Embed Size (px)
Citation preview

The Facts About
“DIRTY BOMBS”
Prepared forTHE AMERICAN COUNCIL ON SCIENCE AND HEALTH
By Kathleen Meister, M.S.
P. Andrew Karam, Ph.D., CHP
Art DirectorJennifer Lee
June 2005
AMERICAN COUNCIL ON SCIENCE AND HEALTH1995 Broadway, 2nd Floor, New York, NY 10023-5860
Phone: (212) 362-7044 • Fax: (212) 362-4919URLs: http://acsh.org • http://HealthFactsAndFears.com
E-mail: [email protected]

ACSH accepts unrestricted grants on the condition that it is solely responsible for the conduct of itsresearch and the dissemination of its work to the public. The organization does not perform proprietaryresearch, nor does it accept support from individual corporations for specific research projects. All contri-butions to ACSH—a publicly funded organization under Section 501(c)(3) of the Internal RevenueCode—are tax deductible.
Individual copies of this report are available at a cost of $5.00. Reduced prices for 10 or more copies areavailable upon request.
Copyright © 2005 by American Council on Science and Health, Inc.This book may not be reproduced in whole or in part, by mimeograph or any other means, without per-mission.
01 Executive Summary
01 Introduction
02 Radiological Dispersal Devices
03 Differences Between Radiological and Nuclear Weapons
04 History of Radiological Dispersal Devices
05 Health Effects of Radiation
06 Economic Consequences of a Radiological Attack
07 What to Do in Case of a Dirty Bomb Attack
08 Policies and Regulations
09 Summary
09 References
The Facts About
“DIRTY BOMBS”
TABLE OF CONTENTS
1The Facts About
“DIRTY BOMBS”
EXECUTIVE SUMMARY
• Dirty bombs,” more correctly called radiological dis-persal devices, are weapons that are designed tospread potentially harmful radioactivity. The prin-cipal type combines a conventional explosive withradioactive material.
• Dirty bombs are not nuclear weapons. Unlike anuclear bomb, which could cause hundreds of thou-sands of deaths and devastate an entire city, a dirtybomb would most likely cause a few hundreddeaths at the most. Physical damage would be com-parable to that produced by other conventionalexplosions, and radioactive contamination wouldprobably affect an area of only a few city blocks.
• Most deaths and injuries from a dirty bomb attackwould result from the explosion itself, rather thanthe radioactive material. However, the presence ofradioactive contamination could lead to panic, dis-ruption, and the need for costly and time-consum-ing cleanup.
• The cost of recovery after a dirty bomb attack couldbe reduced, without increasing risks to humanhealth, by modifying regulations pertaining to per-missible levels of residual radioactivity so that theyare based on real risk rather than the ability todetect ever-lower levels of contamination.
• In the event of an explosion, experts advise people tomove away from the immediate area (by walking atleast several blocks from the explosion), goindoors, and turn on local radio or TV for instruc-tions (including instructions about testing forradioactive contamination). If it is determined thatthe explosion involved radioactivity, people whowere in the immediate area should remove and saveclothing and take a shower if possible. Experts rec-ommend that people should not handle any objectthrown off by an explosion and should not takepotassium iodide unless specifically advised to doso. Driving away from an attack is also unwise,since it can hamper emergency response and causecrashes.
INTRODUCTION
Of all the possible types of terrorist attacks, thoseinvolving radioactivity are among the most feared.One type of attack that involves radioactivity is the useof a radiological dispersal device (RDD) or “dirtybomb.” Misconceptions about dirty bombs may leadpeople to be more anxious than the facts justify andmight even prompt some people to take inappropriateactions in the event of a dirty bomb explosion.
This report by the American Council on Science andHealth summarizes the scientific facts about radiolog-ical dispersal devices — what they are, how they might
be made, the possible health and economic conse-quences of an attack, the actions that citizens shouldand should not take if a radiological attack occurs, andthe types of policy changes that may need to be consid-ered to facilitate prevention of radiological attacks andrecovery from them. The principal source of informa-tion for this booklet was a technical manuscript enti-tled “Radiological Terrorism,” written by Dr. P.Andrew Karam of the Rochester Institute ofTechnology. Additional information sources are listedat the end of this report.

The Facts About
“DIRTY BOMBS”2
RADIOLOGICAL DISPERSALDEVICES
Radiological dispersal devices, also called radiologi-cal weapons, are devices that are designed to spreadpotentially harmful radioactivity as part of a hostileact. The principal type of radiological dispersal devicecombines a conventional explosive, such as dynamite,with radioactive material. This is the type of devicethat is often referred to as a “dirty bomb.” When adirty bomb explodes, the explosion itself can causeconsiderable damage — just as any explosion can. Inaddition, the area surrounding the explosion maybecome contaminated by radioactive material.1
Although the exact details would vary dependingupon the type and amount of radioactive materialused, as well as the nature of the explosive device,most deaths and injuries from a dirty bomb wouldalmost certainly result from the explosion itself, ratherthan the radioactive material. People who were closestto the explosion — and therefore most likely to havebeen injured by it — would also be the most likely tobe exposed to dangerous amounts of radioactivity.Some radioactive material might be spread beyond thedamaged area — perhaps to a distance of a few cityblocks — but the intensity of contamination would bemuch less than that in the immediate vicinity of theexplosion. Experts expect that there would be few, ifany, deaths or serious illnesses caused by radiation inindividuals who had not been in the immediate vicin-ity of the blast for a prolonged period of time.
Although the radioactive component of a dirty bombwould probably cause few deaths or injuries, problemsof other kinds would result. The presence of radioac-tivity would make the jobs of firefighters and rescuepersonnel who respond to the emergency more diffi-cult. Healthcare facilities might have to cope withinjured patients who are also contaminated withradioactivity. Large numbers of people might seekcare out of concern over possible contamination, pos-sibly overloading healthcare facilities. Widespread panic could develop, and this might prompt people to
take unwise or even unsafe actions. (For example,people who mistakenly believed that they would needto get many miles away from a dirty bomb attack inorder to be safe might drive away at dangerous speedsor crowd the roads with their cars, thus interferingwith access to the scene by emergency vehicles andalso causing a risk of death and injury from motorvehicle crashes far greater than the risk of death orinjury from the attack itself.) Costly cleanup effortswould almost certainly be necessary, and the buildingsand facilities in the affected neighborhood (probablyseveral city blocks) might be unavailable for a pro-longed period of time. In addition, as has been seen inincidents of accidental radioactive contamination,anxiety and economic disruption due to stigmatizationof the affected area might continue for long periods oftime.
Dirty bombs are not classified as Weapons of MassDestruction because the number of deaths and injuriesthey are likely to cause is relatively small. However,they are sometimes referred to as “Weapons of MassDisruption” because of the many disruptive effectsthat they could have on a community.
Although there have been no successful radiologicalattacks, it is possible to get a rough idea of the typeand extent of problems that might result from theradioactive component of a dirty bomb from instancesof accidental radioactive contamination.
One well-known incident that involved widespreadradioactive contamination occurred in Goiania, Brazil,in 1987. A cancer treatment facility had closed, and itsradiation therapy source, which contained radioactivecesium, had been left behind.2 Unsuspecting residentsfound the abandoned equipment, and someone openedthe canister containing the radioactive cesium.Fascinated by the blue powder they found, residentsplayed with it and spread it on their bodies, unawareof its radioactivity. By the time the nature of the mate-
1. It is also possible to design a radiological attack that does notinvolve an explosive. For example, a powerful source of radioactivitymight be hidden in a public place. Terrorists might also spread radioac-tivity covertly or try to contaminate the food or water supply.
