Embed Size (px)
Citation preview

TheeffectsofLow-LevelLaserTherapyandLED-MediatedPhotobiomodulationonthepulpcanalvolumeofhumanpremolarsundergoingorthodontictoothmovement
DRRALUCABALEANU
DISCIPLINEOFORTHODONTICS
FACULTYOFDENTISTRY
UNIVERSITYOFSYDNEY,
AUSTRALIA
A Thesis submitted in conformity with the requirements for the degree of Doctor
of Philosophy, Dentistry (Orthodontics)

Dedication
To my son Rares who support me throughout these years and nevertheless during the
Covid19 pandemic period, my best friends Cosmin G ,Mihaela R, Mary, Anthony and
all the friends that had unconditional love for me during all these years.
To all my supervisors that believed in me. Thank you for being there for me over the
past years.

Candidate Certification
This is to certify that the candidate carried out the work in this thesis in the
Orthodontic Department, University of Sydney, and this work has not been submitted
to any other University or Institution for a higher degree.
………………………………………………….
Dr Raluca Baleanu
Acknowledgments
I would like to express my gratitude to the following people:
Professor M. Ali Darendeliler, Head of Department, Discipline of Orthodontics, University of
Sydney for his supervision and for friendship over these years.
Dr. Oyku Dalci, Senior Lecturer, University of Sydney for being there for me when needed and
for her help in, discussion on study design, and in the editing of the manuscript and thesis.
Dr. Nam(Alice) Wong, Lecturer, University of Sydney for her help in discussion on study
design the editing of the manuscript and thesis.
Dr. Matthew Foley, Australian Centre for Microscopy and Microanalysis, University of Sydney
for his technical expertise and assistance with Avizo.
Associate Professor Peter Petocz, Department of Statistics, Macquarie
University for his assistance with the statistical analysis.

Table of contents
INTRODUCTION 1
ORTHODONTIC TOOTH MOVEMENT 2
RATE OF ORTHODONTIC TOOTH MOVEMENT 4
REPAIR OF ORTHODONTICALLY INDUCED INFLAMMATORY ROOT RESORPTION -OIIRR 6
ACCELERATED TOOTH MOVEMENT 8
BIOLOGICAL METHODS 8
SURGICAL METHODS 9
Corticotomy 10
Piezocision 13
Micro-osteoperforations 15
Periodantal ligament distraction and dentoalveolar distraction 16
Surgery first 17
DEVICE ASSISTED METHODS 18
Electric current 19
Magnetic fields 19
Pulsed electromagnetic fields 20
Vibration 20
Therapeutic whole body vibration 21
Localised therapeutic vibration 22
Vibration and tooth movement 23
Vibration and root resorption 25

LOW INTENSITY PULSED ULTRASOUND-LIPUS 27
LOW LEVEL LASER THERAPY 28
LOW LEVEL LASER THERAPY AND TOOTH MOVEMENT 29
LOW LEVEL LASER THERAPY ROOT RESORPTION 31
LOW LEVEL LASER THERAPY AND PAIN 32
PHOTOBIOMODULATION 33
PHOTOBIOMODULATION USING LASER 33
PHOTOBIOMODULATION USING LED 34
PHOTOBIOMODULATION AND TOOTH MOVEMENT 34
PHOTOBIOMODULATION AND ROOT RESORPTION 35
PHYSIOLOGY OF DENTAL PULP AND FACTORS AFFECTING PULP CANAL VOLUME 35
PULP CANAL VOLUME ALTERATION BY AGE, HORMONES AND NUTRITION 36
THE REACTION OF DENTAL PULP TO ORTHODONTIC FORCE 37
VASCULAR PULP CHANGES 38
FACTORS INFLUENCING THE PULPAL RESPONSE TO ORTHODONTIC FORCES 39
THE RESULTS OF PULPAL MODIFICATIONS 41
VIBRATION AND DENTAL PULP MODIFICATIONS 42
LOW-LEVEL LASER THERAPY AND DENTAL PULP MODIFICATIONS 42

PHOTOBIOMODULATION AND DENTAL PULP MODIFICATIONS 43
RELEVANCE OF THE RESEARCH 45
REFERENCES 46
MANUSCRIPT 63
Effects of Low-Laser Therapy and LED-mediated Photobiomodulation on pulp canal volume of maxillary
first premolars undergoing orthodontic tooth movement.
ABSTRACT 65
INTRODUCTION 67
MATERIALS AND METHODS 70
RESULTS 73
DISCUSSION 74
LIMITATIONS 77
GENERALIZABILITY 77
CONCLUSION 78
REFERENCES 79
LIST OF FIGURES&TABLES 83
MANUSCRIPT 87

Effect of Low-Level Laser Therapy on pulp canal volume of maxillary first premolars undergoing orthodontic
tooth movement and in retention.
ABSTRACT 89
INTRODUCTION 91
MATERIALS AND METHODS 92
RESULTS 95
DISCUSSION 96
LIMITATIONS 98
GENERALIZABILITY 99
CONCLUSION 99
REFERENCES 100
LIST OF FIGURES&TABLES 104
CONCLUSION 108
APPENDIX 119

Abbreviations
2D – Two-dimensional
3D - Three-Dimensional
A – Amplitude
AAC – afibrillar cementum
AL – Loss of anchorage
ANOVA – Analysis of variance
AOO - Accelerated Osteogenic Orthodontics
AST -aspartate aminotransferase
ATP - Adenosine Triphosphate
bFGF - basic fibroblast growth factor
CBCT - Cone beam computed tomography
Cm – Centimeters
CSs– cell sheet
CT - Computed Tomography
ddMSC – dentoalveolar-derived mesenchymal stem cell
ER - Electromagnetic Radiation
ECM –extracellular matrix maturation

F – Frequency
FGF-2 – fibroblast grow factor
g - grams
gm/gms ¬-grams
h - hour
hPDL - human Periodontal Ligament
Hz - Hertz
IGF-1 - insulin derived growth factor
IL-1β-interleukin-1 beta
IR – Infrared light
J - Joulle
LASER - Light Amplification by Stimulated Emission of Radiation
LED - Light Emitting Diode
LIPUS - Low Intensity Pulsed Ultrasound
LLLT - Low Level Laser Therapy
LTV - Localized Therapeutic Vibration
min - minutes
mm – millimeters

MSC - Mesenchymal stem cell
Mw – Mega-watts
N - Newtons
NIR - Near-Infrared Light
Nm – Nano-meters
OIIRR - Orthodontically Induced Inflammatory Root Resorption
OPG - Osteoprotegrin
OTM - Orthodontic Tooth Movement
PAOO - Periodontally Accelerated Osteogenic Orthodontics
PCO – Pulp canal obliteration
PDGF - platelet-derived growth factor
PDL - Periodontal Ligament
PEMF - Pulsed Electromagnetic Fields
PGE2 - Prostaglandin E2
PMB - Photobiomodulation
q-PCR - quantitative Polymerase Chain Reaction
RANKL - Receptor Activator of Nuclear Factor- ĸB ligand
RAP - Regional Acceleratory Phenomenon

RCT – Randomized Controlled Trial
TGF - transforming growth factor
V - Volts
VAS - Visual Analog Scale
VEGF - vascular endothelial growth factor
W - watt
μm - micrometere
Dr Raluca Baleanu 1
Introduction
The Hippocratic Oath includes the promise ‘Primum non nocere’, meaning to abstain from doing harm,
is an important goal when we treat our patients. However, even in the best of hands, and with every
positive intention, it is not always possible.
Since the demand for fast orthodontic treatment has expanded, researchers have focused on
manipulating bone biology to produce accelerated tooth movement.
One of the few pernicious consequences of accelerated tooth movement is described by the
remodeling of dental and paradental tissues as well as causing a response in the pulp.1,34,43
The pulp response to orthodontic force is thought to involve inflammation, wound healing,2 pulp
calcifications/obliterations,3,4 and in the severe cases, permanent pulp destruction with loss of
vitality.5,6 It is postulated that a short duration of orthodontic force causes biochemical and biological
pulp tissue alteration and that orthodontic forces may be less biologically safe for the pulp tissue, as
the age of the patient increases.7
Techniques which have been proposed to accelerate tooth movement include mechanical/physical
methods, biological methods and surgical methods.8,9,10,11 However, some of these methods have
proved to be invasive or impractical to integrate into the orthodontic practice.

Dr Raluca Baleanu 2
Low-level laser therapy (LLLT), also known as soft laser, has been used in accelerating orthodontic
tooth movement by stimulating bone remodeling12 and for pain relief13,14.
Photobiomodulation(PBM) is a current therapeutic approach that uses low level laser (LLL) or light
emitting diode (LED) and has been widely practiced and tested in medicine and dentistry. Research has
shown that photobiomodulation improves wound healing,13,15,17 relieves pain,18 enhance nerve
regeneration19 and stimulates tissue regeneration and tissue growth by promoting fibroblasts,20 and
chondral21 proliferation.
The increased interest into the methods of accelerated tooth movement has paved the way into
numerous studies on its effects on tooth movement. However there are no studies that directly
investigated the effects of those methods when applied during orthodontic tooth movement, on pulpal
volume. Therefore we aimed to study the effects of two popular methods of accelerated tooth
movement that are non-invasive, LLLT and LED PBM, on human pulp canal volume.
Orthodontic tooth movement
Orthodontic tooth movement (OTM) is brought about by reversible injury to the periodontium and
coordinated bone remodeling in response to mechanical strains.22 Pressure-tension, bone bending and
piezoelectric theories are commonly described to explain the biologic processes involved in tooth
movement. Piezoelectric theory postulates that piezoelectric signals generated by bone bending
initiates OTM while the classic pressure-tension theory indicated that it is chemical rather than
electrical signals which initiate cell differentiation and subsequently tooth movement. None of these

Dr Raluca Baleanu 3
theories have been proven,23. though Thilander and colleagues believed that both mechanisms
contribute in the biological control of OTM (Thilander 2011). 24
In general, orthodontic tooth movement depends on the recruitment of precursor cells to facilitate the
biological mechanism required for tooth movement.25 Monocyte precursors form osteoclasts and
osteoprogenitor cells originating in the adjoining periodontal ligament and alveolar bone convert into
osteoblasts and ultimately these osteoblasts, fixed in the bone pattern become osteocytes. To achieve
tooth movement, osteoclasts, osteocytes and osteoblasts, are necessary to produce bone resorption
and apposition.26
Application of light and constant orthodontic force initiates a cascade of events leading to OTM.
Bending of alveolar bone occurs almost immediately due to the incompressibility of periodontal
ligament (PDL) fluid, generating piezoelectric signals. Seconds later, PDL fluid expresses into the
surroundings, causing the alveolar bone to spring back and the tooth moves within the PDL space.
The pressure and tension zone created by constant orthodontic force alters blood flow in the PDL. This
leads to a change in the chemical environment. Specifically, while there is a fall in the oxygen content
and an increase in carbon dioxide levels in the pressure zone, the reverse occurs in the tension zone,
resulting in a release of prostaglandins and cytokines as well as other chemical messengers.27
Approximately four hours following force application, cellular differentiation begins within the PDL with
detectable levels of cyclic adenosine monophosphate (cAMP). Tooth movement begins two days later
as osteoclasts and osteoblasts begin to remodel the bony socket,27,28,29 with bone resorption on the
pressure side and bone deposition on the tension size.30,31
Physiological response to orthodontic force changes as the force level increases. Excessive force
magnitude occludes the blood vessels on the pressure side within three to five seconds following force

Dr Raluca Baleanu 4
application, resulting in pain. This is followed by cessation of blood flow on the pressure side, leading to
cells being distorted mechanically. Subsequently, leakage of cytokines and prostaglandins occur
resulting in sterile necrosis within hours of force application. Hence cells are recruited from adjacent
bone marrow space in about 3-5 days for differentiation into osteoblast and osteoclast. Tooth
movement occurs in 7-14 days following force application as undermining resorption removes lamina
dura adjacent to the compressed PDL. The delay in tooth movement along with other complications
resulted in a consensus that light and constant force is optimal.32
The amount of OTM is driven by mechanical and biological stimulants, as well as magnitude of applied
forces and the rate of bone remodeling.33 Studies have shown that the tissue reactions caused by
orthodontic forces may lead to not only root resorption and iatrogenic damage to the periodontium
but also pulp reaction.1,34,35
The developmental stages of the tooth at the time of stimulation and the magnitude of orthodontic
force used is believed to be related to the response of the pulp. In addition, previous history of pulp
injuries or chronic pulp injuries, such as caries may also alter pulpal response.30
Thus far, numerous published studies have demonstrated that pulpal reactions to the orthodontic
forces include:
● Altered sensation to stimuli36
● Mild hyperemia36
● Pulpal calcifications/obliterations33,37
● In severe cases, permanent pulp damage with loss of vitality23, 28,38

Dr Raluca Baleanu 5
Similar to the process that initiate angiogenesis in wound healing39, OTM generates neurovascular
alterations in the pulp, producing the discharge of certain neurotransmitters that can determine the
cellular metabolism and influence the bloodflow.40
Rate of orthodontic tooth movement
The degree of tooth movement is limited by the rate of physiological change in the paradental tissues,
particularly the alveolar bone and the periodontal ligament.23,40,41,42
Schwarz et. al.43 assumed that the optimal force for tooth movement should be the force required to
produce a change in tissue pressure that approximates 20-26gm/cm2 of capillary pressure. “The
mechanical input that leads to the maximum rate of tooth movement with minimal irreversible damage
to roots, PDL, and alveolar bone” 1 is the current definition of ‘optimal force’. The mechanical input is
seen as a stimulus for a cellular response that aims to restore equilibrium by the remodeling of the
periodontal tissues.
Quinn and Yoshikawa49 originally outlined that there is a correlation between OTM and the extent of
force application.44,45,50 They stated that as the applied force to a tooth is increased, the rate of tooth
movement would also increase up to a certain point. The ‘optimal force’ is also known as the force that
generates the highest level of tooth movement. Optimal forces should not cause any side effects, while
producing the desired tooth movement. Currently there is no consensus on the optimal force levels as
it depends on multiple factors. Some suggested that an increase in force application raised the rate of
canine retraction.44 . However, Boester and Johnston45 found an ‘optimal force’ level for canine
retraction in their study, where forces beyond 140gms did not result in further increases in the rate of
canine retraction. Storey et al.46 studied the effect of various force levels on the rate of canine
retraction and suggested that the ‘optimal force’ value would be 150-200gms. Theoretically, under

Dr Raluca Baleanu 6
ideal conditions, it is possible for osteoclastic resorption to progress at a rate of 100μm/day, translating
to orthodontic tooth movement at a rate of 3mm/month.40
Research47 using a specially designed Drum Spring (without an arch wire) was able to achieve an
average rate of canine distalization of 1.648 +/- 0.576mm per month, with one subject showing
2.755mm/month. This was achieved with only a 50gm force. The level of tooth movement is more
plausible at 0.8-1.2mm/month in clinical practice.48
The relationship between force levels and optimal tooth movement was examined in a systematic
review,51 with no evidence regarding an ‘optimal force’ found. The authors suggested that the reasons
for this finding include:
● The fact that tooth movement can be divided into an Initial phase, Lag phase and Post-Lag
phase; still most studies only have a short experimental period, which includes only the first two
phases;
● The incapacity to calculate the diffusion of stress and strain in the periodontal ligament;
● The failure of studies to control the type of tooth movement performed. Most studies have
tipping tooth movements, which not only result in an uneven distribution of stress and strain,
but also result in an over-estimation of rates of tooth movement when measurements are
made at the crown level;
● Inter-individual variation.
Dr Raluca Baleanu 7
Repair of orthodontically induced inflammatory root resorption -OIIRR
Repair of orthodontically induced inflammatory root resorption appears through new cement
formation and re-organization of periodontal ligament. when active forces are removed.34 Several lines
of evidence established that the rate of root repair appears to increase with time. 52,53,54,55 Owman-Moll
et al.55 compared the reparative potential of OIIRR with the degree of resorption area following
different length of retention, using teeth that were extracted and examined histologically. They found
that following 7 days of retention, repair was 28%, compared to 75% repair following 86 days.
Repair was shown to slow down after day 35 to day 42 and remains at a stable level thereafter.55,56
Cheng et al.56investigated cementum repair following light or heavy orthodontic force application and 4
and 8 weeks of retention and concluded that there was a lot of individual variation in repair response.
The patients that had light forces had steady repair after 4 weeks, whereas in the group that had heavy
forces, the repair only started following 4 weeks of retention.
While Brudvik and Rygh described repair to initiate at the peripheral sites, it was also shown to start at
the base of the crater or from all directions.58,59,60
As signs of repair, at the periphery as well as the lacunae of the resorbed cementum, cementoblasts
with similar characteristics as during cementogenesis and fibroblasts, indicating repair of periodontal
ligament were observed.60,62

Dr Raluca Baleanu 8
It was also shown that the deposit of a fine coating of acellular afibrillar cementum (AAC) induces the
reparative activity. 61,63
Accelerated tooth movement
The 2015 AAO Economics of Orthodontics Survey, revealed a dramatic increase of orthodontic
treatments in adults. On average an orthodontist treated 41 adult patients in 1989 compared to 125
patients in 2014.64 Both adult and adolescent patients can benefit more from accelerated tooth
movement given that with long treatment durations, compliance and oral hygiene declines, creating
more unwanted side effects and . Furthermore, adult patients are more predisposed to periodontal
problems and other time related side effects.
The potential to accelerate OTM is supported by the fact that under ideal conditions, bone can be
resorbed as fast as 100um/day, which translates to orthodontic tooth movement at a rate of
3mm/month. This exceeds the efficiency achievable with any clinical method, indicating a considerable
gap between clinical proficiency and biologic potential (Roberts 1981).40
Clinicians around the globe have been exploring this biological potential aiming to minimize treatment
time, decrease adverse effects such as pain, discomfort, dental caries, and periodontal disease, and
minimize iatrogenic damage such as root resorption and elevated risk of white spot lesions.65,66,67,68
These acceleration methods have been broadly categorized as: Biological, Surgical and Device assisted
methods.29

Dr Raluca Baleanu 9
Biological Methods
There has been large amounts of research performed on the biological methods of accelerated tooth
movement. This was achieved through the use of medications and chemical mediators, manipulation of
selective mediators and hormones that are implicated in bone metabolism via enhanced osteoclastic
action and/or repressing osteoblasts.69
The administration of dihydroxy vitamin D3,70 parathyroid hormone,71 prostaglandin E2(PGE2),72
thyroid hormone,73 and RANKL (Receptor Activator of Nuclear Factor- ĸB ligand),74 osteocalcin,75
relaxin76 have been demonstrated to accelerate the rate of orthodontic tooth movement in animal
studies. It has been proven that other agents, such as fluoride,77 bisphosphonates,78 calcitonin,
corticosteroids,79 interleukin antagonists, anticancer drugs,80 trigger side effects that impact the cells
targeted by orthodontic forces.
Hence, biological approaches are not currently recommended due to their limited applicability and
efficacy, as well as health and safety related concerns.9,69,81
Surgical Methods
Surgically accelerated tooth movement has been practiced for over a century.50 Osteotomy was first
performed in the 1890s.50,53 In 1950, Köle82 described the use of corticotomy for the purpose of
accelerating the rate of tooth movement. Both techniques were not widely practiced owing to their
invasiveness.
Surgical approaches to accelerate OTM are based on the regional acceleratory phenomenon, or RAP
effect and was first proposed by Frost in 1983.83 The phenomenon describes the increased rate of bone
turnover and remodeling in response to localized trauma to bone. Frost also believed that the

Dr Raluca Baleanu 10
magnitude of noxious stimulus was proportional to the intensity of the RAP effect obtained. RAP effect
peaks at 1-2 months, and then reduces after 2-3 months as the density of bone increases. In general,
RAP effect lasts for 4 months duration.83
In 2001 Wilcko et al.51 also described the demineralization and remineralization procedure underlying
surgically assisted accelerated tooth movement as (RAP)-Regional Acceleratory Phenomenon,84 which
consisted of increased bone remodeling. The authors postulated that it is the increased rate of bone
metabolism which elevates the rate of OTM rather than a mere reduction in cortical resistance
following bone injuries.
To date, various surgical approaches of accelerated tooth movement have been proposed, which
include corticotomies, piezocision, micro-osteoperforations, periodontal ligament distraction,
dentoalveolar distraction and the surgery first approach.
Corticotomy
This surgical procedure involves cutting or perforating the cortical layer of bone without the extension
of the cuts into the medullary bone,56,82 to initiate RAP effect.83 Triggering RAP generates an increase
in osteoblastic and osteoclastic activity in the alveolar bone, that could provide up to 4- 6 months of
accelerated tooth movement.85 However, due to the temporary nature of the effect;86 the procedure
needs to be repeated for the continuation of this effect.
Köle82 first described the use of corticotomies for the purpose of accelerating the rate of tooth
movement in 1950. He speculated that the main resistance to tooth movement was the presence of
dense cortical bone around the teeth. The corticotomy procedure involves making full-length
osteotomy cuts on the buccal and lingual alveolar plates of cortical bone and movement of teeth with
the associated ‘blocks’ of bone 86.Cancellous bone was left intact, as this was believed to provide the

Dr Raluca Baleanu 11
necessary nutrients to the bone and teeth to prevent devitalization of teeth, injury to the
periodontium, as well as root resorption.
The method of corticotomy for OTM was refined by the Wilcko brothers applying their certified
‘Accelerated Osteogenic Orthodontics’ (AOO) technique, known later as the ‘Periodontally Accelerated
Osteogenic Orthodontics’ (PAOO), to reduce total treatment time to a quarter to one third that of
common non-extraction and extraction orthodontic therapies.87 The Accelerated Osteogenic
Orthodontics method relies on the development of a transient ‘localized demineralisation-
remineralisation phenomenon in the alveolar bone consistent with the wound healing pattern of the
Regional Acceleratory Phenomenon’.81
Animal88,89,90,91,92,93 and human88,94,95,96,97,9899 studies, consisting of clinical trials, case reports and case
series, have found that there has been an acceleration of tooth movement with corticotomy-facilitated
orthodontic therapy. The degree of acceleration of tooth movement varies widely in the studies, with
up to four times the rate of normal tooth movement in animals92 and two to three times in
humans.88,89,87,94,96,90,97,99,100,101 The variability is likely due to different study design parameters, such as
differences subject species (animals vs humans) and numbers, corticotomy procedure variations, force
magnitudes, types of tooth movement with differing activation/reactivation regimes, and durations of
force activation.
Gantes et al.102 performed a case series that tested the effects of corticotomies on tooth movement.
Five subjects had corticotomy procedures performed and each subject was compared to an age and
malocclusion matched control that, underwent concurrent orthodontic therapy. Treatment time was
reduced on average by 50%. Further, Aboul-Ela et al.96 performed a split mouth study in 13 adult
subjects, the corticotomy side of the mouth had a statistically significant rate of canine distalization

Dr Raluca Baleanu 12
that was double the control side during the first 2 months post-surgery. This reduced to 1.6 times
faster at the 3-month period and only 1.06 times faster by the 4-month period. Similarly, Sanjideh et
al.89 performed a split mouth animal study where the rate of tooth movement peaked at 22-25 days on
the corticotomy side, with the corticotomy peak being 85% greater than the control side. Both sides
then experienced a deceleration in the rate of tooth movement, such that there was no difference
between the corticotomy and control sides at 7-8 weeks. In the same study, the effects of one versus
two corticotomy procedures (separated by a 4-week period) were compared. The side with only one
corticotomy showed a decrease in the amount of tooth movement during the last few weeks of the
experimental period. The side that underwent a double corticotomy showed a steadier rate of tooth
movement throughout the 8-week experimental period. This also translated to maintenance of a
higher rate of tooth movement for a longer period of time. However, the differences between the one
and two corticotomy procedures were small and not considered clinically significant. In addition, Al-
Naoum, Hajeer and Al-Jundi103 found in their randomized clinical trial that the acceleration of tooth
movement varied between 2-4 times that of controls, with the fastest rate in the first 2 weeks post-
corticotomy. The rate of tooth movement decreased over the 12-week experimental period.
In terms of the complications, several pieces of literatures indicate that corticotomy-facilitated
orthodontic tooth movement yet does not increase the risk of unwanted sequelae when compared to
conventional orthodontic treatment. Specifically, there is no increased risk of adverse changes in
periodontal parameters,94,95,100,104,105, root resorption100,99,105,106,112,113 or tooth vitality issues.99,106,107
Further, Düker108 found that corticotomy accelerated tooth movement did not adversely affect the
pulp vitality or marginal periodontium. In addition, in a human split mouth study that aimed to assess
the effect of corticotomies on canine distalization with temporary anchorage devices, Aboul-Ela et al.96

