Embed Size (px)
Citation preview
INTRODUCTIONYou will do it 5,000 times in your career.
Give or take a few…The ADA estimates that most dentists
treat an average of 2 endodontic teeth perweek. If we assume there are at least 2 canalsper tooth, 47 treatment weeks per year for25 years, then most dentists will attemptapproximately 5,000 Glidepaths in theircareer: 2 root canals per week x 2 canals pertooth x 47 weeks x 25 years = approximately5,000 Glidepath attempts.
The amazing fact is that the subject ofGlidepath has no formal training in theendodontic curricula of most dentalschools. In fact, a PubMed Central search ofGlidepath and endodontics reveals 300 ref-erences. However, none of them actuallydescribe how to prepare a Glidepath. Most ofthe references say something like, “Ofcourse you must first make a Glidepath.”That’s all. And so the purpose of this article
is to serve as a reference guide for endodon-tic Glidepath preparation and answer thefollowing questions: What is it? Why is itimportant? How do you predictably preparethe Glidepath?
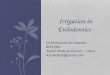
STARTING WITH THE ANSWERThe purpose of endodontics is to preventor heal lesions of endodontic origin.1 Inorder to achieve this purpose, the rootcanal system must be successfully obturat-ed. In order to be obturated, the root canalsystem has to be successfully 3-dimension-ally (3-D) cleaned and rotary shaped. Inorder to be 3-D cleaned and rotary shaped,a Glidepath has to be successfully pre-pared (Figure 1). And so the Glidepath isthe answer. It is the starting point of radic-ular preparations. Without it, cleaningand shaping become unpredictable orimpossible because there is no guide forendodontic mechanics.
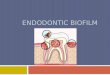
WHAT IS A GLIDEPATH?The endodontic Glidepath is a smooth radic-ular tunnel from canal orifice to physiologicterminus (foraminal constriction). Its mini-mal size should be a “super loose No. 10”endondontic file. The Glidepath must be dis-covered if already present in the endodonticanatomy or prepared if it is not present. TheGlidepath can be short or long, narrow orwide, essentially straight or curved (Figure 2).
WHY IS THE ENDODONTIC GLIDEPATHIMPORTANT?
First, without the endodontic Glidepath, therationale of endodontics cannot be achieved.The rationale states that “any endodonticallydiseased tooth can be predictably saved if theroot canal system can be nonsurgically orsurgically sealed, the tooth is periodontallysound or can be made so, and the tooth isrestorable.”1 A nonsurgical seal requires firstthe creation of a radicular path that can be
cleaned of viable andnonviable bacteria, vitaland nonvital pulp tissue,biofilm, and smear layer;then shaped to a continu-ously tapering funnel thatcanbe predictably and eas-ily obturated.
Second, the Glidepathis necessary for qualitycontrol. Sustainable excel-lent endodontic obtura-tions are not possiblewithout it.
HOW DOES THEDENTIST
PREDICTABLY PRE-PARE THE GLIDEPATH?In order to answer thisquestion, I first surveyedtheAmericanAssociationof Endodontists (AAE)and reported my findingsat the AAE annual scien-tificmeeting in SanDiegoon April 16, 2010.2 Thetitle of my presentationwas “The Magic of Mas-tering the Glidepath:What Every Endodontist
86
John D. West,DDS, MSD
The Endodontic Glidepath:“Secret to Rotary Safety”
ENDODONTICS
Figure 1. Glidepath is key to Rotary Shaping.Pretreatment image (left) shows apparent apical calci-fication. Post-treatment image (right) reveals properapical shaping and obuturation made possible by suc-cessful Glidepath preparation.
Figure 2. Glidepaths occur in multiple widths, lengths,and curvatures. They can be long or short, wide or nar-row, curved or more curved. Root canal system anato-my is often tortuous and in multiple planes notobserved in 2-dimensional images. Glidepaths mustultimately “follow” and replicate the original canal pathin order to preserve the position of nature’s portal ofexit locations.
