Embed Size (px)
Citation preview

THERAPEUTICSTRATEGIES
DRUG DISCOVERY
TODAY
Drug Discovery Today: Therapeutic Strategies Vol. 3, No. 3 2006
Editors-in-Chief
Raymond Baker – formerly University of Southampton, UK and Merck Sharp & Dohme, UK
Eliot Ohlstein – GlaxoSmithKline, USA
Respiratory diseases
The effective treatment of COPD:Anticholinergics and what else?Mario Cazzola1,*, Maria Gabriella Matera2
1University of Rome Tor Vergata, Department of Internal Medicine, Unit of Respiratory Diseases, Via Montpellier 1, 00133 Rome, Italy2Second University of Naples, Department of Experimental Medicine Unit of Pharmacology and Toxicology, Piazza Miraglia 4, 80123 Naples, Italy
Long-acting bronchodilator therapy should be consid-
ered when a COPD patient is symptomatic. For patients
whose conditions are not sufficiently controlled by
monotherapy, combining medications of different
classes seems a convenient treatment for obtaining
better results. The current opinion is that it is advanta-
geous to develop inhalers containing several classes of
long-acting bronchodilator drugs in an attempt to sim-
plify treatment regimes as much as possible and to serve
as a basis for improved ‘triple therapy’ combinations
through co-formulation with novel anti-inflammatory
compounds, such as inhaled PDE4 inhibitors, that could
deliver three complementary therapeutic effects.
*Corresponding author: M. Cazzola ([email protected])
1740-6773/$ � 2006 Elsevier Ltd. All rights reserved. DOI: 10.1016/j.ddstr.2006.09.009
Section Editors:Roy Goldie – Faculty of Health Sciences, Flinders University,Adelaide, AustraliaPeter Henry – School of Medicine & Phamacology, TheUniversity of Western Australia, Nedlands, Australia
Introduction
National and international guidelines [1–4] suggest that long-
acting bronchodilator therapy should always be considered
when patients with COPD are symptomatic, but no distinction
is made as to which class of drugs should be considered first,
althoughanticholinergics agents areofnoteworthyvalue since
parasympathetic cholinergic pathways arising from the vagus
nerveare implicated in the pathophysiology ofairflowobstruc-
tion in COPD [4–6]. In effect, a systematic review with meta-
analysis of current evidence about the effectiveness of tiotro-
pium bromide compared with placebo, ipratropium bromide
or long-acting b2-adrenoceptor (AR) agonists [LABAs], for the
treatment of stable COPD patients [7] has documented that
increases in FEV1 and FVC from baseline were significantly
larger with tiotropium than with placebo, ipratropium and
LABAs. Also, tiotropium reduced COPD-related exacerbations
and hospital admissions compared with placebo and led to
30% reduction in COPD-related admissions compared with
LABAs. Moreover, Adams et al. [8] have recently observed that
tiotropium provided significant improvement in lung func-
tion, health status and dyspnea when used as maintenance
treatment in undertreated COPD patients who were not
previously receiving maintenance bronchodilator therapy.
For patients whose conditions are not sufficiently con-
trolled by monotherapy, combining medications of different
classes, in particular an inhaled anticholinergic with a b2-AR
agonist, seems a convenient way of delivering treatment and
obtaining better results [1–3]. This includes better lung func-
tion and improved symptoms. Specifically, as airflow obstruc-
tion becomes more severe, both a long-acting anticholinergic
plus a long-acting b2-agonist are advocated, although data
supporting this therapeutic approach are still scarce [9].
The aim of this article is to illustrate newer and potential
options that could be considered when monotherapy appears
to be ineffective.
Pharmacological rationale for combining b2-agonists
and anticholinergic agents
Postganglionic, parasympathetic-cholinergic nerves inner-
vate the airways. When activated, these nerves are capable
277

Drug Discovery Today: Therapeutic Strategies | Respiratory diseases Vol. 3, No. 3 2006
of obliterating the lumen of small bronchi and bronchioles,
and markedly increasing airway resistance in larger, cartilagi-
nous airways, by secretion of the bronchoconstricting media-
tor acetylcholine (ACh), which causes activation of muscarinic
receptors at the level of the target cells, such as bronchial
smooth muscle and goblet cells [9]. Conversely, sympathetic
nerves may control tracheobronchial blood vessels, but no
innervation ofhuman airway smoothmuscle has been demon-
strated. b2-ARs, however, are abundantly expressed on human
airway smooth muscle and activation of these receptors causes
its relaxation [9].
Bronchodilation may be obtained either by stimulating the
b2-ARs with b2-AR agonists, or by inhibiting the action of
ACh at muscarinic receptors with anticholinergic agents. In
any case, anticholinergics are more likely to decrease central
airway resistance, although there are muscarinic receptors
that are expressed in the smooth muscle of small airways,
which do not appear to be innervated by cholinergic nerves,
and b2-AR agonists have a greater effect on peripheral airway
resistance in patients with COPD [9]. It is reasonable to
postulate that attempts to reduce bronchoconstriction
through two distinct mechanisms (anticholinergic and sym-
pathomimetic) with a different prevalent site of action may
maximize bronchodilator response [9].
