-
7/29/2019 The Evolution of Contract Research AC4
1/3
by Jerey Staord
The Evolution o Contract ResearchOrganizations
The Drug Development Process: What Do CROs Do?
Drug development, the task pharmaceutical companies most oten
outsource to CROs, is divided into two
phases: preclinical and clinical. During preclinical
development, new compounds are analyzed in test
tubes and in laboratory animals or saety and ecacy. Ater the
preclinical phase is complete (generally
one to three years), testing moves into human subjects, also
known as the clinical development stage.
In the United States, the bulk o in-human clinical work is
divided into three phases. Phase I involves testing
or saety in approximately 20 to 100 healthy volunteers. In Phase
II, a pool o 100 to 500 volunteers
suering rom the specic disease target is tested over a period o
a year or longer. During Phase III,
several thousand people are tested to veriy ecacy and long-term
saety on a larger scale. Most CROs
specialize in either early-stage (preclinical and Phase I
trails) or late-stage development (Phase II-III
trials). Drugmakers spend billions o dollars per year attempting
to discover the next blockbuster drugs,
with the vast majority o potential compounds ailing to reach the
consumer. In act, the Pharmaceutical
Research and Manuacturers o America estimates that a pool o
10,000 potential compounds produces
only one FDA approved drug on average. Furthermore, the process
is very time consuming with an
average development period o about 15 years. As we will explain
in more depth, drug companies out-
source development work or a variety o reasons, such as
temporary or permanent lack o capacity
or inrastructure and to ocus on core competencies.
Early History of Contract Research
For decades, biopharmaceutical companies have enlisted outside
parties to assist in the drug develop-
ment process. Prior to the contract research organization boom,
academic institutions and independent
laboratories handled the bulk o outsourced drug development
work. In 1962, regulatory scrutiny on
the development process increased when Congress passed the
Keauver-Harris amendments, requiring
drug manuacturers to prove ecacy beore marketing a new product.
The new law also took steps
to ensure greater saety. Burdened by a greater workload, drug
companies began to outsource additional
studies that couldnt be handled internally. Private rms sprouted
up to help pharmaceutical companies
manage these new challenges, which included more complex
clinical trial work to gather data or submis-
sion to the Food and Drug Administration. During this period,
drug companies only let clinical develop-
ment pass outside their own walls when internal capacity was
temporarily constrained. Large rms
operated with a vertically integrated model that kept nearly
every step o the process in-house. Develop-
ment outsourcing in this mold continued through the 1980s, with
several o todays major players in
outsourced clinical trial management starting operations,
including Parexel InternationalPRXL (FV: $21)
in 1983 and Pharmaceutical Product DevelopmentPPDI (FV: $42) in
1985.
Continued on Page 02
Morningstar Opportunistic Investor1
-
7/29/2019 The Evolution of Contract Research AC4
2/3
Continued on Page 03
Beginning in the 1990s, the dynamics between the CRO and
pharmaceutical industries began to change.
Pressured by declining research and development productivity and
the looming loss o patent exclusivity
or a number o blockbuster drugs, big pharma was aced with higher
uture expenses to replace its
current revenue stream. Although the total dollars spent on
research and development by drug companies
continued to climb, the number o new drugs submitted or approval
by the FDA was not keeping pace.
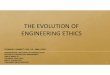
According to a report by the United States Government
Accountability Oce, annual infation-adjustedR&D
expenses increased rom nearly $16 billion to nearly $40 billion
rom 1993 to 2004, an increase o 147%.
However, the number o new drug applications or new molecular
entities increased only 7% over the same
time period. The CRO industry oered a compelling solution or big
pharma. By giving a larger portion
o their noncritical studies to CROs, pharmaceutical rms were
able to lower their development costs, as
CROs paid lower salaries than in-house pharma departments. CROs
also gave pharma companies
the opportunity to turn a portion o xed development costs into
variable costs by shiting studies osite.
With heightened demand rom drug companies, CRO industry revenues
began to take o. Global
industry revenue increased to $7.7 billion in 2001 rom $1.6
billion in 1993, a compounded annual growth
rate o nearly 22% over the period.
To accommodate growing demand, CROs added inrastructure,
personnel, and service capabilities.
