Embed Size (px)
Citation preview
ESPEN Congress Madrid 2018
Peri-Operative Care, More Than 15 Years Of Eras Approach
The Eras Approach In GI SurgeryD. Lobo (UK)

The ERAS Approach In GI Surgery
Dileep N Lobo
Professor of Gastrointestinal Surgery
University of Nottingham, UK

Declaration of Interests
• Unrestricted research grant from BBraun for unrelated work
• Speaker’s honoraria from • Fresenius Kabi• BBraun• Baxter Healthcare
• Chair of the Scientific Committee of the ERAS® Society The Weaning of Furniture-Nutrition, Salvador Dalí

Learning Objectives
•Know the nutritional screening and care procedures
•Know about applicability in malnourished patients
•Know the impact of ERAS on outcome

The metabolic response to trauma
• Foundation for modern nutritional therapy of the seriously ill or injured patient
• First to demonstrate that tissue damage per se could not have been the main
source of nitrogen loss
• Peak in urinary nitrogen loss occurred 3-8 days after injury
• Trauma stimulated net protein catabolism
• Main source of nitrogen excretion in the urine was skeletal
muscle
Cuthbertson DP, Biochem J 1931 & QJM 1932


Kehlet’s regimen
• 9 patients > 70 yrs of age (8 completed the trial)
• Laparoscopic colonic surgery
• Thoracic epidural analgesia
• Avoidance of opioids
• Intraoperative and early postoperative of fluids median 1275 ml (650-2300 ml)
• No drains
• Single dose of antibiotics
• Prokinetics (Cisapride)
• Removal of catheter after 24 h
• Early mobilisation
Bardram L, et al. Lancet 1995

Br J Surg 2009

Undernutrition and the surgical patient
•More intensive treatment
•High dependency nursing
• Increased hospital stay
•Higher cost of care
• Increased morbidity and mortality
•Reduced quality of life
Studley HO JAMA 1936

Nutritional & Metabolic Care of the Surgical Patient• Avoidance of prolonged preoperative fasting
• Re-establishment of oral feeding as early as possible after surgery
• Integration of nutrition into the overall management of the patient
• Metabolic control, e.g. of blood glucose
• Reduction of factors which exacerbate stress-related catabolism or
impair GI function, optimise symptom control
• Early mobilisation
• Screening for malnutrition
Weimann A, et al. Clin Nutr 2017

Preoperative counselling
• Patients should receive oral and written preadmission
information describing what will happen during
hospitalization, what they should expect, and what their role
is in the recovery process.
Nutritional screening
• MUST (malnutrition universal screening tool)
• NRS 2002

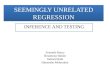
MUST score and clinical outcomes
*
**
*
Ben-Ishay O, et al. Gastro Res Prac 2011

The real world
Breuer JP, et al. Zentralbl Chir 2013
Martin L, et al. JPEN 2018

Malnutrition – ESPEN definition
• option 1: BMI<18.5 kg/m2
• option 2: combined: • weight loss >10% or >5% over 3 months
• and reduced BMI or a low fat free mass index (FFMI).
• Reduced BMI is <20 in patients <70 years
• Or <22 kg/m2 in patients ≥70 years
• Low FFMI is <15 in females
• Or <17 kg/m2 in males
Weimann A, et al. Clin Nutr 2017

