Embed Size (px)
Citation preview
KNOWLEDGE HUBS FOR HEALTHStrengthening health systems through evidence in Asia and the Pacific
The Nossal Institute for Global Health
www.ni.unimelb.edu.au
HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
WORKING PAPER SERIES NUMBER 6 | MAY 2010
The Evolution of Primary Heath Care in Fiji: Past, Present and Future
Joel NeginSydney School of Public Health and Menzies Centre for Health Policy, University of Sydney, Australia.
Graham RobertsFiji School of Medicine.
Dharam LingamFiji School of Medicine.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
ABOUT THIS SERIES This Working Paper is produced by the Nossal Institute for Global Health at the University of Melbourne, Australia.
The Australian Agency for International Development (AusAID) has established four Knowledge Hubs for health, each addressing different dimensions of the health system: Health Policy and Health Finance; Health Information Systems; Human Resources for Health; and Women’s and Children’s Health.
Based at the Nossal Institute, the Health Policy and Health Finance Knowledge Hub aims to support regional, national and international partners to develop effective evidence-informed policy making, particularly in the field of health finance and health systems.
The Working Paper series is not a peer-reviewed journal; papers in this series are works-in-progress. The aim is to stimulate discussion and comment among policy makers and researchers.
The Nossal Institute invites and encourages feedback. We would like to hear both where corrections are needed to published papers and where additional work would be useful. We also would like to hear suggestions for new papers or the investigation of any topics that health planners or policy makers would find helpful. To provide comment or get further information about the Working Paper series please contact; [email protected] with “Working Papers” as the subject.
For updated Working Papers, the title page includes the date of the latest revision.
The Evolution of Primary Health care in Fiji: Past, present and Future
First draft – April 2010 Corresponding author: Joel Negin Address: Sydney School of Public Health and Menzies Centre for Health Policy, University of Sydney, [email protected]
Other Contributors: Graham Roberts, Fiji School of Medicine and Dharam Lingam, Fiji School of Medicine.
This Working Paper represents the views of its author/s and does not represent any official position of The University of Melbourne, AusAID or the Australian Government.
ACKNOWLEDGEMENTS The authors would like to acknowledge the assistance and guidance of Josaia Samuela of the Fijian Ministry of Health and of Alvaro Alonso-Garbayo of the World Health Organization throughout the research and drafting. Erica Mayer provided excellent research support and Anne Marie Thow assisted in the development of the health policy analysis framework. The authors would also like to thank the various interviewees for their time and candour in contributing to the research.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future i
ABSTRACT Health policy development is under-analysed globally and in the Pacific region. Understanding how health policies develop and evolve is a first step towards improving the quality and appropriateness of those policies. Through a document review and key informant interviews, this study examines the evolution of the concept of primary health care in Fiji from 1975 to 2009, focusing on priority-setting, funding, implementation, political economy, the cultural context and interactions between communities, government and donors. Lessons from more than 30 years of experience with community health are highlighted, revealing high levels of contestation over health policy. The study identifies factors for inclusion in any renewed primary health care intervention and calls for greater government ownership of priority setting, more clarity on the links between policy and funding, greater awareness by development partners of the risks of imposing policy and a deeper analysis of political economy and culture in relation to health policies.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
ii The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 1
INTRODUCTION AND METHODSPurpose of the Case StudyThe overarching objective of the research is to understand better the evolution of primary health care in Fiji and, through it, the policy process in the Pacific. Carden (2009) asserts that in order to ‘maximize the influence of development research on public policy and action, the best first step is to assess how that policy is actually made’. Despite its importance, health policy analysis remains neglected, under-researched and under-funded (Gilson and Raphaely 2008). This is particularly true for the Pacific: while many agencies focus on influencing development, there has been a paucity of analysis of regional health policy and the development of national strategic and operational plans.
A 2008 review of global literature, which identified 391 health policy analysis articles concerning low and middle income countries over a 13-year period, noted that none focused on the Pacific (Gilson and Raphaely 2008). Globally, evidence-based policy making is becoming more complex. The World Health Organization (WHO 2006) highlights the strength of development partners, asserting: ‘[N]ot only do these partners have the power to fund, or not to fund, given projects, they also have the power to influence, if not control, policy-making agendas’. Reich and Takemi (2009) note: ‘[P]olicy making in global health has become a multistakeholder process … with competition and confusion both globally and nationally’. The fact that the Pacific is the most heavily aid-assisted part of the world per capita only adds to the challenge and importance of health policy analysis (AusAID 2009).
A recent overview of the health sector in Fiji cited the ‘need for [a] stronger evidence based approach to policy and planning’ (Sutton, Roberts et al 2008). This study investigates the evolution of primary health care in Fiji from 1975 to the present. It aims to understand how health policies develop over time, noting how various actors influence policy and the dynamics between national and international stakeholders. The purpose is:
• ToinformpolicyactorsinFijiandtheregiononthepolicydevelopmentprocess;
• ToinformcurrentdebatesinFijionthedirectionofprimaryhealthcarepolicy.
MethodsThe case study was conducted through a thorough document review, including bilateral and multilateral agency reports and Ministry of Health documents, a review of the published literature and semi-structured key informant interviews.
Empirical data were gathered through historical documents and reports. A search of the PubMed literature database using search terms including ‘Pacific and islands and primary health care’ and ‘Fiji and primary health care’ revealed a limited number of peer-reviewed articles, demonstrating the relative lack of published analysis of primary health care in the region. To complement the literature review, the research included telephone and in-person interviews with representatives of government agencies, multilateral organisations, donor agencies, academic institutions and experienced health consultants to the region. Interviews of approximately one hour each were conducted using a semi-structured questionnaire. In total, 14 interviews were conducted, including 10 with national actors and four with representatives of bilateral or multilateral agencies. The focus was how the interviewees perceived changes to primary health care over time, emphasising influences, language and social construction of ideas. Ethics approval was received through the University of Sydney.
The study used Walt and Gilson’s (1994) health policy analysis triangle to structure the interviews and analysis and particularly focused on decision-making processes and relationships between key actors. However, the Walt and Gilson framework does not sufficiently capture some of what Pollard (2008) calls the Pacific’s ‘below the iceberg’ factors, including: beliefs, culture and values; power, authority and politics; organizational culture and norms of behaviour; and social patterns and relationships. Therefore, in looking to develop a framework for health policy analysis for the Pacific, we have sought to integrate key themes from other frameworks, including Howlett and Ramesh’s (2003) policy cycle, Bowen and Zwi’s (2005) policy and practice pathway and cultural and contextual issues specific to the Pacific (Capstick, Norris et al 2009). Based on these themes and global, regional, local and national influences in the region, a health policy analysis framework was adapted from that of Walt and Gilson (1994). Figure 1 illustrates the framework. During analysis, information was organised

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
2 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
Figure 1. Health Policy Analysis Framework
in each component of the framework and at the various geographic levels before movement between levels or interaction between components was assessed. While the framework does not clarify all possible policy interactions, it serves as an initial tool for conceptualising policy components and interactions.
Such qualitative research has its limitations. The limited number of interviews, covering more than 30 years of history in Fiji, is insufficient to grasp the full complexity of the evolution of primary health care. A number of the key actors in the 1970s and early 1980s are no longer in Fiji or no longer living. Additionally, those willing to be interviewed were more likely to be interested in the topic generally, thus representing some level of bias. Lastly, there is certainly a sense of nostalgia—some interviewees recalled the ‘good old days’—and their recollections of health policy development might not represent the full spectrum of issues of the time. These limitations have been taken into account as much as possible in the analysis.
The Global ContextPrimary health care (PHC) has been a central concept in global health for more than 30 years, since its inception at Alma-Ata in 1978, although the implementation of PHC principles has varied. Over the past two years, however, there has been a renewed interest in PHC, as evidenced by the 2008 World Health Report, ‘Primary Health Care: Now More Than Ever’ (WHO 2008), and the prominent Lancet series on PHC (A renaissance in primary health care 2008; WHO 2008; Lawn, Rohde et al 2008; Lewin, Lavis et al 2008; Rosato, Laverach et al 2008; Rohde, Cousens et al 2008).
Margaret Chan, Director-General of the WHO, has noted with regard to Alma-Ata that there is much that can be ‘gleaned from the experiences of a movement that failed to reach its goal’ (Chan 2008). This is particularly relevant for the Pacific, where, perhaps more than most regions of the world, some countries implemented PHC and realised real benefits (WHO 2001; Jacobs 2002) – some of which were subsequently lost. Recording the lessons from the PHC experience in the Pacific can therefore support policy making in the region.
The International Conference on Primary Health Care was held in September 1978 at Alma-Ata in the then USSR. The conference, jointly sponsored by the WHO and UNICEF, was attended by 600 representatives of 150 WHO member states. The attendees rejected the inequalities in health care of the time as ‘politically, socially and economically unacceptable’ and proposed comprehensive primary health care as the fundamental means for improving health (WHO 1978).
GLOBAL
REGIONAL
LOCALCONTEXT &
CULTUREEVIDENCE & PRIORITIES
ACTORS & CAPACITY

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 3
The Alma-Ata Declaration defined primary health care as ‘the first level of contact of individuals, the family and community with the national health system bringing health care as close as possible to where people live and work, and [it] constitutes the first element of a continuing health care process’ (WHO 1978). The Declaration affirmed health as a fundamental human right and strongly linked it to national development. Importantly, ‘a central tenet of the Alma-Ata Declaration [was] that progress in health [would] depend on many factors—i.e., economics, education, nutrition, health system and culture—and [would be] closely linked to governance, social justice and changes in other sectors’ (Rohde, Cousens et al 2008).