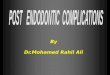
Figure 3. Sample of Glidepath survey letter to endodontists. Answers to Nos.1 through 6 are presented in Figures 4 to 9.
1. What size hand file do you prefer for your Glide Path? (Choose one) A. Size #10________ B. Size #15________ C. Size #20________ D. Larger_________ 2. Do you use straight manual files or do you curve them? (Choose one) A. Straight______ B. Curved_______ 3. Do you “go to length immediately” if you can or do you “do early coronal enlargement”
first? A. Immediately if I can_____ B. Early coronal enlargement______ 4. When making the Glide Path, what is your preferred irrigation solution? (Choose one) A. Sodium hypochlorite_______ B. EDTA_______ C. Viscous chelator such as ProLube, Glide, or RC Prep_______ D. Combination of the above_______ 5. How do you determine your Glide Path length? (Choose one) A. Apex locator_______ B. Radiographic terminus______ C. Both of the above________ 6. When making the Glide Path, what hand motion(s) do you use? i.e.: “watch/wind,” “push/pull,” or other.
7. When blocked, what do you do next?
8. When you first notice a shelf starting, what do you do next?
9. If you were to design the ideal Glide Path file(S), what would you want as your most desired features or characteristics? Please be specific. (Optional)
continued on page 88
DENTISTRYTODAY.COM ¥ SEPTEMBER 2010
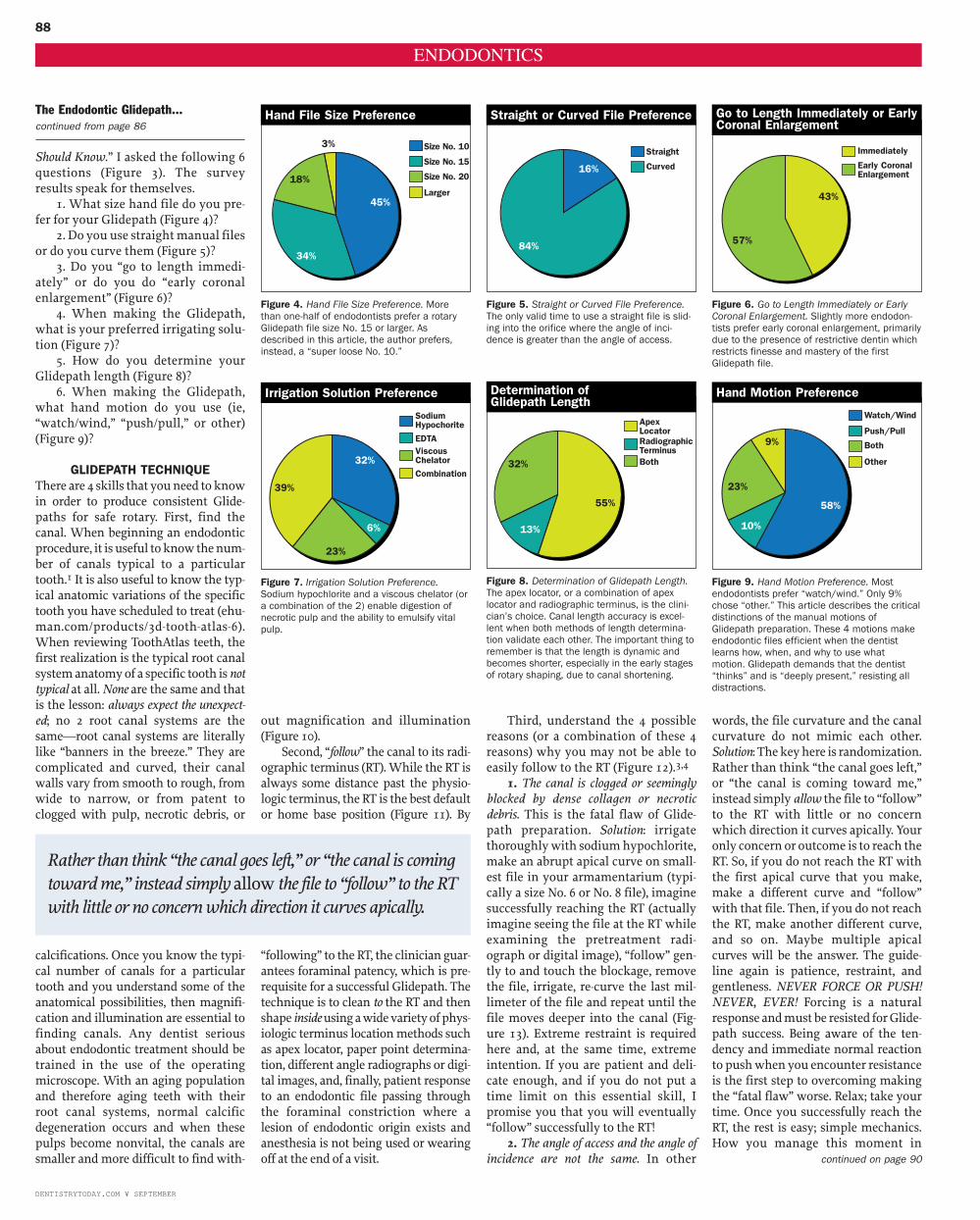
Should Know.” I asked the following 6questions (Figure 3). The surveyresults speak for themselves.
1. What size hand file do you pre-fer for your Glidepath (Figure 4)?
2. Do you use straightmanual filesor do you curve them (Figure 5)?
3. Do you “go to length immedi-ately” or do you do “early coronalenlargement” (Figure 6)?
4. When making the Glidepath,what is your preferred irrigating solu-tion (Figure 7)?
5. How do you determine yourGlidepath length (Figure 8)?
6. When making the Glidepath,what hand motion do you use (ie,“watch/wind,” “push/pull,” or other)(Figure 9)?
