Embed Size (px)
Citation preview
The Henderson Repository is a free resource of the HonorSociety of Nursing, Sigma Theta Tau International. It isdedicated to the dissemination of nursing research, research-related, and evidence-based nursing materials. Take credit for allyour work, not just books and journal articles. To learn more,visit www.nursingrepository.org
Item type Presentation
Format Text-based Document
Title Keeping the Child with Food Allergies Safe at School
Authors Spain, Scarlet R.
Downloaded 10-Jul-2018 07:40:03
Link to item http://hdl.handle.net/10755/603042

THE EFFECTS OF AN EVIDENCE-
BASED FOOD ALLERGY
MANAGEMENT PLAN TO KEEP
CHILDREN WITH FOOD
ALLERGIES SAFE AT SCHOOL
Scarlet R. Spain DNP, CNS, FNP-BC
No Disclosures
Objectives
• Identify key factors to
keeping children with
allergies safe
• Understand
recommendations for
school implementation
Background- Prevalence in children has
increased 18% from 1997 to 2007
- 30,000 visits to the emergency room each year related to food allergies
- More than 200 deaths will occur in the US this year from food allergies
PREVALENCE IN CHILDREN HAS INCREASED 18% FROM 1997 (ALLERGY AND ASTHMA FOUNDATION OF AMERICA, 2014)
- One in 13 kids has a food allergy
- Average classroom has 2 kids with food allergies
- 5.9 million kids with food allergies
(Food Allergy Research and Education, 2014)
School Issues
• 84% of children who have food allergies will experience an allergic reaction while at school
• Reactions are unpredictable in nature and severity– A child who experienced a mild
reaction from a food trigger may quickly experience anaphylaxis with secondary exposure (Powers, Bergren, & Finnegan, 2007)
• Literature shows often the child is not prepared with emergency care plan (ECP) or required medications
Evidence-Based
Practice Project