Interestingly, the presence of small dense-cored vesicles
containing adrenergic nerve varicosities, occasionally in close
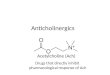
Figure 1. Schematic presentation of the potential alternative role of b2-adren
parasympathetic nerve endings. Bronchodilation may be obtained either by stim
airway smooth muscle, with b2-adrenoceptor agonists, or by inhibiting the actio
with anticholinergic agents. A prejunctional b2-adrenoceptor is present on cho
that its activation can increase acetylcholine release in a concentration-depend
b2-ARs inhibits cholinergic neurotransmission, Abbreviations: A, circulating adr
muscarinic M1 or M3 receptors; , neuronal activity; !, stimulatory effect; ,
278 www.drugdiscoverytoday.com
proximity to morphologically characteristic cholinergic
nerve-endings, has been identified in human airways, sug-
gesting that catecholamines might modulate cholinergic
neurotransmission (Fig. 1) [9]. However, different studies
have led to dissimilar conclusions. Early research papers
based on force measurement alone suggested that stimula-
tion of b2-ARs inhibits cholinergic neurotransmission, most
probably by the release of inhibitory prostaglandins from the
airway mucosa [9]. However, interpretation of these data is
seriously hampered by the large postjunctional effects of
b2-AR agonists. On the contrary, other studies have docu-
mented that activation of b2-ARs can increase ACh release in
a concentration-dependent manner [9]. Whatever the type of
interaction between the two systems may be, combining b2-
AR agonists and anticholinergic agents is pharmacologically
useful. In fact, in the first case, the addition of a b2-AR agonist
decreases the release of ACh because of the modulation of
cholinergic neurotransmission by prejunctional b2-AR and,
consequently, amplifies the bronchial smooth muscle relaxa-
tion directly induced by the anticholinergic agent. On the
contrary, in the second circumstance, the addition of an
anticholinergic agent can reduce the peripheral bronchocon-
strictor effects of ACh, whose release has been facilitated by
the b2-AR agonist, and in this manner can amplify the
bronchodilation elicited by the b2-AR agonist through the
direct stimulation of smooth muscle b2-ARs.
oceptor in the pre-synaptic control of acetylcholine release from airway
ulating the b2-adrenoceptors, which are abundantly expressed on
n of acetylcholine at muscarinic receptors on bronchial smooth muscle
linergic nerves in airways smooth muscle. It has been documented
ent manner, but some papers have suggested that stimulation of
enaline; ACh, acetylcholine; b2-AR, b2-adrenoceptor; M1 and M3,
inhibitory effect.

Vol. 3, No. 3 2006 Drug Discovery Today: Therapeutic Strategies | Respiratory diseases
Evidence from clinical studies showing benefits of
LABA and tiotropium combination therapy in COPD
Considering that formoterol provides a greater degree of early
bronchodilation (in the first 2 h) than tiotropium and
comparable bronchodilation over 12 h [10], the possibility
of combining these two agents was examined in stable COPD
patients. Formoterol 12 mg and tiotropium 18 mg appeared
complementary not only after their acute administration
[11], but also after a regular treatment [12,13]. In fact
tiotropium ensured prolonged bronchodilation; formoterol
added fast onset and greater peak effect. In particular, van
Noord et al. [12] documented that 6 weeks of treatment with
tiotropium 18 mg + formoterol 12 mg once daily (od) in the
morning in patients suffering from moderate-to-severe COPD
had a greater bronchodilator effect compared with individual
agents (tiotropium 18 mg od in morning, formoterol 12 mg
bid), over 24 h (with the greatest differences during the first
12 h) and was significantly better for daytime (but not night-
time) rescue salbutamol use. In any case, the numerical
differences suggested that patients would have benefited
from an evening dose of formoterol. In effects, the results
of 2-week treatments with tiotropium alone or tiotropium
plus formoterol once or twice daily following a 2-week
pretreatment period with tiotropium, have documented that,
although the investigators appear to favour the od combina-
tion in their discussion, the evening dose of formoterol added
clear benefit [13].
Interestingly, the additive effect of a second long-acting
bronchodilator in patients receiving a first long-acting
bronchodilator does not depend on which type of broncho-
dilator is given first [14].
Also the combination of tiotropium 18 mg + salmeterol
50 mg had a greater bronchodilator effect compared with
individual agents, but results excluded the once-daily co-
administration of the two drugs [15]. It was also observed
that the onset of action of the two drugs was faster when they
were combined. This effect is worthy of attention because
both agents elicit a slow onset of action.
It has also been documented that for patients suffering
from a mild-to-moderate acute exacerbation of COPD, com-
bination therapy with formoterol and tiotropium provides
faster and greater peak and overall bronchodilation, with
improved oxygen saturation [16]. In this study, both single
agents had a shorter duration than expected, perhaps because
of increased airways inflammation during an exacerbation –
however, the combination improved FEV1 for 24 h.
Anti-inflammatory approaches in COPD
Unfortunately, COPD is a multicomponent disease with
inflammation and the development of extensive tissue remo-
delling during the course of the disease process at its core, in
which patients experience progressively worsening lung
function, disease symptoms and quality of life (QoL), as well
as increasing exacerbations [4]. Bronchodilators improve the
airflow limitation by only producing airway smooth-muscle
relaxation. Therefore, there is an absolute need to also target
other components of the disease, mainly inflammation.
