Embed Size (px)
Citation preview

(CANCER RESEARCH 52, 2371-2383, May I, 1992]
Perspectivesin CancerResearch
The Evolution of Paradigms for the Management of Breast Cancer: A PersonalPerspective1
Bernard Fisher2
National Surgical Adjuvant Breast and Bowel Project Headquarters, Pittsburgh, Pennsylvania 15261
Introduction
Although female breast cancer remains a major public healthproblem, notable improvements have occurred in its treatment.For most of this century, women with primary breast cancerhave been treated by radical mastectomy or some variation ofthat procedure. In recent years lumpectomy has become therecommended operation for most patients. Before the mid-1970s, postoperative adjuvant systemic therapy was not used;now it is a major component of treatment strategies. How havethese drastic changes come about? Are they the result of anecdotal recitations of personal experiences or the outcome ofmore abstruse circumstances? How are future changes apt tooccur? Are we to believe that science has little or nothing to dowith the process?
Science will continue to determine how breast cancer isperceived and managed in the future. Clinical practice must bebased on a rational foundation that underlies our comprehension of the disease; this understanding relates to the "science"
of the time in which we practice. The science of breast cancerin 1992 is different from that of 1892, and the science of breastcancer in the next decade will differ from that of today. As theburgeoning science of molecular biology unfolds, it is unrealisticto expect that operative procedures and systemic therapy modalities now used to treat breast cancer will remain static, anymore than it could have been assumed that surgery wouldremain unchanged during the past century, given the changesin our understanding of the disease during that time.
The increased use of mammography and recent advances inbasic tumor biology (particularly as they relate to cancer etiology) have resulted in an expanded perception of the breastcancer problem. This essay will describe how breast cancertherapy has evolved and will continue to advance as a consequence of transitions from paradigm to paradigm. It will alsopresent several scientific developments that have the potentialfor creating new paradigms for breast cancer management inthe not too distant future. How adequately past, present, andfuture paradigms relate to the currently expanding view of thedisease is also considered.
An Expanded Perception of the Breast Cancer Problem. In1969, 66,000 new cases of breast cancer were diagnosed and29,000 women died from the disease. By 1975 there were 88,000new cases and 33,000 deaths, with 1 in 14 women at risk fordeveloping the disease. During the 1990s, more than 1.7 millionwomen (about 175,000 per year) in the United States will benewly diagnosed with invasive breast cancer, and about 30% ofthem will ultimately die from it; approximately 1 in 9 women
Received 12/3/91 ; accepted 2/27/92.' The laboratory and clinical investigations referred to in this publication were
supported by USPHS grants from the National Cancer Institute and by grantsfrom the American Cancer Society.
2To whom requests for reprints should be addressed, at National SurgicalAdjuvant Breast and Bowel Project Headquarters. Room 914, Scaife Hall, 3550Terrace Street. Pittsburgh. PA 15261.
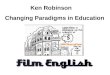
will develop the disease in her lifetime (1). Surveillance, Epidemiology, and End Results program (SEER) data indicatethat, as age increases, so does the incidence of breast cancer(2). Whereas, for women 50-54 years of age the incidence is212 per 100,000, it increases progressively over the next 25years to 435 per 100,000 for women 80 to 84 years old. Asominous as they may seem, these statistics do not begin toportray the magnitude of the problem. The 75,000 or morewomen with invasive breast cancer clinically and/or mammo-graphically diagnosed each year represent only the tip of aniceberg. Those women comprise only one cohort of the femalepopulation whose breasts contain a spectrum of aberrations,among which are the detected cancers (Fig. 1).
At the top of the spectrum (Fig. 1/4) are women whose breastscontain invasive and noninvasive cancers of sufficient size to bedetected clinically. In that same category are women withpalpable benign lesions considered to carry no added risk, aswell as those whose breasts contain lesions that put them atincreased risk for invasive cancer, e.g., atypical ductal or lobularhyperplasia, and florid or solid papillary hyperplasia. Near thisend of the spectrum (Fig. \B) are women with abnormal breastsharboring lesions similar to those above that can be detectedonly by mammography. Among those with "normal" breasts in
the middle of the spectrum (Fig. 1C) are women with thepreviously described lesions that are nondetectable but, if malignant, are likely to eventually become clinically or mammo-graphically identifiable. Near the bottom of the schema (Fig.ID) are women, considered normal, who may have breast tissuethat has undergone biological alteration, a term used to encompass molecular-biologic, genetic, and biochemical factors thatmay play a seminal role in the etiology of invasive breast cancer.If modern concepts of carcinogenesis as they relate to theprocess of initiation and promotion are applicable to breastcancer, there is reason to believe that there are women withinthe so-called normal population who have "biological breastcancers." These lesions have not yet become what we recognize
under the microscope as cancers (phenotypic), but they haveundergone molecular-biologic changes that will result in tumorsthat may, at some future time, be diagnosed by current clinicaland mammographie methods. It is here that a single normalcell is "emancipated" from host controls and that—as a result
of its altered growth regulation—the resulting neoplastic stemcell gives rise to a clone of tumor cells. These phenomena andthose that follow depend upon a series of complex eventsinvolving alterations in cellular oncogenes, tumor suppressorgenes, gene products, and growth factors that can augment orinhibit cell proliferation, and related activities (3-5). As neoplastic growth progresses, new mutations occur and new clones,which have a growth advantage over their predecessors, appear.At some point, genetic alterations may occur which give rise tocells that have acquired competence for establishing métastases.Early in the onset of a tumor, angiogenesis, an event necessaryfor tumor progression, takes place. (6) At the bottom of the
2371
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
en9enLU<-JCE
~jmQQ*Éu°-
ujz9"gzc
2l1BIOLOGICALCHANGES-
GENOTYPIC-(GENEALTERATION,
DNA DAMAGE,etc.)"NO"CHANGES(AT
RISKFORBREASTCANCER)C
•¿�®
•¿�CD
.'.
•¿�.F®*ô
®®°oOx^000".S
O •¿�»0 OO®"•"
•¿�*•' "•
Fig. 1. Spectrum of changes in women with normal and abnormal breasts. •¿�,invasive cancers; O, in situ cancers (DCIS, LCIS); ®,hyperplasia, atypicalhyperplasia, sclerosing adenosis; •¿�,biological cancers; x, fibroadenomas, simplecysts, adenosis, duct ectasia.
spectrum (Fig. IE) are women who may have no phenotypicallyexpressed lesions and no biological changes in their breasts.These women, despite putatively normal breasts, are at risk fordeveloping breast cancer even though they may have no definable risk factors. Although the spectrum depicts a change thatcould exist in the breast of a particular woman at a particulartime, it fails to convey the dynamics of the change that occursover time. It does not indicate how the stepwise progression ofa lesion that travels from one end of the spectrum to the otheris instigated or show how much time elapses between the firstchange that gives rise to a cancer and the presence of a cancerthat can be detected.
The growth rate of a tumor before its clinical detection isobscure, and information regarding its growth after detectionis imprecise. Doubling times of clinically identifiable tumorshave been estimated to be between 75 and 130 days. If 100 daysis selected as the doubling time, and if, as is commonly stated,1 x IO9cells is the minimum tumor burden required for clinical
detection, the time from tumor onset to diagnosis is assumedto span at least 30 tumor doublings, or approximately 8 years.Thus, if the annual rate of detection of invasive cancers is175,000 new cases, there could be at least a million women inthis country with nondetectable biological and pathologicalbreast cancer who are unaware that they have the disease.
As a result of this expanded perspective of breast cancer, itseems appropriate to ask, What might be considered earlybreast cancer? Does "earliness" relate to tumor size? To nodal
status? To occult tumors detected by mammography? To non-invasive cancers? To certain molecular-genetic alterations thathave taken place but that are, as yet, unidentifiable? To tumorswith markers associated with a favorable prognosis? To cancersin women who have lived tumor-free, for example, for 30 yearsafter their removal (a circumstance that gives rise to the well-known pronouncement, "It was gotten early")? Increasing
knowledge prohibits formulation of a simple definition of theterm early. Consequently, use of the term requires more circumspection than is usual, particularly in a court of law, wherepunitive action is brought against physicians for failing to treatpatients when their tumors were "early."
Almost a decade ago, while attempting to put into perspectivemy 30 years of research vis-Ã -vischanges in the treatment of
breast cancer, I became familiar with the work of ThomasKühn,a theoretical physicist, philosopher, and historian ofscience, who described the developmental pathways of physicalsciences as transitions from paradigm to paradigm which occuras a result of scientific revolutions (7, 8). Kühnand others whohave discussed the evolutionary process of science have notgiven meaningful consideration to how radical changes takeplace in biology and medicine (9, 10). Some theorists, in fact,contend that Kuhnian revolutions do not occur at all in thesesciences (11). Others dispute that perspective (12). It is mycontention that Kuhn's interpretation of the nature of scientific
revolution is directly relevant to medicine and that his description of the pathway of paradigmatic change can be used toillustrate how the treatment of breast cancer has evolved to itspresent state. (I hasten to point out that, although retrospectively relating progress in medical science to a particular schemais legitimate, following the steps comprising that pathway doesnot necessarily guarantee success in obtaining new knowledge.)
Developmental Pathways of Science
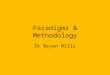
The Transition from Paradigm to Paradigm According toKühn.At some time in history, according to Kühn,a scientificcommunity acknowledges the existence of scientific achievements so unprecedented that they attract an increasing numberof adherents away from the model that governs the community's
activity (Fig. 2). For a time, the new science serves as a foundation for the practice of these "converts." The model governing
their activity is called a paradigm, a term used to encompass"all of the beliefs, values, and techniques shared by members ofa [scientific] community" (7). Although a paradigm is accepted
because it seems better than its competitors, it seldom explainsall of the enigmas that confront it. Consequently, it provides avariety of problems that must be resolved by its adherents. Todo so, they resort to a circumstance known as normal science,which flourishes as long as the paradigm is the exemplar thatgoverns the activity of the community. Most of the researchconducted by a scientific community is normal science, its aimbeing to define more precisely the attributes of a paradigm andto make it more acceptable. Such "mopping-up" activities are
mainly fact-gathering endeavors carried out by experimentationand observation to resolve ambiguities and solve the problemsgenerated by the paradigm.
Sooner or later during these investigations, anomalies occur
Fig. 2. The developmental pathways of physical science according to Kühn.
2312
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
or results from unrelated scientific efforts are reported. Thesegive rise to doubt regarding the merit of the paradigm. Theawareness by paradigm adherents that "something has gonewrong" results in a crisis, which precedes a scientific revolution.
