Embed Size (px)
Citation preview

Nikhil Pai, MD CNSC FAAP FRCPC Associate Professor, Pediatric GI & Nutrition,
McMaster UniversityMedical Lead, Complex Pediatric Nutrition Service
McMaster Children’s Hospital
The Evolving Management of Pediatric
Intestinal Failure

Disclosures
Nutricia, Ferring, Takeda Takeda
ADVISORY BOARDS SPEAKER FEES

Our first talk of today’s session will focus on the management of pediatric intestinal failure (IF) patients.
Common presentations of early onset intestinal failure and principles + pearls of management.
Prognostic factors in intestinal failure patients, and key considerations for long-term monitoring.
GLP-2 AGONISTS
Early experience with the role of GLP-2 agonists in management, including evolving principles of patient selection.
MANAGEMENT
OUTCOMES
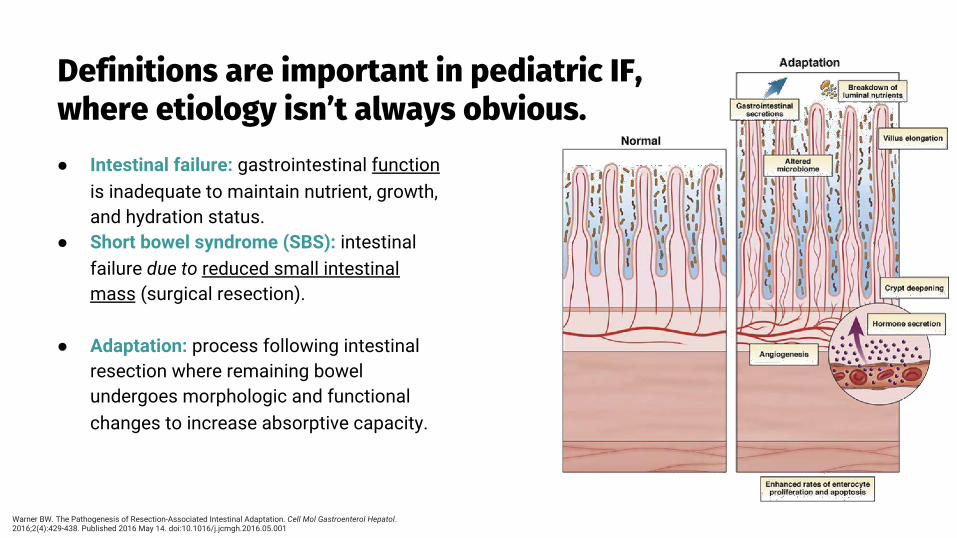
Definitions are important in pediatric IF, where etiology isn’t always obvious.● Intestinal failure: gastrointestinal function
is inadequate to maintain nutrient, growth, and hydration status.
● Short bowel syndrome (SBS): intestinal failure due to reduced small intestinal mass (surgical resection).
● Adaptation: process following intestinal resection where remaining bowel undergoes morphologic and functional changes to increase absorptive capacity.
Warner BW. The Pathogenesis of Resection-Associated Intestinal Adaptation. Cell Mol Gastroenterol Hepatol. 2016;2(4):429-438. Published 2016 May 14. doi:10.1016/j.jcmgh.2016.05.001
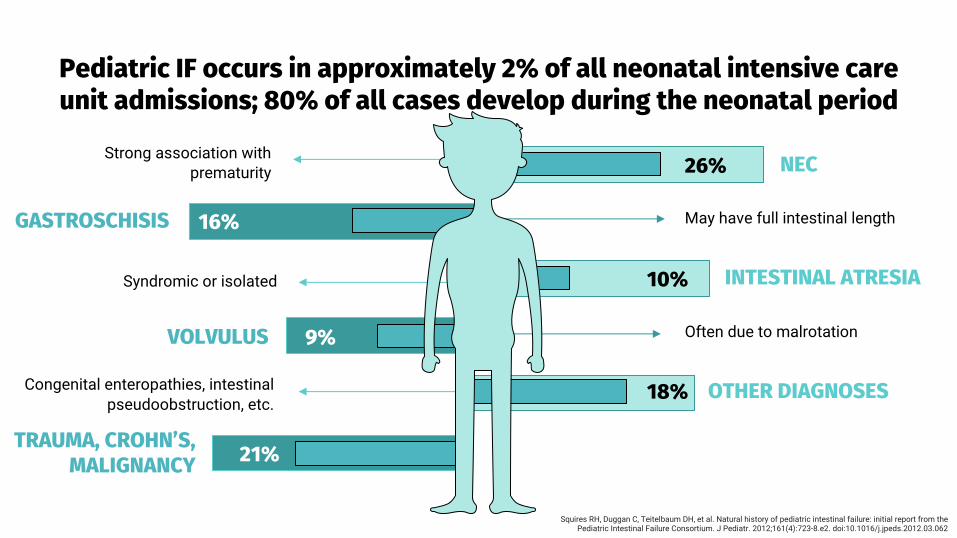
18%
Pediatric IF occurs in approximately 2% of all neonatal intensive care unit admissions; 80% of all cases develop during the neonatal period
26%
May have full intestinal length16%
10%
Congenital enteropathies, intestinal pseudoobstruction, etc.
Often due to malrotation9%
21%
NEC
GASTROSCHISIS
VOLVULUS
INTESTINAL ATRESIA
OTHER DIAGNOSES
TRAUMA, CROHN’S, MALIGNANCY
Squires RH, Duggan C, Teitelbaum DH, et al. Natural history of pediatric intestinal failure: initial report from the Pediatric Intestinal Failure Consortium. J Pediatr. 2012;161(4):723-8.e2. doi:10.1016/j.jpeds.2012.03.062
Strong association with prematurity
Syndromic or isolated

