Embed Size (px)
Citation preview

ARTICLE IN PRESS
Journal of Biomechanics 41 (2008) 3297–3302
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jbiomech
Journal of Biomechanics
0021-92
doi:10.1
� Corr
E-m
www.JBiomech.com
2007 American Society of Biomechanics Young Scientist Pre-Doctoral Award
The effects of the extraocular muscles on eye impact force–deflection andglobe rupture response
Eric Kennedy a,�, Stefan Duma b
a Biomedical Engineering, Bucknell University, Lewisburg, PA 17837, USAb Virginia Tech–Wake Forest University Center for Injury Biomechanics, Blacksburg, VA, USA
a r t i c l e i n f o
Article history:
Accepted 15 July 2008There are over 1.9 million eye injuries per year in the United States, with blunt impacts the cause of
approximately one-half of all civilian eye injuries. No previous experimental studies have investigated
Keywords:
Eye
Extraocular muscles
Eye biomechanics
Eye injury
90/$ - see front matter & 2008 Elsevier Ltd. A
016/j.jbiomech.2008.07.037
esponding author. Tel.: +1570 5771405; fax:
ail address: [email protected] (E. Ke
a b s t r a c t
the effects of the extraocular muscles on the impact response of the eye. A spring-powered blunt
impactor was used to determine the effects that the extraocular muscles have on the force–deflection
and injury response of the eye to blunt trauma. A total of 10 dynamic impact tests were performed at
8.270.1 m/s on five human cadaver heads. With the extraocular muscles left intact, the average peak
force was found to be 271751 N at 7.570.9 mm posterior translation; with the muscles transected, the
average peak force was 268726 N at 7.671.3 mm of posterior translation. From the data available from
this study, the peak impact force and overall amount of translation during the impact are not affected by
the extraocular muscles. Additionally, from the data presented in this study, the eyes with the
extraocular muscles left intact do not rupture with a different injury pattern or display an increased risk
for rupture than the eyes with the extraocular muscles transected. Therefore, it is believed that the
effect of the extraocular muscles is not sufficient to drastically alter the response of the eye under
dynamic impact. This information is useful to characterize the boundary conditions that dictate the eye
response from blunt impact and can be used to define the biofidelity requirements for the impact
response of synthetic eyes.
& 2008 Elsevier Ltd. All rights reserved.
1. Introduction
There are over 1.9 million eye injuries per year in the UnitedStates (McGwin et al., 2005). Some of the most severe eye injuriescan occur in automobile accidents, from sports related impacts, inthe workplace and even at home (Chisholm, 1969; Berger, 1978;Mader et al., 1993; Duma et al., 1996, 2002; Vinger et al., 1997;Kuhn et al., 2000; Rodriguez and Lavina, 2003). Blunt impacts arethe largest single cause of eye injuries at approximately one-halfof all civilian eye injuries (McGwin et al., 2005).
Additionally, the rate of eye injuries has dramatically increasedin warfare from affecting approximately 2% of all casualties duringWorld War I and World War II, to affecting nearly 13% of allcasualties during Operation Desert Storm (Heier et al., 1993;Wong et al., 2000). In order to assess the capability of protectiveequipment in reducing eye and facial injuries, a new advancedheadform is being developed that can predict fracture of facialbones, as well as eye injury from impact loading. Because of itsemphasis on eye and orbital injuries, the name of this new
ll rights reserved.
+1570 577 3659.
nnedy).
advanced headform will be the FOCUS Headform, which stands forFacial and Ocular CountermeasUre Safety Headform. However, inorder to develop a biofidelic eye for the FOCUS headform, it isnecessary to determine the boundary conditions that characterizethe in-situ response of the eye, in particular the effects that theextraocular muscles have on impact response of the eye.
There are a total of six extraocular muscles of the human eye,four rectus muscles, and two oblique muscles, the superior obliqueand the inferior oblique. These extraocular muscles control themovements of the eye. Under typical conditions, these musclesactively control the movements of the eye with less than 0.5 N offorce (Clement, 1987; Simonsz et al., 1986; Miller et al., 2002).
