Embed Size (px)
Citation preview

ARTICLE IN PRESS
1466-853X/$ - s
doi:10.1016/j.pt
�Correspondment, Knowsle
Road, Prescot,
fax: +44 151 43
E-mail addr
Physical Therapy in Sport 9 (2008) 136–147
www.elsevier.com/ptsp
Literature Review
The effects of proprioceptive exercise and taping on proprioception insubjects with functional ankle instability: A review of the literature
Tom Hughesa,�, Patsy Rochesterb
aPhysiotherapy Department, Bradford Teaching Hospitals NHS Trust, St. Luke’s Hospital, Bradford, BD5 0NA, UKbDivision of Rehabilitation Studies, School of Health Studies, University of Bradford, 25 Trinity Road, Bradford, BD5 OBB, UK
Received 7 November 2007; received in revised form 29 May 2008; accepted 9 June 2008
Abstract
Objective: To investigate the effects of proprioceptive exercise rehabilitation and taping techniques on proprioceptive measures in
chronic functional ankle instability (FAI).
Design: Literature review.
Data sources: Keyword search of the AMED, CINAHL, Medline, PEDro and SPORTDiscus online databases from January 1985
to February 2007. Also reference lists of articles obtained were manually searched for relevant literature.
Results: The search yielded nine studies that investigated the effects of proprioceptive exercise training on proprioceptive measures.
Four studies investigated the effects of ankle taping on proprioceptive measures. The exercise literature was limited due to
poor methodological quality. There is some agreement that muscle reaction time, kinaesthetic deficits and postural sway may improve
with proprioceptive exercise; however, due to differences in study methodology and quality, no specific recommendations for
practice can be made. Taping literature is also limited in terms of quantity and methodological quality. The effect on muscle reaction
time, kinaesthesia, and postural sway rely on one study for each element, therefore conclusive recommendations for practice cannot
be made.
Conclusion: There is a paucity of high-quality evidence investigating the effects of proprioceptive exercise and taping. Further high-
quality clinical trials are needed to enhance the evidence base in order to help guide physiotherapists in selecting appropriate,
effective strategies when managing FAI.
r 2008 Elsevier Ltd. All rights reserved.
Keywords: Ankle injuries; Proprioception; Exercise; Taping
1. Introduction
Ankle inversion sprains are common athletic injuries(Denegar & Miller, 2002; Hertel, 2002) with morethan 40% of cases becoming recurrent following theinitial incident (Gerber, Williams, Scoville, Arciero, &Taylor, 1998). Mechanical instability and functional
ee front matter r 2008 Elsevier Ltd. All rights reserved.
sp.2008.06.003
ing author. Present address: Physiotherapy Depart-
y Primary Care Trust, Whiston Hospital, Warrington
Merseyside, L35 5DR, UK. Tel.: +44 151 4301277;
01162.
ess: [email protected] (T. Hughes).
ankle instability (FAI) have been hypothesised asunderlying causes of recurrent sprains (Hertel, 2000).Mechanical instability is defined as laxity and excessivejoint motion of the talocrural, subtalar and/or inferiortibiofibular joints due to structural damage of thesupporting ligamentous tissues (Hertel, 2000). FAI wasoriginally proposed by Freeman, Dean, and Hanham(1965) to describe subjective ‘‘giving way’’ or sensationsof ankle instability, and has been refined to meaningjoint motion occurring beyond voluntary control, butnot necessarily exceeding the physiological range ofmotion (Tropp, Odenrick, & Gillquist, 1985). Mechan-ical instability (MI) and FAI can coexist following ankle

ARTICLE IN PRESST. Hughes, P. Rochester / Physical Therapy in Sport 9 (2008) 136–147 137
inversion sprains although may not be related (Boyle &Negus, 1998), as a high proportion of individualscomplaining of recurrent sprains do not demonstrategross mechanical instability on examination (Hertel,2000).
In normal functioning, proprioceptive informationsuch as kinaesthesia and joint position sense (JPS) areobtained from mechanoreceptors upon detection ofjoint displacements or perturbations. This elicits com-plex responsive reflex neural muscle activation, toincrease muscle stiffness and resist these displacements,to maintain postural stability (Baltaci & Kohl, 2003)and functional joint stability (Riemann & Lephart,2002). Following lateral ankle sprain, ligamentous tissueis thought to heal effectively but mechanoreceptordisruption within the lateral ligaments and talocruraljoint capsule results in reduced ability to detect changesin JPS (Hertel, 2000), a process termed deafferentiationby Freeman et al. (1965). Ankle sprains also causesubstantial deficits to kinaesthetic sense (Konradsen,2002) although it is unclear how this occurs. JPS deficitsresult in improper positioning of the foot prior to and atheel strike during gait, causing susceptibility to inversioninjury (Bernier & Perrin, 1998) whereas kinaestheticdeficits delay reflex neuromuscular response time tosudden inversion, subsequently contributing to FAI(Hertel, 2000).
Experimental studies have demonstrated a correlationbetween impaired proprioception and FAI. Deficitshave been identified in JPS (Boyle & Negus, 1998;Jerosch & Bischof, 1996; Liu, Jeng, & Lee, 2005),postural stability control (Fu & Hui-Chan, 2005;Nakagawa & Hoffman, 2004), kinaesthesia (Garn &Newton, 1988; Lentell et al., 1995; Refshauge, Kilbreath,& Raymond, 2003) and delayed peroneal reaction timeto sudden inversion stresses (Fernandes, Allison, &Hopper, 2000; Konradsen & Ravn, 1990; Lofvenberg,Karrholm, Sundelin, & Ahlgren, 1995; Vaes, VanGheluwe, & Duquet, 2001). Consequently, narrativereviews report that exercise rehabilitation aimed atretraining proprioceptive deficits associated with FAI,such as using multiaxial platforms or wobble boards, isassociated with positive outcome (Baltaci & Kohl, 2003;Mattacola & Dwyer, 2002; Wilkerson & Nitz, 1994)Additionally, therapeutic ankle taping is advocated toenhance proprioception in FAI (Wilkerson, 2002), byproviding cutaneous afferent feedback (Refshauge,Kilbreath, & Raymond, 2000). However, the internalvalidity of these reviews is questionable, as it is unclear ifevidence upon which recommendations are based hasbeen assessed for quality. Also, it is unclear whichaspects of proprioception might be affected.