Several general principles that must be routinely addressed in all patients at each visit.
Adjusting Nutrition for
GrowthIdeal growth curves, Bolus
feeding
Prevention of PN associated liver
disease (PNALD)*Next slide
Renal Function, Metabolic Bone
Disease, Neurocognitive Development
Initiation of Enteral Feeds
Rapid advancement, oral feeding
ONE
FOUR
THREE FIVE
TWOPsychosocial,
Financial Burdens

Newer TPN lipid formulations have reduced previously high rates of PNALD / PNAC.
Historically present in 40-60% of childrenEffects of newer lipid formulations reduced phytosterols
TREATMENT: FOLE effective at treatment PNAC● (2021) n=262, 65% FOLE vs. 16% SOLE had resolution of
cholestasis (p<0.0001)
PREVENTION: MOLE may prevent PNAC● (2021) n=136, 16.4% SOLE vs. 2.5% MOLE
developed cholestasis after >2wk (p=0.007) ● (2021) n=107, 44.8% SOLE vs. 30% MOLE had
cholestasis after >2wk (RR=0.67; 95% CI: 0.39-1.15)
Gura KM, Premkumar MH, Calkins KL, Puder M. Fish Oil Emulsion Reduces Liver Injury and Liver Transplantation in Children with Intestinal Failure-Associated Liver Disease: A Multicenter Integrated Study. J Pediatr. 2021;230:46-54.e2. Jackson RL, White PZ, Zalla J. SMOFlipid vs Intralipid 20%: Effect of Mixed-Oil vs Soybean-Oil Emulsion on Parenteral Nutrition-Associated Cholestasis in the Neonatal Population. JPEN J Parenter Enteral Nutr. 2021;45(2):339-346.Ferguson CL, Perry C, Subramanian M, Gillette C, Ayers K, Welch C. Mixed Oil-Based Lipid Emulsions vs Soybean Oil-Based Lipid Emulsions on Incidence and Severity of Intestinal Failure-Associated Liver Disease in a Neonatal Intensive Care Unit. JPEN J ParenterEnteral Nutr. 2021;45(2):303-308.

Nutritional management is essential to support growth and maximize potential for early adaptation.
Occurs even when only small amounts of feeds are given (“trophic feeds”)
Absence of enteral feeding may induce atrophy of the mucosa
High rates of oral feeding aversion
NUTRIENTS IN THE INTESTINAL LUMEN MAY BE MOST EFFECTIVE IF ENTERAL FEEDS INITIATED EARLY
Maximize enteral feeding early (program-specific “schedules”)
Serial measurements of weight, length used to guide targets
REE is similar to healthy controls, +30-70% from enteral vs. PN feeding
Transition to intermittent bolus feedings: maximize adaptation, cyclical release of intestinal hormones, polymeric formula
Andorsky DJ, Lund DP, Lillehei CW, et al. Nutritional and other postoperative management of neonates with short bowel syndrome correlates with clinical outcomes. J Pediatr. 2001;139(1):27-33. Squires RH, Duggan C, Teitelbaum DH, et al. Natural history of pediatric intestinal failure: initial report from the Pediatric Intestinal Failure Consortium. J Pediatr. 2012;161(4):723-8.e2.