Kühnuses the term revolution because of the similarities between the conditions that exist before scientific upheavals andthe circumstances that precede political revolutions. In thelatter, one segment of society defends the status quo, anotherattempts to introduce a new order, and society is not governedat all. A similar circumstance occurs in scientific revolutions.When one paradigm competes with another, individuals expresstheir uncertainty, discontent, and disillusionment by displayinga willingness to improvise, by trying strategies that may havepreviously been considered inappropriate, and by engaging inendless debate.
The process of paradigmatic change is repetitive. While it isunlikely that one paradigm will ever be completely acceptedbefore another takes its place, a scientific community can begoverned by only a single paradigm. To reject one is a decisionto accept another. To reject one without substituting another isto reject science itself, since a paradigm is based on science andto acknowledge a change in science without accepting theparadigm that arose from that change is illogical. These truismsaccount for much of the perceived confusion that exists inbreast cancer management.
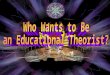
Despite his emphasis on the importance of scientific achievement in the development of a paradigm, Kühnfails to considerhow historic scenarios depicting the scientific method relate tothe science that inspires the paradigm. Although it might beinappropriate to consider such a connection in the physicalsciences, there is justification for noting such an association inthe biological sciences, particularly in medicine. Because aparadigm governs the activity of the members of a given [scientific] community, it is important to examine its origins inorder to estimate the credibility of the science that went intoits construction (Fig. 3). Was that science a product of inductivereasoning, as described by Francis Bacon in the early seventeenth century and John Stuart Mill in the nineteenth, or wasit the result of hypothesis-testing by rigorous experimentation,i.e., deduction, as advocated by Claude Bernard over a hundredyears ago? The late Sir Peter Medawar aptly stated, "Inductionis the arguing from the particular to the general" (13). It is a
scheme of reasoning in which ideas, observations, results ofexperiments, and anecdotal experiences give rise to generalstatements that do more than summarize the information imparted by the data; according to Medawar, "it expands ourpretensions to knowledge" (13). In the view of the inductivist,
this enlargement of experience leads to an enlargement ofunderstanding. Such a misconception continues to plague physicians who attach more significance to anecdotal experiencethan is justified.
Bernard, the French physiologist who focused attention ondeductive scientific research, wrote: "A hypothesis is ... theobligatory starting point of all experimental reasoning," and he
insisted that a hypothesis is of value only if it can be tested(14). Such testing must be carried out by appropriate experiments conducted in the laboratory or, more recently, withinrandomized clinical trials. These mechanisms provide information that can lead to rejection, modification, or support ofthe hypothesis. The greater the number of investigations thatsupport a hypothesis, the more credible it becomes and themore likely that a new paradigm will result. More attentionmust be given to the results obtained from testing a hypothesis
•¿�DEDUCTION"
NON TESTABLE |
H TESTABLE I
I EXPERIMENTALMETHODOLOGY]"' '
CLINICALTRIALS
INFORMATION TO:•¿�REJECT•¿�MODIFY
Fig. i. The inductivist and deductivist origins of past and present breast cancerparadigms.
than to the plethora of anecdotal reports of inductivist-gener-ated findings, which result only in clinical confusion.
It is important to point out that one of the major deficienciesin our knowledge of breast cancer relates to the fact that somuch of how the disease is perceived comes from informationon demographics, natural history, biology, and treatment obtained from patients with tumors large enough to be detectedby clinical examination and by mammography, i.e., those withend-stage or near end-stage disease (Fig. 1, A and B). Becausestudies designed to test the hypotheses upon which currentparadigms are based were conducted almost exclusively inwomen with disease at that stage, these paradigms govern thetreatment of women with clinically detectable cancers.
With the above information as background, it is appropriateto examine how the Kuhnian pathway relates to the evolutionof paradigms that currently govern the management of breastcancer.
Paradigms Governing Breast Cancer Management
The First Surgical Paradigm. This paradigm originated whenWilliam S. Halsted combined the features of various operationsdevised in the late eighteenth century (15) into one operationthat became known in 1890-1891 as the Halsted radical mastectomy (16-19). Evidence indicating the success ofthat operation was derived over the next half-century from anecdotalreports of observational information, i.e., Baconian inductiv-ism. Halsted's writings indicate, however, that there may have
been some biological justification for his efforts. He was influenced by W. Sampson Handley, who contended that cancer ofthe breast spread by extension along lymphatic pathways, preserving continuity with the original growth (20). Handley believed that tumor permeated, not metastasized to, distant sitessuch as bone, that the bloodstream was of little significance asa pathway for métastases,and that regional lymph nodes werean effective barrier to the passage of tumor cells (21).
The anatomical and mechanistic basis for Halstedian cancersurgery gave rise to the "proper" cancer operation, which con
sisted of removing a primary tumor, regional lymphatics, andlymph nodes by en bloc dissection—the hallmark of the operation. Because cancer was believed to be a local-regional disease,it was considered more curable if the surgeon was more expansive in his interpretation of what constituted the "region."
Moreover, this concept was time-oriented, and the management
2373
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
of breast cancer was an "emergency." The concept gave rise to
the Halstedian paradigm, which, for almost a century, governedthe management not only of breast cancer but of most solidtumors as well (15).
It is appropriate to designate Halsted's efforts as a paradigm
as defined by Kühnbecause it arose from beliefs, techniques,and achievements that attracted an ever-widening group ofadherents. It became universally accepted because of lack ofcompetition and because proponents indoctrinated succeedinggenerations, who adopted it without qualification. It is notsurprising that it remained intact for a protracted period despitewhat, in retrospect, might be viewed as weakness in its scientificorigins.
The Halstedian paradigm provided an abundance of problemsto be resolved. Normal science flourished. Almost all effortswere directed toward formulating a more precise definition ofthe operative procedure (15). Arguments, still considered respectable today in some circles, related to how thin skin flapsshould be, how extensive an axillary dissection should be carriedout, and whether supraclavicular and/or internal mammarynodes should be removed. Expansion of the operation was inkeeping with the hypothesis. Super-radical surgery, more adequately than the radical mastectomy, embodied the principleson which the hypothesis was based. Aside from the fact thatmore expansive operations neither provided a basis for challenging Halsted's principles nor aided in the understanding of
the disease, the technical aspects of the operation were beyondthe average surgeon, since he was without the support systemsnecessary to perform them. For these reasons, super-radical
surgery did not attract enough converts and, thus, failed toreplace radical mastectomy.
The Halstedian paradigm also dictated radiation therapy. Itwas believed that, because residual tumor cells could be destroyed by radiation therapy, regional irradiation followingmastectomy had a greater likelihood of effecting a cure thandid mastectomy alone. Less extensive operations, such as mod-ified-radical and simple mastectomy, followed by irradiation,were done because some believed that they better fulfilledHalstedian principles or because of frustration with the inabilityof radical mastectomy to cure more patients. The same dissatisfaction provided a rationale for performing breast-conservingoperations followed by irradiation. Sporadic reports demonstrated that patients could, indeed, survive disease-free for manyyears after breast-preserving surgery. However, because thepractice of local tumor excision was not based upon any newbiological principles, because no studies had been conducted tocompare the merits of this operation with more radical procedures, and because proponents of the Halstedian paradigmcould see no reason to replace the mastectomy with it, breastconservation failed to receive adequate support.
As in the first half of the twentieth century, normal sciencebetween 1945 and 1970 was concerned primarily with "fine-tuning" the Halstedian paradigm (15). New principles of host
and tumor biology were noticeably absent (the concept of breastcancer as a systemic disease remained obscure), and, as a result,no new exemplar surfaced to attract a sufficient number ofsurgeons away from the Halstedian paradigm. Disagreementsthat occurred among disciples of the same paradigm wererelated not to the paradigm itself but to variations in nuancesof treatment proposed to strengthen it. When the era is viewedin retrospect, it appears that the Halstedian paradigm persistedso long because the normal science associated with it failed to
answer all of the questions it posed and because no anomaliesarose to challenge its tenets.
Origin and Development of the Current Surgical Paradigm. Ifthe first surgical paradigm was related to tumor growth andspread, new knowledge questioning that facet of tumor biologymight have been expected to challenge the reigning paradigm.Such was, indeed, the case. During the 1950s and 1960s, newperceptions of metastatic mechanisms arose. Our contributions,as well as those of others, led us to formulate a new hypothesisregarding tumor métastasesand to test our theory in severalclinical trials.
When we began our studies in the late 1950s, the prevailingtheory was that lymph-borne tumor cells had one destination—the lymph nodes—that tumor cells in the blood vascular systemlodged in the first capillary bed they encountered, and thattumor cells disseminated in an orderly pattern based upontemporal and mechanical considerations. Our findings 26 yearsago indicated that the blood and lymphatic systems are sointerrelated that it is impractical to consider them as independent routes of neoplastic dissemination, a major departure fromthe theory of tumor cell dissemination at the time (22, 23). Weproposed that métastasesare not dictated only by anatomicalconsiderations but are, instead, influenced by intrinsic factorsin tumor cells and by the organs to which they gain access, athesis supported and broadened by recent expansion of knowledge in molecular biology. Consequently, we proposed thattumor cells are not spread in an orderly pattern, a theorycontrary to that which provided the basis for the Halstedianparadigm.
Our experiments reported in 1966 revealed for the first time(24) that RLNs3 are not an effective barrier to tumor cell
dissemination, as Virchow proposed in 1863 (21). In the 1960swe adopted the thesis that the RLN is an indicator of host-tumor relations and that negative nodes reflect conditions thatinhibit the occurrence of métastaseselsewhere, whereas positivelymph nodes indicate an interrelationship between host andtumor that permits the development of distant métastases.Thus, RLNs are not the instigators of distant disease. Toconsider RLNs merely as mechanical receptacles for tumorcells and way stations for further dissemination is an anachronism (25, 26).
Our findings failed to coincide with the prevailing theory ofmetastatic mechanisms that provided justification for the Halstedian paradigm. Consequently, based on our concept of tumordissemination, which differed from that of Halsted, we formulated a hypothesis proposing a biological basis for breast cancertreatment that was antithetical to the mechanistic principlesupon which surgery and radiation therapy were based (27). Ourhypothesis contends that operable breast cancer is a systemicdisease involving a complex spectrum of host-tumor interrelations and that variations in local-regional therapy are unlikelyto affect survival. Unlike Halsted's, our theory is not time
oriented. (Although many of these concepts may be self-evidenttoday, such was not the case in the 1950s and 1960s.)
As noted, hypothesis-testing is an integral facet of the scientific method and is necessary in order to support or reject atheory. While the Halstedian hypothesis was accepted withoutsuch testing, we have had the opportunity to conduct twoclinical trials not only to obtain data regarding the credibilityof our hypothesis but also to provide information regarding the
3The abbreviations used are: RLN, regional lymph node; NSABP, National
Surgical Adjuvant Breast and Bowel Project; IBTR. ipsilateral breast tumorrecurrence; ER, estrogen receptor; DCIS. duct carcinoma in situ.