Who may benefit from preoperative nutrition?
• Weight loss >10-15% within 6 months
• BMI <18.5 kg/m2
• SGA Grade C or NRS >5
• Serum albumin <30 g/l (with no evidence of hepatic or renal
dysfunction)
• And perhaps, those with sarcopenia and/or myosteatosis
Weimann A, et al. Clin Nutr 2017
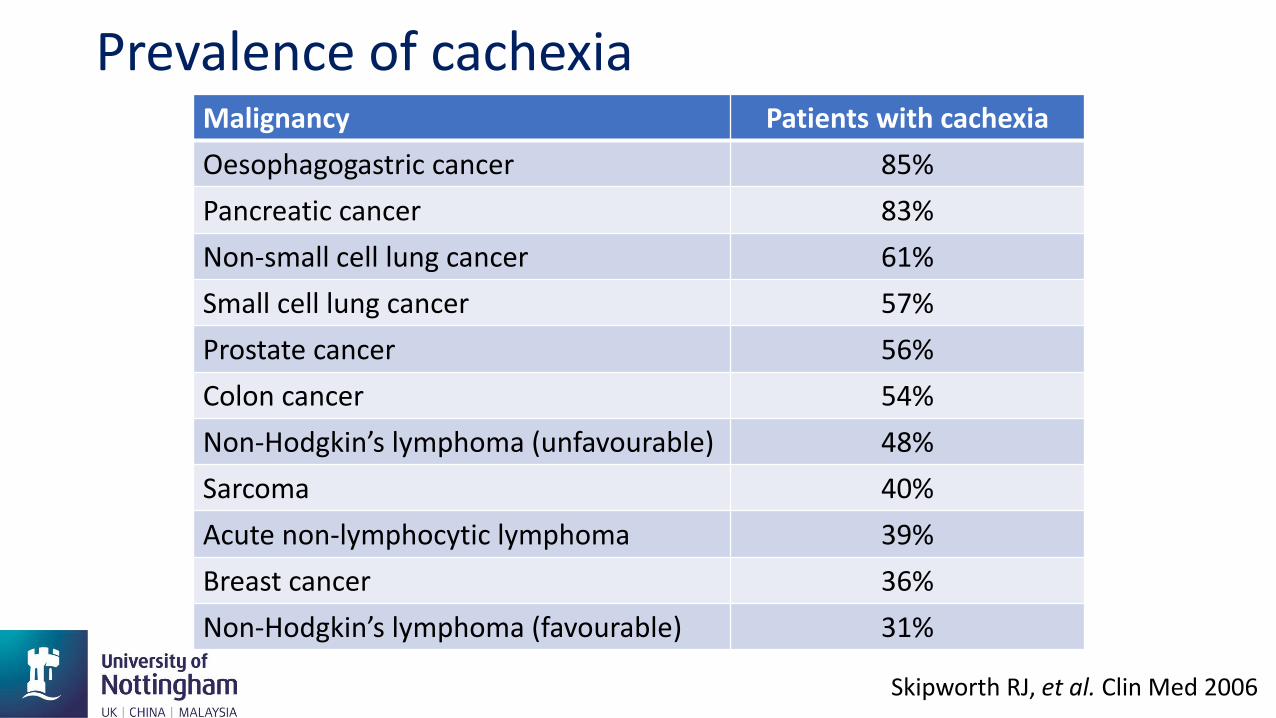
Malignancy Patients with cachexia
Oesophagogastric cancer 85%
Pancreatic cancer 83%
Non-small cell lung cancer 61%
Small cell lung cancer 57%
Prostate cancer 56%
Colon cancer 54%
Non-Hodgkin’s lymphoma (unfavourable) 48%
Sarcoma 40%
Acute non-lymphocytic lymphoma 39%
Breast cancer 36%
Non-Hodgkin’s lymphoma (favourable) 31%
Skipworth RJ, et al. Clin Med 2006
Prevalence of cachexia
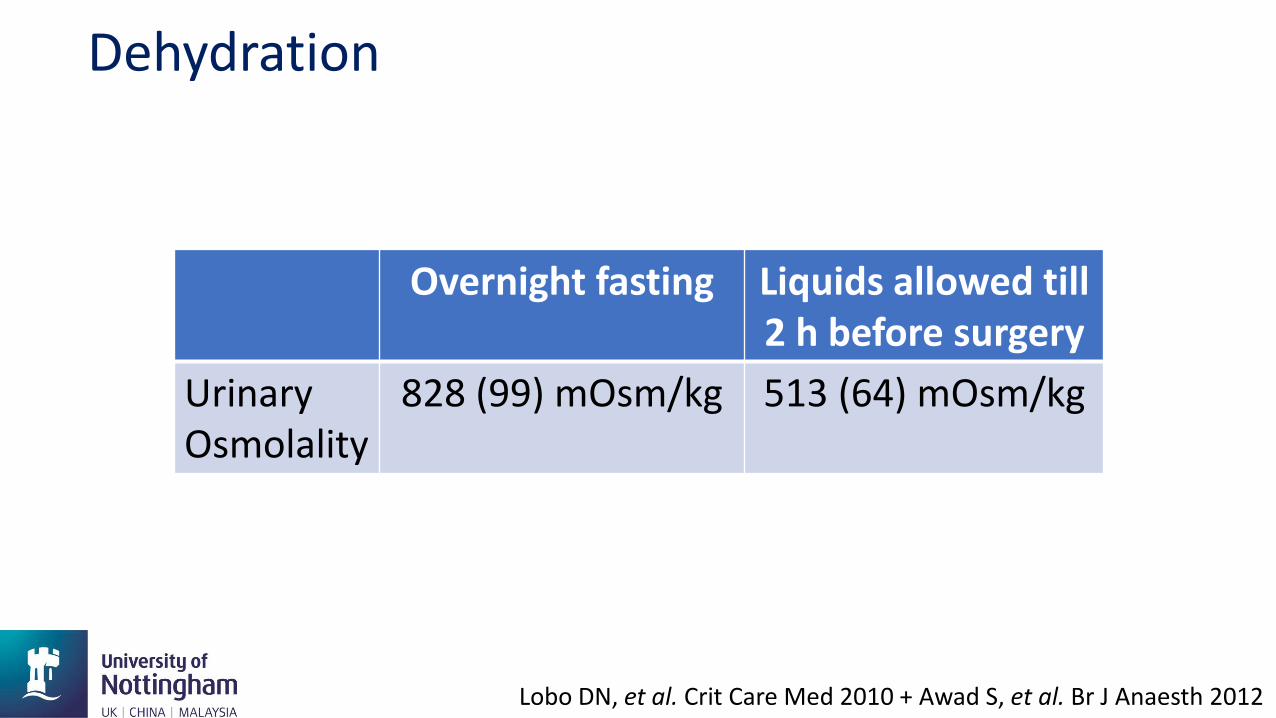
Dehydration
Overnight fasting Liquids allowed till 2 h before surgery
Urinary Osmolality
828 (99) mOsm/kg 513 (64) mOsm/kg
Lobo DN, et al. Crit Care Med 2010 + Awad S, et al. Br J Anaesth 2012

