median, medullary; Memb., membrane; Men., meningeal; Occip., occipital; P.I.C.A., posteroinferior cerebellarartery; Post., posterior; Sp., spinal; Trans., transverse; V., vein; Vent., ventricle; Vert., vertebral.
S160 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

upper edges of the laminae of the axis. This membrane ispierced laterally by the second cervical nerve.
The atlanto-occipital jointsThe atlas and the occipital bone are united by the articular
capsules surrounding the atlanto-occipital joints and by the
anterior and posterior atlanto-occipital membranes (Figs. 6.2-6.4). The articular capsules of the atlanto-occipital joints aresometimes deficient medially where the synovial cavities maycommunicate with the synovial bursa between the dens andthe transverse ligament of the atlas. The anterior atlanto-occipital membrane is attached superiorly to the anterior edge
FIGURE 6.3. E–I. Foramenmagnum. Posterior view.Stepwise dissection. E, theright half of the medulla hasbeen removed. The anteriorspinal artery arises predomi-nantly from the left vertebralartery, but has a small contri-bution from the right verte-bral artery. Two bundles ofright hypoglossal rootletspenetrate the dura. F, en-larged view. The medulla hasbeen removed to expose thevertebral and anterior spinalarteries. The C1 nerve rootspenetrate the dura with thevertebral artery. G, the intra-dural segment of the verte-
bral arteries and the dura lining the anterior margin of the foramen magnum have been removed to expose the tectorial mem-brane, a rostral extension of the posterior longitudinal ligament, and the vertebral venous plexus, which courses just outside thedura. H, the tectorial membrane has been removed to expose the cruciform and alar ligaments. The horizontal portion of the cru-ciform ligament, called the transverse ligament of the atlas, extends laterally to be attached to the medial edges of the lateralmasses of the atlas, and the vertical portion ascends to attach to the anterior margin of the foramen magnum deep to the tectorialmembrane. The alar ligaments pass upward and laterally and attach to the lateral edges of the foramen magnum. Anterior menin-geal arteries pass along the dura and ligamentous structures in the anterior spinal canal. I, the vertical portion of the cruciform lig-ament has been folded downward to expose the synovial joint between the anterior surface of the cruciform ligament and the pos-terior surface of the dens. There is also another synovial joint between the anterior surface of the dens and the posterior surface ofthe anterior atlantal arch. The apical ligament of the dens extends upward to be attached to the margin of the foramen magnum.
Foramen Magnum S161
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.4. Anterior view. Stepwise dissection of a cross section showing the relationship of the foramen magnum and cli-vus to the nasal and oral cavities, pharynx, and infratemporal fossa. A, the soft palate, which has been preserved, is locatedat the level of the foramen magnum. The infratemporal fossa, located below the greater sphenoid wing and middle cranialfossa, contains the pterygoid muscles, maxillary artery, mandibular nerve branches, and the pterygoid venous plexus andopens posteriorly into the area around the carotid sheath, as shown on the left side. B, enlarged view. The soft palate hasbeen divided in the midline and the leaves reflected laterally. The atlanto-occipital joints and the foramen magnum arelocated at approximately the level of the hard palate. The anterior arch of C1 and the dens are located behind the orophar-ynx, and the clivus is located behind the nasopharynx and sphenoid sinus. The prominence over the longus capitis and the
S162 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

of the foramen magnum, inferiorly to the superior edge of theanterior arch of the atlas, and laterally to the capsule ofthe atlanto-occipital joints.
The posterior atlanto-occipital membrane is a thin sheet con-nected above to the posterior margin of the foramen magnumand below to the upper border of the posterior arch of the atlas.The lateral border of the membrane is free and arches behind thevertebral artery and the first cervical nerve root. The lateral edgeof this membrane may be ossified in the area where it archesover the posterior aspect of the vertebral artery, thus creating apartial or complete osseous ring around the artery on the medialside of the atlanto-occipital joint.
Axis and occipital boneFour fibrous bands, the tectorial membrane, the paired alar
ligaments, and the apical ligament, connect the axis and theoccipital bone (Figs. 6.3 and 6.4). The tectorial membrane is acephalic extension of the posterior longitudinal ligament thatcovers the dens and cruciform ligament. It is attached belowto the posterior surface of the body of the axis, above to theupper surface of the occipital bone in front of the foramenmagnum, and laterally to the medial sides of the atlanto-occipital joints. The alar ligaments are two strong bands thatarise on each side of the upper part of the dens and extendobliquely superolateral to attach to the medial surfaces of theoccipital condyles. The apical ligament of the odontoid pro-cess extends from the tip of the dens to the anterior margin ofthe foramen magnum and is situated between the anterioratlanto-occipital membrane and the superior prolongation ofthe cruciform ligament.
Muscular relationships
The foramen magnum is surrounded by the muscles at-tached to the occipital bone and upper cervical vertebrae (Figs.6.4 and 6.5). The trapezius covers the back of the head andneck. It extends from the medial half of the superior nuchalline, the external occipital protuberance, and the spinous pro-cesses of the cervical and thoracic vertebrae and converges on
the shoulder to attach to the scapula and the lateral third ofthe clavicle. The sternocleidomastoid passes obliquely down-ward across the side of the neck from the lateral half of thesuperior nuchal line and mastoid process to the upper part ofthe sternum and the adjacent part of the clavicle. This muscledivides the side of the neck into an anterior triangle and aposterior triangle. The anterior triangle is bounded posteri-orly by the anterior border of the sternocleidomastoid, aboveby the mandible, and anteriorly by the median line of theneck; the posterior triangle is bounded in front by the poste-rior border of the sternocleidomastoid, below by the middlethird of the clavicle, and behind by the anterior margin of thetrapezius. The splenius capitis, situated deep to and partiallycovered by the trapezius and sternocleidomastoid, extendsfrom the bone below the lateral third of the superior nuchalline to the spinous processes of the lower cervical and upperthoracic vertebrae. Two muscles, both of which are situateddeep to the splenius capitis and sternocleidomastoid and at-tach below to the upper thoracic and lower cervical vertebrae,are the semispinalis capitis, which attaches above in the areabetween the superior and inferior nuchal lines beginningmedially at the external occipital crest and extending laterallyto the occipitomastoid junction, and the longissimus capitismuscle, which attaches above to the posterior margin of themastoid process.
The suboccipital muscles, located in the next layer, are a groupof muscles situated deep to the splenius, semispinalis, and lon-gissimus capitis in the suboccipital area. This group includes thesuperior oblique, which extends from the area lateral to thesemispinalis capitis between the superior and inferior nuchallines to the transverse process of the atlas; the inferior oblique,which extends from the spinous process and lamina of the axisto the transverse process of the atlas; the rectus capitis posteriormajor, which extends from and below the lateral part of theinferior nuchal line to the spine of the axis; and the rectuscapitis posterior minor, which is situated medial to and ispartially covered by the rectus capitis posterior major, extends
Š
anterior arch of C1 are seen through the pharyngeal mucosa. C, the mucosa lining the posterior pharyngeal wall has beenreflected to the right, exposing the longus capitis that attaches to the clivus and the part of the longus colli that attaches tothe anterior arch of C1. The eustachian tube has been divided. The rectus capitis anterior extends from the transverse processof C1, posterolateral to the longus capitis, to attach to the occipital bone in front of the occipital condyle. D, the clivus andanterior arch of C1 have been removed. The dura has been opened to expose the vertebral and basilar artery. The dens hasbeen preserved. The structures in the right infratemporal fossa and part of the right carotid artery and mandible have beenremoved to expose the right vertebral artery ascending between the C2 and C1 transverse processes. E, enlarged view of thestep between C and D. The anterior arch of C1 has been removed to expose the odontoid process and the lower part of theclivus. The left longus coli and longus capitis have been reflected out of the exposure. The atlanto-occipital joint is exposed atthe level of the odontoid apex. The transverse part of the cruciform ligament, also called the transverse ligament, extendsacross the back of the dens and attaches to a tubercle on the medial side of each lateral mass of the axis. The tectorial mem-brane, a cephalic extension of the posterior longitudinal ligament, lines the posterior clival surface. The alar ligaments attachto the lateral edges of the foramen magnum. F, enlarged view of the exposure shown in D. G, exposure after opening of theclivus. Both vertebral and anteroinferior cerebellar arteries (AICAs) and the anterior spinal artery are exposed. A., artery;A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Atl., atlanto-; Cap., capitis; Car., carotid; CN, cranial nerve; Eust.,eustachian; For., foramen; Infratemp., infratemporal; Int., internal; Jug., jugular; Lat., lateral; Lig., ligament; Long., longus; M.,muscle; Mandib., mandibular; Max., maxillary; Med., medial; Memb., membrane; Occip., occipital; Pteryg., pterygoid; Rec.,rectus; Sp., spinal; Sphen., sphenoid; Trans., transverse; Vert., vertebral.
Foramen Magnum S163
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.5. Suboccipital muscles. Stepwise dissection. A, the right trapezius and sternocleidomastoid have been preserved.The left trapezius and sternocleidomastoid have been reflected along with the galea aponeurotica to expose the underlyingsemispinalis capitis, splenius capitis, and levator scapulae. B, the right sternocleidomastoid and trapezius have been reflectedto expose the splenius capitis. The left splenius capitis has been removed to expose the underlying semispinalis and longissi-mus capitis. C, the right splenius capitis has been removed to expose the semispinalis and longissimus capitis. The left semi-spinalis and longissimus capitis have been removed to expose the suboccipital triangle formed by the superior oblique, whichpasses from the C1 transverse process to the occipital bone, the inferior oblique, which extends from the transverse processof C1 to the spinous process of C2, and the rectus capitis posterior major, which extends from the occipital bone below theinferior nuchal line to the spinous process of C2. The vertebral artery courses in the depths of the suboccipital triangle as itpasses behind the superior facet of C1 and across the upper edge of the posterior atlantal arch. D, both semispinalis capitismuscles have been reflected laterally to expose the suboccipital triangles bilaterally. E, the muscles forming the left suboccipi-tal triangle have been removed. The vertebral artery ascends slightly lateral from the transverse process of C2 to reach the
S164 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