Corticosteroids are highly effective as an anti-inflamma-
tory treatment in asthma, but in COPD their role is contro-
versial, as the inflammatory phenotype differs from that seen
in asthma [17] and, moreover, COPD has been reported to
respond less favourably in the short term to inhaled corti-
costeroids (ICS) [18]. Nonetheless, regular treatment with ICS
is recommended for symptomatic patients who suffer from
frequent exacerbations, and whose FEV1 is<50% of predicted
[4]. This recommendation is also supported by the observa-
tion that in a pooled analysis of seven randomised studies
involving 5085 patients, ICSs reduced all-cause mortality by
about 25% relative to placebo in patients with stable COPD
[19].
In any case, in severe COPD patients, combinations of ICS
and LABA show an additive effect, suggesting an interaction
between the two moieties that can have a positive effect and
bring to significant improvement of important clinical out-
comes [20]. In effect, LABA + ICS therapy causes a rapid
improvement in lung function, which is sustained for at least
12 months. In addition, greater improvements in cough and
breathlessness are seen with combination treatment, com-
pared to monotherapy with the individual agents alone.
Importantly, the number and severity of exacerbations
experienced by patients is reduced by LABA + ICS combina-
tion therapy, compared with monotherapy, in severe COPD
[21]. However, in patients with mild to moderate COPD, no
additional benefit of LABA + ICS combination therapy has
been shown thus far [23]. Moreover, there are concerns about
the increased risk of side effects and cost of using LABA + ICS
therapy in COPD [22].
Recently, it has been suggested to use antioxidants, iNOS
inhibitors and theophylline for increasing histone deacety-
lase (HDAC) activity because of the reduction in HDAC
activity, owing to a selective reduction in HDAC-2 expres-
sion as a consequence of the increased oxidative and nitra-
tive stress in lungs of smokers, which may account for the
increased pulmonary inflammation and resistance to corti-
costeroids [23]. Nonetheless, this proposal seems to be more
theoretic than practical. In fact, it was documented that both
salmeterol + fluticasone propionate and theophylline + flu-
ticasone propionate combination significantly improved
FEV1, with no difference between the two therapeutic
regimes, and, in addition, fluticasone propionate in combi-
nation with salmeterol was more effective in reducing dys-
pnea and use of salbutamol as rescue medication after 4
months of treatment [24]. Furthermore, the results of the
BRONCUS study suggested that the exacerbation rate might
be reduced with N-acetylcysteine only in patients not treated
with ICS [25].
www.drugdiscoverytoday.com 279

Dru
gD
isco
very
To
day:
Th
era
peu
ticS
trate
gie
s|
Resp
irato
ryd
isease
sV
ol.
3,
No
.3
2006
Table 1. Ultra long-acting b-agonists under development
Pros Cons Latest developments Who is working on this strategy Refs
Arformoterol It has a longer duration of action than currently
marketed LABAsa
It is unlikely that the drug will be approved as a
once-daily dosing regime
A new drug application
submitted to the U.S.
Food and Drug
Administration
Sepracor (http://www.sepracor.com/) [27]
The potential association between LABA and rare,
but potentially serious, respiratory adverse events
Indacaterol It offers a quick onset of action and true
24-hour control.
The potential association between LABA and rare,
but potentially serious, respiratory adverse events
Phase III Novartis (http://www.novartis.com/) [27]
It behaves as a potent b2-ARb agonist with
high intrinsic efficacy that, in contrast to salmeterol,
does not antagonize the bronchorelaxant effect
of a short-acting b2-AR agonist.
Carmoterol It displays a fast onset and long
duration (30 h) of activity.
The potential association between LABA and rare,
but potentially serious, respiratory adverse events
Phase III Chiesi (http://www.chiesigroup.com/2006/) [27]
GSK159797 It produces clinically significant increases
in FEV1c through 24 hours, with little
change in heart rate.
The potential association between LABA and rare,
but potentially serious, respiratory adverse events
Phase IIb Theravance (http://www.theravance.com/)/
GlaxoSmithKline (http://www.gsk.com/)
[27]
GSK159802 Detailed status not disclosed The potential association between LABA and rare,
but potentially serious, respiratory adverse events
Phase II GlaxoSmithKline (http://www.gsk.com/)
GSK597901 Detailed status not disclosed The potential association between LABA and rare,
but potentially serious, respiratory adverse events
Phase II GlaxoSmithKline (http://www.gsk.com/) [27]
GSK642444 Detailed status not disclosed The potential association between LABA and rare,
but potentially serious, respiratory adverse events
Phase IIa GlaxoSmithKline (http://www.gsk.com/) [27]
GSK678007 Detailed status not disclosed The potential association between LABA and rare,
but potentially serious, respiratory adverse events
Phase II GlaxoSmithKline (http://www.gsk.com/) [27]
a Long-acting b-agonist.b b2-Adrenoceptor.c Forced expiratory volume in one second.
