Embed Size (px)
Citation preview
The Five-Factor Model of Personality Disorderand DSM-5
Timothy J. TrullUniversity of Missouri
ABSTRACT The Five-Factor Model of personality disorders(FFMPD; Widiger & Mullins-Sweatt, 2009) developed from the recogni-tion that the popular Five-Factor Model (FFM) of personality could beused to describe and understand the official personality disorder (PD)constructs from the American Psychiatric Association’s (APA) diagnosticmanuals (e.g., DSM-IV-TR, APA, 2000). This article provides an over-view of the FFM, highlighting its validity and utility in characterizing PDsas well as its ability to provide a comprehensive account of personalitypathology in general. In 2013, DSM-5 is scheduled to appear, and the“hybrid” PD proposal will emphasize a 25–personality trait model. Ipresent the current version of this new model, compare it to the FFMPD,and discuss issues related to the implementation of the FFMPD.
This article presents an overview of the Five-Factor Model ofpersonality disorders (FFMPD; Widiger & Mullins-Sweatt, 2009),including its historical development, empirical support, and previoususe in evaluating the DSM-IV-TR personality disorders (AmericanPsychiatric Association [APA], 2000). Next, the proposed “hybridmodel” of personality disorders (PDs) that is being considered forDSM-5 is discussed, focusing primarily on its 25-trait model of per-sonality, as well as its relationship to the FFMPD. I close with issuesrelated to the implementation of the FFMPD.
THE FIVE-FACTOR MODEL OF PERSONALITY
Although a number of personality trait models have been discussedin the context of the DSM personality disorders, the Five-Factor
Correspondence concerning this article should be addressed to Timothy J. Trull,210 McAlester Hall, Department of Psychological Sciences, University of Missouri,Columbia, MO 65211. Email: [email protected].
Journal of Personality 80:6, December 2012© 2012 The AuthorJournal of Personality © 2012, Wiley Periodicals, Inc.DOI: 10.1111/j.1467-6494.2012.00771.x

Model of personality has received both the most research attentionand empirical support in this context (e.g., Allik, 2005; Clark, 2007;Clark & Livesley, 2002; Costa & Widiger, 2002; O’Connor & Dyce,1998; Samuel & Widiger, 2008; Saulsman & Page, 2004; Trull &Durrett, 2005; Widiger & Mullins-Sweatt, 2009; Widiger & Simon-sen, 2005; Widiger & Trull, 2007). As stated by Clark (2007), “Thefive-factor model of personality is widely accepted as representingthe higher-order structure of both normal and abnormal personalitytraits” (p. 246).
Indeed, the Five-Factor Model (FFM) of personality is a popularway to conceptualize major personality traits. It has a long historyand rich tradition, and was derived through factor-analytic studies ofpersonality trait terms from the English language (see Goldberg,1993; John & Srivastava, 1999). As Widiger and Mullins-Sweatt(2009) noted:
Language can be understood as a sedimentary deposit of theobservations of persons over the thousands of years of the lan-guage’s development and transformation. The most importantdomains of personality functioning are those with the greatestnumber of trait terms to describe and differentiate the variousmanifestations and nuances of a respective domain, and the struc-ture of personality is suggested by the empirical relationshipsamong these trait terms. (p. 199)
Thus, the FFM is often termed lexical, in that it reflects the structureof personality descriptions that occur most frequently in the Englishlanguage. It also appears to be fairly universal in that this five-factorstructure in trait terms has been replicated in a variety of otherlanguages, including German, Dutch, Czech, Polish, Russian,Italian, Spanish, Hebrew, Hungarian, Turkish, Korean, and Filipino(Allik, 2005; Ashton & Lee, 2001).
The five major domains of this model are typically referred to asNeuroticism versus emotional stability, Extraversion versus intro-version, Openness versus closedness to experience, Agreeablenessversus antagonism, and Conscientiousness versus negligence. TheFFM was originally developed using nonclinical samples, and thegoal was to provide a comprehensive account of major personalitytraits and dimensions. However, several came to realize that theFFM might also be applied to issues relating to various forms of
Trull1698
psychopathology. Personality traits are indeed dimensional, and per-sonality disorders by definition involve maladaptive or extreme per-sonality traits. Further, the hierarchical structure of FFM traits (i.e.,higher order domains and lower order facets) has been replicatedacross populations (i.e., nonclinical and clinical) and cultures, andevidence suggests a heritable and biological basis for both higherorder and lower order FFM traits (Trull & Durrett, 2005).
Over the last two decades, many studies have assessed therelations between FFM constructs and personality disorders (seeWidiger & Costa, 2002; Samuel & Widiger, 2008, for reviews). Thesestudies have sampled clinical subjects, community residents, andcollege students. For example, perhaps the first study examining therelationship between the FFM and PDs in a clinical sample wasconducted by Trull (1992). Importantly, this study demonstratedstrong relationships between the FFM and personality disorder fea-tures in a clinical sample of psychiatric outpatients. FFM scoresaccounted for significant amounts of variance in individual person-ality disorders in almost every case, and many of the patterns ofFFM relations for individual personality disorders were replicatedacross three different personality disorder measures (i.e., a semistruc-tured interview and two self-report inventories). Many studies usingboth clinical and nonclinical samples have followed; studies haveconsistently demonstrated significant relations between the traitsincluded in the FFM and the DSM PD constructs (Samuel &Widiger, 2008; Saulsman & Page, 2004; Trull & Durrett, 2005;Widiger & Costa, 2002).
However, simply demonstrating that, overall, these traits arerelated to PDs is not particularly surprising. After all, by definitionPDs comprise extreme, maladaptive versions of personality traits(APA, 2000). Instead, what is of interest is the extent to whichPD–personality trait relations may help distinguish among the offi-cial PD diagnoses. Therefore, based on an understanding of theFFM as well as of personality disorders, Widiger and colleagues(Lynam & Widiger, 2001; Widiger et al.,1994; Widiger, Trull, et al.,2002) offered a set of predicted correlates between the five majordimensions of the FFM, as well as the facets composing each dimen-sion, and the DSM-IV personality disorders. Subsequent studieshave found general support for the relevance of the FFM to the fullrange of personality disorders. For example, O’Connor and Dyce(1998) used a confirmatory factor-analytic strategy to evaluate the
Five-Factor Model of Personality Disorder and DSM-5 1699

“fit” of the FFM across 12 data sets of personality disorder symp-toms. The authors used the proposals of Widiger et al. (1994) topredict the covariance structure, and results supported the FFM as away of conceptualizing personality disorder pathology. More recentstudies have examined FFM and personality disorder relations at thefacet level. The main reason for this more detailed focus is that betterdifferentiation among the personality disorders is possible at the levelof first-order versus higher order traits (Samuel & Widiger, 2008).Most of the personality disorders are associated with elevations onNeuroticism, introversion, antagonism, and negligence (Saulsman &Page, 2004; Samuel & Widiger, 2008). However, it appears that thepersonality disorders can be distinguished by the patterns of relationsat the first-order, facet trait level (O’Connor & Dyce, 1998; Samuel &Widiger, 2008; Trull, Widiger, & Burr, 2001).
Although these studies have primarily conceptualized personal-ity pathology and disorder from the perspective of the existingdiagnostic manual, the findings do help explain some of the comor-bidity patterns typically reported among the PDs (e.g., see Lynam& Widiger, 2001). As mentioned, Samuel and Widiger (2008)recently presented findings from a meta-analysis of studies thatexamined the relations between both the five domains and the 30facets of personality traits included in the FFM and the DSM-IVPDs. Their results for the relationships between domain scores ofthe FFM and individual PDs are consistent with the finding thatmost PDs appear to be related to each other and comorbidity ismore the rule than the exception: The majority of PDs are charac-terized by significant positive relations with Neuroticism, signifi-cant negative relations with Extraversion, significant negativerelations with Agreeableness, and significant negative relations withConscientiousness. Second, the facet-level relations provide someunderstanding of comorbidity patterns between certain pairs ofPDs (Lynam & Widiger, 2001). For example, the relatively parallelpattern of FFM facet associations with paranoid, schizoid, andschizotypal PD suggests that these diagnostic constructs mightco-occur with each other (consistent with the finding that thesewithin–cluster A correlations are significant). Finally, Samuel andWidiger’s (2008) FFM facet results also are consistent with thefinding that both antisocial and obsessive-compulsive PD, respec-tively, are consistently less highly associated with other PDs; anexamination of their respective FFM facet profiles indicates that
Trull1700

they show less personality trait overlap with the other PDs. In thecase of antisocial PD, it is characterized primarily by low levels ofAgreeableness facets (i.e., low levels of trust, straightforwardness,altruism, and compliance) and low levels of Conscientiousnessfacets (i.e., low levels of competence, dutifulness, self-discipline,and deliberation). Although borderline PD also shows a similarpattern of associations with these facets, in addition (unlike anti-social PD), borderline PD is significantly positively related to allNeuroticism facets (i.e., anxiousness, angry hostility, depressive-ness, self-consciousness, impulsiveness, and vulnerability). Thisexplains why antisocial PD is often most highly associated withborderline PD. Obsessive-compulsive PD is another case in point.This PD’s FFM facet profile is unique in that there are some smallpositive associations with Neuroticism facets (but not Extraversion,Openness, or Agreeableness facets) but stronger positive associa-tions with Conscientiousness facets (i.e., high levels of competence,order, dutifulness, achievement striving, self-discipline, and delib-eration). Obsessive-compulsive PD is the only PD to show positiverelations with these Conscientiousness facets.
