Embed Size (px)
Citation preview

RESEARCH PAPER
The effects of neuromuscular electrical stimulation on clinicalimprovement in hemiplegic lower extremity rehabilitation in chronicstroke: A single-blind, randomised, controlled trial
NILGUN MESCI1, FERDA OZDEMIR2, DERYA DEMIRBAG KABAYEL2 &
BURCU TOKUC3
1PM&R Department, Van Ercis State Hospital, Van, Turkey, 2Physical Medicine and Rehabilitation Department, Trakya
University School of Medicine, Edirne, Turkey, and 3Department of Public Health, Trakya University School of Medicine,
Edirne, Turkey
Accepted March 2009
AbstractObjective. In this study, the effectiveness of neuromuscular electrical stimulation (NMES) was evaluated in lower extremityrehabilitation in patients with chronic stroke.Method. The study enrolled 40 patients with chronic stroke. Twenty patients each were assigned to the treatment group andthe control group. All patients received a conventional rehabilitation program for a 4-week period. In addition to thisrehabilitation program, patients in the treatment group received NMES treatment for hemiplegic foot dorsiflexor muscles for4 weeks, 5 days a week. The sessions were performed as one session per day and added to a total of 20 sessions. Clinicalparameters were evaluated before and after the treatment.Results. Pre-treatment and post-treatment evaluations showed a significant increase in ankle dorsiflexion and a significantdecrease in the level of spasticity in the treatment group (p5 0.05); however, there were no significant differences in thecontrol group between the pre-treatment and post-treatment measures. Although Brunnstrom Stage, Rivermead leg andtrunk score and Functional Independence Measurement motor subscore showed a significant improvement in pre- and post-treatment comparisons for both groups, the treatment group’s scores were significantly higher than the control group(p5 0.05). Functional Ambulation Categories showed a significant improvement in both groups following the treatment;however, there was no significant difference between the two groups (p4 0.05).Conclusions. Use of NMES in hemiplegic foot dorsiflexion can contribute to the clinical improvement of patients when usedin combination with rehabilitation programs.
Keywords: Neuromuscular, electrical stimulation, stroke
Introduction
Hemiplegia due to stroke accounts for the majority of
admissions to the rehabilitation clinics. The main
goal of hemiplegic rehabilitation is to help patients
gain functional independence. The most important
problem hindering functional independence is ex-
periencing difficulties in walking. Although most of
the patients are ambulatory following rehabilitation,
they are generally discharged with permanent im-
pairment in their gait patterns. Therefore, evaluation
and treatment of the walking disorders constitute one
of the most frequent problems that rehabilitation
clinics encounter [1,2].
The characteristic walking pattern in hemiplegia is
slow, spastic, low in coordination and asymmetrical.
The main goal of walking rehabilitation in patients
with hemiplegia is to develop symmetry and increase
the speed [3]. To achieve this goal, additional
methods such as orthosis, bio-feedback techniques
and electrical stimulation are used along with the
conventional exercise programs and neurophysiolo-
gical treatment methods including Brunnstrom,
Correspondence: Ferda Ozdemir, Physical Medicine and Rehabilitation Department, Trakya University School of Medicine, Edirne, Turkey.
E-mail: [email protected]
Disability and Rehabilitation, 2009; 31(24): 2047–2054
ISSN 0963-8288 print/ISSN 1464-5165 online ª 2009 Informa UK Ltd.
DOI: 10.3109/09638280902893626
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Gaz
i Uni
v. o
n 08
/14/
14Fo
r pe
rson
al u
se o
nly.

Bobath and proprioseptive neuromuscular facilita-
tion [3–5].
Patients with hemiplegia experience the drop foot
due to the spasticity of the gastrocnemius muscle or
the paralysis of the dorsiflexor muscles. The initial
contact with the ground is usually with the front part
of the foot and the lateral side. During the swing
phase of walking, the ankle dorsiflexion and eversion
is insufficient. Drop foot can be prevented by
obtaining a tetanic contraction through the use of
electrical stimulation of the dorsiflexor muscles of
foot. It is possible to use neuromuscular electrical
stimulation (NMES) for this purpose [4,6].
The working principle of NMES relies on forma-
tion of contraction through the electrical stimulation
of the nerve fibers innervating the healthy muscle or
the muscle fibers in the denervated muscles. Various
histochemical, enzymatic, metabolic and membrane
changes occur in the healthy skeletal muscles
because of prolonged increased activity [7]. There
are many studies showing the efficacy of NMES in
strengthening the atrophied muscles and in improv-
ing hemiplegic shoulder subluxation and hemiplegic
upper and lower extremity rehabilitation [8,9].
