Embed Size (px)
Citation preview

The Effects of Aerobic Exercise on Activities of Daily Living
Post Stroke
The Effects of Aerobic Exercise on Activities of Daily Living
Post Stroke
Presented by:Leah Boeckermann-BelangerJessica DulongKendra GilbertJeanine McColl Allison WhyteMeredith Wilson

OutlineOutline Introduction Methods Results Discussion
Participants Interventions Control Outcome
Introduction Methods Results Discussion
Participants Interventions Control Outcome
Conclusion Clinical Implications
Conclusion Clinical Implications

BackgroundBackground
Stroke, a blockage or bleed
in the brain, represents one
of the leading causes
of morbidity in Canada1
Resultant signs & symptoms can have a negative impact on one’s ability to live their daily life1
Stroke places a large economic burden ($2.8 billion) on the Canadian Health Care System1
Stroke, a blockage or bleed
in the brain, represents one
of the leading causes
of morbidity in Canada1
Resultant signs & symptoms can have a negative impact on one’s ability to live their daily life1
Stroke places a large economic burden ($2.8 billion) on the Canadian Health Care System1

Background: Aerobic ConditioningBackground: Aerobic Conditioning
Moderate intensity aerobic exercise has been shown to risk of stroke in a dose response manner2
Post stroke, individuals exhibit an extensive in aerobic conditioning, resulting from the event & subsequent in physical activity3,4
aerobic fitness combined with energy demands greatly affects ability to perform ADLs5,6
Moderate intensity aerobic exercise has been shown to risk of stroke in a dose response manner2
Post stroke, individuals exhibit an extensive in aerobic conditioning, resulting from the event & subsequent in physical activity3,4
aerobic fitness combined with energy demands greatly affects ability to perform ADLs5,6

Background: VO2Background: VO2
Treadmill training energy expenditure & CV demands of gait in individuals with stroke6,7
VO2max of at least 15ml/kg/min for women & 18 ml/kg/min for men is required for independent living8
Individuals with stroke who participated in an aerobic program had an average in VO2max of 13% compared to control3
aerobic fitness has been associated with functional gains including mobility, falls, & ability to carry out ADLs9
Treadmill training energy expenditure & CV demands of gait in individuals with stroke6,7
VO2max of at least 15ml/kg/min for women & 18 ml/kg/min for men is required for independent living8
Individuals with stroke who participated in an aerobic program had an average in VO2max of 13% compared to control3
aerobic fitness has been associated with functional gains including mobility, falls, & ability to carry out ADLs9

Background: Neuroprotective Effect
and Neuroplasticity
Background: Neuroprotective Effect
and Neuroplasticity Aerobic exercise has a neuroprotective effect on
the brain Brain derived neurotrophic factor appears to be
most sensitive to regulation via exercise It may be of importance in mediating the benefits
of exercise on neural plasticity & the benefits of exercise on CNS health
Important post stroke as neuroplasticity is required in order for neural reorganization & regeneration to occur, resulting in function of the individual10
Aerobic exercise has a neuroprotective effect on the brain
Brain derived neurotrophic factor appears to be most sensitive to regulation via exercise
It may be of importance in mediating the benefits of exercise on neural plasticity & the benefits of exercise on CNS health
Important post stroke as neuroplasticity is required in order for neural reorganization & regeneration to occur, resulting in function of the individual10

Why is it relevant to Physical Therapists?
Why is it relevant to Physical Therapists?
To assist in making clinical decisions regarding effectiveness of aerobic training in individuals post stroke, thus ensuring that limited therapy resources are being used effectively
To determine the type, duration & intensity of aerobic activity that is most beneficial for those affected by stroke
To assist in making clinical decisions regarding effectiveness of aerobic training in individuals post stroke, thus ensuring that limited therapy resources are being used effectively
To determine the type, duration & intensity of aerobic activity that is most beneficial for those affected by stroke

Research QuestionResearch Question
What is the effect of aerobic exercise training on the ADLs in individuals with stroke?
What is the effect of aerobic exercise training on the ADLs in individuals with stroke?