2. Obviously, this should not have happened. Regulations should be inplace in all countries to require that sources of radioactivity no longerin use are disposed of safely. Unfortunately, the extent of control overradioactive sources, both at the time of the Goiania incident and today,varies greatly in different parts of the world.

3The Facts About
“DIRTY BOMBS”
A radiological weapon (dirty bomb) is very differentfrom a nuclear weapon (atomic bomb). In a nuclearweapon, energy is produced by splitting uranium or plu-tonium atoms in such a way that enormous amounts ofenergy are released in a very brief period of time. Theresulting explosion is huge and can devastate a very largearea. In a radiological weapon, the explosive itself is aconventional one; it releases a much smaller amount ofenergy and causes much less destruction. The radioactivematerial present in the bomb is dispersed by the explo-sion, but it does not cause or participate in the explosion;the explosion in this instance is not a nuclear blast.
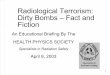
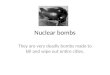
To understand the difference in magnitude between con-ventional and nuclear bombs, it may be helpful to com-pare a large conventional bombing — the bombing of theAlfred P. Murrah Federal Building in Oklahoma City in1995 — with the nuclear bombing of Hiroshima duringWorld War II. The bomb used in Oklahoma City wasequivalent to a few tons of TNT; the bomb detonated overHiroshima was approximately 10,000 times more power-ful. In Oklahoma City, 168 people were killed, the targetbuilding was destroyed, and nearby buildings were seri-ously damaged. In Hiroshima, nearly 100,000 peoplewere killed, and an entire city was virtually destroyed.
An attack with a large radiological weapon might com-bine the physical destruction and casualty level of anOklahoma City-type bombing with a small number ofadditional radiation-related casualties and substantialradiation-related disruption similar to that resulting fromthe Goiania incident.
Nuclear bombing of Hiroshima during World War II.Photo by US Army
Alfred P. Murrah Federal Building after bombing attack.Photo by Oklahoma City Police Department
DIFFERENCES BETWEEN RADIOLOGICAL AND NUCLEAR WEAPONS
rial was known, nearly 250 people had been exposed toelevated radiation levels; four died of radiation sick-ness.
During the response to the Goiania incident, more than3,000 cubic meters of contaminated materials wereremoved for disposal and over 100,000 persons weresurveyed for contamination at the city’s soccer stadium(of whom only a few hundred were actually contami-nated). The recovery process was time-consuming and
expensive. However, the social impact was far greater;even a decade later, Goiania residents were stigmatizedby their association with the region. This stigmatizationincluded an economic impact because sales of agricul-tural products from Goiania declined for absolutely noreason related to food safety or health.

The Facts About
“DIRTY BOMBS”4
HISTORY OF RADIOLOGICALDISPERSAL DEVICES
The idea of radiological weapons is not new. Thepossibility of using bombs that would distributeradioactivity in enemy territory as military weaponswas considered as early as 1941. Today, radiologi-cal weapons are no longer considered practical formilitary use; instead, they are potential terroristweapons.
No radiological dispersal device has ever been suc-cessfully used as a weapon. However, attemptshave been made. In 1997, Chechen terrorists set butdid not explode a device containing radioactivecesium in a Moscow park. In 2002, an arrest wasmade in the U.S. of a person involved in an allegeddirty bomb plot. In several instances, radioactivematerials that might be suitable for use in a radio-logical dispersal device have been stolen, andattempts have been made to smuggle or sell suchmaterials. Thus, it is clear that terrorists continue tobe interested in the possibility of radiologicalattacks.
Constructing and detonating a dirty bomb are noteasy tasks, however. First, radioactive materials
must be obtained — most likely either by theft orby smuggling them from countries where they areavailable for legal or illegal purchase. Second, thematerials must then be incorporated into a bomb —a difficult task, since working with radioactivematerials can be hazardous. Obviously, many ter-rorists are not deterred by sacrificing their lives, buta terrorist would need sufficient working time tocomplete his work; it is hard to construct a device ifthe terrorists working on it receive an incapacitat-ing radiation dose within 15 minutes, for example.Finally, once constructed, the device must be trans-ported to the destination and detonated withoutbeing discovered.
Each of the steps in this process suggests ways inwhich radiological attacks may be prevented. Forexample, increased security at facilities that useradioactive materials, such as hospitals andresearch laboratories, can help to deter theft, andincreased use of radiation detectors at border cross-ings can make it easier to detect smuggling ofradioactive materials.
HEALTH EFFECTS OFRADIATION
The health effects of radiation exposure vary,depending upon the type of radioactive material,the dose of radiation to which a person is exposed,and the route of exposure (e.g., inhalation, inges-tion, external exposure). Exposure to very highdoses of radiation can cause radiation sickness,which is fatal at very high doses but is milder andtemporary at lower doses. Contact with radioactivematerial can also cause radiation burns, which canalso range from mild to severe. In most dirty bombscenarios, however, radiation exposure levelswould be far lower than those shown to cause theseeffects, except perhaps for individuals in immediateproximity to the blast. Unlike the situation with anuclear attack, widespread radiation sicknesswould not result from a dirty bomb attack.
In the event of a radiological attack, people arelikely to find themselves in situations where theyhave an opportunity to aid a victim of the attack,and they may wonder whether it is safe to do this inspite of the possibility of radioactive contamina-tion. For example, a bystander might see an injuredperson with dust on his clothing coming out of abuilding where an explosion had taken place.Would it be safe for the bystander to help the vic-tim move to a safe place or to provide first aid?Experts say that the answer is yes; contaminatedpatients do not pose a hazard to those who are help-ing them. Emergency responders and medical per-sonnel can and should help these people;bystanders can do so as well without jeopardizingtheir own health.

5The Facts About
“DIRTY BOMBS”
It is often reported that the initial symptoms ofradiation sickness include nausea, vomiting, anddiarrhea. This is correct, but it is important toremember that these are nonspecific symptomsthat can also be produced by many other causes,including stress (as millions of people who havebecome “sick to their stomachs” in response toupsetting events can attest). In the aftermath of adirty bomb incident, it is likely that many peoplewould experience such symptoms. However, in allor practically all cases, the symptoms would provenot to be the result of radiation exposure.
Exposure to radiation doses lower than those thatcause radiation sickness, but much higher thanthose normally found in the environment, mayincrease a person’s risk of developing cancer laterin life, especially if exposure is prolonged.However, although radiation is known to be a car-cinogen (cancer-causing agent), it is a weak car-cinogen, and even radiation levels significantly inexcess of natural background levels do not signif-icantly raise cancer risks. Just because a person isnear a source of radioactivity for a short time orcomes in contact with a small amount of dust thatcontains radioactive material does not mean thatthe person will develop cancer. The increase inrisk resulting from such exposures would be quitesmall. In most instances, the detonation of a radi-ological dispersal device would not lead to a sub-stantial increase in the number of cases of cancerin the affected population in later years.
Some recent news accounts have predicted thatexposure to even small amounts of radiation froma radiological attack would cause some additionalcases of cancer. Such predictions are based on thefaulty assumption that effects that occur at highdoses of radiation can be directly extrapolated tomuch lower doses. Increasing scientific evidenceindicates, however, that this type of extrapolationis not valid, and that the health risks associatedwith low-level radiation exposure are smaller thansuch extrapolation would predict.
