Embed Size (px)
Citation preview

JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 41
The effectiveness of structured multidisciplinary rounding in acute care units on length of hospital stay and satisfaction of patients and staff: a systematic review protocol
Angela Mercedes1
Precillia Fairman1
Lisa Hogan1
Rexi Thomas1
Jason T Slyer1,2
1. College of Health Professions, Pace University, New York, USA
2. The Northeast Institute for Evidence Synthesis and Translation (NEST): a Collaborating
Center of the Joanna Briggs Institute
Corresponding author:
Angela Mercedes
Review question
What is the effectiveness of structured multidisciplinary rounding in acute care units on length of
hospital stay and satisfaction of patients and staff?
Background
Communication is defined as a process by which information is exchanged between individuals
through a common system of symbols, signs, language and behavior. Efficient and effective
communication among members of a healthcare team is invaluable for delivering quality patient
care.1,2
Ineffective communication within a team is identified as a contributing factor to the high
rate of adverse events in the inpatient setting.2 Fragmented care occurs as a result of
communication breakdown where important patient care information is not shared timely or
adequately. The Institute of Medicine’s 2001 report, Crossing the Quality Chasm: A New Health
System for the 21st Century, emphasizes safe, effective patient-centered care that is timely,
efficient and equitable.3 Failures in communication within multidisciplinary healthcare teams are
established causes of errors and negative health outcomes, including death.4
Improvements in organizational processes are needed to ensure a culture of patient safety;
paramount to this are processes and factors related to communication and coordination.5 Health

JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 42
care typically involves patient management by a number of different specialists. Coordinating
care through multiple handoffs necessitates effective communication of critical information.6
These are goals outlined in the Patient Protection and Affordable Care Act that was passed in the
United States in 2010.7 Maintaining collaborative efforts within the healthcare team, and between
patients and caregivers in inpatient acute care units depends largely on communication.8
Effective communication directly correlates with patient outcomes,9 adverse events,
10 and length
of stay.11
It is the common denominator of stress within the health care team.12
The ways by
which health care providers communicate can also impact on patient satisfaction.13
The World
Health Organization recommends improved communication between healthcare providers by
allocating sufficient time during patient encounters utilizing a standardized approach.14
Dwindling reimbursement, shifting emphasis on patient outcomes and satisfaction, and rapidly
rising health care costs lend impetus to finding new ways of providing safe, effective care in the
most timely manner possible, utilizing existing resources. Although the concept is not new,
multidisciplinary rounding (MDR), sometimes known as collaborative rounding or interdisciplinary
rounding, is being re-evaluated and refocused in many acute care settings to maximize its
potential impact on patient care issues. Multidisciplinary rounding has been identified as a way to
improve patient care by promoting health care provider communication, leading to a greater
shared knowledge of a patient’s status, smoother patient care flow, decreased length of stay, and
enhanced patient and staff satisfaction.15-18
In order to be considered multidisciplinary, rounds must consist of two or more disciplines
meeting together to review the plan of care, determine priorities, and coordinate and facilitate the
progression from one point of care to the next, either within the hospital, at another health care
facility, or to the community.16,18
Multidisciplinary rounding may be either nurse or physician led
and the make-up of the team may vary, depending on the needs of the patient and the unit.15,18
A
common team composition may consist of any combination of the primary medical provider,
specialty providers, medical residents, nurse practitioners, physician assistants, bedside nurse,
case manager, social worker, unit manager, and/or other ancillary service providers, as needed.18
Rounds may be walking, which has the advantage of allowing a quick visual assessment of the
patient and patient/family involvement,16
or they may be held at a central location, which may
improve the multidisciplinary team’s ability to talk more freely about the plan of care.15
Multidisciplinary rounding may be scripted or unscripted. Reimer and Herbener recommend that
MDR be held at the same time each day, be brief, be organized in such a manner that the
information covered is consistent from patient to patient yet individualized to each patient’s
needs, and occurs independently of any one discipline’s presence or absence.18
Ineffective communication among members of the healthcare team is caused by delays in
communication, failure to communicate with the appropriate team member, provision of