Dr Raluca Baleanu 13
found that corticotomies did not adversely affect periodontal parameters in terms of plaque index,
probing depths, attachment loss or gingival recession.
With regard to root resorption, most studies have found that corticotomy-facilitated orthodontic
procedures do not increase the risk of root resorption when compared to conventional orthodontics.
Interestingly, several studies even found that corticotomy procedures resulted in less root resorption
when compared to conventional orthodontic treatment. Abbas and Hassan109 examined the effect of
corticotomy-facilitated orthodontics on root resorption through the use of Cone Beam-CTs. They found
that for the teeth adjacent to corticotomy, there was on average 0.6mm of root resorption, whilst for
the control teeth, there was 1.5mm of root resorption. This difference was statistically significant.
Another study100 also found that there was a reduction in root resorption in the corticotomy group
when compared to the controls, but the results of this finding were questionable. It is noteworthy that
none of these studies have reported the presence of iatrogenic root damage following corticotomy
surgical procedures.
Despite the promising findings from various studies, a systematic review concluded that “combining
conventional orthodontic treatment with corticotomy reduces the duration of orthodontic treatment
by accelerating tooth movement.110 However, most studies conducted on this topic involved high risk
of bias, therefore, the efficiency/safety ratio is not conclusive.
In addition, drawbacks associated with corticotomy have been reported, including damage to adjacent
vital structures, post-operative pain, swelling, infection and avascular necrosis.111
Piezocision
Piezocision is a variation of the corticotomy technique. 111,112,113 It is a minimal intrusive, flapless
method merging piezo-surgical cortical incisions with selective tunneling to facilitate bone or soft-

Dr Raluca Baleanu 14
tissue grafts. Piezoelectric cuts have a reduced risk of osteonecrosis when compared to corticotomies
as a result of the small size and high precision of the incisions.42
It was suggested that by selective piezocision cuts it is possible to alter the anchorage value of
teeth.101,111,114 The areas not affected by surgery have higher anchorage values because they are
uninfluenced by the demineralization process associated with RAP. A recent article115 described the use
of sequential or segmental piezocision, where selected areas of the arches or segments undergo
piezocision procedures at various planned times during the orthodontic treatment to achieve specific
goals.
The recommended indications for piezocision in terms of case selection include:111
● Rapid adult orthodontic treatment;
● Class I malocclusions with moderate/severe crowding (non-extraction);
● Deep bite correction;
● Some ½ unit Class II malocclusions;
● Rapid intrusion and extrusion of teeth;
● Simultaneous correction of osseous and mucogingival defects;
● Prevention of mucogingival defects.
Dibart et al.112 described the use of the piezocision tool without raising flaps as a more conservative
and less invasive form of corticotomy. The surgical procedure is carried out one week after placing
fixed appliances. Applying anesthesia locally, vertical interdental incisions are created under the
interdental papilla of the jaws, through the periosteum and, preferably, through the attached
gingiva.111,112 Afterwards to produce the cortical alveolar cuts of a 3mm depth to the vertical soft tissue
sections they use a piezo surgical blade. The soft tissue cut ‘tunneled’ is necessary in order to permit

Dr Raluca Baleanu 15
the fixing of bone grafting in areas with thin or no buccal cortical bone. This grafting procedure is said
to allow positive modification of the dental arch that will allow crowding correction without extraction.
While ungrafted areas do not need closure of the sections, the areas that are grafted demand closure
with sutures. Dibart claimed that the active treatment time on the cases was reduced by an average of
3-fold,112 which compared favorably to other forms of corticotomy-facilitated orthodontic
procedures.113
In a recent systematic review it was reported that there is some evidence, although weak, to support
that piezocision is a secure technique to increase OTM in the short term.46 In another recent clinical
trial it was reported that piezocision resulted in a reduction of 43% in treatment time with no
periodontal complications such as recession and increased pocket depth. However, scars were
observed in 50% of patients.44
Apart from scars, root resorption was also mentioned as a piezocision associated complication.
Patterson et al.114 performed a Micro-CT analysis which revealed that the teeth adjacent to the
piezocision cuts had a mean of 0.435 mm³ root resorption versus 0.133 mm³ seen in the control group.
In addition, 5 out of 28 teeth (17%) had iatrogenic root damage due to direct contact with the
piezocision blades. The authors also highlighted that even though the piezocision procedures were
carried out by a highly trained senior periodontic registrar with radiographic aids to assist with the
positioning of the incisions, damage still took place. Further studies focusing on the effects of different
cut lengths and depths should be investigated, given that these techniques were introduced for
patients with crowding.

Dr Raluca Baleanu 16
Micro-osteoperforations
Micro-osteoperforations (MOP) or alveolocentesis is the least extensive with regards to the amount of
local injury amongt the surgical methods of accelerated tooth movement. The technique involves
controlled micro-trauma of the alveolar bone without raising a mucoperiosteal flap. The philosophy in
achieving accelerated tooth movement is again an application of RAP effect, amplifying the expression
of inflammatory mediators that are usually expressed within OTM.116
A human study by Alikhani et al.97 proposed that three perforations by the “Propel” device through
gingiva into maxillary interproximal alveolar bone are enough to generate a regional acceleration of
bone modeling, significantly raising the amount of tooth movement by 2.3-fold. The authors also
observed a raise in the degree of the markers of inflammation in gingival crevicular fluid. However, that
study period lasted only 4 weeks and this research was carried out by the team that invented the
Propel device.
Other more recent studies on humans that showed increase in tooth movement mostly had short
durations of 4 weeks or repeated the procedure during space closure.117,118,119,120 Studies utilizing
different methods for MOP such as Propel and miniscrews, different number and depth/width
perforations with different durations have shown that MOPs did not create a clinically significant
difference in tooth movement.121,122,123,124,125,126
A recent meta-analysis evaluated the effect of micro-osteoperforations (MOPs) performed with Propel
and other mini-screws on the rate of tooth movement, pain, periodontal parameters and root
resorption and concluded that Propel device induced MOP’s do not produce significantly increased
tooth movement.127 Therefore, there is still no consensus regarding the effects of MOP and further
studies are needed.

Dr Raluca Baleanu 17
Periodontal ligament distraction and dentoalveolar distraction
Periodontal ligament distraction was first introduced by Liou and Huang.128 The authors were able to
distalise a canine by 6.5mm in a short period of 3 weeks and they recommend this technique being
utilized particularly in orthodontic treatment that involves first premolar extraction that has anterior
dental crowding. Following the procedure, minimal resorption of canine roots but no significant pain
was reported. An animal study 129 established that the rate of tooth movements is up to 1.2mm/week
when the teeth are moved into the new bone created by distraction osteogenezis.
In 2002 dentoalveolar distraction was described by Kişnişci et al. 130 They have used a rigid distraction
appliance which was applied to retract canines into premolar extraction spaces in a technique similar
to the periodontal ligament technique. They found that canine distraction was completed in a period of
8 to 12 days without anchorage loss (AL) and noticed no deficit in root length or vitality.130
However even though very fast canine distalization is accomplished with dentoalveolar distraction, it is
a very invasive technique and not preferred by clinicians and patients.131
Surgery first
The “surgery-first” theory is a team approach between surgeons and orthodontists for orthognathic
surgery.132 As opposed to conventional surgical approach, surgery first approach manages facial
esthetics before alignment and occlusion. Orthodontics in the surgery first approach is a post-operative
treatment to transfigure the transitional occlusion into a solid final occlusion.
One of the proposed advantages of surgery first approach is that patient’s chief complaint, dental
function and facial esthetics are improved in the beginning of treatment. Another added benefit of
Dr Raluca Baleanu 18
surgery first was shown that it reduced total treatment time to 1-1.5 years depending on the
complexity of the malocclusion.133
In the early days this approach had many issues, such as, postoperative occlusal instability leading to
serious problems in masticatory function and relapse.134 Currently, with the use of three-dimensional
(3D) imaging and simulation, and advances in skeletal anchor plates, an accurate treatment plan and
more predictable outcomes are possible.135
To date, the suggested criteria of malocclusion for surgery first approach includes well-aligned
dentition to mild crowding, flat to mild curve of Spee, normal to mild proclination/retroclination of
incisors, minimal tranverse discrepancy.133 In these patients with RAP, it was shown that during the
period 3-4 months following orthognatic surgery tooth movement is also much faster with the
transient increase in metabolic activity.136 Surgery first approach was also shown to reduce the number
of appointments patients needed to attend.137
Device assisted methods
Device assisted methods, aimed at accelerating tooth movement, trigger activity of the bone cells liable
for bone remodeling during orthodontic tooth movement, therefore enhancing the amount of OTM.138
Device assisted methods include direct electric currents, magnetic fields, pulsed electromagnetic fields,
vibration, low level laser therapy(LLLT), photobiomodulation (PBM), low intensity pulsed
ultrasound(LIPU).

Dr Raluca Baleanu 19
Electric current
The electrical energy has the capability to influence the depository as well as resorptive activities of
bone and cartilage cells by stimulating cell proliferation and metabolism,139,140 applied in the form of
direct currents or pulsed electromagnetic fields.141
The result of these interventions is considered to depend on biological agents, as well as the type and
environment of the cell and the electrical field applied. Davidovitch et al., applied 7V (volts) current to
canine gingiva in cats, and found a notable increase in the rate of OTM43 while others have published
less successful results.142 Pulsed electromagnetic fields
Pulsed electromagnetic fields (PEMF) were previously used to accelerate orthodontic tooth movement
by inducing electricity in bones and tissues. It does not involve using high voltages or implanted
electrodes, to avoid complications related to the use of direct stimulation.141
Bassett et al.141,146 were the first who studied this topic. The authors generated pulsed electromagnetic
fields by placing two coils in parallel manner.141,146 They found that the cellular activities are increased,
lag phase reduced, with increased bone deposition and resorption.144 Darendeliler et al. researched the
outcome of pulsed electromagnetic field vibration on the amount of tooth movement with coils and
magnets in rats as well as guinea pigs, and their results reflected that both intensified the rate of tooth
movement.143 The increase in rate of tooth movement was also demonstrated by several other
studies.144,145
Showkatbakhsh et al. performed a split mouth trial design that used a fixed acrylic device and applied
PEMF for eight hours to the canine tooth. They found that the rate of OTM was over 0.3mm/month for
the experimental group when compared to control. 147 Nevertheless, because of the difficulties in
clinical application, this method did not become popular.

Dr Raluca Baleanu 20
Vibration
Therapeutic vibration (VT) is possible to be conducted locally or on the entire human body and has
been investigated for application in medicine and dentistry approach. Vibration was observed to be an
impulse similar to an oscillatory motion149 that has the frequency-F, magnitude and amplitude-A, which
creates intensity. 150
Magnitude (grams; g): represents the extent of vibration which is conveyed as being a function of the
Terra gravitational force.
Amplitude (millimeters; mm): subject to the extent of the oscillatory motion.
Frequency (Hertz; Hz): subject to the number of oscillation cycles per one second.
It was postulated that the application of decreased magnitude, increased frequency vibration increases
the rate of tooth movement.151 This theory assumes that tooth movement is a consequence of
immediate reaction of the cells of the bone to mechanical stimulation. However, studies on long bones
show osteogenic effects of increased bone density but no resorption outcome.151
This postulation was derived from the Bone Bending hypothesis in which orthodontic forces produce
alteration of the crystalline formations into alveolar bone to generate a piezoelectric current, abetting
osteogenesis.152 Nevertheless, when continuous orthodontic forces are applied, piezoelectric currents
are not created, they are generated when stress is applied or released.153
At a fast rate over a long period, when vibrational forces are used and discharged it is possible for the
vibration to trigger piezoelectric charges caused by stress.153

Dr Raluca Baleanu 21
Therapeutic whole body vibration
Therapeutic whole-body vibration is used in the therapy of a particular condition like diabetes,
osteogenesis imperfecta, osteopenia and fibromyalgia,154,155,156,157,158 but is also recommended for use
in enhancing body function (balance, muscle power).159,160,161
In the 1970’s Nazarov was first to propose therapeutic whole body vibration in astronauts to decrease
the causes of the free gravity bone density and of the loss of muscle mass.162,163
Frost’s mechanostat theory is the basis for using vibration in therapeutic applications through which
the bone adjusts its strength to mechanical forces which are in general inflicted by muscle, in an
exposure-response relationship.164 Extensive research has been carried out on animals and humans to
appraise the outcome of therapeutic whole body vibration on the conservation or development of
muscle and the quality of the bones and strength and aspect for patients who cannot do upper level
exercises.165
Localised therapeutic vibration
The first use of localized therapeutic vibration (LTV) was restricted to application within medicine,
however, afterwards there was some interest in the use of vibration in the alteration of orthodontic
tooth movement.166 Vibration was thought to trigger stress-inducing piezoelectricity signals while
energies are enforced and discharged on a fast rate throughout an extended period.140
In 1979 the application of intermittent forces-induced piezoelectricity to achieve physiologic
orthodontic tooth movement was investigated by Shapiro et al.153
LTV is presumed to encourage the increase and separation of mesenchymal stem cells (MSCs) within
osteogenic cells and chondrocytes.167,168,169 Research done on animals showed the use of low

Dr Raluca Baleanu 22
frequency vibration produced a change in the levels of RANKL and OPG (Osteoprotegrin).169,170,171 The
numbers and the activity of the osteoclast are defined by the balance between OPG and RANKL.170
Studies in vitro showed a reduction in RANKL of up to 55%, suggesting the reduction in osteoclast
thereby impacting the bone and root remodeling cycles and facilitating the anabolic activity, after the
application of LTV.172
Vibration and tooth movement
Extensive studies have been performed on animals which have showed encouraging outcomes
following the application of vibration expressed an increase in the amount of tooth movement.
Darendeliler et al. in 2007 established that OTM, using coils and magnets, can be increased by pulsed
electromagnetic field vibration. The study was conducted on 7-week old Wistar rats, using low-
magnitude vibration, neodymium-iron-boron magnets and sentalloy closed coil springs, evaluating the
effects of high-frequency, low-magnitude vibration on OTM. The study concluded that vibration
stimulated tooth movement by exerting additional mechanical and magnetic forces on teeth.144
Nishimura et al. in 2008 also studied the use of vibration and perpetually changing frequency on root
resorption and amount of tooth movement in Wistar rats.173 It was found that a 15% raise in the
amount of tooth movement resulted when a 60 Hz, 1g vibration stimulus was administered to the
occlusal molar surfaces of rats for 8 minutes, once a week, for 21 days. It was reported that the use of
vibration increases the activation of the RANK-RANKL signaling pathways which intensifies the number
and activity of osteoclasts and stimulates the PDL.173
Kalajzic et al. 2014 used full-body vibration on a rodent model (one-week old Sprague Dawley) and
described the effects of lower frequency (30Hz) and higher magnitude vibration on OTM.174 In
contradiction to the outcomes of Darendeliler et al. and Nashimura et al., they reported that vibration

Dr Raluca Baleanu 23
decreases the amount of OTM and was correlated with elevated numbers among the apoptotic cells.
The differing reported effects of vibration can be linked to the heterogeneity of the study method,
which include the vibration parameter.
Takano-Yamamoto et al. conducted a study on rats (Wistar adults, more than 3 weeks old), evaluated
the outcomes of several vibration regimens on the amount of tooth movement, and they found that
the ideal condition for secondary vibration were 3g/70Hz for 3min., once per week.131 Nevertheless,
the theory concluded that when vibration was combined with static force applied to teeth, it stimulates
the alveolar bone resorption and accelerates the tooth movement via an increase of the osteoclast and
osteoclast genesis function.
Research conducted on rabbits using whole body vibration has revealed anabolic reactions at the
cranial suture following compressed forces at 5N and one cycle per second (1Hz).175
A literature review evaluated the implementation of forces to the upper jaw of ageing rabbits using
histomorphometric analysis.176 They concluded that, after using of each tensile strength and
compression forces, stimulation of the genes and the product of the genes accountable for sutural
increase appeared.
Human studies were also conducted with the first performed by Kriststabet et al. in 1986. The authors
emphasized that vibration at 50Hz for 1-6 min. each 2-3 days minimized the time required for tooth
movement of the teeth with 1.5-to 2-fold.177
OrthoAcel Technologies, the developer of AcceleDent, subsidized a randomized controlled trial that
measured directly in the patients’ mouths the amount of canine’s tooth movement, using calipers, and
found an increase in movement (0.37mm/4 weeks) in the experimental group when compared to the
control. They observed that vibration devices increase the amount of canines distalization throughout

Dr Raluca Baleanu 24
extraction and space closure.150 This publication had some limitations, such as conflict of interest and
potential for bias. Therefore, outcomes should be interpreted with caution.138
Conversely, several other human studies were unable to demonstrate any remarkable differences in
the amount of tooth movement and alignment.178,179 A randomized control trial concluded that
additional vibrational force had no effect on the amount of orthodontic tooth movement and
alignment149,178,179 or the pain experienced.149,179 The initial incisor irregularity was established to be
the determined element that influences the initial and the general amount of alignment.178
DiBiase et al. 2018 studied the results of vibration on orthodontic space closure in terms of treatment
time, in a parallel randomized clinical trial.176 The findings of his research were that there was no
difference in the amount of space closure, final occlusal aftereffect, treatment period or the number of
visits using vibration.
A recent Cochrane review138 evaluated the available literature on vibration and found only two articles
which matched the selection criteria.149,150 The authors emphasized that there was insufficient
evidence supporting the effectiveness of vibration devices to increase OTM movement. Although the
ability of the vibration to accelerate tooth movement was statistically significant, it was not clinically
significant.
Overall, evidence backing up the results of vibration on tooth movement is limited and low-quality.
Vibration and root resorption
Recent studies have proved that localized therapeutic vibration, not only does it increase the amount
of tooth movement,150,151 but also it decreases postoperative pain150,166 and root resorption.169,180

Dr Raluca Baleanu 25
In 2015, Yadav et al. assessed different vibration frequencies (5Hz, 10Hz, 20Hz) on rodent model and
noted different outcomes. They observed an important decline of the Receptor Activator of Nuclear
Factor- ĸB ligand and a consistent growth of the Osteoprotegrin, and the also noticed a reduced root
resorption (not statistically significant) when 20Hz low vibration is applied.169
Grove et al. in a split-mouth RCTs (randomized control trial), used forces (150g) and vibration (50Hz) on
the maxillary first premolars, over 4-week study period, and they found that vibration decreased the
total root resorption volume by 33% when compared to the control group.181
A number of publications on the contrast, found that when therapeutic vibration was applied, the
decrease in OIIRR is not statistically significant.180,182
In 2011, a split mouth experiment was performed to test the outcome of a vibration of 30Hz following
OTM on the maxillary premolars of 15 patients that experienced repair of orthodontically inflammatory
root resorption and no statistically significant differences were found between experimental and
control groups.181
In 2017, Takano-Yamamoto et al. observed no dissimilarities in OIIRR when vibration frequencies (58Hz,
70Hz, 268Hz) were used for 3 min., 6 min., 10 min. and 30 min. for 1-week period.183
DiBiase et al., in a randomized control trial using AcceleDent, found that after an average of 28 weeks
and 5 days, the mean OIIRR is 1.08 (mm).180 That is, the use of vibration did not reduce OIIRR of
maxillary central incisors during alignment phase.

Dr Raluca Baleanu 26
Low intensity pulsed ultrasound-LIPUS
Ultrasound is composed of acoustic pressure waves past the range of human hearing.184 Low intensity
pulsed ultrasound (LIPUS) is widely used in the field of medicine. It is used as a tool in diagnosis and
treatment. At low intensities ((0.5-50Mw/cm2) LIPUS is often used as a diagnostic tool, while an
increased power (0.2-100 W/cm2) produces heat energy, which is favorable for therapeutic purposes.
Animal research has discovered that LIPUS may also stimulate the number of osteoclasts and osteoclast
activity, as well as increasing the numbers of cells in the periodontal ligament, on both the tension and
compression sides.185
Direct comparison between the effects of LIPUS and low level laser therapy (LLLT) on orthodontic tooth
movement was researched by Mohamed M.J.A. et al.,186using gene expressions and histological
evaluation on rats. They divided the animals into four groups, in which the first group had diode laser,
second group LIPUS, third group a combination of LLLT and LIPUS, and the fourth group served as the
control. They highlighted the fact that when LLLT and LIPUS are combined, upregulation of tissue gene
expression was evident and bone remodeling was enhanced, resulting in an increase in the rate of
orthodontic tooth movement.
A meta-analysis concluded that LIPUS also enhanced bony healing, 187 and it was noted that human
periosteal cells can be stimulated to proliferate and evolve into cells with an Osteogenic cell lineage
through the use of LIPUS.187

Dr Raluca Baleanu 27
Low level laser therapy
Since the discovery of the ‘Rubby Laser’ by Maiman,188 studies have been done to introduce laser
technology in the area of dentistry.
Light Amplification by Stimulated Emission of Radiation known as “laser light “is different from normal
sunlight or daylight by its distinctive properties.
Laser light is:
1. synchronized – the light waves travel similar as the surrounding waves in the beam
2. coherent – they circulate in a one-way, well organized, collimated light beam
3. monochromatic – all waves are similar colored189
It has been shown that the use of soft laser synonym with cold laser broadly known as low-level laser
therapy (LLLT) is a non-invasive method with its effects limited to the target tissue.190 LLLT was utilized
in the late 1960s for wound healing and it also caused accelerated hair regrowth.191,192
The technique is based on the semiconductor diode device that uses laser wavelength, which are
assimilated mainly by tissue pigment (melanin) and hemoglobin.197 The suggested process requires the
stimulation of the cell metabolism near-infrared (NIR) or infrared light (IR) at a lower energy density.
The variables such as the quality, quantity, density of the light energy as well as the light source-power,
spot size, number and frequency of administration, administration period, and applied energy create
different effects on the tissues it is applied.194

Dr Raluca Baleanu 28
In the field of dentistry, LLLT has been used in procedures including aesthetic gingival recontouring,
soft tissue crown lengthening, exposure of impacted teeth, removal of inflamed and hypertrophic
tissue, frenectomies, and photo stimulation of aphthous and herpes lesions.195
Low level laser therapy and tooth movement
There are extensive studies on the effects of LLLT on bone remodeling, orthodontic tooth movement as
well as orthodontic pain.196,197,198 Some studies suggested that LLLT is effective in accelerating the rate
of orthodontic tooth movement since it increases the rate of bone remodeling.13,15,17
Application of Low-Level Laser Irradiation in animal198,199 and human clinical research199,200 has
demonstrated the potential for acceleration of tooth movement without increasing the risk of adverse
sequalae such as root resorption and alveolar bone resorption of supporting teeth. The mechanisms
behind Low Level Laser’s stimulatory activity are in the present unknown, but laser is thought to
accelerate metabolism in cells and in bone, increasing the rate of bone resorption as well as new bone
formation.199,200
The first human study done on humans to examine the effect of LLLT on orthodontic tooth movement
using a split-mouth design was performed by Cruz et al,201 in which they showed a 35% rise in the rate
of space closure compared with controls.
Youssef et al. 13 have similar findings in a study which investigated the rate of orthodontic tooth
movement using LLLT in 15 patients. They reported an increase in the tooth movement rate of
experimental LLLT groups compared with the controls. Kreisler et al.,202 in a vitro study, found that the
rate of proliferation of human periodontal ligament (hPDL) fibroblast using low level laser, increased
significantly up to 72 h after 1 dose. However, for the treatment to be effective it needs to be repeated

Dr Raluca Baleanu 29
more than once a week. Both Wu et al.203 and Walsh et al.204 found that the increased rates of hPDL
cells effects of low laser occurred at energy density up to 4j/cm2 whereas the inhibitory effects
occurred at higher energy. Thus, rates increased at day 3 but not observed at day 5 using 2 J/cm2
fluence. Lanzafame et al.,204 using a pressure ulcer model, tested the dose dependent effects of LLLT
on wound healing. Results demonstrated that even when the energy density was maintained (J/cm2),
alteration of the power density and exposure time produced different effects.
LLLT was used by Limpanichicul et al. and Doshi-Metha G. et al. with orthodontic force to accelerate
tooth movement on a human study. However, their findings were not aligned, varying from no
difference to a 30% rate increase.205,206
The use of LLLT to accelerate the amount of tooth movement on animals studies, noted a significant
increase rate between the experimental and control.30,41,43 Nevertheless, it has been suggested that
this was achieved due to accelerated bone remodeling over increased osteoblastic and osteoclastic cell
proliferation and function during tooth movement.
Goulart et al. 207 used LLLT in a dog study and revealed that when the LLLT was applied to the dental
tissue during space closure, it enhances the rate of tooth movement whereas higher rates levels have
been reported to be inhibitory.
Kawasaki et al.,198 showed an increased rate of tooth movement on the experimental rats group
exposed to LLLT versus the controls. Furthermore, they observed, on the tension side, a growth in the
rate of bone formation and cellular proliferation, as well as, on the pressure side an increased number
of osteoclasts on the pressure side.
Dr Raluca Baleanu 30
Low level laser therapy root resorption
Sousa et al. 17 studied the effects of LLLT on root resorption. Canine retraction was performed on 26
canines. Half of them were included in the experimental group and the other half served as controls.
There was no significant difference in root resorption between the experimental and control groups.
Ng et al. (2017)208 studied the effect of LLLT using a split-mouth design comparing the effects of
continuous and pulsed lasers with placebo laser on the contra-lateral sides to investigate differences in
root resorption crater volumes. They found that teeth exposed to LLLT had less total root resorption
than the placebo laser sides.
Low level laser therapy was administered by Vasconcelos et al.209 and in a recent study (2020) and
Yassin et al.,210 to evaluate the effects on root resorption on rats. However, their findings were
different, from no difference, to preventing or reducing orthodontics root resorption in addition to
accelerating the healing and the repair of OIIRR.
Altan et al.211 found that LLLT irradiation applied in combination with orthodontic forces, in rats, had
lower root resorption, as well as a significantly increased osteoblast and fibroblast numbers when
compared with controls group influenced by orthodontic force alone.
Multiple mechanisms behind the association of light energy from LLLT, cellular stimulation, and
negative effects of cells engaged in root repair and resorption, are not well known and may be related
to the relativity of the results. Moreover, there are some difference between rats and human samples
such as tissue density and size which may impact laser energy and penetration to the target tissue, and
nevertheless the cellular metabolism, and the rates of cementum formation may differ.212