Another health issue that is often misunderstood isthe effect of radiation exposure during pregnancy.People often believe, incorrectly, that any expo-sure to radiation during pregnancy, no matter howsmall, will have disastrous effects on the unbornchild. Thus, women who had routine dental X-rays before realizing that they were pregnantsometimes panic and consider abortion, eventhough this is unnecessary (routine dental X-raysresult in insignificant radiation exposure to theunborn child). Low doses of radiation pose muchless risk to an unborn child than most people (andeven some physicians) realize. In the event of adirty bomb attack, most pregnant women in theaffected area would not be exposed to amounts ofradiation sufficient to cause harm and would notneed to consider terminating their pregnancies.

The Facts About
“DIRTY BOMBS”6
Although the number of casualties from a radiolog-ical attack would probably be relatively small (tensto hundreds), the economic impact could be verygreat. Some experts think that the cost of recoveryfrom a dirty bomb attack could equal or evenexceed the $30 to $40 billion cost of restoringlower Manhattan after the September 11 attack,despite a much smaller amount of physical damageand fewer casualties.
The high costs would result primarily from theneed to clean up and decontaminate the affectedarea. Much of this effort would consist of physical-ly removing contaminated material (perhapsincluding a layer of soil, as was done in Goiania)and hauling it away to a low-level radioactivewaste depository. Buildings would also need to bedecontaminated — a process that is difficult and insome instances not technically feasible with currenttechnology. If a structure could not be decontami-nated successfully, it might be necessary to demol-ish it, even if it was not physically damaged by theattack.3
In addition to being expensive, cleaning up an areaafter a radiological attack would be very time-con-suming; it is likely that normal activities in physi-cally undamaged areas surrounding an attack sitewould not be able to resume for much longer thanin the case of a non-radiological attack. After theSeptember 11 attack, much of the surrounding areawas reoccupied within days or weeks; in the case ofa radiological attack, it could be months or longerbecause of the need for decontamination.
It may be possible to substantially reduce the extentof the area that would receive extensive decontam-ination after a radiological attack without increas-ing risks to human health by changing the regulato-ry standards for the amount of radiation permittedto remain after cleanup. This type of change, whichis discussed in more detail below under “Policies
and Regulations,” could decrease the cost of recov-ery after a radiological attack and allow normalactivities to resume more quickly.
People’s fears of radiation could add to the eco-nomic impact of a radiological attack. The biggestlong-term economic problems faced by people inGoiania (an agricultural region) resulted from therefusal of people from outside the region to buy itsagricultural products, even though those productswere safe. In the case of a radiological attack on anurban area, similar fears might lead to a reluctanceto purchase industrial products, conduct business inthe area, or visit tourist attractions, all of whichcould cause lasting economic damage.
ECONOMIC CONSEQUENCES OF A RADIOLOGICAL ATTACK
3. Alternatively, a building or area could be abandoned and fenced off, but this option is unlikely to be practical in a major metropolitan area.

7The Facts About
“DIRTY BOMBS”
It is important to note that radioactivity cannot be seen,felt, or smelled. Therefore, the fact that an explosioninvolved radioactivity would not be immediately obvi-ous (unless a terrorist group announced it). In mostinstances, emergency responders, who routinely haveaccess to radiation detectors, would be able to conductradiation surveys and determine fairly quickly, probablywithin a half hour, that a radiological attack had takenplace. This information would then allow the authoritiesto issue correct instructions to the public via the newsmedia.
If a dirty bomb attack occurred, people would find outabout it in two different ways. Some individuals wouldbe close enough to hear, see, or feel an explosion.Others, who were farther away, would hear about theattack through the news media or official announce-ments.
• For those people who were not close enough to theexplosion to hear, see, or feel it, the most importantthing to do would be to turn on a local radio stationor television channel and wait for advice from emer-gency response authorities. In all likelihood, peoplein this situation would not be at any immediate risk.However, just as with any other type of emergency,the authorities might have important instructions forthe public to follow. For example, people might beadvised to stay away from an affected area to avoidinterference with emergency personnel and perhapsalso to avoid exposure to radioactive contamination.
• For people who heard, saw, or felt an explosion, thesituation would be different. These individualswould know that an emergency had occurred, butthey would not know immediately whether radioac-tivity was involved. Because these individuals wereclose to an explosion and might continue to be indanger, they would need to take some actions thatpeople farther away from the explosion would not.
After an explosion, experts recommend that peopleshould do the following:
• Move away from the immediate area — at least sev-eral blocks from the explosion — and go indoors.
• Turn on local radio or TV channels for advisoriesfrom emergency response and health authorities.
• If it is determined that an explosion involved radioac-tivity and if facilities are available, people who were
within sight of or downwind of the explosion shouldconsider changing clothes and showering if possible.These actions will remove at least 90 percent ofexternal contamination. Contaminated clothingshould be placed in plastic bags and sealed until theamount of contamination can be measured.
• If radioactive material was released, local newsbroadcasts will advise people where to report forradiation monitoring and blood and other tests todetermine whether they were in fact exposed andwhat steps to take to protect their health.
• Because inhaling any kind of dust, and especiallydust that may be contaminated with radioactivematerial, is unhealthful, some experts recommendthat people take simple precautions to avoid inhalingcontaminants during the immediate aftermath of anexplosion, such as breathing through a folded cloth ifone is readily available and going indoors and clos-ing doors and windows as soon as possible.
• Another important precaution is to not handle or pickup any object thrown off by an explosion. In theevent that the object was part of the radioactivesource used in a dirty bomb, it could be quite danger-ous. Handling things without knowing what theywere is what got people into trouble in Goiania; thesame could occur after a dirty bomb explosion.
People sometimes wonder whether they should takepotassium iodide to protect their health if a radiologicalattack occurs. The answer in almost all possible dirtybomb scenarios is no. Potassium iodide protects onlyagainst damage to the thyroid gland from radioactiveiodine; it does not protect other parts of the body, and itis of no use against other radioactive materials. It is veryunlikely that radioactive iodine would be used in a dirtybomb.
Another course of action that is usually unwise (unlessspecifically advised by authorities) is driving away fromthe area of an attack. People can move to a safe distancefrom a radiological attack by walking rather than driv-ing; staying off the roads reduces the risk of traffic con-gestion that can hamper response to the emergency orcause crashes. Also, an automobile that was in the imme-diate vicinity of a dirty bomb explosion could be con-taminated with radioactivity. People who drive away inthat automobile might expose themselves to moreradioactivity than they would if they walked to a safelocation.
WHAT TO DO IN CASE OF A DIRTY BOMB ATTACK

The Facts About
“DIRTY BOMBS”8
As societies make efforts to prevent radiologicalattacks and to ensure the most effective response if anattack occurs, consideration may be given to modify-ing some policies and regulations that were notdesigned with radiological attacks in mind. Citizensneed to understand the rationale behind such propos-als in order to make informed decisions about theirmerits. A proposal that appears “overly restrictive” or“insufficiently protective” on the surface might wellbe found to be beneficial when all its advantages anddisadvantages are taken into consideration. The fol-lowing examples may help to illustrate this point.
Legal purchase of radioactive materials in the U.S.requires possession of a radioactive materials license.These licenses are considered public documents andtherefore are available for public scrutiny. Thismeans that a terrorist organization may be able toobtain copies of the documents and use these to iden-tify likely targets for theft. Thus, it may be worth-while to consider prohibiting public access to thesedocuments. The government — and by extension, thepublic — would need to decide whether the potentialbenefits of this regulatory change justify limiting cit-izens’ freedom of access to this particular type ofinformation.
