Embed Size (px)
Citation preview
THE EFFECTS O F EMBOLIC OBSTRUCTION OF INTRA- RENAL ARTERIES IN THE RABBIT
NATALIE ALEXANDER*, R. H. HEPTINSTALLt and G . w. PICRERING Department of the Regius Profesaor of Medicine, Oxford University, and
Department of Morbid Anatomy, St Mary'a Hospital, London
(PLATES LXX-LXXIII)
DURING the past 25 years many experiments have been performed to demonstrate the relationship between interference with the blood supply of the kidney and elevation of blood pressure. Most of these investigations have been concerned with occlusion of the main renal artery and comparatively little is known about obstruction to its smaller branches. The present experiment was performed to study how embolism of arteries of arcuate or interlobular size would affect renal parenchyma, blood pressure and blood urea levels.
f i T E R I A L S AND METHODS
Operation for introduction of emboli Thirty-six rabbits of either sex, each weighing approximately 2& kg., were
used. Under anesthesia the left femoral artery was exposed in the thigh and the abdomen opened aseptically. In 26 animals the right kidney was removed, weighed and placed in formol-saline. One hundred to two hundred units of heparin were injected intravenously and a 2O-cm.-long catheter (no. 1 nylon tubing) with a bent tip and stiffened with a wire stylus, waa filled with normal saline and threaded through the femoral artery up the aorta into the left renal artery. The catheter waa connected through a glass adapter to a vertical tapered glass tube with a side arm leading to a pressure bottle and mercury manometer. The wire stylus extended from the top of the glass tube into the catheter and waa removed when the catheter was M y in the renal artery. The particles to be injected (suspended in autoclaved 15 per cent. mmia) were then poured into the small amount of sterile saline in the glass tube, which waa then closed with a bung and the pressure raised to 100 or 120 mm. Hg. The particles were seen to flow quickly through the catheter into the renal artery in single file. The catheter was then withdrawn and the incisions closed. The maximum time from insertion of the catheter to its withdrawal waa 10 min., and the usual time 3-5 min. Renal blood flow waa not necessarily cut off during this time because the artery often dilated and blood flowed past the catheter.
Part ich uaed aa emboli Preliminary trials were carried out to find particles of uniform size, which
would not clump, and which would produce the minimum foreign-body reaction in the kidney. Furthermore, no material could be used which would interfere with sectioning or be dissolved in staining.
~ ~~~~ ~~ ~ ~
Research Fellow of The American Heart Association. Present address : Depart-
t. Present address: Department of Pathology, Weshington University School of
J. PATE. DACT.-VOL. 81 (1961) 226 P
ment of Physiology, University of Southern California, Los Angeles 7, U.S.A.
Medicme, St Louis 10, Mo., U.S.A.
226 ALEXANDER, HEPTINSTALL AND PICKEBING
Lobelia (Cambridge blue) seeds were most .satisfactory and were used in 28 rabbits. They are elliptical seeds 430 x 630 ( 30) p in size. In two experiments brine shrimp (Arlemia) eggs were used. When soaked in saline these became spheres of 180-200 p diameter. Polystyrene spheres were used in one rabbit, most of them 100-300 p but some as small as 30 p diameter. In 6 experiments blood clots 1-3 mm. diameter were used. These were made by sucking blood from the animal’s own ear vein into a sterile fine siliconed pipette from which drops were allowed to fall on the inside wall of sterilised beakers coated with paraffin or silicone. The drops were either dried overnight (“ dried ” clots) and then washed into saline, or after coagulation were covered with saline to prevent drying and one hour later washed into saline for injection (“ fresh ” clots) ; the latter were prepared 2-4 hr before injection. Although blood clots made desirable emboli from a physiological standpoint, they were less satisfactory than the other particles for two reasons : fist, in-vivo lysis occurs to a con- siderable degree; and second, such clots are able to squeeze into vessels of different sizes.
Forty to 150 lobelia seeds, 118-125 shrimp eggs, or 100-200 clots were the amounts injected. The number of polystyrene spheres was not known.
Blood preasure and blood urea
Blood-pressure readings were made on the central ear artery by the method of Grant and Rothschild (1934), observing the precautions taken by Pickering and Prinzmetal (1937-38). Several base-line pressures were obtained before operation ; pressures were taken 4 times per week during the first two post- operative weeks and twice per week thereafter.
Blood urea was determined photometrically after nesslerisation of protein- free filtrates obtained by zinc hydroxide precipitation, which prevented turbidity after addition of Nessler’s reagent. Only one control urea was obtained and no attempt was made to standardise time of blood collcction in relation to food and water intake.
Poat-mcwtem and microscopic examidion The rabbits were killed with intravenous Nembutal at intervals of one hour
to 150 days, and the kidneys and hearts weighed and fixed in formol-saline. The carcase was weighed after removal of the viscera. After 48 hours’ fixation the kidneys were photographed and pieces removed for section. These were stained with hamatoxylin and eosin or hsmatoxylin and Van Gieson’s stain, and by the periodic acid-Schiff method, the Hart-Sheridan method for elastin or Wilder’s method for reticulin.
Anatomical location of emboli Additional animals were used to establish the position of the emboli. Im-
mediately after death the renal artery and vein were cannulated. The arterial cannula was connected by a Y-tube to two Erlenmeyer flasks, one filled with saline, the other with lead chromate suspended in 10 per cent. gelatin. These were immersed in warm water and connected to a pressure bottle and manometer. Saline was first perfused through the kidney until clear fluid flowed from the renal vein and lead chromate was then injected at pressurea of 120-140 mm. Hg for 5-10 min. The kidney pediele was then tied and the kidney fixed in formol- saline. It was then frozen firmly to the end of an aluminium rod immersed in dry ice and acetone. The rod with affixed kidney was then clamped to the carriage of an ordinary bacon slicer and the kidney cut into uniform slices 3 mm. or less thick. The slices were stacked between metal disks, dehydrated and cleared in methyl salicylate.