Preoperative Fasting and Carbohydrate Loading
• The duration of preoperative fasting should be 2 hours for liquids and 6 hours for solids (grade A)
• Patients should receive carbohydrate loading preoperatively
• Reduces thirst, hunger and postoperative insulin resistance

21 RCTs 1685 patients – 733 CHO, 952 Control

In-hospital complications: OR 0.99 (0.50-1.53), P=0.640


Preop CHO: Control of Postop. Glucose
Giannotti L, et al. Ann Surg 2017
Major surgeryCHO vs placeboInsulin at [Glu] > 10 mM
Need for Insulin: 2.4 vs 16% p<0..001NNT 7

ERAS and nitrogen balance
Soop M, et al. Br J Surg 2004

Preoperative immune enhancing nutrition
NOTE: Weights are from random effects analysis
Overall (I-squared = 34.8%, p = 0.111)
Xu
McCarter
Mikagi
Braga
ID
Fujitani
Okamoto
Aida
Giger-Pabst
Gunerham
Martin
Braga2
Gianotti
Study
0.94 (0.71, 1.23)
0.25 (0.06, 1.08)
4.14 (1.07, 15.97)
0.33 (0.04, 2.80)
1.33 (0.31, 5.65)
RR (95% CI)
1.18 (0.78, 1.78)
1.00 (0.28, 3.63)
0.88 (0.58, 1.34)
1.06 (0.49, 2.29)
2.03 (0.47, 8.81)
0.50 (0.24, 1.05)
1.33 (0.62, 2.88)
0.73 (0.53, 1.02)
100.00
3.08
3.56
1.55
3.16
Weight
17.45
3.86
17.24
8.75
3.07
9.24
8.73
20.31
%
0.94 (0.71, 1.23)
0.25 (0.06, 1.08)
4.14 (1.07, 15.97)
0.33 (0.04, 2.80)
1.33 (0.31, 5.65)
RR (95% CI)
1.18 (0.78, 1.78)
1.00 (0.28, 3.63)
0.88 (0.58, 1.34)
1.06 (0.49, 2.29)
2.03 (0.47, 8.81)
0.50 (0.24, 1.05)
1.33 (0.62, 2.88)
0.73 (0.53, 1.02)
100.00
3.08
3.56
1.55
3.16
Weight
17.45
3.86
17.24
8.75
3.07
9.24
8.73
20.31
%
.1 1 100
NOTE: Weights are from random effects analysis
Overall (I-squared = 63.9%, p = 0.001)
Mikagi
ID
Gianotti
Giger-Pabst
Fujitani
Xu
Braga2
McCarter
Okamoto
Torrinhas
Horie
Martin
Aida
Braga
Study
0.53 (0.34, 0.82)
0.33 (0.01, 7.50)
RR (95% CI)
0.45 (0.26, 0.80)
0.86 (0.36, 2.05)
1.03 (0.65, 1.61)
0.29 (0.06, 1.26)
1.50 (0.67, 3.35)
2.95 (0.71, 12.34)
0.25 (0.06, 1.08)
0.44 (0.21, 0.91)
0.07 (0.00, 1.16)
0.11 (0.03, 0.34)
0.47 (0.23, 0.94)
0.38 (0.16, 0.88)
100.00
1.73
Weight
11.50
9.08
12.40
5.37
9.62
5.64
5.48
10.17
2.05
7.30
10.41
9.25
%
0.53 (0.34, 0.82)
0.33 (0.01, 7.50)
RR (95% CI)
0.45 (0.26, 0.80)
0.86 (0.36, 2.05)
1.03 (0.65, 1.61)
0.29 (0.06, 1.26)
1.50 (0.67, 3.35)
2.95 (0.71, 12.34)
0.25 (0.06, 1.08)
0.44 (0.21, 0.91)
0.07 (0.00, 1.16)
0.11 (0.03, 0.34)
0.47 (0.23, 0.94)
0.38 (0.16, 0.88)
100.00
1.73
Weight
11.50
9.08
12.40
5.37
9.62
5.64
5.48
10.17
2.05
7.30
10.41
9.25
%
.1 1 100
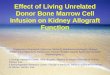
Infectious complicationsOR 0.53 (95% CI 0.34-0.82)( I2 = 63.9%)
Overall morbidityOR 0.94 (95% CI 0.71-1.23) ( I2 = 34.8%)
Skorepa P, et al. ESPEN 2018

