Embed Size (px)
Citation preview

The Foot and Ankle Online Journal Official Publication of the International Foot & Ankle Foundation faoj.org / ISSN 1941-6806
Differences in the degree of stretching applied to Achilles tendon fibers when the calcaneus is pronated or supinated by Mutsuaki Edama1,5*, Masayoshi Kubo1, Hideaki Onishi1, Tomoya Takabayashi1, Takuma Inai2, Hiroshi Watanabe3, Satoshi Nashimoto4, Ikuo Kageyama5
The Foot and Ankle Online Journal 9 (3): 5
Purpose: The purpose of the present study was to examine the degree of stretching (%) that is applied to each of the tendon fiber bundles that compose the Achilles tendon (AT) by twist type when the calcaneus is pronated or supinated. Methods: Three AT twist types (least, moderate, extreme twists), one for each type were investigated. Using the MicroScribe system, the AT and the calcaneal tuberosity were digitized to reconstruct three-dimensional models. Using this system, the calcaneus rotations in the pronation (20°) and supination (20°) directions were simulated, and the degrees of stretching (%) of each tendon were calculated. Results: For all twist types, when the calcaneus was pronated, the medial head of the gastrocnemius (MG) and lateral head of the gastrocnemius (LG) shortened and the soleus muscle (Sol) stretched, and when supinated, MG and LG stretched and Sol shortened. In particular, severe twist type had the largest degree of stretching of Sol when the calcaneus was pronated (Type I: 1.7% ± 3.4%, Type II: 2.4% ± 1.4%, Type III: 3.7% ± 6.0%), and furthermore, each tendon fiber composing Sol had different degrees of stretching. Conclusions: The study results suggest that the degree of stretching applied within the AT with calcaneus pronation is not constant, and that, especially in Type III twists, the risk of developing AT disorders may increase. Keywords: three-dimensional models, twisted structure, Achilles tendon disorder
This is an Open Access article distributed under the terms of the Creative Commons Attribution License. It permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ©The Foot and Ankle Online Journal (www.faoj.org), 2016. All rights reserved.
chilles tendon (AT) disorders are a type of typical skeletal muscle overuse syndrome and are known to affect activities of daily living,
work, and sports activity of an individual [1]. The incidence of AT disorders is 8-15% in recreational runners [2, 3] and approximately 24% in athletes [4], indicating a high incidence among disorders of the lower leg.
These disorders typically appear 2-6 cm proximal to the site where the AT attaches to the calcaneus [5, 6], and they are known to occur more commonly on the medial side than the lateral side [1, 7]. The reasons for the high prevalence at this specific site are that the area 2-6 cm proximal has a poor blood supply [8-10], and that the cross-sectional area of the AT is small [11, 12].
1- Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Shimami-cho 1398, Kita-ku, Niigata City, Niigata 950-3198, Japan 2- Department of Rehabilitation, Oguma Orthopedics Clinic, Niigata 950-2023, Japan 3- Department of Rehabilitation, Nagaoka Chuo General Hospital, Nagaoka, Japan 4- Department of Rehabilitation, Niigata Medical Center, Niigata 950-2022, Japan 5- Department of Anatomy, School of Life Dentistry at Niigata, Nippon Dental University, Niigata 951-8580, Japan * - Corresponding Author: [email protected] ISSN 1941-6806 doi: 10.3827/faoj.2016.0903.0005

The Foot and Ankle Online Journal 9 (3): 5
Therefore, a strong stress onto an area with a small AT cross-sectional area and poor blood supply is considered to be one of the causes for the development of AT disorders. However, the mechanism of onset is not thoroughly understood. This is most likely why the incidence of AT disorders is very high [2-4] and why preventive methods are not well-established [1]. Recently through previous studies, non-uniform strain in the AT has become a focus as a mechanistic factor in the development of AT disorders. Previous studies have shown that, with passive movements of the ankle and contraction of the triceps surae, different strains arise at each fascia that form the triceps surae, including the AT, in human subjects [13-15] and in cadavers [16-18]. In the more recent past, a study in fresh cadavers [19] focused on the twisted structure of the AT as a factor for non-uniform strain in the AT. Since patients with AT disorders have excessive pronation of the rearfoot in midstance during walking [20], it has been postulated that a strong load applied to a condition where AT twist is loosened may be the mechanism for the development of non-uniform strain in the AT. Additionally, Clement et al [21] postulated that the development of a “whipping action” at the AT due to excessive pronation of the foot may be the mechanism for the onset of AT disorders or AT rupture. However, the limitation of these reports is that they did not account for the extent of twisting. There are numerous studies from the past several decades concerning the twisted structure of the AT. Several studies have unanimously reported that ATs are composed of an insertion tendon where the medial head of the gastrocnemius (MG), lateral head of the gastrocnemius (LG), and the soleus muscle (Sol) insert, exhibit twisted structures, and are all twisted in the lateral direction without exception [1, 22-27]. While a consensus has yet to be reached in terms of the extent of twisting, we previously classified the extent of twisting into three types: Type I (least), Type II (moderate), and Type III (extreme) [26]. From this particular study, we postulated that the extent of twisting may greatly affect the strain applied to each fiber bundle that composes the AT.