J. PATH. BACT.-VOL. 81
INTRARENAL EMBOLISX
PLATE LXX
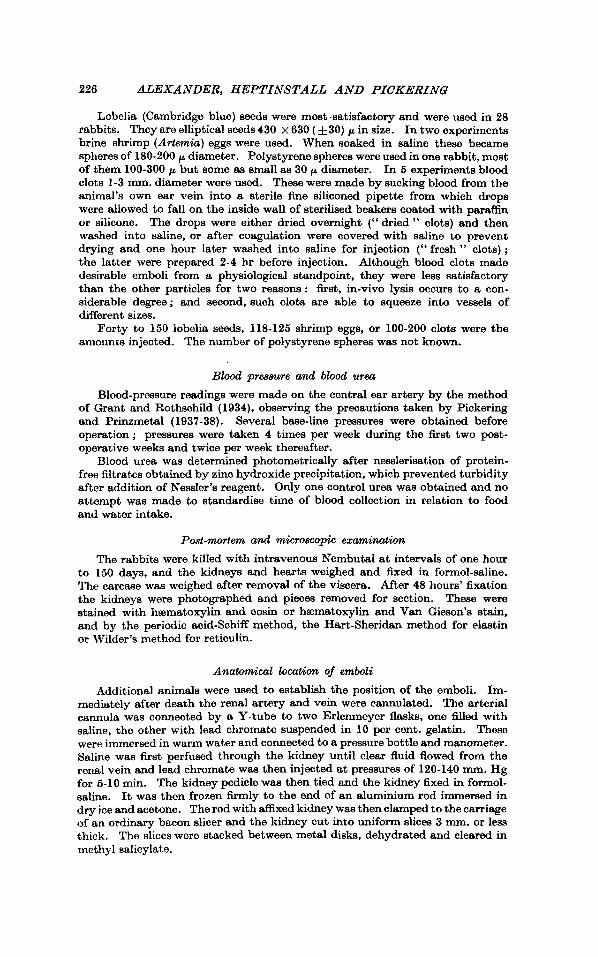
FIG. I.-Cleared kidney slice to show impaction of lobelia seed in arcuate artery. x 25.
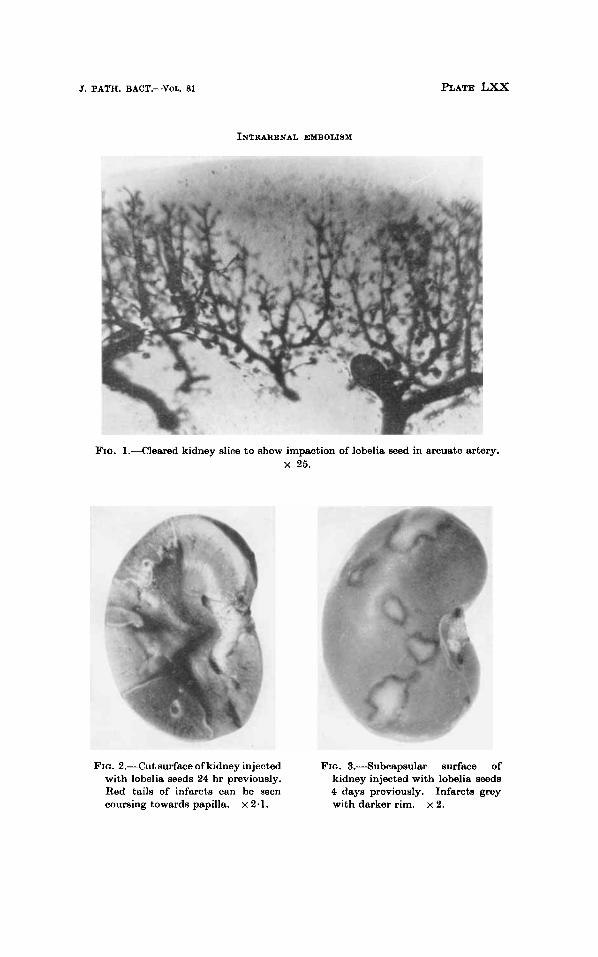
FIG. 2.-Cut surface of kidney injected FIG. 3.Subcapsular surface of with lobelia seeds 24 hr previously. kidney injected with lobelia seeds Red tails of infarcts can be seen 4 days previously. Infarcts grey coursing towards papilla. x 2.1. with darker rim. x 2.
INTRARENAL EMBOLISM 227
RESULTS Anatomical location of emboli
Clearing techniques showed that lobelia seeds became impacted in arcuate arteries and in the early parts of the interlobular arteries (fig. 1). Brine shrimp eggs were found in interlobular arteries, but fibrin clots were inconstant in their distribution and it was clear that considerable fibrinolysis had occurred.
Macroscopic pathological findings One hour after the introduction of emboli red areas of various sizes
were seen beneath the renal capsule, and in cut section these were triangular with the apex pointing towards the papilla.
At 6 hr the subcapsular surface was paler, small infarcts being grey and larger ones grey-red, both having a narrow red rim round the peri- phery. On cut surface the infarcts were mottled grey and red and were triangular in shape, with a prominent deep red tail extending into the papilla. The appearance at 12 hr was essentially the same except that the cortical portion was even paler in contrast with the medullary tail.
At 24 hr the subcapsular lesion was grey and the only redness was a thin peripheral rim less than 0.6 mm. wide, the cortical portion being grey or greyish-red with the red tail still persisting (fig. 2). At 4 days (fig. 3) the appearance was little altered, except that the cut surface of the infarct had a grey-yellow tinge in the cortical portion.
Seven-day infarcts tended to be rather depressed below the sub- capsular surface and the peripheral red rim w w now lost; thin red streamers still coursed towards the papilla. At 14 days both the sub- capsular and cut-surface colour was yellow and there was no red stream- ing in the medulla.
At 28 days the scars were definitely depressed below the surface and firmer than at earlier stages. From this time onwards the depression below the surface became more noticeable and the scars were now grey in colour, much firmer and in general smaller (figs. 4 and 5).
In rabbits receiving emboli, in which the other kidney was not excised, the injected kidneys were heavier than the non-injected up to 7 days from the date of injection. In those killed after 13 days the non-injected ones were heavier.
Histology The terminology of Sheehan and Davis (1958 and 1959) will be
used. At 1 hr the gross red areas show considerable congestion of the
glomerular tufts and the intertubular capillaries, this congestion spreading into the pyramid.
2 28 ALEXANDER, HEPTINSTALL AND PICKERING
By 6 hr the infarcted areas are clearly distinguishable from the surrounding kidney substance. Glomeruli are stuffed with red blood cells and intertubular capillaries are engorged as at 1 hr. Engorgement of the capillaries extends right down to the deeper part of the cortex and to the medulla. Proximal convoluted tubules have a pale granular cytoplasm which has retracted away from the basement membrane (sleeve separation) and occasional nuclei are pyknotic. At this time two clearly demarcated zones can be seen at the edge of the infarct. Continuous with this central dead area is a zone (peripheral dead zone) in which there is karyorrhexis and pyknosis of the nuclei of proximal convoluted tubules, whose cytoplasm is more eosinophilic than that of tubules in the central zone. Glomeruli and intertubular capillaries are engorged with red blood cells. Outside this is a zone (marginal zone) in which the glomeruli are only slightly congested and contain occasional polymorphs, and in which the proximal con- voluted tubules show little change.