280
ww
w.d
rugd
iscoveryto
day.co
m

Vol. 3, No. 3 2006 Drug Discovery Today: Therapeutic Strategies | Respiratory diseases
Future directions
Regrettably, the existing therapy of COPD is far from ideal
because no currently available agent has been shown to slow
the relentless progression of this disease but, with a better
understanding of the inflammatory and destructive process,
several targets have been identified and new treatments are in
development. We do not know, however, if all these new
therapies will reach the market because the therapeutic ratio-
nale behind many of these treatments is mainly speculative
and, moreover, they are fraught with important safety issues
[26].
In any case, there is a pressing need to develop new treat-
ments for this disease. The current opinion is that it will be
advantageous to develop inhalers containing several classes
of long-acting bronchodilator drugs in an attempt to simplify
treatment regimes as much as possible. A once daily inhaler
with a once daily b2-AR agonist and anticholinergic as well as
a once daily inhaler with a once daily b2-AR agonist and a
once daily ICS would, therefore, be ideal.
New bronchodilators
Once-daily b2-AR agonists such as carmoterol, indacaterol,
GSK-159797, GSK-597901, GSK-159802, GSK-642444 and
GSK-678007 are under development for the treatment of
COPD [27] (Table 1), despite the recent FDA public health
advisory that has highlighted the concerns raised by the
SMART study [28]. The majority of these compounds are
(R,R)-isomers to control desensitisation and accumulation.
It is likely that once-daily dosing of an ultra LABA will lead to
increased convenience for the patients, which may also lead
Table 2. Long-acting antimuscarinic agents under development
Pros Cons
NVA237 At doses showing similar efficacy,
NVA237 demonstrated a significantly
lower effect on cardiovascular
parameters than tiotropium.
OrM3 It has been formulated as an oral
tablet, a potentially more convenient
formulation, particularly for less
compliant patients and those who
have difficulty using aerosol therapy.
At a dose that provided effi
less than that of ipratropium
the incidence of dose-relat
mechanism-based side effec
OrM3 exceeded those obs
for ipratropium.
GSK656398 Detailed status not disclosed. Detailed status not disclos
GSK233705 Its long duration of action when
administered via inhalation in
animal models supports the
potential for use as a once-daily
bronchodilator for COPD.
Detailed status not disclos
LAS 34273 Detailed status not disclosed. Detailed status not disclos
LAS 35201 Detailed status not disclosed. Detailed status not disclos
to enhancement of compliance, and may have advantages
leading to improved overall clinical outcomes in patients
with COPD. In any case, the results of a recent study that
has evaluated the bronchodilating activity of the ultra LABA
carmoterol and the muscarinic M3-antagonist tiotropium,
given intratracheally alone or in combination in anaesthe-
tized artificially ventilated normal and actively sensitized
guinea-pigs, provide a clear evidence of a positive interaction
between these two bronchodilators in controlling the
bronchoconstriction elicited by different challenges, anaphy-
lactic reaction included [29]. In particular, in the presence of
doses of tiotropium ineffective per se, the ED50 values of
carmoterol were significantly reduced by 5 to over 30 times,
depending on the challenge.
Also some new long-acting antimuscarinic agents (LAMAs)
such as LAS-34273, LAS-35201, GSK656398 (formerly known
as TD-5742), GSK233705, NVA-237 (glycopyrrolate) and OrM3
are under development (Table 2). In particular, it has been
documented in an experimental setting that at doses showing
similar efficacy, NVA237 demonstrated a significantly lower
effect on cardiovascular parameters than tiotropium, which
may indicate a potential clinical benefit in man [30]. In effect,
inhaled NVA237 has low systemic absorption, and therefore
should not be expected to be associated with typical systemic
antimuscarinic adverse effects. This is supported by the
observed lack of dry mouth (a classic antimuscarinic adverse
effect) with inhaled NVA237, and suggests a favourable safety
profile for this once-daily antimuscarinic bronchodilator [31].
Single doses of NVA237 480 mg demonstrated bronchodilatory
efficacy up to 32 h post-dose in patients with reversible
Latest
developments
Who is working on this strategy Refs
Phase IIb Vectura (www.vectura.com)/Novartis
(http://www.novartis.com/)
[30–33]
cacy
,
ed,
ts for
erved
Phase IIb Merck Research Laboratories
(http://www.merck.com/mrl/)
[34]
ed. Phase I Theravance (www.theravance.com)/
GlaxoSmithKline (http://www.gsk.com/)
ed. Phase II GlaxoSmithKline (http://www.gsk.com/)
ed. Phase II/III Almirall (http://www.almirall.es/)
ed. Phase I/II Almirall (http://www.almirall.es/)
www.drugdiscoverytoday.com 281

Drug Discovery Today: Therapeutic Strategies | Respiratory diseases Vol. 3, No. 3 2006
Table 3. Combination of LABAa + LAMAb under development
Pros Cons Latest
developments
Who is working on this strategy Refs
Formoterol +
tiotropium
The combination of a LABA with
tiotropium is superior to either
single agent alone
Once-daily
administration is
not really possible.
Development of
unit dose oral
inhalation products
for nebulization
Novartis (http://www.novartis.com/),
Boehringer-Ingelheim
(http://www.boehringer-ingelheim.com/),
Dey (http://www.dey.com/)
[11–14,16]
Salmeterol +
tiotropium
The combination of a LABA with
tiotropium is superior to either
single agent alone
Once-daily
administration is
not really possible.