from the medial part and below the inferior nuchal line to thetubercle on the posterior arch of the atlas.
The suboccipital triangle is a region bounded above andmedially by the rectus capitis posterior major, above andlaterally by the superior oblique, and below and laterally bythe inferior oblique (Fig. 6.5). It is covered by the semispinaliscapitis medially and by the splenius capitis laterally. The floorof the triangle is formed by the posterior atlanto-occipitalmembrane and the posterior arch of the atlas. The structuresin the triangle are the terminal extradural segment of thevertebral artery and the first cervical nerve.
The platysma is a broad sheet extending downward fromthe lower part of the face and across the clavicle to the fasciacovering the pectoralis major and deltoid. The anterior verte-bral muscles insert on the clival part of the occipital boneanterior to the foramen magnum. This group includes thelongus colli, which attach to the anterior surface of the verte-bral column between the atlas and the third thoracic vertebra;the longus capitis, which extends from the clivus in front ofthe foramen magnum to the transverse processes of the thirdthrough the sixth cervical vertebrae; the rectus capitis ante-rior, which is situated behind the upper part of the longuscapitis and extends from the occipital bone in front of theoccipital condyle to the anterior surface of the lateral massand transverse process of the atlas; and the rectus capitislateralis, which extends from the jugular process of the occip-ital bone to the transverse process of the atlas.
The muscles described above are embedded in the cervicalfascia. This fascia is divided into superficial and deep layers.The superficial layer is a lamina of loose connective tissuebelow the dermis, which invests the platysma. The deep layerlies internal to the platysma, invests the muscles, and con-denses into fibrous sheaths that bind the arteries and accom-panying veins together. The superficial lamina of the deepfascia attaches in the posterior midline to the ligamentumnuchae, thinly invests the trapezius, continues forward cov-ering the posterior triangle of the neck, divides at the poste-rior border of the sternocleidomastoid to enclose the muscle,and at its anterior margin again forms a lamina that covers theanterior triangle of the neck and reaches the median plane, tobe continuous with the corresponding lamina from the oppo-site side. The carotid sheath is a condensation of the cervicalfascia, which invests the common and internal carotid arter-ies, the internal jugular vein, and the vagus nerve. The pre-vertebral lamina of the cervical fascia covers the prevertebralmuscles, extends laterally to connect with the carotid sheath,and covers the scalene muscles to form a fascial floor for the
posterior triangle of the neck. Superiorly it is attached to thebase of the skull, and inferiorly it continues downward be-hind the pharynx and in front of the longus colli into thesuperior mediastinum. The deep fascia is fused above tothe superior nuchal line, mastoid process, zygomatic arch,styloid process, and mandible, and below to the scapula,clavicle, and sternum.
Neural relationships
The neural structures situated in the region of the foramenmagnum are the caudal part of the brainstem, cerebellum andfourth ventricle, the rostral part of the spinal cord, and the lowercranial and upper cervical nerves (Figs. 6.3 and 6.6) (5, 19).
Spinal cordThe spinal cord blends indistinguishably into the medulla
at a level arbitrarily set to be at the upper limit of the dorsaland ventral rootlets forming the first cervical nerve (Figs. 6.3and 6.6). It is easier to differentiate this level on the ventralthan on the dorsal surface because the ventral rootlets of thefirst cervical nerve are always present, whereas the dorsalrootlets are absent in many cases. The fact that the junction ofthe spinal cord and medulla is situated at the rostral margin ofthe first cervical root means that the medulla, and not thespinal cord, occupies the foramen magnum.
The spinal cord immediately below the level of the foramenmagnum is round, and it is divided by one fissure and severalsulci. The anteromedian fissure and the posteromedian sulcusdivide the spinal cord into symmetrical halves. The antero-median fissure reaches a depth of several millimeters. The pos-teromedian sulcus is much shallower, and from it the postero-median septum penetrates the spinal cord, almost reaching thecentral canal. The posterior lateral sulcus is situated along theline where the dorsal roots enter the spinal cord. The posteriorfuniculus is situated between the posteromedian and poste-rior lateral sulci. At the upper cervical level, the surface ofeach posterior funiculus is divided by another shallow longi-tudinal furrow, the posterior intermediate sulcus, into thefasciculus gracilis medially and the fasciculus cuneatus later-ally. The region of the spinal cord between the posteriorlateral sulcus and the anteromedian fissure is divided intoanterior and lateral funiculi by the exiting ventral rootlets ofthe spinal nerves. The anterior funiculus includes the zone ofemergence of the ventral roots. The lateral funiculus lies betweenthe ventral roots and the posterior lateral sulcus. In the upper
Š
transverse process of C1 and turns medially behind the superior facet of C1 to reach the upper surface of the posterior arch of C1.The C2 ganglion is located between the posterior arch of C1 and the lamina of C2. The dorsal ramus of C2 produces a medialbranch that forms the majority of the greater occipital nerve. F, the muscles forming both suboccipital triangles have beenremoved. The rectus capitis posterior minor, which extends from the posterior arch of C1 to the occipital bone below the inferiornuchal line, has been preserved. The vertebral arteries cross the posterior arch of the atlas and penetrate the posterior atlanto-occipital membrane to reach the dura. A., artery; Atl., atlanto-; Cap., capitis; Car., carotid; CN, cranial nerve; Inf., inferior; Int.,internal; Jug., jugular; Lev., levator; Longiss., longissimus; M., muscle; Maj., major; Memb., membrane; Min., minor; Obl., oblique;Occip., occipital; Post., posterior; Proc., process; Rec., rectus; Scap., scapulae; Semispin., semispinalis; Spin., spinalis; Splen., sple-nius; Sternocleidomast., sternocleidomastoid; Sup., superior; Trans., transverse; V., vein; Vert., vertebral.
Foramen Magnum S165
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.6. Foramen magnum. A–D, posterior views; E and F, anterior views. A, a suboccipital craniectomy and upper cer-vical laminectomy exposes the dura. The vertebral arteries pass medially across the upper surface of the atlas where they giveoff the posterior meningeal arteries that ascend to supply the dura on the posterior aspect of the foramen magnum and poste-rior fossa. Insert, upper right. The upper margin of the left half of the arch of the atlas forms an osseous ring around the ver-tebral artery just proximal to where it enters the dura. B, enlarged view of another foramen magnum after opening the dura.The right PICA arises outside the dura and penetrates the dura with the vertebral artery. The rostral end of the dentate liga-ment passes between the vertebral artery and the PICA to insert into the dura along the lateral margin of the foramen mag-num. The accessory nerve ascends posterior to both the PICA and the vertebral artery. The vertebral artery gives rise to aposterior spinal artery that passes along the posterolateral aspect of the spinal cord and medulla. The hypoglossal rootlets arestretched over the posterior aspect of the vertebral artery. C, the right tonsil has been retracted to expose the caudal end ofthe fourth ventricle, which is located above the foramen magnum. The right PICA ascends through the foramen magnum and
S166 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

cervical region, the rootlets that unite to form the spinal part ofthe accessory nerve emerge through the lateral funiculus.
Dentate ligamentThe dentate ligament is considered with the spinal cord
because it is attached to it (Figs. 6.3 and 6.6). This ligament isa white fibrous sheet that is attached to the spinal cord me-dially and to the dura mater laterally. The medial border ofthe dentate ligament, which is attached to the pia materbetween the dorsal and ventral rootlets along the length ofeach side of the spinal cord, presents a series of triangulartoothlike processes on each side that are attached at intervalsto the dura mater. At the craniocervical junction, the dentateligament is located between the vertebral artery and the ven-tral roots of C1 anteriorly and the branches of the posteriorspinal artery and the spinal accessory nerve posteriorly; inaddition, it is often incorporated into the dural cuff aroundthe vertebral artery at the site of dural penetration. The mostrostral attachment of the dentate ligament is located at thelevel of the foramen magnum, above where the vertebralartery pierces the dura. The ligament courses behind theaccessory nerve at that level, although the dentate ligament islocated anterior to the accessory nerve at lower levels. Thesecond triangular process is attached to the dura below thesite at which the vertebral artery and the roots of C1 pierce thedura. Sectioning the upper two triangular processes will in-crease access anterior to the spinal cord. The first cervicalnerve courses along the posteroinferior surface of the verte-bral artery as it pierces the dura. The ventral root is locatedanterior to the dentate ligament, and the dorsal root, which isinfrequently present, passes posterior to the dentate ligament.There are frequently communications between the C1 nerveroot and the spinal accessory nerve.
BrainstemThe lower medulla blends indistinguishably into the upper
spinal cord at the level of the C1 nerve roots (Figs. 6.3, 6.4, and6.6). The anterior surface of the medulla is formed by themedullary pyramids, which face the clivus, the anterior edgeof the foramen magnum, and the rostral part of the odontoidprocess. The lateral surface is formed predominantly by theinferior olives. The posterior surface of the medulla is dividedinto superior and inferior parts. The superior part is com-posed in the midline of the inferior half of the fourth ventricle,and laterally by the inferior cerebellar peduncles. The inferior
part of the posterior surface is composed of the gracile fascic-ulus and tubercle medially, and the cuneate fasciculus andtubercle laterally.
CerebellumThe suboccipital cerebellar surface rests above the posterior
and lateral edge of the foramen magnum. Only the lower partof the hemispheres formed by the tonsils and the biventrallobules, and the lower part of the vermis formed by thenodule, uvula, and pyramid, are related to the foramen mag-num. The biventral lobule sits above the lateral part of theforamen magnum, and the tonsils rest above the level of theposterior edge (Figs. 6.3 and 6.6). The cerebellar surface abovethe posterior part of the foramen magnum has a deep verticaldepression, the posterior cerebellar incisura, which containsthe falx cerebelli and extends inferiorly toward the foramenmagnum. The tonsils, which sit above the posterior edge ofthe foramen magnum, are commonly involved in herniationsthrough the foramen magnum. Each tonsil is an ovoid struc-ture that is attached along its superolateral border to theremainder of the cerebellum. The cerebellomedullary fissureextends superiorly between the cerebellum and the medullaand is situated rostral to the posterior margin of the foramenmagnum.
Cranial nervesThe accessory nerve is the only cranial nerve that passes
through the foramen magnum (Figs. 6.3 and 6.6). It has acranial part composed of the rootlets that arise from themedulla and join the vagus nerve, and a spinal portionformed by the union of a series of rootlets that arise from thelower medulla and upper spinal cord. In the posterior fossa,the accessory nerve is composed of one main trunk from thespinal cord and three to six small rootlets that emerge fromthe medulla. The most rostral medullary rootlets are function-ally inferior vagal rootlets, since they arise from the vagalnuclei (25). The lower medullary rootlets join the spinal por-tion of the nerve. The upper medullary rootlets enter thejugular foramen without joining the spinal portion, but onceinside the jugular foramen, they join either the vagus oraccessory nerve. The spinal contribution arises from the cer-vical portion of the spinal cord as a series of rootlets situatedmidway between the ventral and dorsal rootlets. The lowestlevel of origin of the rootlets contributing to the accessorynerves was at the C7 root level in 2 of the 50 nerves examined,
Š
along the posterior margin of the medulla to reach the cerebellomedullary fissure. D, another specimen. The rostral end ofthe dentate ligament passes between the posterior spinal artery and vertebral artery and attaches to the dura at the level ofthe foramen magnum. The accessory nerve ascends behind the posterior spinal artery. The C1 nerve root receives a contribu-tion from the accessory nerve and passes through the dura with the vertebral artery and courses along the lower margin ofthe artery. The posterior spinal artery arises inside the dura and passes between the dentate ligament and accessory nerveand gives rise to ascending branches to the medulla and descending branches to the spinal cord. E, the anterior skull base hasbeen removed. The vertebral arteries ascend in front of the brainstem and give rise to the anterior spinal artery. F, enlargedview. The C1 ventral roots penetrate the dura with the vertebral artery. The hypoglossal rootlets pass behind the vertebralarteries. A., artery; Bas., basilar; Cer.Med., cerebellomedullary; CN, cranial nerve; Cond., condyle; Dent., dentate; Fiss., fis-sure; Hypogl., hypoglossal; Lig., ligament; Men., meningeal; Occip., occipital; P.I.C.A., posteroinferior cerebellar artery; Post.,posterior; Sp., spinal; Vert., vertebral.
Foramen Magnum S167
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

C6 in 10, C5 in 13, C4 in 11, C3 in 7, C2 in 5, and Cl in 2 (5).These rootlets unite to form a trunk with a diameter of ap-proximately 1.0 mm, which ascends through the foramenmagnum between the dentate ligament and the dorsal spinalroots to enter the posterior cranial fossa behind the vertebralartery.
Of the 50 accessory nerves examined in our previous study,all had connections with the dorsal roots of the upper cervicalnerves. The most common and largest anastomosis was withthe dorsal root of the first cervical nerve (5, 22). Twenty-eightof the C1 dorsal roots arose solely from the accessory nervewithout there being a contribution from the C1 level of thespinal cord. All of the 15 Cl dorsal roots that received rootletsarising from the spinal cord at the C1 level also had anasto-motic fibers from the accessory nerve. Four of the 50 accessorynerves had an anastomotic connection with the C2 nerve root,10 with the C3, 8 with the C4, and 2 with the C5.
The lower four cranial nerves are sufficiently close to theforamen magnum that they may be involved by lesions aris-ing there (Figs. 6.3 and 6.6). Their intradural anatomy is de-scribed in the chapter of this issue on the cerebellopontineangle and posterior fossa cranial nerves.
Cervical nerve rootsEach dorsal and ventral root is composed of a series of six
to eight rootlets that fan out to enter the posterolateral andanterolateral surfaces of the spinal cord, respectively (Figs. 6.3and 6.6). The dorsal and ventral roots cross the subarachnoidspace and transverse the dura mater separately, then uniteclose to the intervertebral foramen to form the spinal nerves.The rootlets in the region of the foramen magnum pass almostdirectly lateral to reach their dural foramina. The neurons ofthe dorsal roots collect to form ganglia located just proximalto the union of the dorsal and ventral root in the intervertebralforamina, however the first cervical dorsal root and associatedganglion may be absent. The C1, C2, and C3 nerves, distal tothe ganglion, divide into dorsal and ventral rami. The dorsalrami divide into medial and lateral branches that supply theskin and muscles of the posterior region of the neck. The C1nerve, termed the suboccipital nerve, leaves the vertebralcanal between the occipital bone and atlas and has a dorsalramus that is larger than the ventral ramus. The dorsal ramuscourses between the posterior arch of the atlas and the verte-bral artery to reach the suboccipital triangle, where it sendsbranches to the rectus capitis posterior major and minor,superior and inferior oblique, and the semispinalis capitis,and occasionally has a cutaneous branch that accompanies theoccipital artery to the scalp. The C1 ventral ramus coursesbetween the posterior arch of the atlas and the vertebral arteryand passes forward, lateral to the lateral mass of the atlas andmedial to the vertebral artery, and supplies the rectus capitislateralis. The C2 nerve emerges between the posterior arch ofthe atlas and the lamina of the axis where the spinal ganglionis located extradurally, medial to the inferior facet of C1 andthe vertebral artery. Distal to the ganglion, the nerve dividesinto a larger dorsal and a smaller ventral ramus. After passingbelow and supplying the inferior oblique muscle, the dorsal
ramus divides into a large medial and a small lateral branch.It is the medial branch that is most intimately related to thissuboccipital operative field and that forms the greater occip-ital nerve. It ascends obliquely between the inferior obliqueand the semisplenius capitis, pierces the latter and the trape-zius muscle near their attachments to the occipital bone, andis joined by a filament from the medial branch of C3. Itsupplies the semispinalis capitis muscle, ascends with theoccipital artery, and supplies the scalp as far forward as thevertex, and occasionally the back of the ear. The lateral branchsends filaments that innervate the splenius, longissimus, andsemisplenius capitis, and is often joined by the correspondingbranch from the C3 nerve. The C2 ventral ramus coursesbetween the vertebral arches and transverse processes of theatlas and axis and behind the vertebral artery to leave thisoperative field. Two branches of the C2 and C3 ventral rami,the lesser occipital and greater auricular nerves, curve aroundthe posterior border and ascend on the sternocleidomastoidmuscle to supply the skin behind the ear.
The first cervical nerve, located just below the foramenmagnum, deserves special attention (Figs. 6.3 and 6.6). Itdiffers from the other cervical nerves in the consistency andorigin of the dorsal rootlets forming the nerve. The C1 ventralroot is composed of four to eight rootlets that joined andcoursed laterally. Before entering the dural foramina, the C1ventral root, and the corresponding dorsal root if present,attaches to the posteroinferior surface of the initial intraduralpart of the vertebral artery, and both exit the dural sacthrough the funnel-shaped dural foramen around the verte-bral artery. The ventral root joins the dorsal root in or externalto the dural foramen.
The dorsal root of the first cervical nerve is more compli-cated than the ventral root because of the variations in itscomposition and its connections with the accessory nerve. Inthe 25 cervical spinal cords examined, in which one wouldexpect to find 50 C1 dorsal roots arising from the posteriorlateral sulcus, only 15 were found (5). The accessory nervecontributed a root to the C1 nerve in 28 of the 35 roots lackinga dorsal root arising from the spinal cord. In the remaining 7cases, the C1 dorsal root was absent. Each of the 15 dorsalroots that arose from the spinal cord also had a contributionfrom the accessory nerve.
Arterial relationships
The major arteries related to the foramen magnum are thevertebral and posteroinferior cerebellar arteries (PICA), andthe meningeal branches of the vertebral, and external andinternal carotid arteries (Figs. 6.3, 6.4, and 6.6) (16, 20, 21).
Vertebral arteryThe paired vertebral arteries arise from the subclavian ar-
teries, ascend through the transverse processes of the uppersix cervical vertebrae, pass behind the lateral masses of theaxis, enter the dura mater behind the occipital condyles, as-cend through the foramen magnum to the front of the me-dulla, and join to form the basilar artery at the pontomedul-
S168 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