MethodsMethods
Inclusion criteria: English RCTs Individuals with stroke who are medically
stable & capable of performing aerobic exercise Aerobic intervention, min 3x/wk, at least 4
wks3
Reliable & valid outcome measure (OM)12-24
Inclusion criteria: English RCTs Individuals with stroke who are medically
stable & capable of performing aerobic exercise Aerobic intervention, min 3x/wk, at least 4
wks3
Reliable & valid outcome measure (OM)12-24

MethodsMethods
Exclusion Criteria: Participants involved in aerobic activity prior to
study onset Combination of training (e.g. aerobic + strength
training)
Exclusion Criteria: Participants involved in aerobic activity prior to
study onset Combination of training (e.g. aerobic + strength
training)

Methods: Search StrategyMethods: Search Strategy
Sept 2008 - Jan 2009 CINAHL, EMBASE, MEDLINE, Unindexed
MEDLINE, SportDiscus Titles, abstracts, full text, & hand-searching
screened by 2 independent reviewers Discrepancies resolved by discussion or 3rd
reviewer
Sept 2008 - Jan 2009 CINAHL, EMBASE, MEDLINE, Unindexed
MEDLINE, SportDiscus Titles, abstracts, full text, & hand-searching
screened by 2 independent reviewers Discrepancies resolved by discussion or 3rd
reviewer

Methods: Quality Assessment & Data Abstraction
Methods: Quality Assessment & Data Abstraction
PEDro Methodological Quality Assessment Scale
Data Abstraction form 2 independent reviewers Discrepancies resolved by discussion or 3rd
reviewer
PEDro Methodological Quality Assessment Scale
Data Abstraction form 2 independent reviewers Discrepancies resolved by discussion or 3rd
reviewer

Data AnalysisData Analysis
Due to heterogeneous results qualitative analysis was performed
Due to heterogeneous results qualitative analysis was performed

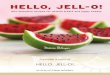
Selected StudiesSelected Studies
Excluded after title screen880
Excluded after de-duplication46
Excluded after abstract screen103
Excluded after full text screen36
Handsearching occurred3
Included after MS study removed6
Included after handsearching7
Included after full text screen4
Included after abstract screen40
Included after de-duplication143
Included after title screen189
Initial Search1069

Reasons for ExclusionReasons for Exclusion
Multi-modality interventions Lack of control group Lack of aerobic intervention Insufficient training frequency & duration Language other than English Absence of a reliable & valid OM
Multi-modality interventions Lack of control group Lack of aerobic intervention Insufficient training frequency & duration Language other than English Absence of a reliable & valid OM

Results: Study DetailsResults: Study Details
1 cycle ergometer, 3 treadmill, 1 gait trainer OM: Frenchay Activity Index (FAI),
Nottingham, Stroke Impact Scale Domain 5 (SIS-5), Rivermead Mobility Index (RMI), Functional Independence Measure (FIM), Barthel Index (BI)
Quality assessment scores: 5-9/ 11
1 cycle ergometer, 3 treadmill, 1 gait trainer OM: Frenchay Activity Index (FAI),
Nottingham, Stroke Impact Scale Domain 5 (SIS-5), Rivermead Mobility Index (RMI), Functional Independence Measure (FIM), Barthel Index (BI)
Quality assessment scores: 5-9/ 11

Results: Demographic InfoResults: Demographic Info
First AuthorParticipant mean
ageInitial # of
participants I:CFinal # of
participants I:CCondition or Type of
StrokeTime post-
strokeKatz-Leurer 63 +/- 11 46 : 46 46 : 44 Hemorrhage,
InfarctionNot specified
Liston 79.1 +/- 6.8 10 : 8 (Treadmill 1st: Conventional PT 1st)
8 : 8 (Treadmill 1st: Conventional PT 1st)
Leukoaraiosis, Infarct, Low Density Area, Leukoaraiosis, Infarct
Not specified
Macko 63 +/- 10
32 : 29 25 : 20 Ischemic > 6 months
Pohl 62.3 +/- 12 (range: 26 - 79)
77 : 78 72 : 72 (After 4 weeks)
Ischemic, Hemorrhagic
< 60 days
Smith 57.8 (range: 42-72)
10 : 10 10 : 10 Ischemic > 3 months, < 2 years

Katz-Leurer et al (2003)25-26
Katz-Leurer et al (2003)25-26
Leg cycle ergometer training Part 1: 5 days/wk for 2 wks, up
to 20 min continuous Part 2: 6 wks: 30min, 3x/wk Intensity: 60% HRR
Control: regular therapy 5 days/ wk OM: FAI, FIM
Leg cycle ergometer training Part 1: 5 days/wk for 2 wks, up
to 20 min continuous Part 2: 6 wks: 30min, 3x/wk Intensity: 60% HRR
Control: regular therapy 5 days/ wk OM: FAI, FIM