In essence, the Alma-Ata Declaration expanded the scope of health care by presenting ‘health not merely as a result of biomedical interventions but also an outcome of social determinants’ (Lawn, Rohde et al 2008). For the first time, prevention was equally as important as cure and ‘there was a shift in attitude from a focus on ill health and hospitals, to a focus on communities and families controlling their own health, putting the “public” into public health’ (Lawn, Rohde et al 2008). The Declaration emphasised greater equity in access to care, community ownership and efficiency in service delivery. There was consensus on the need for a ‘country-by-country approach’ based on ‘sound epidemiological analysis’ that would be ‘relevant to [each] country’s state of development’ (High Hopes at Alma-Ata, 1978). All of this was intended to lead to the ultimate goal of ‘health for all’ by the year 2000.
Alma-Ata emphasised community-focused health, calling for a system that ‘addresses the main health problems in the community, providing promotive, preventive, curative and rehabilitative services accordingly’ and initiatives that require and promote ‘community and individual self-reliance and participation in the planning, organisation, operation and control of primary health care’ (WHO 1978).
The necessary components of PHC as defined by the Declaration included education concerning prevailing health problems and the methods of preventing and controlling them; promotion of food supply and proper nutrition; an adequate supply of safe water and basic sanitation; maternal and child health care, including family planning; immunisation against the major infectious diseases; prevention and control of locally endemic diseases; appropriate treatment of common diseases and injuries; and provision of essential drugs (WHO 1978).
Some, however, saw this approach as ‘overly ambitious, unrealistic and unattainable’ (Brown, Cueto et al 2006). The move to ‘selective’ PHC and then the implementation of structural adjustment policies in many developing countries—accompanied by budget cuts and reduced social spending—meant that the original conception of PHC was, in the main, not fully implemented. Some outstanding local health development programs did demonstrate that a strong commitment to PHC principles could decrease deaths and reduce chronic disease morbidity, in both government and non-government settings with examples in South and Central America (Perry, Shanklin and Schroeder 2003), South Asia (Arole and Arole 1994), and South-East Asia (Perks, Toole and Phouthonsy 2006). These were, however, rarely scaled-up to a national level, with some exceptions such as Thailand (Rohde, Cousens et al 2008).
Nonetheless, the idea has remained alive and there is now a return, in different forms, to the Alma-Ata principles. In 2002, the Western Pacific Regional Office of WHO made a significant evaluation of the experience of national health programs’ (including Fiji) of 25 years of PHC, finding success in a limited number of areas (Jacobs 2002). The former director-general of WHO, Lee Jong Wook, used this and other regional evidence to promote the vision of a ‘health-care system based on primary health care’ (Lee 2003), leading later to the stronger declaration of Primary Health Care: Now More Than Ever (WHO 2008). In 2009, the American Public Health Association’s working group on community based primary health care systematically reviewed health delivery mechanisms underpinning PHC’s success in promoting child survival. This made a strong case for community-oriented interventions such as home visits by health motivators, group meetings for education and support, outreach services and community-based care of high priority diseases (Freeman, Perry et al 2009). An examination of the history of PHC in Fiji helps to locate it in these global movements and also determine how PHC principles and mechanisms can best inform future health policy in Fiji and similar settings.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
4 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
THE ORIGINS OF PHC IN FIJI As the global community declared its ambitious health goals at Alma-Ata in landlocked mountainous Kazakhstan, the newly independent Pacific island nation of Fiji was responding to its own health challenges, already beginning to practise much of what the Alma-Ata Declaration proposed. Interviews with key informants for this paper reveal a commitment among Fiji health planners to many of the principles of the Declaration.
‘PHC Has Always Been Here’During interviews, now retired Ministry of Health (MOH) officials described a newly emerging health system in the 1960s that showed features similar to some central PHC components.
One interviewee described his work starting in 1962 in the interior of Vanua Levu, Fiji’s second largest island, where, as a medical officer (MO), he conducted outreach, often on horseback, to remote villages to discuss hygiene and health issues with the community and even to set up a de facto village dispensary by training the headman’s wife and giving her some basic medication to treat minor ailments. While these activities were not dictated by MOH directives, the interviewee—who noted that many others provided these types of services too—‘just did these things based on intuition’, responding to a need to reach dispersed populations in more than 130 inhabited islands.
Similarly, in interviews, nurses who were working at that time confirmed they were doing outreach, holding village clinics and training traditional birth attendants and traditional medicine practitioners. From the early 1970s, they were working with communities because domiciliary visits and demographic information collection were part of the position description along with their responsibilities at their posts. They would visit every home in their catchment area, discuss health issues with community members and come up with collaborative ways of overcoming challenges, such as protecting water sources or building latrines.
One interviewee who worked in remote areas in the 1970s said, ‘We started PHC even before Alma-Ata’. Most doctors, after their internships, served in rural health centres and nursing stations—which were built throughout the country in villages of more than 200 people—providing services close to where people lived (Sutton, Roberts et al 2008). These nursing stations provided family planning information and services, maternal and child health services, first-aid and health education and also conducted outreach. Fiji’s communitarian culture facilitated a high degree of community engagement and participation. Indigenous Fijians place a great deal of emphasis on village life and the hierarchy of chiefs and traditional clan roles. Doctors and nurses active at that time stated that they were able to work within this community culture, building partnerships with chiefs, to ensure that communities took an active role in their own health status.
Following Alma-AtaBased on the research interviews, however, it is unclear how widespread these positive PHC experiences were in the pre-Alma-Ata phase. Reports of the outreach work by doctors and nurses might be biased by both memory and the selection of interviewees. Despite these caveats, there was a consensus that at least some elements of PHC did exist in Fiji before 1976 even if they were not institutionalised, funded or formalised.
In 1976, even before the conference at Alma-Ata, the World Health Organization held a regional meeting on PHC to introduce the concept. The government of Fiji followed in 1977 with the First National Conference on Primary Health Care (Asuzu, Ram et al 2004), and in the same year the WHO started providing substantial funding for PHC in Fiji. Interviewees who were then working in the health system remember hearing about PHC for the first time during that year. One interviewee noted that she first heard of PHC in 1978, as a doctor in a rural health centre, noting that doctors were already doing much of what the MOH was pushing them to do.
In 1986, the development of primary health care in the South Pacific region was assessed by the World Health Organization and the United Nations Development Programme (WHO and UNDP 1986). PHC has variously been understood as an overarching health system philosophy (based on attaining health for all), as a level of care (first point of contact with the health system) and as a health systems approach emphasising a horizontal manner of facing challenges (Lawn, Rohde et al 2008).

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 5
Meanwhile, the emphasis on PHC was less as a ‘how to’ manual than as a philosophy of holistic health (Lawn, Rohde et al 2008). As a result, Fiji had to adapt the concepts to suit its system and health challenges and chose to pursue a ‘village-based approach to primary health care’ in line with its existing rural health program (WHO 2008). The 1978 MOH Annual Report described PHC as a concept that was being tested (Asuzu, Ram et al 2004).
Even with an existing health system structure that incorporated a number of PHC concepts, a ‘major reorganisation of the administrative structure was made to the health system in the build up to and the period immediately after Alma-Ata. At the national level, a new division of Primary and Preventive Health was set up with all community based health institutions placed under its jurisdiction’ (Waqatakirewa 2001). According to interviewees, the Fijian version of PHC was embraced quickly by health workers. With WHO funding provided to divisional and subdivisional health teams, the new approach became more formalised.
With significant funding, Fiji implemented a broad-based PHC approach after 1978, highlighting a few pillars: expanded access to health services, community engagement, environmental health, multi-sectoral engagement, establishment of village health committees and village health workers. Subdivisional health workers started organising more community workshops as part of a more explicit aim to get community members to see health as their own responsibility. In a 2001 review of PHC in Fiji, Lepani Waqatakirewa (2001) reflected on the years after 1979 and noted that the conduct of subdivision and community workshops was the most memorable activity following the introduction of the PHC concept, when there was more integration of the various programme areas in one sitting.
The major achievement made possible by the WHO funding was the marketing of the Alma-Ata Declaration and community awareness building regarding health. For example, water and sanitation were an area of major concern because of water-borne diseases, so communities were advised and assisted to focus on the construction and maintenance of water and sanitation resources.
However, some components of the emerging PHC concept were new to Fiji. Under the new model, the health sector subdivisions collaborated with representatives of other ministries, including Agriculture, Education and Lands. One interviewee lauded this ‘huge and rich multi-sectoral approach’ as one of the defining elements of PHC, although other interviewees cast doubt on whether this rhetoric was ever achieved, noting that separate budgetary provisions remained during this era and still do.
Another major component of Fijian PHC was the training of community health workers (CHW) in mixed Indo-Fijian communities and village health workers (VHW) in every Fijian village. 1 Communities nominated a local member who would become the CHW/VHW, and that individual would be trained by the MOH through an intensive six-week program followed by organised in-service training (MOH 1994). The MOH would provide equipment and drugs, the community would provide a working location (sometimes building a CHW/VHW dispensary from scratch) and, in many cases, the community committed to supporting the CHW/VHW either with cash or with in-kind contributions such as planting or fishing for them. The CHW/VHW was the first contact point for community members and provided basic drugs and treatments. The CHW/VHW—mostly women—referred patients to nursing stations and reported to the area nurse. Interviewees affirmed that the CHW/VHW were ‘the backbone of PHC, the interface between health and the community’.
Interviewees highlighted the strong community culture at that time, there being an influential village headman in Fijian communities and strong Advisory Committees in Indo-Fijian communities, facilitating PHC implementation. Planting, cultivation and fishing were seen as communal activities, and neighbours supported one another. However, interviewees noted that it was far more difficult to implement PHC in the heterogeneous Indo-Fijian communities than in the homogeneous Fijian villages, where community action was more likely.