2374
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
justification for continuing to use Halstedian principles ofcancer surgery. The first trial (NSABP B-04), implemented in1971, evaluated the outcome of patients having invasive breastcancer and no clinical evidence of axillary node involvement.In that trial, almost 1700 women were randomized among threedifferent treatment regimens: conventional Halstedian radicalmastectomy, total (simple) mastectomy with local-regional irradiation but no axillary dissection, or total mastectomy withno irradiation and removal of axillary nodes only if they becameclinically positive. The significant aspect of that study was that40% of the patients treated by radical mastectomy had histo-logically positive nodes. Thus, about 40% of those in the othertwo groups had positive axillary nodes that were not removed.Despite the therapeutic nonconformity and the fact that positivenodes were unremoved, no significant difference in overalltreatment failure, distant metastasis, or survival was notedamong the three groups after more than 14 years of follow-up(28-30). These findings supported our alternative hypothesisand corroborated our long-held contention that tumor-bearingnodes are "indicators," not "instigators," of metastatic disease.
Because the findings from B-04 negated the radical mastectomy and its principles, they provoked uncertainty about themerits of the Halstedian paradigm as an exemplar for breastcancer therapy and, thus, provided the impetus for a Kuhniancrisis, which resulted in aberrant responses among disciples ofthe Halstedian paradigm. Of primary importance, the findingseliminated most of the biological considerations that mighthave contraindicated evaluating breast-conserving operations.Until that time, any justification for breast preservation hadbeen based upon arguments derived from anecdotal experiences.
To reevaluate our hypothesis and, at the same time, appraisethe worth of lumpectomy and axillary dissection, we initiated asecond trial (NSABP B-06) in 1976. In that study, nearly 2000women were randomly assigned to total mastectomy, lumpectomy alone, or lumpectomy followed by breast irradiation. Allhad axillary dissection. After more than 9 years of follow-up,despite the fact that 43% of the women treated by lumpectomywithout breast irradiation and 12% of those who underwentlumpectomy and breast irradiation experienced an IBTR, therewas no significant difference in distant disease-free survival orsurvival among the three groups (31, 32). (Obviously, none ofthe women treated by total mastectomy had an IBTR.) This ledto the conclusion that no causal relation exists between anIBTR and distant disease or survival, a finding similar to thatdescribed for axillary node involvement in B-04. Most important, the B-06 findings further supported the biological principles that had resulted in the formulation of the alternativehypothesis and provided justification for lumpectomy. Becauseof these changes, even more physicians began to doubt the meritof the Halstedian paradigm. Thus, the crisis that arose afterpublication of the B-04 findings expanded and became a Kuhnian revolution. A réévaluationof prior fact had necessitated arestructuring of prior theory.
With the erosion of the Halstedian paradigm, many of itsdisciples (as well as those yet uncommitted to any paradigm)accepted the validity of the B-04 and B-06 findings, and a newparadigm for the management of breast cancer evolved. Evidence to indicate that it has become established is inherent inthe statement issued after a NIH consensus conference in June1990, when it was concluded that breast preservation is thepreferable treatment for women with stages I and II breastcancer (1). To use Kuhn's analogy, it would seem that those
currently governed in their treatment of breast cancer by the
Halstedian paradigm are being ruled by the science of a previousera. In that regard, it is important to emphasize that thelumpectomy is an operation that has abandoned every principleof the Halstedian paradigm. In the lumpectomy, the surgeonremoves only an amount of normal breast tissue necessary toprovide tumor-free specimen margins as demonstrated by thepathologist. The aim is to ensure that gross tumor is not leftunremoved. A lumpectomy is completely different from a quad-rantectomy. The latter is a procedure that continues to embodythe principles of the Halstedian paradigm, i.e., it employs enbloc dissection and removal of the pectoralis minor muscle andfascia (33). It is either an effort to compromise by using principles of both paradigms simultaneously, which is antitheticalto Kuhn's principle that a scientific community can be governed
by only a single paradigm, or it is a procedure aimed at fine-tuning the Halstedian paradigm.
The new breast cancer paradigm has introduced a new set ofproblems requiring resolution to strengthen its tenets. Normalscience has become active. Technical questions about how muchnormal breast should be removed in a lumpectomy, whetherbreast irradiation is necessary for all patients, whether certaintumor characteristics or host factors preclude the conduct of alumpectomy, and whether systemic chemotherapy will reducethe incidence of postlumpectomy breast recurrence have become the object of study. Differences that have occurred instudies conducted to resolve these issues are not to be construedas uncertainties regarding the credibility of the paradigm.
A recently conducted investigation, which is part of thenormal science associated with the new paradigm, has producedimportant findings regarding the significance of an IBTR following lumpectomy (32). This study was carried out to addressthe reluctance of many physicians to accept the lumpectomy.Despite the similarity in distant disease-free survival and survival between lumpectomy and mastectomy patients, manyphysicians feared that patients treated by lumpectomy whosubsequently developed an IBTR would be at increased risk fordistant métastasesbecause any tumor that might not be removed during the primary operation would grow and disseminate cancer cells during the time between the operation andrecognition of the IBTR. (These physicians are still disciples ofthe Halstedian paradigm.) Our findings, recently reported, indicate that, with the diagnosis of an IBTR after lumpectomy, apatient is, indeed, at increased risk for distant disease (3.41times greater) than she was before the IBTR was recognized,but this increased risk is not because of disseminated tumorcells that could have been avoided had a mastectomy beenperformed. An IBTR is a marker of a risk for distant diseasepresent at the time of primary tumor removal, and that riskwould have been the same even if radical surgery had beencarried out initially. Mastectomy or breast irradiation afterlumpectomy eliminates or reduces the opportunity for identification of a marker of risk (an IBTR) for distant disease butdoes not reduce the development of distant disease. The relationship of an IBTR to distant metastatic disease is analogousto that of a woman without breast cancer who learns on oneparticular day that her sister has been diagnosed with thedisease. On that day, the "normal" sister becomes at greater
risk for developing breast cancer than she was the day before,even though her increased risk existed before her sister's diag
nosis. Thus, although mastectomy and breast irradiation following lumpectomy prevent expression of the marker, they do notlower the risk of distant disease any more than treating thesister who has breast cancer with an effective preventive agent
2375
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
before she develops the disease would eliminate the risk ofbreast cancer in her normal, untreated sibling. The results ofthis study strengthen the paradigm by providing informationthat confirms the biological nature of breast cancer—particularly as local recurrence relates to metastatic disease—andsupport our theory proposed more than two decades ago. Moreover, they continue to justify lumpectomy.
In this section, I have demonstrated how a paradigmatic shifthas occurred in breast cancer management. I have indicatedhow laboratory research in the biology of metastasis gave riseto a hypothesis that was tested by clinical trials and how thefindings from these endeavors refuted the principles that resulted in a paradigm that governed breast cancer managementfor more than three-quarters of a century. With a shift in thesurgical paradigm and an increasing awareness over the pasttwo decades that the curability of breast cancer relates to moreeffective systemic therapy, greater emphasis has been given tothe use ofthat modality. The current systemic therapy paradigmhas evolved in a manner similar to that described for the surgicalparadigms.
Origin and Development of the Current Systemic TherapyParadigm. Observations in the mid-1950s indicated that cancercells could be found in the circulating blood during surgicalremoval of tumors (34) and that chemotherapeutic agents hada cytotoxic effect on disseminated tumor cells in experimentalanimals (35). These findings led to the hypothesis that adjuvantchemotherapy would lower tumor recurrence and improve thesurvival of breast cancer patients. That hypothesis was firsttested in a clinical trial begun by the NSABP in 1958. Thepremise of this trial was that chemotherapy administered duringand for a short period after operation would destroy tumor cellsdisseminated as a result of the surgery. Although study resultsdemonstrated both a decrease in tumor recurrence and animprovement in survival of premenopausal, node-positive patients after 10 years of follow-up, disappointment with theoverall findings led to the conclusion that the hypothesis hadnot been supported (36). Consequently, aside from a few exceptions, practitioners were not attracted to systemic adjuvanttherapy, and, therefore, no paradigm arose to govern its use.Nevertheless, the observations obtained from this trial areimportant. They provided the first evidence that the naturalhistory of breast cancer could be perturbed by adjuvant chemotherapy and that there were differences in the response ofpatient cohorts to a therapy—a prediction of future findings.Subsequent events revealed that the original hypothesis wasvalid but that the premise upon which the trial was based wasinappropriate. The eradication of surgically disseminated tumorcells was probably less important than the response of existingmicrometastases to cytotoxic agents.
Mendelsohn in 1960 (37) and Skipper and associates in theearly 1970s (38-40) defined the concept of a growth fraction ina tumor cell population and provided an array of tumor growthkinetic principles that were instrumental in formulating a hypothesis that postulated the value of adjuvant chemotherapy.The first trial to evaluate adjuvant therapy and to test thishypothesis was begun by the NSABP in 1971. In that study, L-
phenylalanine mustard was administered after radical mastectomy to patients with positive axillary nodes. The results,reported in 1975, indicated that such therapy could alter thenatural history of patients with primary breast cancer (41). Thatconclusion was confirmed by findings from the Milan study,carried out by Bonadonna and associates using cyclophospha-mide, methotrexate, and 5-fluorouracil (42). Both trials lent
support to the hypothesis regarding the use of adjuvant therapy.As a consequence, a new paradigm governing the managementof breast cancer arose. Treating patients who were free ofidentifiable metastatic disease with systemic adjuvant therapybecause some of them might develop distant disease in thefuture was a revolutionary departure from prior treatmentstrategy and became a new exemplar.
Further support for the validity of the systemic therapyparadigm was provided by investigations demonstrating theefficacy of the nonsteroidal antiestrogen tamoxifen (43-52).Subsequent to extensive study of that drug in experimentalsystems, and following its demonstrated benefit in patients withmetastatic breast cancer, clinical trials were undertaken inEurope and the United States to evaluate tamoxifen alone orin combination with chemotherapy for the treatment of stagesI and II breast cancer. Two British randomized trials comparedthe outcome of patients receiving no systemic therapy with thatof those receiving tamoxifen (43,44). By indicating that tamoxifen has an overall advantage that is independent of nodal,menopausal, or ER status, findings from both trials aided instrengthening the paradigm.
Normal science flourished. Laboratory and clinical investigations were undertaken to answer questions about the use ofsystemic therapy. Clinical trials have been conducted to compare treatment regimens; to define optimal duration of therapyand/or drug dose; to evaluate timing and routes of drug administration; to determine the relation of host and tumor factors(e.g., age, tumor size, hormone-receptor content, tumor growth
kinetic characteristics, markers of gene expression, and histológica!type) to therapeutic response; and to assess the effect ofchemotherapy in conjunction with other modalities (radiationtherapy, hormonal agents, and biological response modifiers).As a result, information has accumulated which, on occasion,has resulted in disagreement and even confusion among physicians who treat breast cancer patients. It is often not appreciatedthat these responses are not the result of anomalies that weakenthe credibility of the paradigm but, rather, the consequence ofinvestigations conducted to strengthen it. Evidence to indicatethat the systemic therapy paradigm is firmly entrenched is bestexemplified by the results obtained from systematic overviewsof findings from multiple trials (meta-analyses) (51) and byconclusions from several consensus conferences conducted bythe NIH.