GLIDEPATH TECHNIQUEThere are 4 skills that youneed toknowin order to produce consistent Glide-paths for safe rotary. First, find thecanal. When beginning an endodonticprocedure, it is useful toknowthenum-ber of canals typical to a particulartooth.1 It is also useful to know the typ-ical anatomic variations of the specifictooth you have scheduled to treat (ehu-man.com/products/3d-tooth-atlas-6).When reviewing ToothAtlas teeth, thefirst realization is the typical root canalsystemanatomyof a specific tooth isnottypical at all. None are the same and thatis the lesson: always expect the unexpect-ed; no 2 root canal systems are thesame—root canal systems are literallylike “banners in the breeze.” They arecomplicated and curved, their canalwalls vary from smooth to rough, fromwide to narrow, or from patent toclogged with pulp, necrotic debris, or
calcifications. Once you know the typi-cal number of canals for a particulartooth and you understand some of theanatomical possibilities, then magnifi-cation and illumination are essential tofinding canals. Any dentist seriousabout endodontic treatment should betrained in the use of the operatingmicroscope. With an aging populationand therefore aging teeth with theirroot canal systems, normal calcificdegeneration occurs and when thesepulps become nonvital, the canals aresmaller and more difficult to find with-
out magnification and illumination(Figure 10).
Second, “follow” the canal to its radi-ographic terminus (RT). While the RT isalways some distance past the physio-logic terminus, theRT is the best defaultor home base position (Figure 11). By
“following” to theRT, the clinician guar-antees foraminal patency, which is pre-requisite for a successful Glidepath. Thetechnique is to clean to the RT and thenshape insideusingawidevarietyofphys-iologic terminus location methods suchas apex locator, paper point determina-tion, different angle radiographs or digi-tal images, and, finally, patient responseto an endodontic file passing throughthe foraminal constriction where alesion of endodontic origin exists andanesthesia is not being used or wearingoff at the end of a visit.