PHC was a defining element of the Fijian health system for many of the nurses and doctors who entered the system in those years, and who are now senior officials in the MOH. One noted that ‘PHC was part of our training’ and another that ‘we came into the ministry at a time when we heard lots about PHC’. During this time,
1 In the literature of Fiji’s primary health care initiatives, the terms village health workers and community health workers are used interchangeably. CHW generally refers to those who worked in Indo-Fijian or mixed communities and VHW to those from ethnic Fijian villages. This report uses the term CHW/VHW predominantly unless one or the other term is explicitly used in a quotation or document.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
6 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
PHC became entrenched in educational facilities. The Fiji School of Nursing established a compulsory three-month rural attachment for medical students, and the Fiji School of Medicine introduced the Primary Care Practitioners (PCP) program (Waqatakirewa 2001).
The government, with cabinet approval, strongly endorsed the PCP program and appointed Dr Timoci Bavadra of the MOH to direct it. Interviewees suggested that Dr Bavadra’s leadership of the PCP program contributed significantly to his popularity as a champion of the people, contributing to his eventual election as Prime Minister and highlighting the widespread appeal of PHC values in Fiji.
Challenges and Successes in PHC ImplementationAlong with a generally positive experience in the early days of PHC, a number of challenges arose. One nurse said, ‘PHC is doing seminars in villages’, suggesting how shallow the absorption of key PHC concepts was among some health workers. Many interviewees suggested that the implementation of PHC had been largely top-down, but also thought this may have been appropriate because, at the time, there was very low awareness and understanding of health issues in rural Fijian communities.
This top-down approach, in which health professionals took the main role, meant that PHC was successful mostly where the subdivisional medical officer pushed it. Tembon (1988) identified that the ‘training of CHWs depends on the enthusiasm and energy of the medical officer (MO) of that area’. While one MO stated, ‘At the time, I would eat and sleep PHC’, one might expect that this level of commitment was not true of all doctors and nurses working in rural areas.
Another interviewee noted that while implementation of PHC was successful, it ‘required a lot of sacrifice from the health workers’ of time conducting outreach and working with communities. The personal commitment needed to push PHC forward was perhaps unsustainable on a wide scale without continued external funding. A similar sustainability challenge existed with CHW/VHWs. Although most agreed that the trained CHW/VHWs did a good job, some volunteer CHW/VHWs were not supported with sufficient basic operational costs by their communities, and clinics were not consistently supplied by the MOH, leading to declines in the numbers and commitment of CHW/VHWs.
While the evidence suggests that the introduction of PHC in Fiji was largely driven by WHO and UNICEF funding following Alma-Ata, the model also had strong synergies with local cultures and health worker practices in Fiji. This led to the fairly seamless integration of PHC into the health system. PHC was seen as generally successful by all interviewees. Most village health committees were engaged and involved in PHC, CHW/VHWs were initially warmly embraced by communities, and outreach activities were common. Interviewees lauded the program as ‘really good for Fiji while it lasted’ and noted, ‘We had people who mastered it— PHC specialists—and had great impact.’
Asuzu, Ram et al (2004) report that, based on the progress during the first decade of PHC, many thought that Fiji ‘could be the first in the developing world to achieve health for all’. Key indicators support this attitude. Critical measures improved significantly from 1975 to 1986: the infant mortality rate and maternal mortality ratio declined dramatically and immunisation coverage increased from below 50% to over 80% (Asuzu, Ram et al 2004). Figure 2 illustrates the improvements. A number of interviewees asserted that communicable diseases such as diarrhoea and scabies were reduced during this time (although, as one interviewee who was working as a rural MO at this time noted, there were no lab tests to confirm this reduction). Waqatakirewa (2001) noted that, while ‘it is true that other positive factors affecting the health system could claim credit for the improvement … the single most important event happening around that period was the introduction of the PHC concept’.
In some respects, the positive impact of these early years of PHC has persisted in different forms for 30 years, including the existence of nursing stations throughout the country, nearly universal use of skilled birth attendants (99% of all births, according to AusAID 2009) and the continued presence of VHWs in many communities (which interviewees placed at approximately 70% of all villages). During the first few years of PHC, interviewees stated that many latrines were built, the water supply was improved, and monthly checks were conducted by health inspectors. The visits of health inspectors became well known to the point that one interviewee recalled, ‘My mum used to clean up the house and yard when the inspectors were coming’.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 7
Figure 2. Key Primary Health Indicators in Fiji, 1975-2008
Notes: Infant mortality rate per 1000 live births; maternal mortality ratio per 100,000 live births; family planning protection rate as a percentage of women. Data for some years were not available and were estimated. Sources: World Bank 1994; MOH 1994; 1996; 1998; 1999; 2000; 2006; 2008; Sutton, Roberts et al 2008.
Interviewees noted high levels of community participation, outreach activities and communities taking responsibility for their own health. Some communities embraced PHC thoroughly and provided funds to scale up the community dispensary and pharmacy and to support CHW/VHWs. In fact, in 1991, one community won the WHO’s Sasakawa Health Prize, which acknowledges ‘outstanding innovative work in health development … or notable advances in primary health care’ (WHO 1998). Overall, PHC was seen as a powerful and positive force for better health, leading one interviewee to note that PHC ‘became a phenomenon’ in the field. It was generally agreed that through the 1980s, the PHC approach became entrenched in MOH health system policy and implementation.
THE SLOW DECLINE OF PHCDespite the prominence of PHC in the late 1970s and the early 1980s, all interviewees agreed that this momentum did not last, a judgment confirmed by Waqatakirewa’s (2001) review of PHC. From the 1990s, PHC in Fiji suffered a steady decline.
The decline of PHC is reflected in declining use of primary care facilities. Data from MOH annual reports indicate a marked drop in per capita health centre outpatient utilisation rates from 1989 and, up to 1994, a slight increase in hospital outpatient utilisation (Figure 3). Although some of the observed change in utilisation patterns may be explained by urban migration and the expiry of native rural leases (a form of rural land ownership), interviewees confirmed that villagers began to bypass lower level services to attend general outpatient departments of urban hospitals.
A number of different reasons were posited as the cause of this decline in PHC and diminishing use of village clinics. Each of these reasons will be outlined; the variety of explanations demonstrates the multi-faceted and contested reasons for the waning emphasis on PHC. This contestation of explanations is important and instructive of health policy challenges and will be discussed in more detail later in this section. These explanations are by no means mutually exclusive, but most interviewees highlighted only one explanation as dominant (while acknowledging that others might have had a more limited role). While all the factors should be seen as contributing to the decline of PHC, the fact that most interviewees stressed the primacy of one reason demonstrates the contestation over the decline.
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Infant Mortality Rate
Maternal Mortality Ratio
Family Planning Protection Rate
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Hospitals
Sub-Divisional & Area Hospitals
Health Centres
Total
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
0%
10%
20%
30%
40%
50%
60%
70%
1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Urban Hospitals Sub-Divisional Hospitals
Rural Nursing Stations Public Health Services
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Era of Primary Health Care
Era of Health Promotion
1987CoupAfter-math
Health Reform / Disease Focus
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Infant Mortality Rate
Maternal Mortality Ratio Family Planning Protection Rate

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
8 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
Figure 3. Per Capita Outpatient Utilisation, by Facility Type and Total
Note: Data for 1992 and 2001 to 2005 were not available and were estimated. Population data from SPC 2009 and United Nations Population Division 2008. Sources: World Bank 1994; MOH 1994; 1996; 1998; 1999; 2000; 2006; 2008.
Explanation #1: SuccessSome interviewees suggested that there was a general feeling that PHC had been accomplished successfully and it was simply time to move on. PHC had been pursued for a number of years, communicable disease rates were down, workshops had been held, CHW/VHWs had been trained and ‘it was time for the next thing’.
Explanation #2: The End of WHO FundingThe end of WHO funding for community seminars was cited by a few interviewees as the primary reason for the decline of PHC. 2 For approximately five years from 1979, the WHO had provided FJ$200 for each two-day and FJ$120 for each one-day community seminar on PHC, for travel and meals for participants and health workers. One interviewee noted that he and colleagues ran 14 seminars in one year, with the funding covering food, transport and expenses. The money was substantial and allowed communities to get well prepared to the point that most seminars ended up being ‘feasts of prawns, fish and crabs’. The WHO also provided funding for fortified milk, cooking demonstrations and nutrition information to supplement the PHC sessions.
Ministry of Finance budget reports show donor assistance to the health sector. From 1981 to 1985, donors (the exact donor is not specified) provided a total of FJ$863,800 to ‘rural health services’ (World Bank 1994). This funding abruptly disappeared in the 1986 budget. When the funding ended, interviewees stated, many fewer seminars were held and the push on PHC died out as subdivisional health teams made many fewer trips to villages. Counterpart MOH funding was never provided and was not allocated to replace the WHO funds.
Explanation #3: Lack of Explicit Government-Driven PHC Policy and Budgeting Besides a lack of funding, there was also a lack of a clear written policy from the MOH to guide PHC and a lack of strategic and corporate business planning. Despite a great deal of training of community and village health workers, Tembon (1988) reported that ‘there appears to be no national policy paper on training CHWs’. Together with the lack of a PHC policy, PHC activities never had a separate line in ministry budgets nor an allocation in budget estimate documents. PHC was an idea rather than a program and, while funds were allocated in the early 1980s, that funding declined by the latter part of the decade.