There is currently only one systematic review avail-able that has investigated prevention of ankleligament injuries (Handoll, Roe, Quinn, & de Bie,2001) but this focuses on prophylactic interventions
for subjects at risk of, or following acute lateralligament sprain and their effects on re-injury occurrence,whereas trials investigating treatment effects on pro-prioceptive measures were excluded. There are currentlyno known systematic reviews exclusively investigatingthe effects of proprioceptive exercise and the use oftherapeutic taping on measures of proprioception inFAI management.
As such, there is little high-quality evidence-basedguidance available to physiotherapists to aid selectionof appropriate proprioceptive management strategies.The aim of this paper is to provide a review of primaryevidence relating to the effects of proprioceptive exerciserehabilitation and taping techniques on measures ofproprioception in subjects with chronic FAI.
2. Methodology
2.1. Search strategy
The literature search was date limited from January1985 to February 2007. The AMED, CINAHL, Med-line, PEDro and SPORTDiscus online databases weresearched using the following keywords: ankle jointAND sprains and strains; OR joint instability; ANDproprioception; OR kinaesthesia; OR joint positionsense; OR peroneal reaction time; OR postural control;OR postural sway; AND physiotherapy; OR physicaltherapy; OR exercise therapy; OR therapeutic exercise;OR rehabilitation; OR balance training; OR tape; ORstrapping. Reference lists of all articles obtained weremanually scanned to identify additional studies relevantto the search.
2.2. Study selection criteria
Titles and abstracts identified from the results of thesearch were screened by both researchers. Suitabilityconsensus was reached using the agreed inclusion/exclusion criteria. If the authors were uncertain, the fulltext of a reference was obtained and analysed toestablish suitability.
Randomised controlled trials (RCTs) or quasi-experimental clinical trials were included for assessmentif the criteria in Table 1 were met.
2.3. Assessment of methodological quality and data
collection
All relevant studies were independently assessed bythe researchers without blinding, using the ScottishIntercollegiate Guidelines Network (SIGN) criticalappraisal tool (SIGN, 2006), as this forms a systematicmethod of appraising, scoring and grading evidence interms of validity. Data collection forms were used for

ARTICLE IN PRESS
Table 1
Inclusion and exclusion criteria
Criteria
Inclusion � Trials investigating subjects of any age, classified as
suffering from FAI or chronic, recurrent lateral ankle
sprains with subjective feeling of instability/giving way
� Trials that primarily investigate the effects of
proprioceptive exercise therapy and therapeutic taping
on proprioceptive outcome measures including JPS
(joint reposition tests), kinaesthesia (detection of active/
passive movement), muscle response time (muscle
reaction time to external perturbation) and postural
control (stabilometry/postural sway tests)
� Trials published in peer-reviewed journals only, written
in the English language
Exclusion � Trials investigating healthy, uninjured subjects, subjects
that have experienced only one acute lateral ankle
sprain. Subjects classified as suffering ‘‘ankle injury’’
only
� Trials where the primary outcome measures are not
directly related to proprioceptive testing, such as
reinjury rate and athletic performance tests (i.e. agility/
vertical jump height/sprinting times)
� Trials published in language other than English, and
grey literature
T. Hughes, P. Rochester / Physical Therapy in Sport 9 (2008) 136–147138
each article reviewed to provide a visual representationof each trial’s key points and an evidence level grade wasassigned. Once completed, the researchers met tocompare the results and reach consensus regarding eachstudy’s methodological quality.
2.4. Data synthesis
It was anticipated that following data collection, datafrom each trial that carried a low risk or very low risk ofbias according to SIGN (2006) were to be included foranalysis, whereas trials considered as carrying a highrisk of bias according to SIGN (2006) were to beexcluded from the analysis. Due to the limited quantityand quality of available evidence, however, this was notpossible. Therefore, all trials that met the inclusioncriteria were included for analysis, providing no exclu-sion criteria existed.
Extracted data were summarised by tabulation,allowing descriptive analysis of methodological rigourand whether heterogeneity of methodology and resultsexisted between studies (Deeks et al., 2001).
3. Results
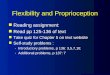
Fig. 1 shows the flow chart for study selection for thispaper.
3.1. Effects of proprioceptive exercise rehabilitation on
proprioception
A summary of trials investigating proprioceptiveexercise rehabilitation is provided in Table 2.
3.1.1. Methodological quality
The methodological quality of all trials investigatingthe effects of proprioceptive exercise training wasconsidered poor. A clear research aim was provided ineight studies (Bernier & Perrin, 1998; Clark & Burden,2005; Eils & Rosenbaum, 2001; Gauffin, Tropp, &Odenrick, 1988; Hess, Joyce, Arnold, & Gansneder,2001; Osborne, Chou, Laskowski, Smith, & Kaufman,2001; Powers, Buckley, Kaminiski, Hubbard, & Ortiz,2004; Rozzi, Lephart, Sterner, & Kuligowski, 1999).However, in comparison, Pintsaar, Brynhildsen, andTropp (1996) presented an unclear aim, thus it wasunknown whether the methodology addressed theresearch question.