Katz-Leurer et al (2003)25,26 cont.Katz-Leurer et al (2003)25,26 cont.
FAI scores pre stroke & at 6 months follow-up Total score 10 pts in both control & intervention
groups Those with more severe stroke showed greater
improvements Trend towards improvement in all parameters of
functional ability in experimental group, but FIM showed no statistical difference
FAI scores pre stroke & at 6 months follow-up Total score 10 pts in both control & intervention
groups Those with more severe stroke showed greater
improvements Trend towards improvement in all parameters of
functional ability in experimental group, but FIM showed no statistical difference

Liston et al (2000)27Liston et al (2000)27
Treadmill: walking as long as comfortable,
rest breaks as needed, up to 60min, 3x/wk, 6 wks
Self selected intensity Control: conventional PT OM: Nottingham No significant differences b/n the groups
Treadmill: walking as long as comfortable,
rest breaks as needed, up to 60min, 3x/wk, 6 wks
Self selected intensity Control: conventional PT OM: Nottingham No significant differences b/n the groups

Macko et al (2005)28Macko et al (2005)28
Treadmill 40 min walking, 3x/wk, 6 months Started at 40-50% HRR for 10-20 min; 5% HRR
every 2 wks; 5 min every 2 wks (as tolerated) Control
40 min stretching & low-intensity treadmill walking 3x/wk for 6 months
OM: RMI No statistically significant difference b/n groups
Treadmill 40 min walking, 3x/wk, 6 months Started at 40-50% HRR for 10-20 min; 5% HRR
every 2 wks; 5 min every 2 wks (as tolerated) Control
40 min stretching & low-intensity treadmill walking 3x/wk for 6 months
OM: RMI No statistically significant difference b/n groups

Pohl et al (2007)29Pohl et al (2007)29
Gait trainer: Up to 20 min + 25 min
conventional PT, 5x/wk, 4 wks Progressed by body wt support
Control: 45 min conventional PT
OM: BI, RMI
Gait trainer: Up to 20 min + 25 min
conventional PT, 5x/wk, 4 wks Progressed by body wt support
Control: 45 min conventional PT
OM: BI, RMI

Pohl et al (2007)29 cont.Pohl et al (2007)29 cont.
BI: significant difference in favour of intervention group (chi-squared test p<0.0125)
RMI: intervention significantly better than control (p<0.0001)
BI: significant difference in favour of intervention group (chi-squared test p<0.0125)
RMI: intervention significantly better than control (p<0.0001)

Smith (2006)30Smith (2006)30
Treadmill: 12 sessions over 4 wks, 20 min walking with unlimited
rest breaks 0.2mph once achieved 10 min continuous at self
selected velocity; <13 on 20 point Borg scale
Control: QOL logs OM: SIS - Domain 5 Trend towards ADL function in experimental
group, not statistically significant
Treadmill: 12 sessions over 4 wks, 20 min walking with unlimited
rest breaks 0.2mph once achieved 10 min continuous at self
selected velocity; <13 on 20 point Borg scale
Control: QOL logs OM: SIS - Domain 5 Trend towards ADL function in experimental
group, not statistically significant

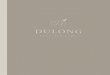
Results: % Change Over TimeResults: % Change Over Time
-5
15
35
55
75
95
115
135
155
175
Katz-Leurer - FIM Smith - SIS Liston - Nottingham Macko -RMI Pohl - BI Pohl - RMIStudy
% c
hang
e
Control %change (final-initial)
Experimental %change (final-initial)
Control %change atfollow up (frominitial)
Experimental %change atfollow up (frominitial)
Control %change atfollow up (fromfinal)
Experimental %change fromfollow up (fromfinal)
-5
15
35
55
75
95
115
135
155
175
Katz-Leurer - FIM Smith - SIS Liston - Nottingham Macko -RMI Pohl - BI Pohl - RMIStudy
% c
hang
e
Control %change (final-initial)
Experimental %change (final-initial)
Control %change atfollow up (frominitial)
Experimental %change atfollow up (frominitial)
Control %change atfollow up (fromfinal)
Experimental %change fromfollow up (fromfinal)

ResultsResults
Based on the 5 data sets in this systematic review, no patterns of improvement in ADLs were found
Based on the 5 data sets in this systematic review, no patterns of improvement in ADLs were found

Discussion: ParticipantsDiscussion: Participants
High variability among the participants, particularly stroke severity, likely contributed to lack of significance
The participants in the Pohl29 study had more severe functional deficits (non-ambulatory or required assistance) & it was the only study that had significant findings
Katz-Leurer25,26 found an interaction effect b/n event severity, FAI, & intervention in favour of those more severely affected
High variability among the participants, particularly stroke severity, likely contributed to lack of significance
The participants in the Pohl29 study had more severe functional deficits (non-ambulatory or required assistance) & it was the only study that had significant findings
Katz-Leurer25,26 found an interaction effect b/n event severity, FAI, & intervention in favour of those more severely affected