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Infant Mortality Rate
Maternal Mortality Ratio
Family Planning Protection Rate
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Hospitals
Sub-Divisional & Area Hospitals
Health Centres
Total
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
0%
10%
20%
30%
40%
50%
60%
70%
1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Urban Hospitals Sub-Divisional Hospitals
Rural Nursing Stations Public Health Services
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Era of Primary Health Care
Era of Health Promotion
1987CoupAfter-math
Health Reform / Disease Focus
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Infant Mortality Rate
Maternal Mortality Ratio Family Planning Protection Rate 2 One interviewee doubted that the funding came directly from WHO, citing the fact that WHO is not a funding agency. Despite this, the majority of interviewees
believed that the funding came from WHO.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 9
Table 1. Percentage of Government Spending for Health by Category, Selected Countries and Years
Fiji 1986 Fiji 1991 Samoa 1992 Marshall Islands 1992 Tonga 1993
Hospital services 71.1 67.0 53.6 48.2 61.6
Rural health facilities 8.7 5.2 22.5 15.4 14.4
Public health programs 3.1 2.7 7.0 23.2 14.4
Source: World Bank 1994
In addition, overall real per capita government health expenditure peaked in 1984 and has declined since. Per capita spending was FJ$25.80 in 1962, rose steadily to FJ$51 in 1984 and then declined to FJ$35.10 in 1992 (prices at 1985 FJ$, World Bank 1994). By the early 1990s, Fiji government expenditure on rural health and public health was markedly lower than that for other Pacific islands countries (Table 1). While Samoa, Tonga and the Marshall Islands all contributed more than 28% of the health budget to rural and public health, Fiji allocated less than 9%.
A World Bank (1994) document asserts that Fiji ‘had been the most successful in grafting primary health care facilities and outreach activities on to its existing system, with spending on rural services averaging more than 10 percent of total recurrent health outlays in the early 1980s’. But the report states that the budgetary share allocated to rural facilities fell by half, while per capita real spending on rural facilities and preventive services decreased from US$6.69 in 1983 to US$2.25 in 1991 (World Bank 1994). By the late 1980s, sufficient budget funding was not provided for continued outreach services, community seminars, transport and the like. Interviewees asserted that with this funding decline, health inspections by ministry officials—to verify water quality, latrines and cleanliness in communities—became considerably less frequent by the early 1990s. PHC activities such as outreach and community seminars, which were once seen as part of Fijian public health culture before Alma-Ata, were supported by the WHO rather than being integrated into MOH functioning.
Explanation #4: Domestic Instability A number of interviewees stated that the decline of PHC started with the 1987 coup, after which a large number of skilled health workers who were instrumental in the development of PHC emigrated. Government positive discrimination towards ethnic Fijians and the waiver of minimum qualifications for senior positions contributed to migration. Health workers from Burma and the Philippines filled the gap—by some counts 50% of doctors were expatriates at this time. The coup also led to an economic downturn, which, as noted above, was reflected in the health budget. The World Bank (1994) noted: ‘[T]he Ministry of Health had a strong health education unit until it was disbanded in the budget cuts following the political upheaval and economic downturn of 1987/88’. The coup also resulted in restrictions on internal movement of people, and meetings were not allowed, further hampering village and community engagement in their own development.
Explanation #5: Cultural Changes in Fijian VillagesA number of interviewees cited changes in community culture as leading to the weakening of PHC in communities. The village structure started to weaken in the 1980s, and the chiefs and leaders were no longer as well respected. As Roberts (1997) writes, ‘[W]hile a strong tradition of communal action exists in Fijian villages, systems for mobilising it have partly broken down with the introduction of Western values centred on improving the lot of the individual’. As a result, there was less community engagement in both Fijian and Indo-Fijian communities. Interviewees suggested that this trend may have been strengthened by the 1987 coup, which eroded chiefly authority in the public mind. One interviewee noted that, whereas before if a village headman called a meeting, there would be 100% attendance, now (in 2009) he would expect around 20% attendance. A few interviewees suggested that doctors and health workers were no longer being listened to in the same way as in the early 1980s; they found community work less rewarding and more difficult and thought, ‘We might as well head back to Suva and focus on clinical medicine’.
Explanation #6: Short Attention Span of Global ActorsOne interviewee noted that the concept of PHC itself was diluted by the global community in the middle to late 1980s, and this dilution trickled down to Fiji. While the original notion comprised comprehensive PHC, by the

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
10 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
mid-1980s a selective approach to PHC had emerged globally, for example in UNICEF’s child survival revolution and the application of the GOBI model (growth monitoring, oral rehydration, breastfeeding and immunisation). Various accounts describe this shift away from comprehensive PHC (Hall and Taylor 2003; Brown, Cueto et al 2006; Haines, Horton et al 2007). Lawn, Rohde et al (2008) describe the selective approach as ‘involving the selection of the few interventions most justified by epidemiological importance and technological affordability and a more top-down management approach’ that was deemed to be ‘more feasible, measurable, rapid and less risky than really empowering communities to make choices’. Some interviewees suggested that the dilution of the PHC message weakened its implementation and funding in Fiji.
Explanation #7: The Emergence of Health PromotionAt the time selective PHC was being developed, another health concept was emerging. The new concept of health promotion was driven by the Ottawa Charter for Health Promotion in 1986 (WHO 1986). The influence of this changes on the approach by WHO and others in Fiji—and its impact on the emphasis on PHC—was noted by interviewees. Several interviewees recalled a belief that health promotion would reduce hospital expenses by focusing on prevention, an idea that was current in the strategic plans of many Pacific health ministries. This was a powerful idea during the emerging global era of neo-liberal economic policies coinciding with the World Bank’s 1987 report ‘Financing health services in developing countries: an agenda for reform’ and the Bamako Initiative, both of which sought ways to reduce public expenditure on health (World Bank 1987).
HEALTH PROMOTION, HEALTHY SETTINGS AND HEALTH REFORMFrom the late 1980s through to the early 2000s, a number of different community health concepts were implemented in Fiji, including health promotion, the Kadavu and Taveuni models and decentralisation. These were also impacted by other developments in the health system. Together, these affected the way that PHC was conceived and implemented in Fiji over this period. These developments are addressed below.
Health PromotionWhile the 1993-94 MOH annual report had a chapter on PHC, describing it as ‘the focus for the delivery of health care services’, the 1995-96 report replaced this with a separate section on health promotion (MOH 1994; 1996). Some interviewees stated that they saw the emergence of health promotion in Fiji not as an imposed global model but rather as a response to shifting power dynamics between communities and health experts, as strengthened communities showed more voice and agency in decisions and direction. The 2000 MOH annual report states that health promotion aims to ensure that ‘each village, each settlement, each school, each health facility is trained to look at their own problems, issues and factors that influence health, list down issues, look at what can be done, develop an action plan and implement it’ (MOH 2000).
Supporting the growing influence of health promotion was the Yanuca Island Declaration, which resulted from the first Pacific Island Ministers of Health Conference, in Fiji in 1995 (WHO 1995). While the meeting had the objective of supporting the role of the Fiji School of Medicine in regional medical training, leading to the beginning of the Master of Medicine program, Yanuca is remembered for its unique Pacific Declaration, which proposed a ‘truly ecological model of health promotion’ emphasising the environment and advancing the concept of ‘Healthy Islands’ (Nutbeam 1996). Fiji, as host country and primary driver of the conference, quickly endorsed the Declaration and sought to achieve healthy villages, healthy workplaces and healthy schools as envisioned. Despite an emphasis on environmental health and integrated development, the language of PHC is missing from the Declaration.
By most accounts, health promotion has persisted in Fiji as the primary community health component. The National Centre for Health Promotion retains responsibility for health education and engaging communities in health activities and has been increasingly involved in addressing the growing chronic disease challenge, with activities focused on nutrition, smoking and exercise.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 11
Fulfilment of, or Departure from, PHC?Debate continues about whether the emergence of health promotion represented a weakening of PHC concepts, the fulfilment of the PHC ideal, or simply the continuation of PHC. Some interviewees saw the Yanuca Declaration as sounding the ‘death knell for PHC as a guiding concept in Fiji’, while others simply saw the Healthy Islands concept ‘as a way of redirecting PHC’. One interviewee asserted that the transition to health promotion was simply an ‘extension of PHC’ with healthy settings as the entry point following the Yanuca Declaration; she noted that ‘the concepts were still very much the same’ and that health promotion managed to get the government machinery re-engaged with the core ideology of PHC. The new term and new declaration revived the multi-sectoral push by establishing the Health Promotion Council with representation from a number of sectors. Interviewees heralded the health promotion model as emphasising community participation and community voice.
Many, but not all, interviewees asserted that health promotion in Fiji had weakened over time and had serious faults. A few interviewees asserted that, with the adoption of health promotion, the MOH had ‘totally moved away from PHC’. Contrary to other views, these interviewees characterised health promotion as being based on a centralised, top-down structure and regarded health promotion as a shift away from the core ideals of PHC. In their eyes, health promotion was less about community work and was instead more disease focused.
Others highlighted the fall in immunisation rates and increases in some mortality indicators as evidence that health promotion was not working. Again, the causality is complicated by factors such as migration and political upheaval. MOH senior officials noted that progress on family planning, maternal health and water and sanitation had stagnated in recent years. Although supporting data are lacking, interviewees suggested that the re-emergence of some communicable diseases such as dengue and typhoid, which had been largely eliminated during PHC, reflects ‘the standard of public health out there in the community’.
One interviewee noted that while health promotion generally continued the PHC concepts, promotion was emphasised at the expense of health protection. The interviewee noted that health promotion focuses mainly on behavioural change and not sufficiently on such critical elements as building latrines and improving water supply. He asserted that the ‘standard of sanitation and hygiene has dropped dramatically’.