NIH consensus conferences held in 1985 (53) and 1990 (1)lent support to the paradigm when they concluded that adjuvantchemotherapy and hormonal therapy are effective treatmentsfor breast cancer patients. Considerable evidence was providedto justify the use of chemotherapy in premenopausal and post-menopausal patients who were node-negative and had ER-negative tumors. Premenopausal and postmenopausal womenwith node-negative, ER-positive tumors also benefited fromtamoxifen. It was recommended that established combinationchemotherapy be used for the treatment of premenopausalwomen with positive nodes, regardless of their tumor hormonereceptor status. For postmenopausal women with positive nodesand positive tumor hormone receptor levels, tamoxifen hasbecome the treatment of choice. Recently, however, the additionof chemotherapy to tamoxifen has been found to be moreeffective than tamoxifen alone in postmenopausal patients withpositive nodes and ER-positive tumors (54). Chemotherapy hasbeen recommended for the treatment of postmenopausal patients with positive nodes and ER-negative tumors. An overviewof 61 randomized trials among 28,896 women conducted by
2376
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
the Early Breast Cancer Trialists' Collaborative Group dem
onstrated reductions in mortality due to treatment when ta-moxifen was compared with no tamoxifen or when any chemotherapy was compared with no chemotherapy (51).
Although adjuvant therapy has not cured all patients—oreven all patients within a defined cohort—and is often accompanied by toxicity, there have been sufficient benefits to justifyits use. Until new modalities demonstrate greater efficacy, it isappropriate to treat patients according to the current systemictherapy paradigm. As previously noted, to abandon the paradigm without a replacement is to abandon science. Currentdissatisfaction with the use of systemic therapy is similar tothat expressed in the era of the radical mastectomy and to thatnow being voiced by some regarding lumpectomy.
In summary, the treatment of breast cancer is currently beinggoverned by two independent paradigms. One is concerned witheradicating local manifestations of the disease without compromising prospects for cure while maintaining the best possiblecosmesis. The other serves as the exemplar for the eradicationof systemic disease.
It is highly unlikely that either paradigm will endure for aprotracted period of time. Laboratory and clinical research isexpanding knowledge so rapidly that the half-life of permanency is becoming shorter and shorter! The following sectionis a commentary on current investigative efforts that have thepotential for either altering currently entrenched paradigms orfor creating new paradigms for breast cancer management.
Preludes to New Paradigms
One pathway of current breast cancer investigation relates tothe development of progressively more effective regimens forthe treatment of clinically detectable disease. New therapeuticmodalities such as taxol (a complex natural product derivedfrom the bark of the Pacific yew tree), antigrowth factors,immunomodulators, or tumor-infiltrating lymphocytes mayone day require evaluation by means of large clinical trials (55).Tumor-infiltrating lymphocytes, for example, may be used tointroduce cytotoxic agents like tumor necrosis factor directlyto tumor cells or to genetically alter tumor cells in order tosuppress their growth. Such approaches may be tested alone orin conjunction with current and new chemotherapeutic agentsand hormonal therapies of proven value. Studies evaluatingmethodologies for overcoming drug resistance and for modulating the action of chemotherapeutic agents based upon pharmacological principles are in progress, as is the testing ofcurrently available modalities in novel ways. Examples of thelatter are two interrelated NSABP trials now under way; oneevaluates the worth of preoperative (neoadjuvant) chemotherapy, and the other tests the worth of dose intensification and/or increased total dose of chemotherapy. Findings from thesestudies could result in another paradigmatic shift—the creationof a unified paradigm—which could profoundly alter currentbreast cancer management.
The Creation of a Unified Paradigm. In 1975, after demonstrating that adjuvant chemotherapy was effective in eradicatingoccult distant métastases,we conjectured that the use of suchtherapy would permit less extensive surgical procedures (56). Itseemed reasonable to predict that, as systemic therapy improved, the surgical and adjuvant chemotherapy paradigmswould eventually unite and become a single "unified" exemplar
and that surgery, as a result, would partially or even completelydisappear from use.
By 1987, clinical information and several hypotheses derivedfrom biological studies provided justification for the conduct ofa trial (NSABP B-18) to evaluate the worth of preoperative
chemotherapy for the treatment of stages I and II breast cancer.Almost all of the clinical findings have come from the use ofsuch therapy in the treatment of head and neck tumors (57),esophageal tumors (58), osteosarcoma (59), and locally advanced (stage III) breast cancers (60). Of particular importancewas the National Cancer Institute study in stage III breastcancer patients treated with a complex preoperative chemotherapy regimen (61). A complete response occurred in 50%and a partial response in 40% of breast tumors. (The study wasconducted not to evaluate preoperative chemotherapy but toascertain the value of cell synchronization in conjunction withchemotherapy.) Several groups of investigators have evaluatedor are investigating preoperative therapy in patients with operable (stages I and II) breast cancer (62-64). In the Milanstudy (64), which was not a randomized trial, preoperativechemotherapy was administered to women with breast cancerwho were candidates for mastectomy because the largest diameter of their tumors was >3 cm. The aim was to reduce thesize of the tumors so that these women might be treated bybreast conservation instead of mastectomy. Sufficient "tumorshrinkage" was reported to have occurred in 127 of 157 women,
allowing for breast preservation. It is of interest that 79% ofthe patients had tumors <5 cm, a size that, according to NSABPcriteria, would have made them initially eligible for lumpectomy. This study, and all others using preoperative chemotherapy, failed to determine whether such therapy more effectivelycontrols disseminated disease than does the same therapy administered postoperatively.
One of the hypotheses that justified our study relates toconcepts promulgated by Skipper in the 1970s (38-40); amongthese were propositions suggesting that responses of primaryand metastatic tumors to chemotherapy may differ. None ofthe numerous trials conducted since that time were designed toconfirm or reject the tenets of the Skipper hypothesis. If theprinciples of this hypothesis are supported by our study, failureto observe a complete or partial primary tumor response tochemotherapy may not necessarily portend a lack of control ofdistant disease.
Another theory that provides a biological rationale for evaluating preoperative therapy was formulated from findings obtained in experimental systems which indicate that primarytumor removal affects the growth kinetics of métastases.Ourinvestigations and those of others have demonstrated that, afterremoval of a primary tumor, an increase in the labeling indexof a distant tumor focus occurs, resulting in an increase intumor size (65). We have determined that the stimulation ofcell growth after removal of the tumor is due to the presence ofa serum growth factor (66) and that chemotherapy, tamoxifen,or radiation therapy given before the operation prevents thekinetic perturbation (67). Consequently, these agents moreeffectively suppress tumor growth and prolong survival thanwhen they are administered after removal of the tumor.
A third hypothesis providing justification for testing preoperative chemotherapy proposes that, as a tumor cell populationincreases, an ever-expanding number of drug-resistant pheno-typic variants that are more difficult to eradicate arise due tospontaneous mutation. This thesis maintains that the increasein resistant cells can be minimized by administering combinations of non-cross-resistant drugs as soon as possible, i.e., whena tumor population contains the fewest number of cells (68).
2377
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
As a result of these hypotheses and the available clinicalinformation, in October 1988, the NSABP implemented a study(B-18) to determine whether (a) preoperative chemotherapywill more effectively prevent tumor recurrence and prolongsurvival than does the same therapy administered postopera-tively, (b) the primary tumor response to preoperative chemotherapy correlates with the prevention of recurrence and prolongation of survival, (e) preoperative chemotherapy will permitmore conservative surgery and decrease the incidence of IBTRfollowing lumpectomy, and (d) downstaging of axillary nodalstatus will occur. More than 1100 patients with operable breastcancer, all diagnosed by fine-needle aspiration or core biopsy,have been randomized to receive either operation followed bysystemic therapy or the same systemic therapy followed byoperation. It is our view that, until information from this oranother large trial indicates that local-regional disease benefitsfrom the use of preoperative therapy are not accompanied byan unfavorable distant disease-free survival and/or survivaloutcome, this therapeutic approach should be limited to theclinical trial setting.
The second study conducted by the NSABP that has implications for creating a unified paradigm was designed to determine whether intensifying and/or increasing the total dose of ademonstrated effective postoperative chemotherapy regimenwill more effectively eradicate distant disease. In that trial, inorder to use higher doses of drug, colony-stimulating factor is
used in conjunction with the chemotherapy. If a greater benefitis obtained using high-dose therapy than has been observedfollowing current "standard" doses of the same therapy, the
high-dose regimen will be administered preoperatively. If, as aconsequence, a substantial number of patients show a reductionin primary tumor size and an improvement in distant disease-free survival and survival, a new paradigm, which unifies thetreatment of local, regional, and systemic disease, is likely tobecome established. Even if a decrease in primary tumor size isunaccompanied by an improvement or a deficit in distant disease-free survival or survival, preoperative therapy would bejustified if its administration permits the use of less extensivesurgical procedures. In those cases where clinical and mammographie examinations indicate that preoperative chemotherapy has completely eradicated a primary tumor, breast irradiation without surgery after completion of the chemotherapy maybe adequate to prevent breast tumor recurrence.
Despite its demonstrated benefit, how durable is a singleparadigm for breast cancer management that advocates preoperative therapy? As more women are examined periodicallywith better mammographie equipment, more tumors will beidentified when they are even more occult than those currentlybeing detected. Consequently, fewer women will have cancersfor which the paradigm dictating the use of preoperative therapyapplies. Because the natural history of patients with occulttumors is uncertain, it is also unclear (although probably unlikely) whether systemic therapy, as it is currently used, shouldbe used in their treatment. On the other hand, occult tumorsmay be the ones that can be cured in all instances by suchtherapy. Despite this uncertainty, the surgeon's role in the
management of such patients will diminish and may evenbecome obsolete. It is likely that the paradigm that will governthe management of such lesions will be dominated by theradiologist, who detects the lesion, localizes it, removes cellsfor cytological examination, and who, subsequent to pathological examination, destroys it by a procedure such as lasertherapy applied directly to the site of the lesion.