Phase III Boehringer-Ingelheim
(http://www.boehringer-ingelheim.com/),
GlaxoSmithKline (http://www.gsk.com/)
[15]
Carmoterol +
tiotropium
In the presence of doses of
tiotropium ineffective per se,
the ED50c values of
carmoterol were significantly
reduced by 5 to over 30 times,
depending on the challenge.
Human data are
still lacking.
Preclinical phase. Chiesi (http://www.chiesigroup.com/2006/) [29]
Indacaterol +
NVA237
(QVA149)
Detailed status not disclosed Detailed status
not disclosed.
In preparation
for Phase II.
Novartis (http://www.novartis.com/)
GSK159797 +
GSK233705
Detailed status not disclosed. Detailed status
not disclosed.
Preclinical phase. Theravance (http://www.theravance.com/)/
GlaxoSmithKline (http://www.gsk.com/)
GSK-961081 It is both a muscarinic
antagonist and a b2-ARd agonist.
Detailed status
not disclosed.
Phase I GlaxoSmithKline (http://www.gsk.com/)
a Long-acting b-agonist.b Long-acting antimuscarinic agent.c Effective dose 50%.d b2-Adrenoceptor.
obstructive airways disease, supporting the potential for once-
daily dosing, and exhibited a rapid onset of action [32]. In
particular, single doses of NVA237 provided a similar degree of
bronchodilation to the short-acting b2-agonist salbutamol
over the first 40 min post-dose [33]. OrM3 is a 4-acetamidopi-
peridine derivative with a high degree of selectivity (120-fold)
for the M3 receptor over M2 receptors [34]. It has been for-
mulated as an oral tablet, a potentially more convenient for-
mulation, particularly for less compliant patients and those
who have difficulty using aerosol therapy. Dosed orally, phar-
macokinetic data demonstrated that OrM3 has a long half-life
(t1/2 = 14.20 h), which would potentially allow for a once-
daily dosing regimen. In effect, OrM3 demonstrated a signifi-
cant dose-related improvement in serial FEV1 and a trend for
Table 4. Combination therapy with an ICS and an ultra LABA
Pros Cons
Carmoterol + budesonide It is two-fold more effective
than the formoterol/
budesonide combination.
Detailed status
not disclosed.
Indacaterol + QAE397 Detailed status not disclosed. Detailed status
not disclosed.
Indacaterol + mometasone Detailed status not disclosed. Detailed status
not disclosed.
GSK159797 + GSK685698 Detailed status not disclosed. Detailed status
not disclosed.
282 www.drugdiscoverytoday.com
dose-related improvement in patient-reported symptoms
compared with placebo [34]. However, at a dosage that pro-
vided efficacy less than that of ipratropium, the incidence of
dose-related, mechanism-based side effects for OrM3 exceeded
those observed for ipratropium [34].
Bronchodilators are still central in the symptomatic man-
agement of COPD [1]. For this reason, the current opinion is
that it will be advantageous to develop inhalers containing
combination of several classes of long-acting bronchodilator
drugs in an attempt to simplify treatment regimes as much as
possible. Consequently, several options for once-daily dual-
action ultra LABA + LAMA combination products are cur-
rently being evaluated (Table 3). Because combination ther-
apy with an ICS and a LABA is now considered a therapeutic
under development
Latest developments Who is working on this strategy Refs
Preclinical phase Chiesi
(http://www.chiesigroup.com/2006/)
Novartis (http://www.novartis.com/)
Novartis (http://www.novartis.com/)/
Schering-Plough
(http://www.schering-plough.com/)
GlaxoSmithKline (http://www.gsk.com/)

Vol. 3, No. 3 2006 Drug Discovery Today: Therapeutic Strategies | Respiratory diseases
option for treating patients suffering from severe to very-
severe COPD, there is a factual interest in developing a once-
daily combination therapy, again in an attempt to simplify
the treatment, and also to overcome the loss of patent pro-
tection (Table 4). The awareness that new ICS such as cicle-
sonide or GSK685698 (Table 4), which can be used as a once-
daily dosing, have been developed or are in development
have further supported the development of new ultra-LABAs
that can be used on a once-a-day basis.
New anti-inflammatory agents
Theophylline has been relegated to a second- or even third-
line therapy in the treatment of COPD, behind corticoster-
oids and b2-agonists, although it possesses anti-inflammatory
and immunomodulatory effects in addition to its well-recog-
nized effects as a bronchodilator [35]. In part, theophylline
has fallen out of favour because of its adverse side-effect
profile, and this has led to the search for more effective
and safer drugs based on the knowledge that theophylline
is orally active and that it is a nonselective phosphodiesterase
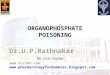
Figure 2. PDE4 Inhibitors in COPD. In contrast to asthma, the key inflammator
cells. These cells release the reactive oxygen species, chemokines, cytokines and p
The ongoing inflammatory processes lead to enlargement of the alveolar spaces
obstruction. Airway hyperresponsiveness is not a feature of COPD. Epithelial met
inhibitors can target the inflammatory processes. Abbreviations. AHR, Airway Hyp
mediates cellular adherence; GM-CSF, Granulocyte/Macrophage Colony Stimula
Interferon; LTB4, Leukotriene B4; LTC4, Leukotriene C4; MIP-1a, Macrophage
Prostaglandin D2; RANTES, Regulated on Activation Normal T Cell Expressed
Factor-a; VCAM1, Vascular Cell Adhesion Molecule 1.