Similarly, interviewees noted that health promotion was but one piece of the whole puzzle and that health care was needed as well as health promotion. A number of interviewees criticised health promotion for being too passive in the face of serious health challenges, describing the model as ‘give them the message and then hopefully they’ll do it … and we wait and wait’. These interviewees noted that the broad health promotion approach, with its focus on individual responsibility and behaviour, ‘is not our way of doing things in the Pacific’. Health promotion was regarded by these interviewees as lacking regulation and action and being too focused on discussions with individuals—imposing a Western-oriented individual human rights approach to Pacific communities.
Funding for Community Health ActivitiesRegardless of the relative merits of health promotion and PHC, it remains true that public health programs have long been underfunded. The World Bank estimated that ‘in most Pacific island countries around 70% of recurrent health budgets are devoted to curative care and treatment overseas, leaving little for preventative services’ (AusAID 2009). This is confirmed by Fijian data, which show that the funding for public health has been only 2-3% of budget provision since 1982 (Figure 4). Importantly, the budget item for rural nursing stations, which was included in MOH annual reports from 1982 to 1996, was not included in subsequent years. Despite the marked increase in funding for subdivisional hospitals between 1996 and 2000, utilisation rates for those hospitals did not increase during that period (Figure 3). As noted above, funding for rural nursing stations was cut in half between 1983 and 1991.
The Kadavu and Taveuni Community Health ModelAnother element of the transition to health promotion was the commitment of additional external resources. In particular, AusAID provided funding to support health promotion and community participation in health, most notably through health projects on the islands of Kadavu and Taveuni—though the bulk of funding was for hospital construction and biomedical equipment.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
12 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
Figure 4. Government Budget Provision for Health, by Category 1982-2000
Note: Data for 1997 were not available and were estimated. Source: MOH 1994; 1996; 1998; 1999; 2000
The Kadavu Rural Health Project ran from July 1994 to June 1997 with the goal of developing an integrated approach to rural health care delivery. The project included community participation, training of MOH staff and community personnel and upgrading health care infrastructure and equipment (AusAID 2001). VHWs and village environmental workers were trained. The director of the project has called the model ‘a primary health care approach’ (Roberts 1997). The project devolved power and decision making to the community, and an AusAID evaluation in 2001 noted that public awareness of health issues had increased dramatically. The Kadavu ‘model’, in which community development aspects were very prominent, in fact emerged during the project’s implementation. Roberts (1997) writes that the project emphasised ‘providing information to assist communities to make sensible decisions to protect their own health’.
One of the great successes of the model was its integration with provincial council decision making. The project believed that success was more likely if activities ‘were vested in local government rather than in the Ministry of Health’ (Roberts 1997). With advocacy from newly formed village health committees, health became a priority of the provincial council and received greater allocation of time and funding (AusAID 2001). Utilisation of health services increased significantly, with VHWs conducting around 30-40% of consultations (AusAID 2001). Environmental health was also emphasised and, over the course of the project, 576 toilets were constructed in 40 villages and water supply was improved in 39.
The project was widely seen as successful, and the model was picked up by NGOs, people in the education sector and environmental health workers. Post-project interviews with senior MOH officers indicated ‘that the project had influenced MOH to place a greater emphasis on preventive’ activities (AusAID 2001). Critical analysis of the project revealed that its limited time span prevented the full institutionalisation of the changes. The AusAID evaluation also highlighted the lack of support from the ‘overcentralised’ health system, which initiated the early steps towards decentralisation.
The Taveuni Integrated Community Health Model was funded by AusAID and implemented from 1999 to 2004. An end of project report written by the Taveuni Medical Sub-Division (Taveuni Medical Sub-Division 2004) outlines the model: upgraded facilities, improved referral system, staff training and ‘supporting community action for health through a community-based health promotion program, the development and support of
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Infant Mortality Rate
Maternal Mortality Ratio
Family Planning Protection Rate
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Hospitals
Sub-Divisional & Area Hospitals
Health Centres
Total
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
0%
10%
20%
30%
40%
50%
60%
70%
1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Urban Hospitals Sub-Divisional Hospitals
Rural Nursing Stations Public Health Services
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Era of Primary Health Care
Era of Health Promotion
1987CoupAfter-math
Health Reform / Disease Focus
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Infant Mortality Rate
Maternal Mortality Ratio Family Planning Protection Rate

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 13
health committees and training and supporting a network of community health workers’. This appears nearly identical to the PHC model in Fiji in the 1980s.
The project established community health committees (CHCs) through consultation with local councils and community meetings. The CHCs were tasked with promoting healthy lifestyles, conducting village health inspections, collaborating with MOH health workers and assisting with patient follow-up—activities that largely mirror PHC. The examples of activities given in the Taveuni report include rubbish disposal, building toilets, improving water sources and improving community cleanliness. In a post-project survey, 80% of community members said that the CHC had made a positive difference, noting social benefits, improvements in cleanliness, health education and improved sanitation (Taveuni Medical Sub-Division 2004).
Similarly, the Taveuni project revived the PHC concept by recruiting and training 91 community members as VHWs for a population of less than 10,000. Based at community dispensaries, the VHWs conducted home visits and referred patients to nursing stations and health centres. They were also involved in health promotion on topics ranging from family planning to non-communicable diseases to food security to environmental health. By the end of the project, the percentage of community members who washed their hands increased, as did the percentage using modern family planning methods. Many households established backyard gardens, and knowledge of sexually transmitted and non-communicable diseases increased (Taveuni Medical Sub-Division 2004).
The Kadavu and Taveuni community development models endorsed some of the core elements of PHC community participation and of health promotion. While some project documentation (Roberts 1997) situates the models in the realm of health promotion, most of the activities outlined hark back to the early days of PHC: environmental health, community outreach, training VHWs, and community health committees. Perhaps most importantly, the projects placed a great deal of responsibility on communities, one commentator asserting, ‘[T]hese projects have resulted in the communities taking a more active role in health issues affecting them’ (Waqatakirewa 2001).
One interviewee commented that the health and medical ‘professional world is based on selling information’, while the success of the Kadavu model required ‘a willingness to give information and power away’. Most interviewees saw the Kadavu and Taveuni models as very successful, one noting that they ‘should have been scaled up’. The AusAID evaluation (2001) affirmed that lessons from these projects were ‘eminently transferable’ to other areas and projects. 3
Health Sector Reform in the Early 2000sHealth reform initiatives that began in 1999 have also had a significant impact on community health care—which by this time was no longer called PHC. The health sector reform program was financed by AusAID with A$9 million for the first five years. The reform began with a focus on devolving power and resources to the divisions, but eventually focused largely on the decentralisation of decision making from head office to the four administrative divisions (Pande 2003). Decentralisation was a policy across all sectors of the Rabuka government, but the Chaudhary government of 1999 reversed those policies for all other ministries—while health continued with decentralisation. Curative and preventive health services, which had been run separately at Suva headquarters, were integrated at the divisional level. This broke down the division between curative and public health programs.
A recent report noted that ‘after five years, the decentralised model was well accepted and there were efficiency gains’ (Sutton, Roberts et al 2008). One interviewee noted that the decentralisation strengthened the PHC concepts of moving power closer to the communities. Despite this, most interviewees suggested that the fact that funding and resource allocation decisions were not decentralised severely limited the effect of the decentralisation and demonstrated the shallow commitment to changing ministerial functioning.
In February 2008 the interim military government rolled back the decentralisation reform and moved decision making back to Suva. Additionally, curative services and preventive services were again separated, and the integrated links between health centres and divisional hospitals were broken. Though the impact of these decisions has yet to be fully felt, many interviewees considered that the change would likely weaken community health care.
3 Caveats on the success of these models must be added, however. The AusAID review notes that the ‘cultural homogeneity of Kadavu simplifies the implementation of this type of project’, suggesting that operating the model in other parts of the country might be somewhat more difficult (AusAID 2001; Roberts 1997).

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
14 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
A few interviewees noted that the major donor partners’ support for reform ran counter to the PHC approach. Health reform was consistent with the approach outlined in the World Bank’s 1993 World Development Report, Investing in Health (World Bank 1993), which focused more narrowly on delivering a cost-effective minimum package of services, omitted the term primary health care and neglected the role of other sectors and communities (Lawn, Rohde et al 2008). In Fiji, the reform was characterised by work on human resources, health information systems and financial management, activities that may be needed but that have been divorced from health service delivery.
During this same period, the global health arena became more crowded with a substantial increase in actors and funding highlighted by the Millennium Development Goals, the Global Fund for AIDS, Tuberculosis and Malaria and many other disease-focused initiatives. The significant impact of these global health initiatives on PHC and on national priority setting has recently been highlighted (Biesma, Brugha et al 2009).
For example, Das Gupta and Gostin (2009) attribute the decline in environmental health services in many parts of the world, including Fiji, to a global policy failure created by the international community. They argue that the intellectual shift away from population-wide health services has become so extreme that interventions to improve environmental sanitation have come to be classified as being ‘outside the health sector’. The authors note that sanitation was even excluded from the original Millennium Development Goals, and believe that by this logic the health sector’s response to diarrheal diseases is confined to treating cases or improving personal health behaviors rather than reducing people’s exposure to fecally-transmitted diseases. They argue that a core function of public health agencies is, in fact, to monitor the quality of sanitation services and pressure the providers to improve them.
HEALTH STATUS AND SERVICE DELIVERYAs early MOH documents make clear, the main aim of health policy is ‘to promote, protect, maintain, restore and improve the health and well-being of the citizens of the Republic of Fiji’ (MOH 1994). However, the policy changes during the last 30 years—from PHC to health promotion to Healthy Islands to health sector reform—have not been paralleled by a consistent improvement in health status. On the contrary, in some key areas health status has declined. Progress against key health indicators has stagnated somewhat since the end of the PHC era, and, in fact, the maternal mortality ratio has increased since 1990. 4Figure 5 illustrates changes in indicators during the main periods of health policy change in Fiji.