Measured REE - kcals/day
0
500
1000
1500
2000
2500
0 500 1000 1500 2000 2500 3000
Esti
mat
ed R
EE -
kcal
s/d
ay
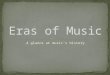
Energy Expenditure in Patients

How much is needed?
•Give 1.0 – 1.3 RMR• Most patients need 30-35 Cal/kg/day
• 50% non-protein energy requirement from fat and50% from carbohydrate.
• Protein requirements range from 1.2-1.5 g/kg/day.
•Permissive underfeeding?• 20 Cal with 1 g protein/kg/day.

What to give?
• Macronutrients• Protein, CHO, Fat
• Micronutrients• Fat soluble vitamins: A, D, E & K• Water soluble vitamins: B group, C, etc.
• Electrolytes• Na, K, Ca, Mg, PO4
• Elements• Fe, Zn, Cu, Se, Mn
Weimann A, et al. Clin Nutr 2017
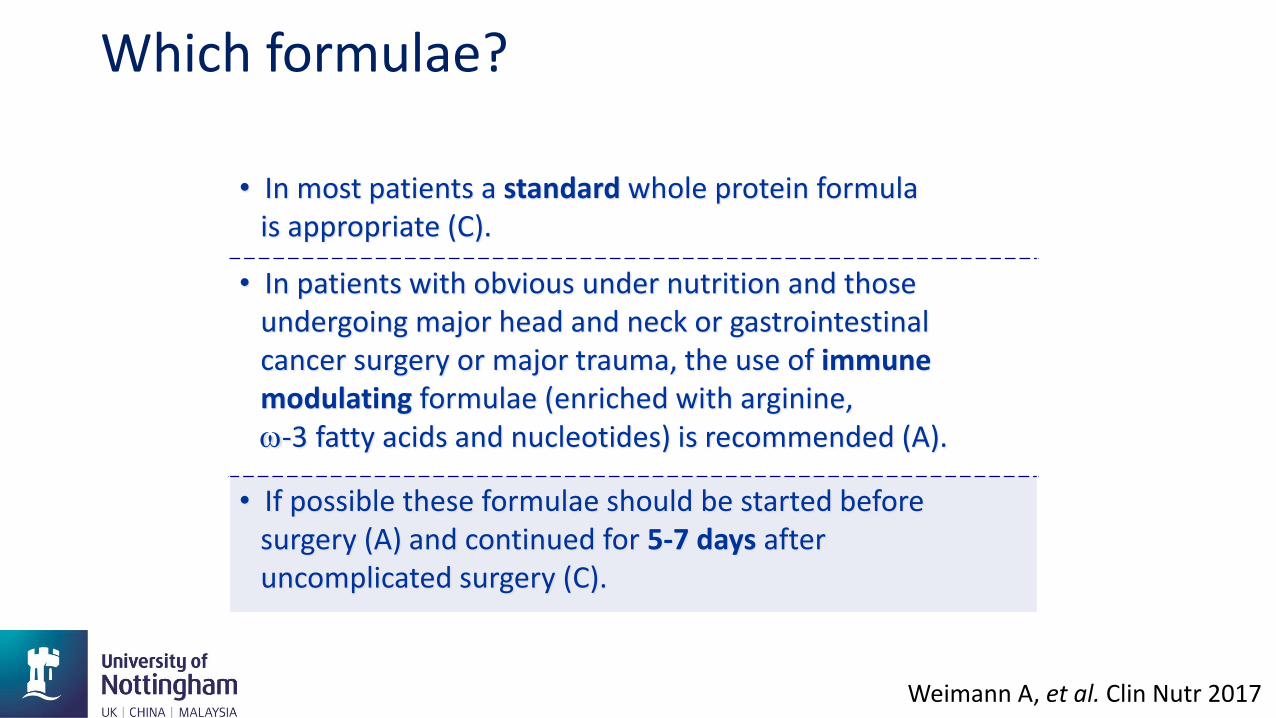
• In most patients a standard whole protein formulais appropriate (C).
• In patients with obvious under nutrition and thoseundergoing major head and neck or gastrointestinal cancer surgery or major trauma, the use of immunemodulating formulae (enriched with arginine,-3 fatty acids and nucleotides) is recommended (A).
• If possible these formulae should be started beforesurgery (A) and continued for 5-7 days afteruncomplicated surgery (C).
Which formulae?

