Embed Size (px)
Citation preview

Lung Cancer (2004) 45, 137—142
The epidemiology of bronchioloalveolarcarcinoma over the past two decades: analysis ofthe SEER database�
William L. Reada,c, Nathan C. Pagea, Ryan M. Tierneya,Jay F. Piccirilloa,b, Ramaswamy Govindana,c,*
a Division of Oncology, Washington University School of Medicine, Campus Box 8056, 660 South EuclidAve, St Louis, MO 63110, USAb Divison of Otolaryngology, Washington University School of Medicine, St Louis, MO, USAc Alvin J Siteman Cancer Center, Washington University School of Medicine, St. Louis. MO, USA
Received 23 September 2003 ; received in revised form 13 January 2004; accepted 15 January 2004
KEYWORDSLung cancer;Bronchioloalveolar;Epidemiology;SEER
Summary Bronchioloalveolar carcinoma of the lung (BAC) is a subtype of adeno-carcinoma of the lung. Although traditionally grouped with other non-small cell lungcarcinomas (NSCLC), BAC has uniquemorphological features and clinical behavior suchas bilateral lung involvement, indolent course and lack of association with smoking.Some epidemiologic studies report a significant increase in the incidence of BAC. Weused the SEER database to compare the incidence, demographics, and overall sur-vival of BAC patients as compared to other NSCLC types over the past two decades(1979—1998). Although the incidence of BAC has increased over the past two decades,BAC represents less than 4% of all NSCLC in every time period evaluated. The 1 yearsurvival rate is significantly better for BAC patients relative to other histological sub-types of NSCLC. There has not been amarked increase in the incidence of BAC reportedto SEER over the past 20 years.© 2004 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Bronchioloalveolar carcinoma (BAC) is a rare sub-type of adenocarcinoma of the lung with mor-phology and natural history distinct from otherhistological subtypes of non-small cell lung car-cinoma (NSCLC). Malassez first described BAC ina 47-year-old woman in whom the lungs were
� Data in this manuscript has been presented as an ASCOabstract (A1267, 2002).
*Corresponding author. Tel.: +314-362-4819;fax: +314-362-7086.
E-mail address: [email protected] (R. Govindan).
extensively involved with tumor nodules with‘‘l’aspect du fromage de Roquefort’’ [1]. Malasseznoted the characteristic histology of BAC, withwell differentiated neoplastic cells spreading alongalveoli with little stromal reaction, no invasion,and preservation of alveolar architecture. Thiscontrasts with more typical lung adenocarcinoma,which replaces lung parenchyma with pleiomorphiccells forming disordered glands. BAC is also re-markable for its tendency to remain confined to thelungs, as opposed to other types of NSCLC, whichrapidly metastasize. The epidemiology of BAC isdifferent from other NSCLC. It has been noted forover 50 years that BAC afflicts men and women in
0169-5002/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.lungcan.2004.01.019

138 W.L. Read et al.
equal proportion–—this contrasts with the historicpredilection of NSCLC for men [2]. Several serieshave also reported that BAC patients are youngeron average than patients with other types of NSCLC[3]. This may reflect a gender difference; Liu etal found that women with BAC were significantlyyounger thanmen (63.9 years versus 69.6 years) [4].These differences may be the reason that patientswith BAC are reported to have longer survival timesthan patients with other types of NSCLC [4,5]. BACwas a very uncommon disease in the early part ofthe 20th century [6]. However, several recent seriessuggest an increase in the occurence of BAC overthe past 40 years. A series of 505 cases from theVeterans Administrations hospital found a steadyrise in the percentage of lung cancers representedby BAC, from 9.1% in 1978 to 20.3% in 1986—1989[7]. Another series of 1527 reported from UCLAfound BAC to have risen from less than 5% of allNSCLC in 1955 to 24% in 1990 [8]. The reason for thisreported rise in incidence is not known. The Surveil-lance, Epidemiology and End Results (SEER) pro-gram administered by the National Cancer Institutemaintains a cancer incidence and survival databasewhich in 1998 had a catchment area representingapproximately 14% of the population of the US. Weanalyzed the SEER database to determine changesin the incidence and epidemiology of BAC in thislarge population, and to determine if the incidenceof BAC continued to increase during the 1990s.