Service Delivery ChallengesA number of challenges confront the Fiji health system. Interviewees noted that political upheaval had ‘weakened community leadership’, while the old community structures were more encouraging of community ownership. Others stated that, while Fiji used to have a strong ‘whole of government approach’ at subdivisional level, communication between sectors was now weaker and activities more fragmented.
The political upheaval exacerbated human resource challenges. Again, following the coup of 2000, 30 general practitioners, who had been keeping the last remnants of PHC alive, left the country (Sharma 2002). By 2002, well over 65% of hospital-based and public primary care doctors were expatriates, and private health services were expanding (Sharma 2002). From 2003 to 2007, 160 medical officers and 545 nurses exited the public health system, going either overseas or into the private sector (Sutton, Roberts et al 2008; Negin 2008). By 2008, 36% of senior medical posts were vacant, and 120 medical officers (25% of the total medical workforce) were in private practice (Sutton, Roberts et al 2008).
As a result, there has been a significant reduction in services available in subdivisional health facilities over the past decade. Specifically, the lack of anaesthetists has forced surgical facilities to lie unused and patients to be referred to higher level facilities. Interviewees also agreed that VHWs were no longer very active, some estimating that only 60-70% of communities have an active VHW, some of whom have not had refresher training for years. While 15-20 years ago VHW training was a regular activity of the ministry, ‘no one talks about VHWs now in 2009’, and turnover rates for VHWs, especially in peri-urban areas, are very high.
3 Caveats on the success of these models must be added, however. The AusAID review notes that the ‘cultural homogeneity of Kadavu simplifies the implementation of this type of project’, suggesting that operating the model in other parts of the country might be somewhat more difficult (AusAID 2001; Roberts 1997).
HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 15
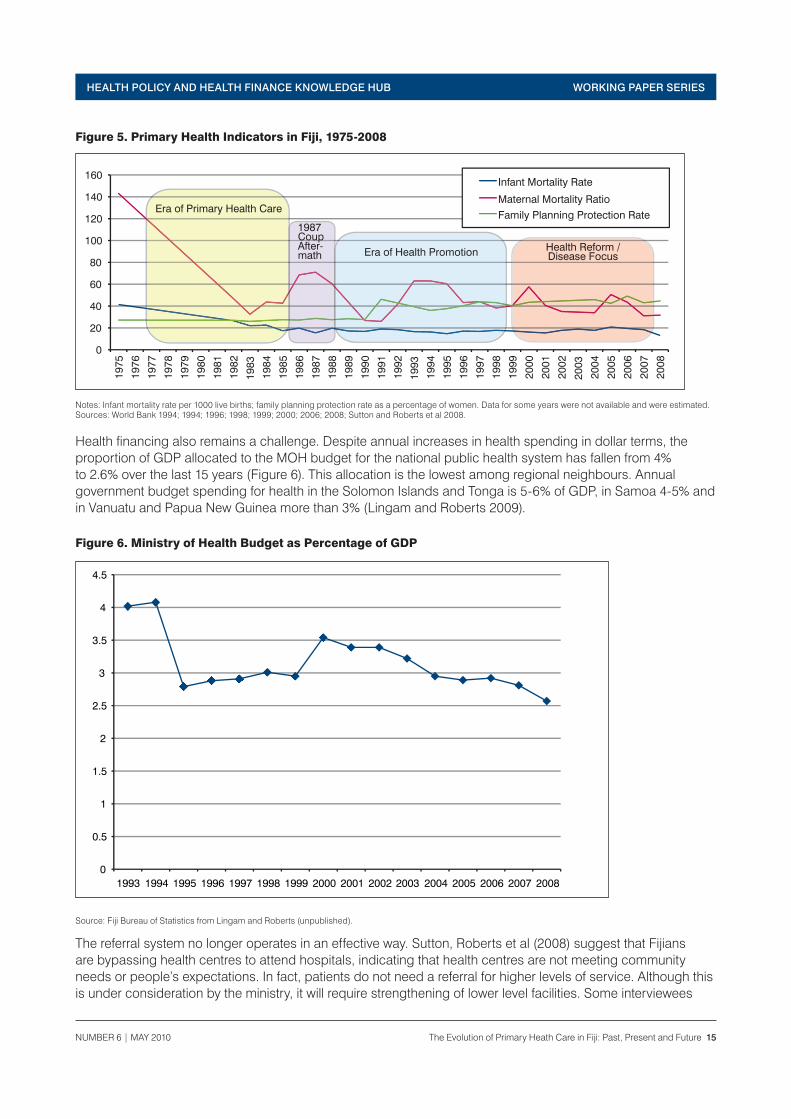
Figure 5. Primary Health Indicators in Fiji, 1975-2008
Notes: Infant mortality rate per 1000 live births; family planning protection rate as a percentage of women. Data for some years were not available and were estimated. Sources: World Bank 1994; 1994; 1996; 1998; 1999; 2000; 2006; 2008; Sutton and Roberts et al 2008.
Health financing also remains a challenge. Despite annual increases in health spending in dollar terms, the proportion of GDP allocated to the MOH budget for the national public health system has fallen from 4% to 2.6% over the last 15 years (Figure 6). This allocation is the lowest among regional neighbours. Annual government budget spending for health in the Solomon Islands and Tonga is 5-6% of GDP, in Samoa 4-5% and in Vanuatu and Papua New Guinea more than 3% (Lingam and Roberts 2009).
Figure 6. Ministry of Health Budget as Percentage of GDP
Source: Fiji Bureau of Statistics from Lingam and Roberts (unpublished).
The referral system no longer operates in an effective way. Sutton, Roberts et al (2008) suggest that Fijians are bypassing health centres to attend hospitals, indicating that health centres are not meeting community needs or people’s expectations. In fact, patients do not need a referral for higher levels of service. Although this is under consideration by the ministry, it will require strengthening of lower level facilities. Some interviewees
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Infant Mortality Rate
Maternal Mortality Ratio
Family Planning Protection Rate
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Hospitals
Sub-Divisional & Area Hospitals
Health Centres
Total
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
0%
10%
20%
30%
40%
50%
60%
70%
1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Urban Hospitals Sub-Divisional Hospitals
Rural Nursing Stations Public Health Services
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Era of Primary Health Care
Era of Health Promotion
1987CoupAfter-math
Health Reform / Disease Focus
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Infant Mortality Rate
Maternal Mortality Ratio Family Planning Protection Rate
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Infant Mortality Rate
Maternal Mortality Ratio
Family Planning Protection Rate
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Hospitals
Sub-Divisional & Area Hospitals
Health Centres
Total
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
0%
10%
20%
30%
40%
50%
60%
70%
1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Urban Hospitals Sub-Divisional Hospitals
Rural Nursing Stations Public Health Services
0
20
40
60
80
100
120
140
160
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Era of Primary Health Care
Era of Health Promotion
1987CoupAfter-math
Health Reform / Disease Focus
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Infant Mortality Rate
Maternal Mortality Ratio Family Planning Protection Rate

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
16 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
highlighted the re-emergence of typhoid as a sign that a revived PHC model is needed. And a recent report highlighted the need for a new push on environmental health, noting: ‘[M]any of the rural water supply systems … are now deteriorated to the degree that village water systems are sources of diarrhoeal diseases’ (Sutton, Roberts et al 2008).
Recognition of these health system challenges has led to some recent positive changes. Following the first stage of its health reform project, AusAID initiated the Fiji Health Sector Improvement Program (FHSIP) during 2004-09. The FHSIP has contributed to a recent strengthening of primary care delivery through an emphasis on community development and outreach. When immunisation rates had declined by 2004 to just over 60% coverage for measles vaccine, from 86% in 1988 (AusAID 2009), FHSIP and MOH partners started working with nurses to get them back out into the communities (Sharma 2009). FHSIP interviewees asserted that immunisation rates have now increased and that rates of diarrhoea and other maladies have likewise started to decline, in part because the increased activity of nurses in communities allows greater health education and more prompt treatment. Even so, FHSIP staff acknowledged that its Healthy Settings community development initiatives did not match PHC objectives and that a renewed push would be needed to strengthen peripheral care.
Revitalising Community Health CarePublication of the 2008 World Health Report indicated a return, in some form, to the ideas of primary health care and a new commitment by WHO to revitalising community health care. In a recent Lancet article, WHO Director Margaret Chan writes that it will not be possible to reach the health-related MDGs unless there is a return to the values, principles and approaches of PHC. She says that when countries at the same level of economic development are compared, those where health care is organised around the tenets of primary health care produce a higher level of health for the same investment. As part of a preventive approach, primary health care is people-centred, regards prevention as important as cure, and tackles the root causes of ill health (Chan 2009).
The WHO’s 62nd World Health Assembly, held in Geneva in May 2009, reaffirmed the Alma-Ata principles along with the MDGs and the importance of social determinants of health and called for a renewed push on primary health care, including health system strengthening. The Assembly called for accelerated ‘action towards universal access to primary health care by developing comprehensive health services and by developing national equitable, efficient and sustainable financing mechanisms’, as well as putting ‘people at the centre of health care by adopting, as appropriate, delivery models focused on the local and district levels that provide comprehensive primary health care services’. The assembly also called on countries ‘to promote active participation by all people and re-emphasize the empowering of communities, especially women, in the processes of developing and implementing policy and improving health and health care, in order to support the renewal of primary health care’ (WHO 2009).