Previous studies have been performed to determine the injurytolerance of the eye to globe rupture from blunt impact(Weidenthal, 1964; Green et al., 1990; Vinger et al., 1999; Basset al., 2002; Stitzel et al., 2002; Kennedy et al., 2006); however,nearly all of the reported tests were conducted using enucleatedeyes mounted in a gelatin solution without the extraocularmuscles intact. No known prior study has investigated the effectsof the extraocular muscles on the impact response of the eye. It ishypothesized that the presence of the extraocular muscles mayalter the response of the eye compared to these enucleated ex-vivo
tests, both in the injury response of the eye (to globe rupture) and

ARTICLE IN PRESS
BallImpactForces
Superior ObliqueTension Force
Inferior ObliqueTension Force
Equatorial Globe Rupture
BallImpactForces
Superior ObliqueTension Force
Inferior ObliqueTension Force
Equatorial Globe Rupture
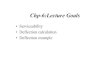
Fig. 1. Under dynamic impact, the oblique extraocular muscles of the eye may
resist posterior translation of the eye, leading to localized stress concentrations
and globe rupture for lower-energy impacts compared to tests conducted on
enucleated eyes. (The four rectus muscles are not shown.)
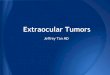
Compression Spring
EmbeddedAccelerometer
Eye w/woIntact Muscles
Mounting Box
Rubber Stop
Guide Track
Eye Impactor
Fig. 2. Test apparatus for dynamic extraocular muscle force–deflection impact
tests.
E. Kennedy, S. Duma / Journal of Biomechanics 41 (2008) 3297–33023298
the overall force–deflection response of the eye. It is hypothesizedthat intact extraocular muscles, in particular the two obliquemuscles, would develop tension to oppose anterior–posteriortranslation of the eye under impact. This tension may lead to astress concentration on the corneo-scleral shell, in turn leadingto globe rupture under lower severity impacts when in-situ,compared to ex-vivo experiments where the extraocular muscleshave been transected (Fig. 1).
The influence of the extraocular muscles is expected tomanifest itself in the force–deflection response of the humaneye to blunt impact, with more force being required to force theeye a given distance into the orbit with the muscles intact versusthe muscles transected. Therefore, the purpose of this study isto perform dynamic impact testing of human eyes in order todetermine the effects that the extraocular muscles have on theforce–deflection and specifically the globe rupture injury responseof the eye to blunt trauma. This is important for the determinationof relevant eye impact tests that can be used for the developmentof eye injury criteria as well as determining biofidelity require-ments for a synthetic human eye.
2. Methodology
A total of 10 tests were performed on five human cadaver heads. All tests were
performed on fresh refrigerated cadavers which were never frozen, tests were
performed after the specimens equalized to room temperature. All test procedures
were reviewed and approved by the Virginia Tech Institutional Review Board.
In order to make a comparison on the effects of the extraocular muscles, in each
head the extraocular muscles were left intact on one eye and transected on the
contra-lateral eye.
The post-mortem human head was mounted in a rigid plastic container using
urethane expandable foam. Prior to impact, the eyes were repressurized via a
needle insertion through the limbus using a column of water to achieve the
physiologic pressure of 15 mmHg (Klein et al., 1992); as a note, none of the injuries
sustained during testing passed through the insertion site. Tests were randomized
such that extraocular muscle transections varied between left and right sides of
the test specimens. Testing order was also randomized between the transected and
intact muscles sides.