• Project developed for local charter school
– School in Northwest, IN
– 500 students, K to 8th grade
– 18 children with food allergies Spring 2014; 22 children with food allergies enrolled Fall 2014
PICOT
“In the elementary school setting,
how does implementation of a
revised food allergies management
policy affect staff adherence to best
practice recommendations and
students’ episodes of food allergy
reactions over a 4 month period?”
Literature Review
- Conducted to gather evidence
- Sought to identify safety measures related to food
allergy management in school
- Multiple types of evidence was found

Review of
Literature
Key terms used- Food allergy- Food hypersensitivity- Peanut allergy- Education- School- Class- Teacher- School nurse- School health nursing
Inclusion criteria- Less than 10 years old- English language- Peer reviewed
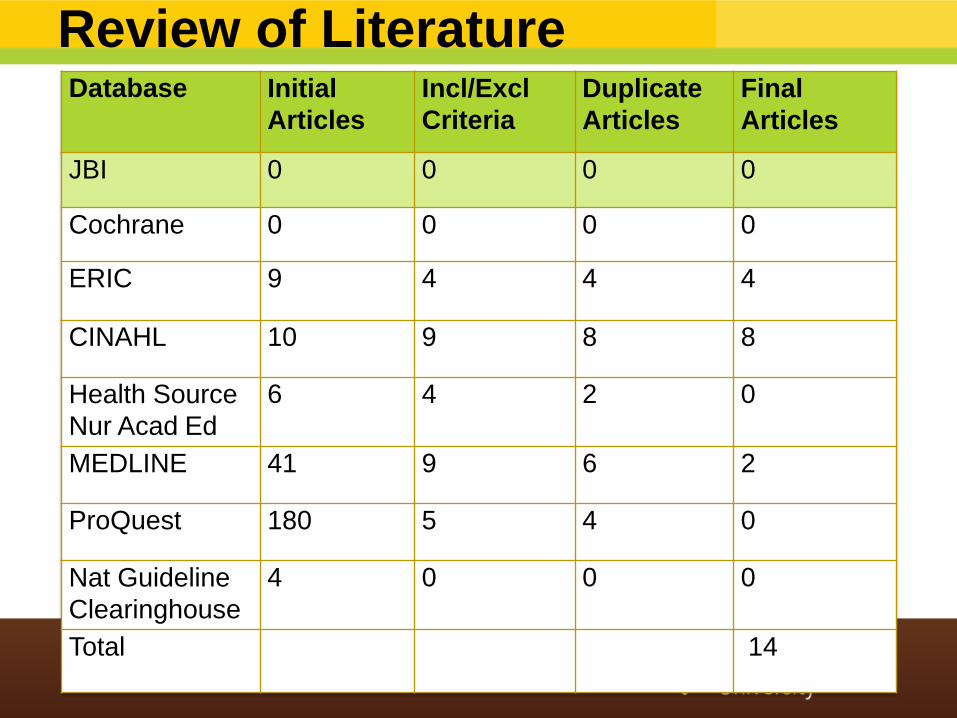
Review of LiteratureDatabase Initial
Articles
Incl/Excl
Criteria
Duplicate
Articles
Final
Articles
JBI 0 0 0 0
Cochrane 0 0 0 0
ERIC 9 4 4 4
CINAHL 10 9 8 8
Health Source
Nur Acad Ed
6 4 2 0
MEDLINE 41 9 6 2
ProQuest 180 5 4 0
Nat Guideline
Clearinghouse
4 0 0 0
Total 14
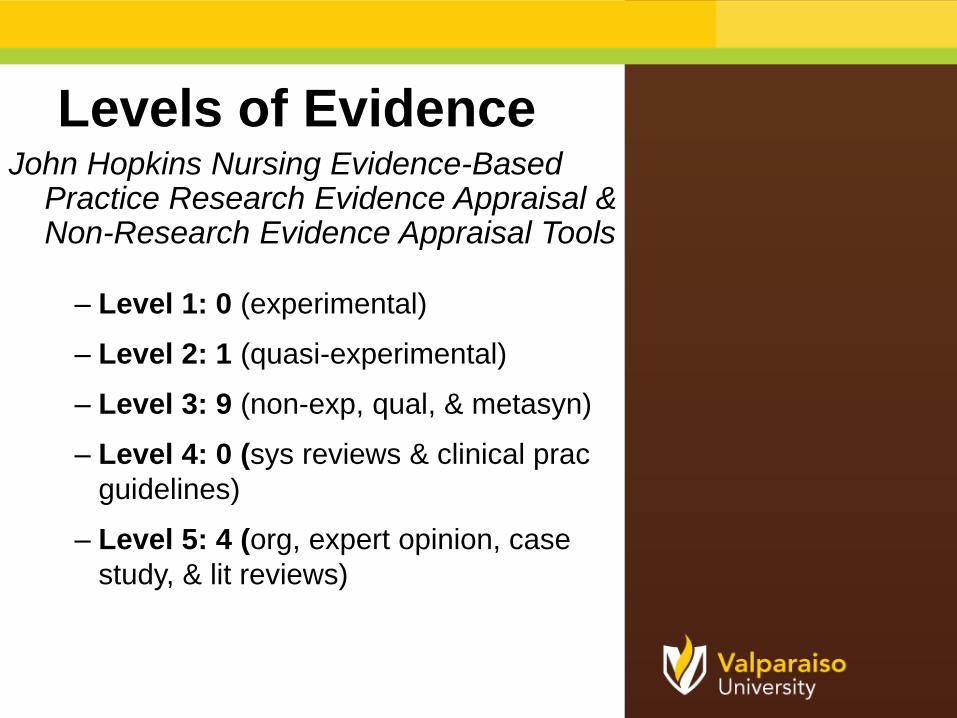
Levels of EvidenceJohn Hopkins Nursing Evidence-Based
Practice Research Evidence Appraisal & Non-Research Evidence Appraisal Tools
– Level 1: 0 (experimental)
– Level 2: 1 (quasi-experimental)
– Level 3: 9 (non-exp, qual, & metasyn)
– Level 4: 0 (sys reviews & clinical prac
guidelines)
– Level 5: 4 (org, expert opinion, case
study, & lit reviews)
Decision to Change Practice
• Best practice for management of food allergies in the
school setting remains complete avoidance of trigger
foods for the affected child (Carlisle et al., 2010; Cavanaugh &
Strickland, 2011; Gupta, 2014; Weiss et al., 2014).
