Embed Size (px)
Citation preview
The European health policy:strategies and objectives
Prof. Dr. Helmut Brand MSc MFPHDepartment of International HealthCAPHRI, FHMLMaastricht [email protected]
23.6.09

Which Role for Europe?

Rome 1957

2007:50th anniversary of the Treaty of Rome

Overview
• 1. Role of Community on health
• 2. Current and future health challenges
• 3. EU health strategy• Why an EU-health strategy?• Structure• Implementation
• 4. Example EUREGIO I
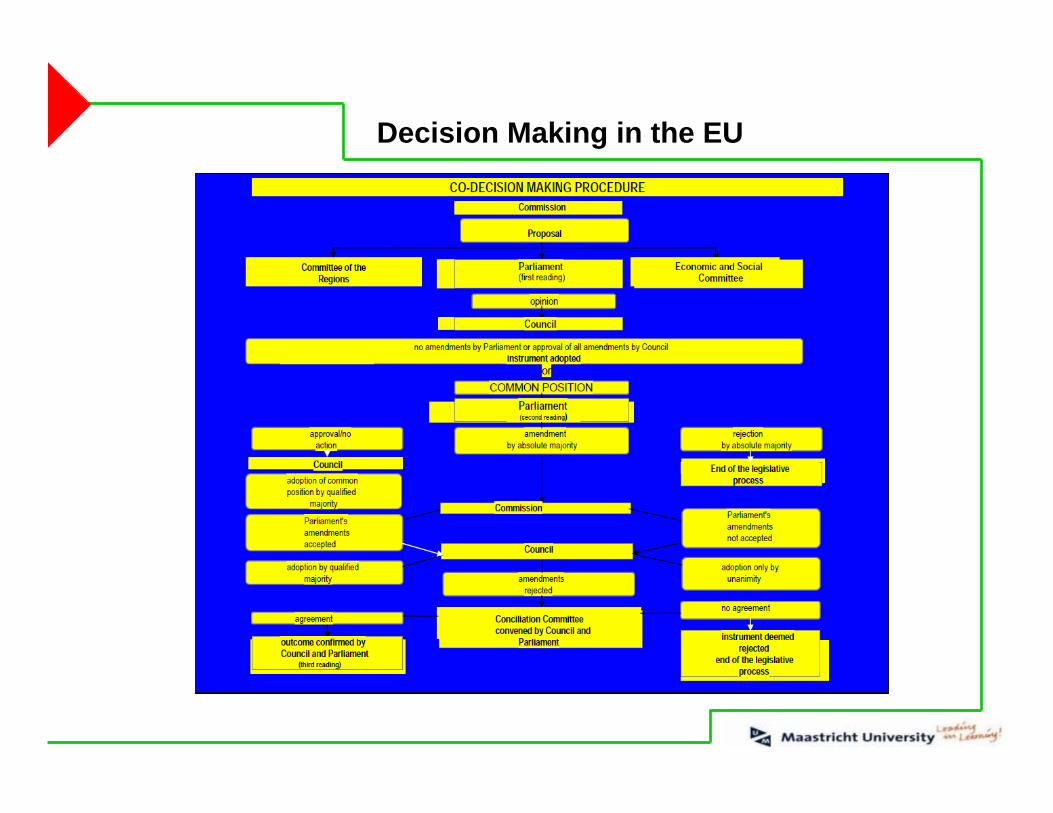
Decision Making in the EU

Evolution of health action
• specific public health role created in 1992 by the Maastricht Treaty –and still developing
• but health has always been an important part of Community policies

The public health article
• Support to Member States through networks and projects
• Policy actions
• Legislation to set European standards