lary junction. Each artery is divided into intradural andextradural parts (Figs. 6.3-6.6).
The extradural part is divided into three segments. The firstsegment extends from the origin at the subclavian artery tothe entrance into the lowest transverse foramen, usually at theC6 level. The second segment ascends through the transverseforamina of the upper six cervical vertebrae in front of thecervical nerve roots. This segment deviates laterally just abovethe axis to reach the laterally placed transverse foramen of theatlas. The third segment, the one most intimately related tothe foramen magnum, extends from the foramen in the trans-verse process of the atlas to the site of passage through thedura mater. The artery, after passing through the transverseprocess of the atlas, is located on the medial side of the rectuscapitis lateralis. The third segment passes medially behind thelateral mass of the atlas and atlanto-occipital joint and ispressed into the groove on the upper surface of the lateral partof the posterior arch of the atlas, where it courses along thefloor of the suboccipital triangle. It enters the vertebral canalby passing anterior to the lateral border of the atlanto-occipital membrane. It is partially covered by the posterioratlanto-occipital membrane and semispinalis capitis, the rec-tus capitis posterior major, and the superior and inferioroblique muscles. It is surrounded by a venous plexus com-posed of anastomoses between the deep cervical and epiduralveins. The C1 nerve root passes through the dura mater on thelower surface of the vertebral artery between the artery andthe groove on the posterior arch of the atlas with the vertebralartery. This bony groove is frequently transformed into abony canal that completely surrounds a short segment of theartery. Of the 50 arteries we examined, 24 (48%) were in ashallow groove, 12 (24%) were partially, but incompletely,surrounded by bone, and 14 (28%) coursed through a bonyring that completely surrounded the artery (Fig. 6.6) (5). Theterminal extradural segment of the vertebral artery gives riseto the posterior meningeal and posterior spinal arteries,branches to the deep cervical musculature, and infrequentlythe PICA.
The intradural segment begins at the dural foramina justinferior to the lateral edge of the foramen magnum. The durain this region is much thicker than in other areas, and it formsa funnel-shaped foramen around a 4- to 6-mm length of theartery. The first cervical nerve exits the spinal canal, and theposterior spinal artery enters the spinal canal through thisdural foramen with the vertebral artery. These three struc-tures are bound together at the foramen by fibrous duralbands. The initial intradural segment of the vertebral arterypasses just superior to the dorsal and ventral roots of the firstcervical nerve, and just anterior to the posterior spinal artery,the dentate ligament, and the spinal portion of the accessorynerve.
Once inside the dura mater, the artery ascends from thelower lateral to the upper anterior surface of the medulla. Theintradural part of the artery is divided into lateral and anteriormedullary segments (5, 16). The lateral medullary segmentbegins at the dural foramen and passes anterior and superioralong the lateral medullary surface to terminate at the preo-livary sulcus. The anterior medullary segment begins at the
preolivary sulcus, courses in front of, or between, the hypo-glossal rootlets, and crosses the pyramid to join with the othervertebral artery at or near the pontomedullary sulcus to formthe basilar artery. In its ascending course, the anterior andlateral surfaces of the lateral medullary segments face theoccipital condyles, the hypoglossal canals, and the jugulartubercles. The anterior medullary segment rests on the clivus.The branches arising from the vertebral artery in the region ofthe foramen magnum are the posterior spinal, anterior spinal,PICA, and anterior and posterior meningeal arteries.
Posterior spinal arteryThe paired posterior spinal arteries usually arise from the
posteromedial surface of the vertebral arteries, just outsidethe dura mater, but they may also arise from the initial intra-dural part of the vertebral arteries, or from the PICA (Figs. 6.3and 6.6) (5, 16, 21). Care should be taken to preserve theposterior spinal artery during dural opening because it maybe incorporated into the dural cuff around the vertebral artery.As each posterior spinal artery passes through the dura mater, itis surrounded by the same fibrous tunnel as the vertebral arteryand the first cervical nerve root. In the subarachnoid space, itcourses medially behind the rostral-most attachments of thedentate ligament, and on reaching the lower medulla, it dividesinto ascending and descending branches. The ascending branchcourses through the foramen magnum and supplies the resti-form body, the gracile and cuneate tubercles, the rootlets of theaccessory nerve, and the choroid plexus near The foramen ofMagendie, and may give rise to branches that anastomose withbranches of the PICA. The descending branch passes downwardbetween the dorsal rootlets and the dentate ligament on theposterolateral surface of the spinal cord, and supplies the super-ficial part of the dorsal half of the cervical spinal cord. It anas-tomoses with the posterior branches of the radicular arteries thatenter the vertebral foramen at lower levels. The descendingbranch gives rise to collateral branches, each lower one beingsmaller and less constant than the last one, which course medi-ally across the posterior surface of the spinal cord, and join toform an artery that courses in the midline, parallel to the poste-rior spinal arteries.
Posteroinferior cerebellar arteryThe PICA is the largest branch of the vertebral artery (Figs.
6.3 and 6.6). It usually originates with the dura mater, but itmay infrequently originate from the terminal extradural partof the vertebral artery. It may arise at, above, or below thelevel of the foramen magnum; of the 42 arteries found in 50cerebellae examined, 35 arose above and 7 arose below theforamen (16). The tonsillomedullary PICA segment, whichforms the caudal loop related to the lower part of the tonsil, ismost intimately related to the foramen magnum. The lowerend of the caudal loop was found to be above the edge of theforamen magnum in 37 of the 42 arteries examined, below theedge in 4, and at the level of the edge of the foramen in 1.
Anterior spinal arteryThe anterior spinal artery is formed by the union of the
paired anterior ventral spinal arteries, which originate from
Foramen Magnum S169
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

the anterior medullary segment of the vertebral arteries nearthe origin of the basilar artery (Figs. 6.3, 6.4, and 6.6). Thejunction of the anteroventral spinal arteries was located abovethe level of the foramen magnum near the lower end of theolives in 84% of our specimens (5). In some cases, one ofthe anterior ventral spinal arteries continued inferiorly as theanterior spinal artery, and the other terminated on the ante-rior surface of the medulla or in a rudimentary channel con-nected the smaller anterior ventral spinal artery with a dom-inant one.
The anterior spinal artery descends through the foramenmagnum on the anterior surface of the medulla and the spinalcord in or near the anteromedian fissure. On the medulla, itsupplies the pyramids and their decussation, the medial lem-niscus, the interolivary bundles, the hypoglossal nuclei andnerves, and the posterior longitudinal fasciculus (17). It anas-tomoses with the anterior branches of the radicular arteriesentering the cervical foramina. There are few anastomoseswith the anterior radicular branches if the descending channelis large, but it has frequent connections with the anteriorradicular arteries if it is small.
Meningeal arteriesThe dura mater around the foramen magnum is supplied
by the anterior and posterior meningeal branches of the ver-tebral artery, and the meningeal branches of the ascendingpharyngeal and occipital arteries (Figs. 6.3 and 6.6) (5, 20).These arteries, plus the dorsal meningeal branch of meningo-hypophyseal trunk that arises from the intracavernous seg-ment of the internal carotid artery, supply all of the duralining the posterior cranial fossa. Infrequently, the PICA, theposterior spinal artery, and the intradural part of the vertebralartery give rise to meningeal branches.
The anterior meningeal branch of the vertebral artery arisesfrom the medial surfaces of the extradural part of the verte-bral artery immediately above the transverse foramen of thethird cervical vertebra (Fig. 6.3). The artery enters the spinalcanal through the intervertebral foramen between the secondand third cervical vertebrae, and ascends between the poste-rior longitudinal ligament and the dura mater. At the level ofthe apex of the dens, each artery courses medially to join itsmate from the opposite side and forms an arch over the apexof the dens. Its branches supply the dura mater in the regionof the clivus and the anterior part of the foramen magnumand upper spinal canal, and they anastomose with thebranches of the ascending pharyngeal and dorsal meningealarteries that supply the dura mater covering the anterior andanterolateral part of the posterior fossa. The anterior menin-geal artery also gives rise to muscular and osseous branchesthat supply the body and odontoid process of the axis and thearticulate plate of the atlanto-occipital and atlantoaxial joints.
The posterior meningeal artery arises from the posterosu-perior surface of the vertebral artery as it courses around thelateral mass of the atlas, above the posterior arch or just beforepenetrating the dura; however, it may have an intraduralorigin, in which case, it penetrates the arachnoid to reach thedura (Fig. 6.6) (5). It pursues a tortuous ascending course and
penetrates the dura before reaching the posterior edge of theforamen magnum. After passing through the foramen mag-num, it ascends near the falx cerebelli and divides near thetorcula into several branches that terminate in the posteriorpart of the tentorium and cerebral falx. It supplies the duramater lining the posterolateral and posterior part of the pos-terior cranial fossa, and anastomoses with the meningealbranches of the ascending pharyngeal and occipital arteries.
The ascending pharyngeal branch of the external carotidartery usually sends two branches to the dura above theforamen magnum. One branch passes through the hypoglos-sal canal and the other enters through the jugular foramen(14). The branch passing through the hypoglossal canal di-vides into an ascending branch that passes upward in thedura covering the clivus and anastomoses with the branchesof the dorsal meningeal artery, and a descending branch thatcourses inferomedially toward the anterior edge of the fora-men magnum and anastomoses with branches of the arcadeabove the odontoid process formed by the anterior meningealarteries. This anastomotic rete in the dura anterior to theforamen magnum and on the clivus gives osseous branches tothe clivus. The branches that enter through the jugular fora-men divide into branches that course posteriorly and postero-superiorly to anastomose with the meningeal branches of theoccipital and posterior meningeal arteries, and supply the duramater in the posterior and posterolateral parts of the posteriorcranial fossa.
The meningeal branch of the occipital artery is inconstantand, if present, it penetrates the cranium through the mastoidemissary foramen. It divides into one branch that coursesposterosuperiorly to join the branches of the posterior men-ingeal artery that supplies the dura mater in the posterior partof the posterior fossa, and another branch that courses antero-laterally and joins the meningeal branches of the ascendingpharyngeal artery.
Venous relationships
The venous structures in the region of the foramen magnumare divided into three groups: one composed of the extraduralveins, another formed by the intradural (neural) veins, and athird constituted by the dural venous sinuses (13, 18). The threegroups anastomose through bridging and emissary veins.
Extradural groupsVenous flow in this area empties into two systems: one
drained by the internal jugular vein and another draining intothe vertebral venous plexus. The internal jugular vein and itstributaries form the most important drainage system in thecraniocervical area. The internal jugular vein originates at thejugular foramen by the confluence of the sigmoid and inferiorpetrosal sinuses (14, 18, 25). The venous plexus surroundingthe vertebral artery in the suboccipital triangle is formed bynumerous small channels that empty into the internal verte-bral plexuses (between the dura and the vertebrae), whichissue from the vertebral canal above the posterior arch of the
S170 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