For example, employee headcount at CovanceCVD (FV: $74)
ballooned to 7,900 by the end o 2000 rom
5,400 at the end o 1996. Signicant industry consolidation also
occurred, as CROs armed with strong
valuations and newound cash needed to expand rapidly to meet
demand. Large CROs expanded
into nontraditional areas, such as post-approval services, and
used acquisitions to ll therapeutic and
unctional holes. In 1998 and 1999 alone, CROs acquired 39
smaller competitors in total (CenterWatch).
To the chagrin o drugmakers, rapid CRO growth and the
integration o newly acquired companies led to
quality issues, straining the industrys already delicate
relationship with large pharmaceutical rms.
During the consolidation period, a Covance insider compared
integrating newly acquired companies to
changing tires at 80 miles per hour (Bridging the Gap, Lamb).
Failed trials and the mishandling o
some projects made pharmaceutical rms weary o handing over
important projects to CROs. In one o
the more notable cases o quality deciency, Bloomberg News
exposed SFBC International, now
Research & Development Productivity
R&D Expenditures Total NDA Submissions NDA or NME
Submissions
93 94 95 96 97 98 99 00 01 02 03 04
200
160
120
80
40
0
Source: Study by the United States Government Accountability
Office:
New Drug Development, November 2006.
40($Bil)
32
24
16
8
0
Morningstar Opportunistic Investor2
-
7/29/2019 The Evolution of Contract Research AC4
3/3
part o PharmaNetPDGI, or its lack o patient saety in a 2005
article. Bloomberg outlined numerous
inadequate quality controls at SFBC and questioned the strength
o regulatory bodies paid to monitortrials. Stories like this are a
prime example o the reasons many CROs still lacked the trust o big
pharma.
Biotech Surge & Relationship Building
Despite heightened interest, big pharma was still not ready to
ully jump into bed with CROs. Intellectual
property, quality, and productivity concerns all remained at the
turn o the century. Two trends helped
drive the gradual acceptance o the major CROs: the surge o the
biotechnology industry and preerred
provider lists.
Fueled by a bolus o scientic breakthroughs, a rash o venture
capital unding, and the maturing o
the industry, biotechnology rms began to take o in the late
1990s. Mapping o the human genome gave
biotech rms a blueprint to create new and exciting treatments.
Moreover, newly introduced biologics,
such Genentechs DNA (FV: $91) Herceptin, were gaining steam in
the market. While large companies
like Genentech and AmgenAMGN (FV: $71) had been successul or
some time, many smaller biotech
rms were just beginning to turn a prot developing new drugs
(CNNMoney). This wave o drug develop-
ment meant the prospect o more preclinical and clinical studies.
However, these newly successul
companies oten lacked the internal resources, personnel, and
expertise necessary to conduct clinical
trials. Without the required inrastructure, biotech rms relied
on CROs to conduct much o the preclinical
and clinical development work related to new candidates. As CROs
conducted more and more work
or biotech rms, solid relationships developed between each
industry. During this period, CROs proved
capable o handling important drug studies. Also, biotech
customers diversied the revenue base o
CROs, decreasing the impact o cancellations rom big pharma
clients. For example, PPDs composition
o revenue changed rom 72% pharma and 19% biotech in 2002 to 56%
pharma and 31% biotech in
the third quarter o 2008.
In addition to building relationships with biotech companies,
CROs were also slowly gaining the trust
o large pharmaceutical companies through the use o preerred
provider lists. Big pharma realized
that using a large number o CROs was inecient and didnt allow or
strong relationships to orm
between sponsor and CRO. As a result, pharmaceutical rms began
whittling down the number o CROs
used or outsourcing until the companies were let with a handul o
preerred providers. Only the
most reputable and capable CROs made these lists, driving even
more business to the top echelon o
the industry, and separating the Covances and PPDs o the world
rom their smaller competitors.
As drug company sponsors and CROs worked more closely together
on more projects, a level o trust
was ostered. Moreover, making a preerred list gave big CRO
players more condence to increase
capacity and invest in additional inrastructure.K
This article originally appeared in Morningstar
HealthcareObserver (January 2009).
To learn more, visit http://healthcare.morningstar.com
Morningstar Opportunistic Investor3