Reinforcing these sentiments, Lawn, Rohde et al (2008) write that it is understood that effective ‘primary health care services [require] consistent political and financial commitment, incremental implementation based on local epidemiology, use of data to direct priorities and assess progress, especially at district level and effective linkages with communities and non-health sectors’. AusAID (2009) recently stated that ‘involving communities in service delivery can help service providers be more responsive and accountable to local needs and provide additional resources for service delivery’.
A number of issues emerge if a return to PHC principles is to be successful as a result of this ongoing discussion in Fiji.
Domestic Political OwnershipMost interviewees agreed that some return to community health principles was needed. One said that there are ‘lots of lessons we can learn from PHC days’ and another noted the ‘need to evaluate the strengths of PHC and understand what health promotion has achieved’. Many interviewees emphasised the political aspects, arguing that the MOH needs to drive the dialogue towards the model it wants rather than simply respond to inappropriate external models. The Minister of Health held an internal meeting on PHC issues on returning from the World Health Assembly meeting in 2008 and emphasised the topic after both the 2008 and 2009 meetings.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 17
Some interviewees, however, saw this as still responding without adequate thought to models imported from abroad. One said, ‘Some decisions are picked up by politicians overseas and are put on our agenda without discussion’, as in 2008: when the Minister of Health returned from Geneva ‘with PHC, there was no discussion of strengths and weaknesses but rather more a directive to get PHC back’. Some interviewees recommended that a revitalised PHC approach should be adopted by Cabinet, endorsed by the Minister and/or supported by legislation, in contrast to the PHC policies of the 1980s. The Public Health Act focuses mainly on health inspection, and other health-focused legislation is almost exclusively curative.
Integrating Urban and Non-Communicable Disease IssuesA number of interviewees argued that the new approach to PHC should be adapted to changed disease patterns and other circumstances including urbanisation, particularly the emergence of non-communicable diseases (MOH 2008). Interviewees understood that PHC and/or health promotion are important in addressing risk factors such as obesity, nutrition and exercise. Many noted that supportive community- and home-based care for amputees and stroke victims could be a core element of a resurgent ‘21st century version of PHC’ (WHO 2002). Additionally, the new approach should move beyond the view of PHC as a rural health mechanism to include urban issues. As one interviewee noted, ‘This isn’t just about village health care’. In a recent document on the Pacific, AusAID (2009) acknowledged the challenge, noting that the ‘level of poverty in urban centres is considerably higher than in rural areas’. In Fiji, there are high levels of poverty among the 52% of the population living in urban areas (including 100,000 squatters). While much of the rural health challenge is about access and availability, urban challenges include access, quality, waiting times and opening hours.
This concern for attention to emerging diseases—while not neglecting long-standing communicable disease issues—reflects international opinion. Julio Frenk (2009) has highlighted how the new PHC needs to be able to address not just acute care, as in the original model, but chronic care as well: ‘Primary health care should also move from episodic to continuous care, going beyond the simplicity implied in the original notion of first level of care’. Rohde, Cousens et al (2008) write: ‘30 years after Alma-Ata, many countries still have a high burden of disease with infections and maternal and child health challenges, but also emerging chronic diseases. Primary health care offers solutions and approaches to address these burdens but the increasing complexity threatens to overburden the system.’ The design of the new PHC should focus on the most critical components during early phases because ‘with an ever increasing array of health service programmes, each a priority in the mind of the designers, there is a danger of overwhelming primary health care workers with a massive menu’ (Lawn, Rohde et al 2008).
Human and Financial ResourcesThis new approach to PHC will require additional resources, both human and financial. One interviewee stressed the implementation issues and lamented, ‘We have been importing concepts that we have failed to apply’. Despite the current human resources challenges, more health workers will be required for a revitalised PHC program.
The Fiji School of Medicine and the Fiji School of Nursing are in a position to supplement training in PHC for public health staff and through continuing professional education. But curriculum changes will be needed. The 2001 PHC review noted, ‘[M]ost younger staff are unaware of the scope and dimension of PHC’ (Waqatakirewa 2001). Asuzu, Ram et al (2004) refer to a study of medical students that shows a ‘poor inclination to specialise in community medicine/public health’. More recently, both schools have emphasised rural placements and community health in their curricula, and the School of Medicine has revitalised a year 3 community placement. Government-sponsored students are also required to do a rural placement after graduation. As well, outreach by nurses and MOs can be reinvigorated, and a renewed push to train and support CHW/VHWs is needed in a manner already trialled by the Kadavu and Taveuni projects.
Sufficient funding for PHC activities is needed and should be included in the preparation of national health accounts. Within the MOH, one interviewee noted that while there is the impression that ‘curative is expensive and preventative is cheap’, ‘this is not true any more … preventative is also expensive’. Within new health project that may follow Fiji Health Sector Improvement Programme (FHSIP) (scheduled to end in 2010), there is

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
18 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
an opportunity for the MOH to request funding for priority areas such as PHC. Additionally, government funding for health must increase. Significantly, the new government recently issued a People’s Charter, pillar 10 of which calls for an annual increase of 0.5% of GDP in its allocation to health for the next 10 years.
New Political and Social ConditionsMany interviewees acknowledged that changes in community culture from communalism to more individualism would make implementing PHC harder now than in the late 1970s, but they remained optimistic. While the nature of communities has changed, many of the biggest health challenges remain with the poorest communities, which are likely to benefit most from a new PHC approach. New issues are posed by urban community structures in squatter areas, and as one interviewee noted, working through existing mechanisms like NGOs and churches would be critical to success.
The new PHC must be accompanied by a clear and actionable divisional and subdivisional work plan, as evidenced in the Taveuni Integrated Community Health Model. Some interviewees recommended that greater decision rights and funding rights be provided to divisions and subdivisions to make the health system more responsive to lower level needs, not only in the amount of choices but also in the types of choices and their significance. As one author lamented when writing about Pacific islands, ‘[H]ealth systems are centrally dominated and controlled and there are few local opportunities to influence resource allocation’ (Newell 1983).
The new PHC must maintain a long-term vision. As one interviewee noted, ‘One of the problems with PHC in Fiji is that we keep redefining it’. Another noted that Fiji has been ‘bombarded by different models’.
A New Terminology for Primary Health CareThere was significant disagreement regarding the appropriate terminology for the new PHC. One interviewee preferred to retain ‘health promotion’ as the guiding term for community health, noting that while ‘PHC seems to focus on care and the care-giver, promoting health is wider’. Another interviewee noted that maintaining the term health promotion would also cause less confusion among MOH staff and partners. Another noted that PHC concepts of outreach, community engagement and environmental health were not owned by the term PHC and therefore new terminology would be workable. Finally, one interviewee stated, ‘The family in the village doesn’t care what you call it … they want access to quality health services’.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 19
RECOMMENDATIONS AND CONCLUSIONSRecommendations emerge from this report, based particularly on the testimony of interviewees in Fiji who are now looking carefully at the process of revitalising the PHC approach. Interviewees agreed that a re-galvanised community health model was needed, one that would learn from past approaches and respond to current health and political realities. The main recommendations include:
• ImplementationofanewcommunityhealthmodeldrivenbytheMinistryofHealth(MOH)withsupportfromthe Minister and Cabinet and framed as a long-term vision rather than a short-term project;
• Increasedfundingforcommunityhealth,publichealthandoutreachservices,followedbyanapproachtoAusAID and other development partners to support a new approach;
• Arenewedpushfortrainingofdoctors,nursesandCHW/VHWsincommunityhealth;
• Framingcommunityhealthasbothanurbanandruralapproach,withemphasisonimprovinghealthindicators in squatter communities, leveraging existing strengths of churches and NGOs in these areas;
• Anexplicitfocusonnon-communicablediseasesriskfactorssuchasobesity,nutritionandexercise;
• Inclusionofsocialdeterminantsofhealthincludingeducation,housingandlivelihoodsintheapproach;
• Greaterdecisionrightsandfundingdecisionsfordivisionsandsubdivisionstomakecommunityhealthmore responsive to local needs.
This study provides important lessons for Fiji, the region and the wider health policy community on how health policy develops and evolves over time. Global health policy is often short-sighted and focused on short-term targets, and lessons from past experiences are often not fully considered in the development of new policies. This analysis of PHC in Fiji from the mid-1970s serves as a microcosm of health policy challenges. It highlights the importance of political economy to health policy development and emphasises a greater understanding of community and political culture. It shows that there is often a one-sided relationship between development partners and national governments in which outside policies are often imposed without due recourse to the evidence and local country conditions. It also highlights the contestation over policy changes and the many factors that influence the evolution of policy.
The basic tenets of the Paris Declaration and Pacific Aid Effectiveness Principles (2005), which call for greater government ownership of development priorities and place the impetus for decisions in the hands of domestic government, need to be fully taken into account in developing a new model of PHC implementation in Fiji and the region. Development partners and other international actors will therefore have to be more responsive to national priorities in their planning, resource allocation and technical support.

WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
20 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
REFERENCESA renaissance in primary health care,2008, Lancet 372: 863.
Arole, M. and Arole, R. 1994. Jamkhed: a comprehensive rural health project. London, MacMillan Press.
Asuzu, M.C., B.P. Ram, M. Salusalu, M. Lal and S. Tuqa. 2004. Participatory operational research of the dynamics of the primary health care programme in Fiji. Pacific Health Dialog Mar, 11(1): 31-37.
AusAID. 2001. Developing integrated rural health care systems: an evaluation of the Kadavu rural health project in Fiji. Quality Assurance Series No. 24. Canberra: Commonwealth of Australia.
AusAID. 2009. Tracking development and governance in the Pacific. Canberra: Commonwealth of Australia.
Biesma, R.G., R. Brugha, A. Harmer, A. Walsh, N. Spicer and G. Walt. 2009. The effects of global health initiatives on country health systems: a review of the evidence from HIV/AIDS control. Health Policy and Planning 24: 239-252.