atlas. This vertebral venous plexus and multiple small veinsfrom the deep muscles communicate with the dense venousplexus, which accompanies the vertebral artery into the fora-men in the transverse process of the atlas and descendsthrough the transverse foramina of successive cervical verte-brae into the brachiocephalic vein. The posterior condylaremissary vein, which passes through the posterior condylar canal,forms a communication between the vertebral venous plexus andthe sigmoid sinus. The venous plexus of the hypoglossal canalpasses along the hypoglossal canal to connect the basilar venousplexus with the marginal sinus, which encircles the foramenmagnum. Obliteration of a portion of the venous plexus exposesthe upper extradural segment of the vertebral artery.
Dural venous sinusesThe venous channels in the dura mater surrounding the
foramen magnum are the marginal, occipital, sigmoid, infe-rior petrosal, and basilar venous plexus. The marginal sinus islocated between the layers of the dura in the rim of theforamen magnum. It communicates anteriorly, through a se-ries of small sinuses, with the basilar sinus on the clivus, andposteriorly with the occipital sinus. It is usually connected tothe sigmoid sinus or jugular bulb, by a sinus that passesacross the intracranial surface of, and communicates with, theveins in the hypoglossal canal. These anastomoses provide analternative route for venous drainage in the case of obstruc-tion of the internal jugular vein. The occipital sinus courses inthe cerebellar falx. Its lower end divides into paired limbseach of which courses anteriorly around the foramen mag-num to join the sigmoid sinus or the jugular bulb and itsupper end joins the torcula.
The basilar venous plexus is located between the layers ofthe dura mater on the upper clivus. It is formed by intercon-necting venous channels that anastomose with the inferiorpetrosal sinuses laterally, the cavernous sinuses superiorly,and the marginal sinus and epidural venous plexus inferi-orly. The inferior petrosal sinuses extend along the petroclivalfissure and communicate above with the basilar sinus andbelow with the jugular bulb. The sigmoid sinus descendsalong the sigmoid groove and exits the cranium through thesigmoid part of the jugular foramen, and descends anterolat-eral to the occipital condyle, and anterior to the transverseprocess of the atlas.
Intradural (neural) veinsThe intradural veins in the region of the foramen magnum
drain the lower part of the cerebellum and brainstem, theupper part of the spinal cord, and the cerebellomedullaryfissure. The veins of the medulla and spinal cord form longi-tudinal plexiform channels that anastomose at the foramenmagnum. The median anterior spinal vein that courses in theanteromedian spinal fissure deep to the anterior spinal arteryis continuous with the median anterior medullary vein thatcourses on the anteromedian sulcus of the medulla. The lat-eral anterior spinal vein courses longitudinally along the or-igin of the ventral roots and superiorly joins the lateral ante-rior medullary vein that courses longitudinally in the
anterolateral medullary (preolivary) sulcus along the line oforigin of the hypoglossal rootlets. The lateral posterior spinalvein, which courses along the line of origin of the dorsal rootsin the posterior lateral spinal sulcus, is continuous above withthe lateral medullary vein that courses along the retro-olivarysulcus, dorsal to the olive. The median posterior spinal vein,which courses along the posteromedian spinal sulcus, is con-tinuous above with the main vein on the posterior surface ofthe medulla, the median posterior medullary vein thatcourses along the posteromedian medullary sulcus. The trans-verse medullary and transverse spinal veins cross the medullaand spinal cord at various levels, interconnecting the majorlongitudinal channels. Bridging veins may connect the neuralveins with the dural sinus in the region of the foramenmagnum.
DISCUSSION
Herniations
Herniation of cerebellar tissue into the foramen magnummay cause neural compression and even death. These hernia-tions are commonly referred to as tonsillar herniations (8, 27),but the herniation usually involves the tonsils and biventrallobules, both of which are deeply grooved by the edge of theforamen magnum. The herniation may compress the medullaand be so severe that the herniated tissue undergoes necrosis.Patients with herniation at the foramen magnum may be asymp-tomatic; or may present with pain, signs of neural compression,increased intracranial pressure, and sudden unexpected death.Symptoms caused by dysfunction of the cerebellum, brainstem,and lower cranial and upper spinal nerves include pain in theneck and upper arms, dizziness, ataxia, disturbances of gait,diplopia, dysphagia, tinnitus, decreased hearing, nystagmus,weakness up to the degree of quadriparesis, and sensory deficit inthe extremities. Coughing or sneezing may aggravate the symp-toms and cause syncope. Some patients without previoussymptoms who die suddenly are found to have herniationsthrough the foramen magnum at autopsy. The occurrence ofsudden death in these patients means that herniation at theforamen magnum is a precarious situation that can be aggra-vated by minor stresses (8). The common denominator inthese cases with sudden death is herniation of the tonsils andadjacent part of the biventral lobule into the foramen mag-num. The herniation may be bilateral and symmetrical, al-though more commonly it is not strictly symmetrical and maybe unilateral. The herniated tonsils are tightly pressed againstthe medulla. Acute or chronic herniations may be seen withspace-occupying lesions, such as cerebellar astrocytomas orcystic tumors. Chronic herniation is seen with the Arnold-Chiari malformation.
Tumors
Tumors arising in the region of the foramen magnum aredivided by Cushing and Eisenhardt (4) into a craniospinalgroup that arises above and grows downward toward theforamen magnum, and a spinocranial group that arises below
Foramen Magnum S171
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

and grows upward toward the foramen magnum. The intra-dural extramedullary tumors in this region are usually be-nign, with meningiomas and schwannomas being the mostfrequent. The intramedullary tumors are represented mainlyby astrocytomas and ependymomas. Cerebellar tumors, espe-cially those originating in the fourth ventricle and those aris-ing in the lower part of the cerebellar hemisphere or vermis,may extend into or through the foramen magnum into theupper spinal canal. Chordomas and metastases are the mostcommon extradural tumors. The chordomas usually arise atthe level of the clivus and may extend caudally into theforamen magnum.
Foramen magnum tumors have frequently eluded earlydiagnosis because they cause bizarre symptoms that simulate
cervical, spondylosis, multiple sclerosis, or degenerative dis-eases (1, 23, 30). Symptoms or signs, common in other disor-ders that should also suggest the presence of a tumor in theregion of the foramen magnum include neck stiffness andpain, involvement of the lower cranial nerves, especially thespinal accessory nerve, unilateral upper extremity weaknessand atrophy, incoordination of the hands, gait disturbances,vague sensory disturbances or paresthesia in the extremities,objective sensory loss in a nonanatomic pattern, incoordina-tion in the upper extremities, and pyramidal tract findingswith spastic gait. Those tumors arising in the caudal part ofthe fourth ventricle or cerebellum may cause increased intra-cranial pressure by obstructing cerebrospinal fluid drainageat the level of the fourth ventricle.
FIGURE 6.7. Surgical approaches to the foramen magnum. The posterior operative approach is commonly selected for intra-dural lesions. An anterior approach is frequently selected for extradural lesions situated anterior to the foramen magnum. Alateral approach may be selected for intradural lesions located lateral to and/or in front of the brainstem, especially if theyinvolve or are contiguous with the temporal bone. The lateral approaches directed through the temporal bone are consideredin a later section of this issue.
S172 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.8. Suboccipitalapproaches. Either a verticalmidline or hockey-stickincision is used, dependingon the site of the lesion. A,the patient is mostcommonly placed in thethree-quarter prone position.B, the vertical midlineincision is selected forlesions situated in the upperspinal canal and for thoselocated posteriorly orposterolaterally in the areaabove the foramen magnum.The subcutaneous tissues areseparated from theunderlying fascia near theinion to gain room for a Y-shaped incision in themuscles. The upper limbs ofthe “Y” begin at the levelof the superior nuchal lineand join below the inion. C,the incision is of sufficientlength to complete asuboccipital craniectomy anda laminectomy of the axisand atlas (oblique lines). D,the dural incision is outlined(interrupted lines). E,intradural exposure. Themajor extracranial hazard isinjury to the vertebral arteryas it courses below theatlantoaxial joint and acrossthe posterior arch of theatlas. The vertebral arteriesand PICAs are in the lowerpart of the exposure. Theaccessory nerve ascendsposterior to the dentateligament. Theglossopharyngeal, vagus, and
accessory nerves pass toward the jugular foramen. F, upper left. Hockey-stick retrosigmoid exposure. Skin incision (solid line)and bone removal (oblique lines). Lower right. Intradural exposure. The hockey-stick incision extends superomedial from themastoid process along the superior nuchal line to the inion and downward in the midline. This incision is selected if thelesion extends anterolateral or anterior to the brainstem toward the jugular foramen or cerebellopontine angle. This exposurepermits the removal of the full posterior rim of the foramen magnum, the posterior elements of the atlas and axis, and, inaddition, the ability to complete a unilateral suboccipital craniectomy of sufficient size to expose the anterolateral surface ofthe brainstem and the nerves in the cerebellopontine angle. Tumors in this area may extend upward through thecerebellomedullary fissure to be attached to the roof or floor of the fourth ventricle. Laterally situated tumors may beattached to the initial intradural segment of the vertebral artery and the thick dural cuff around the artery, which alsoincorporates the posterior spinal arteries and the C1 nerve root in fibrous tissue. As one moves superiorly along the lateralsurface of the medulla, the origin of the PICA and the glossopharyngeal, vagus, accessory, facial, vestibulocochlear, andtrigeminal nerves are encountered. The dura is closed with a dural substitute if closure of the patient’s dura constricts thecerebellar tonsils or the cervicomedullary junction. A., artery; A.I.C.A., anteroinferior cerebellar artery; Lig., ligament;P.I.C.A., posteroinferior cerebellar artery; Vert., vertebral.
Foramen Magnum S173
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

Surgical approaches
The foramen magnum is most commonly approached fromposteriorly or anteriorly, and less frequently from laterally(Fig. 6.7). The posterior operative approach is commonly se-lected for intradural lesions, and an anterior approach isfrequently selected for extradural lesions situated anterior tothe foramen magnum. A lateral approach may be selected forlesions located lateral to or in front of the brainstem, espe-cially if they involve, or are located contiguous to the tempo-ral bone and clivus. The lateral approaches directed throughthe temporal bone are reviewed in the chapter on the tempo-ral bone.
Posterior approaches
The vertical midline incision is used for lesions situated inthe upper spinal canal and posterior or posterolateral at thelevel of or above the foramen magnum (Figs. 6.3, 6.6, and 6.8).The vertical midline skin incision is of sufficient length tocomplete a craniectomy above the foramen magnum and alaminectomy of the axis and atlas. The subcutaneous tissuesare separated from the underlying fascia near the inion to gainroom for a Y-shape muscle incision. The upper limbs of the“Y” begin at the level of the superior nuchal line, lateral to theexternal occipital protuberance, and join several centimetersbelow the inion, leaving a musculofascial flap along the su-
FIGURE 6.9. Transnasal route to the upper clivus. A, the section of the facial structures extends across the nasal cavity,superior and middle turbinates, maxillary sinuses, the orbits near the apex, and the ethmoid sinuses in front of the sphenoidsinus. The zygomatic and infraorbital nerves arise from the mandibular nerve in the pterygopalatine fossa, which is locatedbehind the posterior wall of the maxillary sinus. B, the turbinates and posterior ethmoid air cells have been removed toexpose the vomer and the anterior face of the sphenoid sinus. The nasolacrimal duct descends along the lateral wall of thenasal cavity and opens below the inferior turbinate into the inferior meatus. C, the anterior face of the sphenoid sinus hasbeen removed to expose the multiseptated sphenoid sinus and the anterior wall of the sella. The bony prominences over theoptic canals are situated in the superolateral margins of the sphenoid sinus. D, the anterior wall of the sella and the lateralwalls of the sphenoid sinus have been removed to expose the petrous and cavernous carotid and the pituitary gland. The pos-terior wall of the sphenoid sinus, which forms the anterior surface of the upper clivus, has been preserved. A., artery; Car.,carotid; Cav., cavernous; CN, cranial nerve; Gang., ganglion; Gl., gland; Inf., inferior; Infraorb., infraorbital; M., muscle;Max., maxillary; M.C.A., middle cerebral artery; Med., medial; Mid., middle; N., nerve; Nasolac., nasolacrimal; Pet., petrous;Rec., rectus; Sphen., sphenoid; Sup., superior; Turb., turbinates.
S174 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