Postoperative nutrition
Martindale R, et al. JPEN 2013

Postoperative nutrition
Martindale R, et al. JPEN 2013

Nutr Hosp 2014

Clin Nutr 2009

World J Surg 2014

• Advice by specialised dietitian
• Aim: weight increase by energy intake 1.3-1.5 x REE
• Encouragement for oral intake and supplementation with ONS
• Neoadjuvant period: once or twice a week phone call – nutritional problems weight
control – in case of inadequate oral intake tube feeding
• Intraoperatively FNCJ
• Postoperatively until discharge: twice a week visit by the dietitian
• Post discharge or during adjuvant chemo- or radiotherapy every 1-2 weeks for 3 months,
afterwards regular contact at least once per month until the end of the first year
Ligthart-Melis GC, et al. Dis Esophagus 2013
The patient at high risk
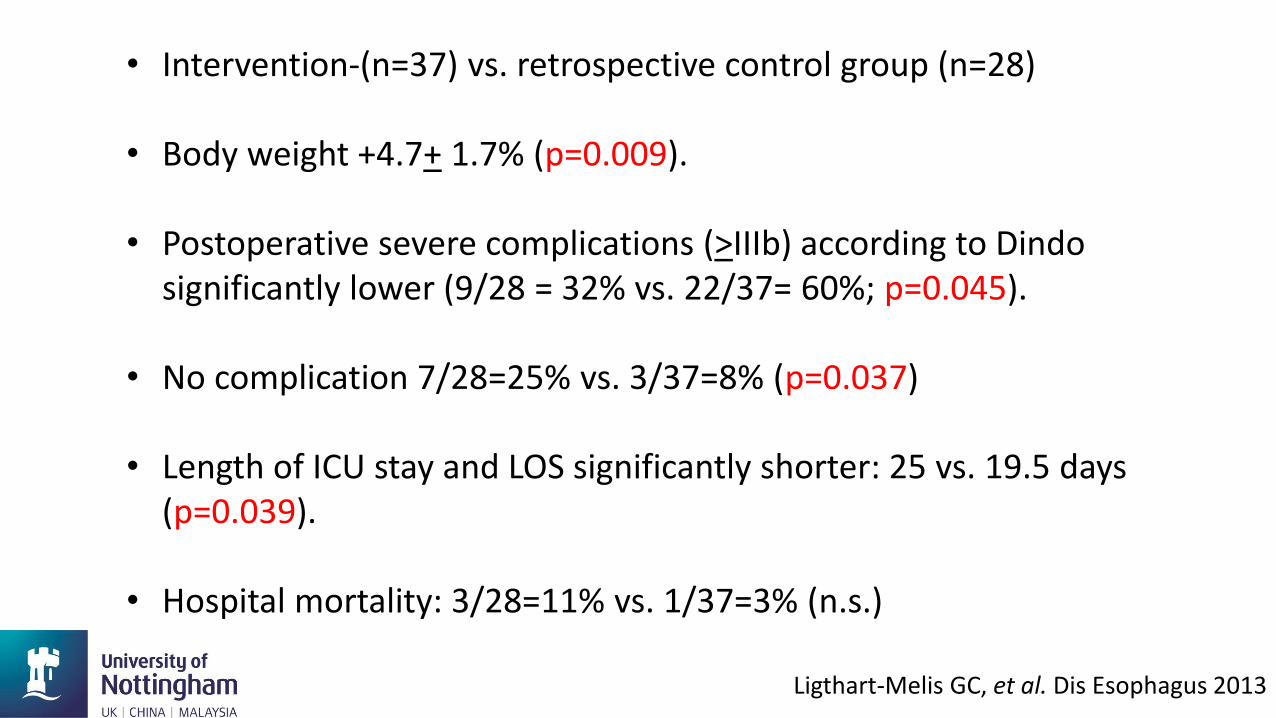
• Intervention-(n=37) vs. retrospective control group (n=28)
• Body weight +4.7+ 1.7% (p=0.009).
• Postoperative severe complications (>IIIb) according to Dindosignificantly lower (9/28 = 32% vs. 22/37= 60%; p=0.045).
• No complication 7/28=25% vs. 3/37=8% (p=0.037)
• Length of ICU stay and LOS significantly shorter: 25 vs. 19.5 days (p=0.039).
• Hospital mortality: 3/28=11% vs. 1/37=3% (n.s.)
Ligthart-Melis GC, et al. Dis Esophagus 2013

