Embed Size (px)
Citation preview

The Effectiveness of Health Care Teams
in the National Health Service
Report
Carol S. Borrill, Jean Carletta,Angela J. Carter, Jeremy F. Dawson, Simon Garrod,
Anne Rees, Ann Richards,David Shapiro and Michael A. West
Aston Centre for Health Service Organization Research,
Aston Business School, University of Aston
Human Communications Research Centre,
Universities of Glasgow and Edinburgh
Psychological Therapies Research Centre, University of Leeds

Contents______________________________________________
__
Key Findings
Acknowledgements
Health Care Team Effectiveness Project: Summary
Chapter 1 Teamwork, Communication and Effectiveness in Health Care: A Review Page 1
Chapter 2 Primary Health Care TeamResearch Methods and Sample Details Page 25
Chapter 3 Primary Health Care Team Results from Surveyand External Ratings Page 44
Chapter 4 Qualitative Research: Developing Objectives andEffectiveness Measures for Primary Health Care Teams Page 57
Chapter 5 Community Mental Health TeamsResearch Methods and Sample Details Page 78
Chapter 6 Community Mental Health TeamsResults from Survey and External Ratings Page 103
Chapter 7 Community Mental Health TeamsResults from Qualitative Research Page 121
Chapter 8 Secondary Health Care TeamsResearch Methods and Sample Details Page 141
Chapter 9 Secondary Care Teams Ratings Page 157
Chapter 10 Meetings and CommunicationResearch Methods Page 172
Chapter 11 Analysis of Communication in PHCT Teams Page 182
Chapter 12 Analysis of Communication in CHMT's Page 197
Chapter 13 Conclusions and Recommendations Page 215
Appendix I Survey Instruments/Rating Measures/Interview Schedules

Appendix II Knowing the way: Effectiveness in Primary Health Care
Appendix III Developing Effectiveness Measures for Primary Health Care Teams
Appendix IV Training Programme – Tools and Techniques for AssessingPerformance
Bibliography

Acknowledgements________________________________________________________
Liaison Officers: Liz MeerabeauSue LongsdateJohn Wilkinson
Advisory Group Members: Debbie MellorsNHS Executive
Sarah ConnorsNHS Executive
Jim FordNHS Executive
Bonnie SibbaldNHS Executive
Eileen RobertsonNHS Executive
Sheila RobertsDepartment of Health
Terry BreughaUniversity of Leicester
Anne NettonUniversity of Kent
Thelma SackmanNHS Executive
Research Team:
Dr Carol Borrill January 1997 - December 1999Aston Business SchoolAston UniversityBirmingham
Sam Bedlingham June 1997 - December 1999City UniversityLondon
Jean Carletta January 1997 - December 1999Human CommunicationResearch CentreEdinburgh

Christine Carmichael June 1997 - February 1998Institute of Work PsychologySheffield UniversitySheffield
Angela Carter January 1998 - December 1999Institute of Work PsychologySheffield UniversitySheffield
Jeremy Dawson July 1999 - December 1999Aston Business SchoolAston UniversityBirmingham
Simon Garrod January 1997 - December 1999Human Communications Research CentreGlasgow UniversityGlasgow
Heidi Frazer-Krauss January 1997 - June 1997Medical SchoolGlasgow UniversityGlasgow
Anne Rees January 1997 - June 1997Psychological Therapies Research CentreLeeds UniversityLeeds
Anne Richards January 1997 - December 1999Psychological Therapies Research CentreLeeds UniversityLeeds
Carein Todd April 1997 - May 1998Institute of Work PsychologySheffield UniversitySheffield
David Shapiro April 1997 - May 1998Psychological Therapies Research CentreLeeds UniversityLeeds
Michael West January 1997 - December 1999Aston Business SchoolAston UniversityBirmingham
David Woods January 1998 - June 1999Institute of Work PsychologySheffield University

______________________________________________
Summary______________________________________________
________
A primary prescription that policy makers and practitioners have offered for meeting
the challenges facing the National Health Service is the development of
multidisciplinary team working. The importance of team working in health care has
been emphasised in numerous reports and policy documents on the National Health
Service. One particularly emphasised the importance of team working if health and
social care for people are to be of the highest quality and efficiency:
"The best and most cost-effective outcomes for patients and clients are
achieved when professionals work together, learn together, engage in clinical
audit of outcomes together, and generate innovation to ensure progress in
practice and service."
Over the last thirty years this has proved very difficult to achieve in practice because
of the barriers between professional groupings such as doctors and nurses. Other
factors such as gender issues also influence team working. For example, G.P.s are
predominantly men while the rest of the primary care service population is
predominantly women; community mental health psychiatrists are predominantly
men, whereas the rest of the population of community mental health teams is
predominantly women, and in hospital settings the ranks of consultants continue to
be largely made up of men. Other factors which impede the creation of effective
multidisciplinary teams include multiple lines of management, perceived status
differentials between different professional groups, and lack of organisational
systems and structures for supporting and managing teams.
The Health Care Team Effectiveness Project was commissioned by the Department
of Health. The overall aim of the research described here was to determine whether
and how multidisciplinary team working contributes to quality, efficiency and
innovation in health care in the NHS.

The objectives of the research were to establish:
• which team member characteristics such as age, gender, occupational group,
experience, qualifications, and team size, influence how well the teams work
together;
• how team working processes, such as participation, reflexivity, communication,
decision-making and leadership contribute to the effectiveness of teams,
particularly the quality of health care and the development of innovative practice;
The research programme was carried out over a three year period by a team of
researchers based at the universities of Aston, Edinburgh, Glasgow, Leeds and
Sheffield. During the course of the study information on team working was gathered
from some 400 health care teams. This involved consulting over 7,000 NHS
personnel and a large number of NHS clients. Five national workshops were held
with key representatives from primary health care and community health care. A wide
range of research methods was used, including questionnaire surveys, telephone
interviews, in-depth interviews, observation, focus groups and video and audio tape
recordings of meetings
The research was carried out in two stages: quantitative data collection from 100
primary health care teams (PHCTs), 113 community health care teams (CMHTs) and
193 secondary health care teams (SHCTs), and in-depth work with a sub-sample of
teams.
Key findings
Effectiveness
Quality of teamworking is powerfully related to effectiveness of health care teams:
Ø The clearer the team's objectives
Ø The higher the level of participation in the team
Ø The higher the level of commitment to quality
Ø The higher the level of support of innovation
…. the more effective are health care teams across virtually all domains of
functioning

Innovation
Quality of teamworking is powerfully related to innovation of health care teams:
• The clearer the team's objectives
• The higher the level of participation in the team
• The higher the level of commitment to quality
• The higher the level of support of innovation
….. the more innovative are health care teams across virtually all domains of
functioning
Mental Health
Those working in teams have much better mental health than those working in looser
groups or working individually. The benefits appear to be due to:
• Greater role clarity
• Better peer support
Those working in teams are also buffered from the negative effects of organizational
climate and conflict.
The better the functioning of team with respect to…
• Clarity of objectives
• Levels of participation
• Commitment to quality
• Support for innovation
… the better the mental health of team members across all domains of health care.
Organisational performance
There is a significant and negative relationship between the percentage of staff
working in teams and the mortality in these hospitals, taking account of both local
health needs and hospital size. Where more employees work in teams the death
rate is significantly lower (calculated on the basis of the Sunday Times Mortality

Index, Dr Foster; deaths within 30 days of emergency surgery and deaths after
admission for hip fracture)1.
Retention and turnover
Within health care, those working in well functioning teams are more likely to stay
working in their settings than those working in poorly functioning teams.
Leadership
In Community Mental Health and Primary Health Care, where there is no clear
leader/co-ordinator or where there is conflict over leadership team objectives are
unclear, and there are….
Ø Low levels of participation
Ø Low commitment to quality
Ø Low support for innovation
Ø Poor team member mental health
Ø Low levels of effectiveness and innovation
Communication
Communication, integration and regular meetings in PHC and CMC health care
teams are associated with higher levels of effectiveness and innovation, yet the
quality of meetings (particularly in Primary Health Care) is often poor.
Professional diversity
Diversity of professional groups in Primary Health Care is clearly linked to levels of
team innovation. In newly formed Community Mental Health Teams, this relationship
does not appear. The same findings emerged from research carried out with 85
breast cancer care teams2.
1 This finding is based on research recently completed by the research team at the Aston Centre forHealth Services Organisation Research (further details available from West or Borrill).
2 This finding is based on research recently completed by the research team at the Aston Centre forHealth Services Organisational Research (further details available from West or Borrill).

Conclusions
• Systematic and revolutionary organizational change is necessary if the positive
results of this research are to be implemented in practice.
• NHS organizations have to developed as team-based, rather than hierarchical.
• Structure, culture, work design, HRM and management have to accommodate
and enable rather than impede team-based working.
• NHS employees should be trained in the KSAs for working in teams.
• NHS managers should be trained to manage team-based organizations.

Chapter 1
Teamwork, Communication and Effectiveness in HealthCare:
A Review
The challenges of organising health care in the modern United Kingdom context are
considerable. There are continual improvements in medical technologies, greater
levels of knowledge and awareness amongst patient populations and increasing
demands for the variety of sources of health care available within the National Health
Service. The provision of free health care at the point of delivery to the population
has become one of the most important issues in the national political agenda in the
early part of the twenty-first century. At the same time the National Health Service
has become a massively complex institution characterised by large organisations,
repeated restructurings, and subject to a wide range of political and economic
pressures. The response of the government has been to promise a huge increase in
spending on the NHS; a key question to be answered in relation to this political
agenda is how can we organise health care and achieve good, fair and cost effective
services for the whole population. This report focuses on determining whether, and if
so, how teamworking can help.
In this first chapter we review the research evidence about the potential benefits of
teamworking and the factors that influence the effectiveness of teams, focusing
particularly upon their use in health care settings. We draw on empirical evidence
from research conducted in the United Kingdom, mainland Europe, North America
and Australia. The literature on team composition and the processes which influence
team performance is briefly reviewed with particular emphasis on communication,
decision-making and problem-solving. We then explore the influences of
organisational context and leadership, before presenting the theoretical model which
guided the research programme described in this report.
First we consider what a ‘team’ means. The activity of a group of people working
co-operatively to achieve shared goals is basic to our species (Baumeister & Leary,
1995). The current enthusiasm for teamworking in health care reflects a deeper,

perhaps unconscious, recognition that this way of working offers the promise of
greater progress than can be achieved through individual endeavour. Mohrman,
Cohen, and Mohrman (1995) define a team as:
“a group of individuals who work together to produce products or deliver
services for which they are mutually accountable. Team members share
goals and are mutually held accountable for meeting them, they are
interdependent in their accomplishment, and they affect the results
through their interactions with one another. Because the team is held
collectively accountable, the work of integrating with one another is
included among the responsibilities of each member".
Benefits of teamwork
The belief that teamwork is the most effective way of delivering products and
services has gained increasing ascendancy within diverse organisational settings
(Guzzo & Shea, 1992; West, 1996). As organisations have grown in size and
become structurally more complex, the need for teams of people to work together in
co-ordinated ways to achieve objectives that contribute to the overall aims of
organisations has become increasingly urgent. Mohrman et al. (1995) offer ten
reasons for implementing team-based working in organisations:
• Teams are the best way to enact the strategy of organisations, because of the
need for consistency between organisational environment, strategy and design
(Galbraith, Lawler, & Associates, 1993).
• Teams enable organisations to speedily develop and deliver services cost
effectively, while retaining high quality.
• Teams enable organisations to learn (and retain learning) more effectively
(Senge, 1990).
• Cross-functional teams promote improved quality of services (Deming, 1986;
Juran, 1989).
• Cross-functional teams can undertake effective process re-engineering
(Davenport, 1993).
• Time is saved if activities, formerly performed sequentially by individuals, can be
performed concurrently by people working in teams (Myer, 1993).
• Innovation is promoted within team-based organisations because of cross-
fertilisation of ideas (Senge, 1990; West & Pillinger, 1995).

• Flat organisations can be monitored, co-ordinated and directed more effectively if
the functional unit is the team rather than the individual (Galbraith, 1993, 1994).
• As organisations have grown more complex, so too have their information
processing requirements; teams can integrate and link in ways individuals cannot
(Lawrence and Lorsch, 1969, Galbraith, 1993, 1994).
This approach to the delivery of services and products is not simply a managerial fad,
since there is substantial empirical evidence that the introduction of teamwork can
lead to increased effectiveness in the delivery of both quantity and quality of goods or
services (Guzzo & Shea, 1992; Weldon & Weingart, 1993).
Macy and lzumi (1993) conducted an analysis of 131 organisational change studies
in order to determine their effectiveness. Those interventions with the greatest
effects on organisational performance and 'the bottom-line' were team-related
interventions. They also reduced turnover and absenteeism more than did other
interventions, showing that team oriented practices can have broad positive effects in
organisations. Other research by Kahleberg & Moody (1994), who studied over 700
work establishments, found that those in which teamwork was developed were more
effective in their performance than those in which teams were not used. Finally,
Applebaum and Batt (1994) offer similar evidence. They reviewed the results of a
dozen surveys of organisational practices, as well as 185 case studies of innovative
management practices. They too found compelling evidence that teams contribute
to improved organisational effectiveness, particularly increasing efficiency and
quality.
Teamwork in health care
The importance of teamworking in health care has been emphasised in numerous
reports and policy documents on the National Health Service (NHS). One (NHSME,
1993) particularly emphasised the importance of teamworking if health and social
care for people were to be of the highest quality and efficiency:
"The best and most cost-effective outcomes for patients and clients are
achieved when professionals work together, learn together, engage in
clinical audit of outcomes together, and generate innovation to ensure
progress in practice and service."

Some limited research has suggested the positive effects of multidisciplinary
teamworking in health care. However, there are many difficulties inherent in
comparing evaluation studies, which include teams having different objectives and
organisation patterns, studies variously controlling for other concurrent changes in
local services and the pre-existing variations in services and cultures (Jackson,
Gater, Goldberg, Tantam, Loftus & Taylor, 1993).
In terms of the delivery of care, teams have been reported to reduce hospitalisation
time and costs, improve service provision, enhance patient satisfaction, staff
motivation and team innovation. We review the literature relevant to each of these
outcomes below.
Reduced hospitalisation and costs
Sommers and colleagues (2000) compared primary health care teams with physician
care across 18 private practices, and concluded that primary health care teams
lowered hospitalisation rates and reduced physician visits while maintaining function
for elderly patients with chronic illness and functional deficits. Significant cost savings
were born from reduced hospitalisation, which more than accounted for the costs of
setting up the team and making regular home visits. Jones (1992) also reported that
families who received primary health team care had fewer hospitalisations, fewer
operations, less physician visits for illness and more physician visits for health
supervision than control families. A similar pattern emerged for terminally ill patients,
where their increased utilisation of home care services more than offset savings in
hospital costs, such that there were average savings of 18% in hospital costs
(Hughes, Cummings, Weaver, Manheim, Brown & Conrad, 1992).
In another study in the U.S., Eggert and colleagues (1991) concluded that a team
focussed case management system generated similar benefits for elderly, chronically
ill patients. The team approach reduced total health care expenditures by 13.6%,
when compared to an individualised case management system. The team combined
earlier discharge, more timely nursing home placement and better-organised home
support and care, to reduce patient hospitalisation by 26%. Similarly, the cost
increases in ambulatory and nursing home care were offset by fewer and shorter stay
hospital admissions and reduced home care utilisation. For patients with dementia in
this study, the team model of case management reduced overall costs even further,
by 41% (Zimmer, Eggert & Chiverton, 1990). At the end of the 27-month study, there
were more team than control patients living at home and fewer in nursing homes. An

audit of the case managers' records highlighted more intense management activity in
the team group, where patients were referred more frequently for medical evaluation,
respite and day care. Team case managers had smaller caseloads, made more
home visits and had more case conferences. Teams were more familiar with local
community resources and were reported as being more responsive to patient crises.
The team approach was reported to offer greater intensity of case management,
which resulted in more efficient care provision in hospitals and home health services.
Improved service provision
Primary care teams appear to produce better detection, treatment, follow-up and
outcome in hypertension (Adorian, Silverberg, Tomer & Wamosher, 1990).
Specifically, nurses in England reported that working together in primary health care
teams reduced duplication, streamlined patient care and enabled specialist skills to
be used more cost-effectively (Ross, Rink & Furne, 2000).
Jansson, Isacsson and Lindholm (1992) analysed the records of general practitioners
and district carers over 6 years in Sweden. Care teams (GP, district nurse, assistant
nurse) were introduced into one region but were absent in another comparative
region. The care teams reported a large rise in the overall number of patient contacts
and in the proportion of the population who accessed the district nurse. Concurrently,
there was a reduction in emergency visits, which they attributed to better accessibility
and continuity of care in the teams.
Jackson and colleagues (1993) reported a similar pattern twelve months after the
introduction of a community mental health team in England. They reported a
threefold increase in the rate of inception to care, a doubling in the prevalence of
treated psychiatric disorder and a reduction in demand on the hospital’s outpatient
services. It was suggested that the team was making specialist care more available
to patients with severe mental illness who would not have previously received care
from mental health services. The team also provided care in a timelier manner that
was accessible and continuous.
Enhanced patient satisfaction
Hughes and colleagues (1992) compared the provision of hospital-based team home
care and customary care for 171 terminally ill patients in a large U.S. Department of
Veterans Affairs hospital. They noted increased access to home care services and
improved patient and carer satisfaction with hospital-based team home care. Both

patients and caregivers of the team expressed significantly higher levels of
satisfaction with continuous and comprehensive care at one month, and they
continued to express higher levels of satisfaction at six months. The team program
maintained patients at home for significantly more days than the control group, who
were kept in hospital in general wards for longer. Patients of the team received
almost twice as many home visits as the control group and visited the clinic
significantly fewer times.
Increased satisfaction by patients who had access to a primary health care team was
reported to include a higher mean number of social activities, fewer symptoms and
slightly improved overall health. These differences were noted in comparison to
patients who only had access to a physician (Sommers et. al., 2000).
Staff motivation
Primary care teamworking has been reported to improve staff motivation (Wood,
Farrow, & Elliott, 1994). In a study in Spain, Peiro, Gouzalez-Roma & Romos (1992)
showed relationships between work team processes, role clarity, job satisfaction and
leader behaviours. Effectiveness of teamwork was also related to job satisfaction
and mental health of team members. Sommers and colleagues (2000) suggested
that lower rates of hospitalisation for patients of primary health care teams were more
likely to be found in teams where individual members were most satisfied with their
working relationships.
Innovation
Teamwork is reputed to promote innovation in organisations including those in the
health care sector. In order to promote organisational innovation, policy makers and
practitioners are increasingly asking for clarification of the factors that determine
innovation in teams. Many input and process variables have been demonstrated to
predict innovation in teams.
In relation to inputs, there is some evidence that heterogeneity of team composition
is related to team innovation (Hoffman & Maier, 1961; McGrath, 1984; Jackson,
1996). West and Anderson (1996) carried out a longitudinal study of the functioning
of top management teams in 27 hospitals and examined relationships between team
and organisational factors and team innovation. Their results suggested that team
processes best predicted the overall level of team innovation, while the proportion of
innovative team members predicted the rated radicalness of innovations introduced.

Specifically, West and Wallace (1991) found that team collaboration, commitment to
the team and tolerance of diversity were positively related to team innovativeness.
By what means are these various benefits of teamworking in health care realised?
Partly at least through their composition and through effective team processes such
as communication, decision-making and problem-solving. We therefore briefly
review research in these areas before turning to consider the influence of the
organisations within which teams function.
Team composition and Processes
There is considerable agreement that heterogeneity of skills in teams performing
complex tasks is good for effectiveness (e.g., Campion et. al., 1994; Guzzo &
Dickson, 1996; Jackson, 1996; Millikan & Martins, 1996; Maznevski 1994).
Heterogeneity of skills and knowledge automatically implies that each team member
will bring a different knowledge perspective to the problem, a necessary ingredient
for creative solutions (Sternberg & Lubart, 1990; West, 1997).
However, teams that are diverse in task-related attributes are often diverse in
individual attributes. Variation in individual characteristics can trigger stereotypes
and prejudice (Jackson, 1996) which, via interteam conflict (Tajfel, 1978; Tajfel &
Turner, 1979; Hogg & Abrams, 1988), can affect team processes and outcomes. As
an example, Alexander, Lichtenstein and D’Aunno (1996) found that individuals in
multidisciplinary treatment teams in U.S. Department of Veterans Affairs hospitals,
who were members of larger and more heterogeneous teams, reported poor team
functioning. Physicians and social workers assessed team functioning more
positively than did nurses. The greater the diversity of individual characteristics of
team tenure, age and occupation within teams, the more negatively did team
members assessed team functioning.
Gender
Gender is an important influence on communication within teams. Not only are men
consistently more assertive in public situations and confrontations (Kimble, Marsh &
Kiska, 1984; Mathison & Tucker, 1982), but also communication expectations differ
for men and women. Sex-role stereotypes prescribe passive, submissive and
expressive communication for women while men are expected to be active,
controlling and less expressive communicators (LaFrance & Mayo, 1978).
Punishment for violation of expectations (Jussim, 1986; Jussim, Coleman & Lerch,

1987; Jackson, Sullivan & Lodge, 1993) may influence both the perceptions of
women in teams and their willingness to participate in team communication. Such
considerations are vitally important in health care teams where women dominate in
number, but men predominate in the highest status positions (in the present
research, GPs and psychiatrists, for example).
In support, Alexander, Lichtenstein and D’Aunno (1996) reported that the greater the
gender diversity, the more positive were team members’ assessment of how
cohesively and harmoniously teams operated. Their research suggested that mixed
gender teams included different orientations to work, namely a female focus on
workplace processes and relationships and a male focus on tasks and outcomes.
Team roles
It is important that teams have the appropriate mix of clearly defined team roles.
Jansson, Isacsson and Lindholm (1992) analysed the records of general practitioners
and district carers over a six-year period across 2 districts in Sweden following the
introduction of care teams into one region. They found that through the independent
roles of nurses and doctors were retained in the primary health care teams, all team
members interacted with the population in various situations, including home visits
and complemented each other across different competencies.
Team affective tone
Another important, but more controversial approach to understanding work team
processes and effectiveness, is offered by research on team affective tone. George
(1990) suggests that if members of a team experience similar kinds of affective
states at work (either negative or positive), then affect is meaningful not only in terms
of their individual experiences, but also at a team level. A number of studies have
demonstrated a significant relationship between team affective tone and behaviour
such as absenteeism (George, 1989, 1990, 1995). George proposes that teams that
are interested, strong, excited, enthusiastic, proud, alert, inspired, determined,
attentive and active, enable cognitive flexibility, creativity and effectiveness (George,
1996). However, she argues that team affective tone may not exist for all teams, so
it cannot be assumed a priori that it is a relevant construct for every team. George
(1996) sees team affective tone and team mental models as having a reciprocal
influence. So in a team with a negative affective tone, members would have different
cognitive processes from those in a team with a positive affective tone, which then
may influence team effectiveness.

There is some evidence that team mental models play an important role in team
decision-making (Klimoski & Mohammed, 1994), impacting on aspects of team
decision-making such as problem definition, speed and flexibility, alternative
evaluation and implementation (Walsh & Fahey, 1986: Walsh, Henderson &
Deighton, 1988). A team that has a high negative affective tone may tend to be more
rigid when making decisions. The nature and outcomes of team decision-making are
therefore likely to be affected by the interaction between team affective tone and
team mental models.
Communication
The study of communication in teams has a long history in social psychology, but
recent reviews by Guzzo & Dickenson (1996) and Guzzo and Shea (1992) reveal the
paucity of thorough industrial and organisational research in this area. Blakar (1985)
proposes five pre-conditions for effective communication in teams. Team members
must have shared social reality within which the exchange of messages can take
place, including a shared language base and perception. Team members must be
able to “decentre”, to take the perspective of others into account in relation to both
their affective and cognitive position (Redmond 1989, 1992). Team members must
be motivated to communicate. There must be “negotiated and endorsed contracts of
behaviour” (i.e. agreement among team members about how interactions take place).
Finally, the team must attribute communication difficulties appropriately, so if one of
the other preconditions is not being met, the team is able to correctly identify the
problem and develop a solution.
Several research studies in England have highlighted interprofessional
communication problems within primary health care teams. West and Field (1995)
and Field and West (1995) interviewed 96 members of primary health care teams
and described factors that impacted upon teamworking and communication in health
care. Structured time for decision-making, team cohesiveness and team-building all
influenced communication within teams. They highlighted the failure of health care
teams to set aside time for regular meetings to define objectives, clarify roles,
apportion tasks, encourage participation and handle change. Other reasons for poor
communication included differences in status, power, educational background,
assertiveness of members of the team, and the assumption that the doctors would be
the leaders (see also West & Pillinger, 1995; West & Slater, 1996).

Communication difficulties between different professional groups have been
highlighted particularly. Bond, et. al., (1985) surveyed 161 pairs of General
Practitioners (GPs) and health visitors, and 148 pairs of GPs and district nurses who
had patients in common. They reported low levels of communication and
collaboration between GPs and community nursing staff and suggested that GPs had
a very poor understanding of the health visitor's role. Similarly, McClure (1984)
describes low levels of communication in a survey of 48 health visitors and 45 district
nurses attached to general practices. Community nurses reported that
communication with practice staff was usually only about specific immediate patient
issues rather than team objectives, strategies, processes and performance review.
Health visitors were noted to be similarly unenthusiastic about progress in teamwork.
Ross, Rink and Furne (2000) found that health visitors perceived teams as less
effective. They suggested that health visitors were comparatively more defensive
about the benefits of changing role boundaries and considered themselves less able
to contribute to the teams as currently constituted. Cant and Killoran (1993) reached
similar conclusions, based on their research study with 928 practice nurses, 682
health visitors and 679 district nurses. They argued that joint professional training
and the instigation of regular team meetings were necessary to promote good
communication.
Cott (1997) used a social network analysis of 93 health care workers across 3
multidisciplinary long-term care teams to explore communication processes within
teams. She concluded that higher status multi-professional members communicated
most openly and worked fairly autonomously across loosely structured tasks, with
low levels of authority. In contrast, hierarchical nursing sub-teams did not report high
levels of information sharing.
West and Slater (1996) reported that much of the potential benefit of teamwork was
not being realised, with less than one in four health care teams building effective
communication and teamworking practices (see also West & Poulton, 1997). In a
similar vein, the Audit Commission report in 1992 drew attention to a major gap
between the rhetoric and reality:
"Separate lines of control, different payment systems leading to suspicion
over motives, diverse objectives, professional barriers and perceived
inequalities in status, all play a part in limiting the potential of multi-
professional, multi-agency teamwork. . . for those working under such

circumstances efficient teamwork remains elusive" (Audit Commission,
1992).
A number of researchers in different countries have highlighted the impact of
communication problems on patients across different types of teams. Nievaard
(1987) interviewed 112 nurses and 298 patients across 6 medical and surgical wards
of 2 general hospitals in the Netherlands. The study demonstrated the phenomenon
of problem shifting, where communication problems within the team were transferred
onto patients. It was reported that for hospital teams with a good communication
climate, nurses perceived patients as more attractive and interesting and less
dependent. However, if nurses viewed relationships with doctors, managers and
nurses in the team as problematic, their images of patients tended to be more
negative (unattractive, non-cooperative, dependent) and they did not want to
increase their contacts with patients.
Yeatts and Seward (2000) reported similar findings when they compared 3 self-
managed work teams in a medium size U.S. rural nursing home. They concluded that
enhanced communication between team members positively affected the service to
residents. Observations of a high performing team’s meetings showed that team
members had a high level of respect for each other, listened to each other, and were
not afraid to disagree when they held different views. Team members sought and
valued approval from each other, and they assisted each other to complete tasks.
Several studies have demonstrated how individual perceptions about teamwork and
roles can influence communication in teams. Dreachslin, Hunt & Sprainer (2000)
developed a grounded theory of the role that race plays in the self-perceived
communication effectiveness of nursing care teams in the U.S. They concluded that
racially diverse team members evaluated team communication according to different
perspectives and alternative realities.
When team members develop belief systems that are consistent with their
perspective and incongruent with other vantage points, differences in
perspective can result in alternative realities. Alternative realities encourage
participants to attribute causality differently which in turn fuels team conflict and
miscommunication by diminishing the team’s ability to reach a common
understanding of both the source of the conflict and the optimal path to its
resolution through effective communication (p. 1408).

Black participants were more likely to suggest that race exacerbated team conflict
and miscommunication, whereas white participants attributed problems to role and
status in the team. Further, different emphases and responsibility for communication
were acknowledged amongst the diversity of races, ethnicities, ages and genders.
Social isolation, selective perception and stereotypes also served to reinforce these
differences and deepen communication problems. Fewer occasions for social
interaction reduced opportunities to develop shared beliefs and a common social
reality across racial groups. The researchers therefore suggested that team
members be encouraged to understand different perspectives and appreciate
alternative realities, in order to lessen social isolation and reduce selective
perceptions and stereotyping behaviours.
Freeman, Miller and Ross (2000) also developed a grounded theory about
collaborative practice at the levels of the organisation, group and individual. They
conducted case studies of 6 teams working in a variety of specialist healthcare
services (diabetes, medical ward, primary healthcare, neuro-rehabilitation unit, child
development assessment, community mental health) and concluded that the
meanings different professionals ascribed to teamwork shaped how they
communicated and what they communicated about. When there was a lack of
congruence about aspects of teamwork, communication could potentially be
compromised. Individual perceptions determined the level of role understanding
considered necessary, and the value assigned to others’ contributions. Differences in
the understanding and valuing of team roles and levels of team learning exacerbated
underlying resentments, undermined professional esteem and created conflict.
Individual perceptions also influenced communication regarding tasks and about
sharing professional knowledge and ideas.
Decision making
Effective decision-making processes are central to team performance. Several
studies have reported the positive benefits of participative decision making in health
care teams. Yeatts and Seward (2000) compared 3 self-managed work teams in a
medium size U.S. rural nursing home. Team members of highly performing teams
reported that their ability to participate in work related decisions greatly increased
their job satisfaction and desire to come to work. These team members adopted a
consensus model of decision making, in which they clarified the problem, considered
alternatives, weighed the strengths and weaknesses of each alternative, and

selected the best option. Following their participation in making decisions, team
members reported an enhanced self-image and self-confidence, and they described
more positive interactions amongst themselves and with residents.
In contrast, Cott (1997) suggested that team members may not be equally
empowered to participate in decision making. Using a social network analysis of 93
health care workers across 3 multidisciplinary long-term care teams, she reported
that the highest status nurses and the core multidisciplinary professionals
participated most in decision making and problem solving activities. In comparison,
the lower status nursing sub-team primarily planned and assisted each other with
their more mechanistic tasks.
Problem solving
Team problem solving improves when members examine their definitions of a
situation to ensure they are solving the "right" problem (see for example, Bottger &
Yetton, 1987; Hirokawa, 1990; Landsberger, 1955; Maier, 1970; Schwenk, 1988). In
contrast, teams that detect problems too slowly or misdiagnose them often are
ineffective. Attributing problems to the wrong causes, or not communicating about
potential consequences, often undermine team effectiveness, especially when team
members fail to reflect on the possibility of error (Schwenk, 1984; Staw & Ross,
1989).
Teams that engage in more extensive scanning and discussion of their environments
perform better than those which do not identify problems (Ancona & Caldwell, 1988;
Main, 1989; Billings, Milburn & Schaalman, 1980). Tjosvold (1985; 1990) linked the
open exploration of opposing opinions within teams with effectiveness. Maier and
colleagues also suggested that cognitive stimulation produced novel ideas, and that
team effectiveness could be improved if teams were encouraged to be "problem
minded" rather than "solution minded" (Maier & Solem, 1962; see also Maier, 1950,
1970). Effectiveness was improved when teams questioned current approaches or
considered other aspects of problems (Maier, 1952). Similarly, Hackman & Morris
(1975) found that additional process discussions facilitated the quality of team
performance. The judged creativity of team decisions was related to the number of
comments made about performance strategy. When teams produced alternative
solutions to a problem, or separated and recombined problem solving strategies,
enhanced productivity was reported (Maier, 1970).

Teams that have to make complex decisions report that planning enhances their
performance (Hackman, Brousseau & Weiss, 1976; Smith, Locke & Barry, 1990).
However, when the environment becomes more uncertain, problem identification is
more difficult (Hedburg, Nystrom & Starbuck, 1976; Kiesler & Sproull, 1982).
Ineffective teams tend to deny, distort or hide problems (Stein, 1996). In some
teams, the identification of problems is discouraged as problems are regarded as
threats to morale, or a source of conflict (Janis, 1982; Miceli & Near, 1985; Smircich,
1983).
Thus far we have reviewed the benefits (and potential difficulties) of teamworking in
health care organisations - but the fact that teamworking takes place within
organisations is often ignored in the zeal to promote team effectiveness.
Accordingly, we now turn to address what is currently known about the influence of
their organisations upon teams.
Organisational context
Recent research suggests the broader context within which teams work has an
influence on their performance. Indeed the major change in emphasis in research on
teams in the last 15 years has been the shift from discussion of intrateam processes
to the impact of organisational context on teams. The organisation within which a
health care team functions can influence team effectiveness in a variety of powerful
ways. Researchers, such as Hackman (1990) and Tannenbaum, Beard and Salas
(1992) have suggested that the following are among the contextual factors that
influence team effectiveness:
• Team and organisational rewards
• Team objectives and performance feedback
• Training and technical assistance
• Physical work conditions
• Organisational climate
• Inter-team relationships
• Contracts and management structures
• Team size
These factors will be discussed further, in turn.

Team and organisational rewards
It has long been known in the social sciences that rewards are important for
improving performance. Reward systems, such as public recognition, preferred work
assignments and money enhance motivation and performance, particularly when the
rewards are contingent upon task achievement (Hackman, 1990; Sundstrom et al.,
1990; Vroom, 1964). However, team performance is most effective when rewards
are administered to the team as a whole and not to individuals, and when they
provide incentives for collaboration and communication rather than individualised
work (Hackman, 1990). This reinforces individuals working together as a team.
Gladstein (1984) found that in sales teams, pay and recognition affected the leader’s
behaviour and the way the team structured itself. Yet, NHS management directly
undermines teamwork in primary health care when they provide bonus systems to
GPs as independent contractors, despite the whole team contributing to the final
outcome.
Clear team objectives and performance feedback
In healthcare environments, team members need information about local health
needs and services, and national policies and guidelines, in order to set objectives
and target their activities appropriately. Further, feedback on team performance is
important for setting realistic goals and fostering high team commitment (Lathom,
Erez & Locke, 1988). Job satisfaction requires accurate feedback from both the task
and other team members (Drory & Shamir, 1988). However, team feedback can be
difficult to provide to teams with either long cycles of work or one-off projects
(Sundstrom et. al., 1990).
Training and technical assistance
Hackman (1990) argued that training and technical assistance is required for teams
to function successfully. Knowledge and training about team functioning is needed to
supplement team members’ own technical and medical skills and knowledge
(Poulton & West, 1993; Poulton & West, 1994a, 1994b; Poulton & West, 1997).
Limited empirical evidence suggests training is correlated with both self-reported
effectiveness (Gladstein, 1984) and managers’ judgements of effectiveness
(Campion et. al., 1993) in teams.
Physical Work Conditions
Physical conditions are another situational constraint that affect the relationship
between performance dimensions and team effectiveness. For example, a health

care team whose members are dispersed across sites, will find decision making
more difficult and ineffective than a team whose members share the same physical
location.
Organisational Climate
The climate of the organisation - how it is perceived and experienced by those who
work within it - will also influence the effectiveness of teams (Allen, 1996). Where the
climate is one characterised by high control, low autonomy for employees, lack of
concern for employee welfare and limited commitment to training, it is unlikely
teamworking will thrive (Markiewicz & West, 1997).
The extra commitment and effort demanded in team-based organisations requires
organisational commitment to the skill development, well-being and support of
employees (Mohrman, Cohen & Mohrman, 1995). Competition and intrigue can
further undermine team based working in health care, since teamwork depends on
shared objectives, participative safety, constructive controversy and support (West,
1990; West & Anderson, 1996). Ross, Rink and Furne (2000) reported that team
members’ willingness to work in teams was limited by the lack of a common set of
values about the benefits of teamwork. They recommended the need for clear
objectives, leadership, commitment and wide organisational ownership as precursors
for working in teams.
Professional subcultures also influence team effectiveness. Kinnunen (1990) used
an anthropological approach to distinguish different subcultures between medical,
nursing and management staff in a large primary health care organisation in Finland.
These three professional groups described different relationships to formal power
structures, which influenced their group behaviour, leadership style, administrative
orientation, decision-making preferences and patient interactions. In general, doctors
and managers shared basic assumptions about work that were paternalistic,
proactive, dominant and emphasised loyalty to authorities. In contrast, nurses
stressed participation, delegation, traditions and symbiotic harmony in work relations.
Inter-team relationships
In a comprehensive study of team-based organisations involving both questionnaire
and case study methods, Mohrman et. al. (1995) demonstrated that inter-team
competition is a major threat for team-based working. Teams that compete may
develop greater commitment to the team’s success than the organisation’s success.

Thus the health care team may focus on increasing the financial benefits to their
team at the expense of the wider National Health Service. Teams competing against,
rather than supporting each other may withhold vital information or fail to offer
valuable support in the process of trying to achieve team goals, without reference to
the wider goals of the organisation. Thus, health care teams may fail to pass on
information about former patients to other teams, focusing their efforts on their own
team’s immediate demands.
Ross, Rink and Furne (2000) reported a lack of focus on patient care in their
evaluation of primary care nursing teams in England. Nurses perceived that current
organisational change promoting teamwork was concerned with structure,
professional and organisational issues rather than with patient care. Some nurses
were concerned that moves towards integrated nursing were primarily motivated to
cut costs.
Contracts and Management Structures
Other relevant aspects of the organisational environment in health include the
independent contractor status of GPs and different management structures. There
are very few organisations where one or more senior team members work as
independent contractors and the rest of the team work within a variety of
organisations. Even the most sophisticated management practices, in environments
such as the oil and gas industry, are struggling with notions of how to operate joint
venture systems - whereas health care teams must deal with these issues constantly
but without the training and support given to teams in these other sectors.
Team size
The size of the team is also important, since bigger teams experience much greater
strains on effective communication. In most other sectors, teams tend to be divided
once they reach 12 or 13 members. But primary and secondary health care teams
(for example) can be 20, 30, 40 or more members in size. These ‘teams’ would be
more correctly termed ‘organisations’. In and of itself, this would not be a problem, if
those who run such organisations are adequately trained to manage large
operations. They require knowledge of the management of culture, power, conflict,
spans of control, strategies, innovation and above all, people. Yet primary health
care team leaders are rarely given such training (West, 1994). It is to the topic of
leadership that we now turn.

Leadership
There is considerable research evidence that leaders affect team performance (e.g.
Brewer, Wilson & Beck 1994; Komaki, Desselles & Bowman, 1989) and evidence of
the relationship between leadership style and team effectiveness. Eden (1990)
examined the effects of platoon leaders’ expectations on team performance. His work
with the Israeli Defence Forces showed that those platoons which trained under
leaders with high expectations, performed better on physical and cognitive tests.
Podsakoff and Todor (1985) investigated the relationship between team members’
perceptions of leader reward and punishment behaviours and team cohesiveness,
drive and productivity. Results showed that both leader contingent reward and
punishment were positively related to team drive and productivity. Leader contingent
reward was also related to cohesiveness, while leader noncontingent punishment
behaviour was negatively related to team drive. Jacob and Singell (1993) examined
the effects of managers on the won-lost record of professional baseball teams over
two decades and found that leaders did influence team performance by exercising
tactical skills and improving the performance of team members. George and
Bettenhausen (1990) studied teams of sales associates reporting to a store manager
and found that the favourability of leader’s moods was negatively related to related to
employee turnover.
Primary health care team members in England rated their effectiveness more highly
when they had strong leadership and high involvement of all team members (Ross,
Rink & Furne, 2000). In nursing care teams, Dreachslin, Hunt and Sprainer (2000)
concluded that leadership mitigated the influence of race in self-perceived
communication effectiveness. Participants’ comments supported the theme that
team leaders who encouraged discussion about differences enhanced perceived
team effectiveness. They suggested that leaders provided a unifying force through
validating the alternative realities and appreciating the different perspectives of team
members, thus moderating the potentially negative effects of racial diversity on team
processes.
Developing Teams in Organisations
To what extent is it possible to develop team working to ensure higher levels of
effectiveness? Tannenbaum, Salas, & Cannon-Bowers (1996) have reviewed
research in this area and related results to a comprehensive model of team which

integrates interventions (Tannenbaum, Beard and Salas, 1992). They describe a
number of intervention types include team member selection and teambuilding:
Team member selection
Although organisations tend to use quite sophisticated methods for
selecting employees for individual jobs, they rarely use systematic
methods for selecting for teams. But systematic selection methods can
help identify people with greater skill levels. There is strong evidence
that a team composed of skilled and motivated people will be more
effective than other teams (Tziner, 1988). Selection interventions could
improve team effectiveness by increasing the professional or skill
diversity of health care team members, thereby increasing the range of
competencies in the team.
Teambuilding
Some teambuilding interventions focus on role clarification, some on
interpersonal relationships or conflict resolution issues, while others take
more of a general problem-solving approach (Tannenbaum, Salas &
Cannon-Bowers, 1996). Team norms, attitudes, climate and power
distribution can be affected by teambuilding approaches. Many team
processes, including communication, decision-making and mutual role
understanding, are often direct targets of team building interventions.
Weldon and Weingart (1993) describe the importance of planning in teams for
achieving team goals, and suggest that team members are characteristically slow to
respond to changes in their tasks or their environments that make their strategies
ineffective or their goals obsolete. They propose five ways of supporting team work.
Goals should be set for all dimensions of performance that contribute to the overall
effectiveness of the team; feedback should be provided on the team's progress
towards its goal; the physical environment of the team should remove barriers to
effective interaction (consider the difficulties faced by members of a dispersed health
care team); team members should be encouraged to plan carefully how their
contributions can be identified and co-ordinated to achieve the team goal; and team
members should be helped to manage failure, which can damage the subsequent
effectiveness of the team.

Pritchard, Jones, Roth, Stuebing and Ekeberg (1988) tested some of these ideas by
measuring the effects of team feedback, goal setting and incentives on productivity.
Five organisational units in the military were studied. One, a maintenance section,
repaired a variety of electronic equipment used for aircraft communications. The
other four sections together made up a material storage and distribution branch.
Productivity baselines were established before each team received new "treatments"
(i.e., performance feedback eight months after the study began, goal setting five
months later, and incentives a further five months later) to determine the incremental
effects of these "treatments". First, the level of performance of the teams was
measured over a period of eight months and then information on their performance
was given to each unit for five months. The teams next set clear targets in addition to
the performance feedback, and their performance was measured for another five
months. Feedback was in the form of computer-generated reports, given monthly to
the personnel of each unit. Finally, incentives were offered for high performance, in
the form of time off from work. Using these approaches, the average increase over
baseline productivity was 50% for feedback, 75% for goal setting and 76% for
incentives. The results showed a major increase in productivity among the teams,
though the unique contribution of each component of the intervention is difficult to
estimate accurately. Both goal setting and feedback had powerful effects on
performance.
Transition of organisations to teamworking
One of the most exciting developments in the field is the new emphasis upon the
development of team-based working in organisations (Mohrman, et. al., 1995;
Markiewicz & West, 1996, 2001). This reflects a concern amongst practitioners with
how team-based working can be effectively introduced into organisations. Mohrman
et. al., studied 25 teams in four companies using a grounded research methodology,
involving managers and internal customers. In the second phase of their research
they surveyed 178 teams across seven corporations, involving team members,
managers and customers. In this way, they developed a five stage design sequence
for the transition to a team-based organisation:
1. Identifying work teams and the nature of the task
This involves process analysis to determine essential work activities that have to be
conducted and integrated to produce products or services; deliberations analysis
which identifies dialogues about issues that have to be repeatedly resolved in order

to provide shared direction and enable people to complete their tasks; and task
interdependence analysis which determines where and to what extent individuals and
teams have to rely on each other to complete their tasks.
2. Specifying integration needs
In order to integrate across multiple teams and components of business units,
Mohrman et al recommend management teams, representative integrating teams
(where an overall co-ordinating team had representatives from each of those teams
collectively involved in producing a product or service), individual integrating roles,
and improvement teams.
3. Clarifying management structure and roles
This stage involves putting as much self-management responsibility into the teams
as possible; involving team members in determining how leadership tasks will be
performed and by whom; using lateral mechanisms for cross-team and organisation-
wide integration so that teams participate in that integration; and creating
management roles which link teams to the organisational strategy and ensure they
are responsive to the organisational and wider environmental context.
4. Designing integration processes
The research evidence suggests that team-based organisations should set clear
directions in the organisation, (for example by defining, communicating and
operationalising a strategy at all levels, aligning goals, assigning rewards in
accordance with organisational goals, and planning collectively); managing
information distribution and communication; and developing an appropriate decision
making strategy (by clarifying decision making authority, and appropriately involving
organisational contributors).
5. Developing performance management processes
Finally, the model suggests the need to manage performance - defining, rewarding
and reviewing performance and involving internal and external customers, and team
members. Mohrman et. al., report that the more people were rewarded for individual
performance, the worse team performance was. The more people were rewarded for
team performance, the better was the team and the business unit’s performance and
the more process improvements the team and the business unit instituted.

Conclusions and Research Mode
A review of the literature reveals that progress has been made in understanding the
factors that influence the ability of people to work effectively together in teams.
However, in the health care domain progress is still patchy and only a few studies are
constructed on firm theoretical bases. Progress is further inhibited by the added
difficulty of operationalising the concept of effectiveness. In the research described
in this report we attempted to build our research on a well-accepted theoretical base
and to engage a large number of health care teams in the research endeavour.
Moreover, we were charged with grasping the nettle of effectiveness in health care
and developing robust and sufficiently broad measures of this difficult concept.
Finally, the research team, drawn from a wide range of epistemological backgrounds
and theoretical orientations, determined to employ diverse, powerful and innovative
research methods to answer the question of what factors influence the effectiveness
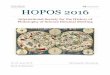
of health care teams. The starting point for the research was a model of the factors
influencing team effectiveness and which distinguishes between at least three major
domains of effectiveness. Theoretical approaches to understanding teams at work
have been dominated by the input-process-output structure, mainly because of its
categorical simplicity and utility (see Figure 1 below) (West, Borrill, & Unsworth,
1998). This is the model used to guide the research described in this report.
Figure 1: Input, process, output model of team effectiveness
INPUTS GROUP PROCESSES OUTPUTS
Domain
Health CareEnvironment
Organisationalcontext
Team task
Team composition
Leadership
Clarity of objectives
Participation
Task orientation
Support for innovation
Reflexivity
Decision making
Communication/integration
Effectiveness - self andexternally rated
Clinicaloutcomes/quality ofhealth care
Innovation - self andexternally rated
Cost effectiveness
Team member mentalhealth
Team member turnover

Inputs
Teams work within a domain such as primary care, secondary care or community
mental health. They also work in a health care environment that may be more or less
deprived. The team works for and within an organisation; thus it will be affected by
the interaction with the surrounding organisational context. A team has a task that
potentially impacts upon team processes and effectiveness (the management of
immunisation for children under five years; intensive care nursing; or care of the
elderly with mental health problems). The team consists of a collection of individuals
- who represent the group’s composition – varying in professional background,
gender, age, personality etc. Finally, the team exists within a wider society that will
affect the teams’ fundamental beliefs and value systems, i.e., the cultural context.
Processes
Processes within teams enable them to achieve their goals. A fundamental
requirement for effectiveness is that teams have clear objectives to which their
members are committed. Other processes include participation in decision-making,
emphases on quality, and support for innovation. Another fundamental process is
the extent of coordination and integration of team members’ work (Worchel, Wood, &
Simpson, 1992). And of course, leadership and communication are likely to be
important to team effectiveness. Another potentially important process variable is
reflexivity or the extent to which team members collectively reflect on the objectives,
strategies, processes and environment of the team and make changes appropriately
and accordingly.
Outputs
Six principle outputs can be distinguished: overall effectiveness, clinical outcomes,
team
member mental health, innovation, team member turnover, and cost effectiveness.
In the research programme described in this report we explore the relationships
between inputs and processes; inputs and outputs; and processes and outputs in
390 UK NHS teams, during the course of which we consulted with over 7,000 NHS
personnel and with a large number of NHS clients.

Using this model, we determined to explore the extent to which team working was
associated with better quality health care for patients and to identify the factors
associated with effective teamwork.

Chapter 2
Primary Health Care TeamResearch Methods and Sample Details
The research with Primary Health Care Teams had two stages. The first was a
questionnaire survey, and related data collection methods, involving large numbers
of teams conducted in order to gather data on team inputs, processes and outcomes.
The second stage involved intensive examination of a sub-set of teams to explore in
more depth targeted team processes and outputs.
Quantitative Methods
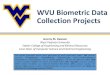
An overview of the methods used is given in Figure 2.1.
Figure 2.1: Details of the three samples and research methods
Sample size Survey data Additionalquestionnaires/Telephoneinterviews
External ratings
100 teams1156 respondents
Team compositionTeam functioningTeam effectivenessTeam innovationMember stress
Team composition
Team meetingsTeam managementDecision making
Team effectivenessTeam innovation
The Sample
The research design required data to be gathered from 100 Primary Health Care
teams (PHCTs) varying across a number of dimensions, including size (number of
team members, number of GPs, list size); Jarman index; location (urban, rural, inner
city), and geographical location. Databases of GP practices were accessed from 19
Health Authorities and 300 teams were randomly selected.
Letters explaining the objectives of the research and inviting teams to participate in
the research, together with an information sheet were sent to the senior GP partner,

senior health visitor and practice manager/senior receptionist in each practice. A
reply slip was included, which also solicited additional information about the team
(fund holding status, frequency and type of meetings, Jarman index, number of GPs,
list size etc.)3
The initial letter was followed up with a telephone call to the practice manager/senior
receptionist at all 300 practices. If teams had already indicated a willingness to
participate, practical arrangements for questionnaire distribution were made.
Researchers requested the name of a contact person in the team to enable
continued effective liaison. The contact person was telephoned at a later date to
determine whether the team was willing to take part in the research. Teams that did
not return a reply slip were also telephoned and provided with additional information.
Further follow-up telephone calls were made until the team made a decision about
participation in the research (some PHCTs were contacted six or seven times before
a decision was made). When teams agreed to collaborate in the research,
questionnaires were sent to the contact person for distribution to team members.
After three months the response rate from 10 teams was below 30% and 23 had not
returned any questionnaires. These teams were dropped from the sample and
replaced with 7 teams based in an inner city area, and 7 from a rural location,
resulting in a final sample of 100 teams. The total response rate was 55.8%.
Response rates for teams ranged from 21.4% to 100%, with a mean of 57.6%.
Data Collection Methods
Data on team functioning and effectiveness were collected using three methods: self
report questionnaires completed by individual team members; self report and
telephone interview surveys with the team contacts; and external ratings from
primary health care representatives and health authority staff.
1156 respondents from 100 PHCTs completed questionnaires on their perceptions of
team functioning and team effectiveness. Of these, 85% were female; 15% were
GPs; 14.2 % practice nurses; 23% trust nurses (health visitors, district nurses,
3 Copies of interview schedules, questionnaires and all data collection instruments areavailable from the first author of this report.

midwives); 33.5% administrative staff, 7.3% managers and 4.3% professions allied to
medicine (PAMs).
Team contacts from 77 PHCTs provided information on team context, team
composition and team processes in a self-report questionnaire survey, and 100
provided information via a telephone interview. This enabled a reliability check on the
data for 77 of the teams.
Questionnaires completed by individual team members
This questionnaire was in four sections (a copy of the primary health care
questionnaire is included in Appendix I).
Section 1: Team working
This contained seven measures of team working. Four of these were drawn from the
Team Climate Inventory (Anderson & West, 1994,1998) that is based on a well-
developed theoretical model of team functioning (West, 1990). The four measures
assess levels of:
• team participation
• clarity of and commitment to team objectives
• emphasis on quality
• support for innovation.
Three other measures were included:
• reflexivity – the extent to which team members reflect upon their team
objectives, strategies and processes and make changes accordingly (West,
1996; Swift & West, 1998).
• team innovation – the extent to which the team has introduced innovations in
objectives, work strategies, processes and relationships
Respondents were also asked to write descriptions of the major changes or
innovations introduced by the team in their work in the previous 12 months.
Section 2: Effectiveness
This included 21 measures of primary health care team effectiveness adapted from
Poulton and West (1999). There are three underlying dimensions:

• team working
• patient orientation
• organisational efficiency
Section 3: Team member stress
This included a measure of psychological stress, the GHQ-12 (Goldberg, 1972;
Goldberg & Williams, 1991). The GHQ-12 is widely used as a screening tool for
detecting minor psychiatric disorder in the general population, and in occupational
mental health research. It covers feelings of strain, depression, inability to cope,
anxiety based on insomnia, lack of confidence and other psychological problems.
Within a Department of Health-funded study of the mental health of the NHS
workforce, the GHQ-12 showed good validity against a psychiatric interview (Hardy,
Shapiro, Haynes, & Rick, 1999).
Section 4: Biographical information
This section included questions on biographical and team characteristics (e.g. age,
gender, ethnic origin, job title, employer, team composition, team leader).
Additional Practice Information – Survey
This was completed by the contact person in the PHCT (usually the practice
manager). It included questions on: team context (relationships with external
agencies such as health authorities and trusts); type of primary health care practice
(fundholding, non-fundholding, dispensing) quality of premises; team composition
number in each occupational group, grade, hours worked, time working in the team);
staff development; and team processes (communication and decision making in
meetings).
Additional Practice Information - Telephone Interview Schedule
The contact person in the team (usually the practice manager) responded to the
telephone interviews. The focus of the questions was on decision-making and
communication in the team: specifically who was involved in making operational,
strategic and clinical decisions in the team, how these decisions were communicated
in the team and what mechanisms were in place within the team to promote
communication (memo systems, message books, informal meetings, email).
Information was also gathered on the services and clinics provided by the team.