2. Current and future health challenges

Life expectancy in the EU at birth1970-2005
65
70
75
80
85
1970 1980 1990 2000 2010
AustriaBelgiumBulgariaCyprusCzech RepublicDenmarkEstoniaFinlandFranceGermanyGreeceHungaryIrelandItalyLatviaLithuaniaLuxembourgMaltaNetherlandsPolandPortugalRomaniaSlovakiaSloveniaSpainSwedenUnited Kingdom
Life expectancy at birth, in years
0
10
20
30
40
50
1970 1980 1990 2000 2010
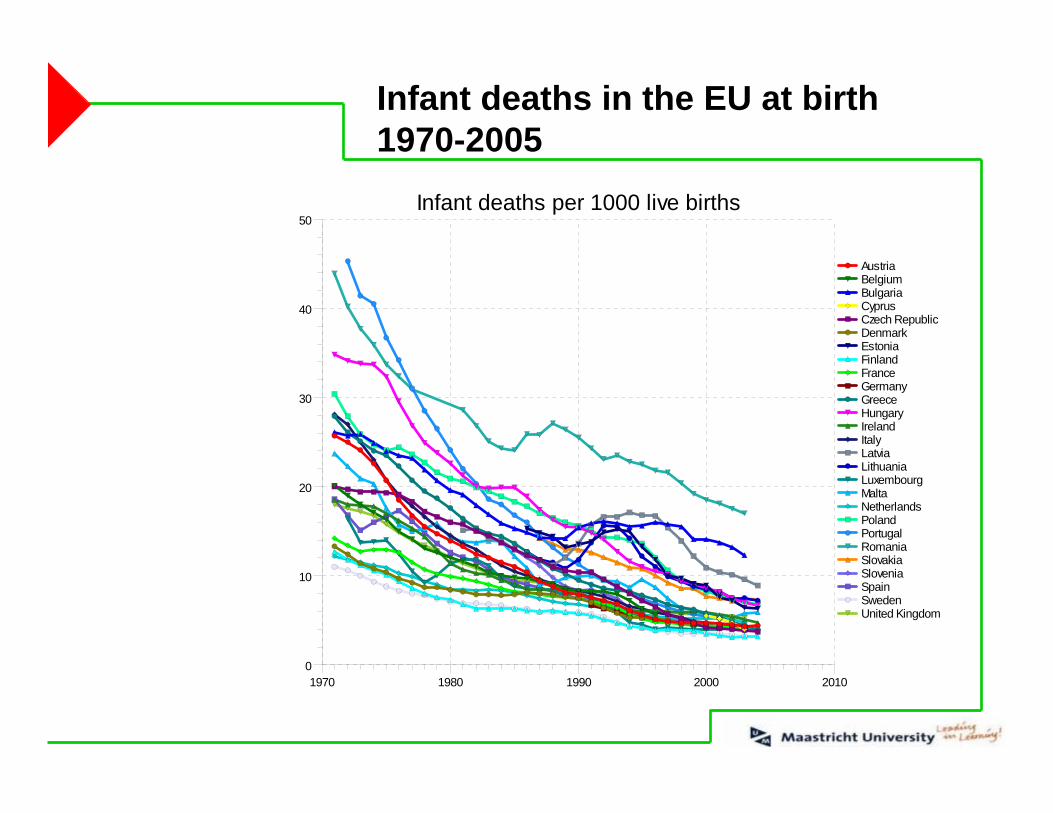
AustriaBelgiumBulgariaCyprusCzech RepublicDenmarkEstoniaFinlandFranceGermanyGreeceHungaryIrelandItalyLatviaLithuaniaLuxembourgMaltaNetherlandsPolandPortugalRomaniaSlovakiaSloveniaSpainSwedenUnited Kingdom
Infant deaths per 1000 live births
Infant deaths in the EU at birth1970-2005


Health Inequalities: Life Expectancy at BirthSelected EU-countries, 1990 and 2004
62
6466
68
70
7274
76
7880
82
Germany Hungary SlovakRepublic
Sweden
year
s 19902004
Source: OECD 2006
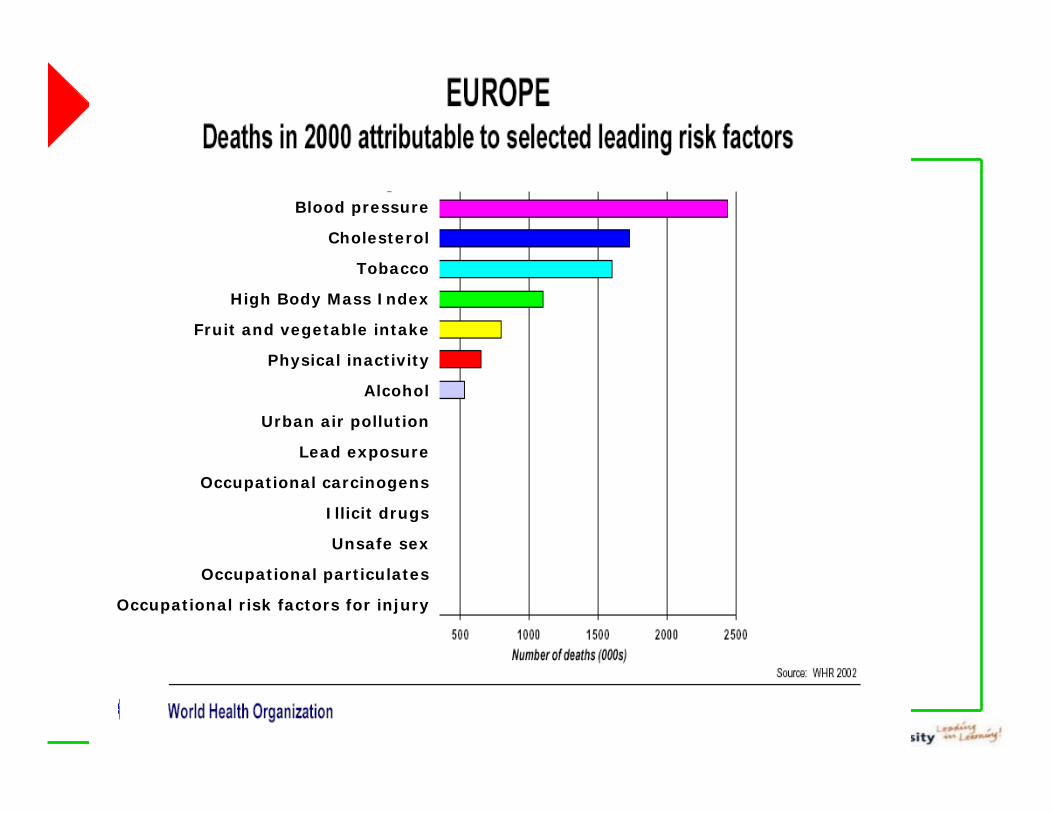
Blood pressure
Cholesterol
Tobacco
High Body Mass Index
Fruit and vegetable intake
Physical inactivity
Alcohol
Urban air pollution
Lead exposure
Occupational carcinogens
Illicit drugs
Unsafe sex
Occupational particulates
Occupational risk factors for injury