2. Methods
We used the SEER Cancer Incidence Public UseDatabase 1973—1998 (issued April 2001). The catch-ment area of this database has expanded severaltimes between 1978—1998 (http://seer.cancer.gov).Lung tumors (site codes C33 and C34) wereextracted from the database from the years1979—1998. Tumors were classified with histologycodes as follows:
• 8041—45: small cell carcinoma.• 8012, 8013, 8022, 8030, and 8031: large cell car-cinoma.
• 8050—52, 8070—76: squamous cell carcinoma.• 8140—8239, 8260—8550: non-BAC adenocarci-noma.
• 8250—54: bronchioloalveolar carcinoma (BAC).
Lung tumors with other nonspecific types (butnot metastatic disease) were included in the‘‘undifferentiated’’ group. The great majority ofthese were coded as 8010 (carcinoma NOS) or8000 (neoplasm NOS). We used the SAS system for
Windows version 8.02 to analyze the data for thefollowing:
• Incidence of each histologic subtype as a percent-age of all reported lung cancer.
• Mean age at diagnosis of patients with each histo-logic subtype of lung cancer. To statistically com-pare differences in each group’s mean age withthat of BAC, t-tests were used.
• Sex ratio of patients with each histologic sub-type of lung cancer, SEER stage distribution (lo-cal, regional, distant) for each histologic subtypeof NSCLC, and percentage of patients surviving 1year by histologic subtype and stage. To statisti-cally compare differences in these rates and pro-portions, chi-square analysis was performed.
Two-tailed tests of significance were used with analpha level of P < 0.05 selected for significance.Because overall survival for a histologic subtype
is affected by the different proportions of advancedstage tumors within each subtype, overall survivalwas adjusted for stage using the direct standardiza-tion method in the following manner. For each can-cer subtype, the stage distribution of NSCLC lungcancer overall was multiplied by the total numberof patients to derive the stage-adjusted numberof patients. The adjusted number of patients ineach stage for each cancer subtype was multipliedby the stage-specific survival rate for that cancersubtype. For each cancer subtype, the adjustednumber of survivors for each stage was added to-gether and divided by the total number of patientsto derive the direct standardized adjustment ofsurvival.
3. Results
The entire lung cancer cohort consisted of 310,280patients, including 48,389 small cell and 261,891NSCLC. The mean age, in years (standard devia-tion), for all patients was 67.1 (10.9); 37.8% of pa-tients were female; and the overall 1 year survivalrate was 36.6%. The mean age, gender ratio and1 year survival rates for each histologic subtypeare shown in the Table. In addition, the differencebetween each histologic subtype and BAC in age,gender, and survival is shown. As can be seen inTable 1, BAC patients were significantly different inage than patients with other cancer types, althoughthe differences were small and not consistently inone direction (i.e., younger). The majority (53.7%)of BAC patients were female, which contrasts withthe male predominance of other histologic sub-types. One year survival rate for BAC patients was

Analysis of the SEER database 139
Table1
Differencein
meanage,
distribu
tion
ofsex,
and1year
survival
betw
eenBA
Candothe
rhistological
subtypes
ofNSC
LC
Histologicsubtype,
all
cases(1979—
1998)
Meanage,
(years)
Differencefrom
BAC(years,95%CI)
Female
cases(%)
Differencein
sex
from
BAC(%,95%CI)
One
year
survival
rate
(%,95%CI)
Differencein
survival
from
BAC(%,95%CI)
BAC(n
=8777)
67.1
N/A
53.8
N/A
64.9
N/A
Non
-BAC
aden
ocarcino
ma
(n=86,583)
65.4
−1.7
(−1.5to
−1.9)
44.0
−9.8
(−8.7to
−10.9)
39.8
−25.1(−
24.1
to−2
6.2)
Squamou
scell(n
=76,217)
67.8