The purpose of this study was to investigate the degrees of stretching applied to each of the tendon fiber bundles of MG, LG, and Sol that compose the AT when the calcaneus is rotated, focusing on the differences among twist types. Material and methods Cadavers: Three legs from three Japanese male cadavers (mean age: 83 ± 18 years old, left side) that had been switched to alcohol after placement in 10% formalin were used in this study. This study was approved by the Ethics Committee of our university. Methods: AT dissection was conducted referring to a procedure reported previously [27]. First, from the facies posterior cruris, skin, subcutaneous tissue, and crural fascia were removed, and the triceps surae was extracted along with a portion of the calcaneus. Next, the AT fiber bundle attached to the muscle belly of MG and LG and the AT fiber bundle attached to the Sol muscle belly were separated. Since these fiber bundles are extremely strongly fused to each other, the fiber bundles were separated with care. Next, the connective tissue surrounding the AT was removed carefully, and the AT fiber bundle attached to the muscle belly of MG and LG was separated. Although these AT fiber bundles are strongly fused, by following the path of a relatively thick tendon fiber that represents each of these tendon fiber bundles, the border between them could be identified for separation. Furthermore, each fiber bundle was finely separated into 3 to 4-mm tendon fibers. In general, MG was separated into 4-9 tendon fibers, LG was separated into 3-9 fibers, and Sol was separated into 10-14 fibers (Figure 1). Subsequently, each leg was defined as Type I (least), Type II (moderate), or Type III (extreme), one leg for each type, based on a classification determined in a previous study [27]. In the next step, the collected triceps surae muscle specimens were firmly fixed to the table such that they did not move, and a 3D Digitizer MicroScribe system (G2X-SYS, Revware, NC, USA) was used to create a three-dimensional reconstruction by digitizing the furthest distal end of the muscle-tendon junction of MG, LG, and Sol and the calcaneal tuberosity insertion site. Rhinoceros 3D software (McNeel, Seattle, WA) was used for three-dimensional construction (Figure 2).
Copyright © 2016 The Foot and Ankle Online Journal

The Foot and Ankle Online Journal 9 (3): 5
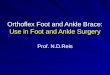
Figure 1 The methods of fine dissection of each fiber bundle, the left Achilles tendon, posterior view. L, lateral; M, medial; LG, fascicle from the lateral head of the gastrocnemius; MG, fascicle from the medial head of the gastrocnemius; Sol, fascicle from the soleus muscle. Finally, the midpoint of the 4 points on the lateral side of the calcaneal tuberosity was defined as the center of rotation, and an absolute coordinate system was created with this center of rotation set at the origin (Figure. 3). The degrees of stretching of each tendon were calculated when calcaneus pronation (20°) and supination (20°) were simulated on this coordinate system. The degree of stretching (%) was calculated using: [(length of tendon fiber after calcaneus rotation ÷ length of tendon fiber before rotation) x 100) - 100] (Figure 3). SCILAB-5.5.0 (Scilab Enterprises, Orsay, France) was used for analysis.
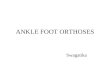
Figure 2 The threedimensional construction diagrams, the left Achilles tendon. A: The lateral view. B: The vertical view. C: The proximal view. Red line: The fiber bundles from the medial head of the gastrocnemius. Blue line: The fiber bundles from the lateral head of the gastrocnemius. Yellow line: The fiber bundles from the soleus muscle. The MicroScribe system is an instrument with high precision (manufacturer specification: 0.23 mm precision in measurements). However, measurements must be made manually, and, furthermore, the study cadavers have soft tendon tissues because they were switched to alcohol after formalin fixation. In addition, although the study cadavers were thoroughly fixed to the examination table such that they did not move, it was necessary to test whether or not they had moved, since the measurements entail the dissection of the tendon tissue. Therefore, the reliability and validity of the measurements made with the MicroScribe system were verified by measuring 10 arbitrary tendon fibers 3 times and determining the intraclass correlation coefficient (ICC(1,1)). Moreover, to assess whether the cadavers had moved during these measurements, the intraclass correlation coefficients (ICC (1,1)) of the 4 points lateral to the calcaneal tuberosity were determined using pre- and post-measurement values.