Pathophysiology of Postoperative Ileus
Bragg D, et al. Clin Nutr 2015

Strategies to Prevent POI
Bragg D, et al. Clin Nutr 2015

Fluid gain on the ITU
▪ Sodium and water over load may be an inevitable consequence of the resuscitation process.
▪ Septic patients on the ITU gain as much as 12.5 L of body water during the first two days of resuscitation.
▪ It may take up to 3 weeks for patients to excrete this excess load.
Plank L, et al. Ann Surg 1998

Changes in weight and albumin post ITU
Mean weight (kg) Mean serum albumin (g/l)
Admission Nadir Admission At lowest weight
79.3 69.2 21.9 29.8
P<0.00001 P<0.00001
Lobo DN, et al. Clin Nutr 1999

Combining the Elements

Complications
Experimental group= Enhanced Recovery After Surgery (ERAS) Control = Traditional Care (TC)
Varadhan KK, et al. Clin Nutr 2010

Length of hospital stay (days)
Experimental group= Enhanced Recovery After Surgery (ERAS) Control = Traditional Care (TC)
Varadhan KK, et al. Clin Nutr 2010

Readmissions
Experimental group= Enhanced Recovery After Surgery (ERAS) Control = Traditional Care (TC)
Varadhan KK, et al. Clin Nutr 2010

Varadhan KK, et al. Clin Nutr 2010

When is nutritional assessment and therapy indicated in the surgical patient?
• Assess nutritional status before and after major surgery.
• Perioperative nutritional therapy is indicated in patients with
malnutrition and those at nutritional risk.
• Should also be initiated, if it is anticipated that the patient will be unable to
eat for more >5 days perioperatively.
• Also indicated in patients expected to have low oral intake and who cannot
maintain above 50% of recommended intake for >7 days.
Weimann A, et al. Clin Nutr 2017

• If energy and nutrient requirements cannot be met by oral and enteral intake alone (<50% of caloric requirement) for >7 days, a combination of enteral and parenteral nutrition is recommended.
• Parenteral nutrition shall be administered as soon as possible if nutrition therapy is indicated and there is a contraindication for enteral nutrition.
Weimann A, et al. Clin Nutr 2017

When are preoperative oral nutritional supplements and enteral nutrition indicated?
• When patients do not meet their energy needs from normal food it is
recommended to encourage them to take oral nutritional
supplements during the preoperative period unrelated to their
nutritional status.
• Preoperatively, oral nutritional supplements shall be given to all
malnourished cancer and high-risk patients undergoing major
abdominal surgery. A special group of high-risk patients are the
elderly people with sarcopenia.
Weimann A, et al. Clin Nutr 2017