Four studies were RCTs (Bernier & Perrin, 1998;Clark & Burden, 2005; Hess et al., 2001; Powers et al.,2004) whereas five were considered of quasi-experimentaldesign (Eils & Rosenbaum, 2001; Gauffin et al., 1988;Osborne et al., 2001; Pintsaar et al., 1996; Rozzi et al.,1999). Although randomised subject allocation was usedin all RCTs, none reported details of the actualprocedure, nor were any details regarding concealmentmethods documented. As such, it is unknown whetherthe allocation methods were robust against researcherbias, and as inadequate allocation concealment isassociated with selection bias (Schulz, Chalmers, Hayes,& Altman, 1995), the reliability and internal validity ofthese studies is questionable.
Of the quasi-experimental trials, Gauffin et al. (1988)and Eils and Rosenbaum (2001) did not report sampleselection methods used, although Rozzi et al. (1999)used a volunteer sample of FAI subjects. Pintsaar et al.(1996) also reported on selection methods implemented,but their description was ambiguous. As such, in allthese studies it is questionable whether the sampleswere truly representative of the target population, inaddition to potentially introducing selection bias asdiscussed previously. In contrast, Osborne et al. (2001)provided adequate detail of sample selection methods,where a medical records database was reviewed forsubjects with the diagnosis of ‘‘ankle sprain’’. Recordsretrieved were then randomly reviewed to establishinclusion suitability, and those applicable were invitedto participate.
Anthropometric data of subject groups were notdescribed by Gauffin et al. (1988), Pintsaar et al. (1996)and Bernier and Perrin (1998), whereas characteristicssuch as age, weight and height were reported for thesample as a whole by Hess et al. (2001) and Powers et al.(2004). Therefore, it was difficult to ascertain whether

ARTICLE IN PRESS
239 potentially relevant studies identified by title, following cross-
referencing in bibliographic software.
Abstracts screened of all 239 potentially relevant studies
retrieved for detailed analysis
214 studies excluded as inclusion criteria not met/exclusion criteria
present
25 full text articles of studies potentially appropriate for
inclusion in review obtained and analysed in detail
12 studies excluded as inclusion criteria not met/exclusion criteria
present
13 studies included in systematic review
Fig. 1. Flow chart illustrating study selection for inclusion.
T. Hughes, P. Rochester / Physical Therapy in Sport 9 (2008) 136–147 139
samples used were comparable. Conversely, Rozzi et al.(1999), Osborne et al. (2001) and Clark and Burden(2005) presented descriptive anthropometric data ac-cording to the conditions subjects were allocated,indicating comparable cohorts, although this was nottested statistically. Although Eils and Rosenbaum(2001) analysed anthropometric data in groups bothdescriptively and statistically, the statistical test usedwas not reported, therefore it was unknown whetherappropriate analyses were conducted, and subsequentlyif groups were actually comparable.
Only three trials reported subject drop out. Pintsaaret al. (1996) found that two subjects dropped out of theexercise group, whereas Osborne et al. (2001) found onlyone subject failed to complete the study. Bernier andPerrin (1998) documented that two subjects droppedout of the control group, and one dropped out of thesham electrotherapy group. In these studies, this
represents a degree of attrition bias. As all other trialsdid not report drop out, it is questionable whether thedata were afflicted with such bias, threatening internalvalidity.
Detailed procedural descriptions were provided byBernier and Perrin (1998), Rozzi et al. (1999), Eils andRosenbaum (2001), Hess et al. (2001), Powers et al.(2004) and Clark and Burden (2005). However, descrip-tion of the exercise intervention was limited by Osborneet al. (2001), whereas inadequate description of theprocedure was provided by Gauffin et al. (1988) andPintsaar et al. (1996), therefore threatening methodolo-gical reliability.
Powers et al. (2004) utilised examiner blinding in anattempt to eliminate researcher bias, but how this wasachieved was unclear. However, all other trials did notstate whether blinding was used. Surprisingly, instru-mental validity was not reported in any trial, and only

ARTIC
LEIN
PRES
STable 2
Summary of trials investigating proprioceptive exercise rehabilitation
Author Number of
subjects (N)
Intervention Testing and follow up
time
Outcome measurement Results
Gauffin et al.
(1988)
10 FAI subjects 1. Affected leg trained only using single leg
standing on an ankle disk, for 10min, 5
times per week for 8 weeks
Pre-test and following 8
weeks
Postural sway calculated by
measure of centre of pressure
in single leg stand on force
plate
There was a significant decrease in postural
sway following ankle disk training (po0.001)
Pintsaar et al.
(1996)
12 uninjured
subjects
1. Uninjured control subjects measured once
for reference
Control subjects tested
once for reference (not
stated when)
Postural sway measured by
calculating postural control
latency in response to
perturbation on force plate in
single leg standing
No differences observed in latencies of any
group
15 FAI subjects 2. FAI subjects underwent an 8-week
proprioceptive training session (3–5 sessions
per week) using an ankle disk
In FAI subjects, ankle strategies used less at
pre-test, and returned to ‘‘normal’’ post-test
(no p-value given)
11 MI subjects 3. MI subjects used an ankle brace for 6 weeks
and measured in barefoot, with shoe, and
with shoe and brace
FAI subjects pre-tested
and after 2 weeks
Degree of use of ankle
strategy/hip strategy in
maintaining postural
equilibrium following
perturbation calculated using
force plate data in
biomechanical equation
MI subjects used less ankle strategy in barefoot,
increasing with a shoe in situ. No further
differences observed with brace and shoe
combined (no p-value given)MI subjects only tested
after 6 weeks (no pre-
test measure taken)
Bernier and
Perrin (1998)
48 FAI subjects Subjects randomised into:
1. Control: requested not to participate in
strength/balance training for 6 weeks
2. Sham: sham electrical stimulation of
peroneal muscles for 6 weeks
3. 10min sessions per week of standardised
progressive proprioceptive exercises: single
leg balancing on stable surface, on uniaxial
tilt board (in the plantar/dorsiflexion,
inversion/eversion and combined plantar/
dorsiflexion and inversion/eversion planes),
on wobble board, and hopping activities, all
repeated with eyes open/closed
Pre-test and 6 weeks Active and passive angle
reproduction using isokinetic
dynamometer
Modified equilibrium score significantly
improved in group 3 compared to 1 and 2 at
post-test (po0.05)
Postural sway using single leg
stand on balance platform
and calculating sway index
and modified equilibrium
score
No significant differences observed for sway
index or angle reproduction measures
Rozzi et al.