DSM-IV-TR AND PERSONALITY TRAITS
As has been documented for some time now, the categorical model ofpersonality disorders, as exemplified in the DSM-IV-TR and itsimmediate predecessors, is fraught with problems. These includeexcessive heterogeneity within diagnoses, excessive diagnosticcomorbidity, inadequate coverage, arbitrary boundaries with normalpsychological functioning, and an inadequate scientific foundation(Clark, 2007; Livesley, 2001; Trull & Durrett, 2005; Widiger & Trull,2007). Although the DSM-IV-TR embraces the categorical approachto personality pathology diagnosis, it does at least mention the pos-sibility of an alternative dimensional approach: “An alternative tothe categorical approach is the dimensional perspective that Person-ality Disorders represent maladaptive variants of personality traitsthat merge imperceptibly into normality and into one another”(APA, 2000, p. 689). In addition, DSM-IV-TR acknowledges therelevancy of major personality trait models (e.g., the FFM) to thePDs.
Five-Factor Model of Personality Disorder and DSM-5 1701
But how are personality traits and the DSM-IV-TR personalitydisorders connected? DSM-IV-TR states:
Personality traits are enduring patterns of perceiving, relating to,and thinking about the environment and oneself that are exhibitedin a wide range of social and personal contexts. Only when per-sonality traits are inflexible and maladaptive and cause significantfunctional impairment or subjective distress do they constitutePersonality Disorders. (APA, 2000, p. 686)
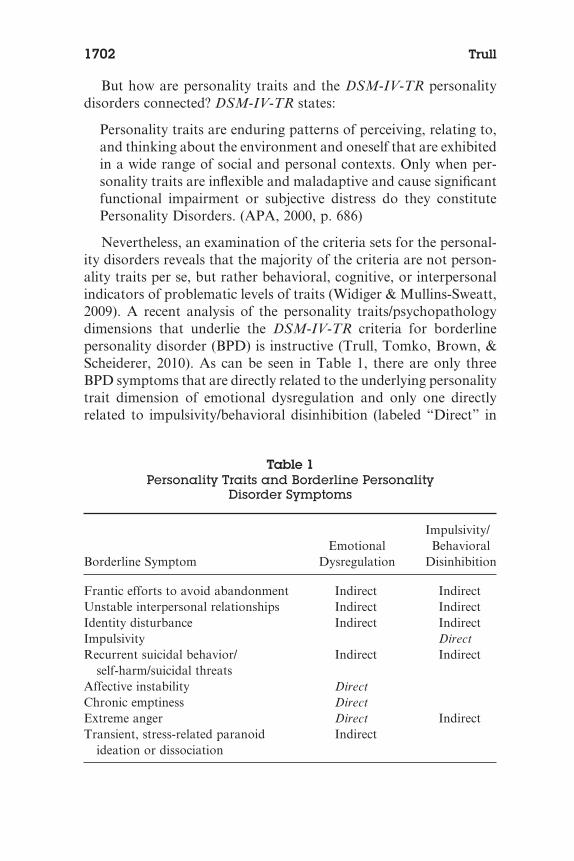
Nevertheless, an examination of the criteria sets for the personal-ity disorders reveals that the majority of the criteria are not person-ality traits per se, but rather behavioral, cognitive, or interpersonalindicators of problematic levels of traits (Widiger & Mullins-Sweatt,2009). A recent analysis of the personality traits/psychopathologydimensions that underlie the DSM-IV-TR criteria for borderlinepersonality disorder (BPD) is instructive (Trull, Tomko, Brown, &Scheiderer, 2010). As can be seen in Table 1, there are only threeBPD symptoms that are directly related to the underlying personalitytrait dimension of emotional dysregulation and only one directlyrelated to impulsivity/behavioral disinhibition (labeled “Direct” in
Table 1Personality Traits and Borderline Personality
Disorder Symptoms
Borderline SymptomEmotional
Dysregulation
Impulsivity/Behavioral
Disinhibition
Frantic efforts to avoid abandonment Indirect IndirectUnstable interpersonal relationships Indirect IndirectIdentity disturbance Indirect IndirectImpulsivity DirectRecurrent suicidal behavior/
self-harm/suicidal threatsIndirect Indirect
Affective instability DirectChronic emptiness DirectExtreme anger Direct IndirectTransient, stress-related paranoid
ideation or dissociationIndirect
Trull1702
Table 1). The other criteria for BPD may be seen as either indirectindicators of these personality traits or combinations of traits.Although some might disagree with specific entries in Table 1, themajor point should not be lost. With the exception of affective insta-bility, chronic emptiness, excessive anger, and impulsivity, thesecriteria seem better conceptualized as possible indicators of traits(which may be inferred but are not identified by name). The criteriasets for other personality disorders are similar in their mix of traitsand of indicators of unnamed traits. Therefore, the DSM-IV-TR PDcriteria are really a mixture of personality traits per se and indicatorsof these traits, the latter of which differ in the degree of inferencerequired for assessment as well as for making the connection to theunderlying personality trait.
FIVE-FACTOR MODEL OF PERSONALITY DISORDER
To this point, I have evaluated the FFM in reference to its ability tocharacterize and account for the DSM-IV-TR PDs. It is clear thatPDs can be understood as maladaptive variants of the FFM (Clark,2007; Livesley, 2001; Samuel & Widiger, 2008; Saulsman & Page,2004), and the predominant models of normal and abnormal person-ality functioning converge onto at least four of the five broaddomains of the FFM (Bouchard & Loehlin, 2001; Clark, 2007; John& Srivastava, 1999; Livesley, 2003; Markon, Krueger, & Watson,2005; Trull & Durrett, 2005; Watson, Clark, & Harkness, 1994;Widiger & Simonsen, 2005).
Findings such as these have encouraged investigators to go evenone step further. Clearly, the DSM-IV-TR does not present a com-prehensive catalog of all personality pathology, nor is it an efficientclassification system (given rampant comorbidity among the PDs,heterogeneity within diagnosis, and the high prevalence of the PDnot otherwise specified diagnosis; Trull & Durrett, 2005). It makesmuch more sense to characterize and define personality pathologyand disorder through the lens of a widely accepted, comprehensive,and empirically validated model of personality as opposed to thecurrent PD diagnostic system embodied in the official diagnosticmanual. Such an approach is likely to improve the weak constructvalidity of the DSM-IV diagnostic categories (Mullins-Sweatt &Widiger, 2006).
Five-Factor Model of Personality Disorder and DSM-5 1703
The Four Steps
So how can the FFM characterize personality pathology and diag-nose PD? Widiger, Costa, and McCrae (2002) proposed a four-stepprocedure for an FFM diagnosis of personality disorder. Briefly, thefirst step is to obtain a personality trait description of an individual interms of the five domains and 30 facets of the FFM. This descriptionwill provide a comprehensive description of the person’s adaptive aswell as maladaptive personality traits. There are a number of psy-chological measures that can be used for this FFM description (DeRaad & Perugini, 2002), including, for example, the questionnaire-based Revised NEO Personality Inventory (NEO PI-R; Costa &McCrae, 1992) and the Structured Interview for the Five FactorModel (SIFFM; Trull & Widiger, 1997), a semistructured interviewfor the assessment of the FFM. Other FFM self-report inventoriesand brief clinician rating scales can also be used (De Raad &Perugini, 2002; Mullins-Sweatt, Jamerson, Samuel, Olson, &Widiger, 2006). For example, Few et al. (2010) demonstrated the useof a brief rating form for FFM facets to evaluate patients.
The second step involves an assessment of any social and occupa-tional impairments and distress associated with extreme scores on theFFM personality traits. For example, Widiger, Costa, et al. (2002)and McCrae, Löckenhoff, and Costa (2005) identified problems likelyto be found in people scoring high or low on each of the FFM domainsand facets. In the case of the SIFFM interviews, there are questionsincluded that assess these maladaptive variants of each of the 30 traitfacets of the FFM. Further, both the SIFFM and the Five FactorModel Score Sheet (FFMSS; Mullins-Sweatt et al., 2006) includeseparate, independent assessments of many of the problems identifiedby Widiger et al. (2002) and McCrae et al. (2005).