If terrorists are to construct and transport a radiolog-ical dispersal device with reasonable safety to them-selves, they would need to obtain large quantities oflead to use as shielding. Accordingly, a case could bemade for requiring lead vendors to report large salesof their products. If such a proposal is considered, itspotential benefits would have to be weighed againstthe additional burdens that would be placed on thelead industry and the likely resulting increases in thecost of this industry’s products.
Some current regulations pertaining to permissiblelevels of radioactive contamination may have beenbased more on what is achievable or what isdetectable than on what is truly necessary to protecthealth and the environment. In the event of an attack,
these unnecessarily stringent regulations might ham-per a community’s ability to recover by increasingthe amounts of time and money mandated for cleanupwithout providing any benefits that would offsetthese costs. Therefore, society may wish to revisitregulatory guidance so that regulations are based onreal risk rather than the ability to detect ever-lowerlevels of contamination.
It has been proposed, for example, that the standardfor the amount of added radioactivity allowed toremain after cleanup from a radiological attack beincreased tenfold.4 This might decrease the cost ofrecovery by perhaps 90 percent and somewhatdecrease the time needed for cleanup.
The current standard set by the Nuclear RegulatoryCommission is 25 mrem (millirems) of addedradioactivity per year5; the Environmental ProtectionAgency’s standard is 15 mrem per year. For compar-ison, it helps to know that the natural backgroundradiation to which people are normally exposed isseveral hundred millirems per year, with substantialvariations from place to place. Residents ofWashington, D.C., for example, are exposed to 300mrem/year, which is close to the national average.Residents of Denver, Colorado, which is at a higheraltitude (therefore allowing more exposure to cosmicradiation) and has underground uranium deposits, areexposed to about 500 mrem/year.
Increasing the standard for residual radioactivity ten-fold would mean allowing about 200 mrem/year ofadded radiation to remain in the environment aftercleanup from a radiological attack; this is the same asthe additional exposure that would come from livingin Denver rather than Washington. No radiation-asso-ciated health risks have been associated with living inDenver; cancer rates there are similar to those inWashington. Similarly, no adverse effects on humanhealth would be expected if a residual radioactivitystandard of around 200 mrem/year were adopted.
POLICIES AND REGULATIONS
4. This proposal is recommended and discussed in detail inZimmerman, Peter D. with Cheryl Loeb, Dirty Bombs: The ThreatRevisited, National Defense University, January 2004. Availableonline at http://hps.org/documents/RDD_report.pdf
5. A rem is a unit that relates the absorbed dose of radiation in humantissue to the effective biological damage of the radiation. Differenttypes of radiation have different biological effects; expressingamounts of exposure in rems allows these different types of radiationto be compared.

9The Facts About
“DIRTY BOMBS”
SUMMARY
Dirty bombs, more correctly referred to as radio-logical dispersal devices or radiological weapons,are conventional explosive devices with addedradioactive material. They are designed to spreadradioactive contamination — and with it, panic,anxiety, and social and economic disruption — ina community. To ensure appropriate responses inthe event of a radiological attack, citizens need tounderstand that the principal danger from a dirtybomb lies in the explosion itself; in most
scenarios, few if any people who were not closeenough to the blast to be injured by it would expe-rience any adverse health effects from radiationexposure. Citizens can help to minimize the harm-ful impact of a radiological attack by followingthe instructions of emergency response authoritiesand by avoiding hasty actions prompted by panicor unwarranted fears of even small amounts ofradioactivity.
REFERENCES
Karam, P. Andrew, Radiological Terrorism. Human and Ecological Risk Assessment, in press.
Ferguson CD and Potter WC. 2004. The Four Faces of Nuclear Terrorism. Monterey Institute forInternational Studies Center for Nonproliferation Studies, Monterey CA.
Ferguson CD, Kazi T, and Perera J. 2003. Center for Nonproliferation Studies Occasional Paper #11,Commercial Radioactive Sources: Surveying the Security Risks. Monterey Institute Center forNonproliferation Studies, Monterey, CA.
NCRP (National Council on Radiation Protection and Measurements). 2001. Report #138.Management of Terrorist Events Involving Radioactive Material.
U.S. Nuclear Regulatory Commission, Dirty bombs [fact sheet], March 2003. Available online athttp://www.nrc.gov/reading-rm/doc-collections/fact-sheets/dirty-bombs.html
U.S. Nuclear Regulatory Commission, Backgrounder on dirty bombs, April 2005. Available online athttp://www.nrc.gov/reading-rm/doc-collections/fact-sheets/dirty-bombs.html
U.S. Centers for Disease Control and Prevention, Frequently asked questions about dirty bombs,March 2005. Available online at http://www.bt.cdc.gov/radiation/dirtybombs.asp
Zimmerman, Peter D. with Cheryl Loeb, Dirty Bombs: The Threat Revisited, National DefenseUniversity, January 2004. Available online at http://hps.org/documents/RDD_report.pdf
Elizabeth M. Whelan, Sc.D., M.P.H., President
A C S H B O A R D O F D I R E C T O R S
John H. Moore, Ph.D., M.B.A. Chairman of the Board, ACSHGrove City College
Elissa P. Benedek, M.D. University of Michigan
Norman E. Borlaug, Ph.D. Texas A&M University
Michael B. Bracken, Ph.D., M.P.H. Yale University School of Medicine
Christine M. Bruhn, Ph.D. University of California
Taiwo K. Danmola, C.P.A.Ernst & Young
Thomas R. DeGregori, Ph.D.University of Houston
Henry I. Miller, M.D.Hoover Institution
A. Alan Moghissi, Ph.D. Institute for Regulatory Science
Albert G. Nickel Lyons Lavey Nickel Swift, inc.
Kenneth M. Prager, M.D.Columbia College of Physicians and Surgeons
Stephen S. Sternberg, M.D. Memorial Sloan-Kettering Cancer Center
Mark C. Taylor, M.D.
Physicians for a Smoke-Free Canada
Lorraine Thelian Ketchum Public Relations
Kimberly M. Thompson, Sc.D. Harvard School of Public Health
Elizabeth M. Whelan, Sc.D., M.P.H. American Council on Science and Health
Robert J. White, M.D., Ph.D. Case Western Reserve University
A C S H B O A R D O F S C I E N T I F I C A N D P O L I C Y A D V I S O R S
Ernest L. Abel, Ph.D.C.S. Mott Center
Gary R. Acuff, Ph.D.Texas A&M University
Alwynelle S. Ahl, Ph.D., D.V.M.Tuskegee University, AL
Julie A. Albrecht, Ph.D.University of Nebraska, Lincoln
James E. Alcock, Ph.D.Glendon College, York University
Thomas S. Allems, M.D., M.P.H.San Francisco, CA
Richard G. Allison, Ph.D.American Society for Nutritional Sciences(FASEB)
John B. Allred, Ph.D.Ohio State University
Philip R. Alper, M.D.University of California, San Francisco
Karl E. Anderson, M.D.University of Texas, Medical Branch
Dennis T. AveryHudson Institute
Ronald Bachman, M.D.Kaiser-Permanente Medical Center
Robert S. Baratz, D.D.S., Ph.D., M.D.International Medical Consultation Services
Nigel M. Bark, M.D.Albert Einstein College of Medicine
Stephen Barrett, M.D.Allentown, PA
Thomas G. Baumgartner, Pharm.D.,M.Ed.University of Florida
W. Lawrence Beeson, Dr.P.H.Loma Linda University School of PublicHealth
Barry L. Beyerstein, Ph.D.Simon Fraser University
Steven Black, M.D.Kaiser-Permanente Vaccine Study Center
Blaine L. Blad, Ph.D.University of Nebraska, Lincoln
Hinrich L. Bohn, Ph.D.University of Arizona
Ben Bolch, Ph.D.Rhodes College
Joseph F. Borzelleca, Ph.D.Medical College of Virginia
Michael K. Botts, Esq.Ames, IA
George A. Bray, M.D.Pennington Biomedical Research Center
Ronald W. Brecher, Ph.D., C.Chem.,DABTGlobalTox International Consultants, Inc.