(1999)
13 FAI subjects Both groups underwent:
1. 4-week balance training programme using
Biodex Stability System (three sessions per
week) consisting of: balancing on single
limb on a stable and unstable setting,
balancing on single limb, actively moving
platform anterior/posterior, medial/lateral,
and multiplane circles
Pre-test and 4 weeks Postural sway calculated by
measuring single leg balance
using Biodex Stability System
FAI group subjects had significantly greater
pre-training postural sway scores than controls
(po0.05), though no significant differences at
the stable setting
13 uninjured
control subjects
At unstable and stable settings, post-training
postural sway significantly improved compared
to pretraining scores (po0.05). There was no
significant difference in post-training scores
between either group
T.
Hu
gh
es,P
.R
och
ester/
Ph
ysica
lT
hera
py
inS
po
rt9
(2
00
8)
13
6–
14
7140

ARTIC
LEIN
PRES
SEils and
Rosenbaum
(2001)
30 FAI subjects Subjects randomised into:
1. Exercise group (N ¼ 20) completed
6-week circuit (20min sessions, once per
week) consisting of: warm up, single leg
stance on mobile platform, ankle disk, with
contralateral leg performing resisted
abduction with exercise band, trampette.
Maintaining balance during; double and
single leg stand on air cushion, tilt board,
horizontal/vertically mobile platform,
Biodex Stability system
2. Control group (N ¼ 10) only participated in
test procedures
Pre-test and following 6
weeks
JPS measured with footplate
and goniometer to measure
reproduction of passive
dorsiflexion and
plantarflexion angle
Exercise group demonstrated significant
improvements in passive angle reproduction at
all angles other than 101 dorsiflexion
(p ¼ 0.057), whereas non-significant differences
with control scores existed
Postural sway measured in
single leg stance on force plate
Postural sway significantly improved in both
groups at post-test (po0.01)
Surface electrode EMG of
tibialis anterior, peroneus
longus and peroneus brevis
muscular reaction time to
simulated inversion injury
Muscle reaction time of peroneus longus and
brevis significantly improved in the exercise
group (po0.001), but no other differences
observed
Hess et al.
(2001)
20 FAI subjects Subjects randomised into:
1. Control condition, where pre-test and post-
test measures taken, but no training
performed for the duration of the study
2. 4-week agility training programme using
agility ladder (3� 20min sessions/week)
consisting of 3–5min warm up and the
following drills: forward 2 feet in, lateral
2 feet in, forward shuffle, 1 foot in shuffle,
forward slalom jumps, forward cross steps
and 901 angle exercises
Pre-test and 4 weeks Postural sway measured by
calculating sway index during
single leg stand on Chattex
Balance System
No significant differences observed between
pre-test and post-test sway index scores for
either group
Osborne et al.
(2001)
9 subjects with
history of non
rehabilitated ankle
sprains
1. 8-week training programme using an ankle
disk for 15min per day
Pre-test and following 8
weeks
Indwelling fine wire EMG of
tibialis anterior, posterior,
peroneus longus and flexor
digitorum longus assessing
onset latency
A significant decrease (p ¼ 0.02) in tibialis
anterior onset latency was observed in ankles
following training
Powers et al.
(2004)
38 FAI subjects Subjects randomised into:
1. Progressive plantarflexion, dorsiflexion,
inversion, eversion strength training using
theraband
2. Proprioception training using theraband
kicks
3. A combination of the above
4. Control, where no exercise permitted
Pre-test and following 6
weeks
Postural sway using single leg
stand on force plate
No significant effects of any condition between
groups of pre-test and post-test measure of
postural sway or muscle fatigueEMG of tibialis anterior and
peroneus longus, to assess
muscular fatigue
Clark and
Burden, (2005)
19 FAI subjects Subjects randomised into:
1. Exercise programme completed 3-times per
week; standing on wobble board-rocking
board forward/backward, side/side, circular
Pre-test, 2 weeks and
following 4 weeks
Surface EMG of tibialis
anterior and peroneus longus
assessing onset latency
Exercise group showed significant
improvement in AJFAT score post-test
(po0.01) compared to the control
Ankle joint functional
assessment tool (AJFAT)
Significant improvements occurred between pre
and post-test scores for the exercise group,
T.
Hu
gh
es,P
.R
och
ester/
Ph
ysica
lT
hera
py
inS
po
rt9
(2
00
8)
13
6–
14
7141

ARTICLE IN PRESSTable
2(c
onti
nu
ed)
Author
Number
of
subjects(N
)
Intervention
Testingandfollow
up
time
Outcomemeasurement
Results
movem
ents.Allexercisesrepeatedwith
flexed
kneesandhandsonbuttocks.Also
single
legstandingonthewobble
board
completed
2.Control—
notraining
(po0.01),withsignificantdifferencesobserved
betweenweeks0–2(po0.05)fortibialis
anterior(po0.05)andperoneuslongus
(po0.01)onsetlatency
FAI¼
Functionalankle
instability,MI¼
Mechanicalinstability,JP
S¼
Jointpositionsense.
T. Hughes, P. Rochester / Physical Therapy in Sport 9 (2008) 136–147142
Rozzi et al. (1999) provided data highlighting thereliability of the instrumentation used. The intraclasscorrelation coefficient of the Biodex Stability Systemwas reported as between 0.6 and 0.95 at varying levels ofstability (Rozzi et al., 1999), which represents fair toexcellent reliability. Therefore, data presented in alleight other trials must be interpreted with caution, as itis unknown whether the instruments used are valid andreliable measures of proprioception.