Copyright © 2016 The Foot and Ankle Online Journal

The Foot and Ankle Online Journal 9 (3): 5
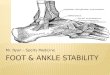
Figure 3 The center of rotation of the calcaneal tuberosity, the left Achilles tendon. A: The center of rotation of the calcaneal tuberosity. B: The local coordinate system of calcaneal tuberosity. Green points: the four points of the outside of the calcaneal tuberosity. Red point: The center of rotation of the calcaneus, the midpoint of the four points of the outside of the calcaneal tuberosity. The origin is the center of rotation of the calcaneus, the Xaxis is defined toward the proximal, the Yaxis is defined toward the medial, and the Zaxis is back. Black arrow: the pronation direction, the opposite direction is the supination direction.
Figure 4 The threedimensional construction diagrams, Type I, Type II, Type III, the left Achilles tendon, back view. A: Type I; B: Type II; C: Type III. Red line: The fiber bundles from the medial head of the gastrocnemius. Blue line: The fiber bundles from the lateral head of the gastrocnemius. Yellow line: The fiber bundles from the soleus muscle.
Figure 5 The threedimensional construction diagrams, the left Achilles tendon, back view. A: The left Achilles tendon of type III. B: The fiber bundles from the soleus muscle. Red line: The fiber bundles from the medial head of the gastrocnemius. Blue line: The fiber bundles from the lateral head of the gastrocnemius. Yellow line: The fiber bundles from the soleus muscle.
Figure 6 The degree of stretching applied to each of the tendon fiber bundles. Values represent means ± SD. The degree of stretching (%) = [ (the fiber length of the motion ÷ the fiber length of the rest)×100)-100]. deg (°): Angle of pronation direction and supination direction. A: The degree of stretching applied to each of the type I tendon fiber bundles, B: The degree of stretching applied to each of the type II tendon fiber bundles, C: The degree of stretching applied to each of the type III tendon fiber bundles. MG: Fascicle from the medial head of the gastrocnemius (Red bar). LG: Fascicle from the lateral head of the gastrocnemius (Blue bar). Sol: Fascicle from the soleus muscle (Yellow bar).
Copyright © 2016 The Foot and Ankle Online Journal

The Foot and Ankle Online Journal 9 (3): 5
Results Reliability and reproducibility of a MicroScribe 3-dimensional digitizer measurement: The ICC (1,1) of the measurements at the tendon fiber was 0.97. The ICC (1,1) of the measurements at the calcaneal tuberosity was 0.99. The three-dimensional construction diagrams, Type I, Type II, Type III (Figure 4) In Type III, the Sol located at a deep layer under the AT inserted onto the medial aspect of the surface of the calcaneal tuberosity. Therefore, the paths of each tendon fiber that compose the Sol varied greatly (Figure 5). The degree of stretching applied to each of the tendon fiber bundles by twist type: The degrees of stretching were as follows: for Type I, MG: -1.6% ± 0.9%, LG: -2.2% ± 0.2%, Sol: 1.7% ± 3.4% with 20° pronation and MG: 1.3% ± 0.7%, LG: 2.0% ± 0.3%, Sol: -1.4% ± 3.3% with 20° supination; for Type II, MG: -1.2% ± 0.7%, LG: -0.4% ± 0.6%, Sol: 2.4% ± 1.4% with 20° pronation and MG: 0.8% ± 0.7%, LG: 0.4% ± 0.5%, Sol: -3.2% ± 1.5% with 20° supination; and for Type III, MG: -1.7% ± 0.4%, LG: -0.4% ± 1.4%, Sol: 3.7% ± 6.0% with 20° pronation and MG: 1.3% ± 0.4%, LG: 0.4% ± 1.3%, Sol: -5.4% ± 6.2% with 20° supination. In all twist types, different degrees of stretching were applied to MG, LG, and Sol. In addition, in all twist types, MG and LG shortened and Sol stretched with a pronated calcaneus, and MG and LG stretched and Sol shortened with a supinated calcaneus (Figure 6). Type III had the greatest degree of Sol stretching with 20° pronation of the calcaneus (Type I: Sol: 1.7% ± 3.4%, Type II: Sol: 2.4% ± 1.4%, Type III: Sol: 3.7% ± 6.0%). Moreover, each tendon fiber of Sol had different degrees of stretching (Figure 7).