Case Study – Mental Health
– 18 million work days lost to depression in Germany in 2002 -cost for employers: € 1.59 billion
– Mental health is 10% of the disease burden but 2% of spending

Case Study – Obesity
18% of school children are overweight (EU 25)
Direct costs for diabetes in the EU varies between 2 and 7% of total health expenditure.
80% of CVD and type II diabetes and 40% of cancer could be prevented if lifestyle factors eliminated
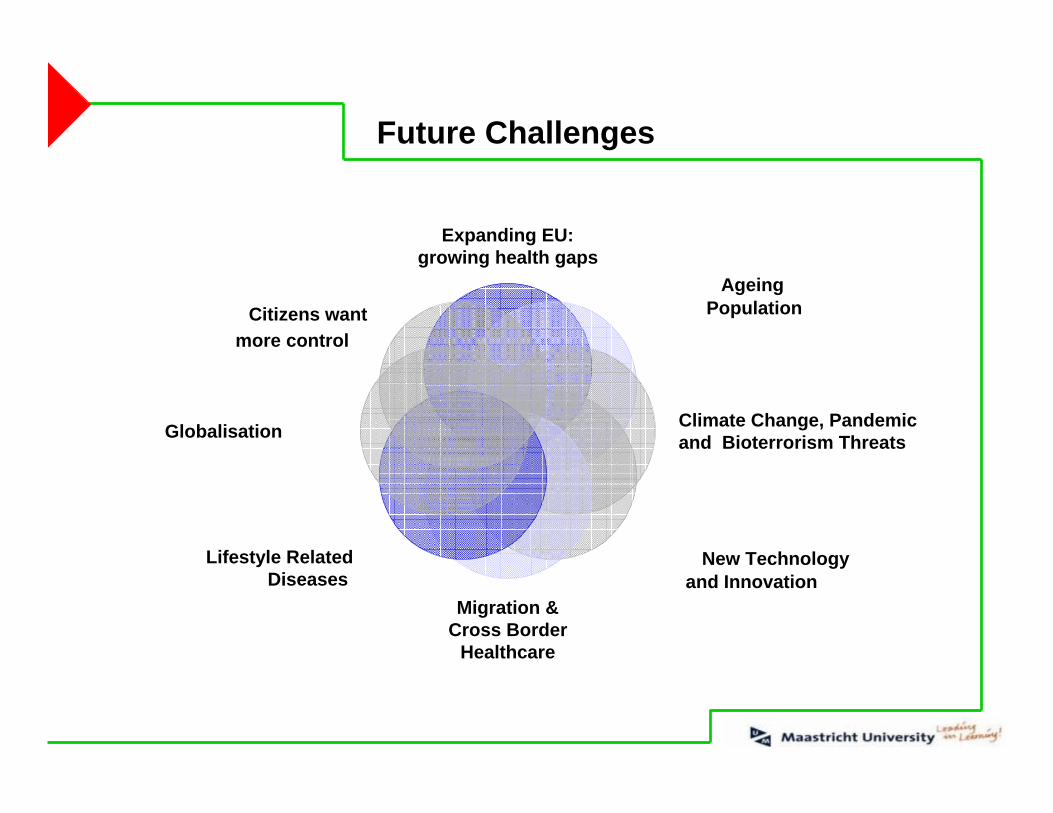
Future Challenges
Expanding EU:growing health gaps
Ageing Population
Climate Change, Pandemic and Bioterrorism Threats
New Technology and Innovation
Migration &Cross Border
Healthcare
Lifestyle Related Diseases
Globalisation
Citizens wantmore control

Future Challenges - Current Strategies
Expanding EU:growing health gaps
Ageing Population
Climate Change, Pandemic and Bioterrorism Threats
New Technology and Innovation
Migration &Cross Border
Healthcare
Lifestyle Related Diseases
Globalisation
Citizens want more control
Pharmaceutical Forum, PHGEN
Health information and Health Portal
ECDC, Organe Donation
Interactions with WHO
Health services Initiative
Health investments in the Structural Funds
White paper on NutritionCommunication on AlcoholTobacco control strategy
Projects fundedCross-sectoral work

EU Health Strategy as a Research Agenda
Expanding EU:growing health gaps Ageing
Population
Climate Change, Pandemic and Bioterrorism Threats
Lifestyle Related DiseasesMigration &
Cross BorderHealthcare
New Technology and Innovation
Globalisation
Citizens wantmore
control
White paper on NutritionCommunication on AlcoholTobacco control strategy
Health information and Health PortalProject HLS-EU
ECDC
Interactions with WHO
Health Services InitiativeProject EUREGIO II
Health investments through Structural Funds etcProject Euregio II/III
E-HealthPublic Health Genomics
Cross-sectoral work
EC 2007

3. The EU Health Strategy

Health Strategy – Process 2006/2007
1. Open Consultation with 152 responses received
2. Health Impact Assessment
3. Adoption of the Strategy White Paper – 2007
4. Implementation and regular monitoring of results

Health Strategy: Consultation Results 1/2
2004 „Reflection Process“ and 2006-2007 Consultation:
- Health in All Policies Approach
- Focus on health promotion
- Bridge health inequities
- Tackle global health issues

Health Strategy: Consultation Results 2/2
2004 „Reflection Process“ and 2006-2007 Consultation:
- Address other key issues: ageing, technology, cross-border issues
- Take action where EU added value is clear
- Development of and access to comparable data
- EU, Member States and stakeholders should worktogether for concrete results: the strategy´s successlinked to the sense of ownership at local, regional and national level.

