Embed Size (px)
Citation preview

The Effects of Music Therapy on Vital Signs, Feeding, andSleep in Premature Infants
WHAT’S KNOWN ON THIS SUBJECT: Recorded music, parentvoices, and sung lullabies have been shown to increase oxygensaturation, nonnutritive sucking, and weight gain in prematureinfants.
WHAT THIS STUDY ADDS: Parent-preferred melodies andentrained live rhythm and breath sounds can enhance quiet alertand sleep states, suck response, and oxygen saturation inpremature infants and significantly reduce fear and anxietyperception in parents.
abstractOBJECTIVES: Recorded music risks overstimulation in NICUs. The liveelements of music such as rhythm, breath, and parent-preferredlullabies may affect physiologic function (eg, heart and respiratoryrates, O2 saturation levels, and activity levels) and developmentalfunction (eg, sleep, feeding behavior, and weight gain) in prematureinfants.
METHODS: A randomized clinical multisite trial of 272 prematureinfants aged $32 weeks with respiratory distress syndrome, clinicalsepsis, and/or SGA (small for gestational age) served as their owncontrols in 11 NICUs. Infants received 3 interventions per week withina 2-week period, when data of physiologic and developmentaldomains were collected before, during, and after the interventionsor no interventions and daily during a 2-week period.
RESULTS: Three live music interventions showed changes in heart rateinteractive with time. Lower heart rates occurred during the lullaby(P , .001) and rhythm intervention (P = .04). Sucking behaviorshowed differences with rhythm sound interventions (P = .03).Entrained breath sounds rendered lower heart rates after the inter-vention (P = .04) and differences in sleep patterns (P , .001). Caloricintake (P = .01) and sucking behavior (P = .02) were higher withparent-preferred lullabies. Music decreased parental stressperception (P , .001).
CONCLUSIONS: The informed, intentional therapeutic use of live soundand parent-preferred lullabies applied by a certified music therapistcan influence cardiac and respiratory function. Entrained witha premature infant’s observed vital signs, sound and lullaby mayimprove feeding behaviors and sucking patterns and may increaseprolonged periods of quiet–alert states. Parent-preferred lullabies,sung live, can enhance bonding, thus decreasing the stress parentsassociate with premature infant care. Pediatrics 2013;131:902–918
AUTHORS: Joanne Loewy, DA, LCAT, MT-BC,a KristenStewart, MA, LCAT, MT-BC, SEP,a Ann-Marie Dassler, RN,MSN, FNP, IBCLC,b Aimee Telsey, MD,b and Peter Homel,PhDc
aThe Louis Armstrong Center for Music & Medicine; bNICU, andcDepartment of Biostatistics, Beth Israel Medical Center, NewYork, New York
KEY WORDSmusic therapy, music medicine, acoustic stimulation, NICU musicinterventions
ABBREVIATIONSCI—95% confidence intervalES—effect sizeHR—heart rateIRB—institutional review boardRR—respiratory rateSGA—small for gestational age
Dr Loewy conceptualized and designed the study, drafted theinitial manuscript, and approved the final manuscript assubmitted; Ms Stewart designed the data collection materialsand trained the multisite researchers, and analyzed the dataand reviewed the final manuscript; Ms Dassler assisted in thestudy design, interpreted the results of the outcomes, andedited the final manuscript; Dr Telsey assisted in the studydesign, implemented methods of data collection andinterpretation, and analyzed the data, writing about theimplications of the findings, and she also edited the finalmanuscript; and Dr Homel provided randomization before datacollection, provided statistical analysis of the outcomes, andedited the final manuscript.
Dr Homel’s current affiliation is Maimonides Medical Center,Brooklyn, New York. Ms Stewart’s current affiliation is VA -Hudson Valley Healthcare System, Castle Point, New York.
This trial has been registered at www.clinicaltrials.gov(identifier NCT0151195).
www.pediatrics.org/cgi/doi/10.1542/peds.2012-1367
doi:10.1542/peds.2012-1367
Accepted for publication Jan 3, 2013
Address correspondence to Joanne Loewy, The Louis ArmstrongCenter for Music and Medicine, Beth Israel Medical Center,6 Silver 21 1st Ave and 16th St, New York, NY 10003. E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: All aspects of this study were supported by theHeather on Earth Music Foundation.
902 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from

Research in NICU practice supports theuse of music in critical areas such assucking,1 weight gain,2 sleep,3 and re-covery from painful procedures.4,5
Parents’ voices have also been shown toenhance vocalization in prematureinfants.6 Endurance of the traumaticeffects of premature birth and sub-sequent NICU admission7,8 expends vitalenergy for the premature infant and cancomplicate or impair development.9–11
An infant’s capacity to recognize his orher mother’s voice indicates that atten-tion to this function may be valuable ifintegrated with NICU care practices.12
Vocal familiarity within the infant’ssound environment may provide an es-sential domain of consistency, security,and comfort that even the most modernNICUs cannot replicate. Studies ofmothers singing select, live, infant-directed lullabies to newborns indicatestabilizing effects.13 Although there isgood evidence that the mother’s voiceand her singing of lullabies have posi-tive outcomes, some studies haveimplemented recordings of Mozart’smusic,14,15 and 1 study hypothesizeda “Mozart effect” as an outcome.11
Several studies have implementedtherapist-selected music15,16 and otherapplications including children’s sing-ing,18 male or female singing,19 and theuse of specific music genres commonto the region of study1,20 with varyingresults. Several studies designed bya physician/musician implemented re-corded womb sounds and interwovenmusic with positive results.21–23 Thespecific elements of replicated livewomb sounds inclusive of the in-dependent variables of rhythm (heartbeat) and timbre (intrauterine fluidsounds) have not been studied. Acollective view of clinical trials withnewborns indicates that music, par-ticularly live singing,24,25 has thera-peutic benefits in comparison withspeaking.26 Although some studieshave examined lullabies,3,18 most of the
aforementioned research is incon-sistent regarding the inclusion ofparents and the use of parent-preferred music,27 which imbues cul-tural practices central to a family’sestablished sense of containment andresiliency.
Early attachment research has com-pared the effects of live versus artificialnurturance in the earliest days of life.28
Infants instinctively entrain to breathingsounds to develop life-sustaining respi-ratory regulation. NICU infant respira-tory regulation, particularly challengeddue to the severe immaturity of pre-term infant lungs, can be further com-plicated by an NICU sound environment,which impedes opportunities for self-regulation. Even though this circum-stance is so prevalent for preterminfants in NICU environments, little re-search has investigated an educativeapproach where parents are instructedand guided to entrain their breathing,and to use audible breath sounds andmusic with their infant’s vital rhythms.Education and execution of entrainedmusic application require an informedspecialist to safeguard and supervisethese specialized interventions thatmust be adapted to follow the frequentchanges of preterm infant heart rate(HR), respiratory rate (RR), and activitylevel. Such attuned music applicationsprovide a potentially therapeutic alter-native to an infant’s tendency to habitu-ate to their environment for survival.29,30
Entrainment (ie, synchronization andcontrol of a physiologic rhythm by anexternal stimulus) involves the appli-cation of livemusic elements catered toan infant’s vital signs that influence thebody’s ability to regulate.31 Recordedmusic differs in its application frommusic therapy in a medical setting,where direct entrainment princi-ples are applied and achieved ex-clusively through the application oflive, moment-by-moment, musical ele-ments. Efficacy of familiarity is ach-
ieved when the music of culture isadministered by the family and is nat-ural to their unique supportive con-text.1,27
Neurobehavioral research reveals thathumans developmore efficiently withina constructive social learning envi-ronment in which nurturance occurs inresponse to a live human rather thana surrogate or machine. Bonding andattachment most effectively developthrough physical contact and early in-volvement between the infant andcaregiver.32 Much research has ad-dressed the sterile, technological, andprocedure-driven environment of theNICU and its adverse effects on parent–infant bonding. While critical topreterm infant survival, the complexrelationships among health care pro-fessionals, parents, infants, and theNICU environment may be acutelyproblematic for the healthy de-velopment of parent–infant bonding.33
Health care providers have paid closeattention to the conditions that in-fluence optimal care for preterminfants. The NICU sound environmentrepresents an increasingly familiararea of concern.34 The abundance ofabrasive acoustic stimuli commonlyidentified with an NICU notably inter-feres with both rest and growth forpreterm infants.35 It is difficult to con-trol volume levels, as well as the pitch,timbre, and unpredictable patterns ofNICU sounds.
Recorded music, while often madeavailable for therapeutic purposes, mayinvolve multiple elements of instru-mentation on a variety of instrumentswhere rhythms, timbres, melodies, andharmonies might overstimulate infants.These conditions contradict the en-closed sound environment of the womb.Neonatesrelyontheorganicstructureofthe rhythms of mother’s heart, herbreath patterns, and overtone vibra-tions of her voice36,37 to support orga-nizational development.