Figure 7 The degree of stretching applied to each of the tendon fiber bundles of the Sol of type III. Values represent means ± SD. The degree of stretching (%) = [ (the fiber length of the supination 20°÷the fiber length of the start)×100)-100]. deg (°): The angle of pronation and supination of calcaneus. Sol: The fascicles from the soleus muscle. Discussion This study revealed the degree of stretching of each of the tendon fiber bundles of MG, LG, and Sol that compose the AT by twist type when the calcaneus was pronated or supinated. To the best of our knowledge, there are no other reports that focused on the twist type in assessing the degree of stretching of each of the tendon fiber bundles when the calcaneus is pronated or supinated. The MicroScribe system used in the present study has been used in recent years as a three-dimensional measurement device in numerous studies involving different organs, including bone, skeletal muscle, and nerves [28-32]. The MicroScribe system has a 0.23-mm precision in measurements (manufacturer specification), indicating an extremely high precision. Furthermore, the present study demonstrated that the ICC(1,1) of measurements made by the MicroScribe system was 0.98, verifying high reliability and reproducibility of the system.
Copyright © 2016 The Foot and Ankle Online Journal

The Foot and Ankle Online Journal 9 (3): 5
In the present study, the degree of Sol stretching was -5.45% ± 6.2% to 3.7% ± 6.0% when the calcaneus was pronated (20°) and supinated (20°). A previous study reported that cadaveric calcaneal pronation (15°) and supination (15°) resulted in a maximum strain of -9.4% to 12.5%. This confirmed that the degrees of stretching calculated in the simulation from this study were all within the range of biological movements. When the calcaneus was pronated and supinated in the present study, different degrees of stretching were applied to MG, LG, and Sol. It has been demonstrated in studies that used diagnostic ultrasound imaging systems or MRI in human subjects [13-15] or studies that used strain-gauges in cadavers [16-18] that, with passive movements of the ankle and contraction of the triceps surae, strain is applied to a different extent at each fascia that compose the triceps surae. Moreover, gross anatomical studies revealed that the AT comprises an insertion tendon where MG, LG, and Sol muscles insert, and that the insertion sites to the calcaneal tuberosity differ between each muscle [25-27, 33]. It was therefore considered that, due to such anatomical characteristics, differences in the extent of stretching occurred at the MG, LG, and Sol that compose the AT when the calcaneus was rotated. When the calcaneus was pronated, MG and LG shortened and Sol stretched in all twist types. Furthermore, a common trend among twist types was observed where MG and LG stretched and Sol shortened with supination. Numerous studies on the twisted structure of the AT have been reported for decades [1, 22-27]. Although there are some discrepancies among the reports regarding the extent of twisting, the general consensus is that MG and LG insert to the lateral side and Sol inserts to the medial side of the calcaneal tuberosity. Types I-III used in the present study also exhibited similar structures. It was therefore considered that the Sol, which attaches to the medial side, stretched, while MG and LG shortened, when the calcaneus was pronated, and Sol shortened, while MG and LG stretched, when the calcaneus was supinated.
Furthermore, Type III (extreme) exhibited the greatest degree of Sol stretching with pronation compared to the other types, and each tendon fiber that composed the Sol also showed various degrees of stretching. In Type III, the Sol, which is located at a deep layer under the AT, inserts to the medial side of the surface of the calcaneal tuberosity, resulting in a large variation in the path of each of its tendon fibers. This may have led to the greater degree of stretching than other types, as well as differences in the degree of stretching between tendon fibers that compose the Sol. As a mechanism of AT disorder development, the non-uniform strain in the AT with calcaneal pronation has been reported as a cause [19]. Moreover, it has been reported that AT disorders typically present 2-6 cm proximal to the calcaneal tuberosity [5, 6] and occur more commonly on the medial side than the lateral side [1, 7], and that this site is where Sol is located [27]. Based on these reports, it is presumed that the primary injured tissue is Sol. The present study not only demonstrated that Type III exhibited different degrees of stretching of MG, LG, and Sol that compose the AT when the calcaneus was pronated, but also presented a greater degree of Sol stretching compared to other twist types. Furthermore, Type III had different degrees of stretching in each tendon fiber that composed the Sol. These findings indicate that there may be a greater risk of developing AT disorders in Type III twists. The present study demonstrated the degrees of stretching of each of the tendon fiber bundles (MG, LG, and Sol) that compose the AT when the calcaneus is pronated and supinated in different twist types. However, there are a few limitations to this study. The first is that the AT was separated finely for determining the twisted structure and making 3D measurements, and the binding between each of the tendon fiber bundles was not taken into account. The second limitation is that, although the degrees of stretching of each tendon fiber with calcaneus rotation were examined under the assumption that the center of the calcaneal tuberosity is its center of rotation, the moments of the actual ankle axis, specifically of the talocrural and subtalar joints, were not taken into consideration. Future directions include a mechanical analysis that accounts for the movements of the talocrural and subtalar joints.