perior nuchal line for closure. The inferior limb of the “Y”incision extends downward in the midline. The major ex-tracranial hazard is injury to the vertebral artery as it coursesalong the lateral part of the posterior arch of the atlas. Thisartery is not encountered if the incision is strictly midline, butit is frequently encountered in the floor of the suboccipitaltriangle if the muscle incision deviates laterally, or when the
muscles are stripped from the lateral part of the posterior archof the atlas. The emissary veins and vertebral venous plexusshould be obliterated quickly if they are opened.
The hockey-stick incision is selected if the lesion extendsanterior or anterolateral to the brainstem toward the jugularforamen or the cerebellopontine angle. The skin incision ex-tends from the mastoid process along the superior nuchal line to
FIGURE 6.10. Nasal pathway to the clivus. Stepwise dissection showing the structures that form the lateral limit of the trans-nasal route to the clivus. A, the entire clivus is located above the level of the hard palate and, in most cases, can be accessedthrough the nasal cavity and nasopharynx. The nasal turbinates and meati and the eustachian tubes are in the lateral marginof the exposure. B, a portion of the superior, middle, and inferior turbinates has been removed and the area between the sphenoidpterygoid process and the posterior wall of the maxilla has been opened to expose the pterygopalatine fossa in the lateral wall ofthe nasal cavity. The ostia of the maxillary and frontal sinuses opens into the middle meatus located below the middle turbinate.The nasolacrimal duct opens below the lower turbinate into the inferior meatus. The eustachian tube, located in front the foramenmagnum and lower edge of the clivus, opens into the nasopharynx at the posterior edge of the pterygoid process. Accessing theclivus plus the atlas and axis requires an approach that can be directed above and below the level of the palate. Rosenmuller’sfossa is located behind the eustachian tube. C, the medial wall of the maxillary sinus has been opened to expose the infraorbitalnerve, which arises in the pterygopalatine fossa and passes forward in the sinus roof. The maxillary nerve passes through the fora-men rotundum to enter the pterygopalatine. The upper cervical carotid and eustachian tube form the lateral limit of the exposureof the lower clivus and the junction of the petrous and cavernous carotid limits the lateral exposure of the upper clivus. D,enlarged view. The bone and dura covering the optic canal in the superolateral part of the sphenoid sinus has been opened toexpose the optic nerve and ophthalmic artery in the optic canal. The junction of the petrous and cavernous carotid limits the expo-sure below the level of the sella. The maxillary nerve exits the foramen rotundum and enters through the pterygopalatine fossawhere it gives rise to the infraorbital, zygomatic, and greater palatine nerves, plus communicating rami to the pterygopalatine gan-glion. Terminal branches of the maxillary artery intermingle with the neural structures in the pterygopalatine fossa. A., artery; Ant.,anterior; Car., carotid; Cav., cavernous; Eust., eustachian; For., foramen; Gang., ganglion; Gr., greater; Inf., inferior; Infraorb.,infraorbital; Max., maxillary; Mid., middle; N., nerve; Ophth., ophthalmic; Palat., palatine; Pet., petrosal; Proc., process; Pteryg.,pterygoid; Pterygopal., pterygopalatine; Sup., superior.
Foramen Magnum S175
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.11. Nasal route to the clivus. A, this cross section extends through the nasal cavity, orbits, and maxillary and eth-moid sinuses. The ethmoid sinuses are situated in front of the sphenoid sinus. The middle and inferior turbinates have beenpreserved. B, the anterior wall of the sphenoid sinus has been opened to expose a multiseptated sinus and the anterior sellarwall. The left turbinates have been removed. Part of the posterior wall of the left maxillary sinus has been removed to exposethe greater palatine artery which arises from the maxillary artery in the pterygopalatine fossa. The internal carotid arteries
S176 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

the inion, and downward in the midline. A muscular cuff is leftattached along the superior nuchal line to facilitate the closure.This incision permits removal of the full posterior rim of theforamen magnum, the posterior elements of the atlas and axis,and, in addition, to complete a unilateral suboccipital craniec-tomy of sufficient size to expose the anterolateral surface of thebrainstem and the nerves in the cerebellopontine angle.
In opening the dura mater, using either the midline orhockey-stick approach, the marginal and occipital sinuses,along with the bridging veins passing from the neural sur-faces to these and the sigmoid sinus, are encountered. Poste-rior intradural lesions may separate easily from the surface ofthe brain and spinal cord. On the other hand, they may beattached to the nerve roots and spinal cord, or they mayextend upward through the cerebellomedullary fissure to beattached to the inferior medullary velum, choroid plexus, orthe floor of the fourth ventricle. Opening the tela choroideaand inferior medullary velum may facilitate the exposure oftumors in this area. Care is required to avoid injury to thePICA as it courses around the tonsil and through the cleftbetween the superior pole of the tonsil and inferior medullaryvelum and tela choroidea.
Laterally situated tumors may be attached to the initialintradural segment of the vertebral artery and the thick duralcuff around the artery, which also incorporates the posteriormeningeal and posterior spinal arteries, Cl nerve root, acces-sory nerve, and the dentate ligament. Dealing with theselesions may be facilitated by using a far-lateral approach,which is extended to include exposure of the atlanto-occipitaljoint, extradural vertebral artery, and transverse process ofC1, combined with drilling of the occipital condyle, as de-scribed in detail in the chapter on the far lateral approach (29,33). Dividing the attachments of the upper triangular pro-cesses of the dentate ligaments may facilitate the exposure ofanteriorly situated lesions. Structures encountered in expos-ing superiorly along the lateral surface of the medulla includethe PICA and the glossopharyngeal, vagus, accessory, andhypoglossal nerves. The vertebral artery may be followedupward to its junction with the basilar artery through thehockey-stick exposure. The most difficult lesions to removeare those situated anterior to the glossopharyngeal, vagus,and accessory nerves and the lateral medullary segment of the
vertebral artery. Before sacrificing any rootlets of thesenerves, an attempt should be made to gently separate therootlets and to operate through the interval between the root-lets. Often, tumors expand and widen the interval betweenthe rootlets, thus providing some access to medially placedlesions. Another route through which it may be easier to reacha lesion anterior to the medulla and pons is the intervalbetween the lower margin of the vestibulocochlear and facialnerves and the upper margin of the glossopharyngeal nerve.It is uncommon to be able to work between the vagal rootlets;however, the lower cervical rootlets of the accessory nerve arevery fine and are often separated by a wide interval. Consid-eration might be given to sacrificing a few of the lower acces-sory rootlets if it will make an otherwise incurable lesioncurable. The intracapsular contents of the tumor are removed,and the remaining tumor capsule is separated from the sur-face of the brainstem and nerves rather than attempting todeliver the whole intact tumor through the limited exposure.Extreme care should be used when cutting into tumors situ-ated anterolateral to the brainstem, since these tumors, espe-cially meningiomas, may encase a segment of the vertebralartery or the PICA. The dura mater is closed with a duralsubstitute if closure of the patient’s dura mater constricts thecerebellar tonsils or the cervicomedullary junction. A pseudo-meningocele may form at the operative site if there is anytendency toward the development of hydrocephalus. Spinal drain-age, repeated spinal punctures, or a shunting procedure may berequired to decompress a postoperative pseudomeningocele.
Anterior operative approachesThe anterior approach was first used to reach lesions ante-
rior to the spinal cord, and was subsequently used to exposelesions anterior to the brainstem (Figs. 6.4, 6.5, and 6.9-6.11).The greatest advantage of the anterior approach is the directroute to the lesion, and the major disadvantages are the con-taminated field and the frequency of cerebrospinal fluid fis-tula, pseudomeningocele, and meningitis after the exposureof intradural lesions by this approach. The depth of the op-erative field was once considered a disadvantage, but the useof the operating microscope has reduced the importance ofthat factor.
Š
form serpiginous prominences in the lateral wall of the sphenoid sinus. C, the mucosa and bony wall of the sphenoid sinushave been removed to expose both the internal carotid arteries, which form the lateral limit of the transnasal exposure of theupper clivus. The pituitary gland has been exposed. Additional posterior wall of the left maxillary sinus has been removed toexpose the infratemporal fossa, which contains the branches of the maxillary artery, the pterygoid muscles, pterygoid venousplexus, and branches of the mandibular nerve. The nasopharyngeal mucosa covering the longus capitis and the lower clivus isexposed in the interval between the palate and the vomer. D, enlarged view of the sphenoid sinus and sellar region. Theanterior surface of the upper clivus is exposed below the pituitary gland. The lateral clival exposure is limited at this level bythe internal carotid arteries. E, oblique view. The medial wall of the left cavernous sinus has been opened to expose theabducens and oculomotor nerves. The pterygopalatine fossa is located below the orbital apex. The maxillary nerve passesthrough the foramen rotundum and gives rise to the communicating rami to the pterygopalatine ganglion and the infraorbitalnerve that courses along the floor of the orbit. F, enlarged view of the structures in the medial cavernous sinus. The ophthal-mic artery courses below the optic nerve in the optic canal. A., artery; Car., carotid; Cav., cavernous; CN, cranial nerve; Gl.,gland; Gr., greater; Inf., inferior; Infratemp., infratemporal; Max., maxillary; Mid., middle; Ophth., ophthalmic; Palat., pala-tine; Pterygopal., pterygopalatine; Sphen., sphenoid; Turb., turbinates.
Foramen Magnum S177
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

Anterior approaches have been used to reach tumors of theatlas, axis, and clivus; for the resection and fixation of the odon-toid process after ligamentous and osseous injury; for decom-pressing bony malformations of the craniovertebral junction,
such as basilar invagination, which compress the medulla orspinal cord from anteriorly; and for approaching aneurysms ofthe lower third of the basilar artery, the vertebrobasilar junction,and the upper part of the vertebral arteries.
FIGURE 6.12. A–F. Transoral,transpalatal, and transmaxillaryapproaches to the clivus and foramenmagnum. A, forced opening of the mouthpermits the clivus to be exposed belowthe palate. B, anterior view through theopen mouth. The soft palate, whichextends backward from the hard palate,will block the view of the upper clivus. C,an incision has been outlined in themidline of the soft palate. D, the softpalate has been divided to expose themucosa lining the lower clivus. E, thepharyngeal mucosa has been opened inthe midline and the longus capitis andlongus coli have been exposed andthe longus capitis reflected laterally.F, the left longus capitis and longus colihave been reflected laterally. A., artery;
A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Bas., basilar; Cap., capitis; CN, cranial nerve; For., foramen; Gr.,greater; Infratemp., infratemporal; Jug., jugular; Long., longus; M., muscle; Max., maxillary; N., nerve; P.I.C.A., posteroinferiorcerebellar artery; Sp., spinal; Sphen., sphenoid; Temp., temporal; Vert., vertebral; Vert., vertebral; Zygom., zygomatic.
S178 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

The transoral route through the mouth and the posteriorpharyngeal wall, referred to as the buccopharyngeal ap-proach, is the anterior approach most commonly selected. Thebasic transoral approach may be modified to include a trans-palatine approach in which the soft palate, or both the softand hard palates, are opened, and a labiomandibular or la-bioglossomandibular approach in which the lip, mandible,and possibly the tongue and floor of the mouth are split toincrease the exposure. Other types of anterior approaches are:the transcervical approach directed through the submandib-ular area along the anterior border of the sternocleidomastoidmuscle (31); the transcranial-transbasal approach in which theclivus is reached through a bifrontal craniotomy after resectionof the sphenoid and ethmoid sinuses (6); the extended frontalapproach in which the bifrontal craniotomy is combined with anosteotomy of the orbital rims; and the transsphenoidal approachdirected under the lip, along the nasal septum, and through thesphenoid sinus to the upper part of the clivus.
Transoral approachesFor the transoral approach, the soft palate is retracted to
reach the anterior part of the atlas and axis, and the posterior
pharyngeal wall is incised longitudinally in the midline (Figs.6.4, 6.12, and 6.13). The mucosa and prevertebral muscles areelevated as a single mucoperiosteal layer using subperiostealdissection, and are retracted laterally. To expose the clivus, itis often necessary to split the soft palate in the midline. Ifadded craniad exposure is needed, laterally based mucoperi-osteal flaps may be elevated from the lower surface of thehard palate, and the posterior part of the hard palate may beremoved. The mucosa covering the upper surface of the hardpalate should be retracted and not opened. This permits thepharyngeal incision to be extended upward through the vaultof the nasopharynx to the posterior border of the vomer.When elevating the mucoperiosteal layer from the clivus, thelateral margins slope dorsally into “gutter-like” depressionsin which the tissue becomes thicker and more adherent. De-pending on the lesion, the clivus, the anterior arch of the atlas,the dens, and bodies of C2 and C3 may be removed with adrill and rongeurs. The clival exposure between the occipitalcondyles is 2- to 2.5-cm wide and 2.5- to 3.0-cm long. Caremust be taken to avoid the sixth through the twelve cranialnerves, the internal carotid arteries, the internal jugular veins,and the inferior petrosal sinuses that are on the periphery of
FIGURE 6.12. G–J. Transoral, transpalatal, and transmaxillary approaches to the clivus and foramen magnum. G, the lower clivushas been opened to expose both vertebral arteries, lower part of the basilar artery, right PICA, left AICA, and the abducens andhypoglossal nerves. H, the anterior arch of C1 has been removed to expose the odontoid process. I, a degloving subperiosteal dis-section exposes the anterior face of the maxilla and the lower part of the anterior piriform aperture. J, the transverse maxillary(LeFort I) osteotomy extends through the maxillary sinus above the apex of the teeth and below the infraorbital canals.
Foramen Magnum S179
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