External ratings – team effectiveness and innovation
Health Authorities employ staff to provide support to primary health care teams, a
role involving working closely with a wide range of teams. Contact was made with
staff in this role at each of the Health Authorities where the teams in the sample were
located. They were asked to provide ratings of effectiveness and innovation for all of
the teams from their area that were participating in the research. External ratings of
effectiveness were obtained for 84 teams. They were rated on the same 21
effectiveness dimensions included in the primary health care team questionnaire.
Examples of the dimensions include:
Ø The extent to which teams made efficient use of the practice budget
Ø The extent to which teams previewed and adjusted skills in line with
the identified health care needs of the practice population
External ratings – changes introduced by teams
Three representatives from Primary Care rated the changes or innovations
introduced by the teams (reported in the questionnaire for individual team members).
One of the raters was employed by a Local Health Authority and had responsibility
for developing team working in primary care. Another was employed by a community
trust, also in a role which supported primary care teams. The third rater was a part
time general practitioner who had been involved in development and research
projects in primary care. They rated teams on four dimensions (West & Anderson,
1996):
• magnitude - how great would be the consequences of changes introduced
• radicalness - to what extent the status quo would change as a consequence
• novelty - how new in general were the changes
• impact - to what extent changes would improve PHCT effectiveness.
Using the ICC (2) (Shrief & Fleiss, 1979) the inter rater agreement was calculated for
each dimension: Magnitude - 0.663, Radicalness - 0.630, Novelty - 0.539, Impact -
0.779.
Sample Details
In this section we describe characteristics of the primary health care team sample
that participated in the questionnaire and interview component of the research

programme. Following the model used to guide this research (see page 1) we
describe four categories of inputs:
• team task - Indicated by the size of the practice population and its
fundholding status
• team composition - team size, ratio of part-time team members, gender mix,
number of occupational groups represented in the team
• health care environment - the Jarman Index (an index of social deprivation),
its location (city, urban, urban/rural or rural)
• organisational context - the NHS Region within which the team is located.
We also describe the relationships between these four domains of inputs. The
reader will also find an account of the frequency and content of meetings held in the
teams, and of the team members’ perceptions of leadership in the team in
subsequent chapters.
Team Task
Practice population or ‘list’ size
The practice population or ‘list’ size ranged from 1500 to 21,850. The mean size was
6,902 patients with a standard deviation of 4,692 (see Figure 2.2).
Figure 2.2: Percentages of primary health care teams with patient populations or ‘listsizes’ of various sizes
Fundholding status
Forty one percent of teams in the sample had fundholding status.
0 %
5 %
1 0 %
1 5 %
2 0 %
2 5 %
3 0 %
<25
00
2501
-
5000
5001
-
7500
7501
-
1000
0
1000
1-
1500
0
1500
1-
2000
0
>20
000
List Size
List Size


Location
Four location categories were used: city, urban, urban/rural and rural. Sixty-five
percent of teams were located in urban areas other than cities, 20% in cities, 6% in
areas described as both urban and rural, and the remaining 8% were in rural
locations.
Health care environment
Jarman index
The Jarman index is a measure of social deprivation. The higher the score the
greater the health needs of the practice populations served by the team.
Scores in the sample included in this research programme ranged from 0% to
100. The mean Jarman score was 15.52 and the standard deviation 22.72.
Figure 2.3 shows the percentage of teams with each category of Jarman
score.
Figure 2.3: Team Location
Figure 2.4: Jarman index
0
5
10
15
20
25
0%0%
1 - 10%
1 - 10%
Frequency
0%
10%
20%
30%
40%
50%
60%
70%
City Urban Urban/Rural Rural

Whole time equivalents
Using hours worked to calculate team size enabled an estimate to be made of the
number of ‘whole time equivalents’. This statistic shows that team size varied from
1.49 to 31.9 members. The mean size was 9.35 with a standard deviation of 6.75.
The size of teams working in so-called ‘single handed GP practices’, ranged from
1.88 to 16.13, with a mean of 7.48 and a standard deviation of 3.74.
Number of GPs
The number of GPs in the teams ranged from 1 to 11. The mean number of GPs
was 3.7 and the standard deviation was 2.4 (Figure 2.5).
Whole time equivalent GPs
The range of whole time equivalent GPs was from one toten. The mean was 3.16 and the standard deviation 2.0.
Figure 2.5: Number of GPs in the primary health care teams
Gender
The majority of team members (85.5%) of the Primary Health Care team sample
were female. The break down for gender by occupational group is shown in Figure
2.7 and this reveals that the only imbalance in favour of men is in the highest status
group – GPs. Otherwise, primary health care is a domain in which women form the
vast majority of the workforce. Primary health care is largely in the hands of women
in the UK. And of course, this has important implications for our understanding of its
0 %
5 %
10%
15%
20%
25%
30%
1 2 3 4 to 5 6 to 8 9 to11
Team Size (no of GP's)

functioning, issues of team processes and, given the anomalous preponderance of
male GPs, of leadership issues.
Fig 2.7: Distribution of gender by occupational group in primary health care teams
GPs Practice
Nurses
Trust
Nurses
Admin
staff
Managers PAMs Other
Male 99 5 16 10 24 8 1
Female 75 160 249 378 61 42 4
Fig 2.8: The distribution of mean age across the occupational groups
Mean Age Standard Deviation
GPs 41.2 7.6
Practice Nurses 42.1 7.6
Trust Nurses 42.2 8.3
Admin/clerical 43.7 10.2
Managers 44.3 8.4
PAMs 41.6 11.0
Others 40.8 8.2
Age
The distribution of age across the occupational group is shown in Figure 2.8.
Occupational Groups
The majority of teams comprised: GPs, practice nurses,administrative staff, district, health visitors and one ormore practice managers. Less than 15% of teams did notinclude trust nurses, and only 6% of teams had nomanager. Twenty four percent of teams included ‘other’types of staff (counsellors, community psychiatricnurses, physiotherapist etc).
Proportion of occupational groups
The proportion of each of the main occupational groups in the teams is shown in
Figure 2.9.

Figure 2.9: Proportion of occupational groups in the sample
A different picture of team composition emerges when hours worked is taken into
account and team membership calculated using 'whole time equivalent' figures. This
shows that largest grouping is GPs, with only 10.7% of the input to the team being
provided by trust nurses.
2.10: Proportion of occupational groups in the sample
GPs
Practice Nurses
Trust Nurses
Admin/clerical
ManagersPAM's Others
GPs
Practice NursesTrust
Nurses
Managers
Admin/clerical
PAM's Others

Organisational Context
Figure 2.11 Regional variations
Location Number of teams
South East and London 18
Midlands 4
East Anglia 4
Nottinghamshire 18
South Yorkshire 43
West Yorkshire 13
Teams were distributed across six regions with thedistribution shown in Figure 2.11.
Relationships between Input Factors
In this section we describe the relationships between aspects of team task, team
composition, health care environment and organisational context. As we might
predict, there are some important and significant relationships between them.
• The number of team members and the number ofpatients on the team’s list were positively correlated(0.85), with an average of 291 patients on a team’slist per member of staff. This ratio did not varyacross location (city, urban, urban/rural, rural),Jarman index, or average of number of hoursworked by team members.
• There were no significant differences in the composition of the teams
between different types of locations (city, urban, urban/rural, rural). Nor were
there differences in the composition of fundholding and non-fundholding
practices.

• There was a significant relationship between Jarman score and number of
managers; teams with fewer managers had a higher Jarman score.
• Teams with a higher Jarman index also had significantly more ‘other’ types of
staff in the team. This may reflect the fact that the range of services required
is much greater in socially deprived than socially enriched areas.
• There was a higher proportion of Professions Allied to Medicine (PAMs) in
teams with a larger list size.
Jarman index / location
73 teams provided a Jarman index score of more than 0%. The mean score was
15.52 and the standard deviation 22.72. These were distributed across locations as
follows:
City – 18
Urban – 39
Urban / rural - 5
Rural – 6
Unclassified - 5
• The Jarman index for city practices was significantly higher (mean = 32.6%)
than for urban practices (mean = 11.9%)4
Qualitative Research Methods
Research in the second stage of the research programme explored in depth, and
using a variety of consultation and qualitative research methods, all issues of team
functioning and effectiveness. The methods used are shown in Fig 2.12.
4 The data collected as part of this research can be subjected to much further analysis andinformation extraction. The researchers are committed to working with others to ensure themaximum exploitation of this hard won data set. If there are analyses readers wish to conductthe researchers would urge them to contact the first author of this report.

Figure 2.12: Consultation and Qualitative Research Methods used for Primary HealthCare Teams
Analysing PHCteam processes
Development of PHCobjectives
Development of PHCeffectiveness measures
§ Audio and videorecording of twomeetings for eachof twelve teams
§ Series of four nationalworkshops withdomain relevantexperts from primarycare.
§ Work with 12 teams tovalidate objectives.
§ In-depth work with two PHCTsto develop measures.
§ Training and dissemination toten PHCTs.
§ Training team facilitators.
Video and audio recordings of team processes
All teams involved in the questionnaire and interview components of the research
programme were invited to participate in the next stage of the research. This involved
analysis via video and audio recording of two of their team meetings. Teams were
selected randomly for this element of the research. Twelve teams volunteered.
We selected meetings that were multidisciplinary in composition and that involved
decision-making (as opposed to information dissemination only). This is because
understanding team working in this context demands that we observe professionals
from different backgrounds working together dynamically, and integrating their
different perspectives to initiate action and change. Multi-disciplinary meetings were
those in which a range of disciplines (doctors, nurses, health visitors, practice
managers, etc.) was represented and participated. For the most part, primary health
care teams allowed us to observe the practice business meetings, in which the day-
to-day running of the practice was discussed. In one team, the GP partners made all
decisions affecting the practice. In this case we recorded the partners’ meeting.
Wherever possible, we recorded two meetings of the same type for each team.
Dates for meeting recordings were at the discretion of the practice, so the two
meetings recorded were not always in sequence. Researchers requested that
recorded meetings should be held in their usual locations, with their usual meeting
protocols (agendas, minutes, chairing procedures, etc.), and that attendance should
be the same as if the meeting was not being recorded. The researcher who managed
the recording equipment made herself as unobtrusive as possible. Meeting size
ranged from three people to twenty-five.

Audio recording was done with two omni-directional PZM tabletop microphones
linked to different channels of a high quality audiotape recorder; the microphones
were set up so as to maximise channel differentiation but to be unobtrusive enough
that participants would not move them. A single static video camera on a tripod was
trained to record the gross movements of as many of the participants as possible;
this record was used only to aid speaker identification during transcription. Before
each meeting was opened all participants introduced themselves and their
occupation and upon the basis of this each was allocated a speaker number.
Therefore the first person to introduce him or herself became speaker 1, the second
speaker 2 and so on.
Meetings were transcribed from the audiotapes by an audio typist who had not
attended the meeting. Audio typists transcribed complete contributions in order,
according to when they began, labelling each contribution by speaker number, but
did not code finer timing information. Speaker identification was facilitated both by
the video recording and by a seating plan drawn up during the meeting by the person
recording the meeting. A contribution was defined as a period of speech from one
individual in which the only major pauses coincided with silence from the other
speakers, so that the pause was likely to be caused by the speaker thinking and not
by the speaker listening to someone else's contribution. Under this definition,
speakers cannot follow themselves in the speaking order. Overlapped speech was
transcribed, with the extent of the overlap roughly marked. Infrequently, parts of the
meetings were omitted because they were so badly overlapped that we could not
track individual contributions. After transcription, the transcripts were completely
anonymised taking out all staff, patient, place names, place and local authority
names or possible team or person identifiers.
An example transcription excerpt is given in Figure 2.13. Transcription proceeds one
contribution per row. Column one contains the speaker number. Column two
contains the words said, with coding information in a different font, and column three
contains any notes which the transcriber wished to make (for instance, about people
entering or leaving the room).5
5 In previous work using these methods on four to twelve person meetings, transcribers wereable to agree very reliably who made any one contribution; using the kappa statistic, K=.93, k= 2, N = 230, with an average of 2% and a maximum of 6% non-backchannel contributionsleft as unidentified.

Figure 2.13: An example of the layout of the transcription format used for PHCTmeeting transcription
1 Shall I open /4 the meeting
4 Yep, let’s get on with it.
3 My apologies I am going to have to leave beforethe end. I have an appointment in Place 1.
1 Are you skiving off?
Group laughter
Because one of the factors of interest in our study is how well teams communicate
across disciplines, our analysis relies on a classification of meeting participants by
occupation. For ease of reference, categories are identified by colour as well as
number. For primary health care teams, Figure 2.14. shows the categories used.
Figure 2.14: Categories used for PHCT meeting participants
1 GPs
2 practice managers
3 practice nursing staff, including nurse practitioners
4 attached staff (mostly health visitors, midwives and district nurses)
administrative staff (mostly secretaries and receptionists)
6 miscellaneous (visitors, resident caretakers, medical students)
Development of Performance Measures for PHCTs
In the broader organisational literatures on team effectiveness, a widely adopted
approach is the Productivity Measurement and Enhancement System (ProMES)
based on research by Naylor, Pritchard & Ilgen (1980) (see also Pritchard, 1995).
Effectiveness criteria are established in group discussions with team members and
managers. The variables are then “psychologically scaled” to a common
effectiveness scale. Based on group consensus about expected levels of
effectiveness, which are given a zero value, maximum effectiveness levels (set at
+100), and minimum levels (-100) are set. Each variable is also weighted in terms of

its perceived contribution to the overall effectiveness of the team or organisation.
The system is then used to set objectives, develop indicators, monitor and improve
performance and give feedback to the team (Pritchard, 1995). The approach has
been spectacularly successful in many settings (Pritchard, 1995) and is promising for
primary health care, because of the sophistication of the approach, its theoretical
robustness and practical utility in complex contexts.
The ProMES was implemented in three main stages:
1. Core objectives for primary health care teams were developed using the
constituency approach and ProMES in four national workshops with
representatives from Primary Care.
2. Usable ProMES effectiveness measures were developed and applied within
primary health care teams.
3. Primary health care team members and trust representatives were trained to
develop and implement effectiveness measures using ProMES in primary
health care teams.
An initial ‘stakeholder analysis’ identified 13 stakeholders in primary health care.
These included:
Ø GPs
Ø Health Visitors
Ø District Nurses
Ø Practice Nurses
Ø Midwives
Ø Administrative staff
Ø Department of Health
Ø NHS Executives
Ø Patients
Ø Health Authority
Ø Researchers
Ø PAMs
Ø CPN
Advice was sought from contacts in primary health care about key experts who could
represent the views of each stakeholder group, and about whether the initial list of

stakeholders was sufficiently comprehensive. The experts suggested by the contacts
were sent information about the research programme, invited to attend the four one-
day workshops, and asked to suggest additional or alternative key experts who could
also make a contribution. In addition, professionals who were currently engaged in
clinical practice in primary health care teams were invited. The majority of those
contacted were able to commit themselves to attending two or three of the
workshops. A full list of those attending and their institutional affiliations is given in
Appendix II.
During the workshops focus group methods were used. Delegates were divided into
three working groups. These were designed so that (a) a range of stakeholder views
was represented, and (b) one or two or group members had attended most or all of
the workshops and so could share with new members the learning and experience
from previous workshops. Each group worked with a trained facilitator, and a note
taker recorded the group discussion and the decisions made.
Workshop 1
Objective: to develop objectives for primary health care.
The delegates were presented with a set of objectives for primary health care
developed by the researchers (based on the work of Poulton & West, 1994) and then
worked together to discard, add or refine objectives. The revised objectives were
discussed with members of four primary health care teams (who endorsed their
relevance and value), and combined into a single list.
Workshops 2 and 3
Objective: to develop measures of effectiveness in relation to the primary health care.
Delegates were presented with the refined and agreed objectives for primary health
care. Each group worked on developing effectiveness measures for objectives.
Workshop 4
Objective: to plan the implementation of effectiveness measures in primary healthcare.

In the fourth Workshop, participants critically appraised the objectives and measures
developed, and considered how they could be applied in practice by PHC teams and
others. This session was used to plan the implementation and evaluation of the
effectiveness measures in practising teams. Seven core objectives, with associated
sub-objectives, were identified and agreed by the professionals attending the
workshops and 19 effectiveness measures were developed (see Appendix II).
Work implementing performance measures was carried out in two phases. In the
first phase, we carried out in-depth work with two primary health care teams to
develop performance measures, based on the objectives and measures developed in
the four national workshops, and used these to provide feedback on team
performance. Details of this work are provided in Appendix III. We worked with one
team over a period of 15 months, and with the second for a period of 8 months. A
design team was established in each PHCT that included at least one representative
from each of the occupational groups in the team. In one-hour workshops held every
fortnight, ProMES was used to develop performance measures specific and
appropriate to each team. Teams carried out further development work between
meetings such as gathering data and consulting colleagues.
In the second phase, PHCT representatives and trust employees attended a
‘ProMES in Primary Health Care’ training programme. etters inviting representatives
from PHCTs to attend the ProMES training were sent to 60 PHCTs that had
participated in the first stage of the research (all teams with a response rate of 50%
and above). Letters were sent to the practice manager, senior health visitor and
senior partner. Follow-up phone calls were made to the teams, but representatives
from only two attended the training. The other participants were service
representatives, employed by community trusts, to support and develop primary care
team working.
The training programme included an overview of the ProMES approach; the
development of performance measures; guidance on running ProMES workshops in
PHCTs; training in how to collect and use performance information. The programme
for the training is outlined in Appendix IV. After the training, three follow-up
workshops were held with participants. The purpose of these was to provide support
to those using ProMES with primary health care teams, and to critically review the
measures developed in the training. Feedback from the participants about the
success of their interventions in teams has been positive and suggests there is real

benefit to all aspects of primary health care team functioning from employing this
approach. At the same time, it is a demanding exercise that requires commitment by
team members to implement.
The results from stage 1 and 2 of the research programme are described in the
following two chapters. Details of the findings from the primary health care team
surveys and external ratings are outlined in Chapter 3, and the objectives and
effectiveness measures developed for primary care, outlines in Chapter 4.

.Chapter 3____________________________________________________________________________
Primary Health Care TeamResults from Survey and External Ratings
Summary of Findings
• Large PHC teams are rated as more effective and innovative by external raters.
• The greater the number of professional groups represented in the primary health
care teams, the more highly rated is the innovativeness of the team.
• The better the team processes and reflexivity, the more innovative they are rated
by external raters.
• The greater the number of team meetings, the higher the level of innovation in
primary health care teams.
• PHC teams with clear leaders have good team processes.
• Conflict over leadership leads to poor quality team working. However, teams
where leadership roles are shared are more innovative.

Introduction
The data analysis explored two main questions
• Is there an association between the composition of a primary health care teamand team processes?
• Is there an association between the composition and processes of the primaryhealth care team and the effectiveness of the team?
The team characteristics, team processes and measures ofteam effectiveness are summarised in Figure 3.1.
Figure 3.1: Team Inputs, Processes and Effectiveness Variables
Characteristics Processes Effectiveness
IndividualAgeGenderEthnicityGradeTime in jobTime in team
TeamOccupational groupsSize (number of members)Number of GP'sHours workedGrade MixTraining
Team contextList sizeLocation (urban, rural, city)Jarman indexFundholding statusDispensingPurchasingQuality of premisesExternal contactsRelationships with HA
Team processesParticipationInnovationObjectivesEmphasis on qualityReflexivityNumber meetingsTypes of meetingsFrequency of meetingsDecision makingLeadershipIntegration andcommunication in the group
Team ratingsOrganisationTeam workingPatient focusInnovation
External ratings (innovation)MagnitudeRadicalnessNoveltyImpact
External ratings (effectiveness)OrganisationTeam workingPatient focus
Types InnovationsQuality of careExternal collaborationResponsibility of healthUse of resourcesProfessional developmentTeam satisfactionResponsivenessStress (GHQ 12)
Team inputs
Information about the team members’ ages, gender, ethnicity, grade, professional
group, employer, tenure and team leadership was collected from each team member.

Information was also gathered on team size, hours worked, qualifications, training,
list size, practice location (urban/rural/city), Jarman index, fundholding status, and
whether the practice was purchasing and/or dispensing.
Team Processes
Individual team members rated team processes on six dimensions: participation;
support for innovation; clarity of team objectives; emphasis on quality; reflexivity; and
integration. The variables participation, support for innovation, clarity of team
objectives and emphasis on quality were very highly correlated and were combined
to form one variable describing team processes. Information about decision-making
processes, communication, number and types of meetings, who attended meetings,
and how the team was managed was collected from practice managers. The
information on team meetings was categorised according to who contributed to
operational, strategic and clinical decisions. In addition, a new variable
‘interdependence’ was developed which assessed the extent to which there were
mechanisms within the team to encourage interdisciplinary communication.
Team effectiveness
This was assessed using information from a variety of sources. Team members
rated their teams’ effectiveness on three dimensions: team working, organisational
efficiency and patient orientation. Team members also rated their teams’
innovativeness and described the innovations implemented by the team in the
previous year. These reports were categorised to determine the types of innovations
implemented. External raters assessed the innovations reported by the teams on
four dimensions: magnitude; radicalness; novelty and impact on team effectiveness.
External ratings of team effectiveness were provided by Health Authority
representatives on two dimensions – clinical and organisational. Individual team
members also completed the GHQ-12 (a measure of mental health or psychological
stress). The measures of interest for this report are overall effectiveness,
effectiveness of patient-centred care (both externally rated and self-rated), overall
innovation (both externally rated and self-rated), number of innovations to do with
healthcare, and mental health measured by GHQ-12.
Results
The main method of analysis was multiple regression. For each dependent variable,
possible predictors were split into groups according to type of variable (e.g.
occupational group, team context), and stepwise regression was used to identify

those which might ultimately predict the dependent variable. The second stage of
each analysis involved entering all those identified into a further stepwise regression,
to find out which variables had significant effects independent of other predictors.
This way, process variables were predicted by team characteristics, and
effectiveness, innovation and mental health were predicted by team characteristics
and team processes.
Since there was often evidence of relationships between size and other variables,
this was always dealt with first. Where relationships were apparent, later analysis
revealed whether this was due to team size per se or another feature of having a
larger team.
Question 1 – Is there an association between the composition of a primary
health care team and team processes?
There was no evidence that PHC team size had an association with any team
process except frequency of meetings. Here we see that teams of 20 or less have,
on average, 2.6 meetings a month; teams of 20-30 members have 6.1 meetings a
month, and teams of over 30 have 6.5 meetings a month.
Other predictors of team processes (after the second stage of analysis) are shown in
Figure 3.2.
Figure 3.2: Relationships between Team Composition and Team Processes
Dependent variable Predictor variables β p R2
Team processes Proportion of managers 0.305 0.010Proportion of “other” staff 0.253 0.032No. of GPs (WTE)1 -0.244 0.036 0.192
Reflexivity None
Integration Proportion of managers -0.256 0.035 0.065
Number of meetings No. of practice nurses 0.418 0.001 0.175
Consensus on leadership Proportion of “other” staff 0.366 0.002No. of managers -0.290 0.012 0.237
1WTE = whole time equivalents
Patterns emerging here are mainly to do with the representation of managers and
“other” staff types in the teams (anyone other than GPs, nurses, admin/clerical staff,

managers and PAMs). Having a larger proportion of “other” staff in the team has a
positive effect on team processes and consensus on leadership. A larger number of
managers also has a positive effect on team processes, but has the opposite effect
on integration. There is a negative association between a larger number of managers
and agreement about who leads the team.
Question 2 – What affects the effectiveness and innovation of a primary
health care team?
Team size was positively associated with a number of dimensions of effectiveness
and innovation, as shown in Figure 3.3. Generally, larger teams were rated as more
effective by external raters and introduced more innovations overall, and specifically
in relation to patient care.
Figure 3.3: Relationship between team size and ratings of effectiveness, innovationand mental health
Variable Correlation p
Overall effectiveness (external) 0.284 0.012
Overall effectiveness (self-rated) 0.086 0.401
Effectiveness of patient care (external) 0.255 0.002
Effectiveness of patient care (self-rated) 0.125 0.222
Innovation (external) 0.403 < 0.001
Innovation (self-rated) 0.123 0.226
Number of innovations re: patient care 0.255 0.013
Mental health 0.056 0.585
Further analysis revealed that the relationships between team size and all the
innovation variables was curvilinear, with teams of sizes around 40 being the most
innovative. Notice that there were no relationships between team size and self-rated
effectiveness, innovation or mental health.
It is also interesting to note the associations between team size and the individual
items of the external effectiveness ratings, to see what aspects of effectiveness are
most related to team size. These are shown in Figure 3.4. Larger teams appear to
be more responsive to patients and are more likely to conduct clinical audit.

Figure 3.4: Relationship between team size and individual externally ratedeffectiveness items
Effectiveness item Correlation p
Provision of information about services 0.131 0.236
Implementing procedures for dealing with patients’comments, suggestions and complaints
0.269 0.015
Maintaining clinical competence in line with patientneeds
0.186 0.083
Auditing clinical practice 0.263 0.017
Setting protocols 0.373 0.001
Commitment to professional and personal development 0.273 0.012
Understanding and valuing roles of all members 0.003 0.981
Implementing a clear strategy for communication 0.132 0.203
Profiling health needs and targeted interventions 0.160 0.165
Reviewing and adjusting skill mix 0.209 0.068
Collaborating with other agencies 0.094 0.389
Making effective use of budget 0.126 0.265
Implementing recommendations of the PHC Charter 0.311 0.004
Concentration on achievement of The Health of theNation targets
0.258 0.024
The main reasons for larger teams being more effective appear to be their
effectiveness in setting protocols and implementing recommendations of the PHC
charter.
Results of the stepwise regression analyses of effectiveness on team characteristics
and processes are shown in Figure 3.5.
Figure 3.5: Relationships between Team Composition and Processes, and
Ratings of Effectiveness
Dependent variable Predictor variables β P R2
Overall effectiveness No. of admin. staff 0.400 0.003(external) Proportion of GPs -0.279 0.035 0.199
Overall effectiveness (self-rated)
None
Effectiveness of patient care(external)
Team size 0.357 0.010 0.127
Effectiveness of patient care Team processes 0.632 <0.001 0.400

(self-rated)
The relationship between self-rated effectiveness of patient care and team processes
is not entirely surprising, given that both variables were constructed from the
individual questionnaires sent out and hence this analysis is prone to common
method variance. The relationship between team size and externally rated
effectiveness of patient care is shown in Figure 3.6. This relationship is more reliable
and suggests that better patient care is delivered in larger primary health care teams
sizes, up to 30 to 40 members.
Figure 3.6: Relationship between team size and effectiveness of patient care(externally rated)
Team size
706050403020100
Effe
ctiv
enes
s of
pat
ient
car
e
6
5
4
3
2
1
Figure 3.7: Relationships between Team Composition and Ratings of Innovation
Dependent variable Predictor variables β P R2
Innovation – overall Professional diversity 0.308 0.002Reflexivity 0.318 0.001Team size 0.290 0.003 0.363
No. of healthcare innovations Professional diversity 0.263 0.024No. of practice nurses 0.299 0.011Team processes 0.342 0.005Lack of clear leadership 0.274 0.023 0.298
Innovation (self-rated) Reflexivity 0.384 0.018Team processes 0.315 0.050 0.454

It seems that professional diversity in the team, reflexivity (taking time out to review
objectives, strategies and processes) and team processes all have positive effects on
innovation. Some of these relationships are illustrated in figures 3.7 to 3.11.
Figure 3.8: Healthcare innovations and professional diversity
Figure 3.9: Overall innovation and professional diversity
1
1.5
2
2.5
3
3.5
4
4.5
5
6 or fewer 7 8 9 10 11 12 or more
Number of professions represented in team
Ove
rall
inno
vatio
n -
exte
rnal
rat
ing
0
1
2
3
4
5
6
7
< 7 7 8 9 10 11 12 > 12
Number of professions represented in team
Mea
n nu
mbe
r of
inno
vatio
ns r
e:
qual
ity o
f he
alth
care

Figure 3.10: Relationship between reflexivity and overall innovation
Reflexivity
6.05.55.04.54.03.53.02.5
Ove
rall
inno
vatio
n
2.0
1.5
1.0
.5
0.0
-.5
-1.0
-1.5
LFigure 3.11: Relationship between team processes and number of innovations inhealthcare
Team climate
4.24.03.83.63.43.23.02.82.62.4
Inno
vatio
ns in
hea
lthca
re
10
8
6
4
2
0
-2

Bearing in mind that a larger score represents poorer mental health, results show
that teams which are composed of members who are relatively similar in terms of
age, have a larger proportion of managers, and avoid conflict over who leads the
team, are characterised by better mental health for their members. This is shown in
Figure 3.12.
Figure 3.12: Relationships between Team Composition, Processes and TeamMembers’ Mental Health
Dependent variable Predictor variables β p R2
Mental health Proportion of managers -0.420 <0.001
Age diversity 0.363 0.001
Conflict over leadership 0.253 0.017 0.375
Frequency of team meetings
Frequency of meetings was also examined as an explanatory variable. Figure 3.13
shows that frequency of meetings in primary health care team predicted external
ratings of innovation. Coming together to discuss objectives, exchange information
and make decisions is likely to lead to the generation of ideas for new and improved
services and ways of working.
Figure 3.1: Frequency of PHC team meetings as a predictor of innovation
Dependent variable β p R2
Innovation – overall (external) 0.242 0.026 0.059
Number of innovations re: healthcare 0.198 0.072 0.039
This result is illustrated in Figure 3.14.

Figure 3.14: External Ratings of Overall Innovation and Number of Meetings
2
2.2
2.4
2.6
2.8
3
3.2
3.4
3.6
3.8
4
1 or less 1 to 4 4 to 6 6 to 10 More than 10
PHCT Meetings per month (average)
Ove
rall
inno
vatio
n
It was also shown that this effect is independent of both self-rated processes and
team size.
Leadership
Research evidence suggests that leadership is an important factor contributing to
team effectiveness. We therefore explored the contribution of leadership to team
effectiveness and innovation in primary care teams separately. We explored the
extent to which there was a clear leader in the PHC teams, and who was regarded as
the leader. Only a third of PHC teams reported having a single clear leader. Nearly
half reported having a number of people lead the team, which, in most contexts, is
likely to cause considerable confusion. The most frequently named leader of PHC
teams is the Practice Manager. Only a third of team members nominated a GP.
Clarity of leadership was examined as an explanatory variable. Figure 3.15 shows
that team processes were poorer where there was no clear leadership, (from either
one individual or several people), or where there was conflict over leadership.

Figure 3.15: Clarity of Leadership in the PHC team predicting processes
Dependent variable Predictor variables β p R2
TCI mean score Lack of clear leadership -0.311 0.001Conflict over leadership -0.294 0.002 0.180
Reflexivity Lack of clear leadership -0.366 <0.001Conflict over leadership -0.250 0.008 0.193
Integration All having leadership roles 0.214 0.035 0.046
Figure 3.16 shows that lack of clarity about leadership inthe teams also predicted lower levels of effectiveness asrated by the team. Figure 3.16 also shows thatinnovation, rated externally, was higher in teams withshared leadership, or in teams where more peoplereported that everyone had leadership roles. Of course, itmay be that shared leadership is itself an innovation withprimary health care. Teams which had no clearleadership or conflict over leadership were less likelythan others to reviews and modify their objectives,strategies and team processes.
Figure 3.16: Clarity of Leadership in the PHC team predicting externally ratedeffectiveness and innovation
Dependent variable Predictor variables β p R2
Overall effectiveness(external)
Lack of clear leadership -0.249 0.029 0.062
Overall effectiveness (self-rated)
Lack of clear leadership -0.299 0.003 0.089
Effectiveness of patientcare (external)
None
Effectiveness of patientcare (self-rated)
Lack of clear leadership -0.215 0.034 0.046
Innovation (external) Shared leadership 0.237 0.020All having leadership roles 0.216 0.033 0.087
Innovation (self-rated) Lack of clear leadership -0.365 <0.001 0.133
No. healthcare innovations None
Mental health Conflict over leadership 0.294 0.003 0.086

These effects, and those for externally rated effectiveness, are all entirely mediated
by group processes suggesting that the mechanism by which leadership influences
effectiveness is through developing good team processes, such as shared
objectives, participation, emphasis on quality and support for innovation.
We also find that there is less clarity of leadership in teams which have a greater
proportion of part time workers (r = 0.309, p = 0.016), and there is less likely to be a
single clear leader in teams with greater professional diversity (r = 0.309, p = 0.016).
Both of these support the finding in Figure 3.2 that there is less consensus on who
the team leader is in teams with a larger proportion of “other” staff types.
Overall, the findings from this stage of the research reveal a very clear picture
of the factors predicting the effectiveness and innovations of primary health
care teams: size, clear leadership, professional diversity and integration
through regular meetings are key factors in predicting PHC team
performance. Of course, it could be that teams that innovate and are effective
have the confidence to recruit members from diverse professional
backgrounds, and are required to meet more often because of the innovations
they introduce. Clear leadership may emerge as a consequence of innovation
and as a consequence of the cohesiveness arising from effective
performance. Such interpretations are feasible and need to be explored
empirically. However, the interpretation implied in our presentation of results
(inputs and process predict performance) is consistent with research into
effectiveness of teams from across a range of sectors and countries (Cohen &
Bailey, 1998, West, Borrill & Unsworth, 1999).

Chapter 4
Qualitative Research:
Developing Objectives and Effectiveness Measures
for Primary Health Care Teams
Summary of Findings
• Using the constituency approach seven core objectives were developed which
were judged relevant and covered all the main aspects of primary health care
activity.
• Measures which could be used to measure performance on each of the
objectives were developed in workshops with a range of primary health care
stakeholders.
• Primary health care teams used the ProMES approach to develop measures
which could be used to measure their performance against the objectives for
primary care.
• Primary health care teams were able to use the measures developed to get
feedback on their performance, and use this information to introduce
improvements in patient care.

Measuring Effectiveness in Health Care
There is little agreement in primary health care about what constitutes effectiveness.
One reason for this is that primary health care comprises a wide range of
stakeholders (health care professionals, trusts, health authorities, patients, carers,
voluntary groups) each with their own aims, objectives and priorities which influence
how effectiveness is conceptualised. In addition, there is considerable variation in
philosophies of care among the professionals groups within primary care (Toon,
1994), and different approaches and perspectives on what is judged to be high
quality of care (Maxwell, 1992). One consequence of this is that health care will be
judged as more or less effective depending upon the criteria adopted by the
particular stakeholder, or on the philosophy or care espoused by a professional
group.
To enable these differing priorities and perspectives within health care to be taken
into account the qualitative research carried out by the research team used the
constituency approach (Connolly 1990) to develop objectives, and the Productivity
Measurement and Enhancement System (ProMES) developed by Naylor, Pritchard
and Ilgen (1980) to develop effectiveness measures. There were two main stages to
the work: developing objectives and effectiveness measures in national workshops;
developing effectiveness measures with primary health care teams.
Stage 1 - National Workshops: Developing Objectives and EffectivenessMeasures for Primary Health Care
The aim of this stage of the qualitative research was:
• To develop a set of objectives for primary health care which was acceptable to all
perspectives in primary health care
• To develop effectiveness measures which were acceptable to all perspectives in
primary health care.
The constituency approach was used to develop objectives for primary health care in
four national workshops with representatives from primary health care (see chapter
2). These objectives were then validated in workshops with representatives from 12
primary health care teams. The objectives and sub-objectives developed as a result

of the workshops and consultations with primary health care team representatives
are shown in Fig 4.1.
Figure 4.1: Core Objectives for Primary Health Care teams
Promote, maintainand improve health
§ Provide high quality health care
§ Accurate identification of individual and population healthcare needs
§ Review and improve the effectiveness of health careprovision
§ Manage illness, injury and disease taking account ofagreed standards and evidence based practice
Enable personaland communityresponsibility forindividual health
§ Enable patients/clients to make informed decisions abouttheir own health.
§ Proactively encourage positive health behaviour
§ Implementation of health education and preventativecare programmes
Efficient use ofresources
§ Human resources – skills, knowledge, expertise, time
§ Physical resources – budgets, equipment, premisesContinuouspersonal andprofessionaldevelopment
§ Individual annual training plans which take account of theplans of the PHCT
§ Equal access to training/development resources
High team membercommitment, stressand satisfaction
§ Team working
§ Mechanisms for reviewing and acting upon staffdissatisfactions, conflicts and complaints
Responsiveness toclients andcommunity
§ Gather information and feedback from clients/communitystakeholders/opinion leaders
Collaboration andpartnership withother relevantorganisations
• Build external relationships with clear objectives and highlevels of participation, interaction and trust
The first aim of the national workshops was to get agreement on the objectives for
primary health care, and to develop a set of objectives that cover all aspects of team
activity. The work carried out by workshop participants, and the subsequent
amendments made as a result of the rating and discussions with PHCT
representatives, enabled this main objective to be achieved. Given the diversity of

views, agendas and perspectives in primary health care it was a major achievement
that by the end of the four workshops agreement had been reached.
The second aim of the workshops was to develop effectiveness measures for primary
health care. A preliminary set of effectiveness measures was developed during the
workshops that reflect the range of stakeholder perspectives. These can be
developed further and used by primary health care teams. The research team
carried out additional work on some of the preliminary measures, developing
indicators of team effectiveness that could be used to measure performance.
Effectiveness Measures Developed in the Workshops
Objective 1 - Promote, maintain and improve health
Quality of care
• Patient Charter taken into account
• health promotion activities carried out
• appropriate skill mix in the team to meet patient needs
• measure - % of appropriate consultations as % of total consultations
• measure - appropriate immunisation rates (without adverse incidents)
• measure - effective management and knowledge of chronic diseases (epilepsy,
diabetes, asthma)
• measure - quality of patient consultations
• measure - appropriate admissions to hospital
Accessibility of service
• appropriate number of surgeries offered and times (also flexibility)
• appropriate length of consultation (also flexibility)
• waiting times. Time taken to get routine and emergency appointments (with any
member of the PHCT)
• availability of non face to face contact i.e. telephone access
• clients seen consistent with the severity of their needs (e.g. emergencies seen
quickly)

Chronic disease management
• effective management and knowledge of incidence of critical diseases: E.g.
Epilepsy, Diabetes, Asthma
In terms of -
Diagnosis
Registers
Protocols
Interviews
Referral/use of other services
• appropriate referrals to other services. Such a measure could indicate a lack of
skills in the team or illness in the community
• number of effective or appropriate contacts with agencies such as palliative care,
social services etc. i.e. good network of services
• level of appropriate access to the right services. Quality of partnerships and
alliances in referrals is important here. This indicator might also be linked with
the range of skills in the team
• identification and reduction of health and social care “grey areas” e.g., when
health care professionals do social care activities
• appropriate waiting times for admission to hospital i.e., for treatment from other
agencies
• rates of emergency admissions/self referrals
Treatment
• use of evidence based treatment and prescribing protocols
• appropriate intra-team referral. The group felt this was possibly more important
than referral to other agencies
• low adverse complications incidence
• care delivery derived from plan of care. Having action plans helps evaluation of
goals
• the team produces R&D strategy (based on consensus)
• the team produces clinical audit and clinical supervision action plans (based on
consensus)

• care packages/episodes of care (rather than just number of contacts)
• progress towards Health of the Nation targets
Identification of health needs
• identification of health needs and the mechanisms to adjust efforts to match
these needs
• utilisation of external bodies to identify service plans and needs met
Data Collection: Practice level
• measure - types of information collected demographics/diseases/conditions/
activity levels)
• measure - accessibility of data collected to PHCT
• measure - PHCT contributing to data
• compare with national/regional data
Data collection: Local, regional and national sources
• Assess completeness of data set
Use of data for:
• daily planning
• longer term planning - strategy/direction
• identifying gaps in provision and skill mix
• measure - number of action taken/changes made
- up-take of training
- modification of skill mix
- review process
- formal service plans
• budget allocation consistent with priorities
• Identifying and utilising opinion leaders in the community and community
networks

Accountability
• meeting NHS care standards
• meeting NHS reporting requirements
• meeting requirements of other appropriate external agencies
• progress towards Health of the Nation targets
Objective 2 - Enable personal and community responsibility for individualhealth
• effective health education and preventative health care programs
• appropriate immunisation rates (without critical adverse incidents). What is
appropriate will vary in accordance with local needs)
• information to patients and health education
- includes information and knowledge and explanation for patients
- making it personalised - so patient is recognised as an individual
• increasing knowledge about health in the population
- i.e. with employers, teachers etc.
• patients educated to make appropriate self-referrals to members of the PHCT.
Where is the locus of control, within the team or with the patient?
• number of health problems revealed by screening
• provision and take up of preventative health care programmes
Objective 3 - Efficient use of resources
• monitor appointment management - DNAs
• protocols: new, renewed, rejected
• use of accommodation/equipment
• develop skills inventory and monitor use of skills
• measure - input costs: GP: practice size
• measure - initiatives developed to use time effectively and review process
• measure - balance between outputs and resources/monitor over time
• measure - % of time with patients
• review duplications of roles/effort

• existence of evidence based prescribing protocols for practice (and review of
these). There is a need to close the loop between cost effectiveness and clinical
effectiveness of prescribing
• existence of evidence based treatment protocol (including shared protocols and
reviews)
• use of clinical guidelines (not just medical - so incorporates everyone in team)
• planned clinical audit
• degree to which safety standards were being complied with (Baseline could be
minimum standards set by Health and Safety Executive)
• how effectively the PHCT computer systems are being used
Objective 4 - Continuous personal and professional development
Development of skills
• Regular development and learning needs to be considered at the level of the
individual, the team, the national governing bodies, and the professional bodies
that monitor health care professionals
• strategy plan for training and development
- long term and short term
- individual skills/job description
- match health needs/individual needs
- match to organisational objectives
- who contributes to developing the plan
- take account of each individual’s understanding of ‘development’
• measure - commitment to development of skills in the team
• equal access to/management of training budget
• research activities carried out - how funded, quality and quantity.
• utilisation of a full range of training methods (e.g., on the job, networking)
• opportunities for job exchange
• skill sharing - opportunities and time spent
• mechanism in place to evaluate the effectiveness of training and development
that is done, including publication of the existence of training opportunities, time
available, equipment, instructors, etc.
• job performance of staff should be assessed on a regular basis using an agreed
upon procedure

Checklist of activities which contribute to the development of skills:
• availability of peer support/mentoring (inside and outside)/advocacy
• individual career development plans
• reviews of development plans
• IIP in place
• staff appraisal - linked to short term and long term goals
• identification of training needs - and review of these
• training equally available across team
• feedback on training attended/portfolio maintained/accreditation
• protected time available for professional development
• access to resources to support training and development
• indicators for learning and training
Team member mental health/stress
• procedures to resolve conflict between patient/practitioner needs
• procedures for taking account of personal needs/family commitments
• staff allowed to be off sick
Objective 5 - High team member commitment, stress and satisfaction
• measure - staff turnover/absence
• measure - how valued staff feel/commitment/grievances
• mechanism in place for reporting satisfaction levels back to team members and
dealing with dissatisfaction when it becomes a problem
Team development
• team participate in team development activities?
• availability of social budget
• shared understanding of roles and values
• the team contribute to the annual report/business plan?
• the team has regular meetings
• procedure for coordinating sub-groups and whole team
• procedures for communication

• procedures to integrate roles/expectations across professional groups
• processes for critically evaluating and improving decision making
• equal opportunity for participation in decision making
Learning organisations
• measure - support for innovation
• measure - resulting changes
Objective 6 - Responsiveness to clients and community
• a commitment to client satisfaction within the team
• complaints procedures in place
• accessible information produced for patients
• patient choice re health care
• take account of patient perceptions of improved health and stress
• use questionnaires/surveys to assess patient satisfaction
• user involvement in decisions about their own health
• actions taken in response to patient suggestions for improvement not the same
as complaints - giving patients the opportunity to make comments without feeling
as if they are complaining.
• carefully listening to the client
• giving clients the information to make informed choices
• getting inputs on client needs from clients, community and opinion leaders,
groups representing clients
Objective 7 - Collaboration with other organisations
• measure - staff use of skills and resources available
• effective contacts with related agencies and groups outside the PHCT
Development Work Carried Out by the Research Team
The research team carried out additional work after the national workshops refining
some of the measures of effectiveness identified in the workshops. These are
described below.

Objective 1 - Promote, maintain and improve health
• The PHCT would have a monthly (or more frequent) staff meeting where a
sample of cases was reviewed. This review would include the appropriateness of
who saw the client, what procedures used, and whether that client was handled
appropriately in all aspects. The measure would be the percentage of cases
which were considered as being managed appropriately. This would also be the
basis for discussion of what improvements need to be made for those specific
clients and for clients in general.
• The task of developing a health needs analysis can be broken down into
definable steps, e.g. get information on how to do such an analysis, decide on a
plan for doing the analysis for that particular PHCT, gather the information, put
the information together into a form that the PHCT can use to make decisions.
Each of these steps would be given a time for completion. The indicator would
be the percentage of the analysis completed compared to the anticipated time for
completion.
Survey on client perceptions of health improvement after treatment. For
example, each client is given a questionnaire or a sample of clients are called by
phone and asked about improvements. Measure is the percentage of clients
improving. For the various specific targets given by agencies outside the PHCT
such as immunisation rates, develop a scoring system whereby each level of
meeting the objective gets a certain number of points, e.g. if the target
immunisation rate was 80%, actually doing 80% would give 100 points, 60%
immunised would be 20 points, 70% 80 points, 90% 130 points, etc. The
number of points would be based in the importance of that target. The index
would be the percentage of actual points earned compared to the maximum
possible points received if all targets were met.
• The percentage of required reports completed on time
• The number of required reports returned by agencies requesting corrections or
additional information. (This would be an index of the quality of the reports.)

Objective 3 - Effective use of Resources
• Number of new initiatives developed that are designed to help team members
use their time better. These initiatives should also be reviewed on a regular basis
to ensure they are still effective.
• Percent client contact time as a percentage of total time. This measure gets at
how much time is devoted to clients. It does not measure how well that time is
being spent. Other indicators are needed to address this issue. (Note that this
indicator is one where there is probably an optimal level between the extremes.
Too little time with clients may suggest too much administration time. Too much
time with clients may suggest too little administration time.)
• Percentage of staff turnover over time. High staff turnover leads to inefficient
resource utilisation because it takes time to teach procedures to new staff and
work is lost as a departing staff member leaves. This measure would also be an
indicator for the satisfaction of team members.
• Percentage of appointments which are unfilled or where the client did not come.
Objective 4 - Continuous personal and professional development
• Training and development. A list of training and development experiences for
each person on the team would be developed each year. For example,
attendance at a certain type of conference, training on a piece of office
equipment, learning a new procedure, etc. This list would be the development
plan for that person for that year. There would be two measures for training and
development. The first would be the percentage of team members who had the
written plan. The second measure would be the percentage of the development
plan items actually completed.
• Which team members are reviewed, given feedback, and have a formal, jointly
developed action plan for making improvements.

Objective 5 - High team member commitment, stress and satisfaction
• Measure overall satisfaction on a monthly or bi-weekly basis with a very brief
questionnaire that would take no more than 2 minutes to compete. Measure
would be the percentage of staff indicating Satisfied or Very Satisfied with their
jobs.
• Staff turnover is also a satisfaction measure. Note this measure under Effective
Management of Resources.
Objective 6 - Responsiveness to clients and community
• Establish a formal procedure where clients can make complaints including a
process for following up on these complaints. Measure is the number of such
complaints which were not concluded to the client’s satisfaction within one week.
Stage 2 - Effectiveness Measures Developed by Primary Health Care Teams
The ProMES approach is based on a theory of motivation which proposes that effort
is maximised when there is a clear link between effort and outcomes, there is
agreement about what are valued outcomes, feedback is provided on performance
and the evaluation of performance is judged to be fair (Pritchard, Jones, Roth,
Stuebing & Ekeberg (1988). Research evidence shows that involving individuals in
the process of agreeing the valued outcomes from their work and developing
methods for assessing their performance has a greater impact on performance than
when these are imposed (Pritchard, 1995). The research team therefore carried out
ProMES work with primary health care teams so they had the opportunity to develop
their own effectiveness measures.
There were two main aims for this work:
• To demonstrate that primary health care teams could develop effectiveness
measures using the ProMES approach
• To demonstrate that primary health care teams could use the measures
developed to get feedback on their performance.

Qualitative work using ProMES was carried out with two PHCTs (see Chapter 2).
There were four distinct stages to the work:
1. Establishing a 'design team', these were representatives from the team who were
primarily responsible for developing the measurement and feedback system.
2. Reaching agreement that the objectives developed in the constituency
workshops, were relevant and related to all the main activities of the
organisation/team.
3. Develop measures that could be used to assess the extent to which these
objectives are being achieved.
4. Using measures to gather information about how well the team was performing.
The researchers worked with the primary health care design teams over a period of
eighteen months, meeting for one hour once a fortnight. As a result of this work the
primary health care teams successfully developed effectiveness measures that they
could use to assess performance on all of the objectives for primary health care. A
major issue in primary health care is the considerable work pressures and demands
made on all members of the team. This is a major constraint on the time team
members have available to engage in activities which do not directly contribute to the
delivery primary health care team services. It was therefore a significant
achievement that teams were able to develop measures, and demonstrates what can
be achieved as result of a relatively small investment of time.
The measures developed by the teams are listed below. Information on how to use
the measures is provided in Appendix III.
Objective 1: Promote, maintain and improve health
Measure 1 - Review of quality in case management
Percentage of cases judged to be managed appropriately on the most relevant
quality dimensions.

Measure 2 - Young People’s Sexual Health
Percentage unwanted teenage pregnancies in a 6-month period
Percentage of teenagers prescribed the morning after pill in a 6-month period
Percentage of teenagers requesting pregnancy tests in a 6-month period
Measure 3 - Young People’s Health - Alcohol and Drug Misuse
Number of teenagers attending A & E after drug overdose in a 3-month period
Number of teenagers attending A & E after excessive alcohol consumption in a 3-
month period.
Measure 4 - Patient access to consultations with a GP
The number of days that patients wait to see a GP of their choice
Measure 5 - Patient access to a quality consultation with GPs
Percentage of patients whose appointment with a GP is minutes duration in a
3-month period.
Measure 6 - Use of out of hours services by patient
Percentage reduction in the use of private out of hours services by patients in a 6-month
period.
Measure 7 - Patients have access to an appropriate health professional
Percentage of patients, in a 6 month period, who have contact with a
health professional from the team at a time and location most appropriate
to them and to the professional.
Measure 8 - Patients have access to a home visit from an appropriate health
professional.
Percentage of patients in a 6 month period who have a home visit from the
health professional judged by the patient and the health professional to be
most appropriate.
Objective 2: Enable personal and community responsibility for individualhealth
Measure 9 - Patients understand the role and function of the PHCT.

Number of patient requests, use health professionals’ time and PHCT services which
are inappropriate in a 3 month period.
Objective 3: Efficient Use of Resources
Measure 10 - Patients able to manage minor illness
Percentage of patients seen by health professionals in the team who had a minor
illness which could have been managed themselves.
Measure 11 - Patients/clients who do not attend for an appointment
Average percentage of total patients' appointments not kept in a week
(calculated over a 3-month period).
Measure 12 - Efficient use of administrative systems
Percentage of patients not attending appointments with health professionals in the team which
result from errors in the administrative system.
Measure 13 - Efficient use of GP resources in the team
Average number of patients seen by a GPs in a week
Objective 4: Continuous personal and professional development
Measure 14 - Team member access to training
Percentage of who are satisfied with the extent to which their training needs are assessed and
met in the previous year.
Objective 5: High team member commitment, stress and satisfaction
Measure 15 - Team member commitment and satisfaction
Percentage of staff in the team who feel committed and satisfied
Measure 16 - Team members use each other's skills, knowledge and expertise
appropriately

Percentage of team members who report that skills,
knowledge and expertise within the team are used
appropriately in 3-month period.
Measure 17 - Effective team working
Percentage of requests for help and information and referrals from other team
members which are inappropriate in a 3 month period.
Objective 6: Responsiveness to client and community
Measure 18 - Patients’ Experiences of the PHCT service (1)
Percentage of patients who report that their experiences of the PHCT services match
the range and standard agreed by the PHCT.
Measure 19 - Patients’ experiences of the PHCT services (2) (Using the existing
measure)
Percentage of patients whose experiences of the PHCT services meet the standard
set by the team.
Measuring Performance
The second aim of the qualitative work with primary health care teams was to
demonstrate that it was possible for primary health care teams to use effectiveness
measures to obtain feedback on performance. Both of the primary health care teams
were able to used effectiveness measures to gather feedback information. Below we
detail the procedure used by one of the teams to develop a measure of patient
satisfaction, gather feedback from patients and then make changes on the basis of
this feedback
Measure 19 = Percentage of patients who report that their experiences of the
PHCT services match the standard agreed by the PHCT.
The measure was developed by the design team as follows.
The team listed all of the services they provided (e.g. consultations with a health care

professional, clinics, district nursing and health visiting services) and also considered
features of the delivery of services which they believed would be associated with
patients satisfaction (e.g. short waiting times, prompt repeat prescriptions, phone
answered quickly, access to advice).
A questionnaire was developed which enabled patients to report their experiences of
the services and the features associated with satisfaction (see Appendix III, p…..).
The areas covered by the questionnaire were: waiting time to see a GP; waiting time
for the phone to be answered; waiting time for a repeat prescription; waiting time to
see a practice nurse; awareness of health visitor services, waiting times at health
visitor clinics; and waiting time for district nurse visits. Patients were also asked to
provide comments on how different services they had experienced could be
improved.
Patients were asked factual questions about their experiences, not for opinions.
For example:
The last time you wanted an appointment with any of the GPs, how soon did you get
one?
Same day [ ]
Next day [ ]
After 2 days [ ]
Longer_________
The last time you asked for a repeat prescription, how long did you have to wait to
get it?
1st time ___________ days. Not Applicable [ ]
2nd time___________ days
The team identified additional patient information that would help to understand the
information collected on patients’ experiences (age, gender, number of visits to the
surgery in the previous month).
Before distributing the questionnaires the team determined the standards they
wanted to achieve. For each question they decided what would be acceptable and
unacceptable responses, and the standard they would like to achieve. They

determined the percentage of patients they would expect to experience the service in
a particular way, the percentage that was unacceptable, and the percentage that
would be an ideal. For example, the team decided what percentage of patient they
would expect to see a GP on the same day, the next day, after 2 days, or after a
longer period of time, the percentages for each which was unacceptable and the
percentages that they would like to achieve.
Over a one week period all patients (or for children, their carers) attending the
surgery were asked to complete a questionnaire. 100 questionnaires were sent to
home addresses, and an additional 100 distributed via district nurses and health
visitors. The information from patients was collated and a mean score calculated for
each item on the survey.
The score for each item was then compared with the expected standard,
unacceptable standard and ideal standard, and the differences between the actual
mean and these percentages calculated. This provided the team with feedback
about the extent to which the experiences of patients matched the standards the
team were trying to achieve, where experiences fell below standards, and where they
were achieving the ideal standard.
Results from the patient satisfaction survey
Responses were received from 320 patients which provided a valuable source of
feedback on the services provided by the primary health care team. On many
aspects the reported experiences of patients matched or exceed that of the
standards set by the team. Where the reported experiences fell below the team's
standards the reasons for this were explored by the design team and changes made
to the provision of this service. For example, the survey revealed that 50% of
patients had waited for between 10 and 15 minutes to see the practice nurse after
their appointment with the GP. This was below the target set, 90% of patients
waiting a maximum of 5 minutes.
Two main reasons were identified for the longer waiting time: patients were not clear
about the procedure for seeing the practice nurse after their GP consultation; and
there were insufficient consultation rooms to accommodate the patients who needed
to see these nurses. Two changes were proposed to reduce the waiting time.
Firstly, an information slip explaining the procedure for seeing the practice nurse was

produced which GPs could give to patients when they referred them to the nurse.
Secondly, the use of consultation rooms was reviewed. An antenatal clinic, which
used two consulting rooms, was held at the same time as the morning surgery. It was
proposed that this clinic was run at a different time thus providing two additional
rooms the practice nurses could use for patient consultations.
Discussion
The aims of the qualitative research were to develop agreement among primary
health care professional about the objectives for primary health care, to develop
measures that would provide feedback on the extent to which effectiveness was
being achieved, and to demonstrate that primary health care teams could develop
and use effectiveness measures.
The national workshops brought together a wide range of primary care stakeholders;
representatives from district nursing, health visiting, general practice, practice
nursing, midwifery, mental health, professions allied to medicine, social services,
health authorities, the Department of Health, NHS Executive, NHS trusts, patient
actions groups and academia. During the course of the workshops these
stakeholders, who had differing aims, objectives, priorities and philosophies of care
were able to reach agreement about the objectives for primary health care. The
practitioners at the workshops judged these objectives relevant and useful, as did
members of primary health care teams who were consulted during the development
process.
Using the objectives developed in the workshops, the ProMES approach was used
with two primary health care teams to develop measures. This stage of the research
also involved working with multidisciplinary groups of health professionals who
developed a set of effectiveness measures that could be used to assess the team's
performance. These measures were used by the teams to get feedback on how
effectively they functioned, and, as illustrated in the example discussed above, this
feedback was used to improve the quality of care to patients and to use the
resources available to the team more efficiently.
The second stage of the research demonstrated that it is possible for primary health
care teams to develop and use effectiveness measures. Further work is required to
improve and refine the measures developed by the primary health care teams, and to

test their generalisability for primary health care teams in a range of settings.

The qualitative research has demonstrated that a combination of the constituency
approach and ProMES provides a practical method that can be used to help primary
health care teams clarify their objectives and to obtain feedback on the effectiveness
of the services provided. This will help health professionals to prioritise resources
and to deliver high quality, cost-effective health care.