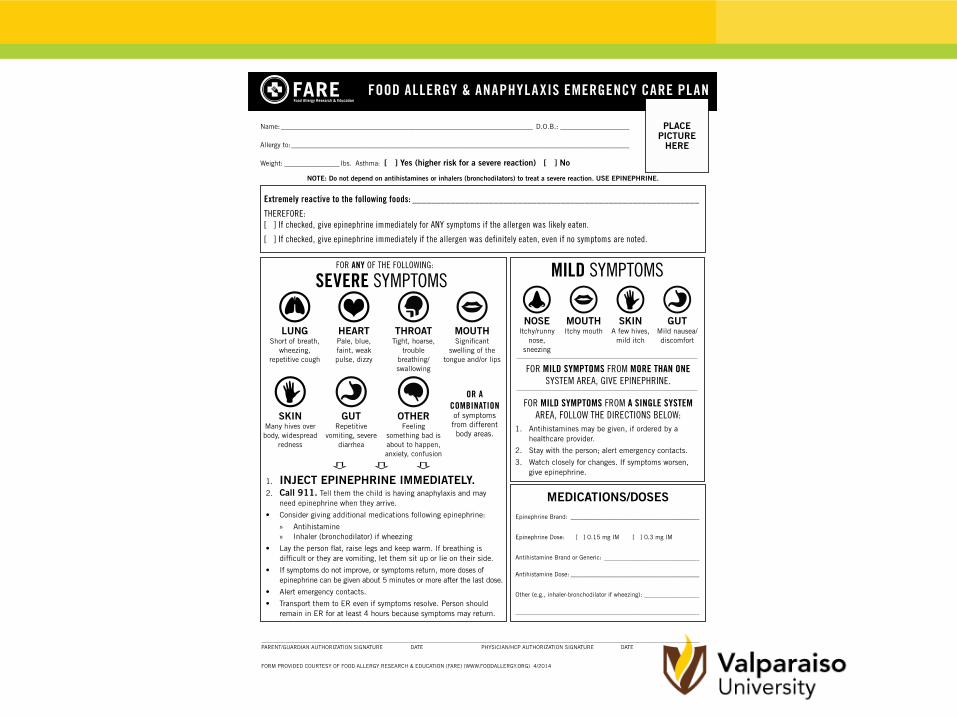
• Food allergies and anaphylaxis demonstrate a wide
variability in symptoms and triggers. Each student
should have their own emergency care plan available
at all times with required medications (Carlisle et al., 2010;
Cavanaugh & Strickland, 2011).
• Evidence supports staff education regarding food
allergies in school systems (Weiss et al., 2004; Young et al., 2004).
ImplementationSetting and Sample:
–Local charter school
–Children with food allergies in grades K to 8
Theoretical Frameworks:
–Adult Learning Theory & ACE Star Model
Intervention:
–Policy development with educational in-service
Outcomes :
–Primary - Food allergy reactions
–Secondary - Policy compliance
Best Practice Project
Policy Development
– Avoidance
– ECP/ Medication
– Staff Education
Educational In-
Services
• 4 educational in-services were held that educated staff and volunteers. (n=115)– PowerPoint Presentation
– Demo and Return Demo by all participants of two common epinephrine auto-injectors
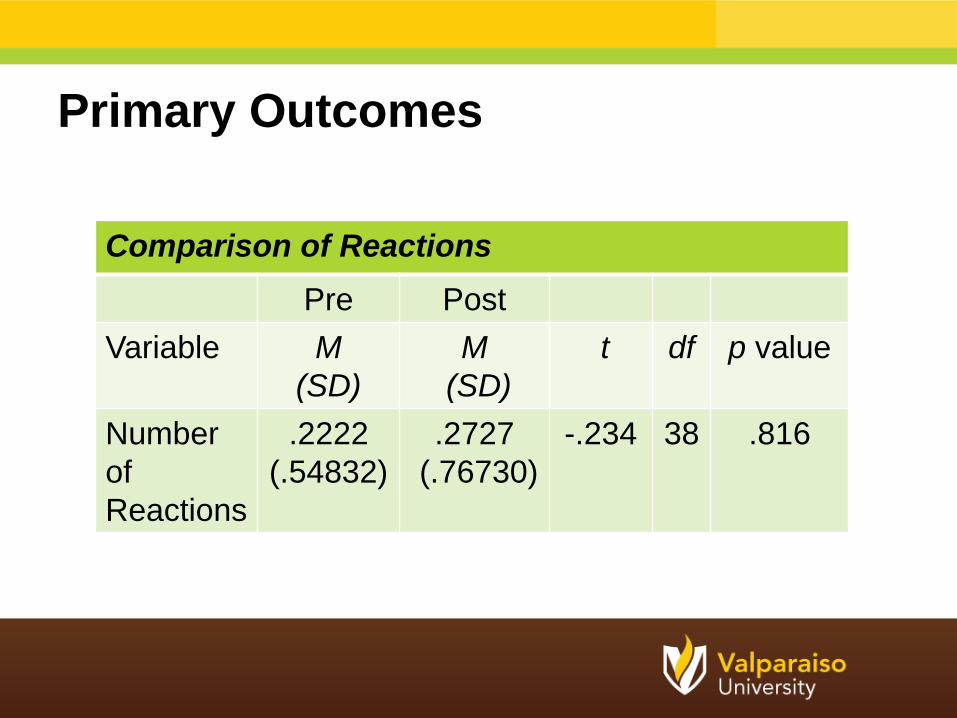
Primary Outcomes
Comparison of Reactions
Pre Post
Variable M
(SD)
M
(SD)
t df p value
Number
of
Reactions
.2222
(.54832)
.2727
(.76730)
-.234 38 .816
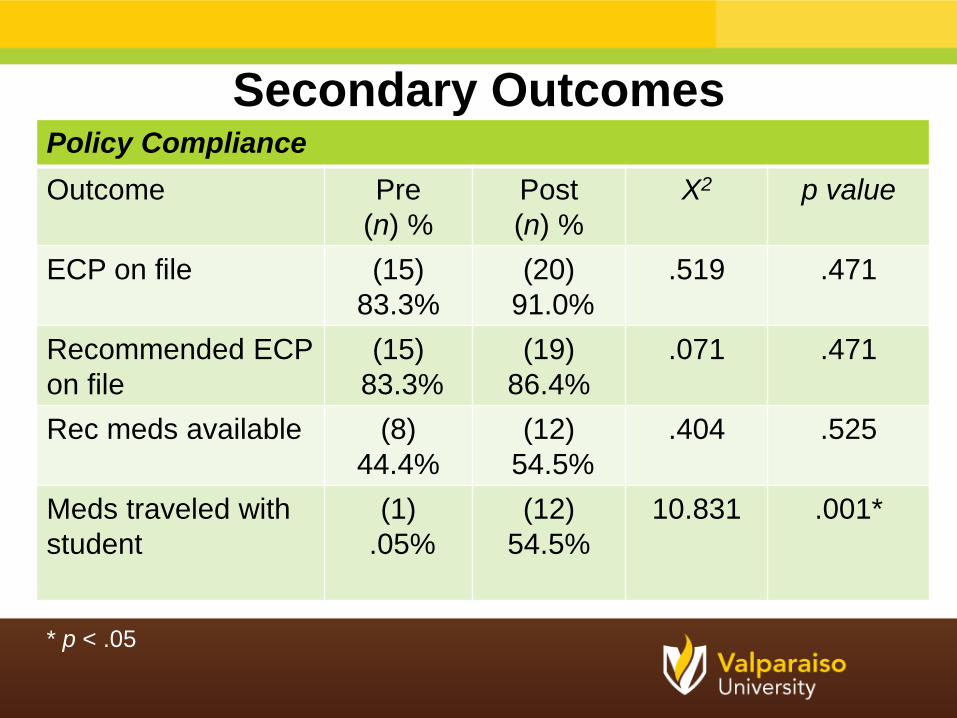
Policy Compliance
Outcome Pre
(n) %
Post
(n) %
X2 p value
ECP on file (15)
83.3%