The third step is to determine whether the dysfunction and distressreach a clinically significant level of impairment that would warranta diagnosis of personality disorder. There are several possibilities forthis assessment. For example, one could use the Global Assessmentof Functioning (GAF) scale currently used for Axis V of the DSM-IV-TR (APA, 2000). Other possibilities, measures that purport tomeasure personality-related impairment and dysfunction specifi-cally, include the General Assessment of Personality Dysfunction(GAPD; Livesley, 2010) and the Severity Indices of PersonalityProblems (SIPP-118; Verheul et al., 2008).
Trull1704
The fourth step is necessary only if one desires a single quantita-tive index of the match between an individual’s FFM personalityprofile and prototypic profiles of diagnostic constructs (e.g., Miller,2012; Miller & Lynam, 2003; Trull, Widiger, Lynam, & Costa,2003). Although this can be used to assess a match between anindividual’s FFM profile and a FFM characterization of the DSM-IV-TR PD constructs, it is also possible for clinicians and research-ers to develop FFM profiles for personality disorder constructs notincluded within DSM-IV (e.g., successful psychopath). However,prototypal matching with the DSM PDs is not generally recom-mended, as the purpose of the FFM diagnosis would not simplybe to provide a roundabout method of returning to the DSMdiagnostic categories (Clark, 2007).
DIAGNOSING PDS IN DSM-5: COMPARISONS WITHTHE FFMPD
Before comparing the DSM-5 revisions for PD with the FFMPD, itis useful to briefly outline this new proposal for PD diagnosis. Thenew version of the DSM (DSM-5) proposes that a diagnosis of PDinvolves a series of determinations concerning overall personalitydysfunction as well as specific personality trait elevations(www.dsm5.org). It is important to note that the original DSM-5 PDproposal (published on the Web site in February 2010) was revised toaddress concerns and clarify confusion (Skodol et al., 2011). Mostimportantly, it is now clearer how to arrive at a diagnosis of PD, andthe prototype matching approach for PD types has been dropped.
According to the latest version of the proposal (updated June 21,2011, on the DSM-5 Web site: http://www.dsm5.org/proposedrevision/Pages/PersonalityDisorders.aspx), the diagnostician is askedto first determine whether impairment in personality functioning ispresent and, if so, to what degree. The clinician is asked to rate apatient’s level of personality functioning; specifically, ratings aremade as to the level of self and interpersonal functioning for eachindividual (see also Livesley, 2001, 2003). Self functioning is defined intwo areas (identity and self-direction), as is interpersonal functioning(empathy and intimacy). A 5-point scale is used to rate overall level ofpersonality functioning for this purpose (0 = no impairment; 1 = mildimpairment; 2 = moderate impairment; 3 = serious impairment; and4 = extreme impairment). Descriptions of each quantitative rating are
Five-Factor Model of Personality Disorder and DSM-5 1705

provided, and the diagnostician is reminded that the ratings mustreflect functioning that is of multiple years in duration, not due solelyto another mental disorder/physical condition/effect of a substance,and not a norm within a person’s cultural background.
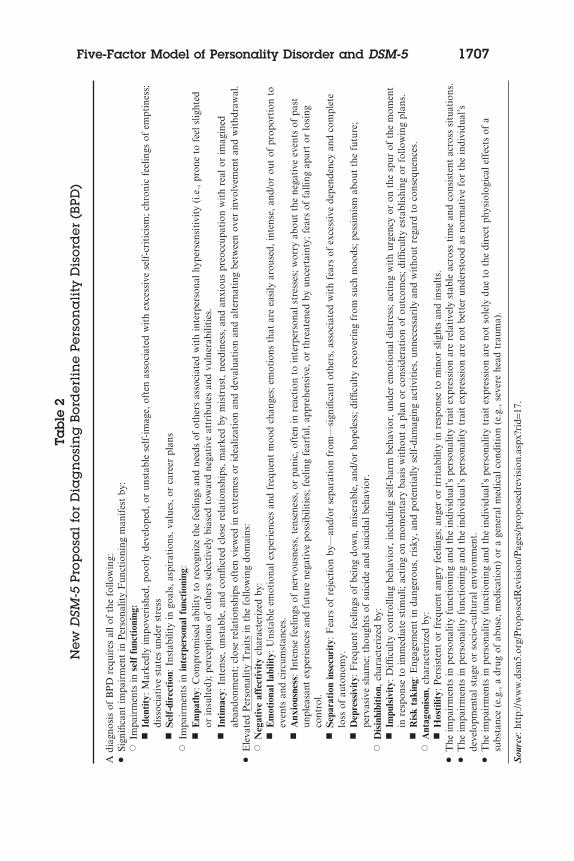
Next, if significant personality dysfunction is present, the clinicianconsiders whether one (or more?) of the six proposed personalitydisorder types are present: borderline, obsessive-compulsive,avoidant, schizotypal, antisocial, or narcissistic. For each of theseproposed PD types, a listing of characteristic trait elevations is pro-vided. Table 2 presents the current DSM-5 proposal for borderlinepersonality disorder, and one can see that for this PD type theclinician is asked to consider whether there are elevations on seventraits tapping negative affectivity (emotional lability, anxiousness,separation insecurity, and depressivity), disinhibition (impulsivity,risk taking), and antagonism (hostility). For obsessive-compulsive,the clinician considers two primary traits, for avoidant four primarytraits, for schizotypal six primary traits, for antisocial seven primarytraits, and for narcissistic two primary traits.
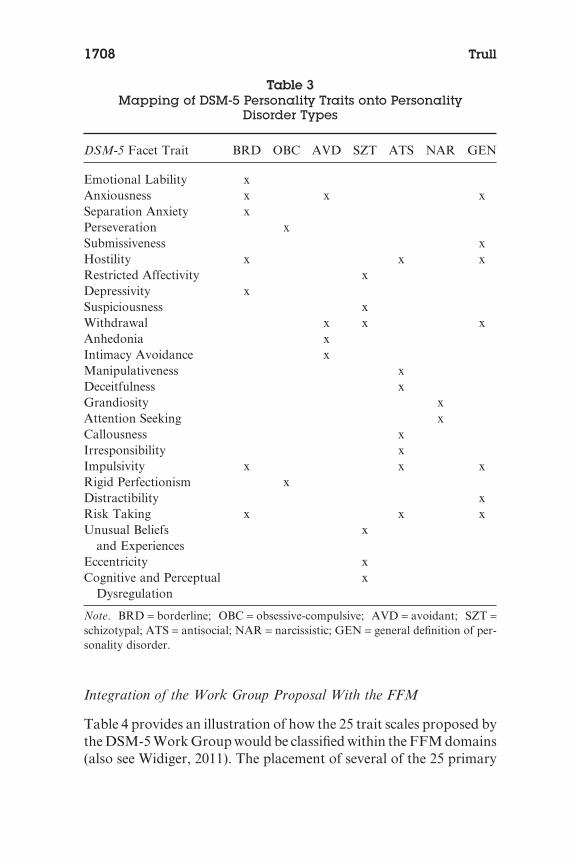
If a specific PD type is not indicated but personality dysfunctionis present, then the clinician may designate a diagnosis of personalitydisorder trait specified (PDTS), which replaces the DSM-IV-TR des-ignation of personality disorder not otherwise specified (PDNOS).Table 3 indicates how each of the 25 proposed DSM-5 PD primarytraits is mapped onto the PD types (as well as the “General definitionof personality disorder”), according to the latest proposal.
Of most relevance to the present article are the 25 traits, as well asthe higher-order trait domains, included in the DSM-5 PD proposal.The current proposal lists 25 maladaptive personality traits, orga-nized within five broad domains, which can be rated for each indi-vidual. The 25 facet traits are organized into five higher order traitdomains: Negative Affectivity (emotional lability, anxiousness,separation anxiety, perseveration, submissiveness, hostility, restrictedaffectivity [lack of], depressivity, and suspiciousness); Detachment(restricted affectivity, depressivity, suspiciousness, withdrawal, anhe-donia, and intimacy avoidance); Antagonism (hostility, manipulative-ness, deceitfulness, grandiosity, attention seeking, and callousness);Disinhibition (irresponsibility, impulsivity, rigid perfectionism[lack of], distractibility, and risk taking); and Psychoticism (unusualbeliefs and experiences, eccentricity, and cognitive and perceptualdysregulation).