Chapter 5
Community Mental Health TeamsResearch Methods and Sample Details
Introduction
NHS secondary mental health care is delivered primarily through multidisciplinary
community mental health teams (CMHTs). These face many challenges. They are
tasked with complex statutory and professional responsibilities (Peck & Parker,
1998). The demands of a primary care-led NHS often conflict with the policy
imperatives of the sensitive area of risk management relating to severe mental health
problems (Onyett, 1995). In addition, the voice of service users gains strength,
adding to workload and pressures. Team members are employed within two very
different bureaucracies; those of health and social care, and come from diverse
professional backgrounds. However, the development of joint commissioning
approaches between health and local authority social services requires them to
function as integrated teams (Hannegan, 1999). Their constituent professions may
jibe at the adjustments this requires (Mistral & Velleman, 1997), for which their
training may not prepare them well.
The current policy agenda is increasingly outcomes-focussed. Accordingly, CMHTs
are required to monitor their performance (Bhugra, Bridges, & Thompson, 1995) and
effectiveness, as a strong commitment to monitoring and evaluation is considered
essential for adequate management of CMHT services (Carter Evans, Crosby,
Prendeergast & De Sousa Butterworth, 1997). The competition for resources
amongst elements of health and social care provision requires that each provide data
to demonstrate the value of its contribution. More positively, effectiveness measures
may also bring some clarity to teams' efforts to chart their own progress towards
meeting diverse expectations.
The organisation of CMHTs is central to their functioning (Bhugra, et. al., 1995;
Onyett, 1997). Their core rationale is to bring together a range of professions in
order to deliver more effective care co-ordination than could be achieved without an
integrated, multidisciplinary team. Achieving that integration is by definition an
organisational task (Onyett, 1995; Pincu, Zarin & West, 1996), requiring that the team

be more than the sum of its diverse constituent members acting individually. This
task is rendered considerably more challenging by the need for multi-agency working
across the health-social services divide (Department of Health, 1995).
User and carer perspectives are increasingly important. The National Health Service
Patients' Charter for Mental Health Services (Department of Health, 1997) sets out
rights and expected standards of service for users and potential users of these
services. It aims to ensure that the NHS 'listens and acts upon people's views and
needs'. A continuing push for users and carers to be involved in decisions relating
to mental health care (Faulkner, 1997), and also to be included at the level of
planning and developing services, presents a further challenge to teams which
deliver integrated care within the Care Programme Approach (Department of Health,
1990).
There is a growing international literature on CMHTs as a mode of delivery of mental
health care. Within the UK, a notable source of this has been the Sainsbury Centre
for Mental Health. The key issues with emerge from the research literature include
the following, for each of which a representative citation is provided:
• The many managerial, professional and clinical barriers to effective
multidisciplinary teamwork (Peck & Norman, 1999).
• The importance of integrated operational management of CMHTs (Onyett,
1997).
• Leadership, integration and agency as key precursors of effectiveness
(Grusky, 1995).
• The threats to effectiveness arising when resource constraints lead teams to
over-emphasise control and efficiency at the expense of creative thinking and
innovation (Drolen, 1990).
• The mismatch between current training arrangements and current and future
service needs (Sainsbury Centre for Mental Health, 1997).
• The specific leadership skills required by CMHTs, in which training is
necessary (Reed, 1995; Sluyter, 1995.
• The highly demanding nature of CMHT work (Prosser, Johnson, Kuipers,
Szmukler, Bebbington & Thornicroft, 1996).
• Detriments to morale and effectiveness from excessive workload (King,
LeBas & Spooner, 2000).

As the Health Team Effectiveness research programme was nearing completion, the
National Service Framework for Mental Health (NSF; Department of Health, 1999)
was published. This seeks to establish national standards for mental health care.
Within the NSF, national support for local action includes workforce planning,
education and training. This aims to enable mental health services to ensure that
their workforce is sufficient and skilled, well led and supported, to deliver high quality
mental health care. A Workforce Action Team (WAT) has been established to
provide national leadership in developing and taking forward the workforce action
plan. We have identified within the WAT interim report (dated April 2000) several
themes that a study of mental health team-working can usefully address:
• Education and training: What are the training requirements for effective
teamworking and how might these be met?
• Recruitment and retention: What are the salient features of team
composition? What factors are associated with staff turnover, and how might
retention be improved?
• Leadership: How does this impact on quality of care? How can it be best
developed?
• Primary care: What characteristics of primary health care teams are
conducive to high-quality mental health care?
• Professionally non-affiliated staff: What can the contributions of support
workers tell us about the potential for further development of non-affiliated
staff?
Before offering answers to some of these questions, we describe the methods used
in our research.
The research with Community Mental Health Teams (CMHTs) had two stages. The
first was a questionnaire survey, and related data collection methods, involving large
numbers of teams to gather data on team inputs, processes and outputs. The
second stage involved intensive examination of a sub-set of teams to explore in more
depth targeted team processes and outputs. An overviews of the methodology for
stage 1 is given in Figure 5.1.
Figure 5.1: Details of CMHT research methods stage 1
Additional questionnaires/

Sample size Survey data Telephoneinterviews
Externalratings
113 teams
1443respondents
Team compositionTeam functioningTeam effectivenessTeam innovationStress
Team compositionTeam meetingsTeam managementDecision makingClinical systemsmanagement
Teameffectiveness
Teaminnovation
Summary of Research Methods
A. National workshop to derive CMHT effectiveness criteria
B. 113 Community Mental Health Teams
§ Survey of all team members
§ Questionnaires or telephone interviews with team leaders
§ External ratings of team effectiveness
§ External ratings of innovations introduced by the teams
C. 10 Community Mental Health Teams
§ Videotaping and analysis of team meetings
§ Caseload analysis and client selection
§ Interviews with practitioners on two occasions, 6 months apart
§ Use of HoNOS to record client outcomes
§ User and Carer Service Satisfaction Questionnaires
Quantitative methods
The Sample
The research design required data to be gathered from 100 CMHTs. Initially, chief
executives of 101 community mental health trusts in 4 regions, Northern and
Yorkshire, North West, Trent, and North Thames, were approached, to inform them
of the study and to encourage participation of all CMHTs managed by that trust. The
aim was to limit the geographical spread while accessing representative CMHT’s, in
terms of different socio-economic locations, skill mix and client base. Three months
after the first mailshot, follow-up letters were sent to all trusts not responding. Of the
101 approached, 81 responded: 11 had no community adult mental health services;
12 declined to participate and the remaining 58 provided names and contacts for all

CMHTs managed. The main reasons for not participating were either that (a)
caseloads were such that teams were too busy (3 trusts); or (b) the Trust was in the
process of reorganisation (7 trusts); or (c) the teams were already taking part in other
research (2 trusts).
With the CMHT names provided we made direct contact with 162 CMHT’s, inviting
participation in the study after consensus to participate had been achieved within
each team. The final number of participating teams was 113 from 45 trusts. Details
of the sample are shown in Table 1. At different stages of the access procedure, it
was open to Trusts or CMHTs to refuse to participate; the sample was therefore
made up of volunteering CMHTs. We performed a post hoc check on socio-
economic representativeness, which indicated that the whole range of deprivation
scores was represented (Mental Illness Needs Index (MINI) range 91.3 (low need) to
118.5 (high need), mean 103.3).
Data collection Methods
Data on team functioning and effectiveness were collected using three methods: self
report questionnaires completed by individual team members; self report or
telephone interviews with team leaders; and external ratings from community health
care representatives, social services and health authority staff.
The named contact for each of the 113 participating CMHTs provided a
comprehensive list of all team members, which included all personnel attending
regular team meetings. Survey questionnaires were sent to 1925 named individuals,
with returns from 1450 (75%). The return rates for professional groups were:
administrative staff 57%; community psychiatric nurses 82%; occupational therapists
83%; psychiatrists 55%; clinical psychologists 90%; social workers 53%; and support
workers 68%. Overall, 925 women (64%) were included in the sample, and the
mean age was 40 (SD 8.37).
Team leaders from 91 CMHTs provided information on team context, team
composition, team processes, and clinical management in a self-report questionnaire
survey.
Questionnaires completed by individual team members
This questionnaire was in four sections (the CMHT survey is included in Appendix I).

Section 1: Team working
This contained six measures of team working. Four of these were drawn from the
Team Climate Inventory (Anderson and West, 1994; 1998) that is based on a well-
developed theoretical model of team functioning (West, 1990). The four measures
assess levels of
§ team participation
§ clarity and commitment to team objectives
§ emphasis on quality
§ support for innovation
Two other measures were included:
• reflexivity, the extent to which team members reflect upon their team objectives,
strategies and processes and make changes accordingly (West, 1996; Swift &
West, 2000)
§ team innovation, the extent to which the team has introduced innovations in
objectives, work strategies, processes and relationships
Respondents were also asked to describe the major changes or innovations
introduced by the team in their work in the previous 12 months.
Section 2: Effectiveness
These included 27 measures of community mental health team effectiveness derived
at a stakeholder workshop (Rees, Stride, Shapiro, Richards & Borrill, in press;
Richards & Rees, 1998). Three underlying dimensions were evident:
§ team working
§ patient/client orientation
§ organisational efficiency
Section 3: Team member stress
This included a measure of psychological stress, the GHQ-12 (Goldberg, 1972). The
GHQ-12 is widely used as a screening tool for detecting minor psychiatric disorder in
the general population, and in occupational mental health research. It covers
feelings of strain, depression, inability to cope, anxiety based on insomnia, lack of
confidence and other psychological problems. Within a Department of Health funded
study of the mental health of the NHS workforce, the GHQ-12 showed good validity
against a psychiatric interview (Hardy, Shapiro, Haynes & Rick, 1999).

Section 4: Biographical information
This section included questions on biographical and team characteristics (e.g. age,
gender, ethnic origin, job title, employer, team composition, team leadership).
Additional Team Information – Survey
This was completed by the team leader or co-ordinator in 92 CMHTs, and combined
the PHCT data collection via survey and telephone interviews. Besides the
information on decision-making and communication systems, data were collected
relating to the clinical systems the CMHT implemented for dealing with referrals, both
emergency and routine, and for accessing inpatient beds.
External ratings – team effectiveness
Each of the 113 CMHTs in the survey sample was approached to nominate three
professionals external to the team, within the local Trust, Social Services, Health
Authority, or GP practices in their catchment area, in order to collect corroborative
data on team effectiveness. Thirty-three teams nominated up to 4 external judges
each. Judges’ ratings were made using the same 27 effectiveness dimensions that
team members had used to rate their team’s effectiveness.
External ratings – team innovation
Two experts known to the research team rated the descriptions of changes or
innovations introduced in each CMHT over the previous 12 months, and which team
members had described in their questionnaire responses. The changes were rated
on the following dimensions (West & Anderson, 1996):
§ magnitude, how great would be the consequences of changes introduced
§ radicalness, to what extent the status quo would change
§ novelty, how new in general were the changes
§ impact, to what extent changes would improve CMHT effectiveness
Sample Details
The aim of the research programme is to determine which team characteristics are
associated with good team functioning and team effectiveness. In this section, we
describe characteristics of the CMHT sample that participated in the survey
components of the research programme. Following the model used to guide this
research see Chapter 1) we describe four categories of inputs:

§ team characteristics – indicated by size, mean age, mean tenure, gender mix,
ratio of full-time members, length of time the team had been in existence.
§ team composition – indicated by the distribution of occupational groups within the
team.
§ team task – indicated by the MINI (high or low deprivation scores), how quickly
the CMHT saw emergency referrals, pooling of referrals, the use of a single
integrated set of client case notes, whether waiting lists were in operation for
client assessment.
§ team environment – indicated by how the CMHT was commissioned and the
English NHS region within which the team was located.
We also describe the relationships between these four domains of inputs. The
reader will also find an account of team members’ perceptions of leadership in the
team.
Team Characteristics
Number of team members
In terms of the number of individuals employed within each team, this ranged from 6
to 51. The mean size was 17.04 members, SD 7.99. Distribution of sample team
size is shown in Figure 5.2 below.
Age and gender distribution
Overall, 925 women (67%) were included in the sample. Figure 5.3 shows the
percentage of women in CMHTs. The mean age was 40, SD 8.37. Across the 113
CMHTs, only one CMHT was made up of only women. The age distribution appears
normal, but it is noteworthy that there are very few CMHT workers below 30 or above
50 years old. This age profile resembles that of qualified nurses.
Figure 5.2: Distribution of team size (number of teammembers) across the sample

0
5
10
15
20
25
30
35
up to 10 11 to 15 16 to 20 21 to 25 > 25
Figure 5.3: Percentage of women in CMHTs in thesample
0
5
10
15
20
25
30
35
80 to100%
70 to79%
60 to69%
50 to59%
25 to49%
% of teams
Tenure
All team members indicated how long they had been in the CMHT. Mean tenure
across teams was 37 months, SD 19 months. This relates to the short life of one
third of teams in the sample, which had been in existence for less than 2 years.
Whole time equivalents
Number of Teams
% of women
Number ofmembers

Taking account of hours worked to calculate team size in terms of whole time
equivalents shows that team size varied from 5.5 to 48.5. The mean size was 15.81
WTEs, SD 7.53. The small size of the mean difference between numbers of
members and WTEs suggests that the great majority of team members were
employed on a full-time basis. Twelve per cent of CMHTs in the sample were
comprised solely of full-time workers. Across the sample, mean percentage of full-
time workers was 77.49, SD 13.74.
Length of time CMHT in existence
CMHTs were formally introduced on a national basis in 1990, to provide integrated
care in the community for mentally ill people. In this sample, the length of time the
teams had been existence varied from 6 months to 7 years. For subsequent
analysis, these were categorised as less than 2 years (n = 31); from 2 to 5 years
(n = 36); and 5 or more years (n = 25).
Team composition
Figure 5.4 gives the breakdown of the sample by professional group and by gender
(n = 1363).

Figure 5.4: CMHT occupational groups by gender
WOMEN MEN
ADMIN 181 7
CPN 316 214
OT 92 14
PSYCHIATRY 27 55
COUNSELLING/PSYCHOLOGY 43 17
SOCIAL WORK 129 83
SUPPORT WORK 68 22
OTHER 62 32
TOTAL 918 444
As expected, the largest occupational group was nursing, making up 39% of the
sample. The next largest groups were social work (16%) and administrative staff
(14%). Occupational therapy (8%), support work (7%), psychiatry (6%) and
psychology/counselling (4%) were the smaller occupational groups. As compared
with the overall preponderance of women, who formed two-thirds of the respondents,
administrative staff were, unsurprisingly, even more predominantly female. Almost
90% of occupational therapists were women. In contrast, two-thirds of psychiatrists
were men. The gender mix of nursing and social work showed a modest
preponderance of women.
At the team level, multidisciplinary mix was as shown in Figure 5.5. Noteworthy here
is the fact that just 12% of teams included members from all disciplines (psychiatry,
social work, psychiatric nursing, clinical psychology, occupational therapy).

Figure 5.5: Multidisciplinary mix within CMHTs
0 5 10 15 20 25 30 35
Number of CMHTs
CPN plus one other Health
CPN Psychiatry and SW
CPN plus 2 other Health
CPN plus SW
All disciplines, no SW
All disciplines except psychology/OT
All disciplines except psychiatry
All disciplines
Team Task
Mental Illness Needs Index (MINI)
MINI scores for the Health Authority areas within which CMHTs’ populations were
based ranged from 91.3 (low need) to 118.5 (high deprivation), mean 103.34, SD
6.91. Figure 5.6 shows the distribution of CMHTs across Health Authorities with low
(30%), medium (40%) and high (30%) deprivation scores.
Figure 5.6: Teams in areas of high of high, medium and low need as indicatedby the MINI
low need
medium need
high need

CMHT response to emergency referrals
CMHTs indicated how quickly, on average, emergency referrals were seen. Elapsed
time before emergencies were seen ranged from ‘within the hour’ to ‘within two
weeks’. Across all teams, the mean wait for emergencies was 26 hours, SD = 44
hours.
Within-CMHT pooling of referrals
CMHTs provided information on how referrals, other than emergencies, were dealt
with. Five CMHTs did not pool referrals; 20 CMHTs pooled some referrals; and 63
CMHTs pooled all referrals.
Use of integrated case notes
In 40 CMHTs, each discipline kept client case notes separately; in 12 CMHTs, notes
were separate but available for reference by other disciplines; and in 34 CMHTs,
each client had one integrated set of case notes.
Assessment waiting list implementation
Fifty-three CMHTs indicated that they did not operate a waiting list prior to
assessment, and 36 CMHTs indicated that they did operate a waiting list.
CMHT Organisational context
NHS Region
CMHTs were sampled from four NHS regions in England. The participating regions
contributed 32, 26, 32 and 23 respectively. To safeguard the anonymity of the
participating teams, these regions are not identified in this report.
Local commissioning arrangements
There were three models of commissioning for these teams: 25 CMHTs were
commissioned by Health Services only; 39 by Health and Social Services jointly; and
33 by Health and Social Services separately. CMHTs are constituted on a multi-
agency basis between health and social services. Most CMHTs necessarily combine
staff working within the management structures of each of the two agencies, tasked
with meeting the objectives of both. However, each CMHT must function as a
coherent entity working towards mutually agreed objectives and following mutually

understood and functionally interdependent practices. Local commissioning
arrangements may impact on integrated team functioning.
CMHT constructed process and outcome variables
Apart from scales derived from survey items, for example, those from the Team
Processes Inventory, CMHTECQ and GHQ, others were computed to measure the
clarity of team leadership, within-team variation in relations to the clarity of team
leadership, the team’s efforts to communicate other than in a formal meeting
environment, and the team’s turnover.
Clarity of CMHT leadership
All team members provided information about the clarity of leadership in the CMHT.
Team means were aggregated from the single survey item: ‘ Does the team have a
single clear leader or co-ordinator?’ where ‘yes’ scored 1 and no entry was
scored ‘0’. Members of 13 CMHTs in the sample were unanimous in reporting that
their team had a single clear leader, while members of six CMHTs were unanimous
in declaring that the team had no single clear leader or co-ordinator. The aggregated
measure was treated as a process variable.
Within-team variation in relation to the clarity of team leadership
Blau’s index of variation was used to calculate the extent of disagreement within the
team about the clarity of leadership. Five variables with values ranging from 0 to 1
were constructed for the proportion of each team giving each of the five possible
responses. The resulting variable was treated as a process variable.
Internal Communication
In the Additional Team Information survey, team leaders were asked two
questions to indicate (a) how much team members had access to information
other than that conveyed in meetings, for example, with the use of memos,
whiteboards, newsletters; and (b) how much social activity team members
participated in together. Responses were combined to give a measure of the
CMHT’s intent to communicate both informally and socially, on a scale of 1
(poor) to 5 (high quality effort to communicate). Figure 5.7 shows how teams
varied on this dimension, which was treated as a team process variable.
Figure 5.7: CMHTs' Intent to Communicate

interdisciplinary communication
4 and above3 to 42 to 31 to 2
num
ber
of te
ams
50
40
30
20
10
0
Turnover
In the Additional Team Information survey, team leaders were asked to indicate how
many staff had left the team in the previous 12 months. Turnover was computed as
the percentage of staff in the team (size) who had left, and was treated as an
outcome variable.

Relationships between ‘input’ dimensions
Team size
Figure 5.8: Scatterplot of CMHT climate against team size
team size going by team members declared
6050403020100
self
repo
rt: c
ombi
ned
TC
I sca
les
4.5
4.0
3.5
3.0
2.5
2.0
Three CMHTs were larger than all others, and scatterplots (e.g. Figure 5.8)showed that on some dimensions of team functioning these were outliners.They were removed from all analysis involving team size. Team size wasclearly associated with the diversity of disciplines within the team: largerteams were more likely to have psychiatrists (r = .20, p < .05) andpsychologists (r = .25, p < .01). Larger teams also had a lower percentageof full-time staff (r = -.22, p < .05). Team size was associated with only oneaspect of the team’s task or organisational environment: larger CMHTs weremore likely to operate a waiting list for assessment,r = .29, p < .01.
Team average age
The average age of the CMHT was likely to be greater if social workers (r =.30, p < .01) and psychologists (r = .25, p < .01) were members. However,it was likely to be lower if the MINI score of deprivation was high (r = -.36, p< .001).

Team average tenure
Average job tenure was lower if there were social workers in the team (r = -.20, p <
.05). Predictably, average job tenure was strongly associated with the length of time
the team had been in existence (r = .51, p < .001).
Length of time CMHT in existence
Beyond the relationship with average job tenure in the team, the life of theteam was associated with whether it operated at separate sites (r = -.23, p <.05), that is, the longer the team had been in existence, the less likely was itthat staff were based at different locations.
Percentage of full-time workersWe saw above that larger teams were likely to have a higher percentage ofpart-time workers. Such part-time practitioners were likely to be psychiatrists(r = -.26, p < .01), psychologists (r = -.31, p < .01) and occupationaltherapists (r = -.28, p < .05). Although they described themselves as being‘part-time’, these disciplines may well have divided their time between theCMHT in question and other responsibilities.
Percentage of women in the team
A lower percentage of women in the team was associated with a higherdeprivation rating, R = .21, p < .05.
Further effects of team composition
When psychiatrists were in the team, it was less likely that the team would implement
a single, integrated set of case notes for each client (R = -.32, p < .01), but if an
occupational therapist was in the team, the opposite was the case (R = .31, p < .01).
Again, psychiatrists were more likely to be in the team if the deprivation rating was
high (R = .23, p < .01). If there were social workers in the team, emergencies were
likely to be seen more quickly (R = -.27, p < .05). The team was more likely to
operate a waiting list for assessment if there were social workers (R = .28, p = .01),
psychologists (R = .23, p < .05) or occupational therapists (R = .23, p < .05) in the
team.
Further effects of clinical system implementation
Where the team pooled referrals at a central point, they were also likely to operate a
single, integrated set of case notes for each client (R = .25, p < .05), although a
single referral point was also associated with lower deprivation scores (R = -.29, p <

.01). Where the deprivation score was higher, waiting lists for assessment were less
likely to be in place (R = -.26, p < .05).
Intensive analysis
Selection procedure
Teams rating themselves as highly effective or as highly ineffective, incomparison to the self-ratings of the full sample of 113 teams, were selected.This recruitment strategy was designed to maximise the power of between-team analyses to detect associations between intensive analysis variables andeffectiveness. We computed aggregate team scores on the CMHTteamworking questionnaire scales. These comprised the Team ClimateInventory (TCI) participation, support for innovation, and task orientationscales; the user orientation, use of resources, and internal process scalesfrom the service delivery effectiveness (SDE) items; and the 12-item GHQ.The standardised team scores on the TCI and the SDE were summed, and thestandard team score on the GHQ-12 subtracted from this total. Thisalgorithm yielded 14 teams above the 80th percentile and 14 below the 20thpercentile. To achieve a target sample size of 16 teams in this phase of thestudy, all 28 were invited to participate after the team had gained consensusamongst members. Ten volunteered, distributed across the 4 NHS regions asfollows: A, 3; B, 2; C, 1; and D, 4. MINI scores for the 10 teams covered awide range, 91.3 to 110.0, with a mean of 101.4. Three of the 10 had ratedtheir activity as effective, leaving 7 who rated their team as ineffective. Wefollowed up the 4 teams rated as effective which had not already responded,but failed to increase the number. To a considerable degree, therefore, thiswas a self-selected sample. The 10 teams comprised three self-rated as‘effective’ and seven self-rated as ‘ineffective’.
Representativeness of sub-sample CMHTs
Independent t-tests were used to compare group means on appropriate dimensions,
together with Levene’s test for equality of variances. This process included
comparisons for:
§ Team characteristics and composition: size; age; tenure; percentage of full-time
workers in the team; percentage of men in the team; length of time the team had
been in existence; professional mix.
§ Task environment: MINI; number of GP’s linked to the CMHT; ; whether the team
held a single, integrated set of case notes for each client; whether referrals were
pooled or not; use of a waiting list for emergency referrals.

§ Team processes: team processes scale; perceived clarity of leadership; intent to
communicate informally; amount of meeting time available; perceived quality of
relationship with GP’s, Health Trust, and Social Services.
§ Team effectiveness: levels of stress; self-report effectiveness; external judges’
ratings of performance; external judges’ ratings of team innovations; self-report
innovativeness; turnover.
For the most part, group means were similar, with t values ranging from .07 to 1.65.
Exceptions are shown in Figure 5.9. Levene’s tests for equality of variances did not
reach significance for any dimension.
Figure 5.9: Significant differences between survey sample and sub-sample
Surveysample mean
(SD)
Sub-sample mean(SD)
T value probability
Percentage offull-time staff
78.48 (13.27) 67.28 (15.09) 2.52 .01
Average tenureof staff (months)
38.66 (18.89) 24.62 (20.39) 2.23 .03
Psychologist inthe CMHT
0.34 (0.48) 0.80 (0.42) 3.26 .007
CMHT stresslevel (GHQ)
0.96 (0.16) 1.09 (0.20) 2.20 .03
External ratingsof CMHTeffectiveness*
3.59 (0.38) 3.25 (0.47) 2.07 .05
* The Ns on this dimension were 25 in the survey group, 8 in the sub-sample group
These comparisons showed that, in relation to most team characteristics, and most
aspects of task environment, team process and effectiveness, the sub-sample group
did appear to be reasonably representative of the full survey sample. However, sub-
sample teams had a lower percentage of full-time staff, their members were likely to
have been in the team for a shorter time, were more likely to have a psychologist or
counsellor in the team, their members experienced a higher level of stress, and
teams were rated lower on effectiveness by external judges. This last finding is not
surprising, given that more self-ratedly ineffective than effective teams had
volunteered to take part in this phase of the research. Chi-square tests showed that
the sub-sample teams were representatively distributed throughout the 4 NHS
regions, but were not representatively distributed in terms of local commissioning

arrangements, chi square = 6.33, p < .05, with 7 teams being jointly commissioned
by Health and Social Services, and 3 by the Health Service only.
Descriptives on the 10 CMHTs in the intensive phase
Figure 5.10 shows the characteristics of the ten teams. All had CPNs, all were
multidisciplinary, although only 3 of the 10 teams had access to psychiatry input
within the team.
Figure 5.10: Team characteristics of sub-sample CMHTs
TeamA
TeamB
TeamC
TeamD
TeamE
TeamF
TeamG
TeamH
Team I Team J
Size 16 12 15 15 22 12 18 17 46 12
Mean age 44.9(11.70)
37.1(7.43)
34.6(7.94)
41.2(7.22)
38.2(7.44)
40.4(8.05)
45.2(6.45)
41.9(8.02)
43.3(9.85)
41.0(8.43)
Mean tenure(months) 13.58 23.56 21.07 35.73 10.55 12.00 9.80 3.85 47.11 69.00Length of life ofCMHT
Less than2 years
2 to 5years
2 to 5years
Over 5years
Lessthan
2years
Lessthan
2years
Lessthan
2years
Lessthan
2years
2 to 5years
Over5 years
Psychiatry in No no no Yes no no No No yes yesOT in Yes yes yes Yes yes no Yes No yes yesPsychology in Yes yes yes Yes no no Yes Yes yes yesSW in Yes no no Yes yes yes Yes Yes yes yes% men 33 38 15 27 36 62 27 23 37 42% full-time 83 56 54 55 64 100 60 77 67 58MINI 97.4 110.0 110.0 91.3 96.6 94.8 97.4 102.6 - 104.2Linked GP’s 34 38 26 30 - - 24 35 120 35Commissioning H & S
jointlyH
onlyH
onlyH & Sjointly
H & Sjointly
H & Sjointly
H & Sjointly
H & Sjointly
H & Sjointly
H only
NHS region B A A B C B B C D A
It is apparent that there were differences between the teams on all structuraldimensions. For example, team 1 stood out as a large team compared withothers, and teams B and C were in Health Authorities which had a higherMINI score than others, indicating localities with higher deprivation. All teamshad a mix of disciplines, although team F had only social work input, over andabove the CPNs who were present in all teams. Percentages of male and full-time workers in these teams varied widely. Half of the teams had been inexistence for less than 2 years, and this partly accounted for shorter tenure ofstaff, although there is commonly high turnover of staff in the CMHTenvironment.
Audio and video recording of Community Mental Health Team meetings
The ten teams volunteering for the intensive stage research also agreed that their
meetings could be recorded; meeting sizes ranged from six to twenty five members.
The meetings were multi-disciplinary business meetings in which decisions were

made about the running of the team. This meeting was chosen by the teams as the
one to record because it is the main forum, outside clinical meetings, that are multi-
disciplinary meetings. Wherever possible, we recorded two meetings of the same
type for each team. Dates for meeting recording were at the discretion of the CMHT.
For details of recording procedures, equipment and transcription see Chapter 2.
Longitudinal data collection: clinical outcomes; use of resources; patient andcarer satisfaction
Two site visits six months apart were arranged with each participating CMHT. Before
the first, every practitioner in the team completed a caseload audit summary to define
as precisely as possible the population the CMHT was serving (Manchester Audit
Tool, recommended by the Kings Fund mental health team). This required a
breakdown by 19 classifications of the care worker’s entire current caseload in terms
of diagnosis, severity, complexity and chronicity. Simple guidelines for completing
the audit questionnaire were included. For the purposes of patient selection, an
individual breakdown was also completed by each practitioner, using either codes or
names. Stratified sampling was carried out by the research team using SPSS
random number generation. Stratification ensured that users selected were
representative of (a) the individual practitioner’s caseload; and (b) the team’s entire
caseload profile. Stratification was based on scores provided by practitioners for
each client for severity, chronicity and complexity. Scores were then summed. For
each of the 10 teams, 40 users were selected.
If practitioners indicated that clients were unable to complete a questionnaire,
because they were in an acute episode, or could not read, or did not read English
well, they were replaced by others on the key worker’s caseload matched for
stratification. Packs of information sheets, consent forms and return envelopes were
sent to each key worker for each of their selected clients (and carers where
appropriate). Practitioners were requested to discuss the research with clients and
hand them information and consent form, and for the purposes of confidentiality, to
ask them to send signed consent direct to the research team. Once the research
team had received signed consent from client or carer, Patient/Carer Service
Satisfaction questionnaires were sent out, to assess the effectiveness and
acceptability of the service received, and users’ quality of life. The questionnaire was
that developed by the Tameside & Glossop Rehabilitation team, who gave
permission for its use.

First site visit
Two researchers visited each team for a day to interview all practitioners with a
caseload. At the interview, practitioners answered questions about each of their
selected clients individually. Biographical data were collected: gender, age ethnic
origin, type of housing, and whether they had a formal carer. Questions relating to a
period of the previous 6 months covered use of resources, for example, types and
dosage of psychoactive medication, day hospital attendance, number of contacts
with CMHT professionals, time spent as an in-patient. Other questions covered
referral, diagnosis, CPA level, care plan targets, whether or not the client was on
section, and projected clinical outcomes for 6 months ahead. Practitioners were
provided with 6 HoNOS forms for each client, to be completed by the practitioner at
each contact over the following 6 months, or up to discharge.
Second site visit, after an interval of 6 months
Self-report key worker schedules were designed, following the model of the
practitioner interviews implemented at the first site visit. The schedules were sent
two weeks in advance of the visit to the site to collect completed schedules and
HoNOS questionnaires, and respond to queries. All team members completed the
survey questionnaire for a second time, so that change over time could be measured.
The costs of use of resources were computed by combining estimates of quantity
and cost per unit. Medication costs were based on the 1997 BNF. Contact costs
were based on Unit Costs of Health and Social Care (Netten & Dennett, 1997).
Elements included in the costs were medication, inpatient days, day hospital
attendance, respite care, day centre use, drop-in use, occupational therapy groups,
outpatient attendance and contacts with CMHT staff.
Data analytic strategy
Psychometric Considerations
The self-report measures of community mental health team process and
effectiveness used in this research were complex and novel. Accordingly, prior to
analysis to address the substantive questions listed above, preliminary psychometric
analysis considered the intercorrelations among these measures at the team level.
Specifically, the extent of specificity vs. redundancy in these measures had not
previously been assessed. To be useful in testing theories relating team processes to
effectiveness, the measures would have to demonstrate sufficient specificity that the
relationships among them not be most parsimoniously explained as reflecting a

single evaluative or morale factor. As shown in Figure 5.11, all intercorrelations were
significant and substantial, ranging from .53 to .89.
Figure 5.11: Team-level correlations among self-report measures of CMHT processand effectiveness
TCI:participation
TCI:support
forinnovation
TCI:clarity of
objectivesreflexivity innovation
CMHTEQ:external
requirements
CMHTEQ:internal
processes
TCI: support for innovation .858TCI: support for innovation .858TCI: clarity of objectives .633 .771TCI: clarity of objectives .633 .771Reflexivity .706 .816 .706Reflexivity .706 .816 .706innovation .531 .743 .662 .732innovation .531 .743 .662 .732SDE: external requirements .642 .701 .652 .566 .526SDE: external requirements .642 .701 .652 .566 .526SDE: internal processes .818 .889 .791 .744 .671 .842SDE: internal processes .818 .889 .791 .744 .671 .842SDE: monitoring/evidence .555 .676 .620 .578 .551 .878 .777SDE: monitoring/evidence .555 .676 .620 .578 .551 .878 .777
All correlations have N = 113, p < .01.

We therefore considered whether the effectiveness of a team as reported by its
members could be distinguished from its climate, also as reported by those same
team members. We entered team means on the four Team Processes Inventory
(TCI) scales and the three SDE scales in a factor analysis. This indicated that a
single factor was the most efficient way to describe the differences among the teams;
attempts to force a two-factor solution did not support a distinction between team
processes and self-reported effectiveness, as the scales with highest loadings on
each factor comprised a mixture of both TCI and SDE scales.
External ratings of effectiveness were available for 33 teams. For this subsample,
we considered whether external ratings of effectiveness were any more highly
correlated with self-reported effectiveness than with the TCI. There was no such
difference. External ratings of effectiveness were as highly correlated with team
members’ ratings of team processes, r = .64, as with their reports of team
effectiveness, r = .60.
The quality of innovations described by the members of all 113 teams was rated by
external judges. These ratings were no more strongly correlated with team
members’ TCI ratings, r = .44, than with their reports of the team’s effectiveness, r =
.39. Considering only the most relevant TCI scale, support for innovation was
correlated at r = .48 (indistinguishable from the overall TCI correlation of .44) with
external ratings of innovation. The fact that the TCI correlates rather more highly, at r
= .64, with external ratings of team effectiveness than with external ratings of
innovations, r = .44, is further evidence against specificity. Meanwhile, self-reported
innovation (considered an effectiveness dimension) correlated very similarly at r =
.55 with external ratings of innovation.
These analyses rather suggest that the self-report measures should be most
parsimoniously considered to reflect a single evaluative or morale factor, rather than
to tap specific aspects of team process or effectiveness. The measures may not,
therefore, be sufficiently precise to reveal subtle relationships between CMHT
process and effectiveness.
Sequencing of Multivariate Analyses
Analysis proceeded in two steps. First, the questions identified above were
addressed in sequence. For each dependent variable in turn, potential predictor
variables were entered in groups. For example, for each team process variable in

turn, team characteristics were entered as one set of predictors, before moving on to
a second analysis looking at team composition factors as predictors, a third analysis
with team task factors as predictors, and a fourth with organisational context factors
as predictors.
Secondly, for each class of dependent variables in turn, variables that had emerged
from the foregoing analyses as showing predictive relationships independent of the
other variables in their respective group were entered into new analyses including all
such variables across the groups. Analyses at this second step identified predictors
that were independent in their effects of other significant predictors across all classes
of predictor. Such predictors warrant closer attention; accordingly, this account of
our findings will emphasise this second phase of the analysis.
In the next chapter we describe the results of these analyses.

Chapter 6
Community Mental Health TeamsResults from Survey and External Ratings
Summary of Findings
• Teams whose members were more positive about team processes are rated
as more effective by external stakeholders
• Teams whose members agree as to how clearly the team leadership role is
defined are rated by external stakeholders as more effective
• Teams whose members describe their team processes positively perceive
their teams as more effective
• Teams whose members report clarity as to the leadership role perceive
their teams as more effective
• Teams that have been in existence for a relatively long time tend to
describe their team as more effective
• Larger CMH teams are rated as more innovative by external judges
• Teams who perceive their performance as highly reflexive are rated as
more innovative by external judges
• Teams who perceive their team processes and reflexive behaviour as
positive also see themselves as more innovative
• Teams who perceive their team processes as poor experience higher
levels of stress
• Teams with older members enjoy more stable membership, as do teams
including social workers

• Teams using integrated client case notes, and teams not including
psychiatrists, are clearer about the leadership role
Introduction
Our analysis was informed by the input-process-outcome model presented in
Chapter 1. This entailed predicting process variables from input variables, and
predicting outcome variables from both input and process variables.
As for the analysis of PHCTs, we addressed two main questions:
• Is there an association between the composition of a community mental
health team and team processes?
• Is there an association between the composition and processes of the
community mental health team and the effectiveness of the team?
The team characteristics, team processes and measures of team effectiveness are
summarised in Figure 6.1.

Figure 6.1: Team Inputs, Processes and Effectiveness Variables
Characteristics Processes Effectiveness
IndividualAgeGenderTime in jobTime in teamTime in team
TeamOccupational groupsSize (number of members)Number of GP'sHours workedMultidisciplinary mixGender mix
Team contextCommissioning typeMINI indexUse of integrated casenotesResponse time foremergenciesWaiting list in operationNHS RegionRelationship with SocialServicesRelationships with GP'sRelationship with Trust
Team processesParticipationInnovationObjectivesEmphasis on qualityReflexivityNumber of meetingsTypes of meetingsFrequency of meetingsPotential time for differentdisciplines to meetDecision makingLeadershipIntegration andcommunication in the group
Team ratingsOrganisationTeam workingPatient focusInnovation
External ratings (innovation)MagnitudeRadicalnessNoveltyImpact
External ratings (effectiveness)OrganisationTeam workingUser/carer focus
Types of InnovationsQuality of CareExternal collaborationResponsibility for healthUse of resourcesProfessional developmentTeam satisfactionResponsivenessStress (GHQ 12)Turnover
Team processes
Individual team members rated team processes on six dimensions: participation;
innovation; team-objectives; emphasis on quality; reflexivity; and interdependence.
Information about decision-making processes, communication, number and types of
meetings, who attended these meetings, and how the team was managed was
collected from Practice Managers. The information on team meetings was
categorised according to who contributed to operational, strategic and clinical
decisions. In addition a new variable ‘integration’ was developed which assessed the
extent to which there were mechanisms within the team to encourage inter
disciplinary communication and working.

Team Inputs
Information about the team members’ ages, gender, ethnicity, professional group,
tenure and team leadership were collected from each team member. Information
was also gathered on team size, hours worked, commissioning type, MINI index,
NHS Region, whether the CMHT made use of a single integrated set of client case
notes, how long the team took to respond to emergency referrals, whether they
operated a waiting list for assessment, and the team’s relationships with GP’s, Trust
and Social Services.
Team Processes
Individual team members rated team processes on six dimensions: participation;
support for innovation; clarity of team objectives; emphasis on quality; reflexivity; and
integration. The variables participation, support for innovation, clarity of team
objectives and emphasis on quality were very highly correlated and were combined
to form one variable describing team processes. Information about decision-making
processes, communication, number and types of meetings, and who attended
meetings was collected from team leaders. An index of the amount of time the
various disciplines in the team could potentially meet was computed. In addition, a
new variable ‘integration’ was developed which assessed the extent to which there
were mechanisms within the team to encourage interdisciplinary communication.
Team Effectiveness
As with PHCTs, this was assessed using information from a variety of sources.
Team members rated their teams’ effectiveness on the three dimensions of the
Community Mental Health Team Effectiveness Questionnaire (CMHTEQ; Rees,
Stride, Shapiro, Richards & Borrill, in press), developed within this project: team
working; organisational efficiency; and patient orientation. Team members also rated
their teams’ innovativeness and described the innovations implemented by the team
in the previous year. External raters assessed the innovations reported by the teams
on four dimensions: magnitude; radicalness; novelty and impact on team
effectiveness. External ratings of team effectiveness on the CMHTEQ were provided
by external experts nominated by the team and based in local GP practices, Social
Services, the Trust or Health Authority. Individual team members also completed the
GHQ-12 (a measure of mental health or psychological stress). The measures of
interest for this report are overall effectiveness of the team in delivery of services,
user-centred care and dealing with the demands of the parent organisation (both
externally rated and self rated), overall innovation (both externally rated and self

rated), team turnover, and mental health measured by the GHQ-12.

Results
The method of analysis was similar to that described for the PHCT data in Chapter 3.
Stepwise multiple regressions were carried out, with possible predictors of each
dependent variable being split into groups according to type of variable, to identify
those which might ultimately predict the dependent variable. As with the PHCT
analysis of Chapter 3, to reduce the complexity of the data set and to guard against
Type 1 errors arising from multiple statistical tests, we focused on a second-level
analysis combining predictors across the groups. Process variables were predicted
by team characteristics or “inputs”; and effectiveness, innovation, turnover and
mental health were conceptualised as “outcomes” predicted by team characteristics
(“inputs”) and by team processes. In a final stage of the analysis, both team
characteristics (inputs) and team processes were considered together as predictors
of the outcome variables (effectiveness, innovation, turnover and mental health).
We found that the CMHT data called for a different approach to the issue of team
size than we adopted for the PHCT data. It transpired that the relationship between
team size and other variables was largely due to 3 outlying teams (with more than 36
members). Accordingly, rather than considering team size first in all analyses as we
had done with the PHCT data, we excluded these teams from analyses including the
size variable, and thereafter treated team size in the same way as other team
characteristics.
Question 1 – Is there an association between the composition of a CMHT and team
processes?
Figure 6.2: Relationships Between Team Composition and Team Processes
Dependent variable Predictor variables β p R2
Consensus on leadership Team size -.250 .017Tenure -.215 .039 .097
Reflexivity Presence ofpsychiatrist(s)
-.225 .018 .042
Integration noneTeam processes nonePotential to meet noneNumber of meetings Tenure .212 .046 .045
Figure 6.2 presents the significant team composition predictors of each team
process variable. Larger teams, and teams whose members had been longer

in their jobs in the team, showed less consensus on the clarity of leadership in
the team. Teams including psychiatrists as members were less reflexive. The
tabled result was obtained after excluding the responses of psychiatrists
themselves, which had inflated the observed relationship. This, our preferred
analysis, is more conservative because it excludes the effect of the tendency
of psychiatrists themselves to rate the team as less reflexive. It may therefore
be interpreted as showing an association, albeit modest, between the
reflexivity ratings of non-psychiatrist team members and the presence of
psychiatrists within the team.
Question 2 – What Affects the Effectiveness and Innovativeness of a Community
Mental Health Team?
Figure 6.3: Relationships Between TeamComposition and Processes, and Ratings ofEffectiveness
Dependent variable Predictor variables β p R2
Overall effectiveness(external)
Team processes .643 <.001 .413
Consensus onleadership
-.311 .046 .487
Overall effectiveness (self-rated)
Team processes .861 <.001 .742
Consensus onleadership
.163 .003 .766
Length of time the teamhad been in existence
.121 .020 .780
As shown in Figure 6.3, two variables predicted, independently of one another, the
ratings of CMHT effectiveness given by their local stakeholders: team processes and
lack of consensus relating to team leadership. In other words, teams whose
members rated their team processes favourably, and teams whose members agreed
amongst themselves as to how clearly the leadership role was defined within the
team, were rated by external stakeholders as more effective. Figures 6.4 and 6.5
below show these predictive relationships graphically.

Figure 6.4: Impact of team processes onexternally-rated team effectiveness(data from 32 CMHTs)
Team Processes
5.04.54.03.53.02.52.0
5.0
4.5
4.0
3.5
3.0
2.5
2.0
Figure 6.5: Impact of clarity of leadership onexternally-rated team effectiveness (data from32 CMHTs)
clarity of team leadership
1.21.0.8.6.4.20.0-.2
exte
rnal
rat
ing
of te
am e
ffect
iven
ess
5.0
4.5
4.0
3.5
3.0
2.5
2.0
Figure 6.3 also presents the three factors predicting self-reported team effectiveness
on the 27-item Community Mental Health Team Effectiveness Questionnaire
(CMHTEQ), each independently of the other two: Overall score on the Team

processes Inventory, as shown in Figure 6.6; clarity of leadership, as shown in Figure
6.7; and the length of time the team had been in existence, as shown in Figure 6.8.
In other words, members of teams whose members described their processes
positively, members of teams whose members reported clarity as to the leadership
role, and members of teams that had been in existence for a relatively long time, all
tended to describe their team as more effective.
Figure 6.6: Impact of team processes on self-reported effectiveness (data from 113 CMHTs)
team processes
4.54.03.53.02.52.0
4.5
4.0
3.5
3.0
2.5
2.0
Figure 6.7: Impact of clarity of leadership on self-reported effectiveness (data from113 CMHTs)

clarity of team leadership
1.21.0.8.6.4.20.0-.2
4.5
4.0
3.5
3.0
2.5
2.0
Figure 6.8: Impact of length of time team inexistence on self-reported effectiveness (datafrom 113 CMHTs)
Length of time team in existence
5 or more years2 to 5 years2 years or less
4.0
3.9
3.8
3.7
3.6
3.5
3.4
3.3
3.2
3.1
3.0
3.5
3.4
3.3
Relationships between Team Composition and Processes, and Ratings ofInnovation

As shown in Figures 6.9 and 6.10, two variables predicted, independently of one
another, the quality of the innovations reported by team members as rated by
independent, expert judges: Reflexivity, beta = .51, t = 6.72, p < .001; and team size,
beta = .38, t = 5.00, p < .001. In other words, teams whose members rated their
teams as highly reflexive, as well as larger teams, described innovations that were
judged to be of higher quality.
Figure 6.9: Impact of reflexivity on expertratings of innovation quality (data from 113CMHTs)
reflexivity
6.05.55.04.54.03.53.02.5
exte
rnal
rat
ing
of te
am in
nova
tions
5
4
3
2
1
0
Figure 6.10: Impact of team size on expertratings of innovation quality (data from 113CMHTs)

team size
403020100
exte
rnal
rat
ing
of te
am in
nova
tion
5
4
3
2
1
0
Three factors, acting independently of one another, were associated with the
innovativeness reported by team members: self-reported reflexivity, beta = .45, t =
3.75, p < .001, as shown in Figure 6.11; overall score on the Team Processes
Inventory, beta = .32, t = 2.65, p = .009, shown in Figure 6.12; and freedom of
interaction (scheduled co-presence of the different disciplines at meetings), beta = -
.15, t = -2.20, p = .03. In other words, teams whose members reported a high level
of reflexivity, teams whose members reported team processes as positive, as well as
teams scheduling relatively little cross-disciplinary interaction in formal meetings, all
tended to be described by their members as relatively strong with respect to
innovation.

Figure 6.11: Impact of team reflexivity on self-reported innovativeness (data from 113CMHTs)
team reflexivity
6.05.55.04.54.03.53.02.5
inno
vativ
enes
s
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
Figure 6.12: Impact of team processes on self-reported innovativeness (data from 113 CMHTs)
team processes
4.54.03.53.02.52.0
inno
vativ
enes
s
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
Relationships between Team Composition and Processes, and Stress Levels inCMHTs
Three variables predicted, independently of one another, the level of stress reported
by team members on the General Health Questionnaire: Team processes (overall
score on the Team Processes Inventory), beta = -.50, t = -5.22, p < .001; informal
communication (social events, message boards, etc.), beta = .21, t = 2.20, p = .03;
and freedom of interaction (scheduled co-presence of the different disciplines at

meetings), beta = -.20, t = -2.20, p = .04. These findings indicate that the following
team characteristics are associated with relatively high stress (or low stress levels)
amongst staff: a positive team processes; plentiful opportunities for informal
interaction among members; and relatively little provision for scheduled, formal,
cross-disciplinary encounters at team meetings. Figure 6.13 shows the impact of
team processes on stress.
Figure 6.13: Impact of team processes on stress
team processes
4.54.03.53.02.52.0
1.6
1.4
1.2
1.0
.8
.6
GHQ = General Health Questionnaire, 12 item version
Relationships between Team Composition andProcesses, and Turnover in the team
As shown in Figures 6.14 and 6.15, two compositional variables predicted staff
turnover, independently of one another: mean age of team members, beta = - .25, t =
-2.21, p = .03; and the presence of social workers in the sample of respondents, beta
= -.23, t = -2.02, p = .05. These findings suggest that teams with older members
enjoyed more stable membership, as did teams including social workers.

Figure 6.14: Impact of mean age of teammembers on turnover (data from 113 CMHTs)
team processes
4.54.03.53.02.52.0
1.6
1.4
1.2
1.0
.8
.6
Figure 6.15: Staff turnover in CMHTs with andwithout social workers (data from 92 teams)
social workers in the team
yesno
20
15
10
5
0
8
15
Relationships between Team Composition and
Leadership

Two factors, acting independently of one another, were associated with the clarity of
leadership described by team members: the use of a single, integrated set of case
notes for each client, beta = .29, t = 2.85, p = .006, as shown in Figure 6.16; and the
presence of one or more psychiatrists amongst team members completing the
questionnaire, beta = -.27, t = -2.63, p = .01, as shown in Figure 6.17. It should be
noted that, before computing the mean clarity of leadership for each team, responses
from psychiatrists themselves were removed from the latter analysis. In other words,
teams using integrated case notes, and teams not including psychiatrists, were
clearer about the leadership role.
Figure 6.16: Integrated case notes and clarity ofleadership (data from 92 CMHTs)
Use of one integrated set of case notes
Yespartial accessNo
.8
.7
.6
.5
.4
.8
.7
.5
Figure 6.17: Psychiatric membership of the team and clarity of leadership (data from113 CMHTs, with responses of psychiatrists themselves removed from the analysis)

psychiatrists in the team
yesno
.8
.7
.6
.5
.4
.5
.7
Discussion
As for primary health care teams, the findings from this stage of the research reveal a
clear message for CMHT policy and practice, in relation to the factors predicting the
effectiveness and innovations of community mental health teams: positive team
processes, and clarity as to the leadership role within the team, make for a more
effective team, as judged by external stakeholders as well as the team members
themselves; requisite size makes for a higher quality of innovation; reflexive
processes aids innovation; longer-established teams are rated more innovative by
external judges and see themselves as more effective.
We have considered policy implications of the findings reported in this chapter in
relation to the Workforce Action Team issues identified in Chapter 1. In terms of
education and training, it is clear that teamworking skills are key to the effective
delivery of mental health care in the community. These skills are specific and
trainable. They are not acquired implicitly through professional socialisation into
such disciplines as nursing, medicine, clinical psychology, or social work. Nor are
they attained through unfocussed, unsustained “team-building” exercises of the kind
that are widely marketed into the NHS and other large organisations. Rather, they
comprise key types of knowledge, skill and ability required for effective teamworking
(Stephens & Campion, 1994). As depicted in Figure 6.18, these fall into 5 domains:
conflict resolution; collaborative problem-solving; communication; goal-setting and
performance management; planning and task co-ordination. Both initial professional
training and continuing professional development for CMHT members should
incorporate systematic training in these. To prepare and enable members of the
constituent professions to function effectively within CMHTs, the NHS should require

that the majority of such training should be delivered in multiprofessional rather than
uniprofessional learning environments. The requirement for such delivery may
create difficulties for HEI’s but the NHS should work with them to ensure that training
funded by the NHS meets the NHS’s pressing requirements for effective
multiprofessional teamwork.

Figure 6.18: Knowledge, Skill and Ability Requiredfor Effective Team-working (Stephens & Campion,1994)
Conflict resolution:• Recognise and encourage desirable but discourage undesirable team
conflict• Recognise type and source of conflict confronting the team and implement
appropriate resolution strategy• Employ integrative (win-win) negotiation strategy rather than traditional
distributive (win-lose) strategy
Collaborative problem-solving:• Identify situations requiring participative group problem solving and utilise
proper degree and type of participation• Recognise obstacles to collaborative group problem solving and implement
appropriate corrective actions
Communication:
• Understand networks and utilise decentralised networks to
enhance communication where possible• Communicate openly and supportively, sending messages which are (1)
behaviour - or event-oriented; (2) congruent; (3) validating; (4)conjunctive; and (5) owned
• Listen non-evaluatively and appropriately use active listening techniques• Maximize consonance between nonverbal and verbal messages, recognise
and interpret the nonverbal messages of others• Engage in ritual greetings and small talk, and recognition of their
importance
Goal-setting and performance management:• Help establish specific, challenging and accepted team goals• Monitor, evaluate, and provide feedback on both overall team performance
and individual team member performance•
Planning and task co-ordination:
• Co-ordinate and synchronise activities, information and task
interdependencies between team members• Help establish task and role expectations of individual team members and
ensure proper balancing of workload in the team
Stephens, M.J., & Campion, M.A. (1994). The knowledge, skill and abilityrquirements for teamwork: Implications for human resource management. Journal ofManagement, 20, 503-530.

In relation to recruitment and retention, we note the disturbing fact that only 12% of
our CMHTs included all 5 key disciplines: nursing, psychiatry, social work,
occupational therapy, and clinical psychology. This presents a challenge to effective
delivery of the full spectrum of mental health care, and confirms the importance of the
Workforce Action Team’s agenda. In that context, we draw attention to certain
features of the demographics of CMHT staff identified by this research. Sixty-seven
per cent of CMHT staff were women; the mean age of the staff was 40, with a
standard deviation of 8.4 years, and most workers aged between 30 and 50. This
profile highlights the importance of flexible working to accommodate family demands
and thereby retain staff. It also confirms the importance of retaining CMHT staff
beyond the age of 50. Within the somewhat restricted age range we observed,
teams with older members experienced less turnover. Turnover was greater among
smaller teams, suggesting that teams should be large enough to provide sufficient
support. Our findings implicate poor team processes in CMHT staff stress, which is
likely to be inimical to staff retention. Longer-established teams rating themselves as
more effective suggests that stability of the team itself may yield greater job
satisfaction through the experience of effectiveness.
In relation to leadership, we see this as a key and integral feature of team functioning
and hence, as shown by our data linking team processes to effectiveness, vital to the
delivery of effective mental health care. We found that clarity in relation to the
leadership role was reflected in external ratings of CMHT effectiveness, as well as in
team members’ own ratings of their team’s effectiveness. Clear and effective
leadership will be essential to delivery of the National Service Framework, and
development of the required leadership skills, which are learnable irrespective of
professional discipline, will require training resources. Training for CMHT leadership
must relate to the complex multi-agency environment, and combine clarity with
flexibility and innovativeness. Such training needs to be evidence-based, locally
available, and ongoing rather than occasional or intermittent.
In relation to primary care delivery of mental health care, we draw attention to
findings from Chapter 3 highlighting the benefits of larger PHCTs, and of a wide
spectrum of professions being members of the PHCT, alongside the value of clear
PHCT leadership. In the course of our PHCT research we obtained ample anecdotal
evidence that PHCT members are highly aware of the challenges presented to them
by their growing responsibilities in this area.

In relation to the Workforce Action Team’s interest in developing the role of
professionally non-affiliated staff in mental health care delivery, we have some
indicative findings on support workers within CMHTs. They comprised 7% of
respondents to our survey, and 75% of them were female. Their ratings of their
teams were very favourable, and interviews with them during the intensive analysis
reported in Chapter 7 were highly positive in tone. The intensive analysis also
revealed the considerable dependence of CMHTs on support workers for the time-
intensive, practical aspects of care of patients with severe and enduring mental
health problems. Accordingly, we strongly endorse the development of
professionally non-affiliated staff as a resource within CMHTs.

Chapter 7
Community Mental Health TeamsResults from Qualitative Research
Summary of findings
• Basic minimum standards of staffing and hence care are not yet universally
fulfilled by NHS mental health care
• The costs of mental health care vary across teams providing it, over and
above the apparent clinical requirements of the caseload as reflected in
diagnosis and severity
• CMHTs face conflicting demands from primary care and from the needs of
patients with severe and enduring mental health problems
• Venturing beyond our immediate data, we suggest that such key issues are
likely to have important effects on the morale, stress and effectiveness of
CMHT staff and on their capacity to initiate and maintain the innovative,
collaborative and flexible patterns of teamworking whose importance is
highlighted by our survey findings
Sub-sample team characteristics
In this section, we report an analysis of the sub-sample of CMHTs taking part in the
second phase of the project. In this qualitative work we looked in greater depth at
CMHT effectiveness by taking account of clinical and economic performance. Its
objectives were:
• To develop methods to assess the economic costs and clinical outcomes for
a representative patients seen by a CMHT
• To examine the relationships between task context (severity of caseload),
inputs (time, costs), team processes, and outputs (clinical improvement, goal
attainment and CMHT practitioner stress)
Process and effectiveness dimensions of the 10 teams

Figure 7.1 gives the aggregated team means for the primary process and
effectiveness variables.
Teams were selected for the second phase of the research on the basis of combined
standardised team processes scores, self report effectiveness score, and stress
levels (see Chapter 5). Figure 7.1 shows that the 10 teams varied on the
performance dimensions as ‘effective’ or ‘ineffective’: Teams B, G and J perceived
their teams as performing effectively, but this was only partly supported by external
judgements of team performance, in which innovativeness, but not effectiveness,
was rated highly for those teams.