(20)
91.0%
.519 .471
Recommended ECP
on file
(15)
83.3%
(19)
86.4%
.071 .471
Rec meds available (8)
44.4%
(12)
54.5%
.404 .525
Meds traveled with
student
(1)
.05%
(12)
54.5%
10.831 .001*
Secondary Outcomes
* p < .05
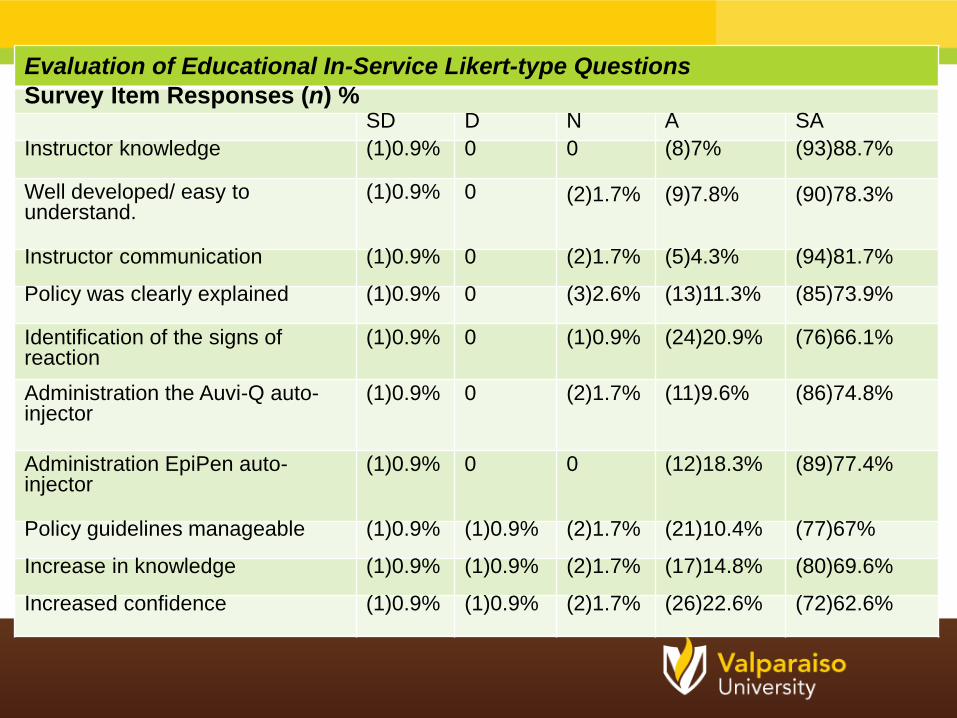
Evaluation of Educational In-Service Likert-type Questions
Survey Item Responses (n) %SD D N A SA
Instructor knowledge (1)0.9% 0 0 (8)7% (93)88.7%
Well developed/ easy to understand.
(1)0.9% 0 (2)1.7% (9)7.8% (90)78.3%
Instructor communication (1)0.9% 0 (2)1.7% (5)4.3% (94)81.7%
Policy was clearly explained (1)0.9% 0 (3)2.6% (13)11.3% (85)73.9%
Identification of the signs of reaction
(1)0.9% 0 (1)0.9% (24)20.9% (76)66.1%
Administration the Auvi-Q auto-injector
(1)0.9% 0 (2)1.7% (11)9.6% (86)74.8%
Administration EpiPen auto-injector
(1)0.9% 0 0 (12)18.3% (89)77.4%
Policy guidelines manageable (1)0.9% (1)0.9% (2)1.7% (21)10.4% (77)67%
Increase in knowledge (1)0.9% (1)0.9% (2)1.7% (17)14.8% (80)69.6%
Increased confidence (1)0.9% (1)0.9% (2)1.7% (26)22.6% (72)62.6%
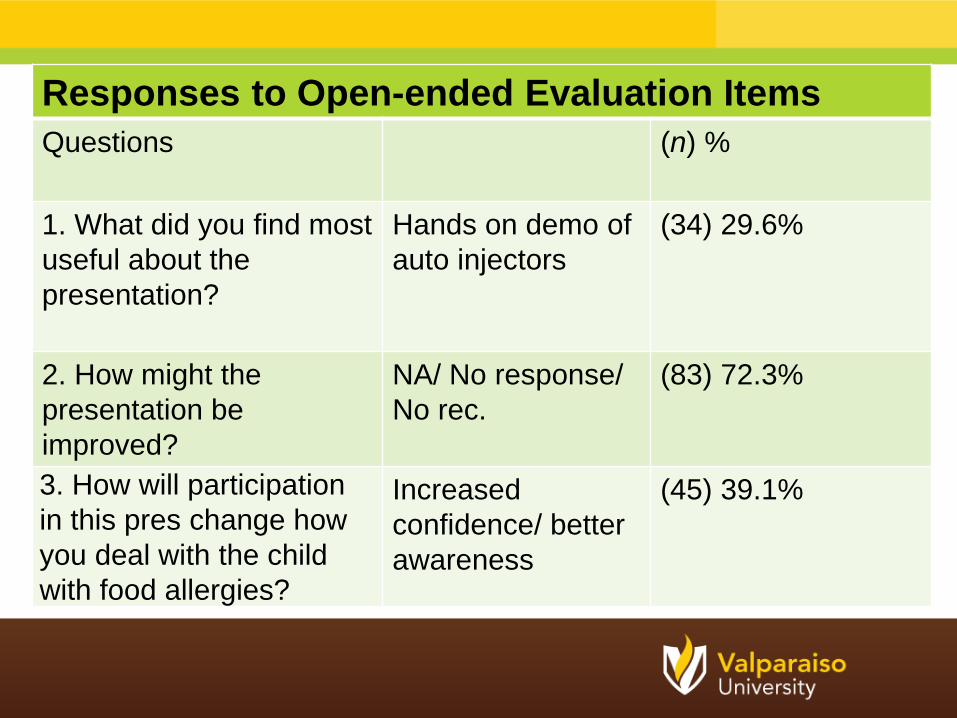
Responses to Open-ended Evaluation Items
Questions (n) %
1. What did you find most
useful about the
presentation?
Hands on demo of
auto injectors
(34) 29.6%
2. How might the
presentation be
improved?
NA/ No response/
No rec.
(83) 72.3%
3. How will participation