Discussion: Participants cont.Discussion: Participants cont.
More severely affected participants likely had lower VO2max due to deconditioning post stroke & thus had more to gain from an aerobic intervention3,4
Therefore, aerobic activity is likely important in ADL function in those with greater functional deficits
Additional research is needed
More severely affected participants likely had lower VO2max due to deconditioning post stroke & thus had more to gain from an aerobic intervention3,4
Therefore, aerobic activity is likely important in ADL function in those with greater functional deficits
Additional research is needed

Discussion: Participants cont.Discussion: Participants cont.
Participants also differed in type & location of stroke & time since stroke
Damage to different areas of the brain may result in altered abilities to recover31
Individuals entering rehab earlier post stroke have a larger window for recovery32
Pohl et al29 accepted individuals who were <60 days post stroke & this was the only study to show improvements in ADLs Spontaneous recovery
Participants also differed in type & location of stroke & time since stroke
Damage to different areas of the brain may result in altered abilities to recover31
Individuals entering rehab earlier post stroke have a larger window for recovery32
Pohl et al29 accepted individuals who were <60 days post stroke & this was the only study to show improvements in ADLs Spontaneous recovery

Discussion: Participants cont.Discussion: Participants cont.
Small sample sizes may have contributed to the lack of significant findings & thus larger sample sizes are required
Pohl et al29, with the largest sample size at 72 participants per group, was the only study to show significant results
Small sample sizes may have contributed to the lack of significant findings & thus larger sample sizes are required
Pohl et al29, with the largest sample size at 72 participants per group, was the only study to show significant results

Discussion: InterventionDiscussion: Intervention
Heterogeneity of exercise dose is the most prominent issue impacting outcomes
Duration: ACSM: 15-20 wk length intervention may be an
adequate min standard for healthy populations to assess effectiveness of various doses of aerobic exercise11
We suggest that the length of intervention should meet this criteria as this is the most evidence based guideline available
Heterogeneity of exercise dose is the most prominent issue impacting outcomes
Duration: ACSM: 15-20 wk length intervention may be an
adequate min standard for healthy populations to assess effectiveness of various doses of aerobic exercise11
We suggest that the length of intervention should meet this criteria as this is the most evidence based guideline available

Discussion: Intervention cont.Discussion: Intervention cont.
Macko et al28 had the longest study period, however had no significant findings This may be due to the use of the RMI, a dichotomous
scale relating specifically to mobility Because participants were ambulatory at study start,
they may have reached a ceiling effect Pohl et al29 used the same OM, but with initially
non-ambulatory participants Less likely to reach same ceiling effect
Macko et al28 had the longest study period, however had no significant findings This may be due to the use of the RMI, a dichotomous
scale relating specifically to mobility Because participants were ambulatory at study start,
they may have reached a ceiling effect Pohl et al29 used the same OM, but with initially
non-ambulatory participants Less likely to reach same ceiling effect

Discussion: Intervention cont.Discussion: Intervention cont.
Intensity: ACSM: to achieve cardiorespiratory benefits from
training, an intensity of 40/50-85% HRR is required in healthy individuals34
2 studies used HRR to measure intensity25,26,28, 1 used the Borg RPE29, & others did not report intensity27,30
Unable to determine if intensity was sufficient in all studies to produce a training effect according to the ACSM guidelines for healthy individuals
Intensity: ACSM: to achieve cardiorespiratory benefits from
training, an intensity of 40/50-85% HRR is required in healthy individuals34
2 studies used HRR to measure intensity25,26,28, 1 used the Borg RPE29, & others did not report intensity27,30
Unable to determine if intensity was sufficient in all studies to produce a training effect according to the ACSM guidelines for healthy individuals

Discussion: Intervention cont.Discussion: Intervention cont.Rest Breaks: Liston et al27 & Smith30 allowed unlimited rest
breaks for the participants - number & duration were not documented
A minimum of 10 mins of continuous aerobic exercise is required in healthy individuals for a training effect34
Unable to determine if 10 mins of continuous aerobic activity was achieved in these studies
Rest Breaks: Liston et al27 & Smith30 allowed unlimited rest
breaks for the participants - number & duration were not documented
A minimum of 10 mins of continuous aerobic exercise is required in healthy individuals for a training effect34
Unable to determine if 10 mins of continuous aerobic activity was achieved in these studies