At 12 hr the central dead area shows little additional change except that sleeve separation is more pronounced. A thin zone of polymorphs is now visible in the outer part of the central dead area, separating this from the peripheral dead zone. The latter shows greater pyknosis and karyorrhexis of nuclei of proximal convoluted tubules than the central area, and the glomeruli which show some nuclear loss are extremely congested. In the marginal zone there is little change except that the cytoplasm of the cells of the proximal convoluted tubules is more basophilic than that of healthy kidney.
A t 24 hr the central dead area shows tubules with paler-staining cytoplasm and some loss of nuclei. Glomeruli and intertubular capil- laries contain the shells of red blood cells which have lost their haemo- globin. There is no change in the reticulin pattern of the area. At the periphery of the central dead area a zone of polymorphs is now well formed (fig. 6). This zone is also well developed on the subcapsular boundary of the infarct, a thin rim of apparently healthy tubules persisting just beneath the capsule. Outside the polymorph zone the peripheral dead zone shows almost complete nuclear loss in proximal convoluted tubules, the cytoplasm showing considerable eosinophilia. Glomeruli, which show loss of nuclei, and ' intertubular capillaries contain large numbers of unaltered red blood cells. Arteries show no remarkable changes. In the marginal zone the cytoplasm of the proximal convoluted tubules is rather pale and finely vacuolated. The glomeruli contain no excess of red cells and apart from early adhesions show no gross change. In the deeper cortex and medullary part of the infarct the loops of Henle and some of the collecting tubules are necrotic. There is intense capillary congestion all the way down to the papilla, but in this position numerous collecting tubules persist. It is this capillary congestion that accounts for the red streaming seen
A t 4 and 7 days the central dead area shows greater loss of nuclei grossly.
J. PATH. BACT.-VOL. 81
INTRARENAL EMBOLISM
PLATE LXXl
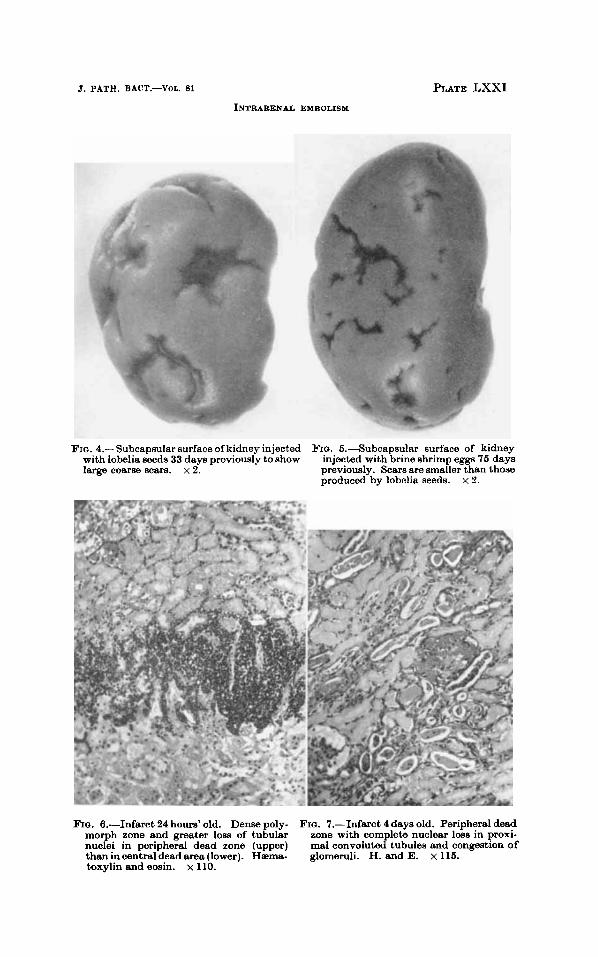
FIG. 4.-Subcapsular surface of kidney injected with lobelia seeds 33 days previously to show large coarse scars. x 2.
FIG. 5.Subcapsular surface of kidney injected with brine shrimp eggs 75 days previously. Scars are smaller than those produced by lobolia seeds. x 2.
BIG. 6.-Infarct 24 hours’ old. Dense poly- morph zone and greater loss of tubular nuclei in peripheral dead zone (upper) than in central dead area (lower). Heme- glomeruli. H. and E. x 115. toxylin and eosin. x 110.
FIG. 7.-Infasct 4 days old. Peripheral dead zone with complete nuclear loss in proxi- mal convoluted tubules and congestion of

INTRARENAL EMBOLISM 229
in proximal convoluted tubules, although some show remarkable persistence. Glomeruli and intertubular capillaries are almost blood- less and there is some loss of nuclei in glomeruli. The polymorph zone now shows karyorrhexis and nuclear powder is sometimes all that is left at 7 days. Immediately outside the polymorph zone the peripheral dead zone (fig. 7) shows complete nuclear loss in proximal convoluted tubules but some collecting tubules persist. Glomeruli show nuclear loss and are stuffed with red blood cells ; some are quite structure- less. At 4 days elongated cells which represent either vasoformative cells or fibroblasts appear between the necrotic tubules. The marginal zone shows patchy death of proximal convoluted tubules. Some proximal convoluted tubules are basophilic and lined by a lower type of cubical epithelium, whilst others are dilated and contain casts and nuclear debris; some contain mitotic figures. Collecting tubules are intact and some contain casts. Glomeruli may show localised necroses, localised areas of hyalinisation, or adhesions between tuft and Bowman’s capsule. In the interstitial tissue there is great cellular activity. Numerous elongated cells, such as were seen in the peripheral dead area, are present, and at 7 days very early fibrosis may be seen. Deep to the infarct are degenerate or necrotic loops of Henle with intact collecting tubules which may contain casts. Capillaries are still engorged in this area, which extends down to the medulla.
By 14 days the central dead area shows glomeruli which have now lost their nuclei and contain no red blood cells. Tubules show loss of nuclei with granular cytoplasm which sometimes contains large P.A.S.- positive granules. Calcification of necrotic tubules is often seen. At this time there is no tubular collapse and the reticulin pattern is normal. Some collecting tubules persist, apparently intact. Arteries and arterioles are usually unaffected but nuclear loss, swelling of the wall and luminal thrombus may be seen. The peripheral zone of poly- morphs has now completely disappeared and the peripheral dead zone is much smaller. In the marginal zone (fig. 8) glomeruli may be normal, show patchy hyalinisation or fibrosis, or have dilated capsular spaces. Many proximal convoluted tubules have disappeared and the predominant type is one with a small lumen and flattened or cubical epithelium and it is probable that these are attenuated proximal convoluted tubules. Sometimes these are dilated and contain casts. The amount of reticulin between the tubules is increased (fig. 9) and fine fibrosis can be seen. Some elongated cells of fibroblast type are present. Arteries and arterioles show no striking changes. At the apex of the scar, loops of Henle have collapsed, but some collecting tubules persist apparently undamaged. Interstitial reticulin is much increased and fine fibrosis is apparent but fibroblasts are uncommon. Arteries in general show no change but an occasional one shows some thickening.