in this pres change how
you deal with the child
with food allergies?
Increased
confidence/ better
awareness
(45) 39.1%
Conclusions
•No significant difference in incidence of
food allergy reactions after policy
implementation
•Adherence to recommended practice
increased after policy implementation
with one parameter, medications
traveled with student, reflecting a
significant difference
•Implementation of policy based on best
practice provides a safer environment for
the child with food allergies
Strengths/ Limitations
• Strengths
- High participation rate
- Use of best practice
recommendations and evidence
• Limitations
– Small sample size
– Short timeframe
Recommendations
•Continue policy monitoring to
assess outcome changes over
longer time period
•Expand policy to include other
schools in system
•Update policy recommendations
with new evidence to reflect most
current guidelines
Acknowledgments
• Valparaiso University
• Sigma Theta Tau
International- Zeta Epsilon
Chapter
*Special Dedication to Lilly Spain*

Questions & Answers…

ReferencesAbbott, C., Dremsa, T., Stewart, D., Mark, D., & Swift, C. (2006). Adoption of a Ventilator-
associated pneumonia clinical practice guideline. Worldviews on Evidence-Based Nursing, 3, 139-152.
Academic Center for Evidence Based Practice (ACE). (2012). University of Texas Health
Science Center. Retrieved from www.acestar.uthscsa.edu
Bonis, S., Taft, L., & Wedler, C. (2007). Strategies to promote success on the NCLEX-RN: An evidence-based approach using the ACE star model of knowledge transformation. Nursing Education, 28, 82-87.
Centers for Disease Control and Prevention. (2013). Voluntary Guidelines for Managing Food Allergies in Schools and Early Care and Education Programs. Washington, DC: US Department of Health and Human Services.
Carlisle, S., Vargas, P., Noone,S., Steele, P., Sicherer, S., Burks, W., & Jones, S.(2010). Food allergy education for school nurses: A needs assessment survey by the consortium of food allergy research. The Journal of School Nursing, 26 (5). 360-367.
Cavanaugh, R. & Strickland, J. (2011). Research to practice: Developing an integratedanaphylaxis education curriculum for school nurses. The Journal of School Nursing, 27 (3), 197- 208.
Fineout-Overholt, E., Stillwell, S., Williamson, K., Cox, J., & Robbins, B. (2011). Teaching evidence-based practice in academic settings. In Melnyk, B. M., & Fineout-Overholt, Evidence-based practice in nursing and healthcare.(2nd ed.), (pp. 291-329). Philadelphia, PA: Lippincott Williams & Wilkins
Food Allergy and Anaphylaxis Network. (2010). School food allergy program. Retrieved from http://www.foodallergy.org/school.html.