The goal of strengthening dorsiflexion of the foot
is to provide a well-integrated walking pattern and
improvement of the functional ambulation, hence
providing the patient with an increased indepen-
dence level in daily life activities.
Despite the use of NMES in a wide range of
medical fields and apprehension of its effects on
tissues for long years, there is no sufficient evidence
to suggest a benefit for especially patients with
chronic stroke. In an era in which evidence-based
medicine is given much increased importance and
evidence is sought in taking decisions for reimburse-
ment of treatment costs by health insurance bodies,
the value of randomised-controlled trials (RCTs) is
more and more increasing.
The main purpose of this study is to evaluate the
effects of NMES on clinical improvement of hemi-
plegic lower extremity rehabilitation in chronic
stroke.
Material and methods
Patient selection
Forty patients with hemiplegia receiving an inpatient
treatment were enrolled in this study. The patients
were randomly assigned into two groups. Randomi-
sation was performed using ‘n, nþ 1’ method.
Twenty patients were assigned to the treatment
group and 20 patients to the control group.
Inclusion criteria are as follows: (1) clinical picture
of hemiplegia or hemiparesis due to a stroke
experienced for the first time, (2) at least 3-month
elapsed after the incident, (3) psycho-social suit-
ability, (4) age between 45 and 80 years, (5) the
mobility of the ankle to permit at least a neutral
position, (6) spasticity value of lower than 4 on the
Modified Ashworth Scale (MAS) and (7) normal
deep sensation.
Exclusion criteria are as follows: all patients with
stroke not meeting the inclusion criteria have been
excluded from the study. Furthermore, we excluded
patients with (1) other disorders of central nervous
system, including vascular malformations, tumors,
multiple sclerosis, infectious diseases of central
nervous system and previous head injury, (2) any
additional medical or psychological condition that
would affect patient’s ability to comply with study
protocol, (3) previous treatment with functional
electrical stimulation (FES) or NMES (4) fixed
ankle or foot contracture, (5) ataxia, disthonia,
dyskinesia and accompanying lower motor neuron
or peripheral neural lesions, (6) a serious cardiac
disease (aorta stenosis, angina, hypertropic cardio-
myopathy, arrhythmia and pacemakers) and (7) skin
and peripheral circulation disorders.
Clinical evaluations
In addition to the demographic characteristics of the
patients, the dominant hand, duration of the disease,
etiological causes and side of hemiplegia were
recorded.
All patients went through a comprehensive clinical
evaluation before and after the treatment. Clinical
evaluations were always performed by the same
investigator and she was blinded to the treatment
that the patients were receiving. The parameters of
this evaluation were as follows:
1. Ankle passive dorsiflexion range of motion
(ROM) was measured goniometrically.
2. Spasticity was measured and recorded using
the MAS, on a scale of 0–4 [10].
3. Neurophysiological improvement in the lower
extremities was graded on a scale of 1–6
according to the Brunnstrom Stage (BS) [11].
4. Function level for daily life activities were
evaluated by the Functional Independence
Measurement (FIM) [12]. Self-care, sphincter
control, transfers and locomotion scores were
added to calculate the FIM motor subscore.
5. Motor functions were evaluated using the
Rivermead Motor Assessment Scale’s two
subscales: 1, general functions were evaluated
using ‘the gross function’ subscale; and 2, leg
and trunk functions were evaluated using the
‘leg and trunk functions’ subscale. If the
2048 N. Mesci et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Gaz
i Uni
v. o
n 08
/14/
14Fo
r pe
rson
al u
se o
nly.

patient completed the activity fully, a score of
1 was assigned, otherwise a score of 0 was
assigned. The maximum score on the test was
23; 13 for the gross function and 10 for the leg
and trunk functions [13,14].
6. Ambulation categories were graded on a scale
of 0–5 using the Functional Ambulation
Categories (FAC) [14].
Treatment modalities
All patients (n¼ 40) were given an inpatient treat-
ment for 4 weeks. Both the treatment group and the
control group were given a conventional exercise
program, and the treatment group received an
additional NMES applied on the foot dorsiflexors.
Exercise program. All patients were enrolled in a
rehabilitation program at the time of their admission
to the hospital to enhance their motor, sensational
and functional improvement. The standard treat-
ment was the traditional treatment exercise program.
This program included the appropriate positioning
of the extremities, range of motion exercises, active
assistive exercises, progressive resistive exercises,
endurance training, standing up and balance train-
ing. In addition to these, self-care skills, mobility
proficiency and basic and advanced daily life
activities were targeted for achieving improvement
throughout the rehabilitation period.