Discussion: ControlsDiscussion: Controls
Large variability in control group therapy 3 of the control groups participated in walking
however at a lower dose than the experimental group27,28,29
Due to similar interventions the ability to detect change between groups may have been confounded
Large variability in control group therapy 3 of the control groups participated in walking
however at a lower dose than the experimental group27,28,29
Due to similar interventions the ability to detect change between groups may have been confounded

Discussion: Controls cont.Discussion: Controls cont. Smith30 found a trend in favour of the intervention
group The control group used only QOL logs
It is likely that a training stimulus may have improved ADLs in those studies that involved conventional PT in the control group
It may be more pertinent to compare aerobic exercise to conventional PT in order to determine if aerobic exercise should be incorporated as part of a conventional PT program
Smith30 found a trend in favour of the intervention group The control group used only QOL logs
It is likely that a training stimulus may have improved ADLs in those studies that involved conventional PT in the control group
It may be more pertinent to compare aerobic exercise to conventional PT in order to determine if aerobic exercise should be incorporated as part of a conventional PT program

Discussion: OutcomeDiscussion: Outcome
Specificity Limited specificity of studies with regards to the
intervention & the ADL tasks being measured 3 studies25-27,30 chose ADL measures that were not
closely related to the intervention & all had insignificant findings
Pohl et al29 used mobility related OM & demonstrated a statistically significant difference in favour of the intervention group
Specificity Limited specificity of studies with regards to the
intervention & the ADL tasks being measured 3 studies25-27,30 chose ADL measures that were not
closely related to the intervention & all had insignificant findings
Pohl et al29 used mobility related OM & demonstrated a statistically significant difference in favour of the intervention group

Limitations Limitations
Lack of high quality primary evidence Broad study question: heterogeneous Qualitative English studies only Authors were not contacted to retrieve
unpublished data
Lack of high quality primary evidence Broad study question: heterogeneous Qualitative English studies only Authors were not contacted to retrieve
unpublished data

ConclusionConclusion
Adequate dose must be achieved to see changes in ADLs in individuals post stroke
Higher quality & more specific studies are required to determine a dose response relationship for aerobic exercise post stroke & to find patterns among studies
OMs must be specific to the intervention
Adequate dose must be achieved to see changes in ADLs in individuals post stroke
Higher quality & more specific studies are required to determine a dose response relationship for aerobic exercise post stroke & to find patterns among studies
OMs must be specific to the intervention

Clinical ImplicationsClinical Implications
Limited evidence suggests that aerobic exercise has positive effects on ADLs in non-ambulatory individuals post stroke
Aerobic exercise should be used in conjunction with conventional PT as there is limited evidence to support its use in improving ADLs in individuals post stroke
Individuals post stroke must persist with an aerobic exercise program to continue to see changes in ADL function
Limited evidence suggests that aerobic exercise has positive effects on ADLs in non-ambulatory individuals post stroke
Aerobic exercise should be used in conjunction with conventional PT as there is limited evidence to support its use in improving ADLs in individuals post stroke
Individuals post stroke must persist with an aerobic exercise program to continue to see changes in ADL function

AcknowledgementsAcknowledgements
Darlene Reid & Elizabeth Dean Charlotte Beck Lara Boyd
Darlene Reid & Elizabeth Dean Charlotte Beck Lara Boyd