Figure 7.1: Process and effectiveness dimensions of the 10 CMHTs
TeamA
TeamB
TeamC
TeamD
TeamE
TeamF
TeamG
TeamH
TeamI
TeamJ
OverallTeamprocessesMax = 5
2.95 3.85 3.20 2.96 3.06 3.46 4.24 3.30 2.92 3.94
Number ofmeetingsMax = 11
2 5 3 2 4 5 2 5 5 1
Multi-disciplinarycommunicationMax = 5
2.75 3.50 3.50 3.00 2.00 3.50 1.50 2.50 3.00 2.75
TeamMean stresslevel: GHQitem meanMax = 3
1.36 0.95 1.33 0.99 1.08 1.35 0.85 1.10 1.03 0.83
Clarity of teamleadershipMax = 1
0.67 1.00 0.77 0.09 0.77 0.89 0.87 0.15 0.22 0.83
Teamrelationshipwith GP’sMax = 5
4 4 4 5 3 3 3 4 3 3
Teamrelationshipwith TrustMax = 5
5 5 3 4 3 4 4 3 3 3
Teamrelationshipwith SSMax = 5
5 4 4 4 4 4 4 3 4 3
AssessmentWLimplemented
no no no yes no no yes no yes No
Integratedcase notes yes yes yes no no no no no no Yes
Referralspooled All some all all some all all all some All
Self reporteffectivenessMax = 5
3.10 3.70 3.28 2.82 2.66 3.41 4.00 2.72 2.85 3.65
External ratingeffectivenessMax = 5
- 3.13 3.28 2.85 3.12 4.19 3.19 3.59 2.67 -
External ratingof innovationsMax = 5
2.75 3.63 2.25 1.00 2.50 2.25 3.13 2.50 3.00 3.38

Caseload profile
But how does all this relate to the quality of care provided by this sub-sample of
CMHTs? In the intensive phase of the research, team practitioners were asked to:
• Complete a caseload analysis describing the diagnosis, severity, chronicity
and complexity for all clients. These factors were used to (a) describe the
team’s caseload profile; and to (b) select a representative sample of around
40 CMHT’s clients following procedures defined by the research team (see
Methods)
• Approach selected clients, and if appropriate their carers, and invite them to
participate in the research by completing a Service Satisfaction questionnaire
• Participate in interviews structured to elicit biographical, resource use, and
clinical information about the team’s 40 selected clients, retrospectively for
the past 6 months. Data on resource usage were collected relating to number
of contacts with practitioners in the team; number of inpatient days; use of
day hospital, day care or drop-in; medication; outpatient appointments
• Complete the HoNOS monthly for selected clients over the following 6 months
or up to discharge
• To provide information during a second site visit relating to resource use and
clinical outcomes for the team’s sample of representative clients.
Clinical and cost data were collected for 372 CMHT clients for the first 6 months of
the 12-month period, although an attrition rate of around 35 per cent meant that, for
the second 6 months, data for only 241 of those clients were available. The high
attrition rate was accounted for primarily by key workers or care co-ordinators leaving
the CMHT, and other key workers or care co-ordinators being unable to supply
clinical data during the second site visit.
Psychiatrists completed a caseload analysis in only two teams, and for Team J in
particular, this increased the number of clients on the team’s caseload. Figure 7.2
shows the client caseload team by team, in terms of severity and diagnostic group.
Oneway ANOVA tests showed that some teams differed in the severity of their
caseloads F(9,362) = 4.44, p < 001. Post hoc Bonferroni tests indicated that Team
B’s caseload (mean 2.18) was significantly milder than Team E’s (mean 2.70), p =
.003; than Team I’s (mean 2.64), p = .019; and Team J’s (mean 2.62), p = .021; and
marginally milder than Team H’s (mean 2.65), p = .054.

Figure 7.2: Client caseload profile by severity and diagnostic group6
Diagnostic category Mild Moderate Severe TOTAL
Team ASubstance misuse 3Depression 42Anxiety 50Psychosis 55PD 14
5 87 82 174
Team BSubstance misuse 3Depression 43Anxiety 51Psychosis 85PD 9
33 97 78 208
Team CSubstance misuse 3Depression 43Anxiety 44Psychosis 85PD 12
20 83 92 195
Team DSubstance misuse 8Depression 59Anxiety 8Psychosis 54PD 8
28 57 70 165
Team ESubstance misuse 6Depression 24Anxiety 9Psychosis 141PD 18
6 56 136 198
Team FSubstance misuse 3Depression 86Anxiety 45Psychosis 68PD 8
52 90 74 216
Team G
Substance misuse 7Depression 38Anxiety 30Psychosis 79PD 8
21 91 70 182
Team HSubstance misuse 8Depression 41Anxiety 24Psychosis 154PD 17
10 88 153 251
Team ISubstance misuse 0Depression 85Anxiety 42Psychosis 144PD 14
38 84 200 322
Team JSubstance misuse 29Depression 180Anxiety 43Psychosis 170PD 16
25 174 236 435
6 Some disorders (e.g. adjustment to disability) presented in low numbers, therefore were notincluded

During the site visits, all CMHTs emphasised that they experienced a tension
between policy requirements that their case load included enduring mentally ill
people, and the referral patterns of local GPs who continued to refer all adults with
mental health problems. The tension was increased by a third demand in some
localities that CPNs from within the team should conduct clinics in primary care
practices. Most teams had attempted to clarify with GPs the appropriate referrals,
but reported little guidance from their Trust management, and little change in types of
GP referrals.
Varying responses to these conflicting demands emerged from the data. An
important finding was that the three teams (B, C and F) carrying caseloads which had
clients who were relatively moderately ill, all provided clinics in primary care, and
inclusion of their primary care patients accounted for their lower overall caseload
severity.
Mental health status, health economic costs and clinical outcomes
Mental health status, first 6-month period
In this section we present more detailed information about the sample of
mental health status clients selected by teams and their clinical outcomes.
The period was 12 months, although as stated there was a 35 per cent
attrition rate for cases. Some of the selected clients who completed the
service satisfaction questionnaire criticised continuity of care, as a result of
practitioners leaving the team and being allocated to a new key worker.
Figure 7.3 gives a summary of the mental health status of a sample of clients
selected in terms of severity and CPA level. These data were collected 6
months into the review period. Comparing the information in Figure 7.3 with
Figure 7.2 above shows that the severity of selected clients' mental health
condition was broadly representative of teams’ entire caseload profiles.
Looking at Team J, for example, Figure 7.2 showed that 236 (54%) clients
were severely ill; Figure 7.3 below shows that 28 (62%) of Team J’s selected
clients were severely ill.

Figure 7.3: Summary of selected clients’ mental health status
Mild Moderate SevereCPA
level 1CPA
level 2CPA
level 3On
sectionNot onCPA
Team A 1 14 19 12 13 6 2 3Team B 5 23 12 22 7 7 2 3Team C 3 17 16 11 21 1 0 1Team D 3 12 26 6 14 6 3 13Team E 1 10 29 9 21 4 4 5Team F 3 14 19 12 16 5 3 0Team G 3 19 13 19 13 1 2 0Team H 0 9 17 5 9 3 4 9Team I 1 12 26 6 23 1 3 9Team J 0 17 28 - - - 2 -
During the site visits, it emerged that teams used different criteria for determining
CPA level. Some teams had produced guidelines for assigning CPA level, while
others had not. Most teams used the labels ‘level 1’ as least severe, but others used
‘level 1’ as most severe. One team in the sample used ‘level A’ as the most severe.
These had been recoded to represent severity as lowest, level 1, highest, level 3.
Thus how CMHTs used the CPA was non-standard, and indicated variation in the
management of CPA.
More importantly, in terms of the role of CPA in maintaining service standards, we
observed firstly that planned CPA reviews for selected clients were often overdue,
and secondly, that part of the difficulty was getting access to all the practitioners who
it was specified in the work plan must be present at the review. Some teams had a
particular difficulty with accessing psychiatry.
Across the teams, the percentage of CMHT clients who had a formal carer, in
the sense that their key workers judged that clients needed carer support to
live in the community, ranged from 22 to 55 per cent across the teams. We
found that many clients did not have a care plan with formal targets; however,
this varied across teams and was related to severity of caseload. Figure 7.4
gives a team breakdown of selected clients’ diagnosis and severity.

Figure 7.4: Selected clients’ diagnosis and severity
Diagnostic group Mild Moderate Severe TOTAL
Team A Substance misuseDepressionAnxietyPsychosis/PD 1/0
16
6/1
115
9/2 33Team B Substance misuse
DepressionAnxietyPsychosis/PD
23
68
8/13
8/1 40Team C Substance misuse
DepressionAnxietyPsychosis/PD
3 75
3/1
21
12/1 35Team D Substance misuse
DepressionAnxietyPsychosis/PD
12
37
2/0
272
12/2 40Team E Substance misuse
DepressionAnxietyPsychosis/PD
1 1
8/1
21
25/1 40Team F Substance misuse
DepressionAnxietyPsychosis/PD
2
0/1
53
5/0
152
10/1 35Team G Substance misuse
DepressionAnxietyPsychosis/PD
3
236
8/0
2
37/1 35
Team H Substance misuseDepressionAnxietyPsychosis/PD 8/0
32
10/0 23Team I Substance misuse
DepressionAnxietyPsychosis/PD
1 7
4/0
156
10/4 38Team J Substance misuse
DepressionAnxietyPsychosis/PD
94
4/0
131
13/1 45
Figure 7.4 illustrates that, although these 10 teams were similar in terms of
diagnostic categories for which care was provided, the numbers seen within the
serious and enduring categories varied. This was most apparent in team E, in which

83 per cent of selected clients were diagnosed with psychosis, in contrast to team G,
in which a diagnosis of anxiety was almost as prevalent as psychosis.

Health economic costs
Figure 7.5 gives a summary of costs 6 months into the period. Costs are derived as
mean cost per client, and rounded to the nearest pound. Economic costs for in-
patient days, outpatient appointments, day care sessions, and contact with
practitioners were calculated using Unit Costs of Health & Social Care compiled by
Ann Netten and Jane Dennett at the PSSRU University of Kent at Canterbury. We
commissioned advice on the analysis and interpretation of these data from the
Centre for Health Economics, University of York.
The following assumptions were made when calculating costs:
• In-patient days were calculated at £136 per day
• Outpatient appointments were calculated at £97 per appointment
• Day care costs were calculated at £32 per session. One session equates to
half-a-day. All contacts reported were assumed to be one session. Day care
included day hospitals, day centres, drop-ins and workshops
• Calculations for contacts with practitioners were based on a generic cost for
all members of the Community Mental Health Team. The unit cost used was
face to face contact calculated at an hourly rate. All contacts were assumed
to last one hour. Both a minimum cost of £26 per hour and a maximum of £50
per hour were calculated
• Medication costs were calculated using the British National Formulary. Costs
of generics were used in all calculations except where these were not
available
• Contact costs have been computed using the minimum generic costing (£26
per contact), so this is an underestimation of the cost of contacts, although
consistent across all teams

Figure 7.5: Summary of health economic costs: first 6-month period
Medication Contacts Day care OPappointments
Inpatientdays
TOTAL
Team A 247 2655 1156 120 1572 5750Team B 199 950 842 99 126 2216Team C 210 939 1043 119 162 2473Team D 100 2140 1304 213 1012 4769Team E 150 5001 1294 172 3515 10132Team F 169 1138 1003 136 382 2828Team G 193 2530 1197 77 1480 5477Team H 225 2727 1816 131 1496 6395Team I 180 3129 1092 246 1806 6453Team J 325 999 440 229 48 2041
One way ANOVA was used to determine significant differences between
teams. Significant differences were apparent in terms of outpatient (F = 3.94,
p < .001), inpatient (F = 3.41, p < .001) and practitioner contact costs (F =
3.01, p < .01). Using univariate analysis of covariance, controlling for
caseload severity, differences between teams remained statistically
significant, as shown in figures 7.6 to 7.8.
Figure 7.6: Inpatient costs, first 6 months
Source df F Sig.Corrected Model 10 3.785 .000
Intercept 1 1.014 .315SEV 1 6.688 .010
TEAM 9 2.854 .003Error 359
Figure 7.7: Outpatient costs, first 6 months
Source df F Sig.Corrected Model 10 4.192 .000
Intercept 1 .570 .451SEV 1 7.039 .009
TEAM 9 2.972 .002Error 231

Figure 7.8: Contact costs, first 6 months
Source df F Sig.Corrected Model 10 6.178 .000
Intercept 1 3.166 .076SEV 1 32.308 .000
TEAM 9 2.648 .006Error 353
Post hoc Bonferroni tests indicated that Team I had significantly higher outpatient
costs than Teams B, C and G. Post hoc tests also indicated that Team E had
significantly higher inpatient costs than teams B, C, F and J, and that Team E had
significantly higher practitioner costs than teams A, C and J.
Pearson’s R correlations were carried out on caseload severity with all health
economic costs for the first 6-month period. Medication costs were not associated
with other costs or caseload severity. Practitioner contact costs were associated with
outpatient (Pearson’s R .14, p < .01) and inpatient costs (Pearson’s R .25, p < .01).
Practitioner contact costs were also associated with caseload severity, Pearson’s R
.30, p < .01. Outpatient costs were associated with inpatient costs, Pearson’s R .17,
p < .01. Caseload severity was also associated with outpatient costs, Pearson’s R
.12, p < .05, and inpatient costs, Pearson’s R .18, p < .01.
Mental health status, second 6-month period
Whereas in some CMHTs we were able to collect cost and clinical data for
most of the sample of representative clients for the second 6-month period, in
others there was high attrition. Figure 7.9 shows the attrition rate within each
team.
Figure 7.9: Summary of selected clients lost at second 6-month period
First 6 months Second 6 months % lost
Team A 34 21 38Team B 40 27 33Team C 36 17 53Team D 41 12 71Team E 40 32 20Team F 36 29 19Team G 35 31 11Team H 26 7 73

Team I 39 26 33Team J 45 39 13TOTAL 372 241 35
Clients were divided into two independent groups, the first made up of clients for
whom data were collected only in the first 6 months, the second consisted of clients
for whom we collected data at both time points. Using independent sample t-tests,
we found that over the first 6 months clients retained in the sample were marginally
less severe (mean = 0.48) than those lost to the sample over the second 6 months
(mean = 6.80; t = 1.70, p = .09).
For those clients who were on CPA at the first time point, and remained in the
sample, 116 remained at the same level, 25 moved to a lower level, and 63 moved to
a higher level.
Health economic costs, second 6-month period
In Figure 7.10 below, costs are shown for the second 6-month period, based
only on the clients still in the sample, and calculated as described above.
Figure 7.10: Summary of health economic costs: second 6-month period
Medication Contacts Day care OPappointments
Inpatientdays
TOTAL
Team A 136 433 4302 185 648 5704Team B 179 216 551 86 584 1616Team C 188 177 452 102 0 919Team D 136 295 891 162 533 2017Team E 258 597 747 173 1466 3241Team F 269 267 164 171 1913 2784Team G 440 265 364 122 715 1906Team H 436 505 1563 83 2273 4860Team I 310 307 411 224 675 1927Team J 258 223 340 259 883 1963
One way ANOVA was used to determine differences between the teams in
terms of costs. Significant differences were found in practitioner contacts and
day care costs, but not for other costs. Post hoc Bonferroni tests indicated
that practitioner contact costs were accounted for by Team E being
significantly higher than all others except A, D, and H (F = 4.50, p < .001).

Day care costs were significantly higher for Team A than all other teams,
except teams C and H (F = 2.75, p < .01). Pearson’s R correlations were
carried out on client caseload severity with all health economic costs for the
second 6-month period. There were clear associations between severity level
and all costs except medication: with practitioner costs, R = .30, p < .001; with
outpatient costs, R = .23, p < .001; with inpatient costs, R = .20, p < .01; and
with day care costs, R = .13, p < .05.
Clinical outcomes, first and second periods combined
It was not until the end of the 12-month period that practitioners were asked to judge
whether clinical targets for each selected client had not been met at all, had been
partly met, had been fully met, or had been exceeded. Often, given the diagnosis
and chronicity of many of these clients, the targets were simply that they should be
stable or maintained in the community. Sometimes, though, there was a clear
objective to discharge the client, and tests were carried out to see how many of the
proposed discharges subsequently took place.
At the team level, in order to determine team differences, client severity level
and whether predicted targets were met were analysed using Oneway
ANOVA. The analysis indicated that Team E clients continued to be
significantly more severely ill (mean 7.19) than those of Teams B (mean 5.63)
and G (mean 5.77), F = 2.97, p < .01. A marginally significant difference was
found in the level of predicted targets met (F = 1.66, p = .10) and post hoc
Bonferroni tests indicated that Team J’s perceived performance in meeting
predicted targets was marginally better than Team C’s.
Team-level tests were carried out to determine whether the costs incurred by
different teams were related to the diagnostic profile of their clients. Univariate
analyses of covariance were carried out, controlling for the effects of diagnosis and
severity, as shown in Figure 7.11.

Figure 7.11: Costs and clinical targets met controlling for diagnosis and severity
Dependentvariable
Effects of diagnosis Effects of severity Team effects(controlling for diagnosis,
severity)
Fp
Fp F (11,351) p
Inpatient costs
< 1 ns 1.70 .19 3.06 < .01
Outpatient costsDf 11,227
3.00 .08 6.24 < .05 3.39 < .01
Medication costsDf 11,266
< 1 ns 1.56 ns 1.30 ns
Overall costsDf 11,352
< 1 ns 6.65 .01 3.68 < .001
Clinical targetsmet
3.94 < .05 < 1 ns 1.81 .07
Taking into account variation across teams in diagnosis and severity of
clients, teams were significantly different in terms of some health economic
costs incurred, although not for medication costs.
Inpatient costs (computed at £136 per day)
In relation to inpatient costs, Team J (mean cost per client £48) made little
use of inpatient facilities; teams B and C (means £125 and £167 respectively)
also incurred low inpatient costs. Inpatient costs for Team E, some of whose
clients were severely psychotic and at high risk, were higher than all others
(mean £3515).
Outpatient costs (computed at £97 per contact)
Outpatient costs were considered only for those clients who attended appointments.
As expected, both diagnosis and severity had an effect on outpatient costs, with
more serious diagnoses and higher levels of severity positively associated with
higher costs. At the team level, H and B (mean cost per client £97 and £161
respectively) incurred lower costs than did teams I (mean £589) and J (mean £499).
Medication costs

Medication costs were not influenced by diagnosis or severity, and teams did
not differ significantly in terms of their outlay on medication.

Overall costs
Overall cost per client was strongly influenced by severity, though not by
diagnosis. Teams differed significantly in relation to overall costs, with Team
E (mean £5001) higher than all other teams, a dimension partly accounted for
by the high use of support workers visiting clients at home, sometimes daily,
and high inpatient costs. Teams B, C and J (means £950, £964 and £999
respectively) incurred lower overall costs than the other teams in the sample.
We saw above that Teams B and C had relatively more moderate caseloads
than other teams, but this did not apply to Team J.
Clinical targets met
Teams differed marginally in terms of practitioners’ judgements of whether
clinical targets were met, although this was also influenced by client
diagnosis. Teams B and J (mean per client 2.67 and 2.74 respectively)
scored relatively high on this dimension, while Teams A, C and H scored low
(means 2.25, 2.07 and 2.25 respectively). However, a score of over 2.00
indicated that for the average client, clinical targets had been at least partly
met.
Psychiatry input
A serious problem for this sample of CMHTs was their lack of effective input from
psychiatrists. This was more of a problem for teams with a higher number of
severely ill clients, for example, Teams E and I. How this problem manifested varied
across the teams. One team reported that they had direct access to a psychiatrist for
over 2 years. Other teams had negative views about access to medical input. Their
clients had to visit outpatient departments for CPA reviews, rather than this being
conducted at the team base. Some teams reported that although a psychiatrist was
based within the team, and clients attended clinics at team premises for some CPA
reviews, these reviews were not conducted as frequently as specified in the client’s
care plan, because no medical input was available. It was difficult to find locum
psychiatrists so long term absence or secondment also resulted in a lack of
psychiatric cover for the team.

Team processes, team performance, team stress, clinical outcomes,user satisfaction and cost effectiveness
At the team level, in order to determine how the different dimensions of
effectiveness were related, correlation analyses were performed on relevant
compositional (age, tenure, severity of caseload, number of linked GPs,
MINI), process (team processes, clarity of leadership, ability to communicate
across disciplines, relationships with GPs, Trust and Social Services, pooling
of referrals, how quickly emergencies are seen), performance (overall self
report and external evaluation, external evaluation of innovations) and
outcome (targets met, overall costs, and user satisfaction variables). Some
associations were apparent, as shown in Figure 7.12. These data must be
viewed as exploratory and interpreted very cautiously, in view of the
probability of both Type I and Type II errors: calculating such a large number
of correlations invites Type I errors, whilst the small sample of teams incurs
substantial risk of Type II errors.
Figure 7.12: Summary of associations across composition, process and outcome
Association Pearson’s R probability
Caseload severity/annual costs .763 .010
Caseload severity/self report effectivenessTeams feel ineffective when they have severecaseloads
-.655 .040
Clinical targets met/team stress levelTeams whose members feel stressed also reportdisappointing clinical outcomes
-.628 .052
External evaluation of innovation/clarity of teamleadershipGood team leadership recognised by innovationraters
.560 .091
Team processes/self report effectiveness .890 .001
User satisfaction/how quickly emergency referrals areseen .789 .011
MINI/team uses integrated case notesIntegrated case notes tend to be used in moredeprived areas
.766 .016

Referrals pooled in the team/number of linked GP’sA central referral system in response to larger N ofGPs
.708 .049
CMHT relationship with Trust/CMHT relationship withSocial Services .642 .045
Tenure/external rating of effectiveness (n = 8) .699 .054

The survey results suggested that ‘good’ processes and outcomes are associated
with:
• small team size
• few part-time workers
• Health Service only commissioning
• single, clear line of leadership or co-ordination
• rapid response to emergency referrals
• effective communication processes
• external judgement about its effectiveness if the team itself rates its
functioning highly
When we looked in more depth at exemplar CMHTs, we found a wide variety in
practice. During the researchers' visits to the 10 CMHTs in four NHS regions, the
team numbers spent an average of around 20 hours with the research team, which
yielded rich anecdotal evidence in support of the ‘hard’ findings at both survey and
intensive stages of the study.
Size We found that in one very large team CHMT where three smaller teams had
been created, and separate meetings were held for nursing staff and social workers,
co-ordination and communication were problematic. The wider team met only once
every two months to debate and decide team policy and practice.
Single, clear leader or co-ordinator Seven of the sub-sample teams had a clear
leader or co-ordinator, but in three teams the lack of clarity about leadership was
problematic. One team had been without a leader for over two years, which was felt
to be an indicator of under-resourcing and lack of support from the local
commissioners. Practitioners agreed that this situation also made team meetings
difficult, not only in terms of process, but in terms of the struggle to implement and
communicate decisions.
Rapid response to emergency referrals One of the primary agenda items at
CMHT meetings was the implementation of duty systems to cover emergency and
urgent referrals. These clients often had to wait longer than practitioners felt was
ideal. Such new systems were also described by many team members across the
sample as one of the major innovations their teams had implemented in the previous

12 months. Of course, some of these teams had only been brought together within
the previous 12 months.
Effective communication processes Observation of team meetings indicated wide
variation in quality of team communication. In general, meetings had an agenda,
either formally written and circulated before the meeting or informally presented at
the start of the meeting. Most teams kept to the agenda and covered all business.
However, there were wide differences in process. In the most effective teams,
interaction was quick, responsive and supportive, and participation was equal; in
some teams though most people attending did not take part and merely ‘listened in’.
The issue then arises that those people who do not participate in discussion or
decisions do not feel they ‘own’ decisions and are slow to implement them.
Inclusion of social workers At the statutory level, social workers must be involved
in the care of the CMHT client group. Our survey findings indicated that social
workers tended to rate their team’s effectiveness lower than other disciplines. What
we discovered in carrying out the study was that the research process itself was not
so thoroughly underwritten by Social Services employees as by Health personnel. At
some site visits, we also observed the negative attitudes of health personnel towards
social workers, and vice versa. In open-ended statements in the survey, this cross-
disciplinary hostility was evidenced in many teams, partly because nurses were
expected to take on the duties previously seen as only related to social work, for
example, giving housing or benefits advice. However, in the most effective teams in
the sub-sample, social workers were well integrated to provide the delivery of care for
this client group.
Discussion
This intensive analysis of a sub sample CMHTs draws attention to some key issues
in delivering mental health care, as well as providing a demonstration methodology
for looking in detail at the effectiveness of services delivered in terms of participant
evaluations in relation to health care costs. However, in view of the small number of
teams we were able to study at this level of detail, our substantive findings cannot be
interpreted as more than tentative.
The intensively-analysed teams were selected on the basis of team member ratings
of team effectiveness, team processes, and personal stress. The 3 teams whose

members perceived them as effective were seen as more innovative, but not as more
effective, than the remaining teams in the sub sample.
We found that teams varied in the perceived severity of their caseloads, in the
proportion of their caseloads who were suffering from severe and enduring mental
health problems, and in the health care utilisation costs incurred in the treatment of
patients on their caseloads. Two of the 3 teams with relatively low overall costs per
case had relatively high proportions of only moderately severe cases. Health care
utilisation costs differed across teams even when controlling statistically for the
variation in caseload severity across the 10 teams. The different categories of cost
incurred (CMHT practitioner contacts, outpatient costs and inpatient costs) were
positively inter correlated across teams. This suggests that teams differ in terms of
their use of more or fewer services of all kinds, rather than differing in the priority or
availability of the 3 types of service in the care packages delivered by each team.
Only medication costs were unrelated to the other categories of cost.
Further analyses controlled statistically for both diagnosis and caseload severity and
showed that inpatient, outpatient, and overall costs all differed across the 10 teams.
In terms of meeting the clinical targets set by keyworkers themselves, however,
teams differed only marginally ( p = .07) when diagnosis and severity were
controlled. The associations between severity and costs were well-illustrated by the
team with the highest costs being the one that judged its patients to be most severely
ill.
In the course of collecting these data we made important supplementary
observations concerning the targeting, integrity, and likely effectiveness of CMHT
care. The most significant problem was the frequency of overdue Care Programme
Approach reviews, suggesting that CPA is often not implemented effectively. This
was attributed to the unavailability of psychiatric input. This echoes the finding from
the larger survey sample that only 12% of CMHTs included all core disciplines.
However, effective CPA requires availability of all relevant staff for review meetings,
a requirement that goes beyond the mere inclusion of relevant disciplines in the
membership of the team. A further problem was the threat to continuity of care
arising from the staff turnover that accounted for most of the 35% attrition when we
returned to collect data for the second 6-month period.

We were also forcibly reminded of the tension experienced by CMHTs between
policy requirements to focus on severe and enduring mental health problems and the
demands of GPs continuing to refer many adults with mental health problems. This
was reflected in the finding that the 3 teams with relatively moderately ill caseloads
all provided clinics in primary care, with inclusion of their primary care patients
accounting for their lower overall caseload severity. Fulfilment of CMHTs’ remit
under the National Service Framework will require primary care to shoulder its full
burden in relation to the less severe but considerably more prevalent disorders with
which it is tasked by the framework.
Finally, this intensive analysis of clinical data lent some further validation to the
measures used in the full sample of CMHTs: teams with relatively severe caseloads
considered themselves less effective; teams whose members felt under stress also
reported disappointing clinical outcomes; users of services provided by teams
reporting rapid response to emergency referrals were more satisfied with their team’s
service.
Although not definitive, on account of the small sample, this intensive analysis
highlights key issues in mental health service delivery.

Chapter 8
Secondary Health Care Team -Research methods and Sample Details
Introduction
Three studies were conducted with secondary health care teams. The first examined
the relationship between team processes and team member stress. The second
explored whether team membership per se, was associated with stress, and if so,
what factors in the team environment accounted for this association. The third was a
longitudinal study of the relationship between team functioning and subsequent
member turnover from the team.
The Sample in Study 1 in Secondary Care
The Association between Team Membership and Sress.
The purpose of this study was to determine whether team membership conferred
upon NHS employees better mental health than did membership of loose working
groups or a work situation which did not involve working in a team or loose staff
grouping. Four Trusts were selected from nineteen Trusts included in a larger study
of stress in the National Health Service (Borrill et. al., 1998) and 4,500 names were
selected from the Trusts’ staff lists. The next step involved selecting individuals from
these hospitals for possible involvement in the study. For small occupational groups,
where the number of possible respondents was a hundred or fewer, all those on the
staff lists supplied by the hospitals were included. For larger occupational groups,
individuals were randomly selected from staff lists, with a minimum proportion of
20%. Hence, greater proportions were sampled from smaller occupational groups
and from smaller hospitals. A total of 4,500 names was thus selected. Individually
addressed questionnaires were distributed either by hand to the person’s area of
work or through the internal post. 2,263 people returned completed questionnaires,
representing a response rate of 50%.
Questionnaires were sent to all those selected for the sample
The questionnaire was in four sections:

Section 1: Biographical information
Respondents were asked to give information about age, gender, marital status,
number of children, number of other dependants, job title, length of service, hours of
work.
Section 2: Work Characteristics
Scales were used to measure perceived job, work and hospital characteristics (e.g.,
work demands, autonomy, role conflict, influence in decision-making). Full details of
these measures can be found in Haynes et al., (in press) and are available from the
first author of this report. Measures of organisational climate were also included,
which examined 12 dimensions of climate.
The climate measure we employed is based on the Competing Values Model of
organisational effectiveness (Quinn & Rohrbaugh, 1981; Hill, 1998). This model
posits two fundamental organisational dimensions: internal versus external
orientation and emphasis on control versus an emphasis on flexibility. These two
orthogonal dimensions create four domains of organisational emphasis:
Rational Goal Approach - external focus with tight internal control
Open Systems Model - external focus and flexible relationships with the
environment
Internal Processes - internal focus with an emphasis on tight internal control
Human Relations - emphasis on well-being, growth and commitment of
employees.
These approaches reflect the rich mix of competing views and perspectives within an
organisation and Quinn (1988) argues that a balance of these competing
organisational values is required for organisational effectiveness.
The organisational climate questionnaire (Hill, 1998) was developed by selecting
scales from an existing team processes measure considered appropriate to service
organisations. Following extensive pilot work in four NHS Trusts, this Organisational
Climate Questionnaire (OCQ) was used to survey 5,275 health service employees
from 27 Trusts (Hill et. al., 1997). The results of this survey suggested seven core

dimensions: innovation, performance monitoring, autonomy, co-worker co-operation,
training, communication and resources (Hill, 1998).
Innovation
This dimension measures the extent to which the Trust is seen to be responsive to
change. More specifically the scale explored the extent to which senior staff were
interested in suggestions and the development of new ideas. This was a six-item
scale with five intervals and three stems ranging from strongly agree to strongly
disagree. An example item from this scale is “New ideas are readily accepted in the
Trust.” The coefficient alpha for the current sample was 0.91.
Performance Monitoring
This dimension addresses the perception of how adequately job performance is
monitored within the Trust as a whole, and how well staff are informed about their
work performance. The scale consisted of five items with five intervals and three
stems ranging from strongly agree to strongly disagree. An example item from this
scale is “Staff performance is measured on a regular basis.” The coefficient alpha for
the current sample was 0.86.
Autonomy
This dimension measures the extent to which employees feel that they have the
freedom to work in their own way and are given adequate scope and responsibility to
work without constant upward consultation. The scale has six items with five intervals
and three stems ranging from strongly agree to strongly disagree. An example item
from this scale is “Management tightly control the work of those below them.” The
coefficient alpha for the current sample was 0.87.
Co-worker co-operation
This factor measures the extent to which there is co-operation and conflict amongst
staff in the Trust. The scale comprised of six items with five intervals and three
stems ranging from strongly agree to strongly disagree. An example item from this
scale is “People can rely on one another in the Trust.” The coefficient alpha for the
current sample was 0.87.
Training
This dimension measures the employee’s perceptions of degree of emphasis within
the Trust on skill development and the availability of training resources. The scale

comprised of six items with five intervals and three stems ranging from strongly agree
to strongly disagree. An example item from this scale is “Staff are strongly
encouraged to develop their skills in the Trust.” The coefficient alpha for the current
sample was 0.86.
Communication
This dimension measures the employee’s perceptions of information sharing
throughout the Trust, particularly top-down/vertical communication between
management and workers. The scale comprised of five items with five intervals and
three stems ranging from strongly agree to strongly disagree. An example item from
this scale is “Communication between management and staff is excellent in the
Trust.” The coefficient alpha for the current sample was 0.85.
Resources
This dimension measures employees' perceptions of resource allocation and usage
within the Trust. The scale consisted of seven items with five intervals and three
stems ranging from strongly agree to strongly disagree. An example item from this
scale is “There is very little waste of financial resources in the Trust.” The coefficient
alpha for the current sample was 0.77.
Scale Structure and Reliability
Factor analyses and other multivariate techniques demonstrated the empirical
distinctiveness of the scales from each other (Hill, 1998). The scale reliabilities
reported for this study compared well with the original work, which quotes a range of
reliability coefficients from 0.69 to 0.89.
The notion of teamness was operationalised by using the definitions of teams
employed in the literature (e.g. Alderfer, 1977; Hackman, 1987; Guzzo & Shea,
1992; Guzzo, 1996, p. 8; West, 1996b). The following characteristics are commonly
used to define a team:
a) The group is perceived as a social entity by others and has an organisational
identity within a defined function.

b) This is a real group with a task to perform in an organisation from which shared
objectives are developed for the team.
c) There is a degree of interdependence between members of the group and
members interact together to achieve group objectives.
d) There is a degree of differentiation of roles and duties in the group.
e) There is collective responsibility for measurable outputs.
f) Groups are not so large that they constitute an organisation, which has vertical and
horizontal relationships and sub-groups. In practice this is usually a group of less
than 20 members (although there may be some exceptions to this number).
Distilling these characteristics suggests five components of teamness:
• Distinct roles for members of the team,
• Task interdependence - team members rely on each other to perform the task,
• Outcome interdependence - team members' achievement of team goals is
dependent on other members' knowledge, skill and task performance,
• Team identity - team members and other organisational members regard the
group as a team with a clear team level task to perform
• Clear team objectives - there are clear team level objectives.
Section 3: Stress
The main measure of stress was the 12-item version of the General Health
Questionnaire (GHQ-12; Goldberg, 1972; Goldberg & Williams, 1991). The GHQ-12
was designed as a self-administered screening test for detecting minor psychiatric
disorder in the general population. It covers feelings of strain, depression, inability to
cope, anxiety based on insomnia, lack of confidence and other psychological
problems.
Section 4: Team working
Respondents were asked to indicate, by ticking a ‘yes’ or a ‘no’ response option,
whether they worked in a team. To differentiate between those who did and did not
work in a clearly defined team according to our criteria of teamness, but who
indicated in answer to the categorical question that they did work in a team, we
summed responses to 4 questions:

• Does your team have relatively clear objectives?
• Do you frequently work with other team members in order to achieve
these team objectives?
• Are there different roles for team members within this team?
• Is your team recognised by others in the hospital as a clearly defined work
team to perform a specific function?
Those who did not answer, “yes” to all four questions were categorised as being in a
‘quasi team’. Out of the total sample, 283 responded clearly that they did not work in
a team. Of the 1,980 who answered “yes” to the question “Do you work as part of a
clearly defined team?” 692 answered “no” to one or more of these questions and
were therefore categorised as members of “quasi teams”. Thus 283 (12.5%) did not
work in a team, 1,288 (56.9%) worked in a team, and 692 (30.6%) worked in a “quasi
team”.
The Sample in Study 2
The Relationship between Team Processes and Team Member Stress
Using data from official records and the expertise of members of the National Health
Service Executive, ten Trusts were selected for inclusion in this part of the study
Identifying a sample of teams in each Trust was a lengthy process. Discussions
were held with senior managers, who identified teams in their organisations and
suggested contact persons from each team. The researchers then telephoned the
contact person, negotiated their collaboration in the study, and once agreement was
reached, secured the names and location of team members. Contact persons were
asked to distribute questionnaires to their team members.
There was considerable variation in the types of team in Trusts, and it was not
possible to identify a sufficiently large sample of a single type of team that was
common across all Trusts. Six team types predominated:
• nursing care
• management
• medical
• multidisciplinary
• support
• quality improvement teams

Members of 225 teams were invited to take part in the study. Members of 14 teams
declined this invitation. Over a period of 16 months, 193 teams in 10 NHS Trusts
continued to collaborate in the research. Questionnaire responses were received
from 1,237 team members. The numbers in each profession/occupation were: 752
nurses, 114 doctors, 98 administrative staff, 78 managers, 125 professions allied to
medicine (PAMs), 26 professional and technical staff, 26 ancillary staff and 18 of
unknown occupational group. Team sizes ranged from 2 to 44 (mean 11.4, SD =
6.93).
Figure 8.1: Characteristics of NHS Trusts
Type Budget*
(in £ million)
Number of
Staff*
Year of
Trust Status
Location
Teaching 100 3,000 1991 City
Teaching 125 5,000 1990 City
Teaching 120 5,000 1994 City
Teaching 90 5,500 1992 City
District 78 3.250 1994 City
District 56 2,500 1994 Rural
District 38 1,200 1991 Rural
Community 40 2,000 1992 City
Community 57 1,200 1992 Rural
Community 45 2,500 1993 Rural
* Data available from 1996
The ten NHS Trusts included four teaching hospitals, three community Trusts and
three full District Trusts. Numbers of staff ranged from 1,200 to 5,500 (as shown in
Figure 8.1).
Women formed 86 % of the sample. Mean age of team members was 39.58 years
(SD = 10.52, range 17 to 64 years). Mean team tenure was 4.3 years (SD = 4.65,
range one month to 38 years). 5% of the sample had worked in their team for less
than one year, 17% between 1 to 5 years, 25% between 6 and 11 years, 18%
between 12 and 16 years, and 36% had over 16 years service.

The mean caseness of teams was 23.3% (SD = 0.25), with a mean GHQ Likert
score of 0.95 (SD = 0.24). This level is comparable to a group of 71 primary health
care teams (caseness = 21.8%, Borrill & West, 1998).
At individual level this can be contrasted to 26.7% for a larger group of British
health care employees (n = 22,298, SD = 3.09, Mullarkey et al., 1999) and 18.4%
for the general working population (BHPS, Taylor, Brice, Buck, et al., 1995).
NHS employees often belonged to three or more teams (48%), with only 14%
belonging to one team. Teams either met infrequently (30% had not met in the last
month, and 39% ha met once), or frequently (21% of team had met four or more time
in the last month). Most people worked in permanent teams (90% of members).
Questionnaire completed by individual team members
Section 1: Biographical Information
Participants were asked for their job title, age, gender, and duration of tenure in the
NHS.
Section 2: Team Composition
Team members were asked to indicate the size of their teams (number of members),
how frequently they interacted together, whether they were members simultaneously
of other teams, team tenure, and the nature of the team‘s task. Teams were
classified as coming from Teaching, District General Hospitals or Community Trusts.
Section 3: Team Processes
This contained eight measures of team working. Four of these were drawn from the
Team Climate Inventory (Anderson & West, 1994,1998) that is based on a well-
developed theoretical model of team functioning (West, 1990). The four measures
assess levels of:
• team participation
• clarity of and commitment to team objectives
• emphasis on quality
• support for innovation.
Four other measures were included:

• Reflexivity – the extent to which team members reflect upon their team
objectives, strategies and processes and make changes accordingly (West,
1996; West, 2000)
• Teamness – The extent to which the team functions as a team versus a loose
grouping
• Roles - Team members' understanding of the distinctiveness of their own role and
the degree of differentiation of roles within the team. Team members are asked
to consider their understanding of their job in the team and the appropriate use of
skills and knowledge needed to carry out the work. Then they are asked to
consider these themes in relation to other members’ roles.
• Interdependence - Task interdependence is when group members interact and
depend on one another in order to accomplish work.
Section 4: Outcomes
This section of the questionnaire elicited members’ perceptions of team performance
and shared understanding of team goals.
Section 5: Objectives
A single item invited team members to describe their team objectives.
Study 3: Do team inputs and processes predict team member retention?
Research Design
This was a longitudinal research design with data collected six months after
participating teams had completed Study 2. 76 teams were selected from four NHS
Trusts (two community, one teaching and one District General Hospital).
Following Study 2 teams were sent feedback reports. This created opportunity for
dialogue with the teams. A single sheet of questions and an introductory letter was
sent to each team contact. Materials were clearly marked with the team name as
some contacts were members of more than one team. A stamped, addressed
envelope was included to return responses.

Response
Fifty-seven teams participated in the survey (31 nursing care, 13 management, 5
multi-disciplinary, 5 Quality Improvement, 2 medical and 1 administrative support
team). Community Trusts gave the most enthusiastic response (17 of 19 teams,
89%) and teaching Trusts the least (15 of 26 teams, 58%) (overall = 57%). Data
from the Quality Improvement teams were removed from analyses as these teams
are not permanent; and several teams had ceased to exist having completed their
tasks. The final sample for analysis comprised 52 teams (mean size 11.8, SD 6.03,
range 2 to 25).
Nineteen teams did not respond to this survey (mean size 9.0, SD 4.9, range 2 to
19). No information is available as to the turnover in these teams. A comparison of
means was undertaken across study variables obtained at Time 1 to identify any
differences between responders and non-responders. No significant differences
emerged.
Team size and type of Trust are associated with turnover. People are more likely to
leave a team if they work in a teaching Trust (mean rank = 36.0 Kruskal-Wallis one
way ANOVA; Chi-square 8.43, df 2, p < .05) and are members of a larger team
(Pearson correlation: r = .23 between log percentage leaver and team size p < .05,
one-tailed test).
Regression analyses showed team size and Trust type account for between 15% to
18% of the variance in turnover.
There is no evidence to suggest that stress at Time 1 is associated with team
viability at Time 2.
Perceptions of clear team objectives and high levels of participation are significantly
associated with low levels of turnover
Regression analysis (controlling for team size and Trust type) reveals that TCI
variables treated as a block (participation, support for innovation, team objectives
and task orientation) explain 10% of the variance in team retention.

Team Tasks
Secondary health care teams diagnose illnesses, plan and administer treatment for
various conditions, conduct health screening, and provide maternity care. These are
complex tasks that require co-ordination and management, both, in a professional
sense to ensure the best outcomes for patient care, and, in an organisational sense
to ensure that the work conforms to organisational objectives, budgets, and internal
and external standards. There were seven main categories of team included in the
sample and these are shown in Figure 8.2 below:
Figure 8.2: Types of Secondary Health Care Team
Classification Description
Medical Teams These are teams of doctors.
Nursing Care Teams This is a broader notion of team covering all nursingcare to patients / clients. These teams included groupsof staff in addition to nurses such as health careassistants, auxiliaries, ancillary staff, clerical staff, andprofessional staff.
Management Teams These were teams which undertook the task ofmanaging a department, group of wards, orspecialty/directorate. Therefore, a senior nursing teamthat manages a number of wards would be describedas a management team.
Multi-Disciplinary Team These were teams, often of professional staff, whichhad the task of delivering care or a service topatients/clients often in a boundary spanning roleacross departments, wards and specialities. Forexample, an Endoscopy team would contain medical,nursing, and professional staff who may work in amedical, surgical, or investigative context.
Support Teams: Administrative These were teams, often of administrative and clericalstaff, which provided support to the four team typesabove. This support may be secretarial, administrativeor record keeping in nature. For example, a medicalrecords team would be responsible for the storage,retrieval, and distribution of patients’ hospital records.
Support Teams: Ancillary These were teams of ancillary staff such as porters,domestics, and catering staff who provided supportservices for both patients and staff. For example, aportering team would provide support to the whole Trustto transfer patients and goods between locations,provide access to restricted areas and other duties suchas security and staff protection.
Quality Improvement Team These were temporary teams assigned discrete tasks inorder to improve quality of services provided in various

health care areas. For example, a bed hire team wouldbe monitoring in-patient admission activities andensuring appropriate mechanisms were created tofacilitate the provision of hospital beds in theappropriate locations depending upon demand.
The frequency of each type of team in the sample is shown in figure 8.3.

Figure 8.3: Frequency of Team Types in Study 2
86
29
10
51
116
0
20
40
60
80
100
NUR MAN MED MD SUPP QI
Type of team
frequency
In order to portray the variety of work that takes place within secondary health care
we offer a few examples from each task category and describe the team
composition, accountability, and work undertaken.
Nursing Care Teams
The Paediatric Nursing Team
This team is part of an urban community Trust. Team members provide for the
nursing care needs of acutely or chronically sick children at home, or, in other
community settings. There are 12 members of this team: a nurse manager, 2
paediatric community nurse sisters, 4 paediatric community nurses, 2 staff nurses, 2
district nurses, and a paediatric diabetes nurse specialist. The nurse manager is the
team leader. Organisationally this team is part of the Child Health Care Group and is
accountable to the Child Health Management Team. This team can be described as
a complex decision making team which performs multiple tasks using both basic and
specialised equipment. This team interfaces with many other specialised teams in
hospital and community organisations.
Key to Task Type
NUR = Nursing care 45%
MAN = Management teams 15%
MED = Medical teams 5%
MD = Multidisciplinary teams 25%
SUPP = Support teams 6%
QI = Quality improvement teams 3%

The Coronary Care Unit
This team is part of a busy urban teaching Trust. This team provides care for patients
with heart disease and problems associated with acute and chronic capacity. There
are 23 team members: 2 nursing sisters, 15 staff nurses, 2 enrolled nurses, one
domestic, and 3 doctors (a consultant, a senior house officer, and a house officer).
This is a complex decision making team that provides specialised care delivered
using highly specialised and technical equipment. Team members are involved with
patients and their families and take an essential role in rehabilitation. In addition, this
unit undertakes training and education of staff. The team leader is the medical
consultant who is responsible, at Trust Board level, to the Clinical Director of
Medicine.
Ward One
Ward One7 is a busy surgical ward that is part of an urban teaching hospital Trust.
The ward practices team nursing and divides patient care between four teams. Team
members provide care for patients in conjunction with other professional staff such as
occupational therapists and physiotherapists during patients’ post-operative
rehabilitation. Ward One has four members: two health care assistants, one primary
nurse (nursing sister), and one associate nurse (staff nurse). The primary nurse is
the team leader and will co-ordinate with the other three team leaders on the ward.
This team is responsible to the ward manager who is part of the Medical Directorate
Management Team.
Management Teams
The Child Health Management Team
This team is part of an urban community Trust. The team co-ordinates the Children’s
Service in the community. There are 10 members of this team: a general manager,
an assistant general manager, a primary care manager, a district dental officer,
manager of speech and language therapy, finance manager, care group planner,
consultant paediatrician, personnel manager, and a nurse manager. The general
manager is the team leader and is accountable for this team at Trust Board level.
This is a complex decision making team which can be considered the top
management team for the Child Health Care Group.
7 Team names are fictitious in order to maintain confidentiality.

The Clinical Management Team
This team is part of a busy district general hospital. The function of the team is to
manage the General Medicine Directorate and they are responsible to the Trust
Board. There are seven team members: one clinical head of service and a deputy
clinical head (both doctors), a speciality manager, two nurse managers, a bed
manager, and a secretary. The clinical head of service is the team leader. This team
can be described as a top management team.
Multi-disciplinary Teams
The Surgical Oncology Team
This team provides treatment for patients with breast cancer in a busy urban teaching
hospital Trust. There are 14 team members: two consultant surgeons, two ward
sisters, two medical secretaries, two senior house officers, four surgical house
officers, and two breast care nurses. This is a complex decision making team which
provides diagnostic services, treatment and follow-up care for breast cancer patients
using in-patient and out-patient resources. The team leader is the senior consultant
and he is responsible, at Trust Board level, to the clinical director of surgery.
The Medical Practice Team
The team is part of an urban community Trust providing a comprehensive health care
service to a practice population that involves working across the boundaries of local
and community care. There are nine members of this team: two district nursing
sisters, a community staff nurse, a district staff nurse, a community nursing auxiliary,
and four health visitors. A district nursing sister is the team leader responsible to the
Locality Management Team. This is a complex decision making team that works
across the boundaries of primary and secondary health care.
Medical Teams
The Transplant Team
This team is part of a busy teaching hospital Trust. The team provides bone marrow
transplants for adults and children and carers for patients before, during and after
their transplant. This specialist team is involved in the development of new
techniques, training, and research at an international level within the medical
community. There are five members of this team who are all doctors: one acts as
programme co-ordinator, and two other consultants take responsibility for adult and
paediatric patient care. The team leader is the specialty director. This is a complex
decision making team which operates across the boundaries of several medical

specialities. The clinicians are involved in highly complex work that requires the use
and understanding of complex medical and surgical techniques, drug therapies, and
highly technical equipment.
The General Medical Team
This team has a broad remit providing treatment for any medical or social problem
and is part of a large district Trust. This team has four members: a consultant
physician, a registrar, a senior house officer, and a pre-registration house officer.
The consultant physician is the team leader and there is a strict medical hierarchy
within this team. This is a complex decision making team which provides care for
patients within the hospital and the community for a wide variety of acute and chronic
conditions.
Administrative Support Teams
The Clinic Notes Team
This small team provides medical records for patients with outpatient clinic
appointments. This team is part of a busy rural whole district Trust. The team is
composed of three administrative staff. This team will undertake tasks that require
co-ordination across many departments within the Trust and will undertake many
problem-solving tasks. Information technology skills are well developed within this
team. This is a non-hierarchical team, which is responsible to the medical records
manager.
Ancillary Support Teams
St. Jane's Domestics
St. Jane’s is a small community hospital in a busy urban Trust. The hospital is due to
close in the next two years and services will be moved elsewhere. St. Jane’s
domestics are a team of 14 ancillary staff who provides domestic services throughout
the hospital over a twenty-four hour period. The team is lead by a supervisor who is
responsible to the domestic services manager. Each domestic assistant will have a
designated geographic area of work but will be required to work in other areas as the
need arises. The team performs domestic duties and assists ward staff in providing
food and beverages, keeping the ward clean, feeding patients, and helping visitors.
It is likely that the team members will feel more part of the ward team than the
domestic team. Although this type of work would appear to be of low complexity,
domestics need to be able to carry out their work in harmony with the health care
environment of the ward. This requires understanding of the health care process in

order to communicate appropriately with patients and visitors and to adequately
clean highly complex equipment. These tasks are of medium complexity.
Quality Improvement Teams
The Outpatients Quality Improvement Team
This is a temporary team, which is part of a busy whole district Trust. The aim of this
team is to improve the quality of patient care within the Outpatients’ Department,
which covers a broad range of care across medical and surgical specialities. There
are six team members: two outpatients' service managers, a quality assurance co-
ordinator, a senior midwife, an outpatient senior sister, and a medical records
manager. This is a complex decision making team which is involved in generating
many problem solving strategies in order to achieve standards set by the Trust and
the external Patients’ Charter standards. This is not the principal team for most of its
members and has many similarities to a quality circle.
In summary, a majority of these teams are complex decision making groups, which
undertake multiple health care tasks. With the exception of the quality improvement
teams, all are permanent teams with an on-going work remit. The composition of a
majority of these teams is made up of a variety of different occupational groups. In
addition, there are differences of status, pay, conditions of service and hours of work
across these teams.
Conclusion
The diversity of team types, tasks, composition and organisational contexts in
secondary care argues against the use of research designs we employed in primary
care and community mental health. There are no unitary measures of effectiveness
common across these diverse types of teams. Moreover, the nature of their tasks
varies across organisational settings as well as across team types. Consequently,
we focused on three questions:
• Does membership of teams buffer NHS employees in secondary care from the
negative effects of stress at work and, if so, why?
• To what extent and in what ways are team inputs and processes related to team
member mental health in secondary care?
• Do team processes predict team member retention in secondary care?
We provide the answers to these questions in Chapter 9.

Chapter 9
Secondary Care TeamsResults from Surveys
Summary of Findings
• Those working in clearly defined teams in secondary care have lower levels
of stress than those not working in teams or working in loose groupings (quasi
teams).
• Differences between team membership types in stress could be accounted for
by the higher levels of social support and role clarity experienced by those
working in clearly defined teams.
• Those working in teams also perceive greater co-operation amongst all staff
and clearer feedback from the organisation on staff performance than those
not working in clearly defined teams.
• This finding suggests that team membership somehow buffers individuals
from the vagaries of organisational climate. Poor training; resistance to
innovation, low levels of resources, co-operation, feedback on performance,
autonomy, communication and training, appear to affect stress levels
deleteriously much less among those working in clearly defined teams, than
among those not working in teams or working in looser groupings.
• It implies that teams can somehow compensate for the limitations and
frustrations of organisational factors in the work experience of their members,
and that this can significantly influence the level of stress experienced by
organisational members.
• Team processes are significantly associated with stress – better team
functioning is associated with lower team member stress.

• The more frequently team members interact and meet, the better does the
team function.
• The longer team members work together, the clearer their understanding
about each other’s roles.
• The more teams people were members of, the less clear they were about the
teams’ objectives. However, they reported higher levels of emphasis on
quality of care and understanding of others’ roles.
• Those working in larger teams reported lower levels of participation in team
decision making and less clear understanding of team objectives.
• Around 10% of teams in the sample ceased to exist in the six-month study
period and there is an average 6% turnover of team members in the
remaining teams.
• Clear team objectives and high levels of team participation positively predict
member retention.
• Data from our recently completed study at the Aston Centre for Health Service
Organisation Research8 show that the percentage of people working in teams
in acute trusts is associated with lower levels of patient mortality. The more
people who work in teams in Trusts, the lower the number of patient deaths
measured by the Sunday Times (Dr Foster) Mortality Index, deaths within 30
days of emergency surgery and deaths after admission for hip fracture.
Is team membership associated with lower stress?
The data from this study revealed that 283 (12.5%) respondents did not work in a
team, 692 (30.6%) were members of “quasi teams” and 1,288 (56.9%) worked in a
clearly defined team (i.e. they conformed to the criteria of teams specified in the
research design – see chapter 8).

Analysis of variance within and between the three groups (team, non-team, quasi-
team) in relation to stress scores on the GHQ-12 revealed significant differences
between those who worked in teams (mean = .95), those who did not work in teams
(mean = 1.09) and those who worked in quasi teams (mean = 1.03) (f = 15.68; df =
2,2250; p = > 0.001). Using the GHQ “caseness” method of scoring, 98 of those who
definitely did not work in a team were categorised as cases (equivalent to 34.9%).
275 of those who worked in a team were categorised as cases (21.8%) and 203 of
those who worked in a quasi team were categorised as cases (29.7%). Caseness
implies the individual is suffering from a sufficiently high level of stress that they
require and would benefit from some professional help.
The next step in the analysis addressed the question of what could explain these
differences in GHQ scores between the teamworking types. We examined, in turn,
demographic, work role and organisational climate factors.
Demographic factors
To determine the extent to which demographic factors accounted for GHQ
differences between those not working in teams, those working in teams and those
working in quasi teams, we conducted Chi-Squared tests of these groups by
demographic factors.
These included occupational group, gender, whether they had children, marital
status (single/married/living with a partner/separated/widowed/divorced), the
organisation, (i.e., membership of which of the four Trusts that participated in the
study), time employed in the National Health Service, time employed in current post,
and age. There was a significant Chi-Square value only in the case of occupational
group (Chi-Square of 47.73; df =12; p = <0.001). We therefore conducted an
analysis of variance by team type (non-team, team, quasi team) and occupational
group by GHQ scores. There were significant main effects for occupational groups
(f = 5.572; df = 6, 2232; p = <0.001) but this did not remove the effect of team type on
GHQ score (f = 18,645; df = 2, 2232; p = <0.001). There were no significant
interactions between occupational group and team type group on the GHQ.
Work role factors
8 Details are available from West or Borrill (co-authors of this report)

Next we conducted analyses of variance to determine whether work role factors
varied between team membership types (those not working in teams, those working
in teams and those working in quasi teams). There were significant differences
between these types in role clarity, supervisory leadership, social support, feedback,
autonomy and control, and influence over decision-making, with those working in
teams reporting higher levels that those in quasi teams, who in turn report higher
levels than those not working in teams. A directly opposite pattern was found in
relation to role conflict and role ambiguity. There were no differences between the
groups in perceived work demands and hours worked.
Which of those clear differences in work role factors between the groups might
therefore account for the variation between team membership types in GHQ scores?
To answer this question we conducted separate analyses of covariance to examine
the variation between team groups in GHQ scores controlling for each of the work
role factors in turn. Figure 9.1 shows the results, which reveal that none of these
work role factors alone accounts for the difference between the team membership
types in GHQ scores. However, the effect is most reduced by using role clarity and
social support as covariates. Indeed, when these two variables are entered as
covariates together, the difference between team membership types in GHQ scores
is no longer significant (F= 0.955; df = 2,221; P = 0.385). Thus it appears to be the
differences in social support and role clarity between those who work in teams (high
social support and role clarity) and those who do not work in teams or work only in
quasi teams, which account for variations in stress levels between these team
membership types.
Figure 9.1: Analysis of variance of GHQ scores by team membership type (team,quasi team, non-team) controlling for work role factors
Covariate F DF Significanceof F
MainEffect (F)
DF Significanceof F
Role Clarity 213.03 1,2231 <.0001 4.51 2,2231 0.011
Role Conflict 284.36 1,2233 <0.001 9.12 2,2233 <0.001
Feedback 273.24 1,2217 <0.001 4.99 2,2217 .007
Influence overDecisions
60.90 1,2232 <0.001 7.15 2.2232 .001
SupervisoryLeadership
124.55 1,2179 <0.001 5.37 2,2239 .03

Role Conflict 148.16 1,2147 <0.001 12.38 2,2147 <0.001
Autonomy andControl
5.30 1,2216 .02 14.67 2,2216 <0.001
We then examined the data to determine if there were any significant interactions
between work role factors, which were significantly associated with GHQ scores, and
team membership types. There was a significant interaction only between team type
and role conflict level in predicting GHQ scores (R2 change = .0025; F = 3.13; p =
.044). This showed that at low levels of role conflict there were no differences
between the team membership types in GHQ scores, but at high levels of role conflict
there were very large differences, principally between those who were members of
teams and the other two team membership types) those not working in teams or
those working in quasi teams). Perhaps health care teams enable their members to
manage role conflict through an overt process of shared role negotiation, whereas
those who do not work in teams do not have easy access to such a process.
Organisational climate
We also conducted analysis of variance to determine whether organisational climate
factors varied between team membership types. There were highly significant
differences between the team types in perceived autonomy, training provision, level
of organisational resources, organisational attitude to change, organisational
feedback on performance, communication and staff co-operation, with more positive
perceptions among those working in teams and the most negative perceptions
amongst those not working in teams. To determine which of these organisational
climate factors might account for the variation between team membership types in
GHQ scores, we conducted separate analyses of variance entering each climate
variable as a covariate. The results revealed that none of these variables could
entirely account for the difference between team membership types in GHQ scores.
However, when we entered co-operation and feedback on performance together, the
difference in GHQ scores between team membership types was removed (F = 2.01;
df = 2, 2208; p = 0.134). Thus, the difference in perceptions of co-operation between
staff working in the organisation, and the perceptions of the quality of the
organisation's performance feedback to staff, between those working in teams, those
not working in teams, and those only working in quasi teams, appears to account for
the differences between these team membership types in stress levels.