NMES application. Patients in the treatment group
received NMES treatment for hemiplegic foot
dorsiflexor muscles for 4 weeks, 5 days a week as
one session per day for a total of 20 sessions. In this
study, the device used for neuromuscular stimulation
was the Compex II (produced by Compex SA in
Switzerland). This is a type of EMG-triggered
electrical stimulation device. The stimulation pro-
grams to be applied were pre-loaded on cards with
specified durations and modulations. In this study,
we used the hemipligia-spasticity card.
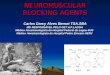
During the application, the patients were in-
structed to remain in sitting position and to keep
their soles of their feet in contact with the floor. The
positive active electrode (the small electrode) was
positioned right below the fibular head where the
peroneal nerve is going through; and the negative
electrode (medium sized electrode) was positioned
on the midpoint of the tibialis anterior muscle on the
front side of the leg. Surface electrode was used for
application. To increase the conductivity of the
electrodes and to relieve the burning sensation of
the patients, a non-allergic water-based gel was used
on the side of the electrodes contacting with the skin.
Electrodes were stabilised on the spots at specific
positions on the leg, using the original velcro tissue
bandages of the device.
The stimulation program used was the first
section of the hemiplegia-spasticity card, which is
set specifically for hemiplegic foot dorsiflexor
muscles. The characteristic of the current in this
section was a symmetrical biphasic wave of 50 Hz
frequency, 400 msn width. The duration of the
treatment was 20 min. In this program a triggering
device was used. It was mounted on the apparatus
in the nest cut out specifically for this purpose.
When the first section of the card was chosen and
the start button was pressed, a clasp sign appeared
on the monitor for the triggering device. Once it
was pressed, the current flow and contraction stage
were set up. For every contraction, the trigger
button needed to be pressed, otherwise the counter
indicating the duration of the treatment did not
proceed. At the same time the triggering button
improved the participation of the patients in the
treatment (Figure 1).
Current density and electrode positions were set
separately for every session so that first the toes and
then the ankle dorsiflexors would be fully contracted
and that there would be no discomfort or pain. When
the contractions decreased, the current was in-
creased to keep the level of contractions at the same
level; however, the contractions were never high
enough to cause contractions on muscles other than
the targeted ones. Special consideration was given to
have the toes and ankle moving on a middle line
instead of a medial or lateral line.
Statistical analysis
The analysis were conducted using the S0064
MINITAB Release 13 (Licence No: WCP
1331.00197) software.
Figure 1. NMES application on the foot dorsiflexor muscles of
hemiplegic patient.
Electrical stimulation in chronic stroke 2049
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Gaz
i Uni
v. o
n 08
/14/
14Fo
r pe
rson
al u
se o
nly.

The differences between the pre-treatment and
post-treatment measures of patients were compared
both between the two groups and within the groups.
In addition, a D score was obtained by measuring the
change in every evaluation parameter’s observed
difference between pre-treatment and post-treatment
values (D, post-treatment clinical score minus pre-
treatment clinical score) and these scores were
compared between the treatment and control groups.
The categorical data was compared between the
two groups using chi-square test. For the differences
between the two groups Mann–Whitney U test was
used. The pre-treatment and post-treatment mea-
sures were compared using a dependent-samples
Wilcoxon Signed Rank test. Obtained values were
reported as mean+ standard deviation values and a
p value of 5 0.05 was considered statistically
significant.
The study has been approved by the local ethics
committee of our University. All patients in the study
have given their informed consent.
Results
This study enrolled 20 patients in the treatment
group, who received an NMES treatment in the
hemiplegic foot dorsiflexors; and 20 patients in the
control group. There were no significant differences
between the two groups in age, gender, body mass
index (BMI), duration of disorder measured as the
time elapsed because of the cerebral vascular
incident, side of hemiplegia and etiological distribu-
tion (p4 0.05). The ages of the patient ranged
between 47 and 76 years (60.87+ 8.16). Twenty-
three of the patients were male and 17 were female.
Treatment group comprised of 12 (60%) male
patients and 8 (40%) female patients, and the control
group comprised of 11 (55%) female and 9 (45%)
male patients. The demographic characteristics of
the patients are shown in Table I.
All patients were right-hand dominant. The
hemiplegic part distribution was exactly the same
for both groups. In both groups, there were 9 right
(45%) and 11 left (55%) hemiplegic patients. The
etiological distribution for the treatment group was
as follows: 8 (%40) atherothrombotic, 8 (40%)
embolic and 4 (20%) haemorrhagic type patients.