The Creation of a Paradigm for the Treatment of NoninvasiveCancer. Because, as has already been indicated, almost allknowledge about invasive and noninvasive breast cancer has,until recently, been obtained from patients with clinically detectable tumors, physicians are at a disadvantage when calledupon to make decisions about the management of occult cancers, particularly those that are noninvasive. The present confusion about how best to treat DCIS is due to the fact that thereis insufficient biological and natural history information toformulate a paradigm that governs the treatment of the type ofDCIS currently being detected with increasing frequency bymammography. The Halstedian paradigm is inappropriate, andthe new surgical paradigm advocating lumpectomy has not beenfully accepted. As Kühnindicates, when such a situation occurs,anarchy is apt to exist. It is not uncommon for a patient withDCIS to receive diverse recommendations for her treatmentthat range from unilateral or bilateral mastectomy with orwithout axillary dissection to lumpectomy with or withoutbreast irradiation. An incongruous situation has resulted.Whereas mastectomy is becoming less justifiable for treatmentof invasive breast cancer, it is more often advocated for DCIS,the rationale being that the operation performed to preventinvasive breast cancer should be more radical than surgeryperformed to "cure" the disease. The turmoil regarding therapy
is related to the absence of definitive information about thefrequency of synchronous or metachronous multicentricity ormult ¡locality(in situ or invasive) in the ipsilateral or contralat-eral breast associated with DCIS. In addition, it remains uncertain how frequently multicentric or multifocal lesions becomeclinically significant, whether DCIS is an obligatory preliminarystep in the development of invasive cancer, and whether allDCIS becomes invasive. Should the progression from DCIS toinvasive cancer relate to somatic genetic events, as is currentlyspeculated, it becomes important to determine whether thechanges can be monitored by any method other than histopa-thology, e.g., oncogene expression.
In 1985 we instituted a clinical trial to obtain natural historyinformation that might address some of these issues. A secondary objective of the study was to test the hypothesis that, inpatients with localized DCIS which can be completely removedby lumpectomy, the addition of postoperative breast irradiationwould effectively prevent recurrence of the disease. While thereis currently no definitive information to indicate that breastirradiation either does or does not effectively eradicate DCIS,there is indirect evidence from a variety of sources (69-74) toindicate its possible value.
After that study completed patient accrual, a second trial wasinstituted using women with more extensive DCIS than that inwomen who were entered into the first study. That trial wasconducted to test a hypothesis that relates to the prevention ofipsilateral invasive breast cancers subsequent to treatment ofDCIS by lumpectomy. The purpose for treating local or diffuseDCIS is to prevent such a lesion from progressing to invasivecancer and to eliminate a focus of invasive cancer that mightexist in conjunction with the DCIS. Although mastectomyeffectively accomplishes that goal, other strategies used withbreast conservation may be equally effective. Because breastirradiation following lumpectomy for invasive cancer effectivelyprevents its recurrence, and because tamoxifen likewise interferes with the development of invasive cancer in both theipsilateral and contralateral breast, these modalities, used withbreast conservation, may have a place in the management ofDCIS, particularly in patients with extensive disease.
2378
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS KOR THE MANAGEMENT OF BREAST CANCER
Because experimental evidence supports the thesis that ta-moxifen possesses both antiinitiator (75) and antipromotercapabilities (76, 77), that drug may inhibit the progression ofDCIS to invasive cancer. Recent evidence that tamoxifen maypossess antiangiogenesis properties may be important, since itis postulated that angiogenesis is required for the progressionfrom noninvasive to invasive breast cancer (78). Thus, thehypothesis that governs our second study relates to the thesisthat, with the use of tamoxifen and radiation therapy foreliminating associated invasive cancer, the clinical significanceof DCIS may become similar to that of atypical hyperplasia orto that of a woman with a family history of breast cancer.
The findings from both of these studies are likely to providethe basis for formulating a paradigm to govern the treatmentof DCIS. Until then, it seems appropriate that the surgicalparadigm associated with the use of lumpectomy for the treatment of invasive breast cancer should govern the managementof this disease.
Comments Regarding the Mammographie Detection of Occult,Invasive Breast Cancer. As has already been pointed out, oneprincipal research strategy directed at making breast cancer aless significant public health problem is aimed at devisingprogressively better regimens for the systemic treatment ofclinically detectable disease. Another strategy is directed towardthe identification of a greater number of nonclinically detectable, phenotypically expressed, occult, invasive breast cancers bymore widespread mammographie screening with the best methodology currently available. This approach should result notonly in an increased incidence of breast cancer but also in achange in the distribution of the size of tumors that are discovered; i.e., the percentage of small cancers will increase. If currentthinking is correct, patients with tumors detected by mammog-
raphy before their clinical appearance should be more curableafter their tumors are removed. Theoretically, as this strategycomes closer to achieving its goal, the first strategy becomesless important, and—taken to the extreme—obsolete, sinceclinically detected tumors would no longer exist. Current biological concepts indicate, however, that as a result of geneticalteration some occult tumors detected by mammography havepopulations of cells that have already attained competence forsuccessfully establishing métastases,have not yet achieved thatcapability but will do so as their cells continue to replicate, orwill never demonstrate that capacity, even after they are detected by clinical examination. (A substantial proportion ofpatients with clinically detected cancers do not develop met-astatic disease during their lifetime.) Thus, if current conceptsare correct, it would seem that the value or limitations ofmammography relate not so much to the number of clinicallyoccult tumors detected as to the biological nature of the cellsin the tumors that are discovered. Perhaps, with more diligentuse of better methodology than is now available, it will bepossible to detect and remove more tumors whose cells havenot yet undergone the biological changes required for them toattain the metastatic capability that would occur if the tumorswere not recognized and not removed.
Pragmatic concerns exist about the extent to which mammography as an independent intervention is likely in the nextdecade or so to become the paradigm for eliminating breastcancer as a major health problem. Despite extensive encouragement of women to have mammograms, it is estimated that, inthe United States, of the new patients diagnosed with invasivebreast cancer in 1990, only 50% had stage I disease, whereas20-25% demonstrated stage II and 20-25% stage III cancers—
hardly a testament to the current impact of mammography ( 1).Another concern is that, after the removal of mammographi-cally diagnosed tumors too small to be detected clinically,women will be at increased risk for the development of secondbreast cancers and, thus, require continued surveillance. Mostfrustrating is the realization that organized mammographieprograms with sophisticated equipment used on a regular basisby well-trained personnel are unlikely to be available to asubstantial number of women in this country. The hundreds ofthousands of women worldwide who live with and die of breastcancer treated either in the most rudimentary way or not at allbecause they lack access to health care are unlikely to bebenefactors of mammography. These comments are not to beinterpreted as criticisms of mammography; indeed, muchgreater effort must be directed toward promoting it. Such effortis justified, however, only if systems are available to properlytreat women who have abnormalities detected as a consequence.
As is shown in Fig. 1, there is a time when a phenotypicallyexpressed breast cancer exists prior to its detection and, evenbefore that, a time when cancer as we recognize it has notoccurred, even though the molecular-genetic components forsuch an event may exist. Neither the two research strategiesdiscussed herein nor current paradigms governing breast cancerare apt to be relevant for patients with either biological oroccult, nondiagnosable cancers.
A third investigative approach that might be contemplated isone directed toward devising strategies capable of interferingwith the initiation and/or the growth (promotion) of breastcancers so that they never become clinically or mammographi-cally evident. Is now the time to consider implementing such astrategy? If so, has enough experimental and clinical information been obtained to justify formulating a hypothesis that canbe appropriately tested and that, if supported, could give riseto a new paradigm—one that relates to prevention of thedisease? The following section of this essay considers thesequestions.
The Origins of a Breast Cancer Prevention Paradigm. Thereis a consensus that enough information from laboratory andclinical investigations is available to permit the formulation ofa hypothesis which contends that an appropriate intervention(such as a low-fat diet, retinoids, or tamoxifen) can prevent theoccurrence of biological or phenotypically expressed breastcancers. When deciding whether or not a particular agentshould be evaluated in a cancer prevention study, there shouldbe evidence of its worth for preventing the initiation and/orpromotion of undiagnosable breast cancer. While several candidates merit evaluation, one agent particularly worthy of appraisal is the nonsteroidal antiestrogen tamoxifen, currently themost widely prescribed antineoplastic agent used to treat breastcancer in the United States. An extensive body of literatureexists on the pharmacokinetics. metabolism, and antitumoreffects of tamoxifen in experimental animals and in humans—results that provide support for evaluating the worth of thatdrug as a breast cancer preventive agent (79-82). Althoughtamoxifen acts as an estrogen antagonist, it may also act as apartial-to-full agonist. The precise mechanism(s) by which itachieves its antitumor effect are unknown. The drug appears toact primarily by competing with estradiol for receptor sites inthe cell nucleus, causing estrogen blockade that leads to growthinhibition of malignant cells (83). Several alternative mechanisms of action have been described. Tamoxifen may inhibitcell proliferation by modulating the production of transforminggrowth factors («and fi) that help regulate breast cancer cell
2379
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
proliferation (84); binding to cytoplasmic antiestrogenic binding sites, increasing intracellular drug levels (85); increasing sexhormone-binding globulin, which may decrease the availabilityof free estrogen for diffusion into tumor cells (86); increasinglevels of natural killer cells (87); and decreasing circulatinginsulin-like growth factor 1 which may, in turn, modify theendocrinological regulation of breast cancer cell kinetics (88).It has recently been reported that tamoxifen may act as aninhibitor of tumor angiogenesis (78).
Tamoxifen impairs tumor initiation. When laboratory animals were treated with it, carcinogen-induced mammary tumorsdid not appear (75). Investigations using a variety of modelshave evaluated the effect of tamoxifen on tumor promotion andhave shown that, when tamoxifen is given after a carcinogenbut before the appearance of a tumor, it prevents the occurrenceof a palpable tumor as long as administration of the drug ismaintained (76, 77).
Studies have demonstrated a benefit from tamoxifen administration in the treatment of advanced breast cancer (89-92)and in stages I and II disease when the drug has been used aspostoperative adjuvant therapy (43-51). The significant reduction in the incidence of cancers of the contralateral breast withtamoxifen is particularly relevant when it is considered as apreventive agent (43, 47, 93-95).
The ideal tumor preventive agent should produce minimaltoxicity during prolonged therapy. Adverse reactions to tamoxifen are relatively rare and only infrequently severe enough torequire discontinuing treatment. Although doses of tamoxifenmany times greater than those given to humans have beenfound to increase the incidence of liver tumors in animals (96-98), no such increase has been reported in humans treated withconventional doses (20 mg/day). It is likely that the risk ofthromboembolic events and endometrial cancer will be nogreater after prolonged tamoxifen administration than it is afterthe use of estrogen-replacement therapy in normal women.When considering the use of tamoxifen as a breast cancerpreventive agent, its effect on coronary artery disease andosteoporosis cannot be ignored. Estrogen administration hasbeen associated with an alteration in serum lipoproteins, i.e., adecrease in cholesterol and low-density lipoproteins with anincrease in high-density lipoproteins and with decreased mortality from coronary artery disease. Tamoxifen results in similarlipid changes (99-103). Thus, it may also favorably affectmortality from that disease. Similarly, since estrogen lowersthe incidence of fractures by decreasing the bone résorptionthat accompanies surgical or natural menopause (104,105), theestrogen agonist effect of tamoxifen may prevent bone loss(106). It has been estimated that osteoporosis affects 24 millionwomen in the United States and that 1.3 million fractures occureach year as a result. Consequently, a clinical trial conductedto evaluate the worth of tamoxifen as a breast cancer preventiveagent should concomitantly assess its effect in reducing mortality from coronary artery disease and in decreasing the riskof fractures due to osteoporosis.