The impact tests were performed using a spring-powered Delrin cylindrical
impactor, which was accelerated to a velocity of approximately 8 m/s (4 J) before it
impacted the eye (Fig. 2). The impactor energy level of 4 J was selected to be
approximately twice the energy level of previously reported blunt impact studies
investigating globe rupture which used similarly sized impactors (Weidenthal,
1964; Green et al., 1990). The 19 mm diameter of the blunt impactor corresponds
to a nominal 25 mm average diameter of the eye and was selected to maximize the
anterior translation of the whole eye in order to fully engage the extraocular
muscles. The impactor had approximately 30 mm of free travel prior to impacting
the eye and after contacting the eye, had approximately 25 mm of travel prior to
striking the rubber stops.
An embedded accelerometer (Endevco 7264B-2000, Endevco Corporation, San
Juan Capistrano, CA) was used to collect data at a sampling rate of 100 kHz for the
duration of the test on each eye. Acceleration data was filtered to CFC 1000, then
double integrated to determine impactor tip displacement and also multiplied by
the impactor mass (112.55 g) to determine impactor force, these data were used to
determine the force–deflection characteristics of the in-situ eyes.
For both test conditions—muscles intact and muscles transected—the
characteristic average response was determined using a method similar to that
described by Lessley et al. (2004). This method is a universal technique for
averaging a series of curves by accounting for variability in both the x- and
y- coordinates. In this case, this method essentially determines the average
force–deflection response curve for each test series: muscles intact and muscles
transected. Additionally, force–deflection corridors were calculated using the
characteristic average force–deflection response plus or minus the standard
deviation of the force at each displacement step.
The force–deflection response is the amount of force required to displace the
eye a given distance into the orbit. The force–deflection corridor defines the region
where the typical response may be expected, it is defined as the average response
plus or minus a standard deviation. For consistency, all plots are cut off at the time
of peak force, regardless of whether globe rupture was observed, this is further
elaborated in the discussion. Student’s t-tests were conducted to compare the peak
force and displacement at peak force between intact and transected extraocular
muscle scenarios. The F-statistic was used to compare the variation in peak force
and displacement at peak force between test groups.
Because other common types of eye injuries such as hyphema, lens damage,
and retinal damage are not possible to inspect on post-mortem eyes, the eyes were
evaluated only for globe rupture at the conclusion of each impact test. After the
eye was physically assessed in-situ, the eye was enucleated and the injury outcome
of each of the matched pairs of eyes documented to assess whether or not different
injury patterns were seen between the two test conditions.
3. Results
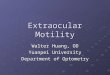
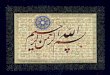
The 10 impact tests were conducted with an overall averageimpact velocity of 8.270.1 m/s on five human cadaver heads(Table 1). With the extraocular muscles left intact, the averagepeak force was found to be 271751 N with 7.570.9 mm posteriortranslation at the time of peak force. With the muscles transectedthe average peak force was 268726 N with 7.671.3 mm ofposterior translation at the time of peak force. The force–deflectionresults, along with the calculated characteristic average responsefor tests conducted with the extraocular muscles intact andtransected are shown in Figs. 3 and 4, respectively. Differencesbetween both the peak force, and displacement at peak force werenot found to be significant between the intact and transectedmuscle scenarios (p ¼ 0.86 and 0.90, respectively).
Combining the standard deviation of force to the characteristicaverage force–deflection, corridors are created for both musclesintact and muscles transected (Figs. 5 and 6). Overall, theforce–deflection corridors for the eyes with extraocular musclesintact and with muscles transected were very similar, with thecorridor being slightly wider for the extraocular muscles intact

ARTICLE IN PRESS
Table 1Individual test results indicating the incidence of globe rupture, impactor velocity, peak force, and displacement at the time of peak force for both muscles intact and
transected tests
Specimen Intact Transected
Aspect Globe
rupture
Impact
velocity
(m/s)
Peak
force (N)
Displacement
at peak force
(mm)
Aspect Globe
rupture
Impact
velocity
(m/s)
Peak
force (N)
Displacement
at peak force
(mm)
1 Right Yes 8.5 321 9.0 Left Yes 8.3 263 6.9
2 Left No 8.2 280 6.7 Right Yes 8.0 293 9.7
3 Left No 8.2 270 6.8 Right No 8.3 248 7.1
4 Right No 8.1 187 7.3 Left No 8.1 239 6.5
5 Left No 8.3 299 7.5 Right No 8.3 297 7.8
Average 8.3 271 7.5 Average 8.2 268 7.6
Standard deviation 0.2 51 0.9 Standard deviation 0.1 26 1.3
0
50
100
150
200
250
300
350
0 1 2 3 4 5 6 7 8 9 10 11 12Displacement (mm)
For
ce (
N)
Individual Test (No Rupture)
Individual Test (Rupture)
Characteristic Average
Fig. 3. Force–deflection responses of the five in-situ eye impact tests with
extraocular muscles left intact, the characteristic average force–deflection
response of these tests is shown in bold. Tests that resulted in globe rupture are
denoted with triangular markers.