Nutritional management is essential to support growth and maximize potential for early adaptation.
Occurs even when only small amounts of feeds are given (“trophic feeds”)
Absence of enteral feeding may induce atrophy of the mucosa
High rates of oral feeding aversion
NUTRIENTS IN THE INTESTINAL LUMEN MAY BE MOST EFFECTIVE IF ENTERAL FEEDS INITIATED EARLY
Maximize enteral feeding early (program-specific “schedules”)
Serial measurements of weight, length used to guide targets
REE is similar to healthy controls, +30-70% from enteral vs. PN feeding
Transition to intermittent bolus feedings: maximize adaptation, cyclical release of intestinal hormones, polymeric formula
Andorsky DJ, Lund DP, Lillehei CW, et al. Nutritional and other postoperative management of neonates with short bowel syndrome correlates with clinical outcomes. J Pediatr. 2001;139(1):27-33. Squires RH, Duggan C, Teitelbaum DH, et al. Natural history of pediatric intestinal failure: initial report from the Pediatric Intestinal Failure Consortium. J Pediatr. 2012;161(4):723-8.e2.

Ongoing monitoring required for short- and long-term complications.
Neurocognitive delayD-lactic acidosis
Ostomy breakdown
Psychosocial, family burdenMental health
Deficiencies of ADEK, Fe, B12EFA deficiency
Risks highest with weaning PN
Diarrhea, dysmotility Anastomotic ulcers EsophagitisPeptic ulcer diseaseSIBO
Metabolic bone disease (Vit D, Ca)
Kidney stones (calcium oxalate), increased rate of CKD
Catheter related complications: CLABSI, thrombi, occlusion, breakage
PNALDCholelithiasis
Eosinophilic diseaseAllergic disorders

Candidates for autologous intestinal rehabilitation surgeries (AIRS) + intestinal/multivisceral transplant.
TRANSPLANT LESS COMMON (26% to 5.4%, PRE/POST 2007)
Progressive PNALD
Dilated small intestine (often with complications)
Loss of vascular access (≥3 CVC sites)
Congenital enteropathies (ie. MVID, Tufting, IED, aganglionosis, etc.)
Adequate bowel lengthening predicted
Absence of underlying gastrointestinal motility disorder
Burghardt KM, Wales PW, de Silva N, et al. Pediatric intestinal transplant listing criteria - a call for a change in the new era of intestinal failure outcomes. Am J Transplant. 2015;15(6):1674-1681. doi:10.1111/ajt.13147

Two main AIRS procedures used to increase bowel length and absorptive area: STEP, and Bianchi.
● No comparative data to support its use● Improves: feed tolerance, SIBO, bowel continuity● Indications: dilatation, >1st year, sepsis, IFALD
● STEP: Serial transverse enteroplasty procedure● Bianchi procedure/LILT: Longitudinal intestinal
lengthening and tailoring (challenges: intestinal blood flow, segments of variable dilatation)
Post-STEP anastomotic bleeding concerns:● 2014 J Ped Surg: n=23 post-STEP; 13% GIB● 2021 J Ped Surg: n=16; 1 GIB required resection● Both studies: 2.75-3.14yr followup
Kim HB, Fauza D, Garza J, Oh JT, Nurko S, Jaksic T. Serial transverse enteroplasty (STEP): a novel bowel lengthening procedure. J Pediatr Surg. 2003;38(3):425-429.Bianchi A. From the cradle to enteral autonomy: the role of autologous gastrointestinal reconstruction. Gastroenterology. 2006;130(2 Suppl 1):S138-S146. doi:10.1053/j.gastro.2005.09.070
Lemoine C, Larkin K, Brennan K, Zoller-Thompson C, Cohran V, Superina R. Repeat serial transverse enteroplasty procedure (reSTEP): Is it worth it? Journal of Pediatric Surgery, 2021. doi.org/10.1016/j.jpedsurg.2020.12.026.Fisher JG, Stamm DA, Modi BP, Duggan C, Jaksic T. Gastrointestinal bleeding as a complication of serial transverse enteroplasty. J Pediatr Surg. 2014;49(5):745-749.