Dr Raluca Baleanu 31
Low level laser therapy and pain
The effects of Low-laser therapy on orthodontic pain has also been investigated numerous
studies.196,213 They reported that LLLT relieve discomfort and also delays the pain from orthodontic
adjustment. A research done on 76 patients by Turhani et al.214 found that the pain reduction effect of
a single irradiation of LLLT following orthodontic banding lasted for an average of 30 hours. In a double
blinded randomized study12 on thirty-nine adults that had separators placed between their premolars
pain perception was investigated using Visual Analog Scale (VAS)for 5 successive days. Teeth irradiated
by LLLT had less pain compared to controls. In a meta-analysis that included studies using LLLT after
separator placement215 concluded that the analgesic effect was statistically significant at 6h, 1 day, 2
days and 3 days and not significant at 2h, 4 days and 5 days and suggested further studies are needed
due to the heterogeneity of results.
Photobiomodulation
Another therapy that has been in the focus of accelerated tooth movement studies is
photobiomodulation (PMB). Generally, approved therapeutic tools for photobiomodulation are known
as low level laser (LLL) or light-emitting diode (LED). Light is formation of electromagnetic radiation
(ER), which has a dual nature, viewed as both particles and waves, that exist on the electromagnetic
spectrum and is ranging from gamma rays to radio waves.216 The LED light beams are monochromatic
but not synchronized or coherent like lasers. LED light is not consistent therefore has fewer side effects
and can be safely applied to a large area of the body surface.217

Dr Raluca Baleanu 32
Photobiomodulation using laser
Some animal studies in the field of orthodontics have shown that laser-mediated photo biomodulation
notably raises the amount of orthodontic tooth movement relative to controls,15,198,207,218 due to
accelerate bone remodeling via increased osteoblastic and osteoclastic cell proliferation.
Laser-mediated PBM has also shown the potential to reduce pain related to orthodontic
adjustments.12, 159,176,219 The mechanism is thought to include a stabilization of membrane potential
and release of neurotransmitters associated with analgesia.220,221,222
First time when the photochemical interaction of low powered laser with biological tissues has been
mentioned as photostimulation, photobiomodulation, photobiostimulation and biostimulation, was in
the 1960s.223,224
Endre Mester in 1967 uncovered photobiomodulation, and he found that the irradiation of laser light
to the skin of shaved mice could accelerate hair growth.225 Nevertheless he also found that light
irradiation could enhance non-healing skin ulcers226,227 and stimulate wound healing,217in humans.
Photobiomodulation using LED
Depending on the light parameters used, PMB can generate both stimulatory and inhibitory
responses.213 It has been used for its beneficial effects in clinical practice in orthodontics, distraction
osteogenesis, methicillin-resistant Staphylococcus aureus-induced osteomyelitis, accelerating wound
healing and preventing cell death and tissue damage, improved blood circulation and to reduce pain
and inflammation.14
The biological mechanism that supports the therapeutic effects of PBM are not yet fully understood.190
It is suggested that PBM increases the blood supply through vasodilation, increased production of Nitric

Dr Raluca Baleanu 33
Oxide and other pro-inflammatory mediators and adenosine triphosphate (ATP ) production 228,229,230
and increased cellular metabolism.
Photobiomodulation and tooth movement
Gkantidis et al. in a meta-analysis and systematic review, compared nine trials on photobiomodulation
and laser, and found that there is some evidence that photobiomodulation accelerates tooth
movement.148
Kau et al. investigated the effects of PBM on alignment and showed that the experimental group had
more than double the rate of tooth movement compared with controls, using an extraoral light source
for a period of 20 to 30 minutes daily or 60 minutes a week, on 90 subjects of which 17 were
controls.231 However, there is again conflict of interest in this study as one of the researchers was a
financial stockholder in the company that produced the device and another was an employee,
therefore the results should be interpreted with caution.
Ekizer et al.232 in a randomized control trial found a statistically increased rate of tooth movement of
21% - 58% when canine retraction was performed after the removal of two upper first premolar teeth.
They measured the movement over three time points, one-month apart, utilizing digitized study
models. Another study applying an intraoral LED appliance on the rate of initial alignment, found a 54%
minimization in alignment period and 2.9-fold rise in the rate of tooth movement when compared with
controls (11 subjects were in the experimental group, 8 control).233
Photobiomodulation and root resorption
At present there are a limited number of studies that examining the effects of LED on orthodontic root
resorption.211,234,235

Dr Raluca Baleanu 34
Fonseca et al.235 investigated the effect of LED PBM on OIIRR on 25 Wistar rats over a 7 day period They
divided the rodents into four groups: force and light (1), no force, no light (2), no force (3), light force,
no light (4). Group four showed the highest amount of root resorption among all groups. The
irradiation group displayed a raised number of fibroblasts per unit of the periodontal ligament area, as
well as an increased density of capillaries. Hence there was a decreased amount of inflammation and
root resorption following the application of orthodontic forces, and an enhanced periodontal tissue.
Nimeri et al.236 applied an extraoral LED device on root resorption on 20 orthodontic patients with class
I malocclusion. LED was applied during the initial stage of the orthodontic treatment and all along the
space closure or completion of alignments. Results indicated a wide range of root resorption
determined on CBCT. Therefore, it was concluded that irradiation did not cause root resorption more
than ordinary notice in orthodontic treatments.236,237,238 However, no control group was included in the
study and treatment protocol was not mentioned.
Sambevski et al. in a split mouth randomized controlled trial investigated effects of PBM on maxillary
first premolar root resorption using a sham control device on the contralateral side following 4 weeks
of force application. They did not find any statistically significant difference in the amount of resorption
experienced by the PBM side in comparison to controls.239
More investigations with longer study durations and improved study designs are needed to draw sound
conclusions.

Dr Raluca Baleanu 35
Physiology of dental pulp and factors affecting pulp canal volume
Dental pulp has three main functions, which include maintaining the calcified tissue of the tooth,
responding to external stimuli in form of pain sensation, as well as maintaining the vitality of the
cellular contents.
The odontoblasts and the undifferentiated mesenchymal cells, which can differentiate into dentine-
forming cells, contributes to the repair and maintenance of the hard. As part of the aging process,
secondary dentine is formed by odontoblasts at the periphery of the pulp, at a rate of 0.4µm/day.240 It
has the same tubular arrangement as the primary dentine which was formed prior to tooth eruption.241
In response to irritants such as caries, dental treatment or attrition, reparative, reactionary dentine
sclerotic dentine or are formed, depending on the degree of the damage.241 Reactionary dentine was
formed by primary odontoblast in response to a slowly progressing caries lesion. It has a reduced
number of tubules with a mildly irregular structure. As the carious lesion becomes more noxious,
reparative dentine is deposited by dentine forming cells derived from fibroblasts in the cell-rich zone,
endothelial cells or pericytes of the blood vessels in response to tissue growth factor-b.242,243This layer
of dentine contains tubules that are highly irregular or even absent, reducing the permeability to the
irritants.241,244
The sensory property of the pulp forms a crucial part of the defense mechanism against inflammation,
thermal and mechanical trauma.245 The dental pulp is innervated by the maxillary and mandibular
divisions of the trigeminal nerve. Once the nerve endings are stimulated, all stimuli will be transported

Dr Raluca Baleanu 36
in A-delta, A- beta or C fiber to the brain where they are interpreted as pain regardless of their
nature.246For example, the proprioceptive function protects teeth from excessive occlusal
loading.247,248 In addition, pain sensation from a carious lesion would urge the patient to seek
treatment to prevent further damage of tooth substance. The same would not happen in root-treated
tooth unless the damage is substantial.
The dental pulp is highly vascularized, which is comparable to that of the brain and the tongue.249 The
microcirculation serves to apply oxygen and nutrients to pulpal cells, as well as removing metabolic
wastes. The capillaries in the pulp are innervated by the maxillary artery which branches off from the
external carotid artery, which provides a high blood flow of 40-50ml/min/100g.250The rate of blood
flow to the pulp is higher than the flow to organs such as skin and muscles at rest, indicating the high
metabolic rates of pulp cells and low compliance of pulp.251
Noxious stimulants such as caries, dental procedure or occlusal trauma trigger depending on the
severity of the damage the formation of reparative, reactionary dentine sclerotic dentine which reduce
the pulp canal volume.241
Pulp canal volume alteration by age, hormones and nutrition
• Age:
Secondary dentine accumulation252in the pulp cavity which occurs throughout the life as part of the
aging process resulting in the reduction of the pulp tissue volume 253,254,255,256and is formed by
odontoblasts at the periphery of the pulp, at a rate of 0.4µm/day240.

Dr Raluca Baleanu 37
● Hormones:
Research into estrogen deficiency done one rats conclude that the dentin-pulp of the incisors complex
is reduced compared to sham side. Hence the estrogen plays an important role in dentinogenesis257.
It has been reported that oestrogen deficit can cause menopause 258 also generates mineralization
damage and decrease regeneration function of the dentin-pulp complex.259
● Nutrition:
In a recent study done on tax concluded that the abrasive diet it is related to increase molar pulp
volume.260
The reaction of dental pulp to orthodontic force
Dental pulp is known as the “heart of the teeth“. It is an unmineralized viable tissue.23 If it gets affected
and not treated in time, oral sepsis may occur. The connection between orthodontic force application
and dental pulp tissue has been the subject of research in recent years.3,4,5
Proffit et al.3 described that light continuous forces have little or no effect on dental pulp. However,
several studies postulated that orthodontic tooth movement induce side effects on the dental pulp
tissue.1, 6,46 It creates inflammatory alterations, cellular injuries and circulatory variations to the dental
pulp.261. Clinical signs of pulp modifications include the following:
● pulp obliterations,49,50
● changes in perception to stimuli, mild pulp hyperemia 45

Dr Raluca Baleanu 38
● extreme cases: irreversible destruction with the damage of pulp vitality24, 47,48
Vascular pulp changes
The pulp is one of the most sensitive tissues in the body because to the absence of collateral
circulation. The blood flow and cellular metabolism of the pulp neurovascular system can be affected
by specific neuropeptides that are generated as a result of OTM.46
Rana et al. utilized the dental pulp tissues of rats and applied orthodontic force to establish the point at
which the highest apoptotic activity appears.262 They concluded that apoptotic activity occurred at the
highest rate 3 days following force application.
Another study done on rats evaluated the response of the blood vessels after the application of
orthodontic forces. They concluded that there was an important rise in the density of blood vessels
after six hours of force application in the experimental group compared to controls. Nevertheless, they
found that in day one and day three there was a minimum change and decrease in the density of blood
vessels between the experimental and control groups.263
A research done on rats, which studied polypeptide growth agents involved in the angiogenic response
of the dental pulp after application of orthodontic force, found that VEGF (vascular endothelial growth
factor), FGF-2 (fibroblast growth factor), TGF (beta transforming growth factors), and PDGF (platelet-
derived growth factor) had a major role in the angiogenic reply of the pulp. 52

Dr Raluca Baleanu 39
The connection between vascular modification and increased angiogenesis in the pulp through OTM
have been described in different studies. A study using laser analyzed the blood flow of the human
maxillary canine’s pulp through OTM and found that a decrease in the pulp blood flow started after
about 32 min. of force application, succeeded by a gradual increase of blood flow which lasts for 2
days.264 On average, blood flow returned to normal in 3 days.
A study done on human premolars receiving orthodontic forces assessed the levels of AST (aspartate
aminotransferase), which is an enzymatic marker showing that the cell is dead, and found that after a
week of orthodontic force application, the experimental premolars showed a rise in the level of AST
compared to controls.261 Derringer et al. used the pulp from human teeth extracted after OTM found
an increased number of micro-vessels in the pulp teeth compared to controls.262 Nevertheless,
polypeptide growth factors are able to diffuse and cause angiogenesis in other tissues, using the same
process comparable to wound healing.265 Overall, existing studies concluded that if the mechanical
challenge lies within the biological limits of the pulp’s healing potential, the dental pulp tissue has the
ability to adjust when orthodontic loading is applied.263
Factors influencing the pulpal response to orthodontic forces
The frequency and the amplitude of the dental pulp modifications can be affected if there is history of
trauma or caries. Furthermore, the biological results of orthodontic force on the dental pulp are
considered to have a connection to the developmental status of the tooth. The effect produced was
also proposed to be in proportion to the degree of the applied orthodontic force.46

Dr Raluca Baleanu 40
It has been stated that when force of higher amount and intrusive type is applied the pulp calcification
is increased.49,50
Adults and younger individuals have been observed to have a lag in cellular reactions and changes in
vascularization of the pulp succeeding orthodontic force administration.7 It was stated that when
orthodontic forces are applied the pulp respiratory rate is heightened with age46 an average of 27.4%.7
The increased respiratory rate of pulp cells is linked with higher dentinogenic activity.266 In addition,
teeth with closed apical foramen experience regression and/or swelling reaction of the dental pulp.
Teeth with incomplete apical development, though not protected to unfavorable consequences
experience less severe form of unwanted effects.46
A study analyzed dental pulp reactions of adults and adolescents after 1 month of moderate intrusive
force49. They discovered that, though no major histologic changes were noticed within the
experimental group, following 1 month of intrusive force in adults a severe inflammatory-related
histologic pulpal alteration may appear.
A number of studies have been reviewed to evaluate the different outcomes of tooth vitality with a
history of trauma when distinct orthodontic movements were applied.200,201,202 After receiving
orthodontic treatment, teeth with a record of trauma were at-risk of pulp necrosis (orthodontic
intrusion 10.4% with trauma, 267, 268 orthodontic extrusion 9.1% with trauma269), while on teeth with no
history of trauma, receiving orthodontic force, the risk is 0.5% (no trauma) and 1.6% (trauma with no
orthodontic procedure).

Dr Raluca Baleanu 41
Bauss et al. assessed the effects of trauma during orthodontic treatment and found that pulp necrosis
happened in 18.6% of the teeth if trauma happened during treatment, whereas trauma without
orthodontic treatment triggered tooth necrosis in only 1.6% of patients otherwise.270 Necrosis was
most common with extrusive, intrusive and lateral injuries.270
The results of pulpal modifications
Application of orthodontic force leads to an immediate change in the metabolism of the pulp cell. Over
time, the coronal and radicular pulp experiences a rise in irregular dentine deposition.271 The growth in
dystrophic mineralization could result in total obliteration of pulp canal (PCO).272
In general, inflammatory modifications after orthodontic loading are frequently thought to be
reversible, presuming that the pulp has not encountered prior abuse as well as challenges.46
Several studies have reported decrease in pulp volume preceding orthodontic loading.273,274 However,
other studies found no alterations.51 The first prospective study that evaluated the result of OTM on
the volume of dental pulp tissues, found a statistically important decrease in pulp volume in the
experimental group compared to controls.275 Lazzaretti et al. also discovered a notable rise in the
amount of pulp calcifications after orthodontic movement of the premolars,50 which was also
confirmed in another study.261
Teeth with total PCO is at greater probability of pulp problems throughout orthodontic treatment in
contrast to teeth that has incomplete or no obliterations.268

Dr Raluca Baleanu 42
A systematic review has indicated there is not enough scientific proof that orthodontic loading could
reduce the blood flow and create irreversible modification.277 They concluded that previous dental
trauma might be one of the risk factors to compromise the vitality pulp tissues.277
Overall, up to now there is no consensus regarding the pulp reaction and orthodontic loading;49,50, 210
due to the shortcomings, including short trial duration, paucity of randomization and control group,
usage of 2D radiography scans to investigate the volume of pulp changes.276
Vibration and dental pulp modifications
Thus far, little is known about the outcome of vibration on the dental pulp tissue. There was only one
animal study on this topic. In 1945 a study analyzed the aircraft vibration on animals.278 They applied an
amplitude of 0.05 inches on 2600 cycles/min., 8 hrs./day and for 6 days/week, over a 4-week
investigation. Histological evaluation revealed no difference in the dental pulp tissue, dentine, alveolar
periosteum and the bone of the teeth.
Low-Level Laser therapy and dental pulp modifications
Dominquez et al.263 were the first to investigate the histological changes in the human pulp tissue
during orthodontic tooth movement undergoing low laser therapy. They found an increased
vascularization which accelerates the pulp repair and a widening of the odontoblast layer which was

Dr Raluca Baleanu 43
exposed to LLLT versus the control group. Furthermore, they suggest that the pulp tissue has an
adaptive response and favored the repair from the initial injury produced by the orthodontic force.
Alsulaimani et al.,234 found an increased effect of LLLT on cemental modeling and repair, using
histologic and immunohistochemical methods in rats. They used a laser with a wavelength of 830-nm
on the exposed group for a period of two weeks and the other group served as control, no orthodontic
forces were applied. The volumetric hard tissue changes and root surface were analyzed with Micro-Ct.
Abi-Ramia BP. et al.,280 administered LLLT to study the microscopic pulpal response form
orthodontically induced tooth movement on rats. They use 45 rodents divided in 3 groups (1 – had
orthodontic tooth movement, 2–LLLT and orthodontic tooth movement, 3- served as control). In the
first and second groups, the pulpal response was more intense in the region of application of the force
or laser. The main finding was that LLLT applied currently with orthodontic force to accelerate tooth
movement, showed a quicker repair of the pulp tissue.
Photobiomodulation and dental pulp modifications
Photobiomodulation (PBM) can create both stimulatory and inhibitory responses determined by the
light parameters used.213 Currently, no published information is available in regards to the effects of
LED-PBM on pulp tissue. However, in vitro studies have been done to investigate the effects of laser-
mediated PBM on human dental pulp cells. Garrido et al. 238 investigated the effect of laser-mediated
PBM on extracellular matrix (ECM) of human dental pulp cell sheets (CSs). It was found that laser-
mediated PBM, especially those in lower energy density, improves the characteristics and the ECM in
CSs as well as fibronectin synthesis, but, when utilized at higher energy(5J/cm2) could cause destruction

Dr Raluca Baleanu 44
of some dental pulp steam cells in the cell sheet. Similarly, Ferreira et al. concluded that in the short-
term, PBM stimulates the proliferation of dental pulp stem cells.260 In addition, Vitor et al. suggested
that PBM stimulates the synthesis and secretion of angiogenic proteins by pulp fibroblasts from human
primary teeth.261

Dr Raluca Baleanu 45
Relevance of the research
Published studies investigating the effect of LLLT on tooth movement provided very limited information
on whether they imposed any side effects on dental pulp canal volume.Researchers attempted to
evaluate the impact of age252-256, nutrition260 and hormones257-259 on pulp volume but , there was no
published human study about the effect of LED PBM on pulp canal volume. Therefore, the aim of this
present study was to investigate the effects of LLLT and LED PBM on pulp canal volume of maxillary first
premolars undergoing orthodontic force application for 4 weeks using MicroCT.

Dr Raluca Baleanu 46
References
1. Krishnan V, Davidovitch Ze. Cellular, molecular, and tissue-level reactions to orthodontic force. American Journal of Orthodontics and Dentofacial Orthopaedics,2006.-469.e1-32. :Vol 129 (4).
2. Derringer KA, Jaggers DC, Linden RWA. Angiogenesis in Human Dental Pulp Following Orthodontic Tooth Movement. Dent Res, 1996. - 1761-1766 : Vol. 75(10).
4. Cohn SA ,Disuse atrophy of the periodontium in mice. Archives of Oral Biology, 1965.-909-19: Vol. 10(6).
5. Cohn SA ,Disuse atrophy of the periodontium in mice following partial loss of function. Archives of Oral Biology, 1966. - IN23, 103, IN25, 5-2, IN24, 4, IN26.5.-95-105: Vol.11(1)
6. Kaneko S Ohashi K, Soma K, Yanagishita M. Occlusal hypofunction causes changes of proteoglycan content in the rat periodontal ligament. Journal of Periodontal Research, 2001.- 9-17:Vol. 36(1).
7. Hamersky PA, Weimer AD, Taintor JF. The effect of orthodontic force application on the pulpal tissue respiration rate in the human premolar. Am J Orthod, 1980.– 368-78:Vol.77(4).
8. Ersahan S, Sabuncuoglu FA. Effects of magnitude of intrusive force on pulpal blood flow in maxillary molars. Am J Orthod Dentofacial Orthop, 2015. - 83-9 : Vol. 148.
9. Sabuncuoglu FA, Ersahan S. Changes in maxillary molar pulp blood flow during orthodontic intrusion. Aust Orthod J, 2014 Nov. - 152-60 : Vol. 30(2)
10. Choi YJ Kim KH, Lee KJ, Chung CJ, Park YC. Histomorphometric evaluation of maxillary molar roots and surrounding periodontium following molar intrusion in rats .Orthod Craniofac Res, 2015. - 12-20 : Vol. 18.
11. Dernaut LR, De Munk A. Apical root resorption of upper incisors caused by intrusive tooth movement. A radiographic study. Am J Orthod Dentofacial Orhop, 1986. - 321-6 : Vol. 90.
12. Lim HM, Lew KK, Tay DK. A clinical investigation of the efficacy of low-level laser therapy in reducing orthodontic post adjustment pain. Am J Orthod Dentofacial Orthop., 1995. - 614-22 : Vol. 108(6).
13. Youssef M,Ashkar S, Hamade E, Gutknecht N, Lampert F, Mir M. The effect of low-level laser therapy during orthodontic movement: a preliminary study. Lasers Med Sci., 2008. - 27-33 : Vol. 23(1).
14. Turhani D, Scheriau M, Kapral D, Benesch T, Jonke E, Bantleon HP. Pain relief by single low-level laser irradiation in orthodontic patients undergoing fixed appliance therapy. Am J Orthod Dentofacial Orthop, 2006. - 371-377 : Vol. 130.
15. Seifi M,Shafeei HA, Daneshdoost S, Mir M. Effects of two types of low-level laser wave lengths (850 and 630 nm) on the orthodontic tooth movements in rabbits Lasers Med Sci, 2007. - 261-264 : Vol. 22.
17. Sousa MV, Scanavini MA, Sannomiya EK, Velasco LG, Angelieri F. Influence of low-level laser on the speed of orthodontic tooth movement Photomedicine Laser Surgery, 2011. - 191-196 : Vol. 29.