Robert L. Brent, M.D., Ph.D.Alfred I. duPont Hospital for Children
Allan Brett, M.D.University of South Carolina
Kenneth G. Brown, Ph.D.KBinc
Gale A. Buchanan, Ph.D.University of Georgia
George M. Burditt, J.D.Bell, Boyd & Lloyd LLC
Edward E. Burns, Ph.D.Texas A&M University
Francis F. Busta, Ph.D.University of Minnesota
Elwood F. Caldwell, Ph.D., M.B.A.University of Minnesota
Zerle L. Carpenter, Ph.D.Texas A&M University System
Robert G. Cassens, Ph.D.University of Wisconsin, Madison
Ercole L. Cavalieri, D.Sc.University of Nebraska Medical Center
Russell N. A. Cecil, M.D., Ph.D.Albany Medical College
Rino Cerio, M.D.Barts and The London Hospital Institute ofPathology
Morris E. Chafetz, M.D.Health Education Foundation
Bruce M. Chassy, Ph.D.University of Illinois, Urbana-Champaign
Dale J. Chodos, M.D.Kalamazoo, MI
Martha A. Churchill, Esq.Milan, MI
Emil William Chynn, M.D.Manhattan Eye, Ear & Throat Hospital
Dean O. Cliver, Ph.D.University of California, Davis
F. M. Clydesdale, Ph.D.University of Massachusetts
Donald G. Cochran, Ph.D.Virginia Polytechnic Institute and StateUniversity
W. Ronnie Coffman, Ph.D.Cornell University
Bernard L. Cohen, D.Sc.University of Pittsburgh
John J. Cohrssen, Esq.Public Health Policy Advisory Board
Neville Colman, M.D., Ph.D.St. Luke’s Roosevelt Hospital Center
Gerald F. Combs, Jr., Ph.D.Cornell University
Michael D. Corbett, Ph.D.Omaha, NE
Morton Corn, Ph.D.John Hopkins University
Nancy Cotugna, Dr.Ph., R.D., C.D.N.University of Delaware
Roger A. Coulombe, Jr., Ph.D.Utah State University
H. Russell Cross, Ph.D.Future Beef Operations, L.L.C.
James W. Curran, M.D., M.P.H.Emory University
Charles R. Curtis, Ph.D.Ohio State University
Ilene R. Danse, M.D.Novato, CA
Ernst M. Davis, Ph.D.University of Texas, Houston
Harry G. Day, Sc.D.Indiana University
Robert M. Devlin, Ph.D.University of Massachusetts
Seymour Diamond, M.D.Diamond Headache Clinic
Donald C. Dickson, M.S.E.E.Gilbert, AZ
John DieboldThe Diebold Institute for Public PolicyStudies
Ralph Dittman, M.D., M.P.H.Houston, TX
John E. Dodes, D.D.S.National Council Against Health Fraud
Sir Richard Doll, M.D., D.Sc., D.M.University of Oxford
John Doull, M.D., Ph.D.University of Kansas
Theron W. Downes, Ph.D.Michigan State University
Michael Patrick Doyle, Ph.D.University of Georgia
Adam Drewnowski, Ph.D.University of Washington
Michael A. Dubick, Ph.D.U.S. Army Institute of Surgical Research
Greg Dubord, M.D., M.P.H.RAM Institute
Edward R. Duffie, Jr., M.D.Savannah, GA
David F. Duncan, Dr.Ph.Duncan & Associates
James R. Dunn, Ph.D.Averill Park, NY
Robert L. DuPont, M.D.Institute for Behavior and Health, Inc.
Henry A. Dymsza, Ph.D.University of Rhode Island
Michael W. Easley, D.D.S., M.P.H.State University of New York, Buffalo
J. Gordon Edwards, Ph.D.San José State University
George E. Ehrlich, M.D., F.A.C.P.,M.A.C.R., FRCP (Edin)Philadelphia, PA
Michael P. Elston, M.D., M.S.Rapid City Regional Hospital
William N. Elwood, Ph.D.Center for Public Health & EvaluationResearch
James E. Enstrom, Ph.D., M.P.H.University of California, Los Angeles
Stephen K. Epstein, M.D., M.P.P.,FACEPBeth Israel Deaconess Medical Center
Myron E. Essex, D.V.M., Ph.D.Harvard School of Public Health
Terry D. Etherton, Ph.D.Pennsylvania State University
R. Gregory Evans, Ph.D., M.P.H.St. Louis University Center for the Study ofBioterrorism and Emerging Infections
William Evans, Ph.D.University of Alabama
Daniel F. Farkas, Ph.D., M.S., P.E.Oregon State University
Richard S. Fawcett, Ph.D.Huxley, IA
John B. Fenger, M.D.Phoenix, AZ
Owen R. Fennema, Ph.D.University of Wisconsin, Madison
Frederick L. Ferris, III, M.D.National Eye Institute
David N. Ferro, Ph.D.University of Massachusetts
Madelon L. Finkel, Ph.D.Cornell University Medical College
Jack C. Fisher, M.D.University of California, San Diego
Kenneth D. Fisher, Ph.D.Washington, DC
Leonard T. Flynn, Ph.D., M.B.A.Morganville, NJ
William H. Foege, M.D., M.P.H.Emory University
Ralph W. Fogleman, D.V.M.Doylestown, PA
Christopher H. Foreman, Jr., Ph.D.University of Maryland
E. M. Foster, Ph.D.University of Wisconsin, Madison
F. J. Francis, Ph.D.University of Massachusetts
Glenn W. Froning, Ph.D.University of Nebraska, Lincoln
Vincent A. Fulginiti, M.D.University of Colorado
Arthur Furst, Ph.D., Sc.D.University of San Francisco
Robert S. Gable, Ed.D., Ph.D., J.D.Claremont Graduate University
Shayne C. Gad, Ph.D., D.A.B.T., A.T.S.Gad Consulting Services
William G. Gaines, Jr., M.D., M.P.H.Scott & White Clinic
Charles O. Gallina, Ph.D.Professional Nuclear Associates
Raymond Gambino, M.D. Quest Diagnostics Incorporated
Randy R. Gaugler, Ph.D.Rutgers University
J. Bernard L. Gee, M.D.Yale University School of Medicine
K. H. Ginzel, M.D.University of Arkansas for Medical Sciences
William Paul Glezen, M.D.Baylor College of Medicine
Jay A. Gold, M.D., J.D., M.P.H.Medical College of Wisconsin
Roger E. Gold, Ph.D.Texas A&M University
Reneé M. Goodrich, Ph.D.University of Florida
Frederick K. Goodwin, M.D.The George Washington University MedicalCenter
Timothy N. Gorski, M.D., F.A.C.O.G.Arlington, TX
Ronald E. Gots, M.D., Ph.D.International Center for Toxicology andMedicine
Henry G. Grabowski, Ph.D.Duke University
James Ian Gray, Ph.D.Michigan State University
William W. Greaves, M.D., M.S.P.H.Medical College of Wisconsin
A C S H E X E C U T I V E S T A F F
A C S H B O A R D O F S C I E N T I F I C A N D P O L I C Y A D V I S O R S
Kenneth Green, D.Env.Reason Public Policy Institute
Laura C. Green, Ph.D., D.A.B.T.Cambridge Environmental, Inc.