Tamoxifen has been selected by the NSABP as the agent toevaluate in a prevention trial in which 16,000 women will berandomized so that 8,000 will receive placebo and 8,000 tamoxifen, both groups at 20 mg daily. The study population willconsist of women 60 years of age or older and those aged 35 to59 who have additional breast cancer risk factors, such thattheir minimum predicted risk of developing breast cancer withinthe next 5 years is at least as great as that of women aged 60years or older. The choice of women 60 years of age or older is
related to the fact that age is one of the strongest risk factors;rates increase steeply from age 30 to 60 and then plateau.Moreover, postmenopausal women have a substantial and increasing risk of coronary artery disease.
When the trial was in the planning stage, it became increasingly evident that younger women should be included. Not onlydoes a sizable proportion of the morbidity and mortality ofbreast cancer occur in younger women, but there are also well-established risk factors for breast cancer in women under 60that identify those with projected lifetime risks sufficiently greatto merit their inclusion in the trial. Moreover, because yearsmay elapse between a tumor's inception and its detection, a
preventive intervention may be more effective in women at anearly age, even though tumors may appear later in life. In thatregard, women with a first-degree relative who had breast cancer
when premenopausal are apt to develop the disease at an earlierage. In premenopausal patients, tamoxifen appears to be moreeffective in reducing the incidence of contralateral breast cancer,life-threatening toxicity from the drug is rare, and non-life-
threatening toxicity is much the same as in postmenopausalpatients. These observations support its use in younger women.In addition, because younger women at increased risk for breastcancer are often subjected to alternative therapies, such asbilateral mastectomies, which are worse than the side effectsobserved from tamoxifen, they should not be denied the opportunity to participate in the trial. Finally, the generalizability ofthe findings would be seriously limited if premenopausal womenwere excluded from participation in the study. If a benefit wasobserved in a trial using only postmenopausal women, wouldthose findings justify use of the drug in a premenopausalpopulation, or would another study involving many years ofuncertainty be required before it could be used? Thus, there isample evidence for allowing women aged 35-59 years who have
a substantially increased risk of breast cancer the option ofparticipating in the study.
A logistic regression model (107) will be used to estimate, bycombining individual risk factors, each potential participant's
composite risk of developing breast cancer. Her percentageprobability of developing breast cancer over her lifetime, adjusted for competing mortality risks by initial age and years offollow-up, will also be determined. The variables selected forinclusion in the model are number of first-degree relatives with
breast cancer, nulliparity or age at first live birth, number ofbenign breast biopsies, age at menarche, atypical hyperplasia,and lobular carcinoma in situ.
If a benefit from tamoxifen is demonstrated, a drastic paradigmatic change in the treatment of breast cancer could result—a change from current therapy, which is directed toward thedisease at or near end stage, to treatment of the disease whenit is nondetectable by any available means, and, perhaps, evenbefore phenotypic expression has occurred. Most significantly,the impact of the findings from this trial on the health ofwomen in the United States and elsewhere could be substantial.It cannot be too emphatically emphasized, however, that theimplementation of a trial to evaluate the worth of a hypothesis—and an agent—does not provide physicians with an impri
matur to administer, outside of the clinical trial setting, thetherapy being tested in the trial. Before that can occur, thepathways of science must be carefully traversed and a newparadigm established.
2380
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
Acknowledgments
The author acknowledges the contribution of the associates in hislaboratory, of those in the NSABP Operations Office and NSABPBiostatistical and Pathology Centers, and of the physicians in theUnited States and Canada who have entered patients into NSABPtrials. He is also grateful to Tanya Spewock for her editorial assistance.
References
1. National Institutes of Health Consensus Development Conference Statement: Treatment of Early-Stage Breast Cancer. Bethesda, MD: NIH. June18-21. 1990.
2. Cancer Statistics Review 1983-1987. In: L. A. B. Ries, B. F. Hankey, andB. K. Edwards (eds.). National Cancer Institute Division of Cancer Prevention and Control Surveillance Program. NIH Publication no. 90-2789.
3. Sobel. M. E. Metastasis suppressor genes. J. Nati. Cancer Inst.. 82: 267-276, 1990.
4. Wright, J. A., Egan, S. E., and Greenberg, A. H. Genetic regulation oftnetastatic progression. Anticancer Res., 10: 1247-1256, 1990.
5. Kerbel, R. S. Growth dominance of the metastatic cancer cell: cellular andmolecular aspects. Adv. Cancer Res., 55: 87-132, 1990.
6. Folkman. J., and Klagsburn, M. Angiogenetic factors. Science (WashingtonDC), 235: 442-447, 1987.
7. Kühn.T. S. The Structure of Scientific Revolutions, Ed. 2. Chicago:University of Chicago Press, 1970.
8. Kühn.T. S. The Essential Tension. Chicago: University of Chicago Press,1977.
9. Cohen, J. B. Revolution in Science. Cambridge. MA: Harvard UniversityPress. 1985.
10. Hull, D. L. Science as a Process. Chicago: University of Chicago Press.1988.
11. Hersher. L. On the absence of revolutions in biology. Perspect. Biol. Med..31: 318-323, 1988.
12. Doyle. R. J. Letter to the editor. Perspect. Biol. Med.,.}2:467-468, 1989.13. Medawar, P. Pluto's Republic. Incorporating the Art of the Soluble and
Induction and Intuition in Scientific Thought. Oxford: Oxford UniversityPress, 1982.
14. Bernard, C. Introduction à l'éludede la medicine expérimentale.Paris.
1865.15. Fisher, B. The surgical dilemma in the primary therapy of invasive breast
cancer: a critical appraisal. Curr. Probi. Surg.. 3-53. 1970.16. Halsted. W. S. The treatment of wounds with especial reference to the value
of the blood clot in the management of dead spaces. Johns Hopkins Hosp.Rep.. 2:255-314, 1890-1891.
17. Halsted. W. S. The results of operations for the cure of cancer of the breastperformed at the Johns Hopkins Hospital from June 1889 to January 1894.Arch. Surg.. 20: 497-555, 1894.
18. Halsted. W. S. A clinical and histological study of certain adenocarcinomaof the breast: and a brief consideration of the supraclavicular operation andof the results of operation for cancer of the breast from 1889 to 1898 at theJohns Hopkins Hospital. Ann. Surg.. 28: 557-576. 1898.
19. Halsted. W. S. The results of radical operations for the cure of carcinomaof the breast. Ann. Surg.. 46: 1-19, 1907.
20. Handley. W. S. The inadequacy of the embolie theory. In: A. Murray (ed.).Cancer of the Breast and Its Operative Treatment, p. 2. New York: P. B.Horber. 1922.
21. Virchow, R. Cellular Pathology. Frank Chance (trans.). Philadelphia: J. B.Lippincott Co., 1863.
22. Fisher, B., and Fisher. E. R. The interrelationship of hematogenous andlymphatic tumor cell dissemination. Surg. Gynecol. Obstet., 122: 791-798.1966.
23. Fisher, B., and Fisher, E. R. The organ distribution of disseminated "Cr-labeled tumor cells. Cancer Res., 27: 412-420, 1967.
24. Fisher, B., and Fisher, E. R. Transmigration of lymph nodes by tumor cells.Science (Washington DC). 752: 1397-1398. 1966.
25. Fisher, B., and Fisher, E. R. Barrier function of lymph node to tumor cellsand erythrocytes. I. Normal nodes. Cancer (Phila.). 20: 1907-1913. 1967.
26. Fisher, B., and Fisher, E. R. Barrier function of lymph node to tumor cellsand erythrocytes. II. Effect of X-ray, inflammation, sensitization and tumorgrowth. Cancer (Phila.). 20: 1914-1919, 1967.
27. Fisher, B. Laboratory and clinical research in breast cancer—a personaladventure: the David A. Karnofsky memorial lecture. Cancer Res., 40:3863-3874, 1980.
28. Fisher, B.. Redmond, C., Fisher. E. R., Bauer, M.. Wolmark, N., Wicker-ham, D. L., Deutsch, M., Montague, E., Margolese, R., and Foster. R. Ten-year results of a randomized clinical trial comparing radical mastectomyand total mastectomy with or without radiation. N. Engl. J. Med., 312:674-681. 1985.
29. Wickerham, D. L.. and Fisher, B. Surgical treatment of primary breast
2381
cancer. Semin. Surg. Oncol.. 4: 226-233, 1988.30. National Surgical Adjuvant Breast and Bowel Project Progress Report.
Presented at the 35th NSABP meeting. February 24, 1991.31. Fisher. B., Redmond. C., Poisson, R.. Margolese. R.. Wolmark. N., Wick
erham, D. L., Fisher. E.. Deutsch. M., Caplan. R.. Pilch. Y., Glass, A.,Shibata. H.. Lerner. H.. Terz. J.. and Sidorovich, L. Eight-year results of arandomized clinical trial comparing total mastectomy and lumpectomy withor without irradiation in the treatment of breast cancer. N. Engl. J. Med.,320: 822-828, 1989.
32. Fisher, B., Anderson. S.. Fisher. E. R., Redmond, C., Mamounas, E. P.,Wickerham, D. L., Wolmark, N., Margolese, R. G., and Poisson. R.Significance of ipsilateral breast tumor recurrence after lumpectomy. Lancet,338: 327-331, 1991.
33. Veronesi, U., Saccozzi, R., Del Vecchio, M.. Banfi, A., Clemente, C. DeLena, M., Gallus. G., Greco, M., Luini. A.. Marubini. E.. Muscolino, G.,Rilke, F., Salvadori, B., Zecchini, A., and Zucali, R. Comparing radicalmastectomy with quadrantectomy, axillary dissection, and radiotherapy inpatients with small cancers of the breast. N. Engl. J. Med., ¿05:6-11, 1981.
34. Fisher, E. R.. and Turnbull, R. B., Jr. The cytologie demonstration andsignificance of tumor cells in the mesenteric venous blood in patients withcolorectal carcinoma. Surg. Gynecol. Obstet., 100: 102-108. 1955.
35. Shapiro. D. M., and Fugmann. R. A. A role for chemotherapy as an adjunctto surgery. Cancer Res., 17: 1098-1101. 1957.