Finally, we checked the data to determine whether there were any significant
interactions between perceptions of organisational climate factors and team
membership types that predicted GHQ scores. There were significant interactions
between team membership type, innovation, feedback on performance, co-operation
between staff, communication, autonomy, and training and organisational resources
when predicting GHQ levels. They show that those working in clearly defined teams
seem less strained than those not working in teams, or working in ‘quasi teams’, by
perceptions of low levels of these organisational climate factors. It is as though, by
working in a team, team members achieve a shared level of self-sufficiency that
buffers team members from the inadequacies of their organisations. Those who are
not members of clearly defined teams seem more affected both positively and
negatively respectively, by the relative presence or absence of those organisational
factors.
Discussion
The results suggest that being part of a team in the high-strain setting of the NHS is
associated with lower levels of stress than if one is not a member of a team or
belongs to only a loosely defined and weakly interdependent team (what we have
called a ‘quasi team’). The results could not be accounted for by demographic
factors, or by individual work role and organisational climate factors. However, the
results clearly suggested that differences between team membership types in stress
could be accounted for by the higher levels of social support and role clarity
experienced by those working in clearly defined teams. This finding is consistent
with theoretical explanations of some of the beneficial effects of teamworking that
propose that teams contribute to a greater and shared sense of role clarity and social
support (Cohen & Bailey, 1997; West, Borrill & Unsworth, 1998; Mohrman, Cohen &
Mohrman, 1995). Roles are socially negotiated sets of mutual expectations and, by
working closely with those in one’s role set, role clarity results. Moreover, since
teamworking, by definition, involves interdependent working with close social contact
and communication, it is likely that team members will experience more support from
colleagues than those whose working relationships are less tightly linked.
Similarly, in relation to organisational climate perceptions, those working in teams
derive a sense of greater co-operation amongst all staff and clearer feedback from
the organisation on staff performance, as a consequence of their team membership
than those not working in clearly defined teams, and this accounts for the differences

between team membership types in stress levels. It is easy to appreciate how
membership of a team (whose members co-operate to achieve shared goals) might
lead to the illusory sense of high levels of co-operation among staff more generally in
the organisation. Another possibility is that staff do co-operate more with those who
are members of teams, perhaps because of their clearer roles and goals, or because
of the greater power conferred by their membership of a group, or as a result of their
more clearly defined social and functional identity - "This person is a member of the
Accident and Emergency Resuscitation Team and I know about their functional
significance and understand what information or resources they require"
Similar explanations can be offered for the effect of the relatively high level of
organisational feedback perceived by team members which accounts (in concert with
perceptions of staff co-operation) for the differences between team membership
types in stress levels These may be illusory perceptions with team members
mistakenly assuming that the higher level of feedback on their performance that they
experience (as a consequence of their team members' feedback to them), can be
attributed also to organisational feedback to staff on performance. It could also be
that as a result of the clear functional identity of the team in the organisation, the
team does get clearer feedback on performance.
Particularly intriguing is our finding of significant interactions between team
membership types and organisational climate perceptions as predictors of stress.
This finding suggests that team membership somehow buffers individuals from the
vagaries of organisational climate. Poor training, resistance to innovation, low levels
of resources, co-operation, feedback on performance, autonomy, communication and
training, appear to affect stress levels deleteriously much less among those working
in clearly defined teams, than among those not working in teams or working in poorly
defined teams. The consistency of these interactions and the fact that they are
largely absent when we examine interactions between work role factors and team
membership types, suggest their robustness. It implies that teams can somehow
compensate for the limitations and frustrations of organisational factors in the work
experience of their members, and that this can significantly influence the level of
stress experienced by organisational members
We can speculate about a number of possible explanations for our findings First, it
may be that those who have lower levels of stress, self select into teams People who
are relatively well-adjusted socially and have lower levels of anxiety may be attracted

to work closely with others since the challenges of teamworking are more
manageable for them than they are for those who experience high levels of anxiety
and uncertainty. Alternatively, it may be that those who are more relaxed and cope
with stress better are selected into teams by existing team members as they offer
less of a threat to the effective social functioning of the team. Finally, of course, it
may be that those who have relatively low levels of stress are less likely to leave
teams, than those with high levels of stress.
Thus those who experience high levels of stress may find teamworking too
demanding and challenging and their stress may also create social dysfunction that
leads to their attrition from the team. These attraction-selection-attrition explanations
for our findings are credible alternatives to the suggestion that it is the effect of
working in teams upon stress that we have discovered in this first study.
Study 2
Do the composition of and the way secondary health care team members work
together affect member stress?
• Team processes are significantly associated with stress – better team
functioning is associated with lower team member stress.
• The more frequently team members interact and meet the better does the
team function.
• The longer team members work together the clearer their understanding
about each other’s roles.
• The more teams people belonged to, the less clear they were about the
teams’ objectives. However, they reported higher levels of emphasis on
quality of care and understanding of others’ roles.
• Those working in larger teams reported lower levels of participation in team
decision making and less clear understanding of team objectives.
Questionnaires were distributed to team members as described in the previous
chapter. 193 teams from 10 NHS Trusts responded. The responses consisted of 1,

237 team members (752 nurses, 114 doctors, 98 administrative staff, 78 managers,
125 professions allied to medicine (PAMs), 26 professional and technical staff, 26
ancillary staff and 18 of unknown occupational group). Team sizes ranged from 2 to
44 (mean 11.4, SD = 6.93).
The overall response rate to this survey was 54%. There were variations in
response across organisational type (from teaching 42% to community 72%) and
across team task type (Support team 30% to Management team 65%). Women
formed 86 % of the sample. Mean age of team members was 39.58 years (SD =
10.52, range 17 to 64 years). Mean team tenure was 4.3 years (SD = 4.65, range
one month to 38 years). 5% of the sample had worked in their team for less than
one year, 17% between 1 to 5 years, 25% between 6 and 11 years, 18% between
12 and 16 years, and 36% had over 16 years’ service in their teams.
Nearly a quarter of those working in teams scored above the cut-off point on the
GHQ, indicating a high levels of stress. The mean caseness of teams was 23.3%
(SD = 0.25), with a mean GHQ Likert score of 0.95 (SD = 0.24). This level is
comparable to the primary health care and community mental health teams
(caseness = 21.8%) but somewhat lower than the 26.8% recorded amongst a
larger group of NHS employees (n = 22,298, SD = 3.09, Borrill et al., 1998) though
higher than the figure of 18.4% for the general working population (BHPS, Taylor,
et al., 1995).
Team Interaction
Teams either met infrequently (30% had not met in the previous month, and
39% had met once), or frequently (21% of teams had met four or more times in
the previous month). Team interaction frequency was significantly related to all
team process variables (with eight of the ten possible relationships being
significant). All relationships were in a positive direction suggesting that
higher frequency of team interaction facilitates team processes.
Team Task
A simple classification of six team task types was used (see previous chapter).
Quality improvement teams rated support for innovation higher than did medical and
ancillary support teams. Managerial teams described their team objectives in greater
detail than support and multidisciplinary teams. Administrative support teams report

greater understanding of each other’s roles compared to teams undertaking medical
and managerial tasks.

Multiple Team Membership
Most people worked in permanent teams (90% of members). Nearly half of this
sample belonged to three or more teams (48%). Multiple team membership was
negatively associated with clarity of and commitment to team objectives and
positively associated with emphasis on quality of care, interdependence, and role
understanding. This suggests a lack of clarity about team objectives may be
counterbalanced by a more vigorous emphasis on quality of care: working in other
teams may enable members to be more vigilant about and aware of quality issues.
Team Size
Team size is positively related to interdependence and negatively related to
participation and clarity of and commitment to team objectives. Many of the larger
teams are ward or department teams, which administer care or undertake
investigations over a 24-hour period. Dependency on other team members is critical
for the safe and efficient delivery of these services. However, membership of larger
teams is also associated with low levels of information sharing and influence over
decision making, and less clear understanding of the team’sobjectives. These
findings are consistent with previous studies (Blau, 1970; Shaw, 1981; Stahelski &
Tsukuda, 1990; Sundstrom et. al., 1990) that demonstrate that as group size
increases there are increased difficulties in communication, co-ordination and
interpersonal relationships.
Team Tenure
Team tenure was not related to stress but was related to mutual role understanding.
Relationships between Team Processes and Stress
Partial Pearson product moment correlations were undertaken with pair-wise
deletion, controlling for team size. Eight of the ten-team processes variables
examined were significantly and negatively associated with stress. This suggests that
good team processes are associated with lower stress. Five process variables
predicted stress: participation, support for innovation, emphasis on quality, team
objectives, and role understanding.

Team Processes and StressRegression analysis at team level revealed team processes accounted for 22.8% of
between team variance in stress. These results are summarised below. After
controlling for team size, three process variables negatively predicted stress (task
reflexivity, p < .01; emphasis on quality; p < .05; interdependence, p < .01).
Figure 9.2: Hierarchical Regression Analysis for Team Processes Predicting Stress(n=193)
Variable B SEB
β
Step 1Team Size .0043 .002
.5.13
R2 .016 df 1 p <.08Step 2Participation .098 .069 .20Support for Innovation -.0074 .060 -.014Team Objectives .065 .045 .14Emphasis on quality -.12 .051 -.31*Reviewing Processes -.14 .05 -.32**Social Relations -.016 .046 -.039Interdependence .11 .043 .24**Team Objectives .008 .02 .030Role -.11 .059 -.19Outcome .0033 .054 .0068
R2 .228 df 10 p <.001
Note * p < . 05, ** p < . 01, *** p < . 001.
Relationships between Stress and Team Processes at the Individual Level ofAnalysis
Process variables were entered in blocks to avoid suppresser effects and finally
entered together. Several process variables significantly predict stress at the
individual level: participation, emphasis on quality (p < .01), social reflexivity (p <
.001), role understanding, and knowledge of team outcomes (p < .05).
Stress and Team Processes Across Two Levels of Analysis
The analysis of this study is complex as a cross-level model (Rousseau, 1985) is
being explored: individual level of stress and team level processes. These levels
are “nested” (hierarchically ordered systems) and exist within the context of a

higher level unit (organisation, the NHS Trust). Strategies that examine
relationships at one level of analysis ignore the influence events at another level
may have on the data. In this case events may occur in the team that might
influence individual stress as well as individual events influencing team morale
(such as team members leaving).
Hierarchical Linear Modelling (HLM; Bryk & Raudenbush, 1992) is a strategy that
investigates data at more than one level of analysis. This analysis takes into
account both individual and team level variance. To explore the relationships in
this study the following research questions were examined. How much does
stress vary across teams? Do team process variables influence stress?
Data from 136 teams (n = 1,121) were analysed using HLM (teams with 4 or less
members were removed from analysis to improve reliability). Variables were
chosen that significantly correlated with stress: participation, support for
innovation, team objectives, emphasis on quality, reflexivity, social relations, role
understanding, knowledge of team outcomes and teamness (a composite of the
four criteria variables to identify team membership). Team tenure, age and gender
were used as control variables.
HLM demonstrates that 3.4% of the total variance in stress is explained by team
factors (this is significant, given that the GHQ measures general life stress rather
than work-related stress in particular). More than75% of this variance can be
explained by team processes (as measured by the TCI scales – clarity of team
objectives, emphasis on quality, participation and support for innovation).
Study 3:
Do Team Inputs and Processes Predict Team Member Retention?
• Around 10% of teams in the sample ceased to exist in the six-month study
period and there is an average of 16% turnover of team members in the
remaining teams.
• Larger teams have lower levels of retention.
• Clear team objectives and high levels of team participation predict
member retention.

Results
57 teams from 4 NHS trusts (75% of those originally participating) participated in the
survey (31 nursing care, 13 management, 5 multi-disciplinary, 5 quality improvement
teams, 2 medical teams and 1 administrative support team). Data from the quality
improvement teams were removed from the data set as these teams were not
permanent and several had ceased to exist having completed their tasks. The final
sample for analysis comprised 52 teams (mean size 11.8, SD 6.03, range 2 to 25).
Nineteen teams did not respond to the survey (mean size 9.0, SD 4.9, range 2 to 19.
No information is available as to the turnover in these teams. A comparison of means
was undertaken across study variables obtained at Time 1 to identify any differences
between responders and non-responders. No significant differences emerged.
A high rate of turnover was reported amongst the teams surveyed. 10% (5) of the
teams ceased to exist and only 12% (6) of teams reported no change in membership
(either joiners or leavers) over the six months period of the study. On average, there
were two leavers per team (mean = 1.90; SD = 1.94; range 0 to 8), and an average
16% turnover during the study period (mean = 16.1; SD = 15.8; range 0 to 71.4%).
26.3% of teams reported no leavers.


Team size and type of Trust are associated with turnover. People are more likely to
leave a team if they work in a teaching Trust (Chi-square 8.43, df 2, p < .05) and are
members of a larger team (Pearson correlation: r = .23 between log percentage
leaver and team size p < .05, one-tailed test). Regression analyses revealed that
team size and Trust type accounted for 15% and 18% of the variance in turnover
respectively. There was no evidence to suggest that stress at Time 1 was
associated with team turnover at Time 2.
Perceptions of clear team objectives and high levels of participation were significantly
associated with low levels of turnover, such that in teams whose members were clear
about and committed to the team objectives, and who reported high levels of team
participation at Time 1, there were lower levels of turnover between the two
measurement points. (See Figure 9.3).
Regression analysis (controlling for team size and Trust type) revealed that team
process variables treated as a block (participation, support for innovation, team
objectives and emphasis on quality) explained 10% of the variance in team turnover
or team member retention.
Conclusions
Overall these three studies suggest the value to NHS employees in secondary care
of working in teams, and particularly in teams that are characterised by clear
objectives, high levels of participation, emphasis on quality and support for
innovation. Taken together with the findings reported in earlier chapters, it
suggests teamworking is a means for promoting effectiveness in the NHS and the
well-being of employees. Perhaps most striking is the finding from a recently
completed study by the Aston research team (West, Borrill and colleagues)
revealing that the percentage of Trust staff working in teams in acute trusts is
associated with lower levels of patient mortality. The more people who work in
teams in Trusts, the lower the number of patient deaths measured by the Sunday

Times (Dr Foster) Mortality Index, deaths within 30 days of emergency surgery and
deaths after admission for hip fracture.
We now turn to examine the results of the intensive analysis of team meetings and
communication amongst primary health care and community mental health teams,
carried out by the Human Communications Research Centre at the Universities of
Glasgow and Edinburgh in collaboration with the Leeds and Aston research groups.

Chapter 10
Meetings and CommunicationResearch Methods
Introduction
Meetings are important for effective teamworking, providing teams with their main
opportunity for communicating. They are particularly important in health care teams
where the team members often work in different locations and therefore have little
opportunity for communication. For this part of the work, we have compiled two
different sources of information about team meetings. The first source details the
range of meetings held within the team and who is invited or expected to attend
them. This information was derived from the practice manager interviews in PHCTs
and the CMHT. This allows us to assess how much communication took place in a
team, especially across different disciplines, where links are usually the poorest.
However, even within teams which hold many meetings, with good links across
disciplines, communication can be good or poor, depending on how those meetings
are conducted. Therefore our second source of information is recordings of team
meetings, from which we draw both quantitative measures and observations about
meeting practice.
Communication and decision making in teams
Communication in meetings is important in teams for two different reasons. First,
effective teamworking requires everyone to be both well-informed and to be invested
in the team's overall goals and plans. Although there are other methods for keeping
team members informed, such as newsletters, bulletin boards, and informal
conversations, meetings are a common way of doing it. Meetings are the most
effective method of involving a group of people in activities which require discussion.
Team members who have been involved in the discussions of the team's goals or
plans, or in the decision-making process itself, are more likely to feel that they "own"
those goals and plans and to work actively to bring them about (Weldon & Weingart,
1993). Second, the plans which a team develops are likely to be better, the wider the
pool of views they take into consideration. Each individual in a team will have their
own unique perspective on how health care can best be provided in that team's
circumstances; in particular, team members from different disciplines encounter very

different situations in their daily working lives and therefore will have different ideas
about what should be done. Providing the best care means synthesising this
diversity of views into a co-ordinated plan which is understood and accepted by
everyone on the team. Therefore two important properties of team communication
are that everyone participates and especially that every discipline is involved in
discussion.
Barriers to effective communication
One of the classic problems for all teams, and not just ones from the health care
sector, is that when there are status differences between team members, higher
status members are more likely to attend the most important meetings. Even within a
single meeting, higher status members are likely to make the contributions which
drive the meeting, such as giving information, asking questions, and making
suggestions; lower status members are usually restricted to relatively short,
responsive contributions such as answering questions or expressing agreement with
something that has been said (Berger, Rosenholtz, & Zelditch Jr., 1980; Berger,
Fisek, Norman, & Zelditch Jr, 1977). This tends to make lower status members less
invested in the team's plans and to limit the range of ideas about potential changes to
increase effectiveness that the team actively discusses. In manufacturing industry,
for instance, it has been argued that strictly hierarchical management structures are
insufficient to deal with the rate of change in the modern business world because
they promote the flow of information downward but not upward, making it difficult to
adapt using information gained "on the ground." (Burns & Stalker, 1966)
Another classic problem, again universal, is that the larger a group discussion, the
more one person will come to dominate that discussion and the more people will sit
silently rather than contributing actively (Bales, Strodtbeck, Mills, & Roseborough,
1951). In fact, the optimal group size for free discussion is five people, and in any
group larger than around eight, no more than eight people say virtually anything
which is said. In status-differentiated groups, it tends to be the high status individuals
who speak and the low status ones who remain quiet (Berger et. al., 1980); where
one person has authority for decision-making, they tend to control the interaction
(Carletta, Garrod, & Fraser-Krauss, 1998). This can create difficulties for larger
teams unless they can find a way to discuss freely issues in small, cross-disciplinary
groups and then pass ideas forward from them. Finally, there are differences in the
properties of very small groups which make them more suitable for free discussion.

Even in relatively small groups, active discussion in a meeting tends to involve just a
few people at a time, but there is evidence that people who participate actively in a
discussion understand and react to it differently from those who simply overhear it
(Schober & Clark, 1989). In non-status-differentiated groups of five people,
discussions are highly interactive, with people's opinions influenced by whoever they
interacted with the most. Even in groups of just ten people, speakers make longer
utterances as if lecturing to the whole group, and whoever speaks the most has the
most influence (Fay, Garrod, & Carletta, 2000). This means that for good discussion
across disciplines, it is important to keep the groups small and make sure that status
is not an issue as far as that is possible, so that everyone has at least some chance
to interact with everyone else. Because people are more likely to have informal
conversations outside meetings with people they encounter and see as similar to
themselves — i.e., staff from the same discipline — this makes cross-disciplinary
discussion in meetings all the more important.
Methods
Our general interview methods have already been detailed in chapter 3; interviews
were held with the practice manager for primary health care teams and the team
leader in the community mental health care teams answered a questionnaire.
Information was collected about the set of meetings held within the team, who was
invited or expected to attend them, how long the meetings were, the purpose of the
meetings, and how frequently they were held. The sample sizes for primary health
care teams and community mental health teams are 67 and 92, respectively. The
rest of this section describes the methods used in order to obtain a corpus of
recorded meetings.
Team Selection
Within the primary health care sector, all teams undertaking the questionnaire and
interview section of the Health Care Team Effectiveness study were invited to
participate in recording of meetings for further study; selection was first-come first-
served, with no additional selection criteria. In particular, we did not select teams
based on meeting size or on the results of the effectiveness questionnaires. Twelve
teams volunteered for this part of the study. Meeting size ranged from three people
to twenty-five. The teams recorded were reasonably representative of the larger
sample of primary health care teams.
Meeting Selection
Recordings were made of multi-disciplinary decision-making meetings as it was
expected that these meetings would best reflect effective teamworking. Multi-
disciplinary meetings were defined as those attended by a range of disciplines.

Decision-making meetings were defined as those where in addition to exchanging
information decisions were made during them, again with active participation from the
different disciplines. Primary health care teams provided access to the team’s
business meetings, in which the day-to-day running of the practice was discussed. In
one team, all decisions affecting the practice were made solely by the partners, all of
whom were doctors, and therefore there were no multi-disciplinary decision-making
meetings to record. In this case the partners’ meeting was recorded. For community
mental health teams, the meetings again were multi-disciplinary business meetings in
which decisions were made about the running of the team. Wherever possible, two
meetings of the same type were recorded for each team. Dates for meeting
recording were at the discretion of the practice; therefore the two meetings recorded
were not always in sequence.
Before each meeting was recorded, the primary contact for the team, usually the
meeting chairman, was briefed that the meeting was to be kept as naturalistic as
possible. It was requested that recorded meetings should be held in their usual
locations, with their usual meeting protocols (agendas, minutes, chairing procedures,
etc.), and that attendance should be the same as if the meeting were not being
recorded. The researcher who tended the recording equipment made herself as
unobtrusive as possible.
Equipment used
Audio recording was conducted with two omni-directional PZM tabletop microphones
linked to different channels of a high quality audiotape recorder; the microphones
were set up so as to maximise channel differentiation but to be unobtrusive enough
that participants would not move them. A single static video camera on a tripod was
trained to record the gross movements of as many of the participants as possible;
this record was used only to aid speaker identification during transcription.
Transcription
Before each meeting was opened all participants introduced themselves and their
occupation and on the basis of this was allocated a speaker number. Therefore the
first person to introduce him/herself became speaker 1, the second speaker 2 and so
on. Each participant was referred to by the same speaker number for the transcripts
of both meetings regardless of when they spoke during the second meeting.
Meetings were transcribed from the audiotapes by an audio typist who had not
attended the meeting. Audio typists transcribed complete contributions in order
according to when they began, labelling each contribution by speaker number, but

did not code finer timing information. Speaker identification was facilitated both by
the video recording and by a seating plan drawn up during the meeting by the person
recording the meeting. In previous work using these methods on four to twelve
person meetings, transcribers were able to agree very reliably who made any one
contribution; using the kappa statistic, K=.93, k = 2, N = 230, with an average of 2%
and a maximum of 6% non-backchannel contributions left as unidentified (Carletta et
al., 1998). A contribution was defined as a period of speech from one individual in
which the only major pauses coincided with silence from the other speakers, so that
the pause was likely to be caused by the speaker thinking and not by the speaker
listening to someone else's contribution. Under this definition, speakers cannot follow
themselves in the speaking order. Overlapped speech was transcribed, with the
extent of the overlap roughly marked. Infrequently, parts of the meetings were
omitted because they were so badly overlapped that we could not track individual
contributions. After transcription, the transcripts were completely anonymised taking
out all staff, patient, place names, place and local authority names or possible team
or person identifiers.
An example transcription excerpt is given in Figure 10.1. Transcription proceeds one
contribution per row. Column one contains the speaker number. Column two
contains the words said, combined with some coding information, and column three
contains any notes which the transcriber wished to make (for instance, about people
entering or leaving the room). Column two codes include /num for the approximate
location of the start of another contribution during overlap, italics for anonymised
text, @ for words from the tape which could not be heard clearly, and some common
descriptions of non-linguistic behaviour such as general laughter within the group.
To make the example clear, everything but transcribed speech is indicated in red.
Figure 10.1: An example of the format used for meeting transcription
1 Shall I open /4 the meeting
4 Yep, let’s get on with it. phonerings

3 My apologies I am going to have to leave before the end. I havean appointment in Place 1.
1 Are you skiving off?
Group laughter
Analytical techniques
The primary interest is in how well teams communicate not just overall but also
across disciplines. The analysis therefore relies on a classification of meeting
participants by occupation. For ease of reference, categories are identified by colour
as well as number. For primary health care teams, we have used the following
categories.
1 GPs2 practice managers3 practice nursing staff, including nurse practitioners4 attached staff (mostly health visitors and district nurses)5 administrative staff (mostly secretaries and receptionists)6 Miscellaneous
For community mental health teams, the categories are instead:
1 Psychiatrists2 nursing staff3 occupational therapists4 psychologists, psychotherapists, and other therapists5 Managers6 staff from social services7 Miscellaneous
Both kinds of teams rarely had miscellaneous staff or miscellaneous meeting
attenders who were not included in the analysis. In most cases, these were visitors,
students, or staff associated with the physical location such as caretakers and
security staff; for community health care teams, there were also sometimes
representatives of user, carer, or voluntary groups and liaisons to local GPs.
For both the entire range of meetings described in interview and for the recorded
meetings, descriptions were produced of which staff categories interact with each
other. These descriptions are best explained in terms of diagrams. For instance,
consider the following diagrammatic representation of one of the recorded primary
health care team meetings:

Figure 10.2: Communication in a primary health care team meeting
1
2
3456
7
8
9
10
11
12
1 314 15
16
1 7
18
1 9
heavy: > 2 1
medi um: > 14
l i ght : > 7
70 minutes68% of team present
In the diagram, each person is represented by a coloured circle, where the colour
represents their occupational category. How often each person spoke immediately
before or after each other person is represented by the line between their two circles.
Heavy lines mean the people took adjacent turns relatively often; light or no lines
means that they took adjacent turns relatively rarely. When people take adjacent
turns in meetings of this type, they are usually (but not always) communicating
directly with each other and addressing the same topic. The actual line darknesses
are determined by the maximum number of times anyone followed anyone in the
meeting and using that to construct quartiles; no line is shown when the number of
adjacent turns the two people took is less than a fourth of this maximum, a light line
when it is less than half, and so on. For instance, in the diagram shown, nineteen
people attended the meeting, of which seven were doctors (indicated in red), and the
heaviest interaction was between participants 3 and 6, 3 and 8, and 8 and 1. Despite
the fact that no pairs were able to interact very many times (as indicated by the
numbers in the legend) this was a quite long meeting. Although the numbers in the
legend are affected by meeting length, smaller meetings are more likely to have high
numbers because there are fewer possible pairs to interact, and therefore the
potential for any given pair to interact is greater. High numbers in the legend of a
large meeting, unless it is unusually long, indicate that most of the possible pairs of

people do not interact with each other at all, and usually means that many of the
people attending the meeting say little or nothing.
In the diagram just observed, quite a few pairs of people interact, showing that, at
least among those who participate actively, the interaction is quite free. However,
although there are many people present at the meeting and they represent all of the
occupational categories, the interaction is almost exclusively among the GPs and
practice manager. It is also possible for interaction to occur primarily between one
person and others within the meeting (see Figure 10.3).
Figure 10.3: Communication in a primary health care team meeting
1
2
3456
7
8
9
10
11
12
1 314 15
16
1 7
18
1 9
heavy: > 7
medi um: > 4
l i ght : > 2
30 minutes40% of team present
This usually indicates strong chairing of the meeting, although the chair may only be
choosing who will speak next rather than actively controlling the topic of the
discussion or making contributions to the topic him or herself. Alternatively, it may
indicate that the purpose of the meeting was for the dominant person to give a report,
with others asking clarification questions as needed. Whether the diagrams indicate
interaction among many pairs or interaction through one central person, the
interaction which exists can be more or less cross-disciplinary, depending on the mix
of people who actively contribute to the meeting.
The same sort of diagram serves for the interview data. Consider the following
depiction of the set of meetings in a community mental health team:

Figure 10.4: Communication in a community mental health team
Here, instead of representing individuals, the coloured circles represent staff
categories. Instead of representing the number of times people took adjacent turns,
the lines show the number of minutes per month which representatives of the two
categories spend in the same meetings. Lines around a circle show all meetings
which someone from that staff discipline attended. For instance, this diagram shows
a team in which psychiatrists never attended meetings, not even ones only with other
psychiatrists. As in the diagrams for the recorded meetings, the darker the line, the
more communication occurred.
As well as providing a descriptive account of meeting practice in health care teams,
we also derive quantitative measures of communication from what we observed.
Recall that good communication among the pairs of individuals in a team and among
the pairs of disciplines is theoretically important for effective teamworking. To
measure this, we have devised a score for freedom of interaction (Carletta et. al.,
1998). For a recorded meeting, the freer the interaction, the more pairs of
participants take adjacent turns. This is reflected in the diagrams by how "starry"
they appear. Similarly, starriness in the diagram for a set of meetings reflects how
free the interaction is in general among the different staff disciplines. Freedom of
interaction is scored based on either the meeting transcripts or the interview data.
The scores vary between 0 and 1, with high scores reflecting high freedom of
interaction. Similarly, for the individual meetings, since it is important to know
whether high status individuals are over-represented in the communication, we score
12
3
4
5
6
v er y l i gh t : < 2 1 3
l i gh t : < 4 2 7
m edi u m : < 6 4 1
h eav y : < 8 5 5

equality of participation from 0 to 1. Meetings with equal participation have the same
darkness of lines coming from each of the participants if they are added together, but
do not necessarily link all the pairs and therefore do not necessarily have very free
interaction. Other measures for both individual meetings and the set of meetings for
a team as a whole consider the amount of communication which occurs, sometimes
divided by individual or discipline, and who attends meetings.

Chapter 11
Analysis of Communication in PHCT teams
Summary of Findings
§ Meetings in primary health care are often badly managed and dysfunctional
§ Attached staff (i.e. health visitors and district nurses) often miss team meetings,yet support for innovation is higher in teams where they attend.
§ Better meeting attendance in PCHTs is associated with care that is more patientcentred.
§ In primary health care, team meetings are often re-arranged, cancelled or start
late.
§ When teams do meet many PHCT team members remain silent throughout themeetings.
§ In over half the meetings we recorded no group decisions are taken.
Types of meetings
"A meeting" is defined as a set of people, who meet usually at some regular interval,
for a particular purpose. Adding together the time devoted to the different meetings
reported - all the meetings which involved any part of the team - shows that primary
health care team members spend relatively little of their time in meetings. On
average, there was a meeting involving some part of the team for 325 minutes per
month (range 22 - 1190, S.D. 240); that is team members spent about 3% of their
time in meetings. The primary health care teams in the sample had between 1 and 6
meetings. The frequency of these meetings ranged from weekly to yearly. Primary
health care meetings tended to fall into the following categories, divided by who
attended them:

Figure 11.1: Primary health care meetings
1
2
3
4
5
Whole team meetings, usually held monthly and attended byeither the whole team or at least by representatives of each ofthe disciplines (22% of sample).
1
2
3
4
5
Single discipline meetings for doctors or for administrativestaff, sometimes with practice management also attending (28%and 3% of sample, respectively). Doctors meetings weretypically weekly or monthly; administrative meetings wereusually monthly or every two months.
1
2
3
4
5
Practice clinical meetings attended only by those cliniciansbased in the practice, and sometimes by the practicemanagement (43% of sample). These meetings were usuallymonthly but some practices held them weekly.
1
2
3
4
5
Full practice meetings, usually held monthly and attended byall staff based at the practice: management, doctors, practicenurses, and administrative staff (7% of sample).
1
2
3
4
5
Clinical staff meetings, usually held monthly and attended byall clinicians included attached ones, and sometimes by thepractice management (16% of sample).
1
2
3
4
5
Nursing meetings attended by the practice nurses andattached staff such as health visitors and district nurses (6% ofsample).
Diagrams shown are representative of the types, but not all meetings in the category
conform completely to the diagram. Nursing meetings were the only ones which were
never attended by the practice management. For each meeting type, there was no
relationship between whether or not a team held a meeting of that type and the

team's size (unrelated t-tests, allowing for unequal sample sizes). The set of
meetings which a team held divided teams into the following categories, with the
following typical diagrams. For each category, we give the mean, minimum, and
maximum size of team with that meeting practice.
• Unitary: Teams with whole team meetings and nothing else (mean team size
14, min. 8, max. 26).
• Multiplex: Teams with both a clinical staff meeting which included attached staff
and either a full practice, practice clinical, or single discipline doctors meeting.
One-quarter of these teams also held a whole team meeting (mean team size 23,
min. 10, max. 51).
• Unitary-plus: Teams which hold whole team meetings plus either a separate
doctors meeting or a separate practice clinical meeting (mean team size 23, min.
10, max. 45).
• Practice-based: Teams whose most inclusive meetings were full practice clinical
ones. These teams sometimes had additional single discipline meetings. In this
category, attached staff such as health visitors never attended any meetings and
administrative staff never met with anyone outside of their single discipline
meeting (mean team size 21, min. 8, max. 64).
• Isolated: Teams which had nothing which could be categorised as a team
meeting. In these cases, the only cross-disciplinary meetings might mix practice
nurses and health visitors. These teams tended to report some single discipline
meetings (mean team size 24, min. 17, max. 37).
Of these types, multiplex, unitary-plus, and practice-based were the most common,
with relatively few teams having just a whole team meeting (the unitary category) or
no true cross-disciplinary meetings (isolated). (See Figure 11.2).

Figure 11.2: Proportions of multiplex, unitary-plus, unitary, practice-based, andisolated Teams
29%
28%7%
27%
9%
Multiplex
Unitary-plus
Unitary
Practice-based
Isolated
In practice-based and isolated teams, communications with attached staff could be
insufficient, causing inefficiencies and lack of direction. Unitary teams might require
a great deal of informal communication to supplement meetings; this is more likely to
be a successful strategy for fairly small teams, which is in fact where the meeting
practice tends to occur.
One might expect teams which have more inclusive meetings - those with whole
team, full practice, or clinical staff meetings - to have higher self-reported
team-working effectiveness scores, because these teams tend to have more chances
for cross-disciplinary communication. Although the occurrence of a whole team
meeting is unrelated to self-reported teamworking effectiveness (unrelated t-test,
t = -1.32, NS), the occurrence of full practice and clinical staff meetings is (for full
practice meetings, t = -2.44, df = 6S, p<.O2 with a mean teamworking score of 4.66
for teams without a meeting and 5.30 for teams with one; for clinical staff meetings,
Levene's F = 4.64, p <.04, with teams without a meeting having the more varied
scores; t with unequal variances = -2.11, df = 48.78, p<.05; mean without meeting
4.63, mean with meeting 5.01). Since the meetings we recorded are whole team

meetings, we will return to why this might be the case after we have considered what
form they take.
Processes within meetings
Meeting practice in PHCTs varies considerably. In this section we describe the
meetings recorded in terms of who attended, how long they were, meeting practice,
and interactional characteristics.
Interpreting date relating to the relationships between communication in the recorded
sample and other variables such as effectiveness and team processes, is
challenging. Primary health care teams are highly variable, not just in terms of input
factors, involving team context. For instance, one of the recorded teams, identified as
Team A, was made up half of new staff who had been brought in with the explicit aim
of changing the ethos of the practice. We observed that the atmosphere in this
practice was quite tense, and, they were one of only three teams in the wider sample
not to hold a Christmas party. This team had very low self-report effectiveness
scores compared to the rest of the recorded sub sample for all but the sub scale
reflecting professional delivery of care. They also declined to have a second meeting
recorded. For this reason, the team was omitted from analyses involving
effectiveness and team processes variables, but shown in graphs. In addition,
differences in meeting practice made it necessary to omit further teams for certain
parts of the analysis.
Because of the small sample size, it is not always possible to test whether
assumptions of normality and linearity are warranted for our statistical analysis. In
order to make the analysis more robust, we categorise teams into two sets, high and
low, for each of the properties of communication which we investigate, and employ
tests. Where these show a difference, we then go on to show the relationship
graphically and to characterise it using correlations.
In most cases, the teams held one meeting which they considered to be for the whole
team. These meetings were open, with all team members expected to attend.
Although the meeting remit was not always clear, the teams used these meetings as
their opportunity to discuss matters affecting the practice. There were three obvious
exceptions. One of the teams, identified as Team B, was strictly controlled by the
partners and never held multi-disciplinary meetings. Their team meetings were

attended by the partners and practice manager only, and even took place away from
the practice, in one of the partners' kitchens. This team had very low effectiveness
and team processes scores compared to the other teams in the sub sample. Like
Team A, they also declined to have a second meeting recorded. Another team,
identified as Team C, did not hold one whole team meeting, but had two highly multi-
disciplinary sub-teams with specific remits which were meant to improve the working
of the practice. One sub-team discussed how to make the best use of the nursing
staff within the practice, while the other discussed initiatives to improve preventative
care (for instance, an anti-smoking campaign). A third team reported that they held
team meetings and gave us permission to record them. However when we
attempted to arrange to record meetings, the team claimed that they were not holding
any meetings which would be appropriate. This team had average self-reported
effectiveness scores.
Figure 11.3: Length of recorded PHCT meetings
meeting length (minutes)
The recorded sample is larger than the set of analysed meetings due to recording difficulties.
PHCTs had regular time set aside for weekly or monthly team meeting. However they
were quite often rearranged or cancelled completely. Meetings often started late,
with people coming in late and leaving early in order to complete their other duties.
Many of those attending were silent throughout and appeared bored: many
commented informally to the researcher that the issues discussed in meetings were
irrelevant to them. Meeting agendas were quite vague. Early business in the
meetings, tabled on the agenda, tended to consist of items which the practice
manager felt it was important to discuss. However, most of the meeting time was

taken up by "any other business" raised by other people present. In many cases,
items which the practice manager were put off in order to accommodate unscheduled
discussion. We observed that for many teams, items raised at the beginning of the
first meeting we recorded had not been dealt with by the end of the second meeting.
Only one team kept rigidly to the agenda, with no unscheduled discussion. Meeting
chairs were usually practice managers, GPs, or practice nurses. (See Figure 11.4).
However, the degree of control which chairs exerted over the meetings varied
considerably, with some chairs, particularly those who were nursery and
administrative staff, merely announced the next step on the agenda as prior
discussion came to a close.
Figure 11.4: Who chaired the recorded PHCT meetings, by occupational class
In the meetings we recorded the decisions made which affected the entire team.
Often the issues discussed were logistical; financial or business issues were
discussed in different meetings. The official agenda in individual meetings tended to
focus on one or two large issues, such as auditing team performance or clinic
management. However, the majority of meeting time was spent discussing less
weighty, more social issues such as what to do on practice nights out, whether to
have a fish tank in the waiting room, and where to go for a Christmas party. These
discussions rarely remained focused therefore they tended to take up more time than
the critical issues.
Who cha ir ed t he r ecor ded PHCT meet ings,by occupa t iona l cla ss.
GP
PM
PN
ATTACHED
ADMINMISC

Although the meetings we recorded had been identified by teams as decision-
making, we found that decisions were not made in the meetings. Where decisions
were made, they were often about how to proceed with the issues discussed; for
instance, in these meetings, the team might decide to call another, often smaller,
meeting for more discussion. Major decisions affecting the team members, such as
changing a clinic date or recruiting more staff, were taken in a different forum and
reported back to the 'decision making' meetings. Thus these meetings were largely
for exchanging information and a forum so that there would be a place where team
members could express their opinions. Some of the individual participants
complained informally to the researcher carrying out the recordings that the meetings
were boring and that the issues which they addressed were completely irrelevant to
them.
Figure 11.5: Primary health care meetings vary considerably in size
Number of People attending PHCT meetings
..
.
To score general attendance, one can use the average proportion of team members
who attended recorded meetings. All of the recorded teams considered their
meetings to be open to all team members except for Team B, which openly restricted
20 75 100 125 200 225 300
Meeting
size
Number of People

attendance to GPs and the practice manager, and Team C, which was organised into
sub-teams. Omitting these two teams, there is a relationship between team size and
the proportion of members attending recorded meetings (see Figure 11.60 (dividing
teams into two sets, small and large, (t = -3.64, df = 7, p = .01 two-tailed; small teams
have the higher proportions).
Figure 11.6: The relationship between team size and meeting attendance for whole team meetings
Team C
Other teams
The relationship between team sizeand
meeting attendance for whole teammeetings.
Team B is omitted from the graph because team size isunavailable. Fitshown without TeamC.
team size
5040302010
.9
.8
.7
.6
.5
.4
.3
.2
.1
One likely reason for this is the workload of health care team members. The bigger
the team, the harder it is to schedule meetings at times that are suitable for
everyone, and the more likely is that members will be unable to attend. This needs to
be taken into account when interpreting results based on this general attendance
score. Team A was omitted from the analysis because it had disproportionately low
effectiveness and Teams B and C because they did not hold whole team meetings.
When the average attendance was divided into two sets, low and high, a relationship
was found with one of the self- reported effectiveness sub scales, patient-
centredness of care (see Figure 11.7) (t = 2.42, df=6, p= 0.5 two tailed). Among the
teams that have a higher proportion of team members attending meetings, the
effectiveness score is higher. If a linear correlation between general attendance and

this effectiveness sub scale is assumed, the same result emerged (r = .73, df = 8, p =
.04). This is the case despite the fact that there is no relationship between team size
and patient-centredness of care, either in the sample of teams we recorded or in the
wider sample.
Figure 11.7: The relationship between general attendance and patient-centredness of care
Team A
Other Teams
The relationship between general attendance
and patient-centredness of care.
Teams B and C have been omitted because their meetings are not open to
the whole team. Fit shown without Team A.
average proportion of team members attending meetings
.9.8.7.6.5.4.3.2.1
6.5
6.0
5.5
5.0
4.5
4.0
These results show that higher levels of attendance at meetings is associated with
effectiveness with respect to quality of patient care. The explanation for this, even
though there are no relationships with the other effective variable, can be found if we
consider how the team use meetings. Even during the meetings, agenda items were
often delayed while team members passed on information about individual patients to
other members who were also involved in their care. Team members also used the
time just before and after meetings to have such discussions, although there the
opportunities were less certain because people often came late or left early.
Although these discussions were only useful to a few of the people present and
therefore might be seen as wasting team time, this was the only opportunity many
had to exchange information.
Team members from the differing occupational groups were not equally likely to go to
the meetings recorded; whereas GPs and practice managers nearly always attended.

(See Figure 11.8). The graph includes team members whether they work full or part-
time with the team. Although some categories are more likely to be part-time than
others, and therefore have difficulty attending meetings, all team members still need
some opportunity to communicate with each other.
Figure 11.8: Who attended at least one meeting (in solid), by occupational class,versus total team membership (complete bars)
In addition, not all meetings recorded had at least one representative from each
of the constituent disciplines; whereas all meetings had at least one GP and one
practice manager present, nearly half the recorded meetings did not involve any
attached staff.
Who attended at least one meeting (in solid),by occupational class, versus total team
membership (complete bars).
0
10
20
30
40
50
60
70
80
90
GP PM PN ATTACHED ADMIN MISC
occupational class
numberinsample

Figure 11.9: For each occupational class, percentage of meetings recorded whichhad someone from that class attending
Team B deliberately excluded all members except GPs and the practice manager.
Two teams where we were able to record two meetings did not have any attached
staff present at either one. Some practice managers remarked informally that for
some individuals, failure to attend was quite regular and tended to cause resentment
among the other team members.
The meetings which we recorded were in all cases the largest and most
multi-disciplinary meetings which the teams held. As a result, we can use who
attended the recorded meetings as a measure of integration in between the different
disciplines. Although team meetings were only one of many ways in which a team
communicated internally, it is likely that team members and disciplines that had poor
attendance at meetings would be less well-informed and less involved in decision-
making. This was most likely to apply to attached staff such as health visitors and
district nurses. Not only were they least likely to attend team meetings, as the
interview data shows, in most team these were the only meetings they were
expected to attend. Much of the work of attached staff was carried out away from the
practice premises, therefore they were least able to communicate with other team
F o r e a c h o c c u p a t io n a l c la s s , p e r c e n t a g e
o f m e e t in g s r e c o r d e d wh ic h h a d s o m e o n e
f r o m t h a t c la s s a t t e n d in g .
0 %
2 0 %
4 0 %
6 0 %
8 0 %
1 0 0 %
1 2 0 %
GP P M P N A T T A DM IN M IS C
o c c u p a t i o n a l c l a s s

members in other ways. From the content of the meetings it was clear that because
attached staff do most of the home visits for the practice more than other team
members, they were more in touch with both the circumstances of individual patients
and patient needs in general. The recordings of team meetings also suggested that
detached staff were the most aware of inefficiencies within the practice arising from
GP's performing tasks that other team members could do (for instance/GPs making
home visits on the same day as an attached team member). Thus for this analysis,
we use two measures to reflect the discipline mix of meeting attendance. The first, a
score for multi-disciplinarity of meetings, is the average number of occupational
categories present at a team's recorded meetings, out of our list of five. The second
is simply whether or not at least one attached staff member was present at one of the
meetings we recorded. These scores are highly related, since no teams ever had an
attached staff member present unless all of the other disciplines were represented as
well; that is, for teams that ever had an attached staff member present, the multi-
disciplinarity rating was over 4.
There is no relationship between self-reported effectiveness and either of these
measures. However, the data suggest a relationship between self-reported support
for innovation and multi-disciplinarity of team meetings, if we omit Team A on the
grounds of its disproportionately poor team processes. If Team A is omitted, support
for innovation is higher when attached staff are present for at least one of the team's
recorded meetings (t = -3.76, df = 8, p = .006 two-tailed).
Dividing the multi-disciplinarity score into two sets, low and high, more multi-
disciplinary teams have higher support for innovation (t = -2.8, df = 8, p = .02 two-
tailed; r = .8347, df = 10, p = .003 two-tailed).

Figure 11.10: Fit shown with (solid) and without (dotted) Team A
This result suggests that team members viewed these meetings as their chance to
raise new ideas within the team. For this sample, as for the wider study, only around
a quarter of the team members providing self-reports for team processes were
attached staff (in this sample, mean 22.56%, min 8.33%~ max 38.46%). Therefore it
is unlikely that the differences were a result of attached staff themselves reporting
that they feel the team supports innovation; a more likely explanation is that their
presence affects the entire team.
We used the 'freedom of interaction' and 'equality of participation' scores previously
to study interactions during meetings in small to medium-sized manufacturing firms.
In that study we confirmed that the scores differentiate groups which operate as
teams, with equal responsibility among the members, from groups in which one
person has overall authority. Equality of participation and freedom of interaction
were higher for the teams, showing that they engage in freer discussion. Primary
health care teams behave like equal responsibility teams and not like the managed
groups. Restricting consideration to teams in the same size range (fewer than
thirteen members), PHCT scores are higher and less varied than the industry scores
as a complete set (for equality of participation, F = 6.725, p = .014 two-tailed;
t = 3.76, df = 3l.53, p = .001 two-tailed; for freedom of interaction, F = 5.028, p = .032
two-tailed; t = 2.50, df = 33.05, p = .017 two-tailed), but indistinguishable from the
T e a m A
O th er te am s
i t sho w n w ith (so lid) andwithout (dotted) TeamAA.
A t least one attached mem ber w as presen t fo r at least one
m eeting if number o f categories presen t exceeds 4.
number of occupational categories present
5 .55.04 .54.03.53.02.52 .01 .5
4.0
3.8
3.6
3.4
3.2
3.0
2.8 *

equal responsibility subset (for equality of participation, F = .72l, NS; t = l.57, df = 22,
NS; for freedom of interaction, F = 3.582, NS; t = .60, df = 22, NS). Although the
teams have nominal chairs, for the most part the meetings are not strictly led. This is
surprising because it is generally difficult to have free discussions in such large
groups. In addition, status differences tend to make interaction less free, and GPs
are both traditionally high status and the employers of many of the team members.
Under the circumstances, if free discussion is what is required, these teams are
doing better at allowing them to occur than one would ordinarily expect.
Conclusion
In primary health care teams, good general attendance at team meetings was linked
to self-reported patient-centredness of care. An explanation for this seems to be that
meetings gave individuals the opportunity to have conversations and exchange
information about patients. However, whole team meetings do not appear to make
the team believe they are more effective in other ways. In particular, teams that have
whole team meetings do not believe they are any better at teamworking than teams
that do not, even though full practice meetings and clinical staff meetings do improve
a team's impression of their teamworking skills. These differences may arise from a
sense of the purpose of a meeting. Team members may have felt that it was
important to meet, but have been unsure about who should go to the meeting and
what should be discussed. Being aware that a meeting is necessary requires that
team members know that people need to communicate, but knowing how to
communicate requires more preparation. Where there is uncertainty about the
purpose of the meeting, the practice was to suggest that everyone (or at least
representatives from each staff group) attended just in case something important was
discussed. It was only possible to know which staff could be excluded when the
remit of the meeting was clear. Although whole team meetings could be useful if
they had a clear purpose that included everyone who attended, the meetings that we
observed often did not have this character. Instead, because of the lack of direction,
many staff members saw the meetings as irrelevant and a waste of their time.
Attending meetings that are seen as irrelevant may have a demoralising effect on
staff with further ramifications for the team's work. Therefore it is important for teams
to consider their meeting practice and to make sure it is designed to best fit their
circumstances.

Chapter 12
Analysis of Communication in CMHT's
_____________________________________________________________________
Summary of Findings
• CMHT members spent three times more time in meetings than PHCT members
• The more cross-disciplinary meetings held in a CMHT the lower the stress levels
in the team
• CMHT meetings were generally well organised and multi-disciplinary
• In 90% of CMHT meetings effective group decisions were taken
• The prototypical CMHT meeting combined operational and clinical decision
making and contained about 9-13 members
• CPNs and Social workers were the best represented in the meetings but there
was also regular attendance of occupational therapists, psychologists and
psychiatrists

Types of Meetings
The number of different meetings was larger and more varied in community mental
health teams than in primary health care teams (range 1 to 11, mean 4.36, SD 1.77).
(See Figure 12.1).
Figure 12.1: Number of meetings
Number of meetings in total
111087654321
30
20
10
0
Teams identified over 20 types of meeting, which we considered to fall within fourcategories:
• Clinical, including audit/quality; day care meetings; ward rounds; representation
at PHCT meetings; CPA reviews; allocation; referrals
• Operational, including MDT meetings; business; locality, sector or patch
meetings; team leader meetings; management; communication
• Strategy, including planning meetings, away days, and team building
• Professional development, including education or training meetings;
professional group meetings; supervision; support
Some of the meetings described, for example, PHCT, ward rounds, locality, sector,patch, or team leader meetings, were not strictly team meetings, although the CMHTwas represented and received clinical, operational or strategic input from such

meetings. There is some confusion between clinical and operational meetings in thedata set because teams tended to mix these two functions, for instance, by callingone meeting which first performed case allocation and then handled business issues.81% of teams reported having clinical meetings and 97% reported having operationalmeetings; these two types of meetings are probably ubiquitous, with the teamsreporting no meetings of a type performing that function as part of another meeting.Strategy and professional development meetings were reported by 16% and 48% ofthe teams, respectively. Probably because they held so many different meetings,counting up the number of minutes per month that at least part of the team is in ameeting gives an average of around 1000 minutes per month (range 140-2940, S.D.608). This means that on average, there was a meeting happening a tenth of thetime involving at least part of the team.
Because of the variety of meeting types, it is less useful to characterise team practice
as a whole in terms of the set of meetings which a team holds than to consider which
disciplines engage in meetings with each other. In these teams, communication was
usually very strong across the constituent disciplines. Teams generally fell into one
of four categories of practice. (See Figure 12.2).

Figure 12.2: Four Categories of Practice
12
3
4
5
6
Teams exhibiting complete connectivity might have somedirect links missing --- for instance, in the example shown,managers never met directly with occupational therapists --- butall disciplines were involved in some cross-disciplinary meetings.In just under half of these teams, all disciplines encountered allothers in meetings.
12
3
4
5
6
Team with one isolate exhibited complete connectivity for five ofthe six disciplines, but one discipline was never involved incross-disciplinary meetings. In two-thirds of these cases, theisolated discipline was management; the remaining cases weredistributed evenly among psychiatry, occupational therapy, andpsychology.
12
3
4
5
6
Teams with a psychiatry + nursing + social services axisshowed good connectivity for these three disciplines. Just overhalf of these cases only ever had these three disciplinescommunicate together in meetings. In the remaining cases,these three disciplines were included, but so was one other, withall the others equally likely to be the additional inclusion.
12
3
4
5
6
Teams with a nursing + social services axis showed goodconnectivity between these two disciplines, and also usuallyincluded cross-disciplinary meetings with one or two otherdisciplines, but never with psychiatry. In over half of thesecases, occupational therapists were involved in meetings, butthere were also examples with management and psychologyinvolvement.
All of these categories were reasonably common in the sample, but the categories
showing better overall connections were more prevalent:

Figure 12.3: Cross-disciplinary communication in CMHT meetings
Cross-disciplinary communication inCMHT Meetings
33%
32%
23%
12%
Complete connectivity
One isolate
Psychiatry+nursing+socialservices axis
Nursing+social services axis
Processes in Meetings
What we can see from this analysis is that in terms of communication in meetings,
nursing and social services staff tend to form the core of the team, with psychiatry in
close contact and management most likely to be isolated. Although what happens in
meetings is not necessarily indicative of communications in the team as a whole,
meetings provide opportunities to discuss work and develop good relationships not
just during the meetings themselves, but also beforehand and afterwards. Therefore
we would expect this pattern to hold for the teams overall, even outside their
meetings.
Which meeting communication pattern a team has is not completely arbitrary.
Omitting three teams with more than 35 members and six teams which were
strangely constituted (usually nursing-only teams rather than cross-disciplinary
teams), freedom of interaction is related to commissioning (one-way ANOVA F (2,79)
= 3.41, p<.05). In our descriptive analysis, the categories divided according to
whether psychiatry was connected to the core team and whether management was
ever involved in cross-disciplinary meetings. Whether or not psychiatrists ever met
with staff from social services is related to how the team was commissioned (X2 =
6.78, df = 2, p<.05).

Teams which are commissioned by health service and social services separately are
more likely to have psychiatrists meet with social services than teams which are
commissioned jointly or by the health service only. Whether managers were
involved in meetings at all was also related to commissioning (X2 = 6.45, df = 2, p<.05
two-tailed); again, they were more likely to be involved in teams commissioned
separately. The general pattern is that teams which are commissioned separately
have stronger cross-disciplinary links than the other types.
The complete details of how our quantitative measures of communication in meetings
relate to other variables within our theoretical model of teamworking are given in
Chapters 1, 2 and 5. Summarising from this analysis, the number of minutes per
month a team's meetings takes is related to the length of time the team has been set
up, the percentage of staff full-time in the one team, and the age of the team
members (younger team members spend more time in meetings). Although we can
not be certain why these relationships occur, they do have reasonable explanations.
Part-time staff are simply harder to schedule into meetings than full-time ones.
Teams which have younger and presumably less-experienced members may provide
a somewhat less complicated service for their local clientele or may be less status-
differentiated than other teams, and therefore meet together rather than dividing by
function into smaller meetings. Mature teams have had more opportunity to structure
themselves to fit their circumstances; they presumably divided their meetings by
function to involve smaller sets of people, or, as sometimes happens, they may
accumulate new meetings for new functions without remembering to end ones which
are no longer useful.
Social workers are one of the key disciplines involved in meetings. If there are social
workers in the CMHT itself rather than accessible from outside the team, then the
overall meeting time for the team was lower. This may be because under these
circumstances more of the team's communication can occur informally. The higher
the percentage of men on the team, the more overall meeting time the team had;
percentage of men is almost certainly standing in for some hidden variable, but the
real cause is not clear. The more meeting time a team had, the more quickly the
team deals with emergency referrals and the more quickly emergencies are seen;
this is probably a result of being able to communicate information related to the
emergency itself. Finally, the freer the interaction among disciplines exhibited by the
set of meetings the team holds, the lower the average level of stress for team
members and the lower a team's self-reported innovativeness. This relationship is

probably complex, since communication with colleagues should, by and large, reduce
work stress and allow team members to express ideas which eventually turn into
team innovations, but innovative teams undergo more changes than non-innovative
teams, and change increases stress.
Results derived from CMHT recorded meetings
Meeting practice in CMHTs followed a more consistent pattern than with the PHCTs.
Overall we found the communication in these meetings to be extremely effective. The
meetings were used to make important group decisions and the content of the
meetings was appropriate to their stated purpose. In this section we describe the
recorded meetings in terms of their purpose, meeting practice, multidisciplinary
representation, and the general interactional characteristics. We then use the
analysis to identify good practice in such meetings and highlight what we believe to
be important contributory factors toward good practice.
As in the case of the recorded PHCT meetings we did not think it appropriate to try
and draw strong conclusions about the relationships between communication in the
recorded sample and other variables such as effectiveness or team processes. The
sample is not sufficiently large or diverse to do this. Instead we describe the results in
more qualitative terms and use them to identify prototypical meeting practices in a
CMHT. On the basis of the purpose, content and general interactional characteristics
of the meetings we then define a good practice prototype for CMHT meetings of the
kind recorded.
The purpose of the recorded CMHT meetings
Teams were asked to select for recording routine meetings with strong
multidisciplinary membership. Generally, they chose meetings that fell into the
operational category described earlier. So the meetings were typically weekly team
business meetings, but frequently they also had a clinical component. We recorded
18 meetings from 9 teams and where possible ensured that they were two
consecutive meetings of the same type from each team in the sample. Unfortunately,
for one of the meetings there was a technical problem in recording so it had to be
dropped from the sample. Hence, the analysis was based on a sample of 17
meetings in 9 CMHTs.