ReferencesReferences1. Canadian Brain and Nerve Health Coalition. The burden of neurological diseases, disorders, and
injuries in canada. . 2007. 2. Hu FB, Stampfer MJ, Colditz GA, et al. Physical activity and risk of stroke in women. J Am Med
Assoc. 2000;283(22:ate of Pubaton: 14 Jun 2000. 3. Potempa K, Lopez M, Braun LT, Szidon JP, Fogg L, Tincknell T. Physiological outcomes of
aerobic exercise training in hemiparetic stroke patients. Stroke. 1995;26:101-105. 4. Landin S, Hagenfeldt L, Saltin B, Wahren J. Muscle metabolism during exercise in hemiparetic
patients. Clin Sci Mol Med. 1977;53:257-269. 5. Ivey FM, Macko RF, Ryan AS, Hafer-Macko CE. Cardiovascular health and fitness after stroke.
Topics in Stroke Rehabilitation. 2005;12:1-16. 6. Macko RF, Smith GV, Dobrovolny CL, Sorkin JD, Goldberg AP, Silver KH. Treadmill training
improves fitness reserve in chronic stroke patients. Arch Phys Med Rehabil. 2001;82:879-884. 7. Silver KH, Macko RF, Forrester LW, Goldberg AP, Smith GV. Effects of aerobic treadmill
training on gait velocity, cadence, and gait symmetry in chronic hemiparetic stroke: A preliminary report. Neurorehabil Neural Repair. 2000;14:65-71.
8. Shephard RJ. Maximal oxygen intake and independence in old age. Br J Sports Med. 2009;43:342-346.
6. Kalapotharakos VI, Michalopoulos M, Strimpakos N, Diamantopoulos KBS, Tokmakidis SP. Functional and neuromotor performance in older adults: Effect of 12 wks of aerobic exercise. American Journal of Physical Medicine & Rehabilitation. 2006;85:61-67.
7. Vaynman S, Gomez-Pinilla F. License to run: Exercise impacts functional plasticity in the intact and injured central nervous system by using neurotrophins. Neurorehabil Neural Repair. 2005;19:283-295.
8. Armstrong L, Balady GJ, Berry MJ, et al. ACSM's Guidelines for Exercise Testing and Prescription. 7th ed. Baltimore Maryland: Lippincott Williams & Wilkins; 2006.
9. de Bruin AF, de Witte LP, Stevens F, Diederiks JPM. Sickness impact profile: The state of the art of a generic functional status measure. Social Science and medicine. 1992 Oct;35:1003-1014.
1. Canadian Brain and Nerve Health Coalition. The burden of neurological diseases, disorders, and injuries in canada. . 2007.
2. Hu FB, Stampfer MJ, Colditz GA, et al. Physical activity and risk of stroke in women. J Am Med Assoc. 2000;283(22:ate of Pubaton: 14 Jun 2000.
3. Potempa K, Lopez M, Braun LT, Szidon JP, Fogg L, Tincknell T. Physiological outcomes of aerobic exercise training in hemiparetic stroke patients. Stroke. 1995;26:101-105.
4. Landin S, Hagenfeldt L, Saltin B, Wahren J. Muscle metabolism during exercise in hemiparetic patients. Clin Sci Mol Med. 1977;53:257-269.
5. Ivey FM, Macko RF, Ryan AS, Hafer-Macko CE. Cardiovascular health and fitness after stroke. Topics in Stroke Rehabilitation. 2005;12:1-16.
6. Macko RF, Smith GV, Dobrovolny CL, Sorkin JD, Goldberg AP, Silver KH. Treadmill training improves fitness reserve in chronic stroke patients. Arch Phys Med Rehabil. 2001;82:879-884.
7. Silver KH, Macko RF, Forrester LW, Goldberg AP, Smith GV. Effects of aerobic treadmill training on gait velocity, cadence, and gait symmetry in chronic hemiparetic stroke: A preliminary report. Neurorehabil Neural Repair. 2000;14:65-71.
8. Shephard RJ. Maximal oxygen intake and independence in old age. Br J Sports Med. 2009;43:342-346.
6. Kalapotharakos VI, Michalopoulos M, Strimpakos N, Diamantopoulos KBS, Tokmakidis SP. Functional and neuromotor performance in older adults: Effect of 12 wks of aerobic exercise. American Journal of Physical Medicine & Rehabilitation. 2006;85:61-67.
7. Vaynman S, Gomez-Pinilla F. License to run: Exercise impacts functional plasticity in the intact and injured central nervous system by using neurotrophins. Neurorehabil Neural Repair. 2005;19:283-295.
8. Armstrong L, Balady GJ, Berry MJ, et al. ACSM's Guidelines for Exercise Testing and Prescription. 7th ed. Baltimore Maryland: Lippincott Williams & Wilkins; 2006.
9. de Bruin AF, de Witte LP, Stevens F, Diederiks JPM. Sickness impact profile: The state of the art of a generic functional status measure. Social Science and medicine. 1992 Oct;35:1003-1014.