The control group’s etiological distribution was as
follows: 9 (45%) atherothrombotic, 5 (25%) em-
bolic, 2 (10%) lacunar ve and 4 (20%) haemorrhagic
type patients (Table I).
An intergroup comparison was conducted on the
pre-treatment values of clinical evaluation para-
meters. There was a statistically significant difference
between the two groups in ankle dorsiflexion ROM
degree and MAS (p5 0.05), however, no significant
differences were observed in lower extremity BS,
FIM, FAC and Rivermead motor scales (p4 0.05)
(Table II).
When an intergroup comparison was conducted
for the post-treatment clinical evaluation parameters,
no significant differences were observed (p4 0.05)
(Table II).
An intragroup comparison between the pre-treat-
ment and post-treatment evaluations was also con-
ducted. It was observed that there was a significant
improvement in the ankle dorsiflexion ROM degree
and a significant decrease in the MAS in the
treatment group; however, there were no significant
differences in the control group on these measures
(p4 0.05). Both groups showed a significant change
in lower extremity BS, FIM, FAC and Rivermead
motor scores when the pre-treatment and post-
treatment values were compared (p5 0.05)
(Table II).
The pre-treatment and post-treatment measures
were compared on an intergroup level to see if any
differences existed. For this purpose, the delta values
(the difference between the post- and pre-treatment
measures; post-treatment values minus pre-treat-
ment values¼D) were calculated. This delta value
was compared between the treatment and the control
groups, allowing a comparison of the degree of
improvement. The results showed that the improve-
ment in the ankle dorsiflexion ROM (p¼ 0.000),
Table I. Demographic information and the characteristics of the disorders of the participants.
Group 1 (n¼ 20) Group 2 (n¼20) p
Age (mean+SD) 62.65+ 7.52 59.10+8.58 0.172
BMI (mean+SD) (kg/m2) 25.81+ 3.54 25.55+3.84 0.821
Sex 12 men, 8 women 11 men, 9 women 0.749
Duration of the disease
(month) (mean+SD)
9.45+ 4.80 7.30+4.42 0.149
Side of hemiplegia 9 right, 11 left 9 right, 11 left 1.000
Etiological causes of stroke 8 Atherothrombotic,
8 embolic, 4 haemorrhagic
9 Atherothrombotic, 5 embolic,
4 haemorrhagic, 2 lacunar
0.432
SD, standard deviation, BMI, body mass index.
2050 N. Mesci et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Gaz
i Uni
v. o
n 08
/14/
14Fo
r pe
rson
al u
se o
nly.

decrease in the MAS (p¼ 0.000), increase in the
lower extremity BS (p¼ 0.005), improvement in the
Rivermead leg and trunk scores (p¼ 0.004) and
improvement in the FIM motor subscore (p¼ 0.018)
were greater in the treatment group than the control
group (Table II).
Discussion
In this study, we investigated whether NMES
applications on ankle dorsiflexor muscles have a role
in the improvement of hemiplegic gait patterns and
functional independence.
Following a cerebral vascular incident, neurologi-
cal and functional healing is the fastest in the first 3–6
months and then continues with a slower speed
[15,16]. In this study, patients with a disorder
duration of less than 3 months were excluded to be
able to exclude the effects of spontaneous recovery.
The disorder duration is consistent with the relevant
literature [17,18].
Studies conducted so far vary in the wave forms of
the electrical stimulation and the width and fre-
quency of the current applied. Although there is no
consensus on the ideal waveform for NMES, some
studies argue that symmetrical biphasic waveform is
easier to apply than asymmetrical biphasic and
monophasic waveforms [19]. Many studies in the
literature used symmetrical biphasic waveforms for
electrical stimulation and reported significant gains
in treatment outcomes [17,20–22]. Laufer et al. [20]
suggested that biphasic waveforms were better than
monophasic rectangular and poliphasic sinusoidal
waveforms. This study, too, used symmetrical
biphasic waveforms.
In general stimulation, a frequency of 30–50 Hz
and duration of 1–400 msn are sufficient for generat-
ing muscle contraction [7,19]. Many studies used
similar frequency and duration were reported sig-
nificant decrease in spasticity, increase in ROM and
improvement in walking functions [17,18,23]. This
study employed a stimulation of 50 Hz frequency
and 400 msn stimulus duration and had similar
findings.