36. Fisher, B., Slack, N., Katrych, D., and Wolmark, N. Ten-year follow-upresults of patients with carcinoma of the breast in a cooperative clinical trialevaluating surgical adjuvant chemotherapy. Surg. Gynecol. Obstet., 140:528-534, 1975.
37. Mendelsohn. M. L. The growth fraction: a new concept applied to tumors.Science (Washington DC). 132: 1496. 1960.
38. Skipper. H. E. Kinetics of mammary tumor cell growth and implicationsfor therapy. Cancer (Phila.). 28: 1479-1499, 1971.
39. Skipper, H. E. Some Thoughts on Surgery-Chemotherapy Trials againstBreast Cancer, Southern Research Institute Monograph no. 1. Birmingham,AL: Southern Research Institute. 1971.
40. Skipper, H. E., and Schabel, F. M.. Jr. Quantitative and cytokinetic studiesin experimental tumor models. In: J. F. Holland and E. Frei. Ill (eds.),Cancer Medicine, pp. 629-650. Philadelphia: Lea and Febiger, 1973.
41. Fisher, B., Carbone, P., Economou, S. G., Frelick, R.. Glass, A., Lerner.H.. Redmond. C.. Zelen, M.. Band. P.. Katrych. D. 1... Wolmark, N., andFisher. E. R. i.-Phenylalanine mustard (L-PAM) in the management ofprimary breast cancer: a report of early findings. N. Engl. J. Med., 292:117-122, 1975.
42. Bonadonna, G., Brusamolino, E., Valagussa. P.. Rossi, A.. Brugnatelli, L.,Brambilla. C.. De Lena, M., Tancini. G.. Bajetta. E.. Musumeci, R., andVeronesi, U. Combination chemotherapy as an adjuvant treatment in operable breast cancer. N. Engl. J. Med., 294: 405-410, 1976.
43. Bartlett. K.. Eremin. O.. Hutcheon. A., Preece, P.. Scott, J. S., Forrest, P.,Chetty. U., Prescott, R. J., Rodger. A.. Smyth. J., and George. D. Adjuvanttamoxifen in the management of operable breast cancer: the Scottish trial.Report from the Breast Cancer Trials Committee, Scottish Cancer TrialsOffice (MRC), Edinburgh. Lancet, 2: 171-175, 1987.
44. Baum, M., Brinkley. D. M.. Dosset. J. A., McPherson, K.. Jackson, I. M.,Rubens. R. D.. Smiddy. F. G.. Stoll. B. A.. Wilson, A. J.. Birch, I. H., andPalmer. M. K. Controlled trial of tamoxifen as a single adjuvant agent inthe management of early breast cancer. Analysis at eight years by Nolvadexadjuvant trial organisation. Br. J. Cancer, 57:608-611, 1988.
45. Fisher, B., Redmond, C., Brown. A., Wolmark. N., Wittliff. J., Fisher, E.R., Plotkin, D.. Bowman. D.. Sachs, S., Wolter, J., Frelick, R., Dessen R.,Licalzi. N., Geggie, P., Campbell, T., Elias, E. G., Prager, D., Koontz, P.,Volk, H., Dimitrov, N., and Gardner. B. Treatment of primary breast cancerwith chemotherapy and tamoxifen. N. Engl. J. Med.. 305: 1-6. 1981.
46. Fisher, B.. Redmond. C.. Brown. A., Fisher. E. R.. Wolmark. N.. Bowman,D.. Plotkin, D., Wolter, J., Bornstein. R., Legault-Poisson. S.. and Saffer,E. A. Adjuvant chemotherapy with and without tamoxifen in the treatmentof primary breast cancer: 5-year results from the National Surgical AdjuvantBreast and Bowel Project trial. J. Clin. Oncol., 4: 459-471. 1986.
47. Fisher, B., Costammo, J., Redmond. C., Poisson, R., Bowman, D., Couture,J., Dimitrov, N. V., Wolmark. N., Wickerham, D. L., Fisher, E. R.,Margolese. R.. Robidoux, A., Shibata, H., Terz, J.. Paterson, A. H. G..Feldman, M. L, Farras. W., Evans, J., Lickley. H. L., and Keiner, M. Arandomized clinical trial evaluating tamoxifen in the treatment of patientswith node-negative breast cancer who have estrogen-receptor-positive tumors. N. Engl. J. Med., 320: 479-484. 1989.
48. Hubay. C. A., Gordon, N. H.. Pearson, O. H.. Marshall. J. S.. and McGuire.W. L. Eight-year follow-up of adjuvant therapy for stage II breast cancer.World J. Surg., 9: 738-749, 1985.
49. Rose. C., Mouridsen. H. T.. Thorpe, S. M., Andersen, J., Blichert-Toft. M..and Andersen, K. W. Anti-estrogen treatment of postmenopausal breastcancer patients with high risk of recurrence: 72 months of life-table analysisand steroid hormone receptor status. World J. Surg.. 9: 764-774. 1985.
50. Ludwig Breast Cancer Study Group. Randomised trial of chemo-endocrinetherapy, endocrine therapy, and mastectomy alone in postmenopausal pa-
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
tienls with operable breast cancer and axillary node metastasis. Lancet, /:1253-1256.1984. 73.
51. Early Breast Cancer Trialists' Collaborative Group. Effects of adjuvant
tamoxifen and of cytotoxic therapy on mortality in early breast cancer. N.Engl. J. Med.. 319: 1681-1692. 1988.
52. Tormey, D. C. Gray. R.. Taylor. S. G.. IV. Knuiman. M.. Olson. J. E.. and 74.Cummings, F. J. Postoperative chemotherapy and chemohormonal therapyin women with node-positive breast cancer. Nati. Cancer Inst. Monogr., 1:75-80, 1986. 75.
53. Abeloff, M. D.. and Beveridge. R. A. Adjuvant chemotherapy of breastcancer. The consensus development conference revisited. Oncology, 2: 21-33, 1988. 76.
54. Fisher. B.. Redmond. C.. Legault-Poisson. S.. Dimitrov, N. V.. Brown, A.M., Wickerham. D. L.. Wolmark. N.. Margolese. R. G., Bowman. D., Glass.A. G., Kardinal, C. G.. Robidoux. A.. Jochimsen. P.. Cronin. W., Deutsch.M.. Fisher. E. R.. Myers. D. B., and Hoehn. J. L. Postoperative chemo- 77.therapy and tamoxifen compared with tamoxifen alone in the treatment ofpositive-node breast cancer patients aged 50 years and older with tumorsresponsive to tamoxifen: results from NSABP B-16. J. Clin. Oncol.. 8:1005-1018. 1990. 78.
55. Rosenberg, S. A., Aebersold, P.. Cornetta, K., Kasid, A., Morgan, R. A.,Moen, R., Karson, E. M., Lotze, M. T., Yang, J. C., Topalian, S. L.,Merino. M. J., Culver, K., Miller, A. D., Blaese, M., and Anderson, W. F.Gene transfer into humans—immunotherapy of patients with advanced 79.melanoma, using tumor-infiltrating lymphocytes modified by retroviral genetransduction. N. Engl. J. Med., 323: 570-578, 1990. 80.
56. Fisher, B., and Wolmark, N. New concepts in the management of primarybreast cancer. Cancer (Phila.). 36: 627-632, 1975.
57. Schuller. D. E. Preoperative reductive chemotherapy for locally advanced 81.carcinoma of the oral cavity, oropharynx, and hypopharynx. Cancer (Phila.).51: 15-19, 1983.
58. Leichman, L., Seydel. H. G., and Steiger, Z. Preoperative adjuvant therapyfor squamous cell cancer (SCC) of the esophagus: a potentially curativeapproach. J. Clin. Oncol., 2: 75-79, 1984. 82.
59. Rosen, G. Preoperative chemotherapy for osteogenic sarcoma. Cancer(Phila.), 49: 1221-1230. 1982. 83.
60. Shick. P.. Goodstein. J.. Moor, J.. Butler, J., and Senter. K. L. Preoperativechemotherapy followed by mastectomy for locally advanced breast cancer.J. Surg. Oncol.. 22: 278-282. 1983.
61. Sorace, R. A.. Bagley. C. S.. Lichter. A. S.. Danfort, D. N.. Jr., Wesley, M. 84.W., Young, R. C., and Lippman. M. E. The management of nonmetastaticlocally advanced breast cancer using primary induction chemotherapy withhormonal synchronization followed by radiation therapy with or withoutdebulking surgery. World J. Surg.. 9: 775-785, 1985. 85.
62. .1.ioiiull.ii. C. I., Weil. M.. Auclerc. G.. Sellami. M., Auclerc, M. F., Khayat,D., and Baille!. F. Neoadjuvant chemotherapy in the conservative management of breast cancers: study of 143 patients. In:}. Ragaz. P. R. Band, andJ. H. Goldie (eds.). Recent Results in Cancer Research, pp. 113-119. New 86.York: Springer-Verlag. 1986.
63. Mansi. J. L., Smith. I. E.. Walsh. G.. Ahern. R. P., Harmer, C. L.. Sinnett,H. D., Trott, P. A., Fisher. C., and McKinna, J. A. Primary medical therapy 87.for operable breast cancer. Eur. J. CanecûClin. Oncol.. 25: 1623-1627.1989.
64. Bonadonna. G., Veronesi, U.. Brambilla. C., Ferrari, L., Luini, A., Greco, 88.M., Bartoli, C., de Yoldi. G. C., Zucali. R.. Rilke. F.. Andreola. S.,Silvestrini. R.. Di Fronzo, G., and Valagussa. P. Primary chemotherapy toavoid mastectomy in tumors with diameters of three centimeters or more.J. Nail. Cancer Inst., 82: 1539-1545. 1990. 89.
65. Gunduz. N., Fisher. B.. and Saffer, E. A. Effect of surgical removal on thegrowth and kinetics of residual tumor. Cancer Res.. 39: 3861-3865. 1979.
66. Fisher, B., Saffer, E. A., Rudock. C.. Coyle, J., and Gunduz. N. Presence 90.of a growth-stimulating factor in serum follow ing primary tumor removalin mice. Cancer Res., 49: 1996-2001, 1989.
67. Fisher, B., Saffer, E. A.. Rudock, C., Coyle, J., and Gunduz. N. Effect of 91.local or systemic treatment prior to primary tumor removal on the production and response to a serum growth-stimulating factor in mice. CancerRes.. 49: 2002-2004. 1989. 92.
68. Goldie. J. H.. and Coldman. A. J. A mathematical model for relating thedrug sensitivity of tumors to their spontaneous mutation rate. Cancer Treat.Rep., 63: 1727-1733. 1979.
69. Recht. A.. Danoff. B. S.. Solin. L. J., Schnitt. S.. Connolly, J.. Botnick. L.. 93.Goldberg. I.. Goodman. R. L., and Harris. J. R. Intraductal carcinoma ofthe breast: results of treatment with excisional biopsy and irradiation. J.Clin. Oncol.. 3: 1339-1343. 1985.