13. Duncan PW, Wallace D, Lai SM, Johnson D, Embretson S, Laster LJ. The stroke impact scale version 2.0: Evaluation of reliability, validity, and sensitivity to change. Stroke. 1999 Oct;30:2131-2140.
14. Hartigan I. A comparative review of the katz ADL and the barthel index in assessing the activities of daily living of older people. International Journal of Older People Nursing. 2007 September:204-212.
15. Harwood RH, Ebrahim S. A comparison of the responsiveness of the nottingham extended activities of daily living scale, london handicap scale and SF-36. Disability & Rehabilitation. 2000 Nov;22:786-793.
16. Loewen SC, Anderson BA. Reliability of the modified motor assessment scale and the barthel index. Physical Therapy. 1988 Jul;68:1077-1081.
17. Parker CJ, Gladman JRF, Logan PA. Development and validation of the nottingham leisure questionnaire Clinical Rehabilitation. 2001 Dec;15:647-56.
18. Rossier P, Wade DT, Murphy M. An initial investigation of the reliability of the rivermead extended ADL index in patients presenting with neurological impairment. Journal of Rehabilitation Medicine. 2001 Mar;33:61-70.
19. Salter K, Jutai JW, Teasell R, Foley NC, Bitensky J, Bayley M. Issues for selection of outcome measures in stroke rehabilitation: ICF activity. Disability & Rehabilitation. 2005 Mar;27:315-40.
20. Schepers VPM, Ketelaar M, van de Port IGL, Visser-Meily JMA, Lindeman E. Comparing contents of functional outcome measures in stroke rehabilitation using the international classification of functioning, disability and health. Disability & Rehabilitation. 2007 February;29:221-230.
21. Schlote A, Krüger J, Topp H, Wallesch C. Inter-rater reliability of the barthel index, the activity index, and the nottingham extended activities of daily living: The use of ADL instruments in stroke rehabilitation by medical and non medical personnel Rehabilitation. 2004 Apr;43:75-82.
22. Streppel KRM, van Harten WH, Warmerdam CGM. Short version of the sickness impact profile for evaluating rehabilitation programs. Journal of Rehabilitation Sciences. 1996;9:66-71.
23. Van de Port IGL, Ketelaar M, Schepers VPM, Van den Bos GAM, Lindeman E. Monitoring the functional health status of stroke patients: The value of the stroke-adapted sickness impact profile-30. Disability & Rehabilitation. 2004 Jun;26:635-640.
Wilkinson PR, Wolfe CDA, Warburton FG, et al. Longer term quality of life and outcome in stroke patients: Is the barthel index alone an adequate measure of outcome? Quality in Health Care. 1997 Sept;6:125-130.
13. Duncan PW, Wallace D, Lai SM, Johnson D, Embretson S, Laster LJ. The stroke impact scale version 2.0: Evaluation of reliability, validity, and sensitivity to change. Stroke. 1999 Oct;30:2131-2140.
14. Hartigan I. A comparative review of the katz ADL and the barthel index in assessing the activities of daily living of older people. International Journal of Older People Nursing. 2007 September:204-212.
15. Harwood RH, Ebrahim S. A comparison of the responsiveness of the nottingham extended activities of daily living scale, london handicap scale and SF-36. Disability & Rehabilitation. 2000 Nov;22:786-793.
16. Loewen SC, Anderson BA. Reliability of the modified motor assessment scale and the barthel index. Physical Therapy. 1988 Jul;68:1077-1081.
17. Parker CJ, Gladman JRF, Logan PA. Development and validation of the nottingham leisure questionnaire Clinical Rehabilitation. 2001 Dec;15:647-56.
18. Rossier P, Wade DT, Murphy M. An initial investigation of the reliability of the rivermead extended ADL index in patients presenting with neurological impairment. Journal of Rehabilitation Medicine. 2001 Mar;33:61-70.
19. Salter K, Jutai JW, Teasell R, Foley NC, Bitensky J, Bayley M. Issues for selection of outcome measures in stroke rehabilitation: ICF activity. Disability & Rehabilitation. 2005 Mar;27:315-40.
20. Schepers VPM, Ketelaar M, van de Port IGL, Visser-Meily JMA, Lindeman E. Comparing contents of functional outcome measures in stroke rehabilitation using the international classification of functioning, disability and health. Disability & Rehabilitation. 2007 February;29:221-230.
21. Schlote A, Krüger J, Topp H, Wallesch C. Inter-rater reliability of the barthel index, the activity index, and the nottingham extended activities of daily living: The use of ADL instruments in stroke rehabilitation by medical and non medical personnel Rehabilitation. 2004 Apr;43:75-82.
22. Streppel KRM, van Harten WH, Warmerdam CGM. Short version of the sickness impact profile for evaluating rehabilitation programs. Journal of Rehabilitation Sciences. 1996;9:66-71.
23. Van de Port IGL, Ketelaar M, Schepers VPM, Van den Bos GAM, Lindeman E. Monitoring the functional health status of stroke patients: The value of the stroke-adapted sickness impact profile-30. Disability & Rehabilitation. 2004 Jun;26:635-640.
Wilkinson PR, Wolfe CDA, Warburton FG, et al. Longer term quality of life and outcome in stroke patients: Is the barthel index alone an adequate measure of outcome? Quality in Health Care. 1997 Sept;6:125-130.