Glomeruli are now present only in ghost form and calcification is plentiful in
At 25-33 days the central dead area shows collapse.
J. PATH BACT.-VOL. 81 (1961) P 2

230 ALEXANDER, HEPTINSTALL A N D PICKERING
the collapsing necrotic tubules. The reticulin pattern is still more or less preserved although reticulin is somewhat increased in the collapsed areas. The peripheral dead zone and marginal zone merge with each other, but in general are divided into two areas as regards tubular changes: an inner one where tubules are decreased in numbers and interstitial fibrosis is present, and an outer zone with no great decrease of tubules, which are, however, all lined by a relatively simple type of cubical epithelium. Glomeruli in this latter zone may be normal or show areas of fibrosis or hyalinisation of the tuft (fig. 10) and adhesions between the tuft and Bowman's capsule; the capsular space is frequently dilated. Because of the loss of tubules, arteries appear relatively increased in number but are not materially altered. In the apical area there is much loss of loops of Henle, relative persistence of collecting tubules, and great increase in fibrous tissue.
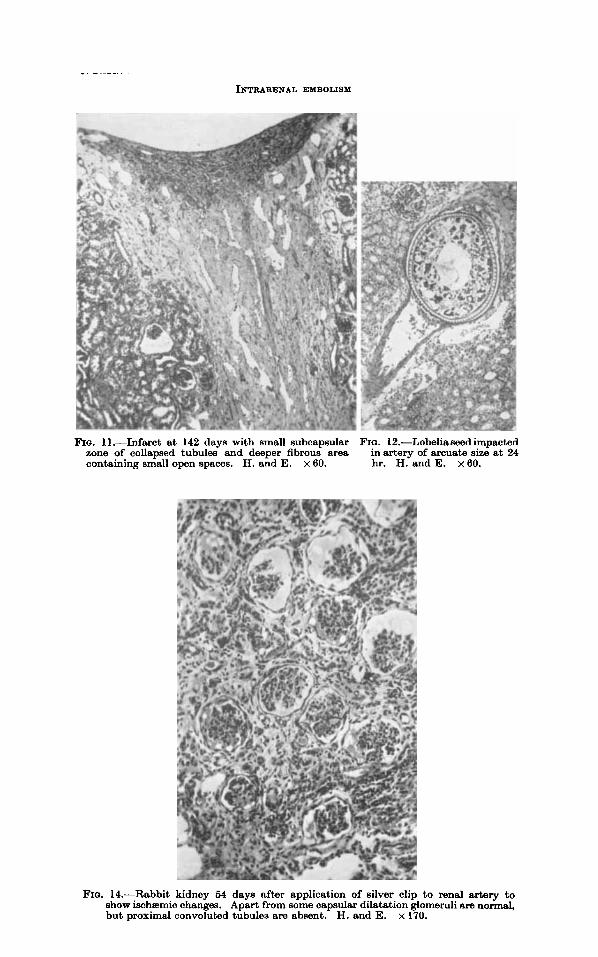
At 70 days considerable changes have taken place in the infarcted areas, varying according to the initial size of the infarcted area. Where the initial area was small there is little evidence of any necrotio tissue in the firm depressed scars. There is a small area under the capsule made up of collapsed basement membranes of dead tubules, and occasional vague ghosts of glomeruli are seen. Deep to this there is a zone of fibrosis containing small open spaces, the origin of which is not clear, and occasional simple tubules (fig. 11). At the edges of the triangular scars there are glomeruli either hyalinised or showing no change in the tuft, with dilated capsular spaces. Proximal convoluted tubules have disappeared and only simple tubules, often dilated, still persist. In cases where the initial areas of infarction were larger, necrotic tubular remnants, sometimes partially calcified, persist. The peripheral part with loss of tubules and deformed glomeruli is wider and shows much fibrosis.
At 140-150 days the picture resembles that at 70 days, except that the scars are in general less obtrusive and peripheral fibrosis is greater.
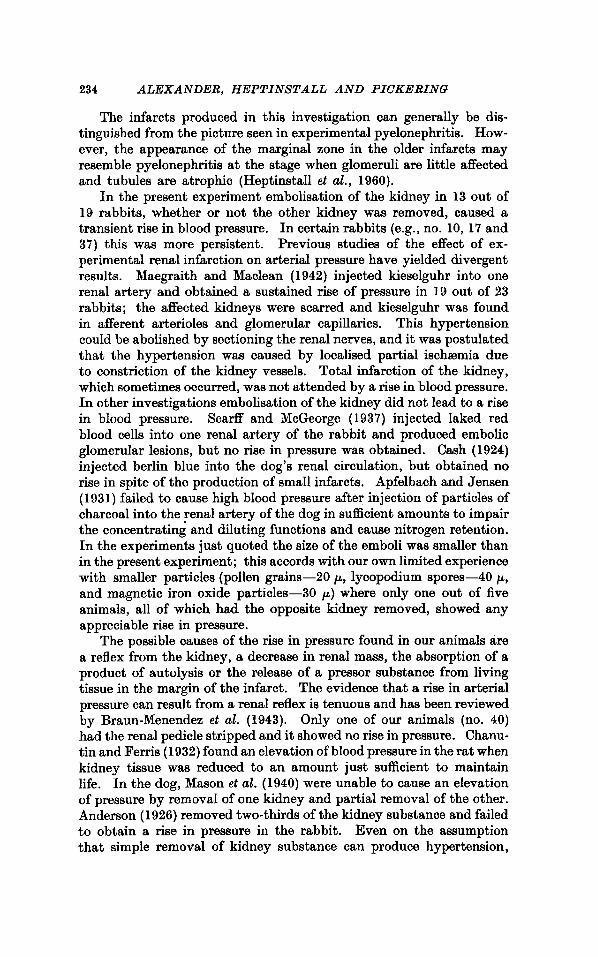
As brine shrimp eggs are found in the interlobular arteries usually early in their course, whilst lobelia seeds are found in interlobular arteries and in larger arteries of arcuate size (fig. 12), the infarcts were larger with lobelia seeds. Polystyrene spheres and fibrin emboli are found in both interlobular and arcuate arteries.