ARTICLE
PEDIATRICS Volume 131, Number 5, May 2013 903
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from

Emphasis on infant–caregiver bondingduring anNICU admission is a significantaspect of family-centered practice.38,39
The impact of potentially long-lastingtraumatization for parents and pre-term infants, however, is often over-looked.40 The carefully applied useof live music by a trained music ther-apist may provide a valuable approachto addressing overwhelming circum-stances and events common to an NICUadmission for both parent and infant.Music therapists may also assist inenhancing family cohesion and bond-ing, which are important aspects ofcare in working toward the critical goalof parental inclusion in the NICU.41 Re-search is needed to address the effectsof applied live music on the course ofpreterm infant growth, with specificattention to rhythm, timbre, and en-trained familiar sounds.
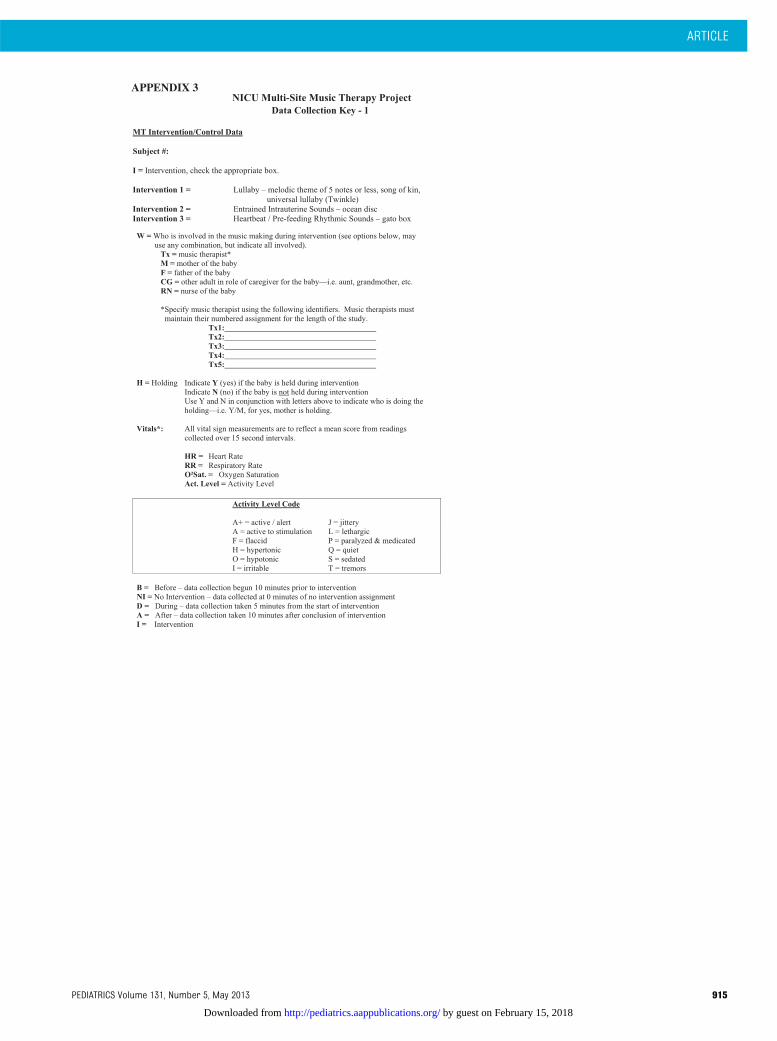
This study is the first to implement livemusical elements provided by a musictherapist that replicate womb sounds.The Remo ocean disc is a musical in-strument that was used to replicate the“whoosh”-like timbre of the placenta. Itis a round disc that encases numeroussmall metal beads. It is played to mirrorthe infant’s breath pattern, which can bemanipulated when entrained to thepeak of an inhalation and the prolongedflow of an exhalation. The gato box isa 2- or 4-tone wooden box that encasestones. The box is played with the fingersto ensure soft control. The rhythm isentrained to the infant’s heartbeat, andthe intervals played are 1, the tonic,and/or the 3rd, as in a minor third. Thesongs implemented in the study wereparent-preferred lullabies or, in thecase where one was not identified,“Twinkle, Twinkle Little Star.”*
Investigation of sound42 and music’spotential to affect a growing infant’swell-being and treatment is necessaryto understand the importance of cul-tural (musical) preferences which be-gin developing in the womb.42
RATIONALE FOR THE APPLICATIONOF LIVE MUSIC INTERVENTIONS
The developing neonate first hears themother’s heartbeat as early as 16weeks.43 There is evidence that beatperception may be an innate charac-teristic in the developing fetus.44 Thetimbre of the intrauterine environmentoccurs for 9 months, and the infantsregulate in accordance with these vitalsounds of the placenta. The element oftimbre, in music, is the quality ofsound, which integrates the physicalcharacteristics that determine per-ception. When this enclosed sound en-vironment is compromised, the infantis deprived of the accustomed nurtur-ing soundscape that was a familiar andacoustically active part of their de-velopmental history. NICU conditionsare not acoustically regulated to pro-vide for an optimal environment.
There is evidence that infants havea natural tendency to entrain to thesounds that surround them.45 Themusictherapist’s attention to sound andmusicplayed within the environment ofa growing infant is instrumental to se-curing conditions that enhance growth.
METHODS
Patients
This study compared infant reaction to 3live music interventions that were ran-domized to be applied in either themorning or afternoon each week, overa 2-week period. Before enrollment, thestudy coordinator recruited certifiedmusic therapists through mid-Atlanticpediatric hospital searches whereestablished music therapy programs inthe NICU were identified or where NICU
physician directors allowed for musictherapy research to take place. Prepa-ration involved the training of 17 certi-fied music therapists and 8 graduateinterns before and during the in-vestigatory period for a period of 2½years to ensure the applications wereoffered in a replicable method. Therewere 7 physicians and numerousnurseswho assisted in the developmentand application of the protocol. The hy-potheses investigated the informed useof live music and elements of appliedsound across multiple domains offunctioning among premature infantswith the following diagnoses: re-spiratory distress syndrome, small forgestational age (SGA), and clinical sep-sis. The SGA infants were in the ,10thpercentile for age. Our intention was toinclude infants who were $32 weeks’premature. These specific diagnoseswere selected on the basis of beingcommon admitting diagnoses to all 11of the hospitals that were included inthe study. We did not exclude infantswho met other criteria or infants withlow Apgar scores. Each infant’s de-velopment involved observation andcollection of data by a blinded datacollector over a variety of physiologicdomains before, during, and after theintervention itself and daily throughoutthe 2-week period of investigation.
Wewereeager totest the influenceof theappliedwomb, heart, andbreathsoundsentrained live to the infant’s vital signsand lullabies specifically identified byparents as important to their culturalheritage. When one could not be iden-tified, we used “Twinkle Twinkle LittleStar”* as the default lullaby. The multi-ple studies in NICU music therapy sug-gesting “therapeutic lullabies” or adefined applied pitch range “higher” or“lower” for singing seem random,46 andinvestigations of the most scientific lit-erature implies by methodologic de-sign that the sounds and music beneither high nor low voices but rather
*“Twinkle” is a melody that is well known toparents of all cultures in the United States and isthe basis for familiar infant folk themes such as“A,B,C” and “Ba Ba Black Sheep.” It is based ona perfect 5th and has a small melodic range andrepetitive patterns, with a simplified structureeasily sung by “nonmusician” adults.
904 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from

suggestive of a range that is “familiar”and “recognized.”47,48 It is ideal thatthese sounds come from the physicalorigin, whereby the mother or father isthe source. In the current study, themusic therapists met with parents andprovided a survey, and the evaluationinvolved their identification of a song ofkin27 or parent-preferred lullaby. In ad-dition, the vocal range of the motherwas notated, and, when possible, thesung melodies were provided in therange of the parent (alto-soprano)whenthey could not be there or chose not tosing. They were encouraged to sing asa first option of intervention.49 Weinstructed participating parents andcaregivers in how to entrain to theirbaby’s breath rate or activity level. Theinterventions included a mix of musictherapist and parent applications of thelullabies over the course of the studyperiod of 2½ years.