Dr Raluca Baleanu 47
18. Ahmeida-Lopes L, Rigau J, Zangaro RA, Guidugli-Neto J, Jaeger MM. Comparison of the low level laser therapy effects on cultured human gingival fibroblasts proliferation using different irradiance and same fluence. Lasers Surg Med, 2001. - 577-588 : Vol. 5.
19. Eels JT, Wong-Riley MT, VerHoeve J, Henry M, Buchman EV et al. Mitochondrial signal transduction in accelerated wound and retinal healing by near infrared light therapy .Mitochondrion,2004.- 559-567 : Vol. 4.
20. Lowe AS, Walker MD, O'Byrne M, Baxter GD, Hirst DG. Effects of low intensity monochromatic light therapy(890nm) on a radiation impaired wound healing model in murine skin. Lasers Surg Med, 1998. - 291-298 : Vol. 23.
21. Hawkins D, Abrahamse H. Effect of multiple exposures of low-level laser therapy on the cellular responses of wounded human skin fibroblasts. Photomed Laser Surg, 2006. - 705-714 : Vol. 24.
22. Meikle MC. The tissue, cellular, and molecular regulation of orthodontic tooth movement: 100 years after Carl Sandstedt . Eur J Orthod, 2006. - 221-40 : Vol. 28.
23. Roberts-Harry D, Sandy J. Orthodontics. Part 11: Orthodontic tooth movement Br Dent J, 2004. - 391-4 : Vol. 196.
24. Thilander B, Rygh P, Reitan K. Tissue reactions in orthodontics. Orthodontics: Current Principles and Techniques. Elsevier, Philadelphia, PA. 2011 Jul 14:247-86.
25. Davidovitch Z, Nicolay OF, Ngan PW, Shanfield, JL. Neurotransmitters, cytokines and the control of alveolar bone remodelling in orthodontics. Dent Clin North Am, 1988. - 411-35 : Vol. 32.
26. Lerner UH. Osteoblasts, Osteoclasts and Osteocytes: Unveiling Their Intimate-Associated Responses to Applied Orthodontic Forces. Semin Orthodod: Elsevier, 2012. - 237-48 : Vol.18 (4).
27. Meeran N. Biological response at the cellular level within the periodontal ligament on application of orthodontic force - An update. Journal of Orthodontic Science, 2012. -2-10:Vol.1(1).
28. Yamaguchi M, K. Kasai. The Effects of Orthodontic Mechanics on the Dental Pulp. Seminars in Orthodontics, 2007.-272-280: Vol.13(4).
29. Nimeri G, et al. Acceleration of tooth movement during orthodontic treatment - a frontier in Orthodontics. [Progress in Orthodontics, 2013. - 1-8 : Vol. 14.
30. Reitan K. Clinical and histologic observations on tooth movement during and after orthodontic treatment. American Journal of Orthodontics, 1967.- 721 -745: Vol.53(10).
31. Rygh P. Ultrastructural changes in tension zones of rat molar periodontium incident to orthodontic tooth movement. American Journal of Orthodontics, 1976. 70(3): p. 269-281.
32. Proffit, William R. Contemporary Orthodontics . 5th ed. St. Louis, Mo: Elsevier/Mosby, 2014. Print.
33. Abtahi M, et al., The effect of intrusive orthodontic force on dental pulp of adults versus adolescents. Journal of Dental Research, 2016. 13(4): p. 367-372.
34. Reitan K. Initial tissue behavior during apical root resorption. The Angle Orthodontist, 1974. 44(1): p. 68-82.
35. Brezniak N, Wasserstein A. Orthodontically induced inflammatory root resorption. Part I: The basic science aspects. The Angle Orthodontist, 2002. 72(2): p. 175-179.

Dr Raluca Baleanu 48
36. Burnside RR, Sorenson FM, Buck DL. Electric vitality testing in orthodontic patients. The Angle Orthodontist, 1974. 44(3): p. 213-217
37. Rygh P. Orthodontic root resorption studied by electron microscopy. The Angle Orthodontist, 1977. 47(1): p. 1-16
38. Han G,et al. Pulp vitality and histologic changes in human dental pulp after the application of moderate and severe intrusive orthodontic forces. American Journal of Orthodontics and Dentofacial Orthopaedics, 2013. 144(4): p. 518.
39. Derringer KA, RWA. Linden. Vascular endothelial growth factor, fibroblast growth factor 2, platelet derived growth factor and transforming growth factor beta released in human dental pulp following orthodontic force. Archives of Oral Biology, 2004. 49(8): p. 631-641.
40. Roberts W, Goodwin Jr W, Heiner S. Cellular response to orthodontic force. Dent Clin North Am, 1981. - 3-17 : Vol. 25.
41. Roberts WE, Huma S, Roberts JA. Bone modelling: biomechanics, molecular mechanisms, and clinical perspectives. Semin Orthod: Elsevier, 2004. - 123-61.
42. Reitan K .Tissue behaviour during orthodontic tooth movement .Am J Orthod, 1960. - 881-900 : Vol. 46.
43. Schwarz AM .Tissue changes incident to orthodontic tooth movement. AM J Orthod, 1932. - Vol. 18.
44. Hixon E, Aitkian H, Callow G, McDonal H, Tacy R. Optimal force, differential force, and anchorage .Am J Orthod, 1969. - 437-57 : Vol. 55.
45. Boester C, Johnston LA. Clinical investigation of the concepts of differential and optimal force in canine retraction. Angle Orthod, 1974. - 113-19 : Vol. 44.
46. Storey E, Smith R. Force in orthodontics and its relation to tooth movement. Aust J Dent, 1952. - 11-8 : Vol. 56.
47. Darendeliler MA, Darendeliler H, Uner O.The drum spring (DS) retractor: a constant and continuous force for canine retraction.Eur J Orthod, 1997. - 115-30 : Vol. 19.
48. Buschang PH, Campbell PM, Ruso S Accelerating. Tooth Movement with Corticotomies: Is It Possible and Desirable? Semin Orthod, 2012. - 286-94 : Vol. 18.
49. Quinn RS, Ken Yoshikawa D. A reassessment of force magnitude in orthodontics. Am J Orthod, 1985. - 252-60 : Vol. 88.
50. Burstone CJ ,Groves M. Threshold and optimum force values for maxillary anterior tooth movement . J Dent Res, 1961. - 695 : Vol. 39.
51. Ren Y, Maltha JC, Kujipers-Jagtman AM. Optimum force magnitude for orthodontic tooth movement: a systematic literature review.Angle Orthod, 2003. - 86-92 : Vol. 73.
52. Owman-Moll P, Kurol J. The early reparative process of orthodontically induced root resorption in adolescents--location and type of tissue. Eur J Orthod 1998;20:727-732.
53. Langford SR, Sims MR. Root surface resorption, repair, and periodontal attachment following rapid maxillary expansion in man. Am J Orthod 1982;81:108-115.
54. Barber AF, Sims MR. Rapid maxillary expansion and external root resorption in man: a scanning electron microscope study. Am J Orthod 1981;79:630-652
55. Owman-Moll P, Kurol J, Lundgren D, . Repair of orthodontically induced root resorption in adolescents. Angle Orthod 1995;65:403-408.

Dr Raluca Baleanu 49
56. Vardimon AD, Graber TM, Pitaru S. Repair process of external root resorption subsequent to palatal expansion treatment. Am J Orthod Dentofacial Orthop 1993;103:120-130.
57. Cheng LL, Turk T, Elekdag-Turk S, Jones A, Petocz P, Darendeliler MA. Physical properties of root cementum: Part 13. Repair of root resorption 4 and 8 weeks after the application of continuous light and heavy forces for 4 weeks: A microcomputed-tomography study. Am J Orthod Dentofacial Orthop 2009;136 (3):320.e321-320.e310.
58. Brudvik P, Rygh P. Transition and determinants of orthodontic root resorption—repair sequence. Eur J Orthod 1995;17:177-188.
59. Brudvik P, Rygh P. The repair of orthodontic root resorption: an ultrastructural study. Eur J Orthod 1995;17:189-198.
60. Faltin, RM, et al. Ultrastructure of cementum and periodontal ligament after continuous intrusion in humans: a transmission electron microscopy study. European Journal of Orthodontics, 2001. 23(1): p. 35-49
61. Sismanidou C, Lindskog S. Spatial and temporal repair patterns of orthodontically induced surface resorption patches. Eur J Oral Sci 1995;103:292-298.
62. Lindskog S, Blomlöf L, Hammarström L. Cellular colonization of denuded root surfaces in vivo: cell morphology in dentin resorption and cementum repair. J Clin Periodontol 1987;14:390-395.
63. Henry JL, Weinmann JP. The pattern of resorption and repair of human cementum. Am J Dent Assoc 1951;42:270.
64. AAO Economics of orthodontics survey (2015) https://www.aaoinfo.org/news/2015/12/economics-orthodontics-survey-indicates-practice-management-data-mostly-stable-growth Google Scholar
65. Sameshima GT, PM Sinclair. Predicting and preventing root resorption. Am J Orthod and Dentofacial Orthopaedics, 2001. - 511-515 : Vol. 119.
66. Harris EF, WC Baker. Loss of root length and crestal bone height before and during treatment in adolescent and adult orthodontic patients Amer J Orthod and Dentofacial Orthop, 1990. - 463-469 : Vol. 98.
67. Geiger AM .Reducing white spot lesions in orthodontic populations with fluoride rinsing. Am J of Orthod and Dentofacial Orthop, 1992. - 403-407 : Vol. 101.
68. Naranjo A, et al. Changes in the subgingival microbiota and periodontal parameters before and 3 months after bracket placement. Am J of Orthod and Dentofacial Orthop, 2006. - 275.e17-275.e22 : Vol. 130.
69. Bartzela T, et al. Medication effects on the rate of orthodontic tooth movement: a systematic literature review. Orthod Dentofacial Orthop. - 2009. - 135.(1): 16-26.
70. Kawakami M, T Takano-Yamamoto. Local injection of 1,25-dihydroxyvitamin D3 enhanced bone formation for tooth stabilization after experimental tooth movement in rats. J Bone Miner Metab, 2004. - 541-546 : Vol. 22.
71. Soma S, et al. Effects of continuous infusion of PTH on experimental tooth movement in rats. J Bone Miner Res. 1999. - 546-554 : Vol. 14.
72. Yamasaki K, Shibata Y and Fukuhara T. The effect of prostaglandins on experimental tooth movement in monkeys (Macaca fuscata). J Dent Rest. - 1982. - 61. :1444-1446.
Dr Raluca Baleanu 50
73. Shirazi M, Dehpour AR and F Jafari. The effect of thyroid hormone on orthodontic tooth movement in rats. J Clin Pediatr Dent. – 1999; 23 : 259-264.
74. Kanzaki H, Chiba M, Arai K, Takahashi I, Haruyama N, Mitani H. Local RANKL gene transfer to the periodontal tissue accelerates orthodontic tooth movement. Gene Ther 2006;13:687-685
75. Hashimoto F, et al. Administration of osteocalcin accelerates orthodontic tooth movement induced by a closed coil spring in rats. Eur J Orthod. – 2001: 23: 16-26.
76. Madan MS, Liu ZJ, Gu GM, King GJ. Effects of human relaxing on orthodontic tooth movement and periodontal ligaments in rats. 2007;131:8. Am J Orthod 2007;
77. Hellsing E, Hammarstrom L. The effects of pregnancy and fluoride on orthodontic tooth movement in rats. Eur J Orthod. - 1991. - 13. - pp. 223-30.
78. Igar K et al. Inhibitory effect of the tropical administration of a bisphosphonate (risedronate) on root resorption incident to orthodontic tooth movement in rats. J Dent Res. - 1996. - 75. - pp. 1644-9.
79. Kalia S, Melsen B, Verna C. Tissue reaction to orthodontic tooth movement in acute and chronic corticosteroid treatment . Orthod Craniofac Res. - 2004. - 7. - pp. 26-34.
80. Krishnan V,Davidovitch Z .The effect of drugs on orthodontic tooth movement [Journal] // Orthod Craniofac. Res. - 2006. - 9. - pp. 163-71.
81. McGorray SP, et al. A randomized, placebo-controlled clinical trial on the effects of recombinant human relaxing on tooth movement and short-term stability. Am J Orthod Dentofacial Orthop. - 2012. - 141. - pp. 196-203.
82. Kole H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. J Surg Oral Med Oral Pathol, 1978. - 515-29 : Vol. 12.
83. Frost HM. The regional acceleratory phenomenon: a review; [Journal] // Henry Ford Hosp Med J. - 1983. – 31(1). - p. 3-9.
84. Fitzpatrick BN. Corticotomy. Aust Dent J, 1980. - 255-258 : Vol. 25. 85. Murphy KG, et al. Periodontal accelerated osteogenic orthodontics: a description of
the surgical technique. Oral Maxillofac Surg. - 2009. - 67. - pp. 2160-66. 86. Wilcko W, Ferguson D, Bouquot J, Wilcko M. Rapid orthodontic decrowding with
alveolar augmentation: case report. World J Orthod 2003; 4:197-205. 87. Wilcko WM, et al. Rapid orthodontics with alveolar reshaping: two case reports of
decrowding. Int J Periodontics Restorative Dent. - 2001. - 21. - pp. 9-19. 88. Lino S, et al. Acceleration of orthodontic tooth movement by alveolar corticotomy
in the dog. Am J Orthod Dentofacial Orhop, 2007. - 448 : Vol. 131. 89. Sanjideh PA, et al. Tooth movements in foxhounds after one or two alveolar
Corticotomies . Eur J Orthod, 2010. - 106-13 : Vol. 32. 90. Mostafa YA, Mohamed Salah Fayed M, Mehanni S, ElBokle NN, Heider AM.
Comparison of corticotomy-facilitated vs standard tooth-movement techniques in dogs with miniscrews as anchor units. Am J Orthod Dentofacial Orthop 2009; 136:570-77.
91. Teng GY, Liou EJ. Interdental osteotomies induce regional acceleratory phenomenon and accelerate orthodontic tooth movement. J Oral Maxillofac Surg 2014; 72:19-29.
92. Cho KW, Cho SW, Oh CO, Ryu YK, Ohshima H, Jung HS. The effect of cortical activation on orthodontic tooth movement. Oral Dis 2007; 13:314-19.

Dr Raluca Baleanu 51
93. Baloul SS, Gerstenfeld LC, Morgan EF, Carvalho RS, Van Dyke TE, Kantarci A. Mechanism of action and morphologic changes in the alveolar bone in response to selective alveolar decortication–facilitated tooth movement. Am J Orthod Dentofacial Orthop 2011;139: S83-S101.
94. Bhattacharya P, Bhattacharya H, Anjum A, Bhandari R, Agarwal DK, Gupta A et al. Assessment of Corticotomy Facilitated Tooth Movement.2014;8(10):ZC26-30.
95. Fischer TJ. Orthodontic treatment acceleration with corticotomy-assisted exposure of palatially impacted canines. Angle Orthod 2007; 77:417-20.
96. Aboul-Ela SMBE-D, El-Beialy AR, El-Sayed KMF, Selim EMN, El-Mangoury NH, Mostafa YA. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am J Orthod Dentofacial Orthop 2011; 139:252-59.
97. Alikhani M, Raptis M, Zoldan B, Sangsuwon C, Lee YB, Alyami B et al. Effect of micro-osteoperforations on the rate of tooth movement. Am J Orthod Dentofacial Orthop 2013; 144:639-48.
98. Suya H. Corticotomy in orthodontics. In: Hosl E, Baldauf A, editors. Mechanical and biological basics in orthodontic therapy. Heidelberg, Germany: Huthig Buch Verlag; 1991. p. 207-26.
99. Sakthi SV, Vikraman B, Shobana VR, Iyer SK, Krishnaswamy NR. Corticotomy-assisted retraction: an outcome assessment. Indian J Dent Res 2014; 25:748-54.
100. Shoreibah EA, Salama AE, Attia MS, Abu-Seida SM. Corticotomy-facilitated orthodontics in adults using a further modified technique. Journal Int Acad Periodontol 2012; 14:97-104.
101. Wu J Jiang JH, Xu L, Liang C, Bai Y, Zou W. A pilot clinical study of Class III surgical patients facilitated by improved accelerated osteogenic orthodontic treatments. Angle Orthod. 2015;85:616-24.
102. Gantes B, Rathbun E, Anholm M. Effects on the periodontium following corticotomy-facilitated orthodontics. Case reports. J Periodontol 1990; 61:234-8.
103. Al-Naoum F, Hajeer MY, Al-Jundi A. Does alveolar corticotomy accelerate orthodontic tooth movement when retracting upper canines? A split-mouth design randomized controlled trial. J Oral Maxillofac Surg 2014; 72:1880-9.
104. Abbas NH, Sabet NE, Hassan IT. The effect of using Piezocision technique in orthodontic tooth movement on the periodontal condition. Egypt Dent J 2011; 57:3047.
105. Shoreibah EA, Ibrahim SA, Attia MS, Diab MM. Clinical and radiographic evaluation of bone grafting in corticotomy-facilitated orthodontics in adults. Journal Int Acad Periodontol 2012; 14:105-13.
106. Hernandez-Alfaro F, Guijarro-Martinez R. Endoscopically assisted tunnel approach for minimally invasive Corticotomies: a preliminary report. J Periodontol 2012; 83:574-80. doi: 10.1902/jop.2011.110233. Epub 2011 Sep 26.
107. Abed SS, Al-Bustani AI. Corticotomy assisted orthodontic canine retraction. J Bagh College Dentistry 2013; 25:160-66.
108. Düker J. Experimental animal research into segmental alveolar movement after corticotomy. J Maxillofac Surg 1975; 3:81-84.
109. Abbas NH, Sabet NE, Hassan IT. Effect of corticotomy - facilitated orthodontics on root resorption. Egypt Dent J 2011; 57:3039-45.

Dr Raluca Baleanu 52
110. Fernández-Ferrer L, et al. Corticotomies as a surgical procedure to accelerate tooth movement during orthodontic treatment: A systematic review. Med Oral Patol Oral Cir Bucal. - 2016. - 21. - pp. 703-712.
111. Dibart S , JP Dibart. Practical Osseous Surgery in periodontics and implant dentistry. West Sussex : John Wiley & Sons, 2011.
112. Dibart S, Sebaoun JD, J. Surmenian. Piezocision: a minimally invasive, periodontally accelerated orthodontic tooth movement procedure. [Journal] // Compend Contin Educ Dent. - 2009. - 30. - p. 342.
113. Dibart S et al. Rapid treatment of class II malocclusion with Piezocision: two case reports .Int J Periodontics Restorative Dent. - 2010. - 30. - p. 487.
114. Patterson BM Dalci O, Papadopoulou AK, Madukuri S, Mahon J, Petocz P and et.al. Effect of Piezocision on root resorption associated with orthodontic force: A microcomputed tomography study. Am J Orthod Dentofacial Orthop. - 2017. - 151. - pp. 53-62.
115. Kaeser El, Dibart S ,Sequential. Piezocision: a novel approach to accelerated orthodontic treatment .Am J Orthod Dentofacial Orthop. - 2013. - 144. - pp. 879-89.
116. Alikhani M Alansari S, Sangsuwon C, Alikhani M, Chou MY, Alyami B, et al. Micro-osteoperforations: Minimally invasive accelerated tooth movement.Semin Orthod. - 2015. - 21. - pp. 162-169
117 Attri S, Mittal R, Batra P, Sonar S, Sharma K, Raghavan S et al. Comparison of rate of tooth movement and pain perception during accelerated tooth movement associated with conventional fixed appliances with micro-osteoperforations–a randomised controlled trial. Journal of orthodontics 2018;45:225-233.
118 Feizbakhsh M, Zandian D, Heidarpour M, Farhad SZ, Fallahi HR. The use of micro-osteoperforation concept for accelerating differential tooth movement. Journal of the World Federation of Orthodontists 2018;7:56-60.
119 Kundi I, Alam MK, Shaheed S. Micro-osteo perforation effects as an intervention on canine retraction. The Saudi Dental Journal 2020;32:15-20.
120 Haliloglu-Ozkan T, Arici N, Arici S. In-vivo effects of flapless osteopuncture-facilitated tooth movement in the maxilla and the mandible. Journal of Clinical and Experimental Dentistry 2018;10:e761.
121 Fattori L, Sendyk M, de Paiva JB, Normando D, Neto JR. Micro-osteoperforation effectiveness on tooth movement rate and impact on oral health related quality of life: A randomized clinical trial. Angle Orthod (2020) 90 (5): 640–647.
122 Babanouri N, Ajami S, Salehi P. Effect of mini-screw-facilitated micro-osteoperforation on the rate of orthodontic tooth movement: a single-center, split-mouth, randomized, controlled trial. Progress in Orthodontics 2020;21:1-10.
123. Sivarajan S, Doss JG, Papageorgiou SN, Cobourne MT, Wey MC. Mini-implant supported canine retraction with micro-osteoperforation: A split-mouth randomized clinical trial. Angle Orthod. 2019;89(2):183-9.
124. Aboalnaga AA, Salah Fayed MM, El-Ashmawi NA, Soliman SA. Effect of micro-osteoperforation on the rate of canine retraction: a split-mouth randomized controlled trial. Prog Orthod. 2019;20(1):21.
125. Alkebsi A, Al-Maaitah E, Al-Shorman H, Abu Alhaija E. Three-dimensional assessment of the effect of micro-osteoperforations on the rate of tooth movement during canine retraction in adults with Class II malocclusion: A

Dr Raluca Baleanu 53
randomized controlled clinical trial. Am J Orthod Dentofacial Orthop. 2018;153(6):771-85.
126. Alqadasi B, Aldhorae K, Halboub E, Mahgoub N, Alnasri A, Assiry A, et al. The Effectiveness of Micro-osteoperforations during Canine Retraction: A Three-dimensional Randomized Clinical Trial. J Int Soc Prev Community Dent. 2019;9(6):637-45.
127 Dos Santos CCO, Mecenas P, de Castro Aragón MLS, Normando D. Effects of micro-osteoperforations performed with Propel system on tooth movement, pain/quality of life, anchorage loss, and root resorption: a systematic review and meta-analysis. Progress in orthodontics 2020;21:1-15.
128. Liou EJ, Huang CS. Rapid canine retraction through distraction of the periodontal ligament. Am J Orthod Dentofacial Orthop 1998;114:372-82.
129. Liou EJ-W, Figueroa AA, Polley JW. Rapid orthodontic tooth movement into newly distracted bone after mandibular distraction osteogenesis in a canine model. Am J Orthod Dentofacial Orthop 2000;117:391-98.
130. Kişnişci RS, Işeri H, Tüz HH, Altug AT. Dentoalveolar distraction osteogenesis for rapid orthodontic canine retraction. Journal of Oral and Maxillofacial Surgery. 2002;60(4):389-394.
131. Kharkar VR, Kotrashetti SM, Kulkarni P. Comparative evaluation of dento-alveolar distraction and periodontal distraction assisted rapid retraction of the maxillary canine: A pilot study. International Journal of Oral and Maxillofacial Surgery. 2010;39(11):1074-1109.
132. Hernández-Alfaro F, Guijarro-Martínez R, Molina-Coral A et al.(2011) “Surgery first” in bimaxillary orthognathic surgery. J Oral Maxillofac Surg 69:e201–e207.
133. Liou EJ, Chen PH, Wang YC, Yu CC, Huang CS, Chen YR. Surgery-first accelerated orthognathic surgery: Orthodontic guidelines and setup for model surgery. J Oral Maxillofac Surg. 2011;69:771–80.
134. Bell WH, Creekmore TD (1973). Surgical-orthodontic correction of mandibular prognathism. Am J Orthod 63:256–270.
135 Lee YC, Sohn HB, Kim SK, Bae OY, Lee JH (2015). A novel method for the management of proximal segment using computer assisted simulation surgery: correct condyle head positioning and better proximal segment placement. Maxillofac Plast Reconstr Surg.2015; 37:21.
136 Liou EJ, Chen PH, Wang YC, Yu CC, Huang CS, Chen YR. Surgery-first accelerated orthognathic surgery: postoperative rapid orthodontic tooth movement. J Oral Maxillofac Surg. 2011 Mar;69(3):781-5.
137 Uribe F, Adabi S, Janakiraman N, et al. Treatment duration and factors associated with the surgery-first approach: a two-center study. Prog Orthod. 2015;16:29.
138.
El-Angbawi A, et al. Non-surgical adjunctive interventions for accelerating tooth movement in patients undergoing fixed orthodontic treatment. The Cochrane Database of Systematic Reviews 2015(11): p. CD010887.
139. Norton LA, Rodan GA, Bourret LA . Epiphyseal cartilage cAMP changes produced by electrical and mechanical perturbations. Clinical Orthopaedics and Related Research, 1977(124): p. 59-68.
140. Martin RB, Gutman W. The effect of electric fields on osteoporosis of disuse. Calcified Tissue Research, 1978. 25(1): p. 23-27.