(PDE) inhibitor. In view of the fact that PDE4 isoenzyme is the
predominant isoenzyme in the majority of inflammatory
cells, including neutrophils, which are implicated in the
pathogenesis of COPD [35] (Fig. 2), selective PDE4 inhibitors
have been developed or are under development for the
treatment of COPD [35] (Table 5).
Roflumilast and cilomilast are currently the most advanced
PDE4 inhibitors undergoing clinical trials for COPD. In a large
placebo-controlled trial, roflumilast 500 mg once daily pro-
duced a significant improvement in postbronchodilator
FEV1, and reduced exacerbations by 34% over placebo [36].
Roflumilast was safe and well tolerated, although the class-
associated side effects of diarrhoea, nausea, and headache
were still apparent [36]. Also cilomilast 15 mg twice daily
resulted in an improvement in FEV1 compared with placebo.
There was also a clinically significant improvement in the St
George’s respiratory questionnaire score and a greater per-
centage of exacerbation-free weeks in cilomilast-treated
patients [37]. These data demonstrate that PDE4 inhibitors
can improve clinical symptoms in patients with COPD,
y cells involved in COPD include: neutrophils, macrophages and CD8+ T
roteases that are instrumental in producing a chronic inflammatory state.
, destruction of the lung parenchyma, loss of elasticity and small airways
aplasia and mucus hypersecretion are prominent features of COPD. PDE4
erresponsiveness; CD11b, subunit of receptor on human neutrophils that
ting Factor; IL-2, -4, -5, -8, -10, -13, Interleukin-2, -4, -5, -8, -10, -13; IFN,
inflammatory protein 1a; PAF, Platelet Activating Factor; PGD2,
and Secreted; ROS, Reactive Oxygen Species; TNF-a, Tumor Necrosis
www.drugdiscoverytoday.com 283

Dru
gD
isco
very
To
day:
Th
era
peu
ticS
trate
gie
s|
Resp
irato
ryd
isease
sV
ol.
3,
No
.3
2006
Table 5. Antiinflammatory therapies under development
Pros Cons Latest developments Who is working on this strategy Refs
Inhaled corticosteroids
Ciclesonide (Alvesco) It can be used as a once-daily dosing. It passes through the airways tissues
too fast and splits too fast in the
airways and in the body to have a
significant impact on effect duration
and airway selectivity of its active
metabolite.
It has been approved in
37 countries and is now
available in 18 countries
Altana (http://www.altanapharma.com/)
It is inactive until it reaches the lungs,
where it is converted to its active metabolite
desisobutyryl-ciclesonide.
Other favourable pharmacokinetic and
pharmacodynamic characteristics such as high
protein binding, low oral bioavailability and
rapid clearance contribute to its efficacy and
improved systemic safety profile.
Fluticasone furoate
(GSK685698,
Avamys/Allermist)
It can be used as a once-daily dosing. Allergic rhinitis is its main indication. Phase III GlaxoSmithKline (http://www.gsk.com/)
GSK799943 Detailed status not disclosed Detailed status not disclosed Phase II GlaxoSmithKline (http://www.gsk.com/)
GSK870086 Detailed status not disclosed Detailed status not disclosed Phase I GlaxoSmithKline (http://www.gsk.com/)
Etiprednol
dicloacetate (BNP-166)
It is rapidly converted to an inactive form
after absorption, which reduces the
likelihood of side effects.
Detailed status not disclosed Phase II IVAX Corporation (http://www.ivax.com/)
QAE397 Detailed status not disclosed Detailed status not disclosed Phase I Novartis (http://www.novartis.com/)
PDE4a inhibitors
Roflumilast (Daxas) It is the most advanced PDE4 inhibitors
undergoing clinical trials for airways disease.
At least in asthmatic patients there are
early dose-limiting adverse events with
the 500 mg dose that abate with
longer-term treatment.
Phase III Altana (http://www.altanapharma.com/) [35,36,
38,39]
Cilomilast (Ariflo) It significantly improves lung function
and quality of life to a clinically meaningful
extent.
The results of Phase III studies
are unremarkable and disappointing,
raising doubt over the future of
cilomilast as a novel therapy for COPD.
Phase III GlaxoSmithKline (http://www.gsk.com/) [37]
Arofylline Detailed status not disclosed Detailed status not disclosed Phase II/III: Almirall (http://www.almirall.es/)
AWD12-281 It causes no side effects in animal
models in opposite to other PDE4 inhibitor.
Detailed status not disclosed Phase II Elbion AG (http://www.elbion.de/) [35]
GRC-3886 Detailed status not disclosed Detailed status not disclosed Phase I Glenmark Pharmaceuticals Ltd
(http://www.glenmarkpharma.com/)
[35]
HT0712 Detailed status not disclosed Detailed status not disclosed Phase I Inflazyme Pharmaceuticals Ltd
(http://www.inflazyme.com/)
[35]
a Phosphodiesterase4.