inaccurate or incomplete information, and matters left unresolved until the point of urgency.19
Many healthcare settings are implementing various communication strategies to add structure to
the MDR process with the goal of improving communication among the healthcare teams. One
strategy is the use of a standardized communication tool during MDR. A standardized
communication tool is a systematic approach that is used to enhance the ability to communicate

JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 43
effectively within or between disciplines.20
According to Narasimhan, Eisen, Mahoney, Acerra,
and Rosen, a standardized communication tool may be an important means to achieve reliable,
consistent and efficient communication that supports collaborative work in healthcare settings.20
Examples of standardized communication tools include checklists, daily goals sheets, door
communication cards, or the situation, background, assessment, and recommendation (SBAR)
tool. The SBAR tool is for the purpose of communicating changes on patients’ status in a timely
fashion.19
As per Diaz-Montes, Cobb, Ibeanu, Njoku, and Geraldi, the use of a checklist during
MDR may enhance communication as it acts as an agenda, triggering consistent information
exchange, and clarifying patient goals.21
The main purpose of a checklist is to organize and
outline criteria to be considered during MDR.21
A daily goals sheet clarifies a patient’s goals and
provides an accurate information source for each patient.20
The use of structured tools with a systematic approach to communication, either written or verbal,
may be a way of improving communication between different team members.19
A structured
communication tool used during MDR may be helpful in the busy healthcare environment where
important information could be missed resulting in treatment delay. A structured tool may also be
useful for informing all healthcare providers involved in a patient’s care on changes in the
patient’s status. Concerns can be addressed quickly, thus ensuring quality patient care.22
Cornell,
Townsend-Gervis, Vardaman, and Yates demonstrated decreased time for treatment, increased
staff satisfaction with communication, and higher rates of resolution of patient issues when a
communication tool was implemented during MDR on an inpatient unit.19
Narasimhan et al.
showed that the use of a daily goals sheet improved communication among the healthcare team
and decreased the length of stay in an intensive care unit.20
However, Ainsworth, Pamplin, Allen,
Linfoot, and Chung reported no improvement in communication during MDR with the use of a
daily goals door communication card, a tool similar to the daily goals sheet.23
Ambiguity remains
in the literature regarding the overall effectiveness of standardized communications tools used
during MDR and which type of tool may yield better outcomes.
The goal of MDR is to improve care coordination with the aim of reducing length of stay while
improving the satisfaction of the multidisciplinary team involved in the rounding and the
satisfaction of the patient being cared for. Efficient and effective healthcare improves the quality
of care delivered which decreases length of stay and provides a seamless transition to the next
level of care.20
Length of stay is defined as the number of days admitted to a healthcare facility or
a specific healthcare unit, and is calculated by totaling the number of days from admission to
discharge or the transition to the next point of care.
Patient satisfaction is an individual’s evaluative judgments concerning the quality of care received
from healthcare providers. Improved quality of care increases patient satisfaction.24
The use of a
structured communication tool may increase patient satisfaction by improving collaboration of
care.17
Multiple tools are available to measure patient satisfaction. An example of one measure is
the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey.
The HCAHPS survey evaluates a patient’s perspective of their care across nine essential
topics.25
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 44
Staff satisfaction is defined as a pleasurable or positive emotional state resulting from the
appraisal of one’s job or job experiences. Structured MDR utilizing a communication tool may be
one method to improve staff satisfaction.26
A number of surveys are available to measure staff
satisfaction. The Press-Ganey Employee Partnership Survey and the Gallup Consulting Survey
are two widely used survey tools.27
Multidisciplinary rounding is important for coordination of patient care across various specialties in
an inpatient setting; however, communication among the members of the healthcare team may
sometimes be less than optimal.10
This systematic review aims to determine the effectiveness of
using a standardized communication tool during MDR in acute care units on length of stay,
patient satisfaction and staff satisfaction. A search of MEDLINE, Cumulative Index to Nursing and
Allied Health Literature (CINAHL), the Joanna Briggs Institute Database of Systematic Reviews
and Implementation Reports, and the Cochrane Database of Systematic Reviews was performed
and no existing or ongoing systematic review on this topic was identified.