0.7(0.5
to0.9)
27.4
−26.4(−
25.3
to−2
7.5)
41.4
−23.5(−
22.4
to−2
4.6)
Largecell(n
=24,156)
65.4
−1.7
(−1.4to
−2.0)
36.8
−17.0(−
15.8
to−1
8.2)
32.0
−32.9(−
31.7
to−3
4.1)
Smallcell(n
=48,389)
66.2
−0.9
(−0.7to
−1.1)
42.8
−11.0(−
9.9to
−12.13)
31.6
−33.3(−
32.2
to−3
4.4)
Und
ifferentiated(n
=66,158)
69.6
2.5(2.2
to2.8)
40.1
−13.7(−
12.6
to−1
4.8)
28.4
−36.5(−
35.4
to−3
7.6) 64.9% and this was both clinically and statisti-
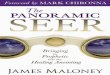
cally significantly better than survival for all othersubtypes.Fig. 1 depicts the incidence of lung cancer, by
histologic subtype, between 1979 and 1998. Thepercentage of lung cancer represented by BAC was3.0% in 1979, 2.1% in 1989, and 3.4% in 1994. Theincidence of non-BAC adenocarcinoma steadily in-creased from 23.0% in 1979 to 31.9% in 1998 atrend which has been previously reported [9]. Theincreases in BAC and non-BAC adenocarcinomaare matched by a large decrease in squamous celland smaller decreases in both small and largecell carcinoma. Fig. 2 shows the SEER stage atpresentation for the different histologic types oflung cancer. BAC is much more likely to presentwith localized disease than the other subtypesof lung cancer. Conversely, BAC presents less of-ten with distant disease than do other histologicsubtypes.Fig. 3 shows the 1 year survival rate, by
SEER summary stage, for each subtype. As ex-pected, for each histologic subtype, survival isbest for localized tumors, worse for regional,and worst for distant spread of disease. Addi-tionally, Fig. 3 shows that within each SEER sum-mary stage BAC patients had the best survivalrate.Fig. 4 shows the unadjusted and stage-adjusted
1 year survival rates for each histologic subtype.After adjusting for stage, the 1 year survival ratefor BAC decreases from 65 to 54% yet remainsgreater than all other subtypes. The unadjustedrates are the same as in Table 1 and are presentedhere to facilitate comparison with the adjustedrates.
4. Discussion
Our analysis suggests that there has not beena significant increase in the incidence of BACamong tumors reported to SEER during the period1979—1998. BAC comprised less than 4% of all re-ported lung cancers during the past two decades.The SEER results are very different from the re-sults reported by the two series cited above,which found a marked increase in the incidenceof BAC. In both of these reports, the authors cen-trally reviewed the histology of tumors in theirseries. Both series also have fewer tumors in the‘‘undifferentiated’’ or ‘‘NOS’’ categories thanthe SEER database–—probably a result of morecareful pathologic review. No central review wasdone for the cases reported here from the SEERdatabase. In the series from UCLA, Barsky et al

140 W.L. Read et al.
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
19791981
19831985
19871989
19911993
19951997
BAC
Non-BAC Adeno
Squamous
Large Cell
Small Cell
Undifferentiated
Fig. 1 SEER lung cancer incidence by histologic subtype 1979—1998.
Fig. 2 Frequency of each SEER stage by histologic subtype.
used liberal criteria for the diagnosis for BAC,stating ‘‘the presence of solid areas of moder-ately to poorly differentiated adenocarcinoma alsodid not exclude the tumor from the BAC cate-gory if areas of classic BAC were also present.’’The definition of BAC is ‘‘an adenocarcinomawith a pure bronchioloalveolar growth patternand no evidence of stromal, vascular or pleuralinvasion’’ [10]. Most pathologists do categorizea tumor according to the most aggressive com-ponent, since this component will determine theclinical course [11]. Barsky et al report that in theperiod 1986—1990, adenocarcinoma overall rep-
Fig. 3 One Year survival rate by SEER stage and histo-logic subtype.