Although the meetings fell into the operational category, as business meetings, they
did vary in terms of purpose and this affected their style. In one case the team
selected for recording two special meetings designed to respond to and influence
health department policy on CMHTs. Membership was much larger than for other
meetings in the sample and was quite different. For example, it included health care
managers and a ward manager. The content and communicative style of these
meetings was also quite different from others in the sample. We refer to these as
High Level Policy (HLP) meetings to differentiate them from the others.
A second kind of meeting associated with two of the teams involved dissemination of
policies imposed from above. The purpose of these meetings was to ensure a
detailed understanding of Trust or DoH policy initiatives. In many respects
communication in these particular meetings was less effective than in others. For one
of the teams much of the meeting time was spent reading documents that would
have been better dealt with outside the meetings and decisions about how to deal
with the policy initiatives were regularly put off to subsequent meetings. However,
this team had adopted a rotating chair practice for their meetings and this limited the
ability of the team leader to control the team’s decision making. It could well have
been this factor which led to the apparent ineffectiveness of the decision making. We
take up this issue in the section on meeting practice. We refer to this kind of meeting
as a Policy Dissemination (PD) meeting.
The most frequent kind of meeting in the sample was the weekly team meeting in
which both clinical issues, such as deferrals, and team policy were formulated.
Typically, teams split the meeting into a section on clinical reporting and case
allocation and a subsequent business section. In most cases the business section of
the meeting dealt with team operational issues rather than high-level policy issues.
We shall refer to these as Mixed Purpose (MP) meetings.

Running meetings in CMHTs
Members of CMHTs spend much more time at meetings than do members of
PHCTs. This greater experience is reflected in a generally high standard of meeting
management. In the majority of recorded cases, team meetings were held regularly,
they were well organised and chaired, and had clear agendas. However, there was
some variation in the organisation and style of chairing that did affect the quality of
the decision making at the meetings.
Three important factors in the running of meetings are their regularity, their size and
their duration. In all cases except the rather anomalous HLP type, the team meetings
took place on a weekly basis. The HLP meetings only occurred every two months.
Twenty-one people attended the HLP meetings, but this was also not representative
of the sample. For the meetings as a whole the average size was 11 and it varied
between 5 and 21. (See Figure 12.4). The average duration of the meetings was 71
minutes and it ranged from 38 to 140 minutes. (See Figure 12.5). In most cases the
meetings were scheduled for no more than an hour, but there were a few occasions
when this was extended to two hours for both clinical and business meetings.
Figure 12.4: Size of meetings in terms of number of people present
0
3
6
9
12
15
18
21
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
People present
Num
ber
of p
eopl
e
Meeting

Figure 12.5: Duration of meetings in minutes
For multidisciplinary decision making teams choosing the right size of meetings is
always going to be difficult. On the one hand, groups of more than about 8 or 9 tend
to fall into a non-interactive mode of communication in which each speaker
broadcasts information to the rest of the group. This hinders the process of finding a
true consensus in the group. On the other hand, it is important to have a sufficient
number of people present to ensure effective representation of the different
disciplinary interests. In this situation meetings should be restricted to no more than
about 12 or 13 members and there needs to be an experienced chair. The chair can
then ensure that all relevant voices are heard and promote interactive discussion
when it is needed. This was the practice in a large proportion of the MP type
meetings that we recorded.
For example, in one of the MP meetings the team was confronted with a crucial
decision about how to respond as a team to a change in the sectors they were to
cover. This change, which had been introduced without consultation, meant that
there would be a reduced overlap between the areas covered by team members. The
question was whether they should respond by splitting into two separate groups for
their meetings or remain as a single group. The meeting contained 13 members and
up until this point was characterised by a non-interactive broadcast style of
discussion. So the team leader and chair of the meeting first promoted an extensive
discussion of this issue in which he did not intervene. Then, when everyone had had
0
20
40
60
80
100
120
140
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Leng
th o
f Mee
ting
Meeting

their say, he went round the whole group and allowed each member to indicate their
feelings on the issue before confirming the decision. So although the group contained
13 members it was possible to establish a clear consensual decision about this
important matter. Interestingly, this meeting also managed to get through as much
business as most of the others. Yet, this was all achieved in 40minutes; it was one of
the shortest meetings in our sample.
By contrast, one of the much larger HLP meetings (21 members) faced a situation in
which a group decision should have been made, but it was left up in the air. A young
CNP raised a problem of risk management and safety in the light of a recent
traumatic experience. She had been on a routine visit and on arrival confronted a
suspected suicide. Because she had no portable ‘phone and was in a poorly
provisioned area of the City, she had to return to base before being able to call for
support. The question confronting the meeting was whether to push for provision of
portable phones to all staff engaged in domiciliary visits. This item received
considerable discussion, but because the group was so large the discussion
amounted to a series of long broadcasts where different members expressed their
opinions on everything to do with risk management. After nearly 10 minutes
discussion the problem had not been resolved and was not deferred for subsequent
decision. This does not reflect on the will of the people at the meeting or the ability of
the chair, but rather on the extreme difficulty of making effective group decisions in
meetings of 21 members. In a smaller MP meeting, when confronted with a less
dramatic example of the same problem, the team managed to come up with a co-
ordinated policy, including the provision of portable phones, for just such cases as
this one.
The point illustrated here is that meeting size is crucial to effective group decision
making and that even with relatively small groups of around 12 or 13 members the
process relies on skilful chairing. In relation to this point, two of the teams in our
sample adopted a practice of rotating chairs for meetings. Both had relatively small
meetings (between 6 and 9 members at each). However, it was apparent that the
quality of the group decision making was affected by the practice. For instance, in
one case there was real confusion about who was to monitor and control the
decision; whether it should be the team manager or the chair. In another case at
least 5 minutes was wasted establishing who was to chair the meeting and who to
take the minutes. Although it may seem helpful to give members experience of

chairing meetings, such cases illustrate that ineffective chairing will certainly reduce
the effectiveness of the team’s decision making processes.
For about half of the teams in this sample meeting size was restricted to less than 9
members, which is quite an appropriate size for effective interactive discussion and
group decision.
The content of CMHT meetings and decision making
The content of the recorded meetings fit in with the goals of the meetings. There
were three main areas of discussion: policy, team operations and clinical allocations.
The proportion of meetings in the sample that covered each of these topics is shown
in the Figure 12.6.
The three broad categories of meetings HLP, PD and MPD discussed the three kinds
of issue according to their goals. The HLP meeting predominantly discussed a “green
paper” on mental health care provision in their city. This was quite appropriate to the
meeting because the team had been chosen to elicit feedback from relevant
community groups on the content of the paper. The PD type meetings also discussed
policy, but more in the context of detailed policy documents that had been sent to
their team leader. In MP type meetings there was often also reference to policy, but
only in so far as it was pertinent to particular issues arising from either clinical cases
or team operation.
The second main topic of discussion was what we have called team operation: by
this we mean practices or policies to be adopted by the team that affect the way the
team works. Not surprisingly this topic arose in most of the meetings we recorded. It
was also the source of most team decision making that occurred in the meetings.
Finally, the MP teams also discussed clinical matters. In the meetings we recorded
most clinical (i.e., patient oriented) discussion concerned allocation of cases.
However, there was also discussion of particular problems associated with difficult
cases. For example, in one such case a sectioned patient had been on leave in her
hometown in India. She had written to indicate that she was being held by the family
against her will and was requesting repatriation as a British subject. The team had to
work out an appropriate response to this situation.

Figure 12.6: Content and decision making in CMHT team meetings in terms of %meetings discussing these topics and making group decisions
The figure also shows the proportion of meetings which resulted in 1 or more group
decisions. As can be seen such decisions were made in 88% of the recorded
meetings. These decisions varied from straightforward matters of how to co-ordinate
reports between the nurses, social workers and occupational therapists to more
complicated matters such as formulating an effective security policy for staff on
domiciliary visits. Interestingly these two issues arose in a number of the meetings
and the teams tended to come up with slightly different solutions. The diversity of
decision in operational matters reflected the different circumstances of the teams and
seemed perfectly appropriate.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Policy Teamoperation
Clinical GroupDecision
% o
f mee
tings
Type of decision

Attendance at meetings
The CMHT meetings were attended by a broad range of different categories of staff
representing different professional groups. The figure shows percentages of
meetings attended by each of the major staff categories (see Figure 12.7).
Figure 12.7: Percentage of meetings with a representative from each staff category
All the meetings had representation of both the nursing staff and the social services.
In fact, community psychiatric nurses and social workers were nearly always in the
majority at the meetings. Across all meetings 37% of attendees were CPNs and 24%
were social workers. In more than half of the meetings there were also occupational
therapists, but they only represented 9% of the membership across all meetings. The
two other staff categories of psychiatrists and psychologists were less well
represented. Psychiatrists represented 6% of the attendees and psychologists only
4%.
In a situation where different disciplines are associated with marked differences in
status (e.g., between consultant psychiatrists and CPNs) multidisciplinary
representation at meetings can become a barrier to group decision making. On the
one hand, it is important to have representation from as many groups as possible;
but on the other hand, it is also important to minimise any major disparities in the
0%10%20%30%40%50%60%70%80%90%
100%
psyc
hiat
rists
nurs
ing
staf
f
occu
patio
nal t
hera
pist
s
psyc
holo
gist
s, p
sych
othe
rap.
..m
anag
ers
staf
f fro
m s
ocia
l ser
vice
sm
isce
llane
ous
staf
f
% of meetings

status of the group members. This is especially true for larger groups in which high
status dominant speakers exert a disproportionate influence on the discussion. This
means that notional group decisions tend to become individual decisions that do not
reflect the broader interests of the group.
So it is interesting that there were psychiatrists at only 1 in 10 of the meetings.
Furthermore, we had the strong impression that the meetings in which they were
present were not so effective at making group decisions. They tended to be longer
(average 91 minutes compared to 72 minutes for the others) and generally the
communication was less interactive.
One strategy adopted by CMHTs was to have nursing staff from the hospitals
represent the consultant’s cases at the meeting. This seemed to be a very effective
way of ensuring broader representation without introducing marked disparities of
status within the meeting itself.
Communication dynamics in CMHT
Unfortunately, we encountered some problems with the quality of the video recording
for CMHT meetings. This made it difficult to establish quantitative measures of the
degree of interaction of the kind made with the PHCT meetings. Also the mixed
nature of many meetings with a clinical reporting section followed by a business
section would have made it difficult to interpret overall measures of interactivity and
participation.
From other sources of information, such as the relative length of contributions it is
possible to draw general conclusions about the interactivity of the discussion in the
meetings in the sample. The major contributory factor to interactivity was simply the
size of the meeting. In general, the larger the discussion group the lower the
interactivity in the discussion and this was reflected in the CMHT meetings.
The prototypical CMHT meeting: recommendations on good practice
On the basis of this sample, which represents around 20 hours of discussion in
CMHTs, it is possible to define a prototypical meeting. This can be used both to

describe the overall nature of CMHT team meetings as they occur in our sample and
as a framework for giving recommendations about good practice.
Within our sample of meetings a clear pattern of practice emerged that corresponded
to the results from the interview data. The most common type of meeting was an
operational meeting, which included both a clinical component and a separate
business component. This was the case for more than half of the recorded meetings.
In terms of size this prototypical type of meeting ranged from 5 to 13 members. In
terms of multi-disciplinary representation it fit into the one isolate style of meeting. In
other words, the meeting always contained representatives from nursing and social
work but had either psychiatrists or occupation therapists or psychologists not
represented. We feel that this is probably quite satisfactory in terms of group decision
making because it allows for a sufficiently broad representation without
compromising the size of the group or producing disparities in status.
In relation to this prototype, meetings with around 9-13 members were generally the
most satisfactory for both routine reporting and case management as well as more
general group decision making. However, for the larger meetings to be effective there
had to be skilled chairing of the meetings. We would strongly recommend that
meetings be chaired by team leaders where possible and that they be given some
training in effective meeting management.
In contrast, the three meetings with membership of 15 or more were noticeably less
effective in terms of decision making. It seemed that the very small team meetings
with 5 or 6 members were also less effective. Despite often being very interactive in
terms of the discussion they seemed to have more trouble making group decisions
and on one occasion ended in conflict between two of the groups being represented.
This was the only occasion in all the recorded meetings where such a conflict arose.
Conclusions
The prototypical CMHT meeting contains between 9 and 13 members, it combines
clinical discussion with team business and is used to make team decisions.
Communication in community mental health care teams was much more effective
than in the primary health care teams. On average team members spent three times
as much time at meetings as members of PCHTs. Also, there was strong cross-
disciplinary interaction over the range of meetings that they held. Interestingly, the

freedom of cross-disciplinary interaction was associated with reductions in team
stress levels (as derived from the interview data). Furthermore, the meetings we
recorded showed evidence of high quality chairing and were generally well
organised. Unlike many of the PHCT meetings group decisions were made in 90% of
the meetings and many teams came up with effective ways of ensuring
multidisciplinary representation without introducing too much disparity in the status of
the members.
General Conclusions
In Chapters 11 and 12 we have looked at communication in both primary andcommunity mental health care teams. The analysis was based both on the interviewdata from a large sample of teams in the two health sectors and the detailed analysisof recorded team meetings from a sub-sample of teams. The findings highlight majordifferences in the quality of communication and group decision making betweenPHCTs and CMHTs. In PHCTs there are few occasions where the whole team getstogether in a recognized forum to discuss their activities as a team. When they do soin team meetings the communication and decision making is not particularly effective.In less than half the meetings we recorded not group decisions were taken. Teammembers who are attached to a practice regular do not attend the team meetings.Yet, there was evidence that teams were they do attend have stronger support forinnovation. To the extent that the team meetings are effective, they enable pairs ofmembers to sort out bilateral problems, such as coordination of patient visits.
In contrast, meetings play an important role in the day-to-day operation of CMHTs.On the basis of the interview data it seems that members spend about 3 times asmuch of their time at meetings as do members of PHCTs. Most of the meetings thatthey attend are multidisciplinary and there is generally good connectivity across thedifferent disciplines in teams at these meetings. Overall, the recorded meetings werewell managed and spent most of their time discussing topics on their agendas. Inabout 90% of meetings appropriate group decisions were made and there wasevidence in some meetings of skilled management of this process by the chair.
In relation to the primary health care teams we would recommend that someattention is given to training in the management of multidisciplinary meetings. We feelthat PHCTs should recognize the importance of group decision-making processes insupporting an effective team. For CMHTs the communication and meeting practicesare in general more professionally organized and on occasion match the higheststandards observed in industrial team meetings in which the members have hadtraining in communication and decision making. However, we would also like tounderline how important it is for these meetings to be chaired effectively. This wasone of the most striking observations from the CMHT meetings.

Chapter 13
Conclusions and Recommendations
We began this research programme by asking whether team working in healthcare
was associated with better quality patient care. We also asked what factors were
associated with effective teamwork in healthcare organisations. Using a model that
related team inputs and team processes to healthcare outcomes we were able to
conduct research which has directly addressed these questions. The results paint a
clear picture and provide firm answers to the questions we addressed.
§ Inputs such as team composition and organisational factors have a strong
influence upon innovation and effectiveness in healthcare teams.
§ Team processes are directly related to the innovation and effectiveness of health
care teams across sectors.
§ The quality of teamwork is directly and positively related to quality of patient care
and innovation in healthcare.
• There is a significant and negative relationship
between the percentage of staff working in teams
in acute hospitals and the mortality rate in those
hospitals, taking account of local health care
needs and hospital size1. Where more
employees work in teams the death rate among
patients is significantly lower (calculated on the
basis of the Sunday Times Mortality Index Dr.
Foster; deaths within 30 days of emergency

surgery and deaths after admission for hip
fracture)9.
§ Effective teamwork in primary healthcare teams is associated with lower stress
among team members.
§ In those teams characterised by clear leadership, high levels of integration, good
communication and effective team processes, team members have good mental
health and low stress levels. In secondary health care settings the retention rates
of staff are higher in those teams characterised by good team processes.
§ In this setting also, the research demonstrated that team membership itself
confers role clarity and social support on team members, helping them to achieve
better mental health or lower stress than their counterparts not working in clearly
defined teams.
§ Good team processes means clear, shared objectives amongst team members;
high levels of participation including frequency of interaction, quality of
information sharing and shared influence over decision making; emphasis on
high quality patient care within teams and a preparedness to encourage
constructive controversy but to discourage interpersonal conflict; and practical
support for ideas for new and improved ways for providing healthcare.
§ Effective and innovative teams are characterised by a pattern of reflexivity. Team
members collectively and individually take time out to review the objectives,
strategies and processes of the team; they prepare plans for making changes
accordingly; and they implement those plans in action.
§ Such reflexivity leads to both better quality healthcare and higher levels of
innovation.
9 This finding is based on separately funded research recently completed by the research
team at the Aston Centre for Health Services Organisation Research (further details availablefrom West or Borrill).

§ Leadership also emerges as critical in healthcare teams but is often absent. A
single clear leader in highly complex large teams is associated with higher levels
of effectiveness and innovations
§ As teams develop and become more sophisticated in their ability to work
effectively, distributed leadership or shared leadership amongst different
functions is associated with higher levels of effectiveness, innovation and better
quality teamwork
§ Clear shared leadership is associated also with better team processes - clear
objectives, participation, emphasis on quality, support for innovation and
reflexivity.
§ But conflict over leadership is disastrous for teams. Where conflict over
leadership exists, teams are ineffective, not innovative and team processes tend
to be very poor.
The implications of our research are clear. First it is important that teamwork is
encouraged in healthcare organisations and second that leaders are trained and
encouraged to work effectively in teams. Leadership should be group-centred rather
than traditional.
The traditional approach to leadership of healthcare teams is that the leader
is responsible for the group and has control over final decisions. He or she
guards their position power and perceives the group as individuals to be
managed by the leader. The leader shapes the task for the team and
ignores the socio-emotional processes within the teams. He or she
discourages expression of needs or feelings during team meetings.
Our research suggests that healthcare teams needs group centred leaders
who see responsibility as shared by both the leader and the team; where
control over final decisions is vested in the team; where leader position
power is de-emphasised; where the leader perceives the team as a
collective entity and shares responsibility for shaping the tasks of the team.
Moreover, the team leader should emphasise and share with the group the
responsibility for maintaining the group as a social entity. He or she should

closely observe socio-emotional processes in the group and encourages
discussion in meetings of team members' needs and feelings.
§ The research reveals that multi-professional working is associated with high
levels of innovation in healthcare. Where a variety of professional groups are
involved in healthcare teams it is much more likely that innovation will be a
consequence. This is particularly so when the team processes are healthy.
§ Larger teams are seen as more innovative and effective, partly because they
have the resources, organisational structures and processes in place which
enable radical changes in the delivery of healthcare to be accomplished.
Policy makers should be cautious about how they respond to these findings.
Teams cease to exist above around twelve to 14 members. They become
small organisations. Primary health care "teams" consisting of around 40
members are in effect medium sized enterprises. As these teams transform
at around 15 to 20 members into organisations it is likely that they will divide
into sub-teams. This is a normal structural process in organisations.
Leaders and managers then have to make decisions about the appropriate
sub-teams to be formed. These should be formed taking account of the
team's context and tasks. The purpose of these sub-teams should be to
manage uncertainties in relation to particular patient groups, particular
stakeholder groups and particular illness categories.
A wise differentiation within healthcare teams is necessary as they develop
into organisations. This differentiation or specialisation of activities is
necessary for the team to cope effectively with its environment. But at the
same time it creates new pressures upon the organisation. The sub-groups
must learn to integrate effectively with one another to communicate, liase
and co-operate. The danger is that sub-teams, particularly if they are
composed of like professional groups, end up competing rather than
collaborating and co-operating for the greater good of patients. Therefore,
managers and leaders must ensure that these groups and sub-teams liase
and collaborate together. It is harder to work as a single team as the
organisation grows in size and the required differentiation and integration
processes necessary require sophisticated leadership. Leaders of health

care teams must therefore be trained in appropriate leadership knowledge,
skills and attitudes.
These observations are reinforced by our finding that higher levels of integration in
healthcare teams are associated with innovation and effectiveness. Communication,
quality of meetings and information sharing activities to increase integration are all
associated with innovation and effectiveness in healthcare teams. However, our
research also reveals that quality of communication and meetings varies
considerably. In general meetings are very poorly managed in primary health care
and professionals in this domain have much to learn from their colleagues in
community mental health teams. Indeed, another important conclusion which can be
drawn from the research is the importance of training for those working in primary
health care to better plan and manage their meetings.
Recommendations
There are a number of key elements to effective teamwork (Guzzo and Shea, 1992).
1. Conditions for effective teamwork
• First, Individuals should feel that they are important to the success of the team.
When individuals feel that their work is not essential in a team, they are less likely
to work effectively with others or to make strong efforts towards achieving team
effectiveness. Roles should be developed in ways which make them
indispensable and essential.
• Individuals' roles in the team should be meaningful and intrinsically rewarding.
Individuals tend to be more committed and creative if the tasks they are
performing are engaging and challenging.
• Teams should also have intrinsically interesting tasks to perform. Just as people
work hard if the tasks they are asked to perform are intrinsically engaging and
challenging, when teams have important and interesting tasks to perform, they
are committed, motivated and co-operative (Hackman, 1990).

• Individual contributions should be identifiable and subject to evaluation. People
have to feel not only that their work is indispensable, but also that their
performance is visible to other team members.
• Above all there should be clear, shared team goals with built-in performance
feedback. Research evidence shows that where teams are set clear targets at
which to aim and they receive feedback on their performance, their performance
is generally improved.
2. Selecting team members
Regardless of their task specialism, there are certain attributes that all team
members need to demonstrate if the team is to achieve its goal. Selection should
focus not just on professional skills but also on knowledge skills and attitudes (KSAs)
for teamworking. (See Figure 13).
Figure 13: Knowledge, Skills and Abilities for Teamworking
A Conflict resolution KSAse.g.
Fostering useful conflict, whileeliminating dysfunctional conflict.Using integrative (win−win) strategiesrather than distributive (win−lose)strategies.
B Collaborative problem solving KSAse.g.
Having the right level of participationfor any given problem.Avoiding obstacles to team problemsolving (e.g. domination by some teammembers).
C Communication KSAs e.g. Employing communication patternsthat maximise an open flow.Using an open and supportive style ofcommunication.Using active listening techniques.Paying attention to non-verbalmessages.
D Goal-setting and performance Management KSAs
. e.g. Setting specific, challenging andattainable team goals.Monitoring, evaluating and providingfeedback on performance.
E Planning and task co-ordination KSAse.g.
Co-ordinating and synchronising tasks,activities and information.Establishing fair and balanced rolesand workloads among team members.
Source: Stevens & Campion, 1999 (Reprinted with permission).

3. Team composition
Today’s health care teams are being formed to respond to increased complexity and
demands in the environment; and they bring together people from diverse
professional backgrounds. Such diverse teams therefore embody different attitudes
and working practices as a result of differences in age, gender, educational
background, nationality, organisational culture, etc.
There is growing evidence, supported by the results from our research, that teams
that are diverse in terms of skill and educational specialisation produce high levels of
innovation and clear strategic thinking.
To date however it seems that other forms of diversity produce less positive effects
on team performance. Teams whose members have diverse cultural backgrounds
initially tend to perform more poorly than culturally homogenous teams, although this
effect diminishes over time. Turnover rates are higher in teams which are diverse in
terms of demographic features such as age, educational level, status and non-
industry work experience.
Diverse teams are not only advantageous if team performance is to be maximised: in
current health care settings, it is simply not practical to select teams that are highly
homogeneous. The challenge is to achieve the positive effects of diversity whilst
building stable teams that will grow and develop together. It is essential therefore to
provide induction and training for individual team members which will minimise the
impact of differences that can be disruptive.
Susan Jackson (1996) has drawn a distinction between team-member differences
that are task related (for example, educational level, work specialisation,
organisational function) and those that are relations-oriented (e.g. gender, age,
nationality, political views). It would seem that difficulties in teams are more often, in
the short term at least, related to relations oriented-differences. In these areas,
individuals will tend to make shallow or stereotyped decisions about others. Both
awareness training and opportunities for social or informal contact between team
members therefore play an important part in breaking down stereotypical reactions
and developing more appropriate judgements.

4. Team Leadership
• Leadership is creating alignment around shared objectives and strategies to
attain them.
• Leadership is increasing enthusiasm and excitement about the work and
maintaining a sense of optimism and confidence.
• Leadership is helping people appreciate each other and helping them to learn
how to confront and resolve differences constructively.
• Leadership is helping people to co-ordinate activities, continuously improve,
develop their capabilities, encourage flexibility, encourage an objective analysis
of processes, and foster collective learning about better ways to work together.
• Leadership is representing the interests of the group or organisation, protecting
its reputation, helping to establish trust with external stakeholders and helping to
resolve conflicts between internal and external partners.
• Leadership is creating a unique group or organisational identity.
Organisations that introduce team based working stress the importance of selecting
the right people to lead teams at the very beginning. Leaders who find it difficult to
move from a directive/controlling supervisory role to one of participative leadership
can cause lasting problems. Those organisations which have successfully overcome
this difficulty actively encourage all members of staff to apply for team leader
positions. This begins the process of breaking down stereotypical thinking about who
can lead teams, the criteria for application, etc. In addition, these organisations
provided considerable training and support for new team leaders in the initial months
of their appointment.
In the early stages of a team’s development, training should be made available for
team leaders to enable them to design and implement appropriate team processes
and to develop the skills needed for effective team leading.
Team leaders need to be skilled in responding appropriately to meet the needs of
their teams, i.e. to be more or less directive in supporting a team. Their aim should

always be to move as quickly as possible away from being directive and towards
allowing the team to be autonomous. When supported by a team leader who
provides an autonomous environment, a team can achieve more highly by becoming
self-directing in its development and its work.
5. Organisational Support for Teams
Hackman and his colleagues at Harvard University have concluded that there are six
principal areas within which teams need organisational support: targets, resources,
information, education, feedback and technical/ process assistance in functioning.
Examining the extent to which organisations provide team support in these areas can
help in discovering the underlying causes of team difficulties.
Targets
Teams need support from an organisation in determining targets or objectives.
Surprisingly few health care teams are given clear targets by their organisations often
because organisational targets and aims have not been clarified sufficiently. It is
striking, when team members are asked to outline their objectives and team targets,
how few have clear notions of what is required of them. There is an implication that
teams should derive their targets and objectives by scrutinising the organisational
objectives or mission statements. However, these are often such vague good
intentions or positive but abstract sentiments that it is almost impossible for a team to
derive clear targets and objectives. Where, through a process of negotiation, teams
are able to determine their targets in consultation and collaboration with those
hierarchically above them, there is usually a better level of performance.
Resources
The organisation is required to provide adequate resources to enable the team to
achieve its targets or objectives.
Resources include: having the right number and skill mix of people; adequate
financial resources to enable effective functioning; secretarial or administrative
support; adequate accommodation; adequate technical assistance and support (such
as computers, blood pressure testing equipment, or appropriate equipment for testing
infants' hearing, etc).

Information
Teams need information from the organisation which will enable them to achieve
their targets and objectives. Changes in strategy or policy which are not
communicated to teams can hamper their effective functioning. Ensuring that
relevant information reaches a team to enable it to perform effectively is an essential
component of an organisation's management. For example, GPs need to provide
health visitors with ready access to age/ sex registers, medical records and other
information about the practice population, in order for the health visitors to function
effectively within the teams.
Education
Part of an organisation's responsibilities for effective team functioning is to provide
the appropriate levels and content of education for staff within teams. The purpose of
such training and education is to enable team members to contribute most effectively
to team functioning and to develop as individuals. This includes on-the- job training,
coaching via supervisor, training courses, residential training courses or distance
learning courses. There should be adequate access to training which is relevant to
the team's work and of a sufficient quality and quantity to enable them to perform to
maximum effectiveness. And, as indicated above, team members should be trained
in the knowledge, skills and abilities, for team working.
Feedback
Teams require timely and appropriate organisational feedback on their performance if
they are to function effectively. Timely feedback means that it occurs as soon as
possible after the team has performed its task, or occurs sufficiently regularly to
enable the team to correct inappropriate practices or procedures. Appropriate
feedback means that it is accurate and gives a clear picture of team performance.
For some teams it is difficult to gain accurate feedback. For example, primary health
care teams have almost no feedback at all. For a team responsible for providing
training in one division of, say, a major oil company, organisational feedback might
take the form of senior managers' satisfaction with improved performance. This could
include measuring the results from technical training courses in customer service in
retail outlets (i.e. filling stations). Such information could come from surveys of

customer satisfaction with retail operators' services. Clearly there are large
differences in the extent to which organisations can and do provide feedback to
teams, but the aim should be for the organisation to improve continuously in the
extent to which it provides useful, accurate and timely feedback to teams.
Technical and process assistance
Organisations have to provide the specialised knowledge and support which will
enable teams to perform their work effectively. A primary health care team engaged
in developing its practice objectives, by identifying the health needs of the practice
population, might need the health authority to deploy a community medical officer to
advise the team on patterns in local health and ill-health. For a training team in an oil
company, technical assistance might take the form of specialist computing experts
and marketing strategists, advising the company on how to communicate most
effectively to managers throughout Europe, in order to market their training courses
to managers in different functions.
Process assistance refers to the organisational help available when team process
problems are encountered. Are consultants and facilitators available to help the team
identify, diagnose and overcome problems of team functioning from time to time?
But the implication of this work is that NHS organisations should not simply create
teams. They should recreate themselves as team-based. We now turn to address
this important issue.
6. Developing team-based organisations
Teams working within team-based organisations have more discretion and scope
than those working within traditionally managed organisations. In practice, team-
based organisations reflect a management philosophy that incorporates certain
fundamental principles.
In team-based organisations, most employees are clear about and committed to the
objectives of the organisation as a whole. Senior management take time to
communicate information to all employees about organisational objectives and also
encourage team members and teams to influence the development of organisational
objectives.

In team-based organisations employees are more fully involved. They are
encouraged to contribute ideas, opinions and information to decision-making
processes, and their teams have influence over decisions that are made. The
organisation as a whole promotes acceptance of and commitment to processes of
debate about how to perform work most effectively.
Managers within team-based organisations are committed to encouraging
constructive debate within the organisation. They listen carefully to the views of team
members and take time to explore diverse views and differences of opinion. They
also encourage the expression of minority points of view and value opportunities for
careful discussion about the best ways of delivering products and services.
In team-based organisations there must necessarily be a climate supportive of
creativity and innovation. Teams are hothouses for creative ideas, and the
organisation must encourage the expression and implementation of ideas for new
and improved health care processes and ways of working. If it fails to do this, both
the impetus for and the value of team-based working are lost.
To ensure the achievement of these aims, team-based organisations must reflect the
belief that organisational goals will largely be achieved not by individuals working
separately but by groups of people who share responsibility for outcomes and who
work in efficient and effective teams.
In traditional organisations, there tend to be individual command structures with
various status levels representing particular points in the hierarchy. There are
supervisors, managers, senior managers, assistant chief executives and so on. In
team-based organisations, the structures are collective. Teams orbit around the top
management team or other senior teams, both influencing and being influenced
rather than being directed or directive. The gravitational force of different teams
affects the performance of the teams around them. This is a flexible, fluid structure in
contrast to the mechanical, hierarchical structure of traditional organisations.
In traditional organisations, the manager monitors the performance of employees. In
team-based organisations, the team monitors the performance of members within the
team and the team as a whole is appraised by those it provides services and
products for. Thus the Human Resource Management team may be appraised by all
of the teams within the organisation for which it provides services.

In traditional organisations, power is invested in the hierarchy. The further up the
hierarchy you go, the more power you find located there. In team-based
organisations, the emphasis is on integration between teams and on reducing the
number of levels in the organisation so that there is less vertical difference between
different teams and groups. Whereas in traditional organisations the emphasis is on
maintaining power and control through the use of a clear hierarchy of command
(which may be important for example in an organisation dealing with crises), in team-
based organisations the emphasis is on achieving shared purpose across teams and
achieving shared understanding and integration across teams.
In traditional organisations the emphasis is on stability and keeping things the same.
Rules and regulations, formalisation and bureaucracy encourage uniformity and
control. In team-based organisations the emphasis is on encouraging innovation,
change and flexibility in order that the organisation can adapt appropriately to its
changing environment and be innovative health care services.
Traditional organisations tend to adopt ‘one best way’ and to seek for universal
models of effective organisational functioning. The team-based organisation
emphasises its uniqueness, adopts ways of working that are appropriate to the
organisation in its current circumstances, environment and economic context, and
adapts as the environment changes.
In traditional organisations, managers manage and control; whereas in team-based
organisations, the teams are self managing and take responsibility for setting their
(perhaps in consultation with senior managers) and monitoring the effectiveness of
their strategies and processes. Changes in the process of achieving the team-based
organisation are therefore deep, wide and pervasive.
In the face of the inevitable complexities within organisational environments, within
teams themselves and between the people who constitute those teams, there are no
simple prescriptions for implementing effective team based working. In order to be
effective, team members must therefore learn to reflect upon, and intelligently adapt
to, their constantly changing circumstances as the team develops.
There are however certain areas where problems can be predicted and where
effective initial design greatly improves the chances of success. Many of the

common problems in the introduction of team-based working (TBW) result from
impatience: effective TBW takes time to implement and requires multiple changes
that create almost inevitable difficulties. Long-term benefits can only be achieved
through persistent and consistent action in each of these three key areas:
• organisational context
• team structure
• team processes
Organisational context
The top management team’s level of commitment towards TBW is a key factor in an
organisation's introduction of TBW. But the attitude towards TBW amongst
employees generally is another powerful issue under this heading. Reward systems
that focus on competition between individual employees for bonuses undermine the
introduction of TBW. Similarly, information systems that are characterised by secrecy
rather than openness will impede the implementation of TBW. The training and
education priorities of the organisation must also be geared towards developing the
knowledge, skills and abilities required for TBW, including leadership skills and
teamworking skills. The organisation will also need access to coaching expertise to
support teams both during their development and when they experience difficulties in
the course of their work (such as conflicts between team members), either provided
by someone within the organisation or an outside consultant.
Team structure
Teams structure refers to the composition of the teams, i.e. who will be the team
members. This is not simply a matter of the skills required to perform the task, but
also raises questions of variety in functional background and balance in demographic
characteristics such as background culture, gender, age and even personality.
A key aspect of team structure is the nature of the task that the team is required to
do. The goals should be clear, the task should be motivating and team members
should have clear feedback on how effective their performance has been. It also
refers to effective team leadership, as we have emphasised above, and the need to
appoint team leaders who know how to lead teams and are not hierarchical,
traditional supervisors.

Team processes
When TBW is introduced, most organisations focus initially on team processes and
send prospective team members on team-building workshops. Though the motive
behind this is valid, i.e. to build cohesion, the first step in building effective teams is to
ensure that team members:
• make sufficient effort (that they are motivated to perform the task).
• have adequate knowledge and skill within the team both to perform the task and
to work in a team.
• have developed appropriate ways of performing their task, i.e. task performance
strategies.
As organisations implement TBW, there are major pitfalls in each of these three key
areas that must be avoided, any of which could considerably delay or impede the
process.
• the creation of teams throughout the organisation, regardless of the need or the
nature of the tasks.
• setting up teams but continuing only to appraise, reward and manage individuals.
• creating teams but neglecting to train people to function effectively within and
across teams.
• introducing TBW while leaving teams without expert assistance when problems
such as major conflicts arise.
• creating well functioning teams but ignoring the vital need to ensure these teams
communicate with each other, integrate their work and otherwise liaise
effectively.
• failing to negotiate with the teams clear and challenging team-level objectives.
• giving the teams challenging objectives but not the training, skills and resources
to meet those objectives.

Conclusion
The following quotation illustrates just how fundamental team working is to our
species and we include this to remind the reader of the importance of groups and
teams to human societies throughout their development. There is little new about
teamwork.
"He makes tools (and does so within more than one technical tradition),
builds shelters, takes over natural refuges by exploiting fire, and sallies out
of them to hunt and gather his food. He does this in groups with a
discipline that can sustain complicated operations; he therefore has some
ability to exchange ideas by speech. The basic biological units of his
hunting groups probably prefigure the nuclear family of man, being founded
on the institutions of the home base and a sexual differentiation of activity.
There may even be some complexity of social organization in so far as fire-
bearers and gatherers or old creatures whose memories made them the
data banks of their 'societies' could be supported by the labour of others.
There has to be some social organization to permit the sharing of co-
operatively obtained food, too. There has to be some social organization to
permit the sharing of co-operatively obtained food, too. There is nothing to
be usefully added to an account such as this by pretending to say where
exactly can be found a prehistoricial point or dividing line at which such
things had come to be, but subsequent human history is unimaginable
without them."
[Extract from J.M. Roberts (1995), The History of the World, page 18].
The activity of a group of people working co-operatively to achieve shared goals via
differentiation of roles and using elaborate systems of communication is basic to our
species. The current enthusiasm for team working in and in health care reflects a
deeper, perhaps unconscious, recognition that this way of working offers the promise
of greater progress than can be achieved through individual endeavour or through
mechanistic approaches to work. That is what this report has demonstrated in
relation to health care teams to and quality and innovation in patient care.

Appendix I
Measures Used
Primary Health Care Team Questionnaire
Section 1 Team working. This contained seven measures of team working. Five of
these form the Team Climate Inventory (Anderson and West, 19xx): participation, a
15 item scale covering information sharing (α = ); innovation, an eight item scale
covering support from new ideas (α = ); team objectives, covering clarity and
relevance of objectives (α = ); task style, covering the monitoring and appraising of
work in the team (α =). Three other measurers were included: reflexivity, covering
the reviewing process in the team (α = ) and XXX was measured using XX (xx
19xx) (α = ); and team innovation measured using (West?) (α = ). Respondents
were also asked to list the major changes introduced by the team in the previous 12
months.
Section 2 included measures of team effectiveness adapted from Poulton and West
(199x). This includes three dimensions: team working (α = ); , patient orientation (α
= ); and organisational efficiency (α = ).
Section 3 included a measure of psychological stress, the GHQ-12 (Goldberg, 1991)
(α = .88 ).
Section 4 included questions eliciting biographical and team information (e.g. age,
gender, ethnic origin, job title, employer, team composition, team leader).
Initial construction of the effectiveness measure
Effectiveness criteria were generated using an iterative process within the
constituency model approach (Connally et al., 1980). After consultation with the local
Health Authority and Community Mental Health Trust, the Department of Health, and
local community mental health teams, representatives of the range of stakeholders in
the provision of mental health care were invited to a one-day workshop. A total of 13

interest groups were approached: users, carers, advocacy agencies, mental health
charities, consultant psychiatrists, community mental health nurses, occupational
therapists, psychologists, social workers, managers, policy makers, researchers in
mental health, and general practitioners. All groups were represented by the 50
people attending the workshop.
The aim of the workshop was to provide the basis for an agreed set of definitions of
effectiveness in CMHTs. Stakeholders sharing a perspective were grouped together,
so that consensus could be achieved more easily within each working group.
Participants were asked to generate a set of criteria which they agreed would
measure CMHT effectiveness, with the proviso that any criterion must be supported
by concrete examples of how good practice could be audited. Groups then
reconsidered their criteria in order to prioritise aspects of practice.
Output from the workshop was analysed and categorised by the research team.
Duplication and ambiguity were removed. The 76 remaining criteria, grouped into the
three broad categories of user and carer issues, team development and viability, and
organisational issues, were re-circulated to all workshop participants. They were
invited to comment on wording and clarity, to suggest modifications, indicate
significant omissions, and approve priority ratings. Items rated as less important by a
majority of respondents were removed, and any items rated down in the final
consultation were respositioned. Remaining ambiguities and duplication were
removed, together with items already covered in other sections of the proposed
survey questionnaire.
The reduced set of CMHT effectiveness criteria, together with supporting measures
of good practice, were piloted amongst local community mental health nurses, a
CMHT, psychologists and other mental health professionals. Practitioners agreed
that they captured the complexity of the work and the diversity of environments in
which CMHTs operate. The final set of 27 criteria was incorporated into the main
survey questionnaire, along with the Team Climate Inventory (Anderson & West,
1994) and the 12-item General Health Questionnaire (Goldberg, 1970.)
Each statement was clarified by additional concrete examples of elements of practice
which individuals could use to aid their rating. A 5-point Likert-type scale was used
to rate how effective the team was on each criterion. Thus, to illustrate, the content
of the first criterion was

Accessibility of the service to users and carers has been identified as a measure of CMHT effectiveness.
[For example: identification and contactability of a key worker; clear referral procedures; time taken to respond to users and or carers; a clear point of access.]
Not at all To a great extent Overall, to what extent does your CMHT make services accissible to users and carers? 1 2 3 4 5

Appendix I I
Knowing the Way:
Effectiveness in Primary Health Care
A description of national workshops aimed at defining
effectiveness criteria for primary health care

Introduction
The World Health Organisation define primary health as:
“..essential care based on practical, scientifically sound and acceptable methods and tehcnology made
universally accessible to individuals and families in the community through their full participation and
at a cost that the community and the country can afford to maintain at every stage of their development
in the spirit of self reliance and self determination. It forms an integral part of the countries health
care system, of which it is a central function and main focus, and of overall social and economic
development of the country. It is the first level of contact of individuals, the family and community with
the national health system, bringing health care as close as possible to where people live and work”.
World Health Organization, 1978.
In order to enable primary health care professionals and the populations they serve to develop the
health and stress of those populations, it is important that clear objectives for primary health care are
established. Moreover, what constitutes effectiveness in primary health care also has to be determined
by each primary health care team or organization. Indicators of effectiveness, once established,
provide professionals with clear guidelines over how best to allocate resources in order to achieve
effective primary health care. This consultative document represents the endeavours of 63
professionals working in the area of primary care who spent four days in workshops designed to help
achieve this overall aim. 10
The vision of this exercise is to promote health care for the population nationally, by providing primary
health care professionals and others concerned with the health and stress of the population with clear
indicators of effectiveness. These can be used as a basis for discussion and development in primary
health care teams across the country, taking into account their local circumstances, philosophies of
primary care and the needs and views of their local populations.
Effectiveness in Primary Health Care
In an important analysis of the evaluation of health services’ effectiveness, St Leger, Schneiden &
Walsworth-Bell (1992) observe that “Surprisingly, routine data [sources relating to primary care] are
relatively sparse, especially when one considers that the majority of contacts that the general public
have with the health service are with general practice.” (p.41). Indeed, it is striking how little research
has focused on developing theoretically grounded or practically useful indices of effectiveness of
primary health care services. In a rare exception, Pearson & Spencer (1995) employed a two-stage
Delphi questionnaire to determine agreed indicators of effective teamwork in primary care. Using
responses from 137 people involved in primary care teamwork - primarily from FHSAs - they rated the
importance of twenty indicators. Four emerged as particularly significant:
10 Within primary health care, terminology is a source of concern and conflict. For example, someprefer the term ‘primary care’. There are sensitivities around the terms ‘general practice’ and ‘primaryhealth care’ being used interchangeably; and a distinction between medical and nursing care is alsosensitive. Those who attend for treatment or advice are called ‘patients’ by some and ‘clients’ byothers. We have preferred the terms ‘primary health care’ and ‘clients’ in this document.

• Agreed aims, goals and objectives
• Effective communication
• Patients receiving the best possible care
• Individual roles defined and understood
What is effectiveness?
How can the effectiveness of primary health care teams therefore be judged? At the simplest level,
effectiveness might be viewed as the influence the primary health care team has in improving health
and ameliorating ill health within the practice population. Such a criterion of effectiveness begs a
number of questions, however. Examples include:
• Is the population in an area of social deprivation?
• Does the team have unusually good resources, in terms of number of staff or technical equipment?
• Will the effects be long-term?
In the literature on organizational effectiveness, a distinction is made between efficiency (doing things
right) and effectiveness (doing the right things) (Sundstrom, DeMeuse & Futrell, 1990). Efficiency
may be defined as the output for a given input and how a team compares with other similar teams in
this regard. Effectiveness can also be seen as the team’s capacity to perform, adapt, maintain itself and
grow (where growth may refer to size, innovation or skill development) (Goodman, 1986).
Clearly, teams can be seen as more or less effective depending upon the criteria adopted.
Consequently, the assessment of team effectiveness has come to be seen as much a political as an
empirical process. Below we consider (briefly three examples of approaches to managing this problem.
The constituency approach
Recognition that effectiveness is a political concept has led to the use of the ‘constituency approach’
(Connally et al, 1980; Bedeian, 1986) which seeks to incorporate all significant views in the judgement
of team effectiveness. Each of the major constituents is identified (e.g. clients, carers, staff health
authorities, professional organizations) and the effectiveness criteria they would use are adopted as
indicators. Effectiveness is then measured using multiple indicators rather than an aggregate, since, in
many cases, effectiveness in one area will necessarily imply ineffectiveness in another (consumer
satisfaction may not always coincide with quality of care if consumers require prescriptions for drugs,
the use of which is not in their best interest).

From this conceptual, background Poulton & West (1994) developed a set of 23 effectiveness criteria
for primary health care teams using a focus group methodology involving multiple stakeholders in
primary care. In a study involving more than 500 practice nurses (Poulton, 1995) the criteria were then
factor analysed revealing four underlying factors: good teamwork, task excellence, organizational
effectiveness and patient-centred care. More recent analyses with larger samples suggest only three:
quality of health care, organizational efficiency, and teamworking.
Poulton and West (1997) employed these outcome measures in a six month longitudinal study of the
impact of teamworking on effectiveness. The research demonstrated that clarity of and commitment to
objectives was the most important and statistically significant predictor of effectiveness in all four
areas.
Multidisciplinary auditAnother important approach to measuring effectiveness is multidisciplinary audit. A major centre for
research and advice is the Eli Lilley National Clinical Audit Centre (Hearnshaw, Baker & Robinson,
1994; Baker, et al 1995). In a study conducted by this Centre of three practices, those supported in the
development of multidisciplinary audit showed a significant improvement in specific areas of
functioning. The procedure involves teams identifying particular problems (in a diagnostic area or an
area of team functioning) and a priority is identified. The team then sets standards in the specific area,
observes current practice and achievements, and compares these with the standards. Discrepancies
prompt changes in practice and the results are then regularly reviewed. Such an approach clearly
enables teams to assess and improve performance in specific areas, although the approach is somewhat
atomistic and relies on the effective identification of priorities. An excellent overview of this approach
is provided by Crombie, Davies, Abraham & Florey (1993).
ProMES
In the broader organizational literatures on team effectiveness, a widely adopted approach is the
Productivity Measurement and Enhancement System (ProMES) based on research by Naylor, Pritchard
& Ilgen (1980). Effectiveness criteria are established in group discussions with team members and
supervisors. The variables are then “psychologically scaled” to a common effectiveness scale. Based
on group consensus about expected levels of effectiveness, which are given a zero value, maximum
effectiveness levels (set at +100), and minimum levels (-100) are set. Each variable is also weighted in
terms of its perceived contribution to the overall effectiveness of the team or organization. The system
is then used to set objectives, develop indicators monitor and improve performance and give feedback
to the team (Pritchard, 1990). This is promising for primary health care, because of the sophistication
of the approach, its theoretical robustness and practical utility in complex contexts. It was therefore
used as a basis for developing effectiveness measures by the Health care Team Effectiveness project.
Overall, however, it is clear that conceptual and empirical development in evaluating the effectiveness
of primary health care is urgently required, if cost, clinical and community value are to be convincingly

demonstrated. In order to take this forward a series of four workshops on primary health care team
effectiveness was sponsored by the Institute of Work Psychology. The methods are described below.
Prior to detailing these we consider the need for a manageable set of objectives or effectiveness
indicators; and the need for a theoretical framework within which to locate any set of dimension.
(i) The need for relative simplicity
It is apparent from any analysis of research in the domain of effectiveness that the development of
indicators and effectiveness dimensions for primary health care is a complex task (West, 1996). A
major problem is that many measures of effectiveness and many indicators can be developed. Trying
to use this large number of measures within an organization as an effective means of targeting
resources simply becomes overwhelming for the practitioners concerned. The sheer multiplicity of
potential indicators is cognitively too complex for people within the organization to cope with the task
effectively. Indeed, some research suggests we can only cope with 7 plus or minus 2 categories,
whereas other organizational researchers specifies to more than 8 to 12 key dimensions. Consequently,
we sought a parsimonious theoretical model which would provide guidance for researchers and
practitioners.
(ii) The Competing Values Model
The most useful model appears to be the Competing Values Model. This model incorporates two
fundamental dimensions;
• flexibility of the organization versus control within the organization;
• external orientation versus internal orientation (see figure 2).

M e e t i n g t a r g e t s
E m p h a s i s o n p e r f o r m a n c e
‘C u s t o m e r ’ s a t i s f a c t i o n
C o m p e t i n g V a l u e s M o d e l
H u m a n R e l a t i o n s M o d e l O p e n S y s t e m s M o d e l
I n t e r n a l P r o c e s s M o d e l R a t i o n a l G o a l M o d e l
T r a i n i n g
T e a m d e v e l o p m e n t
L e a r n i n g o r g a n i s a t i o n
T e a m m e m b e r m e n t a l
h e a l t h
C o m m i tm e n t &
s a t i s f a c t i o n
S c a n n i n g o f t h e
e n v i r o n m e n t
R e s o u r c e a c q u i s i t i o n & c o -
o r d i n a t i o n
I n n o v a t i o n
C o l l a b o r a t i o n w i t h o t h e r
o r g a n i s a t i o n s
E f f i c i e n t c o n t r o l o f
r e s o u r c e s
C l i n i c a l a u d i t
R e v i e w i n g & e v a l u a t i n g
e f f e c t i v e n e s s
B u d g e t m a n a g e m e n t
C o n t r o l
I n t e r n a l
O r i e n t a t i o n
E x t e r n a l
O r i e n t a t i o n
F l e x i b i l i t y
F i g u r e A . 1
Combining these dimensions identifies 4 domains of effectiveness:
human relations,
open systems,
rational goal,
internal process
• Human relations model
The primary emphasis is on norms and values associated with belonging, trust, respect, skill
development, growth and stress. Motivational factors are attachment, cohesiveness and
organization membership. Areas of effectiveness include:
• development of skills
• team development
• learning organization skills
• team member mental health
• commitment and satisfaction

• Open systems model
The primary emphasis is on change and innovation and appropriate scanning of the environment.
Norms and values are associated with knowledge of the environment, resource acquisition,
innovation and adaptation. Motivating factors are:
• development of services
• resource acquisition and co-ordination
• innovation
• collaboration with other organizations
• Rational goal model
The primary emphasis in this model is on the pursuit and attainment of well-defined objectives. Norms
and values are associated with good performance, goal-fulfilment and achievement. Motivators
are: successful achievement in pre-determined areas. Effectiveness dimensions include:
• meeting ‘production’ targets
• ensuring high quality
• high client or customer satisfaction
• Internal process model
The emphasis here is on stability, internal organization and adherence to rules and protocols,
where norms and values are associated with efficiency, co-ordination and uniformity. Motivating
factors are needs for order, rules, regulations and efficiency. Effectiveness dimensions include:
• efficient control of resources
• reviewing and evaluating effectiveness
• good budget management
The model of competing values stresses how the allocation of resources to any one area, for example
the open systems model, is likely to lead to a restriction of resources in the opposite domain (internal
process). Similarly a focus on external control (rational goals) may well lead to a neglect of the area of
human relations (internal flexibility). Effectiveness in organizations, is likely to be maximised when
emphasis is placed equally in each of the four domains of effectiveness. Using this framework as a
guide we embarked on a series of 4 workshops to clarify our thinking about effectiveness in primary
care.
The Workshops
MethodThe methodology used to develop effectiveness measures for primary health care was developed taking
account of the following: the importance of including the complexity and diversity in primary health

care and of taking into consideration the wide range of views and perspectives held by the professional
groups who contribute to meeting patient needs; the need to develop a method which would most cost-
effectively use the time of primary health care professionals; and the importance of developing
measures which were generalisable across primary health care.
The measures were therefore developed in two stages:
i) Indentifying objectives for primary health care and developing indicators for these objectives, was
carried out in four workshops with domain relevant experts from primary health care, based on an
approach developed by Connolly et al, 1990. Such an approach enabled the views of a range of
professionals to be taken into account. Working intensively with an expert group enabled considerable
knowledge and insight to be gained in a short space of time. In addition, these professionals, who had
a background in primary care but were mainly working in an advisory, policy or research role,
provided a broader, more generalisable perspective on effectiveness in primary health care.
ii) The measures developed were used by primary health care teams teams and feedback provided on
effectiveness.
Workshops
Objectives
There were three principle overall objectives for the workshops:
♦ to identify the important issues relating to developing effectiveness measures for primary health
care,
♦ to develop a set of effectiveness measures acceptable to all perspectives in primary health care,
♦ for participation in the workshops to be a valuable experience for the participants.
Participants
An initial stakeholder analysis identified 13 stakeholders in primary health care. Advise was sought
from contacts in primary health care about key experts who could represent the views of each
stakeholder group, and about whether the initial list of stakeholder was sufficiently comprehensive.
The experts suggested by the contacts were sent information about the research programme, invited to
attend the four workshops, and asked to suggest additional or alternative key experts who could also
make a contribution. In addition, representatives from primary health care teams were invited, that is,
professionals who were currently engaged in clinical practice. The majority of those contacted were
keen to attend the workshops, and were able to commit themselves to attending two or three. X were
able to attend all four. Each workshop was planned so that the participants covered the main
stakeholder views.
Workshop process

A focus group methodology was used.
The delegates were divided into three working groups. These were designed so that (a) a range of
stakeholder views were represented, and (b) one or two or group members had attended most or all of
the workshops and so could share with new members the learning and experience from previous
workshops. Each group worked with a facilitator, trained in ProMES, and a notetaker who recorded
the group discussion and the decisions made.
Workshop 1
Objective: to develop objectives for primary health care.
After an initial introduction to the Health Care Team Effectiveness project and a presentation on
ProMES, the delegates were presented with a set of objectives for primary health care developed by the
researchers. Each group worked on (a) refining the objectives, (b) critically evaluating the objectives
in relation to the criteria for objectives (see appendix xx).
The outputs from each group were presented at the end of the workshop in a plenary session. After the
workshop the outputs were discussed with members of four primary health care teams (who endorsed
their relevance and value), combined into a single list and then circulated to delegates.
Workshops 2 and 3
Objective: to develop indicators for the objectives for primary health care.
Both workshops started with a presentation on team working in primary health care and issues relating
to the development of effectiveness measures.
Delegates were presented with the final version of the objectives for primary health care. Each group
worked on (a) developing indicators for an objective, (b) critically evaluating the indicators in relation
to the criteria for indicators (see appendix xx).
In Workshop 2 the working groups selected the objective to discuss. The objectives - Quality of Care
and Client Satisfaction were selected. In Workshop 3 groups were assigned an objective so that each
was discussed at least once. The objectives - Effective Management of Resources, Development and
Satisfaction of Primary Health Care Team Members and Quality of Care, were discussed. In the third
workshop the output from each working group was given to another group in the afternoon session for
discussion and refinement.
The output from each group were presented at a plenary session at the end of both workshops.
After Workshop 2 and 3 the outputs were amended and the circulated to delegates. In addition, after
the third workshop the outputs from all three workshops was written-up in the document ‘Knowing the
Way: Effectiveness in Primary Health Care’ and circulated to delegates.
Workshop 4
In the fourth Workshop, those attending critically analysed the objectives and indicators developed, and
considered how they could be applied in practice by PHC teams and others. A review of the data

derived from 100 teams, examining their definitions of effectiveness was also presented. The focus
groups commented on the next steps in taking forward the work completed to date.
1. Objectives were identified in the first of the four workshops and after an additional three
workshops with somewhat differing attendees who worked with them, they remained unchanged.
(The point is they have been tested and found acceptable by lots of different people.)
2. In addition, they were shown to a number of primary health care teams. These teams found the
objectives useful and accurate.
3. The themes in these objectives are similar in principle to the themes of objectives that other types
of professional organizations and in other settings have developed. Thus, there is some consensual
validation.
Bearing in mind the problems of deluging primary health care teams/organizations with long and
unmanageable lists of objectives and indicators of effectiveness, we endeavoured to produce a core list
of key objectives
Below we describe each and suggest possible indicators.
Effectiveness measures are a guide not stone tabletsThe key objectives identified and the indicators developed for each are a synthasis of the outputs from
the four workshops. Some of the contributions made by the working groups have been modified by the
researchers, and the Competing Values Model used to provide a conceptual structure. The majority of
objectives and indicators described below, however, were suggested and critically reviewed by the
Primary Health Care professionals who attended the workshops. The objectives and indicators are not
definitive, nor are they comprehensive and applicable to every primary health care team. They are
meant to be used as an aid for teams which wish to measure and enhance their effectiveness. In
relation to each objective, the focus groups developed a set of indicators by which progress towards
objectives could be measured. Again, these indicators are meant as examples. If they fit and make
sense to individual primary health care teams, fine; but they may well not fit. Primary health care
teams have different missions and the measurement must be tailored to that mission. Moreover, the
focus groups produced many more possible objectives and measures of them are described below.
These can be used as a resource for teams wishing to explore areas beyond those we have designated as
likely to be core.
Objectives and Indicators for Primary Health
The core key objectives developed in the workshops are showh in Figure A2, mapped
in to the competing value model.