Copyright © 2016 The Foot and Ankle Online Journal

The Foot and Ankle Online Journal 9 (3): 5
In conclusion, although AT disorders do not typically become severe, they occur frequently and are considered to be one of the disorders that are difficult to manage. Recently, several effective treatment methods were reported; however, there are currently no effective methods to prevent this disorder [1, 34, 35]. The reason for this could be that the mechanism of the disorder itself is not completely understood. We believe that the results from the present study will lead to the mechanistic elucidation of AT disorders, the development of effective preventive or treatment methods, and the functional analysis of the twisted structure. References 1. Schepsis AA, Jones H, Haas AL. Achilles tendon disorders
in athletes. Am J Sports Med 2002 MarApr;30(2):287305. 2. Lysholm J, Wiklander J. Injuries in runners. Am J Sports
Med 1987 MarApr;15(2):16871. 3. Van Ginckel A, Thijs Y, Hesar NG, Mahieu N, De Clercq
D, Roosen P et al. Intrinsic gaitrelated risk factors for Achilles tendinopathy in novice runners: a prospective study. Gait Posture 2009 Apr;29(3):38791.
4. Kujala UM, Sarna S, Kaprio J. Cumulative incidence of achilles tendon rupture and tendinopathy in male former elite athletes. Clin J Sport Med 2005 May;15(3):1335.
5. Maffulli N, Kader D. Tendinopathy of tendo achillis. J Bone Joint Surg Br 2002 Jan;84(1):18.
6. Hess GW. Achilles tendon rupture: a review of etiology, population, anatomy, risk factors, and injury prevention. Foot & ankle specialist 2010 Feb;3(1):2932.
7. Arndt A, Bruggemann GP, Koebke J, Segesser B. Asymmetrical loading of the human triceps surae: I. Mediolateral force differences in the Achilles tendon. Foot & ankle international / American Orthopaedic Foot and Ankle Society [and] Swiss Foot and Ankle Society 1999 Jul;20(7):4449.
8. Saltzman CL, Tearse DS. Achilles tendon injuries. J Am Acad Orthop Surg 1998 SepOct;6(5):31625.
9. Carr AJ, Norris SH. The blood supply of the calcaneal tendon. J Bone Joint Surg Br 1989 Jan;71(1):1001.
10. Clain MR, Baxter DE. Achilles tendinitis. Foot & ankle 1992 Oct;13(8):4827.
11. Magnusson SP, Kjaer M. Regionspecific differences in Achilles tendon crosssectional area in runners and nonrunners. European journal of applied physiology 2003 Nov;90(56):54953.
12. Kongsgaard M, Aagaard P, Kjaer M, Magnusson SP. Structural Achilles tendon properties in athletes subjected to different exercise modes and in Achilles tendon rupture patients. Journal of applied physiology (Bethesda, Md : 1985)2005 Nov;99(5):196571.
13. BojsenMoller J, Hansen P, Aagaard P, Svantesson U, Kjaer M, Magnusson SP. Differential displacement of the human soleus and medial gastrocnemius aponeuroses during isometric plantar flexor contractions in vivo. Journal of applied physiology (Bethesda, Md : 1985)2004 Nov;97(5):190814.
14. Finni T, Hodgson JA, Lai AM, Edgerton VR, Sinha S. Nonuniform strain of human soleus aponeurosistendon complex during submaximal voluntary contractions in vivo. Journal of applied physiology (Bethesda, Md : 1985)2003 Aug;95(2):82937.
15. Kinugasa R, Shin D, Yamauchi J, Mishra C, Hodgson JA, Edgerton VR et al. Phasecontrast MRI reveals mechanical behavior of superficial and deep aponeuroses in human medial gastrocnemius during isometric contraction. Journal of applied physiology (Bethesda, Md : 1985)2008 Oct;105(4):131220.