Finally, small sample sizes may affect overall statis-tical power in the trials by Gauffin et al. (1988), Hesset al. (2001) and Osborne et al. (2001).
3.1.2. Summary
The evidence investigating effects of proprioceptiveexercise therapy was limited due to poor methodologicalquality, therefore the data should be interpreted withcaution. However, there is some agreement thatperoneus longus muscle reaction time may improveafter proprioceptive retraining (Clark & Burden, 2005;Eils & Rosenbaum, 2001). Nevertheless, differences intraining activities, duration and frequency of bothrehabilitation programmes make it difficult to recom-mend specific evidence-based exercises that may influ-ence this. There is some agreement that ankle disktraining improves tibialis anterior reaction time (Clark& Burden, 2005; Osborne et al., 2001), though there isno consensus regarding specific types, duration andfrequency of training required to influence this, due tomethodological differences.
There is consensus that proprioceptive exercise mayimprove postural sway in FAI subjects (Bernier &Perrin, 1998; Eils & Rosenbaum, 2001; Gauffin et al.,1988; Rozzi et al., 1999), with agreement from twostudies that 6-week composite exercise programmesusing modalities, such as ankle disks, tilt boards andsingle-leg standing activities are effective (Bernier &Perrin, 1998; Eils & Rosenbaum, 2001). However, thereis no agreement in optimum exercise frequency due tomethodological differences.
Other exercises in isolation may improve posturalsway, such as single-leg stand ankle disk training(Gauffin et al., 1988) and Biodex Stability Systemprogrammes (Rozzi et al., 1999). Conclusive recommen-dations, however, cannot be made as each approachrelies on data from one trial in isolation, and as bothmodalities have been used in the composite programmespresented by Bernier and Perrin (1998) and Eils andRosenbaum (2001), it may be more appropriate toutilise these combined with other activities.
Training using agility ladders (Hess et al., 2001),theraband kicks, theraband strengthening and bothcombined may not improve postural sway (Powerset al., 2004). These results are based upon limitedevidence of one study for each component, therefore,further research is required before conclusive

ARTICLE IN PRESST. Hughes, P. Rochester / Physical Therapy in Sport 9 (2008) 136–147 143
recommendations could be given regarding the use ofthese modalities in rehabilitation.
There is conflicting evidence regarding the effect of6-week composite proprioceptive exercise programmeson JPS, therefore recommendations for practice cannotbe made. In light of the limited evidence relating to theeffects of proprioceptive exercise rehabilitation, there isa clear need for further high-quality research into thisarea.
3.2. Effects of ankle taping on proprioception
A summary of trials investigating the effects of tapingon proprioception are included in Table 3.
3.2.1. Methodological quality
The evidence related to the effects of taping onproprioception in subjects with FAI was consideredpoor. The research aim was adequate but lacking insome specificity in one study (Karlsson & Andreasson,1992), but was clear and detailed in the other threestudies (Leanderson, Ekstam, & Salomonsson, 1996;Matsusaka, Yokoyama, Tsurusaki, Inokuchi, & Okita,2001; Refshauge et al., 2000). Three studies were ofquasi-experimental design. Leanderson et al. (1996) andRefshauge et al. (2000) used non-equivalent pre-testpost-test designs, and Karlsson and Andreasson (1992)utilised a repeated measures design. The study byMatsusaka et al. (2001) was the only RCT included.Despite using randomised subject allocation, the meth-od implemented was not documented, nor were detailsprovided regarding allocation concealment, subse-quently creating a source of potential researcher andselection bias.
Sample selection methods were not reported byKarlsson and Andreasson (1992), and Leandersonet al. (1996), although Refshauge et al. (2000) high-lighted that a volunteer sample was obtained. Therefore,for all three trials it was unclear whether the sampleswere representative of the FAI population, in additionto being potential sources of selection bias.
Anthropometric data of subject groups were notdescribed by Karlsson and Andreasson (1992), and onlyage ranges of both groups were reported by Leandersonet al. (1996) with a mean age difference of 7 yearsbetween groups. Therefore, it is questionable whethergroups were comparable. This was addressed byRefshauge et al. (2000), who matched groups on age,height, weight and activity level factors. However,although descriptively comparable, inferential statisticswere not performed to establish significant differences.Matsusaka et al. (2001) was the only trial to address thisto ensure appropriate group comparability.
Participant drop out rate was reported by Matsusakaet al. (2001) only, where no attrition was observed. Assuch the internal validity of the other three trials is
threatened, as it is unclear whether the results wereinfluenced by attrition bias. Blinding was not addressedby Karlsson and Andreasson (1992), Leanderson et al.(1996) and Matsusaka et al. (2001), although Refshaugeet al. (2000) implemented subject blinding in an attemptto reduce detection bias. However, it was unclear howthis was achieved. Procedural descriptions lacked detailin three trials thus limiting reliability. Karlsson andAndreasson (1992) provided adequate description of theankle inversion platform used, but limited detailsregarding electrode placement, taping techniques usedand when testing procedures were completed. Leander-son et al. (1996) provided no details regarding tapingtechnique used, which undermines the external validityof the results. Also an adequate description wasprovided regarding outcome measurement, although itwas unclear whether the control group underwent thesame intervention, and whether they participated in afootball practice session. Refshauge et al. (2000)provided adequate procedural description and detaileddiagrams demonstrating the taping method used,although details were lacking regarding duration andfrequency of rest periods. In contrast Matsusaka et al.(2001) provided specific procedural details.
Reliability and validity of outcome measures used wasnot addressed in any study, therefore all data should beinterpreted with caution as it is unknown whether thetechniques and instruments used are reliable or valid inmeasuring proprioception.