Third, understand the 4 possiblereasons (or a combination of these 4reasons) why you may not be able toeasily follow to the RT (Figure 12).3,4
1. The canal is clogged or seeminglyblocked by dense collagen or necroticdebris. This is the fatal flaw of Glide-path preparation. Solution: irrigatethoroughlywith sodiumhypochlorite,make an abrupt apical curve on small-est file in your armamentarium (typi-cally a size No. 6 or No. 8 file), imaginesuccessfully reaching the RT (actuallyimagine seeing the file at the RT whileexamining the pretreatment radi-ograph or digital image), “follow” gen-tly to and touch the blockage, removethe file, irrigate, re-curve the last mil-limeter of the file and repeat until thefile moves deeper into the canal (Fig-ure 13). Extreme restraint is requiredhere and, at the same time, extremeintention. If you are patient and deli-cate enough, and if you do not put atime limit on this essential skill, Ipromise you that you will eventually“follow” successfully to the RT!
2. The angle of access and the angle ofincidence are not the same. In other
words, the file curvature and the canalcurvature do not mimic each other.Solution: Thekeyhere is randomization.Rather than think “the canal goes left,”or “the canal is coming toward me,”instead simply allow the file to “follow”to the RT with little or no concernwhich direction it curves apically. Youronly concern or outcome is to reach theRT. So, if you do not reach the RT withthe first apical curve that you make,make a different curve and “follow”with that file. Then, if you do not reachthe RT, make another different curve,and so on. Maybe multiple apicalcurves will be the answer. The guide-line again is patience, restraint, andgentleness. NEVER FORCE OR PUSH!NEVER, EVER! Forcing is a naturalresponse andmustbe resisted forGlide-path success. Being aware of the ten-dency and immediate normal reactionto pushwhenyou encounter resistanceis the first step to overcoming makingthe “fatal flaw” worse. Relax; take yourtime. Once you successfully reach theRT, the rest is easy; simple mechanics.How you manage this moment in
88
DENTISTRYTODAY.COM ¥ SEPTEMBER
ENDODONTICS
continued on page 90
Figure 4. Hand File Size Preference. Morethan one-half of endodontists prefer a rotaryGlidepath file size No. 15 or larger. Asdescribed in this article, the author prefers,instead, a “super loose No. 10.”
Size No. 10
Size No. 15
Size No. 20
Larger
Hand File Size Preference
Figure 5. Straight or Curved File Preference.The only valid time to use a straight file is slid-ing into the orifice where the angle of inci-dence is greater than the angle of access.
Straight
Curved
Straight or Curved File Preference
Figure 6. Go to Length Immediately or EarlyCoronal Enlargement. Slightly more endodon-tists prefer early coronal enlargement, primarilydue to the presence of restrictive dentin whichrestricts finesse and mastery of the firstGlidepath file.
Immediately
Early CoronalEnlargement
Go to Length Immediately or EarlyCoronal Enlargement
Figure 7. Irrigation Solution Preference.Sodium hypochlorite and a viscous chelator (ora combination of the 2) enable digestion ofnecrotic pulp and the ability to emulsify vitalpulp.
SodiumHypochorite
EDTAViscousChelatorCombination
Irrigation Solution Preference
Figure 9. Hand Motion Preference. Mostendodontists prefer “watch/wind.” Only 9%chose “other.” This article describes the criticaldistinctions of the manual motions ofGlidepath preparation. These 4 motions makeendodontic files efficient when the dentistlearns how, when, and why to use whatmotion. Glidepath demands that the dentist“thinks” and is “deeply present,” resisting alldistractions.
Watch/Wind
Push/Pull
Both
Other
58%
10%
23%
57%
18%
3%
43%
9%
Hand Motion Preference
Figure 8. Determination of Glidepath Length.The apex locator, or a combination of apexlocator and radiographic terminus, is the clini-cian’s choice. Canal length accuracy is excel-lent when both methods of length determina-tion validate each other. The important thing toremember is that the length is dynamic andbecomes shorter, especially in the early stagesof rotary shaping, due to canal shortening.
ApexLocatorRadiographicTerminusBoth
Determination ofGlidepath Length
32%
6%
32%
55%39%
23%
13%
84%
16%
45%
34%
Rather than think “the canal goes left,” or “the canal is comingtoward me,” instead simply allow the file to “follow” to the RTwith little or no concern which direction it curves apically.