Analysis of the SEER database 141
Fig. 4 Unadjusted and stage-adjusted 1 Year survival rate by histologic subtype.
resented 46.5% of all lung cancers, and that 52%of these adenocarcinoma were BAC. In the SEERdatabase, the overall frequency of adenocarcinomafor this time period is 29.6%, 7.6% of which wereBAC.As mentioned above, the series by Auerbach
and Garfinkel found a much higher incidence ofBAC in their series–—for example, in the period1986—1989 Auerbach et al found 20.3% of lungcancers were BAC, as opposed to only 2.2% fromthe SEER over the same period. The Auerbach andGarfinkel series differs from the SEER in that theSEER contains diagnoses made based on biopsyspecimens of living patients while the VA seriesis of autopsy cases. Auerbach and Garfinkel notethat BAC may be an incidental finding on au-topsy, but do not report how many of their caseswere known to have lung cancer before death.Autopsy studies might reveal a substantial num-ber of these small tumors in patients who died ofreasons other than lung cancer. If the high fre-quency of BAC in this autopsy series reflects thetrue prevalence of these tumors, this does notseem to have translated to a comparably highnumber of clinical cases reported to SEER. Thismay change in the next few years: the increas-ing popularity and publicity of screening helicalCT scans may result in the discovery of manysmall BAC, which would never otherwise havebeen brought to medical attention. In conclu-sion, our analysis of the SEER data did not findthat bronchioloalveolar carcinoma had becomemore common in recent years. Rather, this tumorrepresents a relatively stable, small subset of re-ported lung cancers. Changes in the incidence ofBAC did not mirror those of non-BAC adenocarci-
noma, as one would expect if BAC was simply ahistologic variant. Our analysis of the SEER dataconfirmed the reported comparatively good prog-nosis for BAC. This is due in part to the tendencyof BAC to present with localized disease, but thisdoes not entirely explain the better survival ofBAC patients. The differences in epidemiology andnatural history suggest that BAC is distinct fromother NSCLC, and may warrant study as a separateentity.
References
[1] Malassez L. Examen histologique d’un cas de can-cer encephaloide du poumon (epithelioma). Archivesde Physiologie Normale Pathologique 1876;3:353—72.
[2] Liebow A. Bronchiolo-alveolar carcinoma. Adv Int Med1960;10:329—58.
[3] Barkley JE, Green MR. Bronchioloalveolar carcinoma. J ClinOncol 1996;14(8):2377—86.
[4] Liu YY, Chen YM, Huang MH, Perng RP. Prognosis and re-current patterns in bronchioloalveolar carcinoma. Chest2000;118(4):940—7.
[5] Breathnach OS, Ishibe N, Williams J, Linnoila RI, CaporasoN, Johnson BE. Clinical features of patients with stage IIIBand IV bronchioloalveolar carcinoma of the lung. Cancer1999;86(7):1165—73.
[6] Adler I. Primary and malignant growths of the lungsand bronchi. New York: Longmans, Green and Co.,1912.
[7] Auerbach O, Garfinkel L. The changing pattern of lungcarcinoma. Cancer 1991;68(9):1973—7.
[8] Barsky SH, Cameron R, Osann KE, Tomita D, HolmesEC. Rising incidence of bronchioloalveolar lung carci-noma and its unique clinicopathologic features. Cancer1994;73(4):1163—70.
[9] Charloux A, Quoix E, Wolkove N, Small D, Pauli G, Kreis-man H. The increasing incidence of lung adenocarcinoma:

142 W.L. Read et al.
reality or artefact? a review of the epidemiology oflung adenocarcinoma. Int J Epidemiol 1997;26(1):14—23.
[10] Travis WD, Sobin LH. Histological typing of lung and pleuraltumors. Berlin, New York: Springer, 1999.
[11] Feldman ER, Eagan RT, Schaid DJ. Metastatic bronchi-oloalveolar carcinoma and metastatic adenocarcinomaof the lung: comparison of clinical manifestations,chemotherapeutic responses, and prognosis. Mayo Clin Proc1992;67(1):27—32.