Keywords
Multidisciplinary rounds, length of stay, patient satisfaction, staff satisfaction
Inclusion criteria
Types of participants
This review will consider studies that include samples of healthcare providers, including, but not
limited to, physicians (both primary care and specialty providers), medical residents, nurse
practitioners, physician assistants, bedside nurses, case managers, social workers, unit
managers, and/or other ancillary services who provide direct care for adult patients (18 years and
older) hospitalized on inpatient acute care units for the management of any acute or chronic
illness. Studies focusing on pediatric, mental health or obstetric patients, or adult outpatients will
be excluded.
Types of intervention(s)
This review will consider studies that evaluate the implementation of a structured MDR process
on adult patients (18 years and over) hospitalized in acute care units for the management of any
acute or chronic illness. For the purpose of this review, structured MDR is defined as the process
of patient rounds by a multidisciplinary team utilizing a standardized communication tool.
Examples of standardized communication tools include, but are not limited to, checklists, SBAR
tools, and daily goal communication tools. A multidisciplinary team consists of two or more
disciplines involved in a patient’s care meeting to outline the plan of care. A multidisciplinary team
may consist of medical providers, nurses, case managers, social workers and/or other ancillary
service providers actively involved in the patient’s care.
Comparator intervention
This review will consider studies that compare structured MDR with MDR without the use of a
standardized communication tool or rounds without a multidisciplinary approach.
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 45
Types of outcomes
The review will consider studies focusing on three primary outcomes of interest: length of stay,
patient satisfaction and/or staff satisfaction. Length of stay is defined as the number of days
admitted to a healthcare facility or a specific healthcare unit. Length of stay is calculated from the
day of admission to discharge or the transition to the next point of care. Patient satisfaction is an
individual’s evaluative judgment concerning the quality of care received from healthcare
providers. Staff satisfaction is defined as a pleasurable or positive emotional state resulting from
the appraisal of one’s job or job experiences. Studies that evaluate patient satisfaction and/or
staff satisfaction, as measured by valid and reliable tools, such as, but not limited to, the Hospital
Consumer Assessment of Healthcare Providers and Systems (HCAHPS), which measures
patient satisfaction, or the Press Ganey Employee Partnership Survey, which measures staff
satisfaction, will be considered for inclusion.
Types of studies
The review will consider randomized controlled trials and quasi-experimental studies for inclusion.
In the absence of these, the review will consider other quantitative research designs such as
observational or descriptive designs for inclusion.
Search strategy
The search strategy aims to find both published and unpublished studies. A three-step search
strategy will be utilized in this review. An initial limited search of PubMed and CINAHL will be
undertaken followed by an analysis of the text words contained in the title and abstract, and of the
index terms used to describe the article. A second search using all identified keywords and index
terms will then be undertaken across all included databases. Third, the reference list of all
identified reports and articles will be searched for additional studies. Studies published in or
translated into the English language will be considered for inclusion in this review. Studies
published from the inception of the databases searched through the current date of the review will
be considered for inclusion in this review.
The databases to be searched include: PubMed, CINAHL, Excerpta Medica Database
(EMBASE), Cochrane Central Register of Controlled Trials (CENTRAL), Health Source:
Nursing/Academic Edition, and Scopus.
The search for unpublished studies will include: New York Academy of Medicine, ProQuest
Dissertation and Thesis, ClinicalTrials.gov, Google Scholar, and the Virginia Henderson
International Nursing Library.
Initial keywords to be used will be: acute care unit, multidisciplinary rounds, rounding, length of
stay, patient satisfaction, and staff satisfaction.