The Endodontic Glidepath...continued from page 86

90
Glidepath preparation is the differencethat makes the difference.
3. The diameter of the file is too widefor the canal that it is following. In otherwords, the file does not fit. Solution:Easy. Choose a smaller file. At no timedo you know what solution will be theanswer. You use all the solutions 1, 2,and 3 all at once. Be delicate. Changethe curve. Go to a smaller file. You donot care what the solution is; you onlycare that you reach the RT.
4. The shaft of the file is too wide for thecanal. In other words, the file cannot“follow” deeper into the canal becauserestrictive coronal dentin will notallow it. Remember, pulps not onlyinflame and necrose coronal-apically,they also calcify coronal-apically.
Solution: Sometimes changing to asmaller file with a narrower coronaldiameter will allow the file to “follow”deeper. A second method to removerestrictive dentin is to mechanically
remove the restrictive dentin usingGates Glidden drills or nickel titaniumrotary files short of the depth followedby the manual file. Historically, thisapproach has been referred to as early
coronal enlargement. Progresssivelytapered files (such as ProTaper Uni-versal [DENTSLPY Tulsa Specialties]),used in a brushingmotion, are particu-larly effective and efficient for restric-tive dentin removal through the tech-nique.5 A third method for restrictivedentin removal is the “envelope ofmo-tion” manual motion which is de-scribed below.
Seemingly, while all 4 Glidepath“following” skills are separate, theyare not. Often combinations of the 4conditions exist, requiring a combina-tion of solutions. For example, a canalmight be packed apically with necrot-ic debris, have restrictive dentin, andyou may choose a file that is too wide.Without being delicate, removingrestrictive dentin and choosing a nar-rower file all at the same time is arecipe for failure to follow to the RT,which is the critically essential step ofa successful Glidepath.
The fourth skill for consistentGlidepath preparation is to understandand master the 4 manual motions toprepare the rotary Glidepath.
1. “Follow.” Identify the entrance tothe canal and remove any dentin orenamel triangles that are preventingstraight-line access. Irrigate thorough-ly with sodium hypochlorite beforegently “slipping and sliding” down the
ENDODONTICS
The Endodontic Glidepath...continued from page 88
Figure 10. Severely calcified canal (left) can be successfully “followed” using microscope andcolor differentiations. Note canal patency (right) did not occur until a few millimeters from thecanal terminus and yet the procedure was entirely safe and minimal tooth structure was removed.
Figure 11. Physiologic Terminus may actuallyhave different lengths. The walls of the canalon the left are the same, while the walls of thecanal on the right have a longer one and ashorter one. Canal length determination is notan exact science; it is an art form. What therationale of endodontics requires is the entirelength of the root canal system be cleaned andshaped. Glidepath is perquisite to this mechan-ical objective.
Figure 12. Four reasons a file will not “follow”to its terminus: (1) Canal is blocked (2) Filecurvature does not replicate canal curvature(3) Diameter of file is too wide at its tip (4)Diameter of file is too wide in its shaft. (Often,a combination of reasons one to 4, or all 4 arethe situation.)

canal (Figure 14). If a plug ofdentin covers the orifices thathave been identified usingultasonics, high-speed burs,or Mueller burs, first agitatechamber sodium hypo-chlorite using EndoActivator(DENTSPLY TulsaSpecialties). Then dense ori-fice dentin will be removed orsoftened, and small files canpenetrate easily and the “fol-lowing” motion can begin.Take the smallest file that fitsthe canal easily, and slightlyprecurve the apical a few mil-limeters using metal cottonpliers. If you are using a mi-croscope, hold the handle offile with cotton pliers so yourfingers do not block the lineof sight to the orifice. Oncethe file can stand upright inthe canal on its own, “follow”the file down the canal. Allowit to go whatever direction itwants. Be intentional aboutreaching the RT but stop
attempting to “follow” shortof maximum resistance andimplement the No. 3 motioncalled “Envelope” (describedbelow). When following tothe RT, use watchwords suchas gentle, caress, slip and slide,stroke, trail, and restraint. IfRT is reached easily with thefirst “follow,” identified withapex locator and validatedwith radiographic or digitalimage, then proceed withmanual motion No. 2:“Smooth.”