70. Stotter. A. T., McNeese, M.. Oswald. M. J., Ames, F. C.. and Rohmsdahl.M. M. The role of limited surgery with irradiation in primary treatment of 94.ductal in situ breast cancer. Int. J. Radiât.Oncol. Biol. Phys., 18: 283-287.1990.
71. I imII.iv P. L.. and Goodman. R. Radiation therapy for treatment ofintraductal carcinoma of the breast. Am. J. Clin. Oncol.. 6: 281-285. 1983. 95.
72. Zafrani. B.. Fourquet, A.. V'ilcoq. J. R.. Legal, M.. and Calle. R. Conserv
ative management of intraductal breast carcinoma with tumorectomy and
2382
radiation therapy. Cancer (Phila.). 57: 1299-1301, 1986.Silverstein, M. J., Rosser. R. J.. Gierson, E. D., Waisman. J. R., Gamagami.P.. Hoffman. R. S., Fingerhut. A. G.. Lewinsky. B. S.. Colburn, W., andHandel. N. Axillary lymph node dissection for intraductal breast carcinoma—is it indicated? Cancer (Phila.). 59: 1819-1824. 1987.Fisher. E. R.. Sass. R., Fisher. B., Wickerham. L.. and Paik. S. M. Pathologic findings from the National Surgical Adjuvant Breast Project (Protocol6) I. Intraductal carcinoma (DCIS). Cancer (Phila.). 57: 197-208, 1986.Jordan, V. C. Effect of tamoxifen (ICI 46,474) on initiation and growth ofDMBA-induced rat mammary carcinomata. Eur. J. Cancer Clin. Oncol..72:419-424. 1976.Jordan. V. C. The anti-tumor effect of tamoxifen in the dimethylbenzan-thracene-induced rat mammary carcinoma model. In: Proceedings of aSymposium on the Hormonal Control of Breast Cancer, pp. 11-17. AlderleyPark. Cheshire. England: Pharmaceutical Division. ICI. 1975.Jordan. V. C.. and Allen, K. E. Evaluation of the antitumor activity of thenonsteroidal antiocslrogen monohydroxytamoxifen in the DMBA-inducedrat mammary carcinoma model. Eur. J. Cancer Clin. Oncol.. 16: 239-251,1980.Tanaka. N. G.. Sakamoto, N., Korenaga, H.. Inoue. K.. Ogawa. H., andOsada, Y. The combination of a bacterial polysaccharide and tamoxifeninhibits angiogenesis and tumour growth. Int. J. Radiât.Biol., 60: 79-83,1991.Adam. H. K. Pharmacokinetic studies with Nolvadex. Rev. Endocr.-Rel.Cancer. (Suppl. 9): 131-143. 1981.Adam. H. K. A review of the pharmacokinetics and metabolism of Nolvadex.In: R. L. Sutherland and V. C. Jordan (eds.), Non-Steroidal Antiestrogens,pp. 59-74. New York: Academic Press. 1981.Patterson. J. S., Adam, H. K., Kemp. J. V.. and Settatree. R. S. Serumconcentrations of tamoxifen and major metabolites during long-term Nolvadex therapy, correlated with clinical response. In: H. T. Mouridsen andT. Palshof (eds.). Breast Cancer—Experimental and Clinical Aspects, pp.89-92. Oxford: Pergamon Press. 1980.Furr, B. J. A., and Jordan, V. C. The pharmacology and clinical uses oftamoxifen. Pharmacol. Ther.. 25: 127-205. 1984.Wakeling, A. E., Valcaccia, B.. Newboult, E., and Green, L. R. Nonsteroidal antioestrogens: receptor binding and biological response in ratuterus, rat mammary carcinoma and human breast cancer cells. SteroidBiochem., 20: 111-120, 1984.Knabbe, C.. Lippman. M. E.. Wakefield. L. M.. Flanders. K. C., Kasid, A.,Derynck, R., and Dickson, R. B. Evidence that transforming growth factorli is a hormonally regulated negative growth factor in human breast cancercells. Cell, 48: 417-428, 1987.Murphy. L. C.. and Sutherland. R. L. Antitumor activity of clomipheneanalogs in n'fro: relationship to affinity for the estrogen receptor and another
high affinity antiestrogen-binding site. J. Clin. Endocrinol. Metab., 57:373-379. 1983.Jordan. V. C. Long-term adjuvant therapy with tamoxifen: effects on sexhormone binding globulin and antithrombin III. Cancer Res.. 47: 4517-4519. 1987.Berry. J.. Green. B. J.. and Matheson. D. S. Modulation of natural killercell activity by tamoxifen in stage I postmenopausal breast cancer. Eur. J.Cancer Clin. Ã’ncol.. 23: 517-520. 1987.Pollak, M., Costantino, J.. Polychronakos, C., Blauer. S-A.. Guyda. H..Redmond. C., Fisher. B., and Margolese, R. Effect of tamoxifen on seruminsulinlike growth factor I levels in stage I breast cancer patients. J. Nati.Cancer Inst.. 82: 1693-1697. 1990.Lerner. H. J., Band. P. R.. Israel. L.. and Leung, B. S. Phase II study oftamoxifen: report of 74 patients with stage IV breast cancer. Cancer Treat.Rep., 60: 1431-1435. 1976.Manni. A., and Pearson, O. H. Antiestrogen-induced remissions in premenopausa! women with stage IV breast cancer: effects on ovarian function.Cancer Treat. Rep.. 64: 779-785. 1980.Margreiter. R., and Wiegele. J. Tamoxifen (Nolvadex) for premenopausa!patients with advanced breast cancer. Breast Cancer Res. Treat.. 4: 45-48.1984.Legha. S. S.. Buzdar, A. U., Hortobagyi, G. N., Wiseman. C.. Benjamin.R. S., and Blumenschein. G. R. Tamoxifen: use in treatment of metastaticbreast cancer refractory to combination chemotherapy. J. Am. Med. Assoc.,.?Â¥2:49-52, 1979.Rutqvist, L. E.. Cedermark, B., Glas. U.. Johansson. H., Nordenskjold, B.,Shoog. L.. Somell. A., Theve. T., Friberg. S.. and Askergren, J. TheStockholm trial on adjuvant tamoxifen in early breast cancer: correlationbetween estrogen receptor level and treatment effect. Breast Cancer Res.Treat.. 10: 255-266. 1987.Fornander. T.. Cedermark. B.. Mattson. A.. Skoog. L.. Theve, T., Askergren, J., Rutqvist. L. E., Glas, U., Silfversward, C., Somell, A., Wilking, N.,and Hjalmar. M. L. Adjuvant tamoxifen in early breast cancer: occurrenceof new primary cancers. Lancet. I: 117-120. 1989.Abram. W. P.. Baum. M.. Berstock. D. A., Brinkley. D., Cuzick. J., Durrani,K. R., Elston, C. Farndon. J. R.. Houghton, J.. and Riley, D. L. Cyclo-phosphamide and tamoxifen as adjuvant therapies in the management of
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

EVOLUTION OF PARADIGMS FOR THE MANAGEMENT OF BREAST CANCER
breast cancer. Preliminary analysis by the CRC Adjuvant Breast TrialWorking Party. Br. J. Cancer, 57:604-607, 1988.
96. Investigational Drug Brochure for Nolvadex (Tamoxifen Citrate). Wilmington, DE: Clinical and Medical Affairs. ICI Pharmaceuticals Group, Divisionof ICI Americas, Inc., February 1990.
97. Gau, T. Open Letter to All U.S. Medical Oncologists Describing theToxicological Findings in Rats with High-Dose Tamoxifen Treatment.Wilmington, DE: Stuart Pharmaceuticals, A Division of ICI Americas,1986.
98. Rattel, B., Loser, R., Dahme, E. G., and Liehn, H-D. Comparative toxicology of droloxilene (3-OH tamoxifen) and tamoxifen: hepatocellular carcinomas induced by tamoxifen (Abstract). Miami, FL: International BreastCancer Research Conference, March 1-5, 1987.
99. Bertelli, G., Pranzato, P., Amoroso, D., Cusimano. M. P., Conte, P. F.,Montagna, G., Bertolini, S., and Rosso, R. Adjuvant tamoxifen in primarybreast cancer: influence on plasma lipids and antithrombin III levels. BreastCancer Res. Treat., 12: 307-310, 1988.
100. Rossner, S., and Wallgren, A. Serum lipoproteins and proteins after breastcancer surgery and effects of tamoxifen. Atherosclerosis, 52:339-346, 1984.
101. Love, R. R., Newcomb. P. A., Wiebe. D. A.. Surawicz, T. S., Jordan, V. C,Carbone, P. P., and DeMets, D. L. Effects of tamoxifen therapy on lipid
and lipoprotein levels in postmenopausal patients with node-negative breastcancer. J. Nati. Cancer Inst., 82: 1327-1332, 1990.
102. Bruning. P. F., Bonfrer, J. M. G., Hart, A. A. M.. DeJong-Bakker, M.,Linders, D., Van Loon, J., and Nooyen, W. J. Tamoxifen, serum lipoproteins and cardiovascular risk. Br. J. Cancer, 5«:497-499, 1988.
103. Bagdade, J. D., Wolter, J.. Subbaiah. P. V., and Ryan, W. Effects oftamoxifen treatment on plasma lipids and lipoprotein lipid composition. J.Clin. Endocrinol. Metab.. 70: 1132-1135, 1990.
104. Hutchinson, T. A., Polansky, S. M., and Feinstein, A. R. Post-menopausaloestrogens protect against fractures of hip and distal radius. Lancet, 2:705-709, 1979.
105. Ettinger, B., Genant, H. K., and Cann, C. E. Long-term estrogen replacement therapy prevents bone loss and fractures. Ann. Intern. Med., 702:319-324, 1985.
106. Türken,S., Siris, E., Seidin, D., Plaster, E., Hyman, G., and Lindsay, R.Effects of tamoxifen on spinal bone density in women with breast cancer. J.Nati. Cancer Inst., 81: 1086-1088, 1989.
107. Gail, M. H.. Brinton, L. A., Byar. D. P., Corle, D. K., Green, S. B., Schairer.C., and Mulvihill, J. J. Projecting individualized probabilities of developingbreast cancer for white females who are being examined annually. J. Nati.Cancer Inst., 81: 1879-1886, 1989.
2383
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1992;52:2371-2383. Cancer Res Bernard Fisher Cancer: A Personal PerspectiveThe Evolution of Paradigms for the Management of Breast
Updated version
http://cancerres.aacrjournals.org/content/52/9/2371.citation
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/52/9/2371.citationTo request permission to re-use all or part of this article, use this link
on June 28, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from