Trull1706
Tab
le2
New
DSM
-5Pr
opos
al
for
Dia
gn
osin
gB
ord
erli
ne
Pers
ona
lity
Dis
ord
er(B
PD)
Adi
agno
sis
ofB
PD
requ
ires
allo
fth
efo
llow
ing:
•Si
gnifi
cant
impa
irm
ent
inP
erso
nalit
yF
unct
ioni
ngm
anif
est
by:
�Im
pair
men
tsin
self
func
tion
ing:
�Id
enti
ty:M
arke
dly
impo
veri
shed
,poo
rly
deve
lope
d,or
unst
able
self
-im
age,
ofte
nas
soci
ated
wit
hex
cess
ive
self
-cri
tici
sm;c
hron
icfe
elin
gsof
empt
ines
s;di
ssoc
iati
vest
ates
unde
rst
ress
�S
elf-
dire
ctio
n:In
stab
ility
ingo
als,
aspi
rati
ons,
valu
es,o
rca
reer
plan
s�
Impa
irm
ents
inin
terp
erso
nalf
unct
ioni
ng:
�E
mpa
thy:
Com
prom
ised
abili
tyto
reco
gniz
eth
efe
elin
gsan
dne
eds
ofot
hers
asso
ciat
edw
ith
inte
rper
sona
lhyp
erse
nsit
ivit
y(i
.e.,
pron
eto
feel
slig
hted
orin
sult
ed);
perc
epti
ons
ofot
hers
sele
ctiv
ely
bias
edto
war
dne
gati
veat
trib
utes
and
vuln
erab
iliti
es.
�In
tim
acy:
Inte
nse,
unst
able
,and
confl
icte
dcl
ose
rela
tion
ship
s,m
arke
dby
mis
trus
t,ne
edin
ess,
and
anxi
ous
preo
ccup
atio
nw
ith
real
orim
agin
edab
ando
nmen
t;cl
ose
rela
tion
ship
sof
ten
view
edin
extr
emes
orid
ealiz
atio
nan
dde
valu
atio
nan
dal
tern
atin
gbe
twee
nov
erin
volv
emen
tan
dw
ithd
raw
al.
•E
leva
ted
Per
sona
lity
Tra
its
inth
efo
llow
ing
dom
ains
:�
Neg
ativ
eaf
fect
ivit
ych
arac
teri
zed
by:
�E
mot
iona
llab
ility
:Uns
tabl
eem
otio
nale
xper
ienc
esan
dfr
eque
ntm
ood
chan
ges;
emot
ions
that
are
easi
lyar
ouse
d,in
tens
e,an
d/or
out
ofpr
opor
tion
toev
ents
and
circ
umst
ance
s.�
Anx
ious
ness
:Int
ense
feel
ings
ofne
rvou
snes
s,te
nsen
ess,
orpa
nic,
ofte
nin
reac
tion
toin
terp
erso
nals
tres
ses;
wor
ryab
out
the
nega
tive
even
tsof
past
unpl
easa
ntex
peri
ence
san
dfu
ture
nega
tive
poss
ibili
ties
;fee
ling
fear
ful,
appr
ehen
sive
,or
thre
aten
edby
unce
rtai
nty;
fear
sof
falli
ngap
art
orlo
sing
cont
rol.
�S
epar
atio
nin
secu
rity
:Fea
rsof
reje
ctio
nby
—an
d/or
sepa
rati
onfr
om—
sign
ifica
ntot
hers
,ass
ocia
ted
wit
hfe
ars
ofex
cess
ive
depe
nden
cyan
dco
mpl
ete
loss
ofau
tono
my.
�D
epre
ssiv
ity:
Fre
quen
tfe
elin
gsof
bein
gdo
wn,
mis
erab
le,a
nd/o
rho
pele
ss;d
iffic
ulty
reco
veri
ngfr
omsu
chm
oods
;pes
sim
ism
abou
tth
efu
ture
;pe
rvas
ive
sham
e;th
ough
tsof
suic
ide
and
suic
idal
beha
vior
.�
Dis
inhi
biti
on,c
hara
cter
ized
by:
�Im
puls
ivit
y:D
iffic
ulty
cont
rolli
ngbe
havi
or,i
nclu
ding
self
-har
mbe
havi
or,u
nder
emot
iona
ldis
tres
s;ac
ting
wit
hur
genc
yor
onth
esp
urof
the
mom
ent
inre
spon
seto
imm
edia
test
imul
i;ac
ting
onm
omen
tary
basi
sw
itho
uta
plan
orco
nsid
erat
ion
ofou
tcom
es;d
iffic
ulty
esta
blis
hing
orfo
llow
ing
plan
s.�
Ris
kta
king
:Eng
agem
ent
inda
nger
ous,
risk
y,an
dpo
tent
ially
self
-dam
agin
gac
tivi
ties
,unn
eces
sari
lyan
dw
itho
utre
gard
toco
nseq
uenc
es.
�A
ntag
onis
m,c
hara
cter
ized
by:
�H
osti
lity:
Per
sist
ent
orfr
eque
ntan
gry
feel
ings
;ang
eror
irri
tabi
lity
inre
spon
seto
min
orsl
ight
san
din
sult
s.
•T
heim
pair
men
tsin
pers
onal
ity
func
tion
ing
and
the
indi
vidu
al’s
pers
onal
ity
trai
tex
pres
sion
are
rela
tive
lyst
able
acro
ssti
me
and
cons
iste
ntac
ross
situ
atio
ns.
•T
heim
pair
men
tsin
pers
onal
ity
func
tion
ing
and
the
indi
vidu
al’s
pers
onal
ity
trai
tex
pres
sion
are
not
bett
erun
ders
tood
asno
rmat
ive
for
the
indi
vidu
al’s
deve
lopm
enta
lsta
geor
soci
o-cu
ltur
alen
viro
nmen
t.
•T
heim
pair
men
tsin
pers
onal
ity
func
tion
ing
and
the
indi
vidu
al’s
pers
onal
ity
trai
tex
pres
sion
are
not
sole
lydu
eto
the
dire
ctph
ysio
logi
cale
ffec
tsof
asu
bsta
nce
(e.g
.,a
drug
ofab
use,
med
icat
ion)
ora
gene
ralm
edic
alco
ndit
ion
(e.g
.,se
vere
head
trau
ma)
.
Sou
rce:
http
://w
ww
.dsm
5.or
g/P
ropo
sedR
evis
ion/
Pag
es/p
ropo
sedr
evis
ion.
aspx
?rid
=17.
Five-Factor Model of Personality Disorder and DSM-5 1707
Integration of the Work Group Proposal With the FFM
Table 4 provides an illustration of how the 25 trait scales proposed bythe DSM-5 Work Group would be classified within the FFM domains(also see Widiger, 2011). The placement of several of the 25 primary
Table 3Mapping of DSM-5 Personality Traits onto Personality
Disorder Types
DSM-5 Facet Trait BRD OBC AVD SZT ATS NAR GEN
Emotional Lability xAnxiousness x x xSeparation Anxiety xPerseveration xSubmissiveness xHostility x x xRestricted Affectivity xDepressivity xSuspiciousness xWithdrawal x x xAnhedonia xIntimacy Avoidance xManipulativeness xDeceitfulness xGrandiosity xAttention Seeking xCallousness xIrresponsibility xImpulsivity x x xRigid Perfectionism xDistractibility xRisk Taking x x xUnusual Beliefs
and Experiencesx
Eccentricity xCognitive and Perceptual
Dysregulationx
Note. BRD = borderline; OBC = obsessive-compulsive; AVD = avoidant; SZT =schizotypal; ATS = antisocial; NAR = narcissistic; GEN = general definition of per-sonality disorder.
Trull1708
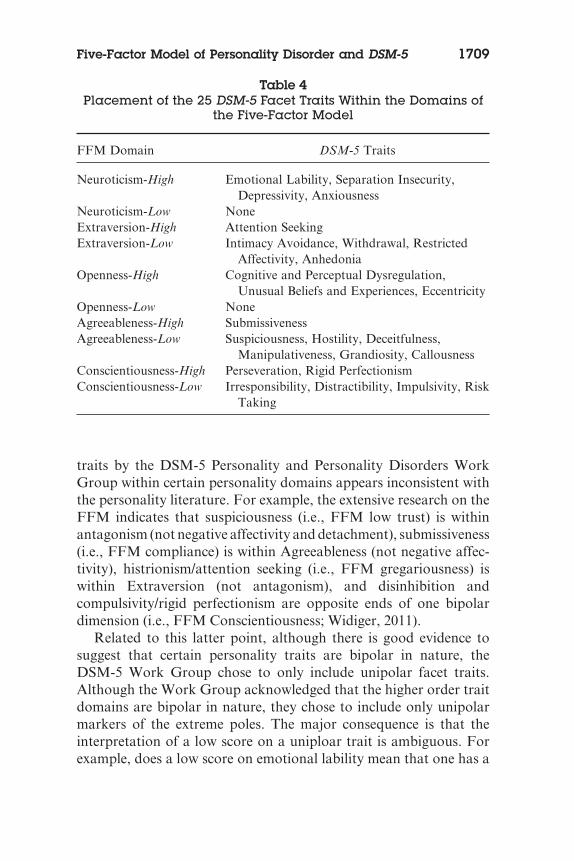
traits by the DSM-5 Personality and Personality Disorders WorkGroup within certain personality domains appears inconsistent withthe personality literature. For example, the extensive research on theFFM indicates that suspiciousness (i.e., FFM low trust) is withinantagonism (not negative affectivity and detachment), submissiveness(i.e., FFM compliance) is within Agreeableness (not negative affec-tivity), histrionism/attention seeking (i.e., FFM gregariousness) iswithin Extraversion (not antagonism), and disinhibition andcompulsivity/rigid perfectionism are opposite ends of one bipolardimension (i.e., FFM Conscientiousness; Widiger, 2011).