284
ww
w.d
rugd
iscoveryto
day.co
m

Vol. 3, No. 3 2006 Drug Discovery Today: Therapeutic Strategies | Respiratory diseases
although unlike theophylline, they have no direct broncho-
dilator activity and are therefore likely to be having a differ-
ent mechanism of action [35]. Interestingly, a significant
reduction in the amount-number of neutrophils and eosino-
phils in sputum of patients with COPD has been observed
after 4 weeks of treatment with roflumilast 500 mg once daily
[38], thus adding clinical evidence to the wide range of anti-
inflammatory effects observed in preclinical studies. In addi-
tion, in a murine model roflumilast has also been shown to
prevent the development of cigarette smoke–induced
emphysema, suggesting that it could be used as a protective
therapy in smokers to prevent deterioration of their lung
function, although this has yet to be explored clinically [39].
Conclusion
Although smoking cessation strategies are important for
reducing the incidence of COPD in the longer term, there
is clearly a need for more effective therapies for patients who
already have the disease. The investigational therapies for
COPD discussed above have shown promising results. It is
likely that the development of once-daily dual-action ultra
LABA + LAMA combination products may serve as a basis for
improved ‘triple therapy’ combinations through co-formula-
tion with novel anti-inflammatory compounds such as
inhaled PDE4 inhibitors, that could deliver three comple-
mentary therapeutic effects for patients with COPD. In any
case, the development of once-daily dual-action ultra
LABA + LAMA combination products may serve also as a
basis for improved ‘triple therapy’ combinations through
co-formulation with novel ICS. The potential for these
therapeutic strategies to be administered once daily simplifies
patient treatment regimens and therefore increases the
likelihood of compliance with therapy.
References1 Celli, B.R. and MacNee, W. (2004) ATS/ERS task force. Standards for the
diagnosis and treatment of patients with COPD: a summary of the ATS/ERS
position paper. Eur. Respir. J. 23, 932–946
2 Chronic obstructive pulmonary disease. National clinical guideline on
management of chronic obstructive pulmonary disease in adults in
primary and secondary care. Thorax 59 (Suppl. 1) 1–232
3 Global Initiative for Chronic Obstructive Lung Disease. (2005) Global
strategy for the diagnosis, management, and prevention of chronic
obstructive pulmonary disease – 2005 update. Available at:
http://www.goldcopd.com/ (accessed July 7, 2006).
4 Barnes, P.J. (2004) The role of anticholinergics in chronic obstructive
pulmonary disease. Am. J. Med. 117 (Suppl. 12A), 24S–32S
5 Cazzola, M. and Matera, M.G. (2004) Long-acting bronchodilators
are the first-choice option for the treatment of stable COPD. Chest 125,
9–11
6 Rodrigo, G.J. and Nannini, L.J. (2006) Tiotropium for the treatment of
stable chronic obstructive pulmonary disease: A systematic review with
meta-analysis. Pulm. Pharmacol. Ther. 10.1016/j.pupt.2006.02.003 (Epub
ahead of print)
7 Currie, G.P. et al. (2006) Effects of tiotropium and other long acting
bronchodilators in chronic obstructive pulmonary disease. Pulm.
Pharmacol. Ther. 19, 112–119
8 Adams, S.G. et al. (2006) Tiotropium in COPD patients not previously
receiving maintenance respiratory medications. Respir. Med. 10.1016/
j.rmed.2006.03.034 (Epub ahead of print)
9 Belvisi, M.G. et al. (1996) Paradoxical facilitation of acetylcholine release
from parasympathetic nerves innervating guinea-pig trachea by
isoprenaline. Br. J. Pharmacol. 117, 1413–1420
10 Richter, K. et al. (2006) Onset and duration of action of formoterol and
tiotropium in patients with moderate to severe COPD. Respiration 73,
414–419
11 Cazzola, M. et al. (2004) The pharmacodynamic effects of single inhaled
doses of formoterol, tiotropium and their combination in patients with
COPD. Pulm. Pharmacol. Ther. 17, 35–39
12 van Noord, J.A. et al. (2005) Comparison of tiotropium once daily,
formoterol twice daily and both combined once daily in patients with
COPD. Eur. Respir. J. 26, 214–222
13 van Noord, J.A. et al. (2006) Effects of tiotropium with and without
formoterol on airflow obstruction and resting hyperinflation in patients
with COPD. Chest 129, 509–517
14 Cazzola, M. et al. (2005) Bronchodilator response to formoterol after
regular tiotropium or to tiotropium after regular formoterol in COPD
patients. Respir. Med. 99, 524–528
15 Cazzola, M. et al. (2004) The functional impact of adding salmeterol and
tiotropium in patients with stable COPD. Respir. Med. 98, 1214–1221
16 Di Marco, F. et al. (2006) Effect of formoterol, tiotropium, and their
combination in patients with acute exacerbation of chronic obstructive
pulmonary disease: a pilot study. Respir. Med. 10.1016/j.rmed.2005.10.008
(Epub ahead of print)