2. “Smooth.” Once RT fileposition has been validated,make short amplitude verticalstokes until the file is loose.This may mean a half a dozenstrokes or it may mean 100strokes. Whatever it takes, doit. If the file is at first too tightto easily make short strokes,ie, the file is apparently bind-ing against 2 or more walls,then wiggle the handle leftand right without any up or
Four manualmotions have beendistinguished that,if used properly,will produce a saferotary result....

92
down motion. This simple, safe nuancewill wear away the small amount ofrestrictive dentin and free the file forthe smoothing motion. The minimalGlidepath file size for safe rotary shap-ing is a loose No. 10 file. While manyendodontists prefer a larger file (55%, asnoted in my spring AAE 2010 survey),every increase in size while making a
theoreticallybiggerpilothole for rotary,also risks creating a shelf in the radicu-lar dentin wall. Rotary files rarelyglance over shelves or ledges and mustbe meticulously removed before pro-ceeding.4 An excellent series of manualfiles for smooth and progressiveGlidepath enlargement are the ProFileSeries 29 invented by Schilder
(DENTSPLY Tulsa Specialties) (Figure15).
3. “Envelope.” If the file does noteasily “follow” to the RT, stop short ofmaximum resistance. You now have 2choices: force or remove. If you force,you may block or ledge. So, DO NOTFORCE or PUSH. The proper next stepis to remove the file using the “enve-
lope of motion.” The envelope willwear away restrictive dentin by with-drawing and carving to the right, orclockwise, direction. Envelope is theonly motion of the 4 manual motionsthat removes dentin on the outstroke.The other 3 motions require that thefile is moving in an apical motion inorder to execute. This is a subtlemotionand gives the impression that you arewasting your time because nothing ishappening. But remember, endodon-tics is not a big job, it is a little job. Theamount of tooth structure that isremoved compared to coronal enameland dentin preparations is minuscule.Endodontics is, however, a smart job.The “envelope motion” is a smart andefficient motion. Test it out yourselfand experience that suddenly, effort-lessly, and evenmiraculously the previ-ous file “follows” deeper. You will expe-rience anewfound freedomandcontrolof the evolving radicular shape which,unfortunately, cannot be observeddirectly like all other restorative. Yourunimpeded files are your eyes in endo-dontics. Now “follow” to the RT withyour smallest file, smooth, and finishGlidepath. If you cannot “follow” to RT,youwill almost always at least “follow”closer toward the RT. Envelope againand repeat until you reach RT, smooth,and finish the Glidepath.
4. “Balance.” Sometimes a file sizelarger than a super loose No. 10 isdesired. The dentist may feel safer witha larger size or the walls may not feel assmooth as possible. If you want to havea smooth No. 15 as your Glidepath size,for example, then use balance motion.It is safe andpredictable.Originally thismotion was referred to as BalancedForce or the Roane Technique, namedafter Dr. James Roane, the first personto describe this manual motion.6Simply put, turn the handle of the fileclockwise, and then turn it counter-clockwise using slight apical pressureso that the file will not “unscrew” itsway out of the canal. During the clock-wisemotion, the file blades cut into thedentin; during the apical counterclock-wise motion, the dentin is collectedinto the file’s flutes. This can be repeat-
ENDODONTICS
Figure 13. “Follow” files are more effective when curved. First squeeze cotton pliers against fileshaft at right angles and sweep the cotton pliers toward the tip (left). The resulting file (right) hasa gentle and continuous curve to and through its tip.
Figure 14. Glidepath “following” requires optimum tactile sense. Loose gloves do not enable thedentist to feel the file handle (left). Gloves must fit tight so that the balls of the fingers togetherallow the finest possible touch and delicacy (right).