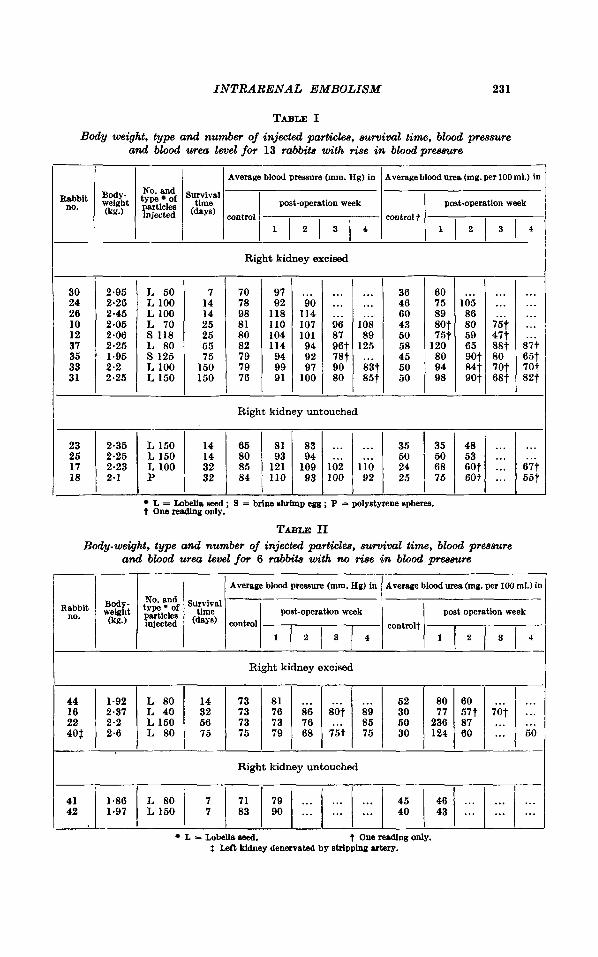
Changes in blood pressure and blood urea Blood pressure and blood urea were measured in 26 rabbits, which
received lobelia seeds (18), shrimp eggs (2), polystyrene spheres (l) , or fibrin emboli (5). Table I summarises up to the fourth week a group of 13 rabbits which showed a definite elevation of blood pressure. Table I1 summarises for the same'period animals in which no appreci- able rise was obtained. Blood pressure did not usually begin to rise until the third day after injection and as a rule reached a peak towards the end of the first week. During the second and third weeks it usually
INTRARENAL EMBOLISM
Average blood pressure (mm. Hg) in
Survival time post-oporation week
(days) cnntrol
231
Averageblood urea (mg. per 100 ml.) in
post-operation week control t
TABLE I Body weight, type and number of injected particles, ~uruival time, blood pressure
and blood urea level for 13 rabbits with h e in bloodpramre
757
80 70t 687
No. and type of particles injected
. . . . . .
. . . . . .
. . . . . . ... sit 65t 70t 82t
30 24 26 10 12 37 35 33 31
2.95 2.26
1 2.45 2.05 2.06 2.25
L 50 L 100 L 100 L 70 S 118 L 80
' 1.95 S 125
2.25 L 150 2.2 1 L 100
23 25 17 18
2.35 L 150 14 65 81 83 . . . . . . 35 48 . . . . . . 2.25 L 150 14 80 93 94 53 . . . . . . 2.23 L 100 32 85 121 109 Ib;i i 0 I 60t ... 67t 2.1 P 32 84 110 93 100 92 60t ... 55t
- 7
14 14 25 25 G5 75
150 150 -
Rabbit ~ o p - no. ?$it
70 78 98 81 80 82 79 79 76
Average blood pressure (mm. Hg) in I Average blood urea (mg. per 100 mi.) in '
$ktn:f survival - particles ''me injected control
post-operation week post operation week
- 97 92
118 I10 104 114 94 99 91
44 1-92 L 80
22 2.2 L 150 402 2.6 L 80
16 2.37 L 40
... 90
114 107 101 94 92 97
100
14 73 81 ... 52 80 60 ... 56 73 73 76 85 50 236 87 . . . . . . 75 75 79 68 i 5 t 75 30 124 60 ... 50
32 73 76 8s Sot 89 30 77 577 iot ...
... ...
... 96 87 get
80 2
...
...
... 108 89
125 ... 83t 85t
- 36 46 60 43 50 58 45 50 50
- 60 75 89 sot 75t
120 80 94 98
... 105 86 80 59 65 90t 84 t 90t
Right kidney untouched
L = Lobella seed ; 9 = brine 6hamp egg ; P = polystyrene spheres. t Onereadingonly.
Right kidney excised
Right kidney untouched I L = Lobella seed. t Onereadlngonly.
: Left kidney denervated by stripping artery.
232 ALEXANDER, HEPTINSTALL A N D PICKERING
1 , 0 ,
R d 8 8 . 1 JJ I PABB'T I?
140 I I
7 I20 ; 8 100 i r
I
I Rioeir e
I I
8 0
2 4 0 ' 2 0
M I30
i I20 ; 110 :lw z 90
00
'O
2 60
I.. . . I . I :. . .4
: ' . * : I . '
. I j 0 ; I
I I 1 -
I D
! 0 1 0 8 .
; I.
j - 1 0 0 . I *
j o B 1. ' :/ RlGNl XIONET EkWSEO $.w KroMEy mAcr fir mo ExcisEo
' . . I 8 0
D j e e 0 -
0 .
* q
L. :I
0 , a 'eon
100 SEE05 INTO LEFT K l O l w l ' too SEEDS i r xtmw I /is s w EGGS i r M
I
C S 10 IS 20 2S 30 35 4 0 4 S SO 55-60 SS 7 0 71 EO SS C 5 10 I5 20 25 30 3S C 5 I0 IS 20 25
232 ALEXANDER, HEPTINSTALL A N D PICKERING
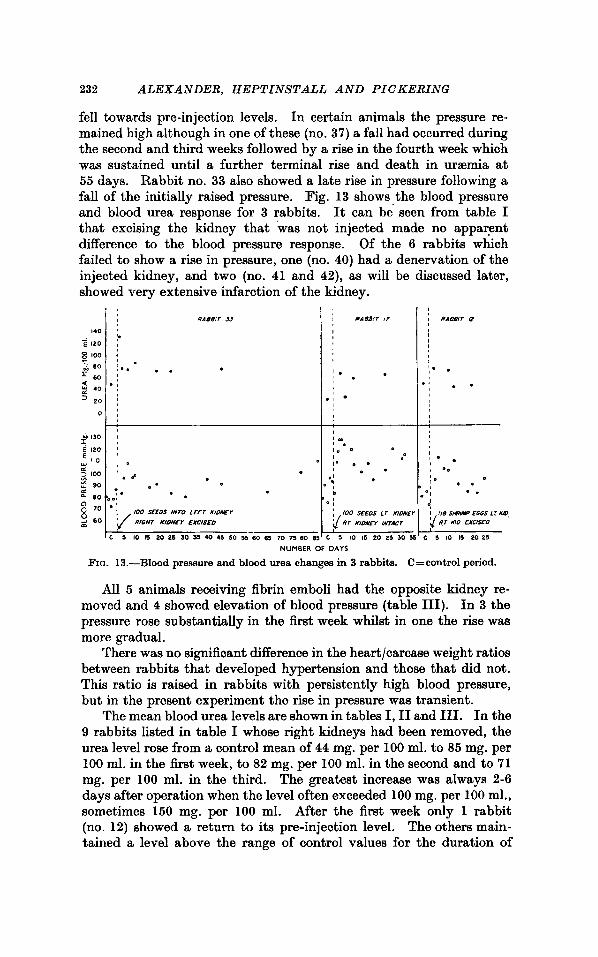
fell towards pre-injection levels. In certain animals the pressure re- mained high although in one of these (no. 37) a fall had occurred during the second and third weeks followed by a rise in the fourth week which was sustained until a further terminal rise and death in uraemia at 55 days. Rabbit no. 33 also showed a late rise in pressure following a fall of the initially raised pressure. Fig. 13 shows the blood pressure and blood urea response for 3 rabbits. It can be seen from table I that excising the kidney that was not injected made no apparent difference to the blood pressure response. Of the 6 rabbits which failed to show a rise in pressure, one (no. 40) had a denervation of the injected kidney, and two (no. 41 and 42), as will be discussed later, showed very extensive infarction of the kidney.