Principles for the Strategy 1/2
1. a Value-Driven approach- Health as a Fundamental Right- Engaging with Citizens, improving information and data,equity, solidarity, etc…
2. „Health is Wealth“- HLY in the Lisbaon Agenda- Recognising the economic benefits of cost-effectivehealth investments

Principles for the Strategy 2/2
3. Health in All Policies (HiaP)- Bilateral work with (e.g.) Regional Policy on HealthInvestments, Employment on healthy workplaces, Enterprise on innovation
- Encouraging new partnerships at all levels
4 . Global Health- Strengthening EU´s voice on global stage- Tackling shared issues such as pandemic, climate change

Strategic Objectives for the Strategy
1. Support Healthy Ageing through a lifecycle approach and reduce inequities in health
2. Protect citizens from the threats to health such as ClimateChange
3. Support a sustainable future for health and health systemsthrough new technologies
Implementation: StructuredCooperation Mechanism
1. „Together for Health“ needs to be implemented by all players in partnership
2. New mechanism will:- Develop guidelines and exchange good practice- Report and make recommendations- Agree indicators and measure progress
3. Accompanied by:- Review of existing mechanisms and bodies and a fresh look
at involvement of other stakeholders

Implementation: a shared process
• Article 152 TEC– Public Health, parag. 2: ‘ The Community shall encourage cooperation
between the Member States (…) and if necessary, lend support to their action. Member States shall in liaison with theCommission, coordinate among themselvestheir policies and their programmes (…) The Commission may, in close contact with the Member States, take any useful initiative to promote such coordination’
• Coming to a new approach to work hand in hand withMember States

Health & Wealth

Health Means Wealth 1/2
Source: M. Suhrcke, M. McKee, R. Sauto Arce, S. Tsolova, J. Mortensen The contribution of health to the economy in the EU, Brussels 2005

Health Means Wealth 2/2
• Healthier citizens ⇒ reduced strain on healthcare system, but also:
• Healthy Adults:– are more likely to be in the workforce – in ageing Europe healthy
active workforce will be a key determinant of sustainable productivity– are more productive– work and live longer and save more for retirement
• Healthy Children– have better schooling outcomes and education ⇒ less school
absenteeism and early drop-out ⇒ indirectly contribute to future productivity.
– lead to lower child mortality ⇒ increased future labour supply and less strain on pension systems
⇓a more competitive economy

Tallinn Charta on Health Systems 2008
The contribution of regions to health and wealthTechnical report for the WHO European Ministerial Conference on Health Systems: “Health Systems, Health and Wealth”, Tallinn, Estonia,25–27 June 2008
www.euro.who.int/Document/
E91414.pdf

Healthy Life years –A Lisbon Structural Indicator
Men 85% of life free of disability
Females 80% of life free of disability
Diverging trends: Increase: AT, BE, IT, FI, DEStable: F, EL, IR, ESDecrease: DK, PT, NL, S, UK
Due to ageing, health care spending is expected to rise in most Member States. However, if healthy life years increase at the same rate as life expectancy, this cost will be halved.
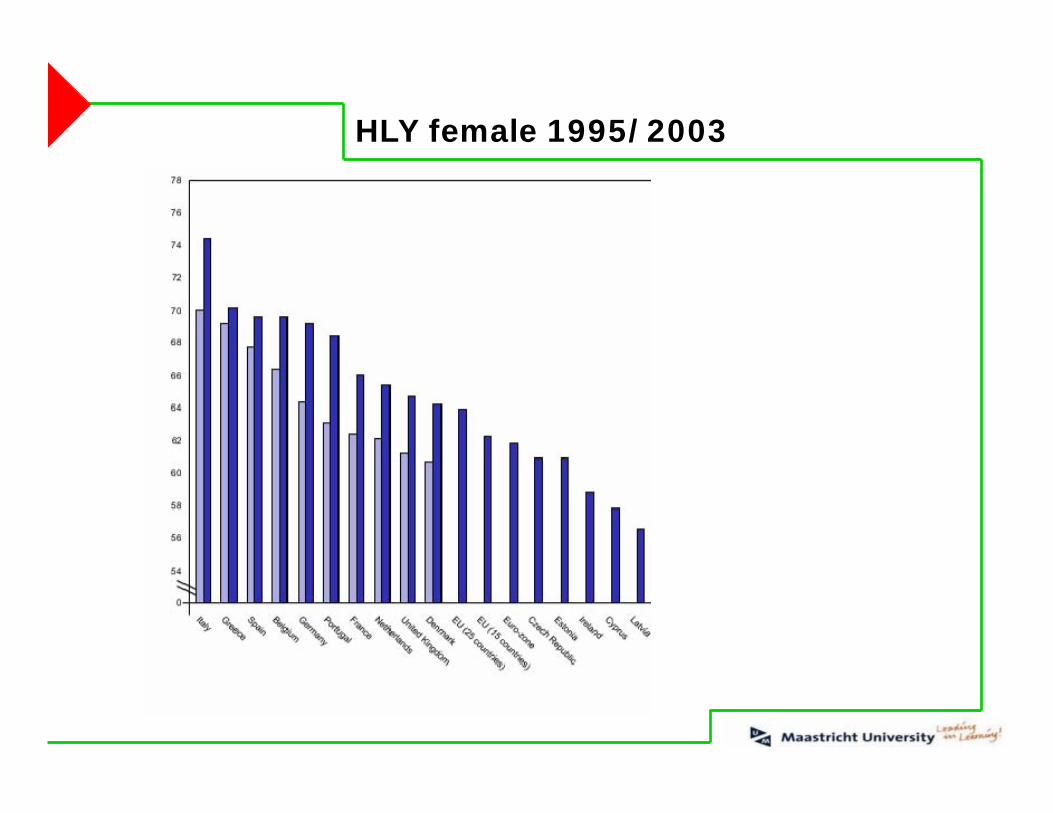
HLY female 1995/2003