The basic concern for choosing electrodes in
NMES applications is the purpose of the application
of the program and convenience for the patients. The
surface electrodes are the most widely used electro-
des for therapeutic and functional applications
because of ease of use [7,18,24]. This study
employed surface electrodes. None of the patients
in the study showed any skin reactions.
There is a variety of duration of NMES applica-
tions in the literature. Kimberly et al. [9] conducted
a study investigating the efficacy of the use of
intensive electrical stimulation at home settings, in
Tab
leII
.C
om
par
iso
no
fp
re-t
reat
men
tan
dp
ost
-tre
atm
ent
valu
eso
fcl
inic
alp
aram
eter
s.
Intr
agro
up
com
par
iso
nG
rou
p1
(n¼
20
)
Intr
agro
up
com
par
iso
nG
rou
p2
(n¼
20
)
Inte
rgro
up
com
par
iso
n
Gro
up
1–
Gro
up
2D
sco
res*
Par
amet
ers
Pre
-tre
at.
mea
n+
SD
Post
-tre
at.
mea
n+
SD
p
Pre
-tre
at.
mea
n+
SD
Post
-tre
at.
mea
n+
SD
pP
re-t
reat
.P
ost
-tre
at.
Gro
up
1G
rou
p2
p
An
kle
pas
sive
do
rsifl
exio
nR
OM
14
.50+
4.8
20.7
5+
6.1
0.0
00
20
.00+
5.6
21
.00+
4.7
0.1
02
0.0
04
0.9
68
6.2
5+
3.6
1.0
0+
2.6
0.0
00
MA
S2
.10+
0.7
0.9
0+
0.9
0.0
00
1.3
0+
1.0
1.1
5+
0.8
0.2
57
0.0
14
0.3
41
71.2
0+
0.5
70
.15+
0.6
0.0
00
Lo
wer
extr
emit
yB
S2
.85+
0.5
3.6
5+
0.5
0.0
00
3.2
0+
0.7
3.4
5+
0.6
0.0
25
0.1
21
0.3
69
0.8
0+
0.5
0.2
5+
0.4
0.0
05
FIM
mo
tor
sub
score
53
.65+
15
.76
0.0
5+
13
.90
.000
53
.95+
13
.95
7.2
5+
14
.30
.00
50
.82
00
.77
96.4
0+
5.4
3.3
0+
4.3
0.0
18
FIM
cogn
itiv
esu
bsc
ore
24
.30+
6.2
24.4
5+
6.1
0.1
80
24
.55+
4.8
24
.55+
4.8
1.0
00
0.7
79
0.6
78
0.1
5+
0.5
0.0
0+
0.0
0.6
02
To
tal
FIM
sco
re7
8.0
0+
18
.38
4.5
0+
16
.70
.000
78
.50+
15
.18
1.8
0+
15
.70
.00
50
.75
80
.79
96.5
0+
5.7
3.3
0+
4.3
0.0
18
FA
C2
.05+
1.2
2.7
5+
1.0
0.0
00
1.9
5+
1.2
2.4
5+
1.3
0.0
04
0.7
38
0.4
61
0.7
0+
0.6
0.5
0+
0.6
0.3
14
Riv
erm
ead
gro
ssfu
nct
ion
5.0
5+
3.5
6.0
0+
3.2
0.0
10
5.3
5+
3.5
6.5
0+
3.2
0.0
02
0.7
58
0.6
20
0.9
5+
1.7
1.1
5+
1.3
0.3
69
Riv
erm
ead
leg
and
tru
nk
fun
ctio
ns
5.2
0+
1.9
7.2
0+
1.8
0.0
00
5.8
0+
2.7
6.7
0+
2.7
0.0
03
0.3
69
0.7
79
2.0
0+
1.3
0.9
0+
1.0
0.0
04
To
tal
Riv
erm
ead
mo
tor
asse
ssm
ent
sco
re1
0.2
5+
5.3
13.2
0+
4.9
0.0
00
11
.15+
6.0
13
.20+
5.8
0.0
01
0.6
20
0.9
04
2.9
5+
2.7
2.0
5+
2.1
0.1
75
RO
M,
ran
ge
of
mo
tio
n;
MA
S,
mo
difi
edA
shw
ort
hsc
ale;
BS
,B
run
nst
rom
stag
e;F
IM,
fun
ctio
nal
ind
epen
den
cem
easu
rem
ent;
FA
C,
fun
ctio
nal
amb
ula
tio
nca
tego
ries
.
*D
sco
res¼
po
st-t
reat
men
tcl
inic
alsc
ore
s–
pre
-tre
atm
ent
clin
ical
sco
res.