200
250
300
350Individual Test (No Rupture)Individual Test (Rupture)Characteristic Average
0
50
100
150
0 1 2 3 4 5 6 7 8 9 10 11 12
Forc
e (N
)
Displacement (mm)
Fig. 4. Force–deflection responses of the five in-situ eye impact tests with
extraocular muscles transected, the characteristic average force–deflection
response of these tests is shown in bold. Tests that resulted in globe rupture are
denoted with triangular markers.
0
50
100
150
200
250
300
350
Displacement (mm)
Forc
e (N
)
Individual Test (No Rupture)
Individual Test (Rupture)
Characteristic Average
Corridor
0 1 2 3 4 5 1211109876
Fig. 5. Force–deflection corridors generated from the five in-situ eye impact tests
with extraocular muscles left intact. Tests that resulted in globe rupture are
denoted with triangular markers.
0
50
100
150
200
250
300
350
0 1 2 3 4 5 6 7 8 9 10 11 12Displacement (mm)
Forc
e (N
)
Individual Test (No Rupture)Individual Test (Rupture)Characteristic AverageCorridor
Fig. 6. Force–deflection corridors generated from the five in-situ eye impact tests
with extraocular muscles transected. Tests that resulted in globe rupture are
denoted with triangular markers.
E. Kennedy, S. Duma / Journal of Biomechanics 41 (2008) 3297–3302 3299
scenario, indicating a larger range of variability for this testscenario.
Of the 10 dynamic impact tests conducted, there were onlythree cases of globe rupture observed. All three injuries weresimilar, and consistent with typically reported cases of globerupture, spanning from the equator of the eye up to the limbus, at
the corneo-scleral interface (Stitzel et al., 2002). Of the threeruptures, two occurred in eyes in which the muscles weretransected, while one occurred in the eye where the muscleswere left intact.
While the peak force and displacement at peak force aresimilar for both test scenarios (Table 1), the variation in peak force

ARTICLE IN PRESS
0
50
100
150
200
250
300
350
Displacement (mm)
Forc
e (N
)
Muscles Intact
Muscles Transected
0 1 2 3 4 5 1211109876
Fig. 7. The characteristic average curves and the force–deflection corridors for
both muscles intact and muscles transected scenarios.
E. Kennedy, S. Duma / Journal of Biomechanics 41 (2008) 3297–33023300
is greater with the extraocular muscles intact (s ¼ 51 N) versusthe extraocular muscles transected (s ¼ 26 N), the difference instandard deviations is not found to be statistically significant(p ¼ 0.11). Similarly, the displacement at peak force for intactversus transected scenarios (s ¼ 0.9 and 1.3, respectively) is notfound to be statistically different (p ¼ 0.26). Overlaying theforce–deflection corridors shows that the extraocular musclestransected scenario lies completely within the corridor for theextraocular muscles transected (Fig. 7).