GLP-2 agonists are emerging onto the Canadian pediatric market for Summer/Fall 2021.
Common presentations of early onset intestinal failure and principles + pearls of management.
Prognostic factors in intestinal failure patients, and key considerations for long-term monitoring.
GLP-2 AGONISTS
Early experience with the role of GLP-2 agonists in management, including evolving principles of patient selection.
MANAGEMENT
OUTCOMES

Role of GLP-2 Agonists in the Pathophysiology of Intestinal Failure.
SITE
TRANSIT
ENTEROCYTES
APPROVE
GLP-2 synthesized in enteroendocrine L cells
Slows intestinal transit time, increases small intestinal nutrient absorption
Administration significantly increases
villous height + SB mass
Approved for use in Canadian adults with
intestinal failure since 2019, and children in
USA/Europe since 2017

Real-world data shows promise in pediatrics.
• 12-month data• Multicentre (N=8) prospective,
observational cohort• N=17 (1-18yo)
• Average SB remnant 52cmAverage PN 55mL/kg/day
• No change in PN, surgery x 3mo• Outcome: >20% PN decrease
Ramos Boluda E, et al (Spain); JPGN Dec, 2020
Ramos Boluda, E et al. Experience With Teduglutide in Pediatric Short Bowel Syndrome: First Real-life Data, JPGN: December 2020 - Volume 71 - Issue 6 - p 734-739.

Ongoing French trial shows smaller benefits (REVE Study).
• Oral abstract (CIRTA 2019)• N=12, 5-16 years old• Average SB remnant <80 cm
Goulet et al (France); Transplant (July 2019)
Lambe, Cecile, Goulet, Olivier et al. The REVE study, preliminary results. A Monocentric Single-arm study to characterize the long-term safety, efficacy, and pharmacodynamic of GLP-2 analog (Revestive®) in the management of short bowel syndrome pediatric patients on home-
parenteral nutrition (HPN), Transplantation: July 2019 - Volume 103 - Issue 7S2 - p S11
3mo: 9/12 children, 30% PN reduction 6mo: 3/12 children, 44% PN reduction• High drop-out rate• Study is ongoing, projected
enrolment n =25

McMaster Children’s Hospital’s Intestinal Failure Team First Experience with Teduglutide.
01.
02.03.
04.
32 CLABSI episodesSeptic hip, Right atrial clotNo CVL access
SUMMER, 2020
Loss of central accessMildly elevated liver enzymes
MULTIVISCERAL TRANSPLANT LIST2 weeks = -15%, +2kg
6 weeks = -1 day PN, +2kgOctober PICC comes out: PN discontinued altogether
GLP-2 AUG, 2020
8 months laterStools 2-3 per day (Bristol 4) , intake 3000mL/day Weight 25.4kg à 30.4kgFirst bath, sleepover, formed bowel movement
APRIL, 2021 (TPN STOPPED)
12yo boy with gastroschisis, 26cm SB, TPN 7d/week2x STEP proceduresLiquid stools (5x/day, Bristol 7)Attempts to wean PN: weight loss, loperamide maximized, multiple formula changes

Key questions remain regarding patient selection for use of GLP-2 Agonists in Canadian patients.
BALANCING FACTORS
Many unanswered questions remain:- QOL- Transplant-free survival- CLABSI rates- Cost benefit analyses
LONG-TERM DATA
$300,000 per year of treatment (estimates).Data suggests return to baseline with discontinuation of treatment.
COST
Patients with loss of functional L-cell mass.
Patient vs. provider goals.
SELECTION
*Emerging dataEARLY VS. LATE INITIATION