the exposure. The most common lesions approached by thisroute are in an extradural location. Opening the dura materwill expose both vertebral arteries and the lower part of thebasilar artery.
To increase the exposure and reduce the operative depth,the lip and chin may be incised vertically and a step-like
mandibular osteotomy accomplished in the midline after re-moval of a central incisor tooth. Spreading the mandibularedges laterally, without splitting the tongue, permits thetongue to be depressed downward between the mandibularhalves. If the exposure is still inadequate, the tongue and floorof the mouth may be split in the midline. Spreading the
FIGURE 6.12. K–N. Transoral, transpalatal, and transmaxillary approaches to the clivus and foramen magnum. K, the lowermaxilla has been displaced downward. The clival window and vertebral arteries can be seen through the exposure. L,enlarged view of the clival opening. M, the maxilla has been split vertically in the midline and the halves reflected laterally,allowing the clival opening to be extended upward. N, enlarged view of the clival exposure. The right AICA passes behind theright abducens nerve and the left AICA passes in front of the left abducens nerve.
S180 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.13. The transoral approach is the anterior approach most commonly selected. Variants of the transoral approach include thetranspalatal variant in which the soft palate or both the soft and hard palates are opened, and the labiomandibular or labioglossoman-dibular variants in which the lip, chin, mandible, and possibly the tongue and floor of the mouth are split in the midline to increase theexposure. The transoral approach and its variants permit removal of the clivus, the anterior arch of the atlas, the odontoid process, andthe bodies of C2 and C3. A, transoral approach. The patient is positioned with the head fixed so that lateral x-ray or image intensificationis available to verify the location. A tracheostomy is commonly performed. Catheters inserted through the nasal passages and broughtbehind the soft palate and out the mouth or a silk suture brought through the base of the uvula and attached to a nasal catheter may beused to retract the soft palate. The posterior pharyngeal wall is incised longitudinally in the midline (interrupted line). B, the mucosa andmuscles are retracted laterally as a single layer, using subperiosteal dissection to reach the atlas, axis, and lower clivus. The anterior archof the atlas, the odontoid process, and the body of the atlas may be removed (interrupted line) to expose the dura. C, it may be necessaryto split the soft palate in the midline to expose the clivus (palatal incision, continuous line; pharyngeal incision, interrupted line). D, theanterior surface of the clivus has been exposed through the transpalatal approach. The anterior arch of the atlas and the odontoid processmay be removed and an opening made in the clivus (interrupted line). E, if further craniad exposure is needed, laterally based mucoperi-osteal flaps may be elevated from the lower surface of the hard palate (interrupted line), and the soft palate split in the midline (continu-ous line). The posterior part of the hard palate may be removed (oblique lines). F, care is taken to retract rather than open the mucosalining the upper surface of the hard palate. The pharyngeal incision is extended upward through the vault of the nasopharynx to the pos-terior border of the vomer. When elevating the mucoperiosteal layer from the clivus, the lateral margins slope dorsally into gutter-likedepressions where the tissue becomes more adherent. The clivus, anterior arch of the atlas, dens, and bodies of C2 and C3 may beremoved. The clival defect is packed with muscle or fat and may be reinforced with a bone graft. The prevertebral muscle and mucosallayers and the palatal openings are closed with absorbable sutures. G, the lower lip and mandible may be split (interrupted line) toincrease the exposure and reduce the operative depth. H, a step-like mandibular osteotomy (interrupted line) is accomplished in the mid-line after removal of a central incisor tooth. I, spreading the mandibular halves laterally without splitting the tongue permits the tongue tobe depressed downward between the mandibular halves. J, if the exposure is still inadequate, the tongue and floor of the mouth may besplit in the midline. Spreading the mandibular-lingual halves exposes the pharynx down to the C3 level. The mucosa and musculature ofthe tongue and floor of the mouth are reapproximated; the mandibular osteotomy is closed with plates; and the lip, chin, and submandib-ular region are carefully closed after dealing with the lesion. (From, Rhoton AL Jr, de Oliveira E: Anatomical basis of surgical approachesto the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. NewYork, Thieme, 1998, pp 13–57 [26].)
Foramen Magnum S181
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

mandibular-lingual halves exposes the pharyngeal wall downto the level of the arytenoid cartilages. After dealing with thelesion, the mucosa and musculature of the tongue and floor ofthe mouth are reapproximated, the mandibular osteotomy isrepositioned with wire, and the lip, chin, and submandibularregion are carefully closed.
Transmaxillary approachTransmaxillary approaches have been advocated for pa-
thology extending to the upper and middle third of the clivus,
which is difficult to reach by the transoral approach (Figs. 6.12and 6.14-6.16). Four different types of transmaxillary ap-proaches have been used (2, 3). In one approach, a LeFort Iosteotomy is completed, and the maxilla and hard palate aredown-fractured into the oral cavity. In the second approach,called the extended maxillectomy, the LeFort osteotomy iscombined with a midline incision of the hard and soft palateand the halves of the maxilla are swung laterally. In the thirdapproach, the unilateral lower subtotal maxillotomy, half ofthe maxilla, and the hard palate are hinged on the soft palate
FIGURE 6.14. A–D. Lower maxillotomy route to the clivus and foramen magnum. A, the approach can be made through adegloving incision inside the mouth; however, in this case, to more fully show the anatomy, a Weber-Fergusson paranasalincision with an infraorbital extension is used to expose the anterior face of the maxilla. The infraorbital nerve has beendivided, although it can usually be preserved with the degloving incision. The masseter is attached along the lower margin ofthe zygoma. B, the mucosal lining the maxillary sinus is exposed below the zygomatic arch. The coronoid process of the man-dible is removed or reflected with the temporalis muscle to expose the medial and lateral pterygoid muscles and the maxil-lary artery in the infratemporal fossa. C, the lateral pterygoid muscles and a segment of the maxillary artery have beenremoved. Removal of the lateral pterygoid exposes the mandibular nerve and its branches in the medial part of the infratem-poral fossa. D, a lower maxillectomy has been completed. In this approach, the maxilla can be folded on a vascularized pedicle ofsoft palate into the floor of the mouth. The pterygoid process, which forms the posterior wall of the pterygopalatine fossa, has beenpreserved. The nasal mucosa remains intact. The maxillary artery exits the infratemporal fossa to enter the pterygopalatine fossa.A., artery; A.I.C.A., anteroinferior cerebellar artery; Alv., alveolar; Ant., anterior; Bas., basilar; Cap., capitis; Car., carotid; Cav., cav-ernous; CN, cranial nerve; Eust., eustachian; Gl., gland; Inf., inferior; Infraorb., infraorbital; Int., internal; Intercav., intercavernous;Lat., lateral; Long., longus; M., muscle; Max., maxillary; Med., medial; N., nerve; Pal., palatini; Pet., petrous; Pteryg., pterygoid;Pterygopal., pterygopalatine; Tens., tensor; TM., temporomandibular; Vert., vertebral.
S182 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

and folded downward into the floor of the mouth (6). Themedial maxillotomy is a fourth and less extensive approachpermitting exposure of the clivus. It involves removing themedial part of the anterior maxillary wall and the part of themaxilla bordering the anterior piriform aperture (Fig. 6.15).This provides an opening through the sinus and adjacent partof the nasal cavity that exposes the clivus above the level ofthe upper side of the hard palate. The sinus wall and theanterior piriform aperture can be reconstructed at the end ofthe procedure. It can commonly be performed through adegloving incision, although a lateral rhinotomy incisionwould be used if there is a need to extend the approach to themedial orbit (11, 12).
In the first approach, with a LeFort osteotomy, the upperlip is elevated and a mucosal incision is made along theupper alveolar margin, extending around the molars onboth sides (Fig. 6.16). The mucosa is stripped off the ante-rior face of the maxilla below the infraorbital foramen. Thesaw cuts extend into the maxillary sinuses below the in-fraorbital foramen and high enough to avoid the dental
roots, and extending into the nasal cavity leaving thebranches of the internal maxillary artery and the nerves tothe maxilla and palate intact. The mucosa on the nasalsurface of the maxilla is dissected off, and the nasal septumis divided just above its attachment to the palate. The freedbone block includes, in one piece, the part of both maxilla andthe maxillary teeth situated below the infraorbital foramenwith their intact blood and nerve supply, which enters in theregion of the infratemporal fossa and pterygoid plates. Thefact that the soft palate is left intact reduces the incidence ofspeech and swallowing disorders. The intact maxillary block,however, blocks access to the craniovertebral junction, al-though it provides reasonable access to the upper and middlethird of the clivus. In an effort to increase access to thecraniovertebral junction, the LeFort osteotomy has been com-bined with a midline incision of the hard and soft palate, thusallowing the maxillary halves, with their attachment, to bereflected laterally (3). The disadvantage of the procedure isthe difficulty obtaining good dental occlusion and properfunctioning of the hard and soft palate.
FIGURE 6.14. E–H. Lower maxillotomy route to the clivus and foramen magnum. E, the nasal mucosa has been opened andthe posterior pharyngeal wall reflected to the opposite side. The longus capitis attachments have been separated from the cli-vus. F, the longus capitis and longus coli have been reflected laterally to expose the anterior arch of the atlas and the densand body of the axis. G, the clivus and the dura have been opened to expose the medulla and vertebral arteries. H, the expo-sure has been extended upward by removing the anterior wall of the sphenoid sinus and sella. The terminal part of thepetrous carotids limits the lateral exposure at the level of the clivus, and the cavernous carotids limit the lateral exposure atthe level of the sphenoid sinus. The intercavernous sinuses interconnect the paired cavernous sinuses.
Foramen Magnum S183
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.15. Medialmaxillotomy approach to theclivus and foramen magnum. A, alateral rhinotomy incision hasbeen extended along the medialorbital rim. The medial canthalligament has been exposed. B, themedial canthal ligament has beendivided to expose the medialaspect of the orbit. The ligamentcan be preserved and the medialorbital wall left intact if orbitalexposure is not needed. Theanterior pyriform aperture isexposed. C, the osteotomies areas outlined to open the nasalcavity and medial maxilla. Themedial one opens the nasal cavityand the lateral bone removalexposes the maxillary sinus. Themedial maxillotomy aids in expos-
ing the clivus. D, the exposure has been directed to the posterior nasopharyngeal wall behind which the clivus sits. The anteriorwall of the sphenoid sinus has been removed, exposing the sphenoid septum. The posterior part of the nasal septum has been re-moved to expose the clivus below the sphenoid sinus. Removal of the medial part of the posterior wall of the maxillary sinus ex-poses the maxillary artery in the pterygopalatine fossa. E, enlarged view of the pterygopalatine fossa exposed by removing the me-dial part of the posterior wall of the maxillary sinus. The maxillary nerve and artery enter the pterygopalatine fossa. The maxillaryartery is the major source of bleeding during surgery in this area. The maxillary artery enters the pterygopalatine fossa by passingthrough the pterygomaxillary fissure. The maxillary nerve enters the fossa by passing through the foramen rotundum and gives offcommunicating rami to the pterygopalatine ganglion. F, the pharyngeal mucosa has been opened, the longus capitis reflected later-ally, and the clivus and dura opened to expose the basilar artery ascending in front of the pons. The pituitary gland is at the uppermargin of the exposure. A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Bas., basilar; Cap., capitis; CN, cranialnerve; Eust., eustachian; Gang., ganglion; Gl., gland; Gr., greater; Lig., ligament; Long., longus; M., muscle; Max., maxillary; Med.,medial; N., nerve; Nasolac., nasolacrimal; Post., posterior; Pterygopal., pterygopalatine; Sphen., sphenoid; Vert., vertebral.
S184 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