Themost innovative aspect of this studywas the novel use of applied inter-ventions of rhythm and breath. Theseinterventions had been piloted at sev-eral hospitals for the past 10 years butwere never formally tested. From a de-cade of pilot trails that used live musicand sound interventions, we hypothe-sized that the Remo ocean disc and thegato box, when played live and carefullyentrained to the infant’s breath rate,would enhance vital signs and that theeffects of these sounds would evoke anenvironment of strength and stabilityfor premature infants who were $32weeks at study entry. As a human’s vi-tality involves rhythm and breath, andas these domains have been addressedwith a variety of medical interventionswith numerous accounts of physiologicsuccessful implications, we were en-couraged by our medical teams topursue this line of investigation.
Design
The study was originally designed totakeplace at 8 hospitals for the durationof 2 years. Eight sites were approved
by their hospital’s institutional reviewboards (IRBs), but 2 sites discontinuedafter year 1, due to music therapistposition changes. Data collection tookplace at a total of 11 hospitals wherethe participation of new sites was co-ordinated with the investigatory team,led by certified music therapists andneonatologists, on their obtaining ofIRB approval. On average, each sitemaintained a total of 30 babies duringthe 2½-year study period, excluding thediscontinued sites. Some infants wereomitted because of early discharge (n= 4) or data collection availability wasnot possible (n = 8). The study wasapproved by the IRB at each partici-pating hospital and was approved forextension at 2 sites (n = 272).
Each music therapist attended trainingsessions at Beth Israel Medical Centerand had the opportunity to observe liveand video-recorded applications of eachof the interventions to ensure accuratereplication of the interventions beforestarting the study. The training includedpreparing each music therapist withorientation onhow touse a soundmeterto ensure that the live music inter-ventions did not go above 65 dB. Thevolume of music application was mea-sured by each researcher to range from55 to 65 dB using an A-weighted scaleplaced at or near the infant ear. Thisvolume level was implemented to meetcriteria consistent with current knowl-edge of infant auditory development inrelationship to the ambient NICU soundenvironment. Carefully applied use ofmusic is chosen for properties that in-duce relaxation, rest, comfort, and op-timal growth and therefore must bedistinguished fromambient noise that isincidental and noxious.50 ContinuousNICU ambient sound at $60 dB is as-sociated with sleep disturbances forinfants51 and may mask music applica-tions. Music applications of 55 to 65 dBfor short-timed interventions met rec-ommendations for infants and support
a variance of 10 dB between the ambientsound floor and sound interventions toensure audibility.50 Although environ-mental sound was not within the scopeof this investigation, the NICUs includedin the study were deliberately selectedas sites that have staff and teams whohave concern for noise and ambientsounds. The music therapy in the cur-rent study included individual infantsand their caregivers, and the live musicinterventions were offered exclusivelyto them at their incubator or bassinette.The infants included in the study whowere in an incubator received themusicintervention through the open midlineportal.
Randomization of the sequence ofpresentation was generated by com-puter to allow for separate sequencesfor morning and afternoon during theweek so that no infant received thesame stimulus .1 day per week overthe course of the study period. Eachinfant had each of the 3 interventionsor control for 3 days per week duringa period of 2 weeks for a total of 6interventions. The staff of registerednurses and physicians who enrolled
TABLE 1 Demographic and ClinicalCharacteristics (N = 272)
CharacteristicFemale gender 152 (56%)a
Gestational age, wk 29.57 6 2.89b
Age at start of study, d 22 (1, 140)c
Apgar 1d 6.81 6 2.08Apgar 5e 8.11 6 1.21Weight at birth, g 1321.22 6 495.32Respiratory distress/
Respiratorydistress syndrome
153 (88%)
Clinical sepsis 87 (32%)SGA 53 (19%)
Values at baselineWeight, g 1596 6 374.99Heart rate 156.30 6 8.45Respiratory rate 50.58 6 7.65O2 saturation 96.83 6 2.65Total calories 128.91 6 50.56Sucking behavior 9.88 6 2.77
a Frequency (%).b Mean 6 SD.c Median (minimum, maximum).d Apgar score at birth.e Apgar score at 5 min.
ARTICLE
PEDIATRICS Volume 131, Number 5, May 2013 905
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
the babies were blinded to the ran-domization schedule that the statisti-cian developed. Allocation sequencingwas generated by the biostatistician,who had no contact with the partic-ipants.
Thestudy involvedacrossoverdesign inwhich all infants received each of the 3possible treatments (lullaby, gato box,oceandisc) orcontrol,wherenoexplicitaural stimulation was presented. Eachtreatment was given 2 times per weekover the course of the 2-week studyperiod. The presentation of the treat-ments was varied by day of the weekwithin each week and by the time of dayand randomized (either morning orafternoon) across the 2 weeks. If theinfant received an intervention in the
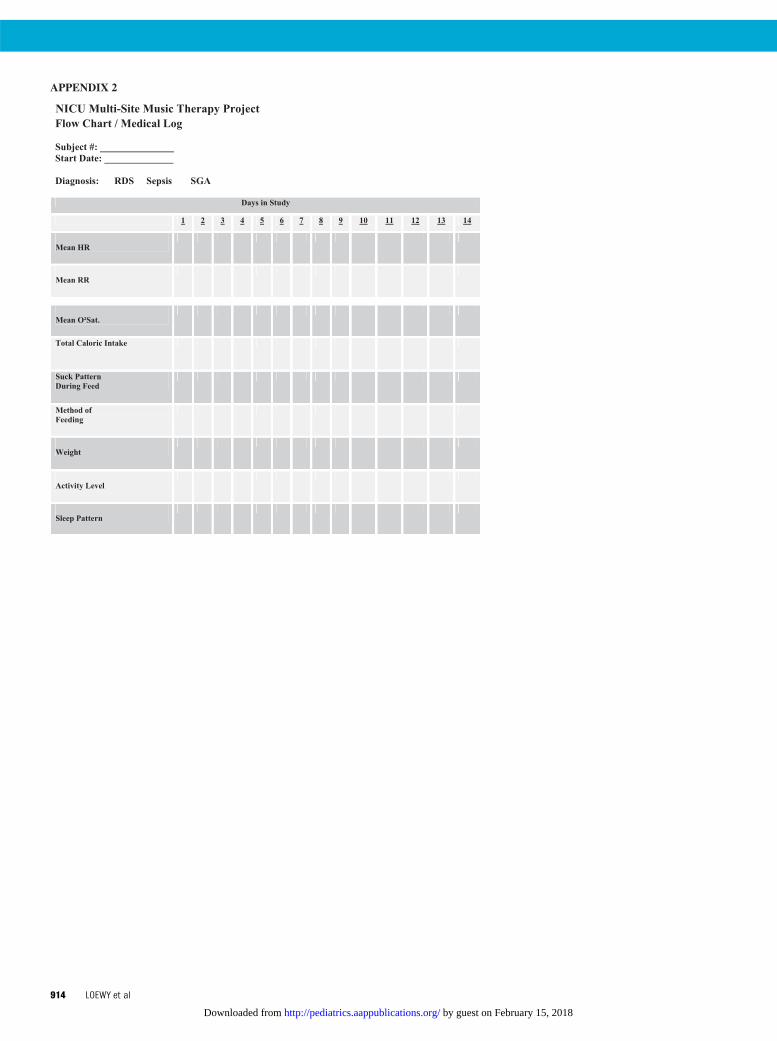
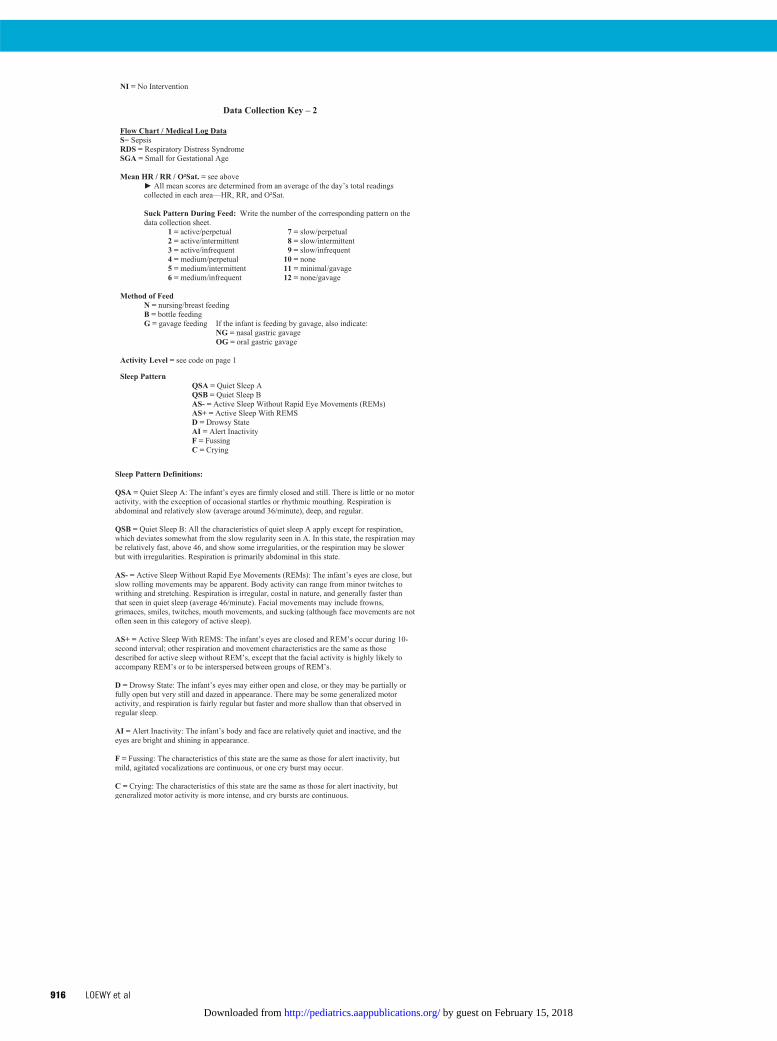
morning, the control condition wasgathered in the afternoon and viceversa (Appendix 1). In addition, theinfant’s vital signs, feeding behaviors,and sleep patterns were recordeddaily throughout the 2-week periodwhich provided additional conditionsto compare intervention with non-intervention analyses (Appendixes 2, 3,and 4).