Dr Raluca Baleanu 54
141. Stark TM, Sinclair PM. Effect of pulsed electromagnetic fields on orthodontic tooth movement. American Journal of Orthodontics & Dentofacial Orthopedics, 1987. 91(2): p. 91-104.
142. Beeson DC, Johnston LE, Wisotzky J. Effect of constant currents on orthodontic tooth movement in the cat. Journal of dental research, 1975. 54(2): p. 251
143. Miles P. Accelerated orthodontic treatment - what's the evidence? Australian Dental Journal 2017; 62:63-70.
144. Darendeliler MA, Sinclair PM, Kusy RP. The effects of samarium-cobalt magnets and pulsed electromagnetic fields on tooth movement. Am J Orthod Dentofacial Orthop 1995;107:578-88.
145. Sakata M, Yamamoto Y, Imamura N, Nakata S, Nakasima A. The effects of a static magnetic field on orthodontic tooth movement. J Orthod 2008; 35:249-254.
146. Bassett CA, Pilla AA, Pawluk RJ. A non-operative salvage of surgically-resistant pseudarthroses and non-unions by pulsing electromagnetic fields. A preliminary report. Clinical orthopaedics and related research, 1977(124): p. 128-143.
147. Showkatbakhsh R, Jamilian A, Showkatbakhsh M. The effect of pulsed electromagnetic fields on the acceleration of tooth movement. World Journal of Orthodontics 2010. 11(4): p. e52-6.
148. Gkantidis N, et al. Effectiveness of non-conventional methods for accelerated orthodontic tooth movement: A systematic review and meta-analysis. Journal of Dentistry, 2014. 42(10): p. 1300-1319.
149. Miles P, Smith H, Weyant R, Rinchuse DJ. The effects of a vibrational appliance on tooth movement and patient discomfort: A prospective randomized clinical trial. Australian Orthodontic Journal 2012;28:213-218.
150. Pavlin D, Anthony R, Raj V, Gakunga PT. Cyclic loading (vibration) accelerates tooth movement in orthodontic patients: A double-blind, randomized controlled trial. Seminars in Orthodontics 2015;21:187-194.
151 Alansari S, Sangsuwon C, Vongthongleur T, Kwal R, Teo Mc, Lee YB et al. Biological principles behind accelerated tooth movement. Seminars in Orthodontics 2015; 21:151-161.
152. Grimm FM. Bone bending, a feature of orthodontic tooth movement [Journal]. - [s.l.]: AMJ, 1972. - Vol. 62. - 384-93.
153. Shapiro E, Roeber FW, Klempner LS. Orthodontic movement using pulsating force-induced piezoelectricity. American Journal of Orthodontics 1979; 76:59-66.
154. Rubin C, et al. Anabolism Low mechanical signals strengthen long bones. Nature, 2001. 412(6847): p. 603-604.
155. Rubin C, et al. Prevention of Postmenopausal Bone Loss by a Low-Magnitude, High-Frequency Mechanical Stimuli: A Clinical Trial Assessing Compliance, Efficacy, and Safety. Journal of Bone and Mineral Research, 2004. 19(3): p. 343-351.
156. Gilsanz V, et al. Low-Level, High-Frequency Mechanical Signals Enhance Musculoskeletal Development of Young Women with Low BMD. Journal of Bone and Mineral Research, 2006. 21(9): p. 1464-1474.
157. Ward K, et al. Low Magnitude Mechanical Loading Is Osteogenic in Children with Disabling Conditions. Journal of Bone and Mineral Research, 2004. 19(3): p. 360-369.
Dr Raluca Baleanu 55
158. Collado-Mateo D, et al. Effects of Whole-Body Vibration Therapy in Patients with Fibromyalgia: A Systematic Literature Review. Evidence - Based Complementary and Alternative Medicine, 2015. 2015: p. 1-11.
159. Ritzmann R, et al. Whole body vibration training--improving balance control and muscle endurance. PloS one, 2014. 9(2): p. e89905.
160. Ko MC, et al. Whole-body vibration training improves balance control and sit-to-stand performance among middle-aged and older adults: a pilot randomized controlled trial. European Review of Aging and Physical Activity, 2017. 14(1)
161. Ebersbach G, et al. Whole body vibration versus conventional physiotherapy to improve balance and gait in Parkinson's disease. Archives of Physical Medicine and Rehabilitation, 2008. 89(3): p. 399-403.
162. Gojanovic B,et al. Physiological Response to Whole-Body Vibration in Athletes and Sedentary Subjects. Physiological Research, 2014. 63(6): p. 779.
163. Nazarov V, Spivak G. Development of athlete's strength abilities by means of biomechanical stimulation method. Theory and Practice of Physical Culture, 1985. 12: p. 445-450.
164. Frost, HM. Bone "mass" and the "mechanostat": a proposal. The Anatomical Record, 1987. 219(1): p. 1.
165. Thompson WR, Yen SS, Rubin J. Vibration therapy: clinical applications in bone. Current Opinion in Endocrinology, Diabetes, and Obesity, 2014. 21(6): p. 447-453.
166. Bowman SJ. The effect of vibration on the rate of leveling and alignment. Journal of Clinical Orthodontics, 2014. 48(11): p. 678.
167. Zhang C,et al. Effects of mechanical vibration on proliferation and osteogenic differentiation of human periodontal ligament stem cells. Archives of Oral Biology, 2012. 57(10): p. 1395-1407.
168. Zhang C, et al. Influence of different intensities of vibration on proliferation and differentiation of human periodontal ligament stem cells. Archives of Medical Science, 2015. 11(3): p. 638-646.
169. Yadav S, et al. The effect of mechanical vibration on orthodontically induced root resorption. The Angle orthodontist, 2016. 86(5): p. 740-745.
170. Lau E, et al. Effect of low-magnitude, high-frequency vibration on osteocytes in the regulation of osteoclasts. Bone, 2010. 46(6): p. 1508-1515.
171. Lacey DL, et al. Osteoprotegerin Ligand Is a Cytokine that Regulates Osteoclast Differentiation and Activation. Cell, 1998. 93(2): p. 165-176.
172. WIlcko MT, et al. Accelerated osteogenic orthodontics technique: a 1-stage surgically facilitated rapid orthodontic technique with alveolar augmentation [Journal]. - [s.l.]: J Oral Maxillofac Surg, 2009. - 2149-59 : Vol. 67.
173. Nishimura M, Chiba M, Ohashi T, Sato M, Shimizu Y, Igarashi K et al. Periodontal tissue activation by vibration: Intermittent stimulation by resonance vibration accelerates experimental tooth movement in rats. Am J Orthod Dentofacial Orthop 2008;133:572-83
174. Kalajzic Z, et al. Effect of cyclical forces on the periodontal ligament and alveolar bone remodeling during orthodontic tooth movement. The Angle Orthodontist, 2014. 84(2): p. 297-303.

Dr Raluca Baleanu 56
175. Kopher RA, Mao JJ. Suture Growth Modulated by the Oscillatory Component of Micromechanical Strain. Journal of Bone and Mineral Research, 2003. 18(3): p. 521-528.
176. DiBiase AT, et al. Effects of supplemental vibrational force on space closure, treatment duration, and occlusal outcome: A multicenter randomized clinical trial. American Journal of Orthodontics and Dentofacial Orthopedics, 2018. 153(4): p. 469-490.
177. Krishtab SI, Doroshenko SI, Liutik GI. Use of vibratory action on the teeth to accelerate orthodontic treatment. Stomatologiia, 1986. 65(3): p. 61.
178. Woodhouse NR, DiBiase AT, Johnson N, Slipper C, Grant J, Alsaleh M et al. Supplemental vibrational force during orthodontic alignment: a randomized trial. J Dent Res 2015; 94:682-689.
179. Miles P, Fisher E. Assessment of the changes in arch perimeter and irregularity in the mandibular arch during initial alignment with the AcceleDent Aura appliance vs no appliance in adolescents: A single-blind randomized clinical trial. Am J Orthod Dentofacial Orthop 2016; 150:928-936.
180. DiBiase AT, et al. Effect of supplemental vibrational force on orthodontically induced inflammatory root resorption: A multicenter randomized clinical trial. American Journal of Orthodontics and Dentofacial Orthopedics, 2016. 150(6): p. 918-927.
181. Grove J. The Effect Of Mechanical Vibration On Root Resorption Associated With Orthodontic Force: A Micro-CT Study [Thesis], in Faculty of Dentistry. 2011, University of Sydney.
182. Tan D. The effect of mechanical vibration (Acceledent) on root resorption and tooth movement after application of orthodontic force. A micro−CT study., in Faculty of Dentistry. 2011, University of Sydney.
183. Takano-Yamamoto T, et al. Synergistic acceleration of experimental tooth movement by supplementary high-frequency vibration applied with a static force in rats. Scientific Reports 2017. 7: p. 1-14.
184. Kristiansen TK, Ryaby JP, McCabe J, Frey JJ, Roe LR. Accelerated healing of distal radial fractures with the use of specific, low-intensity ultrasound. A multicenter, prospective, randomized, double-blind, placebo-controlled study. J Bone Joint Surg Am. 1997;79(7):961-973.
185. El-Bialy T, Lam B, Aldaghreer S, Sloan A. The effect of low intensity pulsed ultrasound in a 3D ex vivo orthodontic model. J Dent 2011;39:693-99.
186. Alazzawi MMJ, Husein A, Alam MK, et al. Effect of low level laser and low intensity pulsed ultrasound therapy on bone remodeling during orthodontic tooth movement in rats. Prog Orthod. 2018;19(1):10. Published 2018 Apr 16.
187. Leung K, Cheung W, Zhang C, Lee K, Lo H. Low intensity pulsed ultrasound stimulates osteogenic activity of human periosteal cells. Clin Orthop Relat Res 2004; 418:253-59.
188. Maiman TH. Stimulated optical radiation in ruby. Nature. 1960;187;493-7. 189. Coluzzi DJ. Fundamentals of dental lasers: science and instruments. Dent Clin North
Am 2004;48:751-770. 190. Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR. (2012). The nuts and
bolts of low-level laser (light) therapy. Ann Biomed Eng.40:516-533.

Dr Raluca Baleanu 57
191. Mester E, Spiry T, Szende B, Tota JG. Effect of laser rays on wound healing. Am J Surg 1971;122:532-5.
192. Mester E, Szende B, Tota J. Effect of laser on hair growth of mice. Kiserl Orvostud 1967;19:628-31.
193. Sun G, Tunér J. Low-level laser therapy in dentistry. Dent Clin North Am. 2004;48(4):1061-viii.
194. Chung H, Dai T, Sharma SK, et al. The Nuts and Bolts of Low-level Laser (Light) Therapy. Ann Biomed Eng. 40, 516–533 (2012).
195. Hilgers JJ, Tracey SG. Clinical uses of diode lasers in orthodontics. J Clin Orthod. 2004;38(5):266-273.
196. Tortamano A, Lenzi DC, Haddad AC, Bottino MC, Dominguez GC, Vigorito JW. (2009) Low-level laser therapy for pain caused by placement of the first orthodontic arch wire: a randomized clinical trial. American Journal of Orthodontics and Dentofacial Orthopaedics.136:662-667.
197.
Carvalho AS, Napimoga MH, Coelho-Campos J, Silva-Filho VJ, Thedei G. (2011) Photodynamic therapy reduces bone resorption and decreases inflammatory response in an experimental rat periodontal disease model. Photomedicine Laser Surgery.29:735-740.
198. Kawasaki, Shimizu N. Effects of low-energy laser irradiation on bone remodeling during experimental tooth movement in rats. Lasers Surg Med. - 2000. - Vol. 26. - pp. 282-291.
199. Torri S, Weber JBB. Influence of Low-Level Laser Therapy on the Rate of Orthodontic Movement: A Literature Review. Photomed Laser Surg 2013;31:411-21.
200. da Silva Sousa MV, Scanavini MA, Sannomiya EK, Velasco LG, Angelieri F. Influence of low-level laser on the speed of orthodontic movement. Photomed Laser Surg 2011; 29:191-96.
201. Cruz DR, Kohara EK, Ribeiro MS, Wetter NU. Effects of low-intensity laser therapy on the orthodontic movement velocity of human teeth: a preliminary study. Lasers Surg Med 2004; 35:117-120.
202. Kreisler M, Christoffers AB, Willershausen B, d'Hoedt B. Effect of low-level GaAlAs laser irradiation on the proliferation rate of hu-man periodontal ligament fibroblasts: an in vitro study. J Clin Pe-riodontol 2003;30:353-8
203. Walsh LJ. The current status of low level laser therapy in dentistry. Part 1. Soft tissue applications. Aust Dent J 1997; 42( 4): 247–254.
204. Lanzafame RJ, Stadler I, Kurtz AF, Connelly R, Peter TA Sr, Brondon P et al. Reciprocity of exposure time and irradiance on energy density during photoradiation on wound healing in a mu-rine pressure ulcer model. Lasers Surg Med 2007;39:534-42.
205. Doshi-Mehta G, Bhad-Patil WA. Efficacy of low-intensity laser therapy in reducing treatment time and orthodontic pain: a clinical investigation. Am J Orthod Dentofacial Orthop 2012;141:289-297.
206. Limpanichkul W, Godfrey K, Srisuk N, Rattanayatikul C. Effects of low-level laser therapy on the rate of orthodontic tooth movement. Orthod Craniofac Res 2006;9:38-43.

Dr Raluca Baleanu 58
207. Goulart CS, Nouer PR, Mouramartins L, Garbin IU, de Fatima Zanirato Lizarelli R. Photoradiation and orthodontic movement: experimental study with canines. Photomed Laser Surg 2006;24:192-6.
208. Ng D, Chan AK, Papadopoulou AK, Dalci O, Petocz P, Darendeliler MA. The effect of low-level laser therapy on orthodontically induced root resorption: a pilot double blind randomized controlled trial. European Journal of Orthodontics 2018;40(3):317-325.
209. Vasconcelos EC, Henriques JF, Sousa MV, de Oliveira RC, Consolaro A, Pinzan A, et al. Low-level laser action on orthodontically induced root resorption: histological and histomorphomet-ric evaluation. J Lasers Med Sci 2016;7:146-51.
210. Yassin, Ahmed & Shehata, Fathy & Al-Sawa, Afaf & Karam, Sahar. (2020). Effect of low-level laser therapy on orthodontic induced inflammatory root resorption in rats.Alexandria Dental Journal. 45. 62-67. 10.21608/adjalexu.2020.79941.
211. Altan AB, Bicakci AA, Mutaf HI, Ozkut M, Inan VS. The effects of low-level laser therapy on orthodontically induced root resorption. Lasers Med Sci 2015;30:2067-2076.
212. Bosshardt DD, Schroeder HE. Cementogenesis reviewed: a comparison between human premolars and rodent molars. Anat Rec 1996;245:267-92.
213. Harazaki M, Isshiki Y. Soft laser irradiation effects on pain reduction in orthodontic treatment. Bull Tokyo Dent Coll, 1997. - 291-295 : Vol. 38.
214. Turhani D Scheriau M, Kapral D, Benesch T, Jonke E, Bantleon HP. Pain relief by single low-level laser irradiation in orthodontic patients undergoing fixed appliance therapy. Am J Orthod Dentofacial Orthop., 2006 Sep. - 371-7 : Vol. 130(3)
215. Shi Q, Yang S, Jia F, Xu J. Does low level laser therapy relieve the pain caused by the placement of the orthodontic separators? --A meta-analysis. Head Face Med 2015;11:28.
216. Coluzzi DJ. Fundamentals of lasers in dentistry: Basic science, tissue interaction, and instrumentation. J Laser Dent 2008;16:4-10.
217. Mester E, Spiry T, Szende B, Tota JG. Effect of laser rays on wound healing. Am J Surg 1971;122:532-535.
218. Altan BA, Sokucu O, Ozkut MM, Inan S. Metrical and histological investigation of the effects of low-level laser therapy on orthodontic tooth movement. Lasers Med Sci 2012;27:131-140.
219. Peptan AI et al. Responses of intramembranous bone and sutures upon in vivo cyclic tensile and compressive loading. Bone, 2007. 42(2): p. 432-438.
220. Vizi ES, Mester E, Tisza S, Mester A. Acetylcholine releasing effect of laser irradiation on Auerbach's plexus in guinea-pig ileum. J Neural Transm 1977;40:305-308.
221. Walker JB, Akhanjee LK. Laser-induced somatosensory evoked potentials: evidence of photosensitivity in peripheral nerves. Brain Res 1985;344:281-285.
222. Fork RL. Laser stimulation of nerve cells in Aplysia. Science 1971;171:907-908 223. Jacques SL. Laser-tissue interactions. Photochemical, photothermal, and
photomechanical. Surg Clin North Am 1992;72:531-558. 224. Sommer AP, Pinheiro AL, Mester AR, Franke RP, Whelan HT. Biostimulatory
windows in low-intensity laser activation: lasers, scanners, and NASA's light-emitting diode array system. J Clin Laser Med Surg 2001;19:29-33.

Dr Raluca Baleanu 59
225. Mester E, Szende B, Gartner P. The effect of laser beams on the growth of hair in mice. Radiobiol Radiother (Berl) 1968;9:621–626.
226. Mester E, Nagylucskay S, Doklen A, Tisza S. Laser stimulation of wound healing. Acta Chir Acad Sci Hung 1976;17:49-55.
227. Mester E, Szende B, Spiry T, Scher A. Stimulation of wound healing by laser rays. Acta Chir Acad Sci Hung 1972;13:315-324.
228. Passarella S, Casamassima E, Molinari S, Pastore D, Quagliariello E, Catalano IM et al. Increase of proton electrochemical potential and ATP synthesis in rat liver mitochondria irradiated in vitro by helium-neon laser. FEBS Lett 1984;175:95-99.
229. Karu T. Photobiology of low-power laser effects. Health Phys 1989;56:691-704. 230. Yu W, Naim JO, McGowan M, Ippolito K, Lanzafame RJ. Photo modulation of
oxidative metabolism and electron chain enzymes in rat liver mitochondria. Photochem Photobiol 1997;66:866-871.
231. Kau CH, Kantarci A, Shaughnessy T, Vachiramon A, Santiwong P, da la-Fuente A. Extra-oral photo biomodulation in the alignment phase of orthodontics Prog Orthod; 2013;14:30.
232. Ekizer A, Turker G, Uysal T, Guray E, Tasdemir Z. Light emitting diode mediated photo biomodulation therapy improves orthodontic tooth movement and miniscrew stability: A randomized controlled clinical trial. Lasers Surg Med. 2016;48(10):936-943.
233. Shaughnessy T, Kantarci A, Kau CH, Skrenes D, Skrenes S, Ma D. Intraoral photobiomodulation-induced orthodontic tooth alignment: a preliminary study. BMC Oral Health 2016;16:3.
234. Alsulaimani M, Doschak M, Dederich D, Flores-Mir C. Effect of low-level laser therapy on dental root cementum remodeling in rats. Orthod Craniofac Res 2015;18:109-116.
235. Fonseca PD, de Lima FM, Higashi DT, Koyama DF, Toginho Filho Dde O, Dias IF et al. Effects of light emitting diode (LED) therapy at 940 nm on inflammatory root resorption in rats. Lasers Med Sci 2013;28:49-55.
236. Nimeri G, Kau CH, Corona R, Shelly J. The effect of photobiomodulation on root resorption during orthodontic treatment. Clin Cosmet Investig Dent 2014;6:1-8.
237. Márcia Martins Marques, Ivana Márcia Alves Diniz, Sueli Patricia Harumi Miyagi de Cara, Ana Clara Fagundes Pedroni, Gabriela Laranjeira Abe, Roberta Souza D'Almeida-Couto, Paula Loures Valle Lima, Tamara Kerber Tedesco, and Maria Stella Moreira. Photomedicine and Laser Surgery.Nov 2016.500-508.http://doi.org/10.1089/pho.2015.4038
238. Garrido PR, Pedroni ACF, Cury DP, et al. Effects of photobiomodulation therapy on the extracellular matrix of human dental pulp cell sheets. J Photochem Photobiol B. 2019;194:149-157.
239. Sambevski J, Darendeliler A, Oyku D, Papadopoulou A, Foley M - The effects of Led Mediated Photobiomodulation on Orthodontic Root Resorption and Pain – A split-mouth randomized controlled clinical trial.
240. Simon S, Smith AJ, Lumley PJ, Cooper PR, Berdal A. The pulp healing process: from generation to regeneration. Endodontic Topics. 2012;26(1):41-56.

Dr Raluca Baleanu 60
241. Olgart, L. & Bergenholtz, G. The dentine-pulp complex: responses to adverse in uences. In: Bergenholtz, G., Hørsted-Bindslev, P. & Reit, C. Textbook of endodontology. (2003). 1st ed, Blackwell Munksgaard, Oxford (pp.21-42).
242. Yamamura T. Differentiation of pulpal cells and inductive influences of various matrices with reference to pulpal wound healing. J Dent Res 1985;64 Spec No:530-540.
243.
Nie X, Tian W, Zhang Y, et al. Induction of transforming growth factor-beta 1 on dentine pulp cells in different culture patterns. Cell Biol Int 2006;30:295-300.
244. Luukko K, Kettunen P, Fristad I, E B. Cohen’s pathways of the pulp. . In: KM H, S C, editors. Structure and functions of the dentin-pulp complex St.Louis Mosby Elsevier; 2011. p. 452-503.
245. Holland GR. Morphological features of dentine and pulp related to dentine sensitivity. Arch Oral Biol 1994;39 Suppl:S3-S11.
246. Foster E, Robinson PP. The incidence and distribution of branched pulpal axons in the adult ferret. Arch Oral Biol 1993;38:965-970.
247. Paphangkorakit J, Osborn JW. Discrimination of hardness by human teeth apparently not involving periodontal receptors. Arch Oral Biol 1998;43:1-7.
248. Matsutani K, Tsuruoka M, Shinya A, Furuya R, Kawawa T. Stimulation of the locus coeruleus suppresses trigeminal sensorimotor function in the rat. Brain Res Bull 2000;53:827- 832.
249. Vongsavan N, Matthews B. The vascularity of dental pulp in cats. J Dent Res 1992;71:1913-1915.
250. Kim S. Regulation of pulpal blood flow. J Dent Res 1985; 64 (special issue): 590–596. 251. Yu C, Abbott PV. An overview of the dental pulp: its functions and responses to
injury. Australian dental journal. 2007 Mar;52:S4-6. 252. Kavas AA, Tümen ECJIDR (2019) Volumetric pulp chambers measurements in
mandibular and maxillary permanent first molar using cone-beam computed tomography by age and gender. Int Dent Res 9(1):30–40
253. Pinchi V, Pradella F, Buti J, Baldinotti C, Focardi M, Norelli GA. A new age estimation procedure based on the 3D CBCT study of the pulp cavity and hard tissues of the teeth for forensic purposes: A pilot study.J Forensic Leg Med. 2015 Nov;36():150-7.
254. Star H, Thevissen P, Jacobs R, Fieuws S, Solheim T, Willems G.Human dental age estimation by calculation of pulp-tooth volume ratios yielded on clinically acquired cone beam computed tomography images of monoradicular teeth. J Forensic Sci 2011 Jan; 56 Suppl 1():S77-82.
255. Tardivo D, Sastre J, Ruquet M, Thollon L, Adalian P, Leonetti G, Foti B Three-dimensional modeling of the various volumes of canines to determine age and sex: a preliminary study. J Forensic Sci. 2011 May; 56(3):766-70.
256. Kazmi S, Mânica S, Revie G, Shepherd S, Hector M (2019) Age estimation using canine pulp volumes in adults: a CBCT image analysis. Int J Leg Med 133(6):1967–1976.
257. Xu T, Yan M, Wang Y et al. (2014) Estrogen deficiency reduces the dentinogenic capacity of rat lower incisors J Mol Histol 45, 11-9
258. Zhu Y, Liu S, Chen W, et al. Epidemiology of low-energy fracture in Chinese postmenopausal women: changing trend of incidence since menopause and

Dr Raluca Baleanu 61
associated risk factors, a national population-based survey. Menopause. 2019;26:286-292.
259. Sturdee DW, Pines A. Updated IMS recommendations on postmenopausal hormone therapy and preventive strategies for midlife health. Climacteric. 2011;14(3):302-320.
260. Selig, K. R., Kupczik, K., & Silcox, M. T. (2021). The effect of high wear diets on the relative pulp volume of the lower molars. Am J Phys Anthropol.2021;174:804–811
261. Ertas E, et al. Dental pulp stone formation during orthodontic treatment: A retrospective clinical follow-up study. Nigerian Journal of Clinical Practice, 2017. 20(1): p. 37-42.
262. Rana M, et al. Detection of apoptosis during orthodontic tooth movement in rats. American Journal of Orthodontics and Dentofacial Orthopaedics, 2001. 119(5): p. 516-521.
263. Santamaria JM, et al. Initial changes in pulpal microvasculature during orthodontic tooth movement: a stereological study. European Journal of Orthodontics, 2006. 28(3): p. 217-220.
264. McDonald FTR, Pitt Ford. Blood flow changes in permanent maxillary canines during retraction. European journal of orthodontics, 1994. 16(1): p. 1-9.
265. Derringer KA, Linden RW. Enhanced angiogenesis induced by diffusible angiogenic growth factors released from human dental pulp explants of orthodontically moved
266. Taintor JF, Shalla CL. Comparison of respiration rates in different zones of rat incisor pulp. Journal of Dentistry, 1978. 6(1): p. 63-70.
267. Brin I, et al. The influence of orthodontic treatment on previously traumatized permanent incisors. European Journal of Orthodontics, 1991. 13(5): p. 372-377.
268. Bauss O,et al. Influence of orthodontic intrusion on pulpal vitality of previously traumatized maxillary permanent incisors. American Journal of Orthodontics and Dentofacial Orthopaedics, 2008. 134(1): p. 12-17.
269. Bauss O,et al. Influence of Orthodontic Extrusion on Pulpal Vitality of Traumatized Maxillary Incisors. Journal of Endodontics, 2010. 36(2): p. 203-207.
270. Bauss O.et al. Pulp vitality in teeth suffering trauma during orthodontic therapy. The Angle Orthodontist, 2009. 79(1): p. 166-171.
271. Seltzer S, Bender IB. The dental pulp: biologic considerations in dental procedures. 3rd ed. 1984, Philadelphia: Lippincott.1984;3rd ed:191.
272. Dougherty HL. The effect of mechanical forces upon the mandibular buccal segments during orthodontic treatment. American Journal of Orthodontics, 1968. 54(1): p. 29-49.
273. Marshall JA. A study of bone and tooth changes incident to experimental tooth movement and its application to orthodontic practice. International Journal of Orthodontia and Dentistry for Children, 1933. 19(1): p. 1-21.
274. Cwyk F. Endodontic implications of orthodontic tooth movement. Journal of Dental Research 1984;63:286.
275. Venkatesh S, Ajmera S, Ganeshkar SV. Volumetric pulp changes after orthodontic treatment determined by cone-beam computed tomography. Journal of Endodontics, 2014.40(11): p. 1758-1763.
276. Bohl MV, et al. Pulpal reactions to orthodontic force application in humans: a systematic review. Journal of Endodontics, 2012. 38(11): p. 1463-1469.
Dr Raluca Baleanu 62
277. Javed F, et al. Influence of orthodontic forces on human dental pulp: a systematic review. Archives of Oral Biology, 2015. 60(2): p. 347-356.
278. Restarski JS. Effect of vibration upon the dental pulp and periosteum of white rats. Journal of Dental Research, 1945. 24(2): p. 205-255.
279. Domínguez, Ballesteros RE, Viáfara JH, Tamayo OM. Effect of low level laser therapy on dental pulp during orthodontic movement. World J Methodol 2013; 3(2): 19-26.
280. Abi-Ramia LB, Stuani AS, Stuani AS, Stuani MB, Mendes Ade M. Effects of low-level laser therapy and orthodontic tooth movement on dental pulps in rats. Angle Orthod. 2010;80(1):116-122.
63
MANUSCRIPT
EffectsofLow-LaserTherapyandLED-
mediatedPhotobiomodulationonpulp
canalvolumeofmaxillaryfirst
premolarsundergoingorthodontictooth
movementDRRALUCABALEANU
DISCIPLINEOFORTHODONTICS
FACULTYOFDENTISTRY
UNIVERSITYOFSYDNEY,
AUSTRALIA2020