3.2.2. Summary
The evidence related to effects of taping on proprio-ceptive measures is severely limited in terms of quantityand methodological quality, and interpretation ofavailable data must be completed with caution. Threestudies suggest that taping may affect some propriocep-tive measures. However, evidence relating to tapingeffects on muscle reaction time and kinaesthesia relyon 1 study each (Karlsson & Andreasson, 1992;Refshauge et al., 2000). Similarly, the effects of tapingin isolation on postural sway has been addressed byone study (Leanderson et al., 1996), and taping incombination with ankle disk training addressed in onestudy (Matsusaka et al., 2001), therefore conclu-sive recommendations for practice cannot be provided.In retrospect, there is a clear need for further high-quality clinical research addressing the areas covered,and relating to other aspects of taping such as effects onJPS.
4. Discussion
The aim of this study was to provide a review ofprimary evidence relating to the effects of proprioceptiveexercise rehabilitation and taping techniques on mea-sures of proprioception in subjects with chronic FAI. It

ARTIC
LEIN
PRES
S
Table 3
Summary of trials investigating effects of taping on proprioception
Author Number of
subjects (N)
Intervention Testing and follow-
up time
Outcome measurement Results
Karlsson and
Andreasson
(1992)
20 FAI subjects All subjects underwent:
1. Muscle reaction time to simulated
inversion sprain measured with no tape
2. Repeated procedure with application of
Gibney taping technique (minus heel
lock strips) using inelastic tape
Conditions tested
consecutively, time
between not stated
Muscle reaction time
measured of peroneus longus
and brevis using
electromyography surface
electrode
Muscle reaction time significantly shorter
(po0.05) with tape in situ than without
Leanderson et al.
(1996)
9 FAI subjects FAI group underwent:
1. Both feet tested before football practice
session
2. Tape applied to ankle and re-tested
prior to practice session
3. Taped ankle tested following 2 hr
practice session
4. Tape removed and untaped ankle
re-tested after 2 hr practice session
Conditions 1 and 2
measured before
football practice,
conditions 3 and 4
measured after
practice session
Postural sway measured by
recording maximum sway
amplitude during disk
perturbation and mean sway
during each trial; measured
with using single leg stand
on ankle disc mounted on
force plate
No significant differences between FAI and
control subjects before practice session
8 uninjured
control subjects
Maximal sway of both groups decreased
when the ankles were taped before the
practice session but unclear if this was
significant
After session no significant differences
existed in maximal or mean sway between
taped and untaped ankles
Maximal and mean sway amplitude
without taping was significantly smaller
after the practice session than beforehand
(po0.01)
Refshauge et al.
(2000)
25 subjects
suffering from
recurrent
inversion sprains
Both groups underwent:
1. Ankle taping applied consisting of heel
lock, stirrup and figure of six inelastic
strips
2. Ankles not taped
2� 1.5 hr testing
periods. Time
between not stated
Detection of angular
displacements of passive
plantarflexion and
dorsiflexion measured with
using linear servomotor
driven by ramp generator
No significant difference (p ¼ 0.27)
movement detection at any velocity tested
between experimental and control groups
18 uninjured,
matched control
subjects
No significant difference (p ¼ 0.28) in
movement detection between taped/
untaped conditions for either subject group
Matsusaka et al.
(2001)
22 FAI subjects Randomised to either
(1) Ankle disk training group completed
single limb stance on affected side,
10min per day, and 3 times per week
for 10 weeks
(2) As above, combined with two strips of
inelastic tape, one anterior and one
posterior to the lateral malleolus from
distal 1/3 of leg to sole of foot
Pre-test and at weeks
2, 3, 4, 5, 6, 8 and 10
Postural sway measured
using stabilometry with
subjects in single limb stance
with affected leg on force
plate
In group 1, postural sway significantly
improved after week 8 (po0.0001), but no
significant differences existed between
weeks 8–10 (p ¼ 0.254)
In group 2 postural sway significantly
improved between 4–6 weeks (po0.0001),
but no significant difference between weeks
6–10 (p40.892)
Postural sway was significantly less in
group 2, compared to group 1 in each test
made at the fourth (p ¼ 0.012), fifth
(p ¼ 0.006) and sixth (p ¼ 0.002) weeks
FAI ¼ Functional ankle instability.
T.
Hu
gh
es,P
.R
och
ester/
Ph
ysica
lT
hera
py
inS
po
rt9
(2
00
8)
13
6–
14
7144

ARTICLE IN PRESS
Table 4
Areas for further research
� Further trials investigating effects of specific proprioceptive
exercises/programmes and taping techniques on reaction time of
other muscles such as peroneus brevis, tibialis posterior, extensor
hallucis longus and extensor digitorum longus
� Trials investigating the optimum duration, frequency and intensity
of specific proprioceptive exercises/programmes on all
proprioceptive measures
� Trials investigating long-term follow-up of subjects who have
completed an exercise or taping rehabilitation programme on
measures of proprioception
� The effects of specific exercises/programmes, specific exercises/
programmes combined with taping techniques or taping in
isolation on measures of proprioception
� The effects of self-management proprioceptive exercise
programmes that are completed independently utilising equipment
commonly found in the home setting, on measures of
proprioception
� The effect of taping or proprioceptive exercises on self reported
measures of disability, and whether this correlates with
proprioceptive measures
� The effect of taping or proprioceptive exercise rehabilitation on
inversion injury recurrence, and whether this correlates with
proprioceptive measures
T. Hughes, P. Rochester / Physical Therapy in Sport 9 (2008) 136–147 145
was anticipated that the results would help guidephysiotherapists in selecting appropriate, evidence-based strategies in the management of FAI, thusimproving efficiency, time and cost effectiveness ofphysiotherapy management. Although the aim of thepaper had been adequately addressed, unfortunately,following completion of the literature search strategy itwas clear that there was a paucity of high-quality RCTsrelating to this subject area. However, the searchstrategy used might have imposed limits on the quantityof literature obtained, and ultimately resulted in asource of publication and selection bias. Trials were onlyconsidered for inclusion if they were published in peer-reviewed journals and written in the English language.As such other important evidence could have beenmissed if written in other languages or available withinunpublished grey literature. Nevertheless, the overallquality of the included evidence was poor, and allstudies were classed as carrying a high risk of biasaccording to the appraisal tool used. Therefore, theoverall validity of the evidence base is questionable andsubsequently, it has been difficult to formulate recom-mendations for physiotherapy practice.