Bowen, S. and A. Zwi. 2005. Pathways to ‘evidence-informed’ policy and practice: a framework for action. PLoS Medicine 2(7): e166.
Brown, T., M. Cueto and E. Fee. 2006. The World Health Organization and the transition from international to global public health. Public health then and now. American Journal of Public Health 96: 62-72.
Capstick, S., P. Norris, F. Sopoaga and W. Tobata. 2009. Relationships between health and culture in Polynesia—a review. Social Science and Medicine 68: 1341-1348.
Carden, F. 2009. Knowledge to policy: making the most of development research. Ottawa: International Development Research Centre.
Chan, M. 2008. Return to Alma-Ata. Lancet 372: 865-866.
Chan, M. 2009. Primary health care as a route to health security. Lancet 373:1586-1587.
Das Gupta, M. and L. Gostin. 2009. How can donors help build global public goods in health? World Bank Policy Research Working Paper 4907. World Bank.
Freeman, P., Perry, H., Gupta, S., and Rassekh, B. 2009 Accelerating progress in achieving the millennium development goal for children through community-based approaches. Global Public Health Nov 3: 1-20.
Frenk, J. 2009. Reinventing primary health care: the need for systems integration. Lancet 374: 170-173.
Gilson, L. and N. Raphaely. 2008. The terrain of health policy analysis in low and middle income countries: a review of published literature 1994-2007. Health Policy and Planning 23: 294-307.
Haines, A., R. Horton and Z. Bhutta. 2007. Primary health care comes of age. Looking forward to the 30th anniversary of Alma-Ata: call for papers. Lancet 370: 911-913.
Hall, J and R. Taylor. 2003. Health for all beyond 2000: the demise of the Alma-Ata declaration and primary health care in developing countries. Medical Journal of Australia 178: 17-20.
High Hopes at Alma-Ata,1978, Lancet 23 Sep, 2(8091): 666.
Howlett, M. and M. Ramesh. 2003. Studying public policy: policy cycles and policy subsystems. Toronto: Oxford University Press.
Jacobs, M. for the World Health Organization Western Pacific Regional Office. 2002. Primary Health Care Review Project, Region Specific Report. WHO WPRO, Manila.
Lawn, J., J. Rohde, S. Rifkin, M. Were, V.K. Paul and M. Chopra. 2008. Alma-Ata 30 years on: revolutionary, relevant, and time to revitalise. Lancet 372: 917-927.
Lee, J. 2003. Global health improvement and WHO: shaping the future. Lancet 362: 2083–2088.
HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 21
Lewin, S., J. Lavis, A. Oxman, G. Bastías, M. Chopra, A. Ciapponi, S. Flottorp, S. García Martí, T. Pantoja, G. Rada, N. Souza, S. Treweek, C.S. Wiysonge and A. Haines. 2008. Supporting the delivery of cost-effective interventions in primary health-care systems in low-income and middle-income countries: an overview of systematic reviews. Lancet 372: 928-939.
Lingam, D. and G. Roberts. 2009. Forty Six Years of Health Financing in Fiji (1962 – 2008).
MOH. 1994. Fiji Ministry of Health Annual Report 1993 and 1994. Suva: Ministry of Health.
MOH. 1996. Fiji Ministry of Health Annual Report 1995 and 1996. Suva, Fiji: Ministry of Health.
MOH. 1998. Fiji Ministry of Health Annual Report 1997 and 1998. Suva: Ministry of Health.
MOH. 1999. Fiji Ministry of Health Annual Report 1999. Suva: Ministry of Health.
MOH. 2000. Fiji Ministry of Health Annual Report 2000. Suva: Ministry of Health.
MOH. 2006. Fiji Ministry of Health Annual Report 2006. Suva: Ministry of Health.
MOH. 2008. Fiji Ministry of Health Annual Report 2008. Suva: Ministry of Health.
Negin, J. 2008. Australia and New Zealand’s contribution to Pacific island health worker brain drain. Australian and New Zealand Journal of Public Health 32: 507-511.
Newell, K.W. 1983. Primary health care in the Pacific. Social Science & Medicine 17(19): 1441-1447.
Nutbeam, D. 1996. Healthy islands—a truly ecological model of health promotion. Health Promotion International 11(4): 263–264.
Pande, M. 2003. Health financing options for Fiji’s health system. Pacific Health Dialog Sep, 10(2):129-140.
Paris Declaration on Aid Effectiveness. 2005. http://www.adb.org/media/articles/2005/7033_international_community _aid/paris_declaration.pdf
Perks, C., Toole, M., and K. Phouthonsy. 2006. District health programmes and health sector-reform: case study in the Lao People’s Democratic Republic. Bulletin of the World Health Organization 84: 132 - 38.
Perry, H., Shanklin D., and D. Schroeder. 2003. Impact of a Comprehensive Community-based Primary Healthcare on Infant and Child Mortality in Bolivia. Journal of Health Population and Nutrition 21(4): 382-395
Pollard, S. 2008. How can aid help build capacity in the Pacific? Presentation to Asian Development Bank seminar, 28 February. http://www.adb.org/Documents/Events/2008/ADB-Staff-Brownbag-Seminar/CD-Presentation-SPollard.pdf. (accessed 17 January 2010)
Reich, M.R. and K. Takemi. 2009. G8 and strengthening of health systems: follow-up to the Toyako summit. Lancet 373: 508-515.
Roberts, G. 1997. The Kadavu health promotion model, Fiji. Health Promotion International 12(4):283-290.
Rohde, J., S. Cousens, M. Chopra, V. Tangcharoensathien, R. Black, Z.A. Bhutta and J.E. Lawn 2008). 30 years after Alma-Ata: has primary heath care worked in countries? Lancet 372: 950-61.
Rosato, M., G. Laverach, L. Grabman, P. Tripathy, N. Nair, C. Mwansambo, K. Azad, J. Morrison, Z. Bhutta, H. Perry, S. Rifkin and A. Costello. 2008. Community participation: lessons for maternal, newborn and child health. Lancet 372: 962-971.
Sharma, N. 2002. Politics and primary care: A focus on Fiji. Asia Pacific Family Medicine 2002, 1: 61-62.
Sharma, N. 2009. Opening remarks for the launch of EPI/RH Symposium, 1 April. http://www.fiji.gov.fj/publish/printer_14605.shtml (accessed 10 November 2009)
Sutton, R., G. Roberts and D. Lingam. 2008. A situational analysis of the Fiji health sector.
Taveuni Medical Sub-Division. 2004. Evaluation of the Taveuni Integrated Community Health Model. Suva, Fiji.
WORKING PAPER SERIES HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB
22 The Evolution of Primary Heath Care in Fiji: Past, Present and Future NUMBER 6 | MAY 2010
Tembon, A.C. 1988. Suggestions for primary health care improvement on an island in Fiji using results from a utilization survey. Public Health 102: 493-500.
United Nations Population Division. 2008. World population prospects: the 2008 revision. Population database. http://esa.un.org/unpp/index.asp (accessed 12 December 2009)
Walt, G. and L. Gilson. 1994. Reforming the health sector in developing countries: the central role of policy analysis. Health Policy and Planning, 9(4): 353-370.
Waqatakirewa, L. 2001. Primary Health Care Review on Fiji. Manila: World Health Organization.
World Bank. 1987. Financing health services in developing countries: an agenda for reform. Washington, DC: World Bank.
World Bank. 1993). World development report: investing in health. New York: Oxford University Press.
World Bank. 1994. Health priorities and options in the World Bank’s Pacific Member countries. Report No. 11 620-EAP. World Bank.
WHO. 1978. Declaration of Alma-Ata. World Health Organization. http://www.who.int/publications/almaata_declaration_en.pdf (accessed 5 May 2009).
WHO. 1986. Ottawa charter for health promotion. World Health Organization. 21 November. http://www.who.int/hpr/NPH/docs/ottawa_charter_hp.pdf (accessed 20 October 2009)
WHO. 1995. Yanuca Island declaration. Manila: World Health Organization Western Pacific Regional Office.
WHO. 1998. Statutes of the Sasakawa Health Prize. World Health Organization. http://www.who.int/governance/awards/sasakawa/sasakawa_statutes/en/index.html (accessed 21 October 2009)
WHO. 2001. Second health sector development technical advisory group meeting on primary health care in the western Pacific region report. Manila: World Health Organization Western Pacific Regional Office.
WHO. 2002. Innovative care for chronic conditions: building blocks for action: global report. Geneva: World Health Organization.
WHO. 2006. Health policy development: a handbook for Pacific island practitioners. Manila: World Health Organization Western Pacific Regional Office.
WHO. 2008. The world health report 2008. Primary health care: now more than ever. Geneva: World Health Organization. http://www.who.int/whr/2008/whr08_en.pdf (accessed 8 May 2009).
WHO. 2009. Primary health care, including health system strengthening. World Health Assembly of the World Health Organization. http://apps.who.int/gb/ebwha/pdf_files/A62/A62_R12-en.pdf (accessed 20 October 2009)
WHO and UNDP. 1986. Development of primary health care in the South Pacific: agency terminal report, 1 January 1983-31 December 1986. World Health Organization and United Nations Development Programme. Manila: World Health Organization Western Pacific Regional Office.

HEALTH POLICY AND HEALTH FINANCE KNOWLEDGE HUB WORKING PAPER SERIES
NUMBER 6 | MAY 2010 The Evolution of Primary Heath Care in Fiji: Past, Present and Future 23

KNOWLEDGE HUBS FOR HEALTHStrengthening health systems through evidence in Asia and the Pacific
A strategic partnerships initiative funded by the Australian Agency for International Development
The Nossal Institute for Global Health