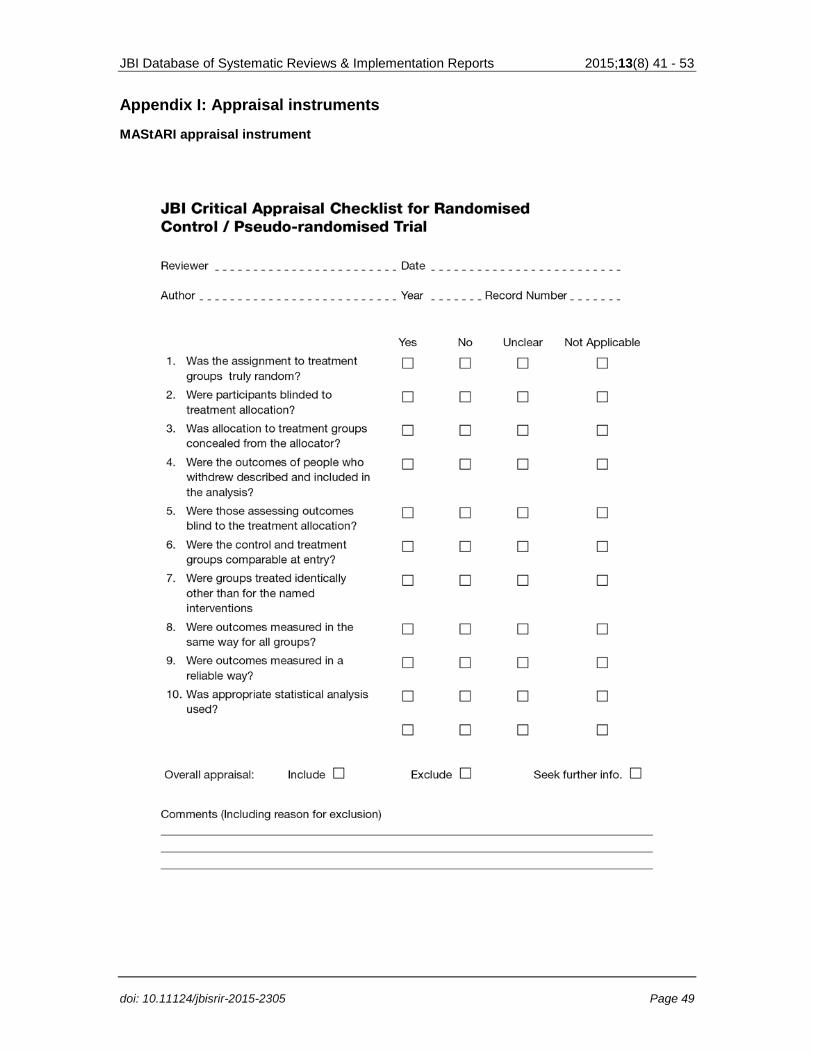
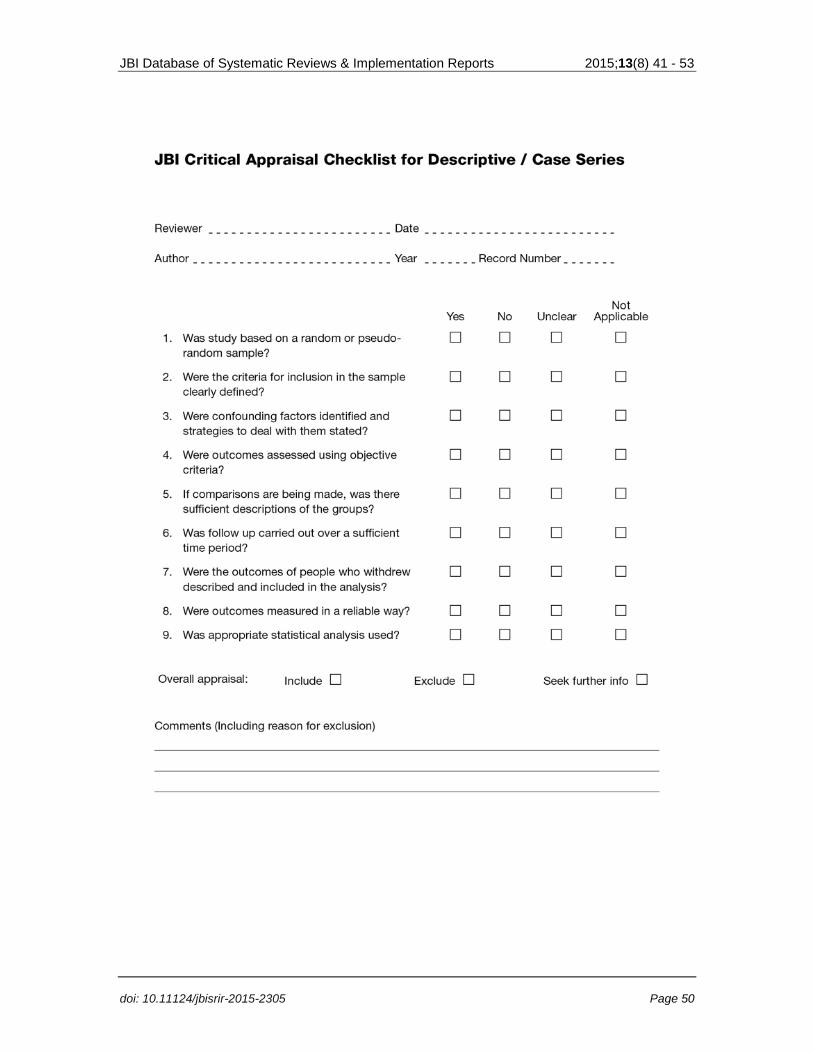
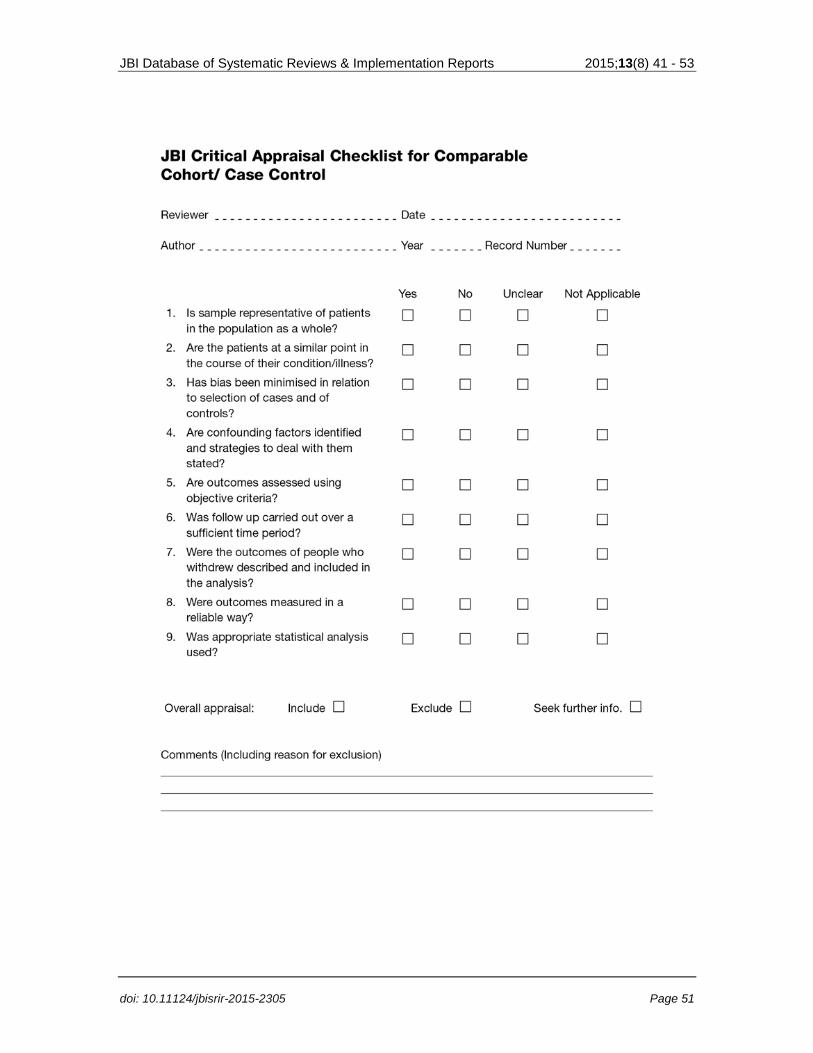
Assessment of methodological quality
Papers selected for retrieval will be assessed by two independent reviewers for methodological
validity prior to inclusion in the review using standardized critical appraisal instruments from the
Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument (JBI-
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 46
MAStARI) (Appendix I). Any disagreements that arise between the reviewers will be resolved
through discussion, or with a third reviewer.