Saul Green, Ph.D.Zol Consultants
Richard A. Greenberg, Ph.D.Hinsdale, IL
Sander Greenland, Dr.P.H., M.A.UCLA School of Public Health
Gordon W. Gribble, Ph.D.Dartmouth College
William Grierson, Ph.D.University of Florida
Lester Grinspoon, M.D.Harvard Medical School
F. Peter Guengerich, Ph.D.Vanderbilt University School of Medicine
Caryl J. Guth, M.D.Hillsborough, CA
Philip S. Guzelian, M.D.University of Colorado
Alfred E. Harper, Ph.D.University of Wisconsin, Madison
Terryl J. Hartman, Ph.D., M.P.H.,R.D.The Pennsylvania State University
Clare M. Hasler, Ph.D.University of Illinois at Urbana-Champaign
Robert D. Havener, M.P.A.Sacramento, CA
Virgil W. Hays, Ph.D.University of Kentucky
Cheryl G. Healton, Dr.PH.Columbia University
Clark W. Heath, Jr., M.D.American Cancer Society
Dwight B. Heath, Ph.D.Brown University
Robert Heimer, Ph.D.Yale School of Public Health
Robert B. Helms, Ph.D.American Enterprise Institute
Zane R. Helsel, Ph.D.Rutgers University, Cook College
Donald A. Henderson, M.D., M.P.H.Johns Hopkins University
James D. Herbert, Ph.D.MCP Hahnemann University
Gene M. Heyman, Ph.D.McLean Hospital/Harvard Medical School
Richard M. Hoar, Ph.D.Williamstown, MA
Theodore R. Holford, Ph.D.Yale University School of Medicine
Robert M. Hollingworth, Ph.D.Michigan State University
Edward S. Horton, M.D.Joslin Diabetes Center
Joseph H. Hotchkiss, Ph.D.Cornell University
Steve E. Hrudey, Ph.D.University of Alberta
Susanne L. Huttner, Ph.D.University of California, Berkeley
Robert H. Imrie, D.V.M.Seattle, WA
Lucien R. Jacobs, M.D.University of California, Los Angeles
Alejandro R. Jadad, M.D., D.Phil.,F.R.C.P.C.University of Toronto, Canada
Rudolph J. Jaeger, Ph.D.Environmental Medicine, Inc.
William T. Jarvis, Ph.D.Loma Linda University
Michael Kamrin, Ph.D.Michigan State University
John B. Kaneene,Ph.D., M.P.H.,D.V.M.Michigan State University
P. Andrew Karam, Ph.D., CHPUniversity of Rochester
Philip G. Keeney, Ph.D.Pennsylvania State University
John G. Keller, Ph.D. Olney, MD
Kathryn E. Kelly, Dr.P.H.Delta Toxicology
George R. Kerr, M.D.University of Texas, Houston
George A. Keyworth II, Ph.D.Progress and Freedom Foundation
Michael Kirsch, M.D.Highland Heights, OH
John C. Kirschman, Ph.D.Emmaus, PA
Ronald E. Kleinman, M.D.Massachusetts General Hospital
Leslie M. Klevay, M.D., S.D.in Hyg.University of North Dakota School ofMedicine
David M. Klurfeld, Ph.D.Wayne State University
Kathryn M. Kolasa, Ph.D., R.D.East Carolina University
James S. Koopman, M.D, M.P.H.University of Michigan
Alan R. Kristal, Dr.P.H.Fred Hutchinson Cancer Research Center
David Kritchevsky, Ph.D.The Wistar Institute
Stephen B. Kritchevsky, Ph.D.Wake Forest University Health Sciences
Mitzi R. Krockover, M.D.Humana, Inc.
Manfred Kroger, Ph.D.Pennsylvania State University
Laurence J. Kulp, Ph.D.University of Washington
Sandford F. Kuvin, M.D.University of Miami
Carolyn J. Lackey, Ph.D., R.D.North Carolina State University
Pagona Lagiou, M.D., DrMedSciUniversity of Athens Medical School
J. Clayburn LaForce, Ph.D.University of California, Los Angeles
James C. Lamb, IV, Ph.D., J.D.Blasland, Bouck & Lee
Lawrence E. Lamb, M.D.San Antonio, TX
William E. M. Lands, Ph.D.College Park, MD
Lillian Langseth, Dr.P.H.Lyda Associates, Inc.
Brian A. Larkins, Ph.D.University of Arizona
Larry Laudan, Ph.D.National Autonomous University of Mexico
Tom B. Leamon, Ph.D.Liberty Mutual Insurance Company
Jay H. Lehr, Ph.D.Environmental Education Enterprises, Inc.
Brian C. Lentle, M.D., FRCPC, DMRDUniversity of British Columbia
Floy Lilley, J.D.Amelia Island, FlF
Paul J. Lioy, Ph.D.UMDNJ-Robert Wood Johnson MedicalSchool
William M. London, Ed.D., M.P.H.Walden University
Frank C. Lu, M.D., BCFEMiami, FL
William M. Lunch, Ph.D.Oregon State University
Daryl Lund, Ph.D.University of Wisconsin
George D. Lundberg, M.D.Medscape
Howard D. Maccabee, Ph.D., M.D.Radiation Oncology Center
Janet E. Macheledt, M.D., M.S.,M.P.H.Houston, TX
Roger P. Maickel, Ph.D. Purdue University
Henry G. Manne, J.S.D.George Mason University Law School
Karl Maramorosch, Ph.D.Rutgers University, Cook College
Judith A. Marlett, Ph.D., R.D.University of Wisconsin, Madison
James R. Marshall, Ph.D.Roswell Park Cancer Institute
Mary H. McGrath, M.D., M.P.H.Loyola University Medical Center
Alan G. McHughen, D.Phil.University of California, Riverside
James D. McKean, D.V.M., J.D.Iowa State University
John J. McKetta, Ph.D.University of Texas at Austin
Donald J. McNamara, Ph.D.Egg Nutrition Center
Michael H. Merson, M.D.Yale University School of Medicine
Patrick J. Michaels, Ph.D.University of Virginia
Thomas H. Milby, M.D., M.P.H.Walnut Creek, CA
Joseph M. Miller, M.D., M.P.H.University of New Hampshire
William J. Miller, Ph.D.University of Georgia
Dade W. Moeller, Ph.D.Harvard University
Grace P. Monaco, J.D.Medical Care Management Corp.
Brian E. Mondell, M.D.Baltimore Headache Institute
Eric W. Mood, LL.D., M.P.H.Yale University School of Medicine
John W. Morgan, Dr.P.H.California Cancer Registry
W. K. C. Morgan, M.D.University of Western Ontario
Stephen J. Moss, D.D.S., M.S.Health Education Enterprises, Inc.