Related to this latter point, although there is good evidence tosuggest that certain personality traits are bipolar in nature, theDSM-5 Work Group chose to only include unipolar facet traits.Although the Work Group acknowledged that the higher order traitdomains are bipolar in nature, they chose to include only unipolarmarkers of the extreme poles. The major consequence is that theinterpretation of a low score on a uniploar trait is ambiguous. Forexample, does a low score on emotional lability mean that one has a
Table 4Placement of the 25 DSM-5 Facet Traits Within the Domains of
the Five-Factor Model
FFM Domain DSM-5 Traits
Neuroticism-High Emotional Lability, Separation Insecurity,Depressivity, Anxiousness
Neuroticism-Low NoneExtraversion-High Attention SeekingExtraversion-Low Intimacy Avoidance, Withdrawal, Restricted
Affectivity, AnhedoniaOpenness-High Cognitive and Perceptual Dysregulation,
Unusual Beliefs and Experiences, EccentricityOpenness-Low NoneAgreeableness-High SubmissivenessAgreeableness-Low Suspiciousness, Hostility, Deceitfulness,
Manipulativeness, Grandiosity, CallousnessConscientiousness-High Perseveration, Rigid PerfectionismConscientiousness-Low Irresponsibility, Distractibility, Impulsivity, Risk
Taking
Five-Factor Model of Personality Disorder and DSM-5 1709
“normal” range level of emotionality or that one’s lack of emotion-ality is pathological (e.g., alexithymia; Luminet et al., 1999; Taylor &Bagby, 2004)? In addition, when viewed though an FFM lens, itappears that the DSM-5 trait model undersamples certain maladap-tive poles of personality trait domains. In particular, there are notraits that assess lower levels of Neuroticism, only one trait thatassesses high Extraversion, no traits for low Openness, and one traitfor high Agreeableness. Therefore, quite a few important traits arestill missing.
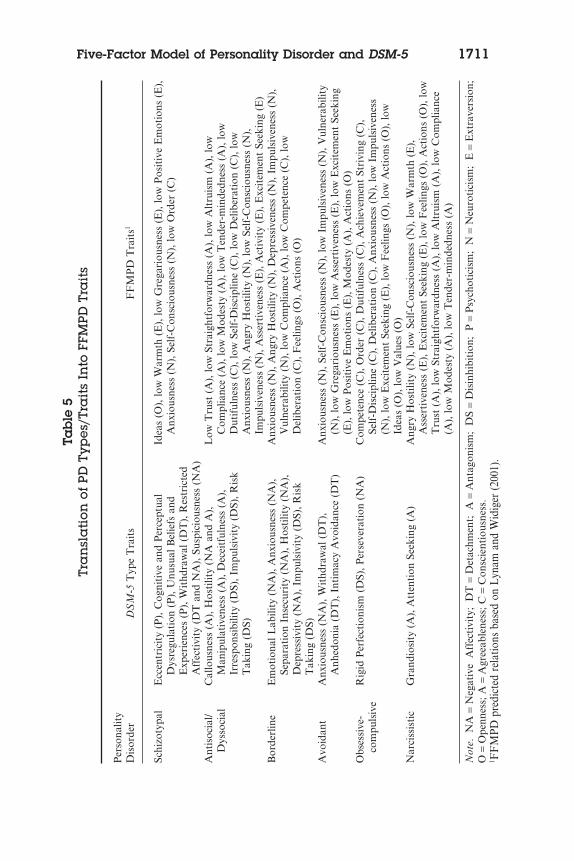
Table 5 presents a “translation” of the DSM-5 PD types into thepersonality traits from the DSM-5 personality model. For compari-son, this table also lists the FFM traits corresponding to each of thefive PDs, as proposed by Lynam & Widiger (2001) in their FFMPDtrait model. Once again, one is struck by the gaps in coverage for thePD types. For example, where is the fearlessness (low Neuroticism)that is crucial to the antisocial/psychopathy construct? Where is thealexithymia and closed-minded dogmatism (low Openness) thatcharacterizes obsessive-compulsive PD? Where is the meekness andmodesty that characterizes avoidant PD? In addition, several traitsare included within two trait domains without explanation (e.g.,restricted affectivity, depressivity, suspiciousness). Finally, some ofthe choices for DSM-5 traits seem odd: Anhedonia for avoidant PD?Why not submissiveness for avoidant PD?
These examples only concern the six PD types retained forDSM-5. Skodol (2010) argued that the personality disordersdeleted from the prior diagnostic manual (paranoid, schizoid,histrionic, dependent) can be recovered from the new traitmodel (see http://www.dsm5.org/ProposedRevisions/Pages/DSM-5TypeandTraitCross-Walk.aspx). However, the “gaps” in trait cov-erage are also apparent when one considers traits relevant todependent PD (high Agreeableness), paranoid and schizoid PD (lowOpenness), and histrionic PD (high Extraversion). Finally, it isunclear whether the four PDs excluded from DSM-5 are “recover-able” from the DSM-5 traits. Specifically, paranoid PD is character-ized by a relatively small number of traits (e.g., suspiciousness,hostility, unusual beliefs and experiences, intimacy avoidance), as istrue for schizoid (e.g., restricted affectivity, withdrawal, intimacyavoidance, anhedonia), histrionic (e.g., emotional lability, manipu-lativeness, attention seeking), and dependent (e.g., anxiousness,separation insecurity, submissiveness) PDs.
Trull1710
Tab
le5
Tra
nsl
ati
onof
PDTy
pes
/Tra
its
Into
FFM
PDTr
ait
s
Per
sona
lity
Dis
orde
rD
SM
-5T
ype
Tra
its
FF
MP
DT
rait
s1
Schi
zoty
pal
Ecc
entr
icit
y(P
),C
ogni
tive
and
Per
cept
ual
Dys
regu
lati
on(P
),U
nusu
alB
elie
fsan
dE
xper
ienc
es(P
),W
ithd
raw
al(D
T),
Res
tric
ted
Aff
ecti
vity
(DT
and
NA
),Su
spic
ious
ness
(NA
)
Idea
s(O
),lo
wW
arm
th(E
),lo
wG
rega
riou
snes
s(E
),lo
wP
osit
ive
Em
otio
ns(E
),A
nxio
usne
ss(N
),Se
lf-C
onsc
ious
ness
(N),
low
Ord
er(C
)
Ant
isoc
ial/
Dys
soci
alC
allo
usne
ss(A
),H
osti
lity
(NA
and
A),
Man
ipul
ativ
enes
s(A
),D
ecei
tful
ness
(A),
Irre
spon
sibi
lity
(DS)
,Im
puls
ivit
y(D
S),R
isk
Tak
ing
(DS)
Low
Tru
st(A
),lo
wSt
raig
htfo
rwar
dnes
s(A
),lo
wA
ltru
ism
(A),
low
Com
plia
nce
(A),
low
Mod
esty
(A),
low
Ten
der-
min
dedn
ess
(A),
low
Dut
iful
ness
(C),
low
Self
-Dis
cipl
ine
(C),
low
Del
iber
atio
n(C
),lo
wA
nxio
usne
ss(N
),A
ngry
Hos
tilit
y(N
),lo
wSe
lf-C
onsc
ious
ness
(N),
Impu
lsiv
enes
s(N
),A
sser
tive
ness
(E),
Act
ivit
y(E
),E
xcit
emen
tSe
ekin
g(E
)B
orde
rlin
eE
mot
iona
lLab
ility
(NA
),A
nxio
usne
ss(N
A),
Sepa
rati
onIn
secu
rity
(NA
),H
osti
lity
(NA
),D
epre
ssiv
ity
(NA
),Im
puls
ivit
y(D
S),R
isk
Tak
ing
(DS)
Anx
ious
ness
(N),
Ang
ryH
osti
lity
(N),
Dep
ress
iven
ess
(N),
Impu
lsiv
enes
s(N
),V
ulne
rabi
lity
(N),
low
Com
plia
nce
(A),
low
Com
pete
nce
(C),
low
Del
iber
atio
n(C
),F
eelin
gs(O
),A
ctio
ns(O
)
Avo
idan
tA
nxio
usne
ss(N
A),
Wit
hdra
wal
(DT
),A
nhed
onia
(DT
),In
tim
acy
Avo
idan
ce(D
T)
Anx
ious
ness
(N),
Self
-Con
scio
usne
ss(N
),lo
wIm
puls
iven
ess
(N),
Vul
nera
bilit
y(N
),lo
wG
rega
riou
snes
s(E
),lo
wA
sser
tive
ness
(E),
low
Exc
item
ent
Seek
ing
(E),
low
Pos
itiv
eE
mot
ions
(E),
Mod
esty
(A),
Act
ions
(O)
Obs
essi
ve-
com
puls
ive
Rig
idP
erfe
ctio
nism
(DS)
,Per
seve
rati
on(N
A)
Com
pete
nce
(C),
Ord
er(C
),D
utif
ulne
ss(C
),A
chie
vem
ent
Stri
ving
(C),
Self
-Dis
cipl
ine
(C),
Del
iber
atio
n(C
),A
nxio
usne
ss(N
),lo
wIm
puls
iven
ess
(N),
low
Exc
item
ent
Seek
ing
(E),
low
Fee
lings
(O),
low
Act
ions
(O),
low
Idea
s(O
),lo
wV
alue
s(O
)N
arci
ssis
tic
Gra
ndio
sity
(A),
Att
enti
onSe
ekin
g(A
)A
ngry
Hos
tilit
y(N
),lo
wSe
lf-C
onsc
ious
ness
(N),
low
War
mth
(E),
Ass
erti
vene
ss(E
),E
xcit
emen
tSe
ekin
g(E
),lo
wF
eelin
gs(O
),A
ctio
ns(O
),lo
wT
rust
(A),
low
Stra
ight
forw
ardn
ess
(A),
low
Alt
ruis
m(A
),lo
wC
ompl
ianc
e(A
),lo
wM
odes
ty(A
),lo
wT
ende
r-m
inde
dnes
s(A
)
Not
e.N
A=
Neg
ativ
eA
ffec
tivi
ty;
DT
=D
etac
hmen
t;A
=A
ntag
onis
m;
DS
=D
isin
hibi
tion
;P
=P
sych
otic
ism
;N
=N
euro
tici
sm;
E=
Ext
rave
rsio
n;O
=O
penn
ess;
A=
Agr
eeab
lene
ss;C
=C
onsc
ient
ious
ness
.1 F
FM
PDpr
edic
ted
rela
tions
base
don
Lyn
aman
dW
idig
er(2
001)
.