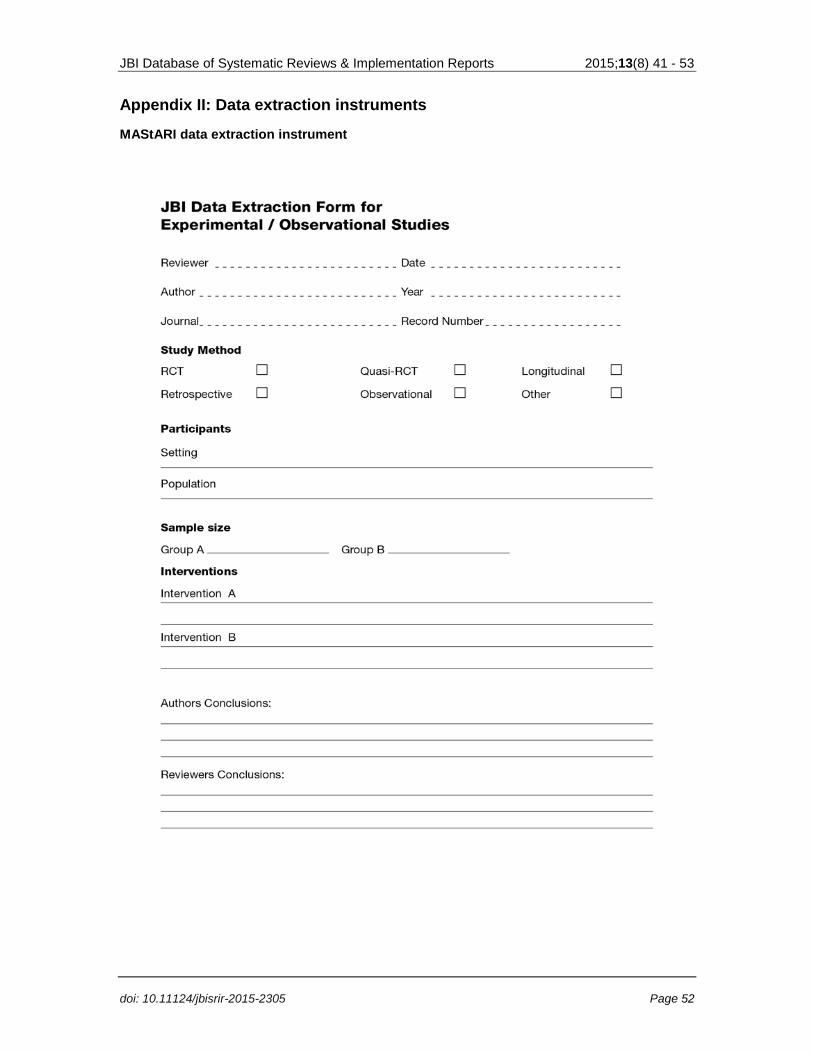
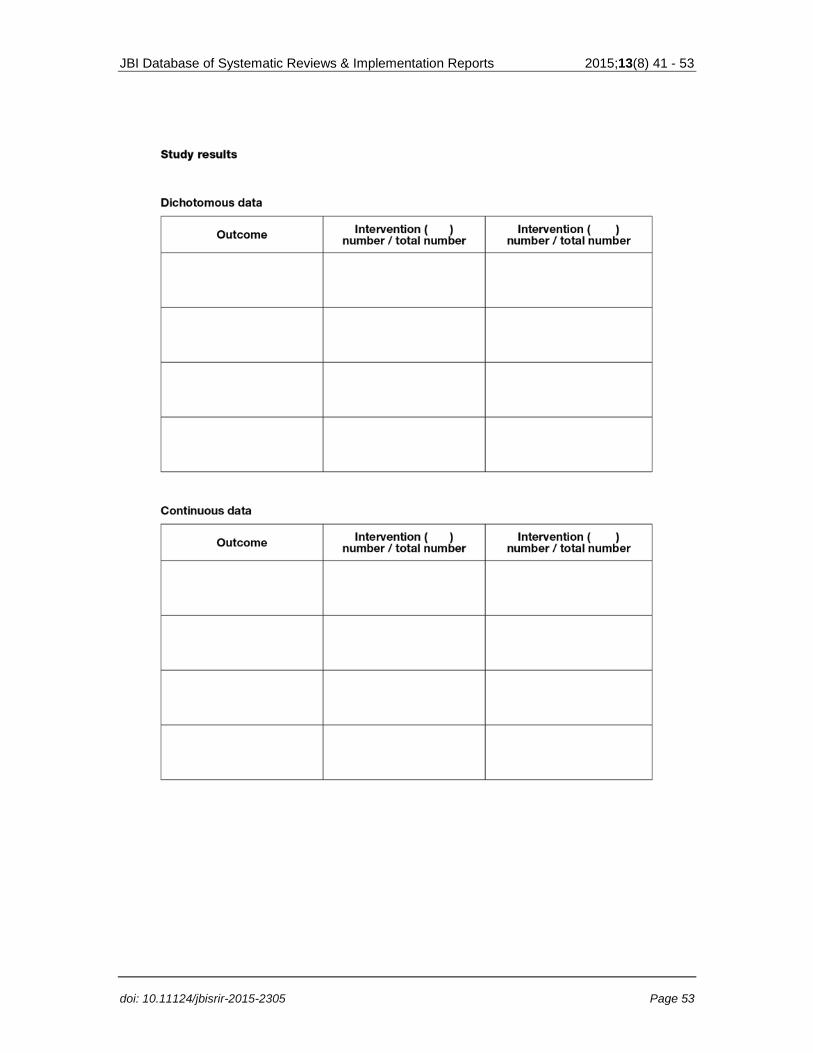
Data extraction
Data will be extracted from papers included in the review by two independent reviewers using the
standardized data extraction tool from JBI-MAStARI (Appendix II). The data extracted will include
specific details about the interventions, populations, study methods and outcomes of significance
to the review question and specific objectives. Any disagreements that arise between the
reviewers will be resolved through discussion, or with a third reviewer.
Data synthesis
Quantitative data will, where possible be pooled in statistical meta-analysis using JBI-MAStARI.
All results will be subject to double data entry. Effect sizes expressed as weighted mean
differences (for continuous data) and their 95% confidence intervals will be calculated for
analysis. Heterogeneity will be assessed statistically using the standard Chi-square and also
explored using subgroup analyses based on the different study designs included in this review.
Where statistical pooling is not possible, the findings will be presented in narrative form including
tables and figures to aid in data presentation where appropriate.
Conflicts of interest
The authors have no conflicts of interest to disclose.
Acknowledgements
This review will partially fulfill degree requirements for successful completion of the Doctor of
Nursing Practice Program at Pace University, College of Health Professions, New York, NY for:
Angela Mercedes, MS, RN, FNP-BC; Precillia Fairman, MS, RN, FNP-BC; Lisa Hogan, MS, RN,
FNP-BC; and Rexi Thomas, MS, RN, FNP.
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 47
References
1. Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective
teamwork and communication in providing safe care. Qual Saf Health Care. 2004;13(suppl 1):i85-