64
Raluca Baleanu BDSc (Hons)
Post-graduate student
Discipline of Orthodontics
Faculty of Dentistry, University of Sydney
Nam(Alice) Wong Lecturer Discipline of Orthodontics Faculty of Dentistry, University of Sydney Peter Petocz
PhD
Associate Professor
Statistician
Department of Statistics, Macquarie University
Matthew Foley Image Analysis & Computer Tomography Specialist Sydney Microscopy & Microanalysis Faculty of Dentistry, University of Sydney Oyku Dalci DDS, PhD, Spec Orth
Senior Lecturer
Discipline of Orthodontics
Faculty of Dentistry, University of Sydney M. Ali Darendeliler
BDS, PhD, Dip Ortho, Certif. Orth, Priv. Doc
Professor and Chair
Discipline of Orthodontics
Faculty of Dentistry, University of Sydney

Dr Raluca Baleanu 65
Abstract
Background and Objective: Since the demand for fast orthodontic treatment has risen,
different techniques have been proposed and implemented with various success. The use of
Low-Level Laser Therapy (LLLT) and LED-meditated photobiomodulation (LED-PBM) to
accelerate orthodontic tooth movement has been widely studied. However, limited
information is available on the effect of LLLT and LED-PBM on pulp volume. Therefore, the
aim of this study was to assess the effects of Low-Level Laser Therapy (LLLT) and LED-PBM on
pulp volume of maxillary first premolars.
Methods: Micro-CT scans of maxillary first premolars that were collected previously as part
of two different split-mouth randomized clinical trials on orthodontic root resorption were
analysed to determine the volumes of tooth root and pulp canal. All maxillary first premolars
were exposed to 150g buccal tipping force for 4 weeks. Additionally, 20 premolars had
received LLLT and 18 premolars had received LED-PBM while their contra-lateral teeth were
served as controls. Premolars were scanned with MicroCT following extraction. Avizo 3D
software was used to digitally measure the volume of the tooth roots and pulp canal.
Results: The average pulp volume for LLLT premolars and controls were 19.71mm3 and
17.95mm3 respectively. There was an average of 1.76± 5.03 mm3(95% CI: -0.60 mm3 4.11
mm3) more pulpal volume in the experimental group than in the controls. However, this was
not statistically significant (p= 0.135). The average pulpal volume for LED PBM premolars and
controls were 14.11mm3 and 15.65mm3 respectively. The 1.54± 4.81 mm3 (95% CI: -3.93

Dr Raluca Baleanu 66
mm3 - 0.85 mm3) mm3 reduction in pulp canal volume in LED-PBM premolars compared to
controls was not statistically significant (p=0.193) either. Univariate analysis of variance
indicated that application of either LLLT or LED-PBM does not result in statistical difference
changes in pulpal volume. There was no correlation between difference in pulp volume
change and difference in the total amount of root resorption caters developed following the
application of LLLT and PBM.
Conclusion: No significant difference was found on the pulp canal volume of maxillary first
premolars between experimental and control groups when LLLT or LED-PBM was applied for
4 weeks in addition to 150g of orthodontic force.
Key words: Low -Laser Therapy (LLLT), LED-meditated photobiomodulation (LED-PBM,
Orthodontic tooth movement, Pulp volume, Micro-CT.

Dr Raluca Baleanu 67
Introduction
Tooth movement is a process that combines pathological and physiological responses to
externally applied forces1 and the rate of the movement is influenced by bone modelling and
remodelling.2 The rate of alveolar modelling and remodeling is determined by the activity of
bone cells (osteoclast, osteoblast and osteocytes) which are under the influence of
mechanical stimulation and biomechanical factors such as prostaglandins and cytokines.2
Absorption’ as root resorption was first reported by Bates in 1856.3 The board definition of all
forms of root resorption including orthodontic root resorption which refers to the
pathological destruction and subsequent removal of the hard tissues of the tooth root as a
result of clastic activity.4
The demand for fast orthodontic treatment has risen in the last decade. A short treatment
time is beneficial to both patients and clinicians as it minimizes the risk of complication such
as caries, periodontal problems, root resorption and patient burnout.5,6,7 Various methods
ranging from invasive to non-invasive methods have been proposed and implemented to
accelerate orthodontic tooth movement. The non-invasive methods include application of
Low-Level Laser Therapy (LLLT) and LED-mediated photobiomodulation (LED-PBM). From the
discovery of the ‘Rubby Laser’ by Maiman,8 studies have been done to introduce laser
technology in the area of dentistry. Laser can be applied to many fields in dental research and
basic research offers new possibilities by advancing laser technology.
Low-level laser therapy (LLLT), also known as soft laser and cold laser, is a non-invasive
method with its effects limited to the target tissue.9 LLLT is carried out by a the
semiconductor diode device and is using laser wavelength, which is absorbed primarily by

Dr Raluca Baleanu 68
tissue pigment (melanin) and hemoglobin.10 The proposed mechanism of action involves the
stimulation of cellular metabolism near infrared or infrared light at a low energy density.10
Many parameters influence the quality, quantity, and density of the light energy delivered to
the target tissue. Such as light source- power, spot size, number and frequency of
applications, application time, and application energy.9
Clinically, LLLT has been used in procedures including aesthetic gingival re-contouring, soft
tissue crown lengthening, exposure of impacted teeth, removal of inflamed and hypertrophic
tissue, frenotomies, and photo stimulation of the aphthous and herpes lesions.11
Orthodontically, LLLT was widely used in attempts to reduce pain following application of
orthodontic force as well as accelerating orthodontic tooth movement. Some studies
reported controversial results and failed to observe any significant difference between the
rates of orthodontic tooth movement on the irradiated sides versus non irradiated side.12
Ng.et al 13 reported a reduction of the total amount of root resorption on first premolars
compared with sham laser and a minimal difference between pulsed or continuous
irradiation with LLLT after 4 weeks of buccal tipping force application to maxillary first
premolars.
Photobiomodulation is a minimally invasive therapy that has been adopted in modern
medicine and dentistry for pain reduction, promoting wound healing and preventing tissue
damage. It can be performed in the form of low level laser (LLL) or light-emitting diode (LED).
Being a non-coherent light source, LED light produces fewer side effects when compared to
LLL which is coherent. Therefore, it can be safely applied to a large area of the body
surface.14,15

Dr Raluca Baleanu 69
Depending on the light parameters used, PMB can generate both stimulatory and inhibitory
responses 16, therefore it potentially allows a wide range of applications in the field of
orthodontics. Various animal and human studies were conducted in attempt to verify these
applications which include orthodontic pain relief,17 enhancement of mandibular growth as
well as osseointegration of mini-screws, accelerating orthodontic tooth movement and
minimizing orthodontically induced inflammatory root resorption (OIIRR).18,19,20
LED-mediated photobiomodulation has been demonstrated to significantly increases the rate
of orthodontic tooth movement in animal studies.21,22,23,24 by encouraging bone remodeling
via increased osteoblastic and osteoclastic cell proliferation and function during tooth
movement. Laser-mediated PBM has also proposed to potentially reduce orthodontic related
pain. 16,17,25,26 The mechanism is thought to involve stabilization of membrane potential and
release of neurotransmitters which induce analgesic effect.27,28,29 LED- PBM did not produce
a statistically significant difference in the amount of root resorption craters in maxillary first
premolars following buccal tipping force for 28 days. 30 However, the results of this study
should be validated on a patient sample undergoing PBM over the full course of orthodontic
treatment.30
The effect orthodontic force application on dental pulp tissue has long been the subject of
studies in decades with conflicting results.31,32,33 Proffit et al.31 described that light and
continuous force has little or no effect on dental pulp. However, Stevik and Reitan reported
that the reaction to the orthodontic tooth movement varies from mild hyperemia to
complete necrosis.34 Dominquez et al.35 showed a favorable histological result with an
adaptive response in the human pulp following the exposure to LLLT. Similarly, Abi-Ramia et

Dr Raluca Baleanu 70
al.36 also observed an increased rate of pulpal tissue repair in a rodent model after LLLT
application during orthodontic tooth movement.
However, the studies investigating the effect of LLLT and LED PBM on pulpal tissues either did
not involve tooth movement or were carried out on animals. Therefore, the aim of this
present study was to investigate the effects LLLT and LED PBM on pulp volume of maxillary
first premolars undergoing experimental orthodontic tooth movement for 4 weeks.
Material and Methods
76 maxillary first premolars were analysed in this study. The teeth were previously extracted
from 38 patients as part of 2 randomized clinical split-mouth trials investigating the effects of
LLLT and PBM over 4 weeks.13,30 Randomization was generated using a computer random
number generator- www.randomization.com, and allocation was concealed in sequentially
numbered, opaque, sealed envelopes.13,30 All premolars were subjected to 150 g buccal
tipping forces for 4 weeks. One side of the mouth in each patient was randomly allocated to
one of the proposed accelerated tooth movement interventions, while the contralateral
premolars served as control with sham light application/ placebo (Ethics approvals:X14-0200
HREC/14/RPAH/263 and X16-0215 & HREC/16/RPAH/266, Registration: Clinical Trials Registry
-ACTRN12616000829415 and Australian New Zealand Clinical Trials Registry -
ACTRN12616000652471).13,30
Intervention 1: LLLT - 808-nm diode laser (Klas-DX6182, Konftec Corporation, New Taipei City,
Taiwan). 13

Dr Raluca Baleanu 71
There was a total of 20 experimental premolars and 20 controls extracted from 20 patients.
There were 10 girls and 10 boys with a mean age of 16.13
On the experimental side, 10 of the premolars received continuous laser delivery LLLT-A (0.18
W, 9 seconds per point) while 10 received pulsed delivery LLLT-B (0.36 W, pulsed at 20 Hz
with 25 ms on/off, 50% duty cycle, 4.5 second per point). The energy dose was 1.6 J per
point. On the control side the placebo-laser was created by blocking out the laser beam by
covering the beam aperture with black absorbent paper. 13
LLLT application regimen was every day for the first 4 days (days 0, 1, 2, and 3) and then
weekly (days 7, 14, and 21) until 28 days. Application of laser was to the mucosal surface of
the premolar root at four points on the buccal and palatal surfaces at the level of the apex,
middle third, cervical thirds on the mesial and distal sides.13
Intervention 2: LED mediated PBM, applied via the Orthopulse™ device.30
There were a total of 18 experimental premolars and 18 controls extracted from 18 patients.
There were 14 girls and 4 boys with a mean age of 15.30
On the experimental side, the Orthopulse™ applied near-infrared (NIR) light with a
continuous 850nm wavelength from approximately 54 LEDs spaced 5mm apart in two banks
of 3x9 elements embedded within a flexible silicone matrix. The LED array is specified to
produce a power density of 60mW/cm². Following randomization of sides, on the
control/placebo side the light emitted from either the left or right banks of LEDs was
deactivated by physical blocking using a single layer of opaque black obstructive film and a
single layer of medical-grade adhesive tape (Leukoflex, BSN medical GmbH Hamburg,

Dr Raluca Baleanu 72
Germany). The light blocking effect of this material was tested with the use of a laser-check
sensor (Lasercheck®, Edmund Optics Inc, Barrington NJ, USA).30
Patients were instructed to use the device for 5 minutes/day on the maxillary arch for 28
days. Compliance was monitored using a smart-phone app which logged each patient’s use of
the device via bluetooth.
MicroCT Scan
Following 28 days of experimental period the maxillary premolars were extracted and were
scanned using SkyScan 1172 desktop X-ray micro-tomograph system (SkyScan, Aartselaar,
Belgium), from the cementoenamel junction (CEJ) to the root apex, with image resolution set
at 17.6 µm.13,30
Specifically designed software, NRecon (version 1.6.9.18, Skyscan, Aartselaar, Belgium),
reconstructed the image data from SkyScan, utilizing a modified Feldkamp cone-beam
algorithm to produce slice-by-slice axial reconstructions. These were saved in 16-bit tagged
image file format (TIFF) format.13,30
Volumetric Measurements
Avizo 3D software 2019 (Thermo Fisher Science) was used to digitally measure the volume of
the tooth structure. All premolars included in this study were segmented into 3 materials
(Crown, Root, Pulp) using threshold intensity values related to material attenuation. To
minimize crown variability between samples, only the volume from the CEJ to the apical tip of
the tooth was considered for evaluation. The pulp was extracted using Avizo as showed in
Dr Raluca Baleanu 73
Table 6. For the digital conversion a threshold of specific grey values were used, altering the
data into a binary format.
The scale for the datasets was 17.66 micron and was used to analyze the volume of calcified
tooth structure with the section reversed to measure the internal volume of uncalcified
matter outlining the pulp tissue. The ‘Material Analysis’ function of the Avizo was used to
analyze the segmented components. All the pulpal and hard tissue volumetric measurements
were performed by the same operator.
Statistical Analysis
Paired t test was used to assess differences in total pulp canal volume of LLLT or LED PBM
versus control teeth. Statistical significance was set at 0.05. Univariate analysis of variance
was used to compare the difference between the experimental and control sides in between
interventions. Pearson Correlation was used to assess the relationship between difference in
pulp volume and difference in the total amount of root resorption craters between the
intervention and sham among all three groups (Table 5). Error measurements were carried
out ten months after initial measurements, on randomly selected teeth (27%). SPSS (version
25) software, was used to analyze the data.
Results
The average pulp volume following the application of buccal tipping force and LLLT was
19.71mm3 and 17.95mm3 for the controls. There was a mean difference of 1.76 mm3
between the LLLT group and the controls which was not statistically significant (p=0.14,
Table1). Similarly, the average pulp volume for LED-PBM teeth measured 14.11mm3 and

Dr Raluca Baleanu 74
15.65mm3 for the controls. (Table1) The mean difference between the LED-PBM teeth and
the controls was statistically insignificant (-1.54mm3, p=0.19; Table1, Chart1). In addition, the
mean difference between teeth treated with continuous LLLT and the control group was
0.01mm3, while the mean difference between teeth treated with pulsed LLLT and the control
group was 3.5mm3 (Table 2). The difference between intervention and sham in terms of the
ratio between pulp canal and calcified tooth structure in all three groups were shown in
figure 2 and figure 3.
Univariate analysis of variance (ANOVA) demonstrated that the pulp volume changes in LLLT
group and LED-PBM group were not statistically different (Table 3). Similarly, the pulp volume
changes in continuous or pulsed LLLT group were not significantly different to that of LED-
PBM group (Table 4).
There was no correlation between difference in pulp volume and difference in the total
amount of root resorption craters between the intervention and sham sides among all three
groups (Table 5).
The intra-rater reliability test revealed the coefficient of variation was less than 1% for all
measurements.
Discussion
This is the first human study assessing human pulp volume changes after treatment with LLLT
and orthodontic tooth movement with Micro-CT. Further, it is also the first human study to
investigate the effect of photomodulation (LED-PBM) on the dental pulp volume during
orthodontic tooth movement.

Dr Raluca Baleanu 75
It was shown that orthodontic force may generate pulpal changes that range from mild
hyperemia to complete necrosis.34 Furthermore LLLT and LED-PBM have recently been
introduced as methods of accelerated orthodontic tooth movement. However, there are no
studies that investigated the effects of either on humans during orthodontic tooth
movement. Therefore, it is worthwhile to investigate their impacts on pulpal tissues. Most of
previous studies investigating the change in pulp tissue following exposure to LLLT utilized 2D
imaging such as SEM and periapical radiographs.37 These evaluation methods provide limited
information because attempts were made to analyse 3D structure with 2D imaging. In the
present study, analysis was performed with micro-CT which is a non-invasive method used to
visualize dental morphology comprehensively in three dimensions without destroying the
extracted teeth. 13,30,38However, owing to the heterogeneity of study designs and evaluation
methods being used, the results of this study were not comparable to previous studies.
LLLT is used for its stimulatory effects that involves tissue regeneration, wound healing as
well as relieving inflammation and pain.17,25 This study aimed to assess the effects of LLLT and
LED-PBM on pulp volume in human maxillary first premolars that were subjected to 150g of
buccal tipping force for 28 days. No statistically significant reduction on the pulp volume was
detected in the control group when compared to that when LLLT or LED PBM was applied.
Similarly, exposure to both continuous and pulsed LLLT resulted in an increased volume of
pulp chamber when compared to sham, however, these results did not reach statistical
significance. Previous studies showed stimulated adaptive response of the pulpal tissues with
application of LLLT. 35,36

Dr Raluca Baleanu 76
Depending on the light parameters used, PMB can generate both stimulatory and inhibitory
responses.16 It has been demonstrated in several studies that there is a correlation between
energy density and dose.39-41 Currently, no published information is available in regards to
the effect of LED-PBM on pulp tissue. However, several in vitro studies postulated that laser-
mediated PBM with low energy density stimulates the proliferation of dental pulp stem
cells.42,43 In the present study exposure to LED-PBM resulted in a decreased volume of pulp
chamber when compared to sham, although the result was not statistically significant.
Perhaps further prospective studies with larger sample size with the use of lower energy
density PBM source might be helpful in elucidating its effect on pulpal tissues.
Similarly, the current study is the first human study investigating the effect of PBM on dental
pulp tissue. Previous In vitro studies42,43,44 showed positive effects of PBM on pulp cells.
However, these studies had different study designs and evaluation methods therefore direct
comparison is not possible.
The connection between orthodontic force application and dental pulp tissue has been the
subject of studies in recent years.31,32,33 The most pertinent research is linked to metabolic,
biochemical and vascularization reaction of the pulp to orthodontic tooth forces that are the
same as angiogenesis in wound healing.45 The molecular process of PBM for angiogenesis of
pulp healing are still undiscovered.46 Angiogenesis through neovascularization generates new
capillaries.47 However, alteration in the blood supply and angiogenesis have a direct impact
upon pulp metabolism.48-50 Orthodontic forces may encourage vasodilation in dental pulp
tissue46 and causes vascular changes. It is prudent to apply orthodontic loading within the
biological limitations of the pulp.52

Dr Raluca Baleanu 77
Regardless of the significant research on orthodontic movement with LLLT21,53,54 or
PBM21,22,23,24, showing an increase of the rate of orthodontic tooth movement, reports on
pulp volumetric changes are limited. A few authors have reported an increased
vascularization which accelerates pulp repair when irradiated with LLLT or PBM.
Limitations
One of the limitations of this research could be the small sample size.13,30 The current sample
was a convenient sample available from previous randomized controlled trials.
The experimental period applied in this study was short due to ethical reasons.13,30 Since
orthodontic treatment are extended over months to years and different types of tooth
movement are applied to teeth throughout treatment, the current study results may not
reflect the actual clinical situation however could be used as a baseline study.
The confounding factors in this study include factors which may affect pulp canal volume
such as age 55,56,57,58,59, hormones 60,61,62, nutrition 63 and infection64. However, the teeth
involved in the study are caries free, and the rate of dentine deposition brought about by
these factors is rather slow, the effect of these factors on the result should be limited.
Generalizability
The generalizability of these outcomes may be limited since the study was carried out for
only 28 days using buccal tipping forces.13,30 In addition, there is considerable individual
variation in pulp tissue response hence the pulp volume changes in response to orthodontic
force. Pulp tissue response vary between individuals and sometimes within the same

Dr Raluca Baleanu 78
individual on difference teeth due to different exposure to trauma. Therefore, the result may
not be able to apply to the general population.
The results of this study were based on specific LLLT and LED PBM parameters. Therefore,
the results are not applicable to different intervention parameters.
Conclusions
LLLT, continuous or pulsed, or LED PBM, using parameters in this study, when applied on
maxillary first premolars undergoing 150 g buccal tipping forces for 28 days, do not create
significant pulpal canal volume changes. However, additional research should be carried out
with patients receiving LLLT or LED PBM application throughout the entire course of
orthodontic treatment.

Dr Raluca Baleanu 79
References
1. Wise GE, GJ King. “Mechanisms of Tooth Eruption and Orthodontic Tooth Movement.” Journal of Dental Research 87, no. 5 (May 2008): 414–34.
2. Huang H, RC Williams, Kyrkanides S, Accelerated orthodontic tooth movement: Molecular mechanisms. American Journal of Orthodontics and Dentofacial Orthopedics, 2014. 146(5): p. 620-632.
3. Bates S. Absorption. Br J Dent Sci 1856;1:256. 4. Brudvik P, Rygh P. Multi-nucleated cells remove the main hyalinized tissue and start
resorption of adjacent root surfaces. Eur J Orthod 1994;16:265-273. 5. Brudvik P, Rygh P. Transition and determinants of orthodontic root resorption—
repair sequence. Eur J Orthod 1995;17:177-188. 6. Sameshima GT, Sinclair PM. Predicting and preventing root resorption: Part II.
Treatment factors. Am J Orthod Dentofacial Orthop 2001;103:138-146. 7. Skidmore KJ, Brook KJ, Thomson WM, Harding WJ. Factors influencing treatment
time in orthodontic patients. Am J Orthod Dentofacial Orthop 2006;129:230-238. 8. MAIMAN T. Stimulated Optical Radiation in Ruby. Nature 187, 493–494 (1960).T 9. Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR.(2012) The nuts and bolts of
low-level laser (light) therapy. Ann Biomed Eng.40:516-533. 10. Sun G, Tunér J. Low-level laser therapy in dentistry. Dent Clin North Am.
2004;48(4):1061-76. 11. Hilgers JJ, Tracey SG. Clinical uses of diode lasers in orthodontics. J Clin Orthod.
2004;38(5):266-273. 12. Marquezan M, Bolognese AM, Araujo MT.(2010) Effects of two low-intensity laser
therapy protocols on experimental tooth movement. Photomedicine Laser Surgery.28:757-762.
13. Ng D, Chan AK, Papadopoulou AK, Dalci O, Petocz P, Darendeliler MA. The effect of low-level laser therapy on orthodontically induced root resorption: a pilot double blind randomized controlled trial. Eur J Orthod. 2018;40(3):317-325. d
14. Limpanichkul W, Godfrey K, Srisuk N, Rattanayatikul C. Effects of low-level laser therapy on the rate of orthodontic tooth movement. Orthod Craniofac Res 2006;9:38-43.
15. Kau CH, Kantarci A, Shaughnessy T, Vachiramon A, Santiwong P, da la-Fuente A. Extra-oral photobiomodulation in the alignment phase of orthodontics Prog Orthod; 2013;19:14-30.
16. Harazaki M, Isshiki Y. Soft laser irradiation effects on pain reduction in orthodontic treatment. Bull Tokyo Dent Coll 1997;38:291-295.
17. Turhani D, Scheriau M, Kapral D, Benesch T, Jonke E, Bantleon HP. Pain relief by single low-level laser irradiation in orthodontic patients undergoing fixed appliance therapy. Am J Orthod Dentofacial Orthop 2006;130:371-377.
18. Cernavin I, Pugatschew A, de Boer N, Tyas MJ. Laser applications in dentistry: a review of the literature. Aust Dent J 1994;39:28-32.