4. Discussion
The purpose of this study was to determine the effects of theextraocular muscles on the impact response of human eyes. Fromthe data available from this study, the peak impact force andoverall amount of translation during the impact are notsignificantly affected by the extraocular muscles. Additionally,from the limited globe ruptures observed in this study, the eyeswith the extraocular muscles left intact did not rupture with adifferent injury pattern than the eyes with the extraocularmuscles transected. One goal of this study was to observe if thepresence of extraocular muscles would increase the likelihoodof globe rupture due to localized stresses developed at theextraocular muscle insertions. Based on the number of injuriesdocumented in this study (one rupture with intact muscles, tworuptures with transected muscles), this increased risk of injurywas not observed under the testing performed for this study. Fromthe observations made in the current study, both of force–deflec-tion and injury response (globe rupture), it is believed that theeffect of the extraocular muscles is not sufficient to drasticallyalter the response of the eye under dynamic impact. It should alsobe mentioned that given the time course of the measured impactevent, �1 ms, the passive response of the extraocular muscles issufficient for comparison between in-situ and in-vivo scenariosgiven the response time for active muscle contractions.
Based on results observed in previous ex-vivo studies (Stitzelet al., 2002; Kennedy et al., 2006), the displacement of the eyeat rupture is approximately 6–8 mm of posterior translation.Because the eyes used in this study were tested in situ, it wasimpossible to visually determine the exact timing of rupture fromhigh speed video, although evidence of rupture can be observed atapproximately 8–10 mm of impactor displacement. Also, becauseof the presence of extraocular tissue around the eye, there was nota sudden drop in load to indicate when failure may have occurred.It is thought that perhaps, even in the case of rupture, the
surrounding tissues of the orbit and the large diameter impactorwould impede the sudden release of intraocular fluids andeffectively shield the impactor from measuring a sharp drop-offin the impactor force. It should again be noted that only three eyesin this study ruptured, so the vast majority of eyes did not ruptureunder this impact event. For consistency, and because of thecorrelation with rupture displacement in other studies, all plotsand data presented in this study are cut off at the time of peakforce.
Of the three injuries observed during testing, two occurred inthe same test subject, potentially suggesting a weaker overalltolerance to injury in that particular subject. Overall, based on theobservation of data from this study, no appreciable differenceswere noted in injury outcome (globe rupture) between the eyeswith muscles transected versus eyes with muscles left intact.The results indicate that the extraocular muscles do not create anappreciable stress concentration at the muscle insertions to theeye. Therefore, the extraocular muscles do not lead to prematurefailure of the eye at lower overall loading than enucleated eyestested ex vivo, for example, in simulated orbits.
The finding that the extraocular muscles do not influence theinjury outcome or the response of the human eye to blunt impactis also important because of the frequent use of porcine and otheranimal species’ eyes as surrogates for human eye impact testing.These species do not have the same anatomical layout ofextraocular muscles as that of human eyes. If the extraocularmuscles were shown to have a significant effect on determiningeye injury response, then the choice of these eyes as surrogates forhuman eyes would be inappropriate due to these anatomicaldifferences. Based on the results from this study, it is believed thatdifferences in the histology of the corneo-scleral shell are moreimportant than the anatomic differences between extraocularmuscles. For instance, previous studies have shown an increasedtolerance to globe rupture of porcine eyes compared to humaneyes (Kennedy et al., 2004, 2006) due, at least in part, to theoverall increased thickness of the porcine sclera to the humansclera (Olsen et al., 1998, 2002).
Additionally, it should be noted that the actual orbitaldimensions vary from individual to individual. It is currentlyunknown how various geometrical changes within the orbitwould affect the force–deflection response of the eye. While it wasdesirable to quantify the orbital geometry of the test subjects usedin this study, the geometric complexity of the orbit renders itdifficult, if not impossible, to accurately measure without CT orMRI imaging technology. This was not possible for the reportedtest series, and thus comparisons of these effects could not beperformed. Additionally, given the amount of variables involved,this would be more appropriate and would also be an interestingtopic for a computational modeling study, especially given theability to isolate test conditions to specific geometric variables.