Although acknowledged that statistical analysis of theobtained data by meta-analysis can increase statisticalpower and precision of conclusions of a review, meta-analyses of poor quality studies may be seriouslymisleading, as if bias is present, errors will be com-pounded leading to inappropriate conclusions (Higgins &Green, 2006). Therefore, following data extraction, it wasclear that meta-analysis was inappropriate for this review.
Despite conflicting results regarding effects of proprio-ceptive exercise on JPS, there is some agreement thatproprioceptive exercise training may improve peronealreaction time, kinaesthetic and postural sway deficitsassociated with FAI. Differences in study quality,methodology and exercise programmes implemented,however, do not allow specific recommendations regard-ing optimum duration and frequency of training sessions,and specific effective exercises to use cannot be made.Unfortunately, due to the paucity of evidence related tothe effects of taping, no recommendations for practice canbe made. As such, it could be argued that the primaryevidence available weakly supports the suggestions fromnarrative reviews published by Wilkerson and Nitz (1994),Mattacola and Dwyer (2002) and Baltaci and Kohl(2003), which suggest proprioceptive exercise rehabilita-tion is correlated with positive proprioceptive improve-ments in FAI management. The argument proposed byWilkerson (2002) that ankle taping facilitates propriocep-tion is not currently supported.
There is a clear need for further high quality andappropriately powered RCTs investigating all areascovered by this review, in order to enhance under-standing of the effects of proprioceptive exercise andtaping on proprioceptive measures. Also, other areas
that require further investigation have been identifiedand are presented in Table 4.
5. Conclusion
This review has highlighted a paucity of high-qualityclinical trials investigating the use of proprioceptiveexercise rehabilitation and taping on proprioceptivemeasures in FAI management. It is essential that furtherhigh-quality clinical trials are conducted to improveknowledge and understanding of the effects of proprio-ceptive exercise and taping on proprioception inindividuals experiencing FAI.
Acknowledgements
Conflict of Interest: No known conflict of interestoccurred during or after completion of this paper.
Ethical Approval: Prior to commencement, this studywas ethically approved by the University of BradfordEthics Panel.
Funding: This study was completely self-funded by theauthors.
References
Baltaci, G., & Kohl, H. W. (2003). Does proprioceptive training during
knee and ankle rehabilitation improve outcome? Physical Therapy
Reviews, 8, 5–16.

ARTICLE IN PRESST. Hughes, P. Rochester / Physical Therapy in Sport 9 (2008) 136–147146
Bernier, J. N., & Perrin, D. H. (1998). Effect of coordination training
on proprioception of the functionally unstable ankle. Journal of
Orthopaedic and Sports Physical Therapy, 27, 264–275.
Boyle, J., & Negus, V. (1998). Joint position sense in the re-
currently sprained ankle. Australian Journal of Physiotherapy, 44,
159–163.
Clark, V. M., & Burden, A. M. (2005). A 4-week wobble board
exercise programme improved muscle onset latency and perceived
stability in individuals with a functionally unstable ankle. Physical
Therapy in Sport, 6, 181–187.
Deeks, J., Khan, K. S., Song, F., Popay, J., Nixon, J., & Kleijnen, J.
(2001). Stage II: Conducting the review. Phase 7: Data synthesis. In
Undertaking systematic reviews of research on effectiveness: CRD’s
guidance for those carrying out or commissioning reviews. Centre for
Reviews and Dissemination. Available: /http://www.york.ac.uk/
inst/crd/pdf/crd4_ph7.pdfS; accessed 05.01.07.
Denegar, C. R., & Miller, S. J., III (2002). Can chronic ankle
instability be prevented? Rethinking management of lateral ankle
sprains. Journal of Athletic Training, 37, 430–435.
Eils, E., & Rosenbaum, D. (2001). A multi-station proprioceptive
exercise program in patients with ankle instability. Medicine and
Science in Sports and Exercise, 33, 1991–1998.
Fernandes, N. M., Allison, G. T. P., & Hopper, D. P. (2000). Peroneal
latency in normal and injured ankles at varying angles of
perturbation. Clinical Orthopaedics and Related Research, 375,
193–201.
Freeman, M. A. R., Dean, M. R. E., & Hanham, I. W. F. (1965). The
aetiology and prevention of functional instability of the foot.
Journal of Bone and Joint Surgery (British), 47B, 678–685.
Fu, A. S. N., & Hui-Chan, W. Y. (2005). Ankle joint proprioception
and postural control in basketball players with bilateral ankle
sprains. American Journal of Sports Medicine, 33, 1174–1182.
Garn, S. N., & Newton, R. A. (1988). Kinaesthetic awareness
in subjects with multiple ankle sprains. Physical Therapy, 68,
1667–1671.
Gauffin, H., Tropp, H., & Odenrick, P. (1988). Effect of ankle disk
training on postural control in patients with functional instability
of the ankle joint. International Journal of Sports Medicine, 9,
141–144.
Gerber, J. P., Williams, G. N., Scoville, C. R., Arciero, R. A., &
Taylor, D. C. (1998). Persistent disability associated with ankle
sprains: A prospective examination of an athletic population. Foot
and Ankle International, 19, 653–660.
Handoll, H. H. G., Roe, B. H., Quinn, K. M., & de Bie, R. A. (2001).
Interventions for preventing ankle ligament injuries. Cochrane
Database of Systematic Reviews, 3(3), Art. No.: CD000018.
doi:10.1002/14651858.CD000018.
Hertel, J. (2000). Functional instability following lateral ankle sprain.
Sports Medicine, 29, 361–371.