Five-Factor Model of Personality Disorder and DSM-5 1711

These problems perhaps reflect that the traits selected were in partthe result of Work Group member nominations (Krueger, 2010),rather than a systematic, comprehensive attempt to adequatelysample major domains of personality (and to do so as distinctly aspossible). Many have decried the overlapping PD constructs thathave appeared in previous diagnostic manuals, as evidenced by thehigh levels of comorbidity (Clark, 2007; Livesley, 2007; Widiger &Trull, 2007). However, many of the 25 traits appear to be closelyrelated and perhaps difficult to distinguish (e.g., separationinsecurity and anxiousness; perseveration and rigid perfectionism;cognitive and perceptual dysregulation and unusual beliefs andexperiences or eccentricity). Therefore, the new proposal does notseem to adequately address the concern regarding overlap andredundancy.
CONCERNS AND COMMENTS ON THE FFMPD
Although the evidence supporting the use of the FFM to characterizeand diagnose personality pathology is strong, there are some criti-cisms and limitations that should be noted as well. In particular,Krueger et al. (2011) argued that there is much confusion over exactlywhat constitutes the FFM. In particular, they highlighted that thereare some differences in the conceptual models of the FFM as opera-tionalized by the various FFM and Big Five measures that are avail-able. Although it is true that there are differences in these measures,we must not conflate measures with conceptual models (Haigler &Widiger, 2001; Krueger et al., 2011). A measure is simply an opera-tionalization of the conceptual model, and some measures mayemphasize certain aspects of the model over others. Further, in thecase of briefer measures, it is sometimes not possible to adequatelysample all aspects of a conceptual model with precision; for example,some brief FFM/Big Five measures do not adequately sample thefacets or primary traits of the five major personality domains of theFFM. In the end, however, Krueger and colleagues’ (2011) argumentcould be applied to other measures of alternative personality models.Ironically, the 25-trait model of personality disorder adopted by theDSM-5 Personality and Personality Disorders Work Group suffersfrom a more damning problem—it is not based on a well-establishedmodel of personality or personality pathology at all. Although the
Trull1712
Work Group noted that it bears some resemblance to the PersonalityPsychopathology Five (PSY-5; Harkness, McNulty, & Ben-Porath,1995), this appears to be more of a post hoc observation instead of theoutcome of a theory-driven approach to measurement.
Although four of the five domains are recognizable from theFFM, the Work Group grafted a “new” personality dimension ontofour of the five personality domains included in the FFM. Specifi-cally, the Work Group included the new domain of Schizotypy,which is now labeled Psychoticism. DSM-5 Psychoticism is definedby only three facet traits, all of which emphasize the quasi-psychoticexperiences and behavior of schizotypal PD. Although there is onlylimited support to date for this “new” personality dimension inclinical samples, when this fifth personality domain is conceptualizedas FFM Openness, there is a wealth of supporting data from clinicalsamples (see Samuel & Widiger, 2008).
One of the strongest arguments being raised against the FFMPD,as well as other dimensional models, is clinical utility (e.g., First,2005). However, the implication of such an argument is that theexisting diagnostic system has clinical utility (Kupfer, First, &Regier, 2002; Rounsaville et al., 2002; Trull & Widiger, 2008; Westen& Arkowitz-Westen, 1998). Although on the surface it might appearthat a categorical diagnosis of PD is congruent with the clinicaldecisions that must be made (i.e., whether to hospitalize, whetherto medicate, whether to provide disability, and whether to provideinsurance coverage), DSM-IV (or even DSM-5) PD diagnoses do notseem suitable for any of these decisions. The diagnostic boundariesand thresholds were not developed with these clinical decisions inmind. Dimensional systems can easily be converted to categoricalsystems, provided appropriate cut-offs are available as well as deci-sion algorithms (Trull & Widiger, 2008).
We believe that a dimensional model of classification has consid-erably greater potential to be clinically useful because one can setdifferent cutoff points along the respective dimensions that areoptimal for different clinical decisions. One can identify the levelof emotional instability that suggests the need for insurance cov-erage, pharmacotherapy, hospitalization, or disability. The diag-nostic system would be constructed explicitly for maximizingutility for different clinical decisions, an approach that is currentlynon-existent and very cumbersome (if not impossible) to imple-
Five-Factor Model of Personality Disorder and DSM-5 1713
ment for the existing diagnostic categories. (Trull & Widiger,2008, pp. 958–959)
Although there are published treatment manuals for many DSM-IV-TR disorders, official treatment guidelines have been developedfor only one personality disorder: borderline (APA, 2001). Oneexplanation is that the DSM-IV-TR PDs are generally not well suitedfor treatment manuals because each PD involves an array of mal-adaptive personality traits, behaviors, and other indicators of thesetraits. Furthermore, there is great heterogeneity within diagnoses(e.g., patients diagnosed with the same PD may share few of the sametraits), and traits may cut across different PD categories (e.g., impul-sivity for both borderline PD and antisocial PD).
In contrast, the FFM appears much better suited to develop spe-cific treatment plans and guidelines. First, because the model wasdeveloped iteratively, the FFM is a more conceptually (as well asempirically) coherent personality structure. For example, by defi-nition, personality disorders are diagnosed when the maladaptivepersonality traits result in “clinical significant distress or impair-ment in social, occupational, or other important areas of function-ing” (APA, 2000, p. 689). The FFM model assesses traits relevantto emotional dysregulation/distress (e.g., Neuroticism traits), tosocial/interpersonal (e.g., Extraversion and Agreeableness traits), towork-oriented behavior and responsibility (e.g., Conscientiousnesstraits), and to cognitive (e.g., Openness traits) domains of function-ing. Further, Miller, Pilkonis, and Mulvey (2006) demonstratedthat FFM traits provided unique information about treatmentutilization and satisfaction above and beyond what could beaccounted for by general distress and by the DSM-IV-TR PDsthemselves.