Electrical stimulation in chronic stroke 2051
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Gaz
i Uni
v. o
n 08
/14/
14Fo
r pe
rson
al u
se o
nly.

patients with chronic strokes. The application
included a 3–6 h frequency everyday or every 2 days
for 3 weeks, summing to a total of 60 h. The findings
suggested that NMES may increase the functional
and motor development through cortical change.
Berner et al. [8] conducted a 4-week study in
patients with acute stroke. They used a treatment
protocol consisting of two sessions per day, gradually
increasing from 10 to 60 min over 3 weeks of time;
and at the end of the treatment they found a
significant change in the FIM and ROM values
when they compared the treatment and control
groups. The duration of that study is longer than
this study. Similarly conducted studies yielded
similar findings with our study [17,23].
Long-term electrical stimulation programs (4–6 h/
day) increase the muscle strength through muscle
fiber hypertrophy in patients with central nervous
system lesions. However, this kind of aggressive
stimulation programs are not possible to apply in
clinical settings [25]. On the contrary, in patients
with stroke, stimulation programs with shorter
duration show a better impact in motor healing
[17,23,26]. In this study, the NMES program was
applied for 4 weeks, 5 days a week as one session per
day, and approximately 20 min per session. By this
way, despite short duration of the application, the
treatment group had a significantly better improve-
ment than the control group in lower extremity BS,
Rivermead leg and trunk score, FIM motor sub-
score, ankle ROM degrees and MAS.
In general, NMES is considered to have therapeu-
tic applications, such as increasing ROM, facilitation
of muscle activation and muscle strengthening. In
FES, which is one of the application modes of
NMES, the main goal is functional improvement,
and stimulation is targeted at the function that needs
to be improved [19]. The present application was not
FES, thus the patient was in a stable sitting position
and not walking. Despite this, our findings showed
functional improvement. We believe that this may be
due to the decrease in the spasticity in the lower
extremity, increase in ROM, as well as the positive
feedback effect of the patients’ active participation in
the treatment procedure. There are studies showing
that NMES may have an impact on neuronal
plasticity and cortical activity depending on the
duration of application and intensity [9,27]. How-
ever, we could not perform functional MRI, for this
reason we could had opportunity to associate our
findings with cortical plasticity.
The findings of this study showed that both the
NMES group and the control group had a significant
improvement in most of the clinical parameters. This
finding may be due to the fact that patients in both
the treatment and the control groups were hospita-
lised rehabilitation patients throughout the study.
Ozdemir et al. [28] showed that inpatient rehabilita-
tion programs yielded better impact on clinical
improvement when compared to home-based reha-
bilitation programs.
In this study, we have found a significant
difference in the ankle dorsiflexion ROM and MAS
scores in pre-treatment measures of the two groups.
The gastrocnemius muscle spasticity of the patients
in the treatment group was more intense and the
ankle dorsiflexion ROM was more limited. However,
in the post-treatment measures, there were no
significant differences between the two groups on
these two parameters. This improvement in the
NMES group was more significant than the control
group. Similar studies using an electrical stimulation
on hemiplegic lower extremity show a decrease in the
ankle MAS level and an increase in ROM measures
[17,23,26,29]. Through electrical stimulation the
antagonist of the spastic muscle is strengthened, and
the treatment effect occurs through the inhibitor
effect on the spastic agonist muscles and a decrease
in the spasticity.
The findings of this study showed a more
significant improvement in the treatment group
compared to the control group in lower extremity
BS, Rivermead leg and trunk score and FIM motor
subscores. Therefore, it is possible to conclude that
NMES treatment on hemiplegic foot dorsiflexor
muscles increases the healing of lower extremity
motor and functional mobility. FAS showed a
significant difference between both groups in pre-
and post-treatment comparisons; however, the dif-
ference between the two groups was not significant.
Our control group patients received only exercise
program. NMES treatment relies on patient’s
experiencing some sensations and generation of
motion. At this end, it differs from other modalities
such as therapeutic laser, therapeutic ultrason or
magnetotherapy where patients experience no sensa-
tion at all. Thus, we did not apply NMES to the
control group. Application of electrical stimulation in
another form might produce some physiological
effects in tissues even if it does not generate motion.
That is why we did not apply an alternative electrical
stimulation forms.
The major aspect of our study is its RCT design.