One of the primary motivations for this study is the develop-ment of a new advanced headform for the prediction of eyeinjuries from eye impact events, in particular for the military.The relative severity of both eye and facial injuries is muchgreater for the military than in the civilian population; however,these injuries in both the civilian and military sectors can beseverely debilitating and pose an enormous health cost. Due to alack of instrumentation, the prediction of eye and facial injuriesusing anthropomorphic test devices is not currently possible.In order to develop an appropriately biofidelically responding eye,it is necessary to understand the boundary conditions of thehuman eye under impact conditions. The current study presentsbiofidelity design requirements for synthetic eyes that can beused for dynamic impact tests. This technology will be useful notonly for the military to evaluate protective equipment prior todeployment, but also will be useful in the civilian population for

ARTICLE IN PRESS
E. Kennedy, S. Duma / Journal of Biomechanics 41 (2008) 3297–3302 3301
evaluation of various facial impact scenarios, such as sportsinjuries and automotive accidents.
A limitation of the current study is that tests were onlyconducted at one impact energy level. All tests were conducted atfrom a range of 8.0–8.5 m/s, with an impactor energy of up to 4.1 J.Due to the large surface area of the flat 19 mm diameter impactortip, the normalized energy of this impactor is a maximum14,400 J/m2. Combining this result with the results of a concur-rently conducted and previously published study, this level ofnormalized energy poses less than a 10% risk of globe rupturebased on the results of other studies (Kennedy et al., 2006). Notsurprisingly, most of the tests in this study did not result in globerupture, with only three out of ten total tests resulting in globerupture—and two of those injuries from the same specimen,suggesting perhaps a weaker overall tolerance to injury. Based onthe results of this study and by Cirovic et al. (2005), it is notexpected that testing at alternative speeds would have elucidateda different response from the extraocular muscles; however,it would be desirable to increase the impact energy to a levelthat offers higher injury probability for further experimentalvalidation.
It should also be addressed that this study attempted to lookonly at the relationship between the extraocular muscles and theincidence of globe rupture, the most catastrophic, but certainlynot the only type of eye injury associated with blunt impacts. Thisis due to the fact that other injuries, such as hyphema, lensdamage, and retinal damage cannot be assessed on post-mortemeyes. Therefore, in a similar manner to other reported studies(Weidenthal, 1964; Green et al., 1990; Vinger et al., 1999; Basset al., 2002; Stitzel et al., 2002; Kennedy et al., 2006), globerupture was the only eye injury that was evaluated in conjunctionwith the impact response. Current computational models of theeye for impact scenarios do not model the interface between thesclera and the retina, or ciliary body/zonules/lens interfaces(Kisielewicz et al., 1998; Uchio et al., 1999, 2001; Power et al.,2002; Stitzel et al., 2002, 2005; Hansen et al., 2003), but may beuseful to compare stress distributions including extraocularmuscle insertion points, and common sites of retinal or lensinjuries. If in-vivo models were used to study these eye injurytypes (hyphema, lens damage, retinal damage) the effects of theextraocular muscles, will be accounted for due to the nature of thetest conditions using in-vivo surrogate models.
5. Conclusion
The purpose of this study was to determine the influence thatextraocular muscles have on eye impact response and injuryoutcome. In order to analyze the effects that the extraocularmuscles have on eye impact response, dynamic eye impact testswere conducted using a custom-designed eye impact device. Eyeswere tested in situ as matched pairs, with the extraocular musclesfrom one eye transected, and the extraocular muscles from thecontra-lateral eye intact. Similar overall force–deflection andinjury responses were observed between the eyes with theextraocular muscles left intact and the extraocular musclestransected and were not statistically significant. Therefore, basedon the data presented in this study the extraocular muscles do nothave an appreciable influence on the force–deflection response ofhuman eyes. The results of this study provide data that can beused to quantify the boundary conditions of in-situ human eyes toblunt impact. These data can be used to assess testing methods foreye injury where extraocular muscles are not accounted for, suchas ex-vivo eyes in gelatin-filled orbits. Similarly, these data can beused to develop a biofidelic synthetic eye for the purposes ofimpact injury risk assessment.