HLY male 1995/2003

Current European Health Potential - (males 2003)
40,00 45,00 50,00 55,00 60,00 65,00 70,00 75,00 80,00
AT BE CY CZ DE DK ES FI FR GR HU IE IT MT NL PL PT SE UK
Lowest HLY Highest HLY Average exit rate labour market HLY at birth

Health in all policies within the Commision
– EMPL: OMC on social protection and social inclusion– ECFIN: Budgetary impact of changes in the demographic and
health status– INFSO: eHealth action plan– Research: FP7, Innovative Medicine Initiative– Environment: Drinking water directive– Education: Social competence being a key European
competence– Taxation: Tobacco taxation– JLS: Action plan on Drugs

Health Programme 2008-2013 1/3
Health Programme 2008-2013 2/3
Health Programme 2008-2013 3/3

Crossborder cooperation in the health sector –lessons learned for future cooperation
Outcomes of the „EUREGIO“ project Project term: 1 June 2004 – 31 May 2007
Now followed up by EUREGIO II (2008 – 2010) and EUREGIO III (2008 - 20100
Funded by the European Union

Background of EUREGIO
- Instruments to support cooperation: Community Initiative INTERREG, Euroregions and similar structures
- Existing multitude of cross-border activities in health
- Increasing need for information, exchange and coordination
Recommendation:
“To evaluate existing cross-border health projects, in particular Euregio projects, and to develop networking between projects in order to share best practice”(High level process of reflection on patient mobility and healthcare developments in the European Union)
Project aims
• to give an overview of cross-border activities in the field of health in Europe
• to evaluate existing cross-border health-related projects
• to identify models of good practice
• to support co-operation among actors
• to identify promoting and hindering factors
Project management & partners
Project Management• Institute of Public Health North Rhine-Westphalia (lögd)
Project Partners• Ministry of Employment, Health and Social Affairs of the State of
North Rhine-Westphalia (MAGS)
• AOK Rheinland (sickness fund)
• Municipal Health Service, District of Heinsberg
• University of Applied Sciences, Bielefeld
• Association of European Border Regions (AEBR)
• European Public Health Centre (EPHC)
• European Hospital and Healthcare Federation (HOPE)
• German-Polish Health Academy

Methods and project development
Survey among 67 Euregios and similar structures & 53 Interreg IIIA-Secretariats
Survey among about 300 projects
Preselection of 40 “Models of good practice”
EUREGIO- Workshop (January 2006)
In-depth interviews with selected “Models of good practice”
Final EUREGIO conference (March 2007)
Final Report

Survey among 67 Euregios and similar structures & 53 Interreg IIIA-Secretariats
Survey among about 300 projects
Preselection of 40 “Models of good practice”
EUREGIO- Workshop (January 2006)
In-depth interviews with selected “Models of good practice”
Final EUREGIO conference (March 2007)
Final Report

Interviewed: 67 Euregios and similar structures (30 countries)
Response: 47 questionnaires (28 countries)
- Heterogeneity of Euregios and similar structures
- for 76 % health is a very important or important issue
- 37 cross-border structures which are/were active in the health sector (at least one working group or one project)
- different kind of activities: - working groups- projects- events- agreements
Euregio-Survey: Results (Overview)

Euregio-Survey: Working Groups
N= 26
0 10 20 30 40 50 60 70 80 90 100
Others
Development of healthtargets
(Co-)decision on projectapproval
Consultation of decisionmakers
Drawing up of conceptsfor action
Expert opinion on projectproposals
Development of their ownproject proposals
Carrying out of projects
Exchange of informationbetween members
(%)