17 Barnes, P.J. (2000) Chronic obstructive pulmonary disease. N. Engl. J. Med.
343, 269–280
18 Culpitt, S.V. et al. (1999) Effect of high dose inhaled steroid on cells,
cytokines, and proteases in induced sputum in chronic obstructive
pulmonary disease. Am. J. Respir. Crit. Care Med. 160, 1635–1639
19 Sin, D.D. et al. (2005) Inhaled corticosteroids and mortality in chronic
obstructive pulmonary disease. Thorax 60, 992–997
20 Cazzola, M. and Dahl, R. (2004) Inhaled combination therapy with long-
acting b2-agonists and corticosteroids in stable COPD. Chest 126, 220–237
21 Cazzola, M., and Hanania, H.A. (2006) The role of combination therapy
with corticosteroids and long-acting b2-agonists in the prevention of
exacerbations in COPD. Intern. J. COPD (in press).
22 van Schayck, C.P. and Reid, J. (2006) Effective management of COPD in
primary care – the role of long-acting beta agonist/inhaled corticosteroid
combination therapy. Prim. Care Respir. J. 15, 143–151
23 Barnes, P.J. (2006) Reduced histone deacetylase in COPD: clinical
implications. Chest 129, 151–155
24 Cazzola, M. et al. (2004) Salmeterol/fluticasone propionate in a single
inhaler device versus theophylline + fluticasone propionate in patients
with COPD. Pulm. Pharmacol. Ther. 17, 141–145
25 Decramer, M. et al. (2005) Effects of N-acetylcysteine on outcomes in
chronic obstructive pulmonary disease (Bronchitis Randomized on NAC
Cost-Utility Study, BRONCUS): a randomised placebo-controlled trial.
Lancet 365, 1552–1560
26 Matera, M.G. and Cazzola, M. (2004) New anti-inflammatory approaches
in COPD. Drug. Discov. Today: Ther. Strat. 1, 335–343
27 Cazzola, M. et al. (2005) Ultra long-acting b2-agonists in development for
asthma and chronic obstructive pulmonary disease. Expert Opin. Investig.
Drugs 14, 775–783
28 FDA Public Health Advisory. (2006) Serevent Diskus (salmeterol xinafoate
inhalation powder), Advair Diskus (fluticasone propionate & salmeterol
inhalation powder), Foradil Aerolizer (formoterol fumarate inhalation
powder). http://www.fda.gov/cder/drug/advisory/LABA.htm (accessed
May 28, 2006)
29 Rossoni, G. et al. (2006) Positive interaction of the novel b2-agonist
carmoterol and tiotropium bromide in the control of airway changes
induced by different challenges in guinea-pigs. Pulm. Pharmacol. Ther.
10.1016/j.pupt.2006.01.004 (Epub ahead of print)
30 Cooper, N. et al. (2006) NVA237 and tiotropium bromide demonstrate
similar efficacy in an anesthetized rabbit model of methacholine-induced
bronchoconstriction. NVA237 demonstrates a reduced systemic
www.drugdiscoverytoday.com 285

Drug Discovery Today: Therapeutic Strategies | Respiratory diseases Vol. 3, No. 3 2006
pharmacological effect on cardiovascular parameters. Proc. Am. Thor. Soc. 3,
A117 (Abstract)
31 Thomas, R. et al. (2006) Low systemic exposure of NVA237, an inhaled
once-daily antimuscarinic bronchodilator, in healthy human volunteers.
Proc. Am. Thor. Soc. 3, A725 (Abstract)
32 Gunawardena, K.A. et al. (2006) NVA237, a once-daily antimuscarinic,
demonstrates sustained bronchodilation and is well tolerated in patients
with reversible obstructive airways disease. Proc. Am. Thor. Soc. 3, A117
(Abstract)
33 Singh, D. et al. (2006) NVA237, a once-daily inhaled antimuscarinic,
provides 24-hour bronchodilator efficacy with comparable
bronchodilation to albuterol in patients with moderate-to-severe COPD.
Proc. Am. Thor. Soc. 3, A113 (Abstract)
34 Lu, S. et al. (2006) Anoral selective M3 anticholinergic receptorantagonist in
COPD. Eur. Respir. J. 10.1183/09031936.06.00126005 (Epub ahead of print)
286 www.drugdiscoverytoday.com
35 Boswell-Smith, V. et al. (2006) Are phosphodiesterase 4 inhibitors just
more theophylline? J. Allergy Clin. Immunol. 117, 1237–1243
36 Rabe, K.F. et al. (2005) Roflumilast – an oral anti-inflammatory treatment
for chronic obstructive pulmonary disease: a randomized controlled trial.
Lancet 366, 563–571
37 Rennard, S.I. et al. (2006) Results of a 6-month, placebo-controlled study
of a potent, selective inhibitor of phosphodiesterase 4. Chest 129,
565–566
38 Grootendorst, C. et al. (2005) Treatment with PDE4 inhibitor roflumilast
reduces sputum neutrophil and eosinophil numbers in patients with
COPD. Proc. Am. Thor. Soc. 2, A543 (Abstract)
39 Martorana, P.A. et al. (2005) Roflumilast fully prevents emphysema in
mice chronically exposed to cigarette smoke. Am. J. Respir. Crit. Care Med.
172, 848–853