w u n n t n ur V A T )
FIG. 13.-Blood pressure and blood urea changes in 3 rabbits. C=control period.
All 5 animals receiving fibrin emboli had the opposite kidney re- moved and 4 showed elevation of blood pressure (table 111). In 3 the pressure rose substantially in the first week whilst in one the rise waa more gradual.
There was no significant difference in the heart/carcase weight ratios between rabbits that developed hypertension and those that did not. This ratio is raised in rabbits with persistently high blood pressure, but in the present experiment the rise in pressure was transient.
The mean blood urea levels are shown in tables I, I1 and 111. In the 9 rabbits listed in table I whose right kidneys had been removed, the urea level rose from a control mean of 44 mg. per 100 ml. to 85 mg. per 100 ml. in the first week, to 82 mg. per 100 ml. in the second and to 71 mg. per 100 ml. in the third. The greatest increase was always 2-6 days after operation when the level often exceeded 100 mg. per 100 ml., sometimes 150 mg. per 100 ml. After the first week only 1 rabbit (no. 12) showed a return to its pre-injection level. The others main- tained a level above the range of control values for the duration of
J. PATH. BACT.-YOL. 81
INTRARENAL EMBOLISM
PLATE LXXII
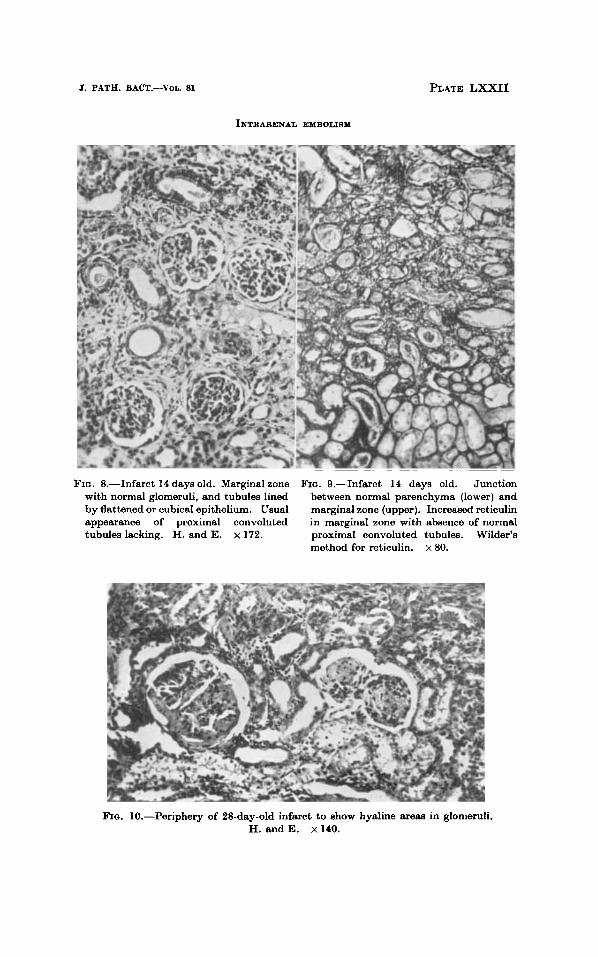
FIQ. 8.-Infarct 14 days old. Marginal zone with normal glomeruli, and tubules lined by flattened or cubical epithelium. Usual appearance of proximal convoluted tubules lacking. H. and E. x 172.
FIG. S.--Infarct 14 days old. Junction between normal parenchyma (lower) and marginal zone (upper). Increased reticulin in marginal zone with absence of normal proximal convoluted tubules. Wilder’s method for reticulin. x 80.
Fro. 10.-Periphery of 28-day-old infarct to show hyaline areas in glomeruli. H. and E. x 140.
INTRARENAL EMBOLISM
FIG. 11.-Infarct at 142 days with small subcapsular FIG. 12.-LobIiaseed impacted zone of collapsed tubules and deeper fibrous area inortery of arcuate size at 24 containing small open spaces. H. and E. x 60. hr. H. and E. x60.
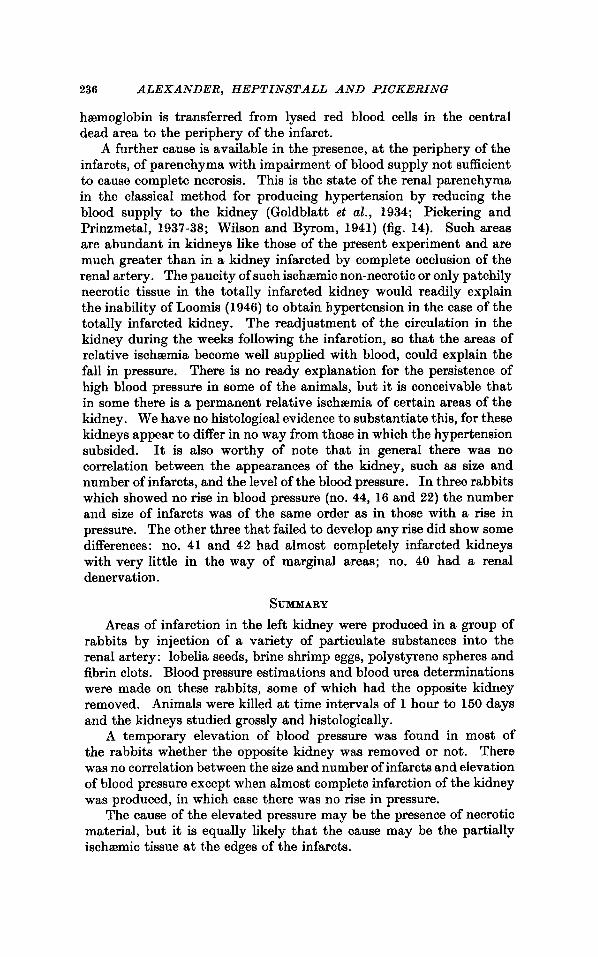
FIG. 14.-Rabbit kidney 54 days after application of silver clip t o renal artery to show ischemic changes. Apart from some capsular dilatation glomeruli nre normal, but proximal convoluted tubules are ahaent. H. and E. x 170.