25. Katz-Laurer M, Carmeli E, Shochina M. The effect of early aerobic training on independence six months post stroke. Clin Rehabil. 2003;17:735-741.
26. Katz-Leurer M, Shochina M, Carmeli E, Friedlander Y. The influence of early aerobic training on the functional capacity in patients with cerebrovascular accident at the subacute stage. Arch Phys Med Rehabil. 2003;84:1609-1614.
27. Liston R, Mickelborough J, Harris B, Hann AW, Tallis RC. Conventional physiotherapy and treadmill re-training for higher-level gait disorders in cerebrovascular disease. Age & Ageing. 2000;29:311-318.
28. Macko RF, Ivey FM, Forrester LW, et al. Treadmill exercise rehabilitation improves ambulatory function and cardiovascular fitness in patients with chronic stroke: A randomized, controlled trial. Stroke. 2005;36:2206-2211.
29. Pohl M, Werner C, Holzgraefe M, et al. Repetitive locomotor training and physiotherapy improve walking and basic activities of daily living after stroke: A single-blind, randomized multicentre trial (DEutsche GAngtrainerStudie, DEGAS). Clin Rehabil. 2007;21:17-27.
30. Smith PS. The effect of treadmill training on functional limitation and disability measures in persons in the chronic stage of recovery from stroke. Texas Woman's University; 2006.
31. Chen C, Tang F, Chen H, Chung C, Wong M. Brain lesion size and location: Effects on motor recovery and functional outcome in stroke patients. Arch Phys Med Rehabil. 2000;81:447-452.
32. Furlan M, Marchai G, Viader F, Derlon J-, Baron J-. Spontaneous neurological recovery after stroke and the fate of the ischemic penumbra. Ann Neurol. 1996;40(2:ate of Pubaton: Aug 1996.
33. Rimmer JH, Rauworth AE, Wang EC, Nicola TL, Hill B. A preliminary study to examine the effects of aerobic and therapeutic (nonaerobic) exercise on cardiorespiratory fitness and coronary risk reduction in stroke survivors. Arch Phys Med Rehabil. 2009;90:407-412.
34. Pollock MLPD, Facsm, Gaesser GAPD, F.A.C.S.M., et al. ACSM position stand: The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Medicine & Science in Sports & Exercise. 1998;30:975-991.
25. Katz-Laurer M, Carmeli E, Shochina M. The effect of early aerobic training on independence six months post stroke. Clin Rehabil. 2003;17:735-741.
26. Katz-Leurer M, Shochina M, Carmeli E, Friedlander Y. The influence of early aerobic training on the functional capacity in patients with cerebrovascular accident at the subacute stage. Arch Phys Med Rehabil. 2003;84:1609-1614.
27. Liston R, Mickelborough J, Harris B, Hann AW, Tallis RC. Conventional physiotherapy and treadmill re-training for higher-level gait disorders in cerebrovascular disease. Age & Ageing. 2000;29:311-318.
28. Macko RF, Ivey FM, Forrester LW, et al. Treadmill exercise rehabilitation improves ambulatory function and cardiovascular fitness in patients with chronic stroke: A randomized, controlled trial. Stroke. 2005;36:2206-2211.
29. Pohl M, Werner C, Holzgraefe M, et al. Repetitive locomotor training and physiotherapy improve walking and basic activities of daily living after stroke: A single-blind, randomized multicentre trial (DEutsche GAngtrainerStudie, DEGAS). Clin Rehabil. 2007;21:17-27.
30. Smith PS. The effect of treadmill training on functional limitation and disability measures in persons in the chronic stage of recovery from stroke. Texas Woman's University; 2006.
31. Chen C, Tang F, Chen H, Chung C, Wong M. Brain lesion size and location: Effects on motor recovery and functional outcome in stroke patients. Arch Phys Med Rehabil. 2000;81:447-452.
32. Furlan M, Marchai G, Viader F, Derlon J-, Baron J-. Spontaneous neurological recovery after stroke and the fate of the ischemic penumbra. Ann Neurol. 1996;40(2:ate of Pubaton: Aug 1996.
33. Rimmer JH, Rauworth AE, Wang EC, Nicola TL, Hill B. A preliminary study to examine the effects of aerobic and therapeutic (nonaerobic) exercise on cardiorespiratory fitness and coronary risk reduction in stroke survivors. Arch Phys Med Rehabil. 2009;90:407-412.
34. Pollock MLPD, Facsm, Gaesser GAPD, F.A.C.S.M., et al. ACSM position stand: The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Medicine & Science in Sports & Exercise. 1998;30:975-991.

Questions?Questions?