Description of the Interventions
The3 interventions included livesingingof the song of kin used as a familiallullaby or “Twinkle, Twinkle” in thecases where parents did not identifya favorite lullaby; entrained breathingsounds, through the live application ofthe ocean disc; and entrained live
heartbeat sounds, through the use ofthe gato box. Interventions were pro-vided live and delivered through theportholes of the incubators, isolettes,or at bassinette side at the infants’midline to encourage fetal positioning.
Lullaby
The song of kin is a melody that isidentified by a parent that has beenused within a family’s history or atpresent that is familiar and/or repre-sentative of the culture of that family’scommunity. Song of kin may be fromchurch or synagogue, it may be anursery rhyme that a parent’s parentsang to them, or it may be a self-composed melody. The identifiedsongs of kin are implemented as lul-labies in the NICU. In this study, we usedthe lullabies as soothing song inter-ventions that were sung live to theinfants.
Ocean Disc
The Remo ocean disc is a musical in-strument that is round and is filled withtiny metal balls. When the disc is ro-tated, the metal balls move slowly tocreate a sound effect that is containedand quiet and meant to simulate thefluid sounds of the womb. The disc as itis played live can be entrained to matchthe infant’s inhalation and exhalationcycles.
Gato Box
The gato box is a small rectangulartuned musical instrument that is usedto provide an entrained rhythm in softtimbre meant to simulate a heartbeatsound that the neonate would hear inthe womb.
Measurements of the outcomes oc-curred at 1-minute intervals during the10-minute phase before intervention,the 10-minute phase during, and the 10-minute phase after intervention. Themean numberof each of these readingscalculated over the minute was then
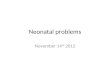
FIGURE 1Comparison of activity level before, during, and after each condition.
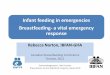
FIGURE 2Comparison of HR before, during, and after each condition.
906 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
calculated for each phase for analysisamong the vital numbers collected fora 1-minute period before, during, andafter the interventions (Appendix 1).
Measurements
Primary outcomes included the infants’vital signs (HR, RR, and O2 saturationlevels) and activity level (Appendix 1).The order of presentation was ran-domized for the morning or afternoonintervention, or control condition, bythe biostatistician. The interventionswere given in the morning or evening,on a daily basis during the 2-weekstudy period. Secondary outcomes in-cluded feeding, sleeping, and caloricintake throughout the 2-week period.
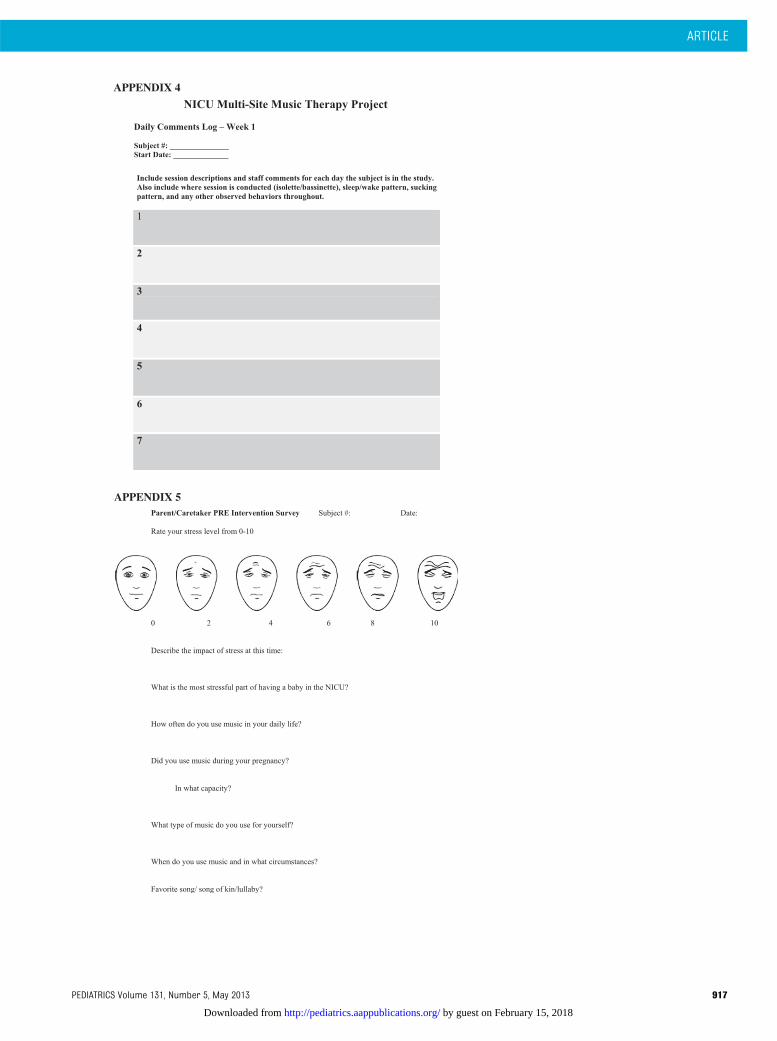
The infants’development as secondaryoutcomes was recorded by blindedresearch assistants, and this occurredon a daily basis via the nursing flowsheet (Appendix 2). Parental/caregiveruse of music during pregnancy and thesong of kin was assessed before in-tervention. Because “Twinkle” was of-fered as the lullaby intervention whenparents presented with no identifiedsong, our analysis includes outcomesof a comparison of their identified songof kin with “Twinkle.” Parental percep-tions of their own level of stress wereassessed by using a Likert rating scaleand questionnaire administered at thebeginning at end of the 2-week in-tervention period (Appendix 5).
Statistical Analysis
Normally distributed variables (eg, HR)were described in terms ofmean6 SD,whereas categorical variables (eg,activity patterns) were describedin terms of frequency (percentage).Repeated-measures mixed-model re-gression was used to analyze changesin normally distributed variables overtime, whereas a generalized linearmodel (generalized estimation equa-tion) was used for categorical out-comes. All analyseswere carried out byusing SAS 9.1 (SAS Institute Inc, Cary,NC). A level of significance of .05 wasused for all analyses. All statisticallysignificant results are reported interms of P value, Cohen d effect size(ES), and confidence limit of ES. Aninitial sample estimate revealed that240 infants allowed for$80% power todetect a small size (Cohen d) of 0.18.The final sample of 272 allowed for 84%power to detect an effect size of thismagnitude.
The study was powered to detect anyoutcome that was measured alonga continuum that had a small ES.
RESULTS
Characteristics of the Infants
The demographic and clinical charac-teristics of the sample are shown inTable 1. The mean age in weeks was32.87 weeks; 88% of the infants pre-sented with respiratory distress, 32%with clinical sepsis, and 19% were SGA.