Which patients will benefit from EN after discharge from the hospital?
• Continuation of nutrition therapy after discharge, is advised for patients who have received nutritional therapy perioperatively and still do not cover appropriately their energy requirements via the oral route.
Weimann A, et al. Clin Nutr 2017

Where is the evidence?
• The quality of evidence is still low and unconvincing.
• Many shortcomings in these studies and subsequent meta-analyses.
• Systematic review of 15 studies with 3474 patients that there is no evidence to support enteral or parenteral feeding after pancreatoduodenectomy.
Gerritsen A, et al. Br J Surg 2013

Why is the science of nutrition so messy?
• Not practical to run randomized trials for most big nutrition questions
• Nutrition researchers have to rely on observational studies — rife with
uncertainty
• Many nutrition studies rely on (wildly imprecise) food surveys
• People and food are diverse - heterogeneity
• Conflict of interest is a huge problem in nutrition research
• Even with all those faults, nutrition science isn't futile
Julia Belluz https://www.vox.com/2016/1/14/10760622/nutrition-science-complicated
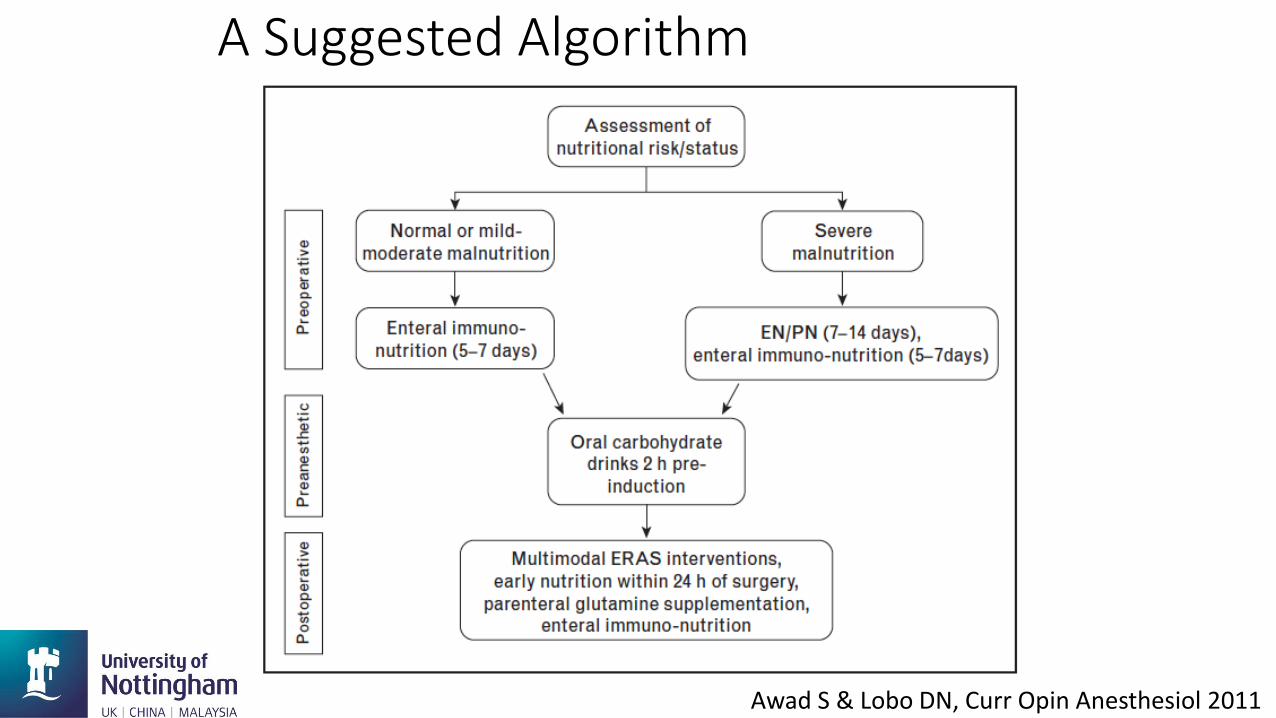
A Suggested Algorithm
Awad S & Lobo DN, Curr Opin Anesthesiol 2011

The Ultimate Nutritional Goal
• To provide optimal nutrition
to all patients, under all
conditions, at all times
Stanley J. Dudrick, MD -1977
Presidential Address, ASPEN