In the lower subtotal maxillotomy approach, the part of halfof the maxilla, located below the orbital floor and infraorbitalcanal, is folded into the floor of the mouth on a hinge ofvascularized tissue, including the internal maxillary arteryand leaving the soft palate intact (Fig. 6.14) (2, 11). The hardpalate is divided in the midline, care being taken to preserve the soft
palate. This opens a route through the nasal and oral cavities to theclivus, foramen magnum, and upper cervical area.
In each of the approaches, the posterior part of the nasalseptum and turbinates may be removed to expose the poste-rior pharyngeal wall and provide access to the clivus andupper cervical vertebrae. These approaches also provide ac-
FIGURE 6.16. Transmaxillary approaches. Three variants of the transmaxillary approaches are shown. All three can be com-pleted through an intraoral incision with degloving. Another type of incision extending onto the face, such as a Weber-Fergusson incision, might be considered. A, the upper lip is elevated and the mucosa is incised along the upper alveolar mar-gin around the molars. The mucosa is elevated from the anterior face of the maxilla below the infraorbital foramen, but highenough to avoid the dental roots. The mucosa is elevated from the nasal surface of the maxilla, and the nasal septum isdivided above its attachment to the palate. B, the saw cuts (solid line) extend into the maxillary sinus on both sides. The freeblock of maxilla is moved downward (arrow) to give access to the clivus. C, the intraoral retractor has been placed. Displac-ing the maxilla downward gives wide access to the clivus. D, a modified technique, called the extended maxillectomy,includes the LeForte I osteotomy with a midline incision of the hard and soft palate (solid lines). E, this allows the halves ofthe maxilla, which are attached to the muscles and vessels in the infratemporal fossa, to be reflected laterally, providingwider exposure to the clivus and upper cervical spine. F, retractors have been placed to expose the clivus and upper cervicalarea. The approach can be extended upward into the sphenoid and ethmoid sinuses and downward to C2 or C3. G–I. Unilat-eral maxillotomy. G, in this approach, half of the maxilla is mobilized by a bone cut, which extends back to the infratemporalfossa in the area just below the infraorbital foramen, and the maxilla is divided in the midline. A mucosal incision is madealong the low surface of the hard palate parallel to the midline on the side opposite the saw cut through the hard palate, andthe anterior face of the maxilla is degloved on one side. The soft palate is left intact. H, the unilateral block of maxilla, whichis still attached to the structures in the infratemporal fossa along the pterygoid plates and to the soft palate, which is notinterrupted, is folded downward into the floor of the mouth. I, the anterior part of the nasal septum is left undisturbed, butthe posterior part is removed along with some of the turbinates and wall of the sinuses to provide a wide exposure of the cli-vus. This exposure can be enlarged to include the walls of the sphenoid and ethmoid sinuses. (From, Rhoton AL Jr: Anatomi-cal basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Sur-gery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)
Foramen Magnum S185
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

cess to the sphenoid and ethmoid sinuses and the sella, andthe medial part of the floor of the anterior fossa. The posteriorpart of the mucosa on both sides of the nasal septum may beprepared to provide flaps that can be folded into the clivaldefect for closure. In addition, planning will allow for a tempo-ralis muscle graft to be folded into the clival defect for closure.The incidence of swallowing and speech difficulties is signifi-cantly greater with those approaches in which the soft palate is
divided than when it is left intact. In each approach, plates andscrews are positioned before making the bone cuts to achievesatisfactory dental occlusion after the procedure. The unilaterallower maxillotomy provides a more rapid recovery of oropalatalfunction because only half of the maxilla is disturbed, and thesoft palate remains intact. That approach to the clivus is slightlyoblique, but can provide as wide an exposure as is achieved withthe approaches involving a bilateral maxillotomy.
Transsphenoidal approachThe transsphenoidal approach along the nasal septum may
be used to expose the upper third of the clivus (Figs. 6.9-6.11and 6.17) (10). The vomer is resected to enter the sphenoidsinus and expose the floor of the sella turcica and the ventralsurface of the clivus. The anterior nasal spine and the anteriorpart of the septal cartilage are preserved. In approaching theclivus, the floor of the sella turcica may be removed and thebony opening extended downward on the clivus to the infe-rior margin of the sphenoid sinus. Lesions extending to theupper third of the clivus may be biopsied or partially re-moved through this approach. The sellar and clival openingsare closed with fat or muscle and nasal septal cartilage. Theadvantage of this approach is the low complication rate, andthe disadvantage is the small operative field limited to thesuperior third of the clivus.
Transcervical approachThe transcervical approach, as performed by Stevenson et
al., is directed through the fascial planes of the neck to theregion of the foramen magnum (Fig. 6.18) (31). It avoidsopening the oropharyngeal mucosa, but is selected infre-quently because of the depth of the exposure and because it isnot a direct midline exposure. A tracheostomy, which allowsthe jaws to be closed tightly, facilitates the exposure. TheT-shaped skin incision includes a submandibular incisionfrom the mastoid tip to the symphysis menti and an inferiorextension carried from the midpoint of the submandibularincision across the sternocleidomastoid muscle. The fascialplane between the pharynx and the prevertebral muscles isreached through an exposure directed along the anterior bor-der of the sternocleidomastoid muscle and between the ca-rotid sheath laterally and the esophagus and trachea medially.The prevertebral fascia and muscles are retracted laterally toexpose the ventral aspect of the clivus, atlas, and axis. Struc-tures that may be divided from below to above to increase theexposure include the ascending pharyngeal and superior thy-roid arteries, external laryngeal nerve, ansa hypoglossi, internallaryngeal nerve, lingual artery, hypoglossal nerve, stylohyoidmuscle, anterior belly of the digastric muscle, stylohyoid liga-ment, glossopharyngeal nerve, and the stylopharyngeus andstyloglossus muscles. The anterior arch of the atlas and theodontoid process, and a 2 cm width of clivus extending from theforamen magnum to the sphenooccipital synchondrosis may beremoved. Deviation laterally may damage the internal jugularvein, internal carotid artery, eustachian tube, and the ninththrough the twelfth cranial nerves.
FIGURE 6.17. Transsphenoidal approach. A, Upper left, thisapproach, directed beneath the upper lip, along the nasalseptum, and through the sphenoid sinus, may be used toexpose the upper third of the clivus. The resectable area(oblique lines) includes the floor and anterior wall of the sella,the vomer, and the upper third of the clivus. This approach issuitable for biopsying some tumors that extend upward fromthe foramen magnum. Lower right, a cup forceps biopsies aclival tumor. B, view through nasal speculum. The anteriornasal spine is preserved and the anterior part of the septal carti-lage remains attached to the septal mucosa on one side. Thenasal speculum is inserted between the left side of the nasalseptum and its mucosa. The nasal septum and the mucosa onthe right side of the septum are pushed to the right by thespeculum, and the mucosa on the left side of the septum ispushed to the left. The keel on the vomer is exposed. C, magni-fied view. The vomer has been removed to open the sphenoidsinus. The sellar floor is above the midline septum. In approach-ing the clivus, the floor of the sella is removed, and the openingin the bone is extended downward on the clivus (interruptedlines) to the inferior margin of the sphenoid sinus.
S186 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.18. A, transcervical approach. A tracheostomy allows the jaws to be closed tightly. The T-shaped skinincision (interrupted lines) includes a submandibular incision extending from the mastoid tip to the symphysismenti and an inferior extension carried downward across the sternocleidomastoid muscle. B, the resectable area(oblique lines) includes the clivus, anterior arch of the axis, and the body of the odontoid process of the axis. C,the exposure is directed along the anterior border of the sternocleidomastoid and between the external andinternal carotid arteries and internal jugular vein laterally, and the esophagus, hypopharynx, and trachea medially.Structures that may be divided to increase the exposure include the ascending pharyngeal and superior thyroidarteries, the external laryngeal nerve, ansa hypoglossi, internal laryngeal nerve, lingual artery, hypoglossal nerve,stylohyoid muscle, anterior belly of the digastric, stylohyoid ligament, glossopharyngeal nerve, and the stylopharyn-geus and styloglossus. The accessory nerve passes behind the sternocleidomastoid. D, the prevertebral fascia and lon-gus capitis and longus colli are separated in the midline from the clivus to C3 and are retracted laterally using sub-periosteal dissection to expose the ventral aspect of the clivus, atlas, and axis. E and F, the anterior arch of the atlasand the odontoid process, and a 2.5-mm width of clivus extending from the foramen magnum to the spheno-occipitalsynchondrosis may be removed. The basilar, vertebral, and anterior spinal arteries are exposed in the dural opening.After dealing with the pathology, the dura is closed, muscle and fat are placed in the clival window, and the preverte-bral and fascia are sutured in the midline. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to theregion of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junc-tion. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].) A., artery; Ant., anterior; Bas., basilar; Car.,carotid; Ext., external; Inf., inferior; Int., internal; Jug., jugular; M., muscle; Sp., spinal; Sup., superior; V., vein; Vert.,vertebral.
Foramen Magnum S187
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.19. A–F. Relationships in the transbasal and extended frontal approaches. A, a bicoronal scalp flap has been reflected forward.The pericranium is commonly reflected as a separate layer for later use in closing the floor of the anterior cranial fossa. B, bone flap andosteotomy. The transcranial-transbasal approach uses only a bifrontal craniotomy bordering the floor of the anterior cranial fossae with-out the osteotomy. A large bifrontal craniotomy and a fronto-orbitozygomatic osteotomy have been completed. The osteotomized seg-ment may extend through the nasal bone and lateral orbital rim, but for most clival lesions a more limited bone flap and osteotomy (dot-ted lines) will usually suffice and can be tailored as needed to deal with involvement of the nasal cavity, paranasal sinuses, or orbit. C, theperiorbita has been separated from the walls of the orbit in preparation for the osteotomies. Division of the medial canthal ligament is notnecessary for most lesions, but may be required for lesions extending into the lower nasal cavity or orbit. The ligaments should bere-approximated at the end of the procedure. D, the right medial canthal ligament has been divided and the orbital contents retractedlaterally to expose the nasolacrimal duct and the anterior ethmoidal branch of the ophthalmic artery at the anterior ethmoidal foramen.E, the osteotomies have been completed and the frontal dura elevated. The dura remains attached at the cribriform plate. The upper partof both orbits are exposed. F, an osteotomy around the cribriform plate leaves it attached to the dura and olfactory bulbs, a maneuver
S188 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

FIGURE 6.19. G–L. Relationships in the transbasal and extended frontal approaches. G, the sphenoid sinus has been opened to exposethe septa within the sinus. The sphenopalatine arteries cross the anterior face of the sphenoid. H, the septa within the sphenoid sinus, thesellar floor, and the lateral sinus wall have been removed to expose the cavernous carotid arteries, pituitary gland, and optic canals. I, theclivus has been opened to expose the dura facing the brainstem. The basilar sinus, which interconnects the posterior parts of the cavern-ous sinus, is situated between the layers of dura on the upper clivus. J, the clivus has been opened to expose the tortuous vertebral arter-ies, which join to form the basilar artery at the left lateral margin of the clival opening. Both AICA origins are exposed. A vein splits theright abducens nerve into two bundles adjacent to the brainstem. K, the frontal dura has been opened and the frontal lobes elevated toexpose the olfactory and optic nerves, the internal carotid, and the anterior and middle cerebral arteries. L, enlarged view. The subfrontaland clival openings are separated by the sella and pituitary gland. The lateral limit of the clival exposure is defined by the internal carotidarteries and optic nerves. The lamina terminalis is exposed above the optic chiasm.Š
that has been attempted to preserve olfaction, but is infrequently successful. The anterior face of the sphenoid sinus and both sphenoidostia are exposed between the orbits. A., artery; A.C.A., anterior cerebellar artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior;Bas., basilar; Car., carotid; CN, cranial nerve; Ethm., ethmoidal; Gl., gland; Lam., lamina; Lig., ligament; M.C.A., middle cerebral artery;Med., medial; Nasolac., nasolacrimal; Pit., pituitary; Sphen., sphenoid; Sphenopal., sphenopalatine; Sup., superior; Term., terminalis; Turb.,turbinates; Vert., vertebral.
Foramen Magnum S189
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

Transcranial-transbasal approachThe subfrontal-transbasal approach may be used to ap-
proach tumors of the anterior side of the foramen magnum ifthe tumor also involves and requires resection of part of theethmoid and sphenoid bones, and the clivus (Figs. 6.19 and6.20). The transbasal approach, as performed by Derome (6), ismade through a bicoronal scalp incision placed behind thehairline and a bifrontal free bone flap situated strictly su-praorbital without regard for the frontal sinuses. The subfron-tal dura mater is separated from the orbital roofs, the olfactorynerves are divided at the cribriform plates, and the extraduraldissection is carried posteriorly to the lesser wings of thesphenoid bone, the tuberculum sellae, and the base of theanterior clinoid processes. Attempts have been made to leavethe olfactory bulbs attached to the cribriform plate, but thishas usually not prevented the loss of the sense of smell seencommonly after these procedures. The clivus is reached afterresecting the posterior part of the floor of the anterior cranialfossa, the upper part of the walls of the ethmoid and sphenoidsinuses, and the floor of the sella turcica. Proceeding down-ward from the sellar floor, the clivus is removed to open the
anterior margin of the foramen magnum. Separation of thepharyngeal mucosa from the front of the spine permits expo-sure of the anterior arch of the atlas, and even the C2 and C3vertebral bodies. The nasal and pharyngeal mucosa are notopened in the transcranial transbasal approach, but are com-monly exposed in those procedures that include a supraor-bital osteotomy in addition to a bifrontal flap. Dural defectsare closed with a leak-proof dural substitute, more than twicethe size of the defect, which is sutured to the dura mater at themost remote margins of the exposure. The orbital roofs andthe remainder of the cranial base are reconstructed usingautogenous bone grafts. If the clivus has been removed, thegraft above the ethmosphenoidal space is fitted into the edgeof a vertical graft extending from the anterior margin of theforamen magnum or the anterior arch of the atlas to the floorof the sella. The advantages of the transbasal approach arethat a tighter closure of the dura mater is possible than can beachieved through the transoral approaches, the subcranialmucosal planes can be preserved, and it can be combined withanother intradural approach without the high risk of infectionassociated with the transoral approaches. The transbasal ap-
FIGURE 6.20. A, the transcranial-transbasal approach may be usedto approach tumors of theanterior edge of the foramenmagnum if the tumor alsoinvolves and requires resection ofpart of the ethmoid and sphenoidbones (oblique lines). B, insert.The souttar scalp incision issituated behind the hairline, andthe bifrontal craniotomy(interrupted lines) is placedstrictly supraorbital withoutregard for the frontal sinuses(oblique lines). Lower right. Thesubfrontal dura is separated fromthe orbital roofs and theextradural dissection is carried tothe lesser wings of the sphenoidbone, the tuberculum sellae, andthe base of the anterior clinoidprocesses. The clivus is reachedafter resecting the posterior partof the floor of the anterior cranialfossa, the upper part of the wallsof the ethmoid and sphenoidsinuses, and the floor of the sella.
Proceeding downward, the clivus is removed to open the anterior margin of the foramen magnum. Separation of the pharyngealmucosa from the front of the spine exposes the anterior arch of the atlas, and even the front of the C2 and C3 vertebral bodies.The nasal and pharyngeal mucosa should not be opened. Dural defects are closed with a leak-proof dural graft after dealing withthe lesion. C, the orbital roof and the remainder of the cranial base are reconstructed using bone grafts. If the clivus has beenremoved, the graft above the ethmosphenoidal space is fitted into the edge of a vertical graft extending from the anterior margin ofthe foramen magnum or the anterior arch of the atlas to the floor of the sella. (From, Rhoton AL Jr: Anatomical basis of surgicalapproaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the CraniovertebralJunction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)
S190 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