Dr Raluca Baleanu 80
19. El-Bialy T, Alhadlaq A, Felemban N, Yeung J, Ebrahim A, Hassan AH. The effect of light-emitting diode and laser on mandibular growth in rats. Angle Orthod 2015;85:233-238.
20. Nimeri G, Kau CH, Corona R, Shelly J. The effect of photobiomodulation on root resorption during orthodontic treatment. Clin Cosmet Investig Dent 2014;6:1-8.
21. Kawasaki K, Shimizu N.(2000) Effects of low-energy laser irradiation on bone remodeling during experimental tooth movement in rats. Lasers Surg Med.26:282-291.
22. Altan BA, Sokucu O, Ozkut MM, Inan S. Metrical and histological investigation of the effects of low-level laser therapy on orthodontic tooth movement. Lasers Med Sci 2012;27:131-140.
23. Goulart CS, Nouer PR, Mouramartins L, Garbin IU, de Fatima Zanirato Lizarelli R. Photoradiation and orthodontic movement: experimental study with canines. Photomed Laser Surg 2006;24:192-196.
24. Seifi M, Shafeei HA, Daneshdoost S, Mir M. Effects of two types of low-level laser wave lengths (850 and 630 nm) on the orthodontic tooth movements in rabbits. Lasers Med Sci 2007;22:261-264.
25. Lim HM, Lew KK, Tay DK. A clinical investigation of the efficacy of low level laser therapy in reducing orthodontic postadjustment pain. Am J Orthod Dentofacial Orthop 1995;108:614-622.
26. Abtahi SM, Mousavi SA, Shafaee H, Tanbakuchi B. Effect of low-level laser therapy on dental pain induced by separator force in orthodontic treatment. Dent Res J (Isfahan) 2013;10:647-651.
27. Vizi ES, Mester E, Tisza S, Mester A. Acetylcholine releasing effect of laser irradiation on Auerbach's plexus in guinea-pig ileum. J Neural Transm 1977;40:305-308.
28. Walker JB, Akhanjee LK. Laser-induced somatosensory evoked potentials: evidence of photosensitivity in peripheral nerves. Brain Res 1985;344:281-285.
29. Fork RL. Laser stimulation of nerve cells in Aplysia. Science 1971;171:907-908. 30. Sambevski J, Darendeliler A, Oyku D, Papadopoulou A, Foley M - The effects of Led
Mediated Photobiomodulation on Orthodontic Root Resorption and Pain – A split-mouth randomized controlled clinical trial.
31. Proffit WR & Fields, HW & Sarver, David. (2007). Contemporary orthodontic appliances. Contemporary Orthodontics. 395-430.
32. Andreasen, Jens & Andreasen, Frances & Andersson, Lars. (2007). Textbook and Color Atlas of Traumatic Injuries to the Teeth.
33. Guevara MJ, McClugage SG Jr. Effects of intrusive forces upon the microvasculature of the dental pulp. The Angle Orthodontist. 1980 Apr;50(2):129-134.
34. Reitan K. Tissue behavior during orthodontic tooth movement. Am J Orthod. 1986;89:453-68.
35. Domínguez &, Ballesteros RE, Viáfara JH, Tamayo OM. Effect of low level laser therapy on dental pulp during orthodontic movement. World J Methodol 2013; 3(2): 19-26.
36. Abi-Ramia LB, Stuani AS, Stuani AS, Stuani MB, Mendes Ade M. Effects of low-level laser therapy and orthodontic tooth movement on dental pulps in rats. Angle Orthod. 2010;80(1):116-122.

Dr Raluca Baleanu 81
37. Bohl MV, et al., Pulpal reactions to orthodontic force application in humans: a systematic review. Journal of Endodontics, 2012. 38(11): p. 1463-1469.
38. Bergmans L, Van Cleynenbreugel J, Wevers M, Lambrechts P. A methodology for quantitative evaluation of root canal instrumentation using microcomputed tomography. Int Endod J 2001;34:390-398.
39. Shimizu N, Mayahara K, Kiyosaki T, Yamaguchi A, Ozawa Y, Abiko Y. Low-intensity laser irradiation stimulates bone nodule formation via insulin-like growth factor-I expression in rat calvarial cells. Lasers Surg Med 2007;39:551-559.
40. Aimbire F, Albertini R, Pacheco MT, Castro-Faria-Neto HC, Leonardo PS, Iversen VV, et al. Low-level laser therapy induces dose-dependent reduction of TNFalpha levels in acute inflammation. Photomed Laser Surg 2006;24:33-37.
41. Khadra M. The effect of low level laser irradiation on implant-tissue interaction. In vivo and in vitro studies. Swed Dent J Suppl 2005:1-63.
42. Vitor LLR, Prado MTO, Lourenço Neto N, et al. Does photobiomodulation change the synthesis and secretion of angiogenic proteins by different pulp cell lineages? Journal of Photochemistry and photobiology. B, Biology. 2020 Jan;203:111738.
43. Garrido PR, Pedroni ACF, Cury DP, et al. Effects of photobiomodulation therapy on the extracellular matrix of human dental pulp cell sheets. J Photochem Photobiol B. 2019;194:149-157.
44. Ferreira LS, Diniz IMA, Maranduba CMS, Miyagi SPH, Rodrigues MFSD, Moura Netto C, Marques MM. Short-term evaluation of photobiomodulation therapy on the proliferation and undifferentiated status of dental pulp stem cells. Lasers Med. Sci.2019;34:659-666.
45. Derringer KA, Linden RWA. Vascular endothelial growth factor, fibroblast growth factor 2, platelet derived growth factor and transforming growth factor beta released in human dental pulp following orthodontic force. Archives in Oral Biology.2004;49:631-641.
46. Marques MM, Diniz IMA, Cara SPHM, Pedroni ACF, Abe GL, D’Almeida-Couto RS, Lima PLV,Tedesco TK, MS. Moreira Photobiomodulation of dental derived mesenchymal stem cells: A systematic review Photomed. Laser Surg., 34 (2016), pp. 500-508.
47. Hamilton RS, Gutmann JL. Endodontic-orthodontic relationships: a review of integrated treatment planning challenges. Int Endod J. 1999;32:343–360
48. Derringer KA, Linden RW. Enhanced angiogenesis induced by diffusible angiogenic growth factors released from human dental pulp explants of orthodontically moved teeth. Eur J Orthod. 1998;20:357–367. [PubMed] [Google Scholar]
49. Derringer KA, Linden RW. Angiogenic growth factors released in human dental pulp following orthodontic force. Arch Oral Biol. 2003;48:285–291. [PubMed] [Google Scholar]
50. Derringer KA, Linden RW. Vascular endothelial growth factor, fibroblast growth factor 2, platelet derived growth factor and transforming growth factor beta released in human dental pulp following orthodontic force. Arch Oral Biol. 2004;49:631–641. [PubMed] [Google Scholar]
51. Yamaguchi M, Kasai K. (2007) The effects of orthodontic mechanics on the dental pulp. Seminars in Orthodontics, 13, 272-280.
Dr Raluca Baleanu 82
52. Santamaria JM, Milagres D, Stuani B, Ruellas A.Initial changes in pulpal microvasculature during orthodontic tooth movement: a stereological study. European Journal of Orthodontics.2006;28:217-220.
53. Tortamano A, Lenzi DC, Haddad AC, Bottino MC, Dominguez GC, Vigorito JW.Low-level laser therapy for pain caused by placement of the first orthodontic archwire: a randomized clinical trial. American Journal of Orthodontics and Dentofacial Orthopaedics.2009;136:662-667.
54. Carvalho AS, Napimoga MH, Coelho-Campos J, Silva-Filho VJ, Thedei G.Photodynamic therapy reduces bone resorption and decreases inflammatory response in an experimental rat periodontal disease model. Photomedicine Laser Surgery. 2011;29:735-740.
55. Kavas AA, Tümen ECJIDR (2019) Volumetric pulp chambers measurements in mandibular and maxillary permanent first molar using cone-beam computed tomography by age and gender. Int Dent Res 9(1):30–40
56. Pinchi V, Pradella F, Buti J, Baldinotti C, Focardi M, Norelli GA. A new age estimation procedure based on the 3D CBCT study of the pulp cavity and hard tissues of the teeth for forensic purposes: A pilot study.J Forensic Leg Med. 2015 Nov;36():150-7.
57. Star H, Thevissen P, Jacobs R, Fieuws S, Solheim T, Willems G.Human dental age estimation by calculation of pulp-tooth volume ratios yielded on clinically acquired cone beam computed tomography images of monoradicular teeth. J Forensic Sci 2011 Jan; 56 Suppl 1():S77-82.
58. Tardivo D, Sastre J, Ruquet M, Thollon L, Adalian P, Leonetti G, Foti B Three-dimensional modeling of the various volumes of canines to determine age and sex: a preliminary study. J Forensic Sci. 2011 May; 56(3):766-70.
59. Kazmi S, Mânica S, Revie G, Shepherd S, Hector M (2019) Age estimation using canine pulp volumes in adults: a CBCT image analysis. Int J Leg Med 133(6):1967–1976.
60. Xu T, Yan M, Wang Y et al. (2014) Estrogen deficiency reduces the dentinogenic capacity of rat lower incisors J Mol Histol 45, 11-9
61. Zhu Y, Liu S, Chen W, et al. Epidemiology of low-energy fracture in Chinese postmenopausal women: changing trend of incidence since menopause and associated risk factors, a national population-based survey. Menopause. 2019;26:286-292.
62. Sturdee DW, Pines A. Updated IMS recommendations on postmenopausal hormone therapy and preventive strategies for midlife health. Climacteric. 2011;14(3):302-320.
63. Selig, K. R., Kupczik, K., & Silcox, M. T. (2021). The effect of high wear diets on the relative pulp volume of the lower molars. Am J Phys Anthropol.2021;174:804–811
64. Olgart, L. & Bergenholtz, G. The dentine-pulp complex: responses to adverse in uences. In: Bergenholtz, G., Hørsted-Bindslev, P. & Reit, C. Textbook of endodontology. (2003). 1st ed, Blackwell Munksgaard, Oxford (pp.21-42).
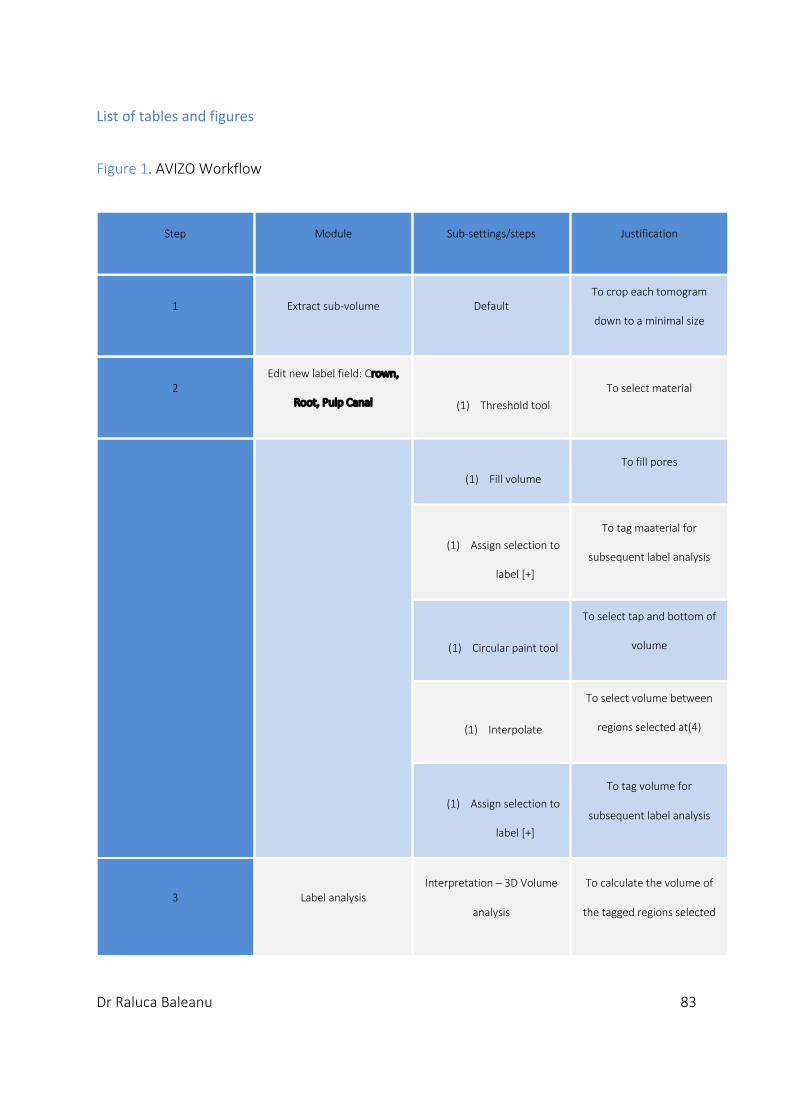
Dr Raluca Baleanu 83
List of tables and figures
Figure 1. AVIZO Workflow
Step Module Sub-settings/steps Justification
1 Extract sub-volume Default To crop each tomogram
down to a minimal size
2 Edit new label field: Crown,
Root, Pulp Canal (1) Threshold tool To select material
(1) Fill volume To fill pores
(1) Assign selection to
label [+]
To tag maaterial for
subsequent label analysis
(1) Circular paint tool
To select tap and bottom of
volume
(1) Interpolate
To select volume between
regions selected at(4)
(1) Assign selection to
label [+]
To tag volume for
subsequent label analysis
3 Label analysis Interpretation – 3D Volume
analysis
To calculate the volume of
the tagged regions selected

Dr Raluca Baleanu 84
Figure 2. Box plot depicting the pulp canal to hard tissue volume of LLLT group and LED PBM
group.
Table 1. Average pulp volume of the maxillary first premolars in the intervention and sham group (mm³)
Experimental group Control group
95% CI
Mean t test SE of Lower Upper
N Mean SD Mean SD difference P value mean bound bound
LED PBM 18 14.11 6.89 15.65 6.33 ⁃1.54 0.19 1.13 -3.93 0.85
LLLT 20 19.71 5.50 17.95 4.74 1.76 0.14 1.12 ⁃0.60 4.11
Descriptive statistics (mean, standard deviation), mean differences of pulp volume between intervention and controls, P values, standard error of the mean, and 95% confidence intervals. Non statistically significant differences were noted between intervention and control group.

Dr Raluca Baleanu 85
Table 2. Pulp volume average and difference and root resorption calculation per root surface (mm³)
Experimental group Control group
95% CI
Mean t test SE of Lower Upper N Mean SD Mean SD difference P value mean bound bound
LED PBM 18 14.11 6.89 15.65 6.33 -1.54 0.19 1.13 -3.93 0.85
LLLT-A 10 19,96 4,61 19,95 4,29 -0,01 1.0 1.23 -2.77 2.8
LLLT-B 10 19,46 6,53 15,96 4,51 3.50 0.08 1.77 -0.51 7.51
Descriptive statistics (total, mean, standard deviation), mean differences, average pulp volume (mm3) between laser and the controls, P values, standard error of the mean and 95% confidence intervals. Non statistically significant differences were noted between laser and the controls for all pulp volume.
Figure 3. Box plot depicting the pulp canal to hard tissue volume of LED PBM group, LLLT-A
group and LLLT-B group.

Dr Raluca Baleanu 86
Table 3. Univariate analysis of variance (ANOVA) investigating difference between LLLT group and LED-PBM group
Sum of squares df Mean square F Sig.
6.451 1 6.451 0.711 0.405
Table 4. Univariate analysis of variance (ANOVA) investigating difference between LLLT-A group LLLT-B group and LED-PBM group
Sum of squares df Mean square F Sig.
16.042 2 8.021 0.885 0.422
Table 5. Correlation between pulp volume changes and difference in total amount of root resorption craters among all three groups
LLLT vs LED-PBM LLLT-A vs LED-PBM LLLT-B vs LED-PBM
Pearson Correlation -0.058 0.152 -0.010
Significance 0.731 0.441 0.959

87
MANUSCRIPT
EffectofLow-LevelLaserTherapyon
pulpcanalvolumeofmaxillaryfirst
premolarsundergoingorthodontictooth
movementandinretention
DRRALUCABALEANU
DISCIPLINEOFORTHODONTICS
FACULTYOFDENTISTRY
UNIVERSITYOFSYDNEY,
AUSTRALIA,2020
Dr Raluca Baleanu 88
Raluca Baleanu BDSc (Hons)
Post-graduate student
Discipline of Orthodontics
Faculty of Dentistry, University of Sydney
Nam(Alice) Wong Lecturer Discipline of Orthodontics Faculty of Dentistry, University of Sydney Peter Petocz
PhD
Associate Professor
Statistician
Department of Statistics, Macquarie University
Matthew Foley Image Analysis & Computer Tomography Specialist Australian Centre for Microscopy & Microanalysis Faculty of Dentistry University of Sydney Oyku Dalci DDS, PhD
Senior Lecturer
Discipline of Orthodontics
Faculty of Dentistry, University of Sydney M. Ali Darendeliler
BDS, PhD, Dip Ortho, Certif. Orth, Priv. Doc
Professor and Chair
Discipline of Orthodontics
Faculty of Dentistry, University of Sydney

Dr Raluca Baleanu 89
Abstract
Background and Objective: The outcome of LLLT research on tooth movement has supplied
very limited information about the aftereffects on dental pulp tissue. The purpose of this study
is to investigate the effects of LLLT on the pulp volume in maxillary first premolars subjected
to 150g of buccal tipping force and 6 weeks after the removal of orthodontic force.
Methods: Micro-CT scans of maxillary first premolars that were attained from two published
randomised clinical trials using split-mouth designs on effects of LLLT orthodontically induced
inflammatory root resorption (OIIRR) and repair. All maxillary first premolars were exposed to
150g buccal tipping force for 4 weeks. 20 premolars in the Tooth Movement group (TM
group) had received LLLT during orthodontic tooth movement while the other 20 premolars
in Retention group (Ret group) received LLLT 6 weeks after the removal of orthodontic force.
The premolars on the contralateral side were served as controls. The volume of pulp canal
and calcified tissue were analysed after MicroCT scans digitally using Avizo 3D software.
Results: There were no statistically significant differences between the LLLT teeth and the
controls in terms of pulp canal to hard tissue volume ratio in both TM group and Ret groups.
Univariate analysis of variance demonstrated that there was no differences between TM and
Ret groups either. Further, no correlation was found between the changes in pulp canal to
hard tissue volume ratio and the amount of root resorption craters in both groups.

Dr Raluca Baleanu 90
Conclusion: No significant difference was found on the pulp canal to hard tissue volume ratio
of maxillary first premolars between experimental and control groups when LLLT was applied
during orthodontic tooth movement or in retention.
Key words: Low-laser therapy (LLLT), Orthodontic tooth movement, Pulp volume, Micro-CT

91
Introduction
Orthodontic treatment aims to improve alignment, occlusion and function.1 In response to
orthodontic force, tooth movement occurs following modification to the local environment
including alteration of vascular permeability, recruitment of inflammatory mediators and
alveolar bone remodeling.1 Sometimes, these changes are accompanied by complications
such as orthodontically induced gingival inflammation, caries, orthodontically induced
inflammatory root resorption (OIIRR) and pulpal changes. 2,3,4
Orthodontic force has been considered by some as a form of controlled trauma to the tooth
supporting structures. 5 Histological studies have revealed various degree of pulpal alteration
occurred, they include vascular compression and angiogenesis,6,7,8 deposition of secondary
dentin and alteration of the odontoblastic layer.10,11Depression of respiration rate of pulp
cells was also demonstrated.12
Literature regarding the clinical implications of these histological findings is inconclusive.
Some authors believe that these effects are transient with no long-term damage,12 however,
whilst others suggest that the changes are permanent.6,13 These clinical manifestations
include narrowing of pulp canals,14 presence of pulp stones,15,16 deterioration of long-term
tooth vitality. 17,18 Specifically, a prospective study with CBCT data demonstrated that teeth
which underwent orthodontic treatment experienced a reduction in pulpal volume.19
Low-level laser therapy (LLLT) is used for pain relief20 and accelerating orthodontic tooth
movement by increasing the rate of bone remodeling21. LLLT with wavelength longer than
600nm offers a stimulatory effect on cellular metabolism.22,23,24,25 Animal26,27 and human
clinical research28 has demonstrated the potential for LLLT to accelerate tooth movement
Dr. Raluca Băleanu 92
when compared to controls, whilst not increasing the chance of adverse sequelae such as
root resorption and alveolar bone resorption of supporting teeth.
Ng et. al.29 conducted a randomized controlled trial which demonstrated that LLLT reduced
the total amount of root resorption on maxillary first premolars compared to the sham laser.
The study also found that there was minimal difference between the effect of pulsed or
continuous LLLT on the amount of root resorption craters. However, Chun et. al.30 reported
in another randomized controlled trial that LLLT did not offer statistically significant
improvement in the amount of repair of root resorption craters on maxillary first premolars
when applied 6 weeks after orthodontic tooth movement.
With the increase in knowledge of biological effect of LLLT, the interest in whether it modifies
the pulpal response to orthodontic force has increased. However, to date there is no study
investigating the effect of LLLT on teeth undergoing orthodontic tooth movement and in
retention. Therefore, the purpose of this study is to assess the effects of LLLT on the pulp
volume in maxillary first premolars subjected to 150g of buccal tipping force and 6 weeks
after the removal of orthodontic force.
Material and Methods
Eighty maxillary first premolars included in this study were formerly removed from 40
patients included in two randomized clinical trials with split-mouth designs. 29,30
Randomization was generated using a computer random number generator-
www.randomization.com, and allocation was concealed in sequentially numbered, opaque,
sealed envelopes. The two trials analysed the effect of LLLT on teeth undergoing orthodontic
tooth movement and in retention respectively. One premolar in each patient was randomly
Dr. Raluca Băleanu 93
assigned to be exposed to LLLT while the contralateral premolars served as the
controls(Ethics approval:X14-0200 HREC/14/RPAH/263 and X16-0276 &
HREC/16/RPAH/347,Registration: Clinical Trials Registry-ACTRN12616000829415, Australian
New Zealand Clinical Trials Registry-12616000682448).29,30
Intervention 1( TM Group): A total of 20 patients (10 female and 10 male) were included in
this study, providing 20 premolars in the experimental group and 20 in the control group. A
buccal tipping force of 150 g was applied to all teeth for 4 weeks. In each patient, one side of
the maxillary first premolars were randomly assigned to the experimental group and received
808nm AIGaAs diode laser(Klas-DX6182, Konftec Corporation, New Taipei City, Taiwan).29
Out of the 20 premolars in the experimental group, 10 experienced continuous laser delivery
,TM-A (0.18 W, 9 seconds per point) and 10 experienced pulsed delivery ,TM-B (0.36 W,
pulsed at 20 Hz with 25 Ms on/off, 50% duty cycle, 4.5 second per point). In the control
group, the placebo-laser was produced through blocking the output by a sham function of
the device.29
LLLT was applied every day for the first 4 days (days 0,1,2 and 3) and then weekly (day 7, 14
and 21) until 28 days. The teeth were irradiated on the mucosal surface of the premolar root
at four points on the buccal and palatal surfaces at the different levels, including the apex,
middle third, cervical thirds on the mesial and distal sides. 29
Intervention 2 (Ret group): A total of 20 patients (10 female and 10 male) were included in
this study, providing 20 premolars in the experimental group and 20 in the control group. A
buccal tipping force of 150 g was applied to all teeth for 4 weeks. After the active force was
removed, teeth in experimental group were exposed to LLLT for 6 weeks. 30

Dr. Raluca Băleanu 94
LLLT regime included weekly application using a continuous beam of 660-nm,75-mW
aluminum-gallium-indium phosphorus laser (Thor Photomedicine, Buckinghamshire, United
Kingdom). Contact application was adopted at 8 points buccally and palatally above the
mucosa over each tooth root for 15s per point. In the control group, the placebo-laser was
produced through blocking the output by a sham function of the device. 30
MicroCT Scan
The samples were scanned with SkyScan 1172 desktop X-ray micro-tomograph system
(SkyScan, Aartselaar, Belgium), from the cementoenamel junction (CEJ) to the root apex, with
image resolution set at 17.6 µm.29,30
NRecon (version 1.6.9.18, SkyScan, Aartselaar, Belgium) software, using a modified Feldkamp
cone-beam algorithm, reconstructed the image data from SkyScan, and produce slice-by-slice
axial reconstructions, which were saved in 16-bit tagged image file format (TIFF). 29,30
Volumetric Measurements
The calcified and non-calcified premolar structure was digitally measured using Avizo 3D
software 2019 (Thermo Fisher Science) to find out the volume of tooth structures. All
samples were segmented into 3 Materials (Crown, Root, Pulp canal) applying threshold
intensity values associated to material attenuation.
‘Material Analysis’ function of the Avizo was utilized to analyse the segmented components.
The volume from CEJ to the apical tip of the premolar was investigated to minimize crown
variability between samples. . The pulp was extracted using Avizo as showed in Table