Conflict of interest statement
I have no financial and/or personal relationships with otherpeople or organizations that could inappropriately influence (bias)this work. Examples of potential conflicts of interest includeemployment, consultancies, stock ownership, honoraria, paidexpert testimony, patent applications/registrations, and grants orother funding.
Acknowledgement
The authors would like to acknowledge the SouthernConsortium of Injury Biomechanics (SCIB) for their support ofthis study.
References
Bass, C., Davis, M., Stitzel, J., Duma, S., 2002. Airbag interaction with night visiongoggles. Report to the United States Army Aeromedical Research Laboratory,Fort Rucker, Alabama.
Berger, R.E., 1978. A model for evaluating the ocular contusion injury potential ofpropelled objects. Journal of Bioengineering 2, 345–358.
Chisholm, L., 1969. Ocular injury due to blunt trauma. Applied Therapeutics 11 (11),597–598.
Cirovic, S., Bhola, R.M., Hose, D.R., Howard, I.C., Lawford, P.V., Parsons, M.A., 2005. Acomputational study of the passive mechanics of eye restraint during headimpact trauma. Computer Methods in Biomechanics and Biomedical Engineer-ing 8 (1), 1–6.
Clement, R.A., 1987. Description of the length-tension curves of the extraocularmuscles. Vision Research 27 (3), 491–492.
Duma, S.M., Kress, T.A., Porta, D.J., Woods, C.D., Snider, J.N., Fuller, P.M., Simmons,R.J., 1996. Air bag induced eye injuries: a report of 25 cases. Journal of Trauma41 (1), 114–119.
Duma, S.M., Jernigan, M., Stitzel, J.D., Herring, I., Crowley, J., Brozoski, F., Bass, C.,2002. The effect of frontal air bags on eye injury patterns in automobilecrashes. Archives of Ophthalmology 120 (11), 1517–1522.
Green Jr., R.P., Peters, D.R., Shore, J.W., Fanton, J.W., Davis, H., 1990. Force necessaryto fracture the orbital floor. Ophthalmic Plastic and Reconstructive Surgery 6(3), 211–217.
Hansen, G.A., Stitzel, J.D., Duma, S.M., 2003. Incidence of elderly eye injuries inautomobile crashes: the effects of lens stiffness as a function of age. In:Association for the Advancement of Automotive Medicine, 47th AnnualProceedings, Lisbon, Portugal.
Heier, J.S., Enzenauer, R.W., Wintermeyer, S.F., Delaney, M., LaPiana, F.P., 1993.Ocular injuries and diseases at a combat support hospital in support ofOperations Desert Shield and Desert Storm. Archives of Ophthalmology 111,795–798.
Kennedy, E.A., Voorhies, K.D., Herring, I.P., Rath, A.L., Duma, S.M., 2004.Prediction of severe eye injuries in automobile accidents: static anddynamic rupture pressure of the eye. In: The Proceedings of the 48thAssociation for the Advancement of Automotive Medicine Conference, KeyBiscayne, Florida.
Kennedy, E.A., Ng, T.P., McNally, C., Stitzel, J.D., Duma, S.M., 2006. Risk functions forhuman and porcine eye rupture based on projectile characteristics of bluntobjects. Stapp Car Crash Journal, 50.
Kisielewicz, L.T., Kodama, N., Ohno, S., Uchio E., 1998. Numerical prediction ofairbag caused injuries on eyeballs after radial keratotomy. Society ofAutomotive Engineers.
Klein, B.E.K., Klein, R., Linton, K.L.P., 1992. Intraocular pressure in an Americancommunity. Investigative Ophthalmology and Visual Science 33 (7),2224–2228.
Kuhn, F., Morris, R., Witherspoon, C.D., Mann, L., Mester, V., Modis, L., Berta, A.,Bearden, W., 2000. Serious fireworks-related eye injuries. OphthalmicEpidemiology (7), 139–148.