Brooke T. Mossman, Ph.D.University of Vermont College of Medicine
Allison A. Muller, Pharm.DThe Children’s Hospital of Philadelphia
Ian C. Munro, F.A.T.S., Ph.D.,FRCPathCantox Health Sciences International
Kevin B. MurphyMerrill Lynch, Pierce, Fenner & Smith
Harris M. Nagler, M.D.Beth Israel Medical Center
Daniel J. Ncayiyana, M.D.University of Cape Town
Philip E. Nelson, Ph.D.Purdue University
Malden C. Nesheim, Ph.D.Cornell University
Joyce A. Nettleton, D.Sc., R.D.Aurora, Co
John S. Neuberger, Dr.P.H.University of Kansas School of Medicine
Gordon W. Newell, Ph.D., M.S.,F.-A.T.S.Palo Alto, CA
Thomas J. Nicholson, Ph.D., M.P.H.Western Kentucky University
Steven P. Novella, M.D.Yale University School of Medicine
James L. Oblinger, Ph.D.North Carolina State University
Deborah L. O’Connor, Ph.D.University of Toronto/The Hospital for SickChildren
John Patrick O’Grady, M.D.Tufts University School of Medicine
James E. Oldfield, Ph.D.Oregon State University
Stanley T. Omaye, Ph.D., F.-A.T.S.,F.ACN, C.N.S.University of Nevada, Reno
Michael T. Osterholm, Ph.D., M.P.H.University of Minnesota
M. Alice Ottoboni, Ph.D.Sparks, NV
Michael W. Pariza, Ph.D.University of Wisconsin, Madison
Stuart Patton, Ph.D.University of California, San Diego
James Marc Perrin, M.D.Mass General Hospital for Children
Timothy Dukes Phillips, Ph.D.Texas A&M University
Mary Frances Picciano, Ph.D.National Institutes of Health
David R. Pike, Ph.D.University of Illinois, Urbana-Champaign
Thomas T. Poleman, Ph.D.Cornell University
Charles Poole, M.P.H., Sc.DUniversity of North Carolina School ofPublic Health
Gary P. Posner, M.D.Tampa, FL
John J. Powers, Ph.D.University of Georgia
William D. Powrie, Ph.D.University of British Columbia
C.S. Prakash, Ph.D.Tuskegee University
Kary D. PrestenU.S. Trust Co.
Marvin P. Pritts, Ph.D.Cornell University
Daniel J. Raiten, Ph.D.National Institute of Health
David W. Ramey, D.V.M.Ramey Equine Group
R.T. Ravenholt, M.D., M.P.H.Population Health Imperatives
Russel J. Reiter, Ph.D.University of Texas, San Antonio
William O. Robertson, M.D.University of Washington School ofMedicine
J. D. Robinson, M.D.Georgetown University School of Medicine
Bill D. Roebuck, Ph.D., D.A.B.T.Dartmouth Medical School
David B. Roll, Ph.D.University of Utah
Dale R. Romsos, Ph.D.Michigan State University
Joseph D. Rosen, Ph.D.Cook College, Rutgers University
Steven T. Rosen, M.D.Northwestern University Medical School
Kenneth J. Rothman, Dr.P.H.Boston University
Stanley Rothman, Ph.D.Smith College
Edward C. A. Runge, Ph.D.Texas A&M University
Stephen H. Safe, D.Phil.Texas A&M University
Wallace I. Sampson, M.D.Stanford University School of Medicine
Harold H. Sandstead, M.D.University of Texas Medical Branch
Charles R. Santerre, Ph.D.Purdue University
Herbert P. Sarett, Ph.D.Sarasota, FL
Sally L. Satel, M.D.American Enterprise Institute
Lowell D. Satterlee, Ph.D.Oklahoma State University
Jeffrey Wyatt SavellTexas A&M University
Marvin J. Schissel, D.D.S.Roslyn Heights, NY
Lawrence J. Schneiderman, M.D.University of California, San Diego
Edgar J. Schoen, M.D.Kaiser Permanente Medical Center
David Schottenfeld, M.D., M.Sc.University of Michigan
Joel M. Schwartz, M.S.American Enterprise Institute
David E. Seidemann, Ph.D. Brooklyn College/Yale University
Patrick J. Shea, Ph.D.University of Nebraska, Lincoln
Michael B. Shermer, Ph.D.Skeptic Magazine

The opinions expressed in ACSH publications do not necessarily represent the views of all ACSH Directors and Advisors. ACSH Directors and Advisors serve without compensation.
Sidney Shindell, M.D., LL.B.Medical College of Wisconsin
Sarah Short, Ph.D., Ed.D., R.D.Syracuse University
A. J. Siedler, Ph.D.University of Illinois, Urbana-Champaign
Lee M. Silver, Ph.D.Princeton University
Michael S. Simon, M.D., M.P.H.Wayne State University
S. Fred Singer, Ph.D.Science & Environmental Policy Project
Robert B. Sklaroff, M.D.Elkins Park, PA
Anne M. Smith, Ph.D., R.D., L.D.The Ohio State University
Gary C. Smith, Ph.D.Colorado State University
John N. Sofos, Ph.D.Colorado State University
Roy F. Spalding, Ph.D.University of Nebraska, Lincoln
Leonard T. Sperry, M.D., Ph.D.Barry University
Robert A. Squire, D.V.M., Ph.D.Johns Hopkins University
Ronald T. Stanko, M.D.University of Pittsburgh Medical Center
James H. Steele, D.V.M., M.P.H.University of Texas, Houston
Robert D. Steele, Ph.D.Pennsylvania State University
Judith S. Stern, Sc.D., R.D.University of California, Davis
Ronald D. Stewart, O.C., M.D.,FRCPCDalhousie University
Martha Barnes Stone, Ph.D.Colorado State University
Jon A. Story, Ph.D.Purdue University
Michael M. Sveda, Ph.D.Gaithersburg, MD
Glenn Swogger, Jr., M.D.Topeka, KS
Sita R. Tatini, Ph.D. University of Minnesota
Steve L. Taylor, Ph.D.University of Nebraska, Lincoln
James W. Tillotson, Ph.D., M.B.A.Tufts University
Dimitrios Trichopoulos, M.D.Harvard School of Public Health
Murray M. Tuckerman, Ph.D.Winchendon, MA
Robert P. Upchurch, Ph.D.University of Arizona
Mark J. Utell, M.D.University of Rochester Medical Center
Shashi B. Verma, Ph.D.University of Nebraska, Lincoln
Willard J. Visek, M.D., Ph.D.University of Illinois College of Medicine
Donald M. Watkin, M.D., M.P.H.,F.A.C.P.George Washington University
Miles Weinberger, M.D.University of Iowa Hospitals and Clinics
Lynn Waishwell, Ph.D., CHESUniversity of Medicine and Dentistry ofNew Jersey
Janet S. Weiss, M.D.University of California at San-Francisco
Simon Wessley, M.D., FRCPKing’s College London and Institute ofPsychiatry
Steven D. Wexner, M.D.Cleveland Clinic Florida
Joel Elliot White, M.D., F.A.C.R.John Muir Comprehensive Cancer Center
Carol Whitlock, Ph.D., R.D.Rochester Institute of Technology
Christopher F. Wilkinson, Ph.D.Burke, VA
Mark L. Willenbring, M.D.Veterans Affairs Medical Center
Carl K. Winter, Ph.D.University of California, Davis
Lloyd D. Witter, Ph.D.University of Illinois, Urbana-Champaign
James J. Worman, Ph.D.Rochester Institute of Technology
Russell S. Worrall, O.D.University of California, Berkeley
Panayiotis M. Zavos, Ph.D., Ed.S.University of Kentucky
Steven H. Zeisel, M.D., Ph.D.The University of North Carolina
Michael B. Zemel, Ph.D.Nutrition Institute, University of Tennessee
Ekhard E. Ziegler, M.D.University of Iowaa
P U B L I C A T I O N S O R D E R F O R M
TITLE QUANTITY
BOOKSAmerica’s War on “Carcinogens”—$15.95 each __Are Children More Vulnerable to EnvironmentalChemicals?—$19.95 each __Cigarettes: What the Warning LabelDoesn’t Tell You—$19.95 each __