Our sample size and the number of patients
completing the study confer advantages compared
to other similar studies in this field. Barth et al. [30]
investigated the impact of a low-dose (20 min/day, 4
weeks) surface electromyography-triggered neuro-
muscular stimulation (ETMS) regimen on affected
ankle movement, balance and ambulation in a
patient with chronic stroke with no active, affected
ankle movement. After intervention, the subject
showed 25 degrees of active ankle flexion and 17
degrees of active ankle extension. Functionally, this
2052 N. Mesci et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Gaz
i Uni
v. o
n 08
/14/
14Fo
r pe
rson
al u
se o
nly.

patient was reported to acquire a safer and more
rapid walking and improved transfers.
In general, there are a few RCTs in the literature
investigating the efficacy of physical therapy mod-
alities in patients with stroke. Also, RCTs evaluating
the efficacy of NMES in both upper and lower
extremities in patients with chronic stroke are scarce.
Moreover, sample size is quite small in several
RCTs. These limitations were mentioned in many
reviews [31]. Meanwhile, it is known that although
the potential for improvement of stroke in acute and
subacute phases and contribution of treatments to
improvement are substantial, chances for beneficial
effects of treatments during chronic phase are lower.
In that respect, it is important to demonstrate the
efficacy of any treatment method in patients with
chronic stroke. In this study, we showed that NMES
could provide changes in some clinical parameters in
chronic stroke.
In conclusion, we believe that use of NMES
treatment in the rehabilitation of hemiplegic lower
extremity decreases gastrocnemius muscle spasticity,
improves ankle dorsiflexion limitations, helping to
achieve a normal gait pattern and faster motor and
functional healing. Furthermore, we suggest that
NMES should be used in combination with, and as
an aid to basic rehabilitation programs and other
techniques. We believe that our study has contrib-
uted to demonstrating the efficacy of NMES in
patients with stroke in chronic period.
Declaration of interest: The authors report no
conflicts of interest. The authors alone are respon-
sible for the content and writing of the paper.
References
1. Kuan TS, Tsou JY, Su FC. Hemiplegic gait of stroke patients:
the effect of using a cane. Arch Phys Med Rehabil
1999;80:777–784.
2. Turnbull GI, Charteris J, Wall JC. Deficiencies in standing
weight shifts by ambulant hemiplegic subjects. Arch Phys Med
Rehabil 1996;77:356–362.
3. Ryerson SD. Hemiplegia. In: Umphred DA, editor. Neuro-
logical Rehabilitation. 3rd ed. St. Louis: Mosby-Year Book;
1995. pp 681–721.
4. Mauritz KH. Gait training in hemiparetic stroke patients.
Eura Medicophys 2004;40:165–178.
5. Hummelsheim H, Mauritz KH. The neurophysiological basis
of exercise physical therapy in patients with central hemipar-
esis. Fortschr Neurol Psychiatr 1993;61:208–216.
6. O’Sullivan SB. Stroke. In: O’Sullivan SB, Schmitz TJ, editors.
Physical rehabilitation assessment and treatment. 4th ed.
Philadelphia: F.A. Davis Co; 2001. pp 519–581.
7. Mysiw WJ, Jackson RD. Electrical stimulation. In: Braddom
RL, editor. Physical medicine and rehabilitation. 2nd ed.
Philadelphia: Saunders Co; 2000. pp 459–487.
8. Berner YN, Lif Kimchi O, Spokoiny V, Finkeltov B. The
effect of electric stimulation treatment on the functional
rehabilitation of acute geriatric patients with stroke – a
preliminary study. Arch Gerontol Geriatr 2004;39:125–132.
9. Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey LL, Lojovich
JM, Carey JR. Electrical stimulation driving functional
improvements and cortical changes in subjects with stroke.
Exp Brain Res 2004;154:450–460.
10. Pandyan AD, Price CI, Rodgers H, Barnes MP, Johnson GR.
Biomechanical examination of a commonly used measure of
spasticity. Clin Biomech (Bristol, Avon) 2001;16:859–865.
11. Brandstater ME. Stroke rehabilitation. In: DeLisa JA, editor.
Physical medicine & rehabilitation. Principles and practice.
4th ed. Philadelphia: Lippincott Williams&Wilkins; 2005. pp
1655–1676.
12. Christiansen CH. Functional evaluation and management of
self-care other activities of daily living. In: DeLisa JA, editor.
Physical medicine & rehabilitation. Principles and practice.
4th ed. Philadelphia: Lippincott Williams&Wilkins; 2005. pp
975–1003.
13. Wade DT. Measurement in neurological rehabilitation. 1st
ed. Oxford: Oxford University Press; 1992. pp 70–284.
14. Collen FM, Wade DT, Bradshaw CM. Mobility after stroke:
reliability of measures of impairment and disability. Int
Disabil Stud 1990;12:6–9.