FFM traits may also have implications for treatment choices aswell as within-treatment behavior. Extraversion and Agreeablenessare relevant to relationship quality both within and outside the con-sultation room. Interpersonal models of therapy, marital and familytherapy, and group therapy might be suggested by maladaptive vari-ants of Extraversion and Agreeableness traits. Neuroticism traits arerelevant to mood, anxiety, and emotional dyscontrol, and problemshere might suggest pharmacologic interventions (e.g., mood stabiliz-ers) or cognitive interventions targeting these dysfunctions. In thecase of Conscientiousness, maladaptively high levels might suggest
Trull1714

treatments that target obsessionality or compulsivity (e.g., exposureplus response prevention or SSRIs). In contrast, low levels mightsuggest treatments for attention deficit, hyperactivity, and impulsiv-ity (e.g., ADHD stimulant medication). Finally, maladaptively highOpenness could indicate cognitive-perceptual aberrations and prob-lems with reality testing, conditions that might be amenable to phar-macologic treatment (e.g., low-dose antipsychotic medication).
These examples are offered to show the treatment implications ofan FFM of personality disorder, and that these are substantiallymore distinct and specific than those for the DSM-IV-TR personalitydisorders. However, an important question is whether cliniciansactually find FFM information useful in their clinical formulations.Several studies have provided encouraging findings. For example,Samuel and Widiger (2006) provided practicing psychologists withdetailed descriptions of actual persons with maladaptive personalitytraits (e.g., Ted Bundy). When asked to describe the person withrespect to the FFM and, alternatively, with the DSM-IV-TR person-ality disorders, clinicians indicated that an FFM dimensional ratingwas more useful than the DSM-IV-TR with respect to providing aglobal description of the individual’s personality, communicatinginformation to clients, encompassing all of the individual’s impor-tant personality difficulties, and even assisting in formulating effec-tive treatment interventions.
Another concern raised regarding the FFMPD is that it is cum-bersome and not user-friendly. However, as detailed above, anFFMPD evaluation can proceed in logical steps, and evaluatingindividuals’ standing on 30 trait facets is much easier and moretime-efficient than assessing almost 100 DSM-IV-TR PD criteria orthan assessing the 25 DSM-5 traits, six PD types, and four variantsof personality functioning called for in the current DSM-5 WorkGroup proposal (Trull & Widiger, 1997; Widiger & Coker, 2002;Widiger & Lowe, 2007).
CONCLUSION
For years, researchers have called for a switch to a dimensionalmodel of personality disorders (Clark, 2007; Livesley, 2007; Widiger& Frances, 1985; Widiger & Trull, 2007), and there have even beenreferences to dimensional models within the text of the DSM-IV-TR
Five-Factor Model of Personality Disorder and DSM-5 1715
(APA, 2000), the most recent diagnostic manual. The time seemedripe for making this change, but, regrettably, the DSM-5 WorkGroup’s proposal for a trait-based PD system falls flat for severalreasons (Widiger, 2011). First, the Work Group had the opportunityto integrate normal personality trait models researched within psy-chology with the personality disorders of psychiatry. Instead, theydecided to construct a “new” five-dimensional model of personalitydisorder. This five-dimensional model excludes normal personalitytraits, does not incorporate years of research on personality andpersonality pathology, and is operationalized in ways so as to missimportant areas of personality functioning.
The DSM-5 Personality and Personality Disorders Work Group’sproposal includes 25 maladaptive personality traits that differen-tially saturate major domains of personality, that are unipolar innature, and that overlap excessively with each other. As notedearlier, the failure to recognize the bipolarity of personality structurecontributes to a number of problems for the DSM-5 proposal,including the failure to include some important traits and the mis-placement of others. Furthermore, as discussed, this 25-trait modeldoes not adequately cover the personality pathology that is assessedin the proposed six PD types as well as that of the excluded PDs fromDSM-IV-TR (the latter which can purportedly be accounted for bythis model).
In the end, the FFMPD seems better suited for the task of repre-senting personality and personality disorder than the DSM-5 WorkGroup 25-trait model. The FFMPD has a strong conceptual andempirical base, its relationship to PD diagnoses has been demon-strated, and it can also point to areas of personality dysfunction thatare not currently represented in diagnostic systems (e.g., racism,alexithymia; Bell, 2004, 2006; Luminet et al., 1999; Taylor & Bagby,2004; Trull, 2005). In addition, the FFMPD holds promise in itsability to inform and guide treatment, as well as in other areas ofclinical utility.
REFERENCES
Allik, J. (2005). Personality dimensions across cultures. Journal of PersonalityDisorders, 19, 212–232.
American Psychiatric Association. (2000). Diagnostic and statistical manual ofmental disorders (4th ed., text rev.). Washington, DC: Author.
Trull1716
American Psychiatric Association. (2001). Practice guidelines for the treatment ofpatients with borderline personality disorder. Washington, DC: Author.
Ashton, M. C., & Lee, K. (2001). A theoretical basis for the major dimensions ofpersonality. European Journal of Personality, 15, 327–353.
Bell, C. C. (2004). Taking issue: Racism. A mental illness? Psychiatric Services, 55,1343.
Bell, C. C. (2006). Reservations and hopes. In T. A. Widiger, E. Simonsen, P. J.Sirovatka, & D. A. Regier (Eds.), Dimensional models of personality disorders:Refining the research agenda for DSM-V (pp. 195–198). Washington, DC:American Psychiatric Association.
Bouchard, T. J., & Loehlin, J. C. (2001). Genes, evolution, and personality.Behavior Genetics, 31, 243–273.
Clark, L. A. (2007). Assessment and diagnosis of personality disorder: Perennialissues and an emerging reconceptualization. Annual Review of Psychology, 58,227–257.
Clark, L. A., & Livesley, W. J. (2002). Two approaches to identifying the dimen-sions of personality disorder: Convergence on the five-factor model. In P. T.Costa & T. A. Widiger (Eds.), Personality disorders and the five-factor model ofpersonality (2nd ed., pp. 161–176). Washington, DC: American PsychologicalAssociation.
Costa, P. T., & McCrae, R. R. (1992). Revised NEO Personality Inventory (NEOPI-R) and NEO Five-Factor Inventory (NEO-FFI) professional manual.Odessa, FL: Psychological Assessment Resources.
Costa, P.T., Jr., & T. A. Widiger. (2002). Personality disorders and the five-factormodel of personality (2nd ed.). Washington, DC: American PsychologicalAssociation.
De Raad, B., & Perugini, M. (Eds.). (2002). Big Five assessment. Bern, Switzer-land: Hogrefe & Huber.
Few, L. R., Miller, J. D., Morse, J. Q., Yaggi, K. E., Reynold, S. K.., & Pilkonis,P. A. (2010). Examining the reliability and validity of clinician ratings on theFive-Factor Model Score Sheet. Assessment, 17, 440–453.
First, M. B. (2005). Clinical utility: A prerequisite for the adoption of adimensional approach in DSM. Journal of Abnormal Psychology, 114,560–564.
Goldberg, L. R. (1993). The structure of phenotypic personality traits. AmericanPsychologist, 48, 26–34.
Haigler, E. D., & Widiger, T. A. (2001). Experimental manipulation of NEO-PI-Ritems. Journal of Personality Assessment, 77, 339–358.
Harkness, A. R., McNulty, J. L., & Ben-Porath, Y. S. (1995). The PersonalityPsychopathology-Five: Constructs and MMPI-2 scales. Psychological Assess-ment, 7, 104–114.
John, O. P., & Srivastava, S. (1999). The Big Five trait taxonomy: History,measurement, and theoretical perspectives. In L. A. Pervin & O. P. John (Eds.),Handbook of personality: Theory and research (2nd ed., pp. 102–138). NewYork: Guilford Press.
Krueger, R. F. (2010, March). Personality traits: Prospects for DSM-V. In C. J.Hopwood (Chair), Personality assessment in context of DSM-V. Symposium
Five-Factor Model of Personality Disorder and DSM-5 1717
conducted at the Annual Meeting of the Society for Personality Assessment,San Jose, CA.
Krueger, R. F., Eaton, N. R., Clark, L. A., Watson, D., Markon, K. E., Derrin-ger, J., et al. (2011). Deriving an empirical structure of personality pathologyfor DSM-5. Journal of Personality Disorders, 25, 170–191.
Kupfer, D. J., First, M. B., & Regier, D. E. (2002). Introduction. In D. J. Kupfer,M. B. First, & D. E. Regier (Eds.), A research agenda for DSM-V (pp. xv–xxiii).Washington, DC: American Psychiatric Association.
Livesley, W. J. (2001). Conceptual and taxonomic issues. In W. J. Livesley (Ed.),Handbook of personality disorders: Theory, research, and treatment (pp. 3–38).New York: Guilford Press.
Livesley, W. J. (2003). Diagnostic dilemmas in classifying personality disorder. InK. A. Phillips, M. B. First, & H. A. Pincus (Eds.), Advancing DSM: Dilemmasin psychiatric diagnosis (pp. 153–190). Washington, DC: American PsychiatricAssociation.