* Im p r o v i n g h e a l t h
* H i g h q u a l i t y o f h e a l t h c a r e
C l i e n t s a t i s f a c t i o n
C o m p e tin g V a l u e s M o d e li n P r im a r y H e a lth
C a r eH u m a n R e la t io n s M o d e l O p e n S y s t e m s M o d e l
I n t e r n a l P r o c e s s M o d e l R a t io n a l G o a l M o d e l
G o o d T e a m w o r k i n g
C o n t i n u i n g
p r o f e s s i o n a l
d e v e l o p m e n t
H ig h t e a m m e m b e r
c o m m itm e n t &
s a t i s f a c t i o n
A c c u r a t e i d e n t i f i c a t i o n o f
h e a lth n e e d s
R e s p o n s i v e n e s s t o c l i e n t s
a n d c o m m u n i t y
E f f e c t i v e c o l l a b o r a t i o n w i t h
o t h e r o r g a n i s a t i o n s
E f f i c i e n t u s e o f
r e s o u r c e s
H e a lth c a r e r e v i e w i n g &
im p r o v i n g e f f e c t i v e n e s s
C o n t ro l
I n t e r n a l
O r i e n t a t i o n
E x t e r n a l
O r i e n t a t i o n
F le x ib i l i ty
F ig u r e A . 1
* In d i c a t o r s m a y d e p e n d o n t h e h e a lth c a r e p h i l o s o p h y o f t h e p r i m a r y h e a l t hc a r e t e a m s e .g . h o l i s t i c , p r e v e n t i v e , b i o m e d i c a l
The indicators developed in the workshops for each of the objectives are listed below.
♦ Improving health
♦ High quality of health care
♦ Improving client satisfaction
♦ Efficient use of resources
♦ Reviewing and improving health care effectiveness
♦ Good teamworking
♦ Continuing professional development
♦ High team member commitment, stress and satisfaction
♦ Accurate identification of health needs
♦ Responsiveness to clients and community
♦ Effective collaboration with other relevant organizations

Rational Goal
Objectives Example Indicators
Improving health ⇒ Improvement in the health of the practice poulation including
reductions in e.g. coronary heart disease, smoking, mental health
problems.
⇒ Percentage of clients improving at the expected rate after treatment.
⇒ Effectiveness of preventive practice in reducing specific treatment
requirements.
High quality of health care ⇒ Effective knowledge of and management of chronic diseases (e.g.
diabetes, epilepsy, asthma) measured by conformance with evidence-
based good practice.
⇒ Effective health education and preventive health care programmes.
⇒ The PHCT holds regular meeting to review a sample of cases. This
review would include the appropriateness of who saw the client,
procedures, and outcomes. Percentage of cases managed entirely
appropriately, based on all staff’s views.
Improving client satisfaction ⇒ Measures of client complaints and adequacy of procedures for
complaints.
⇒ Questionnaire or telephone surveys using standardised measures*.
⇒ Measures of waiting times, satisfaction with consultations,
appropriateness of appointments.
* See Appendix III for examples

Internal Process
Objectives Example Indicators
Efficient use of resources ⇒ Percent client contact time as a percentage of total time (there is an
optimal level between extremes). Assesment of DNA’s.
⇒ Number and effectiveness of initiatives developed to help team
members use time better.
⇒ Review and evaluate budget allocation and improvements in resource
utilisation.
Reviewing and improving health
care effectiveness
⇒ Review and use of evidence-based treatment protocols (all staff).
⇒ Planned clinical audit (all staff).
⇒ Intra-team referral practices regularly reviewed and adapted (all staff).

Human Relations
Objectives Example Indicators
Good teamworking ⇒ Clear, shared objectives (partly related to health needs analysis) set
annually by the team.
⇒ Regular (at least monthly) meetings to review team objectives,
strategies, processes and procedures to coordinate sub-groups and
whole team.
⇒ Positive team/organizational climate assessed annually.
Continuing professional
development
⇒ Clear and specific written annual training and development plans
agreed for each staff member (percentage of staff covered; percentage
of development plan items completed.)
⇒ Research and development budget and plans agreed by team annually.
⇒ Access for all team members to training/development resources.
High team member commitment,
stress and satisfaction
⇒ Annual review of staff commitment, stress and satisfaction using
standardized measures*.
⇒ Mechanisms to deal with and review staff dissatisfaction, conflicts and
complaints.
⇒ Low absenteeism and staff turnover.
*See Appendix III for examples
Open Systems
Objectives Example Indicators
Accurate identification of
population health needs
⇒ Collection of practice level data (demographics, disease patters, socio-
economic patterns, activity levels); and local, regional and national
data.
⇒ Involvement of clients, community groups and other relevant

organizations in health needs analysis.
⇒ Data used to inform daily planning, and longer term strategy and
direction; setting annual objectives; identifying gaps in provision and
skill mix.
Responsiveness to clients and
community
⇒ Involvement of clients and community in team/organization decisions
concerning team objectives, strategies and processes.
⇒ Frequency, quality and usefulness of contacts between team members
and representatives of community stakeholder groups.
⇒ Extent of planning within team/organization to seek feedback from
clients and community stakeholders/opinion leaders/groups.
Effective collaboration with other
relevant organizations
⇒ Appropriate admissions to hospital (and referral rate)
⇒ Number of effective and appropriate contacts with agencies (e.g.
palliative care, social services, education).
⇒ High ratings of team/organizations on salient dimensions*.
*See Appendix III for example
Application of the effectiveness measures
General Principles
There are three levels of application of these effectiveness measures, ranging from simple through to
comprehensive.
• Simple. The simplest way of using the effectiveness measures is to use them as a basis for group
discussions in the primary health care team; for members of the team to consider the areas of
effectiveness described and how they can make use of the measures in facilitating of the
effectiveness of the primary health care team. They may also consider what other measures they
may wish to add, given their local circumstances and which of the measures are not applicable. In
other words, the simple approach is to use the effectiveness measures as a basis for ongoing
discussions about monitoring and improving the effectiveness of the primary health care team.
• Moderate. The primary health care team can use the effectiveness dimensions and indicators to
develop measures of effectiveness within their primary health care organization in relation to each
effectiveness measure (as appropriate). The team can develop measures and make action plans in
terms of how they can improve their performance in this area. Again they may wish to consider
which of the measures are applicable in their organization and which are not, and what measures
which are relevant to them are missing from document.
• Comprehensive. This application involves the use of full productivity measurement and
enhancement system, which has the following steps: (a) a design team, which includes
representatives from all groups of staff in the primary health care team, is formed; (b) in a series of
meetings the design team works with a facilitator identifying objectives and indicators for these,
where necessary consulting with other members of the team; (c) the design team develops

contingencies for each indicator, that is, determines the relative contribution that improvements on
a indicator will make to overall effectiveness; (d) the team uses the indicators and receives
feedback on performance.
Quality of Health Care
Quality of Health Care
• The PHCT would have a monthly (or more frequent) staff meeting where a sample of cases was
reviewed. This review would include the appropriateness of who saw the client, what procedures
were done, and whether that client was handled appropriately in all aspect. The measure would be
the percentage of cases which were considered as being handled appropriately. This would also be
the basis for discussion of what improvements need to be made for those specific clients and for
clients in general.
• Some PHCTs will feel a health needs analysis is valuable but do not know how to do one or how
to use it. For such a PHCT, the task of developing such an analysis could be broken down into
definable steps. E.g. get information on how to do such an analysis, decide on a plan for doing the
analysis for that particular PHCT, gather the information, put the information together into a form
that the PHCT can use to make decisions. Each of these steps would be given a time for
completion. The indicator would be the percentage of the analysis completed compared to the
anticipated time for completion.
Survey on client perceptions of health improvement after treatment. For example, each client is
given a questionnaire or a sample of clients are called by phone and asked about improvements.
Measure is the percentage of clients improving. For the various specific targets given by agencies
outside the PHCT such as immunisation rates, develop a scoring system whereby each level of
meeting the objective gets a certain number of points. E.g. if the target immunisation rate was
80%, actually doing 80% would give 100 points, 60% immunised would be 20 points, 70% 80
points, 90% 130 points, etc. The number of points would be based in the importance of that
target. The index would be the percentage of actual points earned compared to the maximum
possible points received if all targets were met. (Note, this assumes there are lots of such targets.
If this is not true, a composite measure such as this is probably not necessary.
• The percentage of required reports completed on time.
• The number of required reports returned by agencies requesting corrections or additional
information. (This would be an index of the quality of the reports.)
Client Satisfaction
Establish a formal procedure where clients can make complaints including a process for following up
on these complaints. Measure is the number of such complaints which were not concluded to the
client’s satisfaction within one week.

Effective Management of Resources
• Number of new initiatives developed that are designed to help team members use their time better.
These initiatives should also be reviewed on a regular basis to ensure they are still effective.
• Percent client related time as a percentage of total time. This measure gets at how much time is
devoted to clients. It does not measure how well that time is being spent. Other indicators are
needed to address this issue. (RDP: Note that this indicator is one where there is probably an
optimal level between the extremes. To little time with clients may suggest too much
administration time. Too much time with clients may suggest too little administration time.)
• Percentage of staff turnover over time. High staff turnover leads to inefficient resource utilisation
because it takes time to teach procedures to new staff and work is lost as a departing staff member
leaves. This measure would also be an indicator for the satisfaction of team members.
• Percentage of appointments which are unfilled or where the client did not come.
Development and Satisfaction of Primary Health Group/Team Members
• Training and development. A list of training and development experiences for each person on the
team would be developed each year. For example, attendance at a certain type of conference,
training on a piece of office equipment, learning a new procedure, etc. This list would be the
development plan for that person for that year. There would be two measures for training and
development. The first would be the percentage of team members who had the written plan. The
second measure would be the percentage of the development plan items actually completed.
• Who are reviewed, given feedback, and have a formal, jointly developed action plan for making
improvements.
• Satisfaction. Measure overall satisfaction on a monthly or bi-weekly basis with a very brief
questionnaire that would take no more than 2 minutes to compete. Measure would be the
percentage of staff indicating Satisfied or Very Satisfied with their jobs.
• Staff turnover is also a satisfaction measure. Note this measure under Effective Management of
Resources.
Figure A.2 List of participants
NAME JOB TITLE PLACE OF EMPLOYMENT
John Horder President CAIPE
Debbie Mellor Section Head of Workforce
Non-Medical Planning
NHS Executive
Thelma Sackman Nursing Officer NHS Executive
Kate Andrews Clinical Research Fellow Dept. General Practice
Rosemary Field To Be Advised To Be Advised
Nicki Meade Research Associate The National Primary Care
Research & Development

Centre
Steven Campbell Research Associate The National Primary Care
Research & Development
Centre
Brenda Leese * Research Fellow The National Primary Care
Research & Development
Centre
Bonnie Sibbald Research Associate The National Primary Care
Research & Development
Centre
Ann Richards Research Fellow Psychological Therapies
Research Centre
Malcolm McCoubrie Senior Lecturer in Community
Based Medical Education
Standards - Medical Director
Wandsworth Community
Health
Sheelagh Richards * Occupational Therapy Officer London
Jane Cannon* Practice Nurse Larwood Surgery
Sue Jenkins-Clarke Research Fellow University of York
Peter Bundred Senior Lecturer in Primary
Care
University of Liverpool
Judy Mead * Physiotherapist Chartered Society of
Physiotherapists
Richard Brown * To Be Advised To Be Advised
Alan Chapman Management Education &
Development Manager
Primary Care
East Norfolk Health Authority
Lance Gardner Professional Officer The Queens Nursing Institute
Terry Brugha * Senior Lecturer & Honnary
Consultant Psychiatrist
University of Leicester
Rosamund Bryar Professor of Community
Healthcare Nursing Practice
University of Hull
Stephen Rogers Senior Lecturer in Primary
Care
University College London
Joan Lole Director of Nursing & Primary
Care
Mancunian Community Health
Paul Thomas Senior Lecturer Dept. Of
General Practice
Imperial College School of
Medicine @ St.Mary’s
Ruth Hudson Education Officer Community Practitioners &
Health Visitors Association

Jacky Hayden Dean of Postgraduate Medicine University of Manchester
Christiana Johnson Health Promotion Officer Princess Royal Community Health
Centre
Beverley Haynes Senior Health Promotion Specialist Princess Royal Community Health
Centre
Peggy Newton Lecturer in Psychology Dept. Of General Practice
Jeanette Naish Senior Lecturer in Primary Care Dept. General Practice & Primary
Care
Stuart Mee * Practice Manager The Crookes Practice
Kay Robinson Primary Healthcare Facilitator South Humber Health Authority
Brian McAvoy Professor of Primary Health Care Dept. Of Primary Care
Susan Lonsdale Senior Principal Research Officer Dept. Of Health
Sandra Dodgson Senior Development Manager N H S Development Unit
Frances Fogg Primary Healthcare Facilitator North Notts Health Authority
Wendy Whyte Regional Community Nursing
Team Leader
British Forces Overseas
Mike Sharpe Regional General Manager of
Medical Services
British Forces Overseas
Ron Pollock Assistant Director Support &
Development/Finance
Wakefield Health Authority
Mike Vaughan Total Purchasing Project Manager Wakefield Health Authority
Sasha Wishard Research Facilitator Tayside Centre for General Practice
Marion Duffy Education Facilitator Tayside Centre for General Practice
Chris Simmonds * Practice Manager Medical Centre Doncaster
Jane Solomon * Locality Management Nottingham Health Authority
Catherine Booth * General Practitioner G.P. Unit
Ann Netton Assistant Director of PSSRU University of Kent
Gwen Wilson * Development Manager Community
Nursing
Sheffield Community Health

Appendix III
Effectiveness Measures
Developed for Primary Health Care Teams
Core Objectives for Primary Health Care teams
Promote, maintainand improve health
§ Provide high quality health care§ Accurate identification of individual and population health
care needs§ Review and improve the effectiveness of health care
provision§ Manage illness, injury and disease taking account of
agreed standards and evidence based practiceEnable personaland communityresponsibility forindividual health
§ Enable patients/clients to make informed decisions abouttheir own health.
§ Proactively encourage positive health behaviour§ Implementation of health education and preventative
care programmesEfficient use ofresources
§ Human resources – skills, knowledge, expertise, time§ Physical resources – budgets, equipment, premises
Continuouspersonal andprofessionaldevelopment
§ Individual annual training plans which take account of theplans of the PHCT
§ Equal access to training/development resources
High team membercommitment, stressand satisfaction
§ Team working
§ Mechanisms for reviewing and acting upon staffdissatisfactions, conflicts and complaints
Responsiveness toclients andcommunity
§ Gather information and feedback from clients/communitystakeholders/opinion leaders
Collaboration andpartnership withother relevantorganisations
Objective: Promote, maintain and improve health
Techniques for reviewing whether services meet client needs
A. What are the main aims of this service?
B. What does the team (in collaboration or in addition to other agencies)currently do to meet a particular health/health promotion need?
List all the provisions currently available in the team (and from other

agencies, if relevant).
C. How do you know whether these provisions meet these health/healthpromotion needs?
List evidence that can be used to determine this.
D. Which aspects of this evidence suggest that you are meeting thishealth/health promotion need?
E. Which aspects of this evidence suggest that you are not meeting thishealth/health promotion need?
F. What provision would the team ideally like to have in place to meetthis health/health promotion need?
Next steps:
Use the evidence discussed in C, D and E to develop measures to enable the teamto evaluate more systematically whether they are meeting clients needs.

Objective: Promote, maintain and improve health
Measure 1 - Review of quality in case management
Measure =Percentage of cases judged to be managed appropriately on the mostrelevant quality dimensions.
Steps to clarifying the measure:
∗ Determine the types of cases to be reviewed (specific condition, e.g.
diabetes/asthma, or a specific age group or type of patient population).
∗ Decide which of the quality dimensions are most relevant to the cases being
reviewed.
∗ Decide what is an acceptable quality level on each dimension.
∗ decide what is an acceptable % of cases to be judged as having been managed
appropriately.
Using the measure:
∗ Rate each of the selected cases on the quality dimensions and give a total score.
Note the dimensions where quality is above and below the acceptable level.
∗ Calculate % of cases which fall above and below the acceptable level of cases
being managed appropriately.
∗ The review will result in two types of information
⇒ dimension of quality for individual cases which fall below the acceptable
standard.
⇒ % of cases overall which are managed appropriately.
N.B. For this measure need to develop an instrument for rating cases on each
dimension which suggests evidence that can be used to make judgements,
emphasise the importance of standardising ratings across cases and gives guidance
in how to complete the instrument.

Dimensions of Quality
Effectiveness: Is the treatment given the best available in a technical sense,
according to those best equipped to judge?
What is their evidence? What is the overall
result of the treatment?
Acceptability: How humanely and considerately is this treatment/service
delivered? What does the patient think of it? What
would/does an observant third party think of it (“How would I
feel if it were my nearest and dearest?”) What is the setting
like? Are privacy and confidentiality safeguarded?
Efficiency: Is the output maximised for a given input or (conversely) is the
input minimised for a given level of output? How does
the unit cost compare with the unit cost elsewhere for
the same treatment/service?
Access: Can people get this treatment/service when they need it? Are
there any identifiable barriers to service - for example,
distance, inability to pay, waiting lists, and waiting times -
or straightforward breakdowns in supply?
Equity: Is this patient or group of patients being fairly treated relative to
others? Are there any identifiable failings in equity - for
example, are some people being dealt with less
favourably or less appropriately in their own eyes than
others?
Relevance: Is the overall pattern and balance of services the best that
could be achieved, taking account of the needs and wants of
the population as a whole?

Dimensions of Quality
Effectiveness
To what extent......
To a verylittle
extent
To someextent
To a verygreatextent
Is the treatment/service beinggiven technically the bestpossible?
� � � � �
Does the treatment/servicebeing given conform to agreedprotocols/standards?
� � � � �
Is the current outcome fromthe treatment/service as wouldhave been expected, given thepatient’s condition at the start?
� � � � �
Acceptability
To what extent......
To a verylittle
extent
To someextent
To a verygreatextent
Is the patient’s privacysafeguarded?
� � � � �
Is the patient’s confidentialitysafeguarded?
� � � � �
Is the patient treated withconsideration and respect?
� � � � �
Efficiency
To what extent......
To a verylittle
extent
To someextent
To a verygreatextent
Are the inputs to thetreatment/service (e.g. stafftime, medication) minimisedfor a given level of output?
� � � � �
Is the unit cost the same as forthis treatment/servicedelivered elsewhere?
� � � � �

Access
To what extent......
To a verylittle
extent
To someextent
To a verygreatextent
Can patients access thetreatment/service when theyneed it?
� � � � �
Do any of the following pose abarrier to accessing thetreatment/service?:
� � � � �
Location� � � � �
Distance� � � � �
Time of availability� � � � �
Inability to pay� � � � �
Waiting lists� � � � �
Waiting times� � � � �
Lack of appointment times
� � � � �
Lack of resources to supply
treatment/service
� � � � �
Equity
To what extent......
To a verylittle
extent
To someextent
To a verygreatextent
Is this group of patients beingfairly treated relative to others?
� � � � �
Are the resources available forthis treatment/servicecomparable to those availablefor others?
� � � � �

Relevance
To what extent......
To a verylittle
extent
To someextent
To a verygreatextent
Are the resources used for thistreatment/service appropriatein the context of the needs andwants of the practicepopulation as a whole?
� � � � �

Objective: Promote, maintain and improve health.
Measure 2 - Young People’s health - Sexual Health
Measure = Percentage unwanted teenage pregnancies in a 6 month period Percentage of teenagers prescribed the morning after pill in a 6 month
period Percentage of teenagers requesting pregnancy tests in a 6 month period
Steps to clarifying the measure:
∗ Over a 3 month period monitor the number of unwanted teenage pregnanciesand terminations, number of morning after pills prescribed, number of teenagersrequesting pregnancy tests. This will establish a base line.
∗ Compare the numbers (or % of total number of teenager girls on the practice list)with the teenage pregnancies, use of morning after pill, teenagers requestingpregnancy tests in other PHCTs, and/or with regional figures. This enables theteam to assess the extent to which they are meeting the sexual health needs ofyoung people.
∗ Decide what is an acceptable level of unwanted teenage pregnancies, morningafter pill, requests for pregnancy tests.
Using the measure:
∗ Over a 6 month period log each: unwanted teenage pregnancy; request formorning after pill; and request for a pregnancy test.
∗ Note whether it is a small number of teenage girls who make the requests, orspread across a wide range of girls.
∗ Note whether there are any patterns (i.e. times of the week/month).
∗ After 6 months (or sooner if there are sufficient incidents of pregnancies/requestfor morning after pill/requests for pregnancy tests to form a judgement), collatethe information collected.
Next steps:
∗ Compare the % for teenage pregnancies, requests for morning after pills andrequests for pregnancy tests with (a) what were considered to be acceptablelevels, and (b) with figures for other practices.
∗ On the basis of this determine whether the current provision to meet the sexualhealth needs of young women is (a) being met (how do the figures for the PHCTcompare with the acceptable level? Are they better, worse, the same?), and (b)how the extent to which these needs are being met compares with otherPHCTs/regional averages.

∗ If the measures suggest that the sexual health needs of teenagers are not beingmet, introduce interventions to address this. The information about whether it isthe same small number of young women requesting morning after pills/pregnancytests will help to determine the type of interventions required.
∗ Once interventions have been introduced, re-use the measure to determinewhether the provision of services has improved.
Interventions:
∗ What type of follow-up is there when a teenager requests the morning after pill/apregnancy test?
∗ Gather more information about why young people take risks.∗ Implications for HIV/AIDS.

Objective: Promote, maintain and improve health.
Measure 3 - Young People’s Health - Alcohol and Drug Misuse
Measure = Number of teenagers attending A & E after drug overdose in a 3month period.Number of teenagers attending A & E after excessive alcohol
consumptionin a 3 month period.
Steps to clarifying the measure:
∗ Over a month monitor the number of A & E slips which record that a teenager hasattended A & E for drug or alcohol abuse.
∗ Compare these numbers with national/regional figures, and the number of otherPHCTs. This will help establish the extent the team is meeting these healthpromotion needs of young people compared to other PHCTs.
∗ Decide what is an acceptable number of A & E attendances for drug and alcoholabuse among teenagers.
Using the measure:
∗ Over a 3 month period log each A & E attendance by a teenager for (a) drugabuse, (b) alcohol abuse.
∗ Note whether it is a small number of teenagers who attend A & E for drug andalcohol abuse, or if it is spread across a wide range of teenagers.
∗ Note whether there are any patterns (times of the week/month).
∗ After 3 months collate the information requested. Determine (a) number ofincidents of drug and alcohol abuse at A & E, (b) number of teenagers whoattend A & E once, number who attend regularly.
Next steps:
∗ Compare the number of A & E attendances for drug and alcohol abuse with (a)what the team judged to be an acceptable number and (b) with figures from otherpractices and regional/national figures.
∗ On the basis of this determine whether the current health promotion to raiseawareness about the changes of drug and alcohol abuse are (a) being met (howdo the recorded numbers compare with the agreed acceptable level? Are theybetter, worse, the same?) and (b) how the extent to which the health promotionneed is being met compares with other PHCTs/regional figures.
∗ If the measures suggest that health promotion is not being effective, introduceinterventions to assess this. The information about whether is it the same ordifferent young people who misuse alcohol and drugs to determine the type ofinformation required.

Measure 4 - Patient access to consulations with a GP
Measure = The number of days that patients wait to see a GP of their choice
The PHC design team believed that an important part of providingquality care was to ensure continuity of patient care. The aim wasto ensure that patients had access to the GP of their choice (the GPwho ha most often provided health care in the past) by reducing thelength of time they had to wait to see this GP.
Steps to clarifying the measure
• Monitor the length of time patients have to wait to see each GP over a 1 monthperiod.
• If there are variations in the waiting time from week to week note the factorswhich might account for this (eg GP absences, increase in patient demand,services provided by other team members).
• Decide what is the target waiting time for each GP. Set this target taking accountof the factors which increase and reduce the waiting time. This target might bethe number of days a patient has to wait to see a GP of their choice, or it mightbe more realistic to set a target which specifies the maximum and minimumrange, to allow for fluctuation which are outside the team’s control.
Using the measure
• Over a 3 month period monitor the length of time patients have to wait to seeeach GP in the team.
• If there are variations across weeks, months, or between GPs, note the factorswhich might account for these.
Next steps
• Depending on the target set, calculate the average length of time that patientshave to wait to see a GP or calculate the maximum and minimum lengths of timethey have to wait. Compare this with the target set.
• If the target has been met, use the information gathered which explainedfluctuations in the length of time patients had to wait to assess whether it mightbe possible to reduce waiting times further (ie, if increases in patient demandsincreased waiting times, is it possible to anticipate and plan for these increases?).
• If the target was not met, use the information gathered which explainsfluctuations to assess what changes need to be made so that the target can bemet. Also consider whether the target is realistic.

Measure 5 – Patient access to a quality consulation with GPsMeasure 1= Percentage of patients whose appointment with a GP is minutes
duration in a 3 month period.
Much of the discussion in the PHT design team concerned how to most effectivelyuse the staff resources within the team to meet patient needs. The aim was toachieve this by having mechanisms in place which ensured that patients saw thehealth professional in the team most appropriate for their needs and as aconsequence, reduce the number of patients who needed/wanted to see a GP. Thiswould enable GPs to have longer (10 minute) appointments with those patientswhose health needs require a GP consultation.
GPs being able to have a longer appointments with patients was judged by the teamto be a measure of quality of care because it is seen as an indication that patientsneeds are being met by the appropriate health professional in the team.
It can also a measure effective use of resources.
In addition, ithe measure is an indication that the mechanisms put in place to ensurethat patients see the most appropriate health professional are effective (on thecondition that the longer GP appointments do not increase the workloads of the otherhealth professionals in the team).
Steps to clarifying the measure
• Over a month monitor the number of patients who have 10 minute appointmentwith a GP (this is a booked appointment, not a shorter appointment which overruns).
• Calculate the average number or % of patients in a week who can be offered a10 minute appointment.
• Decide what is the target number or % of patients who can be offered a 10minute appointments. When setting the target it may also be useful to considerthe types of patients on the practice list who might benefit from longerappointment so as to establish the level of possible demand. It will also be usefulto consider other factors which might affect the demand. For example, will therebe seasonal variations?
Using the measure
• Over a 3 month period monitor the number or % of patients each week who areable to have a 10 minute appointment.
• Note the types of patients seen and, if there are weekly variations, the factorswhich might account for these variations
• Also note whether there are any unforeseen consequences (eg, increased workload for other team members, administrative difficulties).

Next steps
• Compare the average number or % of patients who could be offered a 10 minuteappointment with the target which was set.
• If the target is achieved consider whether (a) any of the unforeseenconsequences need to be taken into account, (b) whether there are ways that thistarget can be improved.
• If the target is not achieved consider whether any changes to the factors whichaccounted for variations might help the team top achieve the target. Alsoconsider any impact of the unforeseen consequences.

Measure 6 – Use of out of hours services by patient
Measure = Percentage reduction in the use of private out of hours services by patients in a 6
month
period.
The PHC design team believed that using out of hours services did not providepatients which the best quality service (eg, they are seen by a health professionalwho does not know their medical history). Thus reducing the number of patientsusing out of hours services would reduce number receiving poor quality treatment. Areduction would also lead to more effective use of resources in the team – thesavings made from the reduction in the use of out of hours services could be used toemploy an additional health profession in the team, eg a nurse practitioner.
Steps to clarifying the measure
• Over a 3 month period monitor the use of the out of hours services by patients.
• Note the types of patients who use the service (is it a few frequent users orwidely spread). Are the reasons for the reasons for using the out of hoursservices different for frequent users and occasional users? If the reasons aredifferent, would it be possible to reduce the out of hour usage of these twogroups? If there are fluctuations in usage? Note factors which account for thesevariations.
• Decide the acceptable level of out of hours service usage and the target amountof reduction. Set this target taking account of the factors which are associatedwith increases and decreases in usage (eg, seasonal variations, public holidaysetc). It may be necessary to have separate targets for frequent users andoccasional users.
Using the measure
• Over a six month period monitor the use of the out of hours service.
• If there are weekly of monthly variations in usage, note the factors which mightaccount for these.
Next steps
• Calculate the average number of times the out of hours service has been usedeach month over the six month period and compare this with the target set.
• If the target has been met, using the other information collected, considerwhether the most appropriate patients have been using out of hours service, andwhether there are ways that (a) the usage could be reduced further, and (b)

whether steps could be taken to ensure that the out of hours service is used bythe most appropriate patients.
• If the target was not met, use the information collected to consider changes whichneed to made to help ensure that the target is met in the future. Also use theinformation collected to consider whether the target is realistic.

Measure 7 – Patients have access to an appropriate health professional
Measure = Percentage of patients who have contact with a healthprofessional from the
team at a time and location most appropriate to them and to the professional in a 6 month period.
This measure emerged from discussions the PHC design team had about how toachieve quality of care by ensuring that patients’ needs were met by the healthprofessional most qualified to meet those needs.
This is a complex measure and more work is required to develop a measure whichcan be used to assess effectiveness.
Agreement needs to be reached on the following:
- which health needs can be most effectively met by which health professional.- how health needs are assessed- which health needs can be most effectively met in which location (eg, home, one-
to-one consultation, booked appointment, drop-in, clinic etc.) This needs to takeaccount of both patients’ and the health care professionals’ views.
- what % of patients it might be possible for each health care professional in theteam to see at a time and location most appropriate to them and the patient.

Measure 8 – Patients have access to a home visit from an appropriate healthprofessional.
Measure = Percentage of patients who have a home visit from the mostappropriate
health professional in a six month period.
This measure emerged from a discussion of the use of staff resources within theteam. The PHC design team were considering which team members carried outhome visits, the time of day when it was most convenient to carry out home visits andhow to determine whether home visits were appropriate (ie, some home visits meetsocial rather than health needs). The aim is to ensure that only patients who need ahome visit receive one, and that they are visited by the health professional (DN, GP,pharmacist, HV etc) who has the expertise to meet their needs.
This is a complex measure. The following needs to be determined before it can bedeveloped in a measure of effectiveness.
- which health (social) needs can only be met by a home visit- how to assess these needs- which of these health needs can be most effectively met by which health
professional in the team- what % of patients can realistically be seen at home by the most appropriate
health care professional.

Objective: Enable personal and community responsibility for individual health
Measure 9 - Patients understand the role and function of the PHCT.
Measure = Number of patient requests, use health professionals’ time and PHCTservices which are inappropriate in a 3 month period.
Steps to clarify the measure:
∗ Patient understanding is demonstrated by appropriate use of the healthprofessionals’ and other staff in the team, PHCT services, and appropriaterequests for information.
∗ Define what are judged to be inappropriate uses of: health professionals’ time,and other staff in the team; PHCT services; inappropriate requests forinformation.
∗ Develop a checklist of the above and circulate to team members.
∗ Decide what is an acceptable level of inappropriate uses of: health professionals’time, and other staff in the team; PHCT services; inappropriate requests forinformation.
Using the measure:
∗ Over a two week period all members of the PHCT record the number ofinappropriate uses of health professionals’ and other team members’ time, andinappropriate use of PHCT services and requests for information.
∗ Note type of inappropriate use/request, and type of patient.
∗ After two weeks collate the data from all team members and calculate thenumber of (a) inappropriate uses of health professionals’ time, (b) number ofinappropriate uses of other staff members’ time, (c) number of inappropriate usesof PHCT services by patients, and (d) number of inappropriate requests forinformation.
Next steps:
∗ If the number of inappropriate uses of staff time, PHCT resources and/orrequests for information are unacceptable, develop interventions to reduce thenumber.
∗ Use information on the type of inappropriate use of time/services, and type ofpatients to target the information.
∗ After the interventions have been put in place repeat the measuring process toassess progress.

Objective: Efficient Use of Resources
Measure 10 - Patients able to manage minor illness
Measure = Percentage of patients seen by health professionals in the team who hada minor illness which could have been managed themselves.
Steps to clarify the measure:
∗ Define what is meant by ‘minor’ illness.
∗ Develop a checklist of minor illnesses and circulate to all health professionals inthe team.
∗ Decide what is an acceptable level of patients to see with a minor illness 10% or40%?
∗ Decide whether some groups of patients should be excluded.
Using the measure:
∗ Over a two week period the health professionals in the team log each patientseen, and record which patients attend for minor illness.
∗ Note the type of minor illness, type of client.
∗ After two weeks collate the data from team members and calculate (a) totalnumber of patients seen, (b) total number attending with minor illness. It may beuseful to look at % of patients with a minor illness seen by each type of healthprofessional, and to note which types of minor illness patients attended with, andthe types of patients presenting with a minor illness.
Next steps:
∗ If the measure indicates that an unacceptable % of patients are seen who haveminor illnesses decide on interventions to reduce the %.
∗ The data collected on types of minor illness, which health professionals areseeing these patients, the types of illnesses and types of patients can all be usedto target the intervention/s.
∗ After interventions have been put in place repeat the measuring processes toassess progress.

Instructions for Record Sheet
The data are being collected over 5 working days, starting on XXX. You can continueto collect data in w/c XXX, if you miss any days in the previous week.
Please record on the form information about every patient you have contact with oneach of the 5 days.
Codes for each column are also printed on the bottom of the form.
Type of illness
Column one
MA = minor illness, acute C = chronic illnessMC = minor illness, chronic A = acute illness
Column two
Please describe all types of minor illnesses you have recorded in addition to those inyour leaflet, using medical terms. If the illness conforms to the definitions of minorillness in your leaflet, no further information is required.
Type of contact
Column three - 1 = phone 2 = home visit 3 = consultation
Type of consultation
Column four - 1 = routine 2 = emergency
Type of Patient
Column five - 1 = female 2 = male
Column six - Patient’s age in years
Seen before in last 7 days
has the patient seen another health care professional in the last 7 days for the sameillness as recorded in column 1?
Column seven - record which health professional has seen the patient.
1 = GP 2 = PN 3 = DN 4 = HV 5 = CPN 6 = other
Other comments
Column eight - Please write down any other important information, and, if relevant,note if the patient has been referred inappropriately by other agencies such assecondary care/A&E/social services/dentist, as well as inappropriate internalreferrals.
Please give ALL completed recording forms to the Practice Manager.

Date: Day of week: Name: Job title:
Type of illness1) Code 2) Description ofillness
3) Type ofcontact
4) Type ofconsultatio
n
Type of patient 5) Gender 6)Age
7) Seenbefore inlast week
8) Comments
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
1) Minor/Acute = MA 3) 1 = phone 5) 1 = female 7) 1 = GP 8) Please include otherinformation, and Minor/Chronic = MC 2 = home visit 2 = male 2 = PNreferrals from social services and

Chronic = C 3 = consultation 3 = DN secondary care, otherteam members. Acute = A 6) Age in years 4 = HV
5 = Other2) Please describe illness if not 4) 1 = routine minor according to the 2 = emergency agreed definitions.

Measure 11 - Patients/clients who do not attend for an appointment
Measure = Average percentage of total patients appointments not kept in a week (calculatedover a 3
month period).
Steps to clarifying the measure:
∗ Monitor the DNAs for a one month period for each professional group (GP, DN, SN) toestablish the current level in a one week period.
∗ Collect information on DNA levels for other comparable practices (i.e. have a similar typeof practice population).
∗ Decide what is an acceptable DNA level for each professional group.
Using the measure:
∗ Monitor the DNAs for a two month period for each professional group.
∗ Monitor, where possible, the following:⇒ which patients DNA (persistent or across a wide range?)⇒ characteristics of DNAs (age/gender/ethnicity)⇒ when patients DNA (i.e. time of day/a particular GP, PN etc,/regular appointments
booked in advance)⇒ whether DNAs make another appointment⇒ whether DNAs use other services (e.g. out of hours, home visit)
∗ Calculate the average % of patients/clients who DNA for each professional group in aone week period (this is the number of DNAs as a % of the total number of appointmentsmade in each week).
∗ Compare the DNA average with the acceptable level for each occupational group andwith other practices.
∗ Compare the % DNAs for each week in the two month period - does it vary from week toweek? If so, can these differences be explained?
∗ Use the additional information collected to assess whether discernible patterns in theDNAs. Does it happen at certain times of the day, and/or do certain types of patientsDNA more than others? This information can be used to make decisions about how toreduce DNAs. The information about whether DNA patients make another appointmentand/or use other services will provide additional evidence about the cost of DNA to theteam.

Next steps:
∗ If the DNA levels for the team as a whole and/or for specific occupational groups areunacceptably high introduce initiatives to reduce the level, and monitor progress usingthe measure.
∗ The additional information collected will help to establish what types of initiatives might help to reduce DNAs.
∗ It may also be necessary to gather information from patients and clients about the
reasons for DNA (is it because they forgot to attend? Because it is difficult to cancel anappointment? Because they are unaware of the implications to the team of DNA?).

Measure 12 – Efficient use of administrative systems
Measure = Percentage of patients not attending appointments with health professionals in the
team
which result from errors in the administrative system.
The additional work carried out at in the PHCT to explore the reasons why patientsDNA revealed some problems with the administration systems. The result was thatpatients cancelled their booked appointment, but this was not entered on the system.In addition some patients reported that as they had attended the surgery close to abooked appointment they assumed that this had been cancelled.
These findings suggest that some reduce in DNA rates would result from developingand improving current systems.
Developing a measure requires the following:
- further work to identify the range of system problems which could be improved by the team- calculate the current number of DNAs which result from system problems- improve and develop the system- continue to monitor the reasons for DNA and assess whether the number resultingfrom system problems decreases / or monitor the DNA rate and if this decreasesattribute this to the improvements and developments in the system.

Measure 13 - Efficient use of GP resources in the teamMeasure = Average number of patients seen by a GPs in a week
The PHCT had introduced a ‘sit and wait’ session; all patients who went to the surgeybetween 10.00 qnd 11.00 were seen by a GP. Introducing the sit and wait sessionenabled the resources of the GPs to be used differently. Two GPs held patientconsultations while a third carried out administrative tasks, dealt with telephonequeries and carried out home visits. The aim was to offer the same number of face-to-face consultations with patients, but with a reduced GP resource.
It was decided, therefore, that maintaining the number face-to-face consultations withpatients was an indication of the success of the sit and wait.
Data from the practice computer showed that there had been a substantialreduction in the number of patients seen by GPs (comparisons were madebetween a 1 week period in 1999 and the same week in 1998).
Discussion of the reasons why GPs might be seeing fewer patients revealed that thisreduction might indicate that the practice was infact using resources more efficiently.
Reasons proposed were:
- Less use of locum doctors for home visits (therefore fewer patients beingadvised to see their own GP after the home visit).
- Nurses seeing more patients (diabetics, blood clinic, hypertensive), nursepractitioner (available on Fridays).
- Patients can call the surgery and talk to a GP and get advice.- The pharmacist visits some patients at home to discuss medication.
This work emphasises the importance of looking at the activities of the team as awhole when assesses the effectiveness of specific aspects.

Objective: Continuous personal and professional development
Measure 14 – Team member access to training
Measure = Percentage of who are satisfied with the extent to which their training needs are
assessed
and met in the previous year.
Steps to clarifying the measure
q Agree what is an acceptable level of satisfaction within the team.
Using the measure
q Each member of the PHCT completes the measure of satisfaction with training.
q Calculate the mean satisfaction with training score for each person (total theresponses from each question ….. and divide by the number of questions). Thencalculate what % of staff report a satisfaction level at, above and below theageed acceptable level.
Next steps
Analysis of the responses to the individual questions in the training satisfactionmeasure can be used to determine the steps which need to be taken to improveaccess to training within the team. For example, these responses can indictatewhether there are concerns about funding available to support training, or if there areissues relating to the identification of training needs. The former could be resolvedby identifying additional sources of funding, while the latter could be tackled via theappraisal system.

Objective: High team member commitment, stress and satisfaction.
Measure 15- Team member commitment and satisfaction
Measure = Percentage of staff in the team who feel committed and satisfied
Steps to clarify the measure:
• Agree what is an acceptable level of commitment within the team • Agree what is an acceptable level of job satisfaction
Using the measure:
• Each member of the PHCT completes the measures of commitment andsatisfaction. It is important that confidentiality is maintained and that it is notpossible for individual responses to be identified
• Calculate the mean job satisfaction for each person (total the responses from
each question, extremely dissatisfied = 1 to extremely satisfied = 7 and divide bythe number of questions, 16). Then calculate what % of staff report a satisfactionlevel at and above the agreed acceptable level for the team
• Calculate the mean commitment for each person (total the responses from each
question, strongly agree = 5, strongly agree = 1, and divide by the number ofquestions, 6). Then calculate what % of staff report a level of commitment at andabove the agreed acceptable level for the team
Next steps
Analysis of the responses to the individual questions in the commitment and jobsatisfaction measure can be used to determine the steps which need to be taken toimprove the overall levels of commitment and satisfaction within the team.

Measure 16 - Team members use each others skills, knowledge and expertiseappropriately
Measure = Percentage of team members who report thatskills, knowledge and expertisewithin the team are used appropriately in 3 monthperiod.
Steps to clarifying the measure
q Agree what is an acceptable level of appropriate use of skills, knowledge andexpertise.
Using the measure:
• Each member of the team completes the questions on the use of each othersskills, knowledge and expertise.
• For each question, calculate the extent to which skills, knowledge and expertise
are used appropriately (total the responses on each dimension = 1,= 5 and then calculate the mean (divide the total by the number of dimensions).
Next steps
If the levels of awareness and appropriate use of skill, knowledge and expertise arebelow the acceptable level the team could improve this by holding more effectivemeetings (when all members are encouraged to contribute to decision-making), bygetting involved in joint projects together, and carrying out work shadowing.

Measure 17 - Effective team working
Measure = Percentage of requests for help and information and referrals from otherteam members which are inappropriate in a 3 month period.
Steps to clarifying the measure:
• Agree what is an acceptable % inappropriate requests for help and information,and level of inappropriate referrals from other team members
Using the measure:
• Over a specified period (one or two weeks) each member of the team logs eachtime another team member requests help and information, and refers a patient.Against each, each team member notes whether this was an appropriate orinappropriate request for help/information or patient referral. It may also beuseful to note which team member made the request for help/information ormade the referral
• At the end of the specified period calculate what percentage of the total number
of requests for information and patient referrals were inappropriate. Comparethis with the acceptable levels agreed.

Objective: Responsiveness to client and community
Measure 18 - Patients’ Experiences of the PHCT service (1)
Measure = Percentage of patients who report that their experiences of the PHCTservices match the standard agreed by the PHCT.
This can be assessed by measuring patients’ experiences of the PHCT.
Steps to developing a measure:
∗ Identify all the aspects of the PHCT’s work and how it is delivered which areknown to be associated with patients satisfaction, e.g. not having to wait, gettingrepeat prescriptions, phone answered quickly, being able to get advice etc.
∗ Develop a checklist for patient asking if they have experienced each of theaspects associated with satisfaction.
∗ Either ask about experiences of the PHCT in general, e.g.⇒ Do you get your repeat prescription within 48 hours? sometimes
always never
∗ Or ask about the contact with PHCT the patient has just had, e.g.⇒ Did you have to wait more than 2 days to get an appointment with the
GP? yes no
∗ Identify other information you would like to collect from patients which might helpyou to use or understand the information you collect on patients’ experiences(e.g. age, gender, number of visits to the surgery in the previous month). It mightbe useful to ask patients to write their own comments.
∗ Consider what would be acceptable and unacceptable responses to the patient’sexperiences questions, e.g. would you expect 90% of patients to report they got arepeat prescription within 48 hours or 10%? Also consider whether some areasare more important than others.
Using the measure:
∗ Over a one week period ask all patients attending the surgery to complete achecklist. Send a % of questionnaires to home addresses, and distribute via DN,HV etc.
∗ Collate the information from patients. Calculate a total score for each patient andthe mean.
It may be useful to look at responses on each item separately (particularly if youconsidered some patient experiences to be more important), and to identify whetherthe views of different types of patients vary.

Next steps:
∗ If patients’ experiences of some aspects of the PHCT work are not as positive asthe team had anticipated develop interventions to improve these. Or you may findexperiences vary across different types of patients and the team want to takesteps to remedy this.
∗ After interventions have been put in place repeat the patient survey to assessprogress.

Measure 19 - Patients’ experiences of the PHCT services (2) (Using the existingmeasure)
Measure = Percentage of patients whose experiences of the PHCT services meetthe standard set by the team.
Steps to clarifying the measure:
∗ On each of the questions in the patient Opinion survey agree the ideal standardthe PHCT wants to achieve for example question 1, the length of time patientswait to get an appointment with a GP, what % of patients does the team aim tosee on the same day/next day/after 2 days/3 days?
∗ On each of the questions in the Patient Opinion survey agree the expectedstandard that the PHCT currently achieves.
Using the measure:
∗ Over a one or two week period distribute questionnaires to patients attending thehealth centre/surgery, attending clinics, and those seen by the HV, DN, CPN andby other professionals carrying out domicillary care. Also survey a sample ofpatients, selected at random from the practice list, who have not been seenduring the week.
∗ On each question calculate⇒ % of patients whose experiences of the PHCT services meet the ideal
standards set by the teams.⇒ % of patients whose experience of the PHCT services meet the expected
standard.
∗ Calculate a total score for % of patients whose experiences meet the idealstandard (total number of questions where patients’ experiences met the idealstandard and calculate this number as a % of the total number of questions).
∗ Calculate a total score for % of patients whose experiences meet the expectedstandard (total the number of questions where patients’ experiences met theexpected standards and calculate this number as a % of the total number ofquestions).

Date -___________________
Patient Opinion Survey
Please could you answer the questions listed below. Your answers will help us toimprove the service we provide for patients.
Age __________ years Male � Female �
1. The last time you wanted an appointment with any of the GPs, how soon didyou get one?
same day �next day �after 2 days �longer ___________
2. The last time you wanted an appointment with the GP of your choice, howsoon did you get one?
same day �next day �after 2 days �after 3 days �longer ___________
3. How could the appointment service be improved?____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
4. The last two times that you phoned the surgery, how long did you wait forthe phone to be answered?
1st time _________ mins Time of day: morning � afternoon �2nd time _________ mins Time of day: morning � afternoon �

5. The last two times that you asked for a repeat prescription, how long did youhave to wait to get it?
1st time ______________ days2nd time ______________ days Not applicable �
6. Have you ever experienced problems/delays with getting a repeatprescriptions?
Yes � No �
7. If yes, please give details of where the delay occurred e.g. at the HealthCentre or at the chemist____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
8. How could the repeat prescription service be improved?____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
9. Have you ever used the services of the Practice Nurse?
Yes � No �
If No, please go to Question 13.
10. Did you have an appointment?
Yes � No �
11. The last two times you had an appointment with the Practice Nurse, howlong after the appointment time did you have to wait to see her?
1st time ____________ mins2nd time ____________ mins

12. If your GP referred you to the Practice Nurse, how long did you sit in thewaiting room until the practice nurse was available?
_____________ mins
Did you know that you could make an appointment to see the Practice Nurse?
Yes � No �
13. Have you required a doctors appointment and had to wait for the PracticeNurse to phone?
Yes � No �
If No, please go to Question 15.
14. The last two times you used this service how long after 2pm did you haveto wait for the Practice Nurse to phone you?
1st time _____________ mins2nd time _____________ mins
15. How could the Practice Nurse services be improved?____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
16. Which of the following services do you think are offered by HealthVisitors? Which have you used?
offered usedAnte natal care � �Post natal advice/support � �Child development assessment � �Behaviour management � �Childcare advice � �Continence advice � �Adult support/advice � �Elderly support/advice � �
If you do not use the services of the Health Visitor, please go to question 20.
17. Who is your named Health Visitor? _________________________________

18. In the last month:
How many morning clinics did you attend? �How many afternoon clinics did you attend? �
How long did you (your child) wait to be seen at each clinic?
morning afternoon__________ mins __________ mins__________ mins __________ mins__________ mins __________ mins__________ mins __________ mins
19. How could the services offered by Health Visitors be improved?____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
20. Have you ever used of the services of District Nurses?
Yes � No �
If No, please go to Question 27.
21. Have you got a named District Nurse?
Yes � No �
22. If yes, who is your named District Nurse? __________________________
23. How long did you have to wait for a visit from a District Nurse for thefollowing:
(i) Urgent condition ________ hours Not applicable � ________days
(ii) Discharge from hospital ________ hours Not applicable �________ days
(iii) Routine referral from GP________ hours Not applicable � ________days
(iv) Nursing home assessment________ hours Not applicable � ________days

24. Did your GP tell you that they would arrange for the District Nurse to call?
Yes � No �
If yes, did this happen within the time period given by the GP?
Yes � No � Not applicable �
25. Hospital discharge (if you have not been discharged from hospital in thepast month, please ignore this section)
Did the hospital tell you that the District Nurse would call to see you?
Yes � No �
Did you have to contact the Health Centre before the District Nurse made a visit?
Yes � No �
How long did you wait following discharge to see the District Nurse? ________days
26. How could the District Nursing services be improved?____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
27. Please write below any other comments you would like to make about thePractice.____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

__________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Many thanks for your help.
Other measures – developed in training workshop
Qualityq % of patient records which are: relevant; concise; contemporaneous; legible;
dated; signed and actioned.
q % of previouly agreed conditions for which there is an evidence based protocolwhich is reviewed annually.
q % of evidence based protocols which are audited.
q % of time spent on patient and non-patient contact.
q Number of complaints about access to services.
q Number of inappropriate experiences of access.
Team workingq Number of suggestions which are agreed and acted upon.
q % of time in a month when GPs are available for consultation with other membersof the PHCT.
Administrative efficiencyq % of time spent looking for case notes
q % of time spent preparing repeat prescriptions

Appendix IV
Training Programme -
Tools and Techniques for Assessing
Performance
The Productivity Measurement and Enhancement System (ProMES) was used in the
research to develop effectiveness measures from primary care. Objectives were
developed in workshops with domain relevant experts from primary care (see
Appendix III) and effectiveness measures were developed with representatives two
primary health care teams (see Chapter 3 and Appendix II). ProMES is a
theoretically grounded approach, based on the NPI theory of motivation (Naylor,
Pritchard & Ilgen (1980), that has very practical applications. A critical feature of the
ProMES process is that those people who performance is being assessed are
involved in developing their own measurement and feedback systems. Participants
learn to set clear objectives, to identify ways of measuring whether they are
acheiveing these objectives, and to collect and use information to provide feedback
on performance.
Two key lessons were learnt from the Workshops and the work carried out with
primary health care team members developing measures. Firstly, the ProMES
process provides a valuable learning experience, and secondly, it is possible to
identify common objectives for primary care and to develop measures to assess
performance against these objectives.
Having demonstrated the utility and value of ProMES, and encouraged by the
exepriences of the representatives from primary care who had experienced the
ProMES process, the research team developed a ProMES training programme. The
programme was designed to train primary health care team members, and trust and
health authority staff working with primary care teams, in the ProMES technique.

Letters were sent to all the primary health care teams involved in the research
inviting representatives to attend the training programme. Responses were received
from only two teams and four team members attended the training. Letters of
invitation were also sent to representatives working with primary health care teams in
the local community trust and health authority and four people attended from these
organisations.
Details of the training programme are provided below.

Tools and Techniques for Assessing Performance
Training Plan
Day 1
11.00 - 11.15 - Overall objectives of the training programme:IntroductionsOHP - Aims and objectives• To develop skills which enable the participants to develop performance measures
with primary health care teams.• To develop skills which the participants can use to identify and use evidence to
assess performance in primary health care teams.• To teach participants how to use the measures produced by the research team.
What else would the participants want to include? What specifically do they want toget out of the training?
11.15 - 12.00 - IntroductionThe purpose of this session is to:(a) clarify what is meant by ‘performance’(b) provide participants with an understanding of the contribution that measuringperformance can make to team effectiveness in primary care,(c) raise awareness of the complexities of measuring performance in primary care.
What is ‘performance’?It is important to be clear about what it is we are trying to measure.
Discussion session - What do they understand by ‘the performance of a PHCT’?
The definition to use: The outcomes from a team, what they produce, what they aretrying to achieve.
Introduce the basic principles of ProMES(Handout 1)- productivity- motivation- feedback- prioritising effort.
Basic approach:- Design team- Clarify objectives- Develop measures of the objectives- Gather information with the measures and use this to assess extent to whichmeeting objectives, and to identify changes which can be made to improveperformance.(Handout 2, Handout 3)
Measuring performance and team effectiveness.(i) The importance of effective team working in multidisciplinary groups.

(ii) The principles of effective team working (clarity of objectives and feedback onwhether achieving these objectives, participation, task style, support for innovation,reflexivity).Feedback is only useful in the context of clear goals.To measure performance PHCTs need to have clear objectives. Using measurescan provide feedback on performance. In addition the process of developing andusing measures requires participation and reflexivity. Thus measuring performancecan make a considerable contribution to effective team working.Developing and using measures also enables PHCTs to use evidence basedpractice.(Handout 4, Handout 5)
The difficulties of measuring performance in primary careGiven what we are trying to achieve (measure the outcomes from PHCTs) Why mightthis be difficult?Discussion with the group.- multiple stakeholders, therefore, lack of agreement re. objectives, outcomes,desirable outcomes- outcomes difficult to measure (eg quality of care, patient satisfaction)- lack of sound evidence.- aspects not within the team’s control.
12.00 - 1.00 - Basic Principles for Assessing PerformanceThe purpose of this session is to:(a) Agree the objectives for primary care.(b) Identify potential sources of information which could be used to evaluateperformance against these objectives.(c) Consider what are good and bad measures of performance.(Handout 6)
Step 1 - Setting objectivesOutline the process used to develop the Objective for Primary Care (workshop, workwith teams).Present the group with the Objectives. Rate the objectives in terms of importance(purpose of this is to get them thinking critically). Do they disagree with any of theobjectives?(Handout7, Handout 8)
Critically evaluate the objectives using the ‘criteria for good objectives’.(Handout 9)
Step 2 - Identifying sources of feedback informationWork in pairs, each discuss 2 objectives, and identify sources of information availablewhich could provide feedback on performance on these objectives. (the aim at thisstage is to raise awareness about all the sources of information available, notnecessarily to identify the best sources).
Step 3 - What is a good measure?Discussion of good and bad measures. Introduce the idea that what it is easy tomeasure, is not necessarily the best measure.Discuss the ‘criteria for a good measure’.(Handout 10)
2.00 - 3.30 - Measuring Use of Resources

The purpose of this session is to give participants the opportunity to work through theprocess of developing a measure.The task is for the group to develop a measure / measures which will indicatewhether resources are being used effectively in a team.An example of a measure. In manufacturing organisations wastage of raw materialscan add considerable amount to costs. A measure of performance in relation to theobjective ‘Efficient use of Resources’ could be, therefore, % reduction in the waste ofraw materials.ExerciseThe group/s consider the following questions and develop a measure of use ofresources.
• What are the resources used / available to a PHCT? (eg financial, skills,knowledge, equipment, time, rooms)?
• What evidence is available to indicate that resources are being used efficiently?• What evidence is available to indicate that resources are being use inefficiently?• Which resources is it most critical to use efficiently? (Ie which potentially have
the greatest impact on the performance of the team?)• Decide on one aspect of resources and develop a measure.• Critically appraise the measure using the ‘criteria for measures’.
The groups work on their own with support from the trainers.They need to select a scribe and someone willing to feedback in the plenary session.The group give feedback on the process they went through to develop a measure,and the measure developed(Handout 12)
4.00 - 5.30 Plenary SessionFeedback. What aspects of the process did they find easy/difficult? What problemsdid they encounter? Did they develop a good measure?
Review learning (from the whole day)
Day 2
9.00 - 10.45 - Measuring Quality of CareThe purpose of this session is to give participants more experience of workingthrough the process of developing a measure.iReview the learning points from the session on developing measures on use ofresources (ie what have they learnt and will do differently ?)The task is to develop a measure / measures of in relation to the objective Quality ofCare. This is a difficult exercise so we are providing some materials which mighthelp. Introduce the 5 dimensions of quality.(Handout 13, Handout 14)
Exercise.The group/s consider the following questions.• What is meant by quality of care in primary care? Whose perspective should be
taken into account?• What evidence is available to indicate that good quality of care is being provided
by the PHCT?• What evidence is available to indicate that quality of care is not good?