Qty X $19.95 = $
A Citizen’s Guide to Terrorism Preparedness andResponse—$11.95 each __
New Yorker’s Guide to Terrorism Preparedness andResponse—$11.95 each __
Qty X $11.95 = $
BOOKLETS AND SPECIAL REPORTS ($5.00 each)
A Comparison of the Health Effects of AlcoholConsumption and Tobacco Use in America __
A Summary of America’s War on “Carcinogens” __AIDS in New York City: Update 2001 __Alzheimer’s Disease: A Status Report For 2002 __Anthrax: What You Need to Know __Aspirin and Health __Biotech Pharmaceuticals and Biotherapy __Biotechnology and Food __California’s Proposition 65 and Its Impact
on Public Health __Cancer Clusters: Findings Vs. Feelings __Chemoprevention of Breast Cancer __Chemoprevention of Coronary Heart Disease __Colorectal Cancer __Dietary Fiber __Does Nature Know Best: Natural Carcinogens __Eating Safely: Avoiding Foodborne Illness __The Efficacy, Safety and Benefits of bST and pST __Endocrine Disrupters: A Scientific Perspective __Environmental Tobacco Smoke __Ethics of Accepting Money From the
Tobacco Industry __The Facts About “Dirty Bombs” __Facts About Fats __Facts About “Functional Foods” __Facts Versus Fears (fourth edition) __Fat Replacers __Feeding Baby Safely __Fluoridation __Global Climate Change and Human Health __Good Stories, Bad Science:
A Guide for Journalists to the Health Claims of“Consumer Activist” Groups __
Health and Safety Tips for Your Summer Vacation __Holiday Dinner Menu __The Irreversible Health Effects of Cigarette Smoking __Kicking Butts in the Twenty-First Century:
What Modern Science Has Learned aboutSmoking Cessation __
Making Sense of Over-the-Counter Pain Relievers __Marketing Cigarettes to Kids __Moderate Alcohol Consumption and Health __Much Ado About Milk __Nutrition Accuracy in Popular Magazines 1997–1999 __Nutrition Accuracy in Popular Magazines 1995–1996 __
TITLE QUANTITY
Of Mice and Mandates: Animal Experiments, Human Cancer Risk and Regulatory Policies __
Postmenopausal Hormone ReplacementTherapy __
Priorities in Caring for Your Children __Quackery and the Elderly __Risk Factors for Prostate Cancer:
Facts, Speculation and Myths __Risk Factors of Breast Cancer __The Role of Beef in the American Diet __The Role of Eggs in the Diet __School Buses and Diesel Fuel __The Scientific Facts About the
Dry-Cleaning Chemical Perc __Silicone-Gel Breast Implants: Health
and Regulatory Update 2000 __Smoking and Women’s Magazines __Teflon and Human Health:Do the Charges Stick?
Assessing the Safety of the Chemical PFDA __The Tobacco Industry’s Use of Nicotine as a Drug __Traces of Environmental Chemicals in the
Human Body: Are They a Risk to Health? __Vegetarianism __Vitamins and Minerals __Writing about Health Risks:
Challenges and Strategies __
Qty X $5.00 = $
SPECIAL RELEASES ($3.00 each)
A Critical Assessment of “Lies, Damned Lies,& 400,000 Smoking-Related Deaths” __
An Unhappy Anniversary:The Alar “Scare” Ten Years Later __
Analysis of Alleged Health Risk fromDBCP in Drinking Water __
Estrogen and Health: How PopularMagazines Have Dealt with HormoneReplacement Therapy __
Rumble in the Bronx: Mass Hysteria and the“Chemicalization” of Demonology __
Safe, Long-lasting Pressure-Treated Wood __Should Long-Chain Polyunsaturated Fatty
Acids Be Added to Infant Formula? __Three Mile Island: A 20th Anniversary
Remembrance __
Qty X $3.00 = $
BROCHURES ($1.00 each)
What’s the Story: The Scientific Facts About...Drug-Supplement Interaction __The Dry-Cleaning Chemical Perc __Eggs __PCB’s __The Role of Milk in Your Diet __Olestra __MMT’s __Pressure-Treated Wood __
Qty X $1.00 = $
order summary
Membership Total
Publications Total
International Postage
GRAND TOTAL
M E M B E R S H I P / P A Y M E N T
PUBLICATION Summary
Books @ $19.95Books @ $11.95Booklets and Special ReportsSpecial ReleasesBrochures
Subtotal
ACSH Member Discount
Publication Total
Membership ApplicationA financial contribution to ACSH entitles you to receive all new ACSH publications as they are released, and a25% discount on all additional ACSH publication purchases. All contributions are tax-deductible as permitted bylaw.
Yes, I want to join ACSH. I wish to donate
MAIL TO:AMERICAN COUNCIL ON SCIENCE AND HEALTH1995 Broadway • 2nd Floor • New York • NY 10023
URLs: acsh.org; HealthFactsAndFears.comOr call: (212) 362-7044 • Or fax: (212) 362-4919
Or e-mail: [email protected]
METHOD OF PAYMENT
q Check q VISA q MasterCard
Name (please print) ________________________________
Account number _______________________________________________________________________________
Expiration date ______________________________________________
Signature_____________________________________________________________________
MAILING INFORMATION
Name (please print) _________________________
Company ____________________________________
Address1 ________________________________________
Address2 ________________________________________
City/State ____________________________________________________
Zip ______________________________________________
E-mail (optional) ____________________________________
International postage and handling charges are as
follows:(Overseas orders must be prepaid in U.S. cur-
rency, or charged to Visa or Mastercard)
1–2 copies . . . . . . . . . . . . .Add $3.00 to total3–6 copies . . . . . . . . . . . . .Add $7.00 to total7–9 copies . . . . . . . . . . . .Add $12.00 to total10 or more copies . . . .Please contact ACSH
International postageFor books only:
1–2 copies . . . . . . . . . . . . .Add $8.00 to total3–6 copies . . . . . . . . . . . .Add $16.00 to total7–9 copies . . . . . . . . . . . .Add $26.00 to total10 or more copies . . . .Please contact ACSH
q Member $50–249 q Supporter $5,000–9,999
q Friend $250–999 q Sponsor $10,000–14,999
q Contributor $1,000–4,999q Patron $15,000–24,999
A
B
PUBLICATION BULK RATESCall ACSH for special discounts on Book orders
of 50 copies or more.
BOOKLETS AND SPECIAL REPORTS
q Non-Members1–499 copies . . . . . . . . . . . . . . . . . . $5.00 each500–999 copies . . . . . . . . . . . . . . . . $3.00 each1000+ copies . . . . . . . . . . . . . . . . . . $2.50 each
q ACSH Members1–499 copies . . . . . . . . . . . . . . . $3.75 per copy500 or more copies . . . .. . . . see regular bulk rates
$
$
$
$
$
(deduct 25%)—
A
B
C
C(if applicable)
$
$
$
$
$
$
q Benefactor $25,000–and up