Euregio-Survey: Working Groups
Working Groups in Health (N=27)
No Working Groups in Health (N=18)
No information (N=20)
Special case (N=3)
� � � � �
� �
� � � ���
��
�
��
�
�
�
�
� � � �
�� � � � �
��
� � � � �
�������
���
�������������
�������������
������
��������
�����������
������
�������
�����������
������� ���������
�������
�������
��!�"���# $���%��
&'�����!�"���
��%����
(������
)�*��"���
(�����
����'������
������
+�����
�����������"��
�����,+��'���%���
$��������
������
$�������
(�"�����
&�����
��%����
���� �!���
�������
$����
& !���
-����
.�����
)��%��
)��������
$������ /�������0
)�������������
������
��
��
��
��
�
���
��
��
�
�
�
�
�
�
�
�
�
������
��
��
��
�
����
�
�� ��
�
��
����
��
����
��
�
��
��
���
����
�
��
����
�
��
��
��
��
������
��
��
��
��
��
��
Survey among 67 Euregios and similar structures & 53 Interreg IIIA-Secretariats
Survey among about 300 projects
Preselection of 40 “Models of good practice”
EUREGIO- Workshop (January 2006)
In-depth interviews with selected “Models of good practice”
Final EUREGIO conference (March 2007)
Final Report

- general information
- target groups
- project description (e.g. subjects, starting position, objectives)
- project partners and cooperation
- public relation/interest of the public
- project evaluation
- continuation of project activities
- project financing
- promoting and hindering factors
Survey among the Projects: Content of the Questionnaire
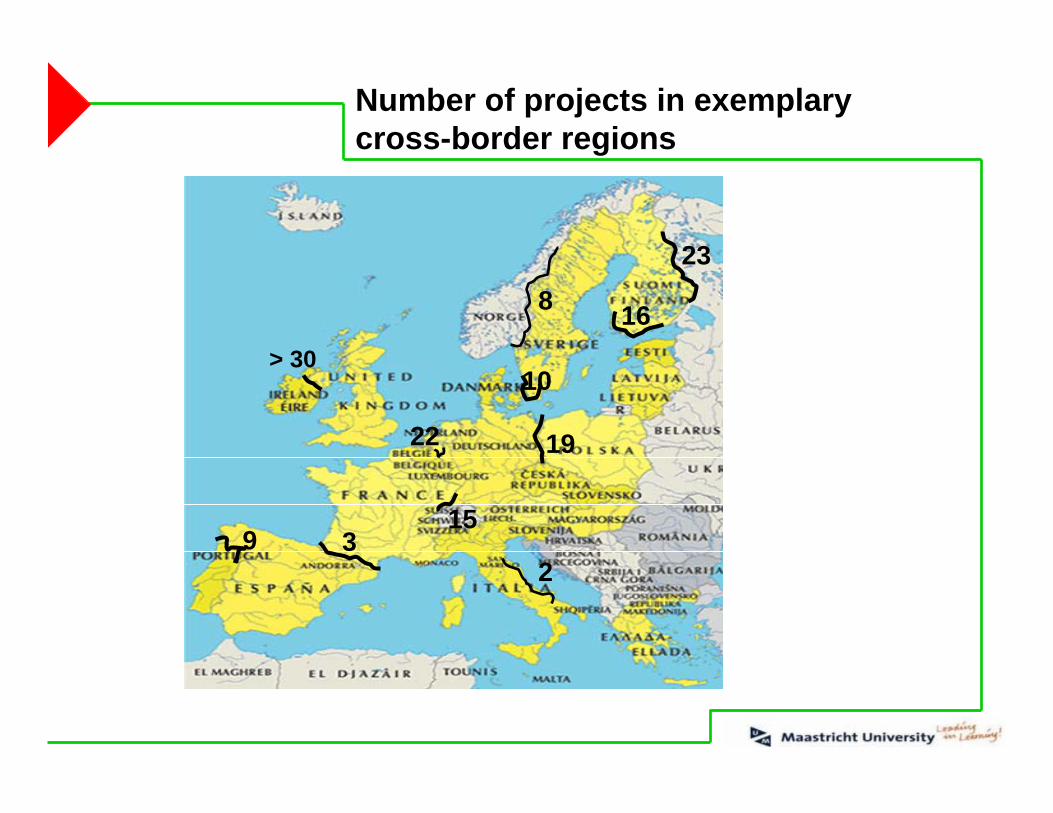
9 3
> 30
22
8
10
Number of projects in exemplary cross-border regions
16
23
15
19
2

0
10
20
30
40
50
60
70
DE NL FR BE FI IT AT SE UK DK IE ES PT LU PL CZ SK EE SL HU RU CH NO LI BA AL CS HR
(N)
N=122
Survey among the Projects: Participating States
EU-15 New Member States
EU non-members

Survey among the Projects: Areas of Activities
11
20
21
22
28
36
40
40
43
47
0 10 20 30 40 50
Telemedicine
Rescue services / Disaster control
Rehabilitation
Nursing care
Research
Quality assurance / development
Prevention / Health promotion
Outpatient / Inpatient treatment
Joint use of resources
Training & further education
(%)
Multiple answers possible, N=122

Survey among the Projects: Topics Influencing Patient Mobility
* Projects with the main focus on outpatient / inpatient treatment only
0
5
10
15
20
25
30
35
Quality assurance / development*
simplified access / useof health services*
Information /transparency
consultation services*
Telemedicine
Northern Europe and Baltic Central and Eastern Europe
North-Western Europe Alpine and Danube region
South Western Europe / Western Mediterranean

Projects are very heterogeneous: issues, duration, number of partners etc.
+ lots of activities to ensure sustainability
+ nearly all projects meet two or more “partnership-criteria”
- Information about the projects (reports, Internet) is only partly available.
- Project-evaluation is not generally common.
- Some projects work without partnership agreements.
Projects rely very much on the personal commitment of actors involved
Survey among the Projects: Strength and Weakness