i90.
2. Lingard L, Espin S, Whyte S, Regehr G, Baker G, Reznick R, et al. Communication failures
in the operating room: an observational classification of recurrent types and effects. Qual Saf
Health Care. 2004;13(5):330-4.
3. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st
Century. Washington DC: National Academy Press; 2001.
4. Brock D, Abu-Rish E, Chiu CR, Hammer D, Wilson S, Vorvick L, et al. Interprofessional
education in team communication: working together to improve patient safety. Postgrad Med J.
2013;89(1057):642-51.
5. World Health Organization. Patient safety research: a guide for developing training
programmes. Geneva, Switzerland: World Health Organization; 2012. [Internet]. [Cited on April 7,
2015]. Available from: http://apps.who.int/iris/bitstream/10665/75359/1/9789241503440_eng.pdf
6. Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures: an insidious contributor to
medical mishaps. Acad Med. 2004;79(2):186-94.
7. Patient Protection and Affordable Care Act of 2010. Pub. L. 111-148. 124 Stat. 119. 23 Mar.
2010. [Internet]. [Cited on March 30, 2015]. Available from: http://www.gpo.gov/fdsys/pkg/PLAW-
111publ148/pdf/PLAW-111publ148.pdf
8. Kelly AE. Relationships in Emergency Care: Communication and Impact. Adv Emerg Nurs J.
2005;27(3):192-7.
9. Hindle D, Braithwaite J, Iedema R, Travaglia J. Patient safety: a review of key international
enquiries. Sydney: Clinical Excellence Commission; 2005.
10. Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L, Hamilton JD. The quality in
Australian health care study. Med J Aust. 1995;163(9):458-71.
11. Sprivulis PC, Da Silva JA, Jacobs IG, Frazer AR, Jelinek GA. The association between
hospital overcrowding and mortality among patients admitted via Western Australian emergency
departments. Med J Aust. 2006;184(5):208-12.