93
ed several times as the file is “balanced”apically. The file is then turned clock-wise and removed having carved awider Glidepath. That same file is thenused in a “smoothing” motion and theGlidepath is once again finished andready for rotary shaping.
A new approach to increasingGlidepath size is mechanically vs.manually. One recent and successfulmethod is the introduction of 3PathFiles (DENTSPLY Tulsa Special-ties) (Figure 16). When properly used,these robust and efficient rotaryGlidepath files can take even furtherrisk out of rotary shaping. As withevery dental instrument, the dentistmust precisely follow the manufac-turer’s directions for use.
SUMMARYThe endodontic Glidepath is the secretto radicular rotary safety. This articlehas offered a definition of Glidepath,explained why it is important in pro-ducing optimum endodontic mechan-ics, and described how to prepare aGlidepath for radicular shaping. Fourobstacles to Glidepath preparationhave been identified along with thesolution for each one. Four manualmotions have been distinguished that,if used properly, will produce a saferotary result and an endodontic experi-ence that you truly control.�
References1. West JD. Endodontic predictability—“Restore or
remove: how do I choose?” In: Cohen M, ed.Interdisciplinary Treatment Planning: Principles,Design, Implementation. Chicago, IL: Quintes-sence Publishing Co; 2008:123-164.
2. West J. The Magic of Mastering the Glidepath:What Every Endodontist Should Know. Paperpresented at: American Association of Endo-dontists Annual Session; April 16, 2010; SanDiego, CA.
3. West J. Endodontic update 2006. J EsthetRestor Dent. 2006;18:280-300.
4. West JD. Perforations, blocks, ledges, and trans-portations: overcoming barriers to endodonticfinishing. Dent Today. 2005;24:68-73.
5. West J. Endodontic brushing: the secret to mas-tering rotary safety. Dental Economics. August2010. In Press.
6. West J, Roane J. Cleaning and shaping of theroot canal system. In: Cohen S, Burns RC.
Pathways of the Pulp. 7th ed. St. Louis, MO:Mosby Year-Book; 1998:203-257.
Dr.West is the founder and director of the Centerfor Endodontics. He received his DDS from theUniversity ofWashington in 1971 and his MSD in
endodontics at the Boston University Henry M.Goldman School of Dental Medicine in 1975. Hehas presented more than 400 days of CE inter-nationally while maintaining a private practice inTacoma, Wash. He co-authored “Obturation ofthe Radicular Space”with Dr. John Ingle in Ingle’s1994 and 2002 editions of Endodontics and wassenior author of “Cleaning and Shaping the Root
Canal System” in Cohen and Burns’ 1994 and1998 Pathways of the Pulp. He recently authored“Endodontic Predictability” in Dr.Michael Cohen’s2008 Quintessence text Interdisciplinary Treat-ment Planning: Principles, Design, Implementa-tion. He is a thought leader for Kodak Digital Den-tal Systems and serves on the editorial advisoryboards for The Journal of Advanced Estheticsand Interdisciplinary Dentistry, The Journal of Es-thetic and Restorative Dentistry, Practical Proce-dures and Aesthetic Dentistry, and The Journalof Microscope Enhanced Dentistry. He can bereached at (800) 900-7668 or at [email protected].
ENDODONTICS
Watch for 2 more articles on thetopic of Glidepath by Dr. West infuture issues of Dentistry Today:
"Manual Versus MechanicalGlidepath: When and
How Do You Do What?”and “Implementing theEndodontic Glidepath:
What Are Your Action Steps?”
Figure 16. New PathFile rotary Glidepath files (DENTSPLY Tulsa Specialties). These robust files,when used properly, can prepare a Glidepath that is safe and precise. While a manual Glidepath isstill recommended, the PathFile is an excellent way to increase rotary shaping safety.
Figure 15. ProFile Series 29 files (DENTSPLYTulsa Specialties). These files offer the finestmanual transition between Glidepath filesbecause of their constant and appropriate sizeincreases.
PathFiles for Mechanical GlidePath