Within-Session Changes in Outcome
Quiet–alert time showed a significantinteraction between time and condition(P = .05, ES 18, 95% confidence interval[CI] 0.001 to 0.36) that was reflected inan increase in activity level from beforeto during in response to lullaby. Activitylevel after lullaby then decreased. Incontrast, ocean disc and gato box bothshowed no significant difference inpattern compared with the controlcondition (P = .82 for both, ES 0.08, 95%
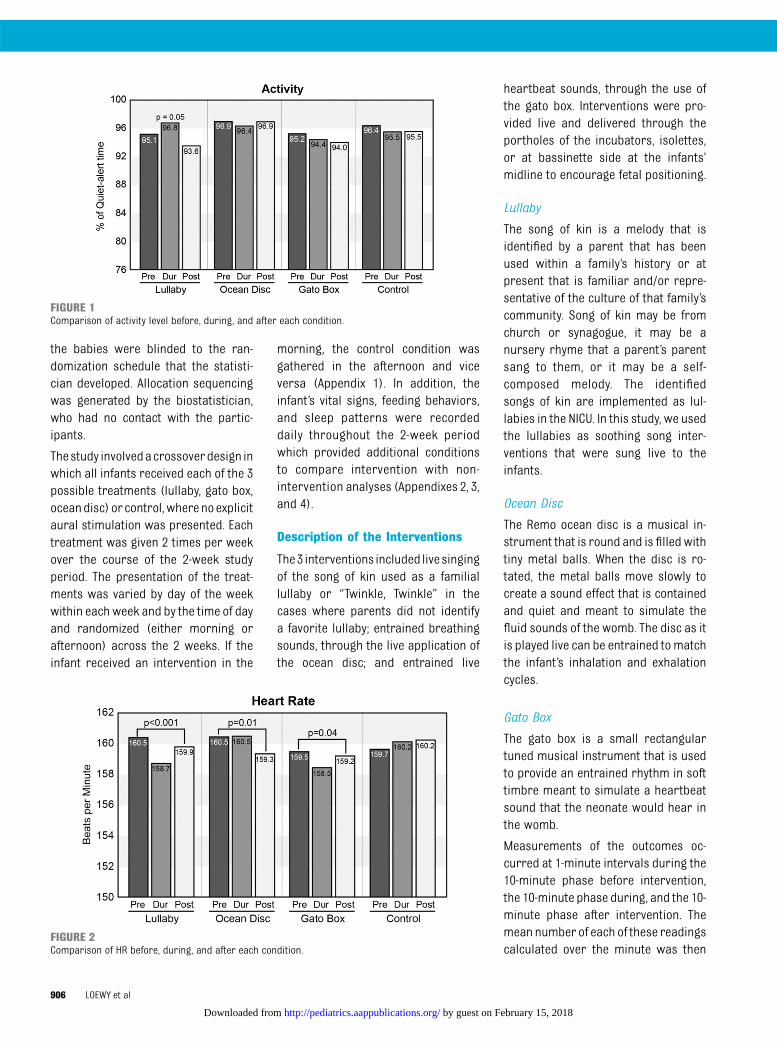
FIGURE 3Comparison of RR before, during, and after each condition.
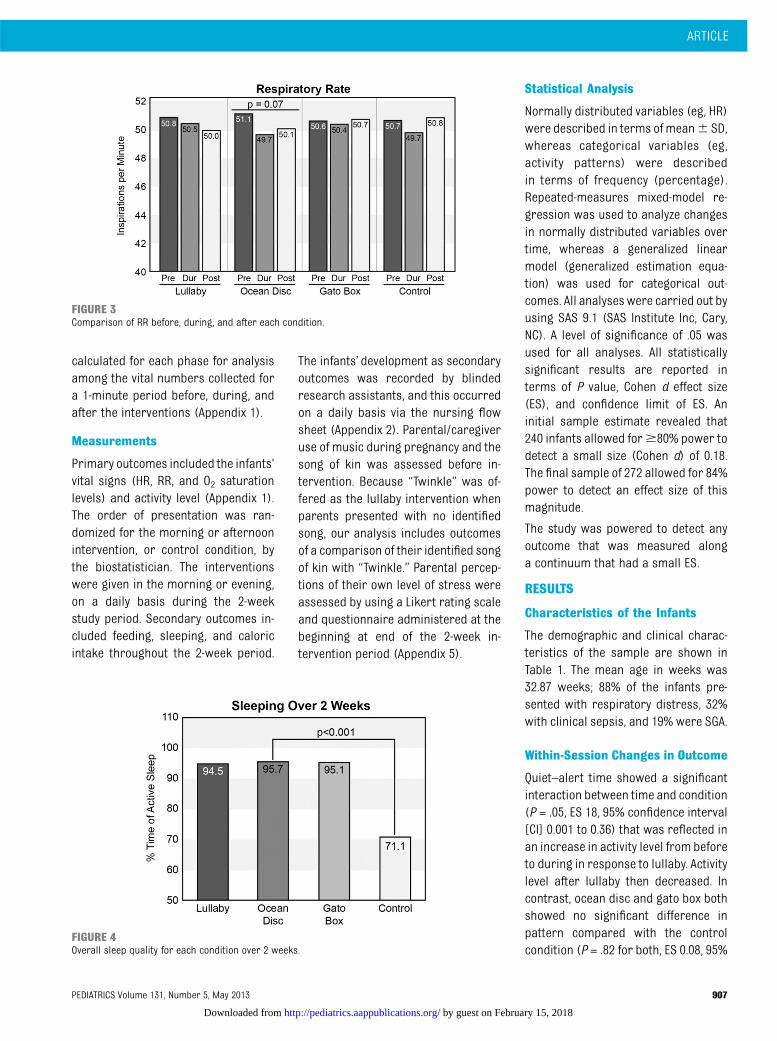
FIGURE 4Overall sleep quality for each condition over 2 weeks.
ARTICLE
PEDIATRICS Volume 131, Number 5, May 2013 907
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
CI 20.10 to 0.26; Fig 1). All 3 inter-ventions showed a significant effect ofintervention over time (before, during,after) on HR (Fig 2). Lower HRs wererecorded during the intervention onlyfor lullaby and gato box. There wasa greater pre–post intervention re-sponse for lullaby (P , .001, ES 0.23,95% CI 0.05 to 0.41) than for gato box(P = .04, ES 0.13, 95% CI20.05 to 0.31).For the ocean disc, the HR decreasedsignificantly after the intervention (P =.01, ES 0.17, 95% CI20.01 to 0.35) Thereappeared to be a trend for RR for theocean disc with higher RRs during in-tervention and after intervention (P =.07, ES 0.11, 95% CI 20.07 to 0.29),whereas the P value for lullaby was0.47 (ES 0.03, 95% CI20.15 to 0.21) and
for gato box was 0.71 (ES 0.01, 95%CI 20.17 to 0.19; Fig 3).
Long-term Changes in Outcome
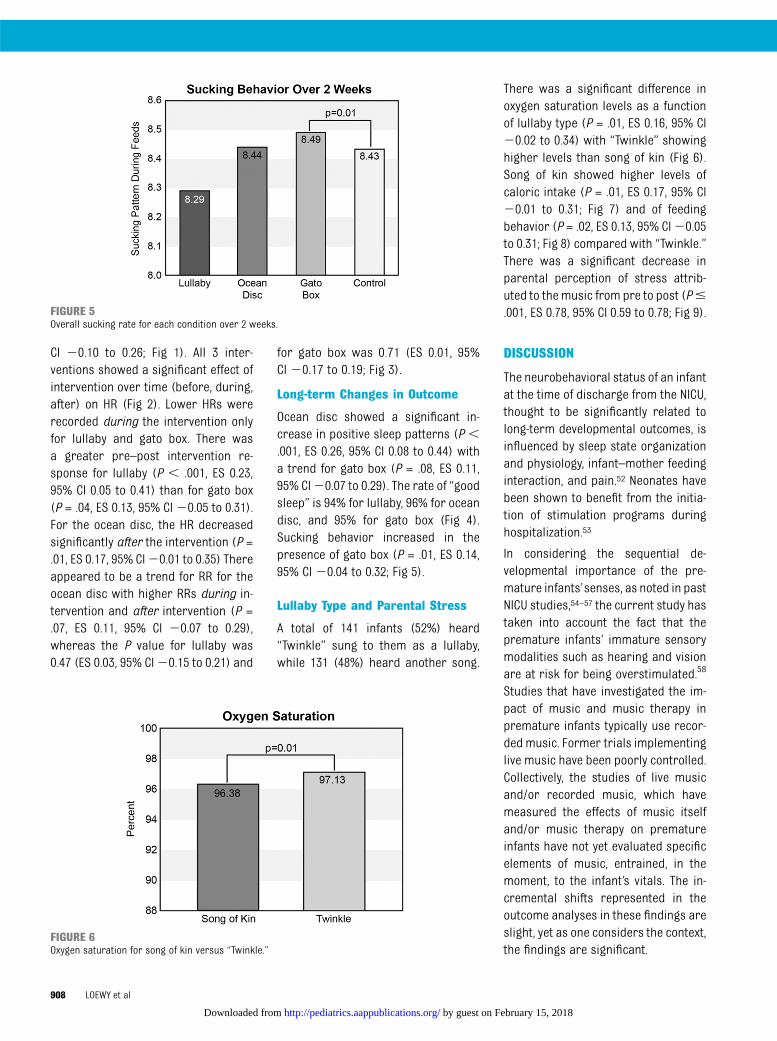
Ocean disc showed a significant in-crease in positive sleep patterns (P ,.001, ES 0.26, 95% CI 0.08 to 0.44) witha trend for gato box (P = .08, ES 0.11,95% CI20.07 to 0.29). The rate of “goodsleep” is 94% for lullaby, 96% for oceandisc, and 95% for gato box (Fig 4).Sucking behavior increased in thepresence of gato box (P = .01, ES 0.14,95% CI 20.04 to 0.32; Fig 5).