16. Defrate LE, van der Ven A, Boyer PJ, Gill TJ, Li G. The measurement of the variation in the surface strains of Achilles tendon grafts using imaging techniques. J Biomech 2006;39(3):399405.
17. Lyman J, Weinhold PS, Almekinders LC. Strain behavior of the distal achilles tendon: implications for insertional achilles tendinopathy. Am J Sports Med 2004 Mar;32(2):45761.
18. Wren TA, Lindsey DP, Beaupre GS, Carter DR. Effects of creep and cyclic loading on the mechanical properties and failure of human Achilles tendons. Annals of biomedical engineering 2003 Jun;31(6):7107.
19. Lersch C, Grotsch A, Segesser B, Koebke J, Bruggemann GP, Potthast W. Influence of calcaneus angle and muscle forces on strain distribution in the human Achilles tendon. Clinical biomechanics (Bristol, Avon)2012 Nov;27(9):95561.
20. Donoghue OA, Harrison AJ, Coffey N, Hayes K. Functional data analysis of running kinematics in chronic Achilles tendon injury. Med Sci Sports Exerc 2008 Jul;40(7):132335.
21. Clement DB, Taunton JE, Smart GW. Achilles tendinitis and peritendinitis: etiology and treatment. Am J Sports Med 1984 MayJun;12(3):17984.
22. Cummins EJ, Anson BJ, et al. The structure of the calcaneal tendon (of Achilles) in relation to orthopedic surgery, with additional observations on the plantaris muscle. Surgery, gynecology & obstetrics 1946 Jul;83:10716.
23. van Gils CC, Steed RH, Page JC. Torsion of the human Achilles tendon. J Foot Ankle Surg 1996 JanFeb;35(1):418.
24. Robert S. Management of partial tears of the gastrosoleus complex. Clin Sports Med 2008 Jan;27(1):21929, x.
25. Szaro P, Witkowski G, Smigielski R, Krajewski P, Ciszek B. Fascicles of the adult human Achilles tendon an anatomical study. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft 2009 Dec;191(6):58693.
26. Edama M, Onishi H, Kumaki K, Kageyama I, Watanabe H, Nashimoto S. Effective and selective stretching of the medial head of the gastrocnemius. Scand J Med Sci Sports 2014 Mar 20.
Copyright © 2016 The Foot and Ankle Online Journal

The Foot and Ankle Online Journal 9 (3): 5
27. Edama M, Kubo M, Onishi H, Takabayashi T, Inai T,
Yokoyama E et al. The twisted structure of the human Achilles tendon. Scand J Med Sci Sports 2014 Dec 30.
28. Agur AM, NgThowHing V, Ball KA, Fiume E, McKee NH. Documentation and threedimensional modelling of human soleus muscle architecture. Clin Anat 2003 Jul;16(4):28593.
29. Davies JC, Fattah A, Ravichandiran M, Agur AM. Clinically relevant landmarks of the frontotemporal branch of the facial nerve: a threedimensional study. Clin Anat 2012 Oct;25(7):85865.
30. Fattah AY, Ravichandiran K, Zuker RM, Agur AM. A threedimensional study of the musculotendinous and neurovascular architecture of the gracilis muscle: application to functional muscle transfer. Journal of plastic, reconstructive & aesthetic surgery : JPRAS 2013 Sep;66(9):12307.
31. Mullen M, Pillai A, Fogg QA, Kumar CS. The anterior approach for the fixation of displaced talar neck fracturesa cadaveric study. Foot (Edinburgh, Scotland)2013 JunSep;23(23):703.
32. Warden JM, Roberts SL, Chang Y, Baker R, Boulias C, Ismail F et al. Neuromuscular partitioning of subscapularis based on intramuscular nerve distribution patterns: implications for botulinum toxin injections. Archives of physical medicine and rehabilitation 2014 Jul;95(7):140815.
33. Ballal MS, Walker CR, Molloy AP. The anatomical footprint of the Achilles tendon: a cadaveric study. The bone & joint journal 2014 Oct;96b(10):13448.
34. Paavola M, Kannus P, Jarvinen TA, Khan K, Jozsa L, Jarvinen M. Achilles tendinopathy. J Bone Joint Surg Am2002 Nov;84a(11):206276.
35. Carcia CR, Martin RL, Houck J, Wukich DK. Achilles pain, stiffness, and muscle power deficits: achilles tendinitis. J Orthop Sports Phys Ther 2010 Sep;40(9):A126.
Copyright © 2016 The Foot and Ankle Online Journal