Early vs. late use of GLP-2 agonists: is there a role for earlier initiation of therapy?
2020 JPEN: Neonatal short‐bowel piglets assigned to 7d teduglutide treatment vs saline● Hyperplasia: Villus hyperplasia occurred at
Day 7 (p=0.003), not durable after 7 days of treatment cessation (p=0.081)
● Length: Length increased at Day 7 (p=0.005), maintained at day 14 (p=<0.001)
Benefit of “spiking” existing L-cell GLP-2 secretion vs waiting for failure to progressGreatest intestinal adaptation in first 1-4yrs?
Intestinal growth may be a lasting outcome of treatment with long-acting GLP-2 analogues
Hinchliffe T, Pauline ML, Wizzard PR, Nation PN, Brubaker P, Campbell JR, Kim Y, Dimitriadou V, Wales PW, Turner JM. Durability of Linear Small-Intestinal Growth Following Treatment Discontinuation of Long-Acting Glucagon-Like Peptide 2 (GLP-2) Analogues. JPEN J Parenter Enteral Nutr. 2020 Nov 25. doi: 10.1002/jpen.2053. Epub ahead of print. PMID: 33241564.

Transitioning the pediatric patient to the adult world: Predictions and prognosis for the future.
Common presentations of early onset intestinal failure and principles + pearls of management.
Prognostic factors in intestinal failure patients, and key considerations for long-term monitoring.
GLP-2 AGONISTS
Early experience with the role of GLP-2 agonists in management, including evolving principles of patient selection.
MANAGEMENT
OUTCOMES

Longterm statistics suggest sepsis rate is the primary modifiable factor associated with mortality.
2019 Am J Clin Nut: Meta-analysis weighted by follow-up duration.
175 cohorts (9,318 patients; 34,549 years)Mortality 5.2%/yr (95% CI: 4.3, 6.0)● Sepsis● IFALD
Sepsis rate predictive of IFALDEnteral autonomy associated with SB length
Sepsis rate associated with mortality and liver failure
Enteral autonomy correlates with small-bowel length
Aureliane Chantal Stania Pierret, James Thomas Wilkinson, Matthias Zilbauer, Jake Peter Mann, Clinical outcomes in pediatric intestinal failure: a meta-analysis and meta-regression, The American Journal of Clinical Nutrition, Volume 110, Issue 2, August 2019, Pages 430–436.
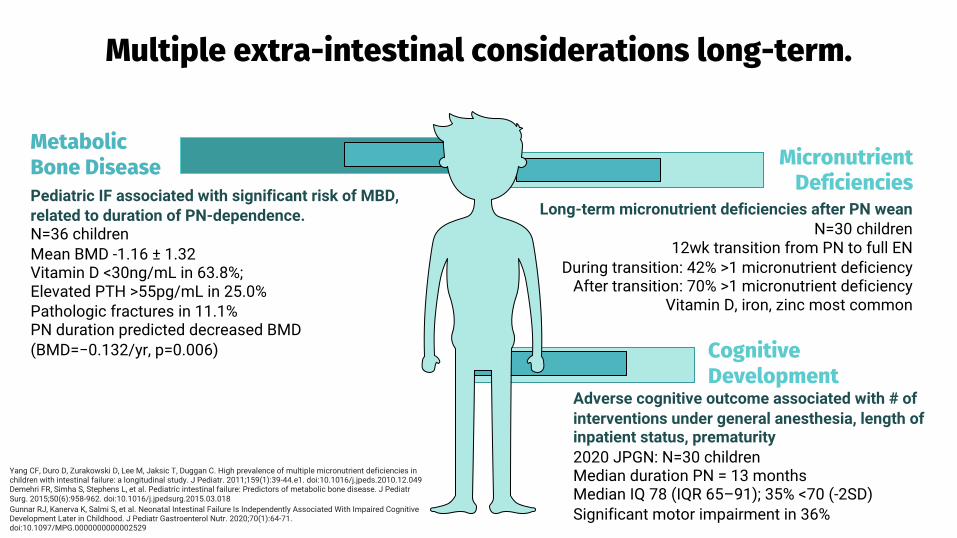
Multiple extra-intestinal considerations long-term.
85%
Micronutrient Deficiencies
Metabolic Bone Disease
Cognitive Development
Long-term micronutrient deficiencies after PN weanN=30 children
12wk transition from PN to full ENDuring transition: 42% >1 micronutrient deficiency
After transition: 70% >1 micronutrient deficiencyVitamin D, iron, zinc most common
Yang CF, Duro D, Zurakowski D, Lee M, Jaksic T, Duggan C. High prevalence of multiple micronutrient deficiencies in children with intestinal failure: a longitudinal study. J Pediatr. 2011;159(1):39-44.e1. doi:10.1016/j.jpeds.2010.12.049Demehri FR, Simha S, Stephens L, et al. Pediatric intestinal failure: Predictors of metabolic bone disease. J PediatrSurg. 2015;50(6):958-962. doi:10.1016/j.jpedsurg.2015.03.018Gunnar RJ, Kanerva K, Salmi S, et al. Neonatal Intestinal Failure Is Independently Associated With Impaired Cognitive Development Later in Childhood. J Pediatr Gastroenterol Nutr. 2020;70(1):64-71. doi:10.1097/MPG.0000000000002529
Pediatric IF associated with significant risk of MBD, related to duration of PN-dependence.N=36 childrenMean BMD -1.16 ± 1.32Vitamin D <30ng/mL in 63.8%; Elevated PTH >55pg/mL in 25.0% Pathologic fractures in 11.1% PN duration predicted decreased BMD (BMD=−0.132/yr, p=0.006)
Adverse cognitive outcome associated with # of interventions under general anesthesia, length of inpatient status, prematurity2020 JPGN: N=30 childrenMedian duration PN = 13 monthsMedian IQ 78 (IQR 65–91); 35% <70 (-2SD)Significant motor impairment in 36%