Lullaby Type and Parental Stress
A total of 141 infants (52%) heard“Twinkle” sung to them as a lullaby,while 131 (48%) heard another song.
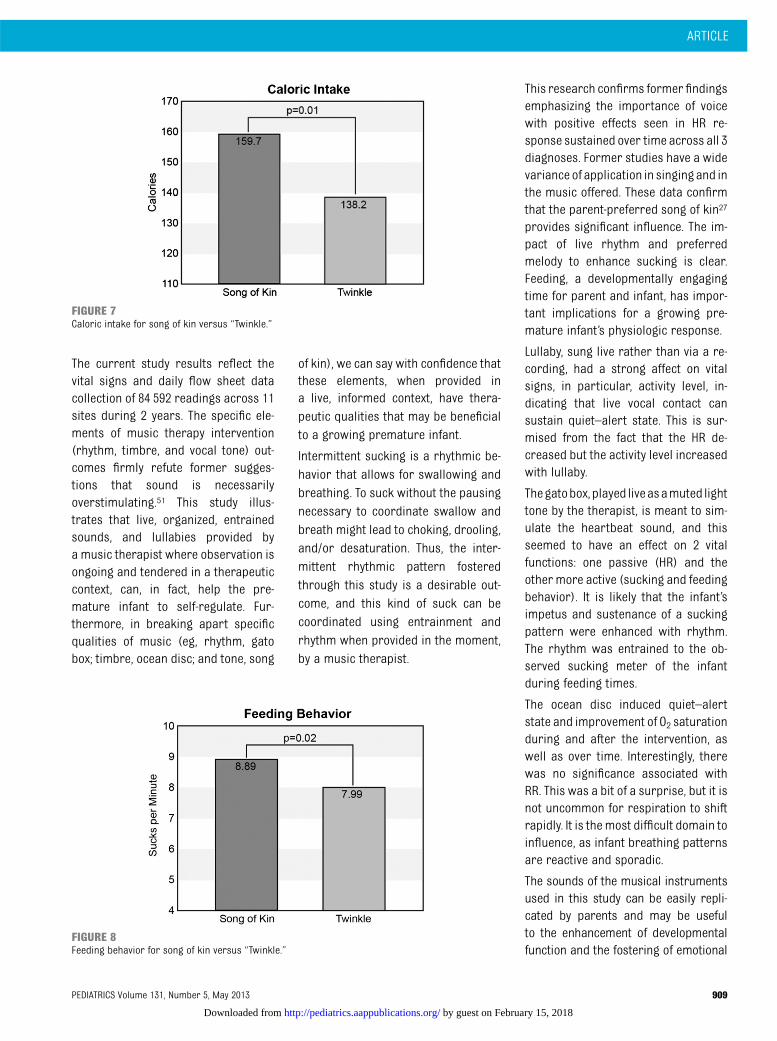
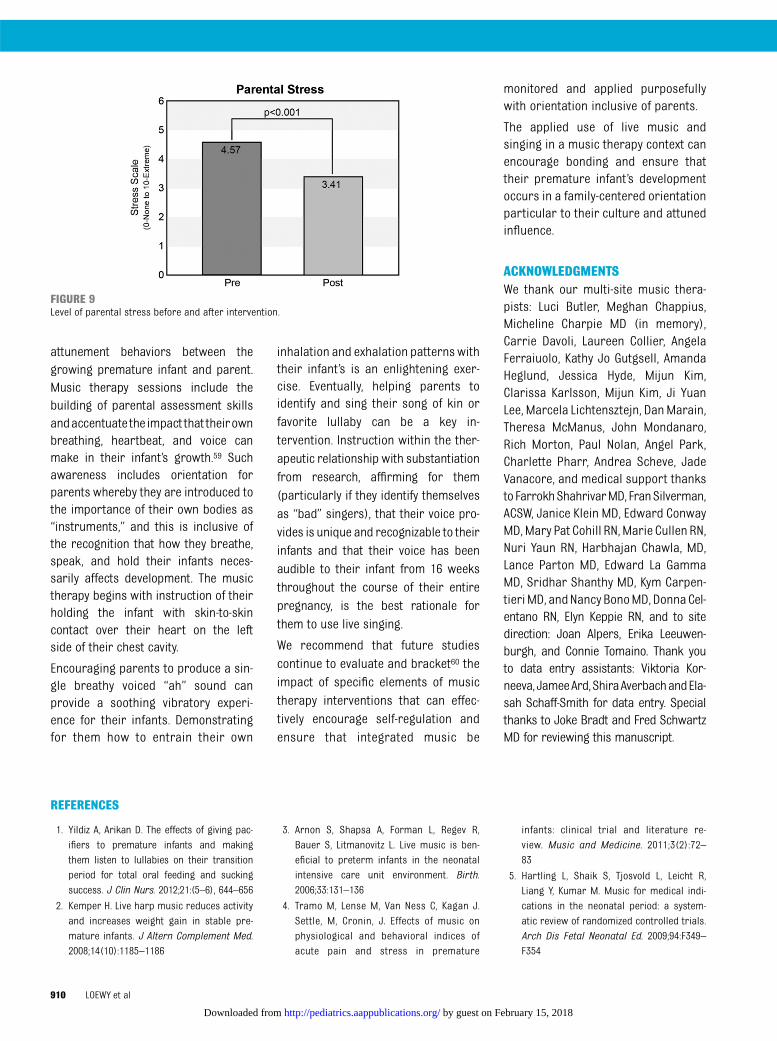
There was a significant difference inoxygen saturation levels as a functionof lullaby type (P = .01, ES 0.16, 95% CI20.02 to 0.34) with “Twinkle” showinghigher levels than song of kin (Fig 6).Song of kin showed higher levels ofcaloric intake (P = .01, ES 0.17, 95% CI20.01 to 0.31; Fig 7) and of feedingbehavior (P = .02, ES 0.13, 95% CI20.05to 0.31; Fig 8) compared with “Twinkle.”There was a significant decrease inparental perception of stress attrib-uted to the music from pre to post (P#.001, ES 0.78, 95% CI 0.59 to 0.78; Fig 9).
DISCUSSION
The neurobehavioral status of an infantat the time of discharge from the NICU,thought to be significantly related tolong-term developmental outcomes, isinfluenced by sleep state organizationand physiology, infant–mother feedinginteraction, and pain.52 Neonates havebeen shown to benefit from the initia-tion of stimulation programs duringhospitalization.53
In considering the sequential de-velopmental importance of the pre-mature infants’senses, as noted in pastNICU studies,54–57 the current study hastaken into account the fact that thepremature infants’ immature sensorymodalities such as hearing and visionare at risk for being overstimulated.58
Studies that have investigated the im-pact of music and music therapy inpremature infants typically use recor-ded music. Former trials implementinglive music have been poorly controlled.Collectively, the studies of live musicand/or recorded music, which havemeasured the effects of music itselfand/or music therapy on prematureinfants have not yet evaluated specificelements of music, entrained, in themoment, to the infant’s vitals. The in-cremental shifts represented in theoutcome analyses in these findings areslight, yet as one considers the context,the findings are significant.
FIGURE 5Overall sucking rate for each condition over 2 weeks.
FIGURE 6Oxygen saturation for song of kin versus “Twinkle.”
908 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
The current study results reflect thevital signs and daily flow sheet datacollection of 84 592 readings across 11sites during 2 years. The specific ele-ments of music therapy intervention(rhythm, timbre, and vocal tone) out-comes firmly refute former sugges-tions that sound is necessarilyoverstimulating.51 This study illus-trates that live, organized, entrainedsounds, and lullabies provided bya music therapist where observation isongoing and tendered in a therapeuticcontext, can, in fact, help the pre-mature infant to self-regulate. Fur-thermore, in breaking apart specificqualities of music (eg, rhythm, gatobox; timbre, ocean disc; and tone, song
of kin), we can say with confidence thatthese elements, when provided ina live, informed context, have thera-peutic qualities that may be beneficialto a growing premature infant.