15. Roth EJ, Harvey RL. Rehabilitation of stroke syndromes. In:
Braddom RL, editor. Physical medicine & rehabilitation. 2nd ed.
Philadelphia: W.B. Saunders Company; 2000. pp 1117–1160.
16. Jorgensen HS, Sperling B, Nakayama H, Raaschou HO,
Olsen TS. Spontaneous reperfusion of cerebral infarcts in
patients with acute stroke. Incidence, time course, and clinical
outcome in the Copenhagen Stroke Study. Arch Neurol
1994;51:865–873.
17. Chen SC, Chen YL, Chen CJ, Lai CH, Chiang WH, Chen
WL. Effects of surface electrical stimulation on the muscle-
tendon junction of spastic gastrocnemius in stroke patients.
Disabil Rehabil 2005;27:105–110.
18. Burridge JH, McLellan DL. Relation between abnormal
patterns of muscle activation and response to common
peroneal nerve stimulation in hemiplegia. J Neurol Neurosurg
Psychiatry 2000;69:353–361.
19. McCulloch KL, Nelson CM. Electrical stimulation and
electromyographic biofeedback. In: Umphred DA, editor.
Neurological rehabilitation. 3rd ed. St. Louis: Mosby-Year
Book; 1995. pp 852–871.
20. Laufer Y, Ries JD, Leininger PM, Alon G. Quadriceps
femoris muscle torques and fatigue generated by neuromus-
cular electrical stimulation with three different waveforms.
Phys Ther 2001;81:1307–1316.
21. Burridge J, Taylor P, Hagan S, Wood D, Swain I. The effect
of common peroneal nerve stimulation on quadriceps
spasticity in hemiplegia. Physiotherapy 1997;83:82–89.
22. Johnson CA, Burridge JH, Strike PW, Wood DE, Swain ID.
The effect of combined use of Botulinum Toxin Type A and
functional electric stimulation in the treatment of spastic drop
foot after stroke: a preliminary investigation. Arch Phys Med
Rehabil 2004;85:902–909.
23. Yan T, Hui-Chan CW, Li LS. Functional electrical stimula-
tion improves motor recovery of the lower extremity and
walking ability of subjects with first acute stroke: a randomized
placebo-controlled trial. Stroke 2005;36:80–85.
24. Veltink PH, Ladouceur M, Sinkjaer T. _Inhibition of the
triceps surae strech reflex by stimulation of the deep peroneal
nerve in persons with spastic stroke. Arch Phys Med Rehabil
2000;81:1016–1024.
25. Newsam CJ, Baker LL. Effect of an electric stimulation
facilitation program on quadriceps motor unit recruitment
after stroke. Arch Phys Med Rehabil 2004;85:2040–2045.
26. Chae J, Fang ZP, Walker M, Pourmehdi S, Knutson J.
Intramuscular electromyographically controlled neuromuscu-
lar electrical stimulation for ankle dorsiflexion recovery in
chronic hemiplegia. Am J Phys Med Rehabil 2001;80:842–847.
Electrical stimulation in chronic stroke 2053
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Gaz
i Uni
v. o
n 08
/14/
14Fo
r pe
rson
al u
se o
nly.

27. Smith GV, Alon G, Roys SR, Gullapalli RP. Functional MRI
determination of a dose-response relationship to lower
extremity neuromuscular electrical stimulation in healthy
subjects. Exp Brain Res 2003;150:33–39.
28. Ozdemir F, Birtane M, Tabatabaei R, Kokino S, Ekuklu G.
Comparing stroke rehabilitation outcomes between acute
inpatient and nonintense home settings. Arch Phys Med
Rehabil 2001;82:1375–1379.
29. Blackburn M, Van Vliet P, Mocket SP. Reliability of
measurements obtained with the modified Ashworth scale in
the lower extremities of people with stroke. Phys Ther
2002;82:25–34.
30. Barth E, Herrman V, Levine P, Dunning K, Page SJ. Low-
dose, EMG-triggered electrical stimulation for balance
and gait in chronic stroke. Top Stroke Rehabil 2008;15:
451–455.
31. Van Peppen RP, Kwakkel G, Wood-Dauphinee S, Hendriks
HJ, Van der Wees PJ, Dekker J. The impact of physical
therapy on functional outcomes after stroke: what’s the
evidence? Clin Rehabil 2004;18:833–862.
2054 N. Mesci et al.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Gaz
i Uni
v. o
n 08
/14/
14Fo
r pe
rson
al u
se o
nly.