Assessment of Promoting Factors
• Commitment of actors (mean 3.8)
• Experiences of partners (3.5)
• Recognizable benefit (3.4)
Four scale assessment from “not promoting/hindering” (1) to “very promoting/hindering” (4)
Assessment of Hindering Factors
• Financial problems (mean 3.3)
• Application procedure (3.2)
• Amount of administrative work (3.1)
• Legal problems (2.7)
• Data protection problems (2.3)
N=105N=104
Survey among the Projects: Promoting and hindering factors
Patient Mobility: Problems and Challenges
• Language, culture
• National budgeting rules
• Differences in compensation systems (DRG vs. DBC)
• Differences in tariffs
• Legal uncertainty, liability
• Lack of information (patients, service providers)
• Complicated processes

Survey among 67 Euregios and similar structures & 53 Interreg IIIA-Secretariats
Survey among about 300 projects
Preselection of 40 “Models of good practice”
EUREGIO- Workshop (January 2006)
In-depth interviews with selected “Models of good practice”
Final EUREGIO conference (March 2007)
Final Report

EUREGIO-Workshop (20/21 January 2006)
Outcomes
- exchange of information and experience (“learning from each other”)
- networking and the building of partnerships
- dissemination of good-practice models
- proposals on how to strengthen cross-border cooperation in health
About 100 representatives from 15 European countries
Plenum sessions and five parallel working groups

Conclusions & Products

Conclusions: Support Needs?!
- Legal certainty
- Cooperation agreements between actors
- Access to subsidies
- Reduction of bureaucratic hindrances
- Exchange of experience and information
- Documentation and public relations
- Project evaluation
Recommendations for action for:
(a) project actors
(b) to European, national and/or regional actors

Outcomes/Products
Events (workshop, final conference)
Workshop documentation
Systematic analysis of the project landscape
Models of good practice
Identification of hindering & promoting factors
Recommendations for action
Website including e.g. project-portal
Interim reports, final report
Products available at:www.euregio.nrw.de
“Models of good practice” in cross-border health

Exclusion criteria e.g.- Project not yet started- Health is only a subordinate issue- Mere study or mere research project - Activity without project character (working group, event)- Substantial information is missing - Framework project
Procedure and methods (I)
1. Survey among responsible bodies of about 300 projects (2005)
2. 149 completed project questionnaires (2005)
3. Pre-selection: exclusion criteria (2005)

Selection criteriaClear aims and outcomes/products Sustainability Cross-border added value Real need for project Contents and methods Collaborative work across bordersPublic relations and documentation Innovative characterEvaluation
Procedure and methods (II)
4. Preselection of 40 “models of good practice“ (2005)
5. Workshop with representatives of the 40 projects (January 2006)
6. In-depth interviews with selected projects (2006)
7. Selection of awarded projects (2006)

“Models of good practice“ in five areas of health care
Hospital collaboration
Prevention / health promotion
Telemedicine
Disaster control / rescue service
Patient mobility

“Models of good practice“in the field of
hospital collaboration

Common Cross-Border Hospital Cerdanya and Capcir (2005-2008)
Aims: Ensure provision of medical care for the local population & tourists and provide special treatment (e.g. dialysis) by building up a joint cross-border hospital
Highlights
• Substantial need in the region, need assessment (study)
• Joint planning, financing, management, leadership, staff and development of joint tools
• preparation of an intergovernmental framework agreement
• So far: unique project in Europe
FR-ES
ES
FR
State-of-the-Art Medicine along the borders (since 06/2004)
Aims: • Improve the hospitals’ efficiency, effectiveness
and quality of topclinical services • Secure competitive advantages • In the long run: to become a “European Centre
for State-of-the-Art Medicine and Research“
Highlights
• Cooperation agreement (2004): Synchronization of strategies, assurance of long-term cooperation
• Multi-faceted spectrum of cooperation
• Dual staff responsibility for the leadership of individual departments
DE-NL

“Models of good practice“in the field of
prevention / health promotion
General aim Promote cross-border cooperation within the EMR in the field of risk behaviour prevention in adolescents (alcohol, drugs, tobacco)
Highlights
• Broad multi-level approach: 1. Survey andresearch, 2. Development and implementation of common policies and measurements
• Extensive documentation of project outcomes
• High number of activities to ensure sustainability
“Risicogedrag adolescenten”(10/2001-12/2005)
DE-NL-BE

“Models of good practice“in the field of tele-medicine

Telemedicine network to support tumourcare in the POMERANIA Euroregion(since 2002)
Aims• improve patient care in the project
area: quality and time lapse in diagnosis, therapy and medical care
• efficient use of scarce resources, cost reduction
Highlights
DE-PL
• Broad spectrum of activities in telemedicine: teleconferences, tele-radiology, telepathology
• Elements integrated through a teleconference server
• Further planned activities: extension to include other areas (tele-cardiology, palliative medicine), integration of clinics in Brandenburg,self-financing by the involved clinics

Standardisation of treatment in patients with HIV, HVC and other infectious pathologies (09/2004 - 09/2006 )
AimImprovement and standardisation of medical care for patients with infectious diseases (HIV/AIDS, tuberculosis etc.)
Highlights
• broad approach (tele-communicationnetwork, staff exchange programmes,joint research, joint use of resources etc.)
• Prospects: Continuation of cooperation andextension to also include other depart-ments are planned
University hospital of NiceArchet
Hospital San Remo
IT-FR