• Which aspects of the PHCT services / types of conditions is it most critical tofocus on? (ie which would improvements in service / care have the greatestimpact on team performance?)
• Decide on one aspect of quality of care and develop a measure.• Critically appraise the measure using the ‘criteria for measures’.
The groups work on their own with support from the trainers.They need to select a scribe and someone willing to feedback in the plenary session.It is a difficult task, but we will be there to help.We want them to feedback on the process they went through to develop a measure,and the measure developed
11.00 - 11.30 - Plenary sessionFeedback. What aspects of the process did they find easy/difficult? What problemsdid they encounter? Did they develop a good measure?
Review learning.Important to emphasise that they are not now experts in developing measures, butare more aware of the process and the difficulties. With support from me they can dothis with teams.
11.30 - 12.30 - Developing measures with teams / PCGsThe purpose of this session is to provide participants with practical skills in runningmeasurement development sessions with PHCTsRun this as a how to do it information giving session.Hightlight pitfalls and problems. Emphasis thet MUST follow the correct process.MUST allow everyone to have a voice. Must NOT impose their own objectives /agenda. In addition , given the nature of primary care, the process can generateconflict - because it starts to make the implicit explicit and hightlight differences inpersepctives and values.Plus give the group the opportunity to discuss concerns, problems, obstacles thatthey foresee. etc.(Handouts 15 - 22)For example - setting-up the design team, explaining the purpose, agreeingobjectives, starting to develop measures, logging progress, action planning,gathering information, assessing the value of information, using information
1.30 - 3.00 - Using Performance MeasuresThe purpose of this session is to:(a) Familarise the participants with the measures developed by the research team sothat they understand how and when ( to use them. (how to gather evidence)(b) Develop an understanding of how to use the feedback from measures to prioritiseactivities within the PHCT, and to change existing working practices/services. (how touse evidence)
Explain how (the process) and why (to help teams to get feedback on aspects of theirperformance which were considered important to improving overall effectiveness) themeasures were developed and used by the researchers.Provide each participant with a pack of measures (need to think on an interestingway of doing this). Discuss when and how the measures might be useful.(Handouts 23, Handout 24)
Present some feedback data from the measures to the participants and discuss:

(a) how they would interpret this, what else they might need to know?(b) what actions might be taken as a result of the feedback?
3.15 - 4.00 - Plenary SessionReview of learningNext steps and action plansContacting the research team for supportSupport network/further meetings/next training.
Handout 1
Measuring and Enhancing Effectiveness inPrimary Health Care Teams
Measuring and enhancing system effectiveness is an important element in anyorganisational system, and Pritchard (Pritchard, Jones, Roth, Stuebing & Ekeberg,1988, 1989; Pritchard, 1990) has developed a sophisticated and widely applicableapproach to this - the productivity measurement and enhancement system(ProMES).
The ProMES approach is based on the theory of motivation presented by Naylor,Pritchard, and Ilgen (1980). In this theory, motivation is maximised when people seeclear connections between their efforts and the behavioural “products” or results ofthese efforts, there are clear perceived connections between a person’s products andtheir evaluations, and there are clear connections between these evaluations andvalued outcomes. When these conditions are met, motivation is high. In addition,motivation is maximised when the different evaluators and controllers of rewards in

the person’s environment such as the person himself/herself, peers, differentsupervisors, top management, and union personnel agree as much as possible onwhat should be done in the work and how it should be evaluated. When suchagreement exists, the efforts of the person are more clearly directed and the sameamount of effort results in greater productivity. In addition, stress and wasted effortare reduced.
The ProMES system develops a formal method to measure productivity and usesthese measurements as feedback to people doing the work to help them increasetheir productivity through maximising motivation. The idea is to maximise thevariables indicated in the theory so that motivation will also be maximised. Peopleare given the tools to do the work better and at the same time help them feel a senseof ownership in the resulting system and empowerment in determining importantaspects of their work.
One of the key elements in ProMES is feedback. People doing the work get regularlyoccurring, high quality feedback about how the work unit is doing. The personnel inthe work unit then use this feedback to develop plans for improving productivity.Feedback after this time tells them how well the plans they developed have actuallyimproved productivity. Furthermore, since they are heavily involved in the design ofthe measurement system and resulting feedback system, they have more confidencein its validity and accept it more than systems imposed from above. The ProMESapproach has been applied and evaluated in a wide range of settings (Pritchard,1995) and substantial improvements in performance have been shown as a result ofusing ProMES.

Handout 2
Practical tips and guidelines
Why use this system?
• it makes you think!• it gives you useful information• it indicates where you should focus your resources• it allows you to define your own measurement system - it puts you in control• it increases your participation• you are the first to know about any problems• people report less stress• people know how they are being evaluated• everyone has to agree the priorities - they are not imposed• you get valuable feedback

Handout 3
Practical tips and guidelines
Key implementation principles
• Measurement is the foundation• It takes a lot of work to measure well• What you measure is what you get• Measures for decision making are different from those for motivation• Good measurement makes feedback easy• Good feedback leads to productivity improvements• People want to do a good job• The key is to give them the tools• People want control over their lives• Acceptance of the system is essential for success• Participation leads to acceptance

Handout 4
Teamworking in Primary Care
The idea that teams are important to modern organisations was established about 70
years ago. However, in only the past 15 years has the idea been seized and widely
acted on by large numbers of organisations in the public and private sectors (Guzzo,
1996). But how effective are teams within organisations generally?
Macy and Izumi (1993) conducted an analysis of 131 organisational change studies
in order to determine their effectiveness. Those interventions with the greatest
effects on financially-related measures of organisational performance were team-
related interventions. These also reduced turnover and absenteeism more than did
other interventions, showing that team-oriented practices can have broad positive
effects in organisations. Abblebaum and Batt (1994) offer convergent evidence.
They reviewed the results of a dozen surveys of organisational practices as well as
185 case studies of innovation in management practices. They too found compelling
evidence that teams contribute to improving organisational effectiveness, particularly
increasing efficiency and quality. Other researchers provide evidence of the impact
of team-based work practices on organisational performance. Kalleburg and Moody
(1994) studied over 700 work establishments and found that those in which
teamwork was developed were more effective in their performance than those in
which were not used.
The importance of teamworking has been emphasised in numerous reports and
policy documents on the National Health Service. One recent document (NHSME
1993) particularly emphasised the importance of teamworking if health and social
care for people in local communities were going to be of the highest quality and
efficiency.

‘The best and most cost-effective outcomes for patient and clients
are achieved when professionals work together, learn together,
engage in clinical audit of outcomes together, and generate
innovation to ensure progress in practice and service.’(para 4.3)
Overall, research based evidence of teamworking in primary health care in the UK is
consistent with research in other sectors in suggesting the value of this way of
working for effectiveness and efficiency. Primary care team working has been
reported to improve health delivery and staff motivation (Wood, Farrow and Elliot,
1994) and to have led to better detection, treatment, follow-up and outcome in
hypertension (Adorian, Silverberg, Tomer and Wamosher, 1990). In a longitudinal
study of 68 primary health care teams, Poulton (1995) found a clear relationship
between teamwork and effectiveness. Those teams with high levels of clarity of team
objectives and team members commitment to those objectives were more effective
than those with unclear objectives.
However, despite these encouraging research studies, there is considerable
evidence that the context of primary health care is such that there are substantial
barriers to co-operation and collaboration in the delivery of primary health care.
Bond et al (1985) found little interprofessional collaboration in primary health care
teams in their study of 309 paired professionals. West and Poulton (1995) examined
primary health care team functioning in 68 practice teams and found that on all 4
dimensions of team functioning primary health care teams scored significantly lower
than the other team types. West, Poulton and Hardy (1994) in a study of 9 primary
health care teams identified structural, managerial and employment patterns in
primary care as crucial in undermining the effectiveness of teamworking. These
barriers to co-operation and collaboration need to be removed or reduced for
teamworking to be effective in primary heath care.

There are a number of key elements to effective teamwork (Guzzo and Shea, 1992):
• First, Individuals should feel that they are important to the success of the team.
When individuals feel that their work is not essential in a team, they are less likely
to work effectively with others or to make strong efforts towards achieving team
effectiveness. Roles should be developed in ways which make them
indispensable and essential.
• Individuals roles in the team should be meaningful and intrinsically rewarding.
Individuals tend to be more committed and creative if the tasks they are
performing are engaging and challenging.
• Teams should also have intrinsically interesting tasks to perform. Just as people
work hard if the tasks they are asked to perform are intrinsically engaging and
challenging, when teams have important and interesting tasks to perform, they
are committed, motivated and co-operative (Hackman, 1990).
• Individual contributions should be identifiable and subject to evaluation. People
have to feel not only that their work is indispensable, but also that their
performance is visible to other team members.
• Above all there should be clear, shared team goals with built-in performance
feedback. Research evidence shows consistently that where people are set clear
targets at which to aim, their performance is generally improved. For the same
reasons it is important for the team as a whole to have clear team goals with
performance feedback.
In primary health care, by and large, the first three conditions for effective
teamworking hold true. However, in primary health care teams it is rare for individual
contributions to be measured and feedback on performance given. Moreover,
primary health care teams tend not to have clear, specific objectives and goals and

feedback on performance against those objectives is rarely available. The
development of teamworking in primary healthcare, therefore, needs to focus on
developing clear, shared objectives and on providing feedback on performance.

Handout 5
The difficulties of measuring performance in primary care
• There are multiple stakeholders in primary care (different professional groups,and organisations), therefore, lack of agreement about objectives, what are theoutcomes from primary care teams, and what are desirable outcomes.
• Many of the outcomes are difficult to measure (e.g. quality of care, patientsatisfaction).
• There is a lack of sound evidence.
• Many of the factors which influence outcomes are not within the team’s control(e.g. other agencies, characteristics of practice population).

Handout 6
Practical tips and guidelines
Setting Objectives
• ask the team what it is they are trying to accomplish for their organisation• focus on larger objectives - give the group examples which are as similar to their
work as possible• this stage is typically not difficult• consensus should be easy to reach at this stage• the discussion at this point sets the tone for the future - there needs to be
balance between the facilitator saving the group time and taking control

Handout 7
Core Objectives for Primary Health Care
♦ To promote, maintain and improve health
Provide high quality health care
Accurate identification of individual and population health and care needs
Review and improve the effectiveness of health care provision
Manage illness, injury and disease taking account of agreed standards and
evidence based practice
♦ Enable personal and community responsibility for individual health
Enable patients/clients to make informed decisions about their own health
Proactively encourage positive health behaviour
Implementation of health education and preventative care programmes
♦ Efficient use of resources
Human resources - skills, knowledge, expertise, time
Physical resources - budgets, equipment, premises
♦ Continuous personal and professional development
Individual annual training plans which take account of the plans for the PHCT
Equal access to training/development resources
♦ High team member commitment, stress and satisfaction

Teamworking
Mechanisms for reviewing and acting upon staff dissatifactions, conflicts and
complaints
♦ Responsiveness to clients and community
Mechanisms for gathering information and feedback from clients/community
stakeholders/opinion leaders.
♦ Collaboration and partnership with other relevant organisations

Handout 8
Core Objectives for Primary Health Care Teams
To what extent do you think your team effectively meets the followingobjectives and sub-objectives?
To promote, maintain and improve health Of no Veryimportance important1 2 3 4 5 6 7
- Provide high quality health care 1 2 3 4
5 6 7
- Accurate identification of individual andpopulation health and care needs 1 2 3 4 5 67
- Review and improve the effectiveness ofhealth care provision 1 2 3 45 6 7
- Managing illness, injury and disease takingaccount of agreed standards and evidence 1 2 3 45 6 7based practice
Enable personal and community responsibilityfor individual health 1 2 3 4 5 6 7
- Enable patients/clients to make informed decisionsabout their own health 1 2 3 4 5 67
- Proactively encourage positive health behaviour1 2 3 4 5 6 7
- Implemention of health education andpreventative care programmes 1 2 3 4 5 67

Efficient use of resources Of no Veryimportance important1 2 3 4 5 6 7
-Human resources (skills, knowledge, expertisetime) 1 2 3 4 5 67
- Physical resources (budgets, equipment, premises)1 2 3 4 5 6 7
Continuous personal and professionaldevelopment 1 2 3 4 5 6 7
- Individual annual training plans which takeaccount of the plans for the PHCT 1 2 3 4 5 67
- Equal access to training/developmentresources 1 2 3 4 5 67
High team member commitment, stressand satisfaction 1 2 3 4 5 67
- Teamworking1 2 3 4 5 6 7
- Mechanisms for reviewing and acting uponstaff dissatisfactions, conflicts and complaints 1 2 3 4 5 67
Responsiveness to clients and community1 2 3 4 5 6 7
- Gather information and feedback from clients/community stakeholders/opinion leaders 1 2 3 4 5 67
Collaboration and partnership with otherrelevant organisations 1 2 3 4 5 67

Handout 9
Criteria for Objectives
• stated in clear terms• if exactly that objective was done, the organisation would benefit• the set of objectives must cover all important aspects of the work• objectives must be consistent with the broader organisation• higher management must be committed to each objective• keep the number of objectives manageable, normally 3 to 8

Handout 10
Practical tips and guidelines
Criteria for measures
• the measure must be consistent with the objectives of the broader organisation• if the measure was maximised would the organisation benefit• all important aspects of each objective must be covered by the set of measures• higher management must be committed to the measures• measures must be under control of the staff• measures must be understandable and meaningful to staff• it must be possible to provide information on the measure in a timely manner• the data must be cost effective to collect• the information provided by the measure must neither be too general or too
specific

Handout 11
Measuring Use of Resources
• What are the resources used / available to a PHCT? (eg financial, skills,knowledge, equipment, time, rooms)?
• What evidence is available to indicate that resources are being used efficiently?• What evidence is available to indicate that resources are being used inefficiently?• Which resources is it most critical to use efficiently? (i.e. which potentially have
the greatest impact on the performance of the team?)• Decide on one aspect of resources and develop a measure.• Critically appraise the measure using the ‘criteria for measures’.
Select a scribe and someone willing to feedback in the plenary session..We want them to feedback on the process they went through to develop a measure,and on the measure/s developed

Handout 12
Practical tips and guidelines
Developing Measures
• ask how they would show that the stated objectives were being met• this is a difficult step for the design team to do• it is frustrating - tell the group they will feel this• you must train the design team to develop and evaluate measures• the design team may not know the answer but they can find out• if someone tells you that you cannot measure what they do then ask them how
they think they are doing?, is it different to last year?. If they have an idea of theirperformance then it can be measured.

Handout 13
Dimensions of Quality
Effectiveness: Is the treatment given the best available in a technical sense,
according to those best equipped to judge?
What is their evidence? What is the overall result of the
treatment?
Acceptability: How humanely and considerately is this treatment/service
delivered? What does the patient think of it? What would/does
an observant third party think of it (“How would I feel if it were
my nearest and dearest?”) What is the setting like? Are
privacy and confidentiality safeguarded?
Efficiency: Is the output maximised for a given input or (conversely) is the
input minimised for a given level of output? How does the unit
cost compare with the unit cost elsewhere for the same
treatment/service?
Access: Can people get this treatment/service when they need it? Are
there any identifiable barriers to service - for example, distance,
inability to pay, waiting lists, and waiting times - or
straightforward
breakdowns in supply?
Equity: Is this patient or group of patients being fairly treated relative to
others? Are there any identifiable failings in equity - for
example, are some people being dealt with less favourably or
less appropriately in their own eyes than others?
Relevance: Is the overall pattern and balance of services the best that could
be achieved, taking account of the needs and wants of the
population as a whole?


Handout 14
Measuring Quality of Care
• What is meant by quality of care in primary care? Whose perspective should betaken into account?
• What evidence is available to indicate that good quality of care is being providedby the PHCT?
• What evidence is available to indicate that quality of care is not good?• Which aspects of the PHCT services / types of conditions is it most critical to
focus on? (ie which would improvements in service / care have the greatestimpact on team performance?)
• Decide on one aspect of quality of care and develop a measure.• Critically appraise the measure using the ‘criteria for measures’.
Select a scribe and someone willing to feedback in the plenary session.
Feedback on the process they went through to develop a measure, and the on themeasure/s developed

Handout 15
Basic ProMES Approach
• Gaining management and staff support • Set-up a design team • Identifying objectives • Develop measures for the objectives • Gather information with the measures • Feedback from the measures • Identify changes which can be made to improve performance.

Handout 16
Practical tips and guidelines
Conditions for success
• Management support - this means public support of the project on a regularbasis, providing the resources of the project regularly, solving project problemsand continuing the project until a clear evaluation can be made
• Trust between management and staff - process needs to be fully explainedincluding advantages and costs, explain why us?, make participation voluntary,explain how the whole team will be involved even though only part will be on thedesign team, explain how the design team will be chosen
• All interested parties approve the project - consider stakeholders, partners,unions
• Values match between management and staff - all see potential improvement asvaluable and have a long range perspective, all see participation/acceptance asessential
• Stable personnel and group structure - are there any major upheavals in staffpremises or technology

Handout 17
Practical tips and guidelines
Resources Needed for Development
• Time for design team meetings• Uninterrupted meeting setting• Full attendance by design team• Access to existing data• Meeting with management for approval of the system
Resources needed for implementation
• Collecting of existing and new data for feedback• Preparation and distribution of feedback results• Regular meetings of the group• Regular meetings of the group members to discuss feedback reports

Handout 18
Practical tips and guidelines
Checklist for starting a project
• All interested constituencies have been involved• Benefits and costs clearly explained to all• Have assessed trust and common values• Have management support (see number 2)• Have staff support (see number 2)

Handout 19
Practical tips and guidelines
Selecting the design team
• people who are respected• must be a cross section of the larger group e.g. practice nurse, senior
receptionist, general practitioner, district nurse, practice manager, health visitor• no-one occupational group should dominate• if someone is unable to attend they must nominate a deputy to represent them• individuals should feel confident about themselves and who/what they represent
and feel able to represent the views of their group

Handout 20
Practical tips and guidelines
Logging progress
• keep an accurate record of the progress made at each meeting• provide the design team with an update of their progress at regular intervals• you may find that between meetings the design team do not any homework and
you will need to review previous sessions at the beginning of new sessions• provide the team with the list of objectives when completed along with their list of
measures• the design team must also report progress to the other members of the larger
group and your updates is a useful way of achieving this• the team will need reassurance that progress is being made even if it is minor to
spur them on to the next stage

Handout 21
Practical tips and guidelines
Action planning
• at the end of each session you will need to plan for the actions to be carried outby the next session
• this may include collecting information and specific data• it must be clear from the outset that this is not the responsibility of the facilitator• members of the team will need to ‘volunteer’ to carry out actions• it is easy to walk away from a session believing that everyone knows what they
are soposed to do - it is more than likely someone does not• check and check until you are satisfied that everyone understands their
responsibilities• if you do this regularly the team will start to check you!• it is a good idea to have a session plan, you must be clear about what you want
to achieve at each session• also record the feedback the team give you at the beginning of the session, it
often proves useful later

Handout 22
Practical tips and guidelines
Possible problems
• lack of commitment from the design team - not present at meetings or lack ofresponse
• getting stuck - cant see how to move forward• design team going off on a tangent - avoiding what can be hard thinking work• disagreement between members - possible personal issues• domineering members - other members passively agreeing• feeling lost with it all - do not know what to do next• not been given the required time and space for the sessions or interrupted• larger team losing interest• management support withheld• no-one willing to collect data• got the data don’t know what to do next

Handout 23
Practical tips and guidelines
Gathering information
• the information gathered must be of good quality• the team must think about the most effective ways to gather information• you will need to discuss their expectations, what do they expect to be the
outcome• they may need to design record sheets or charts or questionnaires which must be
piloted to evaluate their effectiveness• who will distribute, collect, collate, evaluate and present the data to the design
team• these may all be new skills but is an excellent development opportunity• the team will need support in this, from you and from each other Assessing the value of the information • does the data answer the question• are you satisfied that the data is good quality• did you discuss how to asses the data before you began• do you have the resources to assess the data, people, time, technology

Handout 24
Practical tips and guidelines
Using information
• does this data provide you with useful information• you will need to discuss dissemination with the team• you must feedback the results of data gathering if you want people to co-operate
in the future• what next - if you have some useful information you can then use this to plan
ahead and use the information to make your case for change

____________________________________________________________________
BIBLIOGRAPHY___________________________________________________________
Adorian, D., Silverberg, D.S., Tomer, D. & Wamasher, Z. (1990). Group discussionwith the health care team: A method of improving care of hypertension in generalpractice.Journal of Human Hypertension, 4 (3), 265 - 268.
Alderfer, C.P. (1977). Group and intergroup relations in J.R. Hackman and J.L. Suttle(eds) Improving the quality of work life. Pallisades, C.A.: Good year. pp 277 - 296.
Alexander, J. A., Lichtenstein, R. & D’Aunno, T. A. (1996). The effects of treatmentteam diversity and size on assessments of team functioning. Hospital & HealthServices Administration, 41, 37-53.
Allen, N. J. (1996). Affective reactions to the group and organisation. In M. A. West(Ed.), Handbook of Work Group Psychology (pp. 371-396). Chichester: Wiley.
Amabile, T.M. (1983). The social psychology of creativity: A componentialconceptualization. Journal of Personality and Social Psychology, 45, 357-376.
Ancona, D.F. & Caldwell, D.F. (1988). Bridging the boundary: External activity andperformance in organisational teams. Administrative Science Quarterly, 37, 634-665.
Anderson, N.R. & King, N. (1993). Innovation in organisations. In C.L.Cooper &I.T. Robertson (eds). International Review of Industrial and OrganizationalPsychology,Vol 8, Chichester: Wiley.
Anderson, N, & West, M.A. (1994). The Team Climate Inventory: Manual and User’sGuide. Windsor, England: NFER-Nelson.
Anderson, N. & West, M.A. (1998). Measuring climate for work group innovation:development and validation of the team climate inventory: Journal of OrganizationalBehaviour, Vol 19, 235 - 258.
Applebaum, E. & Batt, R. (1994). The New American Workplace. Ithaca, NY: ILRPress.
Audit Commission (1992). Homeward Bound: A New Course for Community Health.London: HMSO.
Bales, R.F., Strodtbeck, F.L., Mills, T.M. & Roseborough, M.E. (1951). Channels ofcommunication in small groups. American Sociological Review, 16, 461-468.
Baumeister, R.F. & Leary M.R., (1995). The need to belong desire for interpersonalattachments as a fundemental motivator. Psychological Bulletin, 117, 497-529.

Berger, J., Fisek, M.H., Norman, R.Z., & Zelditch Jr, M. (1977). Status characteristicsand social interaction. NY: Elsevier.
Berger, J., Rosenholtz, S.J., & Zelditch Jr., M. (1980). Status organizing processes.Annual Review of Sociology, 6, 479-508.
Bhugra, D., Bridges, K., & Thompson, C. (1995). Caring for a community: thecommunity care policy of the Royal College of Psychiatrists. London: Royal Collegeof Psychiatrists.
Billings, R.S., Milburn, T.W. & Schaalman, M.L. (1980). A model of crisis perception:A theoretical and empirical analysis. Administrative Science Quarterly, 25, 300-316.
Blakar, R.M. (1985). Towards a theory of communication in terms of precondition:A conceptual framework and some empirical explorations. In H. Giles and R.N. StClaireds), Recent Advances in Language, Communication and Social Psychology.London: Lawrence Erlbaum.
Blau, Peter M. (1977). Inequality and Heterogeneity. New York: Free Press.
Bobko, P., & Colella, A. (1994). Employee reactions to performance standards:A review and research proposition. Personnel Psychology, 47, 1-29.
Bond, J., Cartilidge, A.M., Gregson, B.A., Philips, P.R., Bolam, F., & Gill, K.M. (1985).A study of interprofessional collaboration in primary health care organisations.Report No 27 (2), Newcastle-upon-Tyne, Health Care Research Unit, University ofNewcastle-upon-Tyne.
Borrill, C.S. & West, M.A. (1997). Effectiveness in primary health care. CAIPEbulletin.No 14.
Borrill, C.S. & West, M.A. (1998). Strain in primary health care. Unpublished report.Institute of Work Psychology, University of Sheffield, England.
Borrill, C.S., Wall. T.D., West, M.A., Hardy, G.E., Shapiro, D.A., Haynes, C.E., Stride,C.B., Woods, D. and Carter, A.J. (1998) Stress among staff in NHS Trusts. Instituteof Work Psychology, University of Sheffield, Psychological Therapies ResearchCentre, University of Leeds.
Bottger, P.C. & Yetton, P.W. (1987). Improving group performance by training inindividual problem solving. Journal of Applied Psychology, 72, 651-657.
Bowers, D.G. & Seashore, S.E. (1966). Predicting organisational effectiveness with afour-factor theory of leadership. Administrative Science Quarterly, 11, 238-263.
Brewer, N., Wilson, C. & Beck, K. (1994). Supervisory behavior and teamperformance amongst police patrol sergeants. Journal of Occupational andOrganizational Psychology, 67, 69-78.
Brown, R.J. (1988). Group Processes: Dynamics Within and Between Groups.London: Blackwell.

Bryk, A. & Raudenbush, S. (1992) Hierarchical Linear Models: Applications and dataanalysis methods. In J. Deleeuw (Ed.) Advanced quantitative techniques in thesocial sciences series. Newbury, CA: Sage Publications.
Burns, T., & Stalker, G.M. (1966). The Management of Innovation. London: TavistockPublications.
Carletta, J., Garrod, S., & Fraser-Krauss, H. (1998). Communication and Placementof Authority in Workplace Groups — The Consequences for Innovation. Small GroupResearch, 29(5), 531-559.
Carter, M.F., Evans, K.E., Crosby, C., Prendeergast, L.A., & De Sousa Butterworth,K.A. (1997). The all-Wales community mental health team survey. Bangor: HealthServices Research Unit.
Campion, M.A., Medsker, G.J. & Higgs, A.C. (1993). Relations between work groupcharacteristics and effectiveness: Implications for designing effective work groups.Personnel Psychology, 46, 823-850.
Campion, M.A., Papper, E.M. & Medsker, G.J. (1996). Relations between workteam characteristics and effectiveness: A replication and extension. PersonnelPsychology, 49, 429-689.
Cant, S. & Killoran, A. (1995) Team tactics: a study of nurse collaboration in generalpractice, Health Education Journal, 52, 203 - 8.
Coch, L. & French, J. R. (1948). Overcoming resistance to change. HumanRelations,1, 512-532.
Cohen, S.G. & Bailey, D.E. (1997) What makes teams work: Group effectivenessresearch from the shop floor to the executive suite. Journal of Management, No 3.239 - 290.
Connolly, T., Conlon, E.J. & Deutsch, S.J. (1980). Organizational effectiveness: amulti-disciple-constituency approach, 98, 310 - 357.
Cott, C. (1997). “We decide, you carry it out”: A social network analysis ofmultidisciplinary long-term care teams. Social Science & Medicine, 45 (9), 1411-1421.
Cowan, D.A. (1986). Developing a process model of problem recognition. Academyof Management Review, 11, 763-776.
D'Zumla, T.J. & Goldfried, M.R. (1971) Problem solving and behaviour modifications.Journal of Abnormal Psychology. 78, 107 - 126.
Davenport, T.H. (1993). Process Innovation: Re-engineering Work ThroughInformation Technology. Cambridge, MA: Harvard Business School Press.
Deming, W.E. (1986). Out of the Crisis. Cambridge, MA: Center for AdvancedEngineering Study, Massachusetts Institute of Technology.

Department of Health (1990). The Care Programme Approach for people with amental illness referred to the specialist psychiatric services. London, Department ofHealth, HC (90) 23/LASSL (90) 11.
Department of Health (1995). Building bridges: a guide to arrangements for inter-agency working for the care and protection of severely mentally ill people. London:HMSO.
Department of Health (1997). The Patient's Charter: mental health services. London,Department of Health.
Department of Health (1999). National Service Framework for Mental Health: Modernstandards and service models. London: Department of Health.
Dreachslin, J.L., Hunt, P.L. & Sprainer, E. (2000). Workforce diversity: Implicationsfor the effectiveness of health care delivery teams. Social Science & Medicine, 50,1403-1414.
Dreachslin, J.L., Hunt, P.L. & Sprainer, E. (1999a). Communication patterns andgroup composition: Implications for patient-centred care team effectiveness. Journalof Healthcare Management, 44, 252-268.
Dreachslin, J.L., Hunt, P.L. & Sprainer, E. (1999b). Key indicators of nursing teamperformance: Insights from the front line. The Health Care Supervisor, 17, 70-76.
Drolen, C.S. (1990). Current community mental health center operations:Entrepreneurship or business as usual? Community Mental Health Journal, 26, 547-558.
Drory, A. & Shamir, B. (1988). Effects of organizational and life variables on jobsatisfaction and burnout. Group and Organization Studies, 13 (4), 441-455.
Eden, D. (1990). Pygmalion without interpersonal contrast effects: Whole groups gainfrom raising manager expectations. Journal of Applied Psychology, 75, 394-398.
Eggert, G.M., Zimmer, J.G., Hall, W.J. & Friedman, B. (1991). Case management:A randomised controlled study comparing a neighbourhood team and a centralizedindividual model. Health Services Research, 26 (4), 471-507.
Faulkner, A. (1997). Knowing our own minds: A survey of how people in emotionaldistress take control of their lives. London: Mental Health Foundation.
Fay, N., Garrod, S., & Carletta, J. (2000). Group discussion as interactive dialogue orserial monologue: The influence of group size. Psychological Science, 11(6), 487-492.
Field, R. & West, M.A. (1995). Teamwork in primary health care. Two Perspectivesfrom practices. Journal of Interprofessional Care, 9, 2, 123-130.
Freeman, M., Miller, C. & Ross, N. (2000). The impact of individual philosophies ofteamwork on multi-professional practice and the implications for education. Journal ofInterprofessional Care, 14 (3), 237-247.

Galbraith, J. R. (1993). The business unit of the future. In J. R. Galbraith, E.E. LawlerIII & Associates (Eds), Organizing for the Future: The New Logic for ManagingComplex Organizations. San Francisco: Jossey-Bass.
Galbraith, J. R. (1994). Competing with Flexible Lateral Organisations (2nd edn).Reading, MA: Addison-Wesley.
Galbraith, J.R., Lawler, E.E. III & Associates (1993). Organizing for the Future: TheNew Logic for Managing Complex Organizations. San Francisco: Jossey-Bass.
George, J.M. (1989). Mood and absence. Journal of Applied Psychology, 74, 317-324.
George, J.M. (1990). Personality, affect, and behavior in groups. Journal of AppliedPsychology, 75, 107-166.
George, J.M. (1995). Leader positive mood and group performance: The case ofcustomer service. Journal of Applied Social Psychology, 25, 778-794.
George, J.M. (1996). Group affective tone. In M.A. West (Ed.), Handbook of WorkGroup Psychology (pp. 77-94). Chichester: Wiley.
George, J.M. & Bettenhausen, K. (1990). Understanding pro-social behaviour, salesperformance and turnover. A group-level analysis in a service context. Journal ofApplied Psychology, 75, 698-709.
Gladstein, D. (1984). Groups in context: A model of task group effectiveness.Administrative Science Quarterly, 29, 499-517.
Goldberg, D.P. & Williams, P. (1991). A user's guide to the General HealthQuestionnaire. Windsor: NFER-Nelson.
Goldberg. D.P. (1972). The detection of minor psychiatric illness by questionnaire.Oxford: Oxford University Press
Goni. S. (1999). An analysis of the effectiveness of Spanish primary health careteams. Health Policy, 48, 107-117.
Grusky, O. (1995). The organization and effectiveness of community mental healthsystems. Administration & Policy in Mental Health, 22, 361-388.
Guzzo, R.A. (1996). Fundamental considerations and about work groups. In M.A.West (ed) Handbook of Work Group Psychology. Chichester: John Wiley.
Guzzo, R. A. & Dickson, M. W. (1996). Teams in organisations: Recent research onperformance and effectiveness. Annual Review of Psychology, 46, 307-338.
Guzzo, R.A., Jette, R.D., & Katzell, R.A. (1985). The effects of psychologically basedintervention programs on worker productivity: A meta-analysis. PersonnelPsychology, 38, 275-291.
Guzzo, R. A. & Salas, E. (Eds) (1995). Team Effectiveness and Decision Making inOrganisations. San Francisco: Jossey-Bass.

Guzzo, R.A. & Shea, G.P. (1992). Group performance and intergroup relations inorganisations. In M. D. Dunnette and L. M. Hough (Eds), Handbook of Industrial andOrganizational Psychology, (Vol 3, pp. 269-313). Palo Alto, CA: Consulting
Psychologists Press.
Hackman, J.R. (1987). The design of work teams. In J.W. Lorsch (ed) Handbook of
Organisational Behaviour. Englewood Cliffs, NJ: Prentice-Hall. Pp 315 - 342.
Hackman, J.R. (1990). (Ed), Groups That Work (and Those That Don't): CreatingConditions for Effective Teamwork. San Francisco: Jossey-Bass.
Hackman, J.R., Brousseau, K.R. & Weiss, J.A. (1976). The interaction of task designand group performance strategies in determining group effectiveness.Organizational Behavior and Human Performance, 16, 350-365.
Hackman, J.R. & Morris, C.G. (1975). Group task, group interaction process, andgroup performance effectiveness: A review and proposed integration. In L. Berkowitz(Ed.), Advances in Experimental Social Psychology, (Vol. 8). New York: AcademicPress.
Hannigan, B. (1999). Joint working in community mental health: prospects andchallenges. Health and Social Care in the Community, 7, 25-31.
Hardy, G. E., Shapiro, D.A., Hayes, C.E. & Rick, J.E. (1999). Validation of theGeneral Health Questionnaire using a sample of employees from the health careservices. Submitted.
Haynes, C.E., Wall, T.D., Bolden, R.I. & Rick, J.E. (1998). Measures of perceivedwork characteristics for health service research: test of a measurement model andnormative data. Submitted.
Hedburgh, B.L.T., Nystrom, P.C. and Starbuck, W.H. (1976) Company on seesaws:prescriptions for a self designing organisation. Administrative Science Quarterley,21, 41 - 65.
Hill, F. (1998). Trying to catch a cloud: organizational climate in the NHS.Unpublished PhD Thesis, Institute of Work Psychology, University of Sheffield.
Hirokawa, R.Y. (1990). The role of communication in group decision-making efficacy:A task-contingency perspective. Small Group Research, 21, 190-204.
Hoffman, L.R. & Maier, N.R.F. (1961). Sex differences, sex composition, and groupproblem-solving. Journal of Abnormal and Social Psychology, 63, 453-456.
Hogg, M. & Abrams, D. (1988). Social Identifications: A Social Psychology ofIntergroup Relations and Group Processes. London: Routledge.
Hughes, S.L., Cummings, J., Weaver, F., Manheim, L., Brawn, B. & Conrad, K.(1992).

A randomised trial of the cost effectiveness of VA hospital-based home care for theterminally ill. Health Services Research, 26 (6), 801-817.
Jackson, G., Gater, R., Goldberg, D., Tantam, D. Loftus, L. & Taylor, H. (1993). Anew community mental health team based in primary care: A description of theservice and its effect on service use in the first year. British Journal of Psychiatry,162, 375-384.
Jackson, L.A., Sullivan, L.A. & Hodge, L.N. (1993). Stereotype effects onattributions, predictions and evaluations: No two social judgements are quite alike.Journal of Personality and Social Psychology, 65 (1), 69-84.
Jackson, S.E. (1996). The consequences of diversity in multidisciplinary work teams.InM.A. West (Ed.), Handbook of Work Group Psychology, pp. 53-76, Chichester: Wiley.
Jacobs, D. & Singell, L. (1993). Leadership and organizational performance:Isolating links between managers and collective success. Social Science Research,22, 165-189.
Janis, I.L. (1982). Groupthink: A Study of Foreign Policy Decisions and Fiascos, 2nded. Boston: Houghton Mifflin.
Jansson, A., Isacsson, A. & Lindhom, L.H. (1992). Organization of health care teamsand the population’s contacts with primary care. Scandinavian Journal of HealthCare, 10,257-265.
Jervis, I.L. (1976). Perception and Misperception in International Politics. Princeton,NJ: Princeton University Press.
Jones, R.V.H. (1992). Teamworking in primary care:how do we know about it?Journal of Interprofessional Care, Vol 6, p25-29.
Juran, J.M. (1989). Juran on Leadership for Quality. New York: Free Press.
Jussim, L. (1986). Self-fulfilling prophecies: A theoretical and integrative review.Psychological Review, 93 (1), 429-445.
Jussim, L., Coleman, L.M. & Lerch (1987). The nature of stereotypes: A comparisonand integration of three theories. Journal of Personality and Social Psychology, 52(3), 536-546.
Kalleburg, A.L. & Moody, J.W. (1994). Human Resource Management andOrganisational Performance. American Behaviourist Scientist, 37, 948 - 962.
Kanter, R.M. (1983). The Change Masters: Corporate Entrepreneurs at work.New York: Simon & Schuster.
Kiesler, S. & Sproull, L. (1982). Managerial responses to changing environments:perspectives in problem solving from social cognition. Administrative ScienceQuarterley, 27, 548 - 570.
Kimble, C.E., Marsh, N.B. & Kiska, A.C. (1984). Sex, age and cultural differences inself-reported assertiveness. Psychological Reports, 55, 419-422.

King, N. (1990). Innovation at work: The research literature. In M. A. West & J. L.Farr (Eds), Innovation and Creativity at Work: Psychological and OrganisationalStrategies, pp. 15-59, Chichester: Wiley.
King, N., Anderson, N.R. & West, M. (1991). Organizational innovation in the UK: Acase study of perceptions and processes. Work and Stress, 5 (4), 331-339.
King, R., Le Bas, J., & Spooner, D. (2000). The impact of caseload on the personalefficacy of mental health case managers. Psychiatric Services, 51, 364-368.
Kinnunen, J. (1990). The importance of organizational culture on developmentactivities in a primary health care organisation. International Journal of HealthPlanning and Management, 5, 65-71.
Klimoski, R. & Mohammed, S. (1994). Team mental model: Construct or metaphor?Journal of Management, 20, 403-437.
Komaki, J.L., Desselles, M.L. & Bowman, E.D. (1989). Definitely not a breeze:Extending an operant model of effective supervision to teams. Joumal of AppliedPsychology, 74, 522-529.
Koshuta, M. & McCuddy, M.K. (1989). Improving productivity in the health careindustry:An argument and supporting evidence from one hospital. The Health CareSupervisor.
LaFrance, M. & Mayo, C. (1978). Moving Bodies: Nonverbal Communication inSocial Relationships. Monterey, C.A.: Brooks/Cole.
Landsberger, H.A. (1955). Interaction process analysis of the mediation oflabormanagement disputes. Journal of Abnormal and Social Psychology, 51, 522-528.
Latham, G.P., Erez, M. & Locke, E.A. (1988). Resolving scientific disputes by thejoint design of crucial experiments by the antagonists: Application to the Erez Lathamdispute regarding participation in goal setting. Journal of Applied Psychology, 73 (4),753-772.
Lawler, E.E. & Hackman, J.R. (1969). Impact of employee participation indevelopment of pay incentive plans: A field experiment. Journal of AppliedPsychology, 53, 467-471.
Lawrence, P.R. & Lorsch, J. (1967). Organization and Environment. Cambridge,NIA:Harvard University Press.
Macy, B.A. & lzumi, H. (1993). Organizational change, design and work innovation:A meta-analysis of 131 North American field studies-1961-1991. Research inOrganizational Change and Design (Vol. 7). Greenwich, CT: JAI Press.
Maier, N.R.F. (1963). Problem-solving Discussions and Conferences: LeadershipMethods and Skills. New York: McGraw-Hill.
Maier, N.R.F. (1970). Problem Solving and Creativity in Individuals and Groups.Monterey, CA: Brooks/Cole.

Maier, N.R.F. & Solem, A.R. (1962). Improving solutions by turning choice situationsinto problems. Personnel Psychology, 15, 151-157.
Main, J. (1989). At last, software CE0s can use. Fortune, 13 March, 77 - 83.
Markiewicz, L. & West, M.A. (1996). Team-based Organisation. Aberdeen:Grampian/ECITB.
Markiewicz, L. & West, M.A. (1996). Team-based Organisation. Aberdeen:Grampian/ECITB.
Mathison, D.L. & Tucker, R.K. (1982). Sex differences in assertive behaviour:A research extension. Psychological Reports, 51(3), 943-948.
Maxwell, R.J. (1992). Dimensions of quality revisited: from thought to action. QualityHealth Care 1, 171-177.
Maznevski, M.L. (1994). Understanding our differences: Performance in decisionmaking groups with diverse members. Human Relations, 47 (5), 531-552.
McClure, L.M. (1984) Teamwork, myth or reality: community nurses effectivenesswith general practice attachment. Journal of Epidemiology and Community Health, 21(1),68 - 74.
McGrath, J.E. (1984). Groups: Interaction and Performance. Englewood Cliffs, NJ:Prentice-Hall.
Miceli, M.P. & Near, J.P. (1985). Characteristics of organisational climate andperceived wrong-doing associated with whistle-blowing decisions. PersonnelPsychology, 38,525-544.
Milliken, F.J. & Martins, L.L. (1996). Searching for common threads: Understandingthe multiple effects of diversity in organizational groups. Academy of ManagementReview, 21(2), 402-433.
Mistral, W., & Velleman, R. (1997). Community mental health teams: Theprofessionals' choice? Journal of Mental Health, 6, 125-140.
Mitrot, I.I. & Featheringham, T.R. (1974) On systematic problem solving and the errorof the third kind. Behavioural Science, 19, 383 - 393.
Mohman, S.A., Cohen, S.G. & Mohrman, A.M., Sr (1995). Designing Team-BasedOrganizations. San Francisco: Jossey-Bass.
Mullarkey, S., Wall, T.D., Warr, P.B., Clegg, C.S. & Stride, C. (1999). Measures ofjob satisfaction, mental health and job-related well-being: A bench-marking manual.Sheffield, England: Sheffield Academic Press Ltd.
Mumford, M.D. & Gustafson, S.B. (1988). Creativity syndrome: Integration,application and innovation. Psychological Bulletin, 103, 27-43.

Myer, C. (1993). How to Align Purpose, Strategy and Structure for Speed. NewYork: Free Press.
Naylor, J.C., Pritchard, R.D., & Ilgen, D.R. (1980). A theory of behaviour inorganisations. New York:Academic Press.
Netten, A. & Dennett, J. (1997). Unit lists of health and social care. London: PSSRU.
Nievaard, A.C. (1987). Communication climate and patient care: Causes and effectsof nurses’ attitudes to patients. Social Science and Medicine, 24 (9), 777-784.
Onyett, S. (1995). Responsibility and accountability in community mental healthteams. Psychiatric Bulletin, 19, 281-285.
Onyett, S. (1997). The challenge of managing community mental health teams.Health and Social Care in the Community, 5, 40-47.
Onyett, S., Pillinger, T. & Muijen, M. (1995). Making community mental health teamswork. London: Sainsbury Centre for Mental Health.
Pearce, J.A. & Ravlin, E.C. (1987). The design and activation of self-regulating workgroups. Human Relations, 40, 751-782.
Peck, E., & Norman, I.J. (1999). Working together in adult community mental healthservices: Exploring inter-professional role relations. Journal of Mental Health, 8,231-243.
Peck, E., & Parker, E. (1998). Mental health in the NHS: Policy and practice 1979-98.Journal of Mental Health, 7, 241-259.
Peiro, J.M., Gonzalez-Roma, V., & Romos, J. (1992) The infleince of work teamclimate on role stress, tension, satisfaction and leadership perceptions. EuropeanReview of Applied Psychology, 42 (1) 49-46.
Pincus, H.A., Zarin, D.A. & West, J.C. (1996). Peering into the 'black box': measuringoutcomes of managed care. Archives of General Psychiatry, 53, 870-877.
Podsakolf, P.M. & Todor, W.D. (1985). Relationships between leader reward andpunishment behavior and group processes and productivity. Journal of Management,11, 55-73.
Porac, J. F. & Howard, H. (1990). Taxonomic mental models in competitor definition.Academy of Management Review, 2, 224-240.
Poulton, B. C. & West, M. A. (1993). Effective multidisciplinary teamwork in primaryhealth care. Journal of Advanced Nursing, 18, 918-925.
Poulton, B. C. & West, M. A. (1994). Primary health care team effectiveness:Developing a constituency approach. Health and Social Care, 2, 77-84.
Poulton, B.C. & West, M.A. (1997). A failure of function: teamwork in primary healthcare. Journal of Interprofessional Care, 11, No 2, 1997.

Pritchard, R. D., Jones, S. D., Roth, P. L., Stuebing, K. K. & Ekeberg, S. E. (1988).Effects of group feedback, goal setting, and incentives on organizational productivity.Journal of Applied Psychology, 73, 337-358.
Pritchard, R.D. (ed) (1995) Productivity Measurement and Improvement:Organisational Case Studies. New York: Praeger.
Pritchard, R.D., Jones, S.D., Roth, P., Stuebing, K.K., & Ekeberg, S.E. (1989). Theevaluation of an integrated approach to measuring organisational productivity.Personnel Psychology, 42 (1) 69-115.
Pritchard, R.D. (Ed) (1995). Productivity Measurement and Improvement:Organisational Care Studies: New York: Praeger.
Pritchard, R.D., Jones, S.D., Roth, P.L., Stuebing, K.K. & Ekeberg, S.E. (1988). Theeffects of feedback, goal setting, and incentives on organisational productivity.Journal of Applied Psychology Monograph Series, 73 (2), 337-358.
Prosser, D., Johnson, S., Kuipers, E., Szmukler, G., Bebbington, P., & Thornicroft, G.(1996). Mental Health, 'Burnout' and job satisfaction among hospital and community-based mental health staff. British Journal of Psychiatry, 169, 334-337.
Quinn, R.E. & Rohrbaugh, J. (1983). Predicting sales success through handwritinganalysis: an evaluation of the effects of training and handwriting sample content.Journal of Applied Psychology 68 (2), 212 - 17.
Redmond, M.V. (1989). The functions of empathy (decentering) in human relations.Human Relations, 42, 593-605.
Redmond. M.V. (1992). A multi-dimensional theory and measure of decentering.Unpublished manuscript.
Reed J. (1995). Leadership in the mental health service: What role for doctors?Psychiatric Bulletin, 19, 67-72.
Rees, A., Stride, C.B., Shapiro, D.A., Richards, A. and Borrill, C.S. (in press).Psychometric properties of the Community Health Team Questionnaire. (CMHTEQ)Journal of Mental Health.
Richards, A. & Rees, A. (1998) Developing Criteria to measure the effectiveness ofcommunity mental health teams. Mental Health Care, 2, 14 - 17.
Roberts, J.M. (1995) The History of the World. Hammondsworth, Middlesex:Penguin.
Ross, F., Rink, E. & Furne, A. (2000). Integration or pragmatic coalition? Anevaluation of nursing teams in primary care. Journal of Interprofessional Care, 14 (3),259-267.
Rousseau, D.M. (1985) Issues of level in organisational research: multi-level andcross-level perspectives. Research in Organisational Behaviour, 7, 1 - 37.
Sainsbury Centre for Mental Health (1997). Pulling together: The future roles andtraining of mental health staff. London: Sainsbury Centre for Mental Health.

Schober, M.F., & Clark, H.H. (1989). Understanding by addressees and overhearers.Cognitive Psychology, 21, 211-232.
Schwenk, C.R. (1988). The Essence of Strategic Decision-making. Cambridge, NIA:Heath.
Senge, P. (1990). The Fifth Discipline: The Art and Practice of the LearningOrganization. New York: Doubleday Currency.
Shaw, M.E. (1976). Group Dynamics: The Psychology of Small Group Behavior. NewYork: McGraw-Hill.
Shaw, M.E. (1981). Group Dynamics: The Psychology of Small Group Behavior.New York: McGraw-Hill.
Sluyter, G.V. (1995). Mental health leadership training: A survey of state directors.Journal of Mental Health Administration, 22, 201-204.
Smircich, L. (1983). Organization as shared meaning. In L.R. Pondy, P. Frost, G.Morgan & T. Dandridge (Eds), Organizational Symbolism (pp. 55-65). Greenwich,CT: JAI Press.
Smith, K.G., Locke, E.A. & Barry, D. (1990). Goal setting, planning andorganizational performance: An experimental simulation. Organizational Behaviorand Human Decision Processes, 46, 118-134.
Sommers, L.S., Marton, K.I., Barbaccia, J.C. & Randolph, J. (2000). Physician, nurseand social worker collaboration in primary care for chronically ill seniors, Archives ofInternal Medicine, 160, 1825-1833.
Stein, M. (1996). Unconscious phenomena in work groups. In M.A. West (Ed.),Handbook of Work Group Psychology, pp. 143-157 Chichester: Wiley.
Stemberg, R.J. & Lubart, T.I. (1990) Defying the Crowd. Cultivating Creativity in aCulture of Conformity. New York: Free Press.
Stevens, M.J., & Campion, M.A. (1994). The knowledge, skill and abilityrequirements for teamwork: Implications for human resource management. Journal ofManagement, 20,503-530.
Stevens, M.J. & Campion, M.A. (1999). Staffing Work Teams: Development andValidation of a Selection Test for Teamwork Settings. Journal of Management, 25,No 2 207 - 228.
Sundstrom, E., De Meuse, K.P. & Futrell, D. (1990). Work teams: Applications andeffectiveness. American Psychologist, 45, 120-133.
Tajfel, H. (1978). Differentiation Between Social Groups: Studies in the SocialPsychology of Intergroup Relations (European Monographs in Social Psychology,No. 14). London:Academic Press.
Tajfel, H. & Turner, J.C. (1979). An integrative theory of intergroup conflict.In W. G. Austin and S. Worchel (Eds), The Social Psychology of IntergroupRelations. Monterey, CA: Brooks/Cole.

Tannenbaum, S.I., Beard, R.L. & Salas, E. (1992). Team building and its influenceon team effectiveness: An examination of conceptual and empirical developments.In K. Kelley (Ed.), Issues, Theory and Research in Industrial/OrganizationalPsychology (pp. 117-153), London: North Holland.
Tannenbaum, S.I., Salas, E. & Cannon-Bowers, J.A. (1996). Promoting teameffectiveness. In M.A. West (Ed.), Handbook of Work Group Psychology, (pp 503-529)Chichester: Wiley.
Taylor, M.F. (Ed), with Brice, J., Buck, N. & Prentice, E. (1995). British HouseholdPanel Survey User Manual. Colchester: University of Essex.
Tjosvold, D. (1982). Effects of approach to controversy on superiors' incorporation ofsubordinates' information in decision making. Joumal of Applied Psychology, 67,189-193.
Tjosvold, D. (1985). Implications of controversy research for management. Journalof Management, 11, 21-37.
Tjosvold, D. (1991). Team Organisation: An Enduring Competitive Advantage.Chichester: Wiley.
Tjosvold, D. & Field, R.H.G. (1983). Effects of social context on consensus andmajority vote decision making. Academy of Management Journal, 26, 500-506.
Tjosvold, D. & Johnson, D.W. (1977). The effects of controversy on cognitiveperspective-taking. Journal of Educational Psychology, 69, 679-685.
Tjosvold, D., Wedley, W.C. & Field, R.H.G. (1986). Constructive controversy, theVroom-Yetton model, and managerial decision making. Journal of OccupationalBehavior, 7,121 -138.
Toon, P.D. (1994) What is Good General Practice? A Philosophical Study of theConcept of High Quality Medical Care.
Tziner, A.E. (1988) Effects of team composition on ranked team effectiveness. SmallGroup Behaviour, 19, 363 - 378.
Vroom, V.H. (1964). Work and Motivation. New York: Wiley.
Wall, T.D. & Lischeron, J.H. (1977). Worker Participation: A Critique of the Literatureand some Fresh Evidence. Maidenhead, UK: McGraw-Hill.
Walsh, J.P. & Fahey, L. (1986). The role of negotiated belief structures in strategymaking. Journal of Management, 12, 325-338.
Walsh, J.P., Henderson, C.M. & Deighton, J. (1988). Negotiated belief structuresand decision performance: An empirical investigation. Organizational Behavior andHuman Decision Processes, 42, 194-216.
Watson, W.E., Kumar, K. & Michaelsen, L.K. (1993). Cultural diversity's impact oninteraction process and performance: Comparing homogeneous and diverse task

groups. Academy of Management Journal, 36, 590-602.
Weldon, E. & Weingart, L.R. (1993). Group goals and group performance. BritishJournal of Social Psychology, 32, 307-334.
West, M.A. (1990). The social psychology of innovation in groups. In M.A. West &J.L. Farr (Eds), Innovation and Creativity at Work (pp. 309-333). Chichester: Wiley.
West, M.A. (1994). Effective Teamwork. Leicester: British Psychological Society.
West, M.A. (1996a). The Handbook of Work Group Psychology. Chichester: Wiley.
West, M.A. (1996b). Reflexivity and Work Group Effectiveness: A conceptualIntegrationin M.A. West (Ed) Handbook of Work Group Psychology (555 - 580), John Wiley &Sons Ltd.
West, M.A. (1997). Developing Creativity in Organisations. Chichester: Wiley.
West, M.A. (2000). State of the art: Creativity and Innovation at work. Psychologist,13, 9 460 - 464.
West, M.A. & Anderson, N.R. (1996). Innovation in top management teams. Journalof Applied Psychology, 81(6), 680-693.
West, M.A., Borrill, C.S. and Stride, C.B. (1998). Strain as a moderator of therelationship between work characteristics and work attitudes. Journal of OccupationalHealth. Vol 4,No 1, 3 - 14.
West, M.A., Borrill, C.S. & Unsworth, K. (1998). Team Effectiveness in Organisations.In C.L. Cooper & I.T. Robertson (eds) International Review of IndustrialOrganisational Psychology. Vol 13. Wiley & Sons: Chichester.
West, M.A. & Field, R. (1995). Teamwork in primary health care. Perspectives fromorganisational psychology. Journal of Interprofessional Care, 9, 2, 117-122.
West, M.A., & Poulton, B.C. (1995). Primary health care teams: Rhetoric versusreality. Paper submitted for publication. Institute of Work Psychology, University ofSheffield.
West, M.A. & Slater,J.A. (1996). The Effectiveness of Team Working in PrimaryHealth Care. London:Health Education Authority.
West, M.A. & Wallace, M. (1991). Innovation in health care teams. European Journalof Social Psychology. Vol 21, 303 – 315.
West, M.A. & Pillinger, T. (1995). Innovation in UK manufacturing (Research report).Institute of Work Psychology, University of Sheffield.
Wood, N., Farrow, S., & Elliott, B. (1994). A review of primary health careorganisation. Journal of Clinical Nursing, 3(4), 243-250.

Worchell, S., Wood, W. & Simpson, J.A. (eds) (1992). Group Processes andProductivity. Newbury Park, CA: Sage.
Yeatts, D.E. & Seward, R.R. (2000). Reducing turnover and improving health care innursing homes: The potential effects of self-managed work teams. The Gerontologist,40 (3),358-363.
Zimmer, J.G., Eggert, G.M. & Chiverton, P. (1990). Individual versus team casemanagement in optimising care for chronically ill patients with dementia. Journal ofAging and Health, 2 (3), 357-372.