12. Perry L. Critical incidents, crucial issues: insights into the working lives of registered nurses.
J Clin Nurs.1997;6(2):131-7.
13. Saunders K. A Creative New Approach to Patient Satisfaction. Adv Emerg Nurs J.
2005;27(4):256-7.
14. World Health Organization. Communication during patient hand-overs. Patient Safety
Solutions. 2007;1(3):1-4. [Internet]. [Cited on April 1, 2015]. Available from:
http://www.who.int/patientsafety/solutions/patientsafety/PS-Solution3.pdf
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 48
15. Geary S, Cale DD, Quinn B, Winchell J. Daily rapid rounds: Decreasing length of stay and
improving professional practice. J Nurs Adm. 2009;39(6):293-8.
16. Sen A, Xiao Y, Lee SA, Hu P, Dutton RP, Haan J, et al. Daily multidisciplinary discharge
rounds in a trauma center: A little time, well spent. J Trauma. 2009;66(3):880-7.
17. Vazirani S, Hays RD, Shapiro MF, Cowan M. Effect of a multidisciplinary intervention on
communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14(1):71-
7.
18. Reimer N, Herbener L. Round and round we go: Rounding strategies to impact exemplary
professional practice. Clin J Oncol Nurs. 2014;18(6):654-60.
19. Cornell P, Townsend-Gervis M, Vardaman JM, Yates L. Improving situation awareness and
patient outcomes through interdisciplinary rounding and structured communication. J Nurs Adm.
2014;44(3):164-9.
20. Narasimhan M, Eisen L, Mahoney C, Acerra F, Rosen M. Improving physician
communication and satisfaction in the intensive care unit with a daily goals worksheet. Am J Crit
Care. 2006;15(2):217-22.
21. Diaz-Montes TP, Cobb L, Ibeanu OA, Njoku P, Geraldi MA. Introduction of checklist at daily
progress notes improves patient care among the gynecological oncology service. J Patient Saf.
2012;8(4):189-93.
22. Wilson FJ, Newman A, Ilari S. Innovative solutions: Optimal patient outcomes as a result of
multidisciplinary rounds. Dimens Crit Care Nurs. 2009;28(4):171-3.
23. Ainsworth CR, Pamplin JC, Allen DA, Linfoot JA, Chung KK. A bedside communication tool
did not improve the alignment of a multidisciplinary team’s goals for intensive care unit patients. J
Crit Care. 2013;28(1):112e7-e13.
24. Atallah M, Hamdan-Mansour A, Al-Sayed M, Aboshaiqah A. Patients' satisfaction with the
quality of nursing care provided: The Saudi experience. Int J Nurs Pract. 2013;19(6):584-90.
25. HCAHPS Project Team. CAHPS® Hospital Survey [Internet]. 2015 [Cited on April 28, 2015].
Available from: http://www.hcahpsonline.org/home.aspx
26. O'Leary K, Wayne D, Haviley C, Slade M, Jungwha L, Williams M. Improving teamwork:
Impact of structured interdisciplinary rounds on a medical teaching unit. J Gen Intern Med.
2010;25(8):826-32.
27. Advancing Excellence in Long Term Care Collaborative. Advancing Excellence in America’s
Nursing Homes: Staff Satisfaction Survey Tools 2010. [Internet]. [Cited on April 7, 2015].
Available from: https://www.nhqualitycampaign.org/files/Staff_Satisfaction_Survey_Tools.pdf
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 49
Appendix I: Appraisal instruments
MAStARI appraisal instrument
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 50
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 51
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 52
Appendix II: Data extraction instruments
MAStARI data extraction instrument
JBI Database of Systematic Reviews & Implementation Reports 2015;13(8) 41 - 53
doi: 10.11124/jbisrir-2015-2305 Page 53






![Multidisciplinary Rounding Presentation[1] · Early Steps • Determined which disciplines to include • Identified the needed frequency of rounding • Daily Monday -Friday •](https://img.pdfslide.us/doc/110x75/5f676336d81aac13ea272fc1/multidisciplinary-rounding-presentation1-early-steps-a-determined-which-disciplines.jpg)






