Hertel, J. (2002). Functional anatomy, pathomechanics, and patho-
physiology of lateral ankle instability. Journal of Athletic Training,
37, 364–369.
Hess, D. M., Joyce, C. J., Arnold, B. L., & Gansneder, B. M. (2001).
Effect of a 4-week agility training program on postural sway
in the functionally unstable ankle. Journal of Sport Rehabilitation,
10, 24–35.
Higgins, J. P. T., & Green, S. (2006). Cochrane handbook for systematic
reviews of interventions 4.2.6 [updated September 2006]. Chichester:
Wiley.
Jerosch, J., & Bischof, M. (1996). Proprioceptive capabilities of the
ankle in stable and unstable joints. Sports and Exercise Injury, 2,
167–171.
Karlsson, J., & Andreasson, G. O. (1992). The effect of external
ankle support in chronic lateral ankle joint instability: An
electromyographic study. American Journal of Sports Medicine,
20, 257–261.
Konradsen, L. (2002). Factors contributing to chronic ankle instabil-
ity: Kinaesthesia and joint position sense. Journal of Athletic
Training, 37, 381–385.
Konradsen, L., & Ravn, J. (1990). Ankle instability caused by
prolonged peroneal reaction time. Acta Orthopaedica Scandinavica,
61, 388–390.
Leanderson, J., Ekstam, S., & Salomonsson, C. (1996). Taping of the
ankle—the effect on postural sway during perturbation before and
after a training session. Knee Surgery, Sports Traumatology,
Arthroscopy, 4, 53–56.
Lentell, G., Baas, B., Lopez, D., McGuire, L., Sarrels, M., &
Snyder, P. (1995). The contributions of proprioceptive deficits,
muscle function, and anatomic laxity to functional instability of the
ankle. Journal of Orthopaedic and Sports Physical Therapy, 21,
206–215.
Liu, Y., Jeng, S., & Lee, A. J. Y. (2005). The influence of ankle
sprains on proprioception. Journal of Exercise Science and Fitness,
3, 33–38.
Lofvenberg, R., Karrholm, J., Sundelin, G., & Ahlgren, O. (1995).
Prolonged reaction time in patients with chronic lateral
instability of the ankle. American Journal of Sports Medicine, 23,
414–417.
Matsusaka, N., Yokoyama, S., Tsurusaki, T., Inokuchi, S., & Okita,
M. (2001). Effect of ankle disk training combined with tactile
stimulation to the leg and foot on functional instability of the
ankle. American Journal of Sports Medicine, 29, 25–30.
Mattacola, C. G., & Dwyer, M. K. (2002). Rehabilitation of the ankle
after acute sprain or chronic instability. Journal of Athletic
Training, 37, 413–429.
Nakagawa, L., & Hoffman, M. (2004). Performance in static, dynamic,
and clinical tests of postural control in individuals with recurrent
ankle sprains. Journal of Sport Rehabilitation, 13, 255–268.
Osborne, M. D., Chou, L., Laskowski, E. R., Smith, J., & Kaufman,
K. R. (2001). The effect of ankle disk training on muscle reaction
time in subjects with a history of ankle sprain. American Journal of
Sports Medicine, 29, 627–632.
Pintsaar, A., Brynhildsen, J., & Tropp, H. (1996). Postural corrections
after standardised perturbations of single limb stance: Effect of
training and orthotic devices in patients with ankle instability.
British Journal of Sports Medicine, 30, 151–155.
Powers, M. E., Buckley, B. D., Kaminski, T., Hubbard, T. J.,
& Ortiz, C. (2004). Six weeks of strength and proprioception
training does not affect muscle fatigue and static balance in
functional ankle instability. Journal of Sport Rehabilitation, 13,
201–227.
Refshauge, K. M., Kilbreath, S. L., & Raymond, J. (2000). The effect
of recurrent ankle inversion sprain and taping on proprioception
at the ankle. Medicine and Science in Sports and Exercise, 32, 10–
15.
Refshauge, K. M., Kilbreath, S. L., & Raymond, J. (2003). Deficits in
detection of inversion and eversion movements among subjects
with recurrent ankle sprains. Journal of Orthopaedic and Sports
Physical Therapy, 33, 166–173.
Riemann, B. L., & Lephart, S. M. (2002). The sensorimotor system,
part I: The physiologic basis of functional joint stability. Journal of
Athletic Training, 37, 71–79.
Rozzi, S. L., Lephart, S. M., Sterner, R., & Kuligowski, L.
(1999). Balance training for persons with functionally unstable
ankles. Journal of Orthopaedic and Sports Physical Therapy, 29,
478–486.
Schulz, K. F., Chalmers, I., Hayes, R. J., & Altman, D. (1995).
Empirical evidence of bias. Journal of the American Medical
Association, 273, 408–412.
SIGN (Scottish Intercollegiate Guidelines Network). (2006). Metho-
dology checklist. Available: /http://www.sign.ac.uk/methodology/
checklists.htmlS; accessed 05.01.07.

ARTICLE IN PRESST. Hughes, P. Rochester / Physical Therapy in Sport 9 (2008) 136–147 147
Tropp, H., Odenrick, P., & Gillquist, J. (1985). Stabilometry
recordings in functional and mechanical instability of the ankle
joint. International Journal of Sports Medicine, 6, 180–182.
Vaes, P., Van Gheluwe, B., & Duquet, W. (2001). Control of acceleration
during sudden ankle supination in people with unstable ankles.
Journal of Orthopaedic and Sports Physical Therapy, 31, 741–752.
Wilkerson, G. B. (2002). Biomechanical and neuromuscular effects
of ankle taping and bracing. Journal of Athletic Training, 37,
436–445.
Wilkerson, G. B., & Nitz, A. J. (1994). Dynamic ankle stability:
Mechanical and neuromuscular interrelationships. Journal of Sport
Rehabilitation, 3, 43–57.