Food Allergy and Anaphylaxis Network. (2014). Resources for Kids. Retrieved from www.foodallergy.org/resources/kids
Food Allergy Research and Education (FARE). (2014). Emergency action plan. Retrieved from http://www.foodallergy.org/document.doc?id=234 .
Food Allergy Research and Education (FARE). (2014). Keeping children with food allergies safe at school. Retrieved from http://www.foodallergy.org/document.doc
Gupta, R. (2014). Anaphylaxis in the young adult population. The American Journal of Medicine,
127(1), S17-S24.
Houle, C., Leo, H., & Clark, N. (2010). A developmental, community, and psychosocial Approach
to food allergies in children. Current Allergy and Asthma Reports, 10, 381-386.
INFED. (2014). Malcolm Knowles, informal adult education, self-direction and
andragogy. Obtained from http://infed.org/mobi/malcolm-knowles-informal-adult-education-
self- direction-and-andragogy
International Food Information Council (IFIC). (2008). IFIC-SNA 2008 school food allergy survey:
Having a food allergy plan is key to prevention, p. 2-6.
Jackson, V. (2013). School nurse’s role in supporting food allergy safe schools. NASN School
Nurse, 28, 76-77.
John Hopkins Nursing Evidence Based Practice Tool. (n.d). Retrieved from
http://www.nursingworld.org/ research-toolkit/johns-hopkins-nursing-evidence-based-
practice
Knowles, Malcolm. (1973). The adult learner: A neglected species. Madison, WI: Gulf.
McIntyre, C., Sheetz, A., Carroll, C., & Young, M. (2005). Administration of epinephrine for life-
threatening allergic reactions in school settings. Pediatrics, 116 (5),1134-1140.
Munoz-Furlong, A. (2004). Food allergy in schools: Concerns for allergists, pediatricians, parents,
and school staff. The Food Allergy & Anaphylaxis Network, 93, S47-S50.
Neilson, W. & Lindsey, K. (2010). When there is no school nurse- Are teachers prepared for
students with peanut allergies?, School Nurse News, 27 (1), 12-5.
Papageorgiou, P. (2002). Plant food allergens: Clinical aspects of food allergy. Biochemical
Society Transactions, 30 (6), 901-906.
Powers, J., Bergren, M., & Finnegan, L. (2007). Comparison of school food allergy
emergency plans to the food allergy and anaphylaxis network’s standard plan. The
Journal of School Nursing, 23, 252-257.
.
Pulcini J., Marshall, G., & Naveed, A. (2011). Presence of food allergy emergency action plans in Mississippi. Annals of Allergy, Asthma and Immunology, 107, p. 127-132
Pulcini, J., Sease, K., & Marshall, G. (2010). Disparity between the presence and absence of food allergy action plans in one school district. Allergy and Asthma Proceeding, 31,141-146.
Shah, S., Parker, C., & Davis, C. (2013). Improvement of teacher food allergy knowledge in socioeconomically diverse schools after educational intervention. Clinical Pediatrics 52(9), 812-820.
Sicherer, S., Noone, S., & Munoz-Furlong, A. (2004). The impact of childhood food allergy on quality of life. Annuals of Allergy, Asthma and Immunology, 87, 461-464.
Twycross, A. (2002). Education nurses about pain management: The way forward, Journal ofClinical Nursing, 11, 705-714.
Wahl, A., Stephens, H., Ruffo, M., & Jones, A. (2014). The evaluation of a food allergy and epinephrine auto injector training program for personnel who care for children in schools and community settings. Journal of School Nursing, Obtained from
http://www.ncbi.nlm.nih.gov/pubmed
Weiss, C., Munoz-Furlong, A., Furlong, T., & Arbit, J. (2004). Impact of food allergies on school nursing practice. The Journal of School Nursing, 20 (5), 268-278.
Young, M. Munoz-Furlong, A, & Sicherer, S. (2009). Management of food allergies in schools: A perspective for allergists. American Academy of Allergy, Asthma & Immunology, 124, 175-182.






