Intermittent sucking is a rhythmic be-havior that allows for swallowing andbreathing. To suck without the pausingnecessary to coordinate swallow andbreath might lead to choking, drooling,and/or desaturation. Thus, the inter-mittent rhythmic pattern fosteredthrough this study is a desirable out-come, and this kind of suck can becoordinated using entrainment andrhythm when provided in the moment,by a music therapist.
This research confirms former findingsemphasizing the importance of voicewith positive effects seen in HR re-sponse sustained over time across all 3diagnoses. Former studies have a widevariance of application in singing and inthe music offered. These data confirmthat the parent-preferred song of kin27
provides significant influence. The im-pact of live rhythm and preferredmelody to enhance sucking is clear.Feeding, a developmentally engagingtime for parent and infant, has impor-tant implications for a growing pre-mature infant’s physiologic response.
Lullaby, sung live rather than via a re-cording, had a strong affect on vitalsigns, in particular, activity level, in-dicating that live vocal contact cansustain quiet–alert state. This is sur-mised from the fact that the HR de-creased but the activity level increasedwith lullaby.
Thegatobox,played liveasamuted lighttone by the therapist, is meant to sim-ulate the heartbeat sound, and thisseemed to have an effect on 2 vitalfunctions: one passive (HR) and theother more active (sucking and feedingbehavior). It is likely that the infant’simpetus and sustenance of a suckingpattern were enhanced with rhythm.The rhythm was entrained to the ob-served sucking meter of the infantduring feeding times.
The ocean disc induced quiet–alertstate and improvement of O2 saturationduring and after the intervention, aswell as over time. Interestingly, therewas no significance associated withRR. This was a bit of a surprise, but it isnot uncommon for respiration to shiftrapidly. It is themost difficult domain toinfluence, as infant breathing patternsare reactive and sporadic.
The sounds of the musical instrumentsused in this study can be easily repli-cated by parents and may be usefulto the enhancement of developmentalfunction and the fostering of emotional
FIGURE 7Caloric intake for song of kin versus “Twinkle.”
FIGURE 8Feeding behavior for song of kin versus “Twinkle.”
ARTICLE
PEDIATRICS Volume 131, Number 5, May 2013 909
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
attunement behaviors between thegrowing premature infant and parent.Music therapy sessions include thebuilding of parental assessment skillsandaccentuate the impact that theirownbreathing, heartbeat, and voice canmake in their infant’s growth.59 Suchawareness includes orientation forparents whereby they are introduced tothe importance of their own bodies as“instruments,” and this is inclusive ofthe recognition that how they breathe,speak, and hold their infants neces-sarily affects development. The musictherapy begins with instruction of theirholding the infant with skin-to-skincontact over their heart on the leftside of their chest cavity.
Encouraging parents to produce a sin-gle breathy voiced “ah” sound canprovide a soothing vibratory experi-ence for their infants. Demonstratingfor them how to entrain their own
inhalation and exhalation patternswiththeir infant’s is an enlightening exer-cise. Eventually, helping parents toidentify and sing their song of kin orfavorite lullaby can be a key in-tervention. Instruction within the ther-apeutic relationship with substantiationfrom research, affirming for them(particularly if they identify themselvesas “bad” singers), that their voice pro-vides is unique and recognizable to theirinfants and that their voice has beenaudible to their infant from 16 weeksthroughout the course of their entirepregnancy, is the best rationale forthem to use live singing.
We recommend that future studiescontinue to evaluate and bracket60 theimpact of specific elements of musictherapy interventions that can effec-tively encourage self-regulation andensure that integrated music be
monitored and applied purposefullywith orientation inclusive of parents.
The applied use of live music andsinging in a music therapy context canencourage bonding and ensure thattheir premature infant’s developmentoccurs in a family-centered orientationparticular to their culture and attunedinfluence.
ACKNOWLEDGMENTSWe thank our multi-site music thera-pists: Luci Butler, Meghan Chappius,Micheline Charpie MD (in memory),Carrie Davoli, Laureen Collier, AngelaFerraiuolo, Kathy Jo Gutgsell, AmandaHeglund, Jessica Hyde, Mijun Kim,Clarissa Karlsson, Mijun Kim, Ji YuanLee, Marcela Lichtensztejn, DanMarain,Theresa McManus, John Mondanaro,Rich Morton, Paul Nolan, Angel Park,Charlette Pharr, Andrea Scheve, JadeVanacore, and medical support thankstoFarrokhShahrivarMD, FranSilverman,ACSW, Janice Klein MD, Edward ConwayMD,Mary Pat Cohill RN,Marie Cullen RN,Nuri Yaun RN, Harbhajan Chawla, MD,Lance Parton MD, Edward La GammaMD, Sridhar Shanthy MD, Kym Carpen-tieriMD, andNancy BonoMD, DonnaCel-entano RN, Elyn Keppie RN, and to sitedirection: Joan Alpers, Erika Leeuwen-burgh, and Connie Tomaino. Thank youto data entry assistants: Viktoria Kor-neeva,JameeArd,ShiraAverbachandEla-sah Schaff-Smith for data entry. Specialthanks to Joke Bradt and Fred SchwartzMD for reviewing this manuscript.
REFERENCES
1. Yildiz A, Arikan D. The effects of giving pac-ifiers to premature infants and makingthem listen to lullabies on their transitionperiod for total oral feeding and suckingsuccess. J Clin Nurs. 2012;21:(5–6), 644–656
2. Kemper H. Live harp music reduces activityand increases weight gain in stable pre-mature infants. J Altern Complement Med.2008;14(10):1185–1186
3. Arnon S, Shapsa A, Forman L, Regev R,Bauer S, Litmanovitz L. Live music is ben-eficial to preterm infants in the neonatalintensive care unit environment. Birth.2006;33:131–136
4. Tramo M, Lense M, Van Ness C, Kagan J.Settle, M, Cronin, J. Effects of music onphysiological and behavioral indices ofacute pain and stress in premature
infants: clinical trial and literature re-view. Music and Medicine. 2011;3(2):72–83
5. Hartling L, Shaik S, Tjosvold L, Leicht R,Liang Y, Kumar M. Music for medical indi-cations in the neonatal period: a system-atic review of randomized controlled trials.Arch Dis Fetal Neonatal Ed. 2009;94:F349–F354
FIGURE 9Level of parental stress before and after intervention.