Dr. Raluca Băleanu 95
6.Threshold of specific grey values was utilized, changing the data into a binary format for
digital conversion. The measurements were performed by the same operator.
Statistical Analysis
The SPSS statistics program was utilized for statistical analysis and P >0.05 was considered
statistically significant. Paired t test was used to assess the relationship between the
experimental group and control group in all TM-A, TM-B and Ret groups. Univariate analysis
of variance was used to compare the results between TM and Ret groups. Pearson
Correlation was used to assess the relationship between pulp volume changes and changes in
amount of root resorption craters between the intervention and sham among all three
groups.
After initial measurements (10 months), on randomly selected premolars (27%), error
measurements were carried out. SPSS (version 25) software, was used to analyze the data.
Results
The average pulp canal to hard tissue volume ratio following the application of buccal tipping
force in TM group was 7.86 and 7.31 for the sham. There was a mean difference of 0.54 mm3
between the two groups which was not statistically significant (p=0.37, Table1). Similarly, in
Ret group the average pulp canal to hard tissue volume ratio for experimental teeth and
control teeth measured 8.01 and 6.85 respectively. (Table1) The difference between the
mean pulp canal to hard tissue ratio between the experimental teeth and the controls was
statistically insignificant (1.16, p=0.11; Table1). In addition, the difference of the mean pulp
canal to hard tissue ratio between the continuous LLLT treated teeth and the control group
was -0.14, while that of pulsed LLLT treated teeth was 1.24 (Table 2). The differences

Dr. Raluca Băleanu 96
between intervention and sham in terms of the ratio between pulp canal and calcified tooth
structure in all three groups were shown in Figure 2 and Figure 3.
Univariate analysis of variance (ANOVA) demonstrated that the pulp volume changes in TM
group and Ret groups were not statistically different (Table 3). There was no correlation
between differences in pulp to hard tissue volume ratio and difference in the total amount of
root resorption craters between the experimental and control groups among all three
groups. (Table 4)
The intra-rater reliability test revealed the coefficient of variation was less than 1% for all
measurements.
Discussion
This is the first human study using Micro-CT to assess the effect of LLLT on pulp volume
changes in maxillary first premolars undergoing orthodontic treatment and retention.
The premolars used in this study were convenient samples obtained from two previous
randomized controlled trials.29,30 Due to the slightly different micro-CT settings used in two
studies, pulp canal to hard tissue volume ratio was analysed instead of the actual pulp canal
and hard tissue volumes. Results of the current study revealed that LLLT teeth exhibited a
larger pulp canal to hard tissue volume ratio than the controls in both TM group and Ret
groups, however, the findings did not reach statistical significance. Results also indicated that
teeth which received continuous LLLT had a lower pulp to hard tissue volume ratio compared
to the controls, while teeth which received pulsed LLLT had a higher pulp to hard tissue
volume ratio compared to the controls. Again, these outcomes were not statistically
significant. Further, there was no statistically significant correlation between pulp canal to

Dr. Raluca Băleanu 97
hard tissue volume ratio and difference in the amount of root resorption craters in all three
groups.
In contrast to the outcomes of this study, literature pertaining to the effects of LLLT on pulp
tissue after the application of orthodontic force were linked to an increase in the repair of
the pulp tissue.31,32 However, it is important to note that due to the difference in study
designs and laser parameters used, as well as the evaluation methods, results of different
studies are not able to be compared directly.
The result of the current study could possibly be explained by the fact that only the portion of
the tooth below the CEJ was analysed as the great individual variation of crown morphology
may have confounded results. Thus, changes such as presence of pulp stones33,34,35 and
deposition of secondary dentin36 occurring at the coronal part of the pulp could not be
detected.
Another possible explanation for the outcome of the current findings could be that the
magnitude and duration of orthodontic force applied in this study did not impose detrimental
effects on pulpal tissue. Pulp tissue has an adaptive response which favors the repair from
the initial injury. 31 A study using laser doppler flowmetry demonstrated that there is an
immediate reduction in blood flow after orthodontic force application. This is followed by a
reactive hyperemia after approximately half an hour. The rate of blood flow was shown to
return to normal within 72 hours. 37
In addition, the extent of immersion and diffraction of LLLT could also be affected by tissue
molecules such as hemoproteins and melanin. 38 Therefore, the amount of light energy
reaching the target tissue also depends on their melanin composition and thickness of

Dr. Raluca Băleanu 98
alveolar bone. Conversely, differences may have occurred due to dental structure variability.
even though in both groups the wavelengths at the range of reported penetration depths,
showed no differences between irradiated groups and sham. Further research should be
undertaken on investigating the energy delivered to the periodontal ligament and the use of
greater range wavelengths.
Further, multiple mechanisms regarding the interaction of light energy from LLLT, aiming to
the target tissue are affected through countless variables such as light source- power, spot
size, number and frequency of applicability, application time, and application energy. 39
Further studies, which take these variables into account, will need to be undertaken.
Limitations
The results of this study could be confounded by the different laser parameters applied
throughout TM group and the Ret groups, along with the different types of tooth movement
that are applied to teeth during treatment.29,30 A previous study has revealed that while LLLT
with a wavelength longer than 600nm offers a stimulatory effect on cellular
metabolism,22,23,24,25 wavelengths in the near-infrared range of 810nm-830nm are
demonstrated to have more superior penetration power hence more effective than
wavelengths in the range of 630-680nm in promoting healing, reduction in inflammation and
pain.38 Another limitation of this study is the small sample size.29,30 LLLT teeth in both TM
group and Ret group exhibited a larger pulp to hard tissue volume ratio than the sham, but
the result did not reach statistical significance.
Factors which affects pulp canal volume such as age 40-44, hormones45-47, nutrition48, and
infection49. may potentially confound the result of the study. However, the teeth involved in

Dr. Raluca Băleanu 99
the study are caries free, and the rate of dentine deposition brought about by these factors is
rather slow, the effect of these factors on the result should be limited.
Generalizability
The interventions could only be carried out for a relative short duration of time due to ethical
reasons30 therefore the results of the current study may not be able to generalized to the
clinical setting. Ideally, prospective research that follows the participants for the full length of
orthodontic treatments should be conducted, however due to the nature of the study which
uses MicroCT, this was not possible.
Conclusions
No statistically significant difference was found in pulp canal to hard tissue volume ratio
between the LLLT teeth and the control teeth subjected to 150g of buccal tipping force
during force application and after 6 weeks of retention.
Dr. Raluca Băleanu 100
References
1. Proffit WR, Fields HW, Larson B, Sarver DM. Contemporary orthodontics-e-book. Elsevier Health Sciences; 2018 Aug 6.
2. Krishnan V, Davidovitch Ze. Cellular, molecular, and tissue-level reactions to orthodontic force. American Journal of Orthodontics and Dentofacial Orthopedics. 2006;129:469.e1-32.
3. Schwarz AM. Tissue changes incident to orthodontic tooth movement.AM J Orthod.1932;18:331-352.
4. Lino S. Acceleration of orthodontic tooth movement by alveolar corticotomy in the dog. Am J Orthodontics Dentofacial Orthopedics.2007;131:448e1-8.
5. Popp TW, Årtun J, Linge L. Pulpal response to orthodontic tooth movement in adolescents: a radiographic study. American Journal of Orthodontics and Dentofacial Orthopedics. 1992;101(3):228-33.
6. Butcher E, Taylor A. The effects of denervation and ischemia upon the teeth of the monkey. J Dent Res .1951;30:265-75.
7. Butcher E, Taylor A. The vascularity of the incisor pulp of the monkey and its alteration by tooth retraction. J Dent Res 1952;31:239-47.
8. Oppenheim A. Human tissue response to orthodontic intervention of short and long duration. AMJ ORTHOD.1942;28:263-301.
9. Marshall JA. A study of bone and tooth changes incident to experimental tooth movement and its application to orthodontic practice: Summary to Date of the Research Conducted Under Grants From the American Society of Orthodontists and the Board of Research of the University of California. International Journal of Orthodontia and Dentistry for Children. 1933;19(1):1-21.
10. Stenvik A, Mj0r A. Pulp and dentine reactions to experimental tooth intrusion. AM J ORTHOD.1970;57:370-85.
11. Anstendig H, Kronman J.A histologic study of pulpal reaction to orthodontic tooth movement in dogs. Angle Orthod. 1972; 42:50-5.
12. Barwick PJ, Ramsay DS. Effect of brief intrusive force on human pulpal blood flow. Am J Orthod Dentofac Orthop .1996; 110(3):273-9.
13. Hamersky P, Weimar A, Taintor J. The effect of orthodontic force application on the pulpal tissue respiration rate in the human premolar. AMJ ORTHOD.1980;77:368-78.
14. Derringer KA, Jaggers D.C. and Linden R.W.A. Angiogenesis in Human Dental Pulp Following Orthodontic Tooth Movement J Dent Res.1996;75:1761-1766.
15. Yadav S, Dobie T, Assefnia A, Gupta H, Kalajzic Z, Nanda R. Effect of low-frequency mechanical vibration on orthodontic tooth movement. American Journal of Orthodontics and Dentofacial Orthopedics. 2015;148(3):440-9.
16. Cohn SA. Disuse atrophy of the periodontium in mice. Archives of Oral Biology.1965;10:917-918.
17. Cohn SA. Disuse atrophy of the periodontium in mice following partial loss of function. Archives of Oral Biology, 1966. - IN23, 103, IN25, 5-2, IN24, 4, IN26.5 : Vol. 11(1):95.

Dr. Raluca Băleanu 101
18. Kaneko S, Ohashi K, Soma K, Yanagishita M. Occlusal hypofunction causes changes of proteoglycan content in the rat periodontal ligament. Journal of Periodontal Research.2001; 36(1): 9-17.
19. Venkatesh S, Ajmera S, Ganeshkar SV. Volumetric pulp changes after orthodontic treatment determined by cone-beam computed tomography. Journal of endodontics. 2014 Nov 1;40(11):1758-63.
20. Youssef M, Ashkar S, Hamade E, Gutknecht N, Lampert F, Mir M. The effect of low-level laser therapy during orthodontic movement: a preliminary study.Lasers Med Sci., 2008; 23(1):27-33.
21. Lim HM Lew KK, Tay DK. A clinical investigation of the efficacy of low level laser therapy in reducing orthodontic post adjustment pain. Am J Orthod Dentofacial Orthop., 1995;108(6):614-22.
22. Basford JR. Low intensity laser therapy: still not an established clinical tool. Lasers Surg Med.1995;16: 331– 42.
23. Pöntinen PJ. Low Level Laser Therapy as a Medical Treatment Modality: a Manual for Physicians, Dentists, Physiotherapists and Veterinary Surgeons. : Tampere: Art Urpo Ltd.; 1992.
24. Ohshiro T, Calderhead RG. Low Level Laser Therapy: a Practical Introduction. Chichester; New York: Wiley; 1988.
25. Sun G, Tuner J.Low-level laser therapy in dentistry. Dent Clin North Am.2004;48:1061–76.
26. Kawasaki K ,Shimizu N. Effects of low-energy laser irradiation on bone remodeling during experimental tooth movement in rats. Lasers Med.2000;26:282-291.
27. Torri S, Weber JBB. Influence of Low-Level Laser Therapy on the Rate of Orthodontic Movement: A Literature Review. Photomed Laser Surg.2013;31:411-21.
28. da Silva Sousa MV, Scanavini MA, Sannomiya EK, Velasco LG, Angelieri F. Influence of low-level laser on the speed of orthodontic movement. Photomed Laser Surg.2011; 29:191-96.
29. Ng D, Chan AK, Papadopoulou AK, Dalci O, Petocz P, Darendeliler MA. The effect of low-level laser therapy on orthodontically induced root resorption: a pilot double blind randomized controlled trial. Eur J Orthod. 2018;40(3):317-325.
30. Ang Khaw CM, Dalci O, Foley M, Petocz P, Darendeliler MA, Papadopoulou AK. Physical properties of root cementum: Part 27. Effect of low-level laser therapy on the repair of orthodontically induced inflammatory root resorption: A double-blind, split-mouth, randomized controlled clinical trial. Am J Orthod Dentofacial Orthop. 2018;154(3):326-336.
31. Domínguez &, Ballesteros RE, Viáfara JH, Tamayo OM. Effect of low level laser therapy on dental pulp during orthodontic movement. World J Methodol. 2013; 3(2): 19-26.
32. Abi-Ramia LB, Stuani AS, Stuani AS, Stuani MB, Mendes Ade M. Effects of low-level laser therapy and orthodontic tooth movement on dental pulps in rats. Angle Orthod. 2010;80(1):116-122.
33. Goga R, Chandler NP, Oginni AO. Pulp stones: a review. Int Endod J. 2008;41(6):457-68.

Dr. Raluca Băleanu 102
34. Han G, Hu M, Zhang Y, Jiang H. Pulp vitality and histologic changes in human dental pulp after the application of moderate and severe intrusive orthodontic forces. Am J Orthod Dentofacial Orthop. 2013;144(4):518-22.
35. Lazzaretti DN, Bortoluzzi GS, Torres Fernandes LF, Rodriguez R, Grehs RA, Martins Hartmann MS. Histologic evaluation of human pulp tissue after orthodontic intrusion. J Endod. 2014;40(10):1537-40.
36. Marshall JA. A study of bone and tooth changes incident to experimental tooth movement and its application to orthodontic practice: Summary to Date of the Research Conducted Under Grants From the American Society of Orthodontists and the Board of Research of the University of California. International Journal of Orthodontia and Dentistry for Children. 1933;19(1):1-21.
37. McDonald F, Pitt Ford TR. Blood flow changes in permanent maxillary canines during retraction. The European Journal of Orthodontics. 1994;16(1):1-9.
38. Yadav A, Gupa A. Noninvasive red and near- infrared wave-length-induced low level laser therapy: promoting impaired cuta-neous wound healing. Photodermatol Photoimmunol Pthotomed .2017;33;4-13.
39. Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng.2012;40:516-533.
40. Kavas AA, Tümen ECJIDR (2019) Volumetric pulp chambers measurements in mandibular and maxillary permanent first molar using cone-beam computed tomography by age and gender. Int Dent Res 9(1):30–40
41. Pinchi V, Pradella F, Buti J, Baldinotti C, Focardi M, Norelli GA. A new age estimation procedure based on the 3D CBCT study of the pulp cavity and hard tissues of the teeth for forensic purposes: A pilot study.J Forensic Leg Med. 2015 Nov;36():150-7.
42. Star H, Thevissen P, Jacobs R, Fieuws S, Solheim T, Willems G.Human dental age estimation by calculation of pulp-tooth volume ratios yielded on clinically acquired cone beam computed tomography images of monoradicular teeth. J Forensic Sci 2011 Jan; 56 Suppl 1():S77-82.
43. Tardivo D, Sastre J, Ruquet M, Thollon L, Adalian P, Leonetti G, Foti B Three-dimensional modeling of the various volumes of canines to determine age and sex: a preliminary study. J Forensic Sci. 2011 May; 56(3):766-70.
44. Kazmi S, Mânica S, Revie G, Shepherd S, Hector M (2019) Age estimation using canine pulp volumes in adults: a CBCT image analysis. Int J Leg Med 133(6):1967–1976.
45. Xu T, Yan M, Wang Y et al. (2014) Estrogen deficiency reduces the dentinogenic capacity of rat lower incisors J Mol Histol 45, 11-9
46. Zhu Y, Liu S, Chen W, et al. Epidemiology of low-energy fracture in Chinese postmenopausal women: changing trend of incidence since menopause and associated risk factors, a national population-based survey. Menopause. 2019;26:286-292.
47. Sturdee DW, Pines A. Updated IMS recommendations on postmenopausal hormone therapy and preventive strategies for midlife health. Climacteric. 2011;14(3):302-320.
48. Selig, K. R., Kupczik, K., & Silcox, M. T. (2021). The effect of high wear diets on the relative pulp volume of the lower molars. Am J Phys Anthropol.2021;174:804–811

Dr. Raluca Băleanu 103
49. Olgart, L. & Bergenholtz, G. The dentine-pulp complex: responses to adverse in uences. In: Bergenholtz, G., Hørsted-Bindslev, P. & Reit, C. Textbook of endodontology. (2003). 1st ed, Blackwell Munksgaard, Oxford (pp.21-42).

Dr. Raluca Băleanu 104
List of tables and figures
Figure 1. AVIZO Workflow
Step Module Sub-settings/steps Justification
1 Extract sub-volume Default To crop each tomogram down to
a minimal size
2 Edit new label field: Crown, Root,
Pulp Canal (2) Threshold tool To select material
(2) Fill volume To fill pores
(2) Assign selection to
label [+]
To tag material for subsequent
label analysis
(2) Circular paint tool To select tap and bottom of
volume
(2) Interpolate To select volume between
regions selected at(4)
(2) Assign selection to
label [+]
To tag volume for subsequent
label analysis
3 Label analysis Interpretation – 3D Volume
analysis
To calculate the volume of the
tagged regions selected
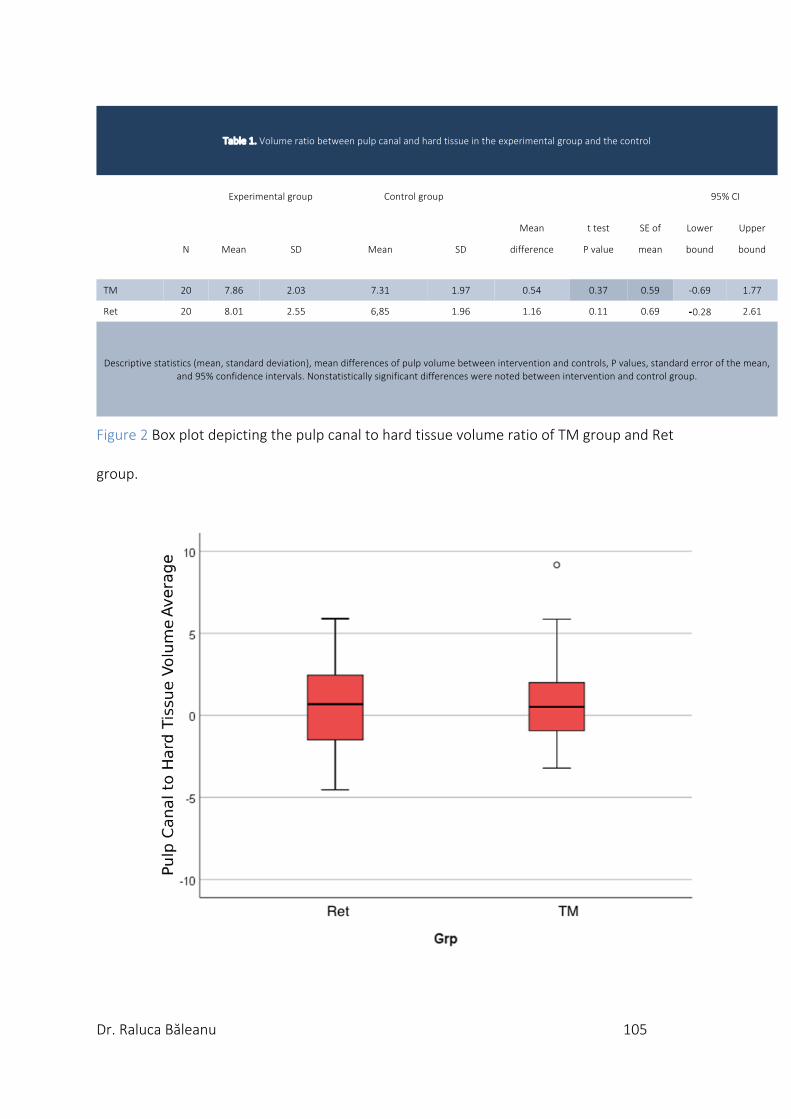
Dr. Raluca Băleanu 105
Table 1. Volume ratio between pulp canal and hard tissue in the experimental group and the control
Experimental group Control group
95% CI
Mean t test SE of Lower Upper
N Mean SD Mean SD difference P value mean bound bound
TM 20 7.86 2.03 7.31 1.97 0.54 0.37 0.59 -0.69 1.77
Ret 20 8.01 2.55 6,85 1.96 1.16 0.11 0.69 ⁃0.28 2.61
Descriptive statistics (mean, standard deviation), mean differences of pulp volume between intervention and controls, P values, standard error of the mean, and 95% confidence intervals. Nonstatistically significant differences were noted between intervention and control group.
Figure 2 Box plot depicting the pulp canal to hard tissue volume ratio of TM group and Ret
group.

Dr. Raluca Băleanu 106
Table2.Volumeratiobetweenpulpcanalandhardtissueintheexperimentalgroupandthecontrol
Experimental group Control group
95% CI
Mean t test SE of Lower Upper N Mean SD Mean SD difference P value mean bound bound
TM-A 10 7.93 1.67 8.10 2.01 -0.14 0.82 0.62 -1.55 1.25
TM-B 10 7.78 2.44 6.54 1.69 1.24 1.26 0.99 -1.10 3.46
Ret 20 8.01 2.55 6.85 1.96 1.16 0.11 0.69 ⁃0.28 2.61
Descriptive statistics (total, mean, standard deviation), mean differences, average pulp volume (mm3) between laser and the controls, P values, standard error of the mean and 95% confidence intervals. Nonstatistically significant differences were noted between laser and the controls for all pulp volume.
Figure 3. Box plot depicting the pulp canal to hard tissue volume ratio of TM-A group, TM-B
group and Ret group.

Dr. Raluca Băleanu 107
Table 3. Univariate analysis of variance (ANOVA) investigating difference between TM group and Ret group
Sum of squares df Mean square F Sig.
3.83 1 3.8 0.47 0.50
Table 4. . Correlation between pulp volume changes and difference in total amount of root resorption craters among all three groups
TM vs Ret TM-A vs Ret TM-B vs ret
Pearson Correlation -0.21 -0.14 -0.19
Significance 0.20 0.48 0.31
Dr. Raluca Băleanu 108
CONCLUSION
To date, there is no consensus regarding the effects of orthodontic treatment on the dental
pulp. Further, despite being a key component in the anatomy and physiology of the dentition,
pulpal tissue is still not well documented and described, especially in regard to our everyday
orthodontic practice. In addition, the effect of LLLT and PBP on the pulp is poorly understood.
Even though interventions aiming to accelerate orthodontic tooth movement, such as the
use of LLLT and PBM, open up huge possibilities in the quest to shorten orthodontic
treatment and reduce complications, such advances in technology cannot replace the
thorough clinical examination as well as good treatment and biomechanical
planning. However, since those accelerated tooth movement methods are out there and
being promoted by companies, it is our duty as researchers to understand their effects on
oral tissues.
The current study contains numerous confounding factors which may affect the reliability
and applicability of the outcomes. It is obvious that the results of the current study may not
have a significant impact on our current practice in orthodontics. However, previous
randomized control trials on this subject have collected valuable images of maxillary first
premolars which had received LLLT/LED-PBM during orthodontic tooth movement and in
retention. It was worthwhile therefore to analyze this readily available data and in doing so
add to the current best available evidence. We do not know whether the results of the pulp
canal volume reflect what happens to the pulp and this needs to be investigated further.
Furthermore, the results of current study could not be generalized to an entire course of

Dr. Raluca Băleanu 109
orthodontic treatment because of the short study duration imposed by ethics criteria and the
singular tooth movement studied.
Despite the shortcomings with this study, it is a pilot study and has provided some framework
on which future studies could be based. For future studies, teeth undergoing longer
durations of these applications as well as different types of orthodontic tooth movement
should be analysed with histology and immunohistochemistry to provide a better
understanding of these interventions on tooth pulp structures.

Dr. Raluca Băleanu 110
Appendix: AVIZO Figures
1.Importing the micro-CT scans of teeth into Avizo 3d software. 2.Using ‘Ortho slice’ function to double check if the dataset has imported correctly.
3.Segment the crown of the tooth using the magic wand in 3D.
4.Applying ‘Convex hull’ function do fill the volume from crown to the CEJ the tooth.

Dr. Raluca Băleanu 111
5.Verifying if ‘Convex hull’ function work out. 6.Selection of the calcified root structure using Magic Wand tool in 3D with “Same material only” limit applied to avoid the crown volume.
7.Selection of the calcified root structure. 8.Applying ‘Fill all slices’ function to crate the non-calcified internal tooth structure representing the pulp tissue.

Dr. Raluca Băleanu 112
9.Digitally extracted pulp canal tissue. 10.Digitally extracted tooth prepared for the volumetric analysis.
11. Applying “Material statistics” function for the volumetric analysis of calcified and non-calcified (pulp canal) tissue.









![Phototherapy, Photochemotherapy, and Excimer Laser Therapy ... · Excimer Laser Therapy Office-based targeted excimer laser therapy (i.e., 308 nanometers [nm]) is considered medically](https://img.pdfslide.us/doc/110x75/5f14ea18414c5a02c231f9fa/phototherapy-photochemotherapy-and-excimer-laser-therapy-excimer-laser-therapy.jpg)



