INTRARENAL EMBOLISM 233
Rabbit no.
survival. The same general trend is found for rabbits receiving fibrin emboli (table 111).
Of the 6 rabbits with the right kidney untouched (tables I and 11) only two showed a definite increase in blood urea (no. 17 and 18) and these also had a greater blood pressure rise than the other 2 shown in table I (no. 23 and 25). To test the effect on blood urea of merely removing one kidney, 5 animals had the right kidney removed. No rise in blood urea occurred.
TABLE I11 Changes in blood pramre and blood urea in 5 rabbito receiving
fibrin emboli. Opposite kidney removed in each m e
Survival time
(days)
RC8 RC6
14 14 14 14 14
Average blood pressure (mm. IIg) in
1
96 98 97
' 87 82
Type of clot
control 2
-I
102 98 91 92 83
D F F D F
72 84 84 82 78
ulood urea (mg. per 100 ml.) in
corltrol
48 46 46 55 50
post-operation week
1
75 120 64 90 58
2
65 100 60 80 62
D =dried; F =fresh.
DISCUSSION Infarction haa frequently been studied in the kidney, but this
investigation hm relatively new features. The arteries stopped have been smaller and more comparable in size to those involved in human disease. Moreover, changes in renal function and arterial pressure have been recorded. Certain findings require further notice, although some of them have been described by Sheehan and Davis (1958 and 1959), who have also reviewed the ancient writings on infarction of the kidney.
The persistence of nuclei in the tubules of the central dead area is striking in comparison with their rapid loss in the peripheral dead zone. The different fates of the two dead zones is interesting; the central area undergoes a passive collapse, the peripheral an invasion by fibroblasts (fig. 11). The polymorph zone separates the central and peripheral dead zones; it is usually stated that polymorphs appear at the junction of dead and healthy tissue. The red rim seen round an infarct on gross inspection is congestion in the peripheral dead zone and not, as is usually supposed, in the healthy tissue surrounding the infarct. We have not always been able to resolve the marginal zone into a partial survival zone and a live margin zone aa described by Sheehan and Davis (1958), and therefore use the simple term marginal zone.
234 ALEXANDER, HEPTINSTALL AND PICKERING
The infarcts produced in this investigation can generally be dis- tinguished from the picture seen in experimental pyelonephritis. How- ever, the appearance of the marginal zone in the older infarcts may resemble pyelonephritis a t the stage when glomeruli are little affected and tubules are atrophic (Heptinstall et al., 1960).
In the present experiment embolisation of the kidney in 13 out of 19 rabbits, whether or not the other kidney was removed, caused a transient rise in blood pressure. In certain rabbits (e.g., no. 10, 17 and 37) this was more persistent. Previous studies of the effect of ex- perimental renal infarction on arterial pressure have yielded divergent results. Maegraith and Maclean (1942) injected kieselguhr into one renal artery and obtained a sustained rise of pressure in 19 out of 23 rabbits; the affected kidneys were scarred and kieselguhr was found in afferent arterioles and glomerular capillaries. This hypertension could be abolished by sectioning the renal nerves, and it was postulated that the hypertension was caused by localised partial ischemia due to constriction of the kidney vessels. Total infarction of the kidney, which sometimes occurred, waa not attended by a rise in blood pressure. In other investigations embolisation of the kidney did not lead to a rise in blood pressure. Scarff and McGeorge (1937) injected laked red blood cells into one renal artery of the rabbit and produced embolic glomerular lesions, but no rise in pressure was obtained. Cash (1924) injected berlin blue into the dog’s renal circulation, but obtained no rise in spite of the production of small infarcts. Apfelbach and Jensen (1931) failed to cause high blood pressure after injection of particles of charcoal into the renal artery of the dog in sufficient amounts to impair the concentrating and diluting functions and cause nitrogen retention. In the experiments just quoted the size of the emboli was smaller than in the present experiment; this accords with our own limited experience with smaller particles (pollen grains-20 p , lycopodium spores40 p , and magnetic iron oxide particles-30 p) where only one out of five animals, all of which had the opposite kidney removed, showed any appreciable rise in pressure.
The possible causes of the rise in pressure found in our animals are a reflex from the kidney, a decrease in renal mass, the absorption of a product of autolysis or the release of a pressor substance from living tissue in the margin of the infarct. The evidence that a rise in arterial pressure can result from a renal reflex is tenuous and has been reviewed by Braun-Menendez et a2. (1943). Only one of our animals (no. 40) had the renal pedicle stripped and it showed no rise in pressure. Chanu- tin and Ferris (1932) found an elevation of blood pressure in the rat when kidney tissue waa reduced to an amount just sufficient to maintain life. In the dog, Mason et al. (1940) were unable to cause an elevation of pressure by removal of one kidney and partial removal of the other. Anderson (1926) removed two-thirds of the kidney substance and failed to obtain a rise in pressure in the rabbit. Even on the assumption that simple removal of kidney substance can produce hypertension,

INTRARENAL EMBOLISM 236
the amount to be removed is considerable. It is unlikely that a simple reduction in parenchymal mass is the cause of the rise in the present experiment, for a rise in pressure occurred in 4 rabbits in which the right kidney was still present.