910 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from

6. Krueger C. Exposure to maternal voice inpreterm infants. Adv Neonatal Care. 2012;10(1):13–18
7. deRegnier R, Wewerka S, Georgieff MK,Mattia F, Nelson CA. Influences of post-conceptional age and postnatal experienceon the development of auditory recognitionmemory in the newborn infant. DevPsychobiol. 2002;41:216–225
8. Caskey M, Stephens B, Tucker R, Vohr B.Importance of parent talk on the de-velopment of preterm infant vocalizations.Pediatrics. 2011;128(5):910–916
9. Porges SW, Furman SA. The early de-velopment of the autonomic nervous sys-tem provides a neural platform for socialbehavior: a polyvagal perspective. InfantChild Dev. 2011;20:106–118
10. Stewart, K. PATTERNS—A model for evalu-ating trauma in NICU music therapy: Part1—Theory and design. Music Med. 2009;1:29–40
11. Lubetzky R, Mimouni FB, Dollberg S, ReifenR, Ashbel G, Mandel D. Effect of Music byMozart on Energy Expenditure in GrowingPreterm Infants. Pediatrics. 2010;125(1):24–28
12. Trainor L. Infant preferences for infant-directed versus non-infant directed play-songs and lullabies. Infant Behav Dev. 1996;19:83–92
13. Shenfield T, Trainor LJ, Nakata T. ‘Maternalsinging modulates infant arousal Psychologyof Music, Society for Education. Music andPsychology Research. 2003;31(4):365–375
14. Kemper KJ, Hamilton C. Live harp musicreduces activity and increases weight gainin stable premature infants. J Altern Com-plement Med. 2008;14(10):1185–1186
15. Cassidy JW. The effect of decibel level ofmusic stimuli and gender on head cir-cumference and physiological responses ofpremature infants in the NICU. J MusicTher. 2009;46(3):180–190
16. Olischar M, Shoemark H, Holton T, WenigerW, Hunt R. The influence of music on aEEGactivity in neurologically healthy newborns$32 weeks’ gestational age. Acta Paediatr.2011;100(5):670–675
17. Calabro L, Wolfe R, Shoemark H. The effectsof recorded sedative music on the physi-ology and behavior of premature infantswith a respiratory disorder. Aust J MusicTher. 2003;14:3–19
18. Cervasco A, Grant R. Effects of the pacifieractivated lullaby on weight gain of pre-mature infants. J Music Ther. 2005;42(2):123–139
19. Coleman JM, Pratt RR, Stoddar RA, GerstmannDR, Abel H. The effects of male and femalesinging and speaking voices on selected
physiological and behavioral measures ofpremature infants in the intensive careunit. International Journal of Arts Medi-cine. 1998;5(8):4–11
20. Hui-Ling Lai HL, Chen C, Peng J. T. C., Chang,F. M., Hsiao, Y. H, Chang, C. Randomizedcontrolled trial of music during kangaroocare on maternal state anxiety and pre-term infants’ responses. Int J Nurs Stud.2006;43(2):139–146
21. Chou LL, Wang RH, Chen SJ. Effects of musictherapy on oxygen saturation in prematureinfants receiving endotracheal suctioning.J Nurs Res. 2003;11(3):209–216
22. Burke M, Walsh J, Oehler J, Gingras J. Musictherapy following suctioning: four casestudies. Neonatal Netw. 1995;14(7):41–49
23. Collins SK, Kuck K. Music therapy in theneonatal intensive care unit. NeonatalNetw. 1991;9(6):23–26
24. De l’Etoile SK. Infant-directed singing:a theory for clinical intervention. MusicTher Perspect. 2006;24:22–29
25. Courtnage A, Chawla H. Loewy J, Nolan P.Effects of live, infant-directed singing onoxygen saturation, heart rates and re-spiratory rates of infants in the neonatalintensive care unit. Pediatr Res. 2002;2346(51):403A
26. Nakata T, Trehub SE. Infants’ responsivenessto maternal speech and singing. InfantBehav Dev. 2004;27:455–456
27. Loewy J,, Hallan C, Friedman E, Martinez C.Sleep/sedation in children undergoing EEGtesting: A comparison of chloral hydrateand music therapy. Journal of Peri-anesthesia Nursing. 2005;20(5):323–331
28. Harlow H, Suomi S. Social recovery byisolation-reared monkeys. Proc Natl AcadSci USA. 1971;68(7):1534–1538
29. Thoman E, Ingersoll E, Acebo C. Prematureinfants seek rhythmic stimulation, and theexperience facilitates neurobehavioral de-velopment. J Dev Behav Pediatr. 1991;12(1):11–18
30. Boukydis CF, Bigsby R, Lester BM. Clinicaluse of the neonatal intensive care unitnetwork neurobehavioral scale. Pediatrics.2004;113(3 pt 2):679–689
31. Bradt J. The effects of music entrainmenton postoperative pain perception in pedi-atric patients. Music Med. 2010;2:150–157
32. Bialoskurski M, Cox CL, Hayes JA. The na-ture of attachment in a neonatal intensivecare unit. J Perinat Neonatal Nurs. 1999;13(1):66–77
33. Hurst I. Vigilant watching over: Mothers’actions to safeguard their prematurebabies in the newborn intensive carenursery. J Perinat Neonatal Nurs. 2001;15(3):39–57
34. Philbin M. Planning the acoustic environ-ment of a neonatal intensive care unit. ClinPerinatol. 2004;31:331–352
35. Byers JF, Waugh WR, Lowman LB. Soundlevel exposure of high-risk infants in dif-ferent environmental conditions. J Neo-natal Nurs. 2006;25:25–32
36. Mazer S. Music, noise, and the environment ofcare. Music and Medicine. 2010;2(3):182–191
37. Ising H, Kruppa B. Health effects caused bynoise: Evidence in the literature from thepast 25 years. Noise Health. 2004;6:5–13
38. Griffin T. Family centered care in the NICU.J Perinat Neonatal Nurs. 2006;20(1):98–102
39. Saunders RP, Abraham MR, Crosby MJ,Thomas K, Edwards WH. Evaluation anddevelopment of potentially better practicesfor improving family-centered care in neo-natal intensive care units. Pediatrics. 2003;111(suppl):437–449
40. Jotzo M, Poets CF. Helping parents cope withthe trauma of premature birth: an evalua-tion of a trauma-preventive psychologicalintervention. Pediatrics, 2005;115(4):915–919
41. Lawhon G. Facilitation of parenting thepremature infant within the newborn in-tensive care unit. J Perinat Neonatal Nurs,2002;16:71–82
42. Abrams A, Gerhardt K. The acoustic envi-ronment and physiological responses ofthe fetus, J Perinatol. 2000;20 (2):S31–S36
43. Hepper PG, Shahidullah BS. Development offetal hearing. Arch Dis Child. 1994;71:F81–F87
44. Winkler I, Háden GP, Ladinig O, Sziller I,Honing H. Newborn infants detect the beatin music. Proc Natl Acad Sci USA. 2009;106(7):2468–2471
45. Ingersoll E, Thoman E. Breathing bear:Effects on respiration in premature infants.J Physiol Behav. 1995;56(5):855–859
46. Tsang CD, Conrad NJ. Does the messagematter? The effect of song type on infants’pitch preferences for lullabies and play-songs. Infant Behav Dev. 2009;33(1):96–100
47. Volkova A, Trehub SE, Schellenberg EG.Infants’ memory for musical performances.Dev Sci. 2006;9:583–589
48. Papousek M. Melodies in caregiver´sspeech: A species-specific guidance to-wards language. Early Dev Parenting. 1994;3(1):5–17
49. Trehub SE. The perception of musical pat-terns by human infants: The provision ofsimilar patterns by their parents. In:Berkley MA, Stebbins WC, eds. ComparativePerception. vol. 1: Mechanisms. New York,NY: John Wiley; 1990:429–459
50. Standley JM. A meta-analysis of the efficacyof music therapy for premature infants. JPediatr Nurs. 2002;17:107–113
ARTICLE
PEDIATRICS Volume 131, Number 5, May 2013 911
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from

51. Graven SN. Sound and the developing infantin the NICU: Conclusions and recom-mendations for care. J Perinatol. 2000;20(8,pt 2):S88–S93
52. Lester B, Miller R, Hawes K, et al. Infantneurobehavioral development. Semin Peri-natol. 2011;35(1):8–19
53. Krywanio M. Meta-analysis of physiologicaloutcomes of hospital-based infant in-tervention programs. Nurs Res. 1994;43(3):133–137
54. Graven SN, Bowen FW Jr, Brooten D, et al.The high-risk infant environment, Part 1.The role of the neonatal intensive care unit
in the outcome of high-risk infants. J Per-inatol. 1992;12:164–172
55. Als HL, Gilkerson FH, Duffy GB, McAnulty DM,Buehler KA, VandenBerg N, et al. A threecenter randomized controlled trial of in-dividualized develop-mental care for very lowbirth weight preterm infants: Med- ical, neu-rodevelopmental, parenting and caregivingeffects. J Dev Behav Pediatr. 2003;24:399–408
56. MacKendrick W. Understanding neuro-development in premature infants: appliedchaos theory. J Pediatr. 2006;148:427–429
57. White-Traut RC, Nelson MN, Silvestri JM, et al.Responses of preterm infants to unimodal
and multimodal sensory intervention.Pediatr Nurs. 1997;23(2):169–176
58. Liu W, Lauder S, Perkins B, MacMillan-YorkE, Martin S,, Graven S. The development ofpotentially better practices to support theneurodevelopment of infants in the NICU. JPerinatol. 2007;27:S48–S74
59. Shoemark H. Infant-directed singing asa vehicle for regulation rehearsal in themedically fragile full-term infant. Austra-lian J of Music Therapy. 2006;17:54–63
60. Haslbeck F. Understanding of active musictherapy in neonatal care. Music and Medi-cine. 2012;4(4):205–214
912 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
ARTICLE
PEDIATRICS Volume 131, Number 5, May 2013 913
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
914 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
ARTICLE
PEDIATRICS Volume 131, Number 5, May 2013 915
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
916 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
ARTICLE
PEDIATRICS Volume 131, Number 5, May 2013 917
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
918 LOEWY et al
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from

originally published online April 15, 2013; Pediatrics Joanne Loewy, Kristen Stewart, Ann-Marie Dassler, Aimee Telsey and Peter Homel
InfantsThe Effects of Music Therapy on Vital Signs, Feeding, and Sleep in Premature
ServicesUpdated Information &
012-1367http://pediatrics.aappublications.org/content/early/2013/04/10/peds.2including high resolution figures, can be found at:
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pediatrics.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
ISSN: . 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from
originally published online April 15, 2013; Pediatrics Joanne Loewy, Kristen Stewart, Ann-Marie Dassler, Aimee Telsey and Peter Homel
InfantsThe Effects of Music Therapy on Vital Signs, Feeding, and Sleep in Premature
http://pediatrics.aappublications.org/content/early/2013/04/10/peds.2012-1367located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: . 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on February 15, 2018http://pediatrics.aappublications.org/Downloaded from