Lessley, D., Crandall, J.R., Shaw, C.G., Kent, R.W., Funk, J.R., 2004. A normalizationtechnique for developing corridors from individual subject responses. SAE,2004-01-0288.
Mader, T.H.L., Aragones, J.V., Chandler, A.C., Hazlehurst, J.A., Heier, J., Kingham, J.D.,Stein, E., 1993. Ocular and ocular adnexal injuries treated by United Statesmilitary ophthalmologists during Operation Desert Shield and Desert Storm.Ophthalmology 100, 1462–1467.
McGwin, G., Xie, A., Owsley, C., 2005. Rate of eye injury in the United States.Archives of Ophthalmology 123, 970–976.
Miller, J.M., Bockisch, C.J., Pavolvski, D.S., 2002. Missing lateral rectus force andabsence of medial rectus co-contraction in ocular convergence. Journal ofNeurophysiology 87, 2421–2433.
Olsen, T.W., Aaberg, S.Y., Geroski, D.H., Edelhauser, H.F., 1998. Human sclera:thickness and surface area. American Journal of Ophthalmology 125 (2),237–241.

ARTICLE IN PRESS
E. Kennedy, S. Duma / Journal of Biomechanics 41 (2008) 3297–33023302
Olsen, T.W., Sanderson, S., Feng, X., Hubbard, W.C., 2002. Porcine sclera: thickness andsurface area. Investigative Ophthalmology and Visual Science 43 (8), 2529–2532.
Power, E.D., Stitzel, J.D., Duma, S.M., Herring, I.P., West, R.L., 2002. Investigation ofocular injuries from high velocity objects in an automobile collision. SAETechnical Paper Series 2002-01-0027, pp. 1–8.
Rodriguez, J.O., Lavina, A.M., 2003. Prevention and treatment of common eyeinjuries in sports. American Family Physician 67, 1481–1488.
Simonsz, H.J., Kolling, G.H., Kaufman, H., van Dijk, B., 1986. Intraoperative lengthand tension curves of human eye muscles including stiffness in passivehorizontal eye movement in awake volunteers. Archives of Ophthalmology 104(10), 1485–1500.
Stitzel, J.D., Duma, S.M., Cormier, J.M., Herring, I.P., 2002. A nonlinear finite elementmodel of the eye with experimental validation for the prediction of globerupture. Stapp Car Crash Journal, 46.
Stitzel, J.D., Hansen, G.A., Herring, I.P., Duma, S.M., 2005. Blunt trauma of the agingeye. Archives of Ophthalmology 123, 789–794.
Uchio, E., Ohno, S., Kudoh, J., Aoki, K., Kisielewicz, L.T., 1999. Simulation model of aneyeball based on finite element analysis on a supercomputer. British Journal ofOphthalmology 83, 1106–1111.
Uchio, E., Ohno, S., Kudoh, J., Kadanosono, K., Andoh, K., Kisielewicz, L.T.,2001. Simulation of air-bag impact on post-radial keratotomy eye usingfinite element analysis. Journal of Cataract Refractive Surgery 27,1847–1853.
Vinger, P.F., Sparks, J.J., Mussack, K.R., Dondero, J., Jeffers, J.B., 1997. A program toprevent eye injuries in paintball. Sports Vision 3, 33–40.
Vinger, P.F., Duma, S.M., Crandall, J.R., 1999. Baseball hardness as a risk factor foreye injuries. Archives of Ophthalmology 117, 354–358.
Weidenthal, D.T., 1964. Experimental ocular contusion. Archives of Ophthalmology71, 111–115.
Wong, T.Y., Smith, G.S., Lincoln, A.E., Tielsch, J.M., 2000. Ocular trauma in theUnited States Army: hospitalization records from 1985 through 1994.American Journal of Ophthalmology 129 (5), 645–650.