The effect of complete infarction on blood pressure has been studied extensively. In the dog, Janeway (1909) caused a rise in pressure by ligating branches of the renal artery and Cash (1924) obtained a rise which was sustained for only 8 weeks by combining decrease of renal tissue with ligation of renal arteries. He considered that before a rise in pressure could occur the total kidney substance must be reduced by 50 per cent. and that in addition a portion of kidney which had been deprived of its circulation must remain in situ. In a later paper (Cash, 1925-26) he showed that bilateral ligation of renal arteries caused a rise in blood pressure, but that bilateral ligation of renal artery, vein and ureter caused no such rise. He maintained that renal tissue under- going destruction within the body contains a substance which causes an elevation of both systolic and diastolic pressures if allowed to escape into the blood stream. Loomis (1946) working with the rat, came to similar conclusions. By tying off branches of renal arteries she showed that partial infarction of one kidney waa followed more promptly by hypertension than was total infarction of one kidney. Total infarction of one kidney in fact did not produce hypertension in 50 per cent. of the animals tested. The conclusion drawn was that revascularisation of the infarct causes a pressor substance from the infarct ‘to be absorbed into the circulation, and the paucity of anastomoses explains why there is no rise in pressure in the case of the completely infarcted kidney. In the rabbit Pickering and Prinzmetal (1937-38) found that no rise in blood pressure was obtained when one renal artery was completely ligated, the other kidney not being disturbed. When one kidney was removed and a very tight silver clip applied to the opposite renal artery, the blood pressure rose by 10-30 mm. Hg within 6 hr of operation and remained elevated until late on the second day when it fell to normal and the animals died. Such kidneys at necropsy showed areas of complete infarction with intervening areas of intact renal cells. Prinz- metal et al. (1940) were unable to demonstrate a rise in blood pressure in the rabbit after release of a clamp which had been on the renal pedicle (artery, vein and ureter) for periods of 3-7 hr, the other kidney having been removed. This was in contrast to the significant rise in pressure in the cat, dog and rat (Lewis et al., 1941).
The mechanism for producing infarction in the present experiment is somewhat diflerent from that in the above-mentioned papers and the kidneys contain numerous small distinct areas of infarction. If the rise in pressure is caused by necrotic tissue, we have an ideal situation for absorption of any pressor substance liberated by the necrotic areas in the form of abundant intervening normal tissue. Although circulation through the central dead area has ceased, liberated pressor substance might find its way into the circulation, just as
236 ALEXANDER, HEPTINSTALL A N D PICKERING
haemoglobin is transferred from lysed red blood cells in the central dead area to the periphery of the infarct.
A further cause is available in the presence, a t the periphery of the infarcts, of parenchyma with impairment of blood supply not sufficient to cause complete necrosis. This is the state of the renal parenchyma in the classical method for producing hypertension by reducing the blood supply to the kidney (Goldblatt et al., 1934; Pickering and Prinzmetal, 1937-38; Wilson and Byrom, 1941) (fig. 14). Such areas are abundant in kidneys like those of the present experiment and are much greater than in a kidney infarcted by complete occlusion of the renal artery. The paucity of such ischemic non-necrotic or only patchily necrotic tissue in the totally infarcted kidney would readily explain the inability of Loomis (1946) to obtain hypertension in the case of the totally infarcted kidney. The readjustment of the circulation in the kidney during the weeks following the infarction, so that the areas of relative ischemia become well supplied with blood, could explain the fall in pressure. There is no ready explanation for the persistence of high blood pressure in some of the animals, but it is conceivable that in some there is a permanent relative ischaemia of certain areas of the kidney. We have no histological evidence to substantiate this, for these kidneys appear to differ in no way from those in which the hypertension subsided. It is also worthy of note that in general there was no correlation between the appearances of the kidney, such as size and number of infarcts, and the level of the blood pressure. In three rabbits which showed no rise in blood pressure (no. 44, 16 and 22) the number and size of infarcts was of the same order as in those with a rise in pressure. The other three that failed to develop any rise did show some differences: no. 41 and 42 had almost completely infarcted kidneys with very little in the way of marginal areas; no. 40 had a renal denervation.
SUMMARY Areas of infarction in the left kidney were produced in a group of
rabbits by injection of a variety of particulate substances into the renal artery: lobelia seeds, brine shrimp eggs, polystyrene spheres and fibrin clots. Blood pressure estimations and blood urea determinations were made on these rabbits, some of which had the opposite kidney removed. Animals were killed at time intervals of 1 hour to 150 days and the kidneys studied grossly and histologically.
A temporary elevation of blood pressure was found in most of the rabbits whether the opposite kidney was removed or not. There wa8 no correlation between the size and number of infarcts and elevation of blood pressure except when almost complete infarction of the kidney was produced, in which case there was no rise in pressure.
The cause of the elevated pressure may be the presence of necrotic material, but it is equally likely that the cause may be the partially ischa?mic tissue at the edges of the infarcts.
INTRARENAL EMBOLISM 237
We would like to thank Professor G. E. Blackman for his advice on emboli, Dr G. S. Dawes for the use of his animal house, Mr W. S. Cook for assistance with the experiments, and Mr Michael Jacobs for the preparation of sections and photomicrographs.
REFERENCES ANDERSON, H. . . . . . . 1926. Arch. Int. Med., 37, 297. APFELBACH, c. w., AND JENSEN, 1931. J . c&. Invest., 10, 162.
C. R.
J. C., LELOIR. L. F., MuRoz, J. M., AND TAQUINI, A. C.
BRAWN-MENENDEZ, E., FASCIOLO, 1943. Hipertensi6n, arterial nefrogena, Buenos Aires, p. 77.
CASH, J. R. . . . . . . . 1924. Johns Hopkina Hoap. Bull., 35,
,, . . . . . . . 1925-26. Proc. SOC. Exp. Biol. Med., 23, 168.
609. CHILNUTIN, A., AND FERRIS, E. B.,
GOLDBLATT, H., LYNCH, J., 1934. J . Exp. Med., 59, 347.
1932. Arch. Int. Med., 49, 767. JR.
HANZAL, R. F., AND SWNMER-
GRANT, R. T., AND ROTHSCHILD, P. H~PTINSTALL, R. H., MICEUELS, 1960. This Journal, 80, 249.
JANEWAY, T. C. . . . . . 1909. Proc. SOC. Exp. B i d . Med., 6 , 109. LEWIS, H. A., LEO, S. D., AND 1941. A ~ w . Heart J . , 21, 319.
LOOMIS, DOROTHY . . . . . 1946. Arch. Path., 41. 231.
VILLE, w. w. 1934. J . Physiol., 81, 265.
L., AND BRUMFITT, W.
PRINZMETAL. M.
MAEGRAITH, B. G., AND MACLEAN, 1942. Brit. J . Exp. Path., 23,239. F. J.
MASON, M. F., ROBINSON, C. S.,
PICKERING, G. W., AND PRINZ- 1937-38. Clin. Sci., 3, 357.
PRINZMETAL, M., LEWIS, H. A., 1940. Amer. Heart J.,ZO, 525.
1940. J . Exp. Med., 72, 289. AND BLALOCK, A.
m T & , M.
TAGGART, J.. WILKINS, H., AND DRURY, D. R.
SCARFF, R. W.. AND MCGEORGE, M.
SHEEHAN, H. L., AND DAVIS, J. C.
WILSON, C., AND BYROM, F. B. . 1941. Quart. J . Med., n.s. 10, 66.
1937.
1958.
Brit. J . Exp. Path., 18, 59.
This Journal, 76, 669. 1, ,, .. ,, 1959. This J o u d , 77, 33.