85%
Stunting
Anastomotic Ulcers
Renal Disease
Frequently develop at resection, anastomosisRisk factors: tissue perfusion, IBD-like syndrome, hyperacidity, AIRS procedures all risk factors2018 J Ped Surg: 8/114 children with SBS had AU- 6/114 had AU persistence after medical Rx- 3/114 required surgical revision
Weaning from PN associated with stunting2018 JPGN: N=52, median followup 3.4 yearsBaseline Height for Age -0.96 SDCatch-up growth achieved during PNHeight for Age decreased after weaning PN (P=0.0001) Lean body mass -1.21 SD
Reduces calcium binding to oxalate, high rate of kidney stones in patientsHyperoxaluria secondary to fat malabsorptionBinding of calcium to free fatty acids in intestine
Fusaro F, Tambucci R, Romeo E, et al. Anastomotic ulcers in short bowel syndrome: New suggestions from a multidisciplinary approach. J Pediatr Surg. 2018;53(3):483-488. doi:10.1016/j.jpedsurg.2017.05.030Neelis E, Olieman J, Rizopoulos D, et al. Growth, Body Composition, and Micronutrient Abnormalities During and After Weaning Off Home Parenteral Nutrition. J Pediatr Gastroenterol Nutr. 2018;67(5):e95-e100. doi:10.1097/MPG.0000000000002090
Multiple extra-intestinal considerations long-term.

Enteral autonomy is contingent upon enteral anatomy: length of retained ileal segment most associated with early adaptation.
Enteral autonomy attributed to residual intestinal length: 96% >50cm vs. 38% <50cm
Preservation of IC Valve, ileum
Underlying diagnosis of NEC (not: gastroschisis, atresias, dysmotility syndromes)
Multidisciplinary intestinal failure team support (rehabilitation vs. transplant)
Patient age
Fallon EM, Mitchell PD, Nehra D, et al. Neonates With Short Bowel Syndrome: An Optimistic Future for Parenteral Nutrition Independence. JAMA Surg. 2014;149(7):663–670. doi:10.1001/jamasurg.2013.4332Pakarinen MP, Koivusalo AI, Rintala RJ. Outcomes of intestinal failure--a comparison between children with short bowel and dysmotile intestine. J Pediatr Surg. 2009;44(11):2139-2144. doi:10.1016/j.jpedsurg.2009.05.002