proach may be combined with a transbasal-transsphenoidalroute to gain access to the sella turcica. In the transbasalapproach the clivus and sphenoid bone can be resected moreextensively than by the transsphenoidal approach, but thesubsellar area is hidden by the bulging dura in the transbasalapproach. Both approaches may be combined to permit re-moval of all of the clivus below the level of the dorsum sellae.Anosmia is the only certain side effect. The most frequentcomplications are cerebrospinal fluid leaks, meningitis, andpseudomeningoceles.
Extended frontal approachThe extended frontal approach is similar to the transcranial-
transbasal approach, except that it includes an orbitofrontoeth-moidal osteotomy (Figs. 6.19 and 6.21) (28). It may also be usedto approach tumors of the anterior side of the foramen magnum,especially if the tumor requires resection of part of the ethmoidand sphenoid bones as well as the clivus. The approach uses asouttar scalp incision, bifrontal bone flaps, and an orbitofronto-ethmoidal osteotomy in which the supraorbital ridges, and partof the orbital roofs and possibly the upper nasion, the roof of theethmoid sinuses, and the cribriform plate are removed in a singleblock. The resection of the lesion may involve an extradural orcombined intradural-extradural approach. The clivus and fora-
men magnum are reached after resecting the posterior part of thefloor of the anterior cranial fossa, the upper walls of the ethmoidand sphenoid sinuses, and the floor of the sella. If needed, thesupraorbital osteotomy can even be tailored in size and site toinclude the lateral orbital rims.
Selection of operative approach
Anterior extradural lesions of the clivus or upper cervicalvertebrae are best reached by one of the anterior approaches.The transoral approach is selected for most anterior extra-dural lesions involving the foramen magnum because it pro-vides a midline exposure and is the most direct route to thepathology. For more extensive lesions, a transmaxillary ap-proach may be considered. Before selecting an anteriorapproach that would require that the dura mater be openedthrough the oropharynx, one should consider choosing a pos-terior approach since the incidence of cerebrospinal fluidleak, meningitis, and pseudomeningocele is high if thedura mater is opened through the oropharynx. The transcer-vical approach has the advantage of reaching the foramenmagnum through the deep fascial planes of the neck ratherthan through the oropharynx; however, the depth of the ex-posure, the length of the time required to complete the dis-section, and the fact that the foramen magnum is not ap-
FIGURE 6.21. Extended frontalapproach. A, the upper left insertshows the scalp flap and the orderof the removal of the cranialbones (1, 2, 3). The third step, theorbitofrontoethmoidal osteotomy,includes both supraorbital ridges,the anterior part of the roof of theorbits, the frontal sinus,cribriform plate, and part of theethmoid air cells in one block. B,sagittal view. The oblique linesalong the skull base show thepossible extent of the boneremoval. The foramen magnum isreached after removing theposterior part of the floor of theanterior fossa, the ethmoid aircells, walls of the sphenoid sinus,and the clivus. C, the periorbita isexposed along both orbital roofs.The bone removal has beenextended into the ethmoid aircells and the sphenoid sinus. Theexposure can be extended alongthe clivus down to the foramenmagnum. D, use of pericranial
flap for reconstruction. A fat graft is placed in the ethmoid and sphenoid sinuses before reflecting the pericranial flap overthem. In addition, a fat graft may also be applied to the inner side of the pericranial flap. (From, Rhoton AL Jr: Anatomicalbasis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgeryof the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)
Foramen Magnum S191
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

proached from the midline have prevented it from gainingcommon usage. The transcranial-transbasal and extendedfrontal approaches offer another anterior route for reachingthe foramen magnum, however these approaches should notbe considered for approaching a tumor strictly localized in theregion of the foramen magnum, but might be used for anextensive lesion involving the ethmoid and sphenoid sinusesas well as the clivus and foramen magnum. The transsphe-noidal approach provides an easy route for biopsying lesionsin the region of the foramen magnum if they extend to theupper third of the clivus, but it does not provide adequateexposure for removing larger lesions of the region. The trans-sphenoidal approach may be combined with another ap-proach in removing lesions involving the clivus and foramenmagnum.
The posterior approaches are preferred for most intradurallesions. The vertical midline incision, and a bilateral suboccipitalcraniectomy and upper cervical laminectomy is used for lesionssituated in the upper spinal canal and posterior or posterolateralin the area above the foramen magnum. The hockey-stick inci-sion and a unilateral suboccipital craniectomy and upper cervi-cal laminectomy is selected if the lesion extends anterolateral oranterior to the brainstem toward the jugular foramen or cerebel-lopontine angle. The far-lateral modification of the lateral sub-occipital approach, described in the next chapter on the farlateral approach, gives a more direct approach to lesions ventralto the brainstem and along the anterior rim of the foramenmagnum, while reducing the need for retraction of neural struc-tures (32, 33). The foramen magnum can also be reached throughthe approaches directed through the temporal bone, the subjectof the chapter on the temporal bone; however, for reaching theforamen magnum and clivus, these approaches may requirerepositioning of the carotid artery or facial nerve, and possiblyresection of the auditory and vestibular labyrinth.
Reprint requests: Albert L. Rhoton, Jr., M.D., Department of Neuro-logical Surgery, University of Florida Brain Institute, P.O. Box 100265,100 South Newell Drive, Building 59, L2-100, Gainesville, FL32610-0265.
REFERENCES
1. Abbott KH: Foramen magnum and high cervical cord lesionsstimulating degenerative disease of the nervous system. OhioState Med J 46:645–651, 1950.
2. Cocke EW Jr, Robertson JH, Robertson JT, Crook JP Jr: The ex-tended maxillotomy and subtotal maxillectomy for excision ofskull base tumors. Arch Otolaryngol Head Neck Surg 116:92–104, 1990.
3. Crockard HA: The transmaxillary approach to the clivus, inSekhar LN, Janecka IP (eds): Surgery of Cranial Base Tumors. NewYork, Raven Press, 1993, pp 169–180.
4. Cushing H, Eisenhardt L: Meningiomas. Springfield, Charles CThomas, 1938, pp 169–180.
5. de Oliveira E, Rhoton AL Jr, Peace DA: Microsurgical anatomy ofthe region of the foramen magnum. Surg Neurol 24:293–352,1985.
6. Derome P: The transbasal approach to tumors invading the baseof the skull, in Schmidek HH, Sweet WH (eds): Current Techniquesin Operative Neurosurgery. New York, Grune and Stratton, 1977,pp 223–245.
7. DiChiro G, Anderson WB: The clivus. Clin Radiol 16:211–223, 1965.8. Friede RL, Roessmann U: Chronic tonsillar herniation: An at-
tempt at classifying chronic herniations at the foramen magnum.Acta Neuropathol (Berl) 34:219–235, 1976.
9. Haas LL: The posterior condylar fossa, foramen, and canal andthe jugular foramen. Radiology 69:546–552, 1957.
10. Hardy J, Grisoli F, Leclercq TA, Marino R: Trans-sphenoidalapproach to tumors of the clivus [in French]. Neurochirurgie23:287–297, 1977.
11. Hitotsumatsu T, Rhoton AL Jr: Unilateral upper and lower sub-total maxillectomy approaches to the skull base: Microsurgicalanatomy. Neurosurgery 46:1416–1453, 2000.
12. Hitotsumatsu T, Matsushima T, Rhoton AL Jr: Surgical anatomyof the midface and the midline skull base, in Spetzler RF (ed):Operative Techniques in Neurosurgery. W.B. Saunders Co., 1999, vol2, pp 160–180.
13. Huang YP, Wolf BS: Veins of the posterior fossa, in Newton TH,Potts DG (eds): Radiology of the Skull and Brain. St. Louis, C.V.Mosby, 1974, vol 2, book 3, pp 2155–2219.
14. Katsuta T, Rhoton AL Jr, Matsushima T: The jugular foramen:Microsurgical anatomy and operative approaches. Neurosurgery41:149–202, 1997.
15. Kirdani MA: The normal hypoglossal canal. Am J RoentgenolRadium Ther Nucl Med 99:700–704, 1967.
16. Lister JR, Rhoton AL Jr, Matsushima T, Peace DA: Microsurgicalanatomy of the posterior inferior cerebellar artery. Neurosurgery10:170–199, 1982.
17. Margaretten I: Syndromes of the anterior spinal artery. J NervMent Dis 58:127–133, 1923.
18. Matsushima T, Rhoton AL Jr, de Oliveira E, Peace DA: Microsur-gical anatomy of the veins of the posterior fossa. J Neurosurg59:63–105, 1983.
19. Matsushima T, Rhoton AL Jr, Lenkey C: Microsurgery of thefourth ventricle: Part 1—Microsurgical anatomy. Neurosurgery11:631–667, 1982.
20. Newton TH: The anterior and posterior meningeal branches ofthe vertebral artery. Radiology 91:271–279, 1968.
21. Newton TH, Mani RL: The vertebral artery, in Newton TH, PonsDG (eds): Radiology of the Skull and Brain. St. Louis, C.V. Mosby,1974, vol 2, book 2, pp 1659–1709.
22. Ouaknine G, Nathan H: Anastomotic connections between theeleventh nerve and the posterior root of the first cervical nerve inhumans. J Neurosurg 38:189–197, 1973.
23. Piehl MR, Reese HH, Steelman HF: The diagnostic problem oftumors at the foramen magnum. Dis Nerv Syst 11:67–76, 1950.
24. Rhoton AL Jr: Anatomical basis of surgical approaches to theregion of the foramen magnum, in Dickman CA, Spetzler RF,Sonntag VKH (eds): Surgery of the Craniovertebral Junction. NewYork, Thieme Medical Publishers, Inc., 1998, pp 13–57.
25. Rhoton AL Jr, Buza R: Microsurgical anatomy of the jugularforamen. J Neurosurg 42:541–550, 1975.
26. Rhoton AL Jr, de Oliveira E: Suboccipital and retrosigmoid ap-proaches to the craniovertebral junction, in Dickman CA, SpetzlerRF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction.New York, Thieme Medical Publishers, Inc., 1998, pp 659–681.
27. Russell DS, Rubinstein LJ: Pathology of Tumors of the NervousSystem. Baltimore, Williams & Wilkins, 1977, ed 4, p 368.
S192 Rhoton
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement

28. Sekhar LN, Nanda A, Sen CN, Snyderman CN, Janecka IP: Theextended frontal approach to tumors of the anterior, middle andposterior skull base. J Neurosurg 76:198–206, 1992.
29. Sen CN, Sekhar LN: An extreme lateral approach to intradurallesions of the cervical spine and foramen magnum. Neurosurgery27:197–204, 1990.
30. Stein BM, Leeds NE, Taveras JM, Pool JL: Meningiomas of theforamen magnum. J Neurosurg 20:740–751, 1963.
31. Stevenson GC, Stoney RJ, Perkins RK, Adams JE: A transcervicaltransclival approach to the ventral surface of the brainstem forremoval of a clivus chordoma. J Neurosurg 24:544–551, 1966.
32. Tedeschi H, Rhoton AL Jr: Lateral approaches to the petroclivalregion. Surg Neurol 41:180–216, 1994.
33. Wen HT, Rhoton AL Jr, Katsuta T, de Oliveira E: Microsurgicalanatomy of the transcondylar, supracondylar, and paracondylarextensions of the far-lateral approach. J Neurosurg 87:555–585, 1997.
Drawings by Leonardo da Vinci of the human cranium and spinal canal. Measurement lines indicate an interest in thestudy of anatomic proportions. Courtesy, Dr. Edwin Todd, Pasadena, California. (Also see pages S6 and S286.)
Foramen Magnum S193
Neurosurgery, Vol. 47, No. 3, September 2000 Supplement