Livesley, W. J. (2007). A framework for integrating dimensional and categoricalclassification of personality disorder. Journal of Personality Disorders, 21, 199–224.
Livesley, W. J. (2010). General Assessment of Personality Dysfunction. Port Huron,MI: Sigma Assessments Systems.
Luminet, O., Bagby, R. M., Wagner, H., Taylor, G. J., Parker, J. D. A., & James,D. A. (1999). Relation between alexithymia and the five-factor model of per-sonality: A facet-level analysis. Journal of Personality Assessment, 73, 345–358.
Lynam, D. R., & Widiger, T. A. (2001). Using the five factor model to representthe DSM-IV personality disorders: An expert consensus approach. Journal ofAbnormal Psychology, 110, 401–412.
Markon, K. E., Krueger, R. F., & Watson, D. (2005). Delineating the structure ofnormal and abnormal personality: An integrative hierarchical approach.Journal of Personality and Social Psychology. 88, 139–157.
McCrae, R. R., Löckenhoff, C. E., & Costa, P. T. (2005). A step toward DSM-V:Cataloguing personality-related problems in living. European Journal of Per-sonality, 19, 269–286.
Miller, J. D. (2012). Five-factor model personality disorder prototypes: A reviewof their development, validity, and comparison to alternative approaches.Journal of Personality, 80, 1565–1591.
Miller, J. D., & Lynam, D. R. (2003). Psychopathy and the five-factor model ofpersonality: A replication and extension. Journal of Personality Assessment, 81,168–178.
Miller, J. D., Pilkonis, P. A., & Mulvey, E. P. (2006). Treatment utilizationand satisfaction: Examining the contributions of axis II psychopathologyand the five-factor model of personality. Journal of Personality Disorders, 20,369–387.
Mullins-Sweatt, S. N., Jamerson, J. E., Samuel, D. B., Olson, D. R., & Widiger, T.A. (2006). Psychometric properties of an abbreviated instrument of the five-factor model. Assessment, 13, 119–137.
Mullins-Sweatt, S. N., & Widiger, T. A. (2006). The five-factor model of person-ality disorder: A translation across science and practice. In R. F. Krueger &
Trull1718

J. L. Tackett (Eds.), Personality and psychopathology (pp. 39–70). New York:Guilford Press.
O’Connor, B. P., & Dyce, J. A. (1998). A test of models of personality disorderconfiguration. Journal of Abnormal Psychology, 107, 3–16.
Rounsaville, B. J., Alarcon, R. D., Andrews, G., Jackson, J. S., Kendell, R. E., &Kendler, K. (2002). Basic nomenclature issues for DSM-V. In D. J. Kupfer,M. B. First, & D. E. Regier (Eds.), A research agenda for DSM-V (pp. 1–29).Washington, DC: American Psychiatric Association.
Samuel, D. B., & Widiger, T. A. (2006). Clinicians’ judgments of clinical utility: Acomparison of the DSM-IV and five factor models. Journal of Abnormal Psy-chology, 115, 298–308.
Samuel, D. B., & Widiger, T. A. (2008). A meta-analytic review of the relation-ships between the five-factor model and DSM-VI-TR personality disorders: Afacet level analysis. Clinical Psychology Review, 28, 1326–1342.
Saulsman, L. M., & Page, A. C. (2004). The five-factor model and personalitydisorder empirical literature: A meta-analytic review. Clinical PsychologyReview, 23, 1055–1085.
Skodol, A. (2010, February 10). Rationale for proposing five specific personalitytypes. Retrieved from http://www.dsm5.org/ProposedRevisions/Pages/RationaleforProposingFiveSpecificPersonalityDisorderTypes.aspx
Skodol, A. E., Bender, D. S., Morey, L. C., Clark, L. A., Oldham, J. M., Alarcon,R. D., et al. (2011). Personality disorder types proposed for DSM-5. Journal ofPersonality Disorders, 25, 136–169.
Taylor, G. J., & Bagby, R. M. (2004). New trends in alexithymia research. Psy-chotherapy and Psychosomatics, 73, 68–77.
Trull, T. J. (1992). DSM-III-R personality disorders and the five-factor model ofpersonality: An empirical comparison. Journal of Abnormal Psychology, 101,553–560.
Trull, T. J. (2005). Dimensional models of personality disorder: Coverage andcutoffs. Journal of Personality Disorders, 19, 262–282.
Trull, T. J., & Durrett, C. A. (2005). Categorical and dimensional modelsof personality disorder. Annual Review of Clinical Psychology, 1, 355–380.
Trull, T. J., Tomko, R. L., Brown, W. C., & Scheiderer, E. M. (2010). Borderlinepersonality disorder in 3-D: Dimensions, symptoms, and measurement chal-lenges. Social and Personality Psychology Compass, 11, 1057–1069.
Trull, T. J., & Widiger, T. A. (1997). Structured Interview for the Five Factor Modelof personality. Odessa, FL: Psychological Assessment Resources.
Trull, T. J., & Widiger, T. A. (2008). Geology 102: More thoughts on a shift to adimensional model of personality disorders. Social and Personality PsychologyCompass, 2, 949–967.
Trull, T. J., Widiger, T. A., & Burr, R. (2001). A structured interview for theassessment of the five factor model of personality: Facet level relations to theaxis II personality disorders. Journal of Personality, 69, 175–198.
Trull, T. J., Widiger, T. A., Lynam, D. R., & Costa, P. T., Jr. (2003). Borderlinepersonality disorder from the perspective of general personality functioning.Journal of Abnormal Psychology, 112, 193–202.
Five-Factor Model of Personality Disorder and DSM-5 1719

Verheul, R., Andrea, H., Berghout, C. C., Dolan, C., Busschbach, J. J. V., van derKroft, P. J. A., et al. (2008). Severity Indices of Personality Problems (SIPP-118): Development, factor structure, reliability, and validity. PsychologicalAssessment, 20, 23–34.
Watson, D., Clark, L. A., & Harkness, A. R. (1994). Structures of personality andtheir relevance to psychopathology. Journal of Abnormal Psychology, 103,18–31.
Westen, D., & Arkowitz-Westen, L. (1998). Limitations of axis II in diagnosingpersonality pathology in clinical practice. American Journal of Psychiatry, 155,1767–1771.
Widiger, T. A. (2011). The DSM-5 dimensional model of personality disorder:Rationale and empirical support. Journal of Personality Disorders, 25, 222–234.
Widiger, T. A., & Coker, L. A. (2002). Assessing personality disorders. In J. N.Butcher (Ed.), Clinical personality assessment: Practical approaches (2nd ed.,pp. 407–434). New York: Oxford University Press.
Widiger, T. A., & Costa, P. T., Jr. (2002). Five-factor model personality disorderresearch. In P. T. Costa, Jr., & T. A. Widiger (Eds.), Personality disorders andthe five-factor model of personality (2nd ed., pp. 59–87). Washington, DC:American Psychological Association.
Widiger, T. A., Costa, P. T., Jr., & McCrae, R. R. (2002). A proposal for axis II:Diagnosing personality disorders using the five factor model. In P. T. Costa,Jr., & T. A. Widiger (Eds.), Personality disorders and the five factor model ofpersonality (2nd ed., pp. 431–456). Washington, DC: American PsychologicalAssociation.
Widiger, T. A., & Frances, A. (1985). The DSM-III personality disorders: Per-spectives from psychology. Archives of General Psychiatry, 42, 615–623.
Widiger, T. A., & Lowe, J. (2007). Five factor model assessment of personalitydisorder. Journal of Personality Assessment, 89, 16–29.
Widiger, T. A., & Mullins-Sweatt, S. N. (2009). Five-factor model of personalitydisorder: A proposal for DSM-V. Annual Review of Clinical Psychology, 5,115–138.
Widiger, T. A., & Simonsen, E. (2005). Alternative dimensional models of per-sonality disorder: Finding a common ground. Journal of Personality Disorders,19, 110–130.
Widiger, T. A., & Trull, T. J. (2007). Plate tectonics in the classification of per-sonality disorder: Shifting to a dimensional model. American Psychologist, 62,71–83.
Widiger, T., Trull, T., Costa, P., McCrae, R., Clarkin, J. F., & Sanderson, C.(1994). Description of the DSM-III-R and DSM-IV personality disorders withthe five factor model of personality. In P. Costa & T. Widiger (Eds.), Person-ality disorders and the five-factor model of personality (pp. 41–56). Washington,DC: American Psychological Association.
Widiger, T. A., Trull, T., Costa, P. T., Jr., McCrae, R., Clarkin, J. F., & Sander-son, C. (2002). Description of the DSM-IV personality disorders with the fivefactor model of personality. In P. T. Costa, Jr., & T. A. Widiger (Eds.),Personality disorders and the five-factor model of personality (2nd ed., pp.89–99). Washington, DC: American Psychological Association.
Trull1720