Enteral autonomy is contingent upon enteral anatomy: length of retained ileal segment most associated with early adaptation.
Enteral autonomy attributed to residual intestinal length: 96% >50cm vs. 38% <50cm
Preservation of IC Valve, ileum
Underlying diagnosis of NEC (not: gastroschisis, atresias, dysmotility syndromes)
Multidisciplinary intestinal failure team support (rehabilitation vs. transplant)
Patient age
Fallon EM, Mitchell PD, Nehra D, et al. Neonates With Short Bowel Syndrome: An Optimistic Future for Parenteral Nutrition Independence. JAMA Surg. 2014;149(7):663–670. doi:10.1001/jamasurg.2013.4332Pakarinen MP, Koivusalo AI, Rintala RJ. Outcomes of intestinal failure--a comparison between children with short bowel and dysmotile intestine. J Pediatr Surg. 2009;44(11):2139-2144. doi:10.1016/j.jpedsurg.2009.05.002

Prevention of central line complications has impact on enteral autonomy, preventing PNALD and need for intestinal transplant.Chronic ethanol lock therapy: 70% indwelling ethanol; impacts of national shortages à 4% EDTA solutionChronic antibiotic lock therapy: concerns about antibiotic resistanceInstillation of thrombolytic agents to restore patency in occlusion
Central line associated blood stream infections- shorter SB length- lower citrulline level- SIBO (OR 7.0; p=0.009)
Central line breakage, occlusion
Thrombosis
Rahhal R, Abu-El-Haija MA, Fei L, et al. Systematic Review and Meta-Analysis of the Utilization of Ethanol Locks in Pediatric Patients With Intestinal Failure. JPEN J Parenter Enteral Nutr. 2018;42(4):690-701. doi:10.1177/0148607117722753Venturini E, Montagnani C, Benni A, et al. Central-line associated bloodstream infections in a tertiary care children's University hospital: a prospective study. BMC Infect Dis. 2016;16(1):725. Published 2016 Dec 1. doi:10.1186/s12879-016-2061-6
Cole CR, Frem JC, Schmotzer B, et al. The rate of bloodstream infection is high in infants with short bowel syndrome: relationship with small bowel bacterial overgrowth, enteral feeding, and inflammatory and immune responses. J Pediatr. 2010;156(6):941-947.e1.

Intestinal failure is a team sport.
McMaster Children’s Hospital Intestinal Failure Team:Nikhil Pai, MD | Rose-Frances Clause, NP | Heather Mileski, RD |
Jillian Owens, RD | Susan Turner, SW | McMaster Adult Gastroenterology & Nutrition Service

Extra Slides

Additional GLP-2 study data.
Kocoshis et al. JPEN (2019) Safety and Efficacy of Teduglutide: 24wk Phase III Study
Kocoshis SA, Merritt RJ, Hill S, et al. Safety and efficacy of teduglutide in pediatric patients with intestinal failure due to short bowel syndrome: a 24-week, phase III study. JPEN J Parenter Enteral Nutr 2019;44:621-31.
Prospective dosing study, n=42 pediatric patients Week 12 response (0.05 mg/kg/day): 25% reduction in PN volume52% reduction in PN kcal/kg/day
3 patients PN independence at 0.05mg/kg/d dose1 patient PN independence at 0.025mg/kg/d dose
Carter et al (2017); J Pediatr12-Week, Open-Label Pediatric Trial of Teduglutide
Prospective PHASE III trial, n=59 childrenWeek 24 response (0.05 mg/kg/day): 69.2% reduction in >20% PN volume
3 (11.5%) = PN independence (0.05mg/kg/d)2 (8.3%) = PN independence (0.025mg/kg/d)
Carter BA, Cohran VC, Cole CR, et al. Outcomes from a 12-week, open- label, multicenter clinical trial of teduglutide in pediatric short bowel syndrome. J Pediatr 2017;181:102.e5 – 11.e5.

Pictorial View of Manifestations in Intestinal Failure
patients
Duggan CP, Jaksic T. Pediatric Intestinal Failure. N Engl J Med. 2017;377(7):666-675. doi:10.1056/NEJMra1602650




![[PPT]OBSTRUCCION INTESTINAL - semio2013 | This … · Web viewOBSTRUCCION INTESTINAL OBSTRUCCION INTESTINAL OBSTACULO AL TRANSITO DEL CONTENIDO INTESTINAL Adinámico o paralítico](https://img.pdfslide.us/doc/110x75/5b36ceb57f8b9a4a728b5103/pptobstruccion-intestinal-semio2013-this-web-viewobstruccion-intestinal.jpg)