“Models of good practice“in the field of
rescue services / disaster control

EUMED (01/2005 – 12/2007)Aim: Immediate assistance in the event of emergencies and serious accidents: cross-border cooperation is vital
Highlights• Multi-faceted spectrum of elements:
routine rescue operations, large-scale disasters, training
• Products for long-term cooperation: Euregional ambulance assistance plan, Euregional casualty distribution plan, Euregional training
• Evaluation by testing and implementinginto practice & by alarm exercises
Meuse-Rhine
DE-NL-BE

“Models of good practice“in the field of
(patient) mobility
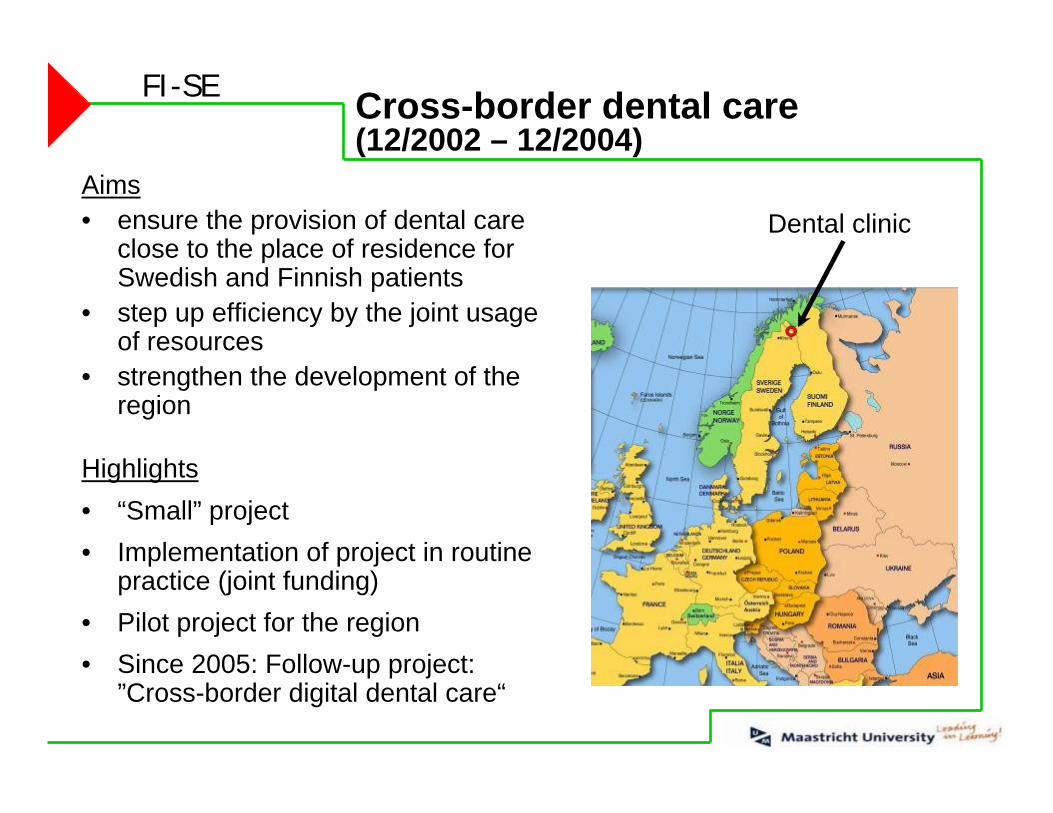
Cross-border dental care(12/2002 – 12/2004)
Dental clinicAims• ensure the provision of dental care
close to the place of residence for Swedish and Finnish patients
• step up efficiency by the joint usage of resources
• strengthen the development of the region
Highlights• “Small” project• Implementation of project in routine
practice (joint funding)• Pilot project for the region• Since 2005: Follow-up project:
”Cross-border digital dental care“
FI-SE

Project package
IZOM- Integration Zorg opMaat (DE-NL-BE)
Contracting Belgian Health Care (NL-BE)
Euregio Health Portal (DE-NL-BE)
Health Card international (DE-NL)
General aim: Eased access to cross-border health care

Project package
IZOM - Integration Zorg op Maat (since 1997)Opportunities for free access to health care services across the border: inpatient and outpatient treatment, specialist treatment, supply of medicines, supply of medical aids (with additional permission)
Health Card international (since 2000)Simplify processes and ease access to health care services across the border by a chip card system (25,000 cards issued)
Contracting Belgian Health Care (since 2001)Ease access to cross-border health care by contracts with hospitals in Belgium (inpatient & outpatient treatment)
Euregio Health Portal (since 2002)Internet platform: information on health care at home and in the neighbouring countries

![[PPT]Health care planning - Home | University of Pittsburghsuper4/36011-37001/36671.ppt · Web viewDr. Hamda Qotba, M.D, MFPH, FFPH * Planning The process of setting goals, developing](https://img.pdfslide.us/doc/110x75/5aa692f67f8b9a1d728e9c6d/ppthealth-care-planning-home-university-of-super436011-3700136671pptweb.jpg)




























